임상진료상황에서 능숙한 의사소통가의 특징 식별하기(Med Educ, 2022)
Identifying characteristics of a skilled communicator in the clinical encounter
Michelle Verheijden1,2 | Esther Giroldi1,2 | Valerie van den Eertwegh3 | Marscha Luijkx4 | Trudy van der Weijden1 | Anique de Bruin2 | Angelique Timmerman1
1 서론
1 INTRODUCTION
의사-환자 커뮤니케이션은 의료 서비스 제공에 중요한 역할을 하며 핵심 의료 역량으로 인식되고 있습니다.1-3 이러한 인식은 현재의 의료 교육 관행과 의료 서비스에서 변화하는 커뮤니케이션 요구 사이의 불일치를 해결해야 함을 의미합니다.1, 4-10
Doctor-patient communication plays an important role in the delivery of health care and has been recognised as a core medical competency.1-3 This recognition implies addressing a signalled misalignment between current medical training practices and changing communication needs in health care.1, 4-10
따라서 의료 교육 프로그램에서는 여러 가지 일반적인 의사소통 지침을 도입하여 이러한 불일치를 해결하려고 시도해 왔습니다.8 예를 들어, '환자의 이야기 요약하기' 또는 '적극적인 경청'과 같이 임상에서 필요한 의사소통 기술을 정의하기 위해 개발된 SEGUE 프레임워크11 및 캘거리-캠브리지 모델12, 13이 있습니다.4-7, 14, 15 스킬 기반 접근법은 학습자에게 유용한 상담 구조와 스킬 도구 상자를 제공하므로 높은 평가를 받고 있지만, 실제 풍부한 진료 환경에서 효과적으로 의사소통하는 것은 충분하게 지원하지 못합니다.2, 4-7, 9, 16 학습자는 직면하는 임상 문제에 의해 도전을 받고 환자의 요구를 고려하여 의사소통을 조정합니다.1, 5-7, 17 이는 Veldhuijzen 등과 Essers 등이 의사소통은 일차적으로 목표 중심적이며, 상담의 여러 맥락적 요인(예: 의료, 환자 또는 의사 관련)에 의해 영향을 받는다고 말한 것처럼 각 임상 상황에서 의사소통을 맞춤화할 필요가 있음을 시사합니다.10, 13, 18
Consequently, medical training programmes have attempted to address this misalignment by introducing multiple generic communication guidelines.8 For instance, the SEGUE framework11 and Calgary–Cambridge model12, 13 were developed to define communications skills needed in the clinical encounter like ‘summarising the patient's story’ or ‘active listening’.4-7, 14, 15 Although a skills-based approach is highly valued as it provides learners a helpful consultation structure and a toolbox of skills, it insufficiently supports them in communicating effectively in the complexity of the authentic rich practice setting.2, 4-7, 9, 16 Learners are challenged by the clinical problems they encounter and adjust communication considering patient needs.1, 5-7, 17 This implies a need to tailor communication in each clinical encounter, as Veldhuijzen et al and Essers et al state that communication is primarily goal driven and influenced by several contextual factors (i.e. medical-, patient- or doctor-related) in the consultation.10, 13, 18
이러한 필요성은 '의사소통 기술'에 초점을 맞추던 것에서 '숙련된 의사소통'으로 전환하는 현재의 담론과 연결됩니다.8, 10 의사-환자 의사소통 학습은 경험적 직장 학습 중 의사소통의 맥락화된 적용을 통해 보다 적절하게 다룰 수 있습니다.7, 9, 10, 16, 17, 19, 20 숙련된 의사소통의 전문성을 얻기 위해서는 성찰과 피드백을 바탕으로, 개인 수행의 [적용, 적응 및 개선 기회]를 제공하는 도전적인 임상 학습 과제에 기반하여 의도적인 연습이 필요합니다.21, 22
This signalled need connects to the current discourse shifting from focusing on ‘communication skills’ towards ‘skilled communication’.8, 10 Learning doctor–patient communication may be more appropriately addressed by a contextualised application of communication during experiential workplace learning.7, 9, 10, 16, 17, 19, 20 For attaining expertise in skilled communication, deliberate practice is required based on challenging clinical learning tasks that provide opportunities for application, adaptation and refinement of personal performance, based on reflection and feedback.21, 22
그럼에도 불구하고 숙련된 의사소통 접근법이 정확히 무엇이며 숙련된 의사소통자의 특성이 무엇인지에 대한 합의가 부족합니다.1, 7, 9, 15, 23 우리는 숙련된 의사소통의 개념을 설명하기 위한 예비 단계로 의료 의사소통과 관련된 이해관계자들의 관점을 종합하기 위해 명목 그룹 기법(NGT)을 사용했습니다.22 NGT는 의학 교육에 널리 적용되었으며, 구조화된 특성상 모든 이해관계자가 자신의 의견을 표현할 수 있는 동등한 기회를 보장하여 토론을 촉진하고 공유된 합의를 형성합니다.24-26
Nevertheless, a lack of consensus exists about what a skilled communication approach exactly entails and what characteristics are of a skilled communicator.1, 7, 9, 15, 23 We used the nominal group technique (NGT) to synthesise viewpoints from stakeholders involved in medical communication as a preliminary step to inform describing the concept of skilled communication.22 NGT has been widely applied in medical education, and its structured nature ensures all stakeholders to have equal opportunities to express their views, stimulating discussion and creating a shared consensus.24-26
본 연구는 현재 의료 커뮤니케이션 연구의 이론 구축에 기여하고 숙련된 커뮤니케이션 교육을 위한 학습자 중심 접근법의 개발을 알리고 향후 임상 실무로의 이전을 지원하는 것을 목표로 합니다.9, 10, 15 다음과 같은 연구 질문이 다루어졌습니다: '임상 현장에서 숙련된 커뮤니케이터의 특징은 무엇인가?'
We aim to contribute to theory building in current health communication research and to inform the development of a learner-centred approach for skilled communication training and support its future transfer to clinical practice.9, 10, 15 The following research question was addressed: ‘What are characteristics of a skilled communicator in the clinical encounter?’
2 방법
2 METHODS
설정
Setting
이 연구는 네덜란드의 일반 진료(GP) 전문 교육 프로그램의 맥락에서 수행되었으며, 8개의 GP 교육 기관 중 5개 기관에서 참가자를 모집했습니다. 일반의의 임상 업무량은 다양한 의학적 및 심리사회적 불만 사항으로 구성되어 있어 임상적 상황에 맞게 커뮤니케이션을 일관되게 조정해야 하기 때문에 GP 환경을 선택했습니다.14, 17, 23, 24, 27, 28 GP 교육 프로그램은 3년에 걸쳐 4일의 직장 기반 교육과 1일의 공식 교육으로 번갈아 가며 구성됩니다.
The study was performed in the context of the general practice (GP) specialty training programme in the Netherlands, recruiting participants from five out of eight GP training institutes. The GP setting was chosen because the clinical workload of a GP consists of a variety of medical and psychosocial complaints, which requires a consistent adjustment of communication to the needs of the clinical encounter.14, 17, 23, 24, 27, 28 The GP training programme consists of 3 years, alternating 4 days of workplace-based training with 1 day of formal education.
연구 설계
Study design
숙련된 커뮤니케이터의 특성을 규명하기 위해 2020년 4월부터 10월까지 네덜란드의 GP 교육 프로그램 이해관계자를 대상으로 6번의 NGT 세션이 진행되었습니다. NGT는 특정 주제에 대한 아이디어를 도출하기 위한 합의 그룹 방식으로, 참가자들이 구조화된 상호작용을 통해 생각을 공유하고 토론에 참여하도록 지속적으로 자극함으로써 여러 이해관계자의 관점을 통합하는 데 도움이 됩니다.29, 30 COVID-19 팬데믹으로 인해 모든 NGT 세션은 Zoom 플랫폼을 사용하여 전자 환경에서 진행되었습니다.31, 32
Six NGT sessions were conducted between April and October 2020 among Dutch stakeholders of the GP training programmes to elucidate characteristics of a skilled communicator. The NGT is a consensus group method to generate ideas on a certain topic and facilitates the integration of multiple stakeholders' perspectives by constantly stimulating participants to share their thoughts and engage in the discussion through a structured interaction.29, 30 Due to the COVID-19 pandemic, all NGT sessions took place in an electronic environment using the Zoom platform.31, 32
참가자 Participants
각 NGT 세션의 최적 참가자 수는 5~7명으로, 6개의 세션에 최소 30명이 참여해야 합니다.25, 33 의도적 표본 추출을 사용하여 의사-환자 커뮤니케이션에 대한 경험과 전문성을 바탕으로 잠재적 이해관계자 목록을 구성했습니다.34 이 목록에는 (1) GP, (2) GP 연수생, (3) GP 트레이너, (4) GP 연수 프로그램의 조정자 및 교육과정 개발자, (5) 의료 커뮤니케이션 분야 연구자가 포함되었습니다. 75명의 잠재적 이해관계자에게 이메일을 통해 연구의 목적과 절차, 필요한 시간 투자에 대한 정보를 제공하면서 참여를 요청했습니다. 각 NGT 세션 전에 모든 참가자로부터 서면 동의서를 받았으며, 참가자는 자발적으로 참여했습니다. 또한 참가자들은 인구통계학적 설문지를 작성했습니다. 참가자를 식별할 수 있는 모든 개인 식별 정보는 하나 이상의 인공 식별자(가명)로 대체되었습니다.
The optimal number of participants for each NGT session is five to seven, resulting in a minimum of 30 participants for six sessions.25, 33 By using purposive sampling, a list of potential stakeholders was composed based on their experience and expertise in doctor-patient communication.34 The list included (1) GPs, (2) GP trainees, (3) GP trainers, (4) coordinators and curriculum developers of the GP training programme and (5) researchers in medical communication. We invited 75 potential stakeholders to participate via e-mail, providing information about the purpose and procedure of the study and needed time investment. Written informed consent was obtained from all participants prior to each NGT session, and participation was on a voluntary basis. Moreover, participants completed a demographic questionnaire. All personally identifiable personal information, which could lead to the participants, was replaced by one or more artificial identifiers (pseudonyms).
데이터 수집
Data collection
90분에서 120분까지 진행된 NGT 세션은 오디오 녹음 후 그대로 필사되었습니다. 모든 NGT 세션은 동일한 프로토콜(부록 S1)을 사용했으며, 두 명의 사회자, 한 명의 교육 연구자 겸 심리학자(AT)와 한 명의 박사 과정 학생 겸 GP 수련의(MV)가 진행했습니다.35, 36 추가 연구자 겸 보건 과학자(EG)가 세션에 참석하여 관찰하고 현장 메모를 작성했습니다. 연구팀은 숙련된 의사소통에 대한 현재 과학적 담론에서 아이디어를 수집하기 위해 문헌 연구와 의사소통 전문가와의 세 차례의 반구조화 인터뷰를 수행하여 명목 질문을 구성했습니다.29, 36, 37
- 세션 절차에 대한 간략한 설명 후 다음과 같은 명목 질문이 제기되었습니다: '숙련된 GP 의사소통자의 특징은 무엇인가요? NGT 세션에서 우리는 특성을 '임상 상황에서 숙련된 의사소통자를 설명하는 전형적이거나 눈에 띄는 특징'으로 소개했습니다.
- 둘째, 명목상의 질문에 대해 참가자들은 개별적으로 자신의 아이디어를 적었습니다.
- 셋째, 참가자들은 하나의 아이디어를 '라운드 로빈' 방식으로 그룹에 공유했습니다. 진행자 중 한 명이 모든 아이디어를 워드 문서로 옮겨 모든 참가자가 디지털 화면에서 볼 수 있도록 했습니다.
- 넷째, 참가자들은 자신의 아이디어를 명확히 밝히고 비슷한 아이디어를 결합할 수 있는 기회를 제공받았습니다.
- 다섯째, 모든 참가자는 숙련된 커뮤니케이터에게 가장 중요하다고 생각되는 특성을 기술한 7가지 아이디어를 개인적으로 선택하고 1점부터 7점(총 28점)까지 점수를 매겼으며, 7점이 가장 높은 점수를 받았습니다. 웹 기반 플랫폼인 Qualtrics(버전 XM; Qualtrics, 유타주 프로보: 2020)를 사용하여 익명으로 순위를 매기는 과정을 조정하고 보안을 유지했습니다.
- 마지막으로 참가자들은 총 순위에 대해 토론하여 그룹 합의를 도출했습니다. 진행자는 모든 참가자에게 돌아가면서 토론에 참여하도록 개별적으로 초대하고, 각 토론 라운드에서 참가자들이 아이디어와 의견을 공유할 수 있는 충분한 기회를 제공했으며, 최종 순위가 디지털 화면에 표시될 때 각 참가자에게 명시적인 합의를 요청했습니다. 그룹 합의에 도달하지 못한 경우 한두 차례에 걸쳐 순위를 다시 정하는 과정을 거쳤습니다. 그룹 합의는 그룹에서 생성된 특성의 총 순위에 대해 모든 참가자가 구두로 동의하는 것으로 정의되었습니다. 앞서 언급한 단계에 대한 자세한 개요는 부록 S1에서 확인할 수 있습니다.
The NGT sessions, ranging in time from 90 to 120 min, were audio-recorded and transcribed verbatim. All NGT sessions used the same protocol (Appendix S1) and were facilitated by two moderators, one educational researcher and psychologist (AT) and one PhD student and GP trainee (MV).35, 36 An additional researcher and health scientist (EG) was present during the sessions to observe and make field notes. The research team constructed the nominal question by performing a literature study and three semi-structured interviews with communication experts to assemble ideas from the current scientific discourse on skilled communication.29, 36, 37
- After a brief explanation of the sessions procedure, the following nominal question was posed: ‘What are characteristics of a skilled GP communicator?’ During the NGT sessions, we introduced characteristic as ‘a typical or noticeable feature describing a skilled communicator in the clinical encounter’.
- Second, in response to the nominal question, participants individually wrote down their ideas.
- Third, participants shared a single idea to the group in a ‘round robin’ fashion. One of the moderators transcribed all ideas in a word document, which was visible for all participants on the digital screen.
- Fourth, participants clarified their ideas and were provided with the opportunity to combine similar ideas.
- Fifth, all participants privately selected seven ideas, which described characteristics deemed most important for a skilled communicator and scored them from 1 to 7 (total of 28 points), 7 being the highest rank score. The web-based platform Qualtrics (version XM; Qualtrics, Provo, Utah: 2020) was used to coordinate and secure the anonymous ranking process.
- In the end, participants discussed the total ranking to reach group consensus. The moderators invited all participants individually to take part in the discussion by giving turns to all participants, providing sufficient opportunities for participants to share ideas and views during each round of discussion and asking explicit consensus from each participant when the final ranking was presented on the digital screen. If no group consensus was reached a re-ranking process occurred in one or two rounds. Group consensus was defined as a voiced agreement of all participants on the total ranking of characteristics generated by the group. A more detailed outline of the aforementioned steps is available (Appendix S1).
데이터 분석
Data analyses
모든 NGT 세션의 결과물은 양적, 질적으로 모두 분석되었습니다. 분석 결과 숙련된 커뮤니케이터의 특성과 임상에서 숙련된 커뮤니케이션 접근법의 개념적 모델을 파악할 수 있었습니다.
The output of all NGT sessions was analysed both quantitatively and qualitatively. The analyses resulted both in the identification of characteristics of a skilled communicator and a conceptual model of a skilled communication approach in the clinical encounter.
2.5.1 분석 접근법
2.5.1 Analysis approach
인구통계학적 변수는 Windows용 SPSS 26.0(IBM Corp. Armonk, NY)의 서술적 통계를 사용하여 분석했습니다. 설명적 통계를 사용하여 NGT 세션의 양적 구성 요소를 분석했습니다. NGT 세션의 내용은 5단계에 걸쳐 수행된 (반복되는) 주제를 식별, 분석 및 보고하는 주제별 내용 분석을 사용하여 분석했으며, 이는 흐름도(그림 1)에 설명되어 있습니다.38, 39
Demographic variables were analysed using descriptive statistics in SPSS 26.0 for Windows (IBM Corp. Armonk, NY). We analysed the quantitative components of the NGT sessions using descriptive statistics. The content of the NGT sessions was analysed using thematic content analysis by identifying, analysing and reporting (recurring) themes performed in five phases and is illustrated in the flow diagram (Figure 1).38, 39
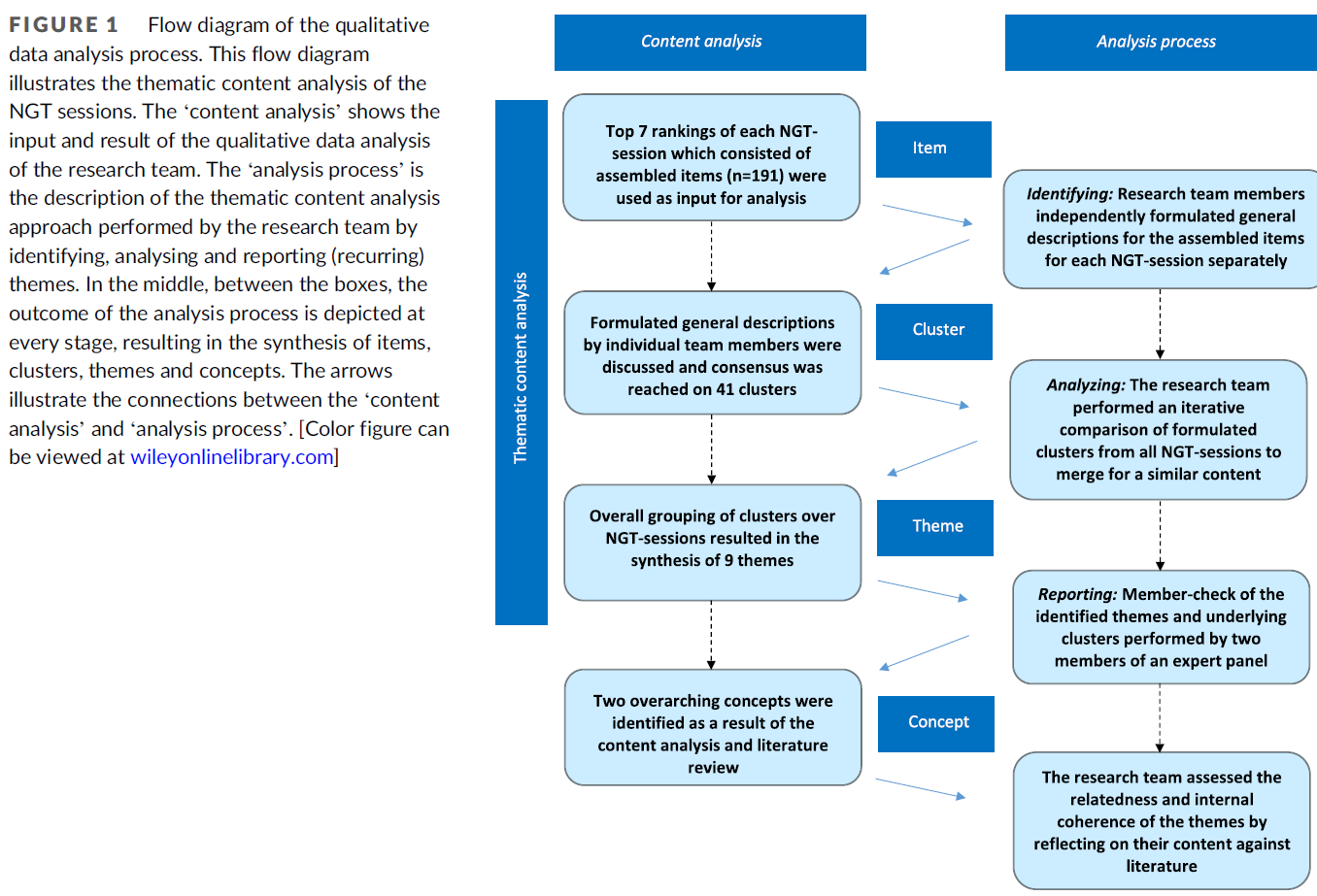
- 먼저, 연구팀원(MV, AT, EG)은 각 NGT 세션에 대해 개별적으로 조립된 항목에 대한 일반 설명을 독립적으로 작성했습니다(부록 S3 참조).
- 다음으로, 개별 팀원들이 작성한 일반적 설명을 연구팀이 합의에 도달할 때까지 논의하여 클러스터를 만들었습니다(부록 S4 참조).
- 셋째, 연구팀은 모든 NGT 세션에서 도출된 클러스터를 반복적으로 비교하여 유사한 내용을 병합하여 주제를 종합했습니다(부록 S5 참조).
- 넷째, 의사-환자 전문가 패널의 두 연구자(ML, VvdE)가 식별된 주제와 기본 클러스터에 대한 구성원 점검을 수행하여 모든 NGT 세션의 내용이 포함되었는지 평가하여 최종 주제 및 클러스터 목록을 도출했습니다.
- 마지막으로, 연구팀은 문헌에 대한 내용을 반영하여 테마의 관련성과 내부 일관성을 평가하여 개념을 식별했습니다(사용된 용어의 정의는 부록 S2 참조). 전문 번역가가 최종 주제와 클러스터를 영어로 번역한 후, 영어에 능통한 네덜란드 원어민 연구팀원이 다시 네덜란드어로 번역하여 번역의 정확성을 검증하고 연구팀 전체가 승인했습니다.
- First, research team members (MV, AT, EG) independently formulated general descriptions for the assembled items for each NGT-session separately (see Appendix S3).
- Next, these general descriptions by individual team members were discussed by the research team until consensus was reached, resulting in clusters (see Appendix S4).
- Third, the research team performed an iterative comparison of formulated clusters from all NGT sessions to merge for a similar content, resulting in the synthesis of themes (see Appendix S5).
- Fourth, two researchers (ML, VvdE) of a doctor–patient expert panel performed a member check of the identified themes and underlying clusters to assess if the content of all NGT sessions was covered, resulting in the final list of themes and clusters.
- Finally, the research team assessed the relatedness and internal coherence of the themes by reflecting on their content against literature, resulting in the identification of concepts (see Appendix S2 for definition of used terms). A professional translator translated the final themes and clusters into English, and then members of the research team as native Dutch speakers proficient in English translated them back into Dutch to verify the accuracy of the translations, which was approved by the whole research team.
반사성
Reflexivity
저희는 이 연구의 결과가 연구자와 참여자 간의 상호작용에 의해 공동으로 구성되었음을 인정합니다. 연구팀은 인구통계학적 특징(예: 여성, 백인, 국적)은 비슷했지만 의사-환자 커뮤니케이션 연구 및 교육과 관련된 전문 지식과 관점에는 다양성이 있었습니다. 일반의 수련의 및 박사 과정 학생(MV), 일반의 교육 기관에서 일하는 심리학자(AT), 학부 의료 교육 프로그램에서 일하는 커뮤니케이션 연구자 및 트레이너(EG), 자기조절 학습에 대한 연구 전문성을 갖춘 교육 심리학자(AdB) 등이 참여했습니다. 이러한 다양한 전문적 배경은 팀 토론에 깊이와 풍성함을 더했습니다. 편견을 방지하기 위해 연구팀 내에서 개별 데이터 분석 결과를 논의할 때 비판적인 입장을 견지했으며, 데이터의 의미를 도출하는 과정에서 다른 관점을 모색했습니다.40
We acknowledge that outcomes in this study are co-constructed by interactions between researchers and participants. While our research team was similar in terms of demographic features (i.e. female, white and nationality), there was diversity in expertise and perspectives related to doctor–patient communication research and training. A GP trainee and PhD student (MV), a psychologist working at a GP training institute (AT), a communication researcher and trainer working at a undergraduate medical training programme (EG) and an educational psychologist with research expertise in self-regulated learning (AdB). These different professional backgrounds provided depth and richness to the team discussions. To prevent biases, we kept critical of our stances in discussing findings from individual data analysis within the research team and explored alternative viewpoints during the process of making meaning of the data.40
3 결과
3 RESULTS
결과는 사회 인구학적 특성, NGT 세션 순위 결과를 설명하는 연구 특성, 주제별 내용 분석 결과 숙련된 커뮤니케이터의 특성, 숙련된 커뮤니케이션 접근 방식을 설명하는 개념적 모델 개발로 제시됩니다.
The results will be presented as socio-demographic characteristics, study characteristics describing the NGT session ranking results, characteristics of a skilled communicator as a result of thematic content analysis, and the development of a conceptual model describing a skilled communication approach.
사회 인구학적 특성
Socio-demographics characteristics
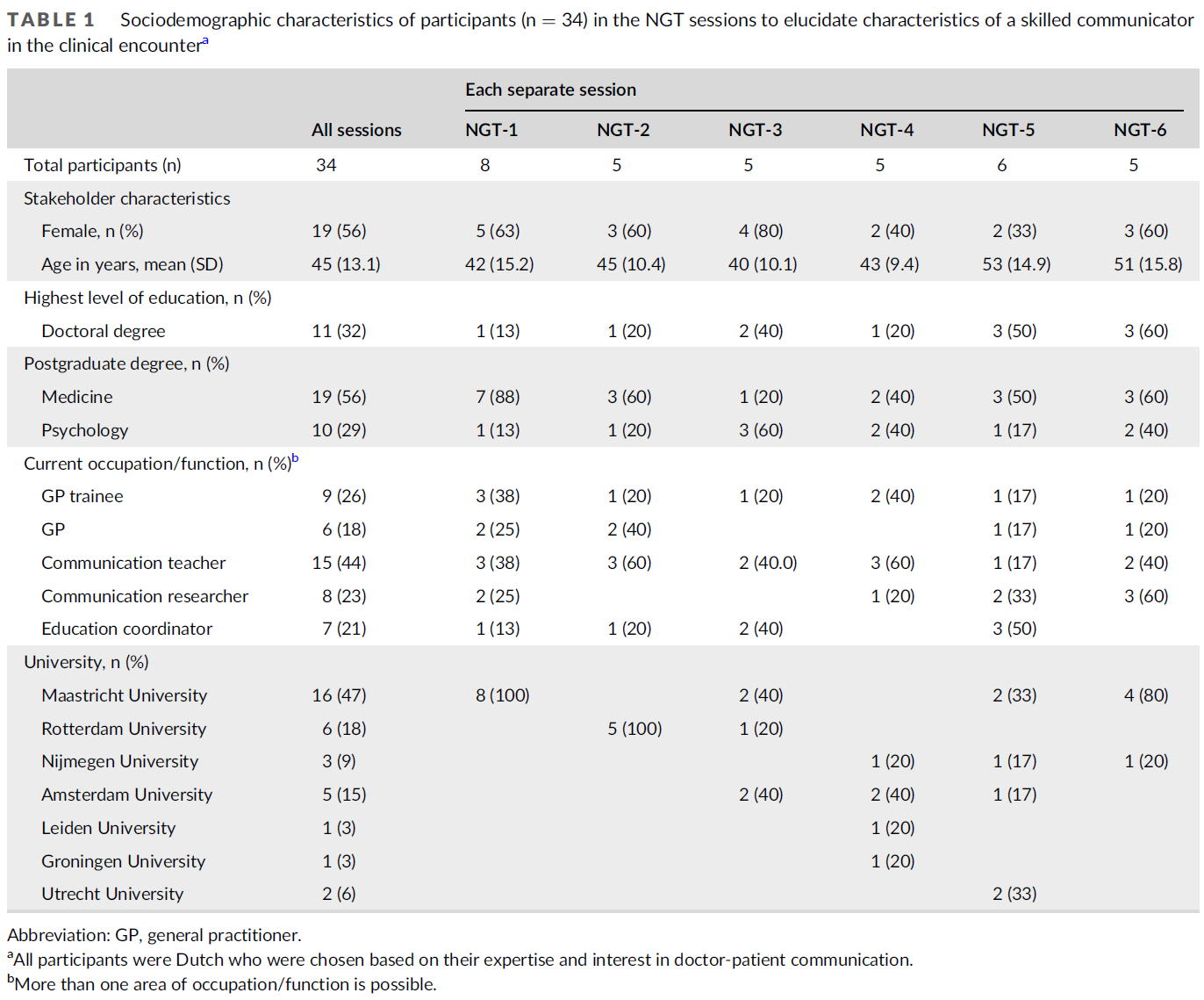
총 34명의 이해관계자가 6개의 NGT 세션 중 하나에 참여(응답률 48%)했습니다. 이해관계자의 연령은 26세에서 65세(평균 45세, SD 13.2세)였으며, 여성이 19명(56%)이었습니다. 표 1은 이해관계자의 특성 및 직업적 배경 구성에 대한 정보를 제공합니다.
A total of 34 stakeholders participated (response rate 48%) in one of the six NGT sessions. The stakeholders' ages ranged from 26 to 65 years (mean 45, SD 13.2 years), and 19 were female (56%). Table 1 provides information on stakeholders' characteristics and the composition of their professional backgrounds.
연구 특성
Study characteristics
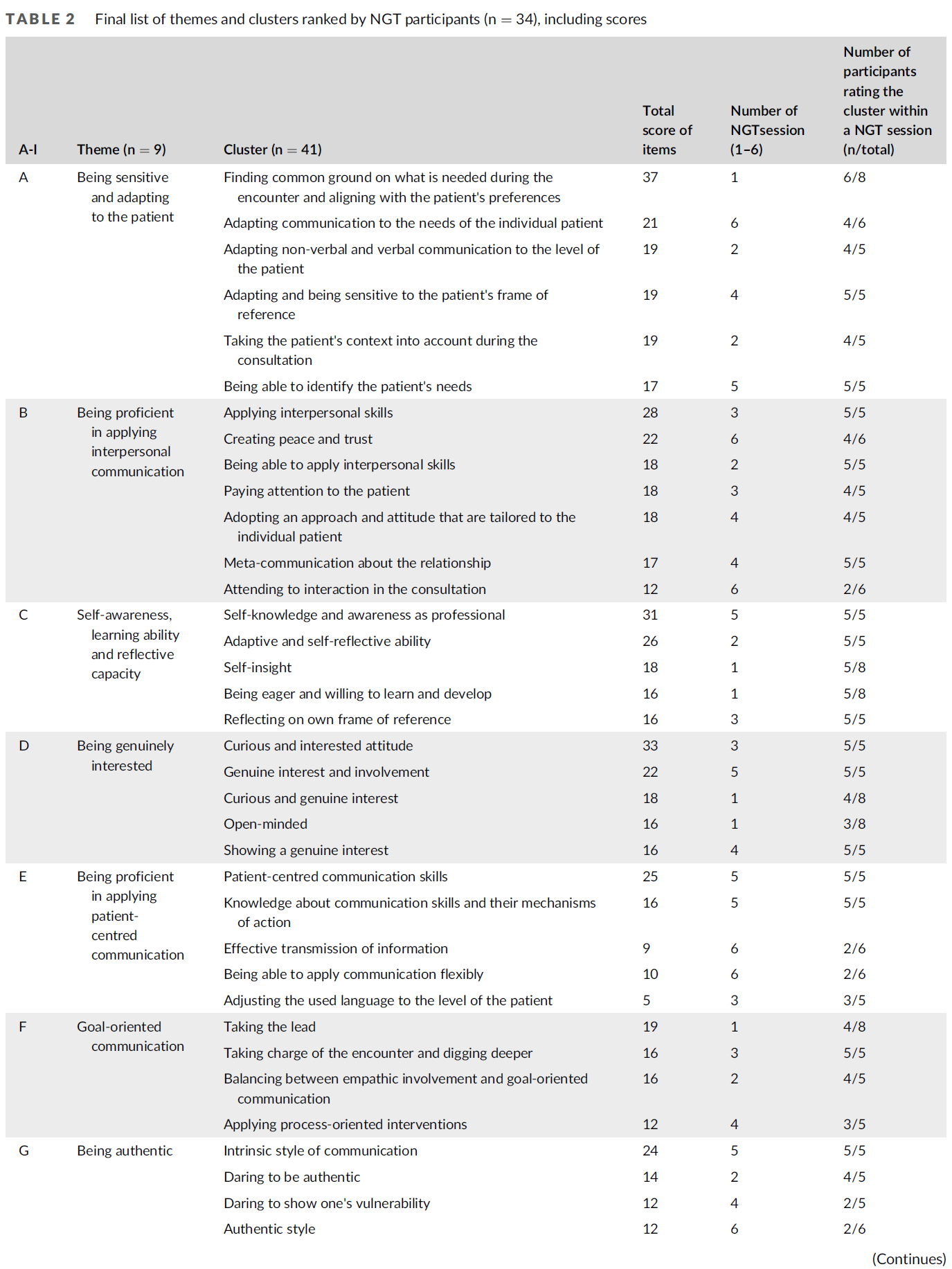
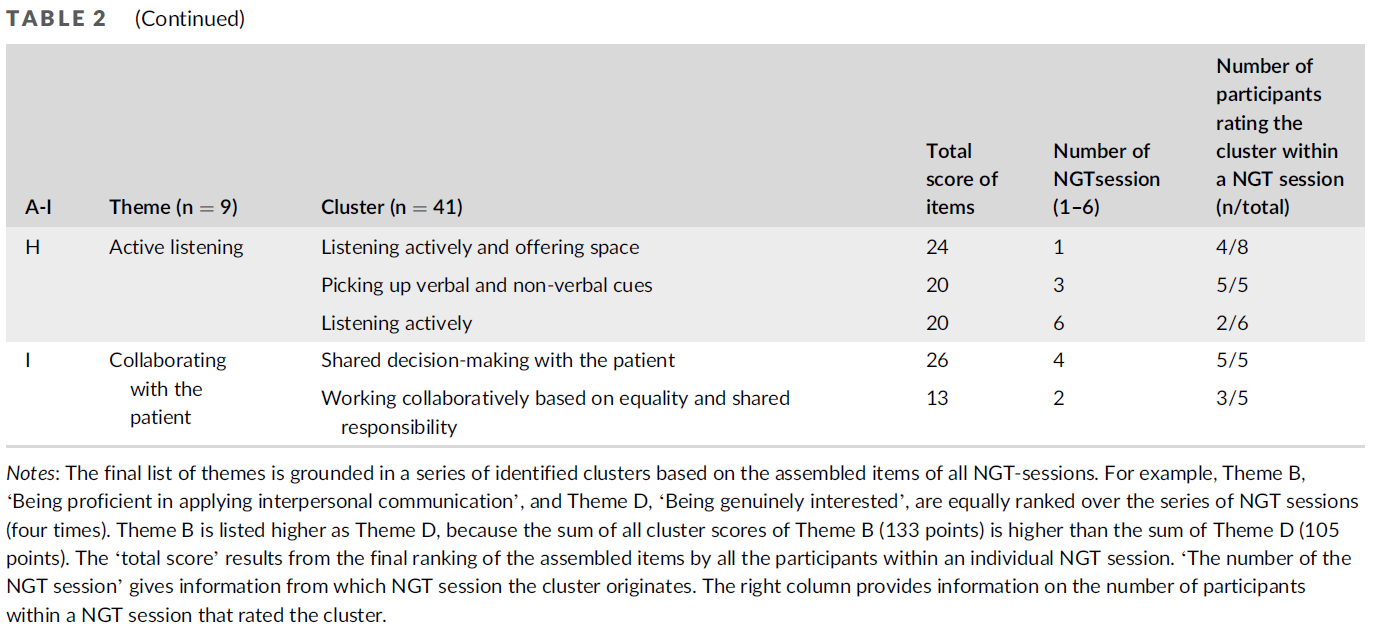
6번의 NGT 세션이 진행되었으며, 각 세션마다 참가자들이 NGT 세션에서 정리한 여러 항목(n = 191)으로 구성된 '상위 7가지 특성'(부록 S3 참조)이 도출되어 41개의 클러스터로 이어졌습니다. 질적 분석 결과, 숙련된 커뮤니케이터의 특성을 설명하는 9개의 테마가 도출되었습니다. 표 2는 주제와 해당 클러스터의 순위를 보여줍니다. 테마는 이러한 결합된 기준에 따라 나열되어 있습니다: (1) 일련의 NGT 세션에서 가장 높은 순위를 차지한 클러스터와 (2) 특정 테마 내의 모든 클러스터 점수의 합입니다.
Six NGT sessions were conducted, each resulting in its own ‘Top 7 of characteristics’ (see Appendix S3) consisting of multiple items (n = 191) that were organised by the participants during the NGT sessions, leading to 41 clusters. Qualitative analysis resulted in nine themes, describing characteristics of a skilled communicator. Table 2 shows the rankings of the themes and corresponding clusters. The themes are listed according to these combined criteria:
- (1) the clusters ranked the most often over the series of NGT sessions and
- (2) the sum of all cluster scores within a specific theme.
숙련된 커뮤니케이터의 특성
Characteristics of a skilled communicator
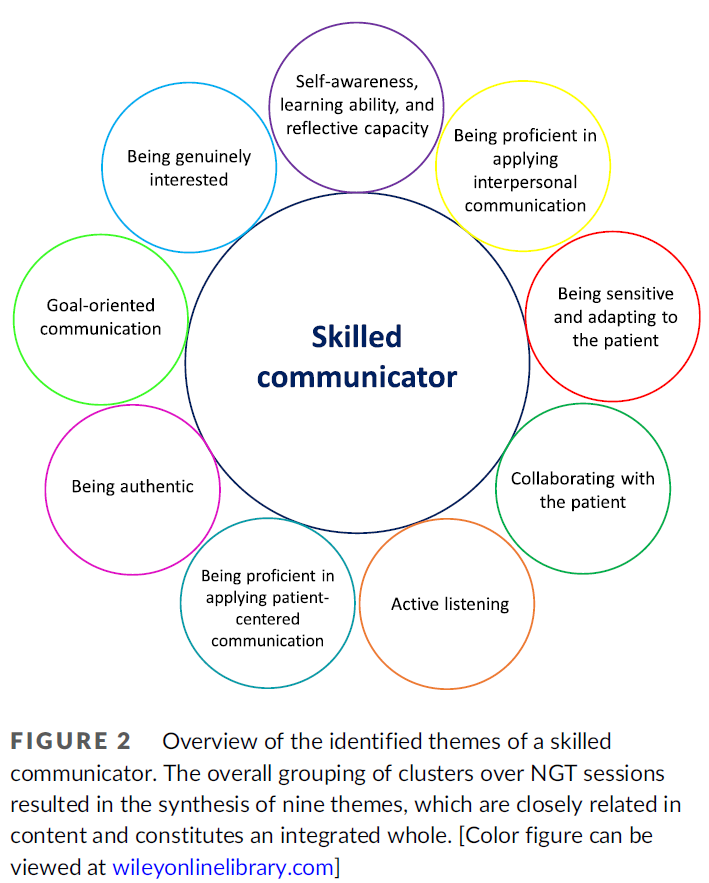
이 섹션에서는 숙련된 커뮤니케이터의 특성을 설명하는 식별된 주제를 그림 2에 설명된 내러티브로 개괄적으로 설명합니다. 주제는 참가자들이 순위를 매겨 조립한 항목에 대한 주제별 콘텐츠 분석의 결과로 식별됩니다.
In this section, the identified themes describing characteristics of a skilled communicator will be outlined and described as a narrative, which are illustrated in Figure 2. Themes are identified as a result of the thematic content analysis of the rank-ordered assembled items by the participants.
3.3.1 A: 환자에게 민감하고 적응하기
3.3.1 A: Being sensitive and adapting to the patient
5번의 NGT 세션 동안 '환자에게 민감하고 적응하기'라는 주제를 나열하고 점수를 매겼습니다. 이 주제는 환자의 경험과 요구에 민감하게 반응하는 것과 환자와의 언어적, 비언어적 의사소통을 조정하는 것으로 세분화할 수 있습니다. 또한, 공통점을 찾는 것은 환자와의 만남에서 무엇이 필요한지 민감하게 파악하고 그에 따라 의사소통을 조정하는 것으로 언급되었습니다.
During five NGT sessions, the theme ‘Being sensitive and adapting to the patient’ was listed and scored. It can be subdivided into being sensitive to the patient's experience, and needs and adjusting verbal and non-verbal communication to the patient. Moreover, finding common ground was mentioned as being sensitive to what is needed in the encounter and adapt communication accordingly.
3.3.2 B: 대인 커뮤니케이션을 능숙하게 적용하는 것
3.3.2 B: Being proficient in applying interpersonal communication
네 개의 NGT 세션에서 '대인 커뮤니케이션을 능숙하게 적용하기'라는 주제를 나열하고 점수를 매겼습니다. 센트럴은 대인 커뮤니케이션을 적용하는 방법을 알고 언제 상담에 적용해야 하는지 아는 측면에서 의사와 환자 간의 관계를 증진하는 대인 커뮤니케이션을 시연하고 있습니다. 이 주제에 따라 평화와 신뢰 형성, 완전한 존재감 드러내기, 충분한 시간 갖기, 희망과 현실 사이의 균형 잡기 등 다양한 목표와 기술이 보고되었습니다. 또한 참가자들은 대화 과정에 대해 상호적으로 논의하고 상호 기대치를 명확히 할 필요성에 대해 언급했습니다.
Four NGT sessions listed and scored the theme ‘Being proficient in applying interpersonal communication’. Central is demonstrating interpersonal communication fostering the relationship between doctor and patient, both in terms of knowing how to apply it and knowing when to apply it in the consultation. Under this theme, different objectives and skills were reported, for example: creating peace and trust, displaying full presence, taking sufficient time and balancing between hope and realism. In addition, participants mentioned the need to attend to reciprocity discuss the dialogical process and articulate mutual expectations.
3.3.3 C: 자기 인식, 학습 능력 및 반성적 역량
3.3.3 C: Self-awareness, learning ability and reflective capacity
'자기 인식, 학습 능력 및 반성적 역량'이라는 주제는 네 번의 NGT 세션에서 나열되고 채점되었습니다. 여기에는 규범과 가치, 경계, 함정, 의사소통 스타일에 대한 개인의 인식이 포함됩니다. 환자와 동료의 피드백에 개방적이고 자신의 의사소통의 단점을 성찰함으로써 자신의 관점이나 편견과 같은 개인적 기준 프레임에 대한 인식이 강화됩니다. 또한, 이 주제에서는 학습에 대한 의지, 즉 이전 경험을 바탕으로 다양한 커뮤니케이션 전략을 실험할 수 있는 성장 마인드가 언급되었습니다.
The theme ‘Self-awareness, learning ability and reflective capacity’ was listed and scored by four NGT sessions. It includes personal awareness of norms and values, boundaries, pitfalls and communication style. By being open for feedback from patients and colleagues and reflecting upon shortcomings in one's communication, performance awareness of own personal frame of reference (e.g. perspectives and prejudices) is fostered. Moreover, within this theme willingness to learn was mentioned: a growth mind-set, which enables experimenting with different communication strategies based upon prior experiences.
3.3.4 D: 진정으로 관심 갖기
3.3.4 D: Being genuinely interested
네 번의 NGT 세션에서 '진정으로 관심 갖기'라는 주제를 나열하고 점수를 매겼으며, 호기심을 보이는 태도를 통해 환자와 열린 대화를 나누는 것이 중요하다고 언급했습니다. 호기심을 갖고, 쉽게 접근하고, 비판적이지 않고, 열린 마음을 갖는 것이 필수적입니다.
Four NGT sessions listed and scored the theme ‘Being genuinely interested’ and to establish an open dialogue with the patient by displaying an attitude of curiosity. It is essential to be curious, easily accessible, non-judgmental and open-minded.
3.3.5 E: 환자 중심 커뮤니케이션을 능숙하게 적용하기
3.3.5 E: Being proficient in applying patient-centred communication
네 번의 NGT 세션 동안 '환자 중심 의사소통을 능숙하게 적용하기'라는 주제가 나열되고 점수가 매겨졌습니다. 이 주제는 의사소통 전략의 메커니즘과 잠재적 효과에 대한 지식과 효과적인 정보 교환 개발로 세분화할 수 있습니다. 의사는 상담 시 환자의 눈높이에 맞게 언어를 유연하게 조정하고, 질문과 설명을 구체적으로 하고 이해 여부를 확인해야 합니다.
During four NGT sessions, the theme ‘Being proficient in applying patient-centred communication’ was listed and scored. This theme can be subdivided into knowledge about the mechanisms and potential effects of communication strategies and developing an effective information exchange. In their consultations, doctors need to flexibly adjust their language to the level of the patient, being concrete in questioning and providing explanations and checking for understanding.
3.3.6 F: 목표 지향적 의사소통
3.3.6 F: Goal-oriented communication
네 번의 NGT 세션 동안 '목표 지향적 의사소통'이라는 주제를 나열하고 점수를 매겼습니다. 이는, 필요할 때마다, 환자와 의사 모두의 의제를 다루고 추가적인 주의가 필요한 문제와 불필요해 보이는 문제를 구분하기 위해 주도적으로 행동하는 것을 의미합니다. 시간 제한적 개입은 상담 과정에 관한 선택을 할 때 목표 지향적으로 일할 수 있도록 지원합니다. 동시에 분석적이고 깊이 탐구하는 자세는, 임상과 환자의 목표를 모두 고려하고 이를 연결하면서, 내용과 과정 사이의 균형을 맞출 수 있게 해줍니다.
During four NGT sessions, the theme ‘Goal-oriented communication’ was listed and scored. It means taking the lead, whenever it is necessary, to address the agenda of both patient and doctor and differentiate between issues that require additional attention and those that seem superfluous. Time-contingent interventions support goal-oriented working in making choices regarding the course of the consultation. Concomitantly, being analytic and exploring deeper enable balancing between content and process while taking into account both clinical and patients' goals and bridging them.
3.3.7 G: 진정성 확보하기
3.3.7 G: Being authentic
네 개의 NGT 세션에서 '진정성'을 주제로 선정하고 점수를 매겼습니다. 이는 의사소통 성과가 환자에게 거의 감지되지 않는다는 것을 의미합니다. 진정성 있는 방식으로 목표를 달성하면 자연스럽고 개인적인 스타일의 커뮤니케이션으로 이어집니다. 이를 위해서는 공감, 취약성, 그리고 필요한 경우 불안감에 대한 소통을 보여줘야 합니다.
Four NGT sessions listed and scored the theme ‘Being authentic’. It means that communication performance is almost imperceptible to the patient. Achieving goals in an authentic manner leads to a natural and personal style in communication. This necessitates showing empathy, vulnerability and communication about insecurities, if needed.
3.3.8 H: 적극적인 경청
3.3.8 H: Active listening
'적극적 경청'이라는 주제는 세 번의 NGT 세션에서 목록화되어 점수를 받았다. 경청 능력으로 묘사되었다.
- 환자가 자신의 이야기를 할 수 있는 여지를 만들고, 만남에서 환자의 단서와 환자가 강조하는 것에 대해 적극적으로 경청하며 (비)언어적 의사소통에 집중하는 것으로 설명되었습니다.
The theme ‘Active listening’ was listed and scored by three NGT sessions, which was described as the ability to listen:
- attentively and thereby creating room for patients to tell their story, and actively for patient cues in the encounter and what is stressed by the patient, and focus on (non-)verbal communication.
3.3.9 I: 환자와 협력하기
3.3.9 I: Collaborating with the patient
두 개의 NGT 세션에서 '환자와 협력하기'라는 주제를 나열하고 점수를 매겼습니다. 이는 의사와 환자가 투명성을 위해 노력하고 상호 계획에 도달하는 평등에 기반합니다. 다른 한편으로, 협업은 환자가 문제 해결의 공동 파트너가 되어 환자의 자율성을 높이고 공동 의사 결정을 내릴 수 있는 공동 책임에 기반합니다.
Two NGT sessions listed and scored the theme ‘Collaborating with the patient’. On the one hand, this is based on equality: doctor and patient striving towards transparency and reaching a mutual plan. On the other hand, working collaboratively is based on a shared responsibility where the patient becomes co-partner in problem solving enhancing the patients' autonomy and enabling to shared decision making.
숙련된 의사소통 접근법의 개념적 모델
Conceptual model of a skilled communication approach
이 개념적 모델(그림 3 참조)에서는 두 가지 순환적이고 중요한 프로세스가 실제 커뮤니케이션 행동과 커뮤니케이션에 대한 성찰의 중심이 됩니다. 이러한 작업을 수행하려면 다음과 같은 특성이 필요합니다. 의사는 첫 번째 과정인 의사소통에 민감해야 하며, 의사소통을 만남의 필요에 맞게 조정해야 합니다. 관찰된 의사소통 행동은 의사의 적용된 기술과 표시된 태도에 영향을 받습니다.
- 연구 결과에서 첫 번째 구성 요소는 대인 관계 및 환자 중심 커뮤니케이션을 적용하는 숙련도로 확인되었습니다. 또한, 능동적 경청은 고도로 숙련된 과정으로 확인되었으며, 이는 (대인관계 및 환자 중심) 의사소통을 적용하기 위한 조건부 도구로 볼 수 있습니다.41
- 두 번째 구성 요소인 태도적 측면은 진정성과 진정한 관심으로 확인되었으며 숙련된 커뮤니케이터의 핵심으로 간주됩니다. 이러한 태도적 측면은 임상적 만남에서 환자에게 민감하게 반응하고 의사소통을 조정하는 과정을 용이하게 합니다.
In this conceptual model (see Figure 3), two circular and overarching processes are central actual communication behaviour and reflection on communication. The following characteristics are needed to perform these tasks. The doctor needs to be sensitive and adapt communication to the needs of the encounter, which is the first process. The communication behaviour observed is influenced by applied skills and displayed attitudes of the doctor.
- The first component is identified in our findings as the proficiency to apply interpersonal and patient-centred communication. Moreover, the characteristic Active listening was identified as a highly skilled process, which could be seen as a conditional tool to apply (interpersonal and patient-centred) communication.41
- The second component, attitudinal aspects, are identified in as authenticity and genuine interest and considered as core for a skilled communicator. These attitudinal aspects facilitate the process of being sensitive and adapting communication to the patient in the clinical encounter.

또한 숙련된 커뮤니케이터가 환자와 협력하고 필요한 경우 주도권을 잡으면서 임상 진료 중에 목표를 조정할 수 있도록 하는 데 있어 기술과 태도는 조건적인 요소입니다. 이는 의사소통이 본질적으로 맥락적이고 목표 중심적이라는 점과 일맥상통합니다.14, 18, 28 또한, 상담에서 환자와 의사의 관련 목표를 다룰 때 상호 합의점을 찾는 것이 촉진됩니다.14 숙련된 커뮤니케이터는 또한 임상 진료 중 의사소통 과정을 스스로 모니터링할 수 있어야 하며, 이는 두 번째로 확인된 병행 과정과 일맥상통합니다: '자기 인식, 학습 능력 및 반성적 능력'과 일치합니다.42, 43
Skills and attitudes are also conditional in enabling a skilled communicator to adjust goals during the clinical encounter while working collaboratively with a patient and taking the lead if needed. This resonates with communication being inherently contextual and goal driven.14, 18, 28 Furthermore, finding mutual agreement is fostered in addressing both patients' and doctors' related goals in the consultation.14 A skilled communicator should also be able to self-monitor communication processes during the clinical encounter, which resonates with the second identified parallel process: ‘self-awareness, learning ability, and reflective capacity’.42, 43
4 논의
4 DISCUSSION
이 연구의 목적은 의료 커뮤니케이션 분야의 다양한 이해관계자의 관점을 종합하여 숙련된 커뮤니케이션의 개념을 알리는 것이었습니다. 6차례에 걸쳐 진행된 NGT 세션에 참여한 이해관계자들은 총 191개의 항목을 종합적으로 해명했습니다. 이러한 결과를 주제별 내용 분석에 사용하여 임상 현장에서 숙련된 커뮤니케이터의 특성을 설명하는 9가지 주제를 식별했습니다.
- (A) 환자에 대한 민감성과 적응력,
- (B) 대인 커뮤니케이션 적용에 능숙함,
- (C) 자기 인식, 학습 능력 및 성찰 능력,
- (D) 진정으로 관심 있음,
- (E) 목표 지향적 커뮤니케이션,
- (F) 진정성,
- (G) 환자 중심 커뮤니케이션 적용에 능숙함,
- (H) 적극적인 경청,
- (I) 환자와 협력하는 것
식별된 주제는 각 특성이 의사의 개인 레퍼토리의 일부이며 통합된 전체를 구성하기 때문에 내용상 밀접한 관련이 있습니다.9, 14, 16, 44
The purpose of this study was to inform the concept of skilled communication by synthesising viewpoints from different stakeholders in the field of medical communication. Stakeholders participating in the six conducted NGT sessions collectively elucidated 191 items. We used these findings in a thematic content analysis and identified nine themes, describing characteristics of a skilled communicator in the clinical encounter:
- (A) being sensitive and adapting to the patient;
- (B) being proficient in applying interpersonal communication;
- (C) self-awareness, learning ability and reflective capacity;
- (D) being genuinely interested;
- (E) goal-oriented communication;
- (F) being authentic;
- (G) being proficient in applying patient-centred communication;
- (H) active listening; and
- (I) collaborating with the patient.
The identified themes are closely related in content as each characteristic is part of the doctor's personal repertoire and constitutes an integrated whole.9, 14, 16, 44
또한, 확인된 주제를 바탕으로 (1) 환자에 대한 민감성과 적응력, (2) 자기 인식, 학습 능력, 반성적 능력이라는 두 가지 병렬 프로세스를 추출할 수 있고 임상에서 핵심이 되는 숙련된 의사소통 접근법의 개념적 모델을 개발했습니다. 이 모델은 전문적 성과를 모니터링하고 조절하는 넬슨과 나렌스(1990)의 이론적 모델에서 설명하는 순환 과정과 일치합니다.42, 45
Moreover, based on the identified themes, we developed a conceptual model of a skilled communication approach in which two parallel processes could be distilled and are key in the clinical encounter:
- (1) being sensitive and adapting to the patient and
- (2) self-awareness, learning ability and reflective capacity.
This model is concordant with the circular processes described by the theoretical model of Nelson and Narens (1990) of monitoring and regulating professional performance.42, 45
연구 질문에 비추어 볼 때, 의사 소통 행동은 임상적 만남의 필요에 민감하게 반응하고 의사소통을 조정함으로써 조절되며, 이는 환자 중심의 상담 결과에 도달하기 위해서는 의사 행동 적응성(PBA)이 필수적이라고 제안한 Carrard 등의 문헌에 의해 뒷받침됩니다. 의사가 환자의 선호도를 정확하게 해석하고 그에 따라 커뮤니케이션 행동을 조정할 수 있을 때 PBA가 달성됩니다.46 숙련된 커뮤니케이터는 임상 상담의 필요에 따라 다양한 커뮤니케이션 전략을 적응적으로 적용해야 한다는 점에서 PBA는 우리의 연구 결과를 반영합니다.46
In reflecting on our research question, communication behaviour is regulated through being sensitive and adapting communication to the needs of the clinical encounter, which is supported in literature by Carrard et al, who suggest that doctor behavioural adaptability (PBA) is essential to reach patient-centred consultation outcomes. PBA is achieved if the doctor is able to correctly interpret patients' preferences and adapt communication behaviour accordingly.46 PBA mirrors our findings in that a skilled communicator should apply different communication strategies adaptively in response to the needs of the clinical encounter.46
결과적으로 숙련된 커뮤니케이터는 임상 진료 중 의사소통 과정을 스스로 모니터링할 수 있어야 하며, 이는 두 번째로 확인된 병행 과정인 자기 인식, 학습 능력 및 반성적 역량과도 일치합니다. 의사는 의사소통 수행을 평가할 때 진료 중 내면의 생각과 감정을 모니터링하는 것이 필수적입니다.47 이 두 번째 과정과 일치하는 개념은 Hall과 Mast가 소개한 대인관계 정확성입니다.47 대인관계 정확성은 환자의 비언어적 및 단서에 민감하여 환자의 감정, 요구, 의도를 정확하게 인식하는 능력으로 설명됩니다.46, 47
Subsequently, a skilled communicator should also be able to self-monitor communication processes during the clinical encounter, which resonates with the second identified parallel process: self-awareness, learning ability and reflective capacity. Essential is that the doctor monitors internal thoughts and feelings during the encounter in evaluating communication performance.47 In line with this second process is the concept of interpersonal accuracy, introduced by Hall and Mast.47 Interpersonal accuracy is described as the ability to accurately perceive patients' feelings, needs, and intentions by being sensitive to patients' non-verbal and cues.46, 47
의료 교육에서 일상적 전문성과 적응적 전문성을 개발하는 것의 차이는 임상 상황에서 자기 인식, 학습 능력 및 성찰 능력을 병행 과정으로 파악하는 것으로 설명할 수 있습니다.48
- 일상적 전문성을 보이는 의사는 익숙한 임상 상황에서 의사소통할 때는 능숙하지만, 미지의 예상치 못한 상황으로 자신의 성과를 이전하는 데 어려움을 겪을 수 있습니다.48-51 에릭슨의 전문성 습득 모델에서 볼 수 있듯이 이러한 의사소통은 안정되고 자동적이고 쉽게 실행되는 수준에 도달하게 됩니다.22 그 결과 의사소통이 환자의 요구에 유연하게 적응하지 못합니다.21, 48, 52
- 반면 적응적 전문성을 보이는 의사는 모든 임상 상황에서 창의적이고 혁신적인 방식으로 의사소통 행동을 조정할 수 있습니다.22, 53 적응적 전문성에 도달하려면 의도적인 연습에 기반한 상황 학습이 핵심이며 성찰과 피드백이 개인 개발을 이끄는 수단이라고 Eraut는 지적합니다.20, 21, 48
The differentiation between developing routine and adaptive expertise in medical training may explain identifying self-awareness, learning ability and reflective capacity as a parallel process in the clinical encounter.48
- Doctors demonstrating routine expertise are proficient when communicating in a familiar clinical situation but may have difficulties in transferring their performance to unknown and unexpected situations.48-51 As Ericsson's model of expertise acquisition shows, this communication will become stable and will reach a level of automaticity and effortless execution.22 This results in communication not becoming flexibly adapted to patient needs.21, 48, 52
- In contrast, doctors demonstrating adaptive expertise are able to tailor their communication behaviour in a creative and innovative manner in every clinical situation.22, 53 To reach adaptive expertise, Eraut indicates that situated learning based on deliberate practice is key and reflection and feedback are vehicles to steer personal development.20, 21, 48
의료 교육에서는 학습자가 자신의 학습 과정에 능동적으로 참여할 수 있도록 성과에 대한 자기 인식을 촉진하는 학습자 중심 접근법을 촉진하는 데 중점을 두어야 하며, 이를 통해 진료 현장에서 환자의 요구에 맞게 의사소통을 조정할 수 있고, 궁극적으로 개인의 발전을 촉진할 수 있습니다.9, 10, 16, 44, 53-55 그리고 이후 성찰과 정기적인 피드백을 통해 자신의 생각과 느낌을 모니터링합니다.20, 42
In medical training, emphasis should be on facilitating a learner-centred approach to promote self-awareness of performance for learners to become actively involved in their own learning process, which enables them to adapt communication to patient needs in the encounter, and eventually fosters their personal development,9, 10, 16, 44, 53-55 and, subsequently, monitor their own thoughts and feelings by reflection and regular feedback.20, 42
학습은 실제 임상 환경에서 구성되며, 학습자는 이러한 환경이 학습자에게 영향을 미치기 때문에 이 환경에 적극적으로 영향을 미치는데, 이를 경험적 학습 '현장 학습'이라고도 합니다.20, 56 학습자의 필요와 학습 목표에 따라 학습자가 자신의 개인적인 의사소통 스타일(예: 진정성, 진정한 관심)을 개발하도록 안내하고 학습자의 개인적 발전을 촉진하려면 교육이 종적 지향적이며 적극적인 지원과 안내된 성찰을 제공하는 것이 필수적입니다.56-58
Learning is constructed from the authentic clinical setting, and learners actively influence this setting as this same setting influence learners, also known as experiential learning ‘learning on the job’.20, 56 To guide learners in their needs and learning goals to develop their own personal communication style (e.g. authentic, genuine interested), fostering the personal development of learners, it is essential that training is longitudinal oriented and provides active support and guided reflections.56-58
시사점
Implications
커뮤니케이션 교육 및 연구를 위한 권장 사항을 공식화할 수 있습니다. 이 개념적 모델은 숙련된 커뮤니케이션 학습을 위한 템플릿으로 사용할 수 있는 식별된 특성을 뒷받침합니다. 의사소통 훈련은 임상 현장에서 의사소통에 대한 반복적인 실험을 촉진하고 의사소통 수행에 대한 체계적인 성찰을 지원하여 숙련된 의사소통의 전문성을 확보할 수 있도록 해야 합니다. 이를 통해 학습자는 학습 목표를 설정하고 학습 활동을 계획하는 데 있어 학습 과정을 능동적으로 이끌어갈 수 있으며, 개인의 발전을 촉진할 수 있습니다.9, 16, 21, 47
Recommendations can be formulated for communication training and research. The conceptual model underpins the identified characteristics that may be used as a template for learning skilled communication. Communication training should facilitate repeated experimentation with communication in the clinical encounter and support systematic reflection on communication performance to attain expertise in skilled communication. This may enable learners to actively steer their learning processes in setting goals and planning learning activities, stimulating their personal development.9, 16, 21, 47
또한, 우리의 개념 모델은 숙련된 커뮤니케이션을 운영하며 학습자가 숙련된 커뮤니케이터가 되기 위해 개발해야 하는 두 가지 중요하고 순환적인 프로세스를 설명합니다. 교육은 학습을 평생의 연속체로 생각하고 학습자가 실제 임상 환경에서 접하는 경험에 의미를 부여할 수 있도록 학습자를 적극적으로 지원해야 합니다.20, 56, 57 향후 연구에서는 확인된 숙련된 의사소통 접근법이 임상 업무 환경 학습 중에 어떻게 최적으로 지원될 수 있는지 탐구해야 합니다.
Moreover, our conceptual model operationalises skilled communication and describes two overarching and circular processes learners need to develop to become skilled communicators. Training requires the need to actively support learners as learning is to be thought of as a lifelong continuum and help learners to make meaning of the experiences they encounter in the authentic clinical setting.20, 56, 57 Future research should explore how the identified skilled communication approach can be optimally supported during clinical workplace learning.
강점 및 한계
Strengths and limitations
이번 연구 결과는 강점과 한계를 고려하여 해석해야 합니다. 강점은 다음과 같습니다:
- (1) 상대적으로 많은 이해관계자 그룹이 다차원적 개념을 세분화하여 총체적인 복잡성을 파악하는 과정에서 광범위한 숙련된 의사소통 특성을 생성했다는 점,
- (2) 다양한 참여 이해관계자(예: GP, GP 수련의, 교수진 및 연구자)가 있었다는 점,
- (3) 다수의 NGT 세션이 식별된 특성의 일반화 가능성을 높였다는 점 등이 있습니다.
Our findings should be interpreted considering the strengths and limitations present. The strengths include:
- (1) a relatively large group of stakeholders generated an extensive number of skilled communication characteristics during the process of breaking down a multidimensional concept to get to grips on its holistic complexity,
- (2) the variety of participating stakeholders (i.e. GPs, GP trainees, faculty members and researchers) and
- (3) multiple NGT sessions increasing the generalisability of the identified characteristics.
또한 한계도 알고 있습니다.
- 첫째, 코로나19 팬데믹으로 인해 세션이 전자 환경에서 진행되었기 때문에 직접 눈을 마주치지 않고 비언어적 제스처를 취하는 데 어려움이 있을 수 있습니다.54 그러나 NGT 방식은 구조화된 템플릿을 채택하고 진행자가 세션 중 모든 참가자를 개별적으로 초대하여 토론에 참여하도록 했습니다. 따라서 이러한 한계가 연구 결과에 영향을 미치지는 않았을 것으로 예상합니다.
- 둘째, 우리는 본질적으로 복잡하고 다차원적인 개념을 매핑하려고 시도했고, NGT 방법은 풍부한 데이터를 생성했기 때문에 참가자들이 데이터를 개념적으로 심층적으로 탐색할 수 없었다는 점을 알고 있습니다.
- 셋째, 이 연구의 초점은 앵글로색슨 국가의 의료 환경과 특히 GP 교육 프로그램에 맞춰져 있었습니다. 이러한 환경과 이에 대한 사람들의 인식은 국가마다 다를 수 있다는 점을 알고 있습니다. 반면, 네덜란드의 8개 GP 수련 기관 중 5개 기관의 참가자를 포함했기 때문에 연구가 수행된 환경이 강점이라고 생각합니다. 비슷한 교육 시스템과 역량 프레임워크를 고려할 때 본 연구 결과는 다른 앵글로색슨 국가의 의료 교육 및 의료 환경에 일반화할 수 있을 것으로 기대합니다.
- 마지막으로, 본 연구는 의사-환자 커뮤니케이션 교육 영역에서 의료 전문가와 교육자의 관점을 규명하는 데 중점을 두었기 때문에 환자를 포함하지 않은 것은 본 연구의 한계로 볼 수 있습니다.
We are also aware of limitations.
- First, due to the COVID-19 pandemic, the sessions were held in an electronic environment, which can be a challenge due to, for example, the absence of direct eye contact and non-verbal gestures.54 However, the NGT method adopts a structured template and the moderators invited all participants individually to take part in the discussion during the sessions. Therefore, we expect that this limitation did not alter our findings.
- Second, we realise that we have tried to map a concept that is complex and multidimensional in nature, and the NGT method generated a richness of data, which does not enable participants to explore the data in-depth conceptually.
- Third, the focus of this study was on health care settings of Anglo-Saxon countries and on the GP training programme in particular. We are aware that the setting, and people's perceptions thereof, may differ across countries. On the other hand, we consider the setting in which the study was performed a strength as we included participants from five out of eight GP training institutes in the Netherlands. We expect the outcomes of our study to be generalisable to medical training and health care settings in other Anglo-Saxon countries, given comparable educational systems and their competency frameworks.
- Finally, not including patients can be seen as a limitation of this study as we decided to exclude patients as our focus is on elucidating the perspectives of health care professionals and educators within the domain of training doctor–patient communication.
결론
Conclusion
이번 연구 결과는 숙련된 커뮤니케이터의 특성을 밝히고 숙련된 커뮤니케이션 접근 방식을 개념화했으며, 이는 개념적 모델에 요약되어 있습니다. 임상 현장에서 숙련된 의사소통의 전문성을 갖추기 위해서는 (1) 환자에 대한 민감성과 적응력, (2) 자기 인식, 학습 능력, 반성적 역량이라는 두 가지 과정이 병행되어야 합니다. 전문성을 갖추기 위해서는 환자의 요구와 목표에 맞게 커뮤니케이션을 조정하고 임상 진료 중 커뮤니케이션 과정을 지속적으로 모니터링하는 방법을 배우는 것이 상호 의존적입니다. 개념 모델에 제시된 식별된 특성은 의사가 숙련된 커뮤니케이터가 될 수 있도록 지원하는 학습자 중심 접근법을 개발하는 데 도움이 될 수 있으며, 이는 의료 교육에서 직장 학습을 하는 동안에도 마찬가지입니다. 이는 교육에서 학습자의 학습 과정을 적극적이고 종적으로 안내하여 개인 개발을 촉진할 필요가 있음을 의미합니다.
Our findings elucidate characteristics of a skilled communicator and conceptualise a skilled communication approach, which is outlined in a conceptual model. Two parallel processes are essential to attain expertise in skilled communication in the clinical encounter: (1) being sensitive and adapting to the patient and (2) self-awareness, learning ability and reflective capacity. To attain expertise, learning to adapt communication to patients' needs and goals and continuously monitor communication processes during the clinical encounter are interdependent. The identified characteristics laid out in the conceptual model may inform the development of a learner-centred approach in supporting doctors to become skilled communicators, during workplace learning in medical training. For training, this implies the need to actively and longitudinally guide learners in their learning processes to facilitate personal development.
Identifying characteristics of a skilled communicator in the clinical encounter
PMID: 36223270
DOI: 10.1111/medu.14953
Abstract
Background: In medical communication research, there has been a shift from 'communication skills' towards 'skilled communication', the latter implying the development of flexibility and creativity to tailor communication to authentic clinical situations. However, a lack of consensus currently exists what skilled communication entails. This study therefore aims to identify characteristics of a skilled communicator, hereby contributing to theory building in communication research and informing medical training.
Method: In 2020, six nominal group technique (NGT) sessions were conducted in the context of the general practitioner (GP) training programme engaging 34 stakeholders (i.e. GPs, GP residents, faculty members and researchers) based on their experience and expertise in doctor-patient communication. Participants in each NGT session rank-ordered a 'Top 7' of characteristics of a skilled communicator. The output of the NGT sessions was analysed using mixed methods, including descriptive statistics and thematic content analysis during an iterative process.
Results: Rankings of the six sessions consisted of 191 items in total, which were organised into 41 clusters. Thematic content analysis of the identified 41 clusters revealed nine themes describing characteristics of a skilled communicator: (A) being sensitive and adapting to the patient; (B) being proficient in applying interpersonal communication; (C) self-awareness, learning ability and reflective capacity; (D) being genuinely interested; (E) being proficient in applying patient-centred communication; (F) goal-oriented communication; (G) being authentic; (H) active listening; and (I) collaborating with the patient.
Conclusions: We conceptualise a skilled communication approach based on the identified characteristics in the present study to support learning in medical training. In a conceptual model, two parallel processes are key in developing adaptive expertise in communication: (1) being sensitive and adapting communication to the patient and (2) monitoring communication performance in terms of self-awareness and reflective capacity. The identified characteristics and the conceptual model provide a base to develop a learner-centred programme, facilitating repeated practice and reflection. Further research should investigate how learners can be optimally supported in becoming skilled communicators during workplace learning.
© 2022 The Authors. Medical Education published by Association for the Study of Medical Education and John Wiley & Sons Ltd.