역량있는 건강 애드보커시에 대한 환자와 의사의 관점 탐색(Med Educ, 2020)
Exploring patients’ and physicians’ perspectives about competent health advocacy
Kori A. LaDonna1 | Christopher J. Watling2,3 | Sayra M. Cristancho2,4 | Sarah Burm5
1 소개
1 INTRODUCTION
전 세계의 의학교육자들은 의사가 환자를 옹호해야 한다는 것을 인식하고 있습니다. 이를 인식하여 캐나다 왕립 의사 및 외과의사 대학은 수련의가 역량을 입증해야 하는 7가지 의사 역할 중 하나로 옹호를 명시적으로 지정했습니다.1 그러나 옹호 교육을 가로막는 무수한 도전 과제2-4, 즉 옹호의 의미가 무엇인지, 건강 옹호가 일상적인 진료 업무와 구별되는지에 대한 임상 교사의 불확실성5이 옹호 교육을 가로막고 있습니다, 6 임상 교사들은 옹호자로서 자신의 업무를 인식하거나 효과적인 교육으로 전환하기 위한 충분한 참조 프레임워크가 없기 때문에, 많은 프로그램에서 이 중요한 진료 측면을 위해 수련생들을 어떻게 준비시키는지 입증하는 데 어려움을 겪고 있습니다.
Medical educators around the world recognise that physicians should advocate for their patients. Recognising this, the Royal College of Physicians and Surgeons of Canada has explicitly named advocacy as one of seven physician roles for which trainees must demonstrate competence.1 Myriad challenges roadblock advocacy training2-4 however, namely clinical teachers’ uncertainty about what it means to advocate, and whether health advocacy is distinct from the everyday work of good doctoring.5, 6 Because clinician teachers do not have a sufficient frame of reference for either recognising their own work as advocates, or for translating it into effective teaching, many programmes struggle to demonstrate how they prepare trainees for this critical aspect of care.
이 과제의 핵심은 '역량 문제'7 또는 비기술적 기술에 대한 '필수 지식, 기술, 태도 및 개인적 자질'8입니다. 각 교육 단계별로 역량에 대한 기대치가 보다 명확하게 규정되어 있는 의료 전문성과 같은 다른 역량과 달리, 건강 옹호는 광범위하고 다양하게 정의되어 있어5,19 유능한 옹호에 대한 기준이 불투명합니다. 역량은 또한 '변화하는 사회적 구성'이며,7 의료 전문성을 평가하는 데 적합한 심리측정 접근법은 맥락, 문화 및 사회적 요인이 의사의 성과 전개 방식과 판단 방식에 영향을 미치는 건강 옹호와 같은 비기술적 역량을 평가하는 데는 덜 유용할 수 있습니다.20
Central to this challenge is the ‘question of competence’,7 or the ‘knowledge, skills, attitudes and personal qualities essential’8 for non-technical skills. Unlike other competencies such as medical expertise where expectations for competence are more clearly delineated for each stage of training, health advocacy is broadly and variably defined,5, 19 rendering criteria for competent advocacy opaque. Competence is also a ‘shifting social construction’,7 and the psychometric approaches appropriate for assessing medical expertise may be less useful for assessing non-technical competencies like health advocacy where context, culture and social factors influence both how a physician's performance unfolds and how it is judged.20
현재까지 건강 옹호자 역할을 명확히 하려는 시도는 주로 자문 의사와 수련의의 관점을 중심으로 이루어졌습니다.13, 16, 19, 21-26 의사들은 일반적으로 대리인과 활동가라는 두 가지 형태의 옹호에 참여한다고 보고합니다.27
- 대리인 옹호를 하는 사람들은 정보와 교육을 제공하고, 환자가 시스템을 탐색하도록 돕고, 추가 건강 관련 지원을 적시에 의뢰할 수 있도록 촉진합니다.
- 행동주의에 참여하는 사람들은 사회적 자본27을 활용하여 건강 불평등에 대한 인식을 높이고, 자원을 동원하고, 정책을 설계하고 실행합니다.
- 예를 들어, 대리인 옹호 활동에는 환자가 필요한 의약품에 대한 재정적 혜택을 받을 수 있도록 양식을 작성하는 것이 포함될 수 있습니다.
- 이와는 대조적으로 활동가 옹호에는 정부 위원회에 참여하여 의약품 보험 적용과 관련된 정책을 형성하는 것이 포함될 수 있습니다.
두 가지 유형의 옹호는 모두 환자, 지역사회 또는 집단과 공유하거나24 의사가 직접 수행할 수 있으며, 둘 다 개인 또는 시스템 수준에서 발생할 수 있습니다.28 다시 말해, 옹호는 환자의 필요에 대한 공유된 이해와 의사 결정에 대한 환자의 적극적인 참여를 전제로 하는 팀 스포츠10입니다.29
To date, attempts at clarifying the Health Advocate role have largely centred around the perspectives of consultant physicians and trainees.13, 16, 19, 21-26 Physicians report that they typically engage in two forms of advocacy: agency and activism.27
- Those doing agentic advocacy provide information and education, help patients navigate the system, and facilitate timely referrals for additional health-related support.
- Those engaging in activism use their social capital27 to raise awareness about health inequities, to mobilise resources, and to design and implement policy.
- Agentic advocacy, for example, might involve completing forms to ensure that patients can access financial coverage for a medication they require.
- Activist advocacy, in contrast, might involve joining a government committee and shaping policy related to drug coverage.
Both types of advocacy can be either shared with patients, communities or populations,24 or directed by physicians, and both can occur at either the individual or systemic level.28 In other words, advocacy is a team sport10 predicated on both a shared understanding of patients’ needs and on their active participation in decision-making.29
옹호는 공유 활동으로 개념화되지만, 건강 옹호를 정의하고 교육 및 평가를 위한 모범 사례 초안을 작성하는 연구 논의에서 환자는 대부분 소외된 것으로 보입니다. 환자의 관점이 없으면 수련생에게 환자의 필요와 목표에 맞지 않는 방식으로 옹호하도록 가르칠 위험이 있을 뿐만 아니라, 옹호를 집단적 노력이 아닌 개인적 활동으로 잘못 인식할 수도 있습니다. 옹호는 환자 중심 치료와 불가분의 관계에 있을 수 있으므로,30 우리는 건강 옹호에 대한 대화에 의사와 함께 환자를 참여시키면 보다 진정한 교육과 평가에 도움이 될 뿐만 아니라 의료 서비스에서 옹호의 역할에 대한 더 나은 이해를 얻을 수 있다고 제안합니다. 따라서 본 연구의 목적은 건강 옹호자 역할에 대한 역량의 의미에 대한 다양한 관점의 이해를 생성하여 이 작업의 출발점을 제공하는 것입니다.
Although advocacy is conceptualised as a shared activity, patients appear to have been largely sidelined in research conversations about defining health advocacy and drafting best practices for its teaching and assessment. Without their perspectives, we not only risk teaching trainees to advocate in ways that may be misaligned with patients’ needs and goals, but we may also mistakenly position advocacy as an individual, rather than a collective effort. Since advocacy may be inextricable from patient-centred care,30 we propose that engaging patients alongside physicians in conversations about health advocacy may not only inform more authentic teaching and assessment but also generate a better understanding about the role of advocacy in health care. Therefore, the purpose of our research is to provide a starting point for this work by generating a multi-perspective understanding about the meaning of competence for the Health Advocate role.
2 연구 방법
2 METHODS
우리는 구성주의적 근거 이론(CGT)31을 사용하여 선험적 이론이 아닌 환자와 의사의 관점에 근거한 유능한 건강 옹호에 대한 이론적 이해를 도출했습니다. 이를 위해 기록, 주제 및 이론적 범주 내에서 데이터를 지속적으로 비교하여 데이터 세트 전반의 패턴을 식별하고 해석을 '확인'31하는 체계적인 프로세스인 지속적 비교 방법을 사용하여 반복적인 방식으로 데이터를 수집하고 분석했습니다.
We used constructivist grounded theory (CGT)31 to generate a theoretical understanding about competent health advocacy that is grounded in patients’ and physicians’ perspective, not framed by an a priori theory. To do this, we collected and analysed data in an iterative fashion using the constant comparative method, a systematic process where we continuously compared data within and across transcripts, themes and theoretical categories to both identify patterns across the dataset and to ‘check’31 our interpretations.
2.1 데이터 수집
2.1 Data collection
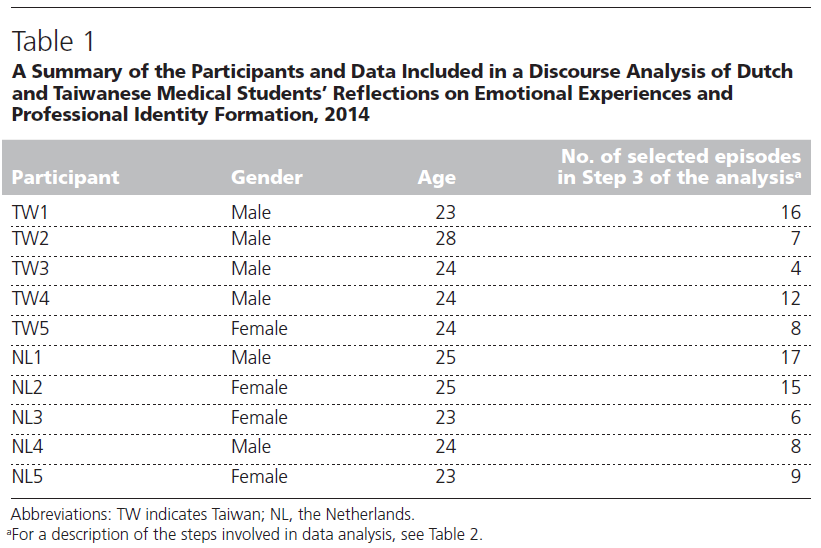
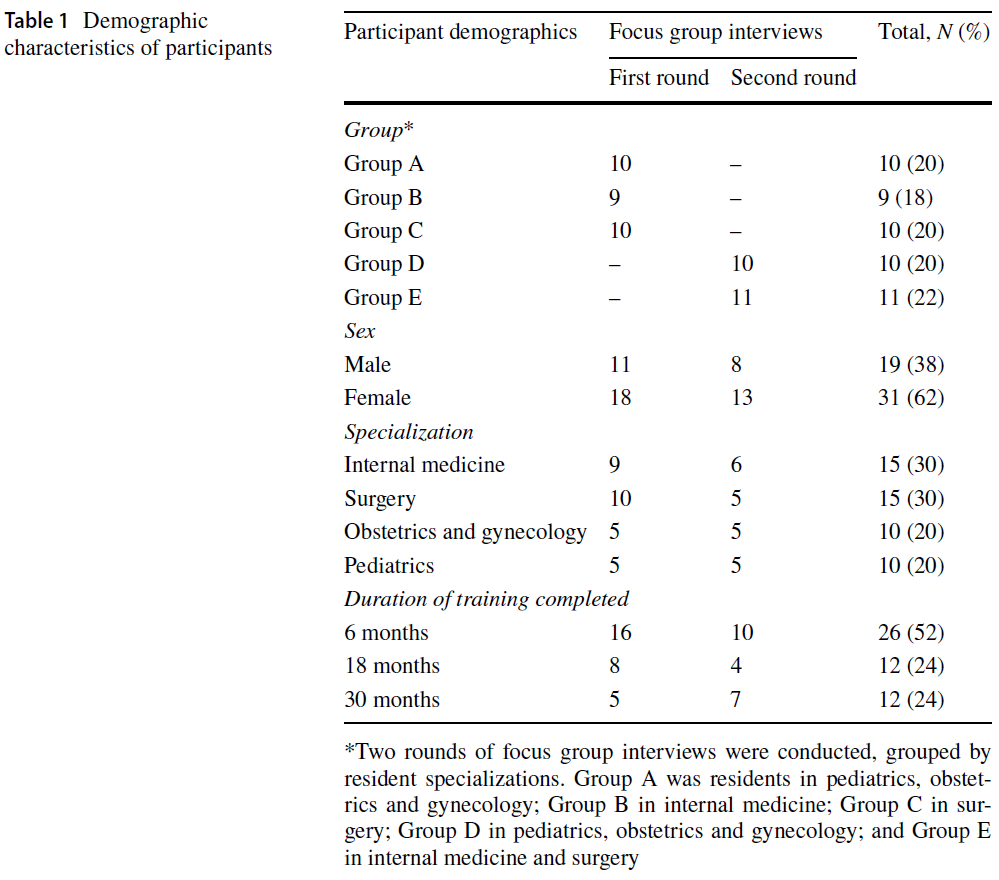
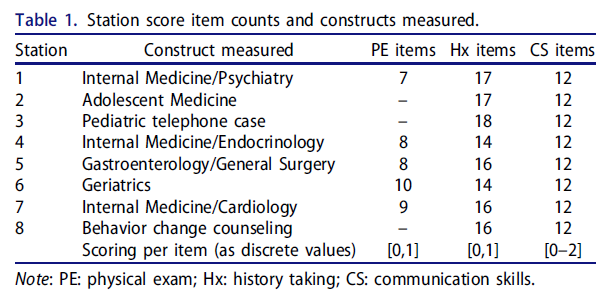
우리는 환자와 의사 모두에게 건강 옹호의 의미에 대한 관점을 공유하고, 이 역할에 대한 역량을 정의하고, 교육 및 평가에 대한 도전과 기회를 파악하도록 초대했습니다. 충분한 이해를 돕기 위해 연구 참여는 건강 옹호 교육을 받을 수 있는 환경에서 진료를 받거나 제공하는 모든 환자와 의사에게 개방되었습니다. 캐나다의 한 중형 의과대학과 가장 규모가 큰 부속 병원 3곳에 모집 자료를 게시하고 해당 기관에서 근무하는 모든 교수진 의사에게 이메일 초대장을 보냈습니다. 채용 포스터를 보고 두 명의 레지던트가 관심을 표명했지만, 주로 HA 교육을 담당하고 있는 교수진 모집에 집중했습니다. 개인이 옹호자라고 밝히지 않아도 참여할 수 있었지만, 저희는 표본에 다양한 옹호 경험이 포함되도록 하는 것을 목표로 했습니다. 이를 위해 환자 옹호 단체의 도움을 받아 이러한 단체에 종사하는 환자와 의사를 모집했습니다. 24명(환자 10명, 교수진 12명, 레지던트 2명)이 참여에 동의했습니다(표 1).
We invited both patients and physicians to share their perspectives about what health advocacy means, to define competence for this role, and to identify challenges and opportunities for its teaching and assessment. To generate a fulsome understanding, study participation was open to all patients and physicians obtaining or providing care in settings where HA training presumably occurs. We posted recruitment materials at a medium-sized Canadian medical school and three of its largest affiliated hospitals, and we sent email invitations to all faculty physicians working at these institutions. Of note, while two residents expressed interest after seeing our recruitment poster, we focused on recruiting faculty because they are primarily responsible for training HA. Although individuals did not need to identify as advocates in order to participate, we aimed to ensure that our sample contained a breadth of advocacy experiences. To do this, we enlisted the help of patient advocacy groups to recruit patients and physicians engaged with these organisations. Twenty-four participants (n = 10 patients, n = 12 faculty physicians, n = 2 residents) consented to participate (Table 1).

반구조화된 인터뷰와 사진 도출32(참가자가 직접 촬영한 사진을 사용하여 개인의 관점을 이끌어냄으로써 데이터의 풍부함을 높이는 시각적 연구 방법)을 결합하여 두 차례의 연구 방문을 통해 데이터를 수집했습니다.
- 첫 번째 연구 방문은 카메라 오리엔테이션 세션으로, SB는 참가자들에게 연구 목적을 설명하고 건강 옹호의 의미에 대한 짧은 인터뷰를 진행하며 사진 촬영의 윤리에 대해 논의했습니다.33
- 그런 다음 SB는 참가자들에게 3~6주 동안 옹호에 대한 이해를 나타내는 사진을 찍도록 초대했습니다.
- 참가자들은 두 번째 인터뷰를 위해 다시 돌아왔고, SB는 각 사진에 대해 설명하고 옹호자에게 필요한 기술에 대해 토론하고 유능한 옹호자가 된다는 것이 무엇을 의미하는지에 대한 인식을 공유하도록 요청했습니다.
We collected data during two research visits using a combination of semi-structured interviews and photo elicitation32—a visual research method that enhances data richness by using participant-generated photographs to elicit individual perspectives.
- The first research visit was a camera orientation session, where SB described for participants the purpose of the study, engaged participants in a short interview about the meaning of health advocacy, and discussed the ethics of picture taking.33
- SB then invited participants to take pictures over a 3-6 week period that represented their understanding about advocacy.
- Participants returned for a second interview where SB asked them to describe each of their photographs, discuss the skills that advocates require, and share their perceptions about what it means to be a competent advocate.
2.2 데이터 분석
2.2 Data analysis
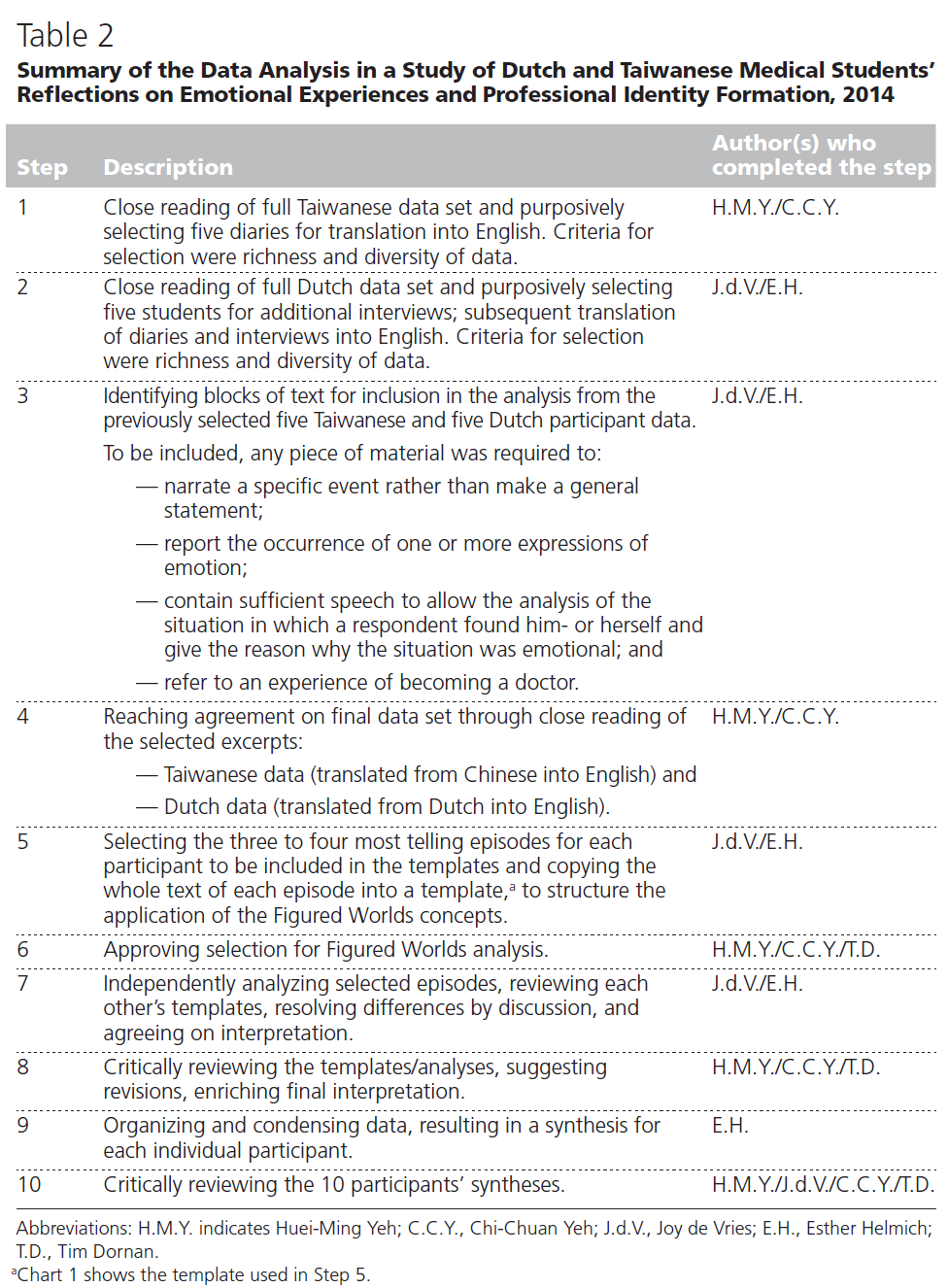
모든 인터뷰는 오디오 녹음하고 그대로 전사한 후 점진적으로 해석하는 초기, 초점, 이론 코딩의 세 단계를 거쳐 분석했습니다.31 초기 코딩에서는 각 참가자 그룹의 처음 두 녹취록을 한 줄씩 읽고 동명사('-ing'으로 끝나는 행동어) 또는 참가자 단어(생체 코드)를 사용하여 SB와 KL이 코딩하여 참가자들이 설명하는 의미와 행동을 포착했습니다. 그런 다음 가장 자주 발생하거나 설득력 있는 초기 코드를 잠정 코딩 체계로 통합하여 다음 3~4개의 트랜스크립트를 초점 코딩하여 관련성을 시험했습니다. 전체 연구팀은 정기적으로 만나 예비 조사 결과를 논의하고, 초점 코딩한 코드를 이론적 범주로 구체화한 다음 병합했습니다. 이러한 분석 단계를 완료한 후, 환자의 관점이 옹호에 대한 의사의 이해에 어떤 영향을 미치는지 이해하는 것뿐만 아니라 유능한 건강 옹호자가 되기 위해 학습자를 교육하는 데 따르는 과제를 더 풀어야 할 필요성을 확인했습니다. 1차 데이터 수집에 참여한 4명의 의사 참가자는 이러한 아이디어를 이론적으로 샘플링하기 위해 결과 회신 인터뷰에 참여하는 데 동의했습니다.
All interviews were audio-recorded, transcribed verbatim, and analysed during three progressively interpretive stages of initial, focused and theoretical coding.31 During initial coding, the first two transcripts from each participant group were read line-by-line and coded by SB and KL using gerunds (action words ending in ‘-ing’) or participants’ words (in vivo codes) to capture the meanings and actions described by participants. The most frequently occurring or compelling initial codes were then consolidated into a provisional coding scheme used to do focused coding of the next 3-4 transcripts to trial their relevance. The entire research team met regularly to both discuss preliminary findings, refine and then merge focused codes into theoretical categories. Once we completed these analytical stages, we identified the need to understand not only how patients’ perspectives impacted physicians’ understanding about advocacy, but also to further unpack the challenges of training learners to become competent health advocates. Four physician participants from the first round of data collection agreed to participate in return of findings interviews to theoretically sample these ideas.
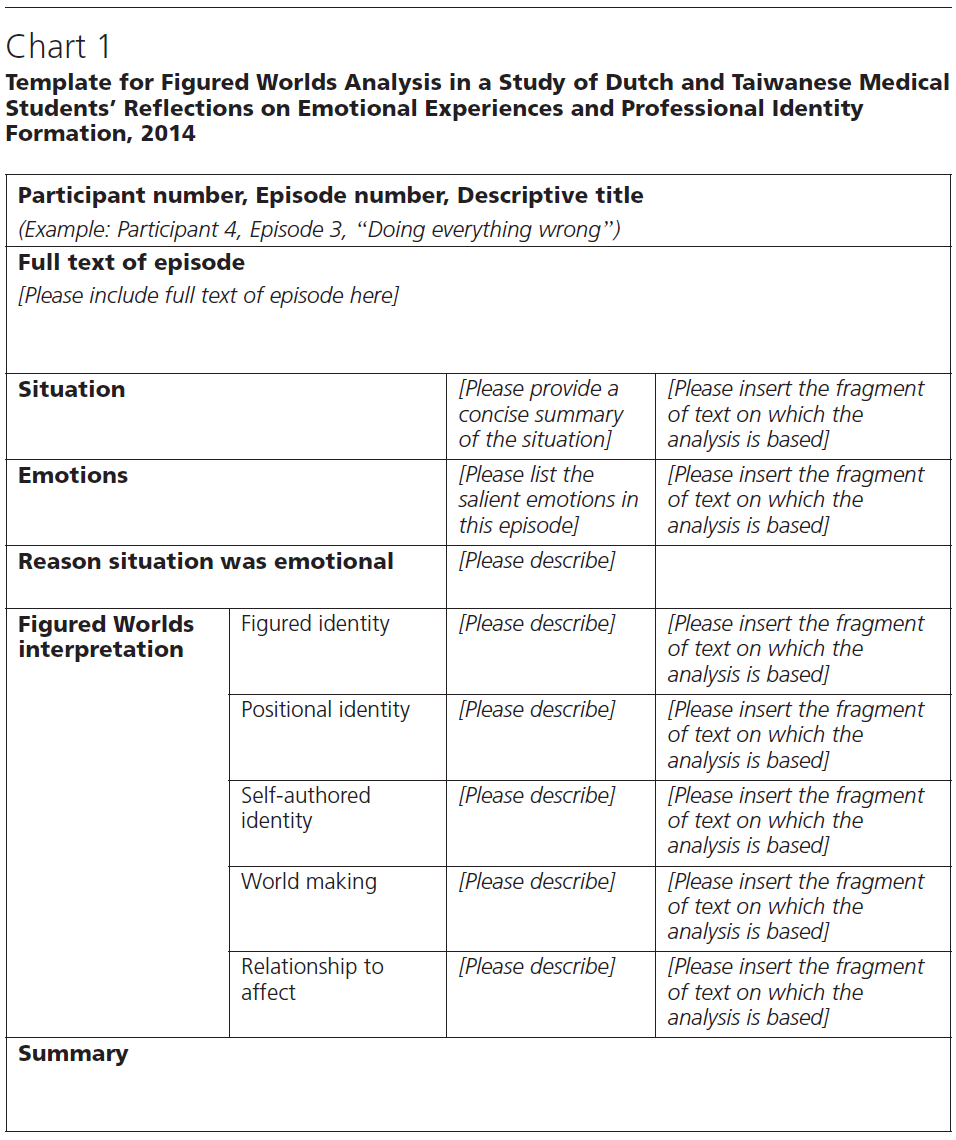
SB는 이러한 이론적 범주를 사용하여 전체 데이터 집합을 코딩했습니다. 다음으로, 우리 팀은 범주 패턴을 조사하기 위해 다이어그램과 메모 초안을 작성하고, 범주를 서로 연결하여 유능한 HA에 대한 이론적 아이디어의 기초가 되는 추상적이고 분석적인 스토리라인을 구성했습니다. 이미지를 미학적으로 분석하지는 않았지만34 인터뷰 중에 공유한 사진에 대한 참가자들의 설명은 이론적 이해에 도움이 되었으며, 건강 옹호 및 유능한 HA 역할에 대한 이전의 개념에 도전하는 새로운 통찰력을 제공했습니다.1, 19 건강 옹호에 대한 참가자들의 관점을 설명하기 위해 몇 장의 사진을 포함했지만, 참가자들이 사진 유도 방법을 사용하여 건강 옹호에 대한 이해를 전달하는 방법에 대한 별도의 심층 분석은 다른 곳에서 보고될 예정입니다(원고 준비 중).
SB used these theoretical categories to code the entire dataset. Next, our team drafted diagrams and memos to examine categorical patterns, linking categories together to form abstract, analytical storylines foundational to our theoretical ideas about competent HA. While we did not aesthetically analyse34 the images, participants’ descriptions of their photographs shared during interviews were instrumental to our theoretical understanding, providing new insights that challenged previous conceptualisations about both health advocacy and competence for the HA role.1, 19 While we've included a few photographs to illustrate participants’ perspectives about health advocacy, a separate, in-depth analysis of how participants used the photo elicitation method to convey understanding about health advocacy will be reported elsewhere (manuscript in preparation).
우리는 이론적 충분성에 도달했다고 판단할 때까지, 즉 우리의 데이터가 탐색적 연구 질문에 대한 풍부한 이론적 통찰력을 제공하기에 적절한 개념적 깊이를 가지고 있다고 판단할 때까지 데이터를 수집했습니다.35 글쓰기는 CGT 분석 과정의 필수 요소이므로 본 원고를 완성할 때까지 이론화를 계속했습니다.31 웨스턴 대학교 연구윤리위원회는 모든 연구 절차를 승인했습니다.
We collected data until we determined that we had reached theoretical sufficiency, or the point at which we determined that our data had appropriate conceptual depth for providing rich, theoretical insights about our exploratory research questions.35 Since writing is an integral component of the CGT analytical process, theorising continued until we completed the present manuscript.31 The Western University Research Ethics Board approved all research procedures.
2.3 반사성
2.3 Reflexivity
구성주의자로서 우리는 각 팀원의 경험, 관심사, 신념이 연구 과정에 영향을 미친다는 것을 잘 알고 있습니다. 우리 팀은 질적 연구(KL, SB, SC, CW) 및 시각적 방법(KL, SB, SC)에 대한 전문성을 갖춘 박사 학위 소지 의학교육 연구자들로 구성되어 있습니다. KL은 비영리 환자 옹호 단체에서 일한 경험에서 비롯된 건강 옹호에 대한 관심을 바탕으로 환자의 전문 지식이 의료 교육에 어떻게 의미 있는 정보를 제공할 수 있는지 탐구합니다. CW는 임상의 교육자이자 전직 대학원 학장으로서 여러 분야의 의사를 교육하고 평가하는 실질적인 과제에 몰두하고 있는 의사입니다. SC는 전문 임상의가 복잡성을 이해하고 탐색하는 방법을 연구하며, SB는 질적 방법론을 사용하여 개인의 소외 경험에 대한 심리사회적, 정서적, 학문적 영향을 더 잘 이해하는 숙련된 교육자입니다.
As constructivists, we are cognisant that each team member's experiences, interests and beliefs influence the research process. Our team consists of PhD trained medical education researchers with expertise in qualitative research (KL, SB, SC and CW) and visual methods (KL, SB and SC). One stream of KL’s research explores how patients’ expertise may meaningfully inform medical training; her interest in health advocacy stems from her experiences working with non-profit patient advocacy groups. CW is a physician who, as both a clinician educator and a former postgraduate dean, is immersed in the practical challenges of training and assessing physicians across disciplines. SC studies how expert clinicians make sense of and navigate complexity, and SB is a trained educator who uses qualitative methodologies to better understand the psychosocial, emotional and academic impact on individuals’ lived experiences of marginalisation.
3 결과
3 RESULTS
환자와 의사 참여자 모두 유능하게 옹호 활동에 참여하는 것은 의료 및 시스템 전문성, 학습 및 실습 환경, 경험, 지위, 정치적 지식 등 개인적 및 직업적 특성의 조합에 달려 있는 것으로 나타났습니다. 환자 참가자들은 정기적으로 옹호 활동에 참여한다고 답한 반면, 의사 참가자들 중 자신이 의미 있는 활동을 하거나 유능한 건강 옹호자라고 인식하는 사람은 거의 없었습니다.
- 결과적으로 의사들은 자신의 역량뿐만 아니라 프로그램 내에서 옹호 교육에 영향을 미치는 요인에 대한 인식이 낮아 학습자의 건강 옹호를 교육하거나 공정하게 평가할 수 있는지에 대한 의문을 제기했습니다.
- PGME 역량 프레임워크와 학습 환경에 익숙하지 않은 환자들은 학습자의 역량에 대한 공식적인 평가에 대해 언급하는 데 한계가 있었지만, 환자들은 개인적인 경험을 바탕으로 훌륭한 의사 옹호자의 속성을 표현하고 그들의 수행능력에 대한 피드백을 생성했습니다.
이러한 각 결과에 대해 예시적인 인용문을 사용하여 자세히 설명하겠습니다. 인용문은 참가자 유형, 수, 인용문이 도출된 인터뷰에 따라 식별됩니다. 예를 들어, 첫 번째 인터뷰에 참여한 환자 6과 결과 회신 인터뷰에 참여한 의사 7의 인용문은 각각 P6, I1, MD7, I3으로 표시되어 있습니다.
For both patients and physician participants, competently engaging in advocacy seemed to hinge on a combination of medical and systems expertise, a conducive learning and practice environment, and personal and professional characteristics including experience, status and political savvy. While patient participants described regularly engaging in advocacy, few physician participants perceived that they were either meaningfully engaged or competent health advocates.
- In turn, physicians’ perceptions about not only their own competence but also the forces that impact advocacy training within their programmes raised questions about whether it was possible to train or to fairly assess learners’ health advocacy.
- Although patients’ unfamiliarity with PGME competency frameworks and learning environments limited their ability to comment on formal assessments of learners’ competence, patients drew on their personal experiences to both articulate the attributes of good physician advocates, and to generate feedback about their performance.
We will expand on each of these findings using illustrative quotes. Quotes are identified by participant type, number and the interview from which the quote derived. For instance, a quote attributed to patient 6 during their first interview, and physician 7 in their return of findings interview, are labelled P6, I1 and MD7, I3, respectively.
3.1 유능한 건강 옹호의 구성 요소
3.1 Components of competent health advocacy
환자와 의사 참여자들은 유능한 건강 옹호의 의미에 대해 때때로 다른 관점을 가지고 있었지만, 두 사람 모두에게 건강 옹호는 일반적으로 '나 자신을 위해 일어서는 것'(P1, I1)과 '현상 유지에 만족하지 않고 개인과 지역사회 및 시스템 수준에서 사람들의 건강과 웰빙을 결정하는 요소를 지속적으로 개선하기 위해 노력하는 것'(MD10, I1)을 의미했습니다. 건강 옹호는 종종 더 잘 작동하는 시스템에서는 불필요한 체계적 또는 구조적 문제에 대한 반응 또는 이에 대한 방어로 개념화되었기 때문에 환자와 의사 참여자 모두 옹호자에게는 일련의 기술이 필요하다는 것을 인식했습니다. 특히, 옹호자는 의료 및 제도 관련 지식과 '환자의 이야기를 파는 것'(MD12, I1)하여 '가능한 한 빨리 상대방에게 내 환자의 진료가 필요하다는 것을 설득'(MD13, I1)할 수 있는 자신감, 단호함, 정치적 감각을 모두 갖추고 있어야 하는 것으로 나타났습니다.
While patient and physician participants sometimes had different perspectives about the meaning of competent HA, for both, advocacy generally meant having to ‘stand up for myself’ (P1, I1) and ‘pushing things forward - not being satisfied with the status quo and really looking at continuously improving at the individual and at the community and system level the factors that determine people's health and well-being’ (MD10, I1). Because health advocacy was often conceptualised as a reaction to, or a defence against, systemic or structural problems that would be unnecessary in a better functioning system, both patient and physician participants recognised that advocates require a constellation of skills. Specifically, advocacy seemed to rely on possessing both medical and systems-related knowledge, and the confidence, assertiveness and political savvy to ‘sell your patient's story’ (MD12, I1) in a way that ‘convinces the other person, as quickly as possible, that your patient needs to be seen’ (MD13, I1).
의사의 대인관계 및 의사소통 능력은 환자에게도 중요했으며, 환자에게 유능한 옹호는 환자 중심주의와 동의어처럼 보였습니다. 즉, 환자 중심의 의사 옹호자는 환자가 치료에 적극적으로 참여하도록 장려하고 의료 시스템의 격차나 한계를 완화하기 위해 다른 사람들과 기꺼이 협력하는 의사였습니다. 또한 '옹호의 큰 부분은 환자와 공감할 수 있는 것'(P7, I2)이기 때문에 환자 참여자들은 의사가 먼저 좋은 경청자가 되지 않으면 효과적으로 옹호할 수 없다고 생각했으며, '환자에게 진정으로 경청하는 의료진과 경청하는 것처럼 행동하는 의료진 사이에는 뚜렷한 차이가 있다'(P4, I1)고 인식했습니다. 참가자들은 이러한 세심한 경청을 드문 일로 인식했기 때문에 일반적으로 불만족스러운 의료 서비스 경험에 대한 이야기를 공유함으로써 좋은 옹호 또는 효과적인 옹호에 대한 인식의 틀을 잡았습니다:
A physician's interpersonal and communication skills also mattered to patients, and for them, competent advocacy seemed synonymous with patient centredness. That is, a patient-centred physician advocate was one who encouraged patients to take an active role in their care and who willingly worked with others to mitigate gaps or limitations in the healthcare system. Additionally, since ‘a big part of advocacy is being able to empathize with a patient’ (P7, I2), patient participants felt that physicians could not advocate effectively without first being good listeners, and they discerned ‘a palpable difference for patients between providers who really listen and those who behave as though they are listening’ (P4, I1). Participants perceived such attentive listening as rare, thus they commonly framed their perceptions of good, or effective, advocacy by sharing stories of unsatisfactory health care encounters:
내가 의사에게 불만족스러울 때는 의사의 태도 때문입니다. 제가 사건의 연대기를 설명할 때 계속 헷갈려하고 제 말에 귀를 기울이지 않는 의사가 있었어요. 제게는 나쁜 의사였어요... 제 말을 한 마디도 듣지 않고 그냥 처방전만 써주고 나가 버렸어요... 그 사람들은 좋은 옹호자가 아니었어요. (P8, I1)
When I’m dissatisfied with a physician, it's because of their attitude. I had one that, I was explaining the chronology of events…They kept on getting it confused, they weren't paying attention to me. That, to me, is a bad physician… didn't listen to a word I said, and just wrote me a prescription, and walked out…those people were not good advocates. (P8, I1)
실제로 자원이 부족한 치료 시스템의 내재적 한계는 환자가 스스로를 옹호하는 것뿐만 아니라, 종종 위협적인 것으로 인식되는 의료 시스템을 탐색하는 데 도움을 줄 수 있는 옹호자 집단을 개발하는 것의 중요성을 강조했습니다:
Indeed, the inherent limitations of a resource-strapped care system reinforced the importance for patients to not only advocate for themselves, but also to develop a circle of advocates who could help them navigate a health care system often perceived as threatening:
먼저 자신을 보호해야 합니다. 필요한 치료를 받고 가능한 한 빨리 병원을 빠져나가야 합니다. 안타깝게도 병원은 너무 바쁘고 혼잡합니다. 항상 누군가와 함께 있지 않으면 그 틈새를 비집고 들어갈 수 있습니다. (P3, I1)
You have to protect yourself first. Make sure that you get what you're going to need and get the hell out of there as fast as you can. Unfortunately, our hospitals are too busy and too over-crowded. If you don't have somebody there with you all the time, you'll drop through the cracks. (P3, I1)
3.2 유능한 건강 옹호 평가하기
3.2 Assessing competent health advocacy
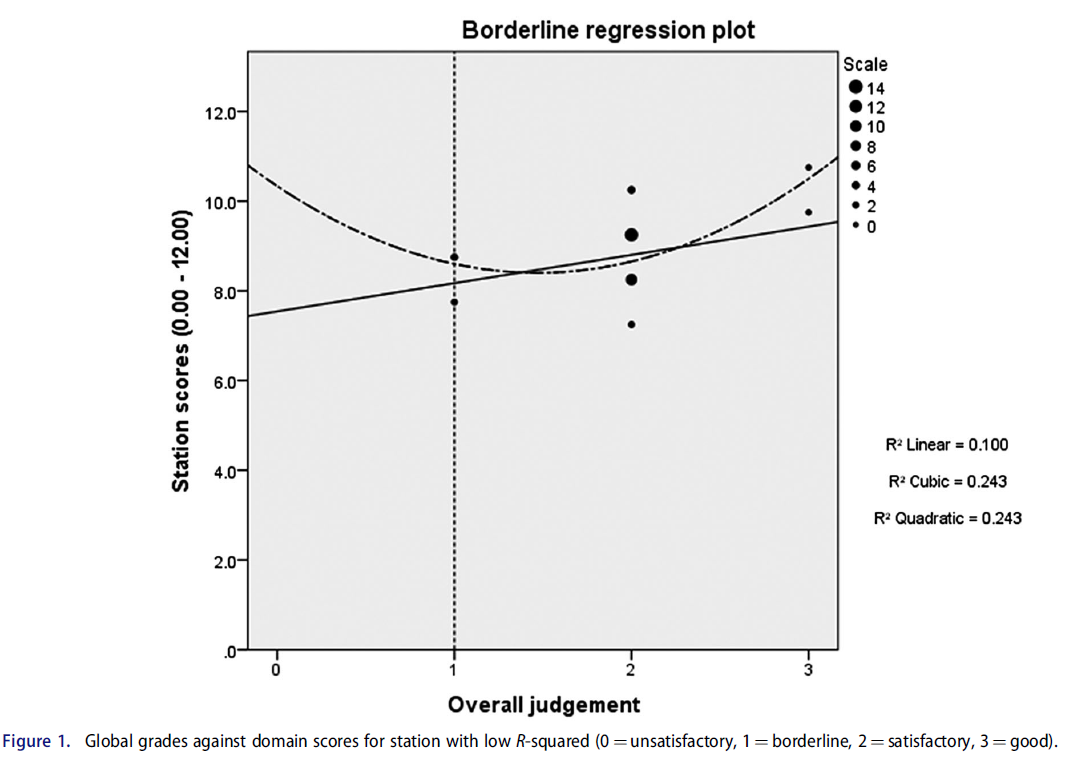
환자들은 훌륭한 의사 옹호자의 특징에 주의를 기울일 뿐만 아니라 그에 대한 피드백을 작성할 준비가 되어 있는 것처럼 보였습니다. 예를 들어, 한 환자는 자신의 상태에 대해 수행한 연구를 공유하여 자신을 옹호한 후 의사로부터 받은 두 가지 대조적인 반응에 대한 예를 공유했습니다(그림 1). 한 의사는 환자의 연구를 완전히 무시한 반면, 다른 의사는 치료 계획을 수립하면서 환자의 연구를 고려했습니다. 의사에게 어떤 피드백을 제공할 수 있느냐는 질문에 환자 참여자 4는 효과적인 옹호를 위해서는 경청하는 것이 기본이라고 반복해서 답했습니다:
Patients not only seemed attentive to the characteristics of good physician advocates, but they also seemed poised to craft feedback about them. For instance, one patient shared an example of two contrasting responses from her physicians after she'd advocated for herself by sharing research she'd conducted about her condition (Figure 1). One dismissed her research outright, while another considered the patient's research while developing a treatment plan. When asked what feedback she might provide to her physicians, patient participant 4 responded by reiterating that listening is fundamental for effective advocacy:
제 말을 잘 들어준다고 생각했던 한 의사에게는 사려 깊은 태도에 깊은 감명을 받았습니다... 저는 '제 말을 잘 들어주고, 제가 치료에 참여할 수 있는 방식에 대한 선택이 어떤 영향을 미칠지 생각해줘서 고맙다'고 말했을 것입니다. 그리고 다른 한 명에게는 '시간을 내어 환자를 단지 많은 인구의 일원이 아니라 미묘한 차이를 가진 개인으로 생각해야 할 필요성을 이해해 주셨으면 좋겠습니다'라고 말했을 것입니다. (P4, I1)
For the one physician who I thought was really listening to me, I was just really impressed with her thoughtfulness…I would have said, ‘thank you for really making me feel like you are listening to me and thinking about the implications of the choices that we make for the way that I think about my ability to participate in my own care.’ And then, for the other, I would have said, ‘I hope you understand the need to take the time and really think about your patients as individuals with subtle differences, rather than just members of a larger population.’ (P4, I1)

환자 참가자들은 유능한 옹호자의 속성으로 인식하는 것을 쉽게 식별할 수 있는 것처럼 보였지만, 의사 참가자들은 옹호를 '약간 추상적인 것'(MD2, I2)이라고 설명했으며, 이 핵심 역량의 본질을 명확하게 표현하는 것이 어렵다고 생각했습니다:
While patient participants seemed readily able to identify what they perceived as attributes of competent advocates, physician participants described advocacy as ‘a bit of an abstract thing’ (MD2, I2), and found it challenging to articulate the essence of this core competence:
'신경외과 전문의 자격증을 취득했다면 환자를 돌보기 위해 입증해야 하는 의학적 지식과 기술에 능숙하다는 것을 의미한다'고 말하는 것은 비교적 간단하지만, 이것이 건강 옹호에 정확히 무엇을 의미할까요? 어느 시점에서 이 사람이 더 이상 환자의 건강 옹호자로서의 책임을 다하지 못하고 있다고 말하겠습니까? (MD13, I1)
It's relatively straightforward to say ‘if you are certified to be a neurosurgeon, this is what it means for you to be competent in the medical knowledge and skill that you have to demonstrate to take care of your patients’ … what exactly does that mean for health advocacy? At what point would you say that this person is no longer fulfilling their responsibilities as a health advocate for their patient? (MD13, I1)
이러한 질문과 씨름한 후, 의사 참가자들은 충분히 좋은 옹호자부터 효과적인 옹호자, 탁월한 옹호자에 이르기까지 다양한 역량을 제시했습니다. 의사 참가자에 따르면,
- 충분히 유능한 옹호자는 건강 옹호에 대한 개념적 이해가 있고, '환자와 환자의 상태, 치료에 대한 매우 강력한 지식'(MD12, I1)을 바탕으로 행동할 기회를 식별할 수 있으며, 자원에 접근하는 방법을 알고 있습니다. 그러나 참가자들은 이러한 개념적 이해만으로는 충분 기준을 충족하기에 충분하지 않다고 지적했습니다.
- 오히려 최소 기준을 충족하기 위해서는 옹호 활동이 결과를 창출할 만큼 효과적인지 여부와 관계없이 옹호 관련 활동에 기꺼이 참여하려는 의지에 의존해야 했습니다. MD11은 '옹호 활동은 결과를 얻는다는 의미가 아니라 옹호한다는 의미이며...[따라서] 노력하는 것만으로도 훌륭한 옹호자가 될 수 있다'고 말함으로써 이러한 개념을 명확히 했습니다(MD11, I3).
- 스펙트럼의 맨 끝에는 '지속적으로 한계를 뛰어넘어 결과를 얻는'(MD11, I3) 드문 예외적인 옹호자가 있습니다.
- 환자와 의사 참가자 모두 의사가 옹호 활동을 하거나 하지 않는다고 인식했지만, 의사 참가자의 경우 옹호 활동을 시도하는 것만으로도 충분히 좋은 것으로 인식했습니다.
After wrestling with such questions, physician participants seemed to suggest a spectrum of competence ranging from good enough to effective to exceptional advocacy. According to physician participants,
- good enough advocates have a conceptual understanding about health advocacy, are able to identify opportunities to act based on ‘a very strong knowledge of the patient, and their conditions, and their treatment…’ (MD12, I1), and know how to access resources. Participants noted that having this conceptual understanding was insufficient for meeting the good enough threshold, however.
- Rather, meeting the minimum bar relied on a willingness to engage in advocacy-related activities—regardless of whether their advocacy efforts were effective enough to generate results. MD11 clarified this notion by saying: ‘advocacy doesn't imply you get a result, it just means that you advocate…[therefore] you can still be a good advocate by just trying’ (MD11, I3).
- At the far end of the spectrum are the rare exceptional advocates who consistently ‘go to bat and push the envelope…and get results’ (MD11, I3).
- Both patient and physician participants perceived that doctors either did or did not advocate; for physician participants, however, any attempt at advocacy was perceived as good enough.
3.3 역량에 영향을 미치는 요인: 경험과 환경
3.3 Forces that impact competence: Experience and environment
환자와 의사 참가자 모두 교육생이 효과적으로 옹호 활동에 참여하는 데 방해가 될 수 있는 여러 가지 요인에 대해 설명하면서, 교육생이 최소한의 역량 기준을 충족하기를 기대하는 것이 가능한지 또는 합당한지에 대한 의문을 제기했습니다. 예를 들어, 의사 참가자들은 유능한 건강 옹호자가 되는 것은 경험에 의존하며, 옹호 활동은 수련생이 '성장'해야 할 일이라고 인식한다고 설명했습니다(MD5, I1). 따라서 수련생이 옹호 활동을 하기 위해서는 먼저 어느 정도의 '의학적 전문성을 개발해야 하며...그 다음에는 학습과 경험을 통해 건강 옹호 활동을 할 수 있다'고 의사 참가자들은 설명했습니다(MD14, I1). 따라서 옹호는 '조미료와 함께 제공된다'(MD3, I2). 그리고 '옹호자가 되려면 시간이 걸리기 때문에 무엇이 정상이고 무엇이 비정상인지 알 수 있을 만큼 충분히 오래 주변에 있어야 한다'(MD3, I2). 경력이 오래된 의사 참가자들도 '어떻게 해야 하는지 더 똑똑해졌지만'(MD11, I1), '옹호하는 방법을 더 잘 배우기 위해 끊임없이 노력하고 있다'(MD3, I1)고 설명했습니다.
Both patient and physician participants described multiple forces that may impede trainees’ ability to effectively engage in advocacy, raising questions about whether it is possible—or perhaps even fair—to expect trainees to meet the minimum threshold for competence. For instance, physician participants described that becoming a competent health advocate relies on experience, perceiving that advocacy was something for trainees to ‘grow into’ (MD5, I1). Consequently, for trainees to be able to advocate, physician participants described that they first had to develop a certain degree of ‘medical expertise…And then the health advocacy comes with learning and experience’ (MD14, I1). Advocacy, therefore, ‘comes with seasoning’ (MD3, I2). And because ‘it takes a while to become an advocate you have to be around long enough to know what is normal and what's not’ (MD3, I2). Even physician participants at advanced stages in their career described that while they've ‘gotten smarter at how to do things’ (MD11, I1), they were ‘constantly learning how to advocate’ better (MD3, I1).
환자 참가자들은 효과적인 옹호 활동의 또 다른 장애물로 의사가 일상적인 질환illness 경험에 대해 충분히 이해하지 못한다는 점을 꼽았습니다. 이들은 이러한 정보가 옹호 활동에 참여하는 데 매우 중요하다고 인식했습니다. 의사 참여자들도 이에 동의하며 레지던트 교육이 수련의가 의료 제공의 '큰 그림'(MD4, I2)에서 옹호가 어디에 적합한지 파악하거나 건강 옹호 업무를 수행할 수 있는 기술을 개발할 기회를 제한적으로 제공한다고 설명했습니다. '레지던트는 양식 작성이나 장애와 같은 일에 관여하지 않습니다 .... 당신이 하는 일의 대부분은 병원에서 이루어지며 환자가 겪는 삶의 경제적 현실로부터 약간 차단됩니다'(MD6, I1).
Patient participants identified another impediment to effective advocacy: physicians’ lack of sufficient understanding of their everyday illness experiences. They perceived this information as critical for engaging in advocacy. Physician participants seemed to agree, and described that residency training provided limited opportunities for trainees to begin to develop the skills to either see where advocacy fits into the ‘big picture’ (MD4, I2) of care provision or to do the work of health advocacy: ‘as a resident, you really don't get involved in the filling out of forms and disability things and that kind of stuff …. a lot of the work that you do is in hospital and you're a bit shielded from the economic realities of life that your patient has’ (MD6, I1).
광범위한 의료 환경 또한 개별 의사가 옹호 활동에 참여하기 어렵게 만드는 것으로 인식되었습니다. 한 환자 참여자는 '훌륭한 옹호자가 되지 못하는 것은 의사 개개인이 아니라 그들이 근무하는 시설에서 옹호 활동이 부족하다고 생각합니다."(P8, I1)라고 제안했습니다. 또한 의사들은 '건강 옹호자가 되도록 훈련받지 않았고'(MD7, I3), '옹호활동이 필요한 만큼 중요하게 여겨지지 않기 때문에'(MD9, I2), 의사 참여자들은 건강 옹호 커리큘럼에 엄격함과 전략적 방향이 모두 부족하여 수련생들이 불이익을 받는다고 우려했습니다.
The broader health care environment was also perceived as making advocacy work challenging for individual physicians to engage in. As one patient participant suggested: ‘It's not so much the individual doctors that aren't good advocates, it's the facilities at which they work, where the advocacy, I think, lacks.’ (P8, I1). Additionally, because physicians are ‘not trained to be health advocates’ (MD7, I3) and because ‘advocacy is not valued as much as it should be’ (MD9, I2), physician participants worried that trainees were disadvantaged because health advocacy curricula lacked both rigor and a strategic direction.
3.4 역량에 영향을 미치는 요인: 권력과 지위
3.4 Forces that impact competence: Power and status
관료주의로 가득 찬 고장난 시스템에서 옹호 활동을 하려면 때때로 의사들은 윤리적으로 문제가 될 수 있는 방식으로 사회적 자본을 사용해야 했습니다. 예를 들어, 한 의사 참가자는 환자를 위한 자원이나 치료를 얻기 위해 규칙과 규정을 우회하여 '합리적인 도둑'이 되어야 하는 경우가 많다는 것을 배웠다고 회상했습니다:
Advocating in a broken system laden with red tape sometimes required physicians to wield their social capital in ways that could be ethically fraught. For instance, one physician participant recalled learning that a good advocate often had to be a ‘reasonable thief’ by circumventing rules and regulations to obtain resources or treatments for their patients:
저는 레지던트 시절, 진단에 관해 저와 이야기를 나누던 교수진과 함께 일했던 아주 분명한 경험을 기억합니다. 그리고 그들은 '어떤 사람들은 제 의견에 동의하지 않을 수도 있지만, 저는 제가 내릴 수 있는 진단이 어린이에게 치료를 받을 수 있는 문을 열어준다면, 저는 어린이가 필요한 임상 치료를 받을 수 있도록 옹호하는 것이기 때문에 후회 없이 그 진단을 서류에 적을 것'이라고 말했습니다. (MD9, I3)
I remember a very clear experience of being a resident, working with a faculty who was talking to me about diagnosis. And they said, ‘some people may disagree with me, but I am of a strong opinion that if a diagnosis that I have the power to give will open doors to access treatment for a child, that I will put that down on paper without any regrets, because I’m advocating for a child to get the clinical treatment that they need.’ (MD9, I3)
이러한 방식으로 옹호하는 경우 '레지던트가 곤경에 처할 위험'(MD9, I3)이 있을 수 있기 때문에, 대부분의 의사 참여자들은 경험과 함께 옹호에는 어느 정도의 권한과 특권이 필요하다는 데 동의했습니다. 결과적으로, 주치의는 특히 '공식적으로 인정받는 지위'(MD10, I2)를 가진 경우 연공서열과 지위 때문에 효과적이거나 예외적인 방식으로 더 잘 개입할 수 있다고 인식했습니다. 효과적인 옹호를 위한 지위의 중요성에 대해 MD10은 다음과 같이 말했습니다:
Since there may be ‘a danger of the resident getting in trouble’ (MD9, I3) for advocating in this way, most physician participants agreed that, along with experience, advocacy required a certain degree of power and privilege. Consequently, attending physicians were perceived to be better able to engage in effective or exceptional ways because of their seniority and status, particularly if they held ‘some sort of formally recognized position’ (MD10, I2). When reflecting on the importance of status for effective advocacy, MD10 said:
의학은 일반적으로 매우 위계적입니다... 저는 수련의였고, 펠로우였고, 누군가의 밑에 있었습니다. ...제 시스템도 아니고 제 환자도 아닙니다. 제 상사의 것이죠, 그렇죠? 졸업하고 교수로 임용된 후에야 비로소 이 시스템이 내 시스템이고, 내가 그 시스템의 일부이며, 변화를 원한다면 내가 그 변화의 일부가 되어야 하고, 그렇게 할 수 있는 권한과 특권이 있다는 것을 깨달았죠.
Medicine typically is just so hierarchal… I was a trainee, I was a fellow, I was under somebody. …it's not really my system or it's not my patients. It's my supervisor's, right? And it was only until I graduated and was on faculty, that I realized, no, now this is my system, I’m part of the system, and if I want to see it change, I have to be part of that change, and I now have the power and privilege to do that.
권력과 지위가 옹호를 촉진하는 데 도움이 되는 것으로 널리 알려져 있지만, 일부 참가자는 권력과 지위가 필수적이라는 생각에 이의를 제기하는 사례를 제시했습니다:
While power and status were widely seen as helpful facilitators of advocacy, some participants offered examples that challenged the notion that power and status were essential:
저는 의대생들이 경이로운 일을 하는 것을 보았습니다. 예를 들어, 한 임상 실습생은 수술실에서 섬망 증상으로 제지당하는 환자를 보고 경악을 금치 못해 의료 윤리 전문가를 찾아갔고, 그 후 수술 스태프를 대상으로 섬망 교육을 실시했습니다. 그는 그저 의대생이었지만 이 모든 것을 움직이게 했습니다. 따라서 지위가 있으면 도움이 되지만 필수는 아닙니다. (MD4, I3)
I’ve seen medical students do a phenomenal job. For example, one clinical clerk was absolutely appalled at how patients on a surgical floor were restrained with delirium and he actually went to the medical ethicist, which then instigated delirium education for the surgical staff. He was just a medical student that got this whole thing moving. So, it's helpful to have status, but it's not required. (MD4, I3)
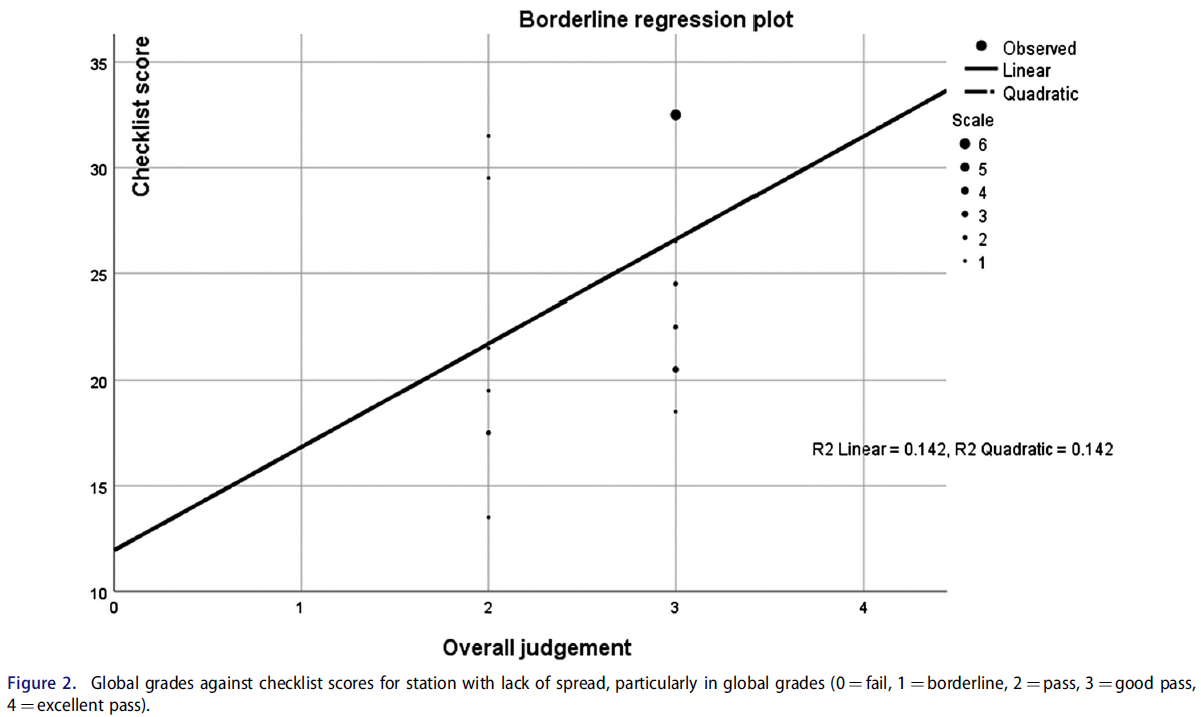
지위나 권력보다 더 중요한 것은 옹호에 참여하는 데 필요한 시간을 할애하는 것뿐만 아니라 옹호에 내재된 위험을 헤쳐나가는 데 기꺼이 헌신하는 것이었습니다. 의사와 환자 참여자 모두 옹호 활동에 시간이 많이 걸린다고 답했으며(그림 2), 의사 참여자들은 여러 가지 경쟁적인 요구 사항을 처리하는 데 어려움을 겪는다고 설명하는 경우도 드물지 않았습니다.
Perhaps more important than status or power was a willingness not only to devote the time necessary for engaging in advocacy, but also to navigating its inherent risks. Both physician and patient participants described advocacy as time intensive (Figure 2), and it was not uncommon for physician participants to describe the struggle they experienced juggling multiple competing demands.

옹호 활동은 또한 문제가 있는 제도적 문제에 반발하기 위한 파괴적이고 위험한 정치 활동으로 인식되었습니다: '당신은 역류하고 있으며 매우 위험합니다. 그리고 누군가의 감정을 상하게 하지 않고 역류하는 것은 어렵습니다. 현재의 기존 관행에 반대하는 사람처럼 보이지 않으면서 역류하는 것은 어렵습니다."(MD3, I1). 열정적이고 적극적인 옹호자라고 스스로 밝힌 두 명의 참가자 중 한 명은 소속 기관으로부터 옹호 활동에 대한 비난을 받았고, 다른 한 명은 목소리를 높이는 옹호자가 되면 동료들로부터 '잠김locked out'(MD3, I1)을 당할 수 있다고 인식하고 있었습니다. 또한 이러한 위험이 교육과 평가에 영향을 미칠 수 있다는 우려도 있었는데, '옹호 활동을 했다는 이유로 처벌을 받는다면, 이는 우리가 사람들이 보여주는 역량에 대해 평가, 평가, 강화 또는 처벌하는 방식에 영향을 미치고 형성할 것이기 때문'(MD9, I3)입니다.
Advocacy was also perceived as a disruptive and risky political activity aimed at pushing back against problematic systemic issues: ‘You're running countercurrent and it's very dangerous. And it's hard to run countercurrent without hurting someone's feelings. It's hard to run countercurrent without looking like a naysayer of the current existing practices’ (MD3, I1). Of two participants who self-identified as passionate and engaged advocates, one was censured for advocacy activities by their institution, and the other recognised that being a vocal advocate can get you ‘locked out’ (MD3, I1) by colleagues. In turn, there were concerns that these risks impacted teaching and assessment because ‘when you're being punished for advocating, then that is going to influence and shape how we assess, evaluate, reinforce or punish people for the competence that they're demonstrating’ (MD9, I3).
3.5 유능한 옹호자 양성
3.5 Training competent advocates
따라서 참가자들에게 옹호 활동은 '약간의 열정과 약간의 화끈함'이 필요한 고위험 활동으로 간주되었습니다(MD3, I1). 환자와 의사 참가자 모두 옹호자에게는 경험, 전문성, 훌륭한 의사소통 기술 이상의 것이 필요하다고 인식했으며, 효과적이거나 뛰어난 옹호자가 되기 위해서는 위험을 감수하려는 의지뿐만 아니라 '타고난 인간의 도덕적 코드'(MD4, I1)에도 의존하는 것으로 보였습니다. 따라서 권력과 특권이 옹호 활동을 촉진할 수도 있지만, 개인의 인성이 옹호 활동을 주도하는 것으로 보입니다. 이 연구에 참여하기로 선택한 참가자들은 옹호자가 되는 것이 개인적, 직업적 정체성의 핵심 특징이라고 설명했습니다: '제가 이 일을 하는 것이 아니라 저라는 사람이 이 일을 하는 것입니다.'(MD3, I2). 결과적으로 의사 참여자들은 레지던트 교육이 수련생들에게 건강 옹호에 대한 표면적인 지식을 전달할 수는 있지만, 유능한 건강 옹호자로 양성하는 것은 달성할 수 없는 목표로 인식했습니다: '전략을 제공할 수는 있지만, 올바른 사람들을 위해 옳은 일을 하고자 하는 도덕적 실체가 있어야 한다'(MD4, I1).
For participants, therefore, advocacy was considered a high-risk activity that required ‘a bit of passion and a bit of fire’ (MD3, I1). Both patient and physician participants perceived that advocates required more than experience, expertise and good communication skills; being an effective or exceptional advocate also seemed to rely on having not only a willingness to take risks, but also on ‘an innate human moral code’ (MD4, I1). Therefore, while power and privilege may facilitate advocacy, an individual's character seems to drive it. For those participants who chose to engage in this work, they described that being an advocate was a central feature of their personal and professional identities: ‘I don't even see myself doing it, it's who I am as a person.’ (MD3, I2). Consequently, physician participants perceived that while residency training may be able to impart surface level knowledge to trainees about health advocacy, molding them into competent health advocates was sometimes perceived as an unattainable goal: ‘I guess you could provide strategies but there still has to be some kind of moral substance in the person that wants to do the right thing for the right people’ (MD4, I1).
그럼에도 불구하고 의사 참가자들은 수련의를 유능한 건강 옹호자로 육성할 책임이 있다는 것을 인정했습니다. 필수적인 환자 경험에 대한 이해와 강력한 공식 커리큘럼이 모두 부재한 상황에서 의사 참가자들은 옹호 교육이 '모델링, 설명, 예시, 내가 이것에 대해 쓴 내용, 앞으로 다른 환자를 볼 수 있도록 읽어볼 수 있는 논문'을 통해 가장 잘 전달될 수 있다고 인식했습니다(MD5, I1). 그러나 대부분의 의사 참가자들은 자신이 옹호에 적합한 모델인지에 대해 의문을 제기하는 듯 보였으며, 학습자에게 옹호를 보여줄 만큼 규칙적으로 옹호에 참여하지 않았다고 인정하는 경우가 많았습니다. 의사 참가자들은 교육생의 건강 옹호를 신중하거나 엄격하게 평가할 수 없을 것이라고 우려했습니다: '그들(임상의사 선생님들)은 항상 건강 옹호자로 '기대에 부응'을 선택합니다, 항상... 건강 옹호자로서 기대에 부응하지 못한 사람을 본 적이 없습니다....'(MD8, I2).
Regardless, physician participants acknowledged that they were responsible for developing their trainees into competent health advocates. In the absence of both an understanding about essential patient experiences and a strong formal curriculum, physician participants perceived that advocacy teaching was best conveyed by ‘modelling, by explaining, by giving examples, by saying, this is what I wrote about this, this is a paper that you can read about it so that you can see another patient in the future’ (MD5, I1). However, most physician participants seemed to question whether they were appropriate models for advocacy, often admitting that they did not engage in advocacy with enough regularity to demonstrate it to learners. In turn, physician participants worried that they would not be able to thoughtfully or rigorously assess a trainee's health advocacy: ‘They (clinician teachers) will always choose ‘meets expectations’ for health advocate, always… I have never had anybody not meet expectations as a health advocate….’ (MD8, I2).
환자 참여자들은 의사를 자신의 주 건강 옹호자로 지목한 적이 거의 없었습니다. 오히려 환자 참여자들은 '의사의 역할은 진단하고 회복 계획을 세우는 것이지, [환자가] 주변 도움을 받을 수 있는 모든 가능한 옵션을 설명하는 것은 의사의 일이 아니다'라고 인식하고 있었습니다. 그들은 그럴 시간이 없습니다'(P8, I2). 환자 참여자에게는 옹호를 다른 사람에게 미루는 것이 의사의 역량을 나타내는 한 가지 지표가 될 수 있으며, 이는 유능한 의사 옹호자는 자신의 한계를 알고 옹호를 다양한 형태의 전문 지식에 의존하는 파트너십으로 간주한다는 것을 시사합니다. 한 의사 참가자는 의사 옹호 활동의 필수 요소는 '의사가 가장 잘 아는 생물 의학 모델을 지속적으로 밀고 나가야 하며, 나 자신을 하나의 파트너로, 환자 치료의 한 전문가로, 나 자신을 전문가로, 환자 가족, 다른 분야를 전문가로 보는 것'이라고 지적하며 이러한 정서를 반영했습니다. (MD10, I2). 환자 참가자 7은 이에 동의하며 유능한 건강 옹호의 의미에 대해 생각한 후 다음과 같이 제안했습니다: '어쩌면 옹호의 일부분은 자신이 모든 것을 알고 있는 의사라는 환상을 제시하기보다는 자신이 그것을 알아낼 수 없으므로 다른 사람에게 이야기해야 한다는 것을 아는 것일지도 모른다'(P7, I2).
Patient participants rarely, if ever, identified a physician as their primary health advocate. Rather, patient participants perceived that ‘the doctor's job is to diagnose and create a plan of recovery… it's not their job to explain every possible option that is out there, where [patients] can get peripheral help. They don't have time for that’ (P8, I2). For patient participants, deferring advocacy to others might be one indicator of a physician's competence, suggesting that competent physician advocates know their limits and view advocacy as a partnership dependent on multiple forms of expertise. One physician participant echoed this sentiment, noting that an essential component of the advocacy work of physicians is ‘having to continuously push back on the biomedical physician knows best model and see myself as one partner, one expert in their care, themselves as an expert, their families, other disciplines being experts.’ (MD10, I2). Patient participant 7 agreed and, after reflecting on the meaning of competent health advocacy, suggested that: ‘maybe part of advocacy is knowing that you can't figure it out so you have to talk to someone else about it, rather than trying to present the illusion that you're the all-knowing doctor’ (P7, I2).
4 토론
4 DISCUSSION
건강 옹호자 역할에 대한 역량을 갖추려면 수련의는 '임상 환경 안팎에서 환자와 함께 옹호함으로써 환자 개인의 건강 요구에 대응'하고, '사회적으로 책임 있는 방식으로 시스템 차원의 변화를 위해 환자와 함께 옹호함으로써 그들이 봉사하는 지역사회 또는 집단의 요구에 대응'할 수 있어야 합니다.1 그러나 건강 옹호를 교육하고 평가하는 데 있어 잘 알려진 어려움은2-4 건강 옹호의 대상과 방법, 또는 환자 개인과 시스템 차원의 요구에 효과적으로 대응하는 데 필요한 행동과 기술에 대한 합의가 부족한 데에 뿌리를 두고 있는 것으로 보입니다. 저희는 건강 옹호자 역할에 대한 역량에 대한 환자와 의사의 관점을 살펴봄으로써 이러한 기대가 실제로 무엇을 의미하는지 명확히 하고자 했습니다. 건강 옹호 활동을 공동의 활동으로 생각했지만, 새로운 커리큘럼 프레임워크와 달리1 참가자 중 매우 작은 숫자만이 건강 옹호를 의사의 기본 역할로 인식하고 있다는 사실(적어도 현재 정의된 것과는 다른)을 발견하고 놀랐습니다. 표면적으로는 이러한 연구 결과가 건강 옹호에 대한 대화를 명확하게 하기보다는 복잡하게 만드는 것처럼 보이지만, 이러한 복잡성을 풀면 건강 옹호 교육에 대한 보다 간소화되고 목표에 맞는 접근법을 찾는 데 유용할 수 있습니다.
To achieve competence for the Health Advocate role, a trainee must be able to ‘respond to an individual patient's health needs by advocating with the patient within and beyond the clinical environment’ and ‘respond to the needs of the communities or populations they serve by advocating with them for system-level change in a socially accountable manner’.1 However, the well-known challenges of teaching and assessing health advocacy2-4 seem rooted in lack of consensus about the what and how of health advocacy, or the actions and skills required to mount an effective response to patients’ individual and systems-level needs. We set out to clarify what these expectations mean in practice by exploring patients’ and physicians’ perspectives about competence for the Health Advocate role. While we thought of it as a shared activity, we were surprised to discover that, contrary to new curricular frameworks,1 few of our participants perceived health advocacy as a fundamental physician role—at least not as it is currently defined. On the surface, our findings seem to complicate rather than clarify conversations about health advocacy; however, we suggest that unpacking these complications might usefully inform more streamlined and targeted approaches for health advocacy training.
4.1 건강 옹호 교육 및 평가의 어려움 미묘하게 조정하기
4.1 Nuancing the challenges of teaching and assessing health advocacy
HA와 달리, 다른 CanMEDS 역할은 역량에 대해 잘 정의되고 단계적으로 진행되거나,1 적어도 주관적일지라도 만족스러운 성과와 불만족스러운 성과를 합리적으로 명확하게 구분하는 것으로 보입니다. 즉, 수련의는 의학 지식과 기술 능력에서 역량을 입증하거나 그렇지 못할 수 있으며, 수련의가 문헌을 비판적으로 평가하거나 효과적으로 의사소통할 수 있는지 여부를 평가하는 것은 비교적 간단합니다. 참가자들은 역량에 대한 기준이 HA 역할에 비해 더 복잡하여 가변적이고 예측할 수 없는 기대치와 평가 기준을 만든다고 제안했습니다. 실제로 의사 참가자들은 의료 전문가 역할에 대해 옹호 시도만 있어도 '충분히 좋은 것'으로 인식되며, 이는 의료 전문가 역할에 고려되지 않거나 심지어 용인되지 않는 기준이라고 제안하는 것 같았습니다. 그리고 탁월한 옹호자로 평가받기 위한 기준, 즉 환자에게 최상의 치료를 제공하기 위해 일관되고 성실하게 일하는 것은 다른 역할에 대한 최소한의 기대치인 것 같습니다.
Unlike HA, other CanMEDS roles appear to have either a well-defined, staged progression for competence,1 or at least a reasonably clear, if subjective, distinction between a satisfactory or unsatisfactory performance. In other words, trainees either demonstrate competence in their medical knowledge and technical skill or they don't, and it is relatively straightforward to assess whether or not a trainee can critically appraise the literature or communicate effectively. Our participants suggested that the threshold for competence is more convoluted for the HA role, creating variable and unpredictable expectations and assessment standards. Indeed, physician participants seemed to suggest that any attempt at advocacy was perceived as ‘good enough’, a bar that would neither be considered—nor perhaps even tolerated—for the Medical Expert role. And the standards for being assessed as an exceptional advocate, namely working consistently and diligently to provide patients with the best possible care, seem to be the minimum expectation for other roles.
이러한 가변성과 예측 불가능성은 일반적으로 모호하거나 너무 넓은 정의에 기인합니다 .5,19 그러나 환자 참여자들이 설명한 바에 따르면 실제로는 HA에 대한 해석이 너무 좁을 수 있으며, 환자 경험을 향상시킬 수 있는 옹호 형태를 간과하고 있을 수 있다고 제안합니다. 환자와 의사 참여자 모두 시스템이 환자의 요구를 충족시키지 못하거나 환자가 스스로 치료를 지시하는 능력을 방해하는 등 문제가 발생했을 때 옹호가 필요한 경우가 많다고 암시했습니다. 따라서 옹호자들은 때때로 프로토콜을 '우회'36하거나 전문적 규범에 도전하는 방식으로 현상 유지를 방해해야 하는 경우가 많습니다. 의사 참가자들은 옹호 활동이 본질적으로 파괴적이고 위험하다고 설명하면서, 특히 정치적으로 현명한 방식으로 수행되지 않을 경우 옹호 활동에 참여하면 비난을 받거나 어려운 사람으로 낙인찍힐 수 있다고 답했습니다. 유능한 옹호자는 이러한 정치적 지뢰밭을 비교적 무사히 통과할 수 있어야 합니다.
This variability and unpredictability is typically attributed to definitions of HA that are nebulous or too broad .5, 19 However, we suggest that interpretations of HA may in fact be too narrow, and from what our patient participants described, might be overlooking forms of advocacy that would enhance the patient experience. Both patient and physician participants implied that advocacy is often necessary when things go wrong—either when the system fails to meet patients’ needs or when it impedes their ability to direct their own care. Consequently, advocates often need to disrupt the status quo, sometimes in ways that ‘work around’ protocols36 or challenge professional norms. Our physician participants described advocacy as inherently disruptive and risky, suggesting that engaging in it—particularly when it is not done in a politically savvy way—can result in censure or being labelled as difficult. A capable advocate should be able to traverse these political minefields relatively unscathed.
그러나 옹호가 항상 파괴적인 것은 아닙니다. 환자 참여자들에 따르면, 자신의 전문성을 인정하고 치료 계획에 반영하며 공감하고 세심하게 경청하는 것 역시 건강 옹호의 한 형태라고 합니다. 즉, 의사 참여자들은 옹호가 진료에 어떻게 적용되는지 개념화하는 데 어려움을 표한 반면, 환자 참여자들은 임상 치료에서 옹호의 역할을 쉽게 파악할 수 있었으며, 이는 옹호가 환자 중심주의 철학과 밀접하게 연관되어 있다는 이전 연구를 뒷받침하는 것으로 보입니다.30 공감적 경청과 효과적인 의사소통 등 환자가 옹호라고 묘사한 많은 부분이 의사에게도 중요하다고 인식되고 있음을 알 수 있습니다. 그러나 의사들은 이러한 요소들을 건강 옹호의 '부수적인' 업무라기보다는 좋은 치료의 기본 구성 요소로 개념화하는 것으로 보입니다.30
Advocacy isn't always disruptive, however. According to patient participants, acknowledging and incorporating their expertise into care plans, empathising, and listening attentively are also forms of health advocacy. In other words, while physician participants expressed difficulty conceptualising how advocacy fit within their practice, patient participants were readily able to see its role in clinical care, seemingly supporting our previous research suggesting that advocacy is closely linked with philosophies of patient centredness.30 We recognise that much of what patients described as advocacy—such as empathetic listening and effective communication—are also viewed as important by doctors. However, physicians seem to conceptualise these as fundamental components of good care rather than the ‘above and beyond’ work of health advocacy.30
모든 환자와 대부분의 의사 참가자들은 보다 파괴적인 형태의 옹호를 반드시 의사의 역할로 간주하지는 않는다는 점을 분명히 했습니다. 환자 참여자들에 따르면, 좋은 의술은 옹호이며, 이는 의사 참여자들과 다른 사람들이 진료에서 옹호의 역할을 파악하는 데 어려움을 겪는 이유를 설명하는 것으로 보입니다.5, 6 그러나 상호 존중, 투명성 및 공감의 환경을 조성하는 것이 기대되는 반면, 환자 참여자들은 자신의 진료가 열악하다고 인식하는 경우를 고려하여 유능한 건강 옹호를 정의할 수 있다는 점을 염두에 둘 필요가 있습니다.37 비록 개인이 의학교육 연속체를 따라 진행함에 따라 공감 능력이 감소한다는 연구가 뒷받침하지만 실망스러운 계시입니다.
All patients and most physician participants made clear that they do not necessarily view more disruptive forms of advocacy as the physician's role. According to patient participants, good doctoring is advocacy, which seems to explain why physician participants and others have a difficult time identifying its role in their practice.5, 6 We do, however, need to be mindful that while cultivating an environment of mutual respect, transparency and empathy should be the expectation, patient participants could only define competent health advocacy by considering instances where they perceived their care as poor—a disheartening revelation, albeit one supported by research suggesting that empathy declines as individuals progress along the medical education continuum.37
4.2 옹호 교육에 대한 재구상
4.2 Re-imagining advocacy training
현재의 프레임워크는 옹호를 파괴적이거나 정치적인 것으로 인식될 수 있는 행동4을 요구하는 것으로 간주합니다. 이러한 일반적인 관념은 환자와 달리 의사 참여자가 옹호자로 식별되는 경우가 드문 이유를 설명할 수 있습니다. 이는 건강 옹호가 도덕적 의무이자 소명이라는 이전 연구 결과와 일맥상통하며,38 옹호자가 되는 것이 훈련에 의존하는지, 개인의 인성에 의존하는지, 아니면 둘 다에 의존하는지에 대한 의문을 제기합니다. 옹호의 도덕적 차원은 의사가 직업적 정체성의 일부로 옹호에 동참하는 데 장애가 될 수 있습니다. 또한 이러한 도덕적 차원은 교육과 평가에 어려움을 야기합니다. 구성 요소로서의 역량에 대한 비판 중 하나는 역량을 평가할 때 수련의의 인성이나 개인적 자질을 거의 고려하지 않는다는 것이지만,39 도덕성이나 인성을 평가할 수 있고, 평가해야 할까요?
Current frameworks see advocacy as requiring actions4 that might be perceived as disruptive or political. This prevailing notion might account for why our physician participants—unlike patients—rarely identified as advocates. This resonates with previous research suggesting health advocacy is both a moral imperative and a calling,38 raising questions about whether becoming an advocate relies on training, an individual's character, or both. Advocacy's moral dimension may be a barrier to physicians aligning with it as part of their professional identity. Further, this moral dimension creates challenges for teaching and assessment. While one of the critiques of competence as a construct is that we rarely consider trainees’ character or personal qualities when we assess competence,39 can we, and should we, be trying to assess morality or character?
또한 수련의는 현 상태를 파괴할 수 있을 만큼 충분한 임상 경험이나 지위를 갖지 못할 수도 있습니다. 따라서 현재와 같은 방식으로는 많은 학습자가 이 역할에 필요한 기본 역량이나 보조 역량을 갖추지 못할 수 있습니다. 옹호활동이 혼란과 행동주의에 관한 것이라는 잘못된 인식이 건강 옹호 문제의 근본 원인일 수 있으며, 이를 해결하기 위해서는 환자가 설명하는 사람 중심 요소를 포함하도록 건강 옹호의 정의를 확장하고 일반적으로 건강 옹호자 역할과 관련이 없는 학습자의 공감과 주의 깊은 경청을 강화하는 데 교육을 집중해야 할 수 있습니다.
Trainees may also not have sufficient clinical experience or status to capably disrupt the status quo. Consequently, as currently framed, many learners may not be able to achieve either the primary or enabling competencies required for this role. Misperceptions that advocacy is only about disruption and activism may be the root cause of the health advocacy problem; solving it may rely on both expanding definitions of health advocacy to include the person-centred elements described by patients, and focusing training on bolstering learners’ empathy and attentive listening, a skillset not typically associated with the Health Advocate role.
많은 의사가 이미 파괴적이지 않은 형태의 대리인 옹호에 참여하고 있으며 학습자를 위한 역할 모델링을 하고 있을 가능성이 높습니다. 그러나 의사는 환자를 대신하여 다른 형태의 옹호 업무를 수행하도록 요청받을 수 있으므로, 건강 옹호사 교육은 복잡성, 긴장감, '그 이상'으로 나아가는 데 따른 잠재적 위험과 불편함에 대해 깊이 있게 다루어야 합니다. 일부 프로그램에서는 이미 두부 손상 예방 프레젠테이션을 개발하여 초등학교에서 강의한 후 그 경험에 대한 에세이를 작성하는 등 창의적인 옹호 활동에 전공의들을 참여시키고 있습니다.40, 41 이러한 종류의 멘토링, 실습 옹호 업무는 유용할 수 있습니다3, 42-44-양식 작성 및 신속한 의뢰와 같은 일상적인 임상 활동도 필수 옹호 업무로 인정하고 명시적으로 교육하는 한.
Many physicians are likely already engaging in—and role modelling for learners—less disruptive forms of agentic advocacy. However, since physicians may be called on to do other forms of advocacy work on behalf of their patients, HA training should delve into the intricacies, tensions, and potential risks and discomfort of going ‘above and beyond’. Some programmes are already engaging residents in creative advocacy initiatives such as developing a head injury prevention presentation and delivering it in elementary schools, then writing an essay about the experience.40, 41 This kind of mentored, hands-on advocacy work may be useful3, 42-44—as long as everyday clinical activities such as completing forms and expediting referrals are also both acknowledged as essential advocacy work and explicitly trained.
의사 참여자들이 스스로 인정한 바에 따르면, 이들은 보다 파괴적인 형태의 HA를 가르치는 데 가장 적합하지 않을 수 있습니다. 의사 참여자들이 스스로 활동가라고 밝힌 경우에도, 그들 스스로가 인식한 한계 때문에 또는 시스템이 음성적 옹호를 가능하게 하도록 설계되지 않았기 때문에 모두가 자신이 효과적이라고 인식하지는 않았습니다. 이전 연구에서30 우리는 HA 교육 및 평가에 전문가 간 접근 방식이 필요하다고 제안했으며, 옹호 교육에 비의사를 더 많이 포함시킬 것을 촉구했습니다. 환자 참가자들은 옹호의 의미에 대해 더 폭넓게 이해하고 있었을 뿐만 아니라, 의사들이 어떤 점을 놓치고 있는지도 잘 알고 있는 것 같았습니다. 우리는 의료 교육에서 환자의 공식적인 역할이 제한되어 있는 것이 옹호를 정의하기 어렵고15 훈련하기 어려운 이유의 일부가 될 수 있다고 생각합니다.17 실현 가능성, 신뢰성 및 윤리에 대한 우려45-47 가 현재 환자의 참여를 제한하고 있지만, 많은 환자가 학습자 교육에 참여하고 싶어하며,48 옹호 교육을 더욱 견고하게 만들 잠재적으로 혁신적이고 의미 있는 기회를 창출할 수 있습니다.
By our physician participants’ own admission, they may not best suited to teach the more disruptive forms of HA. Even when our physician participants identified as being activists, not all perceived that they were effective—either because of their own perceived limitations, or because the system is not designed to enable vocal advocacy. In previous work,30 we suggested that HA teaching and assessment demanded an interprofessional approach, and we called for greater inclusion of non-physicians in advocacy training. Patient participants not only had a more expansive understanding about what advocacy means, but they also seemed to be quite aware of when physicians were missing the mark. We suspect that patients’ limited formal role in medical education may be partly responsible for why advocacy is both difficult to define,15 and challenging to train.17 While concerns about feasibility, credibility and ethics45-47 currently limit their involvement, many patients are keen to participate in educating learners,48 creating a potentially innovative and meaningful opportunity to make advocacy training more robust.
5 제한 사항
5 LIMITATIONS
본 연구에는 의료진과 거의 동일한 수의 환자 참여자가 있었기 때문에 예상했던 것보다 환자들의 목소리가 결과에서 덜 두드러졌다는 점을 인정합니다. 이는 주로 환자들을 옹호에 대한 논의에 참여시키려는 노력이 의사의 역할에서 일관되게 멀어졌기 때문입니다. 이는 우리 연구의 한계이기는 하지만, 동시에 중요한 관찰 결과이기도 합니다. 이는 환자가 의사에게 기대하는 옹호는 적어도 의학 교육 프레임워크에서 일반적으로 설명하는 종류의 옹호가 아닐 수 있음을 시사합니다. 그러나 환자들이 기대하는 것은 공감, 숙련된 경청, 자비로운 의사소통이며, 우리는 이러한 좋은 의술의 기본적 특징이 아닌 다른 것을 만들기 위해 너무 열심히 노력한 것은 아닌지 고민하게 됩니다. 그럼에도 불구하고 소수의 레지던트만을 대상으로 했기 때문에 향후 연구에서는 특히 지위와 전문성, 그리고 그것이 개인의 옹호 의지에 어떤 영향을 미칠 수 있는지에 대한 우리의 주제가 학습자에게도 적용되는지 살펴봐야 합니다. 마지막으로, 이번 연구 결과를 일반화할 수는 없지만, 이전에 밝혀지지 않았던 옹호 교육에 대한 장애물을 밝혀내어 졸업후 의학 교육 전반의 교육 및 평가에 유용한 정보를 제공할 수 있습니다.
We had a nearly equal number of patient participants as MDs; given that, we acknowledge their voices were less prominent in the results than might have been expected. This is primarily because efforts to engage them in discussions of advocacy consistently led away from the physician role. While this is a limitation of our work, it is also a telling observation. It suggests that advocacy may not be expected of physicians by patients—at least not the kind typically described in medical education frameworks. But what they do expect is empathy, skilled listening, and compassionate communication, leading us to wonder if we have perhaps tried too hard to make HA something other than these fundamental characteristics of good doctoring. Regardless, because we only spoke with a few residents, future research should explore whether our themes, particularly about status and expertise and how they may impact an individual's willingness to advocate, also hold true for learners. Finally, while our findings are not generalisable, they shed light on previously underexplored impediments to advocacy training which may usefully inform teaching and assessment across postgraduate medical education.
6 결론
6 CONCLUSION
참가자들이 설명한 의료 및 시스템 수준의 지식, 효과적인 의사소통 기술, 환자 중심주의와 같은 역량 요건은 이전 연구와 공명하지만,27 우리의 연구 결과는 유능한 건강 옹호자가 되는 것이 무엇을 의미하는지, 학습자가 레지던트 수련 기간 동안 건강 옹호 역량을 달성하는 것이 현실적인지, 심지어 가능한지에 대한 몇 가지 가정에 도전합니다. 그러나 옹호가 환자 중심주의와 밀접하게 연관되어 있다는 것이 옳다면, 옹호에 대한 정의를 재정의하거나 충분한 커리큘럼적 관심을 기울이지 않는 것은 환자에게 해가 될 뿐만 아니라 의학의 철학적 토대를 약화시키는 일입니다. 모든 형태의 옹호는 교육 중에 탐구되어야 하지만, 환자에게 가치 있는 것으로 설명된 비방해적 요소에 우선순위를 두는 것이 교육을 간소화할 뿐만 아니라 치료를 최적화할 수 있다고 제안합니다. 환자의 목소리가 옹호와 관련된 역량보다 더 중요한 역량은 없을 것입니다. 우리는 환자가 의료 교육에 의미 있게 참여하는 데 방해가 되는 장벽을 제거하여 의료진 교육을 위한 협력적 교수법을 구축할 수 있는 기회를 모색해야 합니다.
While the requisites for competence such as medical and systems-level knowledge, effective communication skills, and patient centredness described by our participants resonate with previous work,27 our findings challenge several assumptions both about what being a competent health advocate means, and whether it is realistic—or even possible—for learners to achieve competence in health advocacy during their residency training. However, if we are correct that advocacy is closely linked with patient centredness, failing to re-define or devote sufficient curricular attention to advocacy is not only a disservice to patients, but it undermines the philosophical underpinnings upon which medicine is built. While all forms of advocacy should be explored during training, we suggest that prioritising the non-disruptive elements described as valuable to patients would not only streamline training but also optimise care. There may be no set of competencies where the patient voice is more critical than those around advocacy. We need to explore opportunities to build a collaborative pedagogy for training HA, removing barriers that prevent patients from participating meaningfully in medical education.
Exploring patients' and physicians' perspectives about competent health advocacy
PMID: 33152148
DOI: 10.1111/medu.14408
Abstract
Introduction: Many residency programmes struggle to demonstrate how they prepare trainees to become competent health advocates. To meaningfully teach and assess it, we first need to understand what 'competent' health advocacy (HA) is and what competently enacting it requires. Attempts at clarifying HA have largely centred around the perspectives of consultant physicians and trainees. Without patients' perspectives, we risk training learners to advocate in ways that may be misaligned with patients' needs and goals. Therefore, the purpose of our research was to generate a multi-perspective understanding about the meaning of competence for the HA role.
Methods: We used constructivist grounded theory to explore patients' and physicians' perspectives about competent health advocacy. Data were collected using photo elicitation; patients (n = 10) and physicians (n = 14) took photographs depicting health advocacy that were used to inform semi-structured interviews. Themes were identified using constant comparative analysis.
Results: Physician participants associated HA with disruption or political activism, suggesting that competence hinged on medical and systems expertise, a conducive learning environment, and personal and professional characteristics including experience, status and political savvy. Patient participants, however, equated physician advocacy with patient centredness, perceiving that competent HAs are empathetic and attentive listeners. In contrast to patients, few physicians identified as advocates, raising questions about their ability to train or to thoughtfully assess learners' abilities.
Conclusion: Few participants perceived HA as a fundamental physician role-at least not as it is currently defined in curricular frameworks. Misperceptions that HA is primarily disruptive may be the root cause of the HA problem; solving it may rely on focusing training on bolstering skills like empathy and listening not typically associated with the HA role. Since there may be no competency where the patient voice is more critical, we need to explore opportunities for patients to facilitate learning for the HA role.
© 2020 John Wiley & Sons Ltd and The Association for the Study of Medical Education.
'Articles (Medical Education) > 전문직업성(Professionalism)' 카테고리의 다른 글
| 전문직업성의 짧은 역사와 허약한 미래: 의료의 사회계약의 침식( Perspect Biol Med. 2008) (0) | 2023.09.26 |
|---|---|
| 행복은 무엇인가? 의학교육을 위한 비판적 내러티브 리뷰(Perspect Med Educ. 2023) (0) | 2023.09.19 |
| "정말 곤란하게 만들어요", 중국 전공의의 전문직업성 딜레마(Adv Health Sci Educ Theory Pract. 2023) (0) | 2023.09.12 |
| '너의 모든 형태로서의 너 자신': 의과대학생의 정체성 안정에 대한 근거이론 탐색(Med Educ, 2023) (0) | 2023.08.31 |
| 테크니컬 어려움: 테크놀로지에 대한 비판적 철학적 지향 가르치기(Teach Learn Med, 2023) (0) | 2023.08.30 |