CanMEDS 2025의 지구보건(Can Med Educ J.2023) Planetary Health in CanMEDS 2025
소개 Introduction
기후 비상사태가 건강에 미치는 악영향이 점점 더 분명해지고 있습니다. 최근의 문헌 검토에 따르면 지구 보건은 CanMEDS 의사 역량 프레임워크와 관련된 진화하는 개념으로 확인되었습니다.1 의사 역량의 맥락에서 지구 보건은 기후 비상사태에 대한 의료의 영향과 기후 비상사태가 환자 치료에 미치는 영향을 최소화하는 데 관심을 두고 있습니다. 이 원고는 CanMEDS에 지구 보건 관련 내용을 포함하는 것이 얼마나 중요한지 밝히고, 지구 보건 개념을 예시하기 위해 향후 CanMEDS를 반복할 수 있는 기회를 제안하는 것을 목표로 합니다. The worsening impact of the climate emergency on health is increasingly apparent. A recent literature review identified Planetary Health as an evolving concept that is relevant to the CanMEDS physician competency framework.1In the context of physician competencies, planetary health is concerned with minimizing the impact of healthcare on the climate emergency and the impact of the climate emergency on patient care. This manuscript aims to establish the critical importance of including planetary health links in CanMEDS and to propose opportunities for future iterations of CanMEDS to exemplify planetary health concepts.
행성 건강이란 무엇이며 의사의 역량에 중요한 이유는 무엇인가요? What is planetary health and why is it important to physician competency?
지구 보건 연합은 지구 보건을 "지구의 자연 시스템에 대한 인간의 교란이 인간 건강과 지구상의 모든 생명체에 미치는 영향을 분석하고 해결하는 데 초점을 맞춘 솔루션 중심의 초학제적 분야이자 사회 운동"이라고 정의합니다.2 지구 보건은 기후 비상사태와 토지 파괴, 생물 다양성 손실, 오염 등 기타 생태 위기를 모두 다룹니다.3 기후 비상사태는 금세기 인류 생명에 가장 큰 건강 위협으로 여겨지며 2030년부터 매년 25만 명이 추가로 사망할 것으로 예측됩니다.4 The Planetary Health Alliance defines planetary health as “a solutions-oriented, transdisciplinary field and social movement focused on analyzing and addressing the impacts of human disruptions to Earth’s natural systems on human health and all life on Earth.”2Planetary health addresses both the climate emergency and other ecological crises, including land destruction, biodiversity loss, and pollution.3The climate emergency is considered the greatest health threat to human life this century, with predictions of 250,000 additional deaths per year from 2030 onward.4
캐나다 사람들의 건강은 이미 기후 비상사태의 영향을 받고 있습니다.5
2021년에는 섭씨 1.2도의 온난화로 브리티시컬럼비아주(B.C.주)의 열돔 현상으로 700명 이상이 사망했고,6
매니토바와 서스캐처원주의 가뭄으로 농작물이 실패하여 식량 가격이 상승했으며,7
홍수로 B.C.와 뉴펀들랜드의 지역사회 전체가 사라졌고,8
산불이 캐나다 서부9와 온타리오 북부 대부분을 휩쓸고 지나갔습니다.10
극심한 날씨로 인해 주요 인프라가 손상되고 공급망이 중단되면서 의료 서비스 제공에도 차질이 빚어지고 있습니다.11
기후 비상사태는 캐나다 전역의 원주민 건강에 불균형적인 영향을 미치고 있으며,12
환경 파괴는 전통적인 생활 방식을 위협하고 지속적인 식민지화 및 토지 박탈 과정을 악화시키고 있습니다.13
The health of people in Canada is already affected by the climate emergency5:
in 2021, at just 1.2 degrees Celsius of warming, over 700 people died in British Columbia's (B.C.) heat dome event,6
crops failed in Manitoba and Saskatchewan droughts contributing to rising food prices,7
flooding took out entire communities in B.C. and Newfoundland,8and
wildfires engulfed large parts of western Canada9and northern Ontario.10
Healthcare service delivery is also being increasingly disrupted as extreme weather damages critical infrastructure and interrupts supply chains.11
The climate emergency has a disproportionate impact on the health of Indigenous populations across Canada,12
as environmental destruction threatens traditional lifestyles and exacerbates ongoing processes of colonization and land dispossession.13
보건 부문은 이 문제에 크게 기여하고 있습니다. 캐나다 보건 부문은 지구상에서 두 번째로 탄소 집약적인 의료 시스템으로,4 캐나다 온실가스 배출량의 4.6%를 차지하며 이는 캐나다의 항공 산업과 동등한 수준입니다.14영국 국민보건서비스의 모델링에 따르면 배출량의 거의 70%가 의약품, 장비 및 공급망의 기타 측면에서, 10%가 여행에서, 10%가 건물 에너지에서, 5%가 물과 폐기물에서, 5% 전체가 마취 가스 및 용량 측정 흡입기(15)에서 발생한다고 합니다. 연방 정부는 다른 국가들과 함께 기후에 탄력적인 저탄소 의료 시스템을 제공하겠다고 약속했으며, 이러한 전환이 이루어지려면 의사들의 상당한 지지가 필요합니다.16 지속 가능한 의료 모델이 개발되었으며, 이를 실행해야 할 것입니다. 지속 가능한 의료 시스템을 위한 이러한 프레임워크 중 하나는 세 가지 범주의 개입을 제안합니다.17
건강의 사회적 결정요인을 해결하고 건강 증진 및 질병 예방에 참여함으로써 의료 서비스 수요를 줄인다.
의료 서비스 공급을 수요에 맞춰 적절한 치료를 보장하고 불필요한 검사 및 치료를 피한다.
의료 서비스 공급으로 인한 탄소배출을 줄인다.
The health sector is a significant contributor to the problem. The Canadian health sector is the second most carbon-intensive health care system on the planet,4contributing 4.6% of Canada’s greenhouse gas emissions—on par with the country’s aviation industry.14Modelling from the National Health Service in the United Kingdom suggests that nearly 70% of emissions come from medicines, equipment, and other aspects of the supply chain; 10% comes from travel; 10% comes from building energy; 5% from water and waste; and a full 5% from anesthetic gases and Metered Dose Inhalers (15). The federal government, together with other countries, has pledged to deliver a climate-resilient, low-carbon health care system, and significant advocacy from physicians will be required to ensure this transformation occurs.16Models of sustainable healthcare have been developed and will need to be implemented. One such framework for sustainable health systems proposes three categories of intervention:
reduce demand for health services by addressing the Social Determinants of Health and engaging in health promotion and disease prevention;
match the supply of health services to demand, ensuring appropriate care and avoiding unnecessary tests and treatment; and
reduce emissions from the supply of health services.17
존경받는 목소리로서 의사는 지구의 건강과 기후 비상사태에서 고유한 역할을 수행해야 합니다.18 의사는 지구 건강을 위한 옹호자가 될 준비가 되어 있어야 합니다. 의사는 미시적(환자), 중시적(진료소, 병원, 지역사회), 거시적(정책) 수준에서 행동할 수 있습니다.19 의사는 기후 행동 및 완화를 옹호하고 의료에 기후 회복력을 구축할 수 있습니다.11,17 의과대학부터 평생 의학 교육을 통해 지구 건강 및 옹호에 대한 교육을 개선하여 의사가 기후 비상사태에서 진료할 수 있도록 준비시켜야 할 것입니다. As respected voices, physicians have a unique role to play in planetary health and the climate emergency.18They must be prepared to be advocates for planetary health. Physicians can act at the micro (patient) level, meso (clinic, hospital, community) level, and macro (policy) level.19Physicians can advocate for climate action and mitigation and build climate resilience into healthcare.11,17Improved training in planetary health and advocacy from medical school through Continuing Medical Education will be necessary to prepare physicians to practice in a climate emergency.
2015 CanMEDS 역량 프레임워크에서 지구 건강은 어떻게 표현되어 있나요? How is planetary health represented in the 2015 CanMEDS competency framework?
2015 CanMEDS 의사 역량 프레임워크에는 지구 건강에 대한 명시적인 언급이 없습니다. 하지만 건강 옹호자 역할에는 건강의 사회적 결정 요인, 질병 예방, 건강 증진, 건강 감시, 지역사회 건강 개선과 관련하여 지구 건강과 관련될 수 있는 몇 가지 역량이 포함되어 있습니다(표 1B). 기후 과학자들은 수십 년 동안 기후 비상사태에 대한 경종을 울려왔지만, 대부분의 보건 전문가들은 최근에야 기후 비상사태를 악화시키는 데 있어 보건 시스템의 역할과 적응 조치를 채택하여 기후 비상사태로 인한 이환율과 사망률을 줄여야 할 필요성을 인식하기 시작했습니다. There are no explicit references to planetary health in the 2015 CanMEDS physician competency framework. The Health Advocate role does contain some enabling competencies that could be related to planetary health as it relates to the social determinants of health, disease prevention, health promotion, health surveillance, and improving community health (Table 1B). While climate scientists have been sounding the alarm on the climate emergency for decades, most health professionals have only recently begun to acknowledge the health system’s role in causing the worsening planetary emergency as well as the need to reduce the climate emergency’s associated morbidity and mortality by adopting adaptive measures.
2025년 캔메즈 역량 프레임워크 내에서 지구 건강을 어떻게 더 잘 표현할 수 있을까요? How can planetary health be better represented within the 2025 CanMEDS competency framework?
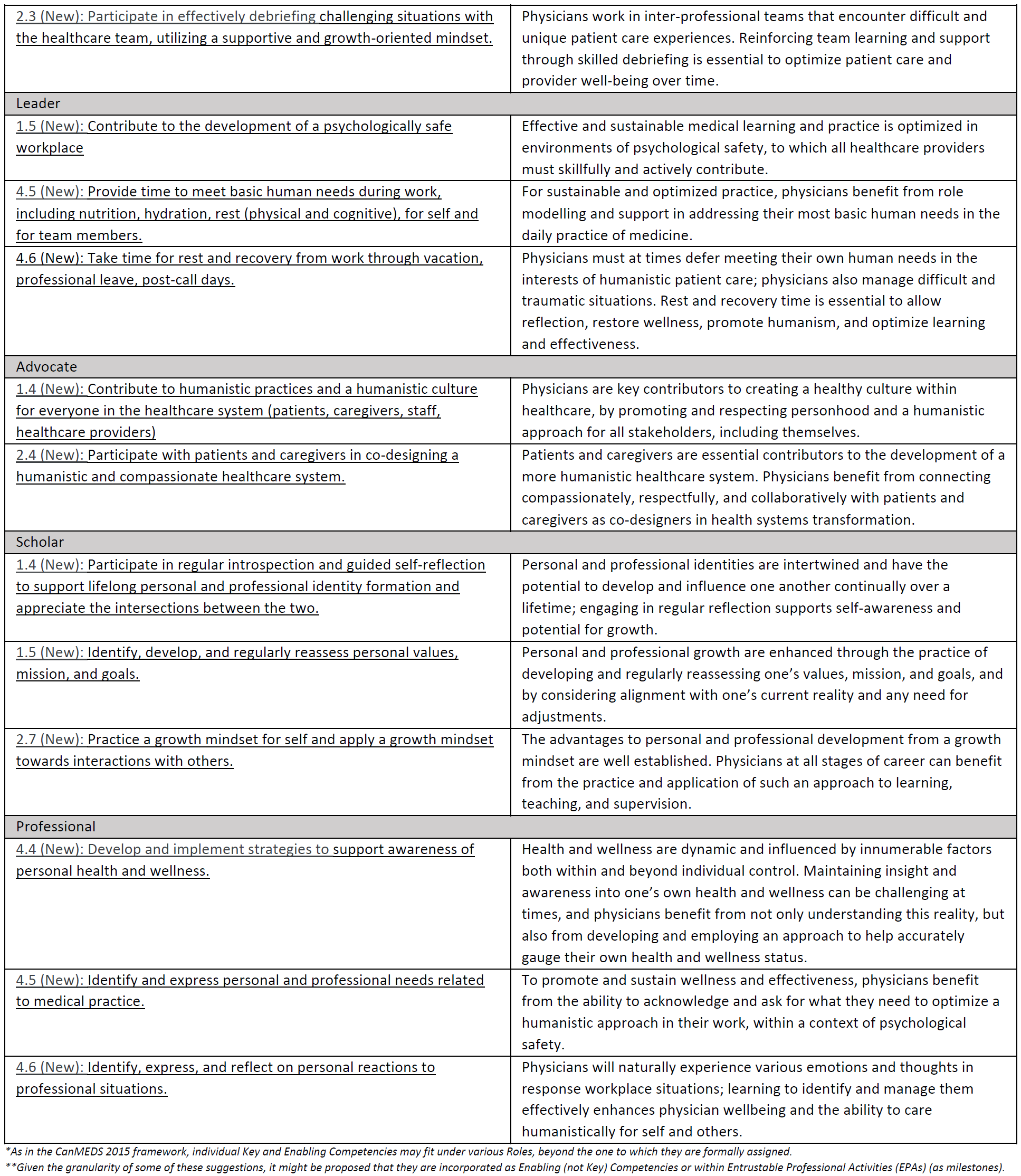
표 1C에서는 지구 건강에 대한 우리의 진화하는 이해를 CanMEDS 의사 역량 프레임워크에 통합하는 데 도움이 될 것으로 생각되는 역량을 포함하거나 수정할 것을 제안합니다. 이러한 제안에는 네 가지 주제가 포함됩니다: InTable 1C, we propose the inclusion or modification of competencies that we believe would help to integrate our evolving understanding of planetary health within the CanMEDS physician competency framework. These suggestions incorporate four themes:
의료 시스템의 지속가능성 개선. 이 주제는 의료 서비스 제공이 환경에 미치는 막대한 영향과 이를 해결함으로써 의사가 "해를 끼치지 않는다"는 직업적 의무를 다해야 할 필요성을 인식하고 있습니다.17 Improving the sustainability of our health system. This theme recognizes the enormous environmental impact of healthcare delivery and the need for physicians to meet our professional obligation to “do no harm” by addressing this.17
기후 비상사태로 인한 혼란에 대한 의료 시스템의 회복력 향상. 캐나다의 의료 시스템은 홍수, 산불, 폭염, 폭풍과 같은 극심한 기상 이변으로 인한 혼란에 취약하며, 이는 기후 회복력 있는 의료 시스템의 구현을 가속화하여 중환자 치료 제공을 유지함으로써 줄일 수 있습니다.4 의사는 의료 분야의 환경적 취약성을 인식하고 기후 회복력을 내재화하기 위한 품질 개선 과정에 기여해야 합니다.20 Improving the resilience of our health system to disruption from the climate emergency. Canadian healthcare systems are vulnerable to disruption by extreme weather events such as floods, wildfires, heatwaves, and storms that could be reduced by accelerating the implementation of climate-resilient healthcare systems to maintain critical care delivery.4Physicians must recognize environmental vulnerabilities in healthcare and contribute to quality improvement processes to embed climate-resilience.20
환경이 환자 건강에 미치는 영향에 대처하기. 의사가 환자의 사회적 맥락을 고려하는 것처럼, 우리도 환자의 환경적 맥락을 고려해야 합니다. 토착민과 인종차별 인구, 빈곤층, 정치적으로 소외된 사람들은 환경 파괴로 인해 불균형적인 영향을 받습니다. 의사는 환자와 그 가족에게 미치는 환경의 광범위하고 다양한 영향을 이해해야 합니다. Addressing the impact of the environment on patient health. Just as physicians consider a patient’s social context, we must also consider their environmental context. Indigenous and racialized populations, those living in poverty, and others who are politically marginalized are disproportionately affected by environmental degradation. Physicians must understand the breadth and variety of environmental impacts on patients and their families.
사회적 책임에서 지구 건강 관점의 중요성. 사회적 책임이란 "의학이 사회와 맺는 사회적 계약"으로 정의됩니다.21 사회적 책임 의료는 환자, 지역사회, 인구의 건강 요구에 대응합니다.19 사회적 책임을 위하여 의사는 질병, 고통, 사망에 기여하는 사회적, 환경적 조건에 대해 목소리를 내야 합니다. The importance of a planetary health lens in social accountability. Social accountability is defined as “the social contract that medicine has with society.”21Socially accountable healthcare is responsive to patient, community, and population health needs.19Socially accountable physicians must speak out about the social—and environmental—conditions that contribute to disease, suffering, and death.
Can Med Educ J. 2023 Mar 21;14(1):46-49.doi: 10.36834/cmej.75438.eCollection 2023 Mar.
CanMEDS 2025의 적응적 전문성(Can Med Educ J.2023) Adaptive Expertise in CanMEDS 2025
소개 Introduction
적응형 전문성은 급변하는 세계에서 효과적이고 혁신적으로 진료하고 학습하는 데 필요한 지식과 기술의 진화, 개선 및 개발과 관련된 역량을 통합합니다. 이 개념은 최근의 문헌 검토에서 CanMEDS 의사 역량 프레임워크에서 잘 드러나지 않는 필수 개념으로 확인되었습니다.1 이 원고는 이 개념과 이전 및 향후 CanMEDS의 반복에 대한 연관성을 요약하는 것을 목표로 합니다. Adaptive expertise incorporates competencies related to the evolution, refinement, and development of the knowledge and skills required to practice and learn effectively and innovatively in a rapidly changing world. It was identified as an essential concept that was underrepresented in the CanMEDS physician competency framework in a recent literature review.1This manuscript aims to summarize the concept and its links to former and future iterations of CanMEDS.
적응형 전문성이란 무엇이며 의사 역량에 중요한 이유는 무엇인가요? What is adaptive expertise and why is it important to physician competency?
적응적 전문성은 잘 알려진 문제에 직면했을 때 이전 지식을 효율적이고 효과적으로 적용하는 것과 이전 지식이 불충분할 때 새로운 지식을 창출하여 해결책을 마련하는 것 사이의 균형을 강조하는 전문가 개발 및 성과 모델입니다. 이와는 대조적으로 일상적 전문성은 적응적 전문성의 효율성 차원만을 반영하는 것으로 이해됩니다. 적응적 전문성의 '효율성'과 '혁신' 사이의 균형은 일상적인 문제 해결을 학습과 개선의 기회로 인식하는 접근법으로 보완됩니다.2,3 따라서 이전 지식의 적용이 불충분한 문제에 직면했을 때
적응적 전문성은 지식을 유연하게 사용하고 새로운 솔루션을 생성하는 능력을 가능하게 하는 반면,
일상적 전문성은 '알려진 솔루션에 미지의 문제를 맞추려는 시도'를 하다가 실패로 이끌게 됩니다."4
Adaptive expertise is a model of expert development and performance that emphasizes a balance between the efficient and effective application of previous knowledge when facing well-known problems and the creation of new knowledge to generate solutions when previous knowledge is insufficient. In contrast, routine expertise is understood to reflect only the efficiency dimension of adaptive expertise. This balance between ‘efficiency’ and ‘innovation’ in adaptive expertise is complemented by an approach to practice that recognizes daily problem solving as an opportunity to learn and improve.2,3Thus, when facing problems for which the application of previous knowledge is insufficient,
adaptive expertise enables the flexible use of knowledge and the ability to generate new solutions while
routine expertise will result in failed attempts to ‘fit unknown problems to known solutions.’4
적응적 전문성은 무엇을 해야 하는지(절차적 유창성)와 왜 해야 하는지(개념적 이해)를 모두 아는 것이 특징입니다.5 이러한 개념적 이해는 새롭고 불확실한 임상 상황의 가변성에 적응할 수 있게 합니다. 즉, 알려진 해결책이 충분하지 않은 경우 적응적 전문가는 근본적인 '이유'를 다루는 새로운 해결책을 생성할 수 있습니다. 적응형 전문성을 키우려면 교육이 효과적인 지식 보유와 적용에만 중점을 두는 것에서 벗어나 학생들이 새로운 지식을 지속적으로 학습하고 생성할 수 있도록 준비시키는 방향으로 전환되어야 합니다. 이러한 역량을 '미래 학습을 위한 준비(PFL)'로 정의할 수 있습니다.6 Adaptive expertise is characterized by both knowing what to do (procedural fluency) as well as knowing why you’re doing it (conceptual understanding).5It is this conceptual understanding that permits adaptation to variability in novel and uncertain clinical situations i.e. if known solutions are insufficient, adaptive experts can generate new solutions that still address the underlying ‘why’. To foster the development of adaptive expertise, education must shift beyond a sole emphasis on effective knowledge retention and application towards preparing students to continue to learn and generate new knowledge. This capacity has been defined as ‘preparation for future learning (PFL).6
보건 전문직 교육에서 PFL을 지원하는 교육적 접근법에는 다음이 포함됩니다.7,8
a) 임상 징후 및 증상을 근본적인 메커니즘과 명시적으로 통합(예: "왜"라고 묻거나 말하기),
b) 학생들에게 의미 있는 변형에 노출(예: "만약에 이렇다면.." 질문하기),
c) 학습에서 투쟁과 발견을 활용한 다음, 즉각적인 피드백과 통합이 뒤따르는 것
불가피하게 보건 전문가는 정식 교육을 받지 않은 질환을 가진 환자를 마주하게 될 것입니다. 따라서 새로운 문제에 직면하여 새로운 지식을 창출하고 학습하는 능력은 의사가 환자의 고유한 요구에 대응하고 끊임없이 변화하는 역동적인 의료 종사자 간 네트워크 내에서 치료를 제공할 수 있도록 보장합니다.9 In health professions education, pedagogical approaches that support PFL include
a) explicit integration of clinical signs and symptoms with underlying mechanisms (e.g asking or telling “why”),
b) exposing students to meaningful variation (e.g asking “what if” questions) and
c) leveraging struggle and discovery in learning followed by immediate feedback and consolidation.7,8
Inevitably, health professionals will face patients presenting with conditions for which they have not received formal training. Thus, the ability to create new knowledge and learn in the face of novel problems ensures that physicians are responsive to the unique needs of their patients, as well as able to provide care within ever-changing, dynamic, interprofessional networks of healthcare workers.9
적응형 전문성은 2015 CanMEDS 역량 프레임워크에서 어떻게 표현되나요? How is adaptive expertise represented in the 2015 CanMEDS competency framework?
의료 전문가 역할은 환자 중심의 임상 평가 및 관리, 임상 의사결정의 복잡성, 모호성, 불확실성, 의사결정 시 진화하는 지식의 활용 등 적응적 전문성의 여러 측면을 반영합니다. 그러나 2015년 프레임워크에는 이러한 역할과 관련하여 적응적 전문성에 대한 구체적인 언급이 부족하여(표 1A 및 및1B),1B) 교육자가 효과적이고 혁신적으로 실습하고 학습하는 데 필요한 지식과 기술을 의도적으로 배양할 수 있는 환경이 조성되지 않을 수 있습니다. 적응형 전문지식을 CanMEDS의 핵심 의료 전문가 역량으로 명시적으로 통합하면 의료 전문지식과의 관계를 강조하고, 일상적인 진료에서 7가지 CanMEDS 역할을 모두 통합하는 데 핵심적인 기능을 강조하며, 전문 역량 및 지속적인 전문성 개발의 지표로서 진료에서 새로운 지식을 혁신하고 창출하는 역량을 장려할 수 있습니다. The Medical Expert role reflects many aspects of adaptive expertise: patient-centered clinical assessment and management; complexity, ambiguity, and uncertainty in clinical decision-making; and drawing on an evolving body of knowledge when making decisions. However, the 2015 framework lacks specific reference to adaptive expertise in relation to this role (Table 1Aandand1B),1B), which may create an environment where educators are not primed to deliberately cultivate the necessary knowledge and skills required to practice and learn effectively and innovatively. Explicitly incorporating adaptive expertise as a key Medical Expert competency in CanMEDS would highlight its relationship with medical expertise, underscore its central function to the integration of all seven CanMEDS roles in daily practice, and promote the capacity to innovate and create new knowledge in practice as a marker of professional competence and continuing professional development.
2025년 CanMEDS 역량 프레임워크 내에서 적응형 전문성을 어떻게 더 잘 표현할 수 있을까요? How can adaptive expertise be better represented within the 2025 CanMEDS competency framework?
임상 의사 결정에서 적응형 전문 지식의 중요성을 인식하여 의료 전문가 역할에 새로운 핵심 역량을 통합할 것을 제안합니다(표 1C). 이 역량에는 효율성과 혁신 사이의 균형을 맞추고, 다양한 관점을 수용하며, 임상 진료 전반에 걸쳐 학습할 수 있는 역량이 포함됩니다. 적응형 전문성을 의료 전문가 역할의 핵심 역량으로 설정함으로써, 우리는 CanMEDS 프레임워크에서 의료 전문성의 중심적인 역할과 내재적인 역할을 자신의 업무 범위에 통합하는 방법을 인식하고 있습니다. 또한 커뮤니케이터, 협력자, 리더, 학자 역할에 속하는 역량들이 이러한 영역에서 적응형 전문성의 중요한 요소를 더 잘 통합할 수 있도록 약간의 제안을 했습니다(표 1C). 발달적 관점에서 볼 때, 분야별 교육에 적응적 전문성을 조기에 도입하는 것은 PFL을 포함하는 교육이 지속적인 전문성 개발에서 임상적 의사 결정의 지속적인 역량과 성장을 보장하는 데 도움이 될 수 있음을 인식하는 것입니다. 초심자에서 숙련자로 넘어가는 CanMEDS 마일스톤의 구성은 적응형 전문성과 더욱 연계되어 전문적 역량의 지표로서 실무에서 새로운 지식을 혁신하고 창조하는 역량을 촉진할 수 있습니다. Recognizing the importance of adaptive expertise in clinical decision-making, we propose incorporating a new key competency into the Medical Expert role (Table 1C). Its enabling competencies incorporate the capacity to balance between efficiency and innovation, to embrace multiple perspectives, and to learn throughout clinical practice. By situating adaptive expertise as a key competency within the Medical Expert role, we recognize the central role of medical expertise in the CanMEDS framework and how it incorporates the intrinsic roles into one’s scope of practice. Additionally, we have made minor suggestions to enabling competencies under the Communicator, Collaborator, Leader, and Scholar roles to better integrate important elements of adaptive expertise in these areas (Table 1C). From a developmental perspective, the introduction of adaptive expertise early within discipline-specific training recognizes that education that includes PFL can help ensure that sustained competence and growth in clinical decision-making is accounted for in continuing professional development. The progression from novice to mastery in the organization of CanMEDS milestones can further align with adaptive expertise to promote the capacity to innovate and create new knowledge in practice as a marker of professional competence.
Can Med Educ J. 2023 Mar 21;14(1):18-21.doi: 10.36834/cmej.75445.eCollection 2023 Mar.
CanMEDS 2025의 임상추론(Can Med Educ J.2023) Clinical Reasoning in CanMEDS 2025
소개 Introduction
임상 추론은 의학교육 연구의 초기 초석 중 하나였으며, 이러한 초기 연구 초점은 의학 교육에서 임상 추론의 중심적인 역할을 반영합니다.1 따라서 임상 추론이 CanMEDS 의사 역량 프레임워크에서 잘 알려지지 않은 개념으로 확인된 것은 놀라운 일이 아닐 수 없습니다.2,3 그러나 프레임워크를 자세히 살펴보면 임상 추론은 그 중심적인 중요성에도 불구하고 CanMEDS에서 명시적으로 언급되거나 통합된 적이 거의 없다는 것을 알 수 있습니다. 임상 추론의 일부 측면이 의료 전문가 역할에 역량으로 포함되어 있기는 하지만, 임상 추론에 대한 우리의 이해는 CanMEDS 2015에서 명시적으로 언급된 몇 가지를 넘어 확장되었습니다. 이 입문서에서는 임상 추론이 CanMEDS 2025의 핵심 개념인 이유, 임상 추론에 대한 우리의 이해가 어떻게 발전해 왔는지, CanMEDS 2015에서 임상 추론이 어떻게 표현되는지, 그리고 임상 추론과 관련된 역량을 보다 신중하고 포괄적으로 통합하기 위해 CanMEDS 2025를 개정할 수 있는 방법을 제안합니다. Clinical reasoning was one of the early cornerstones of medical education research, and this early research focus reflects its central role in medical training.1Therefore, it may be surprising that clinical reasoning was identified as an underrepresented concept in the CanMEDS physician competency framework.2,3However, a close examination of the framework demonstrates that clinical reasoning, despite its central importance, is rarely explicitly mentioned or integrated in CanMEDS. While some aspects of clinical reasoning are woven within the Medical Expert role as enabling competencies, our understanding of clinical reasoning has expanded beyond these few explicit mentions in CanMEDS 2015. This primer will orient readers to why clinical reasoning is a key concept for CanMEDS 2025, how our understanding of clinical reasoning has evolved, highlight how clinical reasoning is represented in CanMEDS 2015, and suggest ways that CanMEDS 2025 could be revised to more deliberately and comprehensively incorporate competencies related to clinical reasoning.
임상 추론이란 무엇이며 의사의 역량에 중요한 이유는 무엇인가요? What is Clinical Reasoning and why is it important to physician competency?
임상적 추론은 환자 치료의 모든 측면에서 핵심적인 요소이기 때문에 의료 분야에서 전문적 진료의 핵심으로 묘사되어 왔습니다.1. 또한 추론 오류는 환자와 의료진에게 높은 비용을 초래하기 때문에 환자 안전을 위협하는 요인으로 지목되었습니다.4 이러한 핵심성과 중요성에도 불구하고,5 임상 추론을 정의하는 방법, 효과적인 추론을 개념화하는 방법, 교육, 평가 및 연구 목적으로 이를 운영하는 방법은 크게 나뉘지는 않았지만 여전히 다양합니다.5,6 Clinical reasoning has been described as the core of professional practice in healthcare,1as it is a key component of all aspects of patient care. Additionally, errors in reasoning have been named as a threat to patient safety given the high cost of errors to patients and practitioners.4Despite its centrality and importance,5how we define clinical reasoning, how we conceptualize effective reasoning, and how we operationalize it for the purposes of teaching, assessment, and research remain varied if not deeply divided.5,6
효과적인 임상 추론의 개념은 의학교육 내 여러 커뮤니티에서 다양한 개념화 또는 추론의 요소를 교육 목표, 평가 대상 또는 집중 연구 영역으로 사용함에 따라 다양하게 설명되어 왔습니다. 임상 추론에 대한 이러한 각 사고 방식은 인간의 인지 구조에서 실천의 인식론에 이르기까지 서로 다른 학문, 영역 또는 이론적 기반에서 비롯되며, 이는 임상 추론 과정의 각기 다른 요소에 초점을 맞춘다는 것을 의미합니다. 임상 추론에 접근하는 이러한 다양한 방식은 중요한 면에서 차이가 있습니다.
일부는 추론의 결과에 초점을 맞춥니다.
의료 오류(추론의 불행한 결과7)에서 진단 정확도(바람직한 결과8)까지
일부는 개별 활동으로서의 임상 추론에 초점을 맞춘다.
의사 또는 학습자의 인지 과정 등
다른 일부는 사회적으로 내재된 활동으로서의 임상 추론을 탐구합니다:
팀의 진료 제공(추론을 상호작용 활동으로 배치9),
상황별 의사 결정(상황 또는 구체화된 활동으로서의 추론10) 또는
공유 의사 결정(파트너로서의 환자11) 등에 주목
어떤 사람들은 의사의 임상 추론에서 발생가능한 한계에 관심을 집중하고 있습니다:
인지적 부하 고려사항(임상 추론 및 작업 수행은 작업 기억 제약에 의해 제한됨12)
편향의 위험성(예: 불평등 및 의료 서비스 격차13)
마지막으로, 일부는 에러에 대한 인적 요인과 시스템 기여4 및 복잡한 맥락에 개인이 어떻게 적응하는지에 초점을 맞춥니다.16
적응적 전문성,14 집단적 역량,15 복잡성 이론 등
The notions of effective clinical reasoning have been variously described by different communities within medical education—as different conceptualizations or elements of reasoning have been used as objectives for instruction, targets for assessment, or areas of focused research. Each of these ways of thinking about clinical reasoning draw from different disciplines, domains, or theoretical homes—from human cognitive architecture to epistemologies of practice; which means each of these ways of thinking about clinical reasoning focus on different elements of the clinical reasoning process. These numerous ways of approaching clinical reasoning vary in important ways.
Some focus on the outcomes of reasoning;
from medical error (an unfortunate outcome of reasoning7) to diagnostic accuracy (an aspired outcome8).
Some focus on clinical reasoning as an individual activity,
focused on the cognitive processes of the practitioner or learner;
while others explore clinical reasoning as a socially embedded activity, with attention paid to
team provision of care (placing reasoning as an interactional activity9),
decisions-in-context (reasoning as a situated or embodied activity10), or
이러한 각 관점은 추론 과정의 서로 다른 구성 요소를 강조하고, 추론의 서로 다른 "결과"를 중요시하며, "효과적인" 추론을 만드는 요소에 대해 서로 다른 개념화를 가지고 있습니다. 이러한 가치 있는 구성 요소, 결과, 효과적인 추론에 대한 개념의 차이는 모두 매우 다른 집중 교육 영역, 다른 평가 목표, 다른 연구 접근 방식에 영향을 미칩니다.17 Each of these perspectives highlight different components of the reasoning process, value different “outcomes” of reasoning, and have different conceptualizations of what makes “effective” reasoning. These differences in valued components, outcomes, and notions of effective reasoning all feed into very different areas for focused teaching, different assessment targets, and different approaches to research.17
임상 추론과 같이 크고 복잡한 개념을 의학교육에서 가르치고, 평가하고, 연구할 수 있는 것으로 만들려면 각 상황이나 전문 분야에서 무엇이 효과적인 임상 추론을 구성하는지에 대한 결정이 내려져야 합니다. 효과적인 추론으로 판단되는 요소에 따라 임상 추론 과정의 다른 구성 요소, 다른 맥락적 변수 또는 임상 추론의 다른 결과가 우선시됩니다.18 예를 들어, 효과적인 추론은 다음으로 특징지을 수 있습니다.12
속도,19
정확성,20
비용 영향,21
환자 욕구와 임상적 권고(즉, 공유 의사 결정)의 균형,10
과도한 검사와 (불)확실성에 대한 욕구의 균형,22
맥락적 변수에 대한 인식 및 적응,23
관리 계획의 효과적인 적응adaptation,24
작업 기억 한계 내에서 인지 부하를 효과적으로 관리할 수 있는 것
이러한 효과적인 추론의 특성은 평가, 학습 및 교육의 대상이 되며, 이는 해당 집단의 전문성 수준, 전문 분야 맥락, 치료 맥락(예: 긴급 치료 대 지역사회 치료)에 따라 달라집니다. To render a large and complex concept such as clinical reasoning into something that can be taught, assessed, or researched in medical education, decisions about what constitutes effective clinical reasoning in each context or specialty must be made. Depending on what is determined to be effective reasoning, different components of the clinical reasoning process, different contextual variables, or different outcomes of clinical reasoning come to the forefront.18For example, effective reasoning can be characterized by
effectively managing cognitive load within working memory limitations.12
These characteristics of effective reasoning become the targets of assessment, learning, and teaching that vary depending on the expertise level of the population in question, specialty context, and care context (i.e., urgent care vs. community care).
임상 추론은 2015 CanMEDS 역량 프레임워크에서 어떻게 표현되어 있나요? How is Clinical Reasoning represented in the 2015 CanMEDS competency framework?
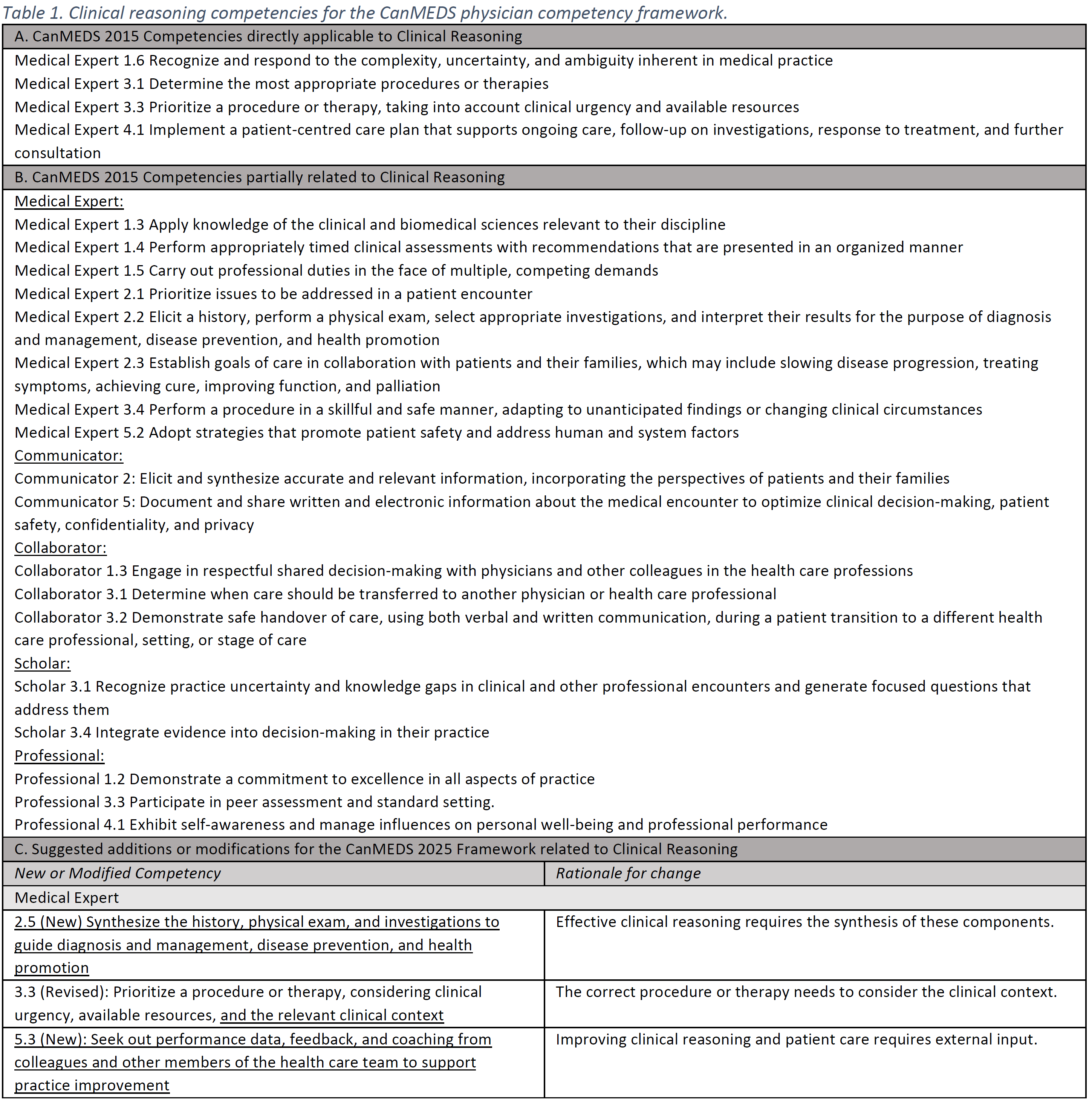
CanMEDS 2015 프레임워크에서 임상 추론의 측면은 주로 의료 수출 역할(표 1A)의 역량으로 나타나며, 일부 요소는 다른 역할(표 1B)에 걸쳐 통합되어 있습니다. 임상 추론의 이론적 및 개념적 이해와 관련된 연구는 CanMEDS 2015 이후 성장해 왔습니다.3 최근의 연구는 개인 인지를 넘어 팀 기반 추론,9 진단적 의사결정에서 관리 추론에 대한 고려,23 그리고 개별 인지 과정에서 복잡한 맥락에 놓인 행동으로서의 임상 추론을 탐구하는 것으로 확장되었습니다.10 훌륭하고 건전한 임상 추론을 구성하는 요소에 대한 우리의 개념은 임상 추론에 대한 이론적 이해의 증가와 진료의 복잡성에 대한 인식의 확대에 따라 확장되어 왔습니다. 임상적 추론은 의료인이 된다는 것의 핵심으로 남아 있지만,1 임상적 추론이 어떤 모습이고 어떻게 교육, 학습 및 평가의 목표로 운영되는지는 확장되었습니다. 임상 추론의 개념은 CanMEDS 2015의 일부 필수 역량에 반영되어 있지만(전문 분야의 맥락에 따라 이러한 역량이 어떻게 구현되는지가 달라질 수 있음을 인식하고 있습니다), CanMEDS 2025에서는 임상 추론이 보다 명시적이고 포괄적으로 표현되어야 한다고 생각합니다. In the CanMEDS 2015 framework, aspects of Clinical Reasoning are found primarily as enabling competencies within the Medical Export role (Table 1A) with some elements interwoven throughout other roles (Table 1B). Research related to the theoretical and conceptual understanding of clinical reasoning has grown since CanMEDS 2015.3More recent work extends beyond individual cognition to include team-based reasoning;9from diagnostic decision-making to consideration for management reasoning,23and from individual cognitive processes to exploring clinical reasoning as a situated behaviour in complex contexts.10Our notions of what constitutes good and sound clinical reasoning have broadened in lockstep with our growing theoretical understanding of clinical reasoning, and our growing acknowledgement of the complexity of care. While clinical reasoning remains at the core of what it means to be a healthcare provider,1what that clinical reasoning looks like and how it is operationalized into targets of teaching, learning, and assessment have expanded. While the concept of clinical reasoning is reflected in some enabling competencies within CanMEDS 2015—recognizing that specialty context will shape how these competencies are enacted - we believe that clinical reasoning should be more explicitly and comprehensively represented within CanMEDS 2025.
임상 추론이 2025 CanMEDS 역량 프레임워크 내에서 어떻게 더 잘 표현될 수 있을까요? How can Clinical Reasoning be better represented within the 2025 CanMEDS competency framework?
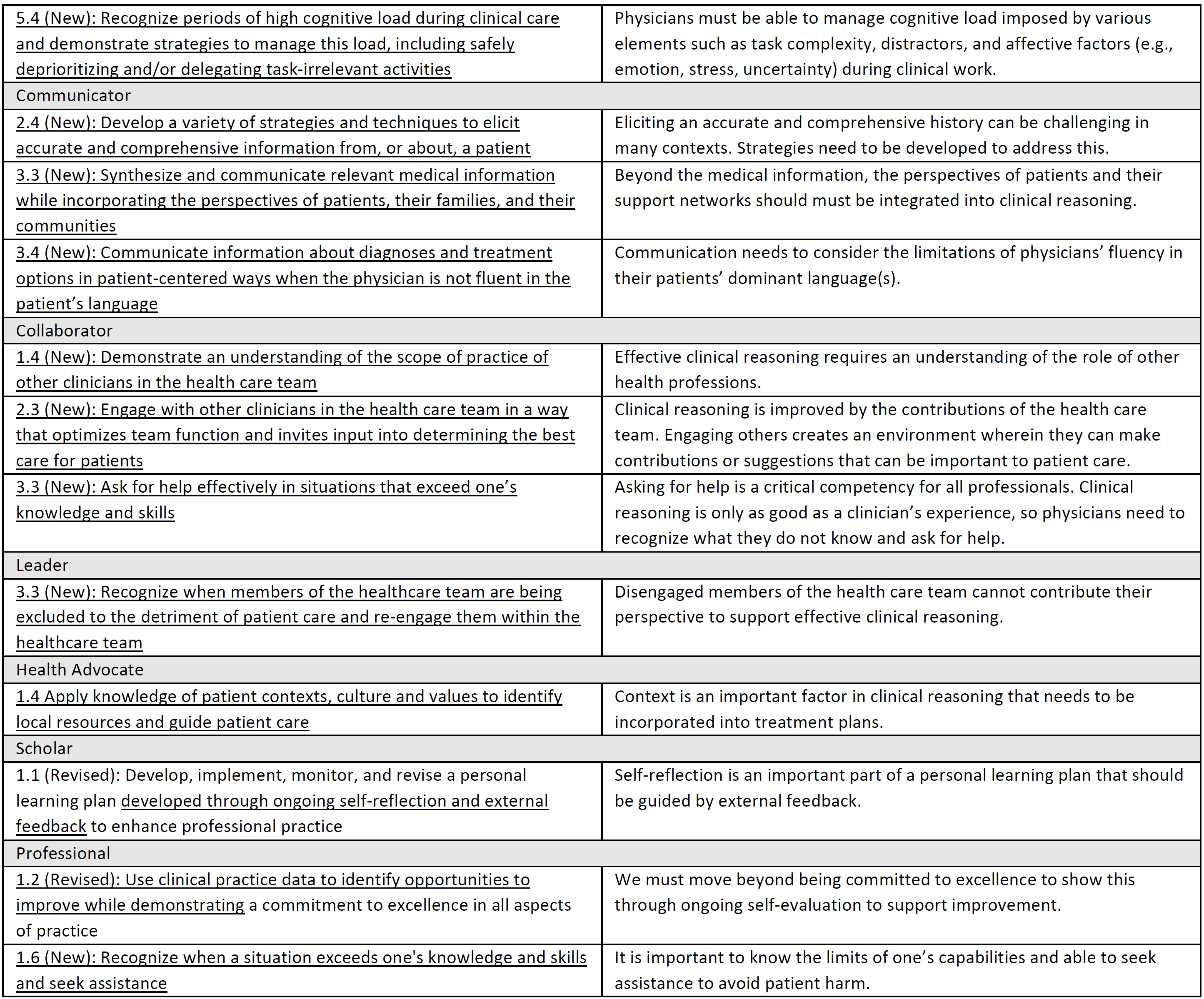
임상 추론에 대한 현재의 이해에 더 잘 부합하기 위해 2025 CanMEDS 역량 프레임워크는 양질의 임상 진료를 제공하는 데 기여하는 임상 추론의 여러 측면을 보다 의도적으로 통합할 수 있으며, 통합해야 합니다. 보다 세분화된 의미에서 임상 추론에는 필요한 기본 지식의 통합과 다양한 맥락에서 시기적절하고 효과적인 방식으로 치료를 제공하면서 해당 지식을 동원하는 능력이 포함됩니다. 효과적인 임상 추론의 일부 핵심 요소는 현재 의료 전문가 역할의 중요한 역량이지만, 임상 추론의 측면은 다른 CanMEDS 역할(예, 의사소통자, 협력자, 학자, 전문가; 표 1 참조).필수 지식의 범위, 진료 표준, "좋은" 추론의 기준, 임상 추론에 영향을 미치는복잡한 맥락적 요인은 CanMEDS 2025에 더 잘 통합될 수 있고 통합되어야 합니다.3 CanMEDS 프레임워크 내에서 임상 추론을 더 잘 반영하기 위해, 우리는 기존의 몇 가지 지원enabling역량을 조정할 것을 제안하며, CanMEDS 2025에서 중요한 고려 사항이라고 생각하는 역량을 명확히 설명합니다. 제안된 지원enabling역량(표 1, 섹션 C)은 모호한 개념의 근거를 마련하고 임상 추론이 여러 역할의 맥락에서 관찰, 교육, 평가 및 연구될 수 있다는 개념을 반영합니다. 즉, 의료 서비스를 제공하려면 효과적인 임상 추론이 필요하고, 효과적인 임상 추론에 필요한 여러 가지 역량이 필요하며, 이러한 역량은 여러 CanMEDS 역할에 걸쳐 통합되어 있습니다. 임상적 추론은 효과적인 치료 제공을 위해 여러 CanMED 역할에 걸쳐 필요한 역량을 통합해야 하는 방법을 보여주는 훌륭한 예입니다. To better align with current understandings of clinical reasoning, the 2025 CanMEDS competency framework can, and should, more deliberately integrate the many aspects of clinical reasoning that contribute to providing high quality clinical care. In a more granular sense, clinical reasoning includes the integration of necessary fundamental knowledge, and the ability to mobilize that knowledge while delivering care in a variety of contexts in a timely and effective way. While some key components of effective clinical reasoning are important current enabling competencies for the Medical Expert Role, aspects of clinical reasoning are also woven throughout other CanMEDS roles (i.e., communicator, collaborator, scholar, and professional; seeTable 1).The scope of requisite knowledge, standards of care, standards of “good” reasoning, and complex contextual factors that influence clinical reasoning could and should be better integrated into CanMEDS 2025.3In order to better reflect clinical reasoning within the CanMEDS framework, we suggest adapting several existing enabling competencies, and articulate those that we believe are important considerations for CanMEDS 2025. The suggested enabling competencies (Table 1; section C) helps ground an already nebulous concept, and reflect the notion that clinical reasoning can be observed, taught, assessed, and studied in the context of several Roles. Meaning, the delivery of care necessitates effective clinical reasoning, several enabling competencies needed for effective clinical reasoning, and these enabling competencies are integrated across several CanMEDS roles. Clinical reasoning is an excellent example of how enabling competencies across multiple CanMEDs roles need to be integrated to effectively deliver care.
표 1C에서 제안하는 지원enabling역량은 임상 환경에서 임상 추론이 어떻게 동원되는지에 대한 이해의 증가를 반영하며, 임상 추론 과정과 결과를 형성하는 치료 환경의 복잡성을 인식합니다. '좋은' 임상 추론이 여러 상황과 진료 환경에 걸쳐 어떤 모습인지에 대한 중요한 차이가 존재하기 때문에, 이러한 역량 제안은 각 의료 전문 분야 내에서 맥락화를 계속 요구할 것입니다. 임상 추론이 독립적인 역량으로 명명되어야 한다고 생각하지는 않지만,25 임상 추론의 복잡성은 CanMEDS 프레임워크 전반에 걸쳐 몇 가지 새로운 역량과 몇 가지 조정된 지원 역량에 더 잘 반영될 수 있다고 생각합니다.
The enabling competencies we propose inTable 1Creflect our growing understanding of how clinical reasoning is mobilized in the clinical environment and recognize the complexity of care environments that shape clinical reasoning processes and outcomes. These suggested enabling competencies will continue to require contextualization within each of our medical specialties, as important distinctions do exist regarding what “good” clinical reasoning looks like across contexts and care environments. While we do not believe clinical reasoning should be named as an independent competency,25we believe the complexity of clinical reasoning can be better reflected in several new, and several adapted enabling competencies across the CanMEDS framework.
Can Med Educ J. 2023 Mar 21;14(1):58-62.doi: 10.36834/cmej.75843.eCollection 2023 Mar.
CanMEDS 2025의 버추어 케어(Can Med Educ J.2023) Virtual Care in CanMEDS 2025
소개 Introduction
가상 진료(VC)는 잘 훈련된 의사의 손에 의해 효과적이고 안전합니다.1 그러나 대면 진료의 역량이 반드시 가상 진료의 역량과 동일하지는 않습니다.2 특정 VC 교육에 대한 여러 요구에도 불구하고,3-6 최근 문헌 검토에 따르면 이러한 개념은 2015 CanMEDS 의사 역량 프레임워크7에서 충분히 반영되지 않은 것으로 확인되었습니다.8 이러한 새로운 역량을 반영하여 오늘날의 의사가 환자와 사회의 진화하는 요구를 충족할 수 있도록 CanMEDS 2025를 업데이트해야 합니다. 이 입문서에서는 효과적인 원격 상담 및 환자 치료를 제공하기 위해 환자 및 동료와 가상으로 연결하는 데 필요한 기술에 초점을 맞춘 CanMEDS 역량에 대한 변경 사항을 제안합니다. Virtual care (VC) is effective and safe in the hands of well-trained physicians.1However, competency in in-person care does not necessarily equate to competency in VC.2Despite multiple calls for specific VC training,3-6these concepts were identified as being underrepresented in the 2015 CanMEDS physician competency framework7by a recent literature review.8CanMEDS 2025 must be updated to reflect these novel competencies, ensuring that today’s physicians are able to meet their patients’ and societies’ evolving needs. For this primer, we propose changes to the CanMEDS competencies that focus on the skills necessary to connect virtually with patients and peers to deliver effective remote consultation and patient care.
가상 의료란 무엇이며 의사의 역량에 중요한 이유는 무엇인가요? What is VC and why is it important to physician competency?
기술의 발전은 사람들이 관계를 맺고, 소통하고, 생활하는 방식을 바꾸고 있습니다. 의료 분야에서도 연구와 진료의 지형을 바꾸고 있습니다. 이 분야에는 때때로 중복되는 용어가 많이 있습니다(표 1의 정의 참조). 이 백서에서는 기술을 활용한 개별 환자 치료 제공에 초점을 맞추기 위해 가상 치료 Virtual Care 라는 용어를 사용합니다. 의료 정보학 및 데이터 분석과 같은 개념은 이 백서의 범위를 벗어나지만 실제로 중요하며 다른 곳에서 다루고 있습니다.9 Technological advances are changing how people relate, communicate, and live. In healthcare, they are altering the landscape of research and practice. There are many, sometimes overlapping, terms in this field (see definitions inTable 1). This paper utilizes the termVirtual Careto focus on the provision of individual patient care using technology. Concepts such as health informatics and data analytics are out of the scope of this paper but are indeed important and are addressed elsewhere.9
Term
용어 정의 Definition
Chatbot
챗봇 "자연스러운 대화를 통해 의료 서비스를 제공하고...차례대로 진행되는 대화를 통해 온라인 의료 서비스를 더욱 사용자 친화적으로 만드는"10 전자 "대화형 시스템"입니다. An electronic “conversational system” that “provides healthcare through natural conversation…making online healthcare more user-friendly…through a turn-taking dialog.”10
Digital Health
디지털 건강 디지털 건강은 정보 기술 및 전자 통신 도구, 서비스 및 프로세스를 사용하여 의료 서비스를 제공하고 더 나은 건강을 촉진하는 것입니다.9 여기에는 "웨어러블 기기, 모바일 건강, 원격 의료, 건강 정보 기술, 원격 의료... 데이터 분석 및 인텔리전스, 예측 모델링... 의료 소셜 미디어", 전자 의료 기록 및 환자 커뮤니케이션 포털의 사용이 포함됩니다.11 Digital health is the use of information technology and electronic communication tools, services and processes to deliver health care services and facilitate better health.9 It includes the use of, “wearable devices, mobile health, telehealth, health information technology, and telemedicine… data analytics and intelligence, predictive modelling…medical social media”, electronic medical records, and patient communication portals.11
eHealth
e헬스 "의료 서비스, 건강 감시, 건강 문헌, 건강 교육, 지식 및 연구를 포함한 건강 및 건강 관련 분야를 지원하기 위해 정보통신 기술을 비용 효율적이고 안전하게 사용하는 것"12. “The cost-effective and secure use of information and communications technologies in support of health and health-related fields, including health-care services, health surveillance, health literature, and health education, knowledge and research.”12
Extended reality
확장 현실 컴퓨터를 사용하여 사용자 환경을 컴퓨터 생성 콘텐츠로 향상(예: 증강 현실[AR])하거나 대체(예: 가상 현실[VR])하는 것.13 Using computers to enhance (ie: augmented reality [AR]) or replace (ie: virtual reality [VR]) a user’s environment with computer generated content.13
mHealth
m헬스 원격 의료를 목적으로 스마트폰 및 웨어러블 디바이스와 같은 모바일 기술을 사용하는 것.5 The use of mobile technology such as smartphones and wearable devices for the purposes of telehealth.5
Telehealth
원격 보건 "건강 관리 또는 의료 교육의 모든 구성 요소를 원거리에서 제공하는 것"5 여기에는 가상 진료와 의료 전문가 및 환자 교육이 모두 포함됩니다.5 “The delivery of any component of health care or medical education at a distance.”5 It includes both virtual care and the education of both healthcare professionals and patients.5
Telemedicine
원격 의료 "정보통신 기술을 통해 원격으로 제공되는 의료 서비스"14로, 화상 또는 전화 상담 등이 이에 해당합니다. A “medical service provided remotely via information and communication technology”14 such as a video or telephone consultation.
Virtual Care
가상 진료 "환자 치료의 질을 촉진하거나 극대화할 목적으로 모든 형태의 통신 또는 정보 기술을 사용하여 원격으로 발생하는 환자 및/또는 환자 치료 서클 구성원 간의 모든 상호 작용"15 여기에는 원격 진료, mHealth, 원격 모니터링, 전자 의료 기록(EMR)을 통한 보안 메시징이 포함되지만 이에 국한되지는 않습니다.15 “Any interaction between patients and/or members of their circle of care, occurring remotely, using any form of communication or information technologies, with the aim of facilitating or maximizing the quality of patient care.”15 This includes but is not limited to telemedicine, mHealth, remote monitoring, and secure messaging via electronic medical records (EMRs).15
VC는 고품질 의료 서비스에 대한 접근성을 제공하고의료 서비스의 도달 범위, 형평성, 효율성, 잠재적 비용 효율성을 향상시킬 수 있는 기회를 제공합니다.1,3 최대 85%의 환자가 VC를 받는 데 관심이 있으며16 여러 의료 분야에서 그 효과가 입증되었습니다.1 명백한 바람직성에도 불구하고 대면 의료 역량이 가상 영역으로 자동 변환되지 않고2 의사가 현장에서 유능하게 진료하기 전에 이해해야 하는 VC의 기술적 및 사회 문화적(예: 정책 및 형평성) 한계가 있기 때문에 특정 교육이 필요합니다.17 실제로 캐나다 의사협회, 캐나다 가정의학회, 캐나다 왕립 의사 및 외과의사 대학은 "[VC] 교육을 의료 서비스 교육에 통합하여 의료 제공자와 관리자가 성숙한 [VC] 생태계에서 기능할 수 있도록 전적으로 준비되도록 해야 한다"고 권고했습니다.17 VC offers the opportunity to provide access to high-quality care and enhance the reach, equity, efficiency, and potentially cost-effectiveness of medical services.1,3Up to 85% of patients are interested in receiving VC16and multiple areas of medicine have demonstrated its effectiveness.1Despite its apparent desirability, VC requires specific training because in-person medical competencies do not automatically translate to the virtual sphere2and there are technological and sociocultural (eg: policy and equity) limitations to VC that need to be appreciated before a physician can practice competently in the field.17Indeed, the Canadian Medical Association, College of Family Physicians of Canada, and The Royal College of Physicians and Surgeons of Canada have recommended that “[VC] training must be integrated into health service education so that providers and administrators are wholly prepared to function in a mature [VC] ecosystem.”17
2015 CanMEDS 역량 프레임워크에서 VC는 어떻게 표현되어 있나요? How is VC represented in the 2015 CanMEDS competency framework?
레지던트3 및 의대생 수준에서 가상 의료에 대한 교육을 강화해야 한다는 요구가 오랫동안 있어 왔습니다.4 이러한 요구를 해결하기 위해 2015 CanMEDS 전자 의료 전문가 실무 그룹은 전자 의료 및 가상 의료 채택을 탐색하기 위한 특정 역량에 대한 권장 사항을 제시했지만,18 이 중 대부분은 최종 역량 프레임워크에 반영되지 않았습니다. 특히, "기술 기반 커뮤니케이션"은 2015 CanMEDS 지원 역량 중 하나에서 찾을 수 있지만(표 2 참조), 디지털 헬스, VC, eHealth 및 기타 관련 용어는 구체적으로 언급되지 않았습니다.7 There have been long standing calls for increased training in VC at the residency3and medical student level.4To address these needs a CanMEDS 2015 expert working group on eHealth made recommendations on specific competencies for navigating eHealth and virtual health care adoption,18though most of these were not reflected in the final competency framework. Notably, while “technology-enabled communication” can be found within one of the 2015 CanMEDS enabling competencies (seeTable 2), digital health, VC, eHealth and other related terms are not specifically mentioned.7
그 이후로 가상 진료는 환자 치료에서 떼려야 뗄 수 없는 부분이 되었으며, 코로나19 팬데믹 기간 동안 공중 보건 조치로 인해 더욱 발전했습니다.16 의사와 의료 시스템이 이러한 전환에 충분히 준비되지 않았기 때문에 가상 진료로의 급격한 변화는 문제가 되었습니다. 곧 발표될 CanMEDS2025 개정판은 가상 의료를 포함한 21세기 의학에서 요구되는 업무에 맞춰 의사의 역량을 조정할 수 있는 기회입니다. Since then, VC has become an inextricable part of patient care, with advances precipitated by public health measures during COVID-19 pandemic.16The rapid change to VC was problematic because physicians and the healthcare system were not fully prepared for this transition. The upcoming CanMEDS 2025 revision is an opportunity to align physician competencies with the tasks required in 21stcentury medicine including virtual care.
2025년 CanMEDS 역량 프레임워크 내에서 가상 의료가 어떻게 더 잘 표현될 수 있을까요? How can VC be better represented within the 2025 CanMEDS competency framework?
가상 진료의 성장에 따라 의사는 가상 환경에서 진료하는 데 적응해야 합니다. 이를 위해서는 의사 역량 프레임워크의 상당한 수정이 필요합니다. 환자 중심의 팀 기반 치료를 최적화하기 위해 여러 의료 전문 분야의 질병 진단 및 치료와 P2P 커뮤니케이션에서 이러한 도구에 대한 의존도가 높아짐에 따라 이를 통합할 필요가 있습니다. With the growth of VC, physicians must adapt to performing in the virtual environment. This will require substantial modification of the physician competency framework. There is need to incorporate the greater dependence on these tools in the diagnosis and treatment of ailments across medical specialties and in peer-to-peer communication to optimize patient-centred team-based care.
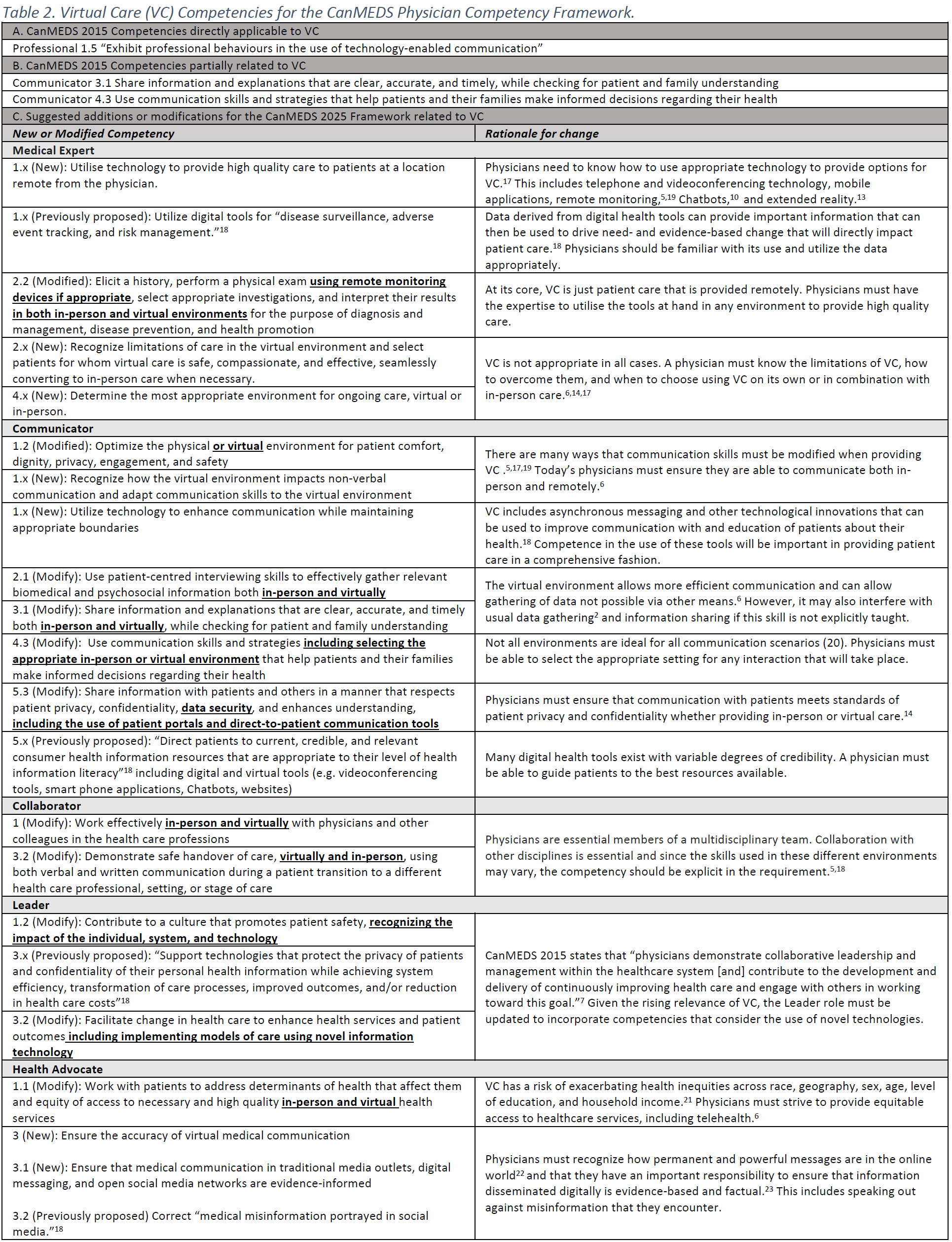
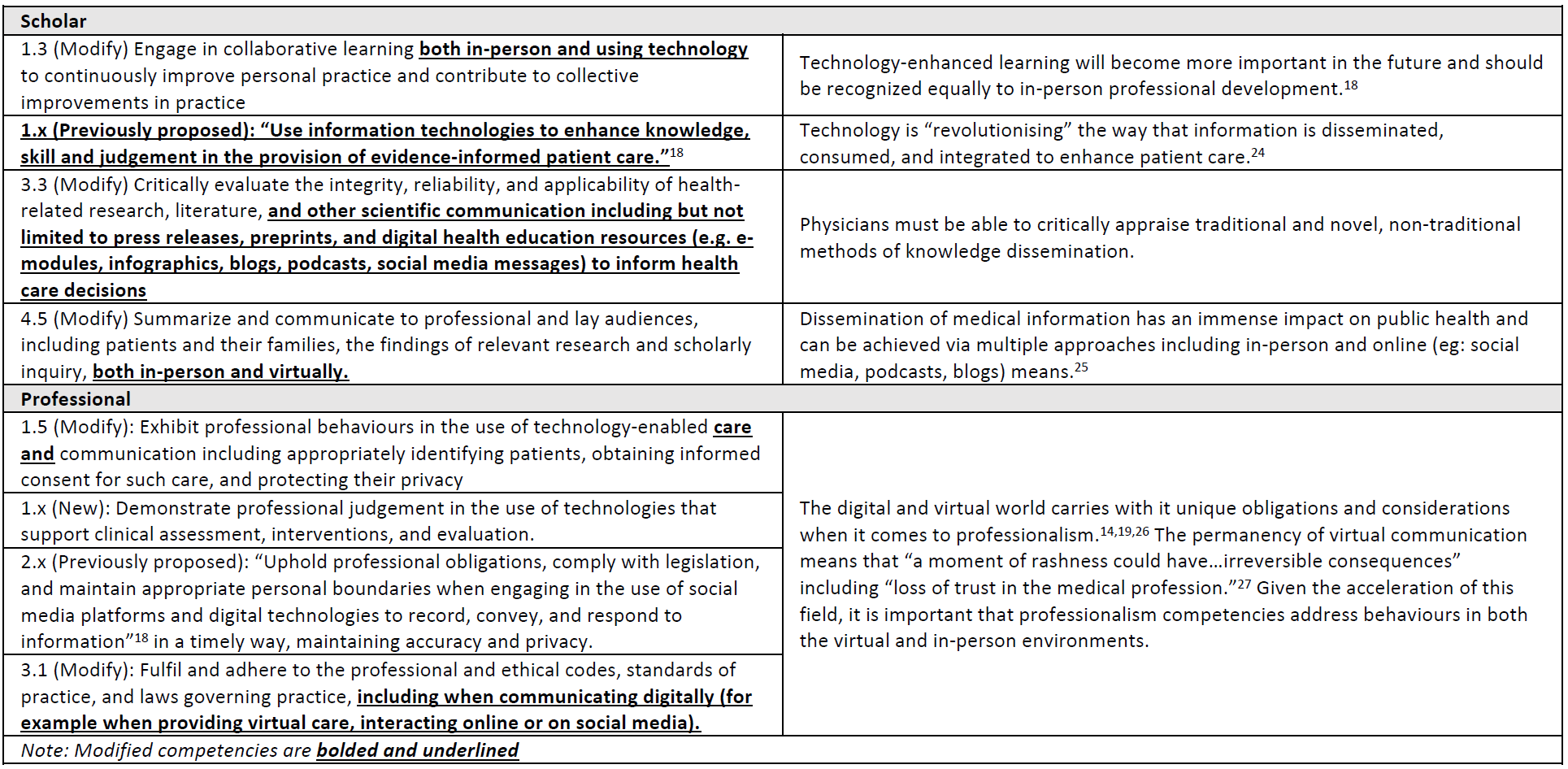
모든 역량을 아우르는 VC를 더 잘 대표할 수 있도록 CanMEDS 의사 역량 프레임워크의 변경을 제안하며, 표 2에서 권장 사항과 그 근거를 CanMED 역할별로 세분화하여 설명합니다. We suggest changes to the CanMEDS Physician Competency Framework to better represent VC spanning all competencies and describe our recommendations and their rationale, broken down by CanMEDs role, inTable 2.
전반적으로 의료 전문가 역할에 대한 변화는 안전하고 포괄적인 환자 치료를 제공하기 위해 가상 도구를 사용하여 전문성을 개발하는 데 중점을 둡니다.
커뮤니케이터 역할은 가상 환경에서는 의사소통 기술이 다르다는 점을 인식하고 의사가 기술 사용과 관계없이 훌륭한 커뮤니케이터가 되어야 한다는 점을 강조합니다.
협력자 역할은 다학제 팀의 대면 및 가상 협업을 포함하도록 수정되었습니다.
리더 역할은 의료 시스템이 가상 현실에 의해 어떻게 영향을 받는지, 그리고 가상 현실을 포함한 새로운 치료 모델이 현재의 의료 서비스 제공 방식을 어떻게 개선할 수 있는지를 강조합니다.
건강 옹호자 역할은 VC에 대한 공평한 접근성, 디지털 헬스를 활용하여 지역사회의 필요를 파악하는 방법, 디지털 시대의 미디어 옹호에 대해 다룹니다.
학자 역할은 기술을 최신 상태로 유지하고 사용하는 데 중점을 두며, 인터넷으로 인해 의료 문헌이 전통적인 저널 논문을 넘어 진화하고 있음을 인식합니다.
마지막으로 전문가 역할은 가상 현실의 사용이 증가함에 따라 이제야 필요성이 대두된 기술과 보호 메커니즘을 포함합니다.
Overall, changes to the Medical Expert role focus on developing expertise using virtual tools to provide safe, comprehensive patient care.
The Communicator role recognizes that communication skills are different in a virtual setting and emphasise that physicians need to be excellent communicators regardless of the use of technology.
The Collaborator role is modified to include in-person and virtual collaboration in multidisciplinary teams.
The Leader role highlights how the healthcare system is impacted by VC, and how new models of care (including VC) can improve upon current approaches to healthcare delivery.
The Health Advocate role focuses on equitable access to VC, how digital health can be leveraged to identify community needs, and touches on media advocacy in the digital age.
The Scholar role focuses on staying up to date with and using technology and recognizes that due to the internet, healthcare literature is evolving past the traditional journal article.
Finally, the Professional role includes the skills and safeguarding mechanisms that have only now become necessary, given the increase in the use of VC.
결론 Conclusion
코로나19 팬데믹으로 인해 VC는 갑작스럽게 환자 치료의 최전선에 서게 되었습니다. 이 기술은 2015년부터 사용되어 왔지만, 당시에는 이 새로운 치료 모델에 대한 역량이 상당히 부족했습니다. 의사들이 사회적 요구와 기대에 부응하는 진료에 진정으로 대비할 수 있도록 기술적으로 개선되었든 그렇지 않든 모든 환경과 관련된 역량을 반영하도록 CanMEDS 2025를 업데이트하는 것이 필수적입니다. The COVID-19 pandemic has abruptly forced VC to the forefront of patient care. Although it has been around since CanMEDS 2015, the competencies at the time focused substantially less on this new model of care. It is imperative that CanMEDS 2025 is updated to reflect competencies relevant to all environments, technologically enhanced or otherwise, so that physicians are truly prepared for practice relevant to societal needs and expectations.
Can Med Educ J. 2023 Mar 21;14(1):22-26.doi: 10.36834/cmej.75439.eCollection 2023 Mar.
CanMEDS 2025에서 임상학습환경 (Can Med Educ J.2023) The Clinical Learning Environment in CanMEDS 2025
소개 Introduction
임상 학습 환경(CLE)은 현재 CanMEDS의사 역량 프레임워크에서 잘 드러나지 않는 다면적 개념입니다.1 의료 환경은 사람 및 관계 중심 치료의 기본 원칙을 바탕으로 구축되며, 우리는 환자 치료 제공과 교육 프로그램 실행이라는 동시적 목표가 학습자와 교수진의 관심을 끌기 위해 어떻게 경쟁할 수 있는지에 대해 생각해 보아야 합니다. 이러한 긴장을 탐구하면 학습자를 포함한 환자, 가족, 지역사회, 의료진 등 학습 환경의 모든 구성원의 요구에 부응하는 개입을 설계하고 실행할 수 있습니다. The Clinical Learning Environment (CLE) is a multi-faceted concept that is currently underrepresented in the CanMEDS physician competency framework.1Healthcare environments are built on the foundational tenet of person and relationship-centered care, and we must reflect upon how the concurrent objectives of delivering patient care and implementing educational programs may compete for the attention of learners and faculty. Exploration of these tensions will enable the design and implementation of interventions that are responsive to the needs of all citizens in the learning environment including patients, families, communities, and the healthcare workforce, including learners.
위계와 권력 비대칭은 의료 시스템, 더 넓게는 CLE에 만연한 요소로, 더 많은 주의가 필요합니다2. 동전의 양면처럼, CLE 내에서 개입을 어떻게 설계하느냐에 따라 팀과 의료 서비스 제공이 기능적으로 또는 역기능적으로 발전할 수 있습니다. 포용적이고 심리적으로 안전한 의료 환경을 조성하면 환자 안전 및 경험 개선, 팀 역학 지원, 학습자 및 모든 팀원의 전문성 개발이 보장되며, CanMEDS는 이러한 목표를 반영해야 합니다. Hierarchies and power asymmetries are pervasive elements of healthcare systems, and the CLE more broadly, that require further attention2. Like two sides of the same coin, how interventions are designed within the CLE, can foster functional or dysfunctional teams and healthcare delivery. Creating inclusive, psychologically safe healthcare environments ensures improved patient safety and experience, supportive team dynamics, and professional development for learners and all members of the team; CanMEDS must reflect these objectives.
임상 학습 환경이란 무엇이며 의사의 역량에 중요한 이유는 무엇인가요? What is the Clinical Learning Environment and why is it important to physician competency?
임상 학습 환경은 "...참여자의 경험, 인식, 학습을 둘러싸고 형성하는 사회적 상호작용, 조직 문화 및 구조, 물리적 및 가상 공간"으로 정의되어 왔습니다.3 다른 정의에서는 "업무 환경과 교육적 맥락 사이의 중첩된 공간"을 언급하기도 합니다. "4
이러한 정의는 학습자 연속체(학부, 대학원 및 평생 의학 교육)와 진료 맥락을 아우르며, 건축적 경계, 디지털 공간, 사회문화적 측면, 교육 커리큘럼, 다양성 및 포용성, 학습의 심리학적 이론, 실천 커뮤니티를 포함한 CLE의 모든 측면을 고려합니다.
5 이러한 정의는 CLE를 복잡하고 중요한 구조, 즉 모든 CanMEDS 역량에 영향을 미치는 규범, 행동, 무언의 행동 강령에 영향을 미치는 구조로 파악합니다.
대인관계는 시스템과 긴밀하게 연결되어 있습니다. 사람은 규범을 알리고 만들고, 시스템은 행동을 가능하게 하고 영향을 미칩니다.
The CLE has been defined as “…social interactions, organizational cultures and structures, and physical and virtual spaces that surround and shape participants’ experiences, perceptions, and learning.”3Other definitions reference “the overlapping space between the work environment…and the educational context.”4
These definitions span the learner continuum (undergraduate, postgraduate, and continuing medical education) as well as contexts of care, and consider all aspects of the CLE including
architectural boundaries, digital spaces, sociocultural aspects, educational curricula, diversity and inclusion, psychological theories of learning, and communities of practice.5
These definitions cast the CLE as a complex overarching structure–one that influences the norms, behaviours, and unspoken codes of conduct that touch on all CanMEDS competencies.
The interpersonal is tightly linked with the systemic: people inform and create norms, while systems in turn, enable and influence behaviours.
따라서 개인이 의료 및 의료 교육 프로그램에 어떤 영향을 미칠 수 있는지, 그리고 이러한 프로그램이 의료 인력의 모든 구성원을 어떻게 형성하는지 이해하도록 하기 위해서는 모든 CanMEDS 2025 역량의 원동력으로서 CLE를 인정하는 것이 중요합니다. Therefore, acknowledging the CLE as an enabler of all CanMEDS 2025 competencies is critical to ensuring that individuals appreciate how they may influence healthcare and medical training programs, and how these programs, in turn, shape all members of the healthcare workforce.
환자안전, 학습자 경험, 대중의 신뢰 필요성, 의료 시스템(그리고 더 일반적으로는 사회 전반)에서의 책무성 강화 요구는 CLE에 대한 비판적이고 지속적인 검토의 원동력이 되고 있습니다. 환자안전 사고5와 그에 따른 대학원 의학 교육 환경 개선에 대한 옹호,6 지역 사회 기반의 운동은 의료 및 의학교육의 지속적인 불평등에 주목하고 있습니다. Patient safety, learner experience, the need for public trust, and calls for increased accountability within the healthcare system (and across society, more generally) are the impetuses for a critical and ongoing examination of the CLE. Policy changes have resulted from patient safety incidents5and subsequent advocacy for improvement in postgraduate medical training environments;6community-based movements have put a spotlight on persisting inequities in healthcare and medical education.
여러 문헌에서는 의학 커리큘럼7,8,9을 통해 중첩된 억압 시스템이 어떻게 유지되고 있으며, 무례, 배제, 인종차별 및 학대를 허용하고 심지어 가능하게 하는 숨겨진 커리큘럼에 의해 지속되고 있는지에 대해 설명했습니다. 의학 교육의 본질적인 위계적 특성뿐만 아니라 사회적 억압의 축을 통해 학문적 의학에 존재하는 많은 권력 비대칭은 모든 학습자 상호 작용에 영향을 미칩니다. 의학 학습자와 교수진이 직면하는 협박, 차별, 괴롭힘의 높은 유병률11,12은 CLE가 대부분 사회적으로 구성되며, CLE를 형성하고 변화시키는 것은 우리의 도덕적, 신탁적 책임이라는 사실을 상기시켜 줍니다. 학습자와 교수진 모두는 긍정적인 변화의 주체가 될 수 있는 잠재력을 가지고 있으며 CLE에 의미 있는 기여를 할 수 있습니다. The literature has described how overlapping systems of oppression are upheld directly through medical curricula7,8,9and are perpetuated by a hidden curriculum that allows and even enables disrespect, exclusion, racism,10and mistreatment. The many power asymmetries that exist in academic medicine, both through the inherently hierarchical nature of medical training but also through societal axes of oppression, influence every learner interaction. The high prevalence of intimidation, discrimination, and harassment faced by medical learners and faculty11,12reminds us that the CLE is largely socially constructed, and it is our moral and fiduciary responsibility to shape and change it. Learners and faculty alike have the potential to be positive change agents and contribute meaningfully to the CLE.
CLE에 대한 다양한 증거 기반 척도가 발표되었습니다.4,13
의학전문대학원 교육 인증위원회에서는 이미 인증 절차에 CLE에 대한 공식적인 검토를 포함시켰는데, 임상 학습 환경 검토(CLER) 프로그램으로 알려진 검토 절차는 미국 인증 기관의 CLE 상태와 졸업생의 향후 진료 스타일에 대한 통찰력을 제공합니다4.
마찬가지로 캐나다 레지던트 인증 컨소시엄도 형평성, 다양성, 포용성 및 기타 학습 환경 고려 사항을 대학원 의학교육 인증 과정에 직접 인정하고 통합하는 것을 우선시하고 있습니다.14
이는 CanMEDS 2025 내에서 CLE를 공식적으로 인정하여 의사 역량 프레임워크를 인증 표준과 일치시켜야 할 필요성을 시사하는 것입니다. Various evidence-based measures of the CLE have been published.4,13
The Accreditation Council for Graduate Medical Education has already incorporated formal review of the CLE into their accreditation processes–a review process, known as the Clinical Learning Environment Review (CLER) Program, provides insight into both the status of American accredited institutions’ CLEs and future practice styles of their graduates4.
Similarly, the Canadian Residency Accreditation Consortium has also prioritized acknowledging and integrating equity, diversity, inclusion, and other learning environment considerations directly into the postgraduate medical education accreditation process.14
This speaks to the need for the CLE to be formally acknowledged within CanMEDS 2025, bringing the physician competency framework into alignment with accreditation standards.
임상 학습 환경은 2015 CanMEDS 역량 프레임워크에서 어떻게 표현됩니까? How is the Clinical Learning Environment represented in the 2015 CanMEDS competency framework?
실무 그룹은 학자, 리더, 전문가 역할 내에서 CLE 관련 지원 역량을 확인했습니다(표 1A 및 및1B).1B). 2015년 CanMEDS 프레임워크 초안이 작성된 이후 캐나다 사회 전반에서 #미투, #흑인 생명도 소중하다, 진실과 화해 등의 지역사회 기반 운동과 관련된 책임에 대한 요구가 증가했습니다. 이러한 운동은 의료진, 특히 환자, 가족, 커뮤니티의 생생한 경험을 반영하기 때문에 의료와 직접적인 관련이 있습니다. 역사적으로 CLE의 사회적 차원에 대한 고려가 이루어졌지만, CLE를 구성하는 규범을 가능하게 하거나 방해하는 데 있어 권력, 특권, 사회적 위치가 어떤 역할을 하는지에 대한 더 많은 조사가 필요합니다. 의사와 기타 의료 서비스 제공자가 모든 행동(및 무행동)을 통해 CLE를 어떻게 형성하는지 이해하려면 여러 CanMEDS 역할에 걸쳐 역량을 업데이트해야 합니다. Our working group identified CLE-specific Enabling Competencies within the Scholar, Leader, and Professional Roles (Table 1Aandand1B).1B). Since the 2015 CanMEDS framework was drafted, there have been increased calls for accountability across Canadian society related to community-based movements such as #MeToo, #BlackLivesMatter, and Truth and Reconciliation, among others. These movements have direct relevance to healthcare as they reflect lived experiences of healthcare teams and, importantly, patients, families, and communities. Historically, although consideration has been given to the social dimensions of the CLE, greater interrogation of the role that power, privilege, and social location play in enabling or disrupting the norms that comprise the CLE is required. Understanding the CLE, and how physicians and other health care providers shape it through their every action (and inaction), will require updates to competencies across multiple CanMEDS Roles.
임상 학습 환경이 2025 CanMEDS 역량 프레임워크 내에서 어떻게 더 잘 표현될 수 있을까요? How can the Clinical Learning Environment be better represented within the 2025 CanMEDS competency framework?
다가오는 CanMEDS 2025 개정판(표 1C)에 CLE의 중심이 되는 개념을 보다 직접적으로 통합할 수 있는 여지가 있습니다. CLE는 전통적인 의미의 '기술'이 아니라는 점을 인정하지만, 심리적 안전, 문화적 겸손, 제도적 문화 변화에 대한 개념은 다른 CanMEDS 역량이 뒷받침할 수 있는 틀을 제공합니다. There is room to more directly incorporate concepts that are central to the CLE in the forthcoming CanMEDS 2025 revisions (Table 1C). While we acknowledge that the CLE is not a ‘skill’ in the traditional sense, it frames notions of psychological safety, cultural humility, and institutional culture change that other CanMEDS competencies would support.
심리적 안전은 "학습자가...자신의 업무 환경을 개인 내적 위험이 내재된 행동에 참여하는 데 도움이 되는 것으로 인식하는 정도"로 정의할 수 있습니다.15 심리적으로 안전한 학습 환경은 학습, 의사소통, 팀 결속, 협업, 환자 경험 및 결과에 긍정적인 영향을 미칩니다.16,17,18 심리적 안전을 증진하는 것에 대해 명시적으로 언급하는 것은 성장 마인드를 촉진하는 데 매우 중요합니다.8 역량 기반 교육에 필요한 특성이며19 의료계에 만연한수치심 기반 교육 접근법과 대조되는 특성입니다.8 Psychological safety can be defined as “the degree to which learners…perceive their work environment as conducive to engaging in behaviours that have inherent intrapersonal risk.”15Psychologically safe learning environments have positive impacts on learning, communication, team cohesion, collaboration, patient experiences, and outcomes.16,17,18Being explicit about fostering psychological safety is critically important to promoting a growth mindset,8a characteristic that is necessary in competency-based training19and contrasts with the shame-based teaching approaches that remain pervasive in medicine.8
문화적 겸손은 자기 성찰과 비판에 대한 평생의 헌신을 반영합니다. 문화적 겸손에는 다음이 포함됩니다.20
자신의 사회적 위치에 대한 인식을 키우고,
타인의 경험을 완전히 이해하는 데 있어 자신의 한계를 인식하며,
타인을 자신의 경험에 대한 전문가로 바라보고,
신뢰에 기반한 관계를 조성하는 것
문화적 겸손에는 지속적인 학습과 탈학습에 대한 헌신과 함께 반인종주의 및 트라우마 정보에 기반한 접근법에 기반한 지식, 기술 및 태도를 개발하는 것이 포함됩니다. Cultural humility reflects a lifelong commitment to self-reflection and critique. It involves
cultivating an awareness of one’s social location,
recognizing one’s limitations in fully understanding the experiences of others,
viewing others as experts of their own experiences, and
Cultural humility involves developing knowledge, skills, and attitudes grounded in anti-racism and trauma-informed approaches, with commitment to ongoing learning and unlearning.
마지막으로, 우리 모두는 다양한 인구의 요구를 대표하고 이에 대응할 수 있는 의료 인력을 양성하고 지원해야 할 공동의 책임이 있습니다. 이러한 목표를 달성하기 위해서는 모든 의료 서비스 제공자가 현재의 대표성 격차를 해소하고 모두가 소속감을 느낄 수 있는 환경을 조성하기 위한 제도적 문화 변화에 동참해야 합니다. Finally, we all have a collective responsibility to be intentional about building and supporting a healthcare workforce that is representative of, and responsive to, the needs of our diverse population. This goal requires all healthcare providers to be part of creating institutional culture change to create environments in which the current representation gap is eliminated, and everyone feels like they belong.
CLE를 비정치적인 실체apolitical entity로 보는 경향은 오늘날 우리가 봉사하는 학습자, 교사, 환자, 가족 및 지역사회의 요구를 충족하는 학술 의학의 능력에 해를 끼쳤습니다. CanMEDS 2025는 모두에게 포용적이고 심리적으로 안전한 환경,그리고 가장 중요한 것은 환자, 가족, 지역사회를 위한 최상의 경험과 결과를 보장하는 데 필요한 역량의 습득과 유지를 적극적으로 지원하는 방법과 CLE에 대해 우리가 생각하는 방식에 필요한 미묘한 차이를 가져올 수 있는 기회를 제공합니다. 광범위한 범위를 고려할 때, CLE는 자연스럽게 CanMEDS의 모든 역량을 다루게 될 것이며, 다른 실무 그룹과 권고 사항이 중복될 것으로 예상됩니다. 선택된 역량의 중요성은 해당 역량이 워킹그룹 활동 전반에서 어떻게 증폭되거나 수렴되는지 관찰함으로써 쉽게 파악할 수 있습니다. The tendency to view the CLE as an apolitical entity has been to the detriment of academic medicine’s ability to meet the needs of the learners, teachers, patients, families, and communities that we serve today. CanMEDS 2025 offers us an opportunity to bring much needed nuance to how we think about the CLE and how we proactively support the acquisition and maintenance of the competencies needed to ensure inclusive and psychologically safe environments for all and most importantly, the best possible experiences and outcomes for our patients, families, and communities. Given its wide-reaching scope, the CLE will naturally touch on all the CanMEDS competencies, and we anticipate overlap in our recommendations with other working groups. The importance of select competencies will be readily identified by observing how they are amplified or converge across working group efforts.
자율 규제 전문직으로서, 우리는 학습자와 교수진 모두에게 CLE와 관련하여 재구상된 역량에 대한 책임을 부여해야 합니다. 이러한 책임을 다하기 위해서는 이러한 역량을 습득하고, 실행하고, 가르치는 방법을 설계, 구현 및 평가하기 위한 리소스가 필요합니다. As a self-regulating profession, we must hold both learners and faculty accountable to these re-imagined competencies relating to the CLE. This accountability will require resources for designing, implementing, and evaluating how these competencies are acquired, practiced, and taught.
Can Med Educ J. 2023 Mar 21;14(1):41-45.doi: 10.36834/cmej.75537.eCollection 2023 Mar.
CanMEDS 2025에서 복잡-적응적 시스템(Can Med Educ J.2023 ) Complex adaptive systems in CanMEDS 2025
소개 Introduction
복합적 적응 시스템은 CanMEDS 의사 역량 프레임워크에서 잘 알려지지 않은 개념입니다.1 복합적 적응 시스템은 환자와 인구를 위한 최적의 의료 결과를 제공하기 위해 복잡한 의료 시스템을 탐색하고 참여하는 것과 관련이 있으며,2 의료 팀이 복합적 적응 시스템으로 기능하는 방식부터 시작합니다.3 이 원고는 이 개념과 현재 및 향후 CanMEDS의 반복에 대한 연관성을 요약하는 것을 목표로 합니다. Complex Adaptive Systems are underrepresented in the CanMEDS physician competency framework.1As a concept, it relates to navigating and engaging with our complex health system in service of optimal health care outcomes for patients and populations,2starting with how healthcare teams function as complex adaptive systems.3This manuscript aims to summarize the concept and its links to current and future iterations of CanMEDS.
복잡적 적응 시스템이란 무엇이며 의사의 역량에 중요한 이유는 무엇인가요? What are Complex Adaptive Systems and why are they important to physician competency?
복잡성이란 사물이 예기치 못한 돌이킬 수 없는 방식으로 상호 작용하는 풍부한 상호 연결성을 말합니다. WHO에 따르면 "보건 시스템은 건강을 증진, 회복 및/또는 유지하는 것을 주된 목적으로 하는 조직, 사람, 행동과 같이 상호 작용하고 상호 의존하는 모든 구성 요소로 이루어져 있다."4 이는 복잡적 적응 시스템의 정의와 일치합니다:
복잡적,다양한 요소 사이에 수많은 비선형 연결이 있는 다양성을 의미하고,
적응적,변화하는 맥락 내에서 경험을 통해 학습하고 변화하는 역량을 시사하며,
시스템, 상호 의존적으로 연결된 에이전트의 집합입니다.5,6
Complexity is about rich interconnectivity whereby things interact in unexpected and irreversible ways. According to the WHO, “The health system consists of all interacting and interdependent components, such as organizations, people, and actions, whose primary intent is to promote, restore, and/or maintain health.”4That aligns with the definition of a complex adaptive system:
complex, implying diversity with a great number of non-linear connections between a wide variety of elements;
adaptive, suggesting the capacity to learn from experience and change within a changing context;
system, a set of interdependently connected agents.5,6
역사적으로 캐나다 의료 시스템은 병원 내 치료를 통한 급성 질환 치료에 중점을 두고 설계되었습니다.7 그 결과, 병원과 의사가 매개하는 치료가 우리 시스템의 조직과 자금에 대한 논의를 지배해 왔습니다. 레지던트 수련은 대부분 이러한 구조에 편입되어 그 틀에 맞춰져 왔습니다. 그러나 건강과 질병 관리의 결정 요인은 다층적이고 상호 의존적인 하위 시스템으로, 서로 지속적으로 상호작용하고 영향을 주고받습니다.8 이러한 시스템의 경계는 반투과적이다. 코로나19 팬데믹 기간 동안 생물학적 조건과 사회적 조건 및 상태가 상호 작용하여 개인의 건강 결과를 악화시키거나 해를 입힐 수 있는 취약성을 증가시킴으로써 이러한 시스템의 상호 연결성이 입증되었습니다.9 As historically designed, the Canadian healthcare system focuses on curing acute disease with in-hospital care.7As a result, hospitals and physician-mediated care have dominated the dialogue on our system’s organization and funding. Resident physician training has been largely embedded in and framed by these structures. However, the determinants of health and management of disease are multilayered and interdependent subsystems that continuously interact and influence each other.8The boundaries of these systems are semipermeable. Their interconnectedness was demonstrated during the COVID syndemic as biologic and social conditions and states interacted to increase a person’s susceptibility to harm or worsen their health outcomes.9
각 의사가 보건 시스템의 모든 요소(예: 식량 안보, 주택, 교육, 기후 변화, 가정 간호, 아동 발달, 불평등 등)에 영향을 미칠 수는 없지만, 의사는 이 생태계를 이해하여 환자 및 이 시스템 내의 다른 에이전트와 어떻게 협력할지 선택할 수 있어야 합니다. 이를 위해서는
시스템에 대한 기본적인 이해가 필요하며, 시스템이 조직 구조와 문화에 미치는 영향을 이해해야 한다
관점의 다양성의 중요성을 강조하고,
명확하고 공유된 목적의 범위 내에서 행동하며,
지속적으로 적응할 수 있는 공간을 만들고,
환경의 새로운 변화로부터 학습해야 한다.
While each physician may not be able to influence all elements of the health system (as for example, food security, housing, education, climate change, home care, child development, inequity, etc.), physicians need to understand this ecosystem in order to make choices about how they will engage with their patients and other agents within this system. This requires
a foundational understanding of systems and their influence on organizational structure and culture,
emphasizing the importance of diversity of perspective,
acting within the boundaries of a clear and shared purpose, and
creating spaces for continuous adaptation to, and
learning from emergent changes in the environment.10
이러한 이해를 바탕으로 의사는
모든 이해관계자를 참여시키고,
체계적으로 높은 레버리지(티핑 포인트)를 찾아서 트리거하며,
의도하지 않은 결과 및 시스템 구조와 같은 개념을 인식할 수 있는 기술을 개발해야 합니다. 마지막으로, 의사는
예측할 수 없는 급변하고 역설적이며 얽히고설킨 상황을 받아들이고 대처할 수 있는 태도와 기술을 갖추고, 자신의 행동과 건강을 신중하게 관리해야 합니다.
Building on this understanding, physicians need to
develop the skills to engage all stakeholders,
find and trigger systemic high leverage (tipping) points, and
be aware of concepts like unintended consequences and system structures. Finally, physicians need to
possess the attitudes and skills to accept and deal with rapid, unpredictable, paradoxical, and tangled situations and thoughtfully manage their behaviours, and own wellness.
2015 CanMEDS 역량 프레임워크에서 복합 적응 시스템은 어떻게 표현되나요? How are Complex Adaptive Systems represented in the 2015 CanMEDS competency framework?
2015 CanMEDS 의사 역량 프레임워크의 주요 변경 사항 중 하나는 '관리자' 역할을 '리더' 역할로 변경한 것입니다.11 이러한 변경은 복잡한 의료 시스템 전반에서 질 향상과 자원 관리에 대한 의사의 역할에 더 초점을 맞추기 위해 이루어졌습니다. 리더 역할에 추가된 핵심 역량 중 두 가지(1, 3번)는 복잡한 시스템에서 기능하는 데 필요한 기술에 가장 큰 기여를 했습니다. One of the major changes in the 2015 CanMEDS Physician Competency Framework was the modification of the ‘Manager’ role to the ‘Leader’ role.11This change was made to bring greater focus on physicians’ role in quality improvement and resource stewardship throughout complex health systems. Two of the key competencies added to the role of Leader (1 and 3) contributed most to the skills needed to function in complex systems.
두 번째 건강 옹호자 핵심 역량은 급성 의료 시스템의 요소를 1차 의료 및 예방 의료의 요소뿐만 아니라 건강과 웰빙에 영향을 미치고 옹호가 필요한 다른 요소와 연결하는 시스템적 사고11와도 관련이 있습니다. 마지막으로, 협력자의 역할에는 '치료의 전환' 및 '지역사회 제공자와의 협력'과 같은 개념을 포함하여 시스템적 사고와 연결되는 몇 가지 요소가 있습니다.11 The second Health Advocate key competency also touches on systems thinking11as it connects the elements of the acute healthcare system upstream, not only with those of primary and preventive care, but also with other factors that affect health and wellness and require advocacy. Finally, the role of Collaborator has a few elements that link with systems thinking, including concepts like “transitions of care” and “collaborations with community providers.”11
복잡한 적응형 시스템을 2025 CanMEDS 역량 프레임워크 내에서 어떻게 더 잘 표현할 수 있을까요? How can Complex Adaptive Systems be better represented within the 2025 CanMEDS competency framework?
최근 CanMEDS와 LEADS 리더십 프레임워크를 비교한 결과, CanMEDS 역량은 개별 환자 치료에 초점을 맞춘 일부 영역(자기 주도, 타인 참여, 결과 달성)에 상당한 관심을 기울이는 반면, 복합 적응 시스템과 관련된 광범위한 역량(연합 및 시스템 전환 개발)에는 덜 관심을 기울이는 것으로 나타났습니다.12 지난 몇 년 동안, 특히 COVID-19 팬데믹에 대응하여 발생한 빈번한 시스템 중단은 모든 의사가 복합 적응 시스템에 대한 이해를 높여야 할 필요성을 입증했습니다.13 이 분야의 역량은 의사들이 스스로를 의료 시스템 혁신의 적극적인 참여자로 인식하는 데 도움이 될 것이며, 이 개념이 CanMEDS 2025에서 더욱 구체화되어야 할 개념으로 식별되는 데 기여했을 수 있습니다. A recent comparison of CanMEDS with the LEADS leadership framework found that CanMEDS competencies pay substantial attention to some of the domains focused on the care of individual patients (lead self, engage others, and achieve results), but less attention to broader competencies related to Complex Adaptive Systems (develop coalitions and systems transformation).12The frequent systemic disruptions that have occurred over the past several years, particularly in response to the COVID-19 pandemic have demonstrated the need for a greater understanding of complex adaptive systems by all physicians.13Competencies in this area will help physicians to see themselves as active participants in the transformation of the healthcare system and may have contributed to this concept being identified as one which needs to be fleshed out further in CanMEDS 2025.
CanMEDS 2025에 복합 적응형 시스템을 더 잘 통합하기 위해 제안하는 변경 사항은 표 1에 요약되어 있습니다.
리더 역할에서 제안된 수정 사항은 환자별 결정과 시스템 전반의 결정 사이의 복잡한 상호작용에 대한 혁신, 출현 및 이해를 촉진하는 품질 개선과 함께 복잡성에 기반한 리더십 패러다임에 초점을 맞출 것입니다.14
협력자에서는 복잡한 결정을 내릴 때 다양성과 관점의 차이에 대한 필요성을 보다 명확하게 인정하고 환자와 가족을 넘어 협력자의 개념을 확장할 것을 제안합니다.
'건강 옹호자'에서는 환자와 건강의 사회적 결정 요인 간의 복잡한 상호 작용을 인정하는 제안을 합니다. 마지막으로,
'학자'에서는 교육 활동의 설계 및 제공에 사회 학습 이론의 요소를 통합해야 하는 역량을 포함할 것을 제안합니다.
The changes that we propose to better incorporate Complex Adaptive Systems in CanMEDS 2025 are outlined inTable 1.
Within the Leader role, the proposed modifications would increase the focus on complexity-informed leadership paradigms alongside quality improvement that promote greater support for innovation, emergence and understanding of the complex interactions between patient-specific and system-wide decisions.14
Under Collaborator, we propose more explicitly acknowledging the need for diversity and differences of perspective when making complex decisions as well as broadening the notion of who is a collaborator beyond the patient and family.
For Health Advocate, we make suggestions that would acknowledge the complex interactions between patients and the social determinants of health.
Lastly, under Scholar we suggest including competencies that require the incorporation of elements of social learning theory into the design and delivery of educational activities.
Can Med Educ J. 2023 Mar 21;14(1):50-53.doi: 10.36834/cmej.75538.eCollection 2023 Mar.
CanMEDS 2025에서 데이터-기반 의학(Can Med Educ J.2023 ) Data-Informed Medicine in CanMEDS 2025
소개 Introduction
건강 데이터 및 정보 사용에 대한 의사의 역량 강화의 필요성은 널리 인정받고 있습니다. 최근 검토1에 따르면 데이터 정보 의학은 CanMEDS 의사 역량 프레임워크2에서 충분히 반영되지 않은 개념으로 확인되었으며, 왕립대학의 "인공지능 및 신흥 디지털 기술에 관한 태스크포스 보고서"는 관련 역량을 CanMEDS에 통합할 것을 권고했습니다.3 데이터 기반 의학은 의사가 양질의 환자 의료 서비스를 제공하는 데 필요한 데이터 및 기타 디지털 정보의 수집, 사용, 공유에 필요한 역량과 관련이 있습니다. 이 입문서에서는 데이터 정보 의학의 개념과 이전 및 향후 버전의 CanMEDS와의 연관성을 요약합니다. 가상 진료의 관련 개념은 이번 호의 다른 기사에서 다룹니다.4 The need for enhanced physician competency in the use of health data and information is broadly acknowledged. A recent review1Identified data-informed medicine as a concept that is underrepresented in the CanMEDS physician competency framework2and the Royal College “Task Force Report on Artificial Intelligence and Emerging Digital Technologies” recommended incorporating related competencies into CanMEDS.3Data-informed medicine relates to competencies required for the collection, use, and sharing of data and other digital information that is needed by physicians to deliver quality patient health service. This primer summarizes the concept of data-informed medicine and its links to former and future iterations of CanMEDS. The related concept of virtual care is addressed in another article in this issue.4
데이터 기반 의료란 무엇이며 의사의 역량에 중요한 이유는 무엇인가요? What is Data-Informed Medicine and why is it important to physician competency?
현대 사회의 많은 부분에서 아날로그 정보 프로세스는 풍부한 데이터를 생성하는 디지털 워크플로우로 대체되었습니다. 이러한 변화는 여행, 상거래, 엔터테인먼트, 정치, 사회적 상호작용 등 대부분의 사회 분야에서 혁신을 가져왔습니다. 그러나 의료 분야에서는 이러한 가치 제안을 활용하는 속도가 느리고 디지털 의료 데이터가 기하급수적으로 증가하고 있음에도 불구하고 제대로 활용되지 않고 있습니다. 데이터 아키텍처를 의도적으로 설계하기보다는 거버넌스, 공공 정책 또는 신기술의 부산물로서 우연히 발생하는 경우가 많기 때문에 의료 데이터 구조가 무질서하게 구성되는 경우가 많습니다. 양질의 의료 서비스를 위한 증거 기반 데이터 아키텍처의 근본적인 중요성에 대한 이해가 널리 부족하다는 점이 이러한 접근 방식의 근간을 이루고 있습니다. In much of modern society, analogue information processes have been replaced by digital workflows that are generating an abundance of data. This has been transformative for most sectors of society including travel, commerce, entertainment, politics, and social interaction. However, the health sector has been slow to harness the value proposition, and digital health data are underutilized despite being collected at an exponentially increasing rate. Rather than being intentional in the design of data architecture, our health data construct is frequently disorganized and occurs by happenstance as a byproduct of governance, public policy, or new technologies. A widespread lack of literacy about the foundational importance of evidence-based data architecture to quality health service underlies this approach.
개인 및 인구 수준의 건강 데이터가 의학적 의사 결정 방식을 변화시키면서 의학은 진화하고 있습니다.5
앞으로 의료계는 데이터의 힘을 활용하여 건강 데이터를 일상적으로 수집하고 분석하여 건강 결정 및 시스템 개선에 필요한 지식을 생성하는 학습 의료 시스템을 개발해야 합니다.6
그 결과 환자 치료에 정보를 제공하고 공익을 증진하기 위해 건강 데이터의 수집, 교환, 집계 및 분석을 통합하는 데이터 기반 의학의 실천이 이루어질 것입니다.
데이터 기반 의학은 인간의 인지능력을 대체하는 것이 아니라 의료 서비스 제공자가 의료 데이터를 전문적으로 활용하여 진료를 최적화하도록 요구할 것입니다.
The practice of medicine is evolving as individual and population-level health data change how medical decisions are made.5
Moving forward, the medical profession will need to harness the power of data to develop learning health systems that routinely collect and analyze health data to generate knowledge to inform health decisions and/or system improvements.6
The result will be the practice of data-informed medicine that incorporates the collection, exchange, aggregation, and analysis of health data to inform patient care and promote public good.
Rather than replacing human cognition, data-informed medicine will require health providers to expertly leverage health data to optimize their practice.
'인간과 기계'의 데이터 협력이라는 새로운 패러다임을 뒷받침하기 위해서는 의료 데이터의 수집, 정리, 저장, 교환, 집계, 해석을 통해 양질의 환자 치료를 촉진하는 새로운 의사 역량이 필요합니다.7,8. 현재 의료 정보 시스템의 품질이 다양하고 의료 데이터 아키텍처, 의료 데이터 사용, 양질의 의료 서비스 제공 간의 관계를 보여주는 커리큘럼 콘텐츠가 부족하기 때문에 의사 수련생이 이러한 영역에서 역량을 갖추도록 하는 것은 어려운 일입니다.
학부 의학교육에 보건 데이터 커리큘럼을 의미 있게 통합해야 한다는 요구에도 불구하고8 가시적인 변화는 거의 일어나지 않았으며, 기본적인 보건 데이터 역량이 부족하고 파편화된 디지털 기술 및 공공 정책 환경에서 활동할 것으로 예상되는 의료 전문가 집단이 계속 양성되고 있습니다.
또한 데이터 리터러시 부족과 제대로 통합되지 않은 기술은 의사의 소진에 기여하고 있습니다.9
포괄적인 디지털 의료 데이터의 잠재력을 활용하여 환자 치료와 인구 건강을 개선하려면 의사에게 기초적인 의료 데이터 리터러시와 전문성을 갖추는 것이 필수적입니다. To support this new paradigm of ‘humanandmachine’data cooperationwill require new physician competencies;7,8the collection, organization, storage, exchange, aggregation, and interpretation of health data to facilitate high-quality patient care. Ensuring that physician trainees are competent in these areas is challenging due to current variability in quality of health information systems and a shortfall of curricular content demonstrating the relationship between health data architecture, health data use, and the provision of quality health services.
Despite calls for the meaningful integration of health data curriculum in undergraduate medical education8 little tangible change has occurred, and a cohort of medical professionals continues to be trained who lack basic health data competencies, and are expected to function in a fragmented digital technology and public policy environment.
Further, the lack of data literacy and poorly integrated technology is contributing to physician burnout.9
Equipping physicians with foundational health data literacy and expertise is essential to harness the potential of comprehensive digital health data to improve patient care and population health.
여기에서는 의사가 데이터를 수집, 교환, 집계, 분석하여 올바른 데이터 기반 의학을 실천할 수 있도록 핵심 역량을 강화하기 위해 CanMEDS의 업데이트를 제안합니다(표 1). Herein, we suggest updates to CanMEDS to promote core competencies that will enable physicians to collect, exchange, aggregate, and analyze data to practice sound data-informed medicine (Table 1).
데이터 기반 의학은 2015 CanMEDS 역량 프레임워크에서 어떻게 표현됩니까? How is Data-Informed Medicine represented in the 2015 CanMEDS competency framework?
데이터 기반 의학은 2015 CanMEDS 역량 프레임워크에 포함된 용어가 아니었다.2 의료 정보학은 리더 역할(1.4)에 언급되어 있지만 구체적으로 정의되어 있지는 않습니다. 이러한 역량을 제안하기 위해 캐나다 의학위원회에서 채택한 정의를 활용하는데, 캐나다 의학위원회는 의료 정보학을 "의료 서비스에서 정보[및 데이터] 설계 및 사용에 대한 연구"로 정의합니다.10 의료 정보학에 대한 정의를 다음과 같이 제안합니다: "양질의 의료 서비스를 증진하기 위해 의사가 의료 정보학 지식을 적용하는 것." 2015년 프레임워크에서는 의료 전문가, 건강 옹호자, 학자의 역할에 따른 정보 활용에 대해 언급하고 있지만, 데이터 기반 의료를 최적화하는 데 필요한 여러 역량은 명시되어 있지 않습니다. Data-informed medicine is not a term that is acknowledged in the 2015 CanMEDS competency framework.2Health informatics is mentioned under the Leader role (1.4), but it is not specifically defined. For the purposes of these proposed competencies, we utilize a definition adapted from the Medical Council of Canada, who define health informatics as “the study of information [and data] design and use in health care.”10In turn we propose the following definition of medical informatics:“the application of health informatics knowledge by physicians to promote quality health services.”While the 2015 framework does mention the use of information under the medical expert, health advocate, and scholar roles, the many competencies required to optimize data-informed medicine are not explicit.
2015 CanMEDS 의사 역량 프레임워크에 이러한 개념이 없다는 점을 고려할 때,2 최근 몇 년간 데이터 기반 의학의 중요성이 강조되면서 의료 정보 교환, 의료 데이터 형평성, 의료 데이터 상호운용성 및 데이터 분석에 대한 관심이 높아진 지난 10년 동안 이 분야에서 일어난 변화를 인식하는 것이 중요합니다. When considering the absence of this concept within the 2015 CanMEDS physician competency framework,2it is important to recognize the changes that have occurred in this field over the past decade, marked by an increased focus on health information exchange, health data equity, health data interoperability, and data analytics that have prompted an emphasis on the importance of data-informed medicine over recent years.
데이터 기반 의학이 2025년 CanMEDS 역량 프레임워크 내에서 어떻게 더 잘 표현될 수 있을까요? How can Data-Informed Medicine be better represented within the 2025 CanMEDS competency framework?
왕립대학의 "인공지능 및 신흥 디지털 기술에 관한 태스크포스 보고서"는 데이터 정보 의학을 지원하기 위한 새로운 역량의 중요성을 강조하면서 '디지털 건강 리터러시'를 8번째 CanMEDS 역할로 추가할 것을 제안했습니다.3 그러나 우리는 이 개념과 관련된 역량(가상 진료에 관한 관련 기사4에서도 다루고 있음)이 기존의 CanMEDS 역할에 포함되어야 한다고 생각합니다. 따라서 고유한 역할을 신설하기보다는 데이터 기반 의료의 핵심 요소를 포함하도록 기존 지원 역량을 수정할 것을 제안합니다. Underscoring the importance of new competencies to support data-informed medicine, the Royal College “Task Force Report on Artificial Intelligence and Emerging Digital Technologies” suggested that ‘Digital Health Literacy’ should be added as an eighth CanMEDS role.3However, we believe that competencies related to this concept (which are also addressed in a related article on virtual care4) should span existing CanMEDS roles. We therefore suggest modification of existing enabling competencies to include key elements of data-informed medicine, rather than the creation of a unique role.
2025 CanMEDS에 통합된 개념에는 다음 등이 포함됩니다.
의료 서비스에서 환자 데이터의 교환, 집계, 분석 및 활용을 촉진하기 위한 환자 데이터의 수집 및 저장,
개인 건강 정보에 대한 환자 접근성 개선,
개인 및 시스템 성과 개선을 위한 건강 데이터 사용 촉진
Concepts that have been integrated include
the collection and storage of patient data to facilitate its exchange, aggregation, analysis, and utilization in medical service;
improving patient access to personal health information; and
promoting the use of health data for individual and system performance improvement.
이러한 역량을 효과적으로 통합하기 위해서는 의료 교육 및 의료 서비스에 대한 접근 방식에 체계적이고 문화적인 변화를 수용하는 디지털 시대의 의학교육을 체계적으로 재구상해야 합니다. 의사는 데이터 기반 의료 서비스를 제공하는 데 있어 필수적인 파트너입니다. 의사들이 진료 과정에서 생성하는 데이터는 임상 치료와 의료 시스템 계획, 혁신, 인구 건강 및 연구에 필수적입니다. 이 백서에 설명된 역량은 의료 데이터와 관련된 기회와 위험이 증가함에 따라 의사가 포괄적이고 조율된 환자 중심적인 방식으로 기여할 수 있는 역량을 보장하기 위한 것입니다. To effectively integrate these competencies, a systematic reimagination of digital-age medical education is required that embraces a systemic and cultural shift in our approach to medical training and health service. Physicians are essential partners in the delivery of data-informed care. The data that their practices generate are essential to clinical care and health system planning, innovation, population health, and research. The competencies described in this paper are intended to ensure the capacity of physicians to contribute in a comprehensive, coordinated and patient-centered way as the opportunities and risks associated with health data grow.
Can Med Educ J. 2023 Mar 21;14(1):54-57.doi: 10.36834/cmej.75440.eCollection 2023 Mar.
CanMEDS 2025에서 의사 휴머니즘(Can Med Educ J.2023) Physician Humanism in CanMEDS 2025
소개 Introduction
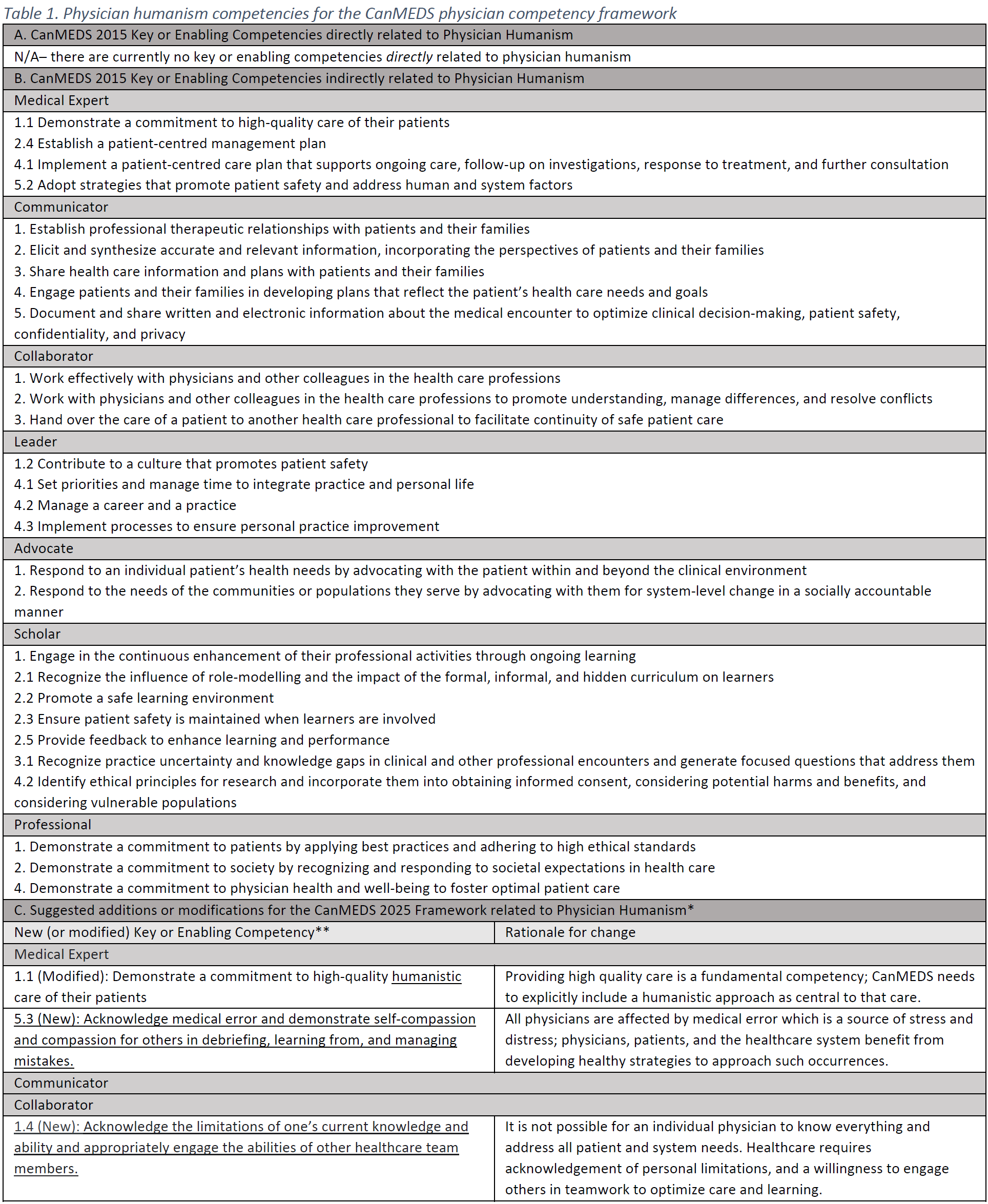
캐나다 의사들은 과중한 의료 시스템에서 일하면서 취약성, 스트레스, 소진에 대한 인식이 부족합니다. 의료 인력 부족, 진료의 복잡성 증가, 코로나19 팬데믹은 이러한 문제를 더욱 심화시켜 환자 치료와 의사의 자기 관리에 영향을 미쳤습니다. 이러한 맥락에서 최근 한 검토에서 의사 휴머니즘이 CanMEDS 의사 역량 프레임워크에서 잘 알려지지 않은 개념으로 확인된 것은 놀라운 일이 아닙니다.1 의사 휴머니즘을 명시적으로 인정하고 존중하는 것은 건강하고 성실한 의사를 개발하고 유지하는 데 필요하며, 이는 환자에게 효과적인 인문학적 치료를 제공할 수 있는 의사의 능력을 뒷받침하는 것입니다.2 Canadian physicians experience underacknowledged vulnerability, stress, and burnout while working in an overburdened healthcare system. Health workforce deficits, increasing complexity of care, and the COVID-19 pandemic have magnified these challenges, impacting patient care and physician self-care. Within this context, it is no surprise that a recent review identified physician humanism as an underrepresented concept in the CanMEDS physician competency framework.1Explicitly acknowledging and honouring physician humanity is necessary to develop and sustain healthy and wholehearted physicians, which also underpins physicians’ ability to provide effective humanistic care for patients.2
의사 인본주의란 무엇이며 의사의 역량에 중요한 이유는 무엇인가요? What is Physician Humanism and why is it important to physician competency?
의사 휴머니즘은 내적 요소와 외적 요소를 모두 포함합니다.
의사가 자신의 인간성을 경험하고 '자기 자신'과의 관계를 발전시키는 것
환자를 인본적으로 돌보고 가족, 동료, 의료 시스템과 상호작용하는 데 기여하는 것
최근 문헌에서 주목받고 있는 주제인 의사의 웰니스는 의사 휴머니즘의 두 가지 측면에 대한 담론과 중요한 연관성을 가지고 있습니다. 역사적으로 의사들은 환자, 팀, 기관 등 타인의 필요를 자신의 필요보다 우선시하는 데 전념해 왔습니다. 의사 사회 계약에 대한 신뢰는 이러한 이타주의에 의해 촉진되며, 이타적인 의사 영웅의 패러다임은 종종 칭송받습니다. 그러나 의사도 개인적인 욕구, 한계, 취약성, 불완전성, 타락성, 사망률을 지닌 인간일 뿐입니다. 의사 휴머니즘의 개념은 의사의 신체적 필요(영양, 수면, 인지적 휴식), 사회적 필요(개인적 안전, 의미 있는 관계), 실존적 필요(가치, 의미)의 정당성과 함께 의사의 고유한 인간성과 인격성을 인정하는 것입니다. Physician humanism has both inward and outward facing components;
physician experiences of their own humanity and development of relationship with “self,” and
physician contributions towards humanistic care of patients and interactions with their families, colleagues, and the healthcare system.
Physician wellness, a prominent topic in the recent literature, has important links to discourse on both facets of physician humanism. Historically, physicians have committed to raise the needs of others—their patients, teams, and institutions - above their own. Trust in the physician social contract is facilitated by such altruism and the paradigm of the selfless physician hero is frequently celebrated. However, physicians are simply human with personal needs, limitations, vulnerabilities, imperfections, fallibility, and mortality. The concept of physician humanism recognizes the inherent humanity and personhood of physicians, along with the legitimacy of their physical needs (nutrition, sleep, cognitive rest), social needs (personal safety, meaningful connection), and existential needs (value, meaning).
실제로 의사가 자신의 인격과 자비로운 관계를 유지하는 것은 환자와 다른 관계에서 인문학적 치료를 확장하는 데 도움이 됩니다. 자기 돌봄은 인간성을 유지하는 데 중요한 기여를 하지만, 휴머니즘은 의사 개인의 필요를 넘어 가치와 관계, 자기와 '존재'가 세상과 타인과의 관계에서 표현되는 방식을 포함합니다.2 타인의 감정에 공감하는 능력인 공감은 의학 교육 과정에서 감소하는 것으로 나타났지만 예술과 인문학에서의 성찰과 경험을 통해 키울 수 있는 휴머니즘의 핵심 요소입니다. 의사가 자기 연민을 발휘하면서 자신의 감정을 파악하고 효과적으로 다룰 수 있는 능력을 유지하는 것은 휴머니즘적 진료의 기본입니다.
In fact, maintaining compassionate connection with their own personhood supports physicians in extending humanistic care to patients and in other relationships. While self-care is an important contributor to maintaining one’s humanity, humanism extends beyond the individual physician’s personal needs to include values and relationships, the ways in which self and “being” are expressed in the world and in relationship with others.2Empathy, an ability to connect with the emotions of another, is a key element of humanism which has been shown to decline throughout medical training but can be nurtured through reflection and experiences in the arts and humanities. It is fundamental to humanistic care that physicians maintain the ability to identify and effectively navigate their own emotions, while employing self-compassion.
의사의 인간성에 대한 부정은 의사의 건강에 해로운 결과를 초래하며, 이는 의사의 건강 악화, 중독, 소진, 자살, 직업 이탈에 대한 통계에서 잘 드러납니다.3 의사와 환자의 인간성에 대한 무시는 현재 시스템에서 인문학적 치료가 부족하다는 피드백에 반영되어 있습니다.4 의료 및 의학교육 시스템은 과도한 업무량, 수면 부족, 부족한 자원, 경쟁 환경, 낙인, 정신건강을 위한 자원 부족 등 의사의 휴머니즘을 위협하는 수많은 요인이 존재합니다.5 의료 및 의학교육 시스템이 의사의 휴머니즘을 포용하고 육성하지 못하면 의사는 환자를 위한 양질의 인문학적 진료를 지속하는 데 어려움을 겪게 될 것입니다. 모든 리더와 이해관계자는 의사의 지속적인 자기 희생의 위험에 함께 맞서야 합니다. 막대한 개인적, 사회적 비용 없이 의사 휴머니즘을 계속 무시하는 것은 현실적이지 않습니다.4 Denial of physician humanity has deleterious consequences for physician wellness that are underscored by statistics on physician ill-health, addiction, burnout, suicide, and exodus from the profession.3Disregard for physician and patient humanity is reflected in feedback on the lack of humanistic care in the current system.4Healthcare and medical education systems present countless threats to physician humanism including excessive workloads, sleep deprivation, insufficient resources, competitive environments, stigma and lack of resources for mental health.5If healthcare and medical education systems fail to embrace and nurture physician humanism, physicians will continue to suffer as will their ability to sustain high-quality, humanistic care for patients. All leaders and stakeholders must together confront the dangers of continuous physician self-sacrifice; it is not realistic to perpetually disregard physician humanism without significant personal and societal cost.4
2015 CanMEDS역량 프레임워크에서 의사 휴머니즘은 어떻게 표현되어 있나요? How is Physician Humanism represented in the 2015 CanMEDS competency framework?
CanMEDS 의사 역량 프레임워크는 "역동적이고 점점 더 까다로워지는 의료 환경에서 사회적 요구"를 충족하기 위해 의사에게 요구되는 역량을 설명합니다.6 이 프레임워크는 "사람으로서의 의사" 역할에 의사 인본주의를 통합한 기초적인 온타리오 미래 의사 교육 프로젝트(EFPO)에서 파생되었습니다.7 이 역할의 일부 개념이 캔메즈 전문가, 의사소통자, 협력자, 리더 역할에 분산되어 있지만(표 1B), 의사의 사람됨은 CanMEDS 에 명확하게 포함되지 않았습니다. 의사의 인격은 인정된 현실이며 역량으로 정의할 수 있는 역할이 아니라고 주장할 수도 있지만, 우리는 의사의 인격이 의사 역량 프레임워크에서 중요한 위치를 차지할 가치가 있다고 생각합니다. 이에 비해 네덜란드에서 채택한 CanMEDS 프레임워크는 꽃의 줄기로서 ' Reflector' 역할을 우선시하며, 의사 수련과 역량에 대한 담론에서 의사 인본주의의 중요성을 강조합니다.8 The CanMEDS Physician Competency Framework describes the required competencies of physicians to meet “societal needs in a dynamic and increasingly demanding health care environment.”6It derives from the foundational Educating Future Physicians of Ontario Project (EFPO), which notably incorporated physician humanism in a “Doctor as Person” role.7While some concepts from this role were distributed among the CanMEDS Professional, Communicator, Collaborator, and Leader roles (Table 1B), physician personhood was not explicitly included in CanMEDS. While it could be argued that physician personhood is an acknowledged reality and not a role to be defined by competencies, we believe it warrants a prominent place in our physician competency framework. Comparatively, the Netherlands’ adaption of the CanMEDS framework prioritizes a “Reflector” role as the stem of the flower, asserting the importance of this aspect of physician humanism in discourse on physician training and competence.8
CanMEDS 2015의 의사 휴머니즘 관련 역량은 타인(환자, 동료, 기관)의 외형적 요구에만 초점을 맞추고 의사 자신의 인간성에 대한 충분한 관심을 소홀히 한다는 점에서 제한적이며 잠재적으로 해로울 수 있습니다. CanMEDS는 의사가 자신의 인간성을 효과적으로 탐구하고 육성하는 데 필요한 역량과 평생의 개인적, 직업적 정체성 형성을 통해 자아에 대한 인문학적 접근을 적절히 인정하지 않습니다. The competencies related to physician humanism in CanMEDS 2015 are limited and potentially harmful in that they focus solely on the outward facing needs of others (patients, colleagues, and institutions), while neglecting sufficient attention to physicians’ own humanity. CanMEDS does not adequately acknowledge the competencies required by physicians to effectively explore and nurture their own humanity and a humanistic approach to self through lifelong personal and professional identity formation.
의사 인본주의가 2025 CanMEDS 역량 프레임워크 내에서 어떻게 더 잘 표현될 수 있을까요? How can Physician Humanism be better represented within the 2025 CanMEDS competency framework?
2025 CanMEDS 프레임워크 업데이트는 의사 휴머니즘을 보다 명시적으로 인정하고 가치를 부여하여 의사, 환자, 의료 시스템의 복지에 필수적인 관련 역량을 강조할 수 있습니다.7-9 그러나 이는 쉽지 않을 것입니다. 복잡한 구조인 의사 휴머니즘은 쉽게 정의하거나 가르치거나 평가할 수 없습니다. 더 큰 문제는 이러한 구조와 관련된 역량을 정의하고 평가하는 것이 애초에 의사의 휴머니즘을 높이는 근본적인 가치와 목표를 훼손할 수 있다는 점입니다.9 예를 들어, 평가를 위해 휴머니즘적 행동을 정의하면 다음의 위험이 따릅니다.
환원주의,
성과 전시,
교과과정에 투자할 가치가 있는 휴머니즘의 관찰 불가능한 측면(예: 감정, 가치) 무시,
자기 관리 및 건강에 대한 개인적인 경험의 부적절한 평가,
평생, 반성, 회복을 목적으로 하는 개발 측면에 대한 총평적 평가 스트레스
The 2025 CanMEDS framework update could more explicitly acknowledge and value physician humanism, underscoring its associated competencies as essential to the wellbeing of physicians, patients, and the healthcare system.7-9However, this will be challenging. As a complex construct, physician humanism is not easily defined, taught, or assessed. Worse, defining and assessing competencies related to this construct may undermine the fundamental value and goals of elevating physician humanism in the first place.9For example, defining humanistic behaviours for evaluation risks
reductionism,
performative display,
neglect of non-observable aspects of humanism worthy of curricular investment (i.e., emotions, values),
inappropriate evaluation of personal experiences of self-care and wellness, and
summative appraisal stress for an aspect of development intended to be lifelong, reflective, and restorative.
이러한 위험을 인식하고 14개의 새로운 핵심 역량을 제안하고 기존의 핵심 역량 1개를 조정하여 의사 휴머니즘이 나아갈 방향을 제시했습니다. 이러한 제안은 전문가 의견과 저자 그룹 간의 합의를 바탕으로 개발되었으며, 의사 휴머니즘을 CanMEDS 2025에 보다 직접적으로 통합할 수 있는 수단으로 제안되었습니다(표 1C). 이러한 역량의 평가로 인한 부정적인 영향을 방지하기 위해, 저자들은 이러한 역량을 평가의 목적으로 규정하지 않고 평생의 개인적 및 전문적 개발, 성찰적이고 협력적인 관행, 성장 마인드 증진을 위한 탐구와 육성을 목적으로 규정할 것을 제안합니다.목표 설정, 등급별 경험, 건설적인 피드백, '실패'를 통한 학습을 통해 시간이 지남에 따라 자신과 자신의 능력을 개발할 수 있다는 믿음을 수용하는 성장 마인드를 보건 전문직 교육에 도입하면 학습 환경 개선, 학습자 복지, 어려움 속에서도 회복력 향상 등의 이점을 얻을 수 있습니다.10 Acknowledging these risks, we have outlined a way forward for Physician Humanism by suggesting 14 new key competencies and adapting one existing key competency. These suggestions were developed based on expert opinion and consensus among our author group as a proposed means by which physician humanism could be more directly integrated into CanMEDS 2025 (Table 1C). To prevent adverse impacts from assessment of these competencies, the authors propose they are not delineated for assessment, but instead for exploration and nurturing of lifelong personal and professional development, reflective and collaborative practices, and promotion of a growth mindset. The benefits of employing a growth mindset in health professions education, whereby belief in the ability to develop oneself and one’s abilities over time through goal setting, graded experiences, constructive feedback, and learning through “failure” is embraced, include enhanced learning environments, learner well-being, and resiliency, even in the face of difficulty.10
이러한 역량을 정교화하는 '인간으로서의 의사' 역할에 우선순위를 두도록 CanMEDS를 확장하면 의사 휴머니즘의 중요성을 더욱 뚜렷하게 부각할 수 있습니다. 이 역할에는 전문성과 타인에 대한 개인적 책임을 넘어 의료 시스템의 어려운 제약 속에서 의사들이 자신에 대한 인문학적 접근 방식을 개발할 수 있도록 지원하는 역량이 포함될 것입니다. 의사 휴머니즘은 모든 역량 역할에 걸쳐 의사의 효과성에 영향을 미치므로, CanMEDS의 업데이트된 그림 표현은 '인격체로서의 의사' 역할을 꽃의 줄기, 잎, 뿌리와 같이 지지하고 양육하는 부분으로 상징할 수 있습니다.7,8 Preferably, expanding CanMEDS to prioritize a ‘Doctor as Person’ role in which these competencies are elaborated would more distinctly highlight the importance of physician humanism. This role would include competencies that extend beyond professionalism and personal responsibility to others, to support doctors in developing a humanistic approach towards themselves as well, within the challenging constraints of the healthcare system. As physician humanism influences the effectiveness of physicians across all competency roles, an updated pictorial representation of CanMEDS could symbolize the ‘Doctor as Person’ role as the supporting and nurturing parts of the flower: the stem, leaves and roots.7,8
Can Med Educ J. 2023 Mar 21;14(1):13-17.doi: 10.36834/cmej.75536.eCollection 2023 Mar.
CanMEDS 2025에서 형평성, 다양성, 포용성, 사회적 정의 (Can Med Educ J.2023) Equity, diversity, inclusion, and social justice in CanMEDS 2025
소개 Introduction
의료 분야의 사회 정의는 각 개인이 속한 다양한 공동체에 관계없이 건강, 복지, 기회 및 특권에 대한 권리가 다른 사람과 동일하다는 것을 지지합니다.1 사회 구조의 모든 측면에서 배제는 다수 인구의 권력을 확보하는 수단이 되어 왔으며, 의료 인력 구성2과 다양한 인구 및 지역사회의 환자에게 제공되는 치료의 가용성과 질 모두에 명백한 영향을 미쳤습니다.3,4 의사 인력은 성별 및 젠더, 원주민으로서의 정체성 또는 비주류 인종, 민족, 문화 또는 종교 집단에 속하는 경우, 다양한 능력, 가족의 사회경제적 지위 등 여러 인구집단을 과소 대표하고 있는 것으로 알려져 있습니다.5,6 Social justice in medicine upholds that each individual, regardless of the diverse communities to which they may belong, has the same right to health, wellbeing, opportunities and privilege as another.1Exclusions in all aspects of societal structure have been a means to secure power for the majority population in Canada, and have unequivocally impacted medicine both through the composition of the medical workforce2and the availability and quality of care provided to patients of diverse populations and communities.3,4The physician workforce is recognized to have underrepresentation of several populations including those defined
by their sex and gender;
their identity as an Indigenous person or belonging to non-dominant racialized, ethnic, cultural or religious groups;
이들 및 기타 억압받는 인구집단의 구성원들은 의학 교육 과정에서 불이익, 차별, 배제를 경험하고 있습니다7. 의학교육 시스템은 능력주의를 강화하고, 위계를 지지하며, 인구 집단 간의 차이를 영속화하고, 다른 지식을 배제하는 생물의학 모델을 장려하기 위해 구축되었습니다.8 캐나다 의료 시스템은 보편적 접근의 원칙에 기초하고 있지만, 의료 시스템에서 인종주의, 성차별, 젠더차별, 능력주의, 연령주의 등 여러 형태의 차별과 그 교차점9에서 겪는 피해에 대해 이용 가능한 치료를 받는 것의 이점을 반드시 평가해야 하는 환자들의 실제 경험과는 다른 경우가 많습니다. 이러한 환자들은 다른 환자들과 동일한 수준의 치료를 받지 못하며10 그 결과 더 나쁜 건강 결과를 겪습니다.11 일부 지역에서는 결과의 격차가 더 커지고 있습니다.11 The experiences of members of these and other oppressed populations throughout their medical training are of disadvantage, discrimination, and exclusion7. Medical education systems have been constructed to reinforce meritocracy, support hierarchy, perpetuate differences between population groups, and promote the biomedical model to the exclusion of other knowledges.8The Canadian health care system is founded on the principle of universal access, yet this is often not the lived experience of patients who necessarily assess the benefits of seeking available care against the harms of racism, sexism, genderism, ableism, and ageism among other forms of discrimination, and all their intersections,9they suffer in the healthcare system. These patients are not afforded the same quality of care as others10and suffer worse health outcomes as a result.11In some areas, the gap in outcomes is widening.11
의료계의 변화에 대한 오랜 요구가 행동의 우선순위로 떠오른 지금,12 기존의 CanMEDS 의사 역량 프레임워크는 형평성, 다양성, 포용성, 사회 정의의 개념과 관련된 의사에 대한 기대치를 명시적으로 제시하는 방향으로 발전할 필요가 있습니다.13 우리는 여기서 이러한 개념을 검토하고, 의학교육(모든 저자), 연구(CB, ND, KOT), 임상 진료(모든 저자)에서 형평성 및 반인종주의 이니셔티브의 리더로서의 경험과 캐나다의 원주민(CB), 아프리카계 캐나다인(KOT), 소수 인종(JMM, SR, BMW), 의학계 여성(CB, ND), 장애인(ND)으로서 살아온 경험을 바탕으로 CanMEDS 의사 역량 프레임워크에 통합하기 위한 권고사항을 제시합니다. 독자들은 반인종주의에 대해 구체적으로 다룬 원고도 참고하시기 바랍니다.14,15 With the long call for changes in medicine now prioritized for action,12the existing CanMEDS physician competency framework requires evolution with explicit statements for expectations of physicians related to concepts of equity, diversity, inclusion and social justice.13We review these concepts here and provide recommendations for incorporating these in the CanMEDS physician competency framework drawn from our experiences as leaders in equity and anti-racism initiatives in medical education (all authors), research (CB,ND,KOT), and clinical practice (all authors) as well as our lived experiences as persons of Indigenous (CB), African-Canadian (KOT), and racial minorities in Canada (JMM, SR, BMW), women in medicine (CB, ND), and disabled (ND). We direct readers to also refer to the manuscripts that speaks specifically on the topic of anti-racism.14,15
형평성, 다양성, 포용성, 사회 정의란 무엇이며 의사의 역량에 중요한 이유는 무엇인가요? What are equity, diversity, inclusion, and social justice and why are they important to physician competency?
형평성, 다양성, 포용성, 사회 정의는 차별을 해결한 결과로 간주되어야 합니다.
(모든 사람에게 동일한 분배를 제공하는 평등equality과는 구별되는) 형평성equity은 개인이 한 집단 또는 다수의 집단에 속해 있다는 이유만으로 기회가 줄어들 뿐만 아니라 다른 구조적, 제도적 장벽에 직면하기 때문에 공정성fairness을 달성하는 데 필요한 행동에 차이가 있을 수밖에 없음을 인정합니다.16
다양성은 집단 내 모든 인구의 대표성을 높이고, 변화와 가능성이 무한하며, 다양한 지식과 경험에서 비롯된 관점과 혁신의 기회를 제공하는 것을 의미합니다.17
포용성은 집단 내 다양한 인구 구성원의 존재뿐만 아니라 그 경험의 성격을 말하며, 그들이 그 집단에서 지지받고 가치 있는 구성원이라고 평가하는 것을 말합니다.18
사회 정의는 각 개인이 다른 사람과 동일한 건강, 복지, 기회 및 특권을 가져야 한다는 권리 기반 접근 방식에서 개념화됩니다.1
Equity, diversity, inclusion, and social justice are to be consideredoutcomesof addressing discrimination.
Distinct from equality (which is the same distribution for everyone), equity necessarily accepts there will be variations in actions required to attain fairness, as individuals encounter different structural and systemic barriers as well as reduced opportunities simply by virtue of their membership in a or many population(s).16
Diversity refers to enhanced representation of persons from all populations in a collective, limitless in variations and possibilities, and yielding the opportunity for perspectives and innovations arising from multiple knowledges and experiences.17
Inclusion speaks not only to the presence of but also the nature of the experience of members of diverse populations in a collective, and that they assess they are a supported and valued member of that collective.18
Social justice is conceptualized from a rights-based approach, valuing that each individual should have the same health, wellbeing, opportunities and privilege as another.1
이러한 용어 및 관련 용어에 대한 간략한 정의는 표 1에서 확인할 수 있습니다. Concise definitions of these and related terms are provided inTable 1.
용어 정의 Term
Definition
Ableism
에이블리즘 모든 형태의 장애(예: 신체적, 지적)를 가진 사람에 대한 차별 및/또는 편견. 장애를 가진 사람을 비장애인에 비해 열등한 존재로 규정하는 것입니다. Discrimination and/or prejudice against persons with any form of disability (e.g., physical, intellectual). Persons are defined by their disabilities, and are characterized as inferior to the non-disabled.
Ageism
연령 차별 일반적으로 나이가 많은 사회 구성원에 대한 고정관념, 차별 및/또는 편견, 나이를 기준으로 한 사람에 대한 고정관념, 차별 및/또는 편견입니다. Stereotyping, discrimination and/or prejudice against persons on the basis of their age, typically against older members of society.
Accessibility
접근성 참여의 장벽을 제거하여 모든 사람이 참여할 수 있는 환경을 조성하기 위한 편의 제공. Accommodations are made to remove barriers to participation, resulting in the ability for all to participate.
Anti-oppression
반억압 억압 체제에 도전하는 전략, 이론, 행동 및 관행 The strategies, theories, actions, and practices that challenge systems of oppression
Cultural Safety
문화적 안전 서비스 제공자와 조직이 불평등을 야기하는 편견과 장벽을 해소하는 성찰적이고 인식 있는 관행과 정책의 결과물입니다. 문화적 안전의 존재 여부를 결정하는 것은 서비스 제공자가 아니라 서비스를 받는 사람입니다. An outcome of reflective and aware practice and policy, where providers and organizations address bias and barriers contributing to inequities. It is the recipient of care, and not the provider, who determines if cultural safety is present or not.
Decolonization
탈식민지화 사회 구조, 서비스 및 투자에 대한 자결권을 위한 고유한 권리와 권한을 회복합니다. Regaining inherent rights and power for self-determination of societal structure, services and investments.
Diversity
다양성 집단 내에 가능한 한 다양한 속성이 존재합니다. The greatest possible representation of attributes are present within the collective.
Equity
형평성 불균형이 해소된 공정성과 정의의 달성. Attainment of fairness and justice, with imbalances addressed.
Homophobia
동성애 혐오 레즈비언, 게이, 퀴어 또는 양성애자라는 이유로 사람을 향한 고정관념, 차별 및/또는 편견. Stereotyping, discrimination and/or prejudice against persons on the basis of being lesbian, gay, queer or bisexual.
Inclusion
포용성 모든 사람이 동등하게 환영받고, 지원받고, 가치를 인정받고, 존중받을 수 있도록 보장하는 행동과 접근 방식. Acts and approaches that ensure that all persons are equally welcomed, supported, valued and respected.
Intersectionality
교차성 불평등에 직면한 여러 인구집단의 일원이 됨으로써 발생하는 상호 작용 또는 시너지 효과로 인해 독특한 경험을 할 수 있습니다. Interactions or synergies which arise from being a member of multiple populations facing inequities, and which results in a unique experience.
Meritocracy
능력주의 능력과 성과에 따라 기회와 지위를 부여하지만 모든 사회 구성원의 기회를 제한하는 구조적 불평등을 인정하지 않는 시스템. System of awarding opportunities and status on the basis of ability and performance, but which neglects acknowledging structural inequities that limit opportunities for all members of society.
Racism
인종차별 인종을 이유로 한 사람에 대한 고정관념, 차별 및/또는 편견. Stereotyping, discrimination and/or prejudice against persons on the basis of their race.
Sexism
성차별 성별에 따른 고정관념, 차별 및/또는 편견 일반적으로 여성으로 식별되는 개인에 대한 편견. Stereotyping, discrimination and/or prejudice against persons on the basis of their sex typically against those individuals that identify as women.
Genderism
젠더차별 젠더에 근거한 사람에 대한 고정관념, 차별 및/또는 편견. Stereotyping, discrimination and/or prejudice against persons on the basis of their gender.
Social justice
사회 정의 각 개인이 경제적, 정치적, 사회적 권리와 기회를 모두 누릴 권리가 있다는 것을 장려하는 접근 방식. Approach promoting that each person has the right to the full spectrum of economic, political, and social rights and opportunities.
의사 인력 및 다양한 배경을 가진 환자에게 제공되는 의료 서비스 모두에서 권력과 특권의 불균형에 대한 인식이 증가하고 있지만, 의사는 기존의 불평등을 식별하거나 사회 정의 목표를 향한 진전을 방해하는 복잡한 요인을 이해하도록 타고나지 않았다.19 의사는 의사 동료와 환자 모두를 위한 동맹allies으로서 정보에 기반한 근거 기반 조치를 취하는 데 필요한 기술을 개발해야 합니다.2 While there is increasing recognition of the power and privilege imbalances in both the physician workforce and the care provided to patients from diverse backgrounds, physicians are not intrinsically able to identify existing inequities, nor understand the complex contributors impeding progress towards social justice goals.19Physicians need to develop the necessary skills to take informed and evidence-based action as allies for both physician colleagues and patients.2
형평성, 다양성, 포용성, 사회 정의는 2015 CanMEDS 역량 프레임워크에서 어떻게 표현됩니까? How are equity, diversity, inclusion, and social justice represented in the 2015 CanMEDS competency framework?
CanMEDS 2015 의사 역량 프레임워크에는 의사 인력 및 환자 치료와 관련된 형평성, 다양성, 포용성 및 사회 정의와 관련된 추론이 있지만(표 2A 및 및2B),2B) 명시적으로 다루고 있는 경우는 드뭅니다. 특히, 이 역량들은 의료계, 더 넓게는 사회에 만연한 차별적 신념 및/또는 관행의 존재를 인정하지 않으며, 의사가 사회 정의를 증진하는 활동을 지원하거나 주도하는 데 유능해야 한다는 명시적인 기대치를 제시하지 않습니다. '리더' 및 '건강 옹호자' 측면의 기존 역량 중 적절하고 권한을 부여하는 의사 교육 및 근무 환경 유지와 관련된 내용은 없습니다. 이는 우리 직업에서 배제를 더욱 영속화하고, 다양하고 포용적인 의료 인력을 확보하기 위해 채용과 유지를 지원하는 데 형평성 이니셔티브가 필요하다는 점을 강조하지 않으며, 의학교육에 내재된 위계질서를 해체하는 데 기여하지도 않습니다.8 There are inferences relevant to equity, diversity, inclusion and social justice related to both the physician workforce and patient care in the CanMEDS 2015 physician competency framework (Table 2Aandand2B),2B), but they are rarely explicitly addressed. Specifically, the competencies do not acknowledge the existence of discriminatory beliefs and/or practices rampant in medicine specifically and more broadly in society, and do not set out explicit expectations for physicians to be competent in supporting or leading activities that promote social justice. None of the existing competencies in ‘leader’ and ‘health advocate’ aspects related to upholding appropriate and empowering physician training and work environments. This further perpetuates exclusions in our profession and does not reinforce that equity initiatives are necessary to support recruitment and retention to achieve a diverse and inclusive medical workforce, nor contribute to dismantling the hierarchy inherent in medical education.8
이번 호 캐나다 의학교육 저널에 게재된 논문에서 Adam 외21는 CanMEDS 역할 설명 및 역량에서 '환자'라는 용어가 어떻게 언급되는지를 강조합니다. 역할 설명에서 환자를 치료의 파트너로 포지셔닝하는 경우가 많지만, 건강 옹호자 역량을 제외한 다른 역할의 핵심 및 활성화 역량에서는 환자를 정보와 치료의 수동적인 수신자로 포지셔닝합니다. 이러한 관점에서 볼 때, 이러한 역량은 지속적인 차별을 허용하는 방식으로 기존의 권력 불균형을 악화시키는 것으로 볼 수 있습니다. In a paper published in this issue of the Canadian Medical Education Journal, Adam et al21highlights how the term ‘patient’ is referenced in the CanMEDS role descriptions and competencies. While the role descriptions frequently position patients as partners in care, with the exception of the Health Advocate competencies, the key and enabling competencies of the other roles position patients as passive recipients of information and care. Viewed from this perspective, the competencies could be seen to exacerbate existing power-imbalances in a way that allows ongoing discrimination.
2025 CanMEDS 역량 프레임워크 내에서 형평성, 다양성, 포용성, 사회 정의를 어떻게 더 잘 표현할 수 있을까요? How can equity, diversity, inclusion, and social justice be better represented within the 2025 CanMEDS competency framework?
2025 CanMEDS 역량 프레임워크에 형평성, 다양성, 포용성 및 사회 정의와 관련된 역량을 명시적으로 포함할 것을 권장합니다. 이러한 역량을 포함하면 이 분야의 전문성 개발을 지원하여 의사가 불평등을 적극적으로 식별하고 대처하는 동시에 인력의 다양성과 포용성을 증진하는 데 도움이 될 것입니다. 또한 의사들이 형평성에 취약한 집단에 속하는 환자들과 효과적으로 소통할 수 있는 기술을 개발하여 의료 서비스 제공을 개선하고 체계적이고 구조적인 변화를 위한 옹호 활동을 지원할 수 있도록 하고자 합니다. 이러한 각 측면과 관련된 기존 CanMEDS 역량은 표 2A 및 및2B2B에 요약되어 있으며 표 2C 및 및2D2D에 수정이 제안되어 있습니다. We recommend competencies explicitly related to equity, diversity, inclusion and social justice for the 2025 CanMEDS competency framework. Including such competencies will support professional development in this area that will help physicians to actively identify and combat inequities while promoting diversity and inclusion in the workforce. We also want to ensure physicians develop skills that allow them to effectively engage with patients belonging to equity-deserving groups to both improve the delivery of healthcare and assist in advocacy efforts for systemic and structural change. Existing CanMEDS competencies related to each of these aspects are outlined inTable 2Aandand2B2Bwith suggested modifications inTable 2Candand2D2D.
의사 인력과 관련하여, 우리는 의사가 변화의 주체로 활동하여 인력의 다양성과 포용성을 지원한다는 기대를 강화하는 협력자 및 리더 역할에 새로운 역량을 추가할 것을 권장합니다. 건강 옹호자 역할에 새로 추가된 내용은 다양한 의사의 중요한 역할과 소외된 지역사회에 대한 의료 서비스 제공에 대한 증거를 반영합니다.22 학자 및 전문가 역할에 대한 수정 사항은 수련 중인 의사의 안전한 학습 환경과 의사 동료의 안전한 근무 환경을 보장하는 데 필요한 활동을 강화하는 한편, 의사가 학습자나 동료를 평가할 때 개인의 암묵적 편견을 인식하고 완화할 것을 촉구합니다. Related to the physician workforce, we recommend new competencies under the Collaborator and Leader roles that reinforce the expectation that physicians act as agents of change to support diversity and inclusion in the workforce. A new addition to the Health Advocate role reflects evidence on the critical role of diverse physicians and care delivery to underserved communities.22Modifications to the Scholar and Professional roles reinforce necessary activities to ensure safe learning environments for physicians in training and safe working environments for physician colleagues, while also calling on physicians to recognize and mitigate their personal implicit biases when assessing learners or peers.
또한 사회 정의를 위해 노력하는 의사의 책임을 강화하고 의료 서비스에서 공평하고 문화적으로 안전한23 환자 경험의 결과를 지원하는 전략을 제정하는 새로운 역량에 대한 권장 사항을 제시합니다. 특히, 우리는 심리사회적 평가와 건강의 사회적 결정요인 및 구조적 요인에 대한 불평등 해결을 포함하도록 치료 상호작용에서 의사의 책임을 확대하는 수정을 제안했습니다. 이를 위해서는 차별을 중단하고, 의사와 환자 간 상호작용에서 권력 불균형을 최소화하며, 지역사회 참여와 파트너십을 구축하고, 각 환자의 현실에 맞게 치료를 맥락화하기 위한 구체적인 기술 개발이 필요합니다. 마지막으로, 아담 외21가 설명한 유형의 의사-환자 상호작용의 틀을 해결하고 환자를 의료 서비스의 능동적 주체 및 파트너로 인식하는 언어를 통합하는 방향으로 전환하는 것이 중요합니다. We also make recommendations for new competencies that reinforce the responsibility of physicians to strive for social justice and enact strategies that support outcomes of equitable and culturally safe23patient experiences in healthcare. Specifically, we have suggested modifications that broaden the responsibility of physicians in care interactions to include psychosocial assessment and addressing inequities in the social determinants of health and structural factors. This will require specific skill development in interrupting discrimination, minimizing power imbalances in the physician-patient interaction, community engagement and partnership, and contextualizing care to the realities of each patient. Lastly, it will be important to address the framing of physician-patient interactions of the type described by Adam et al21and shift towards incorporating languages that recognizes patients as active agents and partners in their healthcare.
형평성, 다양성, 포용성, 사회 정의를 증진하기 위해 기존 CanMEDS 프레임워크에 제안된 추가 및 수정 사항은 의학교육에 필요한 중요한 개선 사항을 다루는 것을 목표로 합니다. 이러한 변화는 의료 인력의 대표성을 강화하는 동시에 의료진에게 지원적이고 안전한 근무 환경을 제공하는 동시에 환자 치료에 도움이 되는 향상된 기술을 명시적으로 요구할 것입니다. The proposed additions and revisions to the existing CanMEDS framework to promote equity, diversity, inclusion, and social justice aim to address critical improvements needed in medical education. These changes will strengthen representation in the medical workforce while providing a supportive and safe work environment for practitioners, while also explicitly requiring enhanced skills to benefit patient care.
Can Med Educ J. 2023 Mar 21;14(1):27-32.doi: 10.36834/cmej.75845.eCollection 2023 Mar.
Equity, diversity, inclusion, and social justice in CanMEDS 2025
CanMEDS 의사 역량 프레임워크에서 새로 등장하는 개념들 (Can Med Educ J.2023) Emerging concepts in the CanMEDS physician competency framework (Can Med Educ J.2023)
소개 Introduction
CanMEDS 역량 프레임워크는 1996년에 발표되어 2005년과 2015년에 업데이트되었습니다.3 캐나다4,5 및 국제적으로 의학교육에 큰 영향을 미쳤으며,6-8 커리큘럼 및 프로그램 설계를 변화시켜 과거에는 의학교육에서 충분히 다루지 않았던 역량에 초점을 맞추도록 했습니다. 캐나다 왕립 의사 및 외과의 대학에서 내부적으로 추적한 결과, 현재 전 세계 50개 이상의 관할 지역에서 최소 12개 전문 분야에서 CanMEDS를 사용하고 있으며 수백만 명의 수련생과 환자에게 영향을 미치고 있는 것으로 추산됩니다. The CanMEDS competency framework was published in 19961with updates in 20052and 2015.3It has had a major impact on medical education both in Canada4,5and internationally,6–8transforming curricular and program design to increase the focus on competencies that were historically not addressed adequately within medical education. Internal tracking by the Royal College of Physicians and Surgeons of Canada estimates that CanMEDS is now used in over 50 jurisdictions around the world by at least 12 professions, impacting millions of trainees and patients.
의학교육에서 의사의 역량 프레임워크가 수행하는 중심적인 역할을 고려할 때, 2025년에 계획된 개정판은 새로운 역량을 추가하고 오래된 역량을 제거함으로써 진화하는 사회적 요구에 부응해야 합니다. 이는 특히 코로나19 팬데믹으로 인해 의료 및 의학교육이 계속 차질을 빚고 있고,9-15 건강 및 행동 모니터링에 기술이 점점 더 많이 사용되고 있으며,16,17 식민주의,18 제도적 차별,19 성차별,20 인종차별,21 기후변화22가 건강에 미치는 영향이 점점 더 많이 인식되고 있는 현재 환경과 관련이 있습니다. Given the central role that the CanMEDS physician competency framework plays within medical education, the planned 2025 revision must respond to evolving societal needs through the addition of new competencies and the removal of outdated competencies. This is particularly relevant in the current environment as healthcare and medical education continue to be disrupted by the COVID-19 pandemic,9–15technology is increasingly used to monitor health and behavior,16,17and the impacts of colonialism,18systemic discrimination,19sexism,20racism,21and climate change22on health are increasingly acknowledged.
2015년 개정된 CanMEDS 역량 프레임워크3는 저자 팀원(Van Melle)이 수행한 문헌 검색 및 주제별 분석을 통해 정보를 얻었습니다.23 이 분석은 7가지 새로운 개념(직업적 자아 정체성, 역량의 한 형태로서의 감정, 시스템 기반 실무/실무 기반 학습 및 개선, 인수인계, 글로벌 보건, 소셜 미디어, 의료 분야의 재정적 인센티브)을 확인하고 설명했습니다. 문헌에 초점을 맞추다 보면 발표되지 않은 개념을 놓칠 수 있지만,24 우리는 2025년 CanMEDS 역량 프레임워크의 개정을 위한 광범위한 환경 조사의 일환으로 이 작업을 복제하고 확장하고자 했습니다. The 2015 revision of the CanMEDS competency framework3was informed by a literature scan and thematic analysis performed by a member of our authorship team (Van Melle).23Their analysis identified and described seven emerging concepts (professional self-identity, emotion as a form of competence, systems-based practice/practice-based learning and improvement, handover, global health, social media, and financial incentives in health care). While focusing on the literature may miss concepts that have not been published,24we sought to replicate and expand upon this work as part of a broader environmental scan that will inform the revision of the 2025 CanMEDS competency framework.
2015년 방법론을 기반으로,23 우리는 분석에 광범위한 이해관계자 그룹을 포함하여 방법론을 자세히 설명하고, 의학교육 커뮤니티의 검토와 논평을 위해 결과를 공개적으로 게시함으로써 검색 및 검토 프로세스의 엄격성, 포용성, 투명성을 높이는 것을 목표로 합니다. Using the 2015 methodology as a base,23we aim to increase the rigor, inclusiveness, and transparency of the search and review process by outlining our methodology in detail, including a broad group of stakeholders in the analysis, and openly publishing our results for review and commentary from the medical education community.
방법론 Methodology
문헌 검색, 제목 및 초록 검토, 일반 주제별 분석25을 통해 문헌을 종합하여 CanMEDS 역할과 관련된 새로운 개념을 파악했습니다. CanMEDS내에서 더 잘 표현되어야 할 개념을 식별하는 광범위한 작업 목표를 고려할 때, 일반적인 문헌 검토 전략으로는 우리의 목표를 달성할 수 없다는 사실을 발견했습니다. 그 대신 2015년 CanMEDS 개정 이전에 Van Melle 23에서 사용했던 실용적인 접근 방식을 기반으로 포함할 문헌을 결정하고 분석에 정보를 제공했습니다. We synthesized the literature using a literature scan, title and abstract review, and generic thematic analysis25to identify emerging concepts related to the CanMEDS roles. Given the broad-based goal of our work to identify concepts that needed to be better represented within CanMEDS, we did not find that any common literature review strategies would meet our goals. Rather, we built upon the pragmatic approach previously used by Van Melle23prior to the 2015 CanMEDS revision to determine the literature to be included and inform its analysis.
2015년 신개념 검토는 한 명의 저자가 수행했지만,23 이 검토를 위해 2025년 CanMEDS 개정을 주도하는 기관/단체인 캐나다 왕립 의사 및 외과의사 대학, 캐나다 퀘벡 의과대학, 캐나다 가정의학과 대학, 캐나다 의학부 협회에서 회원 추천을 받아 실무 그룹을 구성했습니다. 검토의 목적상, 새로운 개념은 의사의 역할 및 역량과 관련된 동료 검토 문헌에서 논의된 아이디어 중 2015 CanMEDS 의사 역량 프레임워크에 없거나 과소 대표되는 개념으로 정의했습니다.3 While the 2015 emerging concepts review was conducted by a single author,23for this review we created a working group by soliciting nominations for members from the institutions/organizations steering the 2025 CanMEDS revisions: the Royal College of Physicians and Surgeons of Canada, Collège des Médecins du Québec, College of Family Physicians of Canada, and Association of Faculties of Medicine of Canada. For the purpose of our review, an emerging concept was defined as an idea discussed in the peer reviewed literature related to the role and competencies of physicians that is either absent or underrepresented in the 2015 CanMEDS physician competency framework.3
논문 포함 기준 Article inclusion criteria
Van Melle이 이전 검토에서 사용한 방법과 유사하게 우리는 CanMEDS와 관련된 새로운 개념을 논의할 가능성이 높은 의학 저널을 선택했습니다. 여기에는 저널 임팩트 팩터 기준 가장 영향력이 높은 의학교육 저널 3종(Academic Medicine, Medical Education, Medical Teacher)과 캐나다(Canadian Medical Education Journal) 및 대학원(Journal of Graduate Medical Education) 의학교육과 관련된 콘텐츠를 게재하는 저널이 포함되었습니다. 이러한 접근 방식은 영향력이 가장 높은 의학교육 저널을 중심으로 한 Van Melle의 연구와는 다소 차이가 있지만,23 캐나다 및 대학원 의학교육에 특별히 초점을 맞춘 저널을 포함시키는 것이 중요하다고 생각했습니다. 2018년 10월 1일부터 2021년 10월 1일 사이에 이러한 저널에 게재된 모든 논문이 포함 대상으로 고려되었습니다. 이 3년의 기간은 실현 가능한 범위 내에서 현재와 관련된 개념에 초점을 맞추기 위해 실용적으로 선택되었습니다. Paralleling the methods used by Van Melle in the prior review.23we selected medical journals that would be likely to discuss emerging concepts related to CanMEDS. They included the three highest impact medical education journals by Journal Impact Factor (Academic Medicine, Medical Education, andMedical Teacher) and journals that publish content specifically related to Canadian (Canadian Medical Education Journal) and postgraduate (Journal of Graduate Medical Education) medical education. This approach differed somewhat from Van Melle’s work which was based specifically on the highest impact medical education journals,23but we felt it was important to include journals focused specifically on Canadian and postgraduate medical education. All articles published within these journals between October 1st, 2018, and October 1st, 2021 were considered for inclusion. This three-year time period was pragmatically selected to focus on currently relevant concepts while still being feasible.
데이터 추출 Data extraction
제목과 초록 검토를 용이하게 하기 위해 선택한 저널에서 검토 기간 내에 출판된 모든 논문에 대해 저널 제목, 논문 제목, 인용 데이터를 포함한 메타데이터를 PubMed에서 추출했습니다. 이러한 데이터를 Zotero26으로 가져와서 각 논문의 초록을 포함한 추가 메타데이터를 추가했습니다. 그런 다음 확장된 메타데이터를 Zotero에서 Google 시트로 내보냈습니다. 토마는 예비 검토를 수행하여 새로운 개념에 초점을 맞추지 않을 것 같은 몇 가지 기사 유형을 제외했습니다. 이러한 기사에는 기관 보고서, 작가 성명서, 정정 및 정오표, 에세이 콘테스트 기사, 편집자에게 보내는 편지, 저널에 초점을 맞춘 사설, 다른 기사 목록을 요약한 기사, 심사자 및/또는 기획위원회 위원에게 감사를 표하는 기사 등이 포함되었습니다. 나머지 기사는 표준화된 형식으로 정리하여 개별 실무 그룹 구성원에게 검토를 맡겼습니다. To facilitate the title and abstract review, metadata including the journal title, article title, and citation data were extracted from PubMed for all articles published within the review period in the selected journals. These data were imported into Zotero26which added additional metadata including each article’s abstract. The expanded metadata were then exported from Zotero into a Google Sheet. Thoma performed a preliminary review and excluded several article types because they were unlikely to focus on emerging concepts. These articles included institutional reports, artist’s statements, corrections and errata, essay contest articles, letters to the editor, editorials focused on the journal, articles summarizing lists of other articles, and articles focused specifically on thanking reviewers and/or planning committee members. The remaining articles were arranged in a standardized format and assigned for review to individual working group members.
논문 검토 Article review
15명의 리뷰어 각각은 2021년 10월 10일부터 2021년 11월 30일까지 검토할 기사를 배정받았습니다. 토마는 팀 또는 개별 가상 회의에서 각 리뷰어에게 방향을 제시했습니다. 각 검토자는 자신의 문서에 대해 다음 질문에 답변했습니다: Each of 15 reviewers was assigned articles for review between October 10, 2021 and November 30, 2021. Thoma oriented each reviewer in a team or individual virtual meeting. Each reviewer responded to the following questions for their articles:
이 기사가 CanMEDS 역할과 관련이 있습니까? (예/아니오/아마도)
이 문서가 위에서 정의한 새로운 개념을 설명하는가? (예/아니오/아마도)
예/아니요/아마도 해당한다면, 이 기사가 관련된 주요 역할은 무엇인가요? (의료 전문가, 커뮤니케이터, 협력자, 학자, 건강 옹호자, 리더, 전문가)
해당 역할과 관련된 추가적인 CanMEDS 역할이 있나요? (의료 전문가, 커뮤니케이터, 협력자, 학자, 건강 옹호자, 리더, 전문가)
새로운 개념을 간단한 제목으로 설명해 주세요. (자유 텍스트)
필요한 경우, 새로운 개념에 대한 간략한 설명을 제공하세요. (자유 텍스트)
이 개념은 2015년 버전의 CanMEDS에 (가) 없거나 (나) 과소 대표되는 개념인가요? (A 및 B 옵션이 있는 드롭다운)
이 글은 새로운 개념을 잘 요약한 예시적인 글인가요? (예, 아니오, 아마도)
Does this article relate to the CanMEDS roles? (Yes/No/Maybe)
Does this article describe an emerging concept as defined above? (Yes/No/Maybe)
If yes/maybe, what is the primary role that it relates to? (Medical Expert, Communicator, Collaborator, Scholar, Health Advocate, Leader, Professional)
Are there any additional CanMEDS roles that it relates to? (Medical Expert, Communicator, Collaborator, Scholar, Health Advocate, Leader, Professional)
Please describe the emerging concept as a brief title. (free text)
If necessary, provide a brief description of the emerging concept. (free text)
Is this a concept (a) absent from or (b) underrepresented in the 2015 iteration of CanMEDS? (dropdown with A and B options)
Is this an exemplar article that summarizes the emerging concept well? (Yes, No, Maybe)
질문 1 또는 2에 대한 답변이 '아니오'인 경우, 질문 3~8에 대한 답변이 없는 것으로 간주하여 추가 검토 대상에서 제외합니다. 검토자가 질문 1 또는 2에 대해 '아마도'로 표시한 기사는 두 번째 검토자(토마)가 검토한 후 응답에 따라 포함 또는 제외했습니다. If the response to questions 1 or 2 was ‘no,’ questions 3-8 were not answered and these articles were excluded from further review. Articles that the reviewer tagged as ‘maybe’ for question 1 or 2 were reviewed by a second reviewer (Thoma) and included or excluded based upon their responses.
주제별 분석 Thematic analysis
제목과 초록 검토가 완료된 후, 나머지 논문은 하나의 Google 스프레드시트에 통합되었습니다. 그런 다음 두 명의 저자(토마, 반 멜레)가 질문 5에 대한 검토자의 답변, 검토자가 파악한 새로운 개념, 필요한 경우 논문의 메타데이터를 바탕으로 주제별 분석25,27을 수행했습니다. 이 분석은 주제 분석의 단계를 따랐습니다.28
예비 검토(숙지)를 거친 후 코드북을 개발하고 공동으로 다듬었습니다.
그런 다음 필요한 경우 코드북을 수정하여 모든 기사를 코딩했습니다(코딩).
모든 기사가 코딩된 후, 토마는 코드를 통합한 예비 주제 세트를 개발하고 정의했습니다(주제 검색).
이렇게 만들어진 주제별 프레임워크는 Van Melle이 각 주제를 명확히 하고 정의하기 위해 수정하여 검토, 수정, 승인했습니다(주제 정의 및 이름 지정).
그런 다음, 전체 워킹 그룹에게 피드백 및 수정을 위해 제시되어 구성원 점검(테마 검토)의 첫 번째 단계로 진행되었습니다.
후속 조치로, 구성원 점검(테마 검토)의 두 번째 단계로 Google 설문조사를 통해 워킹그룹 구성원을 대상으로 설문조사를 실시했습니다. 이 설문조사에서는 각 테마에 대한 검토팀의 지지를 요청하고 테마를 어떻게 더 구체화할 수 있는지 물습니다. 이러한 제안은 분석에 반영되었습니다.
After the title and abstract reviews were completed, the remaining articles were amalgamated into a single Google Sheet. Two authors (Thoma and Van Melle) then conducted a thematic analysis25,27of the reviewers’ responses to question 5, the emerging concept identified by the reviewing author and, when necessary, the article’s metadata. This analysis followed the phases of thematic analysis.28
Following a preliminary review (familiarization), we developed and collaboratively refined a codebook.
We then coded all the articles with refinements to the codebook when necessary (coding).
Once all articles were coded, Thoma developed and defined a preliminary set of themes incorporating the codes (searching for themes).
The resulting thematic framework was reviewed, modified, and endorsed by Van Melle with modifications to clarify and define each theme (defining and naming themes).
It was then presented to the full working group for feedback and revision as the first part of the member check (reviewing themes).
In follow-up, a survey of the working group members was conducted via a Google Forms survey as the second part of the member check (reviewing themes). The survey requested endorsement for each of the themes from the review team and asked how the themes could be further refined. These suggestions were incorporated into the analysis.
분석 내내 토마스와 반 멜레는 각자의 위치를 고려했습니다. 토마는 응급 및 외상 전문 의사로, 기술 기반 의학교육(시뮬레이션, 온라인 교육 리소스, 학습 분석)에 중점을 둔 의학교육 연구를 수행하고 있습니다. Van Melle은 프로그램 평가 및 변화, 특히 역량 기반 의학교육 맥락에 대한 전문성을 갖춘 교육 과학 박사 학위자입니다. 두 사람 모두 캐나다 왕립 의사 및 외과의 대학과 계약을 맺고 캐나다 전역의 전문 의사 양성을 위한 교육 개발에 관한 자문을 제공하고 있습니다. 우리는 가상 회의와 다양한 의료 전문 분야 및 CanMEDS 이해관계자의 관점을 담은 저자 그룹과의 후속 설문조사를 통해 각자의 위치로 인한 편견을 완화하기 위해 노력했습니다. Throughout the analysis, Thoma and Van Melle considered their positionality. Thoma is a practicing emergency and trauma physician who conducts medical education research with a focus on technology-enhanced medical education (simulation, online educational resources, and learning analytics). Van Melle is a PhD education scientist with expertise in program evaluation and change, particularly in competency-based medical education contexts. Both are contracted by the Royal College of Physicians and Surgeons of Canada to provide advice regarding educational developments in the training of specialty physicians across Canada. We attempted to mitigate the biases introduced by their positionality through member checks conducted both in a virtual meeting and a follow-up survey with an authorship group that contained perspectives from a range of medical specialties and CanMEDS stakeholders.
삼각측량 Triangulation
출판 지연과 의학 저널의 게이트키핑으로 인해 일부 새로운 개념이 문헌에 나타나지 않았을 수 있다는 점을 인식하고24, 문헌 검색과 병행하여 수행한 온라인 검색 및 주제별 분석의 결과와 결과를 상호 참조했습니다. 이 검색 및 분석의 전체 방법론과 결과는 보고되지 않았고 본 연구의 공식적인 부분은 아니었지만, 저자 중 한 명(Snell)은 새로운 개념을 식별하고 주제별로 분석하기 위해 여러 키워드로 Google 검색 엔진을 사용하여 회색문헌을 검색했습니다. 이 분석 결과를 자체 분석 결과와 상호 참조하여 검색에서 발견되지 않은 회색 문헌에서 떠오르는 개념을 식별함으로써 결과를 삼각측량했습니다. Acknowledging that publication delays and the gatekeeping of medical journals could have prevented some emerging concepts from appearing in the literature24, we cross-referenced our results with the findings of an online search and thematic analysis that was conducted in parallel to our literature scan. While the full methodology and results of this search and analysis have not been reported and were not a formal part of our study, one of our authors (Snell) searched the grey literature using the Google search engine with multiple key words with the goal of identifying and thematically analyzing emerging concepts. We triangulated our results by cross-referencing the findings of this analysis with our own to identify emerging concepts from the grey literature that were not found in our scan.
전문가 검토 Expert review
앞서 설명한 분석이 완료된 후, 토마는 워킹 그룹 멤버와 캐나다 왕립 의사 및 외과의사 임상의사 교육자들에게 10가지 새로운 개념 각각에 대해 전문가를 추천해 달라고 요청했습니다. 이 원고의 저자 팀원과 설문조사에서 추천된 전문가를 결합하여 집필 그룹을 구성했습니다. 각 집필 그룹은 2022년 3월부터 2022년 7월까지 각 개념을 정의하는 간략한 원고를 작성하고, 2015 CanMEDS 의사 역량 프레임워크에서 어떻게 표현되는지 설명하고,3 CanMEDS 2025의 변경 사항을 제안하는 것을 목표로 2~4회 모임을 가졌습니다. 집필 그룹이 각 개념의 이름에 대해 제안한 변경 사항은 검토 및 승인을 위해 실무 그룹에 이메일로 전송되었습니다. Following the completion of the described analysis, Thoma asked the working group members and the Royal College of Physicians and Surgeons of Canada Clinician Educators to nominate experts for each of the ten emerging concepts. Writing groups were formed, combining members of the authorship team for this manuscript and the experts that were nominated in the survey. Each writing group met 2-4 times from March 2022 through July 2022 with the goal of writing a brief manuscript defining each concept, outlining how it is represented in the 2015 CanMEDS physician competency framework,3and proposing changes for CanMEDS 2025. The changes proposed by the writing groups to the name of each concept were emailed to the working group for review and approval.
결과 Results
그림 1에 요약된 바와 같이 관심 기간 동안 포함된 저널에 4973편의 논문이 게재되었습니다. 이 중 505개 논문은 기관 보고서, 저자의 성명서, 정정 또는 오타, 에세이 콘테스트 논문, 편집자에게 보내는 편지, 저널에 초점을 맞춘 사설, 논문 목록이 포함된 논문, 심사자에게 감사하는 논문, 위원회 위원에게 감사하는 논문으로 간주되어 예비 검토에서 제외되었습니다. 4468편의 논문이 제목 및 초록 심사를 받았습니다. 각 심사자는 142~385편의 논문을 검토했습니다(평균 = 298편). 두 차례의 검토를 거친 후 나머지 4468편의 논문 중 1017편(22.8%)이 주제별 분석에 포함되었습니다. As outlined inFigure 1, 4973 articles were published in the included journals during the period of interest. 505 of these articles were excluded in the preliminary review because they were deemed to be institutional reports, artist’s statements, corrections or errata, essay contest articles, letters to the editor, editorials focused on the journal, articles containing lists of articles, articles thanking reviewers, or articles thanking committee members. 4468 articles underwent title and abstract review. Each of the reviewers reviewed between 142 and 385 articles (mean = 298 articles). Following both rounds of review, 1017 of the remaining 4468 articles (22.8%) were included in the thematic analysis.
질적 분석에서는 81개의 코드를 9개의 예비 테마로 통합했습니다. 저자 검토자들과의 대규모 그룹 회의에서 나온 피드백을 바탕으로, 하나의 주제(형평성, 다양성, 포용성)를 두 개의 주제(1. 의사 형평성, 다양성, 포용성 및 2. 환자 접근성, 형평성, 포용성, 사회 정의)로 나눴다. 모든 워킹그룹 구성원이 구성원 점검 설문조사를 완료했습니다. 설문조사 피드백을 바탕으로 몇 가지 주제 제목의 문구를 수정했지만, 삭제되거나 통합된 주제는 없었습니다. Our qualitative analysis incorporated 81 codes into nine preliminary themes. Based upon feedback at the large group meeting with the author reviewers, one additional theme was created by splitting one of the themes (Equity, Diversity, and Inclusion) into two (1. Physician Equity, Diversity, Inclusion and 2. Patient Access, Equity, Inclusion, and Social Justice). All working group members completed the member check survey. Modifications in wording were made to several of the theme titles based upon survey feedback, but no themes were removed or amalgamated.
10명의 워킹 그룹 멤버와 9명의 임상 교육자가 설문조사를 완료하여 새로운 개념 각각에 대한 집필 그룹에 참여할 전문가를 추천했습니다. 각 개념에 대해 글쓰기 그룹을 구성하여 해당 개념이 CanMEDS에 보다 효과적으로 통합될 수 있는 방법을 설명하는 임무를 맡겼습니다. 환자와 의사의 형평성, 다양성, 포용성에 초점을 맞춘 두 개의 집필 그룹은 이 개념이 단일 원고를 작성하기에는 너무 광범위하다고 판단했습니다. 따라서 초기 분석에서처럼 환자와 의사 중심의 원고로 나누기보다는 반인종주의에 초점을 맞춘 원고와 형평성, 다양성, 포용성, 사회 정의에 초점을 맞춘 두 번째 원고로 나눌 것을 권장했습니다. 이 권고에 따라 집필 그룹은 수정되었고, 이후 집필팀의 승인을 받았습니다. 집필 그룹의 수정에 따른 주제별 분석 결과는 표 1에 제시되어 있습니다.
Ten working group members and nine clinician educators completed the survey nominating experts to participate in a writing group on each of the emerging concepts. A writing group was formed for each concept and tasked with describing how it could be more effectively integrated into CanMEDS. The two writing groups focused on patient and physician equity, diversity, and inclusion determined that this concept was too broad for a single manuscript. However, rather than splitting it into patient and physician focused manuscripts as was done in the initial analysis, they recommended dividing it into one manuscript focused on anti-racism and a second manuscript focused on equity, diversity, inclusion, and social justice. The writing groups were modified in keeping with this recommendation which was subsequently endorsed by our authorship team. The results of the thematic analysis following modification by the writing groups are presented inTable 1.
표 1에는 각 주제에서 논의된 의사의 잠재적 역량에 대한 설명과 1차 구성원 점검 시 각 주제를 새로운 개념으로 지지한 실무 그룹 구성원의 비율도 포함되어 있습니다. 17명의 실무 그룹 구성원 중 최소 14명(82.4%)이 각 주제를 새로운 개념으로 지지했습니다. 주제를 지지하지 않은 이유에 대해서는 해당 주제가 참신하지 않다고 생각하거나, CanMEDS 역량과 어떻게 관련될 수 있는지 알지 못하거나, 주제를 분할하거나 확장하는 것을 선호하는 등 다양한 제안이 있었습니다. 회색 문헌 검색에서는 추가로 떠오르는 개념이 발견되지 않았습니다. Table 1 also includes a description of the potential physician competencies discussed within each theme and the proportion of working group members who endorsed each theme as an emerging concept during the first member check. At least fourteen (82.4%) of the 17 working group members endorsed each of the themes as an emerging concept. There were a variety of suggestions provided for why a member did not endorse a theme such as not identifying the theme as novel, not seeing how it could relate to a CanMEDS competency, or preferring themes be split or expanded. The grey literature search did not identify any additional emerging concepts.
10개 작성 그룹 중 6개 그룹은 개념을 더 정확하게 설명하기 위해 개념의 제목을 변경할 것을 제안했습니다. 새로운 개념의 이름과 정의에 대한 변경과 반인종주의 개념의 추가는 집필 그룹의 만장일치 동의로 승인되었습니다. Six of the 10 writing groups proposed changes to the title of their concept to describe it more accurately. The changes to the names and definitions of the emerging concepts, as well as the addition of the anti-racism concept, were approved by the authorship group with unanimous consent.
토론 Discussion
본 연구에서는 의학 문헌에서 CanMEDS 2025에 기술된 의사 역량에 통합될 수 있는 10가지 새로운 개념을 확인했습니다. 이러한 각 개념은 범위가 상당히 광범위하며, 대부분 현재 의학교육 문헌에서 논의되고 있는 여러 트렌드 또는 문제를 포괄하고 있습니다. 조사 결과 중 몇 가지 주제는 지난 3년간 광범위한 사회적, 경제적, 정치적, 환경적 담론에서 두드러진 현재 주제를 반영하고 있어 주목할 만합니다. Our study identified ten emerging concepts in the medical literature that could be incorporated into the physician competencies described by CanMEDS 2025.29–38Each of these concepts is quite broad in scope, with most encompassing several trends or issues currently being discussed in the medical education literature. Several themes within our results are notable as they mirror current themes of prominence in the broader social, economic, political, and environmental discourse over the past three years.
접근성, 형평성, 다양성, 포용성, 사회 정의, 반인종주의29,30와 관련된 주제가 분석에서 가장 많이 나타났습니다. 이 큰 주제는 궁극적으로 반인종주의에 초점을 맞춘 두 가지 주제로 분리되었습니다.30 의학 문헌에서 이러한 주제가 두드러진 것은 대중 담론에서 제도적 차별의 부정적인 영향에 대한 인식과 유사합니다.19 이 검토의 캐나다적 맥락, 캐나다 의료 시스템에서 원주민 건강의 중심적 중요성,39 그리고 캐나다 진실과 화해 위원회 최종 보고서에 발표된 건강 관련 7가지 행동 촉구를 고려할 때 원주민 건강에 초점을 맞춘 별도의 테마가 독립적으로 나타나지 않았다는 점이 주목할 만합니다. 이는 포함된 학술지들이 국제적인 초점(캐나다 의학교육 저널만이 캐나다 의학교육에 더 중점을 두었음)과 형평성, 다양성, 포용성, 사회 정의,29 및 반인종주의라는 주제 아래 많은 관련 구성 요소를 자주 코딩했기 때문인 것으로 생각됩니다.30 특히 원주민 건강과 관련된 제안 역량은 이러한 주제를 자세히 설명하는 두 원고의 중심입니다.29,30 Themes relating to access, equity, diversity, inclusion, social justice, and anti-racism29,30were prevalent in the analysis. This large theme was ultimately separated into two themes, with one focused specifically on anti-racism.30The prominence of these themes in the medical literature parallels the acknowledgement of the negative impact of systemic discrimination in the public discourse.19Given the Canadian context of this review, the central importance of Indigenous health in the Canadian healthcare system,39and the seven calls to action related to health published in the final report of the Truth and Reconciliation Commission of Canada,40it is notable that a separate theme focused on Indigenous health did not emerge independently. We suspect this is due to both the international focus of the included journals (only theCanadian Medical Education Journalfocused more closely on Canadian medical education) as well as the frequent coding of many relevant constructs under the themes of equity, diversity, inclusion, social justice,29and anti-racism.30Notably, proposed competencies related to Indigenous health are central to both manuscripts further describing these themes.29,30
기후변화가 건강에 미치는 급격한 영향에 대한 과학적 공감대가 형성되고 있는 상황에서 '지구 보건' 주제38 의 존재는 놀라운 일이 아닙니다.22 특히 의사와 의료 수련생들은 기후변화가 인구의 건강과 복지에 미치는 영향에 관한 교육 및 옹호에서 두드러진 목소리를 내왔습니다.41-43 그러나 일부 저자는 개별 의사와 관련된 역량 틀 내에서 이러한 구조를 동원하는 것이 어려울 것이라는 우려를 표명했습니다. The presence of the ‘Planetary Health’ theme38is unsurprising given the scientific consensus building on the drastic impacts of climate change on health.22Notably, physicians and medical trainees have had a prominent voice in education and advocacy relating to the impacts of climate change on the health and wellbeing of the population.41–43However, some authors were concerned that it would be challenging to mobilize this construct within a competency framework relevant to individual physicians.
데이터 및 기술 사용과 관련된 추가 역량의 필요성에 대해서는 폭넓은 공감대가 형성되었습니다.32,35 정밀 의학을 둘러싼 논의가 증가하는 가운데, '가상 진료' 및 '데이터 정보 의학' 테마로 통합된 이 코드는 신흥 기술의 보급16,17 과 개인 및 건강 데이터를 윤리적이고 안전하게 사용해야 할 필요성에 대한 사회적 인식의 증가와 병행합니다.44 There was broad consensus regarding the need for additional competencies related to the use of dataand technology.32,35Beyond the growing dialogue surrounding precision medicine, the codes consolidated into the ‘Virtual Care’ and ‘Data-Informed Medicine’ themes parallel growing societal awareness of the pervasiveness of emerging technologies16,17and the need for personal and health data to be used ethically and securely.44
코로나19 팬데믹의 영향은 여러 테마에서 확인할 수 있었습니다. 특히 '가상 치료' 주제35는 팬데믹 기간 동안 여행 및 모임 제한으로 인해 상당한 영향을 받은 개념인 가상 교육 및 가상 의료와 밀접한 관련이 있습니다.15,45 코로나19 팬데믹의 영향을 받은 다른 개념으로는 의료 시스템에 대한 복잡하고 지속적인 영향으로 인한 '복합 적응 시스템'33,46과 의사와 기타 의료 제공자에게 미치는 부담으로 인한 '의사 휴머니즘'31,47이 있습니다. The influence of the COVID-19 pandemic was seen in numerous themes. In particular, the ‘Virtual Care’ theme35relates strongly to virtual education and virtual healthcare, concepts that were substantially impacted by travel and gathering restrictions during the pandemic.15,45Other concepts that were likely influenced by the COVID-19 pandemic included ‘Complex Adaptive Systems’33,46due to its complex ongoing impacts on the healthcare system and ‘Physician Humanism’31,47due to its strain on physicians and other healthcare providers.
'적응적 전문성'37 및 '임상적 추론'36 주제는 복잡한 임상 진료 영역에서 얼마나 빠른 변화가 일어나고 있는지를 인정합니다.48 의사가 이러한 과제를 해결하기 위해 진료 방식을 발전시킬 수 있는 역량이 있지만, 진화하는 의사의 역량을 적시에 CanMEDS에 통합하는 방법도 고려해야 합니다. 과거에는 약 10년에 한 번씩 개정을 실시하는 것이 CanMEDS에 도움이 되었지만, 이 원고의 발행과 CanMEDS 2025의 시행 사이에 새로운 역량이 등장할 것으로 예상할 수 있습니다. 정기적인 업데이트에서 지속적인 반복 프로세스로 전환하는 것을 고려해야 합니다. 이는 레지던트 수련 프로그램에서는 물류적으로 어려울 수 있지만, 미국심장협회와 같은 기관에서 지침을 지속적으로 업데이트하는 최신 프로세스에 부합하며, 더 작은 규모의 더 빈번한 업데이트가 가능할 수 있습니다.49 The ‘Adaptive Expertise’37and ‘Clinical Reasoning’36themes acknowledge how rapidly changes are occurring within the complex realm of clinical practice.48While there are competencies that enable physicians to evolve their practices to meet these challenges, it will also be important to consider how evolving physician competencies are integrated into CanMEDS in a timely manner. While performing revisions approximately once per decade has served CanMEDS well in the past, it is conceivable that new competencies will emerge between the publication of this manuscript and the implementation of CanMEDS 2025. Consideration should be given to transitioning CanMEDS from periodic updates to an ongoing iterative process. While this may be logistically challenging for residency training programs, it is in keeping with modern processes for the continuous updating of guidelines by organizations like the American Heart Association and could allow for smaller, more frequent updates.49
새롭게 등장한 각 개념이 CanMEDS 2025에 어떻게 통합될 수 있는지 설명하기 위한 추가 작업이 진행되었습니다. 집필 그룹은 각 개념을 정의하는 원고의 초안을 작성하고, CanMEDS 2015에 어떻게 표현되었는지 설명하고, CanMEDS 2025에 어떻게 통합할 수 있는지 제안했습니다.29-38 이 작업은 이 논문과 함께 캐나다 의학교육 저널 특별호에 게재되었으며, CanMEDS 2025 의사 역량 프레임워크 업데이트를 담당하는 전문가 실무 그룹에 정보를 제공할 것입니다. 이러한 새로운 개념이 공개됨으로써 캐나다 및 국제 의료계가 이 작업에 대해 논의하고 의견을 제시할 수 있는 기회가 될 것입니다. Further work has been conducted to describe how each of the emerging concepts can be incorporated into CanMEDS 2025. Writing groups have drafted manuscripts that define each concept, outlined how it was represented in CanMEDS 2015, and proposed how it could be incorporated into CanMEDS 2025.29–38This work has been published along with this paper in this special issue of theCanadian Medical Education Journaland will inform the CanMEDS 2025 Expert Working Groups responsible for updating the CanMEDS physician competency framework. The open publication of these emerging concepts should provide Canadian and international medical communities with an opportunity to discuss and comment on this work.
강점과 한계 Strengths and limitations
이 검토의 강점은 상세하고 투명한 방법과 이해관계자 단체의 폭넓은 참여에 있습니다. CanMEDS2015 개정 이전에 관련 문헌 검토가 수행되었지만,23 그 방법론이 자세히 설명되거나 동료 검토를 거치지 않았습니다. 저희는 상세한 방법론을 발표하고 동료 검토 과정을 거침으로써 이 작업을 개선했습니다. 또한 캐나다 왕립 의사 및 외과의사 대학, 퀘벡 의과대학, 캐나다 가정의학과 대학, 캐나다 의과대학 학부 협회의 대표를 포함한 광범위한 이해관계자 그룹에 의해 논문 검토가 수행되었습니다. 저자 팀의 다양성으로 인해 중요한 개념이 누락될 가능성이 줄어듭니다. The strength of this review rests in the detailed, transparent methods and the broad engagement of stakeholder organizations. While a related literature review was conducted prior to the CanMEDS 2015 revision,23its methodology was not described in detail or peer reviewed. We have improved on this work by publishing a detailed methodology and by putting our work through the peer review process. Additionally, the article review was conducted by a broader group oof stakeholders (including representatives from the Royal College of Physicians and Surgeons of Canada, Collège des Médecins du Québec, College of Family Physicians of Canada, and Association of Faculties of Medicine of Canada). The diversity of our authorship team decreases the chance that important concepts were missed.
이 리뷰에는 몇 가지 한계가 있었습니다.
첫째, 포함 기간을 3년으로, 출처를 5개 저널로, 특정 논문 유형을 제한하여 검토 범위를 제한했습니다. 이러한 제한은 새로운 개념을 파악하는 동시에 타당성을 유지하기 위해 내린 의도적이고 실용적인 결정이라고 생각합니다. 일부 주제를 놓쳤을 가능성에도 불구하고 회색 문헌 스캔을 통한 삼각 측량으로 추가 개념을 식별하지 못했다는 점은 안심할 수 있습니다.
둘째, 수많은 리뷰어가 문헌 검색에 참여했기 때문에 새로운 개념 기준과 라벨링의 일관성을 보장하기 어려웠습니다. 또한, 대부분의 초록 검토는 추가 검토를 위한 플래그가 지정되지 않는 한 독립적으로 수행되었습니다. 멤버 점검을 통해 이러한 문제가 결과에 미치는 영향을 완화할 수 있을 것으로 기대합니다.
마지막으로, 확인된 수많은 개념을 테마로 통합하는 것이 어려웠습니다. 우리의 분석은 일부 테마 내에서 광범위한 수의 코드를 집계했다는 비판을 받을 수 있습니다. 일부 워킹그룹 참가자들은 일부 테마가 새로운 개념이 아니거나 지나치게 광범위하다고 느꼈습니다. 이러한 도전은 연구 단계에 걸쳐 형평성, 다양성, 포용성과 관련된 주제가 진화하는 과정에서 잘 드러났습니다. 그럼에도 불구하고 대다수(실무 그룹 구성원의 82.4% 이상)는 각 주제가 더 깊이 탐구할 가치가 있는 중요한 새로운 개념이라고 생각했습니다.
This review had several limitations. First, we restricted the scope of our review by limiting the inclusion period to three years, the source to five journals, and specific article types. We see these limitations as intentional, pragmatic decisions that we made to maintain feasibility while identifying emerging concepts. Despite the potential to have missed some themes, it is reassuring that triangulation with the grey literature scan did not identify any additional concepts. Second, with numerous reviewers participating in the literature scan, it was difficult to ensure consistency in emerging concept criteria and labelling. Further, most abstract reviews were done independently unless flagged for additional review. We anticipate that the member checks mitigated the impact of this challenge on the results. Finally, consolidating the numerous identified concepts into themes was difficult. Our analysis could be criticized for aggregating a broad number of codes within some of the themes. Some of the working group participants felt that some themes were either not emerging concepts or were overly broad. This challenge is well-represented by the evolution of the themes related to equity, diversity, and inclusion throughout the phases of the study. This said, a large majority (≥82.4% of working group members) felt that each theme represented an important emerging concept that deserved further exploration.
결론 Conclusion
이 검토 및 분석을 통해 CanMEDS 2025의사 역량 프레임워크에 통합하기 위해 고려해야 할 10가지 새로운 개념이 확인되었습니다. 이 작업의 결과는 이번 특별호에 자세히 설명되어 있으며, 여기에는 각 개념에 대한 확장된 기사와 함께 CanMEDS 2025.29-38에 통합할 수 있는 방법에 대한 제안이 포함되어 있습니다. 이 작업의 공개를 통해 CanMEDS의 개정을 알리는 것 외에도, 개정 과정에 대한 투명성을 높이고 의사 역량에 관한 학술 문헌에서 조기 대화를 촉진할 수 있기를 바랍니다. This review and analysis identified ten emerging concepts that should be considered for incorporation into the 2025 CanMEDS physician competency framework. The results of this work are elaborated upon in this special issue, which contains an expanded article on each concept along with suggestions for how it could be incorporated into CanMEDS 2025.29–38.We hope that in addition to informing the revision of CanMEDS, the open publication of this work will create greater transparency around the revision process while facilitating an early dialogue in the academic literature on physician competence.
Can Med Educ J. 2023 Mar 21;14(1):4-12.doi: 10.36834/cmej.75591.eCollection 2023 Mar.
Emerging concepts in the CanMEDS physician competency framework
Background:The CanMEDS physician competency framework will be updated in 2025. The revision occurs during a time of disruption and transformation to society, healthcare, and medical education caused by the COVID-19 pandemic and growing acknowledgement of the impacts of colonialism, systemic discrimination, climate change, and emerging technologies on healthcare and training. To inform this revision, we sought to identify emerging concepts in the literature related to physician competencies.
Methods:Emerging concepts were defined as ideas discussed in the literature related to the roles and competencies of physicians that are absent or underrepresented in the 2015 CanMEDS framework. We conducted a literature scan, title and abstract review, and thematic analysis to identify emerging concepts. Metadata for all articles published in five medical education journals between October 1, 2018 and October 1, 2021 were extracted. Fifteen authors performed a title and abstract review to identify and label underrepresented concepts. Two authors thematically analyzed the results to identify emerging concepts. A member check was conducted.
Results:1017 of 4973 (20.5%) of the included articles discussed an emerging concept. The thematic analysis identified ten themes: Equity, Diversity, Inclusion, and Social Justice; Anti-racism; Physician Humanism; Data-Informed Medicine; Complex Adaptive Systems; Clinical Learning Environment; Virtual Care; Clinical Reasoning; Adaptive Expertise; and Planetary Health. All themes were endorsed by the authorship team as emerging concepts.
Conclusion:This literature scan identified ten emerging concepts to inform the 2025 revision of the CanMEDS physician competency framework. Open publication of this work will promote greater transparency in the revision process and support an ongoing dialogue on physician competence. Writing groups have been recruited to elaborate on each of the emerging concepts and how they could be further incorporated into CanMEDS 2025.
졸업후의학교육에서 공유의사결정을 위한 EPA 식별하기: 국가 델파이 연구(Acad Med, 2021) Identifying Entrustable Professional Activities for Shared Decision Making in Postgraduate Medical Education: A National Delphi Study Anouk Baghus, MD, MSc, Esther Giroldi, PhD, Jean Muris, MD, PhD, Anne Stiggelbout, PhD, Marjolein van de Pol, MD, PhD, Angelique Timmerman, PhD, and Trudy van der Weijden, MD, PhD
공유 의사 결정(SDM)은 현재 환자를 의료 의사 결정에 참여시키기 위해 선호되는 접근 방식이며 좋은 환자 치료의 정점으로 간주됩니다.1-6 이 대화형 프로세스에서 임상의와 환자는 함께 환자의 정보에 입각한 선호도와 임상 증거를 바탕으로 신중한 결정을 내리기 위해 협력합니다.7 Shared decision making (SDM) is the current preferred approach to involve patients in medical decision making and is considered the pinnacle of good patient care.1–6In this interactive process, clinicians and patients work together to make deliberate decisions based on the patient’s informed preferences and clinical evidence.7
임상의와 환자 모두 SDM의 중요성을 인식하고 있지만,8,9 SDM은 임상에서 일상적으로 적용되지 않습니다.10,11 이러한 성과 격차로 인해 전 세계적으로 SDM 교육이 더욱 강조되고12,13 중요한 의료 역량 프레임워크에 SDM이 포함되었습니다.14,15 일상적인 임상에서 SDM 적용의 낮은 일관성은 SDM 기술 학습과 실행 사이의 전이가 복잡하다는 것을 반영하는 것일 수 있습니다.12,13,16 Although the importance of SDM is recognized by both clinicians and patients,8,9SDM is not routinely applied in clinical practice.10,11This performance gap has resulted in more emphasis on training in SDM worldwide12,13and including SDM in important medical competency frameworks.14,15The low consistency in application of SDM in routine clinical practice may reflect the complexity of transfer between learning and practicing SDM skills.12,13,16
우리는 이러한 전이transfer를 지원함으로써 전문적 실무에서 SDM의 지속 가능한 구현을 강화할 수 있을 것으로 기대합니다. 이러한 전이는 실제 임상 환경에서 복잡한 기술을 학습하고, 강력한 경험에 의해 촉발되고, 임상 성과에 대한 성찰에 의해 주도될 때 가장 효과적이라고 가정합니다.17-19 우리는 자기 주도적 직장 학습에 SDM을 통합하는 것이 효과적일 것으로 기대하지만, 임상 실습에서 SDM에 필요한 역량에 대한 합의가 부족하면 원하는 교육 결과에 부정적인 영향을 미칠 수 있습니다.20,21 We expect that supporting this transfer will enhance sustainable implementation of SDM in professional practice. This transfer is assumed to be most effective when complex skills are learned within the authentic clinical environment, triggered by powerful experiences and driven by reflection on clinical performance.17–19Although we expect that integrating SDM in self-directed workplace learning will be effective, the lack of consensus on the needed competencies for SDM in clinical practice may negatively affect desired training outcomes.20,21
졸업후 의학 교육은 복잡한 역량의 자기주도적 직장 학습을 위한 이상적인 학습 환경으로 여겨집니다.22 복잡한 역량을 임상 실무로 이전하는 것은 많은 졸업후 의학 교육 프로그램에서 위탁 가능한 전문 활동(EPA)을 공식화함으로써 최적화됩니다.23-26 역량은 태도, 지식, 행동을 결합하는 일반적인generic 성격이지만, EPA는 이러한 역량을 임상 실무로 전환하는 전문직의 언어로 공식화됩니다. EPA는 집중적인 관찰과 피드백을 지원하는 데 사용되므로 학습자의 레퍼토리에 복잡한 SDM 행동을 통합하는 데 사용할 수 있습니다.18,19 이 연구의 목적은 졸업후 의학 교육 중에 가르쳐야 하는 SDM 및 관련 행동 지표에 대한 EPA에 대한 합의를 도출하는 것이었습니다. Postgraduate medical education is believed to be the ideal learning environment for self-directed workplace learning of complex competencies.22The transfer of complex competencies to clinical practice is optimized in many postgraduate medical training programs by formulating entrustable professional activities (EPAs).23–26While competencies are generic in nature—combining attitude, knowledge, and behavior—EPAs are formulated in the language of the profession that translates these competencies into clinical practice. EPAs are used to support focused observation and feedback and can therefore be used to foster the integration of complex SDM behavior into the learner’s repertoire.18,19The aim of this study was to reach consensus on EPAs for SDM and associated behavioral indicators that need to be taught during postgraduate medical education.
방법 Method
배경 Context
우리는 모든 의학 전문과에서 사용할 수 있는 SDM을 위한 EPA를 개발하는 것을 목표로 했습니다. 네덜란드에서는 네덜란드 왕립 의학협회에서 정한 국가적 요구사항에 따라 의학 전문 부서가 네덜란드 졸업후 의학 교육의 커리큘럼을 조정합니다. 교육 기간은 전문 분야에 따라 2년에서 7년까지 다양하며, 프로그램은 직장 기반 교육과 정규 교육이 균형을 이루고 있습니다. 2015년부터 네덜란드의 졸업후 의학 전문 교육 프로그램에서는 CanMEDS 역량 프레임워크에 따라 레지던트를 교육해야 합니다. 대부분의 전문과목에서 이러한 역량은 레지던트의 개발과 필요한 감독 수준을 결정하는 데 사용되는 특정 EPA로 변환됩니다.24,27 일부 졸업후 커리큘럼에서는 임상에서 필요한 구체적인 업무와 행동이 명시되어 있지 않지만 SDM이 중요한 주제 또는 커뮤니케이션 역량 중 하나로 언급됩니다.
We aimed to develop EPAs for SDM that can be used in all medical specialties. In the Netherlands, medical specialty departments coordinate the curricula of Dutch postgraduate medical education, based on national requirements set by the Royal Dutch Medical Association. The duration of the training programs varies between 2 and 7 years, depending on the specialty, and the programs balance workplace-based training and formal education. Since 2015, postgraduate medical specialty training programs in the Netherlands have been required to train residents according to the CanMEDS competency framework. For most medical specialties, these competencies are translated into specific EPAs used to determine the development of the resident and the level of supervision needed.24,27In some postgraduate curricula, SDM is mentioned as an important theme or as one of the communication competencies although the specific tasks and behaviors that are needed in clinical practice are not spelled out.
디자인 Design
우리는 2017년 4월부터 8월까지 네덜란드 전문가들을 대상으로 수정된 온라인 델파이 연구를 실시하여 졸업후 의학교육을 위한 SDM EPA 및 기본 행동 지표에 대한 합의를 도출했습니다.
델파이 기법은 의학교육 연구에 널리 사용되는 합의 방법입니다.28-31 이 기법은 특정 주제에 대한 합의에 도달하기 위해 설문지 또는 "라운드"를 여러 번 반복하여 사용하며, 각 연속 라운드마다 연구자는 이전 라운드의 결과를 피드백합니다. 합의에 도달하려면 최소 2번의 라운드가 연속적으로 진행되어야 합니다.32-34
We conducted a modified online Delphi study among Dutch experts between April and August 2017 to reach consensus on SDM EPAs and underlying behavioral indicators for postgraduate medical education.
The Delphi technique is a widely used consensus method for medical education research.28–31This technique uses multiple iterations of questionnaires or “rounds” to reach agreement on a specific topic; for each successive round, the researcher feeds back the results of the previous round. At least 2 successive rounds must be carried out to reach consensus.32–34
우리는 기존 문헌과 인터뷰 연구를 통해 첫 번째 델파이 라운드에서 사용된 EPA 및 행동 지표 목록을 개발했습니다.
첫째, A.B.는 SDM 프레임워크, 역량 및 행동을 설명하는 주요 출판물을 검토하고13,21,35-37 스노우볼 방법과 웹 오브 사이언스에서 관련 인용을 통해 보완했습니다.
둘째, 네덜란드의 SDM, 의사-환자 커뮤니케이션, 의학교육 전문가를 대상으로 인터뷰 연구(다른 곳에 보고될 예정)를 실시했습니다. A.B.는 17회의 반구조화된 대면 인터뷰를 실시했습니다. 모든 인터뷰는 데이터 수집 및 분석의 반복적인 과정을 통해 오디오 녹음, 전사, 주제별 분석이 이루어졌습니다.
문헌 검토와 인터뷰 결과를 종합하여 ten Cate의 가이드라인에 따라 EPA와 행동 지표를 공식화했습니다.24
우리는 이 목록을 SDM 전문가로 구성된 국가 자문위원회와 논의하고 다양한 배경(의사, SDM 연구자, 교육자)을 대표하는 연구팀이 설문지의 내용과 형식에 대해 합의에 도달할 때까지 이 목록을 편집했습니다.
We developed the list of EPAs and behavioral indicators used in the first Delphi round by using existing literature and an interview study.
First, A.B. reviewed key publications describing SDM frameworks, competencies, and behaviors,13,21,35–37complemented by the snowball method and relevant citations from the Web of Science.
Second, we conducted an interview study (which will be reported elsewhere) with Dutch experts in SDM, doctor–patient communication, and medical education. A.B. conducted 17 semistructured face-to-face interviews. All interviews were audiotaped, transcribed, and thematically analyzed during an iterative process of data collection and analysis.
Combining the findings of the literature review and interviews, we then formulated the EPAs and behavioral indicators according to ten Cate’s guidelines.24
We discussed this list with our national advisory board, consisting of SDM experts, and edited this list until our research team, representing a variety of backgrounds (medical doctors, researchers in SDM, and educationalists), reached consensus regarding the content and formatting of our questionnaire.
참여자 Participants
우리는 의도적 표본 추출을 통해 잠재적 전문가 패널의 명단을 작성했으며,38 SDM, 의사-환자 커뮤니케이션, 의학 교육에 대한 전문성과 특별한 관심을 기준으로 삼았습니다. 가정의학과 직업 교육에는 의료 커뮤니케이션 교육이 포함된 오랜 전통이 있기 때문에 이 분야에서 일하는 전문가를 우선적으로 고려했습니다. 전체 목록에는 다음 등이 포함되었습니다.
(1) 일상적인 환자 진료에 종사하는 임상의,
(2) SDM에 특별한 관심이 있는 환자 대표,
(3) 의료 커뮤니케이션, SDM 또는 근거 기반 의학(EBM) 분야의 트레이너, 코디네이터, 교육 개발자,
(4) SDM, 의료 커뮤니케이션, 환자 참여 분야의 연구자
연구 목적, 절차, 시간 투자에 대한 정보를 담은 이메일을 통해 57명의 잠재적 전문가 패널을 초대했습니다. 그런 다음 사전 동의를 얻은 후 참여에 동의한 사람들을 첫 번째 델파이 라운드에 초대했습니다(네덜란드 의학교육협회 윤리심의위원회, 파일 번호 894). 연구 기간 동안 이전 라운드를 완료한 모든 전문가 패널은 다음 델파이 라운드에 초대되었습니다. 연구 조교가 전문가들의 익명성을 유지하기 위해 분석 전에 모든 설문조사 데이터를 가명 처리했습니다. We compiled a list of potential expert panel members using purposive sampling,38based on expertise and special interest in SDM, doctor–patient communication, and medical education. Because family medicine vocational training has a long tradition of including training in medical communication, experts working in this field were preferred. The full list included
(1) clinicians active in routine patient care;
(2) patient representatives with a special interest in SDM;
(3) trainers, coordinators, and educational developers in medical communication, SDM, or evidence-based medicine (EBM); and
(4) researchers in SDM, medical communication, and/or patient participation.
We invited 57 potential expert panel members via an email with information about the purpose of the study, procedure, and time investment. We then invited those who agreed to participate to the first Delphi round after obtaining informed consent (Ethical Review Board of The Netherlands Association for Medical Education, file number 894). During the study, all expert panel members who finished a previous round were invited to participate in the next Delphi round. A research assistant pseudonymized all survey data before analysis to maintain the experts’ anonymity.
데이터 수집 Data collection
웹 기반 서비스 도구인 Qualtrics(미국 유타주 프로보 소재)를 사용하여 3라운드의 수정된 온라인 델파이 연구를 수행했습니다. 그림 1은 각 라운드의 중점 사항과 그 결과를 요약한 것입니다. 델파이 1, 2, 3라운드는 각각 2주, 3주, 6주 동안 진행되었습니다(1라운드, 4월 19일~5월 2일, 2라운드, 5월 29일~6월 19일, 3라운드, 7월 13일~8월 25일). 연구에 참여하지 않은 전문가 7명을 대상으로 1차 설문지를 시범 실시한 후 설문지의 텍스트와 레이아웃을 수정했습니다.
We performed a 3-round modified online Delphi study using the web-based service tool Qualtrics (Qualtrics, Provo, Utah).Figure 1summarizes the focus of each round and their outcomes. The first, second, and third Delphi rounds lasted 2, 3, and 6 weeks, respectively (Round 1, April 19 to May 2; Round 2, May 29 to June 19; Round 3, July 13 to August 25). After piloting the first-round questionnaire with 7 experts who did not participate in the study, we modified the text and layout of the questionnaire.
우리는 졸업후 교육을 마친 후 전공의들이 수행할 수 있는 EPA에 대한 합의를 도출하는 것을 목표로 했습니다. 각 EPA와 행동 지표에 대해 다음 두 가지 문항을 제시했습니다:
"나는 이 EPA/행동 지표를 교육 커리큘럼에 포함시키고 싶다",
"이 EPA/행동 지표는 임상에서 적용할 수 있다".
전문가들은 7점 리커트 척도(1=강력히 동의하지 않음~7=강력히 동의함)로 EPA와 행동 지표를 평가하도록 요청받았습니다. 첫 번째 탐색 라운드에서 응답자들은 이 두 가지 문항에 대해 EPA 및 행동 지표 목록을 평가했습니다. 각 라운드에서 의견과 피드백(예: 점수 설명, 텍스트 변경에 대한 제안, 추가 EPA 및 행동 지표)을 위한 열린 텍스트 상자를 제공했습니다. 첫 번째 라운드에서는 참가자의 인구통계학적 특성을 평가했습니다. We aimed to achieve consensus on EPAs that residents are able to carry out after completing their postgraduate education. We presented these 2 statements for each EPA and behavioral indicator:
“I do like to include this EPA/behavioral indicator in the educational curriculum” and
“this EPA/behavioral indicator is applicable in clinical practice.”
Experts were asked to rate the EPAs and behavioral indicators on a 7-point Likert scale (1 = strongly disagree to 7 = strongly agree). In the first exploratory round, respondents rated a list of EPAs and behavioral indicators on these 2 statements. In each round, we provided open text boxes for comments and feedback (e.g., clarification of scores and suggestions for textual changes and additional EPAs and behavioral indicators). We assessed the demographic characteristics of the participants during the first round.
각 설문 항목에 대한 1차 결과의 개인 절대 점수와 그룹 평균 점수에 대한 개요를 제공하고, 1차 분석 후 EPA 및 행동 지표에 대한 수정 사항을 반영한 새로운 버전의 설문지를 제공하는 것으로 2차 조사를 시작했습니다. 다시 한 번 전문가들에게 1차에서 사용된 2개의 문항에 대해 각 EPA와 행동 지표를 평가해 달라고 요청했습니다. 이번 라운드에서는 다음을 목표로 삼았습니다.
(1) 최종 목록에 포함해야 할 EPA 및 행동 지표에 대한 합의를 도출하고,
(2) 여전히 합의가 이루어지지 않은 EPA 및 행동 지표를 다시 수정하는 것
We started the second round by providing an overview of the absolute personal scores and mean group scores resulting from the first round, for each questionnaire item, and a new version of the questionnaire, reflecting revisions we had made to the EPAs and behavioral indicators after our analysis of the first round. Again, we asked experts to rate each EPA and behavioral indicator on the 2 statements used in the first round. In this round, we aimed
(1) to reach consensus on which EPAs and behavioral indicators needed to be included in a near-final list and
(2) to revise again those EPAs and behavioral indicators for which there was still not consensus.
3차 회의는 두 부분으로 진행되었습니다.
먼저, 2차 라운드에서 전문가들이 합의에 이르지 못한 행동 지표와 2차 라운드 분석 후 재구성한 행동 지표를 제시했습니다. 전문가들에게 재구성한 행동 지표에 대한 평가를 요청하고, 이번 라운드에서 합의에 도달하면 새로운 버전이 최종 EPA 및 행동 지표 목록에 추가될 것임을 알렸습니다.
둘째, 두 번째 라운드에서 합의에 도달한 EPA 및 행동 지표의 목록을 제시했습니다. 전문가들에게 다음과 같은 질문을 던졌습니다: "졸업후 의학교육을 위한 거의 최종 단계에 이른 이 SDM EPA 및 행동 지표 목록에 동의하십니까?" 응답 옵션은 "예"와 "아니오"였습니다.
The third round had 2 parts.
First, we presented the behavioral indicators on which our experts had not reached consensus in the second round and which we had reformulated after the analysis of the second round. We asked the experts to rerate the reformulated behavioral indicators, informing them that the new versions would be added to the final list of EPAs and behavioral indicators if they reached consensus during this round.
Second, we presented a list of EPAs and behavioral indicators on which they had reached consensus in the second round. We asked the experts this question: “Do you agree with this near-final list of SDM EPAs and behavioral indicators for postgraduate medical education?” Response options were “yes” and “no.”
데이터 분석 Data analyses
설문지의 정량적 구성요소는 Windows용 SPSS 24(IBM Corp., Armonk, New York)의 기술통계 프로그램을 사용하여 분석했습니다. 델파이 연구에서 합의에 대한 표준 정의가 없기 때문에2 연구팀은 첫 번째 두 라운드에서 개별 EPA 및 행동 지표에 대한 합의를 중앙값이 6점 이상이고 전문가 패널의 75% 이상이 "나는 이 EPA/행동 지표를 교육 과정에 포함시키고 싶다"는 문항에 6점 이상을 부여하는 것으로 정의하기로 합의했습니다. 우리는 교육 커리큘럼에 포함되어야 하는 SDM EPA 및 행동 지표에 대한 전체 개요를 개발하는 것을 목표로 했기 때문에 이 문항에 중점을 두었습니다. 우리는 3라운드에서 거의 최종 단계에 이른 EPA 및 행동 지표 목록에 대한 합의를 전문가 패널의 80% 이상 동의로 정의했습니다. We analyzed the quantitative components of the questionnaires using descriptive statistics in SPSS 24 for Windows (IBM Corp., Armonk, New York). Since there are no standard definitions for consensus in a Delphi study,2the research team agreed to define consensus on individual EPAs and behavioral indicators in the first 2 rounds as a median score of ≥ 6 and ≥ 75% of the expert panel assigning a score of ≥ 6 to the statement, “I do like to include this EPA/behavioral indicator in the educational curriculum.” We focused on this statement since we aimed to develop a complete overview of SDM EPAs and behavioral indicators that need to be included in the education curriculum. We defined consensus on the near-final list of EPAs and behavioral indicators as ≥ 80% agreement of the expert panel in Round 3.28
A.B.는 열린 텍스트 상자에 제공된 모든 정성적 피드백을 그룹화하여 반복되는 주제를 식별했으며, 연구팀은 각 라운드가 끝난 후 EPA와 행동 지표를 재구성해야 하는지, 그렇다면 어떻게 재구성해야 하는지 논의하는 데 사용했습니다. 전문 번역가가 최종 EPA와 행동 지표를 영어로 번역한 다음, 영어와 SDM 및 의학교육 관련 용어에 능통한 네덜란드 원어민이 이를 다시 네덜란드어로 번역하여 번역의 정확성을 검증했습니다. 연구팀은 최종 영어 번역본을 승인했습니다. A.B. grouped all the qualitative feedback provided in the open text boxes to identify recurring themes, which the research team used after each round in discussing whether the EPAs and behavioral indicators should be reformulated and if so, how. A professional translator translated the final EPAs and behavioral indicators into English, and then a native Dutch speaker proficient in English and terms specific to SDM and medical education translated them back into Dutch to verify the accuracy of the translations. The research team approved the final English translation.
결과 Results
델파이 절차 Delphi procedure
초청된 57명의 잠재적 전문가 패널 중 35명이 참여에 동의했습니다(응답률 61%). 32명의 전문가 패널이 1차 설문을 완료했습니다(응답률 91%). 2명의 전문가가 시간 부족으로 설문지를 작성하지 않았고, 1명의 전문가가 의학교육에 대한 지식 부족으로 불참을 결정했습니다. 1차 설문을 완료한 전문가 32명 전원이 2차 및 3차 설문에도 참여했습니다. 전문가들의 연령은 31세에서 61세(평균 47세)였으며, 여성이 21명(66%)이었습니다. 전문가 패널에는 관련성이 있다고 판단되는 모든 직업적 배경이 포함되었습니다(참가자 특성은 표 1 참조). Of the 57 invited potential expert panel members, 35 consented to participate (a response rate of 61%). The first round was completed by 32 expert panel members (a response rate of 91%). Two experts did not complete the questionnaire due to a lack of time, and 1 expert decided not to participate due to a lack of knowledge of medical education. All 32 experts who completed the first round also completed the second and third rounds. The experts’ ages ranged from 31 to 61 years (a mean of 47 years), and 21 were women (66%). All professional backgrounds that we considered relevant were represented in our expert panel (seeTable 1for participant characteristics).
델파이 결과 Delphi results
1라운드: 1라운드에서는 전문가 패널에게 6개의 EPA와 26개의 행동 지표를 제시했습니다(라운드 요약은 그림 1과 디지털 부록 1(https://links.lww.com/ACADMED/A997)을 참조하세요). 전문가들의 피드백을 바탕으로 5개의 EPA를 수정했습니다.
2개의 EPA("레지던트는 환자의 개인적 상황에 맞게 의사소통을 조정한다" 및 "레지던트는 환자에게 공유 의사 결정의 바람직성에 대해 알린다")와 관련 행동 지표가 중복되어, 이 두 개의 EPA를 "레지던트는 환자와 공유 의사 결정의 바람직성에 대해 논의한다"로 통합하고 관련 행동 지표를 이 새로운 EPA에 따라 재배치했습니다.
전문가들은 다른 두 가지 EPA의 중복에 대해서도 언급했습니다: "레지던트는 환자의 선호도를 탐색한다" 및 "레지던트는 환자가 옵션을 숙고하는 데 도움을 준다"와 관련된 행동 지표가 중복된다는 점을 언급했습니다. 따라서 새롭게 구성된 이 EPA에 따라 모든 행동 지표를 재정렬했습니다: "레지던트는 환자의 선호도와 숙고를 탐색한다."
전문가들은 "레지던트가 환자에게 관리 옵션에 대해 알려준다"는 EPA가 너무 지시적이라고 평가했기 때문에, "레지던트가 환자와 관리 옵션에 대해 논의한다"로 다시 공식화했습니다.
"전공의는 환자와 함께 충분한 논의를 거쳐 결정을 내린다"는 EPA는 전문가들이 긍정적으로 평가하고 수정 제안을 하지 않아 변경하지 않았습니다.
Round 1. In the first round, we presented 6 EPAs and 26 behavioral indicators to the expert panel (for a summary of the rounds, seeFigure 1and Supplemental Digital Appendix 1 athttps://links.lww.com/ACADMED/A997). We revised 5 EPAs using the experts’ feedback.
Due to overlap between 2 EPAs (“The resident tailors the communication to the patient’s personal context” and “the resident informs the patient about the desirability of shared decision making”) and their associated behavioral indicators, we combined those 2 EPAs into “the resident discusses the desirability of shared decision making with the patient” and rearranged their associated behavioral indicators under this new EPA.
Experts also mentioned overlap between 2 other EPAs: “The resident explores the patient’s preferences” and “the resident assists the patient in deliberating the options” and their associated behavioral indicators. Therefore, we rearranged all behavioral indicators under this newly formulated EPA: “The resident explores the patient’s preferences and deliberations.”
Because the experts evaluated the EPA “the resident informs the patient about the options for management” as too directive, we reformulated this EPA as “the resident discusses the options for management with the patient.”
We did not change the EPA “the resident takes a well-argued decision together with the patient” because the experts evaluated it positively and made no suggestions for revision.
"레지던트는 환자의 선호도가 환자의 관점, 개인적 목표 및 가치와 어떻게 관련되는지 명확히 설명한다"와 "레지던트는 환자가 선택지를 고려할 때 관점, 개인적 목표 및 가치를 고려하여 상담한다"라는 두 가지 행동 지표를 새로운 행동 지표로 통합했습니다: "레지던트는 환자의 선호도가 환자의 관점 및 개인적 목표와 가치에 충분히 부합하는지 논의한다."
또한 15개의 개정된 행동 지표 중 13개의 문구를 약간 변경했습니다. 나머지 11개 행동 지표는 긍정적으로 평가되었거나 전문가들이 수정에 대한 제안을 하지 않았기 때문에 변경하지 않고 그대로 두었습니다.
Of the 26 behavioral indicators presented, we revised 15 before Round 2, using the experts’ qualitative feedback (see Supplemental Digital Appendix 1 athttps://links.lww.com/ACADMED/A997).
We combined the 2 behavioral indicators “the resident clarifies how the patient’s preferences relate to their perspective and personal goals and values” and “the resident counsels the patient in deliberating the options, taking perspectives and personal goals and values into account” into a new behavioral indicator: “The resident discusses whether the patient’s preferences fit in sufficiently with their perspective and personal goals and values.”
Furthermore, we made minor textual changes to 13 of the 15 revised behavioral indicators. We left the remaining 11 behavioral indicators unchanged because they were evaluated positively and/or the experts offered no suggestions for revision.
2라운드. 2라운드에서는 1라운드의 결과물인 4개의 EPA와 25개의 행동지표를 제시했습니다(그림 1 및 디지털 부록 1 참조: https://links.lww.com/ACADMED/A997). 2라운드에서 합의가 이루어졌고 전문가들이 4가지 EPA에 대해 관련 정성적 피드백을 제공하지 않았기 때문에, 변경되지 않은 EPA를 최종 목록에 포함시켰습니다. 17개의 행동 지표에 대한 합의가 이루어졌습니다. 전문가들이 변경에 대한 관련 제안을 하지 않았기 때문에 이러한 지표는 변경하지 않고 최종 목록에 포함시켰습니다. 합의가 이루어지지 않은 8개 행동 지표 중 전문가들의 정성적 피드백을 바탕으로 2개 지표를 재구성했습니다.
"전공의가 중립적인 태도로 자신의 선호도를 심의에 반영한다"는 행동 지표는 "입주자가 표시된 경우 자신의 선호도를 반영한다"로 재구성했습니다.
행동 지표 "레지던트는 (환자의) 선호도에 대한 다른 관련 의료 전문가, 친척, 친구의 정보가 의사 결정 과정에 도움이 되는 경우 심의에 포함한다"를 "레지던트는 선호도 심의에 관련성이 있는 경우 관련 제3자(의료 전문가, 친척, 친구 포함)가 제공한 정보를 포함한다"로 재구성했습니다.
나머지 6개 행동 지표는 전문가들이 합의에 이르지 못했고 관련 수정 제안을 하지 않았기 때문에 삭제했습니다.
Round 2. We presented the 4 EPAs and 25 behavioral indicators resulting from Round 1 in the second round (seeFigure 1and Supplemental Digital Appendix 1 athttps://links.lww.com/ACADMED/A997). Because consensus was reached and the experts provided no relevant qualitative feedback on the 4 EPAs during Round 2, we included the unchanged EPAs in the near-final list. Consensus was reached on 17 behavioral indicators. Because the experts did not provide any relevant suggestions for change, we included these indicators unchanged in the near-final list. Of the 8 behavioral indicators on which no consensus was reached, we reformulated 2 using the experts’ qualitative feedback.
The behavioral indicator “the resident introduces own preferences into the deliberation in a neutral manner” was reformulated as “the resident introduces own preferences where indicated.”
The behavioral indicator “the resident involves information from other concerned health care professionals, relatives, and friends about the (preferences of the) patient in the deliberations, if contributing to the decision-making process” was reformulated as “the resident includes the information provided by involved third parties (including health care professionals, relatives, and friends) if this is relevant for the deliberation of preferences.”
We removed the remaining 6 behavioral indicators because the experts did not reach consensus and did not provide any relevant suggestions for revision.
3라운드. 3라운드에서는 2라운드의 결과로 재구성한 2개의 행동 지표와 2라운드에서 전문가들이 합의에 도달한 4개의 EPA와 17개의 행동 지표의 거의 최종적인 목록을 제시했습니다. 그림 1 및 보충 디지털 부록 1 참조(https://links.lww.com/ACADMED/A997)). Round 3. In the third round, we presented the 2 behavioral indicators we had reformulated as a result of Round 2 and the near-final list of 4 EPAs and 17 behavioral indicators on which the experts had reached consensus in Round 2. SeeFigure 1and Supplemental Digital Appendix 1 athttps://links.lww.com/ACADMED/A997).
전문가들은 재구성된 2개의 행동 지표를 평가했습니다.
"레지던트는 지시된 경우 자신의 선호도를 소개한다"는 행동 지표에 대해서는 합의에 이르지 못했는데, 이는 "이 행동 지표를 교육 과정에 포함시키고 싶다"는 문항에 대해 56%의 전문가만이 6점 이상을 부여했기 때문입니다. 선호도를 중립적으로 진술하기 어렵기 때문에 레지던트의 선호도가 의사 결정 과정에서 환자에게 지나치게 영향을 미칠 수 있다는 의견이 주를 이뤘습니다.
"레지던트는 선호도 심의와 관련이 있는 경우 관련 제3자(의료 전문가, 친척, 친구 등)가 제공한 정보를 포함한다"는 행동 지표를 최종 목록에 추가했는데, 중간값이 6점으로 합의가 이루어졌고 전문가의 81%가 6점 이상이었기 때문입니다(표 2 참조).
The experts rated the 2 reformulated behavioral indicators.
No consensus was reached on the behavioral indicator “the resident introduces own preferences where indicated” because only 56% of the experts scored ≥ 6 on the statement “I do like to include this behavioral indicator in the educational curriculum.” The main argument given was that the resident’s preference might influence the patient too much in the decision-making process since it is hard to state a preference in a neutral manner.
We added the behavioral indicator “the resident includes the information provided by involved third parties (including health care professionals, relatives, and friends) if this is relevant for the deliberation of preferences” to the final list since consensus was reached with a median score of 6, and 81% of the experts had a score ≥ 6 (seeTable 2).
세 차례의 델파이 라운드 끝에 졸업후 의학교육을 위한 4개의 SDM EPA와 18개의 행동 지표에 대한 합의가 이루어졌습니다(표 2 참조). 32명의 전문가 중 30명(94%)이 이 SDM EPA 및 행동 지표 목록에 동의했습니다. 이 목록에 동의하지 않은 2명의 전문가는 어떠한 질적 피드백도 제공하지 않았습니다. 합의에 도달한 4개의 EPA는 모두 "이 EPA/행동 지표는 임상 실무에 적용 가능하다"는 문항에서 높은 평가를 받았지만, 합의에 도달한 18개의 행동 지표 중 11개에 대해서만 75% 이상의 전문가 패널이 이 문항에 6점 이상을 부여했습니다(표 2 참조). After 3 Delphi rounds, consensus was reached on 4 SDM EPAs and 18 behavioral indicators for postgraduate medical education (seeTable 2). Of the 32 experts, 30 (94%) agreed on this list of SDM EPAs and behavioral indicators. The 2 experts who did not agree with this list did not give any qualitative feedback. All 4 EPAs on which consensus was reached also received high ratings on the statement “this EPA/behavioral indicator is applicable in clinical practice”; however, this statement was scored ≥ 6 by ≥ 75% of the expert panel on only 11 of the 18 behavioral indicators on which consensus was reached (seeTable 2).
토론 Discussion
주요 결과 요약 Summary of main findings
이 델파이 연구에서 네덜란드의 다학제 전문가 32명으로 구성된 패널은 SDM의 일상적 적용을 늘리기 위해 전공의가 졸업후 의학교육 과정에서 교육받아야 하는 4개의 EPA와 18개의 관련 행동 지표에 대해 합의에 도달했습니다. 최종 목록에 대한 94%(n = 30)의 동의는 높은 수준의 합의가 이루어졌음을 나타냅니다. In this Delphi study, a multidisciplinary Dutch panel of 32 experts reached consensus on 4 EPAs and 18 associated behavioral indicators for SDM that residents should be trained in during postgraduate medical education to increase the routine application of SDM. The 94% (n = 30) agreement on the near-final list indicates a high degree of consensus.
주요 결과에 대한 반성 Reflection on main findings
개발된 EPA는 잘 알려진 SDM 모델과 일치하며,35,36 졸업후 의학 교육의 최종 숙련도 수준에 맞게 공식화된 SDM 행동을 설명하고 적절한 SDM을 일상적으로 적용할 수 있는 임상의를 배출하는 것을 목표로 합니다.23 기본 행동 지표는 직장 학습 중 개별 학습 요구에 따라 EPA의 구성 요소를 해결할 수 있는 여지를 제공함으로써 맞춤형 학습 과정을 지원합니다. 개발된 EPA의 의도는 이론과 실무를 연계하고 전문적 실무 단위를 설명하여 역량을 연결하는 것입니다.24 2015 CanMEDS 의사 역량 프레임워크에서 SDM의 운영은 일반적으로 3가지 역량에 설명되어 있습니다. 이는 다음에 중점을 둡니다.14
각 환자의 고유한 요구와 선호도, 임상 상태와 상황에 맞게 SDM을 적용하는 것,
환자 및 그 가족을 존중하고 비판하지 않으며 문화적으로 안전한 방식으로 논의하는 것,
환자의 건강에 관한 정보에 입각한 결정을 지원하기 위한 의사소통 기술과 전략을 사용하는 것
The developed EPAs, which are in line with well-known SDM models,35,36describe SDM behaviors formulated for the end-stage proficiency level of postgraduate medical training, and aim to deliver clinicians that are able to routinely apply adequate SDM.23The underlying behavioral indicators support tailored learning processes by providing room to address the building blocks of the EPAs, depending on individual learning needs during workplace learning. The intention of the developed EPAs is to align theory and practice and bridge competencies by describing units of professional practice.24In the 2015 CanMEDS physician competency framework, the operationalization of SDM is generic and described in 3 enabling competencies. These focus on
adapting SDM to the unique needs and preferences of each patient and to his or her clinical condition and circumstances;
facilitation of discussions with patients and their families in a respectful, nonjudgmental, and culturally safe manner; and
use of communication skills and strategies to support informed patient decisions regarding their health.14
SDM EPA는 여러 임상적 만남에서 발생할 수 있는 의사 결정의 기본 과정을 설명하기 위해 고안되었습니다. 여기에는 의학 지식, 커뮤니케이션, 협업, EBM과 같은 역량 영역이 통합되어 있습니다. 이러한 방식으로 진행하면서 우리는 2014년 Warm 등이 레지던트를 위한 관찰 가능한 실습 활동의 매핑에 관한 연구에서 프로세스 지향으로 분류한 EPA를 개발하고자 했습니다. 이러한 EPA는 의료 분야(예: 비뇨기과 의료 분야의 요실금 평가)에 특화된 내용 중심 EPA와 구별되어야 합니다.39 2019년 EPA에 대한 범위 검토에서 Shorey와 동료들은 이러한 전문 분야별 EPA 개발에 초점을 맞춘 12개의 연구를 살펴봤는데, 대부분 의학 졸업후 교육에 관한 것이었습니다.26 SDM은 의학적 요구와 환자의 가치 및 선호도를 고려하여 의료 분야의 구체적인 임상 업무에 매핑된 역량을 상황에 맞게 적용해야 하므로, 이 연구에서 개발된 SDM EPA는 그 실행을 지원할 수 있습니다.40 Our SDM EPAs are intended to describe the underlying process of decision making, which may take place over several clinical encounters. They integrate competency domains, such as medical knowledge, communication, collaboration, and EBM. In proceeding in this manner, we intended to develop EPAs that Warm et al categorized in their 2014 study on the mapping of observable practice activities for residents as process oriented. These EPAs must be distinguished from content-oriented EPAs, which are specific for the medical discipline (e.g., evaluating urinary incontinence in the medical discipline of urology).39In a 2019 scoping review of EPAs, Shorey and colleagues looked at 12 studies that all focused on the development of these specialty-specific EPAs, mostly for medical graduate education.26The SDM EPAs developed in this study may support their implementation, as SDM requires a context-specific application of competencies mapped to concrete clinical tasks of the medical discipline, taking the medical needs and the values and preferences of the patient into consideration.40
시사점 Implications
다음 단계는 기존의 역량 기반 직장 커리큘럼에 SDM EPA를 구현하는 것입니다. SDM 교육의 효과에 관한 문헌을 검토한 결과, 의료 전문가를 대상으로 한 대부분의 개입은 단일 교육 세션으로 구성되었으며, 시간이 지남에 따라 임상에서 SDM의 지속 가능한 적용이 감소하는 것으로 나타났습니다.12,41-43 임상에서 학습과 지속 가능한 적용 사이의 전달 격차를 해소하고 미래 임상의의 전문 레퍼토리에 SDM EPA를 통합하는 것을 지원하기 위해 종단적 직장 교육이 필요합니다.22 확인된 EPA는 임상에서 SDM 과정을 관찰하고 이러한 관찰을 기반으로 의미 있는 피드백을 제공하기 위한 도구로 사용될 수 있습니다. SDM EPA가 전문성 개발을 지원하려면 개별 학습 과정이 시작점이 되어야 하며, 이를 통해 EPA를 박스 체크 연습으로 사용하는 것을 방지할 수 있습니다. 현재 전문의 수련에서 EPA가 사용되는 방식에 따라, 확인된 EPA는 레지던트의 역량 수준을 평가하는 데 지침이 될 수도 있습니다. 또한, 적절한 역할 모델링은 직장 기반 학습에 필수적이므로 임상 수퍼바이저의 지속적인 전문 교육에 EPA를 통합하여 SDM 역량을 강화할 수 있습니다. SDM은 EBM의 핵심 구성요소이며, 문헌에 따르면 레지던트들이 환자 중심 의사소통과 같은 복잡한 기술을 의료 전문 지식과 통합할 때 가장 효과적으로 학습하는 것으로 나타났기 때문에,18,19 졸업후 EBM 커리큘럼에 SDM EPA를 통합할 것을 제안합니다.17,19 추가 연구를 통해 SDM 학습에 대한 잠재적 장벽 및 촉진 요인을 해결하고 학습자에게 임상에서 SDM을 실천할 수 있는 구체적인 언어의 예를 제공할 필요가 있습니다. A next step is the implementation of the SDM EPAs in existing competency-based workplace curricula. A review of the literature on the effects of training SDM showed that most interventions with health professionals consisted of single training sessions and that sustainable application of SDM in clinical encounters diminished over time.12,41–43Longitudinal workplace training is necessary to bridge the transfer gap between learning and sustainable application in clinical practice and to support integration of the SDM EPAs into the professional repertoire of future clinicians.22The identified EPAs can be used as a tool for observing the SDM process in clinical encounters and for providing meaningful feedback based on these observations. For the SDM EPAs to support the development of expertise, individual learning processes should be a starting point to prevent using the EPAs as a box-checking exercise. In line with how EPAs are currently used in medical specialty training, the identified EPAs may also guide the assessment of the resident’s level of competence. Additionally, the EPAs can be incorporated into the continuous professional education of clinical supervisors to enhance their SDM competence since adequate role modeling is essential in workplace-based learning. Because SDM is a key component of EBM and literature shows that residents learn complex skills such as patient-centered communication optimally when these skills are integrated with medical expertise,18,19we suggest integrating SDM EPAs into the postgraduate EBM curricula.17,19Further research needs to address potential barriers to and facilitators for learning SDM and to provide learners with examples of concrete language to practice SDM during their clinical encounters.
강점과 한계 Strengths and limitations
저희가 알기로는 SDM에 대한 EPA와 행동 지표에 대한 연구는 이번이 처음입니다. 델파이 기법은 EPA와 행동지표에 대한 합의를 도출하는 데 적합한 접근법이라고 생각하며, 전문가들이 익명으로 개별적으로 설문지를 작성하도록 하여 다른 패널의 직접적인 영향을 제한하고 개별 의견에 동등한 가중치를 부여했습니다.29-31 이전 라운드의 결과를 다음 라운드에 피드백함으로써 다른 전문가들의 평가와 관련하여 초기 의견을 재고하도록 장려하고자 했습니다. To our knowledge, this is the first study on EPAs and behavioral indicators for SDM. We believe the Delphi technique is a suitable approach to gain consensus on EPAs and behavioral indicators; we limited direct influence of other panel members and weighted individual opinions equally by having the experts fill in questionnaires anonymously and individually.29–31By feeding back the results of the previous round to the next, we intended to promote reconsideration of initial opinions in relation to other experts’ ratings.
참여자의 배경이 다양하고 관련성이 있다고 판단되는 모든 배경이 참여함으로써 개발된 EPA의 품질이 향상되었다고 생각합니다. 이러한 EPA의 품질은 졸업후 의학 교육에 적용하기가 더 쉬워질 수 있습니다. 첫 번째 라운드를 완료한 32명의 전문가 패널은 모두 델파이 프로세스 전체를 완료했는데, 이는 주제에 대한 전문가들의 관심, 연구의 중요성, 그리고 라운드의 빠른 연속성을 반영하는 결과입니다. 첫 번째 델파이 라운드에서는 포괄적인 사전 작업을 바탕으로 개발한 EPA와 행동 지표를 사용했습니다. 전통적인 델파이 연구에서는 전문가들이 직접 EPA와 행동 지표를 생성할 수도 있었지만, 이러한 접근 방식은 전문가들에게 너무 많은 시간이 소요될 수 있다고 생각했습니다. 전문가들이 질적 피드백을 제공하도록 장려하여 이러한 영향을 최소화하고자 했지만, 이러한 선택이 EPA 및 행동 지표 목록의 구성에 영향을 미쳤을 수 있습니다. 전문가들의 의견을 분석한 결과, EPA 및 행동지표의 내용에 큰 변화가 필요하지 않다고 판단했으며, 이 결과는 연구를 위해 개발한 EPA 및 행동지표의 적절성을 확인한 것으로 보입니다. We believe the quality of the developed EPAs was improved by the differences in the participants’ backgrounds and by the presence of all backgrounds we considered relevant. The quality of these EPAs may make it easier to implement them in postgraduate medical education. All 32 expert panel members who completed the first round completed the entire Delphi process, which reflects experts’ interest in the theme, the importance of the study, and the quick succession of the rounds. For the first Delphi round, we used EPAs and behavioral indicators that we had developed based on our comprehensive preliminary work. Although in a traditional Delphi study, experts could have generated EPAs and behavioral indicators themselves, we believe that this approach would have been too time consuming for the experts. Our choice may have influenced the composition of the list of EPAs and behavioral indicators although we intended to minimize such influence by encouraging the experts to give qualitative feedback. Based on our analysis of the experts’ input, we determined no substantial changes to the content of the EPAs and behavioral indicators were needed; this result seems to confirm the appropriateness of the EPAs and behavioral indicators that we developed for the study.
이 델파이 연구는 언어와 문화에 매우 민감하기 때문에 네덜란드의 국가 단위로 한정하여 실시했습니다. 그럼에도 불구하고 EPA에는 다른 국가에서도 각자의 국가적 필요에 맞게 적용할 수 있는 일반적인 요소가 포함되어 있습니다. 졸업후 의학 교육에 적용하려고 했음에도 불구하고 이 델파이 연구에 레지던트를 참여시키지 않은 이유는 EPA와 SDM의 개념이 레지던트에게 너무 복잡하다고 생각했기 때문입니다. 하지만 전공의를 포함시켰다면 SDM 교육을 받을 때 전공의가 직면하는 전이 격차에 대해 더 많은 인사이트를 얻을 수 있었을 것입니다. We limited our implementation of this Delphi study to the national level, in the Netherlands, because SDM is very sensitive to language and culture. Nonetheless, the EPAs include generic elements that other countries can adapt to their national needs. We decided not to invite residents to participate in this Delphi study despite the intended implementation in postgraduate medical training because we believe that the concepts of EPAs and SDM are too complex for residents. However, including residents might have given us more insight into the transfer gap they face when being trained in SDM.
결론 Conclusions
우리는 SDM 교육의 질과 임상에서 SDM의 적용을 개선하기 위해 졸업후 의학 교육을 위한 SDM의 EPA와 관련 행동 지표를 개발하는 데 성공했습니다. We succeeded in developing EPAs and associated behavioral indicators for SDM for postgraduate medical education to improve the quality of SDM training and the application of SDM in clinical practice.
Acad Med. 2021 Jan 1;96(1):126-133.doi: 10.1097/ACM.0000000000003618.
Identifying Entrustable Professional Activities for Shared Decision Making in Postgraduate Medical Education: A National Delphi Study
1A. Baghus is a PhD student and resident, Department of Family Medicine, Care and Public Health Research Institute, Maastricht University, Maastricht, the Netherlands; ORCID: http://orcid.org/0000-0002-6481-9256 .
2E. Giroldi is assistant professor, Department of Family Medicine, Care and Public Health Research Institute and Department of Educational Development and Research, School of Health Professions Education, Maastricht University, Maastricht, the Netherlands; ORCID: http://orcid.org/0000-0003-3254-4849 .
3J. Muris is professor, Department of Family Medicine, Care and Public Health Research Institute, Maastricht University, Maastricht, the Netherlands; ORCID: http://orcid.org/0000-0002-8780-476X .
4A. Stiggelbout is professor, Department of Biomedical Data Sciences, Leiden University Medical Center, Leiden, the Netherlands; ORCID: http://orcid.org/0000-0002-6293-4509 .
5M. van de Pol is associate professor, Department of Primary and Community Care, Radboud University Medical Center, Nijmegen, the Netherlands; ORCID: http://orcid.org/0000-0002-0977-7954 .
6A. Timmerman is assistant professor, Department of Family Medicine, Care and Public Health Research Institute, Maastricht University, Maastricht, the Netherlands; ORCID: http://orcid.org/0000-0002-8114-8802 .
7T. van der Weijden is professor, Department of Family Medicine, Care and Public Health Research Institute, Maastricht University, Maastricht, the Netherlands; ORCID: http://orcid.org/0000-0002-7469-3781 .
Purpose:Although shared decision making (SDM) is considered the preferred approach in medical decision making, it is currently not routinely used in clinical practice. To bridge the transfer gap between SDM training and application, the authors aimed to reach consensus on entrustable professional activities (EPAs) for SDM and associated behavioral indicators as a framework to support self-directed learning during postgraduate medical education.
Method:Using existing literature on SDM frameworks and competencies; input from an interview study with 17 Dutch experts in SDM, doctor-patient communication, and medical education; and a national SDM expert meeting as a starting point, in 2017, the authors conducted a modified online Delphi study with a multidisciplinary Dutch panel of 32 experts in SDM and medical education.
Results:After 3 Delphi rounds, consensus was reached on 4 EPAs-(1) the resident discusses the desirability of SDM with the patient, (2) the resident discusses the options for management with the patient, (3) the resident explores the patient's preferences and deliberations, and (4) the resident takes a well-argued decision together with the patient. Consensus was also reached on 18 associated behavioral indicators. Of the 32 experts, 30 (94%) agreed on this list of SDM EPAs and behavioral indicators.
Conclusions:The authors succeeded in developing EPAs and associated behavioral indicators for SDM for postgraduate medical education to improve the quality of SDM training and the application of SDM in clinical practice. These EPAs are characterized as process EPAs for SDM in contrast with content EPAs related to diverse medical complaints. A next step is the implementation of the SDM EPAs in existing competency-based workplace curricula.
학부의학교육에서 지속적 질 개선의 문화 만들기(Acad Med, 2020) Shaping a Culture for Continuous Quality Improvement in Undergraduate Medical Education Guy W.G. Bendermacher, MSc, Willem S. De Grave, MSc, PhD, Ineke H.A.P. Wolfhagen, MSc, PhD, Diana H.J.M. Dolmans, MSc, PhD, and Mirjam G.A. oude Egbrink, MSc, PhD
지속적인 질 향상(CQI) 전략은 커리큘럼이 발전하는 대중의 요구, 근거 기반 의학, 효과와 효율성에 대한 관심 증가에 발맞춰야 한다는 점에서 의과대학에 매우 중요합니다.1,2 1990년대 초부터 의과대학은 질 관리 접근 방식에 상당한 투자를 해왔으며, 그 결과 직원 성과에 대한 더 나은 통찰력, 개선이 필요한 주제를 알리는 기회, 더 명확하게 정의된 책임 등을 확보할 수 있었습니다.3,4 Continuous quality improvement (CQI) strategies are of key importance to medical schools, given the need for curricula to keep pace with advancing public demands, evidence-based medicine, and an increased attention to effectiveness and efficiency.1,2Since the early 1990s, medical schools have invested considerably in quality management approaches, resulting in better insights in staff performance, further opportunities to signal topics for improvement, and more clearly defined responsibilities.3,4
CQI는 학교가 교육의 질에 대한 다양한 개념을 체계적으로 다루기 위해 도전하는 상태와 유사합니다. 이해관계자의 관점에 따라 교육의 질은 다음과 같이 이해할 수 있습니다.5
목적 적합성(유능한 미래 의사 교육),
비용 대비 가치(교육에 대한 투자 수익),
완벽성(결함 제로에 집중),
탁월성(최고의 프로그램으로 우뚝 서기),
혁신성(교육 학습 효과에 집중)
계획-실행-점검(PDCA) 사이클과 같은 실행 프레임워크는 CQI가 반복적이고 점진적인 과정임을 설명해줍니다. PDCA 사이클에서는 교육 결과를 미리 정해진 목표와 비교하고, 평가를 바탕으로 격차를 해소하기 위한 조치를 취할 수 있습니다.6 CQI resembles a state in which schools take on the challenge to address different notions of educational quality in a methodical manner. Depending on the perspective of a stakeholder, educational quality can be understood as
fitness for purpose (educating capable future physicians),
value for money (a return on investment in education),
perfection (focusing on zero defects),
exceptional (standing out as the best program), or
transformative (focusing on the educational learning effect).5
Implementation frameworks such as the plan–do–check–act (PDCA) cycle illustrate that CQI is a repetitive and incremental process. The PDCA cycle holds that educational outcomes are compared to predetermined goals and that based on evaluations, action can be taken to address disparities.6
현재의 품질 관리 접근법의 긍정적인 효과에도 불구하고 교육 개선이 간단한 과정이 아니라는 공감대가 확산되고 있습니다.7 이 개념을 뒷받침하는 세 가지 주요 주장이 있습니다.
첫째, 질 관리 시스템과 프로세스의 성공 여부는 교수진, 지원 직원 및 학생이 이를 구현하고 수용하는 방식에 달려 있습니다.8 예를 들어, 학문적 자유의 전통은 프로그램 평가의 판단적 성격과 상충될 수 있습니다.9
둘째, 의과대학은 다양한 하위 문화를 포함하는 복잡하고 계층적인 조직입니다.10 이러한 특성은 개선 노력에 대한 집단적 참여를 방해합니다.11
셋째, CQI는 이용 가능한 정보, 시간 및 인센티브에 의해 제한됩니다.12 교육 개선을 위한 추가 노력에 대한 보상이 부족하면 평가가 구체적인 행동으로 이어지지 않는 이유를 설명할 수 있습니다.13
Notwithstanding the positive effects of current quality management approaches, there is a growing consensus that educational improvement is not a straightforward process.7Three main arguments underpin this conception.
First, the success of quality systems and processes depends on the way they are implemented and received by faculty, support staff, and students.8Traditions of academic freedom, for instance, can stand at odds with the judgmental character of program evaluations.9
Second, medical schools are complex, hierarchical organizations, which include different subcultures.10These characteristics hamper a collective engagement in improvement efforts.11
Third, CQI is bounded by available information, time, and incentives.12The lack of rewards for extra efforts to improve education can explain why evaluations are not followed up with concrete actions.13
CQI를 위한 구조와 프로세스는 교육의 질에 대한 관심을 핵심으로 하는 조직(하위)문화에 의해 보완되어야 한다는 생각은 질 문화 개념의 토대를 형성합니다.14,15 이 개념은 조직문화가 "외부 적응과 내부 통합의 문제에 대처하는 방법"16 을 반영한다는 관점과 연결되며 조직(하위)문화와 성과에 대한 이전 연구를 기반으로 합니다.17
질 문화는 신뢰와 참여를 촉진하고
리더십과 커뮤니케이션은 하드(시스템 또는 프로세스 지향)와 소프트(심리적 또는 가치 관련 지향) 차원 간의 연결을 강화할 수 있습니다.18,19
The idea that structures and processes for CQI should be complemented by an organizational (sub)culture with care for educational quality at its core forms the foundation of the quality cultureconcept.14,15This concept is linked to the perspective that organizational cultures reflect “a way to cope with problems of external adaptation and internal integration,”16and builds on previous research on organizational (sub)culture(s) and performance.17
A quality culture promotes trust and involvement, while
leadership and communication can reinforce the link between its hard (system or process oriented) and soft (psychological or value-related oriented) dimensions.18,19
여러 연구가 질 문화 개념을 더 잘 정의하는 데 기여했으며20,21 고등 교육 내 하위 문화를 식별했습니다.22,23 또한 이전 연구는 질 관리의 성공이 문화적 요인 및 교수진 선호와의 얼라인먼트로 설명될 수 있다는 통찰에 기여했습니다.24,25 그러나 품질 문화에 대한 대부분의 연구는 이론적이고 설명적인 성격을 띠고 있습니다.19 질 정책 및 절차에 참여하는 학생과 교수진이 질 문화를 개념화하는 방식에 대한 실증적 연구가 부족합니다. 특히, 업무와 관련된 심리적 태도가 질 관리 및 책임 절차에 어떤 영향을 미치는지에 대한 교육기관 전반의 통찰력 강화가 필요합니다. 이 분야에 대한 지식의 증대는 품질 문화 육성의 장점을 뒷받침할 것입니다. 본 연구는 조직의 질 문화의 주요 특징이 무엇이며 이러한 특징이 학부 의학교육의 지속적인 개선에 어떻게 기여하는지에 대한 질문을 다룹니다. 의과대학의 CQI 시스템과 프로세스가 점점 더 유사해지고 있는 가운데, 우리는 주로 업무 관련 심리적 태도와 조직 가치 지향성이 CQI에 어떤 차이를 만드는지에 초점을 맞춥니다. Several studies have contributed to a better definition of the quality culture concept20,21and have identified subcultures within higher education.22,23Moreover, previous research has contributed to the insight that the success of quality management can be explained by its alignment with cultural factors and faculty preferences.24,25Yet most studies on quality culture are of a theoretical, descriptive nature.19There is a lack of empirical research on the way students and faculty involved in quality policies and procedures conceptualize a quality culture. Specifically, an enhanced insight across institutions is needed in how work-related psychological attitudes counterbalance quality control and accountability procedures. Increased knowledge in this area will support the merit of nurturing a quality culture. Our study addresses the questions what are the key features of an organizational quality culture and how do these features contribute to continuous improvement of undergraduate medical education? As systems and processes for CQI in medical schools are increasingly becoming alike, we mainly focus on how work-related psychological attitudes and organizational value orientations make a difference in CQI.
방법 Method
연구 설계 Study design
우리는 사회 구성주의적 관점에서 다기관 포커스 그룹 연구를 수행했습니다. 연구 설계는 연역적(이론에서 실천으로) 접근법과 귀납적(실천에서 이론으로) 접근법을 결합한 것이 특징입니다.26 포커스 그룹 토론은 참가자들의 다양한 경험, 관점, 태도를 포착하는 데 도움이 되었습니다.27 데이터 수집, 분석, 해석은 순차적으로 진행되어 분석 절차를 반복적으로 조정하고 개선할 수 있었습니다. We conducted a multicenter focus group study, operating from a social constructivist stance. The study design is characterized by combining a deductive (from theory to practice) and inductive (from practice to theory) approach.26Focus group discussions served to capture the broad array of participants’ experiences, perspectives, and attitudes.27Data collection, analysis, and interpretation were conducted sequentially, allowing for iterative adaptations and refinement of the analysis procedure.
설정 Setting
네덜란드의 8개 의과대학의 교육 품질 자문위원회(EC)가 이 연구에 참여하도록 의도적으로 선정되었습니다. EC 위원은 공식적으로 선출된 교수진과 학생 대표로 구성됩니다. EC의 주요 임무는 교육의 질에 영향을 미치는 모든 문제에 대한 권고 사항을 프로그램 경영진에 제공하는 것입니다. EC는 프로그램 평가가 조직되는 방식에 대해 공식적으로 동의하고 조언할 수 있는 권한을 갖습니다. 위원회는 동일한 수의 학생과 교수진으로 구성됩니다(각 EC는 8~12명의 위원으로 구성). EC를 대상으로 포커스 그룹을 실시하는 데는 네 가지 이유가 있습니다.
첫째, EC 교수진은 일반적으로 교육의 개발, 실행, 평가 및 개선에 대한 풍부한 경험을 가진 학자들입니다. 임상, 비임상 또는 전임상, 연구 및 교육 분야의 교수진이 참여 EC에 포함되어 있습니다.
둘째, EC 구성원은 현재 시행 중인 품질 시스템 및 절차에 대해 잘 알고 있으며, EC 구성원은 교육 및 평가 및 정책 부서와의 협력을 통해 이러한 시스템 및 절차에 대한 추가 지식을 습득했습니다.
셋째, EC에는 학생 대표가 포함됩니다. 이러한 대표성을 통해 품질과 품질 개선에 대해 교수진 외에 다른 관점을 반영할 수 있습니다.
넷째, 교수진과 학생의 공통된 EC 멤버십을 통한 친분은 이질적인 그룹 환경에서 열린 토론을 촉진합니다.
Education quality advisory committees (ECs) of the 8 medical schools in the Netherlands were purposively selected to participate in this research. EC members are formally elected faculty and student representatives. The central task of ECs is to provide the program management with recommendations on all matters influencing quality of education. ECs have formal rights of consent and advice on the manner in which program evaluations are organized. The committees consist of an equal number of students and faculty (each EC has 8 to 12 members). Four reasons underpin the choice to conduct focus groups among ECs.
First, EC faculty generally are academics with ample experience in the development, implementation, evaluation, and improvement of education. Faculty with clinical, nonclinical or preclinical, research, and education backgrounds are represented in the participating ECs.
Second, EC members are familiar with the quality systems and procedures in place; EC members have derived additional knowledge on these systems and procedures through training and cooperation with evaluation and policy departments.
Third, ECs include student representatives. This representation allows for the incorporation of a different perspective on quality and quality improvement (besides that of faculty).
Fourth, the acquaintance of faculty and students through their shared EC membership facilitates open discussion in a heterogeneous group setting.
네덜란드의 각 의과대학은 학교의 역사, 연구 및 교육 실적, 학생의 다양성에 따라 다소 독특한 조직 문화를 가지고 있습니다. 또한 학교 내에서 적용되는 교육적 접근 방식도 어느 정도 다릅니다. 그러나 학교마다 적용되는 교육 조직 구조와 품질 관리 접근 방식은 비슷합니다. 모든 프로그램은 학술 의료 센터에서 제공하거나 학술 의료 센터와 긴밀히 협력하여 제공합니다. 모든 참여 학교에서는 PDCA 사이클이 CQI의 지침 구조로 사용되며, 모든 프로그램은 네덜란드 학부 의학교육 프레임워크를 준수합니다.28 Each medical school in the Netherlands has a somewhat distinct organizational culture based on its history, record in research and education, and diversity of student intake. Moreover, educational approaches applied within the schools vary to some extent. The educational organization structures and quality management approaches applied across schools are comparable, however. All programs are offered by, or in close cooperation with, academic medical centers. In all participating schools, the PDCA cycle serves as guiding structure for CQI, and all programs adhere to the Dutch Framework for Undergraduate Medical Education.28
데이터 수집 Data collection
우리는 PDCA 주기에 따라 질문이 구조화된 초기 포커스 그룹 가이드를 개발했습니다. 이 구조를 따르기로 한 것은 이 주기의 각 단계를 최적화하는 것이 CQI로 이어질 것이라는 전제하에 결정되었습니다. 이 가이드(부록 디지털 부록 1: https://links.lww.com/ACADMED/A909)는 연구자의 소속 기관의 전직 EC 위원들과 함께 파일럿 포커스 그룹 세션에서 테스트한 후 질문 순서를 수정하고 이론적 개념의 사용을 제한하는 등 조정을 거쳤습니다. 2018년 5월, 네덜란드에 있는 8개 의과대학의 EC에 모두 연락을 취했습니다. 8개 위원회 중 6개 위원회가 참여하기로 동의했습니다. 참여하지 않은 위원회는 회의 계획에 필요한 시간 투자 및 어려움, EC 구성의 변화 등을 이유로 들었습니다. 총 40명의 EC 위원(학생 18명, 교수진 22명)이 6개의 포커스 그룹에 참여했습니다(표 1 참조). 회의는 2018년 7월부터 12월까지 진행되었습니다. 모든 회의(평균 시간 79분)는 있는 그대로 기록되었고, 익명화 및 코딩된 녹취록이 참가자들에게 전송되어 승인을 받았습니다. 각 포커스 그룹을 시작할 때 참가자들에게 양질의 문화에서 가장 중요한 요소가 무엇이라고 생각하는지 적어달라고 요청했습니다. 이 활동은 사전 지식을 활성화하고 데이터 삼각 측량의 한 형태로 사용되었습니다. 포커스 그룹 회의가 끝날 무렵에는 참가자들에게 그들이 작성한 의견이 토론에 포함되었는지 물어보았습니다. We developed an initial focus group guide, with questions structured according to the PDCA cycle. The choice to follow this structure was based on the presupposition that optimizing each step of this cycle will lead to CQI. The guide (Supplemental Digital Appendix 1 athttps://links.lww.com/ACADMED/A909) was tested in a pilot focus group session with former EC members from the researchers’ home institution and thereafter adjusted; the order of questions was revised, and the use of theoretical concepts was limited. In May 2018, we approached the ECs of all 8 medical schools in the Netherlands. Six of the 8 committees agreed to participate. Reasons given for not participating were the required time investment and difficulty in planning a meeting and changes in the composition of the ECs. In total, 40 EC members (18 students and 22 faculty) participated in the 6 focus groups (seeTable 1). The meetings were conducted between July and December 2018. All meetings (average duration, 79 minutes) were transcribed verbatim, and anonymized and coded transcripts were sent to participants for approval. At the start of each focus group, we asked participants to write down what they considered the most important elements of a quality culture. This exercise activated prior knowledge and was used as a form of data triangulation. At the end of the focus group meeting, we asked participants if their written comments were covered in the discussion.
데이터 분석을 위해 단계적 주제 분석의 일종인템플릿 분석을 사용했습니다. 템플릿 분석에서는 계층적으로 구조화된 테마로 구성된 일련의 코딩 템플릿을 개발하여 데이터에 반복적으로 적용합니다. 분석이 진행됨에 따라 테마는 지속적으로 수정됩니다.29
첫 번째 단계로, G.W.G.B.와 W.S.d.G.는 코딩된 2개의 트랜스크립트를 독립적으로 열어 트랜스크립트 내 및 트랜스크립트 간에 반복되는 코드를 검색합니다. 품질 문화에 관한 최근 문헌고찰에 기술된 주제가 민감성 개념으로 사용되었습니다.19
그 후, 두 저자는 만나서 코드를 비교하고 병합하여 주제를 식별했습니다.
초기 코딩 템플릿은 24개의 주제와 183개의 코드로 구성되었습니다.
그 후 G.W.G.B.는 나머지 기록의 분석을 바탕으로 템플릿을 반복적으로 변경했습니다. 이러한 변경 사항에는 코드의 세부 사항 추가, 병합 및 연결이 포함되었습니다.
이후 G.W.G.B.와 W.S.d.G.가 다시 만나 코딩 템플릿의 최종 버전(25개의 테마와 199개의 코드 포함)을 확정했습니다.
마지막 단계로, G.W.G.B.는 최종 버전의 템플릿을 사용하여 모든 트랜스크립트를 다시 코딩했습니다.
분석 프로세스는 Atlas-ti 8.3 소프트웨어(ATLAS.ti, GmbH, 독일 베를린)를 사용하여 지원되었습니다. 포커스 그룹이 시작될 때 수행한 서면 연습의 코딩, 녹취록 분석, 전체 연구팀과의 녹취록 토론을 통해 5가지 중요한 주제를 식별하는 데 기여했습니다. We used template analysis, a stepwise type of thematic analysis, to analyze the data. In template analysis, a succession of coding templates consisting of hierarchically structured themes is developed and iteratively applied to the data. Themes are modified continuously as the analysis progresses.29
As a first step, G.W.G.B. and W.S.d.G. open coded 2 transcripts independently, searching for codes that recurred within and between transcripts. Topics described in a recent literature review on quality culture served as sensitizing concepts.19
Subsequently, these 2 authors met to compare and merge codes and identify themes.
The initial coding template comprised 24 themes and 183 codes.
Iterative changes to the template were then made by G.W.G.B. based on the analysis of remaining transcripts. These changes concerned further detailing, merging, and linking codes.
Hereafter, G.W.G.B. and W.S.d.G. met again to establish the final version of the coding template (including 25 themes and 199 codes).
As a last step, G.W.G.B. recoded all transcripts using the final version of the template.
The analysis process was supported by application of Atlas-ti 8.3 software (ATLAS.ti, GmbH, Berlin, Germany). The coding of the written exercise performed at the start of focus groups, analysis of transcripts, and discussion of transcripts with the full research team contributed to the identification of 5 overarching themes.
반사성 Reflexivity
데이터 수집 및 분석 단계에서 다양한 해석을 반영하기 위해 전체 연구팀은 여러 차례 회의를 가졌습니다. 이 회의에서는 익명화 및 코딩된 녹취록, 현장 노트, CQI에 대한 각자의 이해에 대해 논의했습니다. 모든 연구팀원은 네덜란드 마스트리흐트 대학교 보건직업교육대학의 보건, 의학 및 생명과학 학부에 소속되어 있습니다. 포커스 그룹 진행자(W.S.d.G.)는 개인 및 그룹 인터뷰 경험이 풍부한 교육 과학자입니다. 양질의 문화 개발 박사 과정 중인 또 다른 팀원은 관찰자이자 메모 작성자(G.W.G.B.)로 활동했습니다. 연구팀에는 품질 보증 경험이 있는 교육 과학자(I.H.A.P.W.), 의학교육 혁신가인 의학 생리학자(M.G.A.o.E.), 혁신적인 학습 준비에 중점을 둔 교육 과학자(D.H.J.M.D.)가 추가로 포함되었습니다. 품질 관리, 정책 결정, 의학교육 등 다양한 전문성을 바탕으로 다양한 관점을 포함할 수 있었습니다. 팀 토론을 통해 연구 결과에 대한 합의에 도달했습니다. To reflect on diverse interpretations in the data gathering and analysis stages, the full research team held several meetings. In these meetings, we discussed the anonymized and coded transcripts, field notes, and our individual understandings of CQI. All research team members are affiliated with the Faculty of Health, Medicine and Life Sciences at the School of Health Professions Education at Maastricht University in the Netherlands. The focus group moderator (W.S.d.G.) is an educational scientist with extensive experience in interviewing individuals and groups. Another team member, who is a doctoral candidate in quality culture development, acted as observer and note taker (G.W.G.B.). The research team further included an educational scientist with experience in quality assurance (I.H.A.P.W.), a medical physiologist who is a medical education innovator (M.G.A.o.E.), and an educational scientist focusing on innovative learning arrangements (D.H.J.M.D.). Our diverse expertise (in quality management, policy making, and medical education) enabled inclusion of multiple perspectives. From team discussions, we reached a negotiated consensus on the study’s results.
윤리적 고려 사항 Ethical considerations
이 연구는 네덜란드 의학교육윤리심의위원회(NVMO ERB-1046)의 승인을 받았습니다. The study was approved by the Dutch Association for Medical Education Ethical Review Board (NVMO ERB-1046).
연구 결과 Results
연구 결과 CQI의 질적 문화 구성 요소를 반영하는 5가지 주요 주제를 확인했습니다.
(1) 개방적 시스템 관점 육성,
(2) 교육 (재)설계에 이해관계자 참여,
(3) 교육과 학습의 가치인정,
(4) 소유권과 책임 사이의 탐색,
(5) 통합적 리더십 구축
지원적인 커뮤니케이션 환경(조직의 리더에 의해 촉진될 수 있음)은 처음 네 가지 주제에 기여하고 그 안에 통합되어 있습니다. 다음 섹션에서는 이러한 주제와 그 특징적인 요소에 대해 논의하고(그림 1 참조), 포커스 그룹 회의(FGn)에서 도출된 학생(Sn) 및 교수진(Fn)의 발언을 인용하여 설명합니다. We identified 5 main themes that reflect quality culture constituents to CQI:
(1) fostering an open systems perspective,
(2) involving stakeholders in educational (re)design,
(3) valuing teaching and learning,
(4) navigating between ownership and accountability, and
(5) building on integrative leadership.
A supportive communication climate (which can be fueled by the organization’s leaders) contributes to, and is integrated within, the first 4 themes. In the following sections, we discuss the themes and their characterizing elements (seeFigure 1) and illustrate them with student (Sn) and faculty (Fn) quotes derived in the focus group meetings (FGn).
조사 결과 참가자들이 양질의 문화에서 가장 중요하게 생각하는 요소에 대한 일관된 그림이 드러났습니다. 따라서 결과는 통합된 방식으로 제시됩니다(학생과 교수진의 의견을 번갈아 제시). 참가자들의 응답은 PDCA 모델에 따라 구조화된 질문과 일치했으며, 이는 교직원과 학생들이 개선을 위한 체계적인 작업 방식을 내재화했음을 의미합니다. 이러한 결과는 포커스 그룹을 시작할 때 실시한 서면 연습에서 응답자들이 체계적인 접근 방식이나 PDCA 주기의 중요성을 자주 언급한 결과로 뒷받침됩니다(보충 디지털 부록 2: https://links.lww.com/ACADMED/A910). Our findings reveal a consistent picture on what participants considered the most important aspects of a quality culture. The results are therefore presented in an integrated manner (alternating student and faculty quotes). Participants’ responses were in line with prompts structured under the PDCA model, which implies that faculty and students have internalized a systematic way of working on improvement. This finding is supported by results from the written exercise performed at the start of the focus groups in which respondents frequently referred to the importance of systematic approaches or the PDCA cycle (Supplemental Digital Appendix 2 athttps://links.lww.com/ACADMED/A910).
개방적 시스템 관점 육성 Fostering an open systems perspective
참가자들은 개방적인 분위기와 외부 지향성, 실험과 혁신의 자유가 CQI에 필수적인 요소로 꼽았습니다. 이들은 내부적 연계(과정 간)와 외부적 연계(현장의 발전 및 요구사항)에 대한 끊임없는 필요성을 표명합니다. 다음 교수진의 사례에서 알 수 있듯이 개방형 시스템 관점을 취하는 것은 다양한 수준에서 관련이 있습니다: Participants identify a general atmosphere of openness, combined with an external orientation and freedom to experiment and innovate as essential for CQI. They express a constant need for internal alignment (between courses) and external alignment (with developments in, and requirements of, the field). As the following faculty member illustrates, taking an open systems perspective is relevant on different levels:
[코스 코디네이터는 엄밀한 의미에서 자신의 임무보다 조금 더 멀리 내다볼 필요가 있습니다. 저는 항상 이를 미시적 수준이라고 부르는데, 교육으로의 전환이 이루어지는 곳입니다. 하지만 중급 수준도 있습니다. 프로그램 내에서 무엇이 선행되고 무엇이 뒤따르는지를 고려해야 합니다. 수평적, 수직적 연결이 어떻게 이루어지고 있는지, 거시적 수준에서는 프로그램에서 사회적 맥락과 전문성에 대한 수요, 대학원 교육과의 연계까지....... 이렇게 복잡한 상황에서 교육을 발전시켜야 한다는 것이죠. 이것이 바로 도전입니다. (FG1, F5) [Course coordinators] need to look a bit further than just their assignment in the strict sense. I always call that the microlevel, where the translation to education is being made. But then, there’s also the mesolevel. Within the program, you should consider what precedes and what comes after. How the horizontal and vertical connections are made, and at the macrolevel, from the program to the societal context and the demand for specialisms, the alignment with postgraduate training…. That you have to develop education in such a complicated situation. That is the challenge. (FG1, F5)
참가자들은 조직의 적응력에 중요한 기여 요인으로 개방성과 외부 지향성을 언급합니다. 프로그램 환경 내부 또는 외부에서 얻은 새로운 인사이트는 CQI의 변화 동인으로 간주됩니다. 인증 패널의 권고, 의료계의 다른 프로그램과의 벤치마킹, 노동 시장의 의견, 교육자, 동료 및 학생의 조언 등을 통해 얻은 새로운 인사이트가 그 예입니다. 이러한 인사이트를 실행에 옮기려면 유연성, 창의성, 실험과 혁신의 여지가 필요합니다: Participants refer to openness and an external orientation as important contributors to the organization’s adaptivity. New insights obtained from within or outside the program environment are seen as drivers of change for CQI. Examples are new insights derived through recommendations by accreditation panels; benchmarking with other programs in medicine; inputs from the labor market; and advice from educationalists, peers, and students. To translate these insights into practice, flexibility, creativity, and room to experiment and innovate are needed:
실수를 해도 괜찮고 실수에 대해 솔직하게 말할 수 있는 문화가 조성되어야 합니다. 모든 것이 완벽하게 이루어지기를 서로에게 요구한다면 이를 억제해야 합니다....... 또한 ... 교육 자료가 완전히 고정되어 있지 않고 약간 유연한 형식으로되어있어 모든 사람이 자신의 길을 찾을 수 있습니다. 이렇게 하면 사람들이 더 많이 참여하고 다양한 접근 방식이 어떻게 작동하는지에 대한 정보를 수집할 수 있습니다. (FG1, F2) The related culture is that it is all right to make mistakes and that you can be open about it. If we demand from each other that everything goes perfect, then you suppress that…. Also … that the educational material is not completely set in stone, but has a bit of a flexible format, so that everyone can find their way in it. That way, people thrive and you can collect information on how different approaches work. (FG1, F2)
교수진이 교육 접근 방식을 과감하게 바꾸는 것이 중요합니다. 예를 들어, 강의가 그 자체로 효과적이지 않다는 말은 종종 있습니다. 그러나 우리는 여전히 강의가 일반적인 관행인 상황에 처해 있습니다. (FG3, S1) It is important that faculty dares to change educational approaches. For instance, it has often been said that lectures are not per se effective. However, we are still in a situation in which lectures are common practice. (FG3, S1)
학생과 교수진은 특히 커리큘럼 내용의 일관성을 유지하기 위해 교수팀 내, 교수 코디네이터 간의 소통에 주의를 기울여야 한다고 지적합니다. Students and faculty point out that communication within teaching teams and between teaching coordinators requires attention, especially to safeguard alignment of the curriculum content.
교육 (재)설계에 이해관계자 참여하기 Involving stakeholders in educational (re)design
EC 위원들은 교육을 (재)설계할 때 교수진과 학생의 참여와 공동의 목표 지향성에 주목해야 한다고 설명합니다. 이러한 참여는 다양한 시나리오, 기회, 과제를 고려하는 데 기여합니다: The EC members elaborate that involvement and a shared goal orientation of faculty and students in the (re)design of education require attention. This involvement contributes to considering various scenarios, opportunities, and challenges:
모든 사람은 그것[교육 발전]에 대해 다른 관점을 가지고 있으며, 모든 사람이 다른 가능성이나 구현을 봅니다. 예를 들어, 일이 잘못될 수도 있습니다. 서류상으로는 훌륭해 보이지만 학생과 교수진이 경험하는 것은 완전히 다를 수 있습니다. 그렇기 때문에 모든 사람의 참여가 필요하다고 생각합니다. (FG5, S2) Everyone has a different view on it [development of education], and everyone sees different possibilities or implementations. Also, for example, where things can go wrong. Something can look great on paper but can be experienced totally different by students and faculty. That is why I think we need everyone on board. (FG5, S2)
응답자들은 또한 기대치를 명확히 하고 불확실성을 제거하여 교육 변화 활동에 대한 지원을 창출하기 위해서는 교직원과 학생의 참여가 중요하다고 언급합니다. 그러나 실제로는 더 큰 규모의 커뮤니티를 참여시키고 소통하는 목표를 달성하기가 어려울 수 있습니다: Respondents further note that involvement of faculty and students is important to clarify expectations, take away uncertainty, and therewith create support for educational change activities. However, in practice, the objective to involve—and communicate with—the larger community can be difficult to meet:
계획 개발의 전체 기간 동안 우리는 계획을 실행해야 하는 사람들을 충분히 참여시키지 못했습니다. 이들에게 충분히 알리지 않았고, 갑자기 이런 일이 발생하니 압박감이 컸습니다. 반드시 필요한 일이었습니다. 사람들이 우리가 왜 이런 일을 하는지 충분히 알지 못했습니다. 이유가 무엇이었는지요. (FG6, F6) During the whole period of plan development, we insufficiently involved the people who eventually needed to implement it. We did not inform them sufficiently and what happens all of a sudden, the pressure was on. It needed to happen. Without people being fully aware of why we were doing this. What the reason was. (FG6, F6)
상향식 개선 접근 방식과 하향식 개선 접근 방식 사이의 균형이 자주 언급됩니다. 한편으로는 기본 틀과 (재)개발 구조를 제공하기 위해 조직 고위층에서 시작된 접근 방식이 필요하고, 다른 한편으로는 교수진과 학생들이 계획에 기여할 수 있는 능력이 중요합니다: The balance between bottom-up and top-down improvement approaches is often referred to. On the one hand, approaches initiated at a high level in the organization are needed to provide a basic framework and (re)development structure, while on the other hand, the ability of faculty and students to contribute to plans is important:
하향식도 상향식도 아닌, 모든 이해 당사자들과 협의하여 문제를 파악하고 그런 방식으로 합의에 도달할 수 있어야 한다는 것이죠. 적어도 그것이 철학입니다. 코디네이터나 교수가 커리큘럼을 설계하고 "이렇게 하세요."라는 식으로 실행하는 것이 아니라 말이죠. (FG5, S3) That it is neither a top-down nor a bottom-up implementation, but that we identify issues in consultation with all parties involved, and that a consensus can be reached that way. At least, that is the philosophy. Instead of a coordinator or professor designing a curriculum and implementing it like “here you go.” (FG5, S3)
구체적인 가치는 대표 기관에 귀속됩니다. 이러한 기구들은 새로운 아이디어를 발굴하고 모범 사례에 대한 통찰과 공유를 바탕으로 조언을 제공함으로써 개선에 기여합니다: Specific value is attributed to representative bodies. These bodies contribute to improvement by identifying new ideas and providing advice based on insights in—and sharing of—best practices:
저는 학생들이 교육 분야의 강점과 모범 사례를 잘 파악하고 있다고 생각합니다..... 제 생각에 학생[대표]으로서 우리가 해결해야 할 과제 중 하나는 이러한 품질 측면이 실제로 무엇인지 인식하고 "이것이 아이디어였고, 이것이 구현되는 방식이며, 품질을 개선하기 위해 주목해야 할 지점"을 고려하는 것입니다. (FG3, S1) I believe that students are very well equipped to map the strong aspects and best practices within education…. In my opinion, part of the challenge for us as students [representatives] is to be aware of what those quality aspects actually are … to consider “this was the idea, this is how it is implemented, and these are the points of attention to improve quality.” (FG3, S1)
응답자들은 이해관계자의 참여를 보장하기 위해 변화 리더에게 프로젝트 관리 및 커뮤니케이션 기술이 필요하다고 지적합니다. 의학교육 환경에서 이러한 기술에 대한 관심이 부족하기 때문에 참여가 부족한 것으로 나타났습니다. The respondents indicate that to safeguard stakeholder involvement, change leaders require project management and communication skills. A lack of attention for such skills in the medical education setting is expressed as reason for experiencing a shortfall of involvement.
교육과 학습의 가치 Valuing teaching and learning
교육을 개선하려는 교수진의 동기는 학생을 향한 (학문적, 직업적) 발전에 대한 헌신에서 비롯됩니다. 예를 들어, 교수진은 교육 활동 후 학생들과의 만남을 통해 동기 부여 효과를 얻을 수 있으며, 이 시간 동안 학생들은 특정 활동의 학습 효과에 대해 감사를 표합니다. 학생들에 따르면 교수진의 헌신은 여러 가지 방식으로 나타납니다(예: 가시성 및 접근성, 학생 질문에 대한 응답, 강의에 대한 열정). 헌신적인 교수진은 자기 성찰적인 태도를 취하는 경향이 더 강하고 피드백에 더 잘 반응하며, 이는 내부적인 개선 의지에서 비롯됩니다: The motivation of faculty to improve education stems, to an important degree, from commitment to the (academic and professional) development of students. Faculty, for example, point to the motivating effect of meeting with students after teaching activities, during which time students express appreciation for the learning effect of certain activities. According to students, faculty’s commitment manifests in several ways (e.g., through visibility and approachability, responsiveness to student questions, enthusiasm in lecturing). Committed faculty are more inclined to attain a self-reflective attitude and are more responsive to feedback, stemming from an internal drive to improve:
네, 우선은 개선하려는 교사의 의지가 중요하다고 생각합니다. 이것은 매우 다양한 개선 계획을 통해 얻을 수 있는 것이기도 합니다: 한 교사는 다른 교사보다 비판에 훨씬 더 개방적입니다. (FG2, S2) Yes, I believe for one thing, it involves the willingness of the teacher to improve. This is also what you get from many very different improvement plans: One teacher is far more open to criticism than the other. (FG2, S2)
교사와 학생 모두 의사 결정 과정에 참여하고 목표를 공유하는 것이 헌신에 기여한다고 보고합니다. 일반적으로 교육에 대한 관심과 인정은 교사의 가르침에 대한 동기를 부여합니다. 다음 교직원의 말은 교육보다 연구를 중시하는 것이 교육에 투자하려는 노력을 방해할 수 있음을 보여줍니다: Both teachers and students report that their participation in decision-making processes and shared goal formulation contribute to commitment. In general, attention to and appreciation of education fuel faculty’s motivation to teach. The following quote from a staff member illustrates that valuing research over education can hamper efforts to invest in education:
학과장은 교수진의 연구와 논문을 작성하는 것에 훨씬 더 많은 관심을 보입니다. 블렌디드 러닝을 구현하거나 새로운 학습 프로그램 청사진을 만들면 그것도 성과가 되지만, 부서장을 행복하게 하는 성과는 아닙니다. (FG5, F2) A head of department is far more interested in faculty members’ research and you producing manuscripts. That is something which pays off … if you implement blended learning or create a new study program blueprint … that’s also output, but it’s not the kind of output that makes the department head happier. (FG5, F2)
6개 기관의 응답자 모두 과도한 업무량이 교육에 전념하는 데 방해가 된다고 답했습니다. 이에 반해 상급 경영진의 교육에 대한 관심과 인정은 헌신을 자극합니다: Respondents from all 6 institutions report that excessive workload hinders the commitment to education. As a counterbalance, attention to—and appreciation of—education from upper management stimulates commitment:
교육에 대한 관심과 열의에 따라 교육의 질이 만들어지기도 하고 깨지기도 하는데, 교육은 하다 보면 좋아지기 시작하고 자동적으로 향상되기 때문입니다. 그래서 주로 시간과 관심, 주변 사람들의 관심이 중요하다고 생각합니다. 그래서 네, 교육 경력 경로와 연례 평가에서 상사의 관심... 그런 모든 종류의... 교육에 대한 조직 내 관심. (FG3, F2) The quality of education is made or broken by the attention to and enthusiasm for education, because if you do it, you will start to like it, and you will also automatically improve. So I think it mostly concerns time and attention and interest from other people. So yes, educational career paths and your superior’s attention during the annual appraisal … all that kind of … attention within the organization for education. (FG3, F2)
교수진은 헌신적인 교직원들이 동료 교사와의 대화나 비공식적으로 학생의 의견을 묻는 등 (표준 교육 평가 외에) 추가적인 피드백을 적극적으로 구한다고 설명합니다. 학생 대표들은 교수와 학생 간의 짧은 거리와 학생이 비공식적으로 피드백을 제공할 수 있는 기회가 이러한 측면에서 매우 중요하다고 덧붙였습니다. 참가자들은 교직원-학생 커뮤니티 구축을 통해 교수와 학습을 중시하는 것이 중요하며, 이는 대면 상호작용의 여지가 많은 소규모 단위의 교육을 통해 달성할 수 있다고 지적합니다. Faculty explain that committed staff members actively seek additional sources of feedback (other than the available standard educational evaluations), for instance, by sparring with peers and by informally asking for student opinions. The student representatives add that a short faculty–student distance and student opportunities to provide feedback informally are instrumental in this respect. Participants point to the importance of valuing teaching and learning through staff–student community building, which can be reached through teaching in smaller units with more room for face-to-face interaction, for example.
소유권과 책임 사이에서 탐색하기 Navigating between ownership and accountability
교수진에 따르면, 자신의 통찰력을 바탕으로 교수 학습 활동을 설계하면 주인의식을 고취하고 지속적으로 개선하려는 동기를 강화할 수 있다고 합니다. 교육 (재)개발을 (팀) 공동의 과제로 삼고 전문가적 자율성의 여지를 두면 팀이 헌신한다면 교육의 질에 영향을 미칩니다: According to faculty, designing teaching and learning activities based on their own insights stimulates ownership and reinforces their motivation to continuously improve. Making the (re)development of education a shared (team) task, with room for professional autonomy, affects educational quality, provided that the team is committed:
최고의 기획 그룹은 광범위한 토론이 이루어지고 토론을 피하지 않는 팀입니다..... 헌신과 함께한다는 느낌이 있어야 합니다. "우리는 무언가를 창조할 것이다." "우리는 무언가를 만들 것이다." 이것이 바로 퀄리티를 얻는 방법입니다. 때때로 관리 기관에서 정한 경계를 넘을 수도 있습니다. 하지만 그런 경우에도 그들은 어쨌든 당신에게 호루라기를 불 것입니다. (FG1, F4) The best planning groups are teams in which extensive discussions take place, and where discussion is not avoided…. There has to be commitment and a feeling of togetherness. “We are going to create something.” “We are going to build something.” That is how you get quality. Maybe you will sometimes cross the boundaries set by the management institute. But yes, in that case, they will blow the whistle on you anyway. (FG1, F4)
자율성과 주인의식은 동료 지원 및 책무성 절차(즉, 체계적인 평가 및 개선 접근 방식으로서의 PDCA 주기)와 연계되어야 합니다. 결과 평가보다 단기적인 학생 만족도와 과정에 중점을 두는 것은 교수진이 선호하는 학생의 종단적 발달에 초점을 맞추는 것과 모순됩니다. 또한 평가가 혁신과 연계되지 않거나 학습 효과를 포착하지 못할 수도 있습니다: Autonomy and ownership need to be linked with peer support and accountability procedures (i.e., the PDCA cycle as systematic evaluation and improvement approach). An emphasis on short-term student satisfaction and process over outcome evaluations contradicts faculty’s preferred focus on the longitudinal development of students. Moreover, evaluations might not be aligned to innovations or fail to capture learning effects:
목표에 도달했는지 훨씬 더 광범위하게 측정해야 하고, 그러면 다시 제 목표로 돌아와야 합니다.제 목표는 시험이 끝나거나 학기가 끝난 후 학생들이 행복해하는 모습을 보는 것이 아닙니다. 제 목표는 학생들이 훌륭한 의사가 되는 것을 보는 것입니다. 그것이 제 목표입니다. (FG6, F5) You need to measure to a much larger extent if you reached your goals, and then I come back to my goal again. My goal is not to see happy students after their exam or after the semester. My goal is to see them become a great doctor. That is my goal. (FG6, F5)
학생과 교수진은 피드백이 건설적인 것이 중요하다고 말합니다. 여기서 응답자들은 내러티브 피드백의 부가가치에 대해 구체적으로 언급합니다. 평가의 후속 조치에 대한 정보와 커뮤니케이션이 부족하면 피드백의 질이 떨어집니다. 평가의 목적과 후속 조치에 대한 추가 설명은 학생이 양질의 피드백을 제공할 가능성을 높일 수 있습니다. 또한 명확한 책임 구조를 포함시키는 것이 중요합니다: Students and faculty report that it is key for feedback to be constructive. Herein, respondents refer specifically to the added value of narrative feedback. A lack of information and communication on the follow-up of evaluations mitigates feedback quality. Further explanation of the purposes and follow-up of evaluations can enhance the likeliness of students’ provision of high-quality feedback. Moreover, embedding clear responsibility structures is key:
저희는 1년 넘게 무슨 일이 일어나고 있는지 알아내려고 노력해 왔습니다. "저 사람은 이렇게 하고, 저 사람은 저렇게 하고, 저 사람은 저렇게 피드백을 준다"라고 말할 수 있는 사람은 아무도 없습니다. 코스를 보면 개선하는 것이 번거롭고 몇 년이 걸립니다. 하지만 어떤 방식으로 구조화되어 있고 누가 무엇을 책임지는지 위에서부터 아래로 명확해야 한다고 생각합니다. (FG4, S1) We have been trying to find out what is going on for more than a year now. There is nobody who can tell us “that person does this, that one does that, and that one gives feedback,” etc. If you look at a course, it is cumbersome to improve and it will take years. But I think it should be clear from the top down that it is structured in a certain way and who is responsible for what. (FG4, S1)
복잡한 조직 구조와 많은 교직원이 조정 및 실행 역할에 관여하는 것은 평가 결과에 대한 후속 조치를 어렵게 하는 요인으로 꼽힙니다. Complex organizational structures and involvement of many faculty members in coordination and implementation roles are considered to frustrate the follow-up on evaluation results.
통합적 리더십 구축 Building on integrative leadership
도표 1은 통합적 리더십이 앞서 설명한 4가지 주제에 존재하는 긴장을 엮어내는 데 어떻게 기여하는지를 요약한 것입니다. 개방적 시스템 관점을 키우는 것과 관련하여 학생을 포함한 다학제적 팀을 구성하는 것이 중요한 것으로 간주됩니다. 이러한 팀을 구성하면 책임과 의사결정을 공유하고 다양한 관점을 포용할 수 있습니다:
Chart 1summarizes how integrative leadership contributes to intertwining the tensions present within the 4 themes described previously. With regard to fostering an open systems perspective, the formation of multidisciplinary teams (including students) is considered important. Such teams allow for shared responsibilities, decision making, and the inclusion of different perspectives:
작업을 수행해야 하는 그룹부터 시작해야 한다고 생각합니다. 그룹은 너무 크지 않고 가능한 한 이질적이어야 하며, 교육 조직 내 모든 구성원으로부터 해당 과제를 수행하도록 승인을 받아야 합니다. (FG3, S1) I think you should start with the group that has to perform the task. The group should not be too large, but as heterogeneous as possible … and it should get approval from everyone within the educational organization to perform that task. (FG3, S1)
리더는 중요한 (프로그램 또는 조직) 목표와 개별 교수진의 야망, 동기 부여 및 전문성 사이의 연결 고리를 자극해야 합니다. 팀이나 개별 교사에게 너무 많은 자유를 제공하면 커리큘럼의 일관성을 해칠 수 있습니다: Leaders ought to stimulate connective links between the overarching (program or organization) goals and individual faculty members’ ambitions, motivations, and specialties. Offering too much freedom to teams or individual teachers can endanger the curriculum coherence:
현재 많은 교사들이 [학습 프로그램 관리자가] 내용을 무시하고 자기 방식대로 교육을 개발하는 것을 볼 수 있습니다. 물론 좋은 의도로 하는 일이라는 점을 분명히 말씀드리지만, 그렇게 되면 모든 것이 뒤죽박죽이 되죠. (FG4, F2) What you see now is that when those people [the study program management] ignore the content, a lot of teachers develop education in their own way. Of course they do this with the best intentions, let me make that clear, but yeah, then everything becomes all jumbled. (FG4, F2)
팀이 자유롭게 운영할 수 있는 일반적인 프레임워크는 혁신을 위한 유연성과 효과와 효율성을 유지하기 위한 안정성 사이에서 균형을 잡는 데 도움이 됩니다: A general framework within which teams have freedom to operate helps to establish a balance between flexibility to innovate and stability to remain effective and efficient:
예, 의도된 목표에 따라 프레임워크가 결정되고, 결국 프레임워크에 따라 사람들에게 "여러분에게는 레버리지와 일정한 자유가 있지만, 주어진 프레임워크의 경계 내에서만 가능합니다."라고 말할 수 있습니다. (FG6, F5) Yes, the intended aims determine the framework and the framework in the end determines that you tell people, “You have leverage and a certain freedom, but within the boundaries of the provided framework.” (FG6, F5)
지지적인 커뮤니케이션 분위기를 조성하는 리더의 능력은 개선 이니셔티브의 성공을 결정하는 중요한 요소로 간주됩니다. 리더는 커뮤니케이션 프로세스를 통해 조직 변화의 비전에 대한 투명성을 높이고 참여를 촉진할 수 있습니다: Abilities of leaders to establish a supportive communication climate are considered important determinants of the success of improvement initiatives. Through communication processes, leaders can foster transparency on the vision behind organizational change and foster involvement:
좋은 비전일지라도 그 비전이 정확히 무엇을 수반하는지 알고 싶을 수 있습니다. 비전을 공유하면 오류가 발생할 여지가 있습니다. 그러면 적어도 지평선에 있는 점이 무엇인지 알 수 있습니다. 누군가 이메일을 보내는 것을 잊어버려도 "괜찮아. 우리가 무엇을 위해 노력하고 있는지 알아요. 왜 이런 일이 지금 일어나야 하는지 알아요."라고 생각할 수 있습니다. (FG2, F2) It could just happen to be a good vision, but then you would like to know what it entails exactly. If you share it, this vision, you have some room for errors. Then at least you know what the dot on the horizon is. It could happen that somebody forgets to send you an email, and you think, “It’s okay. I know what we are working towards. I know why this needs to happen now.” (FG2, F2)
EC 멤버들은 지원과 협력적인 교사 네트워크, 교육 커리어 트랙 구축, 교육에 대한 추가 시간 또는 보상 제공 등 리더가 교수와 학습의 가치를 증진하고 동기를 유발하는 다양한 사례를 제시합니다. 리더는 교육에 대한 인식과 건설적인 피드백 제공을 통해 소유권(및 자율성)과 책임(및 통제)의 균형을 맞추는 데 영향을 미칩니다. The EC members provide various examples of the way leaders promote valuing of teaching and learning and trigger motivation: through support and collaborative teacher networks, establishing education career tracks, and offering additional time or reimbursement for teaching. Leaders affect the balance of ownership (and autonomy) with accountability (and control) through appreciation of education and the provision of constructive feedback.
토론 Discussion
이 연구에서 우리는 의학교육에서 CQI 문화를 형성하는 5가지 주제를 확인했습니다. 차트 1에서 볼 수 있듯이, 조직 내에는 교육의 질을 유지하고 발전시키기 위한 방향성 사이에 다양한 긴장이 존재합니다. 이러한 경쟁적 지향점 간의 통합과 시너지 창출을 위해서는 다학제적 협업, 개방적 의사소통, 교수진 개발 및 인적 자원에 대한 투자, 품질 관리보다 품질 향상에 초점을 맞춘 책임 절차가 강화되어야 합니다. In this study, we identified 5 themes that in concert shape a culture for CQI in medical education. AsChart 1illustrates, various tensions within organizations exist between orientations to maintain and further develop the quality of education. The integration and creation of a synergy between these competing orientations call for increased multidisciplinary collaboration, open communication, investments in faculty development and human resources, and accountability procedures focusing on quality enhancement over quality control.
개방형 시스템 관점(주제 1)은 지식 공유 강화와 창의성 및 혁신의 자극을 통해 질적 발전을 촉진하는 데 도움이 됩니다. 이러한 관점을 취하면 학교가 점진적 단일 루프 학습과 유사한 CQI 노력에 전념하는 것에서 진정한 학습 조직(수정된 목표, 의사결정 규칙 또는 양쪽 모두의 이중 루프 학습과 유사한)으로 전환하는 데 도움이 됩니다.30 CQI 문화를 촉진하려면 의과대학의 현재 가치관을 변화시킬 필요가 분명합니다. 교수진은 일반적으로 유연하고 인간 중심적인 조직을 선호하지만,31,32 의과대학은 여전히 보수적이고, 위계적이며, 단절되고, 인본주의적 성향을 저해하는 것으로 인식되는 경우가 많습니다.22,33-35 An open systems perspective (Theme 1) aids in promoting quality development through intensified knowledge sharing and the stimulation of creativity and innovation. Taking such a perspective aids schools in their shift from devoting to CQI efforts (resembling incremental, single-loop learning) to becoming true learning organizations (resembling modified goals, decision-making rules, or both—double-loop learning).30To stimulate a culture for CQI, a need for change in current values of medical schools is apparent. Whereas faculty typically prefer a flexible and human centered organization,31,32medical schools are still often seen as conservative, hierarchical, disconnected, and discouraging humanistic orientations.22,33–35
광범위한 이해관계자의 참여(주제 2)는 지식, 기술 및 (잠재적으로 경쟁적인) 가치의 다양성이 교육의 질에 대한 다면적인 개념을 다루는 데 도움이 되므로 CQI의 핵심입니다.36 그러나 의료 전문가와 학계는 (임상 서비스 활동, 부서, 학문 분야 등과 관련된) 사일로 내에서 일하고 학습하는 데 익숙하며, 이는 고유한 태도, 문제 해결 능력 및 공통 언어 사용을 강화합니다.37 또한 의사와 연구자는 일반적으로 상당한 자율성을 가지고 있습니다. 이들은 개별적인 책임을 지는 데 익숙하고 자신의 학문 분야의 이익을 옹호하는 데 열심입니다.37 다양한 배경을 가진 교수진이 참여하는 철저한 토론과 공동 창작 세션은 집단적 개선 활동을 시작하는 데 핵심적인 역할을 합니다.38 또한 CQI는 학생을 고객 또는 소비자에서 조직 문화의 적극적인 구성원 및 기여자로의 역할 변화를 수반합니다. Broad stakeholder involvement (Theme 2) is key to CQI, as diversity in knowledge, skills, and (potentially competing) values helps to address the multifaceted notion of education quality.36However, medical professionals and academics are used to working and learning within silos (relating to their clinical service activities, departments, disciplines, etc.), which reinforce distinct attitudes, problem-solving skills, and the use of a common language.37Moreover, physicians and researchers typically have a large degree of autonomy. They are used to taking individual responsibility and are keen to defend interests of their own discipline.37Thorough discussions and cocreation sessions involving faculty from different backgrounds form a keystone to initiate collective improvement activities.38Additionally, CQI entails a role change from students as clients or consumers to active members of and contributors to the organizational culture.
인센티브와 교수진의 요구 만족도에 대한 연구와 함께,39,40 우리는 CQI의 외재적 동기에 대한 몇 가지 예시를 발견했습니다. 자금 지원, 개발 시간, 정보 공유, 교수진 개발 이니셔티브 증가를 통한 교육 및 학습의 가치인정(주제 3)은 조직의 개선 잠재력에 영향을 미칩니다.41,42 따라서 조치를 취하는 데 필요한 자원이 부족하다면 단순히 주인의식과 책임감을 고취하는 것(주제 4)은 유익한 결과로 이어지지 않을 것입니다. In line with research on incentives and faculty needs satisfaction,39,40we found several illustrations of extrinsic motivators for CQI. The valuing of teaching and learning (Theme 3) through increased funding, time for development, information sharing, and faculty development initiatives influence the organization’s improvement potential.41,42Hence, a mere promotion of ownership and accountability (Theme 4) will not lead to beneficial results if required resources to take action are lacking.
우리의 연구 결과는 통합적 리더십(주제 5)이 양질의 문화 발전을 지원한다는 것을 보여줍니다. 의학교육의 리더십은 개별 교수진의 감독, 지도, 지원에서 더 넓은 집단에 초점을 맞추는 것으로 변화하고 있습니다. 리더는 강력한 리더십에 CQI의 책임을 돌리는 대신 동기부여자, 멘토, 촉진자 역할을 해야 합니다. 지식 집약적인 의과대학 환경에서 리더와 직원들은 조직의 문제에 대한 의미와 해결책을 재구성합니다.43 의학교육의 CQI는 다양한 스타일을 결합할 수 있고 다양한 이해관계자의 목표와 야망을 통합할 수 있는 리더가 가장 잘 수행할 수 있습니다.44 Our findings indicate that integrative leadership (Theme 5) supports further quality culture development. Leadership in medical education is changing from individual faculty supervision, guidance, and support to a focus on the broader collective. Instead of attributing responsibility for CQI to strong leadership, leaders are expected to be motivators, mentors, and facilitators. In the knowledge-intensive setting of medical schools, leaders and employees coconstruct meaning and solutions to organizational issues.43CQI of medical education is best served with leaders who are able to combine multiple styles and who are able to coalesce different stakeholder goals and ambitions.44
실천 커뮤니티(CoP)45를 구현하면 지속적인 개선을 위한 문화 주제를 다룰 수 있는 기회의 창이 열립니다. CoP는 다양한 학문적 배경을 가진 교사들 간의 상호작용을 촉진하고 새로운 관점을 얻을 수 있는 기회를 창출합니다. 또한 이러한 커뮤니티 내에서 조직된 (연수) 활동은 참여 의식을 강화하고 역량, 자신감, 신뢰성, 유대감을 향상시킵니다.46 CoP는 교수 학습, 개인 개발, 교사 정체성 확립을 중시하는 환경을 형성합니다. 교육 및 학습 커뮤니티의 건설적인 동료 피드백 프로세스는 교육 개선에 대한 주인의식과 책임감의 균형을 맞추는 데 도움이 됩니다. CoP의 개방적이고 종적인 성격은 그 부가가치에 필수적이며, 단순히 우수한 챔피언들의 일시적인 리그를 구축하는 것을 넘어서야 한다는 점에 유의해야 합니다. The implementation of communities of practice (CoPs)45opens a window of opportunity to address the themes of a culture for continuous improvement. CoPs facilitate interaction between teachers from diverse disciplinary backgrounds and create opportunities to gain new perspectives. Moreover, (training) activities organized within these communities strengthen a sense of involvement and enhance competence, confidence, credibility, and connection.46CoPs form an environment in which the valuing of teaching and learning, personal development, and teacher identity building is central. Constructive peer feedback processes in teaching and learning communities help to balance ownership and accountability for educational improvement. It should be noted that an open and longitudinal character of CoPs is essential to their added value; they should go beyond the mere establishment of a temporal league of quality champions.
이론적 및 실무적 의의 Theoretical and practical significance
본 연구는 표준 품질 관리 접근 방식이 품질 문화 개념에서 도출된 통찰력으로 보완되어야 한다는 교수진과 학생들의 의견을 대변합니다. 보고된 결과는 이 이론적 개념에 대한 더 깊은 통찰력을 얻는 데 기여했습니다. 우리의 연구 결과는 책무성을 강조하는 정적인 접근 방식에서 전문가의 자율성과 커뮤니티 구축의 여지가 있는 유연한 접근 방식으로의 전환을 시사합니다. CQI는 교육의 가치, 교수진의 동기 부여, 학생의 개인적, 학업적, 전문적 개발에 더욱 집중할 것을 요구합니다. The present study gives voice to the opinion of faculty and students that standard quality management approaches should be complemented by insights derived from the quality culture concept. The reported results have contributed to gaining a deeper insight into this theoretical notion. Our findings imply a shift from static approaches emphasizing accountability toward flexible approaches with room for professional autonomy and community building. CQI requires a stronger focus on the valuing of teaching; faculty motivation; and student personal, academic, and professional development.
강점과 한계 Strengths and limitations
이 연구는 질적 문화를 경험적으로 연구한 몇 안 되는 연구 중 하나이기 때문에 이용 가능한 문헌에 기여합니다. 여러 기관에서 데이터를 수집하고 교수진과 학생의 관점을 모두 고려했습니다. 연구 결과에 따르면 의과대학 내 가치 지향성이 품질 관리 접근 방식과 교수진의 업무 관련 심리적 태도가 상호 작용하는 방식을 설명하는 데 매우 관련이 있는 것으로 나타났습니다. 참여 의과대학에서는 이러한 지향점이 다소 동질적이었지만, 다른 상황에서는 다를 수 있습니다. 네덜란드 의과대학(8개 중 6개)만 조사 대상에 포함되었다는 점도 결과의 해석과 적용 가능성에 있어 고려해야 할 사항입니다. 또 다른 한계는 EC 위원들의 견해가 다른 중요한 이해관계자들과 다를 수 있다는 점입니다. 그러나 EC는 일반적으로 조직 중간 수준에서 운영되기 때문에 경영진과 풀뿌리 관점을 모두 파악했다고 가정합니다. 세 번째 (잠재적) 한계는 응답자들이 익명성이 보장되었음에도 불구하고 다른 대학에 소속된 연구자들과 특정 경험을 공유하는 것을 꺼렸을 수 있다는 점입니다. This study contributes to the available literature as it is one of few studies that research quality culture empirically. We gathered data from multiple institutions and took into account both faculty and student perspectives. The findings suggest that value orientations within medical schools are highly relevant in explaining how quality management approaches and work-related psychological attitudes of faculty interact. Whereas these orientations were rather homogeneous in the participating medical schools, they might vary in other contexts. The fact that we included only medical schools from the Netherlands (6 of 8) should be taken into account in the interpretation and transferability of results. A further limitation is that views of EC members might differ from other important stakeholders. However, as ECs typically operate on the organizational mesolevel, we assume to have captured both management and grassroots perspectives. A third (potential) limitation is that the respondents, despite guaranteed anonymity, might have been reluctant to share particular experiences with researchers affiliated with another university.
향후 연구를 위한 제언 Recommendations for future research
CQI의 새로운 길을 개척하기 위해서는 개별적인 교육 개선 접근 방식을 집단적인 노력으로 전환하는 개입에 대한 향후 연구가 특히 유용할 것입니다. 또한 이 연구에서 확인된 5가지 주제와 관련된 모범 사례에 대한 사례 연구는 CQI를 위한 조직의 변화와 개발을 시작하는 데 지렛대가 될 것입니다. To pave new paths for CQI, future research on interventions that convert individual educational improvement approaches to collective endeavors would be particularly valuable. In addition, case studies on best practices relating to the 5 themes identified in this study would provide levers to initiate organizational change and development for CQI.
결론 Conclusions
의과대학의 3대 사명인 교육, 연구, 임상 서비스 중 교육은 전통이 지배적이기 때문에 질적 개선과 변화가 필요하다는 인식이 가장 느린 경우가 많습니다. 의과대학에서 양질의 문화를 육성하기 위한 노력은 이러한 현 상황을 타개하는 데 도움이 될 것입니다.
Of a medical school’s 3 missions—education, research, and clinical services—education is often the slowest to recognize that quality improvement and change are necessary, with traditions being dominant. Efforts to nurture the quality cultures in medical schools will help to unfreeze this status quo.
1G.W.G. Bendermacher is educational policy advisor, Institute for Education, and a PhD candidate, School of Health Professions Education, Faculty of Health, Medicine and Life Sciences, Maastricht University, the Netherlands; ORCID: https://orcid.org/0000-0002-7804-4594.
2W.S. De Grave is an educational psychologist, School of Health Professions Education, Faculty of Health, Medicine and Life Sciences, Maastricht University, the Netherlands.
3I.H.A.P. Wolfhagen is associate professor, Department of Educational Development and Research, and deputy director, Institute for Education, School of Health Professions Education, Faculty of Health, Medicine and Life Sciences, Maastricht University, the Netherlands.
4D.H.J.M. Dolmans is professor of innovative learning arrangements, Department of Educational Research and Development, School of Health Professions Education, Faculty of Health, Medicine and Life Sciences, Maastricht University, the Netherlands; ORCID: https://orcid.org/0000-0002-4802-1156.
5M.G.A. oude Egbrink is professor of implementation of educational innovations, Department of Physiology, and scientific director, Institute for Education, School of Health Professions Education, Faculty of Health, Medicine and Life Sciences, Maastricht University, the Netherlands; ORCID: https://orcid.org/0000-0002-5530-6598.
Purpose:This study sought to identify key features of an organizational quality culture and explore how these features contribute to continuous quality improvement of undergraduate medical education.
Method:Between July and December 2018, researchers from Maastricht University in the Netherlands conducted a multicenter focus group study among 6 education quality advisory committees. Participants were 22 faculty and 18 student representatives affiliated with 6 medical schools in the Netherlands. The group interviews focused on quality culture characteristics in relation to optimizing educational development, implementation, evaluation, and (further) improvement. Template analysis, a stepwise type of thematic analysis, was applied to analyze the data.
Results:Five main themes resembling quality culture constituents to continuous educational improvement were identified: (1) fostering an open systems perspective, (2) involving stakeholders in educational (re)design, (3) valuing teaching and learning, (4) navigating between ownership and accountability, and (5) building on integrative leadership to overcome tensions inherent in the first 4 themes. A supportive communication climate (which can be fueled by the organization's leaders) contributes to and is integrated within the first 4 themes.
Conclusions:The results call for a shift away from static quality management approaches with an emphasis on control and accountability toward more flexible, development-oriented approaches focusing on the 5 themes of a culture for continuous quality improvement. The study provides new insights in the link between theory and practice of continuous quality improvement. Specifically, in addition to quality management systems and structures, faculty's professional autonomy, collaboration with peers and students, and the valuing of teaching and learning need to be amplified.
역량중심의학교육 도입: 앞으로 나아가기(Med Teach, 2017) Implementing competency-based medical education: Moving forward Jason R. Franka,b, Linda Snella,c, Robert Englanderd and Eric S. Holmboee; on behalf of the ICBME Collaborators
배경 Background
큰 혁신은 갑자기 가능한 것이 절실히 필요한 것과 만날 때 일어납니다. Big breakthroughs happen when what is suddenly possible meets what is desperately necessary.
2010년 Medical Teacher 특별호에서 국제 CBME 협력자들은 역량 기반 의학교육(CBME)을 "의학교육 프로그램의 설계, 실행, 평가 및 평가에 대한 성과 기반 접근법으로, 역량에 대한 조직화된 프레임워크를 사용"하며(Frank 외. 2010b, 641쪽) "근본적으로 졸업생의 성과 능력을 지향하고 사회 및 환자 요구 분석에서 도출된 역량을 중심으로 구성된 의사 실습 준비에 대한 접근법"으로 정의했습니다. 이는 시간 기반 교육을 강조하지 않고 더 큰 책임감, 유연성, 학습자 중심성을 약속합니다."(Frank 외, 2010a, 636쪽). In a special issue ofMedical Teacherin 2010, competency-based medical education (CBME) was defined by the International CBME Collaborators as “[a]n outcomes-based approach to the design, implementation, assessment, and evaluation of medical education programs, using an organizing framework of competencies” (Frank et al.2010b, p. 641) and as “an approach to preparing physicians for practice that is fundamentally oriented to graduate outcome abilities and organized around competencies derived from an analysis of societal and patient needs. It de-emphasizes time-based training and promises greater accountability, flexibility, and learner-centredness” (Frank et al.2010a, p. 636).
2009년에 결성되어 여러 의학교육 기관의 후원을 받는 국제 CBME 협력체는 차세대 의료 전문가를 준비시키기 위한 역량 기반 접근법을 탐구, 개발 및 향상시키는 데 관심이 있는 회원들이 모인 학술 네트워크입니다. CBME는 현대 의학 커리큘럼 설계 모델에서 발생하는 특정 과제와 단점을 해결할 수 있는 유망한 수단으로 인정받고 있습니다. 보다 구체적으로, CBME 모델의 개발은 다음에 대한 대응입니다. Formed in 2009 and sponsored by several medical education organizations, the International CBME Collaborators are a scholarly network whose members are interested in exploring, developing, and enhancing competency-based approaches to preparing the next generation of health professionals. CBME is recognized as a promising means of addressing certain challenges and shortcomings attributed to contemporary models of medical curriculum design. More specifically, the development of the CBME model is a response to
환자, 인구, 의료 전문직 교육 프로그램과 관련된 결과에 더 큰 책임을 지고 더 집중해야 한다는 요구(Frenk 외. 2010);
의학 교육 후 졸업생 능력의 용납할 수 없는 변동성을 줄여야 할 필요성(Langdale 외. 2003; Raymond 외. 2011);
일부 졸업생이 안전하고 효과적인 진료를 할 준비가 되어 있지 않다는 증거;
의료 시스템에서 최선이 아닌 아닌 환자 치료 결과의 패턴(예: IOM 2000, 2001; OECD 2000-2015a, 2000-2015b, 2000-2015c);
21세기 실무와의 관련성을 보장하기 위해 커리큘럼 내용을 근본적으로 재검토할 것을 요구합니다. 여기에는 전문 의료 지식을 넘어 의사소통, 협업, 전문성 및 전문적 정체성 형성, 시스템적 사고, 평생 학습, 인구 건강, 지속적 개선에 대한 역량을 포함하도록 교육의 바람직한 성과에 대한 확장된 비전이 포함됩니다;
교육에 소요된 시간이 역량의 대리 지표가 되는 교육 모델은 더 이상 바람직하지도 방어할 수도 없다는 우려.
calls for greater accountability and a greater focus on outcomes relating to patients, populations, and health professions education programs (Frenk et al.2010);
the need to reduce unacceptable variability in graduate abilities after medical training (Langdale et al.2003; Raymond et al.2011);
evidence that some graduates are not prepared for safe and effective practice;
patterns of suboptimal patient outcomes in health care systems (e.g. IOM2000,2001; OECD 2000–2015a, 2000–2015b, 2000–2015c);
calls for a fundamental re-examination of curriculum content to ensure relevance to the twenty-first century practice. This includes an expanded vision of the desired outcomes of training, such that they go beyond expert medical knowledge to include competencies in communication, collaboration, professionalism and professional identity formation, systems thinking, lifelong learning, population heath, and continuous improvement;
concerns that models of education in which time spent in training is a surrogate marker of competence are no longer desirable or defensible.
CBME의 진화 The evolution of CBME
CBME는 2009년에 시작된 것이 아닙니다. 그 역사는 ten Cate(2014)에 의해 기술되었으며, 획기적인 발전은 표 1에 요약되어 있습니다. 미국에서 역량 기반 교육에 대한 아이디어는 거의 한 세기 전에 특정 성과와 행동에 초점을 맞춘 산업 및 비즈니스 모델에서 처음 등장했습니다. 1960년대에는 보다 관련성 있고 성과에 초점을 맞춘 교육에 대한 요구에 따라 교사 교육에 역량 기반 교육 훈련이 도입되었습니다(Houston 1973; Burke 1999). CBME did not begin in 2009. Its history has been described by ten Cate (2014), and landmark developments are summarized inTable 1. In the United States, the idea of competency-based training first surfaced almost a century ago within industrial and business models that focused on specific outcomes and behaviors. In the 1960s, competency-based education training was introduced in teacher education in response to demands for more relevant and outcomes-focused training (Houston1973; Burke1999).
20세기 내내 보건 전문직 교육자들은 커리큘럼 개발에서 수많은 잠정적인 혁신을 고려했습니다.
1978년, 세계보건기구를 위한 비전 보고서에서 맥개히 등은 보건 전문직 교육이 지역 및 지역 인구 보건 요구를 진정으로 충족할 수 있도록 전 세계적으로 CBME를 채택할 것을 촉구했습니다.
사실, 60년 이상 동안 역량 기반 교육은 여러 관할 구역과 사회복지(Menefee & Thompson 1994), 카이로프랙틱 의학(Wangler 2009), 약학(Marshall 외. 1997) 등 여러 직종에서 교육 접근법으로 사용되거나 제안되어 왔습니다.
1990년대에 많은 관할권에서 역량 프레임워크를 교육 및 훈련의 핵심 요소로 사용하는 '결과 지향적 접근법'이 등장했습니다.
오늘날 가장 널리 알려진 세 가지 역량 기반 프레임워크는 영국의 굿 메디컬 프랙티스 표준(General Medical Council 2013), 미국의 의학전문대학원 교육 인증 위원회의 아웃컴 프로젝트(Swing 2007), 캐나다 왕립 의사 및 외과의사 대학의 CanMEDS 역량 프레임워크(Frank 외. 2015)입니다.
2010년, 메디컬 티처는 이 새로운 역량 기반 패러다임을 문서화, 정교화, 개발 및 보급하는 데 전념하는 국제 CBME 협력자들이 널리 인용된 일련의 논문을 발표했습니다(Campbell 외 2010; Dath 외 2010; Frank 외 2010a, 2010b; Harris 외 2010; Holmboe 외 2010; Iobst 외 2010; Snell & Frank 2010; Swing 외 2010; Taber 외 2010; ten Cate 외 2010).
Throughout the twentieth century, health professions educators considered numerous tentative innovations in curriculum development.
In 1978, in a visionary report for the World Health Organization, McGaghie et al. called for the worldwide adoption of CBME to ensure that health professions education could truly meet local and regional population health needs.
In fact, for more than 60 years competency-based education has been used, or suggested, as an approach to education in multiple jurisdictions and across multiple professions, including social work (Menefee & Thompson1994), chiropractic medicine (Wangler2009), and pharmacy (Marshall et al.1997).
In the 1990s, many jurisdictions witnessed the emergence of “outcomes-oriented approaches” that used competency frameworks as a key component of education and training.
Today, the three most widely known competency-based frameworks are the Good Medical Practice standard in the United Kingdom (General Medical Council2013), the Outcomes Project of the Accreditation Council for Graduate Medical Education in the United States (Swing2007), and the CanMEDS Competency Framework of the Royal College of Physicians and Surgeons of Canada (Frank et al.2015).
In 2010,Medical Teacherpublished a series of widely cited papers from the International CBME Collaborators dedicated to documenting, elaborating, developing and disseminating this emerging competency-based paradigm (Campbell et al.2010; Dath et al.2010; Frank et al.2010a,2010b; Harris et al.2010; Holmboe et al.2010; Iobst et al.2010; Snell & Frank2010; Swing et al.2010; Taber et al.2010; ten Cate et al.2010).
시리즈 II Series II
CBME는 관련자들이 이 접근법의 이론, 원리 및 실습에 대해 배우고 경험을 쌓으면서 흥미로운 방식으로 계속 발전하고 있습니다. 지난 10년 동안 CBME와 전 세계 교육자 네트워크는 비약적으로 성장했으며, 이번 메디컬 티처에서는 CBME의 개념과 논쟁뿐만 아니라 CBME의 실행에 초점을 맞춘 두 번째 논문 시리즈를 제공하게 되어 기쁘게 생각합니다. 국제 CBME 협력자들은 2013년과 2016년에 추가로 서밋을 개최했습니다. 참가자들의 관심 주제와 이슈는 델파이 프로세스를 통해 우선순위를 정했고(표 2 참조), 그 결과 논의된 내용을 이 시리즈 논문으로 정리했습니다. CBME continues to evolve in exciting ways as those involved learn and gain experience in the theories, principles, and practices of this approach. Both CBME and our global network of educators have grown dramatically in the last decade, and in this issue ofMedical Teacher, we are pleased to offer a second series of papers focused not just on CBME concepts and controversies, but also on the implementation of CBME. The International CBME Collaborators held further summits in 2013 and 2016. Topics and issues of interest to the participants were prioritized using a Delphi process (seeTable 2), and the resulting discussions were distilled into this series of articles.
입문 논문에서 홀름보에와 동료들은 주요 국제 운동으로서 CBME의 성장에 대해 논의하고 이 모델에 대해 제기된 몇 가지 비판을 다룹니다(홀름보에 외. 2017). 잉글랜드와 공동 저자들은 한 걸음 더 나아가 의학교육자들이 의학교육의 이러한 적응적 변화에 필요한 공유 언어를 향해 나아감에 따라 공통의 정의를 개발하고 특정 핵심 개념 간의 관계를 파악하기 위한 국제 CBME 협력자들의 노력을 제시합니다(잉글랜드 외 2017). In an introductory paper, Holmboe and colleagues discuss the growth of CBME as a major international movement and address some of the criticisms that have been leveled against the model (Holmboe et al.2017). Englander and coauthors take a further step, presenting the efforts of the International CBME Collaborators to develop common definitions and to identify the relationships between certain core concepts, as medical educators move toward a shared language necessary for this adaptive change in medical education (Englander et al.2017).
실행은 많은 사람들에게 현재 문제이기 때문에, CBME를 실행하는 데 있어 가장 중요한 과제는 Caverzagie 외. (2017)에서 논의합니다. (2017)은 CBME로의 전환을 지원하는 데 필요한 구조적 변화를 탐구함으로써 구현 주제를 이어갑니다. 퍼거슨 외(2017)는 의료 전문가 교육을 둘러싼 직업적, 제도적, 조직적 문화에 필요한 변화를 더 깊이 파고듭니다. 이들은 현재 의학교육 문화에서 CBME의 수용을 가로막는 주요 장벽을 파악하고 이를 해결하기 위한 방법을 제안합니다. Because implementation is a current issue for many, overarching challenges to implementing CBME are discussed by Caverzagie et al. (2017). Nousiainen et al. (2017) continue the implementation theme by exploring the structural changes needed to support the transition to CBME. Ferguson et al. (2017) delve deeper to consider changes needed in the professional, institutional, and organizational cultures surrounding the training of medical professionals. They identify key barriers to the acceptance of CBME within the current culture of medical education and propose ways to address them.
평가는 원칙과 실무의 관점에서 여전히 어려운 과제로 남아 있습니다. Harris 등(2017)은 CBME 평가의 최근 발전을 살펴보고, 2013년 CBME에 관한 초청 서밋에서 논의된 평가와 관련된 주요 이슈를 설명합니다. CBME 평가의 핵심 원칙은 Lockyer 외(2017b)에 의해 설명되어 있으며, 이들은 평가 프로그램의 효과를 보장하는 방법도 검토합니다. Assessment remains a challenge from the perspective of principles and practice. Harris et al. (2017) explore recent developments in CBME assessment, describing key issues regarding assessment as discussed at the 2013 invitational summit on CBME. Core principles of assessment in CBME are described by Lockyer et al. (2017b), who also examine ways to ensure the effectiveness of assessment programs.
협력자들은 미래를 내다보기도 했습니다. Lockyer 외(2017a)는 CBME의 원칙이 아직까지 지속적 전문성 개발(CPD)에 널리 채택되지는 않았지만, 레지던트 이후에도 대학원 수련 기간만큼이나 중요하며, 개업의가 경력 전반에 걸쳐 역량을 유지할 수 있도록 CPD 접근 방식에 상당한 변화가 필요하다고 제안합니다. 이 논문에서는 CPD 개혁의 근거를 살펴보고, CBME-CPD 프레임워크로의 전환을 촉진하는 핵심 요소와 직장 내 역량 및 성과 평가를 위한 확장된 역할을 고려하며, CBME 환경에서 CPD를 지원하기 위한 교육 활동을 제안하고, 다양한 이해관계자에 대한 시사점을 강조합니다. 마지막으로, 그루펜 외(2017)는 CBME의 맥락에서 연구가 필요한 다양한 이론적, 실제적 질문을 제시합니다. 저자들은 CBME 실행의 결과와 모범 사례에 대한 증거를 수집하는 데 있어 해결해야 할 방법론적 문제를 추가로 탐구합니다. The Collaborators also looked to the future. Although the principles of CBME have yet to be widely adopted in continuing professional development (CPD), Lockyer et al. (2017a) suggest that they are just as important after residency as they are during postgraduate training, and that significant changes are needed in the approach to CPD to ensure that practicing physicians maintain competence throughout their careers. Their paper explores the rationale for CPD reform; considers the key elements that would facilitate a transition to a CBME–CPD framework and an expanded role for the assessment of competence and performance in the workplace; suggests educational activities to support CPD in a CBME environment; and highlights the implications for different stakeholders. Finally, Gruppen et al. (2017) present a range of questions, both theoretical and practical, that require research in the context of CBME. The authors further explore methodological issues that will need to be addressed in gathering evidence about outcomes and best practices in implementing CBME.
가장 최근에 열린 두 차례의 국제 CBME 협력자 서밋을 통해 다른 저널에 게재된 논문이 추가로 발표되었습니다. 카라치오 외(2016)가 작성한 임상의사-교육자를 위한 헌장에는 의학교육이 사회의 필요에 기반해야 하고, 구조나 과정이 아닌 결과에 초점을 맞춰야 하며, 초기 의대생부터 시니어 개원의까지 전 과정에 걸쳐 원활하게 이루어져야 한다는 CBME의 세 가지 기본 원칙이 명시되어 있습니다. 그런 다음 헌장은 효과적인 실행을 보장하기 위해 9가지 약속을 제안합니다. 위탁 의사 결정에 관한 논문에서 ten Cate 등(2016)은 임상 수련에서 위임 의사 결정을 내리는 과정을 설명하고, 다양한 신뢰 방식을 개괄하며, 위탁으로 이어지는 요인에 대해 논의합니다. 이 논문은 CBME에서 이루어지는 평가 결정의 토대를 마련합니다. Van Melle 등(2016)은 CBME 프로그램을 평가하고 그 영향을 이해하기 위한 엄격한 접근법으로 기여도 분석을 사용할 것을 제안합니다. The two most recent summits of the International CBME Collaborators resulted in additional papers that have been published in other journals. A charter for clinician–educators framed by Carraccio et al. (2016) outlines three basic tenets of CBME: medical education must be based on the needs of society; it must focus on outcomes, not structure or process; and it must be seamless across the continuum from early medical student to senior practitioner. The Charter then proposes nine commitments to ensure that implementation is effective. In a paper on entrustment decision-making, ten Cate et al. (2016) describe the process of making entrustment decisions in clinical training, outline varied modes of trust, and discuss the factors that lead to entrustment. This paper lays a foundation for the assessment decisions made in CBME. Van Melle et al. (2016) propose using contribution analysis as a rigorous approach to evaluate CBME programs and understand its impact.
가까운 미래 The near future
역량 기반의 성과 중심 교육은 현재 여러 관할권에서 시행되고 있습니다. 이는 일련의 열망, 혁신, 개념, 실험에서 수많은 보건 전문직 교육 기관의 체계적이고 지지받는 방향으로 변모했습니다. 많은 일이 있었지만 아직 해야 할 일이 많이 남아 있습니다. 도전과제는 여전히 남아 있고 자원은 무한하지 않지만, 의학교육 및 수련 시스템을 개선할 수 있는 기회가 존재하며, 역량 기반 프레임워크로의 전환은 미래 의사들의 더 나은 교육을 통해 개별 환자와 사회의 건강에 상당한 긍정적 영향을 미칠 것이라고 확신합니다. 시간만을 기준으로 한 수련은 이제 끝날 때가 되었습니다.
Competency-based, outcomes-focused education is now implemented in a number of jurisdictions. It has been transformed from a set of aspirations, innovations, concepts, and experiments into the systematic and espoused directions of numerous institutions of health professions education. Although much has happened, much remains to be done. Challenges remain, and resources are not limitless, but we are certain the opportunities for improvement in our medical education and training systems exist, and that the move to a competency-based framework will have a significant positive impact on the health of individual patients and society through the better education of future physicians. The end of training based only on time is now … and it is about time.
Med Teach. 2017 Jun;39(6):568-573.doi: 10.1080/0142159X.2017.1315069.
Implementing competency-based medical education: Moving forward
For more than 60 years, competency-based education has been proposed as an approach to education in many disciplines. In medical education, interest in CBME has grown dramatically in the last decade. This editorial introduces a series of papers that resulted from summits held in 2013 and 2016 by the International CBME Collaborators, a scholarly network whose members are interested in developing competency-based approaches to preparing the next generation of health professionals. An overview of the papers is given, as well as a summary of landmarks in the conceptual evolution and implementation of CBME. This series follows on a first collection of papers published by the International CBME Collaborators in Medical Teacher in 2010.
적응적 의과대학 교육과정: 지속적 개선을 위한 모델(Med Teach, 2018) The adaptive medical curriculum: A model for continuous improvement Mark Quirk and Heidi Chumley
배경 Background
교실에 코끼리가 있는데도 아무도 알아채지 못합니다. 의과대학에서 강의 출석 정책을 완화하자 학생들은 다른 방법으로 학습하는 것이 더 효과적이라는 것을 알게 되었습니다. 학생들은 강의실을 찾지 않게 되었습니다(Prober and Heath 2012; Groen 외. 2016). 일부 교수들은 출석률이 시험 성적과 관련이 없다는 증거가 늘어나고 있음에도 불구하고 학생들이 실제로 출석하지 않으면 학습에 지장을 받을 것이라고 우려하고 위협을 느낍니다(Deane and Murphy 2013, Paul 외. 2015, Meyer 외. 2016). 오늘날의 학생들은 적응력이 뛰어난 성인 학습자로서 자신의 필요를 가장 잘 해결할 수 있는 리소스를 찾습니다. 오늘날의 교수는 적응형 교사로, 교실 안팎에서 학생의 다양한 요구를 가장 잘 충족할 수 있는 리소스를 제공하고자 노력합니다. 학생이나 교수 모두 학생에게 필요한 것이 무엇인지 정확히 알지 못합니다. 개별 학생에게 필요한 것은 적응형 커리큘럼에서 협력적인 참여를 통해 정확히 발견됩니다.
There is an elephant in the classroom and barely a soul there to notice. As medical schools loosened lecture attendance policies, students explored learning in other ways and found them to be more effective. They stopped coming to lectures (Prober and Heath2012; Groen et al.2016). Some professors feel threatened and worry students will not learn if they’re not physically present, despite growing evidence that attendance is not associated with exam performance (Deane and Murphy2013; Paul et al.2015; Meyer et al.2016). Today’s students are adaptive adult learners, seeking the resources that can best address their needs. Today’s professors are adaptive teachers, seeking to provide the resources that can best meet a variety of student needs inside and out of the classroom. Neither a student nor his/her professors knows exactly what that student needs. Exactly what an individual student needs is discovered through collaborative engagement in an adaptive curriculum.
적응형 커리큘럼은 학생, 교수, 콘텐츠가 학생의 학습을 가속화한다는 목적에 맞춰 서로 시너지 효과를 내며 동시에 적응하는 커리큘럼입니다. 교수자가 안내하고, 학생이 개인화하며, 콘텐츠(종종 테크놀로지의 도움으로)를 통해 활성화되는 적응형 커리큘럼은 지속적으로 진화합니다. 다음 단락에서는 아메리칸 카리브해 의과대학(AUC)에서 학생과 교수가 병행 교육과정을 중심으로 함께 적응하는 학습 환경을 조성하고, 형성 평가를 자주 실시하며, 여정을 이해하기 위한 커리큘럼 포지셔닝을 사용하여 적응형 교육과정을 발전시키는 방법을 간략하게 설명합니다. An adaptive curriculum is one in which the student, the professor, and the content are each simultaneously and synergistically adapting to each other aligned with the purpose of accelerating student learning. Guided by the professor, personalized by the student, and enabled by content (often with the help of technology), the adaptive curriculum continuously evolves. In the following paragraphs, we outline how American University of the Caribbean School of Medicine (AUC) is evolving an adaptive curriculum by purposefully enabling a learning environment where students and professors adapt together around the parallel curriculum, with frequent formative assessments, while using curriculum positioning to understand the journey.
불참을 한탄하기보다 병행 커리큘럼을 수용하기 Embracing the parallel curriculum rather than lamenting nonattendance
교수진과 커리큘럼 개발자가 거의 인식하지 못하는, 가르치는 커리큘럼과 함께 운영되는 '병행 커리큘럼'이 있습니다. 이 공간은 학생들이 가르치는 커리큘럼에서 원하는 대로 제시되지 않은 내용을 학습하는 널 커리큘럼 내의 공간입니다(Hafferty and Gaufberg 2017). 학생들이 수업이 없을 때 "어울리며 배우는" 공간입니다. 저자 중 한 명(HC)은 최근 추가 학위 취득을 위해 정식 학교 교육으로 돌아갈 기회가 생겼을 때 "WhatsApp" 코스 그룹에 가입하여 커리큘럼의 동기식 및 비동기식 부분에서 가상 대화가 진행되는 것을 발견했습니다. 학생들은 공식 수업 중이나 수업 외 시간에 다른 학생들에게 방금 말한 내용에 대한 설명을 요청하고, 제안된 내용 대신 자신이 사용한 리소스를 지적하고, 과제에 대한 예상 노력에 대해 논의했습니다. There is a “parallel curriculum” that runs alongside the taught curriculum that is largely unrecognized by faculty and curriculum developers. It is the space within the null curriculum where students learn what is not presented to their liking in the taught curriculum (Hafferty and Gaufberg2017). It is the space where students “hang out and learn” when they are not in class. When one of the authors (HC) recently had the opportunity to return to formal schooling for an additional degree, she joined a course “WhatsApp” group and noticed the virtual conversation going on during the synchronous as well as asynchronous parts of the curriculum. During and outside of the formal classroom, students asked other students for clarification on what was just said, pointed out resources they used instead of what was suggested, and discussed effort expectations for assignments.
병행 커리큘럼은 학습 앱, 학생 레거시 노트(학생이 이전 학기 또는 몇 년 동안 생성한 팁과 노트), 학습 리소스 웹사이트 및 기타 학습 환경의 고유한 위치로 구성됩니다. 점점 더 많은 학습이 개별적으로 또는 동료와 함께 이루어지는 곳입니다. 또한 교사가 학습자를 적응형 커리큘럼에 참여시킬 수 있는 이상적인 기회를 제공합니다. The parallel curriculum consists of learning Apps, student legacy notes (student generated tips and notes from previous semesters or years), study resource websites, and other unique locations in the learning landscape. It is where increasingly more learning takes place individually and with peers. It also provides an ideal opportunity for teachers to engage the learner in the adaptive curriculum.
호기심 어린 탐구와 이해관계자 간의 정기적인 소통을 통해 병행 교육과정을 활용함으로써 학생, 학습 습관, 교과 분야에 대해 많은 것을 배울 수 있습니다. 학생들은 자신의 학습을 개인화하는 방법으로 병행 교육과정을 활용합니다. 학생들은 동일한 정보를 다양한 방식으로 제공받으며 자신에게 가장 적합하다고 생각되는 것을 선택합니다. 병행 커리큘럼을 활용하는 방법을 배운 교수진은 학생들이 학습을 강화할 수 있도록 지도하는 방법을 기하급수적으로 늘릴 수 있습니다. We can learn a great deal about our students, their study habits, and our subject areas by tapping into the parallel curriculum through curious exploration and regular communication among stakeholders. Students engage the parallel curriculum as a way to personalize their learning. They find the same information presented through different modalities and select what they believe works best for them. Faculty members, who learn to harness the parallel curriculum, can exponentially increase the ways in which they guide students to augment their learning.
AUC에서는 학생들이 병행 커리큘럼에서 사용하는 학습 보조 도구, 신기술 및 교육 리소스에 대해 공식적으로 문의합니다. 조사 결과는 대학에서 구매하는 리소스에 대한 정보를 제공하며 교수진과 공유됩니다. 교수진 혁신가들은 병행 커리큘럼에 참여하는 실험을 합니다. 이들은 강의 캡처, 플래시카드 및 질문을 사용하여 학생들과 소통하고 자신의 영역에서 가르치기 위해 Osmosis, Echo 360, First Aid 및 UWorld와 같은 학습 플랫폼을 사용합니다. 책임감 있는 혁신가들은 종종 교수진 개발 프레젠테이션과 워크샵에서 동료들을 가르칩니다. At AUC, we formally inquire about the learning aids, new technologies, and educational resources that students use in the parallel curriculum. The findings inform resources we purchase as a university, and are shared with faculty members. Faculty innovators experiment with engaging in the parallel curriculum. They use learning platforms such as Osmosis, Echo 360, First Aid, and UWorld to connect with students and teach on their turf, using lecture capture, flashcards, and questions. Often the responsible innovators teach their peers in faculty development presentations and workshops.
학생 혁신을 촉진하여 병행 커리큘럼에 학생들의 참여를 더욱 높일 수 있습니다. 예를 들어, AUC의 학생들이 개발하고 교수진과 공동으로 연구한 혁신 중 하나는 오디오 복습과 반복을 통한 학습 향상에 초점을 맞춘 것입니다. 이 앱은 시각적 관찰에 필요한 물리적, 시간적 제약 없이 메타인지 발달을 촉진함으로써 편의성과 휴대성이라는 적응적 특징을 해결합니다. 이번 특집호(브라운 외, 2018)에 소개된 청각 학습 앱 '렉처키퍼'에 대해 자세히 알아보세요. 이 앱은 '눈과 손이 자유롭기 때문에' 학습자가 운동, 여행, 식사 등과 같은 다른 활동에 연속적으로 참여할 수 있습니다. 이를 통해 학생들은 자신의 필요에 맞는 다양한 환경과 상황에서 자유롭게 학습할 수 있습니다. 이 오디오 학습 환경은 재생 및 표기 기능으로 개인화되어 있으며, 읽기나 비디오 복습 및 대화형 연습과 같은 고급 기술과 같은 기존의 많은 리소스보다 적응형 학습자에게 더 큰 유연성을 제공합니다. 무작위 비교 그룹 연구에서 LectureKeepr를 사용하는 학생들은 MCQ 테스트에서 더 높은 점수를 받았습니다. We can further engage our students in the parallel curriculum by promoting student innovation. For example, one innovation developed by students at AUC and studied collaboratively with our faculty focused on the benefit of enhanced learning through audio review and repetition. It addresses the adaptive features of convenience and portability, by fostering metacognitive development without physical and temporal requirements of visual observation. Their auditory learning App called LectureKeepr is described in this Special Issue (Brown et al.2018). It is “eyes and hands-free” allowing the learner to contiguously engage in other activities such as physical exercise, traveling, eating, and so on. This grants students the freedom to study in a wide range of environments and situations that suit their needs. This audio learning experience is personalized with playback and notation features and affords greater flexibility for the adaptive learner than many traditional resources like reading and advanced technologies including video review and interactive exercises. In a randomized comparison group study, students using LectureKeepr scored better on MCQ testing.
비디오 '강의 캡처' 시스템은 강의식 커리큘럼과 병행 커리큘럼을 연결하는 훌륭한 가교 역할을 합니다. 이 시스템을 통해 학생들은 수업에 참석하는 학생 수가 점점 줄어드는 이유를 설명하는 자료를 비동기적으로 볼 수 있습니다(Prober and Heath 2012; Groen 외. 2016). 이는 교사와 학생의 관계를 극적으로 변화시킬 수 있는 잠재력을 가지고 있습니다. 한 의과대학에서 한 학생이 교수에게 다가와 "혹시 XYZ 박사님이세요?"라고 물었습니다. 교수는 "네, 저예요"라고 대답했습니다. 그러자 학생이 말했습니다: "온라인 강의를 들으면서 교수님의 목소리를 알아봤어요. 소리를 두 배속으로 재생해서 못 알아볼 뻔했어요."(Mirza 2018). Video “lecture capture” systems provide an excellent bridge between the taught and parallel curricula. They allow students to view the material asynchronously explaining why fewer and fewer students are attending classes (Prober and Heath2012; Groen et al.2016). This has the potential to dramatically change the teacher–student relationship. At one medical school, a student approached a professor and asked “Are you Dr. XYZ?” The teacher replied “Yes, that is me.” The student then said: “I recognized your voice from listening to your lectures online. I almost didn’t recognize it because I am playing the sound double speed” (Mirza2018).
비디오가 있든 없든 강의 캡처 시스템은 강의자에게 유용한 정보를 제공하여 학생들의 학습을 향상시킬 수 있습니다. AUC에서는 학생들이 비동기적으로 질문을 게시하고 응답할 수 있는 강의 캡처 시스템을 사용합니다. 수업에서 우수한 성적을 거둔 학생 모더레이터를 선정하여 게시된 질문을 중심으로 온라인 토론 스레드를 진행하도록 했습니다. 교수진은 플랫폼에서 정기적으로 '오피스 아워'을 정하여 학생들이 토론에 참여하고 답변을 게시할 수 있도록 했습니다. 분석 결과, 병행 교육과정에 대한 이러한 참여는 학생들의 퀴즈 점수와 과목 이해도를 높인 것으로 나타났습니다. 교수진과 함께 일하는 학생 진행자의 도입으로 비동기식 학생 질문과 응답의 전체 수가 더욱 증가했으며 퀴즈 성과도 더욱 향상되었습니다. 또한 이 기능의 'raw data'는 적응적 교사에게강의에서 어떤 주제에 추가 설명이 필요한지에 대한 중요한 요구 사항 평가 정보를 제공했습니다. 강의 시스템이 발전함에 따라 학생들이 녹화된 강의를 얼마나 빨리 듣고 있는지, 어디에서 멈추고 다시 듣는지를 분석하면 개념의 복잡성과 전달의 명확성에 대한 정보를 얻을 수 있습니다. Lecture capture systems, with or without video, can also provide useful information to lecturers to enhance students’ learning. At AUC, we use a lecture capture system that enables students to post and respond to questions asynchronously. High performing student moderators within the class were selected to lead online discussion threads around posted questions. Faculty schedule regular “office hours” on the platform to join the discussions and post responses. Our analyses indicate that this engagement in the parallel curriculum increased student quiz scores and subject matter comprehension. The introduction of student moderators working with faculty members further increased the overall number of asynchronous student questions and responses and further enhanced quiz performance. The “raw data” from this feature also gave the adaptive teacher important needs assessment information about which topics in the lecture required additional explanation. As lecture systems evolve, analysis of how quickly students are listening to the recorded lectures and where they stop and re-listen can provide information about the complexity of concepts and clarity of delivery.
이러한 적응형 기술에 대한 인식과 이해, 활용도가 높아지면 교수진은 라이브 세션 밖에서도 학생과 소통하는 데 도움이 됩니다. 경험에 비추어 볼 때 다음 단계가 유용합니다. Greater awareness, understanding, and use of these adaptive technologies will help faculty members connect with their students outside of live sessions. Based on our experiences, the following steps are useful.
코스 디렉터를 프로세스에 참여시켜 학생의 참석이 필요한 수업 및 활동과 그렇지 않은 활동을 결정합니다.
새로운 학습용 앱을 수용하고 관련 결과를 검토할 교수진 챔피언을 찾습니다.
학생에게 어떤 앱을 중요하게 생각하는지에 대한 피드백을 요청하고 그 결과를 모든 학생 및 교직원과 공유합니다.
강의실 안팎에서 생성된 분석을 사용하여 강의 교수진이 학생들의 개념 이해도를 측정하는 데 사용하는 '멍하니 쳐다보기' 피드백을 대체합니다.
Engage course directors in the process to determine which classes and activities require student attendance and which do not.
Find faculty champions to embrace new Apps for learning and examine relevant outcomes.
Solicit feedback from students on what Apps they value and share the findings with all students and faculty
Use analytics (generated in and out of the classroom) to replace the “blank stare” feedback that lecturing faculty use to gage students’ understanding of concepts.
개인별 맞춤 학습자 평가 시스템으로 전환 Toward an adaptive learner assessment system
적응형 커리큘럼은 "질문하는 커리큘럼"입니다. 학생은 자신과 다른 사람의 질문에 묻고 답하면서 자신의 학습 요구를 평가하고 학습에 참여합니다. 적응형 커리큘럼에서 학생이 질문할 수 있는 방법에는 아래 등 여러 가지가 있습니다.
(a) 실시간 교육 세션에서 교수에게 직접 질문하기,
(b) 캡처한 강의 또는 학습 관리 시스템에 게시하기,
(c) 플래시 카드를 만들어 동료에게 정보가 맞는지 질문하기,
(d) 공부하는 동안 스스로 질문하기
The adaptive curriculum is a “questioning curriculum.” Students assess their learning needs and engage in learning by asking and answering their own and others’ questions. In an adaptive curriculum, there are many ways for students to ask questions:
(a) directly to a professor in a live educational session;
(b) posting to a captured lecture or learning management system, or
(c) developing a flash card and asking peers if the information is correct; and
(d) self-questioning while studying.
적응형 커리큘럼 내에서 운영되는 학생과 교사는 개별 학습 요구를 충족하기 위해 커리큘럼을 지속적으로 조정하고 있습니다. 이는 지속적인 커리큘럼 개선을 의미합니다.피드백은 이러한 조정 과정의 핵심입니다. 피드백은 다양한 방법으로 수집되지만, 가장 강력한 피드백 메커니즘 중 하나는 빈번한 형성 평가를 통해 얻은 학생의 성과입니다. 질문과 피드백 통합은 적응 과정에서 핵심적인 '학습 동인'입니다. Operating within an adaptive curriculum, students and teachers are constantly adjusting the curriculum to meet individual learning needs. This represents continuous curriculum improvement. Feedback is key to this adjustment process. It is gathered in many ways, but one of the most powerful feedback mechanisms is student performance, attained through frequent formative assessment. Questioning and integrating feedback are key“learning drivers” in the adaptive process.
교수진은 일반적으로 학생에게 질문을 던집니다.
질문을 전략으로 사용하는 강의식 강의실에서는 학생들이 더 자주 출석하고, 더 많이 참여하고, 객관식 시험에서 더 좋은 성적을 냅니다(Deslauriers 외. 2011).
임상 교육에서 질문을 사용하여 지식을 반복적으로 검색하는 연습을 하는 학생은 지식을 더 잘 유지하고 임상 상황에 적용하는 능력이 향상되는 것으로 나타났습니다. 질문에 응답하는 것은 지식의 임상적 적용을 향상시킵니다(Larsen 외. 2013).
학생들은 더 나은 문제 해결자가 되어 메타인지 수준에서 사건을 예측하고, 자기 모니터링을 하고, 임상적 결정에 편견이 없는지 확인하는 등의 작업을 쉽게 수행할 수 있습니다(Weinstein 외. 2010; Croskerry 2018).
Faculty members commonly pose questions to students.
In the lecture-based classrooms that rely on questioning as a strategy, students attend more often, are more engaged, and perform better on multiple-choice exams (Deslauriers et al.2011).
In their clinical training, students that practice repeated retrieval of knowledge using questions demonstrate enhanced retention and transfer of that knowledge to clinical situations.
Responding to questions improves clinical application of knowledge (Larsen et al.2013). Students become better problem-solvers and readily operate at the metacognitive level, anticipating events, self-monitoring, and checking clinical decisions for biases (Weinstein et al.2010; Croskerry2018).
피드백이 있는 질문, 특히 자기 질문은 학습의 고유한 동인입니다. 이러한 질문은 의사소통과 관점 잡기, 자기 평가, 임상 의사 결정, 계획과 같은 여러 가지 "고차원적" 기술을 개발하는 데 기초가 됩니다(Quirk 2006). 이러한 기술을 사용하는 상황에서 우리는 정보를 발견하고, 행동을 비교 및 대조하고, 사고에 대해 생각하고, 진행 상황을 모니터링하는 데 이러한 동인을 사용합니다. 이러한 기술을 종합하면 전문성이라고 할 수 있습니다. 의학교육의 분명한 목표는 지식과 기술을 갖추고, 효과적으로 계획을 세우고, 자신의 성과와 필요를 평가하고, 자신의 생각, 감정, 행동을 성찰하고, 직업 생활 전반에 걸쳐 다른 사람의 관점을 이해할 수 있는 전문 의사를 양성하는 것입니다. 간단히 말해서, 적응하고 행동하며 발전할 수 있는 전문가를 배출하는 것이 목표입니다. Questioning with feedback and specifically self-questioning are unique drivers of learning. They underly the development of several “higher order” skills such as communication and perspective-taking, self-assessment, clinical decision-making, and planning (Quirk2006). In situations where we use these skills, we use these drivers to uncover information, compare and contrast behaviors, think about our thinking, and monitor our progress. Together, these skills represent expertise. The indisputable aim of medical education is to developexpertphysicians who are knowledgeable and skilled, and can plan effectively, assess their own performance and needs, reflect on their thoughts, feelings, and behaviors, and understand the perspectives of others throughout their professional lives. Stated succinctly, the aim is to produce experts who can adapt, act, and advance.
질문을 통해 학생들은 교사의 도움 없이도 학습의 내용, 수준, 속도를 조정할 수 있습니다. 질문은 학습과 예측 분석의 기초입니다. 반성적 프로세스의 핵심 기능은 사고 과정의 격차나 단점을 파악하는 것입니다. 질문은 반성 연습의 기회를 제공합니다. 여러 연구에서 질문에 답하는 것이 단기 및 장기 기억에 미치는 긍정적인 영향이 입증되었습니다(Smith and Karpiche 2014, Brame and Biel 2015). 고도로 기능적인 적응형 커리큘럼에서는 학습자가 결국 교사가 됩니다. Questions enable students to adapt the content, level and pace of learning with, and ultimately without, the aid of a teacher. They are the foundation of learning and predictive analytics. A key function of the reflective process is to identify gaps or shortcomings in the thinking process. Questions provide an opportunity for retrieval practice. Several studies have demonstrated the positive impact of answering questions on short- and long-term retention (Smith and Karpiche2014; Brame and Biel2015). In a highly functional adaptive curriculum, the learner eventually becomes the teacher.
질문이 학습 유지와 인지 및 메타인지 성장에 미치는 긍정적인 효과는 피드백을 통해 더욱 강화됩니다(Bing-You와 Trowbridge 2009). 퀴즈와 시험이 끝난 후 학생이 받는 맞춤형 코칭 보고서는 신중하게 설계되고 실행될 때 학생이 향상할 수 있는 기회를 제공합니다(Heen and Stone 2014). 반성의 기회와 함께 피드백을 받으면 자기 평가 능력을 향상시킬 수 있습니다. The positive effects of questioning on retention as well as cognitive and metacognitive growth are enhanced with feedback (Bing-You and Trowbridge2009). Tailored coaching reports received by students after quizzes and exams, when carefully designed and implemented, provide an opportunity for the student to improve (Heen and Stone2014). Feedback coupled with an opportunity for reflection can enhance the ability to self-assess.
퀴즈와 모의고사는 적응형 커리큘럼의 핵심 학습 동인으로서 질문을 공식화합니다(McDaniel 외. 2012; Arnold와 McDermott, 2013). 이러한 시험은 강력한 습관을 형성하고 유지력을 강화하기 위해 자기 평가를 사용하여 학생들의 기억을 준비시킵니다. 학습에 대한 입증된 가치에도 불구하고, 의과대학 커리큘럼에서 자기 평가는 눈에 띄게 부재합니다(Gruppen 외. 2000; Davis 외. 2006; Colthart 외. 2008). 최근의 한 연구에 따르면 주간 형성 퀴즈 성적이 기말고사 점수를 예측할 수 있는 것으로 나타났습니다(Chang and Wimmers 2017). 저자들은 낮은 난이도의 퀴즈를 자주 풀면 학생들이 학습을 교정하고 간격과 인터리빙과 같은 효과적인 전략에 집중할 수 있다고 결론지었습니다. Quizzes and practice exams formalize questioning as the key learning driver in the adaptive curriculum (McDaniel et al.2012; Arnold and McDermott,2013). They build strong habits and prepare students’ recall by employing self-assessment to strengthen retention. Despite its proven value to learning, self-assessment is conspicuously absent in the medical school curriculum (Gruppen et al.2000; Davis et al.2006; Colthart et al.2008). A recent study found that performance on weekly formative quizzes was predictive of final exam scores (Chang and Wimmers2017). The authors conclude that frequent low stakes quizzes allow students to calibrate their learning and attend to effective strategies such as spacing and interleaving.
AUC에서는 자기 평가와 개인화된 빠른 피드백을 통해 적응형 학습을 강화하기 위해 모든 코스에서 매주 형성형 퀴즈와 '학습을 위한 시험'을 독특하게 조합하여 사용합니다(Carney 외. 2018, 이번 의료 교사 특별호 참조). 현재 학생들은 퀴즈를 풀어야 하지만 점수가 최종 성적에 영향을 미치지 않습니다. 학생들은 자신의 성과 데이터와 개선 기회가 포함된 상세한 코칭 보고서를 받습니다. 학생들은 모든 문제를 정답으로 맞출 때까지 동일한 퀴즈를 다시 풀도록 권장되며, 대부분의 수업에서 성적에 대한 추가 점수를 받습니다. 퀴즈는 표준화된 시험 형식을 반영하여 리허설을 촉진합니다. 또한 퀴즈는 간격 학습과 인터리빙 학습의 이점을 극대화하도록 설계되었으며 학생의 학습 경험의 구조에 통합되어 있습니다. 학생들은 학기 내내 이전에 공부했던 퀴즈와 리포트로 돌아가 시험 공부를 할 수 있습니다. At AUC, we use a unique combination of weekly formative quizzes and “exams for learning” in every course to enhance adaptive learning through self-assessment and personalized rapid feedback (see Carney et al.2018; in this special issue of medical teacher). Currently, students are required to take quizzes, yet their scores cannot hurt their final grades. They receive detailed coaching reports with their performance data plus the opportunity for improvement. They are encouraged to return to the same quizzes until they answer all of the questions correctly and in most classes receive extra credit toward their grades. The quizzes mirror the standardized examination format to foster rehearsal. They are also designed to maximize the benefits of spaced and interleaved learning and are woven into the fabric of the student’s learning experience. Students can return to their earlier quizzes and reports throughout the semester to study for exams.
또한, 학습을 강화하기 위해 동일한 간격으로 두 번의 학기 시험과 기말시험을 실시하는 구조를 검토하고 있습니다. 각 학기 시험 순서에서, 학생들은 3일 후에 두 번째 시험을 치르고 두 시험 점수 중 더 높은 점수를 받을 수 있습니다. 시험 사이에 학생들은 첫 번째 시험 성적에 대한 심층 분석과 교수진 및 동료로부터 코칭을 받습니다. In addition, we are evaluating a structure of two equally spaced term exams that are designed to enhance learning plus a final examination. During each term exam sequence, students can take a second version of the exams three days later and receive the higher of the two exam scores. Between exams, students receive in-depth analyses of their performances on the first exam and coaching from faculty and peers.
새로운 적응형 평가 시스템을 평가한 결과 학습과 유지에 도움이 되는 것으로 나타났습니다. 이러한 형성 전략과 이러한 전략이 총체적 성과와 적응 행동에 미치는 영향에 대한 예비 결과는 이번 특별호(Carney 외. 2018)에 자세히 설명되어 있습니다. 이 과정은 학습 '을 위한' 평가뿐만 아니라 학습 '에 대한' 평가를 나타냅니다. AUC에서는 다음과 같은 지속적인 적응 평가 순서를 평가함으로써 평가에 대한 학문적 접근을 계속하고 있습니다.
(a) 시간적 간격을 둔 리허설,
(b) 즉각적인 분석,
(c) 구조화된 피드백,
(d) 반복
우리는 역량 기반 의학교육의 평가가 단순히 무능력을 파악하는 것이 아니라 역량을 향상하는 데 초점을 맞춰야 한다는 Schuwirth와 Ash(2013)의 의견에 동의합니다. Evaluation of our emerging adaptive assessment system reveals benefits for learning and retention. These formative strategies and preliminary results of their impact on summative performance and adaptive behavior are described more fully in this Special Issue (Carney et al.2018). The process represents assessment “for” as well “of” learning. At AUC, we continue to take a scholarly approach to assessment by evaluating the continuous adaptive assessment sequence:
(a) spaced rehearsal,
(b) immediate analytics,
(c) structured feedback, and
(d) repetition.
We agree with Schuwirth and Ash (2013) that assessment in competency-based medical education should focus on improving competence, not simply on identifying incompetence.
커리큘럼 포지셔닝을 통한 여정 이해하기 Understanding the journey with curriculum positioning
적응형 평가 시스템은 개별 학습을 보완하고 정보를 제공하며 적응형 커리큘럼에 긍정적인 영향을 미칩니다. 학생 평가 데이터의 일관된 보고는 교육, 멘토링 및 교정의 강력하고 역동적인 조정을 용이하게 합니다. 또한 커리큘럼 개발을 위한 학습 및 예측 분석을 제공하고 여러 교육기관 이해관계자 간의 시너지를 촉진합니다. 평가 데이터는 형성형 및 요약형 모두에서 AUC의 성장하는 적응형 커리큘럼에 필수적인 '적응형' 데이터 소스임이 입증되고 있습니다. The adaptive assessment system complements and informs individual learning and has a positive impact on the adaptive curriculum. Consistent reporting of student assessment data facilitates robust, dynamic adjustments of teaching, mentoring, and remediation. It also provides learning and predictive analytics for curriculum development and facilitates synergy among multiple institutional stakeholders. Assessment data, both formative and summative, are proving to be an essential “adaptive” data source for AUC’s growing adaptive curriculum.
적응형 커리큘럼이 부분의 합보다 더 큰 전체를 구성할 수 있는 능력과 사례 기반 커리큘럼이 기초 과학 자료의 부자연스러운 순서를 가질 가능성이 증가함에 따라 신중한 매핑이 필요합니다. 커리큘럼 맵은 연결성, 범위 및 일관성을 식별하는 데 도움이 됩니다(Harden 2009). 분석은 학습과 교수를 지시하고 원하는 결과를 달성하는 데 있어 미래의 성공을 예측할 수 있는 가시적인 마커 또는 웨이포인트를 제공하는 데 사용됩니다. 분석 목적으로 다각적인 커리큘럼 데이터를 마이닝하는 것은 커리큘럼 맵의 동적 해석으로 포착됩니다. The capacity for the adaptive curriculum to constitute a whole greater than the sum of its parts and an increased potential for case-based curricula to have an unnatural sequence of basic science material requires careful mapping. The curriculum map helps identify connections, coverage, and consistency (Harden2009). Analytics are used to provide tangible markers or waypoints that direct learning and teaching and predict future success in achieving desired outcomes. Mining the multifaceted curriculum data for analytic purposes is captured in a dynamic interpretation of the curriculum map.
이제 데이터에 대한 새로운 기술과 접근 방식을 통해 위성 위치 확인 시스템(GPS)과 유사한 방식으로 이정표와 역량에 이르는 다양한 커리큘럼 경로를 '위성 보기'할 수 있게 되었습니다. 이와 유사하게, 커리큘럼 포지셔닝 시스템(CPS)은 이해관계자가 성과 목적지(역량), 이동 방법(학습 전략), 경유지(마일스톤)를 설정할 수 있는 동적 대화형 교육 도구를 제공합니다. 학생과 교직원은 예상 도착 시간에 대한 정확한 정보를 공유하고 학습을 위한 복잡한 코스를 계획할 수 있습니다. 학생들은 CPS를 통해 개인화된 대체 경로와 여정을 보관하고 반성할 수 있는 공간을 만들 수 있습니다. New technologies and approaches to data now enable us to “take a satellite view” of the multiple curriculum pathways to milestones and competencies in a manner akin to the Global Positioning System (GPS). Analogously, a Curriculum Positioning System (CPS) offers a dynamic interactive educational tool that enables stakeholders to establish performance destinations (competencies), methods of transportation (learning strategies), and waypoints (milestones). Students and faculty will share accurate information about estimated time of arrival and plot complex courses for learning. Our CPS will enable students to create personalized alternative routes and a place to archive and reflect on their journeys.
애널리틱스는 적응형 커리큘럼의 중추입니다. 이를 통해 교사는 학습의 지휘자가 될 수 있습니다. 교사는 학생 개개인의 필요에 따라 학생을 리소스로 안내합니다. 데이터(대부분 개인 및 그룹 성과 데이터)는 목표에 대한 진척도를 평가하고 이 진척도를 표준과 비교하여 미래의 성과를 예측하는 데 사용됩니다. 분석은 각 단계에서 학생의 성과를 추적하여 파악된 요구사항과 연계된 리소스를 보다 정확하게 타겟팅할 수 있도록 합니다. Analytics are the backbone of an adaptive curriculum. They enable the teacher to become a conductor of learning. Teachers direct students to resources based on their individual needs. Data – most often individual and group performance data – are used to assess progress toward objectives and also predict future performance based on this progress compared to a gold standard. Analytics track the student’s performance each step along the way allowing greater precision in targeting the resources that have been tied to the needs identified.
결론 Conclusions
하버드 의과대학의 학장 찰스 헌더트는 '새로운 커리큘럼'을 언급하며 다음과 같이 말합니다: "의학 교육은 정보의 전달이 아니라 학습자의 변화에 관한 것입니다."(Shaw 2015). 커리큘럼은 단순한 강의 계획서나 내용 설명, 심지어는 내용 자체의 전달 그 이상이 되었습니다. 그것은 교사의 의도, 이를 실현하고 결과를 판단하는 방식에 관한 교육 프로그램에서 일어나야 하고 실제로 일어나는 일입니다(Quirk and Harden 2017). Referring to the “new curriculum,” Charles Hundert, Dean of Harvard Medical School states: “Medical education is not about the transmission of information, but about the transformation of the learner” (Shaw2015). A curriculum has become more than just a syllabus, a statement of content or even delivery of the content itself. It is what should and does happen in a teaching program – about the intention of the teachers, about the way they make this happen and judge the results (Quirk and Harden2017).
이로 인해 학습 환경에 대한 관점이 확장되었고 커리큘럼에 대한 새로운 정의가 필요해졌습니다. 교육과정은 역량으로 이어지는 학습 및 평가 경험의 총합으로 정의하는 것이 가장 적합하며, 학부 의학교육부터 평생의학교육까지 지속적인 학습의 총합을 포함해야 합니다. 좀 더 정확한 표현을 빌리자면, 커리큘럼은 한 가지가 아니라 학습으로 이어지는 여러 가지 '커리큘럼 경로'가 있습니다. 가장 전통적인 경로는 "가르쳐진 커리큘럼taught curriculum"입니다. 여기에는 강의 및 소그룹과 같은 강의실 활동과 교수진이 제작한 자료 및 유인물이 포함됩니다. This has resulted in an expanded view of the learning environment and requires a new definition of curriculum. It is best defined as the sum of learning and assessment experiences that lead toward competency and should cover the sum of continuous learning from undergraduate medical education through continuing medical education. Using a more accurate vernacular, there is not just one curriculum, but instead, several “curriculum pathways” that lead to learning. The most traditional pathway is the “taught curriculum.” It includes classroom activity such as lecturing and small groups as well as faculty generated materials and handouts.
의료 학습자의 장기적인 적응 필요성을 고려할 때 커리큘럼의 의료 콘텐츠는 실제 임상 문제를 중심으로 구성되어야 합니다. 이는 학생들이 자신의 학습 요구를 평가하고 피드백을 맞춤화할 수 있는 임상 사례를 통해 가장 쉽게 달성할 수 있습니다. 사례 기반 커리큘럼은 실제 적용 사례를 반영하고 커리큘럼을 개인화하므로 진정성이 있습니다. 대부분의 경우 의학은 '케이스'를 통해 실행되며, 케이스 학습을 통해 학생들은 실습에 대비할 수 있습니다. Considering the medical learner’s long-term adaptive needs, curriculum medical content must revolve around real-world clinical problems. This is most easily accomplished through clinical cases where students can assess their learning needs and feedback can be customized. Case-based curriculum is authentic; it mirrors real-life application and personalizes the curriculum. For the most part, medicine is practiced “in cases,” and learning in cases prepares students for practice.
적응형 의료 교육은 "모든 사람에게 맞는" 접근 방식이 아니라 다양한 수준의 지식과 배경을 가진 학습자의 요구를 해결합니다. 교사는 가르침형, 병행형, 숨겨진 커리큘럼 사이를 유동적으로 이동하며 교육 여정의 어느 단계에서든 학생을 만날 수 있습니다. Adaptive medical teaching addresses the needs of learners that have different levels of knowledge and backgrounds, rather than a “one size fits all” approach. The teacher is able to fluidly move between the taught, parallel, and hidden curriculum – meeting a student wherever they are in their educational journeys.
적응형 커리큘럼은 공통점을 가진 학생들을 유연하게 가르칠 수 있도록 설계되었습니다. 학생들은 자신의 강점과 약점을 이해함으로써 학습하는 법을 배웁니다. 자신과 다른 사람의 사고에 대해 생각하고, 결함을 인식하고, 행동을 취하고, 학습 결과에 영향을 미칩니다. 적응형 학습자 중 리더는 변화를 주도합니다. 실제로 이들은 의학과 의료가 근본적으로 변화해야 하며, 단순히 적응하는 것이 아니라 주도해야 한다고 공통적으로 믿습니다. 이들의 지식과 가치는 감정과 얽혀 있으며, 신념은 끈기가 되고 경우에 따라서는 "의로운 분노"가 되기도 합니다. 발견, 혁신, 권한 부여, 영감, 겸손이 이들의 변화의 도구입니다. The adaptive curriculum is designed to flexibly teach students who share a common thread. They learn to learn by understanding their strengths and weaknesses. They think about their own and others’ thinking, perceive a flaw, take action, and have an impact on their learning outcomes. The leaders among our adaptive learners become transformative. In fact, they uniformly believe that medicine and healthcare must fundamentally change, and they must lead, rather than simply adapt. Their knowledge and values are intertwined with their feelings – conviction becomes persistence and, in some instances, “righteous anger.” Discovery, innovation, empowerment, inspiration, and humility are their instruments for change.
변혁적 학습자는 특별한 부류의 적응 전문가입니다. 이들은 말과 행동을 통해 광범위한 청중에게 다가갑니다. 이들은 소통의 달인으로, 자신의 신념을 표현하고 행동으로 옮길 수 있는 광활한 무대를 구축합니다. 이들은 전통적인 경계를 뛰어넘어 사람들을 이끌고 교육하며, 다른 사람들이 뛰어난 능력을 발휘하도록 영감을 주고 미디어의 관심을 불러일으킵니다. 이들의 개성은 다른 사람들을 변화의 과정으로 끌어들입니다. 변혁적 학습자는 기존의 직업적 경계를 넘어 큰 무대에서 참여하고 영감을 줍니다.
Transformative learners are a special class of adaptive experts. They reach broad audiences through words and actions. They are masters of communication, building an expansive stage from which to express and act upon their beliefs. They lead and educate across traditional boundaries, inspire others to excel and pique interest from the media. Their personalities draw others into the transformation process. Transformative learners engage and inspire on a big stage – beyond traditional professional boundaries.
Med Teach. 2018 Aug;40(8):786-790.doi: 10.1080/0142159X.2018.1484896.Epub 2018 Jul 22.
The adaptive medical curriculum: A model for continuous improvement
This paper describes the medical curriculum designed to foster adaptive expertise. Engaging in the formal and informal curriculum, students learn to achieve desired outcomes in novel situations, perform comfortably with uncertainty, and are often recognized for creative problem-solving. Students learn by asking and answering their own and others' questions. They readily operate at the metacognitive level, anticipating events, self-monitoring, and checking decisions and emotions. A key function of the reflective process is to identify gaps or shortcomings in the thinking process. The adaptive learner shifts into reflective thinking when confronted with complex contextual and situational demands. We are only beginning to understand how to create educational pathways to foster adaptive learning. An essential focus is the adaptive teacher who frames learning and assessment around predictive analytics, reflective spaced practice, and authentic learning material. To be effective, the teacher must engage the learner outside the formal classroom in the parallel curriculum. A major premise is that learning occurs individually and together with peers, teachers, and team members in multiple contexts. During the learning process, the learner readily operates at the metacognitive level, anticipating behavior, self-monitoring and assessing, and checking theirs and others decisions and emotions. The adaptive medical curriculum provides the pathway for such learning.
미국 의료시스템과학 교육의 한국 도입과 그 비판(Korean J Med Hist, 2022) 김택중*
“하나의 유령이 한국의 의학교육계를 떠돌고 있다, 의료시스템과학이라는 유령이.”
1. 들어가는 말
의학은 과학이기에 앞서 인간학이다.1)의(醫, medicine)의 중심에는 치유의 주체이자 치료의 객체인 환자, 곧 아픈 ‘사람’이 있기 때문이다. 이 논문에서 논의하고자 하는 미국의 의료시스템과학(health systems science) 역시 표면적으로는 그 중심에 아픈 ‘사람’이 있음을 강조한다. 의료시스템과학 교육과정의 이른바 핵심 기능 영역(core functional domains)에 속한 7개 요소 가운데 단연 첫 번째로 꼽고 있는 요소가 다름 아닌 ‘환자, 가족, 지역사회’라는 사실이 바로 이를 말해 준다. 그러나 미국의 의료시스템과학은 ‘시스템’을 부각시킨 조어로도 짐작할 수 있듯이 사람보다는 그를 둘러싼 의료적 구조를 더 강조한다. 나머지 6개의 요소가 전부 의료시스템과 관련된 항목들로 채워져 있는 것은 우연이 아니다.2)
=== 1) 이 논문에서 말하는 인간학이란 인간의 본질과 과제를 규명하는 엄밀한 학으로서의 철학적 또는 신학적 인간학(anthropology)을 의미하지 않는다. 글자 그대로 인간에 대한 관심 또는 사랑을 가리킨다.
2) 핵심 기능 영역의 7개 요소를 순서대로 나열하면 다음과 같다.
1. 환자, 가족, 지역사회(patient, family, and community),
2. 의료 구조와 프로세스(Health care structure and process),
3. 의료 정책과 경제(Health care policy and economics),
4. 의료정보과학과 의료 기술(Clinical informatics and health technology),
5. 인구, 공중, 건강의 사회적 결정 요인(Population, public, and social determinants of health),
6. 가치 기반 의료(Value in health care),
7. 의료시스템 개선(Health system improvement)(Skochelak 외, 2021: 8-10).
===
1910년 이후 확립된 미국 의학교육의 핵심 모형은 시스템 중심 교육이 아닌 의사 중심 교육(physician-centric education) 모형이었다. 이는 전통적인 도제식 교육과도 일맥상통하는 것으로서 기본적으로 의료를 선배 의사(들)에게 배우고 터득하는 방식이다. 따라서 의학교육의 정중앙을 차지하고 있는 것은 다름 아닌 의사이다. 즉, 의사가 의료의 주체이자 교육의 주체가 된다. 반면 근래 부상한 의료시스템과학 교육은 환자 중심의 시스템적 정체성(patient-centered systems identity)을 강조한다. 그에 따라 의사는 정중앙에서 주변부로 밀려나의료시스템을 구성하는 일개 요소로서 탈중심화되고 탈주체화된다(Skochelak 외, 2021: 13-15).
문제는 이러한 움직임이 의사 대신 시스템의 정중앙에 자리하게 된 환자라 해서 예외로 작용하지 않는다는 점이다. 비록 의료시스템과학이 환자 중심을 천명하고 있다지만 이는 어디까지나 의료‘시스템’을 전제로 한 것이다. 요컨대 시스템/구조의 강조가 거꾸로 의료의 핵심인 환자/사람을 소외시키는 역설을 드러낼 수 있다는 의미이다.즉, 의료시스템과학은 이미 일상이 되어 버린 환자의 의료 소외 현상을 오히려 가속화시킬 위험성을 내포하고 있다. 이른바 구조주의의 자장 안에서 의료시스템과학은 인간 주체를 중심으로 한 근대주의를 지양하려는 소위 탈근대적 움직임을 보이고 있는 것이다.3)
=== 3) 이 논문에서는 구조주의를 보다 포괄적으로 확대하여 해석하기로 한다. 즉, 구조조의를 철학사적 맥락에서 언어학적인 면에 한정하지 않고 실존주의의 대척점에 서 있다는 점에서 탈근대, 탈주체의 시작을 알리는 한 흐름으로 보았다. ===
그럼에도 의(醫)에 관한 한, 여전히 사람은 구조에 선행할 수밖에 없다. 탈근대적인 시스템적 정체성을 수용하는 것도 결국은 그 시스템을 움직이는 사람(들)이기 때문이다.4)따라서 의학교육의 근본 목표 또한 결국은 환자/사람을 잘 치료하는 좋은 의사/사람의 양성에 있을 수밖에 없다. 이러한 점에서 “의사의 가장 핵심적인 자질 중 하나는 인간에 대한 관심이다. 왜냐하면 환자를 잘 치료할 수 있는 비결은 바로 환자를 염려하는 데 있기 때문”이다(토버, 2003: 56에서 재인용). 의학이 근본적으로 시스템과학이 아닌 인간학인 이유다.
=== 4) 구조주의적 관점은 이와 정반대이다. 즉, 인간중심주의를 철저히 배격하면서 인간이 사회구조/시스템을 만들고 움직이는 것이 아니라, 거꾸로 사회구조/시스템이 인간을 만들고 움직인다고 본다. ===
구조를 강조하면서 구조로써 사람을 대치하려는 의료시스템과학에는 이러한 인간의 모습이 잘 포착되지 않는다. 지식 교육이라는 측면에서 의료시스템과학은 인간을 진열대의 장식품으로만 활용할 뿐, 그 이면을 들여다보면 이내 과학이라는 이름의 차가운 구조만 노출시키고 있을 따름이다. 의사에게 의료시스템과의 적극적이고 공생적인 관계성을 촉진시키면 시킬수록 반대로 그 시스템에 매몰되어 의사도 실종되고 환자도 실종되어 버리는 역설적 현상이 벌어지는 것이다. 이러한 이유로 미국식 의료시스템과학 교육을 단기간에 직수입하려는 공학적 시도는 많은 무리가 뒤따를 수밖에 없다.
물론 의료시스템과학 교육의 도입 자체를 거부할 이유는 없다. 통속적 맥락의 러다이트가 되어 두려워할 필요도 없다. 어차피 한국의 의학교육은 많은 부분 미국 의학교육에 빚지고 있고, 앞으로도 그러할 것이기 때문이다. 가령 미국식 역량바탕교육(competency based education)의 경우 본격적으로 도입된지 10여 년 만에 의학교육 평가인증 제도의 강제력에 힘입어 국내 의과대학 교육체계의 근간을 이루게 되었다.5)이런 점만 보더라도 미국 의학교육의 영향력이 얼마나 큰지를 짐작해 볼 수 있다. 그러나 이런저런 미국식 교육방식이 과연 면밀한 검토를 거쳐 도입되었는가를 질문해 본다면 회의적일 수밖에 없다. 우리 실정에 맞는 착종 과정을 충분히 거쳤다고 보기 어렵다는 얘기다. 사회적 합의 없이 성급하게 도입된 미국식 의학전문대학원 제도가 결국 완전한 실패로 끝난 것이 이를 방증한다.6)이렇듯 착종의 진지한 고민이 없는 미국식 관점의 일방적 이식은 안착이 아니라 거부반응으로 귀결될 가능성이 상존한다. 이는 의료시스템과학 교육의 도입 과정에도 예외일 수 없다.
=== 5) 미국에서 역량바탕교육의 역사는 멀리는 1949년까지 거슬러 올라갈 수 있으며, 1950-60년대에 행동주의 심리학의 영향 아래 이론화되기 시작했다. 그러나 미국에서 역량바탕교육이 의학교육에 본격적으로 적용되기 시작한 것은 1999년에 이르러서였다(Morcke, Dornan, Eika, 2013: 852-853). 한국의 의학교육 평가인증 제도에 역량바탕교육이 성과(outcomes)라는 이름으로 강제화된 것은 한국의학교육평가원이 2010년도 『의학교육 평가인증 기준 및 규정』에 학습성과와 졸업성과를 구체적으로 명시한 동년의 일이다(한국의학교육평가원, 2010: 21-23).
6) 4년제 의학전문대학원(이하 의전원) 제도는 김대중 정부 시기였던 2002년 1월 교육인적자원부가 제도 도입의 기본계획을 발표하면서 본격적으로 시작되었다. 그 이전까지는 모든 의과대학이 의예과 2년과 의학과 4년의 6년제 학부 과정으로 운영되었다. 노무현 정부 시기였던 2005년 첫 입학을 시작으로 2011년까지 의전원으로 전환한 의과대학은 당시 전국 41개교 중 65.9%에 해당하는 27개교(의과대학과 의전원 병행 대학 포함)였다. 그러나 의학계 내부의 지속적인 반대 목소리, 사회적 부작용에 따른 찬반 논란 등이 맞물리면서 2010년 교육부가 각 대학에 학제 선택의 자율권을 주기 위한 계획을 발표하기에 이른다(한국의학교육학회, 2014: 4-6). 이후 2015년-2017년 사이 대부분 의전원이 6년제 의과대학 체제로 복귀하였으며, 2022년 현재 의전원 체제를 계속 유지할 계획인 대학은 1개교뿐이다(이영환 외, 2022: 38-40). ===
이 논문에서는 우선 미국에서 의료시스템과학이 출현한 사회적, 사상적 배경을 살펴본 뒤 한국에 도입된 배경과 그 이유들을 살펴본다. 그리고 의료시스템 과학이 착종 과정 없이 직수입되었을 때의 문제점을 기존 인문사회의학(의료인 문학)과의 비교 분석을 통해 논한 다음, 바람직한 착종의 형태를 제시해 보는 것으로 글을 마무리하고자 한다.
2. 미국의 의학교육, 그리고 의료시스템과학의 출현
1) 프래그머티즘과 미국
미국의 의학교육은 필자가 보기에 현재 한 가지 거시 원리에 의거하여 작동하고 있다. 그 거시 원리란 다름 아닌 미국 유일의 고유 철학인 프래그머티즘(Pragmatism)으로서 그 가운데 특히 효용성을 중시하는 공학적 특성이 두드러진다. 19세기 후반부터 20세기 초에 걸쳐 미국에서 자생적으로 발현된 사상 체계인 프래그머티즘은 여러 이질적인 경로의 조합과 파생 과정을 거쳐 오늘날 미국 의학교육의 실천적, 실험적 특성을 강화시키고 있다. 비록 20세기 후반에 접어들면서 다양한 철학 사조가 영미권 교육철학의 방법과 관점에 변화를 가져왔으나(한기철, 곽덕주, 김상섭, 2010: 183-184), 의학교육 분야는 20세기 전반에 확립된 프래그머티즘 및 그 영향력으로 형성된 진보주의 교육철학의 자장 안에 여전히 머물러 있는 것으로 보인다.
이러한 판단을 하는 근거는 1999년 미국의과대학협회(Association of American Medical Colleges, AAMC)가 역량바탕교육을 옹호하는 보고서를 작성하여 제출한 이래 10년도 지나지 않아 역량바탕교육이 미국뿐 아니라 전 세계적으로 채택되어 널리 이용되고 있는 데서 비롯한다(Morcke, Dornan, Eika, 2013: 852-853). 이 역량바탕교육의 사상적 뿌리는 가위 미국식 프래그머티즘이라 할 만하다. 그것은 프래그머티즘이 의료 현장 등 실세계 문제해결에 도움이 되는 실용적 지식이나 비판적 태도 및 능력 함양의 이론적 근거가 되며, 프래그머티즘의 영향력으로 형성된 진보주의 교육철학이 교수자 중심의 학습목표가 아닌학습자 중심의 학습성과를 더 중시하는 역량바탕교육의 이론적 근거로 작용하기 때문이다.7)
프래그머티즘은 미국이라는 국가의 발전 과정과 불가분의 관계를 갖는 사상 체계이며, 원래 남북전쟁 후 급속한 산업화의 과정에서 발생한 갖가지 사회적 갈등을 점진적으로 해결하기 위한 온건한 대응책으로 마련된 것이었다. 또한 신생 합중국 미국의 새로운 환경에 적응하기 위해 다양한 전통의 이주민들이 기존의 원칙들에 구애받지 않아야 했다는 점을 상기한다면 프래그머티즘이 구체적인 상황에서의 문제해결, 곧 행동에 더 비중을 둘 수밖에 없었음을 어렵잖게 짐작할 수 있다. 이는 프래그머티즘의 어원인 고대 그리스어 프라그마( )가 행동, 행위, 실천, 실험 등을 의미한다는 것으로도 뒷받침된다.결국 프래그머티즘이란 미국인들의 행동 지향적이고 결과를 중시하는 생활관이 반영된 미국적 정서에 기반한 사상 체계인 것이다(신일철, 1987: 160-165;엄정식, 1996: 77-82).8)
신생 합중국 미국인들에게 이러한 ‘행동과 그에 따른 결과’는 인내와 근면을 기반으로 한 개인의 노력에 달린 것이었으며, 그 가시적이고도 구체적인 성과는 측정 가능한 업적으로 치환되어 개인의 존재 가치를 드러낸다고 보았다. 이러한 태도는 프래그머티즘의 경험론9), 실증주의, 과학주의 전통 속에 반영되어 있다. 그리고 이에 의거하여 프래그머티즘을 종합 정리하면 “이론보다는 실험을 강조하고 추상적 진리보다는 실천적 지혜를 선호하며 이것을 체계적 분석을 통해서가 아니라 실증적 경험을 통해서 확인하고 문제의 상황에 실용적으로 적용하는 입장”이라 할 수 있다(엄정식, 1996: 82). 이러한 까닭에 프래그머티즘을 가리켜 “모든 기존 사유 습관을 철폐하려는 행동주의”라는 평가가 나올 수 있는 것이다(듀이, 2020b: 6).
그러나 신생 합중국 미국의 사회적 갈등의 해결책으로서 제시된 프래그머티즘은 경험과 행동과 그에 따른 가시적 결과를 중시한다는 바로 그 이유로 인하여 가치론적 차원에서는 절대성을 부정하고 실제 문제해결에 유용한 상황적 효용성을 강조하게 되며, 따라서 이는 언제든 기계적인 공학적 효용성으로 변질될 위험성을 내포하고 있다. 즉, “미국인들의 가시적 성과에 대한 관심은 경험 개념을 공학화하고 통계적 수량화의 경향을 강화시킨다.” 요컨대 프래그머티즘에 의해 표현된 실제적 결과란 실증주의적으로 통제된 경험에 불과할 수 있다는 것이다. 이는 ‘이성의 도구화’라 할 만한 것으로서 그 이면의 보다 근본적인 가치에 대한 통찰을 방해할 위험이 있다(신일철, 1987: 182-183).
8) 프래그머티즘에 관한 가장 최근의 국내 종합 연구서 저자인 김동식에 따르면 프래그머티즘이란 “유럽의 지적인 유산을 미국의 사회ㆍ문화ㆍ역사적 조건에 부합하게 개변하려는 노력의 일환으로 나온 것”이다(김동식, 2002: 376).
9) 고전적 프래그머티즘을 종합한 존 듀이(John Dewey)에 따르면 프래그머티즘이 말하는 경험은 전통적 경험론이 말하는 감각으로서의 경험이 아니다. 오히려 자연에서 일어나는 모든 것이라 할 만한 것으로, 유기체가 자연과 교섭하는 일련의 상호작용(interaction)과 상호교섭(transaction)의 과정을 경험이라 본다. 여기서 상호작용이란 유기체와 환경 간 맺어지는 통일된 행동의 작용이고, 상호교섭이란 상호작용이 완전히 처리되어 통합된 인식의 과정을 의미한다(듀이, 2020a: 227;김동식, 2002: 162). 이렇게 보면 듀이는 기존의 인식론적 관점을 완전히 폐기했다고 볼 수 있다. 즉, 인식의 대상인 지식(객관적 실재)이 먼저 존재하는 것이 아니라 상호작용과 상호교섭에 따른 유기체의 활동, 곧 행동의 결과로 지식이 획득된다는 것이다. ===
2) 프래그머티즘과 미국의 의학교육: 타일러와 플렉스너
프래그머티즘의 집대성자이자 이를 교육학과 교육철학으로 확대 발전시킨 듀이(John Dewey, 1859-1952)에 따르면 교육이란 “환경에 대한 개인의 적응을 가능하게 하는 습관(habit)을 획득하는 일”로 정의할 수 있다(듀이, 2007: 100). 이는 역으로 말하면 교육을 통해 개인의 습관을 바꿀 수 있다는 것이고, 습관이 바뀌면 그 개인의 본성(nature)도 바뀐다는 것을 의미한다. 실제로 듀이는 습관이 자아를 구성한다고 보았다. 나아가 인간은 이성도 본능도 아닌 습관의 동물이며, 습관이 실제 욕구를 형성하고 활동 능력을 부여한다고 보았다. 이는 곧 인간의 자아가 행동(행위) 과정에서 만들어진다는 것을 의미하며, 역으로 행동에 앞서 미리 정해진 자아 같은 것은 없다는 것을 의미한다(듀이, 2020a;김동식, 2002: 169-170). 이러한 점에서 프래그머티즘은 이미 데카르트적인 불변의 이성 주체를 거부하는 탈근대성의 맹아를 내포하고 있다고 볼 수 있다.
행동을 강조하는 프래그머티즘의 이러한 반(反)사변적 성격은 현대 의학교육의 주류가 된 역량바탕교육의 기원이라 할 수 있는 미국의 교육학자 타일러(Ralph W. Tyler, 1902-1994)에게서도 그대로 드러난다. 그의 주저에서 타일러는 “교육은 인간의 행동 패턴(behavior patterns)을 변화시켜 가는 과정”(Tyler, 1949: 5-6)이며, “학습은 학생의 능동적인 행동을 통해 발생하는 것, 즉 그가 행한 행동에 의한 것이지 교사의 교수 행동에 의한 것이 아니다”(Tyler, 1949: 63)라고 말함으로써 듀이의 철학적 자장 안에 있음을 공개적으로 드러냈다. 실제로 타일러는 듀이의 영향력 아래 형성된 미국 진보주의 교육 운동을 이끌었던 교육학자들의 영향을 많이 받았으며 그들과 깊이 교류하였다(김은정, 2018: 15-18).
타일러가 의학교육 분야에서 중요한 이유는 국내 교육학계의 반복되는 비판에도 불구하고 그의 교육과정 모형이 의학교육계에서는 사실상 무비판적으로 전면 수용되고 있기 때문이다.10)이는 타일러 모형이 교육과정학 분야에서 바이블로 통할 만큼 지금도 여전히 강한 영향력을 행사하고 있다는 사실과 무관치 않다. 실제로 의학교육에 처음 발을 디디게 되면 누구나 타일러가 처음 공식화한 교육과정에 대한 주장, 즉 ‘교육목표의 설정 → 학습경험의 선정 → 학습경험의 조직 → 평가 → 평가 결과를 반영한 교육목표 재설정 및 학습경험 재선정’이라는 순환 구조 모형을 자연스럽게 익히고 당연시하게 된다.11)그러나 교육목표를 절대시하고 학습자의 학습경험을 신성시하는 이러한 타일러 모형의 기본 입장은 그간 많은 비판을 받아 왔다.
=== 10) 국내 교육학계의 비판으로는 다음과 같은 예를 들 수 있다(박채형, 2008; 김학준, 2013; 김은정, 2018; 이홍우, 2018). 심지어 교육과정철학 전공자인 이홍우는 자신의 저서에서 타일러의 교육과정 모형을 가리켜 “미국 교육학의 저주와 재앙”이라는 극한 용어로써 비판하고 있다. 그리고 ‘미국 교육학’이란 “타일러의 ‘교육과정 이론’과 그것을 철학적으로 뒷받침하고 있는 존 듀이의 교육철학, 그리고 양자를 다양한 방면으로 연장 발전시킨 학자들로 구성된 이론적 집합체”라고 규정하고 있다(이홍우, 2018: 1-49).
11) 이 네 가지 요소의 순환 구조를 타일러는 자신의 저서 첫머리에서 교육과정 개발 시의 네 가지 근본적인 질문이라 하여 다음과 같이 공식화하였다.
1. 학교는 어떤 교육목표(educational purposes)를 달성하고자 노력해야 하는가?
2. 이 목표를 달성하기 위하여 어떤 교육경험(educational experiences)이 제공될 수 있는가?
그리고 유감스럽게도 타일러는 저서에서 이 네 가지 질문에 대한 자신의 대답을 제시하지도, 그것에 대해 어떠한 대답이 있는지도 예시하지 않는다(이홍우, 2018: 9). ===
무엇보다도 타일러 모형은 교육을 수단과 목적의 관계로 도식화하였다는 문제가 있다. 즉, 교육이 사전 결정된 교육목표에 의해 주도되어야 한다면수업은 그 교육목표를 달성하기 위해 동원되는 수단에 불과하게 된다는 의미이다. 현재 주류를 점한 역량바탕교육 역시 수업이 사전 결정된 역량(competency)이라는 교육목표를 달성하기 위한 수단이 되고 있다는 점에서 공통된 전제를 공유하고 있다. 물론 타일러나 그의 후계자들이 수업 무용론을 주장한 것은 아니나, 이들의 논리대로라면 효율성의 측면에서 수업보다 우위의 다른 수단이 등장할 경우 수업은 그 대안적인 다른 수단으로 대치될 수밖에 없다(박채형, 2008: 38). 교육목표란 수업의 결과로 달성되는 최종 결과일 뿐인데, 사전 결정된 교육목표가 수업 자체를 압도하고 도구화하는 주객전도의 촌극이 벌어지는 것이다.
그 연장선상에서 학습자의 학습경험을 신성시하는 입장 역시 많은 문제점을 안고 있다. 수업이 교육목표를 달성하기 위한 수단이라고 보는 한, 수업에서 다루어지는 수업내용 역시 수단으로 전락하여 학문적 교과 또는 지식에 내포된 아름다움이 묵살될 위험이 있기 때문이다(박채형, 2008: 44). 현재의 의학 지식이 한시적이라는 지식 자체에 대한 부정적 시각은 교육 내용의 무게 중심을 쉽사리 교수의 지식/학문적 교과에서 학습자의 경험/학습자의 특성으로 이동시킨다. 사실 의과대학에서 어렵게 배운 지식이 졸업 후 의료 현장에서 제대로 활용되지 못하고 있다거나 나아가 쓸모없게 된다는 관점이 의학교육계에 과도하리만큼 팽배해 있다. 이는 자연스레 교수자의 전문성과 중요성을 훼손시키고, 교육목표의 재설정도 교수자가 아닌 외부 전문가에게 넘기는 이른바 ‘교사배제 교육과정(teacher-proof curriculum)’으로 이어질 수밖에 없다.
‘교사배제 교육과정’이란 타일러 모형에 입각한 것으로 “교사라는 변수―교사 개개인의 역량이나 자질, 신념 같은 것―들이 작용할 만한 여지를 배제할 수 있을 정도로 구체적이고 세세하게 계획, 기술되어 있어서 신참이든 경력자든 그 것을 적용하기만 하면 애초 의도했던 대로 동일한 결과가 나올 수 있을 것으로 기대되는 교육과정”을 의미한다(김학준, 2013: 2). 이는 실제 수업뿐 아니라 교육과정 개발 차원에서도 이루어지는 복잡한 정치적, 사회적, 문화적, 인간적 상호작용을 의도적이든 아니든 도외시한 것이라는 점에서 분명한 한계를 안고 있다. 교수자와 수업 및 그 내용이 아닌 교육목표에 입각한 전체 교육과정의 설계라는 행동 절차에 초점을 맞추고 있다는 점에서, 타일러 모형은 학계에서도 ‘통제이론’이라 하여 “실제(practice)에 초점을 두며 교육의 과정(process)에서 효율성을 강조하고 기술공학적인 합리성에 기초하는 이론”이라는 평가를 받고 있다(김은정, 2018: 26).
이는 결과적으로 앞서 말한 미국 프래그머티즘의 부정적 유산, 곧 문제해결을 위한 상황적 효용성이 기계적인 공학적 효용성으로 변질된 결과라 보아야 할 것이다. 그리고 이러한 경향을 그대로 수입한 한국의 현 의학교육계는 그 사상적 뿌리에 대한 천착 없이 교육과정과 관련한 무질서한 공학적 설계만 난무하는 양상을 드러내고 있다. 행동과 실천의 강조가 곧잘 공학적 성과로 귀결되어 버리는 이러한 미국적 현상은 현대 미국 의학교육계에서 가장 중요한 사건으로 꼽는 일명 『플렉스너 보고서(Flexner Report)』의 출간과 그에 따른 사회적 파장에도 그대로 나타난다.
카네기교육진흥재단(The Carnegie Foundation for the Advancement of Teaching)의 위임을 받고 1910년 일명 『플렉스너 보고서』를 작성하여 출간한 플렉스너(Abraham Flexner, 1866-1959)는 타일러와 마찬가지로 교육학자였다. 보고서의 원제인 『미국과 캐나다의 의학교육(Medical Education in the United States and Canada)』이 가리키듯 이 보고서는 미국과 캐나다에 산재한 155개 의학교의 실태를 조사한 것이었다. 플렉스너는 이를 위해 155개 의학교 전부를 직접 현장 방문하여 샅샅이 조사하였고, 그 결과를 담은 보고서의 출간은 놀라운 결과를 가져왔다. 이미 1904년 미국의사협회가 의학교육위원회를 설치하여 의학교 개혁을 최우선 과제로 삼으면서 미국의 의학교 상당수가 폐교되는 조짐을 보이기 시작했으나, 이후 의학교육위원회가 카네기교육진흥재단에 의뢰함으로써 시작된 플렉스너의 조사는 보고서 출간을 계기로 기준 미달의 소규모 상업적 의학교 폐교의 기폭제가 되었던 것이다. 그리하여 1906년 162개였다가 1910년 131개로 감소한 미국의 의학교는 5년 뒤인 1915년에는 95개로 감소했고, 1922년에 이르면 81개로까지 감소했다. 그러나 이는 플렉스너가 보고서에서 31개로의 감축을 건의했던 것에 비하면 한참 못 미치는 결과였다(스타, 2012: 180-186).
의학교 설립 기준이 강화되고, 교육 기간이 연장되고, 교과과정의 일관성이 유지되면서 의사의 질과 수준이 높아졌으나, 급격한 개혁은 그만큼의 부작용도 초래하였다. 우선 의학교육비가 상승했고, 면허를 취득하기 위한 자격조건이 까다로워졌다. 그 결과, 하층 및 노동계급 출신에서 이전과 비교하여 의사가 되기 위한 진입 장벽이 대폭 높아졌다. 또한 이전의 개방적이었던 환경과 달리 여성과 흑인, 유대인에 대한 차별정책으로 의사들의 출신 계층이 백인 남성 부르주아지로 한층 단일화되어 갔다. 이에 더하여 의학교의 감소로 졸업생이 줄어들면서, 플렉스너의 예상과 달리, 빈민촌과 농촌에서 의사가 부족해지는 지역 불균형이 심화되었다. 이에는 의학교육비의 상승도 한몫하였다. 의사가 되기 위한 전체 비용이 상승하자 졸업 후 이를 충당하기 위해 의사들은 진료비를 인상하였고, 인상된 진료비를 감당하기 어려운 지역에서는 의사들이 개원을 회피하였기 때문이다(스타, 2012: 189-192).
의사 사회 내부에서의 비판도 이어졌다. 그것은 기존의 임상의학을 과학적 환원주의를 앞세운 독일식 실험실 의학(laboratory medicine)으로 변환시키려는 데 대한 저항이었다. 플렉스너는 보고서에서 자신이 졸업한 존스홉킨스대학교의 의학교를 의학교육 개혁을 위한 표준으로 삼았는데, 존스홉킨스의학교는 바로 그 연구 중심의 독일식 모형을 채택한 대학이었기 때문이다.12)놀랍게도 당장 존스홉킨스의학교 내부에서 비판의 목소리가 터져 나왔다. 존스홉킨스병원 설립에 기여하였으며 ‘현대 의학의 아버지’라 불리는 오슬러(William Osler, 1849-1919)는“과학을 의학에 적용하는 데는 결코 반대하지 않았으나, 과학적 정신이 의사와 환자 사이에 끼어드는 것에는 강하게 저항했다.” 또한 의학교 교수진을 연구 성과에 따라 임명하면 교수들이 학생과 환자들로부터 멀어질 것이라 경고하면서 플렉스너의 보고서에 근본적으로 반대하였다(토버, 2003: 47-50).
=== 12) 플렉스너는 자서전에서 각 의학교 방문 조사에 착수하기에 앞서 이미 자신의 마음속에 의학 교육의 분명한 원형으로서 존스홉킨스 모형이 자리하고 있었다는 점을 밝히고 있다(Cooke, Irby, O’Brien, 2010: 5). ===
그러나 이러한 소수의 반대 목소리는 이내 묻혀 버렸고, 미국의 의학교육 개혁은 독일식 실험실 의학을 근간으로 한 연구 중심 대학의 추구로 귀결되면서 결국 의사와 과학자의 잡종인 의사과학자(physician scientist) 양성으로 이어졌다. 실증주의와 과학적 환원주의의 물결이 개혁이라는 이름으로 임상의학의 전통적인 인도주의를 압도해 버린 것이다. 플렉스너의 보고서가 이후 미국 의학교육과 의학의 발전에 기여한 부분을 인정하더라도, 이러한 점에서 앞서 타일러 모형의 예에서도 보았던 문제해결을 위한 상황적 효용성이 기계적인 공학적 효용성, 나아가 획일성으로 변질된 프래그머티즘의 부정적 결과를 목도하게 된다. 실제로 플렉스너가 견지한 교육철학 또한 학생들이 기계적인 암기보다는 행동이나 문제해결을 통해 배운다는 듀이의 진보주의 교육철학과 유사한 것이었으며, 이러한 그의 철학이 훗날 미국 의학교육을 변혁시키는 데 적용되었다고 할 수 있다(Duffy, 2011: 270).
3) 프래그머티즘과 미국의 의료시스템과학
지금까지 논의한 바를 토대로 의료시스템과학의 성격과 출현 배경을 검토해 보면, 의료시스템과학의 대두는 지난 한 세기 동안 단단히 유지되어 온 미국의 플렉스너 체제 및 의사과학자 양성 체제를 부정 또는 개혁하려는 의도가 아닌 일개 보완이라는 사실을 깨닫게 된다. 물론 플렉스너 전통의 기존 질병 및 장기 계통별 교과목 중심의 교육과정으로부터 임상 표현 중심, 자기 주도적 문제해결 중심의 통합 교육과정으로의 전환이 미국뿐 아니라 국내에서조차 급속하게 진행되고 있는 상황에서 한 세기 전에 구축된 플렉스너 체제가 현재도 여전히 유효한가라는 질문이 제기될 수 있다. 그러나 플렉스너 체제의 성립부터 이후 현재의 역량바탕교육의 확립에 이르기까지 이 모든 것의 기저에 프래그머티즘의 실리 추구를 위한 공학적 속성이 부정적 유산으로서 자리하고 있다는 것을 알게 된 이상, 이러한 질문은 이제 타당하지 않다. 오히려 앞으로도 플렉스너 체제가 유지, 확장될 수밖에 없는 이유가 무엇인가를 묻는 것이 올바른 질문이 될 것이다.
실례로 2010년 『플렉스너 보고서』 출간 100주년을 맞이하여 카네기교육진흥재단에서는 ‘제2의 플렉스너 보고서’라 할 만한 보고서를 출간하였다.13)이 보고서에서 저자들은 플렉스너 체제를 빛나는 과거라 칭하고이 빛나는 과거가 탁월한 미래를 위한 충분한 안내자가 될 수 있을 것이라면서(Cooke, Irby, O’Brien, 2010: 1) 도입부를 플렉스너 체제의 전개 과정에 대한 역사적 설명에 할애하고 있다. 그러나 이 새 보고서를 살펴보면 플렉스너 체제의 근본적인 폐기를 주장하고 있지 않다. 오히려 반대로 플렉스너 체제의 재조정과 이에 따른 확대 발전을 말하고 있을 뿐이다. 요컨대 새 보고서는 플렉스너 체제의 폐기와 단절이 아닌 성숙한 플렉스너 체제로의 이행을 얘기하고 있다고 보아야 한다. 즉, 빛나는 과거가 곧 탁월한 미래인 셈이다.
이러한 측면에서, 2017년 미국의사협회 교육컨소시엄(AMA Education Consortium)에 의해 공식적으로 첫 모습을 드러낸 의료시스템과학 역시 플렉스너 체제와의 단절이 아닌 심화ㆍ성숙을 의미한다.14)이를 단적으로 보여주는 예가 2017년 출간된 『Health Systems Science』 초판의 5쪽에 실린 두 가지 도식이다(Skochelak 외, 2017: 5). 첫 번째 도식을 가리켜 저자들은 의학교육의 전통적인 ‘두 기둥 모형(two-pillar model)’이라 칭하면서 그 두 기둥을 기초과학(basic science)과 임상과학(clinical science)으로 설정해 놓았다. 이는 곧 과학적 의학을 추구한 현재의 2+2 플렉스너 체제에 해당한다.15)다음으로, 두 번째 도식에 대해서는 의학교육의 새로운 ‘세 기둥 모형(three-pillar model)’이라 칭하면서 기존 두 기둥에 한 기둥을 의료시스템과학(health systems science)이라 하여 새로이 ‘추가’해 놓았다. 기존의 과학적 의학을 그대로 유지한 채 여기에 시스템적 사고(systems thinking)를 연결 고리로 한 의료시스템에 대한 교육과 훈련을 ‘과학’이라는 이름을 붙여 한 축으로 덧붙인 것이다. 의학의 과학화를 추구한다는 점에서는 기존 플렉스너 체제와 전혀 다를 바가 없는 것이다. 의료시스템과학을 가리켜 저자들이 기초과학, 임상과학에 이은 ‘제3의 의과학(the third medical science)’이라 부르고 있는 것이 이를 단적으로 말해 준다(Skochelak 외, 2017: 10).
=== 13) Molly Cooke, David M. Irby, Bridget C. O’Brien, Educating physicians: a call for reform of medical school and residency (Jossey-Bass, 2010).
14) Susan E. Skochelak et al. eds., Health Systems Science (Philadelphia: Elsevier, 2017). 2017년 출간된 이 도서는 미국에서 의료시스템과학의 시작을 알리는 신호탄이 되었다. 4년 뒤인 2021년 벌써 2판이 출간되었으며, 국내에는 2018년에 서평을 통해 초판의 전반적인 내용이 소개된 바 있다(전우택, 2018: 60-61).
15) 미국의 2+2 체제란 의과대학 입학 후 첫 2년간 기초과학과 임상과학을 공부한 뒤 이를 토대로 나머지 2년간 병원에서 임상 실습을 하는 교육 시스템을 가리키며, 미국뿐 아니라 한국의 의학과 4년 역시 이와 같은 시스템으로 운영되고 있다. ===
앞서 필자가 제기한 질문, 앞으로도 플렉스너 체제가 유지ㆍ확장될 수밖에 없는 이유가 무엇인가로 되돌아가 보자. 왜인가? 플렉스너가 19세기 후반의 독일식 의과학 모형을 제시하면서 확립한 ‘의학의 과학화’가 앞으로도 지속될 수밖에 없다는 것이 그 한 가지 답변이다. 19세기까지 의학은 치료라는 측면에서 다른 과학 분야와 비교했을 때 사실상 발전이 없었다. 독일식 실험실 의학의 유산은 그러한 의학의 치료적 비효용성을 실제 효과가 있는 것으로 바꾸어 놓았다는 데에 있다. 구체적으로는 19세기 후반 세균학에서의 혁명적 변화를 가리켜 의학적 지식의 진보가 실제적인 치료적 진보로 이어진 역사적 출발점이라 부를 만하다(우튼, 2007: 9-40). 플렉스너 체제는 그 직후 구축되었다.
치료적 진보라는 측면에서 의학의 진보는 이제 불과 한 세기의 시간이 경과한 데에 불과하다고 할 수 있다. 의학의 인도주의적 요소를 불필요할 정도로 희생시켜 가면서 확립한 과학화, 그리고 그에 기반한 의학교육 체제를 되돌리거나 전환해야 할 확실한 이유를 찾기에는 아직 이른 시간에 해당한다. 그렇다면 의료시스템‘과학’이 희생당한 인도주의의 불씨를 되살릴 수 있을 것인가?
3. 의료시스템과학의 한국 도입 배경과 의도의 정치적 함의
미국의 의료시스템과학이란 “의료시스템 내에서 환자와 인구 집단에 대한 의료 서비스 전달의 질, 결과 및 비용을 개선하는 원리, 방법 및 실행”으로 정의할 수 있다(Skochelak 외, 2017: 11). 그리고 이를 기초과학, 임상과학에 이은 제3의 의과학이라 하여 조직적이고 체계적인 형태로 학생들에게 교육시키겠다는 것이다. 이러한 교육과정이 대두된 이유에 대해 Skochelak 등은 진단 및 치료와 연계된 기초과학 지식의 양적 폭발과 복잡화, 건강과 질병의 생물-정신-사회-환경 모형에 대한 이해의 극적 진전, 그리고 사회적-경제적-정치적 압력 등이 엄청난 데이터와 정보 시스템의 뒷받침 하에 미국 의료의 풍경을 그 사이 극적으로 변화시켰기 때문이라고 설명하고 있다(Skochelak 외, 2017: 5). 간단히 말해서 기존 의사-환자-연구 중심의 과학적 의학 모형, 곧 플렉스너 체제가 의료와 사회의 다변화 및 복잡성 증가로 한계에 봉착하게 되자 이를 보완 또는 타개할 목적으로 특히 사회과학적(예방의학, 사회의학, 의료관리학, 의료사회학 분야를 아우르는) 측면을 도입하고 이를 체계적으로 조직화하여 교육시킴으로써 의사의 전문성을 한층 강화해 나가겠다는 취지이다.
이는 미국 의료의 특성상 이른바 공공성이 사회적으로 한국의 의료 체제보다 뒤떨어져 있는 현실을 감안하면 자연스러운 귀결이라 할 수 있다. 한국은 이미 국가 주도의 전국민의료보험 체제가 갖추어져 있을 뿐 아니라, 의료 자체에 대한 국가의 개입이 미국과는 비교도 할 수 없을 만큼 강력하다. 더욱이 한국의 의과대학은 통칭 예방의학 분야에서 의료시스템과학과 많은 부분 중복되는 영역을 이미 교육하고 있어 의료시스템과학의 풍경이 그리 낯설지 않다. 그럼에도 불구하고 학제(學制)도 상이한 한국의 의학교육계가 미국의 급변하는 의료 현실과 4년제 학제에 맞추어 설계된 의료시스템과학을 서둘러, 그것도 본격적으로 도입하려는 이유는 무엇인가?
프래그머티즘적인 보완재로서의 성격이 강한 의료시스템과학을 도입하려는 이유에 대해 앞서 미국의 저자들이 제시한 복합적인 설명은 미국 의료계의 정황으로선 거의 필연에 가까운 성격의 것이었다면, 한국에서의 설명 방식은 매우 당위적이며 단선적이고 또 정치적이기까지 하다. 가령 의료시스템과학 교육체제 구축 사업을 위해 한국의과대학ㆍ의학전문대학원협회(이하 KAMC)가 제출한 최근의 연구보고서를 살펴보면 연구의 필요성으로 든 첫 번째 이유가 “공공ㆍ지역의료 인력 양성 및 관리를 위한 정부의 다양한 정책 추진이 소기의 목적을 효과적으로 달성하기 위해……”로 서술되어 있다. 그리고 두 번째로 든 이유가 “2020년 의정 사태”이다. “기초의학 및 임상의학 지식, 술기, 태도를 강조하는 전통적인 의학교육 모델에 근거하여 의료와 사회를 통합적 관점에서 이해하고 실천하는 역량과 노력이 정부, 의료계 및 국민 모두 미흡”했음이 이 “의정 사태”(이하 2020년 의사 파업)를 통해 드러났다는 것이다.16)정부의 연구용역보고서임을 감안하더라도 정치적 편향성이 상당한 편이다(한국의과대학ㆍ의학전문대학원협회, 국민건강보험공단, 2021: 3).
2020년 의사 파업은 2000년 의사 파업 이후 20년 사이 발생한 가장 큰 의사와 정부 간 대립이었다. 2000년 의사 파업이 의약분업 시행 여부를 둘러싼 의사ㆍ약사ㆍ정부 간 대립이었다면, 코로나19 팬데믹 와중에 발생한 2020년 의사 파업은 당시 대한의사협회가 규정한 이른바 의료 4대 악법 척결을 명분으로 발생한 의사ㆍ정부 간 대립이었다.17)전자가 개원의 중심의 중년층 의사들 주도로 벌어졌다면, 후자는 전공의 중심의 청년층 의사들 주도로 확대되었다. 쟁점을 둘러싼 이해관계가 서로 달랐기 때문이다.
=== 16) 2020년의 의사 파업을 의료계와 정부가 대립했다는 이유로 흔히 ‘의정 사태’라고 부르나, 전면 파업이라는 점에서는 20년 전 의사 파업 때와 본질이 서로 같다. 따라서 이후 ‘의정 사태’ 대신 ‘2020년 의사 파업’으로 통일해서 칭하고자 한다.
17) 대한의사협회가 규정한 의료 4대 악법이란 한방 첩약 급여화, 원격 의료 추진, 공공의대 신설 추진, 의대 정원 확대 정책을 말한다(김보규 외 70인, 2020: 82-106). 이 가운데 2020년 의정 사태의 핵심 쟁점이 되었던 것은 공공의대 신설 추진과 의과대학 정원 확대 정책이었다(김장한, 김현아, 박형욱, 2021: 32-33) ===
결과적으로 2020년 의사 파업은 의사들이 여론과 언론의 지지를 받지 못한 상태에서, 파업을 주도했던 전공의들이 배제된 채 대한의사협회와 여당인 더불어민주당의 합의로 일단락되었다. 합의서에 따르면 핵심 쟁점이었던 “의대 정원 확대와 공공의대 신설 추진은 코로나19 확산이 안정화될 때까지 관련 논의를 중단하며, 코로나19 안정화 이후 협의체를 구성해 법안을 중심으로 원점에서 모든 가능성을 열어놓고 재논의하기로” 했다. “또한 논의 중에는 관련 입법 추진을 강행하지 않”기로 했다(김장한, 김현아, 박형욱, 2021: 82).
문제는 그 다음부터였다. 정책의 완전 철회나 중단을 요구했던 전공의들과 의대생들 가운데 전공의들은 불가피하게 업무에 복귀한 반면, 의대생들은 의사국가시험 거부라는 단체 행동을 고수했기 때문이다. 국가시험 미응시에 따른 대량 결원 사태는 코로나19 팬데믹 와중에 최전선 의료인력인 인턴의 대량 공백으로 이어짐을 의미하는 것이므로 부담을 느낀 정부도 결국 재응시 기회 부여라는 방식으로 한발 물러났고, 학생들도 우여곡절 끝에 국가시험에 응시하는 것으로 마무리되었다. 그러나 그 과정에서 의사들에 대한 사회적 이미지는 이전보다 더 부정적이 되었고, 특히 청년 의사들과 의대생들의 대사회적 이미지는 세대 논쟁과 연결되면서 한층 부정적이 되어 버렸다.
이를 계기로 의학교육계 내부에서는 상반된 목소리가 터져 나왔다. 하나는 소위 MZ세대 학생들과 전공의들의 이른바 ‘이기주의’에 대한 비판과 불만의 목소리였고, 나머지 하나는 지금까지의 교육이 학생들의 사회화에 도움을 주지 못했으니 새로운 전환을 시도해야 한다는 자성의 목소리였다. 이 가운데 후자를 주장하는 사람들의 시각에 포착된 것이 다름 아닌 의료시스템과학이었다. 이와 동시에 지금까지의 인문사회의학(의료인문학) 교육이 의사의 사회화라는 측면에서 기대에 못 미쳤다는 부정적 시선 및 성급한 재단과 함께 의료시스템, 의료정책, 의료사회학, 리더십 등 사회과학 교육의 필요성에 대한 목소리가 대두되기 시작했다. 그리고 이 모든 것이 코로나19 팬데믹으로 인한 사회적 재난 앞에서 의료의 공공성 및 의과대학 교육의 사회적 책무성 확보를 이유로 합리화 내지 정당화되고 있다.
한편, 더불어민주당 정부는 정부대로 의료의 공공성을 강화한다는 명분으로 2020년 7월 23일 공공의대 신설, 의과대학 정원 확대 정책을 발표하고 시행하려다 곧바로 의사 파업에 부딪혀 정책 추진이 좌절된 바 있다.18)이 실패는 정부가 ‘의사 집단’에 대해 다시 생각해 보게 하는 계기를 마련해 주었을 것이다. 이렇게 보면 미국의 의료시스템과학은 의료의 공공성 확보라는 정부의 입장과 의사에게 결여된 사회적 책무성 함양이라는 의학교육계의 입장 양쪽 모두를 담아낼 수 있는 편리한 그릇이었던 셈이다. 이러한 점에서 국민건강보험공단/정부의 의뢰로 2021년 12월 KAMC/의학교육계 연구팀이 제출한 연구용역보고서 『의료와 사회의 통합적 이해와 실천을 위한 보건의료시스템과학 교육체제 구축 사업』은 그러한 양자의 이해관계가 제대로 부합한 결과물이라 할 수 있다.19)
=== 18) 당정, 의대정원 4,000명 증원ㆍ공공의대 설립 확정」, 『의사신문』, 2020.7.23.
19) 한국의과대학ㆍ의학전문대학원협회, 국민건강보험공단, 『의료와 사회의 통합적 이해와 실천을 위한 보건의료시스템과학 교육체제 구축 사업』 (2021). ===
의료시스템과학의 한국 도입 배경을 살펴보면서 그 정치적 함의가 불순함을 깨닫는 데는 긴 시간이 걸리지 않는다.또한 그로부터 의료시스템과학이 사그라든 인도주의의 불씨를 되살리기에는 역부족이라는 사실도 깨닫게 된다. 그렇다면 의료시스템과학은 기존 인문사회의학(의료인문학) 분야를 대신할 명실상부한 제3의 의과학이 될 수 있을 것인가?
한국에서 의료시스템과학이 2020년 의사 파업이라는 정치적 사건을 계기로 급부상했다면,‘인문사회의학’은 20년 전에 벌어진 한국 최초 의사 파업인 ‘2000년 의사 파업’에 대한 반성적 성찰이 그 직접적 계기가 되어 부상했다. 인문사회의학이라는 용어가 처음으로 공론화된 것도 그즈음으로 의사 파업 3년 뒤인 2003년의 일이다(전우택, 양은배, 2003: 99-103). 그러나 처음부터 명확한 개념 정의가 있었던 것은 아니었다. 다만 그 이전부터 의학계에서 꾸준히 논의되어 왔던 인문학과 사회과학을 배경으로 한 ‘인성교육’ 개념을 확장시켜 “의학과 인문사회과학의 연계 교육 강화”를 통해 “의학 전문가로서 인간과 사회에 대한 깊고 폭넓은 이해를 할 수 있는 능력을 가지도록 교육”하고, “의료가 가진 독특하고도 어려운 문제에 대한 윤리적 고민과 지적인 이해, 그리고 행동에 들어갈 수 있도록 교육”하는 것 등을 인문사회의학 교육 도입의 목적이라 보는 선에서 정리가 되었다(전우택, 양은배, 2003: 36-37, 119).
이러한 최초의 공론화는 2000년대 초 서구 의학계에서 의사의 전문직업성(professionalism)에 대한 논의가 본격적으로 이루어지면서 그 담론의 국내 소개와 더불어 심화되기 시작했다.21)이후 국내 의학교육계는 과학적 의학 모형, 즉 플렉스너 체제를 극복하고자 ‘좋은 의사(good doctor) 만들기’를 의학교육의 궁극적인 목표로 제시하였다(전우택, 김상현, 오승민, 2010: 62). 이에 따라 인문사회의학 교육의 중요성 또한 한층 부각되었으며, 이는 2010년 의학교육 평가인증 기준에까지 반영되어 의과대학의 교육과정을 크게 ‘기초의학, 임상의학, 의료인문학’의 세 영역으로 구성하게 되기에 이르렀다.
=== 20) 4장의 인문사회의학 관련 서술 부분은 2019년 내부 자료로서 발간한 『인제대학교 의과대학 교육요람』 제3판에 실린 필자의 글 가운데 일부의 내용을 보완하고 오류를 수정한 것이다.
그러나 2010년도 의학교육 평가인증 기준에 포함된 ‘의료인문학’이라는 명칭은 개념 정의상 오해와 혼란을 초래할 소지가 다분하였다. 모호하게 “어문학, 사학, 철학, 윤리학, 사회학, 법학, 경영학, 인류학, 심리학, 예술 등의 전공을 의미”한다고만 기술해 놓았기 때문이다(한국의학교육평가원, 2010: 29). 다만 한국에서 인문학이라 하면 대개 협의의 문학, 사학, 철학이 아닌, 자연과학과 대비된다는 의미에서 흔히 사회과학까지 포함하는 광의로 보기도 하므로 이를 반드시 잘못된 정의라 하기는 어려울 것이다(전우택, 김상현, 오승민, 2010: 61).
이상의 기조는 2017년 최초 공개되고 2018년 개정 시행된 최신 의학교육 평가인증 기준(이하 ASK2019)에도 이어져 의료인문학이라는 명칭이 그대로 사용되었다. 그러나 용어상의 혼란을 의식한 까닭인지 의료인문학 교육과정을 다시 “의료인문학, 행동과학, 사회과학, 의료윤리, 의료법규 등”으로 세분화하였다(한국의학교육평가원, 2018: 22). 이는 2015년 세계의학교육연합회(World Federation for Medical Education, 이하 WFME)가 제시한 기본 의학교육 국제 기준(Basic Medical Education WFME Global Standards for quality improvement)을 직접 반영한 결과이다.22)WFME 역시 한국과 마찬가지로 의과대학의 교육과정을 크게 세 영역으로 구분해 놓았는데, 기초의학과 임상의학 영역은 한국과 사실상 동일하지만, 나머지 의료인문학 영역은 한국과 달리 “행동과 사회과학, 의료윤리와 법규(Behavioural and Social Sciences, Medical Ethics and Jurisprudence)”라는 용어 및 내용으로 대신하고 있다. 그리고 행동과학, 사회과학, 의료윤리, 의료법규 이 네 분야가 교육과정에 반드시 포함되어야 한다고 명시하고 있다(World Federation for Medical Education, 2015: 22).
이러한 흐름으로 인해 현재 한국 의과대학의 인문사회의학 교육은 기초의학에 포함시킬 수도 없고 임상의학에 포함시킬 수도 없는 의학의 나머지 전 영역을 포괄하는 것으로 보는 경향이 형성되었다. 심지어 기존 행동과학과 예방의학 관련 교과목까지도 인문사회의학 교육에 포섭되는 결과를 초래하였다. 이러한 경향은 인문사회의학이라는 영역의 모호성을 한층 배가시키는 한편, 삶의 의미를 추구하는 전통적이면서 보다 본질적인 인문학 교육을 의과대학 내에서 더욱 약화시키는 부작용을 낳았다. 더욱이 각 의과대학마다 사용하는 해당 영역의 용어조차 인문사회의학, 인문의학, 의료인문학, 의인문학 등으로 제각각이다 보니 이러한 난맥상이 가중된 상황이다. 이에는 인문사회의학에 대한 개념적 합의가 학계에서든 교육 현장에서든 제대로 이루어져 있지 않은 점도 한몫하였다.
사실 ASK2019에서 사용하고 있는 의료인문학이라는 용어는 ASK2019가 WFME 기준을 본격 도입한 이상, 이제 더는 적절치 못한 것이 되었다고 할 수 있다. 용어와 내용에 따른 이러한 개념적 혼란은 2017년 KAMC가 개발하여 출간한 『기본의학교육 학습성과: 사람과 사회 중심』, 그리고 KAMC가 이를 토대로 현재 출간 준비 중인 가칭 『인문사회의학 교과서』로써 상당 부분 정리될 것으로 보인다. 이 두 책자는 공통으로 의료인문학이 아닌 인문사회의학이라는 용어를 채택하고 있고, 다루는 내용 역시 ASK2019가 제시하는 전 범위를 아우르고 있기 때문이다. 이로써 의학교육계에서 생각하는 인문사회의학은 인문학에 방점을 찍은 의료인문학과는 성격이 다른 것이라는 사실이 아주 분명해졌다. 그 결과 인문사회의학과 의료시스템과학 사이에는 교집합이 형성되었고, 나아가 의료시스템과학 교육이 인문사회의학 교육을 대체할 수 있는 명분이 생기게 되었다.23)
=== 22) ASK2019 자체가 WFME의 기본 의학교육 국제 기준 2015년도 개정판을 근간으로 국내 상황을 고려하여 제작된 것이다(한국의학교육평가원, 2018: ①).
23) 가령 ASK2019가 제시하는 의료인문학 교육과정의 ‘행동과학과 사회과학’에 대한 정의를 보면 WFME의 정의를 그대로 번역한 것으로서 “지역의 요구, 관심과 전통에 따라 공중보건의학, 사회의학, 생물통계학, 국제보건의료, 사회역학, 의료사회학, 의료심리학, 의료인류학, 위생학, 지역사회의학을 포함한다”로 되어 있어 상당 부분 의료시스템과학과 그 내용이 중첩됨을 알 수 있다(한국의학교육평가원, 2018: 22;WFME, 2015: 22). ===
현재 국내외 의과대학의 인문사회의학 교육을 종합 정리하면 크게 두 가지 경향으로 대별할 수 있다. 하나는 직접 의학과 접목한 전문직교육(직업교육) 중심의 경향이고, 다른 하나는 교양과 인성을 강조하는 인문교육 중심의 경향이다. 이 가운데 국내 의학교육계의 주된 경향은 전자로서 미국과 WFME가 주도하고 있으며, 기존 의사의 전문직업성 담론을 확장함으로써 이미 앞서 논한 대로 의사의 역할을 강조하던 이전 관점을 벗어나 환자를 둘러싼 의료환경, 즉 시스템의 역할을 강조하는 쪽으로 크게 선회하였다. 국내 의학교육계에서 인문학보다 사회과학의 중요성이 부각되고 있는 것도 이러한 추세와 무관하지 않다. 그리고 이러한 경향의 정점에 서 있는 것이 바로 미국의 의료시스템과학이다.
그러나 의료시스템과학 교육은 의사로서의 전문직교육의 충실성을 높이는 데는 기여할 수 있겠으나, 한국 의과대학의 교육 실정에는 잘 맞지 않는다는 큰 문제가 있다. 그 이유는 바로 의과대학 학제의 상이함에서 비롯된다. 한국의 의학전문대학원 제도처럼 4+4 학제가 보편화된 미국의 의과대학에서는 의학과 직접 접목된 이러한 의료시스템과학 교육으로의 직행이 타당성을 가질 수 있다. 그러나 이제 거의 모든 의과대학이 6년제로 회귀하여 학제가 의예과 2년과 의학과 4년으로 사실상 단일화된 한국에서는 전문직교육만으로는 부족하다. 미국과 달리 고등학교 졸업 후 바로 의과대학에 진학하는 학생들에게 교양을 중심으로 한 인문학과 사회과학 교육의 제공은 필수일 수밖에 없기 때문이다.24)6년제 학제가 대부분인 유럽의 의과대학들이 미국과 달리 교양 중심의 인문사회의학 교육과정을 운영하고 있는 점이 이를 뒷받침한다(전우택, 김상현, 오승민, 2010: 71).
=== 24) 일제강점기 동안 식민지 조선의 유일한 대학이었던 경성제국대학의 의학부를 예로 들어 보자. 4년제였던 경성제국대학 의학부는 진학 전 반드시 예과 2년 과정을 수료해야 했다(1924년 경성제국대학 설립과 함께 개설된 예과 과정은 1934년부터 3년제로 변경되었고, 1941년에는 2년 반으로 단축되었으며, 1943년부터 다시 2년제로 환원되었다). 즉, 2+4 학제로서 현 한국의 의과대학 6년제 학제와 동일했던 셈이다. 예과 2년 동안 학생들은 외국어 중심의 교양 교육을 이수해야 했다. 구체적으로는 수신, 국어 및 한문, 제1외국어(독일어), 제2외국어(영어), 라틴어, 수학, 물리, 화학, 식물 및 동물, 심리, 도화, 체조 등의 과목을 1학년과 2학년에서 각각 34시간씩 이수했다(기창덕, 1995: 228-229). 요컨대 일제의 식민지 제국대학조차도 의사가 되고자 하는 사람에게는 의학 지식 습득에 앞서 기본적인 교양 지식을 요구했다는 것이다. ===
따라서 한국 의과대학의 인문사회의학 교육은 교양교육 중심의 의예과 교육과정, 그리고 의학과 직접 접목한 전문직교육 중심의 의학과 교육과정 이렇게 두 가지로 개념적인 이원화를 시도할 필요가 있다. 그리고 이러한 추구를 통해 의사라는 직업인이 되기 이전에 삶의 가치와 목적을 찾고 사회 및 세상과 바람직한 관계를 맺을 수 있는 사람과 시민이 되는 데 도움이 되는 전통적인 인문교육의 부활을 기대할 수 있을 것이다. 이는 향후 의예과를 폐지하고 통합 6년제로 의과대학 학제가 개편되었을 때도 유지되어야 함이 마땅하다. 고등교육기관인 대학의 존재 이유는 직업전문학교의 추구 및 단순 기술직의 양산에 있지 않기 때문이다. ASK2019가 WFME 기준을 그대로 차용했음에도 불구하고 WFME 기준에는 없는 별도의 ‘의료인문학’ 분야를 계속 유지한 데에는 이러한 이유도 작용했을 것이라 사료된다(한국의학교육평가원, 2018: 22).
20여 년 전 발생한 의사 파업의 결과에 대한 고민에서 비롯된 인문사회의학 분야가 이제야 비로소 자리를 잡아가고 있는 가운데, 불과 2년 전 발생한 제2의 의사 파업에 대한 의ㆍ정 이해관계의 일치에 따라 선택된 의료시스템과학, 그것도 미국식 4+4 학제에 최적화되어 있는 의료시스템과학 교육을 착종 과정 없이 그대로 수입하여 기존 인문사회의학 분야를 대체하고자 했을 때 과연 어떠한 부작용이 발생할지는 그 누구도 섣불리 예단할 수 없다.
5. 나오는 말: 어떻게 해야 하는가?
플렉스너의 과학적 의학 체제에서 의학은 곧 과학이다. 한국에서 기초의학이 사실상 몰락하다시피 한 현 상황에서도 미국보다 50여 년이나 뒤진 의사과학자 양성을 위해 근래 이와 관련한 공론화의 바람이 불고 있는 것만 보아도 알 수 있는 일이다. 서구 의학이 과학의 힘을 빌려 주류 의학의 위치를 점한 것은 역사적 사실이며, 과학의 힘을 빌려 질병 치료 분야에서 크나큰 진전을 보인 것 역시 분명한 사실이다. 그러나 과학적 의학의 질병 중심주의가 환자/사람 소외 현상을 초래한 것 또한 부정할 수 없는 사실이다. 그리고 이를 보완할 목적으로 의학의 역사, 철학, 윤리, 법, 문학, 예술 등을 교육하고 연구하는 통칭 인문사회의학 분야가 국내에도 등장하기에 이르렀다.
다시 처음으로 돌아가 보자. 의학은 단순하게 과학으로만 볼 수 있는 영역이 아니다. 감각이 없는 물질을 대상으로 한 수학과 물리학 중심의 일반적인 자연과학 분야가 아니라, 희로애락과 생로병사의 생명현상을 가진 환자/사람을 대하는 분야이기 때문이다. 직접 사람/생명을 대하는 분야이므로 과학만으로 해결할 수 없는 영역과 지점이 돌출하는 분야이다. 이러한 까닭에 고전적인 히포크라테스의 ‘선서’ 역시 원문을 확인해 보면 의(醫)에 접근할 때 학문이나 지식으로서의 의학(醫學, medical science) 외에 기술이나 행위로서의 의술(醫術, medical art), 그리고 덕목이나 윤리로서의 의덕(醫德, medical virtue)이라는 삼중적인 차원에서의 접근을 취하고 있다. 이 가운데 의학은 이론적 측면이, 의술은 실천적 측면이, 의덕은 도덕적 측면이 강하다(반덕진, 2006: 62-67). 의과대학에서 역량바탕교육에 따른 학습평가를 시행할 때 흔히 지식(knowledge), 술기(skill), 태도(attitude)라는 세 가지 측면을 모두 고려하여 학생의 역량을 평가하고자 하는 것도 이러한 의학의 전통적인 삼중적 측면 때문이 아니겠는가?
그럼에도 의학은 곧 과학이라는 편견이 지금도 강하게 작용하고 있는 이유는 적어도 한국에서는 의학이 소위 이과 학문이라는 선입견 때문일 것이다. 그러나 의학이 이과 학문이라는 근거는 사실 그 어디에도 없다. 인문ㆍ사회과학과 자연과학을 문과, 이과라는 프레임으로 양분하는 작위적 방식은 그 제도를 메이지(明治) 시기에 처음 시행한 일본과 그 영향을 직접 받은 식민지 조선 및 한국 등 동아시아에서 주로 통용되는 방식이기 때문이다.25)그렇다고 플렉스너 체제에서 의학이 과학을 기반으로 하고 있다는 사실이 곧 의학이 이과 학문이어야 할 근거가 되지도 못한다. 앞서 ‘선서’의 예를 들지 않더라도 굳이 분류를 하자면 오히려 의(醫)로서의 의학이야말로 애초 이과, 문과 구별이 불가능한 타고난 융합학문이기 때문이다.
=== 25) 메이지 44년인 1911년 7월 제정된 고등중학교령(칙령 제217호) 제4조를 보면 “고등중학교의 학과를 나누어 문과 및 이과로 한다(高等中學校ノ學科ヲ分チテ文科及理科トス)”라고 나온다. 김성근은 이것이 고등중학교 과정을 문과와 이과라는 큰 범주로 나눈 최초의 칙령이었던 것으로 보인다고 하였다(김성근, 2021: 209). ===
의학은 중세 유럽의 대학에 의학부가 설치되면서 항구적인 학문으로서의 길을 열게 되었다. 대학에 제도적 기반을 마련하게 된 의학은 타 학문 분과들과도 긴밀히 연결될 수 있었다. 이는 대학 출신 의사 공동체의 영향력을 오늘날까지 제도적으로 보장해 주는 결과를 가져왔으며, 사회적 신분 상승의 계기 또한 마련됨으로써 전문직으로 나아가는 토대를 구축할 수 있었다(린드버그, 2009: 529-536). 그러한 역사적 토대 위에서 의학은 플렉스너 체제 등의 과학화를 통해 치료적 학문으로서 실질적인 진보를 이룩해낼 수 있었고, 이로써 의사들은 전문화와 함께 더 높은 신분 상승도 이루어낼 수 있었다. 현대 의학은 과학이라는 학문을 토대로 실제적인 치료적 효과를 발휘하는 좋은 의학이다. 이 좋은 의학을 앞으로도 계속 유지하고자 한다면 과학 이외에 인간학으로서의 의료와 그 의료를 행하는 좋은 의사라는 존재가 반드시 요구된다. 의료시스템과학은 적어도 한국에서는 이러한 의(醫)의 통합적 측면을 달성하기에는 여러 가지로 부족한 ‘과학’이다.
한국에서 현재 의료시스템과학이란 실체 없는 유령이나 다름없다. 그것도 어느 날 갑자기 출현한 뿌리 없는 유령이다. 한국의 의료시스템을 이해하는 데 미국의 의료시스템‘과학’ 전부를 이식해 올 필요는 없다. 정치적 이해관계에 따라 무조건 이식부터 하고 보자는 식의 성급함보다는 한국화된 학문적, 교육적 시스템에 대한 역사적 선이해와 함께 이에 따른 면밀한 보완이 더 시급한 것 아닐까 싶다. 이러한 점에서 의료시스템과학이 미국처럼 제3의 의과학으로서 전면에 나서 거대 프레임을 구축하려 하기보다는 기존 인문사회의학 분야의 성숙을 보완하는 보완재로서의 역할을 담당하는 것이 더 타당한 수순일 것이다. 그리고 이것이 프래그머티즘의 부정적 자장에 포섭된 한국의 미국식 의학교육이 보여주는 교육과정의 공학적 설계에 대한 강박에서 벗어날 수 있는 하나의 길이라 생각한다.
This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted noncommercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Abstract
Recently, Korean medical education circles have proposed a fullscale introduction of America’s health systems science to replace the existing medical humanities education in Korea. The so-called Flexner education system, formed in the early 20th century, was centered on basic and clinical sciences. America’s health systems science education was introduced to supplement the system. The full-scale introduction of health systems science has been promoted, mainly by the Korean Association of Medical Colleges. However, it does not fit into the current circumstance of Korean medical education circles. It is deemed that there are political reasons behind the push – the alignment of interests between the medical education circles and the government.
This study first examined the social and cultural circumstances behind the emergence of health systems science in America, focusing on pragmatism, a native American ideology, to critique the background of the introduction of the American system. It also discussed the negative aspects of pragmatism in American medical education in the cases of American educators Ralph Tyler and Abraham Flexner. Then, it specifically examined the background and reasons for introducing America’s health systems science to Korea and discussed the problems of directly introducing the health systems science to Korea without any adaptation process through a comparative analysis with existing medical humanities. Finally, it suggested a more desirable adaptation form of health systems science that can be considered for its implementation in Korea.
모든 이해관계자를 위한 핵심 역량 평가 프로그램 만들기: 선박 설계와 건조에서 얻을 수 있는 것( Adv Health Sci Educ Theory Pract.2020) Building a core competency assessment program for all stakeholders: the design and building of sailing ships can inform core competency frameworks W. Dale Dauphinee1,2
유럽 산부인과학회 및 산부인과학대학(EBCOB)의 반 데르 아아(van der Aa) 등은 Advances 최신호에서 대학원 임상 교육에서 핵심 역량 기반 의학교육을 설계하는 데 필요한 대안 전략을 제시했습니다(반 데르 아아 등, 2019). 가장 중요한 것은 제목에서 알 수 있듯이 논리적이고 상향식 방식으로 진행되었다는 점입니다: 처방에서 지침까지: 일반 역량을 위한 유럽 프레임워크. 지난 20년 동안 의학교육 문헌에서 역량 교육에 대해 방대한 분량을 할애한 것을 감안할 때, 왜 처음부터 다시 시작했을까요? 그 이유는 역량 기반 교육(CBE) 및 평가(CBA)를 둘러싼 현장의 혼란스러운 상황에 대한 훌륭한 소개에 잘 설명되어 있습니다. 이는 특히 대학원 임상 교육에서 더욱 그렇습니다. 이에 대응하여 그들은 교육자를 전문 분야별로 안내하도록 설계된 단계별 경로를 개략적으로 설명했으며, 더 쉬운 학습과 더 많은 창의성을 위한 유연성을 거의 제공하지 않는 CBE 및 CBA의 경직된 목표를 사용하는 것을 피했습니다. 특히 산부인과(OB-GYN) 역량 기반 교육의 핵심 문제를 관리하고 구현하는 방법에 초점을 맞추기 위해 두 가지 주요 이니셔티브에 착수했습니다. 첫째, 의료 기관의 기본 운영 핵심 또는 기술 구조 내에서 일하는 의료 전문가들 사이에서 변화를 도입하고 확립하기 위한 모범 관리 사례를 검토하고 확인했습니다. 둘째, 다양한 일선 이해관계자와 대상 전문가들의 더 넓은 시각을 통해 산부인과에 필요한 일반적인 역량에 대한 보다 포괄적이고 새로운 초상을 포착하기 위해 액션 리서치 결과를 활용하여 새로운 프레임워크에 정보를 제공하고 채웠습니다. 두 가지 모두 축하드립니다. In the current issue of Advances, van der Aa et al. from the European Board and College of Obstetrics and Gynaecology (EBCOB) have presented a needed and alternative strategy for designing core competency-based medical education in post-graduate clinical training (van der Aa et al.2019). Most importantly, they have proceeded in a logical and bottom up manner, as clearly implied in the title:From Prescription to guidance: a European framework for generic competencies. Given the vast number of pages devoted to competency education in the medical education literature over the last two decades, why have they started from scratch? The reasons are well described in their excellent introduction on the muddled state of the field surrounding competency based education (CBE) and assessment (CBA). This is particularly true in graduate clinical training. In response, they have outlined a step-wise pathway designed to guide educators in a specialty specific manner and avoided using rigid objectives for CBE and CBA that offer little flexibility for easier learning and more creativity. Critically, they undertook two major initiatives in order to focus on how to manage and implement core issues in competency-based education in Obstetrics and Gynecology (OB-GYN). They reviewed and identified the best management practices for introducing and establishing change amongst health professionals working within the basic operative core or the technostructure of health care institutions. Secondly, they have looked through the wider lens of various front line stakeholders and targeted professionals to capture a more inclusive and refreshing portrait of the generic competencies needed in OB-GYN by utilization the results of action research to inform and populate a new framework. Congratulations on both counts.
그러나 제 의견을 공식화하고 뒷받침하는 데 도움이 되도록, 저는 예전에 목조 범선을 건조하고 장식하던 부모님의 가족으로부터 빌린 비유를 제시하고 싶습니다. 모든 이해관계자의 요구와 기대를 충족하기 위해 실제 일상 세계에서 작동해야 하는 제품이나 서비스를 만들려는 모든 이니셔티브와 마찬가지로, 목조 범선을 만드는 과정에는 여러 개별적이지만 서로 연결된 단계가 포함됩니다. 이러한 모든 단계는 성공적인 결과와 원하는 효과를 얻기 위해 필수적입니다.
즉, 선박의 주요 목적을 가장 적절하게 달성할 수 있도록 설계 및 건조하고(속도를 내기 위해 좁거나 큰 하중을 싣기 위해 넓게),
바람을 최적으로 포착하기 위한 '도구'로서 돛대, 리깅 및 돛을 설계 및 설치하며,
마지막으로 각 설계 가정과 후속 실행의 신뢰성과 타당성을 모두 검증하기 위해 해상 시험을 실행하는 것입니다.
궁극적인 목표는 설계자와 건조자가 이해관계자가 의도한 선박에 대한 비전과 열망을 충족했음을 입증하는 것입니다(Herreshoff 1974).
However, to help formulate and undergird my comments, I want to offer a metaphor borrowed from my parents’ families as builders and outfitters of wooden sailing ships in earlier times. Like any initiative in which one seeks to create a product or service that has to function in the real everyday world in order to meet all stakeholder’s needs and expectations, the creation of a wooden sailing ship involved several discrete but interconnected steps. All of these steps are essential for a successful outcome and the desired impact. They are:
design and build the ship to most appropriately achieve its primary purpose (narrow for speed or wide for large loads),
design and install the masts, rigging and sails as ‘instruments’ to optimally capture the wind; and
lastly execute the sea trials to validate both the reliability and validity of each of the design assumptions and their subsequent execution.
The ultimate goal is demonstrate that the designers and builders have met the stakeholders’ intended vision and aspirations for the ship (Herreshoff1974).
선박 건조 프로세스에는 평가 프로세스 및 도구 구축에 직접적으로 영향을 미치는 특징이 있습니다. 새로운 설계는 일반적인 역량에 대한 이전의 시도에서 쉽게 드러나지 않았던 이슈와 문제를 정의하고 명확히 해야 합니다. 은유는 비교뿐만 아니라 중요한 통찰력도 제공합니다. 은유는 일련의 프로세스가 표현되는 방식에 관한 것입니다. 따라서 각 단계가 프로젝트의 전체 여정에 필수적인 아이디어나 품질을 상징하고 더 나은 결과와 더 큰 영향력을 얻기 위해 어떻게 진행하고자 하는지에 대한 스토리를 제공하기 위해 은유가 선택됩니다. The ship building process has features that directly bear on the building of assessment processes and tools. A new design must define and clarify issues and problems that were not readily apparent in earlier attempts at generic competencies. The metaphor provides comparisons but also important insights. A metaphor is about how a set of processes is expressed. Thus, a metaphor is chosen to offer a story, within which each step symbolizes an idea or quality that is essential to the project’s overall journey and how they intent to proceed to a better outcome and greater impact.
저자의 접근 방식 The authors’ approach
반 데르 아아의 글은 이 새로운 전략을 성공적으로 마무리하기 위해 해결해야 할 일련의 개발 문제 중 첫 번째 단계에 대해 설명합니다. 아직 해야 할 일이 많이 남아 있습니다. 예를 들어, 핵심 역량을 파악하는 아이디어는 새로운 것이 아닙니다. 1999년에 미국의학전문위원회(ABMS)와 미국의학전문대학원교육인증위원회(ACGME)는 ABMS 역량 유지 프로그램 및 대학원 교육 수련 프로그램 인증의 기반이 될 6가지 핵심 일반 역량을 공동 승인하면서 이 개념을 장려했습니다. 6개의 광범위한 역량을 일련의 평가 요소로 분해한 다음 일련의 도구로 재구성해야 한다는 개념은 큰 도약이자 위험한 일이었습니다. 품질 개선을 지원하는 인프라를 구축하지 않으면 이러한 형식은 '제도화'는 되지만 '전문화'는 되지 않는 경향이 있습니다(Audet 외. 2005). 목록과 규칙만으로는 충분하지 않습니다. The van der Aa article describes the first step in a cascade of developmental issues that must be addressed in moving this new strategy to a successful conclusion. Much more remains to be done. For example, the idea of identifying core competences is not new. In 1999, the American Board of Medical Specialties (ABMS) and the Accreditation Council for Graduate Medical Education (ACGME) promoted the concept with their joint endorsement of six core general competencies to serve as the bases for the ABMS Maintenance of Competence program and for the accreditation of post-graduate education training program. The notion of six broad competencies having to be deconstructed into set of assessment elements and then reconstructed into a set of tools was a major leap and risky. Without the building of infrastructure to support quality improvement, such formats tend to be ‘institutionalized’ but not ‘professionalized’ (Audet et al.2005). Lists and rules are not enough.
그러나 EBCOB 개발의 경우, 저자들은 행동 연구를 사용하여 일반적인 역량 프레임워크를 개발했습니다. 연구팀은 이해관계자 매핑을 활용하여 이해관계자 그룹과 협력하여 네 가지 영역을 식별했습니다.
환자 중심 치료,
팀워크,
시스템 기반 진료,
개인 및 전문성 개발
그러나 각 영역에서 '지침'을 제시하기보다는 이해관계자가 파악한 '요구사항'의 예를 설명하여 평가자가 '지침 표준'을 현지 상황에 적용할 때 더 나은 지침을 제공할 수 있도록 했습니다. 또한 평가자가 현장에서 재창조하고 창의적으로 적응할 수 있는 기회를 제공하기 위해 네 가지 영역을 일반적인 용어로 설명했습니다. 이 전략이 주는 시사점은 무엇인가요? However, in the case of EBCOB development, the authors used action research to develop a guiding generic competency framework. Utilizing stakeholder mapping, the research team worked with the stakeholder groups to identify four domains. They were
patient- centered care;
teamwork;
systems-based practice; and
personal and professional development.
However, under each domain, rather than offering ‘directives’, they described examples of the stakeholder’s identified ‘needs’ so as to offer better guidance to assessors when applying the ‘guiding standard’ to local contexts. Furthermore, the four domains were described in general terms so as to offer the evaluators the opportunities for re-invention and creative adaptation in the field. What are the implications arising from this strategy?
세 가지 즉각적인 과제가 있습니다. 프레임워크가 프로그램 디렉터, 학습자 및 교수진을 위해 최적으로 작동하려면 표준 보고 형식, 데이터 시스템 및 성과 데이터 수집을 위한 대시보드 액세스(예: 표준화된 항해 차트와 항해 육분계 및 기압계 데이터)를 설계하고 구현하는 것이 필수적입니다. 교수진을 준비하고 교육하기 위한 교수진 개발 프로그램과 연계된 품질 관리 프레임워크가 분명히 필요할 것입니다. 또한 학회와 이사회는 교수진이 사용할 수 있는 용어집과 허용되는 시험 형식을 제공할 수 있도록 해야 합니다. 저와 제 동료들은 품질 관리의 중요성과 핵심 역량 기반 교육 이니셔티브의 변경 사항을 감독하는 책임 있는 기관의 필요성을 설명했습니다(도피니 외. 2019). 우리는 모든 평가 노력의 장기적인 지속 가능성을 보장하기 위해 더 나은 품질 관리를 가능하게 하는 경로와 프레임워크를 제공했습니다. 우리도 이러한 다음 개발과 현장 테스트('해상 시험')를 기대할 것입니다. There are three immediate challenges. The design and implementation of standard reporting formats, data systems and access to dashboards for the collection of performance data (i.e. standardized navigation charts plus data from navigation sextants and barometers) is essential if the framework is to function optimally for the program directors, the learners and teaching staff. Clearly a quality control framework, in association with a faculty development program to prepare and train the faculty, will be needed. That will also require the Society and Board to ensure that a glossary of terms and acceptable testing formats will be available for the teaching faculty. My colleagues and I have described the importance of quality control and having a responsible authority overseeing any changes in core competency-based education initiatives (Dauphinee et al.2019). We offered pathways and frameworks to enable better quality control to ensure long-term sustainability of any evaluation endeavour. We too will look forward to these next developments and their field testing (‘sea trials’).
고려해야 할 다른 과제 Other challenges that should be considered
그러나 최근 역량 모델에 고려되지 않은 또 다른 위협이 있습니다. 의사의 번아웃 문제는 대학원 교육과 개업 의사 커뮤니티에서 우려할 만한 문제가 되었습니다. 미국 의학 연구소(IOM)의 최근 보고서인 '임상의 소진에 대한 조치 취하기'를 참고하세요: 전문직의 웰빙을 위한 체계적인 접근법이라는 보고서는 전문직의 모든 분야에서 관심을 기울일 것을 요구합니다(미국 과학, 공학 및 의학 아카데미 2019). IOM 보고서의 저자들은 의사 소진의 증가를 20년 전 '인간은 실수할 수 있다' 및 '질적 격차' 보고서의 결과와 동일한 수준의 대중적 관심사 및 조치의 필요성에 놓았습니다. 이 문제는 미국에만 국한된 것이 아닙니다. 이 비극적인 상황과 가능한 전략을 다루는 데 있어 반 데어 아아 보고서와 직접적인 연관성이 있습니다. However, there is another recent threat to any competency model that has not been considered. The challenge of physician burnout has become a worrisome issue within post-graduate education and the practicing physician communities. The recent report of the Institute of Medicine (IOM),Taking Action Against Clinician Burnout: A Systematic Approach to Professional Well-Being,demands the attention from all sectors of the profession (National Academies of Sciences, Engineering, and Medicine2019). The IOM report’s authors have placed the rise in physician burnout on the same level of public concern and need for action as the findings from theTo Err is Humanand theQuality Chasmreports of 20 years ago. The issue is not confined to the USA. In addressing this tragic development and possible strategies, there is a direct link to the van der Aa paper.
EBCOB의 프레임워크에 따르면 네 가지 일반 역량 중 하나는 '개인 및 전문성 개발'입니다. 기본 원칙 중 두 가지는 '일과 삶의 균형'과 '개인의 역량과 한계 인식'입니다. 이해관계자 및 기타 전문가를 대상으로 한 액션 리서치 조사를 통해 이 핵심 역량을 파악한 것은 1990년부터 1998년까지 제가 컨설팅 자문위원으로 참여했던 온타리오 의사의 미래 교육(EFPO) 프로젝트를 떠올리게 합니다. 이 보고서에서는 의료 전문가, 커뮤니케이터, 협력자, 건강 옹호자, 학습자, 관리자("게이트키퍼"), 학자, "인격체로서의 의사" 등 미래의 의사에게 필요한 8가지 핵심 역할을 확인했습니다(Neufeld 외. 1998). 이러한 역할은 문헌 검색, 이해관계자, 환자, 그리고 의사와 학생에 대한 구조화된 인터뷰를 기반으로 확인되었습니다.25년 전의 인터뷰와 연구는 다른 사람을 돕고 치유하는 전문가로서의 의사의 역할 외에도 한 인간으로서의 의사의 역할이 중요하다는 것을 시사했습니다. 이는 주목해야 할 주요 관심사였습니다. 실제로 EFPO 보고서는 온타리오주 의과대학에 졸업생들이 인격체로서의 의사를 포함한 이러한 역할을 수행할 수 있도록 홍보하고 준비하도록 했습니다. 나중에 캐나다 왕립 의사 및 외과의사 대학에서 이러한 역할을 CanMEDS 역할에 맞게 조정할 때 원래 이해관계자의 의견에도 불구하고인간로서의 의사는 삭제되었습니다. CanMDES 역할 프레임워크는 국제적으로 널리 채택되었지만, 현재CanMDES웹사이트의 '인격체로서의 의사'는 '전문가로서의 의사' 아래에 '환자 치료를 촉진하기 위해 의사와 건강 및 복지에 대한 헌신을 보여야 한다'는 작은 언급을 제외하고는 다시 나타나지 않고 있습니다.
Under the EBCOB’s framework, one of the four generic competences is ‘personal and professional development’. Two of the underlying the guiding principles are ‘balance work and life’ and ‘recognize personal competencies and limits’. The identification of this core competency from the action research enquiry of stakeholders and other professionals is reminiscent of Future Education of Physicians for Ontario (EFPO) project, for which I was a consulting advisor from 1990 to 1998. The report identified eight (8) core roles for the physician of the future: medical expert, communicator, collaborator, health advocate, learner, manager (“gatekeeper”), scholar, and “physician as person” (Neufeld et al.1998). Of interest, the identification of these roles was based on literature searches, structured interviews of stakeholders, patients, and of course, physicians and students. The interviews and research from 25 years ago suggested that the physician, as a person, was important, in addition to the physician roles as expert to help and heal others. It was a major concern in need of attention. In fact the EFPO report committed the faculties in Ontario to promote and prepare their graduates for these roles, including physician as a person. Later, when the these roles were adapted by the Royal College of Physicians and Surgeons of Canada for the CanMEDS roles, physician as person was dropped despite the original stakeholder input. The CanMEDS roles framework was widely adopted internationally, but its current version on the CanMEDS Web-site, ‘physician as person’, has not reappeared, except for a small reference under ‘physician as professional’ to ‘demonstrate a commitment to physician and health and well-being to foster patient care’.
의사의 소진이라는 주요 문제와 그에 따른 다른 사람들이 인격체로서의 의사에 대한 원래의 잘 연구된 EFPO 역할에 주의를 기울이지 않는 것을 고려할 때, EBCOB 팀은 일반적인 '개인 및 전문성 개발' 역량을 다시 검토할 수 있을 것입니다. 이 영역이 새로운 도전 과제인 의사 및 전공의의 소진과 중도 탈락 문제를 해결하는 데 어떻게 사용될 수 있는지 고려할 수 있는 기회가 될 것입니다. IOM 보고서는 임상의의 소진과 직업적 웰빙에 대한 시스템 모델을 제안하며, 이를 고려할 가치가 있습니다. 분명 시스템 문제도 중요하지만, 최근 유럽의 산업보건 문헌에서 직무-제작에 관한 Bakker와 동료들의 연구도 앞으로 고려할 가치가 있습니다(Tims 외. 2013). 직무 제작은 인사 고문이나 멘토가 직원이 자신의 업무나 책임 또는 직장 내 다른 사람들과의 상호 작용을 맞춤화할 수 있는 수단을 고려할 수 있는 접근 방식입니다. 조직은 보건 직종을 포함하여 직무의 의미를 높이고 성과를 개선하기 위해 직원들에게 직무 제작을 수행하는 방법을 교육할 수 있습니다. 따라서 보건 서비스에서 개인의 역할이나 업무를 재설계하는 것은 하향식 직위 재설계에 대한 좋은 대안이며 유연성과 창의성이 더 높은 EBCOB 전략에 잘 맞을 수 있습니다. 앞으로 더 많은 규제와 더 많은 책임이 요구되는 상황에서 더욱 중요해질 것으로 보입니다. 더욱 실망스러운 것은 현장 테스트가 제대로 이루어지지 않은 인공지능 '보조 장치'가 의사의 개인 임상 루틴에 점점 더 많이 침투하고 있다는 점입니다. EBCOB 핵심 역량을 새롭게 살펴보는 것은 수련의가 자신의 업무 환경을 재정의하고 더 잘 통제할 수 있는 능력을 강화할 수 있는 추가적인 학습 전략을 고려할 수 있는 기회입니다. 이러한 후자의 고려 사항은 미래의 유럽 의사들에게 흥미롭고 생산적인 기회가 될 수 있습니다. Given the major issue of physician burnout, and the subsequent failure of others to heed the original, well studied EFPO role on physician as person, the EBCOB team may want to revisit the generic ‘personal and professional development’ competency. It would be an opportunity to consider how this domain might be used to address an emerging challenge—the physician and post- graduate trainee problems of burnout and drop-out. The IOM report proposes a systems model of clinician burnout and professional well-being that deserves consideration. Clearly systems issues are important, but the recent work of Bakker and colleagues on job-crafting in the occupational health literature in Europe also deserves consideration going forward (Tims et al.2013). Job crafting is an approach wherein personnel advisors or mentors can consider the means by which an employee can customize their tasks or responsibilities or interactions with others at work. Organizations can train their staff on how to undertake job crafting to increase their meaning and improve their performance, including in the health professions. Thus, the redesign of an individual’s roles or tasks in the health services is a good alternative to top-down position redesign and could fit nicely within the EBCOB strategy more flexibility and creativity. It would seem to be even more important in the future with more regulations and more accountability demands. Even more frustrating is the increasing penetration of artificial intelligence ‘aids’, often inadequately field tested, into the physician’s personal clinical routines. A fresh look at the EBCOB core competencies is an opportunity to consider additional learning strategies to amplify trainees’ abilities to redefine and take more control of their work environment. These latter considerations could be exciting and productive for the future physicians of Europe
결론적으로 이 보고서는 지속적인 전략 개발의 첫 번째 단계이며, 이를 위해 훌륭한 출발점이라고 할 수 있습니다. 기기 개발('장비 및 돛')과 현장 테스트('해상 시험')를 통해 아직 더 많은 작업이 필요한 문제가 밝혀진 후에도 이 이니셔티브를 개선할 기회가 더 많이 있습니다. 모든 규제 기관의 모토는 대중을 보호하고, 남녀노소를 막론하고 전문직을 선도하는 것이어야 합니다. As a concluding comment, this report is the first step in an on-going strategic development, and to that end, it is an excellent start. There are many more opportunities to improve the initiative after instrument development (‘rigging and sails’) and after field testing (‘sea trials’) reveal what issues still need more work. Their mantra should be that of all regulatory organizations: protect the public and guide the profession, young and old.
Adv Health Sci Educ Theory Pract. 2020 Mar;25(1):189-193.doi: 10.1007/s10459-020-09962-1.Epub 2020 Feb 6.
Building a core competency assessment program for all stakeholders: the design and building of sailing ships can inform core competency frameworks
1Clinical and Health Informatics Research Group, Division of Clinical Epidemiology, Department of Medicine, McGill University, 1140 Pine Avenue West, Montreal, QC, H3A 1A3, Canada. dale.dauphinee@mcgill.ca.
2Foundation for Advancement of International Medical Education and Research, Philadelphia, PA, USA. dale.dauphinee@mcgill.ca.
When educators are developing an effective and workable assessment program in graduate medical education by employing action research and stakeholder mapping to identify core competency domains and directives, the multi-stage process can be guided and informed by utilizing the story of designing, building and sea-testing sailing ships as a metaphor. However, the current challenge of physician burnout demands additional attention when formulating medical training frameworks, assessment guidelines and mentoring programs in 2020. The possibility of job-crafting is raised for consideration by designers of core competency frameworks in the health professions.
장미의 다른 이름: Lawrence 등의 잠재 교육과정 스코핑 리뷰에서 몇 가지 흥미로운 점(Acad Med, 2018) A Rose by Other Names: Some General Musings on Lawrence and Colleagues’ Hidden Curriculum Scoping Review Frederic W. Hafferty, PhD, and Maria Athina Martimianakis, PhD
이번 학술 의학 호에서는 로렌스와 동료들이 숨겨진 커리큘럼과 의학교육에 대한 생각을 자극하는 광범위한 검토를 제공합니다.1 이들은 지난 25년 동안2,3 보건 전문직 교육의 학습 환경을 구성하는 모든 임상 및 비임상 맥락과 프로세스에 걸쳐 분석 도구로 활용되어 온 숨겨진 커리큘럼(HC)에 대해 다룹니다. 이 해설에서는 로렌스와 동료들의 데이터와 결론을 바탕으로 네 가지 문제를 다룹니다.
첫째, "이 용어는 뚜렷하고 보편적인 정의가 부족한 것 같다"는 검토 결과와 이러한 '모호성'이 다양한 방법론적 및 개념적 문제에 미치는 영향에 대한 관련 우려를 다루며, 이 모든 것이 HC에 대한 보다 명확한 정의의 통일성을 요구하는 개선 요구로 이어지며, 우리는 특별한 근거에 따라 이의를 제기합니다.
둘째, 우리는 숨겨진 HC 문헌의 존재를 문서화하고, HC와 유사한 분석 프레임워크를 사용하거나 HC 효과를 조사하지만 이 용어를 직접 언급하지 않는 연구에 어떻게 대처하는 것이 가장 좋은지 묻습니다. 최소한 이러한 저급 문헌의 존재는 범위 검토에서 "범위"가 무엇인지에 대한 시사점이 있습니다.
셋째, 로렌스와 동료들의 검토와 밀접한 관련이 있는 두 가지 출판물을 살펴봅니다.
첫 번째는 맥레오드의 HC에 대한 비평으로,4 로렌스와 동료들이 범위 검토의 존재 이유를 스스로 밝힌 것입니다.
두 번째, 마르티미나키스와 동료들의 HC 범위 검토2는 로렌스와 동료들의 검토 초기에 언급되었다가 더 이상 언급되지 않고 사라졌습니다.
두 리뷰 모두 동일한 개념을 탐구하지만 서로 다른 관점에서 다소 다른 결론을 내리고 있기 때문에 이러한 조기 누락은 유감스럽지만, 우리가 강조하고자 하는 차이점은 다음과 같습니다.
마지막으로, 우리는 '이론적 충실성'의 문제와 한 학문적 전통이나 패러다임(예: HC)에서 개발된 이론적 틀이 다른 학문 영역으로 가져올 때 어떻게 개념적 변형을 겪을 수 있는지, 그리고 그러한 변형이 이러한 변형을 생성하는 문화에 대해 무엇을 말할 수 있는지(그리고 어떻게 유익할 수 있는지)를 다룹니다.
In this issue ofAcademic Medicine, Lawrence and colleagues provide a thought-provoking scoping review of hidden curricula and medical education.1They address the hidden curriculum (HC), which for the past quarter century,2,3has been deployed as an analytic tool across the full range of clinical and nonclinical contexts and processes that make up the learning environments of health professions education. In this Commentary, galvanized by Lawrence and colleagues’ data and conclusions, we address four issues.
First, we tackle the review’s finding that “the term seemed to lack a distinct and universal definition,” along with related concerns as to the impact of such “ambiguity” on a variety of methodological and conceptual issues—all leading to a remedial call for more definitional uniformity regarding the HC, a conclusion we challenge on particular grounds.
Second, we document the existence of ahiddenHC literature and ask how best to deal with work that uses an HC-like analytic framework or that examines HC effects, yet never directly mentions the term. At minimum, the existence of this hypogean literature has implications for what is “scoped” in scoping reviews.
Third, we touch on two publications closely linked to Lawrence and colleagues’ review.
The first, a critique of the HC by MacLeod,4is the self-identified raison d’être for Lawrence and colleagues’ scoping review.
The second, an HC scoping review by Martimianakis and colleagues,2is mentioned early in Lawrence and colleagues’ review only to disappear without further mention.
This early disappearance is regrettable because both reviews explore the same concept, but from different vantage points and with somewhat different conclusions—differences we seek to accentuate.
Finally, we tackle issues of “theoretical fidelity” and how a theoretical framework developed within one scholarly tradition or paradigm (such as the HC) might undergo conceptual mutation when imported into another domain of scholarly work, and what such transmutations might say about (and how they may benefit) the culture that generates these alterations.
다른 이름의 장미 A Rose by Other Names
HC가 "모호하고 보편적으로 사용되는 것 같다"는 결론과 함께, 보다 통일된 정의 기반으로 이동하여 이러한 어휘의 과잉을 억제해야 한다는 권고가 로렌스와 동료들의 검토의 핵심입니다. 우리는 이들의 기본 연구 결과를 지지하면서도 여러 측면에 문제를 제기합니다. 우리는 학습 환경이 공식 커리큘럼과 함께 상호 작용과 영향력의 복잡한 그물망을 형성하는 다양한 숨겨진 커리큘럼으로 구성된다는 Lawrence와 동료들의 결론에 동의합니다. 또한 '숨겨진 커리큘럼'이라는 단수 표현을 사용하면 이 중요한 구조적 사실을 모호하게 만들 수 있다는 데 동의합니다. 그럼에도 불구하고 이론적으로 말하자면, 저희는 이 개념에 특이점이 내포되어 있지 않으며, 내포된 적도 없다고 생각합니다. 오히려 그 존재론적 뿌리는 시간적, 공간적 다양성을 구체적으로 가정하는 인식론적 접근을 요구합니다. 따라서 HC 현상은 어디에나 존재하며 단수로 지칭할 수 있지만, 그 발현은 다양하고 역동적일 것으로 예상됩니다. 측정 문제를 중심으로 도출된 유사한 결론은 Haidet과 동료들에 의해 반복적으로 언급되었습니다.5,6 The conclusion that the HC suffers from “ambiguous and seemingly ubiquitous use,” along with recommendations to curb such lexiconic excesses by moving to a more uniform definitional foundation, is central to Lawrence and colleagues’ review. We support, yet also take issue with, different aspects of their underlying findings. We concur with Lawrence and colleagues’ conclusion that learning environments are composed of a multiplicity of hidden curricula, which, together with the formal curriculum, form a complex web of interactions and influence. We also agree that use of the singular (“hidden curriculum”)mayobscure this important structural fact. Nonetheless, and now speaking theoretically, we believe the concept does not, and never has, implied singularity. Instead, its ontological roots demand an epistemological approach that specifically assumes temporal and spatial diversity. Thus, while the phenomenon of the HC is ubiquitous and can be referred to in the singular, its manifestations are expected to be numerous and dynamic. A similar conclusion, generated around measurement issues, has been noted repeatedly by Haidet and colleagues.5,6
우리는 또한 HC 개념(단수이든 복수이든)을 사용하는 학문이 조사 대상을 정의할 필요가 있다는 데 동의합니다. 따라서 우리는 로렌스와 동료들이 검토한 논문 중 21%(197편 중 41편)만이 "'숨겨진 교육과정'이라는 용어에 대한 직접적인 정의를 포함하지 않았고", 포함된 논문 중 17%(33편)만이 이 개념(숨겨진 교육과정과 비공식 교육과정)을 동의어로 사용했다는 사실을 발견하고 고무되었습니다(낙담하지 않았습니다). 논문의 결론을 고려할 때 그 비율은 더 높을 것으로 예상했습니다. 또한 로렌스와 동료들의 범위 검토에서 이 17%가 이 두 개념 사이의 "점점 더 모호해지는" 경계 때문이라는 결론을 뒷받침하는 데이터를 찾지 못했습니다.
We also agree that scholarship employing the HC concept (singular or plural) needs to define what is being examined. As such, we were encouraged (not discouraged) to discover that only (our “only”) 21% of the articles in Lawrence and colleagues’ review (41 of 197) “did not include a direct definition for the term ‘hidden curriculum’” and that even less, 17% or 33, of the included articles used the concepts (hidden and informal) as synonyms. Given the article’s conclusions, we thought the percentages would be higher. We also did not locate data in Lawrence and colleagues’ scoping review supporting the conclusion that this 17% was due to an “increasingly blurred” line between these two concepts.
셋째, 우리는 의학교육 장학의 환경이 HC 명명법으로 가득 차 있다는 로렌스와 동료들의 의견에 동의합니다. 우리 중 한 명(F.W.H.)은 HC 작업에서 접하는 용어에 대한 실행 로그를 작성하고 있습니다. 현재까지 이 목록에는 "공식적인" 교육과정을 지칭하는 데 사용되는 9개의 용어(예: "공식", "명시적", "성문화된")와 학습 환경의 공식적이지 않은 측면을 다루는 29개의 용어가 포함되어 있습니다.7 그러나 우리에게 중요한 문제는 용어의 확산이 아니라
(1) 용어가 어떻게 적용되는지,
(2) 어떤 문제를 다루는지,
(3) 사용 중인 용어가 적절하게 정의되어 있는지입니다.
9개의 공식적인 용어들 사이에는 실질적인 정의상의 차이는 없지만(따라서 상호 교환적으로 사용하는 데 문제가 거의 없음), 29개의 '공식적이지 않은' 프레이밍 사이에는 상당한 차이가 있음을 알 수 있습니다. 로렌스와 동료들이 지적했듯이 비공식 교육과정과 HC 사이에는 중요한 차이점이 있으며, 예를 들어 무형식null 교육과정과 같은 다른 개념들 사이에도 추가적인 차이점이 있습니다.2 Third, we agree with Lawrence and colleagues that the landscape of medical education scholarship is littered with HC nomenclature. One of us (F.W.H.) keeps a running log of terms encountered in his HC work. To date, this list includes 9 terms that are used to refer to the “formal” curriculum (e.g., “official,” “manifest,” “codified”) along with a breathtaking 29 covering the other-than-formal aspects of learning environments.7The central issue for us, however, is not the proliferation of terms but, rather,
(1) how they are applied;
(2) what issue(s) they address; and
(3) whether the term(s) in play is adequately defined.
Although we see no real definitional distinctions among the 9 formal terms (and thus have little issue with their interchangeable use), we do see substantial differences among the 29 “other-than-formal” framings. As noted by Lawrence and colleagues, there are important distinctions between the informal curriculum and the HC—as well as additional dissimilitudes across other concepts, including, for example, the null curriculum.2
그러나 로렌스와 그의 동료들과는 달리, 저희는 대체 또는 대안적 HC 프레임을 사용하는 것이 개념적으로 활력을 불어넣고 풍요롭게 한다는 것을 발견했습니다. 또한 중요한 것은 다른 프레임워크가 검토 범위 설정에 중요한 시사점을 제공한다고 생각합니다. 이 두 가지 요점을 설명하기 위해 로렌스와 동료들의 범위 검토에 '적용'된 연구와 그렇지 않은 연구 두 가지를 살펴봅니다.
전자는 Balmer와 동료들이 수행한 연구로,8 "의대생이 교과목 목표를 학습하기 위해 명시적 교과과정, 암묵적 교과과정, 교과외적 활동의 상호 작용을 어떻게 탐색하는가"를 이해하고자 했습니다.
후자의 똑같이 도발적인 연구인 Ginsburg 등의 연구9는 '거부된 커리큘럼'이 직업적으로 어려운 상황에서 학생들의 추론에 어떤 영향을 미치는지 이해하고자 했습니다.
In contrast to Lawrence and his colleagues, however, we find the use of alternate or alternative HC framings to be conceptually energizing and enriching. Also, importantly, we believe the other framings have important implications for scoping reviews. In speaking to both points, we turn to two studies: one that “made it” into Lawrence and colleagues’ scoping review and one that did not. The former, a study by Balmer and colleagues,8sought to understand how “medical students navigate the interplay of explicit curricula, implicit curricula, and extracurriculato learn curricular objectives.” The latter, an equally provocative study by Ginsburg et al,9sought to understand how the “disavowed curriculum” influenced students’ reasoning in professionally challenging situations.
Balmer 등은 왜 "명시적", "암시적", "교과외적"라는 용어를 사용했고, Ginsberg와 동료들은 왜 "거부된"이라는 용어를 사용했을까요? 저희는 저자들을 대변하는 척하지는 않지만, 각각의 개념이 저자들이 조사하고자 하는 문제를 최적으로 탐구할 수 있게 해주었고, 그렇게 함으로써 데이터가 밝혀냈다고 생각하는 바를 가장 잘 표현할 수 있었다고 가정합니다. 그러나 우리 앞에 놓인 문제는 저자들이 선택한 용어를 선택하면서 우리를 혼란의 길로 인도했는지 여부입니다. 저희는 그렇지 않다고 생각합니다. 오히려 저자들은 고도로 제도화되고 일상화된 교육 관행의 '체계적 부작용'10과 '예상치 못한 결과'11에 대한 우리의 집단적 이해를 풍부하게 했다고 생각합니다. 발머와 긴즈버그가 보다 제한된 개념에서 출발했다고 주장하는 것은 우리가 지지할 만한 답이 아닙니다. HC 현상에 대한 단일한 이해나 진실은 결코 존재할 수 없습니다. Why did Balmer et al employ the terms “explicit,” “implicit,” and “extra,” and why did Ginsberg and colleagues turn to “disavowed?” Although we do not pretend to speak for the authors, we assume that the respective concepts allowed the authors to explore optimally the issue(s) they wished to investigate and, in so doing, best express what they thought the data revealed. The issue before us, however, is whether, in selecting the terms they selected, the authors took us down a garden path of bewilderment. We think not. Instead, we believe that these authors enriched our collective understandings of the “systematic side effects”10and the “unanticipated consequences”11of highly institutionalized and routinized educational practices. Insisting that Balmer et al and Ginsberg et al draw from a more restricted set of concepts is not an answer we would endorse. There can never be a singular understanding or truth about HC phenomena.
마지막으로, Balmer와 동료들의 연구8가 이 범위 검토에 포함되었음에도 불구하고(범주 레이블로 "암시적"을 사용했기 때문에), Ginsburg와 동료들의 연구9는 포함되지 않았음에도 불구하고(세 가지 트리거 용어인 숨겨진, 암시적, 비공식적 모두를 피했기 때문에), 우리는 둘 다 "HC 연구"로 간주하며, 이 결론은 로렌스와 동료들의 검토 측면에서 Ginsberg와 동료들의 연구를 잘못된 부정으로 만드는 것은 우연이 아닙니다. Finally, in spite of the fact that Balmer and colleagues’ study8was captured in this scoping review (because of its use of “implicit” as a category label) and Ginsburg and colleagues’ study9was not (because it eschewed all of the three trigger terms: hidden, implicit, informal), we consider both to be “HC studies”—a conclusion which not-so-incidentally makes Ginsberg and colleagues’ study a false negative in terms of Lawrence and colleagues’ review.
앞의 단락에서 두 가지 중요한 자격 요건과 관련 논거를 살펴봤습니다. 첫째, HC 현상에 대한 모든 연구가 이러한 일반적인 이론적, 방법론적 틀에 속하기 위해 '숨겨진 커리큘럼'(또는 커리큘럼)이라는 용어를 사용해야 하는 것은 아닙니다. 예를 들어, 모든 참가자가 그룹 문제에 대한 대안적 해결책이 공식적인 규칙의 테두리를 벗어난다는 사실을 (연구를 통해) 충분히 알 수 있는 경우에도 해결 방안에 대한 연구를 HC 연구로 간주하는 것이 적절하고 개념적으로도 풍부하다고 생각할 수 있습니다. 이러한 유형의 일탈을 추구할 때 발생하는 상호주관성은 사회적 행위자가 자신의 사회적 지위를 손상시키지 않으면서 규칙을 어디까지, 어떤 맥락에서 구부릴 수 있는지에 대한 암묵적인 이해와 관련이 있습니다. 이 가상의 예에서 우리가 요청하는 것은 가상의 저자가 우회 방법을 실행하는 미시적인 사회적 상호작용을 "숨겨진" 것이 아니라 "비공식적인" 것으로 언급했다는 점입니다.
The preceding paragraph brings us to two important qualifications and related arguments. First, not all studies of HC phenomena need to use the term “hidden curriculum” (or curricula) to fall within this general theoretical and methodological framework. For example, we would consider it appropriate, as well as conceptually enriching, to imagine a study on workarounds to be an HC study, even when it is abundantly clear (from the study) that all participants share understandings that their alternative solution to a group problem stands outside the boundaries of what the formal rules say should be taking place. The intersubjectivity generated from the pursuit of this type of deviancy relates to implicit understandings of how far and in what contexts social actors can bend the rules without compromising their social standing. All we would ask, in this hypothetical example, is that the fictional authors refer to themicrosocial interactions of executing the workaround as “informal” rather than “hidden.”
둘째, 이와 관련하여 로렌스와 그의 동료들처럼 연구자들이 프로젝트를 "HC 연구"라고 명명했음에도 불구하고 숨겨진 것이 아니라 비공식적인 사회적 관행에 대한 연구를 접한 적이 있습니다.3 그러나 이러한 관행이 위에서 언급한 것처럼 이 개념이 공식적인 사회적 과정과 공식적이지 않은 사회적 과정 사이의 단절 가능성을 사고하고 방법론적으로 탐구하기 위한 일반적인 조직 프레임워크이자 휴리스틱한 고안으로 기능할 수 있다는 사실을 바꾸지는 않습니다.3 이러한 탐구가 이루어지는 방식과 현상의 특정 뉘앙스를 분류하는 방식은 다양해야 한다고 주장합니다. 사회 역학의 복잡성은 이러한 이질성과 다양성을 보장합니다.
Second, and related, we, like Lawrence and his colleagues, have encountered studies of social practices that are more informal than hidden even though the investigators have marqueed the project as an “HC study”3; however, this practice does not change the fact that the concept—as noted above—can function as a general organizing framework and a heuristic devise for thinking about and methodologically exploring the potential for disjunctures between formal and other-than-formal social processes.3How this exploration takes place and how particular nuances of the phenomenon are labeled, we argue, should be varied. The complexity of social dynamics warrants such disparateness and diversity.
숨겨진 HC 문학 The Hidden HC Literature
앞서 논의한 내용을 고려할 때, 독자들은 세 가지 벡터를 따라 숨겨진 HC 연구의 사례를 고려해 보시기 바랍니다. 첫째, 긴즈버그와 동료들의 연구에서도 알 수 있듯이,9 관련 연구는 비정상적, 대안적 또는 전자연적 개념을 사용했다는 이유로 주어진 범위 검토에 포함되지 않을 수 있습니다. 로렌스와 동료들이 배포된 개념의 범위를 제한하라는 요구는 개념적 풍요로움의 손실을 초래할 수 있다고 생각합니다. 우리는 이론적 구성의 한계와 다양한 맥락에서의 적용 가능성을 명확히 하는 등 이론적 구성에 대한 지속적인 비교를 통해 한 분야의 개념적 성장이 제한되기보다는 촉진된다고 믿습니다. Given our preceding discussion, we invite readers to consider the case ofhiddenHC studies—and to do so along three vectors. First, and illustrated by Ginsberg and colleagues’ study,9pertinent studies might not be included in a given scoping review by virtue of having used an aberrant, alternative, or preternatural concept. The call by Lawrence and colleagues to restrict the range of concepts deployed would, in our view, fuel a loss of conceptual richness. We believe a field’s conceptual growth is facilitated—rather than limited—by an ongoing comparison of theoretical constructs, including the articulation of their limits and applicability in different contexts.
두 번째 유형의 숨겨진 HC 문헌은 다른 곳에서 언급된 바 있으며3, 겉으로 드러나는 모든 목적이 장르 외부에 있는 작품으로 구성됩니다. Campbell과 동료들의 전국적인 의학 전문직업성 설문조사12가 그 예입니다. 조사 결과 중 저자들은 의사들이 "일반적으로 제안된 전문직 규범에 동의"하지만 "보고된 행동이 ... 항상 그러한 규범에 부합하는 것은 아니었다"고 지적합니다.12 이 결과는 HC와 직접적인 관련이 있지만, 저자들은 HC를 개념으로 전개하지 않았고, 의학교육 문제, 문화적 전달의 한 형태인 역할 모델링 또는 직업 정체성 형성, 사회화 및 학습 환경과 같은 관련 이슈로 논의를 확장하지도 않았습니다. 데이터를 고려할 때 합법적으로 그렇게 할 수 있었을까요? 물론입니다. 그럼에도 불구하고 그들은 그렇게 하지 않았고, 이것이 바로 이 연구가 "숨겨진" HC 연구인 이유입니다. 또한 이 연구는 다른 연구들과 함께13,14 전통적으로 조직화된(즉, 키워드 기반) HC 범위 검토로는 포착되지 않는 연구입니다. A second type of hidden HC literature has been mentioned elsewhere3and consists of work that for all apparent purposes stands outside the genre altogether. Campbell and colleagues’ national survey of professionalism in medicine12is an example. Among their findings, the authors note that although physicians “generally agree with proposed professional norms,” their “reported behavior … did not always conform to those norms.”12Although this finding has direct HC implications, the authors did not deploy the HC as a concept, nor did they extend its discussion to issues of medical education, to role modeling as a form of cultural transmission, or to related issues such as professional identity formation, socialization, and the learning environment. Might they have legitimately done so given their data? Absolutely. Nonetheless, they did not, and this is why this study is a “hidden” HC study. It also is a study, along with others,13,14that would not be captured by a traditionally organized (i.e., keyword-based) HC scoping review.
다른 곳에서 HC 개념을 사용해 본 연구자를 포함하여 HC 개념에 친숙한 연구자라도 자신의 주장에 가장 적합하다고 생각되면 사용을 포기할 수 있습니다. 우리가 보기에, 파워포인트 슬라이드, 역량 및 화면 읽기가 의료 학습 환경에서 어떻게 "완벽한 인지 폭풍"을 구성하는지에 대한 Wear의 분석15은 특히 문제를 구성하고 데이터를 해석하는 방식을 고려할 때 HC 논문이라고 할 수 있습니다. 캠벨과 동료들의 연구와 마찬가지로,12 Wear의 분석은 전통적으로 조직화된(즉, 키워드 기반의) HC 범위 검토로는 포착되지 않으며, 심지어 Wear의 다른(그리고 더 공식적으로 태그가 지정된) 논문16,17이 Lawrence와 동료들의 범위 검토에 포함되었습니다. 우리는 사회생활의 공식적 차원과 공식적이지 않은 차원 사이의 근본적인 차이에 관심이 있는 연구자는 '캠벨식' 및 '웨어식' 연구를 접할 때 열린 '범위 지정 마인드'를 유지해야 한다고 생각하며, 이는 공식적으로 그렇게 분류된 논문만 존재할 수 있다고 믿는다면 일어날 수 없는 일이라고 생각합니다. Even researchers intimately familiar with the HC concept, including those who have used it elsewhere, can forego its use when they feel their arguments are best served by doing so. In our view, Wear’s analysis15—of how PowerPoint slides, competencies, and screen reading constitute a “perfect cognitive storm” within medical learning environments—is an HC article, particularly given how Wear frames her problem and interprets her data. Like Campbell and colleagues’ study,12Wear’s analysis would not be captured by a traditionally organized (i.e., keyword-based) HC scoping review—even as other (and more formally tagged) articles by Wear16,17made the cut for Lawrence and colleagues’ scoping review. We believe that researchers who are interested in the underlying distinction between formal versus other-than-formal dimensions of social life need to keep an open “scoping mind” when encountering “Campbellesque” and “Wear-like” studies, which cannot happen if they believe that the only HC articles that can exist are those formally labeled as such.
셋째, HC에 대한 연구 이전에도, 그리고 지금도 계속되고 있는 풍부한 이론적 프레임워크와 개념적 도구가 있습니다. 의학교육 문헌에서는 HC를 교육 분야의 초기 연구로 추적하는 경향이 있지만, 이 개념은 사회학 분야, 특히 케임브리지(매사추세츠) 학계와 더 밀접하게 연관되어 있습니다.
우리가 알고 있는 가장 초기의 HC 관련 문헌은 1965년 하버드 박사 학위를 받은 프레드 스트로트벡(Fred L. Strodtbeck)18의 보고서/출판물이며, 이후 1970년대 초에 "중산층 가정의 숨겨진 교육과정"에 대한 연구가 하버드 논문과 논문으로 다수 발표되었습니다.3
한편, 매사추세츠 애비뉴에서 1마일 반 거리에 있는 매사추세츠 공과대학(MIT)의 벤슨 스나이더 교수19는 1960년대에 MIT와 웰즐리 대학의 학생 학습 전략을 비교 분석하는 데 기초가 될 데이터를 수집하기 시작했으며, 이를 '숨겨진 커리큘럼'이라고 제목을 붙였습니다.
하버드 대학원생 시절에 발표된 로버트 K. 머튼의 예상치 못한 결과 이론11(1936년), 표면적 기능과 잠재적 기능에 대한 그의 후기 연구,20 그리고 의학교육의 사회학에 대한 그의 획기적인 연구(학생-의사)21 등 여러 하버드 학생 및 교수진의 사회학적 연구와 HC의 관계는 더욱 밀접한 관련이 있으며, 여기서 그는 현대 의학 HC 장학금에서 비공식적이고 숨겨진 교육과정의 전달의 핵심으로 널리 알려진 역할 모델링 개념을 도입했습니다.
1961년(이번에는 북쪽으로 3마일 떨어진 곳에서) 시카고 대학의 사회학자 에버렛 C. 휴즈가 터프츠 대학에 도착했습니다. "공식적인 교육"과 "병동 경험" 사이의 격차를 강조한 휴즈의 간호교육에 대한 초기 연구22는 간호교육이 오랫동안 집중해온 "이론-실무 격차"23에 대한 기초를 형성하는 데 도움이 되었으며, 이는 HC와 강력한 개념적 연관성을 지닌 개념입니다. 우연히도 휴즈는 1950년대 말과 1960년대 초에 의학교육에 관한 두 번째 주요 연구인 하워드 베커와 동료들의 Boys in White를 수행할 연구팀의 멘토가 되기도 했습니다.24
Third, there is a wealth of theoretical frameworks and conceptual tools that precede—yet continue to surround—work on the HC. Although the medical education literature tends to trace the HC to earlier work in the field of education, the concept has more proximal linkages to the field of sociology, in particular to the Cambridge (Massachusetts) academic community.
The earliest HC reference we are aware of is a 1965 report/publication by Fred L. Strodtbeck,18a Harvard PhD, whose study of “the hidden curriculum in the middle class home” was followed by a scattering of Harvard theses and dissertations during the early 1970s.3
Meanwhile, a mile and a half down Massachusetts Avenue, Massachusetts Institute of Technology (MIT) professor Benson Snyder19began collecting data in the 1960s that would form the basis of his comparative analysis of student learning strategies at MIT and Wellesley College—something he titledThe Hidden Curriculum.
More proximal still are the HC’s ties to sociological works by several Harvard students and faculty, including Robert K. Merton’s (1936) theory of unanticipated consequences11(published as a Harvard graduate student), his later work on manifest versus latent function,20and his landmark study on the sociology of medical education (The Student–Physician),21in which he introduced his concept of role modeling, a vehicle widely identified within contemporary medical HC scholarship as core to the transmission of informal and hidden curricula.
In 1961 (and this time three miles to the north), former University of Chicago sociologist Everett C. Hughes arrived at Tufts University. Hughes’ early studies on nursing education,22which highlighted the gap between “formal instruction” and “ward experience,” would help form the basis for nursing education’s long-standing focus on the “theory–practice gap”23—a concept with strong conceptual linkages to the HC. Not so incidentally, Hughes also mentored the research team that would carry out the second major study of medical education in the late 1950s and early 1960s, Howard Becker and colleagues’Boys in White.24
우리의 전반적인 요점은 맥락적 민감성과 포용성입니다. HC를 명시적으로 식별하거나 명시적으로 라벨을 붙인 작품으로 제한하면 HC에 대해 많은 것을 배울 수 있지만, 너무 적게 배울 수도 있습니다. 사회과학, 교육, 간호 분야에서 HC와 유사하고 HC에 대한 정보를 제공하는 풍부한 연구는 특히 학습의 공식적 차원과 공식적이지 않은 차원, 그리고 보다 일반적으로 사회생활 사이의 춤에 대한 이해에 기여합니다.25 우리는 연구자들이 용어를 정의하고 변수를 명확하게 조작해야 한다는 Lawrence와 그의 팀 및 MacLeod4 의 의견에 동의하지만, 개념 어휘를 제한하는 것이 이 저자들이 지적한 문제에 대한 해결책이라고 생각하지 않습니다. Our overall point is one of contextual sensitization and inclusiveness. Although one can learn a great deal about the HC by limiting oneself to works that explicitly identify or expressly label the HC, one also can learn too little. A wealth of work within the social sciences, education, and nursing that is HC-like and HC-informing contributes to our understandings of the dance between formal and other-than-formal dimensions of learning specifically, and social life more generally.25Although we concur with Lawrence and his team and MacLeod4that researchers should define their terms and clearly operationalize their variables, we do not feel that restricting the conceptual lexicon is a solution to the problems identified by these authors.
두 가지 주요 논문 Two Key Articles
위에서 언급한 바와 같이, 맥레오드4 논문은 저자들이 스코핑 검토의 존재 이유를 스스로 밝힌 것입니다. 따라서 이 논문을 다시 살펴봄으로써 로렌스와 공동 저자들이 도출한 결론에서 왜 그리고 어떻게 벗어나는지 더 잘 설명하고자 합니다. 맥리드는 이 개념에 문제를 제기하기 위해 다음과 같은 여러 가지 도발적인 문제를 제기합니다:
(1) 한때 '급진적'이고 '혁명적'이었던 개념이 시간이 지나면서 어떻게 '보편적'이 되었는지,
(2) 한때는 숨겨져 있었지만 지금은 '쉽게 인식되는' 현상을 '비공식적'으로 분류해야 하는지, 아니면 공식적인 교육 환경의 일부로 분류해야 하는지;
(3) '숨겨진 커리큘럼'이라는 단일 명칭은 잘못된 명칭이며, 우리가 분석하고자 하는 것은 여러 개의 '숨겨진 커리큘럼'으로 개념화하는 것이 가장 적합하다는 점,
(4) 그녀가 가장 중요한 문제라고 밝힌 것은, "특정 관행에 '숨겨진'이라는 이름을 붙인 후과"이다. 즉, 그러한 '숨겨진' 이라고 명명함으로써, 그 명칭이 어떻게 행동에 대한 책임을 "스스로 부인하게" 할 수 있는지이다.
As noted above, the MacLeod4article stands as the authors’ self-identified raison d’être for their scoping review. We thus revisit this article to better outline why and how we depart from the conclusions drawn by Lawrence and coauthors. In seeking to problematize the concept, MacLeod raises a number of provocative issues, including the following:
(1) how a once “radical” and “revolutionary” concept may have become “commonplace” over time;
(2) whether a phenomenon once hidden, but now “handily recognized,” should be categorized as either “informal” or perhaps even part of the formal educational landscape;
(3) how the singular (hidden curriculum) is a misnomer, and that what we seek to analyze is best conceptualized as multiple “hidden curricula”; and
(4) what she identifies as her most important issue, “the consequences of naming a particular practice ‘hidden’”—including how such a label might “allow us to disavow ourselves of responsibility” for action.
저희는 위의 모든 내용에 동의합니다. 특히 마지막 문제, 즉 어떤 것을 '숨겨진'이라고 명명하는 것이 어떻게 손댈 수 없거나 심지어 존재하지 않는 상태로 격상시킬 수 있는지에 대해 흥미를 느낍니다. 맥레오드가 제기한 문제 외에도, 누가 '숨겨진 것'을 범위를 벗어난 것으로 분류할 수 있는 권한을 가지고 있으며, 그러한 관행으로 인해 누가 이득을 볼 수 있는지에 대해서도 질문합니다. 이 과정에서 어떤 종류의 특권과 권력이 (재)생산될까요? 실제로 우리는 미시적인 과정을 통해 무언가를 '손댈 수 없는 것'으로 만드는 행위를 HC 효과로 연구할 수 있다고 주장할 수 있습니다. 맥레오드는 다른 주장과 마찬가지로 "우리 의학교육계는 문제가 되는 [HC] 관행을 파악하는 데 탁월한 성과를 거두었다"고 결론을 내리고, 따라서 오늘날의 필요성은 "만연한 교육 문제, 즉 실제로는 그렇게 숨겨져 있지 않은 것들"을 해결하는 것이라고 말합니다. 또는 지금까지 표적이 되어온 문제와 관련 개선 노력이 특권을 반영하고 있는 것은 아닌지 궁금합니다. 보건 전문직 교육 내에서 권력과 특권이라는 보다 근본적인 문제가 계속해서 방해받지 않고 도전받지 않고 방치되고 있는 것일까요?
We agree with all of the above. We are particularly intrigued by the last issue, how the labeling of something as “hidden” might elevate it to the status of untouchable or even nonexistent. In addition to the issues MacLeod raises, we also ask, Who has the power to label something “hidden” as out-of-bounds, and who benefits from such practices? What kinds of privilege and power are (re)produced in this process? Indeed, we would argue that the act of rendering something “untouchable” through micro processes can be studied as an HC effect. In line with her other arguments, MacLeod concludes that “we in medical education have done a superb job in identifying the problematic [HC] practices,” and thus, she continues, today’s need is to address the long list of “pervasive educational issues—the things that really aren’t so hidden.” Alternatively, we wonder if what has been targeted thus far, along with related remedial efforts,reflectsprivilege? Do the more fundamental issues of power and privilege within health professions education continue to lie undisturbed and unchallenged?
HC 개념의 광범위한 사용은 이 용어가 더 광범위한 사회정치적 관계에 어떻게 연관되어 있는지 해체할 필요가 있다는 신호라는 결론을 내렸기 때문에(이 용어를 완전히 추방하라는 요구가 아니라) 로렌스 팀은 MacLeod4 논문과 마르티미나키스 및 동료들의 범위 검토를 연결할 수 있었습니다.2 마르티미나키스 팀2은 HC 구조를 의사 휴머니즘과 명시적 또는 묵시적으로 연결한 6개의 의학 교육 저널에 발표된 200건의 논문을 확인했습니다. 그러나 로렌스 팀과는 달리, 저자가 특정 HC 정의를 적용하지 않았더라도 HC 현상을 언급한 논문도 포함했습니다. 마르티미나키스와 공동 저자들은 전통적인 분류학적 접근법(범위 검토와 일치하는)을 넘어 비판적 담론 분석과 주제 분석 기법을 적용함으로써 검토에 포함된 텍스트를 데이터로 취급하여 HC의 구성과 휴머니즘의 아이디어를 연결함으로써 얻을 수 있는 교육적 효과를 도표화할 수 있었습니다. 그 과정에서 그들은 부정적인 역할 모델링을 초래하는 의사 교사의 도덕적 침식에 대한 강한 집착을 확인했습니다. 인본주의 진료에 대한 이러한 인식은 의대생과 교수진의 문제 행동을 겨냥한 개혁과 같은 특정 유형의 개입/대응을 다른 유형보다 우선시하는 결과를 낳았지만 조직, 기관, 더 광범위한 사회정치적 관계가 그러한 문제 행동을 유발할 수 있는 방식에 대한 고려는 거의 없었습니다. 학생, 다른 수련의, 교수진의 행동을 규제하는 것을 지나치게 강조하다 보니 전문직업성과 인본주의26가 혼동되고, 보건 경제, 정치, 관행에 반영된 직장의 이해관계가 어떻게 그리고 왜 교육적 이상과 어긋나게 되는지에 대한 인식이 부족해졌습니다. 결론적으로, 마르티미나키스와 동료들2은 보건 전문직 교육자들에게 전문직업성 문제와 휴머니즘 문제를 의도적으로 분리하는 것이 어떻게 다른 종류의 HC 연구와 교육 개혁에 기여할 수 있는지, 즉 의료 교육이 사회정치적 진공 상태에서 이루어지지 않는다는 것을 인정하는 것에서 시작되는 것을 고려하도록 도전합니다.
A conclusion that the pervasive use of the HC concept signals the need to deconstruct how the term is implicated in broader sociopolitical relations (rather than a call to banish the term altogether) might have allowed the Lawrence team to bridge the MacLeod4article and Martimianakis and colleagues’ scoping review.2The Martimianakis team2identified 200 articles published in six medical education journals that explicitly or implicitly linked the HC construct to physician humanism. In contrast to the Lawrence team, however, they included articles that referenced the phenomenon of the HC even if the authors did not deploy a specific HC definition. By moving beyond a traditional taxonomic approach (which is consistent with scoping reviews), and by applying critical discourse analysis and thematic analysis techniques, Martimianakis and her coauthors were able to treat the texts in their review as data, and thus chart the educational effects of linking the construct of HC to ideas of humanism. In the process, they identified a strong preoccupation with the moral erosion of physician teachers that results in negative role modeling. These perceived attacks to humanistic care resulted in the privileging of certain types of interventions/responses over others—namely, reforms targeting problematic behaviors of medical students and faculty members—but with very little consideration for how organizations, institutions, and broader sociopolitical relations might give rise to such problematic behaviors. This overemphasis on regulating the behaviors of students, other trainees, and faculty has contributed to the conflation of professionalism and humanism26along with an underappreciation of how and why workplace interests reflected in health economics, politics, and practices become misaligned with(in) educational ideals. In conclusion, Martimianakis and colleagues2challenge health professions educators to consider how the deliberate disentanglement of professionalism issues from humanism issues might contribute to a different kind of HC study and educational reform, one that begins by acknowledging that medical training does not happen in a sociopolitical vacuum.
이론적 전환의 과제 The Challenge of Theoretical Conversion(s)
이제 결론에 도달했습니다. 마르티미나키스 연구팀2의 범위 검토는 HC 구성이 의학교육 연구에서 점점 더 많이 활용됨에 따라 어느 정도 개념적 변이를 겪어온 과정을 보여줍니다. 과거에는 주로 사회 구조 및 시스템 수준의 개입에 초점을 맞추던 의학교육 내 개선 노력이 개인과 해로운 영향에 대한 회복력을 발휘하는 능력에 초점을 맞추기 시작하면서 상대적으로 발견되지 않은 리모델링을 거쳤습니다.
이러한 변화는 Ng와 동료들이 의학교육 내에서 성찰 담론이 "원래의 성찰 및 성찰적 실천 이론과 어떻게 분리되었는가"에 대해 보고한 것과 유사합니다.
마찬가지로, 리츠와 공동저자28는 사회적 책무성의 개념이 어떻게 그 의미에서 "현저한 다양화"("사회적 반응성" 및 "사회적 책임"과 같은 용어와의 혼용 포함)를 겪었을 뿐만 아니라 어떻게 "비판적 분석의 영역을 넘어 독립적으로 존재하는 것처럼 보이는 담론의 영역으로" 격상되었는지를 기록합니다.
마지막으로, 바르피오와 동료들은29 방법론적 틀이나 이론적 개념이 한 학문에서 다른 학문으로 전수될 때 이를 온전하게 유지하는 것이 거의 불가능에 가깝다는 점을 자세히 설명합니다.
This brings us to our concluding point. The scoping review by the Martimianakis team2makes visible how the HC construct has undergone a degree of conceptual mutation as it has become increasingly deployed within medical education research. What once (within education) focused predominantly on social structural and systems-level interventions underwent a relatively undetected remodeling as remediation efforts within medical education began focusing on individuals and their ability to manifest resilience to pernicious influences.
This transmutation is similar to one reported by Ng and colleagues27on how the discourse of reflection within medical education has become “divorced from original theories of reflection and reflective practice.”
Similarly, Ritz and coauthors28document not only how the concept of social accountability has undergone a “marked diversification” in its meaning (including a conflation with terms like “social responsiveness” and “social responsibility”) but also how it has become elevated “to a realm of discourse where it appears to have an independent existence … beyond the realm of critical analysis.”
Finally, in a broadly framed argument, Varpio and colleagues29detail how keeping a methodological framework or theoretical concept intact when it is being expropriated from one discipline to another is nigh impossible.
이 전이 문제를 제기하면서 우리는 다시 맥레오드에게로 돌아가,4 먼저 HC 개념을 문제점으로 도출한 다음, "따라서" HC가 "그 과정을 거쳤다"는 그녀의 우려에 도달합니다. 우리는 맥레오드가 문제를 제기하는 것을 부끄러워하지 않지만, 우리가 우려하는 것은 (마르티미나키스와 동료들이 제안한 것처럼2) 문제가 되는 것은 개념 자체보다는 개념이 특권에 의해 편향적으로 적용될 가능성입니다. 즉, 의학교육자들은 다른 전문직과의 관계에서 의사의 보수가 어떻게 설정되는지를 포함하여 의료 자원 문제와 같은 [구조적 또는 제도적 장치가 직장에서의 비전문적 행동에 어떻게 기여할 수 있는지 탐구하기]보다는, [학습자와 교사의 행동을 규제하는 데] 더 집중할 가능성이 높습니다.
In raising this issue of transmutation, we again reach back to MacLeod,4first to her distillation of the HC concept as a problem, and then to her “therefore” concern that HC has “run its course.” Although we unabashedly endorse MacLeod’s predilection to problematize, our concern is with the possibility (as suggested by Martimianakis and colleagues2) that what is problematic is the concept’s biased-by-privilege application rather than the concept itself. That is, medical educators are more likely to focus on regulating behaviors of learners and teachers rather than exploring how structural or institutional arrangements such as health resourcing issues, including how physician remuneration is set up in relation to other professions, may contribute to unprofessional behaviors in the workplace.
지금까지 공유한 모든 사례에서 우리는 의학을 상당한 문화적 영향력을 가진 힘의 장으로 보고 있으며, 따라서 그 경계 내에서 현상이 전개되는 방식을 "구부리거나", 재구성하거나, 왜곡할 수 있는 분야로 보고 있습니다. 또한, 의학은 "문화가 없는 문화"30라는 공상적인 믿음으로 인해 이러한 힘의 장이 더욱 악화되고 있으며, 따라서 문화의 보다 기본적이고 공통적이며 주관적인 힘의 외부 또는 그 위에 존재하는 사회적 관행의 한 형태라고 생각합니다. 리츠와 동료들을 떠올리면,28 헤게모니는 자기기만적이고 자기 강화적이며 궁극적으로 자기 영속적인 것으로 간주됩니다.
In all the examples we have shared thus far, we view medicine as a force field of considerable cultural influence, and thus a field that can “bend,” reshape, or otherwise distort how phenomena unfold inside its boundaries. Furthermore, we see this force field being exacerbated because of medicine’s fanciful belief that it is a “culture of no culture”30and therefore a form of social practice that resides outside or above the more base, common, and subjective forces of culture. Recalling Ritz and colleagues,28we see hegemony as self-deluding, self-reinforcing, and ultimately self-perpetuating.
따라서 HC 및 보건 전문직 교육의 경우, 계급 투쟁이 의학교육의 포스트 실증주의적 출발점에 거의 포함되지 않았기 때문에 HC의 마르크스주의적 뿌리(그리고 그에 상응하는 체계적 불평등에 대한 초점)는 의학교육 청중에게 거의 보이지 않았습니다.31 Thus, and in the case of the HC and health professions education, the Marxist roots of the HC (and the corresponding focus on systemic inequities) largely have been invisible to a medical education audience because class struggles rarely have been part of medical education’s postpositivist starting points.31
그럼에도 불구하고 우리가 강조하고 싶은 점은, 비록 이 개념이 "잘못 적용"되었지만, (잃어버린 계보의 산물인) HC는 마르크스주의를 포함한 다른 비판적 형태의 학문이 자리 잡을 수 있는 패러다임적 토대를 개발하는 데 기여했다는 점입니다. 예를 들어 Ng와 동료27는 사람들의 일상과 노동에 기반을 두고 있기 때문에 마르크스주의적 기반이 강한 페미니스트 방법론인 제도적 민족지학의 교리를 의학 청중에게 소개합니다. 이들은 제도 민족지학의 초석인 '문제적'이라는 개념을 설명하는 것으로 시작합니다. 이들은 문제적인 것이 "현존하는 문헌에서 발견되는 것이 아니라 사람들의 일과 경험을 뒷받침하는 사회적 관계에서 발견되기 때문에 연구 문제와는 다르다."27(54쪽) 이어서 사람들의 일과 경험을 뒷받침하는 사회적 관계가 어떻게 "즉각적인 시야에서 숨겨져 있으며" "지역 및 지역 외 관행의 복잡한 그물망"의 일부인지를 설명합니다. 의학교육 맥락에서 기관 민족지학을 적용하는 것은 연구자들이 문화와 구조에 대한 설명을 넘어 일상적인 일상적 관행이 커리큘럼 제공과 학습에 미치는 영향을 이해할 수 있게 해준다는 점에서 HC 효과를 차트화하는 학자들의 관심사와 분명히 비교할 수 있습니다. HC 구조와 기관 민족지학을 결합하면 의학교육자와 학자가 암묵적 및 비공식적 영향에 대해 알고 있는 것을 구축하고 향상시킬 수 있는 잠재력이 있으며, 이는 Webster와 동료들이 경험적으로 입증한 바 있습니다.32
Nonetheless, and in a point we wish to emphasize—even as the concept has also been “misapplied”—the HC (a product of the lost genealogy) has contributed to the development of a paradigmatic foundation for other critical forms of scholarship to take hold, including Marxist. Ng and colleagues,27for example, introduce to a medical audience the tenets of institutional ethnography, a feminist methodology with strong Marxist underpinnings because it is grounded in the everyday lives and work of people. They start by explaining the concept of the “problematic” a cornerstone of institutional ethnography. They note that the problematic “is different from a research problem” because it “is not found in the extant literature, but within the social relations underpinning people’s work and experience.”27(p54)They go on to describe how the social relations underpinning people’s work and experiences “are often hidden from immediate view” and are part of a “complex web of local and extra local practices.” The application of institutional ethnography in medical education contexts is clearly comparable with the interests of scholars charting HC effects, for it enables researchers to move beyond the description of culture and structures to understanding how routine day-to-day practices affect curriculum delivery and learning. Combining the use of the HC construct with institutional ethnography signals potential to build and enhance what medical educators and scholars know about tacit and informal influences, a point demonstrated empirically by Webster and colleagues.32
마무리 생각 Closing Thoughts
로렌스와 동료들의 범위 검토는 매우 훌륭합니다. 저자들의 기본 방법론과 논문 식별 및 분석에 대해 제공하는 세부 사항은 다른 검토의 롤모델이 될 수 있습니다. 또한 HC에 대한 네 가지 정의 영역(제도-조직, 대인관계-사회, 상황-문화, 동기-심리)을 구분하고 이러한 영역을 네 가지 학문적 렌즈(각각 정책, 사회학, 인류학, 심리학)에 매핑한 것도 주목할 만합니다. 이러한 맥락에서, 우리는 또한 연구자들이 다루고자 하는 연구 질문의 학문적, 이론적 뿌리(HC에 초점을 맞추든 맞추지 않든)를 어느 정도 파악하고 있어야 한다는 로렌스와 동료들의 요청을 지지합니다. Much of Lawrence and colleagues’ scoping review is admirable. The authors’ underlying methodology and the details they provide on article identification and analyses are a role model for other reviews. Also noteworthy is their discernment of four definitional domains (institutional-organizational, interpersonal-social, contextual-cultural, and motivational-psychological) for the HC, along with their mapping of these domains to four disciplinary lenses (respectively, policy, sociology, anthropology, and psychology). Within this context, we also endorse Lawrence and colleagues’ call for researchers to have some idea of the disciplinary and theoretical roots underscoring the research question(s)—HC focused or not—that they seek to address.
이 네 가지 영역을 통해 우리는 항상 개념적 이질성을 염두에 두어야 한다는 결론에 도달하게 됩니다. 다음 HC 범위 검토에서 '숨겨진', '비공식적', '암시적'(로렌스와 동료들의 검토의 근거)과 같은 키워드를 포기하고 대신 로렌스와 동료들이 제시한 것과 같은(반드시 이에 국한되지는 않음) 규율적 렌즈를 적용하여 기본 개념적 지형을 탐색하고 매핑하려고 한다면 어떻게 될까요? 위에서 살펴본 HC 사고의 사회학적 기원에 대한 간략한 탐구는 저희에게는 흥미로운 여정이었습니다. 다른 탐구도 비슷하게 진행될 수 있다고 생각합니다. 래빗홀은 마음을 확장하는 서식지가 될 수 있습니다. 앨리스에게 물어보세요. These four domains bring us to a closing enticement—always with an eye toward conceptual heterogeneity. What if the next HC scoping review abandons keywords such as “hidden,” informal,” and “implicit” (the basis for Lawrence and colleagues’ review) and, rather, seeks to explore and map the underlying conceptual landscape by applying disciplinary lenses such as (but not necessarily restricted to) those provided by Lawrence and colleagues? Our brief foray above into the sociological origins of HC thinking was an exciting excursion for us. We think other explorations might be similarly undertaken. Rabbit holes can be mind-expanding habitats. Just ask Alice.
결국, HC 프레임워크 내에서 작업하는 데 관심이 있거나 HC 현상을 탐구하는 데 관심이 있는 사람들은 두 가지 문제적인 단어와 싸워야 합니다: "숨겨진"과 "커리큘럼".
첫 번째는 사회적 학습의 대부분이 공식적인 학습 영역과 공식적이지 않은 다양한 학습 영역 사이의 중간 공간에서 일어난다는 것을 알고 있음에도 불구하고 학습의 보다 암묵적이고 의도하지 않은 암묵적인 측면으로 우리를 편향시킵니다.
두 번째는 우리가 부당하게 생각하는 교육이라는 사회적 제도에 대한 제한입니다. 학습의 사회적 역동성과 구조적 구조는 "커리큘럼"이라는 단어에서 일반적으로 떠올리는 것의 벽을 훨씬 뛰어넘습니다.
In the end, those of us interested in working within an HC framework or interested in exploring HC phenomena must contend with two problematic words: “hidden” and “curriculum.”
The first biases us toward the more implicit, unintended, and tacit sides of learning—even as we know that much of social learning takes place within an interstitial space between the formal and a range of other-than-formal domains of learning.
The second restricts us—unduly we think—to the social institution of education. The social dynamics and structural architecture of learning extend far beyond the walls of what commonly comes to mind when we say the word “curriculum.”
1965년 스트로트벡이 중산층 가정에서 HC를 발견한 것에서 교훈을 얻을 수 있을까요? 스트로트벡은 중산층 가정의 아동과 "의존적 빈곤층 아동"이 "거의 무의식적으로" 획득하는 사회적 이점에 대해 관심을 가졌습니다. 물론 스트로트벡이 고민했던 것은 아직 사회학 어휘집에 등장하지 않은 사회적 자본의 문제였습니다. 따라서 앨리스는 또 다른 구성 요소(사회적 자본)가 HC와 어떻게 상호작용할 수 있는지, 따라서 사회적 관계, 사회적 학습, 사회적 삶이라는 마술처럼 광활한 춤 속에서 HC를 재위치시키기 위해 끊임없이 도전받는 우리를 관찰하는 것을 기쁘게 여겼을 것입니다.
Perhaps there is a lesson in Strodtbeck’s181965 identification of an HC in the middle class home? Strodtbeck was concerned with the social advantages differentially and “almost unconsciously” acquired by children from middle class homes versus “children from the dependent poor.” What Strodtbeck was wrestling with, of course, was the issue of social capital—a term that had not yet made its way into the sociological lexicon. Alice would be pleased to thus observe us wrestling with how yet another construct (social capital) might interface with the HC, and thus how we continuously are challenged to resituate the HC within the magically expansive dance of social relationships, social learning, and social life.
1F.W. Hafferty is professor of medical education, Division of General Internal Medicine and Program in Professionalism and Values, Mayo Clinic, Rochester, Minnesota; ORCID: https://orcid.org/0000-0002-5604-7268. M.A. Martimianakis is associate professor and director, Medical Education Scholarship, Department of Paediatrics, and scientist and strategic lead international, Wilson Centre, Faculty of Medicine, University of Toronto, Toronto, Ontario, Canada; ORCID: https://orcid.org/0000-0002-2531-3156.
In this Commentary, the authors explore the scoping review by Lawrence and colleagues by challenging their conclusion that with over 25 years' worth of "ambiguous and seemingly ubiquitous use" of the hidden curriculum construct in health professions education scholarship, it is time to either move to a more uniform definitional foundation or abandon the term altogether. The Commentary authors counter these remedial propositions by foregrounding the importance of theoretical diversity and the conceptual richness afforded when the hidden curriculum construct is used as an entry point for studying the interstitial space between the formal and a range of other-than-formal domains of learning. They document how tightly delimited scoping strategies fail to capture the wealth of educational scholarship that operates within a hidden curriculum framework, including "hidden" hidden curriculum articles, studies that employ alternative constructs, and investigations that target important tacit sociocultural influences on learners and faculty without formally deploying the term. They offer examples of how the hidden curriculum construct, while undergoing significant transformation in its application within the field of health professions education, has created the conceptual foundation for the application of a number of critical perspectives that make visible the field's political investments in particular forms of knowing and associated practices. Finally, the Commentary authors invite readers to consider the methodological promise afforded by conceptual heterogeneity, particularly strands of scholarship that resituate the hidden curriculum concept within the magically expansive dance of social relationships, social learning, and social life that form the learning environments of health professions education.
표면 아래로 긁어보기: 어떻게 조직문화가 교육과정 개편에 영향을 미치는가 (Med Educ, 2022) Scratching beneath the surface: How organisational culture influences curricular reform Adarsh P. Shah1 | Kim A. Walker1 | Lorraine Hawick1 | Kenneth G. Walker2 | Jennifer Cleland3
1 소개 1 INTRODUCTION
커리큘럼 개혁은 종종 의학교육 및 수련의 문제를 해결하기 위한 수단으로 제안됩니다. 그러나 이전 연구에 따르면 커리큘럼 개혁은 최선의 의도를 가지고 있더라도 눈에 띄는 변화로 이어지지 않을 수 있다고 합니다.1-4 실제로 화이트헤드와 동료들1은 회전목마라는 은유를 사용하여 커리큘럼 개혁의 주제가 반복적으로 순환하는 것을 설명합니다. 이 회전목마에서 벗어나려면 근본적으로 한 가지 업무 방식에서 다른 방식으로 변화해야 합니다. Curricular reform is often proposed as the means to address issues with medical education and training. However, previous studies have suggested that curricular reform, even with the best of intentions, may not lead to noticeable change.1-4Indeed, Whitehead and colleagues1use the metaphor of a carousel to illustrate that the returning themes of curricular reform circle around repeatedly. Getting off this carousel fundamentally requires changing from one way of doing things to another.
대부분의 조직 변화와 마찬가지로 커리큘럼 개혁은 리더가 커리큘럼의 비전, 구조 또는 절차를 변경할 것을 제안한 다음 다른 사람들이 그 제안을 실행하도록 설득하여 추진하는 경향이 있습니다.5-8 그러나 이러한 하향식 변화 노력은 종종 의도한 목적을 달성하지 못하고 오히려 개인과 그룹의 혼란, 변화에 대한 저항, 의도하지 않은 결과를 초래합니다.9-11 이는 이전에 커리큘럼 개혁 시도가 도전적이고 파괴적인 것으로 묘사되었던 의학 교육에서도 다르지 않습니다.12 As with most organisational change, curriculum reform tends to be driven by leaders who propose to change the vision, structure or procedures of a curriculum and then persuade others to implement their recommendations.5-8However, such top-down change efforts often fail to meet their intended purposes and instead result in disturbance, resistance to change from individuals and groups, and unintended consequences.9-11This is no different in medical education, where attempts to reform curricula have been previously described as challenging and disruptive.12
커리큘럼을 개혁하려면 조직의 프로세스, 시스템 및 구조를 변경해야 하는데, 어느 것 하나 쉽게 바꿀 수 있는 것은 없습니다. 그러나 문화를 바꾸는 것은 훨씬 더 어렵습니다. 경영 문헌에서는 조직 문화, 즉 '조직 구성원의 당연한 가정과 행동'13(171쪽)이 변화 실행에 중요한, 실제로 가장 큰 장벽이라는 점을 분명히 하고 있습니다.14-16 조직 문화가 변화 과정에 영향을 미친다는 것은 비즈니스,17, 18 고등 교육,19 및 보건 및 의학 교육에서 입증되었습니다.20-26 Reforming a curriculum involves changing organisational processes, systems and structures, none of which is easy to change. However, even more challenging is changing culture: the management literature is clear that organisational culture—‘the taken-for-granted assumptions and behaviours of an organisation's members’13(p171)—is a significant, indeed the greatest barrier, to change implementation.14-16That organisational culture influences change processes has been demonstrated in business,17,18higher education,19and healthcare and medical education.20-26
요컨대, 커리큘럼 개혁을 이해하려면 조직 문화에 대한 이해가 필요합니다. 그러나 의학교육의 변화/교육과정 개혁을 평가하는 경험적 연구들은 종종 관찰 결과를 설명하기 위해 문화를 언급하지만,27-29 이러한 연구들은 교수진의 전통과 가치를 충분히 인정하지 않는다는 비판을 받아왔습니다.9 다른 사람들은 의학교육 학자들이 '문화'라는 단어를 이해하기 위해 이론에 기반한 접근법을 간과했다고 제안합니다.28 따라서 의학교육 문헌에는 조직 문화가 어떻게 변화를 형성하는지 이해하기 위해 이론 중심 접근법을 사용하는 데 공백이 있습니다.30 이러한 이해는 변화를 제한하는 문화의 측면을 식별하고 해결하는 데 필요합니다.31, 32 In short, to understand curriculum reform requires an understanding of organisational culture. However, although empirical studies evaluating change/curricular reform in medical education often invoke culture to explain their observations,27-29these studies have been criticised for insufficiently acknowledging faculty traditions and values.9Others suggest that medical education scholars have overlooked theory-informed approaches to demystify the word ‘culture’.28A gap in the medical education literature thus exists for the use of theory-driven approaches to understand how organisational culture shapes change.30This understanding is necessary to ensure aspects of culture, which may limit change are identified and addressed.31,32
영국에서 초기 외과 수련의 커리큘럼 개혁('개선 외과 수련(IST)')33 이 시행되면서 외과 교육 및 수련에서 변화 실행에 대한 문화적 장벽과 이를 가능하게 하는 요인을 조사할 수 있는 자연스러운 기회가 생겼습니다. 시험 합격률, 외과 수련 지속 의향, 추후 프로그램 충원율과 같은 조잡한 결과 측정에 따르면 IST는 국가 차원에서 성공을 거두었습니다.34, 35 그러나 평가 데이터에 따르면 병원 간 이행과 수련생 및 강사의 IST 성공에 대한 인식에 차이가 있는 것으로 나타났습니다. 이러한 차이와 뿌리 깊은 가치와 관행이 수술에서 외부의 영향에 대해 강력한 저항력을 발휘할 수 있다는 이전 연구 결과를 고려할 때,36-39 우리는 문화가 변화에 미치는 영향을 고려할 가치가 있다고 생각했습니다. 따라서 우리의 구체적인 연구 질문은 조직 문화가 스코틀랜드 전역에서 IST를 구현하는 데 어떤 방식으로 영향을 미쳤는가 하는 것이었습니다. The roll out of a curricular reform of early-years surgical training in the UK (called ‘Improving Surgical Training (IST)’)33was a natural opportunity to examine cultural barriers to, and enablers of change implementation in surgical education and training. IST had met with success at national level according to crude outcome measures as examination pass rates, intention to continue training in surgery and fill rates of onward programmes.34,35However, evaluation data showed variations in implementation between hospitals, and in trainees' and trainers' perceptions of the success of IST. Given these variations, and previous findings that deep-seated values and practices can exert powerful resistance to external influence in surgery,36-39we considered that the influence of culture on change was worthy of consideration. Thus, our specific research question was: in what ways did organisational culture influence the implementation of IST throughout Scotland?
2 방법 2 METHODS
우리는 측정보다는 이해에 관심이 있었기 때문에 질적 접근법을 채택했습니다.40 이 연구는 현실이 사회적으로 구성되므로 지식 구성 및 축적 과정에서 문화와 맥락이 중요하다는 사회 구성주의에 기반을 두고 있습니다.41 우리는 개별 인터뷰를 통해 참가자들의 교육과정 개혁에 대한 경험, 개혁의 문화적 장벽과 조력자에 대한 견해 등을 탐색했습니다. We adopted a qualitative approach given our interest was understanding rather than measuring.40Our study was underpinned by social constructivism, acknowledging that reality is socially constructed and thus culture and context are important in the process of knowledge construction and accumulation.41We used individual interviews to explore participants' experiences of a curricular reform, including their views of cultural barriers to, and enablers of reform.
2.1 연구 배경 2.1 Context
연구 배경은 영국의 외과 수련(레지던트), 특히 의과대학 졸업 후 2년의 일반 파운데이션 프로그램 다음 단계인 대학원 외과 수련의 첫 2년간이었습니다. 핵심 외과 수련(CST)으로 알려진 이 외과 수련의 초기 단계는 수련의에게 다양한 외과 전문 분야에 걸쳐 폭넓은 경험을 제공하는 것을 목표로 합니다. Our context was UK surgical training (residency), specifically the first 2 years of postgraduate surgical training, which follows the 2-year generic Foundation Programme, which in turn follows medical school. This initial stage of surgical training, known as Core Surgical Training (CST), aims to give trainees a broad exposure across different surgical specialties.
2013년 수련의 형태 보고서는 서비스 제공과 수련 사이의 불균형, 수련 시간 부족, 수련 과정의 유연성 부족 등의 문제를 해결하기 위해 대학원 의학 교육에 변화를 권고했습니다.42-44 이러한 문제는 특히 CST에서 두드러지게 나타났습니다. 핵심 외과 수련의(일반적으로 레지던트 1, 2년차에 해당하는 CT1 또는 CT2라고 함)는 교대 근무와 과중한 임상 서비스 업무량으로 인해 수술 경험이 제한되고,43, 49, 50 팀 내 '소속감'이 낮고 수련의와의 관계가 상대적으로 좋지 않아 교육 및 수련 경험에 불만을 오랫동안 보고해 왔습니다.51, 52 이러한 긴장을 해소하고 수련 경험의 질을 개선하기 위해 '외과 수련 개선(IST)'이 제안되었습니다.33 IST의 권고사항은 다음에 중점을 두었습니다.
수련의의 근무 시간을 줄이고 근무 주 동안 수련에 할애하는 시간을 늘리고
교육/임상 감독 역할을 하는 컨설턴트 외과 의사(이하 트레이너)가 수련 제공에 더 많은 시간을 할애할 수 있도록 하고,
로테이션 기간을 늘려 수련의와 트레이너 관계를 개선하며,
더 집중적인 수련 기회(예: 시뮬레이션)를 제공하고,
더 넓은 외과 팀 내에서 의료 전문가가 환자 치료를 제공하도록 참여시켜 수련의가 자유롭게 수련을 받을 수 있도록
In 2013 the Shape of Training report recommended changes to postgraduate medical education to address problems including the imbalance between service provision and training, the lack of time for training and the lack of flexibility during the training process.42-44These problems were particularly notable in CST. Core surgical trainees (usually referred to as CT1 or CT2s, equivalent to residency years 1 and 2) had long reported dissatisfaction with their education and training experiences45-48because of shift working and heavy clinical service workloads, which limited surgical experience,43,49,50and led to a lower sense of ‘belonging’ within teams and relatively poor relationships with their trainers.51,52‘Improving Surgical Training (IST)’ was proposed to redress these tensions and to improve the quality of training experience.33IST's recommendations focused on
reducing trainees' service commitments and increasing the time dedicated to training during the working week,
enabling Consultant Surgeons with educational/clinical supervision roles (henceforth trainers) to dedicate more time to deliver training,
increasing the length of rotations to enhance trainee-trainer relationships, more focused training opportunities (e.g. simulation) and
involving health professionals within the wider surgical team to deliver patient care thereby freeing trainees to seek training.
구체적인 상황은 2018년 8월부터 모든 CST 포스트에서 IST를 시행한 영국 스코틀랜드였습니다. 다른 영국 지역과 비교했을 때, 스코틀랜드에서는 교육 감독관의 추가 시간을 확보하고 CST 전반에 걸쳐 광범위한 시뮬레이션 기반 교육 프로그램을 제공하는 데 특히 우선순위를 두었습니다.53 Our specific context was Scotland, UK, where IST was implemented across all CST posts from August 2018. Compared with the other UK sites, in Scotland particular priority had been put on resourcing Educational Supervisors' additional time, and on providing an extensive programme of simulation-based training throughout CST.53
2.2 참가자 2.2 Participants
스코틀랜드 전역에서 매년 45~55명의 핵심 외과 수련의(CT)가 스코틀랜드 동부와 서부 두 개의 프로그램에 배정되며, 각 프로그램은 교육 프로그램 디렉터가 이끌고 있습니다. CT는 지역 3차 병원, 지역 종합병원, 지방 병원 등 다양한 병원 환경에서 14개 지역 보건위원회에 걸쳐 제공됩니다. 프로그램은 4~6개월의 순환 근무로 구성되며, 각 순환 근무 기간 동안 각 수련의에게는 한 명의 교육 감독관과 여러 명의 지명된 임상 감독관이 배정됩니다. There is an annual intake of 45–55 core surgical trainees (CTs)across Scotland, assigned into two programmes, East and West of Scotland, each of which is led by a Training Programme Director. CST is delivered across 14 territorial Health Boards, in a wide variety of hospital settings: regional tertiary units, district general hospitals and rural hospitals. The programmes consist of 4-to-6-month rotations and during every rotation each trainee is assigned one educational supervisor and several nominated clinical supervisors.
프로젝트 승인과 적절한 기관의 동의(이후 참조)를 받은 후 스코틀랜드 전역의 CT와 트레이너가 연구에 참여하도록 초대되었습니다. 두 명의 교육 프로그램 디렉터가 2020년 4월부터 8월(교육생 및 트레이너)과 2021년 2월부터 5월(트레이너만) 사이에 우리를 대신하여 잠재적 참가자에게 이메일을 통해 초대장을 보냈습니다. 또한 연구팀과 참가자들에게 잠재적 참가자를 식별하는 데 도움을 요청했습니다(스노우볼 샘플링54). 두 차례의 참가자 모집 기간 동안 연구에 대한 알림 이메일을 두 차례 보냈습니다. 관심 있는 참가자는 연구 책임자에게 직접 이메일로 연락하여 연구에 대한 자세한 정보를 제공받았습니다. On receiving project approval and appropriate institutional consents (see later), CTs and trainers from across Scotland were invited to participate in the study. The two Training Programme Directors emailed invitations to prospective participants on our behalf, between April to August 2020 (trainees and trainers) and February to May 2021 (trainers only). We also asked members of the research team and participants for assistance in identifying potential participants (snowball sampling54). Two email reminders about the study were sent during both participant recruitment rounds. Interested participants were asked to contact the main researcher directly by email and were then provided with more information about the study.
2.3 데이터 수집 2.3 Data collection
연구팀은 문헌17, 28 및 팀 내 논의와 스코틀랜드에서 IST를 조직하고 제공하는 관계자들과의 토론을 통해 반구조화된 인터뷰 일정55을 개발했습니다. 인터뷰 질문은 IST 시행 후 참가자들의 감독 및 교육에 대한 개별 경험을 탐색하기 위해 고안되었습니다. 또한 IST에 대한 조직 참여의 장벽과 조력자에 대한 참가자들의 견해를 조사하는 질문도 포함되었습니다. We developed a semi-structured interview schedule55informed by the literature17,28and by discussions both within the team and more widely with those involved in organising and delivering IST in Scotland. Interview questions were designed to explore participants' individual experiences of supervision and training following IST implementation. Questions also probed participants' views of barriers and enablers to organisational engagement with IST.
인터뷰 일정은 일관성을 유지하되, 참가자가 자신의 경험을 충분히 공유했다고 느낄 때까지 반복적으로 인터뷰를 진행했습니다. 가능한 한 개방형 질문을 통해 토론을 유도하고 필요한 경우 질문으로 보완했습니다. 데이터는 코로나19 팬데믹 기간 동안 수집되었기 때문에 인터뷰는 Microsoft Teams 플랫폼을 사용하여 AS가 가상으로 진행했습니다. The interview schedule ensured consistency, but interviews were iterative and continued until the participant felt that they had shared their experiences sufficiently. Open questions guided discussion as far as possible, supplemented by probes where required. Data were collected during the Covid-19 pandemic and so interviews were conducted virtually by AS using the Microsoft Teams platform.
2.4 데이터 분석 2.4 Data analysis
인터뷰는 나중에 필사하기 위해 디지털 오디오 녹음으로 진행되었습니다. 전사 과정에서 참가자는 익명으로 처리되었습니다. 녹취록은 데이터 관리 및 코딩을 용이하게 하기 위해 질적 데이터 분석 소프트웨어 NVivo v12.0(QRS International Pty Ltd, 호주 빅토리아주 동커스터)에 입력되었습니다. 먼저 주제와 하위 주제를 식별하기 위해 주제별 분석을 실시했습니다.56 예비 코드에 대한 팀 토론과 코딩 불일치를 해결한 후, 연구 질문에 초점을 맞춰 반복적이고 귀납적으로 코딩을 진행했습니다. 그 후, 추가 팀 토론과 JC의 경영 이론 및 문헌 지식을 바탕으로 단순한 주제별 분석을 넘어 Johnson의 문화 웹 이론을 사용하여 조직 문화를 비판적으로 분석했습니다.13 이 모델은 조직 문화의 발현과 이것이 IST의 실행에 어떤 영향을 미쳤는지를 드러내는 시각적 접근 방식을 제공했습니다.57-61 Interviews were digitally audio-recorded for later transcription. Participants were anonymised during the transcription process. Transcripts were entered into the qualitative data analysis software NVivo v12.0 (QRS International Pty Ltd, Doncaster, Victoria, Australia) to facilitate data management and coding. We initially conducted a thematic analysis to identify themes and sub-themes.56After team discussions of preliminary codes and resolution of any coding disagreements, coding occurred iteratively and inductively, focusing throughout on the research question. After this, following further team discussion and drawing on JC's knowledge of management theories and literature, we extended beyond simple thematic analysis to critically analyse organisational culture using Johnson's cultural web theory.13This model offered a visual approach to expose the manifestations of organisational culture and how these might have influenced the implementation of IST.57-61
존슨의 문화 웹 모델은 세 가지 전제를 바탕으로 합니다.
첫째, 조직 문화는 '조직 구성원의 당연한 가정과 행동'이라는 전제입니다.13(171쪽) 이러한 '당연함'은 조직 문화를 명확하게 표현하기 어렵게 만들며, 문화 웹 모델은 조직의 문화를 해명하고 시각화하는 데 도움이 됩니다.62
두 번째 전제는 문화 웹 모델의 6가지 요소 또는 인공물(루틴과 의식, 스토리, 상징, 권력 구조, 통제 시스템, 조직 구조)과 이들이 어떻게 관련되어 있는지 이해해야 중심 문화 패러다임을 이해할 수 있다는 것입니다(그림 1 참조). 문화 웹 이론에서 패러다임은 반드시 명시적이지 않고 문제가 되지 않는 가정에 대한 '큰 그림'을 의미하므로 과학 연구에서 패러다임의 의미와는 매우 다르다는 점에 주목할 필요가 있습니다.
세 번째 전제는 조직 내 변화와 같은 역사적 사건을 개인이나 집단이 어떻게 경험했는지가 현재의 행동과 미래 전략을 결정하는 데 중요한 역할을 한다는 것입니다. 예를 들어, 인수합병이나 매각과 같은 사건은 현재의 신념과 행동에 영향을 미치고, 이는 다시 미래의 환경 변화에 대한 대응을 결정합니다.
Johnson's cultural web model is built on three premises.
First, that organisational culture is ‘the taken-for-granted assumptions and behaviours of an organisation's members’.13(p171)This ‘taken-for-grantedness’ makes articulating organisational culture difficult, and the cultural web model helps elucidate and visualise the culture of an organisation.62
The second premise is that the six elements, or artefacts, of the cultural web model—routines and rituals, stories, symbols, power structures, control systems and organisational structures—and how they relate, need to be understood to comprehend the central cultural paradigm(see Fig. 1). It is noteworthy that the paradigm in the cultural web theory refers to the ‘big picture’ of the assumptions that are not necessarily explicit and not considered problematic and thus is very different from the meaning of paradigm in scientific research.
The third premise is how individuals or groups experienced historic events such as change within an organisation, plays a key role in determining current behaviours and future strategies. For example, events such as mergers and acquisitions or devolutions impact current beliefs and behaviours, which in turn determine responses to future environmental changes.
2.5 반사성 2.5 Reflexivity
질적 연구는 연구자와 연구 과정 간의 관계에 따라 달라집니다.41, 63 우리는 서로 다른 학제 간 배경(심리학, 약리학, 간호학, 외과), 외과 교육, 훈련 및 연구 제공 및 관리에 대한 서로 다른 수준의 지식과 경험을 고려하여 우리의 입장과 데이터와의 관계를 지속적이고 비판적으로 고려했습니다. 예를 들어, 다른 영국 국가에서 온 외과 수련의로서 박사 학위를 취득하기 위해 수련을 중단한 AS는 스코틀랜드의 의료 시스템 외부에 있지만 NHS 내에서 수련에 대한 지식을 갖춘 외과 수련의라는 점에서 내부자이자 외부자였습니다. Qualitative research is dependent on the relationship between the researcher and the research process.41,63We considered our positions and relationships with the data continually and critically in view of our different inter-disciplinary backgrounds (psychology, pharmacology, nursing and surgery), different levels of knowledge and experience of delivering and managing surgical education, training and research. For example, as a surgical trainee from another UK country who took time out of training to do a PhD, AS was both an insider and an outsider; external to Scotland's healthcare system but an insider by being a surgical trainee with knowledge of training within the NHS.
2.6 윤리 2.6 Ethics
주관 대학의 연구 거버넌스 팀과 주관 NHS 제공자의 품질 개선 및 보증 팀은 이 연구를 국가 평가 감사(프로젝트 번호 4945)로 분류하여 윤리적 승인 대상에서 제외했습니다. 그러나 잠재적 연구 참여자로부터 (익명으로 처리된) 응답이 연구 목적으로 사용될 수 있고, 참여가 자발적이며, 참여자는 언제든지 철회할 권리가 있다는 서면 동의를 받는 등 핵심 윤리 원칙을 따랐습니다. The host University's Research Governance team and the host NHS provider's Quality Improvement and Assurance Team classified this study as a National Evaluation Audit (project number 4945), thus exempting it from ethical approval. However, we followed core ethical principles: obtaining written, informed consent from potential research participants that their (anonymised) responses could be used for research purposes, that participation was voluntary and that participants had the right to withdraw at any time.
3 결과 3 RESULTS
46명의 교육생과 25명의 트레이너가 이메일 초대에 응답했습니다. 표 1은 참가자의 특성을 보여줍니다. 스코틀랜드의 핵심 외과 수련 기관이 있는 13개 보건청을 모두 대표할 수 있었습니다. 참가자들은 신경외과를 제외한 모든 외과 전문 분야를 대표했으며, 핵심 외과 수련 기간 동안 27개의 다른 병원에서 순환 근무를 했습니다. 수련의와의 인터뷰 시간은 평균 54분(범위: 26~111분), 트레이너와의 인터뷰 시간은 평균 41분(범위: 18~60분)이었습니다. 트레이너의 교육 및 임상 감독 경력은 2~25년 사이였습니다. Forty-six trainees and 25 trainers responded to the email invitations. Table 1reports participant characteristics. Representation from all 13 Health Boards in Scotland with core surgical training posts was achieved. Participants represented all surgical specialties except neurosurgery and had rotated through 27 different hospitals during their core surgical training. The mean duration of interviews with trainees was 54 mins (range: 26–111 min) and with trainers was 41 min (range: 18–60 min). Trainers' experience of educational and clinical supervision ranged from 2–25 years.
참가자는 익명으로 처리되었으며 연수생(CT) 또는 트레이너(TR)로 식별되었습니다. 인용문은 그대로 보도합니다. 줄임표(...)는 관련성이 낮은 부분을 잘라낸 텍스트를 나타내고, 대괄호는 축어체가 아닌 설명 텍스트를 나타냅니다. 인용문은 조사 결과의 확인을 돕고 독자가 이야기의 논리를 따라갈 수 있도록 하기 위해 포함되었습니다. 존슨의 문화 웹의 6가지 요소(그림 1)를 사용하여 데이터를 정리합니다. 이 여섯 가지 요소가 상호 작용하는 방식과 핵심 수술 훈련의 문화적 패러다임을 고려하는 토론에서 이 요소들을 한데 모았습니다. Participants have been anonymised and identified as trainee (CT) or trainer (TR). We report verbatim quotes. An ellipsis (…)indicates text that has been cut out where less relevant, and square bracketsindicate any non-verbatim explanatory text. Quotations are included to aid confirmation of findings and to help the reader follow the logic of the story. We use the six elements of Johnson's cultural web (Fig. 1) to organise the data. We bring these together in the discussion, where we consider how the six elements interacted and the cultural paradigm of core surgical training.
3.1 의식과 루틴 3.1 Rituals and routines
의식과 루틴은 어떤 상황에서 일어날 것으로 예상되는 일, 시간이 지남에 따라 확립된 존재 방식과 행동 방식을 안내하며, 흔히 '우리가 이곳에서 하는 방식'이라고도 합니다. 외과 수련의들은 교대근무에 배치되며, 교대근무 로테이션에 따라 IST 교육 기회가 결정된다는 것이 분명했습니다. 예를 들어, 응급 로테이션에 속해 있는 전공의들은 '수술실에 가는 것은 외과의가 되는 법을 배우러 온 것이 아니라 좋은 행동에 대한 보상으로 여겨질 정도'(CT03)일 정도로 주로 급성 입원 환자('테이크')를 보는 임무를 맡는다고 보고했습니다. 마찬가지로, 선택적 업무의 경우, 일부 지역에서는 CT가 할당된 활동에 참석하기 전에 병동 회진을 완료해야 하는 일상이 있었습니다: '... 선택적 수술 목록에 포함될 예정이었지만 병동 회진을 마쳐야 했다...'(CT27). Rituals and routines guide what is expected to happen in a situation, ways of being and doing established over time, often referred to as ‘the way we do things around here’. Surgical trainees are rostered to shifts, and it was clear that the shift rota determined IST training opportunities. For example, when on the emergency rota, CTs reported being primarily tasked with seeing acute admissions (the ‘take’) such that ‘going to theatre is almost seen as a reward for good behaviour … not you're here to learn how to be a surgeon’ (CT03). Similarly, with elective duties, the routine in some places dictated that CTs complete the ward round prior to attending their allocated activity: ‘… you might have been scheduled to be in an elective operating list but then the ward round needed done …’ (CT27).
IST의 권고(예: 낮 시간대 교육 시간 최대화)에 따라 일부 부서는 교육 기회를 최대화하기 위해 기존 로타를 조정하거나 초과 역할을 도입하는 등 업무 방식을 변경했습니다. 첫 번째 예로 응급 로테이션을 두 개로 나누어 CT가 급성 수술 입원(임상 술기 개발) 또는 응급실(수술 술기 학습)을 담당할 수 있도록 한 것이 있습니다. 이원화된 역할이 생겨나면서 수련의들은 근무에서 해방되었고, 더 자유롭게 수련 기회를 찾을 수 있게 되었습니다: In response to IST recommendations (e.g. maximisation of training time during daytime hours), some departments changed their ways of working, either adapting existing rotas to maximise training opportunities or introducing supernumerary roles. An example of the first of these was dividing the emergency rota into two so that CTs could either be responsible for acute surgical admissions (developing clinical skills) or for the emergency theatre (thus learning operative skills). The creation of supernumerary roles freed trainees from service, and empowered them to seek training opportunities more freely:
'... 어느 병동이나 클리닉에 가야 할지 정해져 있다는 점에서 한 주에 어느 정도 구조가 있었지만... 슈퍼너머리 역할을 맡았기 때문에 부서에서 나만의 목표를 설계하고 달성할 수 있는 사치를 누릴 수 있었습니다'(CT26). ‘… there was some structure to the week in that I was assigned which theatre or clinic to go to … but because I was supernumerary, I had that luxury from the department to kind of design my own and achieve my own goals’ (CT26).
새로운 로타를 도입한 부서의 교육 경험은 로타가 그대로 유지된 부서와 대조적이었습니다: Training experiences between departments that adopted new rotas contrasted with those where rotas remained unchanged:
'그곳에서는 거의 매일 수술했지만, 여기에서는 일주일에 하루 반나절만 있어도 운이 좋다고 생각할 수 있습니다. 그래서 수술 실력이 향상되기는커녕 오히려 떨어졌다고 생각합니다."(CT10). ‘I was pretty much operating there on a daily basis, while here you would consider yourself lucky if you had one and half day a week. So, I think my surgical skills went down instead of up’ (CT10).
IST에도 불구하고 로타가 변하지 않는 경우, '코어 트레이닝에서 전환하면서 진정으로 IST로 전환되는 것은 아무것도 없는 것 같았습니다. 그냥 그대로인 것 같았습니다'(CT07). 요컨대, 로타가 특정 상황에 따라 IST 관련 변화를 지원하거나 차단할 수 있는 것처럼 보였습니다. Where rotas remain unchanged despite IST, ‘it didn't seem that anything was truly translating to IST in the switch from core training. It just seemed to be the same’ (CT07). In short, it seemed that rotas could either support or block IST-related change, depending on the specific context.
3.2 스토리 3.2 Stories
과거 사건에 대한 이야기는 무엇이 중요하다고 인식되는지 파악하는 데 도움이 되며64, 종종 일의 방식, 규범 및 가치에 대한 기대가 전달되고 학습되고 전수되는 방식이 되기도 합니다. 이러한 현상은 트레이너 자신의 교육에 대한 이야기에서 가장 두드러졌습니다. 예를 들어, 수련 기회에 대한 접근성 측면에서 선임 레지던트가 후배 레지던트보다 우대받는 것이 항상 그래왔으며, 이는 수련생들에게 이것이 과거에도 그랬고 앞으로도 그럴 것임을 시사하는 이야기들이 흔했습니다. Stories of past events help identify what is perceived as important64and are often the way in which expectations of ways of doing things, norms and values are transferred, learnt and passed on. Stories were most apparent in respect of trainer stories of their own education. For example, narratives about how it has always been the case that senior residents have preferential treatment over CTs in respect of access to training opportunities were common, indicating to trainees this was the way things were, and would continue to be.
"교육 수퍼바이저에게 이 문제를 제기했더니 그는 '그게 원래 그런 거죠. 선배가 더 많으면 다른 사람보다 우위에 있는 거죠. 그게 내가 교육에서 해온 방식이고, 나중에 교육에서도 그렇게 할 것이다."'(CT10). ‘I brought it up with the educational supervisor and he says, “well, that's just the way it is. If you're more senior, you trump the rest. That's what I've done in my training, and that's what you're going to do later on in your training”’ (CT10).
또한 트레이너들은 교육 기회를 '접시에 담아 전달해서는 안 된다'(TR09), 교육생이 기회를 잡기 위해 자기 주도적이고 본질적으로 동기를 부여받아야 하며 모든 '서비스' 업무에 학습 기회가 내재되어 있다고 생각한다는 이야기도 있었습니다.65, 66 이러한 이야기와 태도는 전통적인 도제식 교육 모델에서 트레이너가 직접 교육생으로 경험한 영향인 것으로 보입니다. 이러한 이야기의 지속성과 지속되는 업무 방식은 변화를 가로막는 장벽으로 작용하는 것처럼 보였습니다: Stories also indicated that trainers believed training opportunities ‘should not be handed on a plate’ (TR09), that trainees needed to be self-directed and intrinsically motivated to seize opportunities and to see learning opportunities as inherent in every ‘service’ task.65,66These stories and attitudes seemed to be an influence of trainers' own experiences as trainees under the traditional apprenticeship training model. The persistence of these stories and the ways of working they perpetuated appeared to be a barrier to change:
"저는 이 직업에서 일렉티브 기회가 전혀 주어지지 않는 것에 대해 우려를 제기했지만, "네, 알고 있습니다."라는 대답만 들었습니다. 인식은 많지만 행동은 많지 않습니다...'(CT44). ‘I have raised concerns about not really having any access to elective opportunities in this job … you're just kind of brushed off and told, “ah yes, I'm aware of that.” There's a lot of awareness and not a lot of action …’ (CT44).
'역사적으로 핵심 훈련생에 대한 태도는 천천히 변했습니다. '역사적으로 핵심 훈련생인 사람들은 병동 원숭이들이고, 우리는 그렇게 여겨지고 있습니다...'(CT03). Historical attitudes towards core trainees were slow to change: ‘historically the people that are core trainees, we're the ward monkeys, and that's what we're seen as …’ (CT03).
3.3 상징 3.3 Symbols
이 요소는 조직의 신념과 가치, 조직 내 관계에 영향을 미치는 방식으로 의미를 갖는 단어, 사물, 조건 및 행위와 관련이 있습니다. This element relates to words, objects, conditions and acts that have meaning in ways that influence organisational beliefs and values, and relationships within organisations.
한 가지 분명한 상징은 교육과 관련된 행위였습니다. 종종 첫 번째 상징은 공식적이든 비공식적이든, 계획적이든 즉흥적이든, 환영이든 아니든 간에 로테이션이 시작될 때 직장으로 안내하는 행위였습니다. 예를 들어, 일부 트레이너는 연수생이 도착하기 전에 연수생과 접촉했는데, 이는 연수생들에게 환영을 받았습니다: '입문 과정을 일찍 시작하는 것 같고 정보 공유를 시작할 수 있다'(TR20). One obvious symbol was the acts associated with training. Often, the first symbol was the act of induction to the workplace at the start of the rotation: whether this was formal, informal, planned or ad hoc, welcoming or not. For example, some trainers made contact with their trainee prior to their arrival, an act that was welcomed by trainees: ‘it feels like you're starting the induction process early and you can start sharing information’ (TR20).
다음 상징은 물체, 특히 교육생의 e-포트폴리오에 학습 계약 및 커리큘럼 역량에 대한 진행 상황을 정기적으로 문서화해야 한다는 것이었습니다. IST의 목표 중 하나는 트레이너-트레이너 듀오 내에서 진행 상황을 더 자주 검토하는 것이었지만, 트레이너에 대한 서비스 제공의 압박은 관찰/감독 및 피드백의 질에 영향을 미쳤습니다: The next symbol was an object, specifically the regular documentation required within the trainee's e-portfolio of their progress against the learning agreement and curricular competencies. Although one of the aims of IST was more frequent reviews of progression within the trainee-trainer dyad, the pressures of service delivery on trainers impacted on the quality of observation/supervision and feedback:
'대부분의 컨설턴트들은 무엇이든 작성하는 것만으로도 만족해했습니다. 일부 컨설턴트는 더 많은 노력을 기울여 "자, 이것들을 읽어보셔야 합니다"라고 말하기도 했습니다. 다른 컨설턴트들은 그냥 "좋았어요. 작성해 주시면 제가 읽어보고 합리적이라고 생각되면 서명해 드리겠습니다."(CT18)라고 말하기도 했습니다. ‘Most of the consultants were quite happy just to fill out anything. Some consultants put more effort in and said, “Ok, these are the things you should go and read”. Others were just happy to say, “that was good. You can write it up and then I'll read through it and if it seems reasonable, I'll sign it off for you”’ (CT18).
또 다른 상징 또는 신호는 부서의 내부 거버넌스 시스템 내에서 교육에 대한 가시성이라는 점입니다. 예를 들어, 소수의 외과 부서만 정기적으로 월별 교육 및 진척도 회의를 개최했습니다. 이러한 회의가 있는 경우, CT는 성과에 대한 여러 컨설턴트의 피드백을 받을 수 있었고 트레이너는 부서별 교육 관련 이슈를 파악할 수 있었습니다. 반면, 교육에 대한 자체 회의가 없거나 문제가 발생했을 때(예: 교육에 영향을 미치는 직원 부족) 월별 비즈니스 회의 안건으로만 상정되는 경우, 참가자들은 교육에 대한 우려 사항이 '표면적인 수준에서 경청되고... 정말 귀에 걸면 귀걸이가 되는 것 같았다'(CT44)고 보고했습니다. Another symbol, or signal, was the visibility of education within the department's internal governance systems. For example, only a few surgical departments regularly held monthly education and progression meetings. Where these did occur, CTs benefited from multi-consultant feedback on performance and trainers kept abreast with departmental training-related issues. On the other hand, where education did not have its own meeting and/or was only tabled on the monthly business meeting agendas if problems occurred (e.g. staff shortages impacting training), participants reported that any concerns they had about training were ‘listened to on a surface level and dismissed … kind of falling on deaf ears really’ (CT44).
마지막으로 컨설턴트가 교육 감독자 역할을 맡게 된 이유에 대해 교육생들은 교육이 얼마나 중요하게 여겨지는지 알 수 있는 신호로 해석했습니다. 트레이너들 사이에는 '[교육] 프로그램이 무엇인지, 또는 역할이 무엇인지에 대한 관심이나 참여도 또는 인식 정도에 있어 매우 광범위한 스펙트럼이 존재했다'(TR22). 트레이너 참여도의 차이는 표면적으로는 개인의 문제로 보일 수 있지만, 시스템 문제, 특히 소규모 부서에서 개별 컨설턴트가 교육에 대한 '부담'을 짊어져야 하는 것과도 관련이 있는 것으로 나타났습니다: Finally, why a consultant took on an educational supervisor role, which was interpreted by trainees as a sign of how education was valued. There existed ‘a very broad spectrum of how interested or engaged or aware of what [the] training programme is, or what the role is’ (TR22) amongst trainers. Although differences in trainer engagement might on the surface seem to be an individual issue, it also appeared to be related to systems issues, specifically individual consultants having to ‘shoulder the burden’ of training in small departments:
'... 제가 맡은 교육 수퍼바이저는 이미 오랫동안 교육 수퍼바이저 일을 해왔어요... 제 느낌은 그가 좋아서 또는 정말 하고 싶어서 하는 것이 아니라는 것입니다. 그는 다른 사람이 귀찮게 할 수 없기 때문에 그것을합니다...'(CT10). ‘… the educational supervisor I have has been doing that educational supervisor thing for a long time already … my feeling is it's not he does it because he likes it, or he really wants to do it. He does it because nobody else could be bothered to do it …’ (CT10).
요약하면, 시스템 구조(상징)는 교육과 훈련의 가치에 대한 인식과 관련하여 핵심적인 역할을 했습니다. 현지에서 교육훈련에 대한 가시성, 즉 인식은 개혁/변화 과정에서 중요한 역할을 했습니다. 가시성이 낮다는 것은 우선순위가 낮다는 신호였습니다. In summary, system structures (symbols) had a key role in respect of how education and training were perceived to be valued. The visibility, or recognition of training locally was instrumental in the process of reform/change. Low visibility was a signal of low priority.
3.4 권력 구조 3.4 Power structures
권력 구조는 가장 큰 영향력을 가진 집단 또는 개인을 말하며, 이들은 영향력이 적은 사람들에게 기대되는 행동과 행동을 결정하고 조직 문화의 핵심 가정에 가장 밀접하게 부합할 것으로 기대될 수 있습니다.64 외과 수련을 제공하는 의료 기관에서 가장 명백한 권력은 Trainer에게 있으며, 일부는 IST를 지렛대로 사용하여 CT에 준하는 의사로 로타 공백을 메우기 위해 추가 자금을 확보함으로써 좋은 수련 경험과 안전한 임상 치료 제공의 잠재력을 극대화했습니다: Power structure refers to the groups or individuals with the most influence, who determine the actions and behaviours expected of those with less power and who may be expected to be most closely aligned with the core assumptions of the organisational culture.64In the healthcare institutions that deliver surgical training, the most obvious power lies with the trainers, some of whom used IST as leverage to maximise the potential for good training experiences and delivery of safe clinical care by obtaining extra funding to fill rota gaps with CT-equivalent doctors:
'... 더 많은 CDF[임상 개발 펠로우]를 확보하는 데 장벽은 재정 문제였습니다. 하지만 파일럿이 당직 근무를 얼마나 해야 하는지에 대한 목표가 바뀌었고, 이를 흑백으로 명시했으니 경영진에게 가서 로테이션을 강화하기 위해 CDF를 고용할 수 있냐고 말할 수 있었죠."(TR16). ‘… the barrier to getting more CDFs [Clinical Development Fellows] was finance. But when you got a pilot saying the goal posts changed to how much on-call they need to do, and having that set out in black and white meant we could go to management and say can we employ some CDFs to bolster the rota to allow this to happen?’ (TR16).
서비스 압력에도 불구하고 IST의 교육 원칙을 강력하게 옹호하는 사람들은 CT들 사이에서 IST의 신뢰도를 높이고 CT들이 가치 있다고 느끼게 만들었습니다: Those who strongly advocated for protection of IST's training principles despite service pressures enriched the credibility of IST amongst CTs and made the CTs feel valued:
'... 제 교육 감독관은 ... 여러분의 교육 시간을 매우, 매우 보호해 줍니다 ... 고위 컨설턴트 중 한 명은 등록 담당자의 부담을 덜어주기 위해 우리[핵심 교육생]가 항상 대기하기를 원합니다 ... 그리고 그 회의에서 제 감독관은 매우, 매우 큰 목소리를 냈습니다. 그는 "안 돼요, 그건 안 돼요. 그것은 그들의 교육 요구를 충족시키지 못합니다."'(CT12). ‘… my educational supervisor … he's very, very protective of your training time … one of the more senior consultants wants us [core trainees] to be on-call all the time to take the pressure off the registrars … And my supervisor, in that meeting was very, very vocal. He was saying, “no, that's not allowed. That does not meet their training needs”’ (CT12).
하지만 다른 사람들도 수술 훈련에서 힘을 발휘했습니다. 예를 들어, 앞서 설명한 것처럼(의식과 루틴), 로타는 교육 경험에 매우 중요한 요소였습니다.로타 관리는 종종 의료진이 아닌 로타 코디네이터의 책임이었습니다. 이들은 교육이 아닌 서비스 제공에 집중하는 것으로 인식되었고, 그에 따라 로타가 채워졌습니다. 이로 인해 CT는 동료 CT와 명단을 교환하거나 로타 마스터와 사전 합의를 통해 선택적 수술 기회 등을 협상해야 했습니다. 대규모 부서, 일반적으로 3차 병원에서는 여러 외과 전문과목과 수련 계층이 공존하기 때문에(사례 참조) CT가 급하게 공백을 메우거나 서비스 요구를 충족하기 위해 '로타 사료'(CT37)로 사용되는 경우가 많았습니다. 이러한 방식으로 로타 코디네이터는 IST의 현지 구현을 활성화하거나 억제할 수 있는 권한을 가졌습니다. 일부 부서는 이 문제를 인식하고 부서 내 임상 활동의 공정한 배분을 감독할 수 있는 트레이너를 지정하여 문제를 해결했습니다. However, other people also had power within surgical training. For example, as discussed earlier (Rituals and routines), the rota was critical to training experiences. Rota management was often the responsibility of a non-medical rota coordinator. These individuals were perceived as focused on service delivery, not education, and populated rotas accordingly. This left CTs having to negotiate, for example, elective operative opportunities by swapping lists with fellow CTs or by making prior agreements with the rota master. In large departments, typically tertiary units, the co-existence of multiple surgical specialties and training hierarchies (seeStories) meant CTs were often used as ‘rota fodder’ (CT37) to plug gaps at short notice or to meet service needs. In this way, the rota coordinator had power that could enable or inhibit local implementation of IST. Some departments recognised this issue and rectified it by nominating a trainer to oversee fair allocation of the department's clinical activities.
3.5 조직 구조 3.5 Organisational structures
조직 구조는 공식적인 구조, 역할 및 관계를 의미하며, 이는 서로 다른 역할을 수행하는 사람들 간의 권력 관계(예: 책임과 권한)를 반영합니다.64 변화의 가능성은 병원 경영진과 외과 트레이너 간의 관계에 의해 영향을 받았습니다. 예를 들어, 모든 병원에서 의학교육 책임자(일반적으로 선임 컨설턴트)는 IST를 지원하는 데 동의했습니다. 그러나 현장에서는 임상 서비스 관리자가 IST에 대한 이해가 부족하고 여전히 서비스 요구와 목표 달성에만 집중하는 것으로 인식되었습니다: Organisational structure refers to formal structures, roles and relationships, which reflect power relationships between people who carry out different roles (i.e. lines of accountability and responsibility).64The potential for change was influenced by relationships between hospital management and surgical trainers. For example, at every hospital, the Directors of Medical Education (who are typically senior consultants) agreed to support IST. But, on the ground, clinical service managers lacked understanding of IST and were perceived to still focus solely on meeting service needs and targets:
'경영진과 약간의 싸움이 있었습니다 ... 경영진은 트레이너들에게 추가 업무를 시키면 된다는 생각을 갖고 있는 것 같았습니다 ... 몇 주 후, 그들[트레이너]은 서비스와 현금보다는 실제로 자신의 훈련이 더 중요하다는 것을 깨달았습니다'(TR21), ‘It's been a bit of a battle with management … Management seemed to be under the opinion they could just flog the trainees into doing extra work … after a couple of weeks, they [trainees] realised that actually their training was more important rather than the service and the cash’ (TR21),
이에 비해 트레이너들은 각 목록 내에서 교육 잠재력을 극대화하여 교육과 사례 처리량의 균형을 맞추려고 노력했습니다: In comparison, trainers tried to balance education and case throughput by maximising the training potential within each list:
'... 제가 여기 앉아서 외과 조교와 함께 탈장 한 무더기를 수술하는 것보다 조직이 훨씬 더 행복할 거라는 걸 알지만... 컨설턴트 수준에서 물어본다면, 우리 모두는 목록에 탈장이 하나라도 적거나 내시경이 하나라도 적으면 그것에 대해 교육할 수 있다고 말할 것입니다.'(TR16). ‘… I know that the organisation would be much happier me sitting here doing a bunch of hernias with a surgical first assistant and battering through it … But if you ask at consultant level, we would all be saying, I would much rather have one less hernia on my list, or one less scope on my list, and be able to train on it’ (TR16).
IST의 목표 중 하나는 CT와 배정된 감독자 간의 정기적인 접촉을 늘리는 것이었습니다. 조직 구조와 관련된 요인이 이를 가능하게 했습니다. 예를 들어, 소규모 팀으로 구성된 교육과 근무는 연속성을 제공했습니다: One of IST's aims was increased, regular contact between CTs and their allocated supervisors. Factors relating to organisational structures enabled this. For example, training and working in smaller teams offered continuity:
'... 팀 기반이었기 때문에 ... 그들과 함께 당직을 서고, 그들과 함께 CEPOD [응급실] 주간을 보내고, 모든 클리닉에 가고, 모든 환자를 돌보는 등... 그게 큰 차이를 만든다고 생각합니다'. (CT32) ‘… because it was team based … you do the on call with them [the team], you do CEPOD [emergency theatre] week with them, you go to all their clinics, you look after all their patients … I think that makes a huge difference’. (CT32)
일대일 직접 감독 하에 풍부한 수술 경험을 쌓을 수 있습니다: and rich operative exposure under one-to-one direct supervision:
'컨설턴트 외에는 다른 사람과 함께 더 많은 일을 할 수 있습니다...'(CT12). ‘you're doing more stuff with nobody else except the consultant…’ (CT12).
IST는 CT 수련 기회와 관련하여 확장 수술팀(EST)을 긍정적인 조직 구조로 옹호했습니다. EST가 있는 조직의 참가자들은 EST 구성원이 제공하는 슈퍼비전 및 교육을 통해 전문직 간 및 직장 기반 학습과 관련하여 이점을 보고했습니다. 그러나 특정 전문과목에서는 그 반대의 결과가 나타났는데, 연장된 외과 팀원들이 CT에 적합한 수술 기회를 빼앗는다고 인식했습니다: IST advocated the extended surgical team (EST) as a positive organisational structure in respect of CT training opportunities. Participants in organisations with EST reported benefits in respect of interprofessional and workplace-based learning from supervision and training delivered by members of the EST. In certain specialties, however, the opposite happened; extended surgical team members were perceived to take away operative opportunities suitable for CTs:
'... 수련의 SNP(외과 전문간호사)가 가는 시간에 제가 심장 수술실에 가면, 그녀는 계속 그곳에서 일할 것이고 정맥을 잡는 방법을 배워야 하는 반면 저는 2개월 후에 떠날 것이기 때문에 수련의 SNP 아래로 강등됩니다. 그래서 저는 강등됩니다...'(CT43). ‘… if I go to cardiac theatre at the same time as the trainee SNP [surgical nurse practitioner] goes, I get demoted below the trainee SNP because she's going to be there to work forever, and needs to learn how to take a vein, whereas I'm leaving in 2 months. So, I get demoted …’ (CT43).
3.6 통제 시스템 3.6 Control systems
통제 시스템은 조직 내에서 개인을 모니터링하고 지원하는 공식적, 비공식적 방법을 말합니다. 이러한 통제 시스템은 무엇이 가치 있는지를 강조하고 어떤 행동과 태도가 기대되는지에 대한 신호를 보냅니다.64 Control systems refers to the formal and informal ways of monitoring and supporting individuals within the organisation. These control systems emphasise what is valued and send signal as to what behaviour and attitudes are expected.64
컨설턴트 외과 의사의 직무 계획 및 교육 거버넌스 구조와 같은 통제 시스템은 변화 실행의 장벽이자 촉진제 역할을 하는 것으로 나타났습니다. 일부 수련의는 병원 경영진과 협상하고 더 많은 수퍼비전 시간을 확보하기 위해 이 시스템을 사용하기도 했습니다: Control systems such as consultant surgeons' job plans and training governance structures seemed to act as both barriers and enablers of change implementation. Some trainers used the system to negotiate with hospital management and manoeuvre more supervision time:
'... 이 기준을 충족하지 못하면 수련생을 잃게 된다'고 말하는 것이 더 쉬웠습니다. 연수생을 잃으면 로테이션이 더 나빠지고 로컴과 이런저런 일에 돈을 다 써야 하니까... 그래서 그들은 자금을 찾았습니다'. (TR16). ‘… it was easier to say, if we don't meet these criteria, we'll lose a trainee. If we lose a trainee, then the rota becomes even worse, and you'd be spending all this money on locums and all of this sort of stuff … So, they found funding’. (TR16).
그러나 고위 경영진의 합의에도 불구하고 대부분의 트레이너의 직무 계획은 IST가 도입되었을 때 변경되지 않았습니다. 이는 과거의 규범을 반영하는 것으로 보였는데(앞의 이야기 참조), 트레이너들은 '실제로 직무 계획에 따라 일한 적이 없었고'(TR25), 대신 바쁜 임상 활동에서 슈퍼비전을 위한 시간을 쪼개서 일했습니다. 또한 많은 트레이너는 관리자가 슈퍼비전이 무엇인지 제대로 이해하지 못하기 때문에 추가 슈퍼비전 시간을 협상하는 것이 의미가 없다고 생각했습니다. However, despite agreement at higher levels of management, most trainers' job plans remained unaltered when IST was introduced. This seemed to be reflective of historical norms (seeStoriesearlier); trainers had ‘never really worked to a job plan’ (TR25), instead usually carving time for supervision out of busy clinical activities. Furthermore, many trainers believed there was no point in negotiating for additional supervision time because managers had a poor understanding of what supervision entailed.
'관리자들은 수퍼비전이 포함된 업무 계획, 이를 인정받기 위해 알아야 하는 업무량, 수련생과 함께 앉아 서류를 작성하는 것, 실제로 수련생과 마주 앉아 대화하는 것, 실제로 얼마나 많은 일이 수반되는지 잘 이해하지 못합니다'(TR21). ‘Managers don't really understand job planning with supervision, to get it recognised, the amount of work you know, sitting down with the trainees, filling out their paperwork, and actually just sitting down and talking to them, how much that actually involves’ (TR21).
4 토론 4 DISCUSSION
우리는 존슨의 문화 웹13 을 분석 프레임워크로 사용하여 외과 교육 및 훈련에 대한 국가 커리큘럼 개혁의 실행을 평가했으며, 평가 데이터에 따르면 각기 다른 곳에서 다르게 경험한 것으로 나타났습니다. We used Johnson's cultural web13as an analytical framework to evaluate the implementation of a national curricular reform of surgical education and training, which evaluation data suggested had been experienced differently in different places.
조직 문화가 스코틀랜드에서 외과 교육 훈련 개선(IST)을 시행하는 데 영향을 미친 방식을 파악하는 구체적인 연구 질문과 관련하여, 일상, 구조 및 시스템에 변화가 없거나 미미한 경우(예: 교육 시간을 확보하기 위해 컨설턴트의 업무 계획에 변화가 없는 경우) 실제로는 아무것도 바뀌지 않았으며 역사적 맥락이 우세한 것으로 나타났습니다. 이러한 문화적 요소에 변화가 발생한 경우(때로는 트레이너가 병원 내에서 IST를 협상 도구로 사용했기 때문)에는 변화의 증거가 일부 있었습니다. 소규모 외과 부서에서 IST 권장 사항을 더 쉽게 수용하는 경향이 있었습니다. 이러한 부서는 대규모 부서보다 상호 작용과 연결 문화가 더 강해 더 효과적인 변화에 기여할 수 있는 것으로 보였습니다.67 In terms of our specific research question, identifying the ways in which organisational culture influenced the implementation of Improving Surgical Training (IST) in Scotland, we found that where there was no or minimal change in routines, structures and systems (e.g. where there were no changes to consultants' job plans to free up time for training), then nothing really changed, and the historical context prevailed. Where changes in these cultural elements did occur—sometimes because trainers used IST as a negotiation tool within their hospital—there was some evidence of change. There was a sense that IST recommendations were more readily embraced in smaller surgical departments. These seemed to have more of a culture of interactions and connections than larger units, which likely to contribute to more effective change.67
우리는 트레이너의 현재와 과거의 감독 및 교육 경험이 핵심 외과 교육/수련의에 대한 가정과 기대 (스토리)에 영향을 미친다는 사실을 발견했습니다. 지역/병원마다 설정, 서비스 구성, 우선순위(조직 구조)가 미묘하게 달랐으며, 이는 변화를 실행하기 위해 과거의 관행과 신념에서 벗어날 준비가 되어 있는지에 영향을 미쳤습니다. 우리는 로테이션의 성격과 관리(의식과 일상, 조직 구조), 기관의 트레이너와 관련 보건 전문가의 태도와 신념(이야기와 상징)을 포함하여 IST의 제정에 대한 구체적인 장벽과 조력자를 확인했습니다. 트레이너와 관리자 간의 긴장도 데이터(통제 시스템)에 기술되어 있습니다. We found that trainers' current and past experiences of supervision and training influenced their assumptions and expectations of core surgical training/trainees (stories). Different localities/hospitals had subtly different set-ups, service configurations and priorities (organisational structures), which influenced their readiness to deviate from historic practices and beliefs to implement change. We identified specific barriers and enablers to the enactment of IST, including the nature of the rota and its' management (rituals and routines, organisational structures) and the attitudes and beliefs of an institutions' trainers and allied health professionals (stories and symbols). Tensions between trainers and managers were also described in our data (control systems).
우리는 몇 가지 요인이 우리가 관찰한 제한적인 변화를 설명할 수 있다고 잠정적으로 제안합니다. 첫째, IST는 외과 커리큘럼을 설정하고 직장 기반 외과 교육을 지원하는 영국의 4개 대학 중 하나인 영국 왕립 외과의 대학에서 개발했습니다. 그러나 외과 교육은 트레이너(컨설턴트)와 수련의를 고용하는 조직인 보건위원회와 병원에서 이루어집니다. 따라서 IST는 외부에서 추진되었습니다. 외부 동인은 강력한 변화의 동인이 될 수 있지만,68, 69 변화의 필요성에 대한 공유된 이해와 변화를 제공할 것으로 기대되는 사람들의 헌신이 있는 경우에만 가능합니다.70 외과의가 수련되는 조직(예: 병원)의 우선 순위는 교육이 아닌 서비스 제공이기 때문에 일부 환경에서는 IST가 변화를 위한 충분한 동인이 되지 못했을 수 있습니다.71, 72 마찬가지로, 병원 관리와 행정이 IST의 성공에 결정적인 역할을 했지만, 그들의 초점은 서비스에 있었으며 변화에 대한 인센티브나 투자는 거의 없었습니다.73-75 이러한 오래된 긴장은 외과나 스코틀랜드에만 국한된 것이 아닙니다.71, 72, 76 We tentatively suggest that several forces may explain the arguably limited change we observed. First, IST was developed by the Royal College of Surgeons of England, one of four UK Colleges responsible for setting the surgical curriculum and providing support to workplace-based surgical education. However, surgical education is delivered in Health Boards and hospitals, the organisations who employ the trainers (consultants) and trainees. IST was thus driven externally. External drivers can be powerful drivers of change,68,69but only where there is a shared understanding of the need for change and a commitment from those expected to deliver change.70IST may not have been a sufficient driver for change in some settings because the priority of those organisations in which surgeons are trained (i.e. hospitals) is service delivery not training.71,72Similarly, while hospital management and administration were crucial to the success of IST, their focus was service, and they had little incentive for or investment in change.73-75These age-old tensions are by no means unique to surgery or Scotland.71,72,76
이와 관련하여 외부 상황, 즉 더 넓은 환경이 변화의 성공에 큰 영향을 미칩니다.77 IST는 2018년에 시행되었으며, 변화에는 시간이 걸린다는 점을 인식하고 2020-2021년에 계획대로 데이터 수집이 이루어졌습니다. 그러나 데이터 수집이 코로나19 팬데믹으로 인해 외과 서비스 제공에 큰 차질을 빚으면서78, 79 서비스 교육에 대한 긴장이80, 81 확대되고 IST의 특정 측면, 즉 계획된 CT를 위한 시뮬레이션 기반 교육 이벤트 프로그램이 일시적으로 무력화되었습니다. 외부 자극이나 사건이 변화에 영향을 미친다는 점을 감안할 때,82 외과 훈련에 관련된 조직들은 코로나19의 혼란을 관리하는 데 너무 집중한 나머지 팬데믹 이전과 '정상 상태'에서 계획된 변화는커녕 다른 어떤 것도 감당할 여력이 없었다고 볼 수 있습니다. 코로나19 관리에 모든 관심과 행동의 초점이 맞춰져 있었습니다.83 Related to this, external context, the wider environment, is a major influence on change success.77IST was implemented in 2018, and appreciating that change takes time, our data collection took place as planned in 2020–2021. However, data collection then clashed with the Covid-19 pandemic, when surgical service delivery was heavily disrupted,78,79service-training tensions80,81magnified and specific aspects of IST—namely, the planned programme of simulation-based training events for CTs—disabled temporarily. Given that external stimuli or events impact on change,82we suggest that the organisations involved in surgical training were so focused on managing Covid-19 disruptions that they had no capacity for anything else, let alone change planned before the pandemic and for ‘steady state’ conditions. Managing Covid-19 was the focus of all attention and action.83
셋째, 외과 수련에는 수련을 제공하는 병원, 수련의 질 보증을 담당하는 스코틀랜드 NHS 교육부, 외과 왕립대학 등 다양한 조직이 관여합니다.84 이러한 다양한 조직은 모두 고유한 문화 또는 맥락을 가지고 있으며, 이는 IST 실행을 직접적으로 촉진하거나 형성했을 수 있으며, 왜 지역마다 (즉, 문화와 문화적 요소의 '조합'이 다른 곳에서) 성공이 다르게 보이는지 설명할 수 있습니다. (반면, 이에 대한 반론은 외과 교육에는 고유한 문화가 있으며,15,16 문화는 하나의 물리적 조직에 포함될 필요가 없으며,26 특정 환경이 고유한 장벽과 조력자를 가져올 수 있지만(데이터에 나타난 바와 같이), 문화는 하나의 물리적 조직에 내장될 필요가 없다는 것입니다.) Third, surgical training involves many different organisations—the hospitals in which training is delivered, the over-arching bodies such as NHS Education for Scotland who are responsible for quality assurance of training, and the Surgical Royal Colleges.84All these different organisations have their own cultures, or contexts, which may have directly facilitated or shaped IST implementation, explaining why it's success seemed to be different in different places (i.e. where the ‘combination’ of cultures and cultural elements differed). (On the other hand, the counter argument to this is that surgical training has its own over-arching culture,15,16and culture does not need to be embedded in a single, physical organisation,26although specific settings might bring their own barriers and enablers (as was indicated in our data).)
새로운 질문은 팬데믹 기간 동안 이루어진 변화가 어느 정도 유지되고 실무에 내재화되었는지, 그리고 외과 교육이 팬데믹 이전으로 돌아가 IST 주도의 변화를 재개할 수 있는지, 또는 실제로 재개해야 하는지에 대한 것입니다. The new questions are to what extent changes made during the pandemic have been maintained and embedded in practice and whether surgical training can—or indeed should—step back to pre-pandemic times, and resume IST-driven change.
모든 데이터 수집 접근법에는 장단점이 있습니다.55 팬데믹 기간 동안 가상 인터뷰는 다양한 상황에서 트레이너와 수련의로부터 응답을 얻을 수 있는 유일한 방법이었습니다. 처음에는 트레이너를 모집하는 데 어려움을 겪었기 때문에 연구 참여 초대를 두 번째로 진행했습니다. 이는 코로나19 팬데믹 때문이라고 판단하여 2차 팬데믹이 끝날 때까지 기다렸다가 트레이너에게만 2차 초대장을 보냈습니다. All data collection approaches have strengths and weaknesses.55During the pandemic, virtual interviews were the only way to obtain responses from trainers and trainees across many different contexts. We encountered difficulty with recruiting trainers initially, hence our second round of invitations to take part in the study. We believe this was due to the COVID-19 pandemic, so we waited until after (what was) the second wave of the pandemic before sending out second invitations to trainers only.
관리자를 참가자로 모집하면 조직 내에서 커리큘럼 개혁을 시행하는 데 있어 그들의 관점을 반영할 수 있었을 것입니다. 그러나 의학교육 책임자를 제외한 의료 관리자들은 IST 제안 논의 및 커리큘럼 개혁의 실행 단계에 참여하지 않았습니다(물론 이 점이 앞서 설명한 바와 같이 보고된 문제에 영향을 미쳤을 수 있습니다). Recruiting managers as participants would have afforded their perspective on enacting curricular reforms within their organisation. However, healthcare managers, other than Directors of Medical Education, were not involved in the IST proposal discussions and implementation stages of the curricular reform (This, of course, may have contributed to the issues reported, as discussed earlier).
다른 자발적 연구와 마찬가지로 참가자가 스스로 선택하는 요소가 있었을 것입니다. 그러나 결국 동일한 아이디어가 반복적으로 제시되고 새로운 주제(주제 포화도 또는 데이터 충분성85)가 나타나지 않자 데이터 수집을 중단하고 데이터가 일반적인 경험을 반영한다고 확신하게 되었습니다. As with any voluntary study, there would have been an element of participant self-selection. However, as eventually we saw the same ideas coming up repeated and no new themes (thematic saturation or data sufficiency85), we stopped data collection and feel confident that our data reflects common experiences.
초기 귀납적 데이터 분석에서 문화의 중요성이 드러났기 때문에 우리는 경영 문헌을 광범위하게 읽고 다양한 이론을 고려한 끝에 문화 웹 이론을 채택했는데, 이는 우리가 보기에 (과정적 모델이 아닌) 변화의 설명적 모델86로서 데이터를 이해하는 데 가장 적합한 프레임워크를 제공했기 때문입니다. 그러나 문화 웹은 조직 문화의 가시적인 측면만을 보여주기 때문에 눈에 잘 띄지 않는 다른 가정을 식별하고 밝혀내지 못하여 문화를 오해할 위험이 있습니다.87 실제로 변화 관리 문헌에서는 대부분의 변화 모델이 조직 변화의 성공에 영향을 미치는 모든 요인을 완전히 탐색하거나 표시하지 못하며88, 89 단일 모델 또는 몇 가지 모델만으로는 다양한 변화 상황을 다루기에 충분하지 않다는 사실에 대한 논의가 광범위하게 이루어지고 있습니다.90, 91 또한 문화 웹 프레임워크는 조직 문화의 다양한 측면을 표현하기 위한 프레임워크를 제공하지만, 6가지 요소가 어떻게 상호 연관되거나 중첩되는지 조사하기 위한 명시적인 메커니즘을 제공하지 않습니다. The initial inductive data analysis indicated the importance of culture so we read the management literature widely and considered many different theories before settling on cultural web theory because, in our view and as a descriptive model of change (rather than a processual one86), it offered the most fitting framework to make sense of the data. However, the cultural web only shows visible aspects of organisational culture: we may not have identified and uncovered other, less visible assumptions, running the potential risk of misunderstanding culture.87Indeed, there has been wider discussion in the change management literature about the fact that most models of change do not fully explore or display all factors that influence the success of organisational change88,89and the use of a single model or few models is not sufficient to cover various change situations.90,91Also, while the cultural web framework provides a framework for articulating different aspects of organisational culture, it does not offer any explicit mechanisms for examining how its six elements interrelate or overlap.
우리의 목표는 변화를 실행하는 것이 아니라 변화의 제정을 검토하는 것이었지만, 여러 가지 변화 모델을 결합하면 IST와 관련된 변화 프로세스에 대한 더 완전한 설명을 제공할 수 있었을 것입니다. 문화 웹 이론과 내부 요인과 외생적 사건 간의 상호 작용을 조사하는 이론을 결합하는 것이 특히 도움이 되었을 것입니다. While our aim was not to implement change, but rather to examine change enactment, combining several change models may have provided a fuller explanation of the change processes associated with IST. Combining cultural web theory with one which examines the interactions between internal factors and exogenous events may have been particularly helpful.
마지막으로, 어떤 이론도 데이터의 한 측면만을 조명할 뿐입니다.92 다른 관점에서는 관리자와 임상의 간의 관계의 성격, 이것이 변화에 미치는 영향93 또는 개별 조직(예: 여러 병원)의 변화 준비도 평가와 같이 문제의 다른 측면을 강조했을 수 있습니다.94 Finally, any one theory only illuminates one aspect of data.92Another lens may have emphasised different aspects of the problem, such as the nature of the relationships between managers and clinicians, and how this might have impacted on change93or an assessment of individual organisations (e.g. different hospitals) readiness for change.94
5 결론 5 CONCLUSION
'... 그래서 저는 올바른 교육 스타일을 찾는 것이 중요한 것이 아니라 어떻게 하면 개별 직장의 환경을 더 좋게 만들 수 있는지에 대한 고민이 더 중요하다고 생각합니다. 예를 들어 상사가 관심을 갖도록 하려면 어떻게 해야 할까요? 어떻게 하면 로테이션을 더 좋게 만들 수 있을까요? 어떻게 하면 사람들이 당신을 진지하게 받아들이게 할 수 있을까요?"(CT16). ‘… so, I think a lot of it is not about finding the right training style; it's just about how do you make what that individual place is like better. Like how do you make the bosses interested? How do you make the rota better? How do you make people take you seriously?’ (CT16).
Johnson의 문화 웹이라는 렌즈를 통해 본 데이터는 여러 병원 현장에서 다양한 수준의 성공을 거둔 커리큘럼 개혁의 작동 방식을 조명합니다. 이는 커리큘럼 개혁이 단순히 권장 사항을 실행에 옮기는 것이 아니라는 점을 강조합니다. 변화를 계획하고 평가할 때는 반드시 컨텍스트를 고려해야 합니다. Seen through the lens of Johnson's cultural web, our data illuminate the workings of a curricular reform that met with varying degrees of success across different hospital sites. This reinforces that curricular reform is not simply about putting recommendations into practice. Context must be taken into account when planning and evaluating change.
Med Educ. 2023 Jul;57(7):668-678.doi: 10.1111/medu.14994.Epub 2022 Dec 12.
Scratching beneath the surface: How organisational culture influences curricular reform
Introduction:Curricular reform is often proposed as the means to improve medical education and training. However, reform itself may not lead to noticeable change, possibly because the influence of organisational culture on change is given insufficient attention. We used a national reform of early-years surgical training as a natural opportunity to examine the interplay between organisational culture and change in surgical education. Our specific research question was: in what ways did organisational culture influence the implementation of Improving Surgical Training (IST)?
Methods:This is a qualitative study underpinned by social constructivism. Interviews were conducted with core surgical trainees (n = 46) and their supervising consultants (n = 25) across Scotland in 2020-2021. Data coding and analysis were initially inductive. The themes indicated the importance of many cultural factors as barriers or enablers to IST implementation. We therefore carried out a deductive, secondary data analysis using Johnson's (1988) cultural web model to identify and examine the different elements of organisational culture and their impact on IST.
Results:The cultural web enabled a detailed understanding of how organisational culture influenced IST implementation as per Johnson's six elements-Rituals and Routines (e.g. departmental rotas), Stories (e.g. historical training norms and culture), Symbols (e.g. feedback mechanisms, visibility and value placed on education), Power Structures (e.g. who has the power in local contexts), Organisational Structures (e.g. relationships and accountability) and the Control System (e.g. consultant job plans and service targets)-and how these interact. However, it did not shed light on the influence of exogenous events on change.
Conclusion:Our data reveal cultural reasons why this curricular reform met with varying degrees of success across different hospital sites, reinforcing that curricular reform is not simply about putting recommendations into practice. Many different aspects of context must be considered when planning and evaluating change in medical education and training.
잠재교육과정이 교수의 교육에 미치는 영향 밝히기: 질적 연구(Med Educ, 2023) Revealing the impact of the hidden curriculum on faculty teaching: A qualitative study Ciara Ann Lee1 | Timothy James Wilkinson2 | Julie Anita Timmermans3 | Anthony Naushad Ali4 | Megan Grayce Anakin5
1 소개 1 INTRODUCTION
교수진은 가르치는 일이 힘들다고 느낀다고 보고합니다. 교직원은 소진,1-3 불만1 및 인정받지 못한다고 느낄 수 있습니다.4-6 이 글에서는 '교직원'을 보건 전문직 프로그램에서 학생들을 가르치고 병원, 지역사회 및 기타 환경에서 사람들에게 의료 서비스를 제공하는 사람으로 정의합니다. 교수진은 급여를 받거나 교육 기관의 직원으로 공식적으로 인정받지 못할 수도 있습니다. 교수진이 가르치는 일이 힘들다고 느끼면 가르치고자 하는 동기가 떨어지고 보건 전문직 교육 프로그램에서 교수직을 떠날 수 있습니다.1 이러한 교수진 손실은 차세대 보건 전문가들이 교수 역할을 맡으려는 의지에 영향을 미치고 보건 전문직 교육을 빈곤하게 만들 수 있습니다.4 따라서 교육에 초점을 맞추는 것은 중요한 추구 사항입니다. Faculty report that teaching can feel demanding. Faculty can feel burnout,1-3dissatisfaction1and unappreciated.4-6In this article, we define ‘faculty’ as people who teach students in health professions programmes and who also provide health care to people in hospital, community and other settings. Faculty may or may not be paid or formally recognised as employees of educational institutions. When faculty feel that teaching is demanding, they may be less motivated to teach and leave their positions as teachers in health professions education programmes.1This loss of faculty may impact willingness of the next generation of health professionals to take on teaching roles and impoverishes health professions education.4A focus on teaching is therefore an important pursuit.
힘든 교수 경험은 개인이 절실하게 느끼지만, 교수직을 힘들게 느끼는 이유를 설명하는 한 가지 방법은 환경적 요인이 교수에게 어떤 영향을 미치는지 고려하는 것입니다.7,8 보건 전문직 교육 프로그램에서 교실 및 직장 학습 환경은 교수, 학생 및 지원 직원의 제도적 규범, 행동 및 태도, 전문직으로서 보건의료 및 교육에 뿌리내린 관행에 의해 형성됩니다. 숨겨진 커리큘럼이라는 개념은 교사가 교사로서의 정체성을 형성하고 유지하는 데 미치는 이러한 영향을 설명하는 데 유용한 방법이 될 수 있습니다.
'숨겨진 교육과정'이라는 용어는 학생들의 학습 경험과 보건의료 전문가로서의 정체성 형성에 암묵적 또는 명시적으로 영향을 미치는 교육 프로그램에서 제정된 기대와 가정을 설명하는 데 자주 사용됩니다.9-11
숨겨진 교육과정은 '우리가 의학교육이라고 부르는 삶의 공간에서 일어나는 일에 대해 일반적으로 통용되는 '이해', 관습, 의식, 당연시되는 측면'으로 광범위하게 정의되어 왔습니다.9 (404쪽)
교육 환경에서 행동에 대한 숨겨진 영향으로서 사회 구조의 영향은 처음에는 사회학에서 고려되었으며,10 '숨겨진 교육과정'이라는 용어는 1960년대에 처음 사용되었습니다.12
숨겨진 교육과정을 설명하는 데 사용된 용어에는 '비공식적', '암묵적', '잠재적', '그림자'12,13 등이 있으며, 모두 교육 구조, 규범 및 관행이 교수 학습에 미치는 복잡하고 종종 암묵적인 영향을 강조하기 위한 것입니다.
Although demanding teaching experiences are felt acutely by individuals, one way to explain why teaching might feel demanding can be to consider how environmental factors may be influencing faculty as teachers.7,8In health professions education programmes, classroom and workplace learning environments are shaped by institutional norms, behaviours and attitudes of faculty, students and support staff and the practices entrenched in health care and education as professions. The concept of a hidden curriculum might be a useful way to describe these influences on faculty to form and maintain their identity as teachers.
The term ‘hidden curriculum’ is often used to describe the expectations and assumptions enacted in educational programmes that tacitly or overtly impact students' learning experiences and the formation of their identity as health care professionals.9-11
The hidden curriculum has been broadly defined as the ‘commonly held “understandings”, customs, rituals, and taken-for-granted aspects of what goes on in the life-space we call medical education’.9(p404)
The impact of social structures as a hidden influence on behaviours in an educational setting was considered initially in sociology,10and the term ‘hidden curriculum’ was first used in the 1960s.12
Terms that have been used to describe the hidden curriculum include ‘informal’, ‘implicit’, ‘latent’ and ‘shadow’12, 13; all meant to emphasise the complex and often tacit influence of educational structures, norms and practices on teaching and learning.
숨겨진 교육과정은 학생들이 학습 기회에 참여하는 방식과 향후 진로에 대한 결정에 영향을 미칩니다.11, 14, 15 학생의 경우 숨겨진 교육과정은 의료 전문가로서의 정체성 형성에 영향을 미칠 수 있습니다.10, 11 마찬가지로 교수진을 위한 숨겨진 교육과정은 암묵적인 메시지를 전달하여 개인의 사회화에 영향을 주는 것으로 Hafler, Thompson 및 동료들에 의해 제안되었습니다. 그러나 교수진을 위한 숨겨진 커리큘럼의 개념은 잘 연구되지 않았습니다.13, 16 교수진을 위한 숨겨진 커리큘럼이 어떻게 운영될 수 있는지에 대한 추가 지식은 교수진 개발자에게 유용할 것이며, 이를 통해 소진 및 높은 교수진 이직률과 같은 부정적인 결과를 완화하는 데 도움이 되는 전략을 설계할 수 있습니다. 또한 이러한 지식은 교수진 개발 이니셔티브에 정보를 제공하는 데 사용될 수 있으므로 교수진은 교수 역할에서 성공할 수 있도록 지원받는다고 느낄 수 있습니다.
The hidden curriculum influences the ways students engage with learning opportunities and the decisions they make about their future careers.11,14,15For students, the hidden curriculum can impact on the formation of their identity as health care professionals.10,11Similarly, a hidden curriculum for faculty has been suggested by Hafler, Thompson and colleagues as communicating tacit messages, which influence an individual's socialisation into life as an academic. However, the notion of a hidden curriculum for faculty has not been well explored.13,16Further knowledge about how a hidden curriculum might operate for faculty would be useful for faculty developers, so they can design strategies to help mitigate negative outcomes such as burnout and high faculty turnover. This knowledge can also be used to inform faculty development initiatives, so faculty feel supported to thrive in their teaching roles.
교수진을 위해 숨겨진 교육과정이 어떻게 운영될 수 있는지 조사하는 한 가지 방법은 '숨겨진 교육과정'이라는 용어의 정의와 의학교육 문헌에서의 적용을 분석한 범위 검토의 결과를 기반으로 하는 것입니다.14 이 검토에서는 주로 학생 경험을 조사했으며 동기-심리, 대인관계-사회, 제도-조직, 맥락-문화 등 네 가지 연결된 개념적 경계를 제안합니다. 이러한 경계는 그림 1에 정의되어 있습니다. 상호 연결된 개념적 경계는 개인이 교육 프로그램 및 기관 내부와 외부에서 커리큘럼, 교수법 및 학습 환경과 관련된 요소와 가질 수 있는 상호작용에 대한 다면적이고 역동적인 관점을 강조합니다.12, 14 명확성을 위해 이 글의 나머지 부분에서는 다음 연구에서 개념적 프레임워크의 설명 및 사용과 혼동을 피하기 위해 이러한 개념적 경계를 숨겨진 교육과정의 '영역'으로 지칭할 것입니다. 우리는 하플러13가 설명한 교수진에 영향을 미치는 숨겨진 교육과정의 개념을 로렌스14의 범위 검토 결과에서 확인된 네 가지 영역과 통합하여 개념적 틀을 구성했으며, 주로 숨겨진 교육과정이 학습자에게 미치는 영향을 탐구했습니다. One way to investigate how a hidden curriculum could operate for faculty might be to build on findings from a scoping review that analysed definitions of the term ‘hidden curriculum’ and their application in the medical education literature.14This review examined student experiences primarily and proposes four linked conceptual boundaries: motivational–psychological, interpersonal–social, institutional–organisational and contextual–cultural. These boundaries are defined in Figure 1. The interlinked conceptual boundaries emphasise a multifaceted and dynamic view of interactions individuals may have with factors related to the curriculum, instructional methods and learning environments from within educational programmes and institutions and beyond.12,14For clarity, we will refer to these conceptual boundaries as ‘domains’ of the hidden curriculum for the remainder of this article to avoid confusion with the description and use of the conceptual framework for our study that follows. We constructed a conceptual framework by integrating the concept of the hidden curriculum impacting on faculty as described by Hafler13with the four domains identified in the results of the scoping review by Lawrence14that primarily explore the impact of the hidden curriculum on learners.
독자를 돕고 교수진을 위한 숨겨진 커리큘럼이 어떤 모습일지 설명하기 위해 가상의 비네팅을 구성하고 분석했습니다(그림 1 참조). 명확성을 위해 숨겨진 커리큘럼의 각 영역에 대해 개별적인 예를 사용했지만 서로 연결되어 있고 중복된다는 점을 인식하고 있습니다. To assist the reader and illustrate what a hidden curriculum for faculty might look like, we have constructed and analysed a fictional vignette (see Figure 1). For the purpose of clarity, we have used discrete examples for each domain of the hidden curriculum but recognise that they are interlinked and overlap.
교수진을 위한 숨겨진 커리큘럼에 대한 이해를 높이려면 더 많은 연구가 필요합니다. 10여 년 전 하플러와 동료들의 요청에도 불구하고,13 교수진을 위한 숨겨진 커리큘럼에 대한 연구는 제한적이었습니다. 200개가 넘는 논문이 Hafler와 동료들의 연구를 인용하고 있지만, 교수진을 위한 숨겨진 커리큘럼의 운영 측면과 관련된 연구 결과를 제시한 논문은 단 세 편에 불과합니다.
첫 번째는 전문성을 커리큘럼에 통합하는 데 실패한 이유를 조사한 연구였습니다.17 선임 교수진이 의도치 않게 전문성 교육의 중요성을 약화시킨 것으로 밝혀졌습니다.
두 번째 연구에서는 임상의가 진료 커뮤니티 내에서 교사로서의 정체성을 어떻게 발전시키는지 조사했습니다.18 숨겨진 커리큘럼은 교사의 정체성에 대한 신념과 실제 교육 관행 사이의 차이에 영향을 미치는 요인으로 제안되었으며, 이는 기관 문화에 의해 지속되는 것으로 생각됩니다.
세 번째 연구에서는 교사의 정체성, 특히 교수 역할이 교사의 정체성에 어떻게 통합되는지를 탐구했습니다.19 저자들은 교사의 정체성이 사회적으로 어떻게 구성되는지를 인식하면서 교사를 위한 숨겨진 커리큘럼의 증거를 제시했습니다.
More studies are needed to further our understanding of the hidden curriculum for faculty. Despite a call by Hafler and colleagues over a decade ago,13research into the hidden curriculum for faculty has been limited. Although more than 200 papers cite Hafler and colleagues' work, we identified only three papers that present findings related to aspects of a hidden curriculum operating for faculty.
The first was a study investigating why the integration of professionalism into a curriculum was unsuccessful.17Senior faculty were found to have unintentionally undermined the importance of teaching about professionalism.
The second study explored how clinicians develop their identities as teachers within communities of practice.18The hidden curriculum was suggested to be an influencing factor in differences between teachers' beliefs about their identities and their actual teaching practices, thought to be perpetuated by the institutional culture.
The third study also explored faculty identity, specifically how teaching roles are integrated into teacher identity.19In recognising how teacher identities are socially constructed, the authors suggested evidence of a hidden curriculum for faculty.
이 세 가지 연구에서 숨겨진 커리큘럼은 연구의 초점이 아니라 교수 경험에 대한 결과를 설명하는 데 사용되었습니다. 이 세 가지 연구는 의학교육 맥락에서만 교수진을 위한 숨겨진 커리큘럼에 대한 인사이트를 제공합니다. 따라서 숨겨진 커리큘럼이 더 일반적으로 교수진의 보건 전문직 프로그램에서 어떻게 운영될 수 있는지에 대한 지식에는 차이가 있습니다. 이 연구의 목적은 보건 전문직 교육에서 교수진을 위해 숨겨진 커리큘럼이 어떻게 운영될 수 있는지 설명하는 것이었습니다. For these three studies, the hidden curriculum was used to explain findings about teaching experiences rather than being the focus of the research. These three studies provide insights about the hidden curriculum for faculty in medical education contexts only. Consequently, there is a gap in our knowledge about how the hidden curriculum might operate with faculty health professions programmes more generally. The aim of this study was to explain how a hidden curriculum might operate for faculty in health professions education.
2 방법 2 METHODS
우리는 교육을 사회적으로 매개되는 활동으로 간주하는해석주의적 관점에서 이 연구에 접근했습니다. 여기서 지식은 개인이 역사적으로 영향을 받은 서로 및 주변 세계와의 상호 작용 패턴을 사용하여 공동 구성합니다. 이러한 관점은 서론에서 제시한 히든 커리큘럼의 정의 및 모델과 일치합니다. 우리는 교사의 숨겨진 교육과정에 영향을 미치는 요인을 도전의 현장이자 동시에 잠재적 혁신의 현장으로 볼 수 있기 때문에 까다로운demanding 교수 경험을 식별하는 것이 교사의 숨겨진 교육과정을 연구하는 생산적인 방법이라고 생각했습니다.20
우리는 까다로운 교수 경험을 보건 전문직 프로그램에서 학생들을 가르치거나 감독하는 동안 교사에게 고통, 불안 또는 기타 기억에 남을 수 있는 불리한 상황 또는 의도하지 않은 상황으로 정의했습니다.
We approached this research from an interpretivist perspective, where education is viewed as a socially mediated activity. Here, knowledge is co-constructed by individuals using historically influenced patterns of interaction with each other and the world around them. This perspective is consistent with the definition and model of the hidden curriculum presented in the introduction. We considered identifying demanding teaching experiencesto be a productive way of studying the hidden curriculum for faculty because the factors that influence the hidden curriculum for teachers can be viewed simultaneously as challenges and the sites of potential innovation.20
We defined a demanding teaching experienceas any unfavourable or unintended situation, while teaching or supervising students in health professions programmes that might have been distressing, disturbing or otherwise memorable to the teacher.
이 연구는 뉴질랜드 더니든과 크라이스트처치의 오타고 대학교에서 진행되었습니다. 다양한 보건 전문직(영양학, 의학, 약학, 간호학, 치과, 물리치료학)과 학습 환경(예: 대학 강의실, 병원 병동, 지역사회 의료기관)의 교수진을 대상으로 의도적인 표본 추출을 통해 개인이나 특정 상황에 국한되지 않고 근본적이고 공통적인 과정을 파악하고자 했습니다. 교수진은 일대일 반구조화 인터뷰에 참여하도록 초대되었습니다. 초청된 교수진은 연구의 목적, 주제, 방법 및 결과에 대한 정보를 제공받고 참여하기 전에 서면 동의를 받았습니다. 참가자들은 힘들었다고 생각되는 강의 경험의 예와 이를 어떻게 관리했는지 설명하도록 요청받았습니다. 참가자들은 개인적, 사회적, 조직적 영향과 영향을 포함하여 각 힘든 경험에 기여했을 수 있다고 생각되는 요인에 대해 설명하도록 권장되었습니다. 인터뷰는 2000년 4월부터 9월까지 제1저자가 직접 또는 화상 회의를 통해 실시했으며 디지털 오디오 녹음으로 진행되었습니다. The study took place the University of Otago in Dunedin and Christchurch, New Zealand. Purposive sampling was used to include faculty from a variety of health professions (dietetics, medicine, pharmacy, nursing, dentistry and physiotherapy) and learning environments (i.e. university classrooms, hospital wards and community health care workplaces) to identify a process that was fundamental and common rather than specific to individuals or particular contexts. Faculty were invited to participate in one-to-one semi-structured interviews. Invited faculty were provided information about the purpose, topic, methods and outcomes of the study and gave written consent before participating. Participants were asked to describe examples of teaching experiences that they felt were demanding and how they managed them. Participants were encouraged to describe factors they thought may have contributed to each demanding experience including possible personal, social and organisational influences and impacts. Interviews were conducted in-person or via video conferencing by the first author from April to September 2000 and digitally audiorecorded.
이 연구를 위해 구축된 개념적 프레임워크에 따라 연구팀은 모든 녹취록을 읽고 토론했습니다.
제1저자는 교사가 의도한 실습과 성취할 수 있는 것 사이의 관계로 까다로운 경험을 대표적 인용문으로 뒷받침되는 간략한 서면 설명으로 요약했습니다.
연구팀원 세 명(CL, TW, MA)이 녹취록을 다시 읽고 참가자가 각 경험을 힘들다고 느낀 이유와 관련된 정보를 코딩했습니다.
모든 녹취록을 독립적으로 코딩한 후, 세 명의 연구원이 만나 제한된 수의 코드에 합의했습니다.
코드는 각 코드 그룹 내의 관계가 식별되고 다른 그룹 내에서 식별된 관계와 구별될 때까지 그룹화 및 재그룹화되었습니다.
이러한 관계는 보건 전문직 프로그램에서 교육할 때 참가자를 위해 숨겨진 커리큘럼이 운영되는 방식으로 해석되었습니다.
분석의 견고성을 높이기 위해 JT와 AA에게 분석 결과를 제시했으며, 이들은 분석과 결과를 독립적으로 검토했습니다.
연구팀은 결과 섹션에 제시된 연구 결과에 대해 논의하고 합의를 도출하기 위해 모임을 가졌습니다.
Informed by the conceptual framework built for this study, the research team read and discussed all transcripts.
The first author summarised demanding experiences as relationships between a teacher's intended practice and what they could accomplish with brief written descriptions supported with representative quotations.
Three members of the research team (CL, TW and MA) re-read the transcripts to code information related to why the participant felt each experience was demanding.
Once all transcripts were coded independently, three researchers met to agree upon a limited number of codes.
Codes were grouped and regrouped until relationships within each group of codes were identified and were distinct from the relationships identified within other groups.
The relationships were interpreted as the way the hidden curriculum was operating for participants when teaching in health professions programmes.
To enhance the robustness of the analysis, the findings were presented to JT and AA who reviewed the analysis and findings independently.
The research team met to discuss and come to consensus about the findings presented in the results section.
2.1 저자의 반성 2.1 Author reflexivity
이 연구를 진행하는 동안 우리는 각 저자가 연구 과정에 가져온 경험과 세계관을 염두에 두었습니다. 연구팀은 고등 교육 및 보건 전문직 교육 학습 환경에서 임상의, 교사 및/또는 교수진 개발자로서의 다양한 경험을 보유하고 있었습니다. 이러한 배경 덕분에 참가자들이 경험하는 사건과 요구의 유형에 민감하게 반응할 수 있었습니다. 모든 저자는 교수진을 위한 숨겨진 커리큘럼이라는 개념에 익숙했고, 이 연구 참여자에게는 어떻게 나타날지 궁금했습니다. 또한 숨겨진 커리큘럼이 종종 강력하지만 항상 부정적인 것만은 아니라는 점을 인식하고 있었기 때문에 데이터에서 요구가 긍정적으로 표현될 수 있음을 알고 있었습니다. Throughout this study, we were mindful of the experiences and worldview that each author brought to the research process. Collectively, the research team possessed a range of experiences as clinicians, teachers and/or faculty developers in higher education and health professions education learning environments. Our backgrounds sensitised us to the type of events and demands experienced by our participants. All authors were familiar with the concept of a hidden curriculum for faculty, and we were curious as to how it might manifest for the participants in this study. We also recognised that a hidden curriculum, while often powerful, may not always be negative, so we were aware that demands could be expressed positively in our data.
3 결과 3 RESULTS
16명의 교수진과의 인터뷰를 실시하고 분석했습니다. 물리치료(5명), 의학(5명), 약학(3명), 치과(1명), 영양학(1명), 간호학(1명) 등 6개 직종에 종사하는 여성 9명, 남성 7명이 참여했습니다. 연구에 참여한 교수진에게 숨겨진 커리큘럼이 운영되고 있는 세 가지 방식을 확인했습니다. Interviews with 16 faculty members were conducted and analysed. Nine female and seven male participants spanned six professions: physiotherapy (five), medicine (five), pharmacy (three), dentistry (one), dietetics (one) and nursing (one). We identified three ways the hidden curriculum was operating for the faculty who participated in our study.
3.1 저평가된 교수 전문성 3.1 Undervalued teaching expertise
히든 커리큘럼의 운영은 교사들이 교육 전문성의 중요성을 저평가하는 이유를 설명할 수 있습니다. 우리는 참여자들이 교육 전문성에 부여하는 가치와 교육 기관이 교육 전문성에 부여하는 가치에 대한 인식 사이에 불일치가 있음을 확인했습니다. 이러한 불일치는 참여자에게 할당된 교수 역할의 유형, 교수 관련 자율성 부족, 임상 교사의 역할에 대한 기관의 이해 부족으로 설명되었습니다. The operation of a hidden curriculum can explain why teachers felt the importance of having teaching expertise was undervalued. We identified a mismatch between the value participants placed on teaching expertise and their perception of the value the institution placed on teaching expertise. This mismatch was illustrated by the types of teaching roles allocated to participants, a lack of teaching-related autonomy and a perceived lack of institutional understanding of a clinical teacher's role.
참가자들은 기관이 교육을 중시한다고 주장하지만, 현대 교육 학습 및 교육 접근법에 대한 사전 경험이나 준비 없이 교육 역할을 할당받았다고 설명했습니다. 전문 임상 지식과 교육 전문 지식이 혼재되어 있어 참가자들은 교육 기술의 중요성이 저평가되었다고 인식했습니다. 예를 들어, 참가자들은 임상 지식만으로는 학생들이 교육 과정의 학습 성과를 달성하는 데 충분하지 않은 과정을 책임지는 위치에 배치되었습니다. 임상적 통찰력에도 불구하고 참가자는 세션을 원하는 수준으로 전달할 수 있는 교육 전문 지식이 부족했습니다. 경험이 풍부한 한 임상의는 '[교육 세션을 진행하기 위한] 교육이 부족하다는 것을 뼛속 깊이 알고 있었다'(P8)고 말했습니다. Although participants perceived that the institution claimed to value teaching, they described being allocated teaching roles without any prior experience or preparation with contemporary educational learning and teaching approaches. The conflation of expert clinical knowledge with teaching expertise led participants to perceive that the importance of teaching skills was undervalued. For example, participants were placed in positions of responsibility for courses where their clinical knowledge alone was not enough to ensure that students achieved the learning outcomes of the course. Despite their clinical acumen, the participant lacked teaching expertise to deliver the session to the desired standard. One very experienced clinician ‘knew it in my bones that I didn't have the training to facilitate [a teaching session]’ (P8).
교육 전문 지식의 가치는 행정적 결정으로 인해 훼손될 수도 있는데, 이로 인해 참가자들은 자신이 가르치는 내용에 대한 통제력이 부족하거나 선배 동료들이 원하지 않는 역할을 할당받았다고 느꼈습니다. 한 참가자는 자신의 상황을 이렇게 설명했습니다. "처음 입사했을 때 저는 신입이었습니다. 그래서 제 전공이 아닌 [코스 설명]을 가르치게 했습니다."(P12). 참가자들은 자신의 전문 분야를 벗어난 강의를 해달라는 요청을 받았을 때 '거절할 수 없었다'(P8)고 느꼈습니다. 이러한 경험으로 인해 참가자들은 때때로 자신이 가르치는 내용이나 가르치는 방식에 대해 발언권이 거의 없다고 느꼈고, 이는 참가자들이 교사로서의 역할에 부여하는 가치와 상충되었습니다. 또한 동료들이 동기를 부여하지 않거나 강의 내용을 변경하지 않으려는 '교수진 화석화'(P1)로 인해 변화를 실행하는 데 어려움을 겪을 때 참여자의 자율성은 더욱 약화될 수 있었습니다. The value of teaching expertise could also be undermined by administrative decisions, which led to participants feeling that they lacked control over the content they taught or were allocated roles that senior colleagues did not want. One participant described their situation: ‘When I first arrived, I was a new guy. So they had me teach [description of course], which is not my specialty’ (P12). When participants were asked to teach outside of their professional scope of practice, they felt like they ‘couldn't say no’ (P8). These experiences led participants to feel, at times, that they had little say in what they teach or how it is taught, conflicting with the value participants placed in their role as a teacher. Participants' autonomy could also be further undermined when they faced difficulties enacting change due to ‘faculty fossilisation’ (P1), where colleagues were unmotivated or unwilling to change course content.
참가자들은 임상의, 연구자, 교사로서의 역할 사이에서 균형을 잡는 것에 대한 이해가 부족하다고 설명했습니다. 참가자들은 자신의 가르침이 학생들의 교육과 전문성 개발에 필수적이라고 생각했지만, 소속 기관에서 자신의 가르침을 우선순위로 여기지 않는다고도 느꼈습니다. '의과대학이 다른 교육 학부와 같지 않다는 대학 측의 이해 부족'이 있었다고 인식했습니다(P9). 참가자들은 교육은 '부업으로 하는 것'이라는 메시지를 받았습니다(P9). 참가자들은 환자 치료와 양질의 교육 사이에서 균형을 찾아야 했습니다: Participants described a lack of understanding about the challenge of balancing their roles as clinician, researcher and teacher. Participants felt their teaching was integral to the education and professional development of their students; however, they also felt that their teaching was not viewed by their institution as a priority. There was a perceived ‘lack of understanding from the university that the med school is not the same [as other teaching faculties]’ (P9). Participants received the message that teaching was something ‘that's done on the side’ (P9). Participants had to find a balance between delivering patient care and high-quality teaching:
환자가 보고, 듣고, 이해받고, 진단받고, 지원받고, 치료받는다고 느낄 수 있는 안전한 공간을 탐색하고, 그 공간에서 학생이 허둥대지 않고 학습할 수 있도록 하는 것입니다. (P15) It's navigating that safe place for the patient to feel seen and listened to, and understood, and diagnosed, and supported, and treated, and to leave the student to learn in that space and not letting them flounder. (P15)
참가자들은 이러한 균형을 유지하는 데 필요한 전문성이 저평가될 때 이러한 균형을 유지하는 것이 얼마나 어려운지 설명했습니다. Participants described how maintaining this balance was difficult when the expertise required to achieve such a balance was undervalued.
3.2 훼손된 교육 목표 3.2 Undermined teaching goals
숨겨진 커리큘럼의 운영은 교사들이 제도적 관습이 교육 목표를 훼손한다고 느낀 이유를 설명할 수 있습니다. 참가자들은 비판적으로 사고하고 자신의 지식을 임상 진료에 적용할 수 있는 참여적이고 전문적이며 독립적이고 혁신적인 의료인을 양성하고자 하는 열망을 설명했습니다. 이러한 열망은 학생 참여, 전문적 행동, 비판적 사고 및 학생 독립성에 영향을 미치는 사용 가능한 교육 방식 및 허용되는 실습 규범과 충돌할 수 있습니다. 학급 규모와 제한된 교사 수와 같은 물류 문제로 인해 학생들의 학습 참여가 더 어려워질 수 있습니다. 한 참가자는 대규모 학생 그룹과 마주했을 때 기술을 교육 전달에 통합하여 학습자의 참여와 협업을 촉진하려고 시도했습니다. 안타깝게도 공유 온라인 문서의 사용은 '의사소통과 토론을 방해'했습니다(P2). 강의 시간과 같은 대학 구조는 협업과 비판적 사고와 같은 학습 결과를 전달하기 어렵게 만들 수 있습니다: The operation of a hidden curriculum can explain why teachers felt that institutional conventions undermined their teaching goals. Our participants described a desire to develop engaged, professional, independent and innovative health practitioners who can think critically and apply their knowledge to clinical care. This desire may conflict with available teaching modalities and permissible practice norms that impact student engagement, professional behaviours, critical thinking and student independence. Engaging students in learning could be made more difficult by logistics, such as class sizes and limited numbers of teachers. One participant attempted to promote learner engagement and collaboration when faced with a large group of students by incorporating technology into the delivery of teaching. Unfortunately, the use of a shared online document ‘stifle[d] communication and discussion’ (P2). University structures, such as the timing of teaching sessions, could make learning outcomes such as collaboration and critical thinking harder to deliver:
목요일 오후 4시에 강의가 잡혀 있는 경우, 가끔은 상호작용을 할 수 없는 경우가 많았습니다. 사람들이 지쳐서 그런 거죠. 그리고 때로는 그 시점에서 큰 백기를 들고 이제 아무것도 배울 수 없으니 다른 것을 해보자고 말해야 할 때도 있습니다(P11). It's often been, often been late in the day sessions, you know, if I've been pinged with a four o'clock on a Thursday, sometimes you just, you're just not going to get that interaction. You're just, people are knackered. And sometimes at that point you just got to wave a big white flag and say, right, you're not going to learn anything now let's do something different (P11).
참가자들은 동료와 학생에게 비전문적인 행동을 용인하면서 전문적인 행동의 중요성을 강조하는 위선에 대해 설명했습니다. 한 참가자는 다른 교육자가 '조금 무례하다고 생각되는 말을 학생들에게 하는 것을 목격했습니다'(P2). 이 동료의 비전문적인 행동은 잘 알려져 있었지만, 학생과 교수진의 문제 제기에도 불구하고 계속 교육에 관여했습니다: '... 학생들이 이 사람에 대해 불만을 제기한 적이 있지만 아무 일도 일어나지 않는 것 같고... 다른 동료들도 고위 경영진에게 이 문제를 언급한 것으로 알고 있습니다'. 마찬가지로 학생들의 프로답지 못한 태도도 방치될 수 있습니다: Participants described the hypocrisy of promoting the importance of professional behaviours when unprofessional behaviours were tolerated from colleagues and students. One participant witnessed another educator ‘saying things to the students that I just thought was a bit rude’ (P2). The unprofessional behaviour of this colleague was well-known; however, they continued to be involved in teaching despite concerns being raised by students and faculty: ‘… students have complained about this person before, but nothing sort of seems to happen … And I know other colleagues have mentioned it to senior management as well’. Similarly, unprofessional attitudes of students could be left unchecked:
다른 컨비너들도 모두 같은 문제가 있었어요. 다른 진행자들도 마찬가지였습니다. 드문 일은 아니지만 경계에 대한 그녀의 존중 부족이 분명하게 반영된 것이죠. 그 어떤 것도 강제되지 않았습니다. (P10) I mean, all the other conveners had the same problem. She did the same thing … on her other runs. It's not unusual, but it is, her lack of respect for boundaries is a clear reflection of that. None had been enforced. (P10)
교사에게 제공되는 커리큘럼 구조는 전반적인 교육 목표와 모순될 수 있습니다. 참가자들은 순전히 지식 전달에만 초점을 맞춘 교수 학습 방법은 학생들이 임상 학습 환경에 들어가면 어려움을 겪을 수 있다고 지적했습니다. 이러한 환경에서 학생들은 적응력이 뛰어나고 제공된 정보에 대해 비판적으로 사고할 수 있어야 합니다: The curriculum structure provided to teachers could contradict the overall teaching goals. Participants noted that teaching and learning methods, which focused purely on knowledge transfer, could lead to student difficulties once students enter clinical learning environments. In these environments, students are expected to be adaptable and think critically about the information that is provided to them:
대학에 입학한 첫 3년 동안은 책이나 YouTube 동영상 등 어디서든 정보를 접할 수 있는 곳이라면 어디에서나 사실을 되새기며 지나갈 수 있습니다. 그러다가 임상 상황에 도착하면 갑자기 흑백으로만 보이던 것이 회색 음영으로 바뀝니다. (P14) The first three years of university, you can get by and regurgitating facts out of books or YouTube videos or wherever you access that information from. And then you arrive in the clinical situation and suddenly what used to be black and white has become a lot of shades of grey. (P14)
참가자들은 학생들을 지식 습득 모드에서 비판적 사고의 관점으로 전환하기 위해 비현실적인 기간이 주어질 수 있다고 설명했습니다. '정말 중요한 기술을 개발할 수 있는 시간이 3개월 정도밖에 없습니다'(P4). Participants described how they could be given unrealistic timeframes to shift students from a knowledge acquisition mode to a critical thinking perspective: ‘we've got like three months to develop these really important skills’ (P4).
환자 치료가 우선시되다 보니 임상 교육자들은 때때로 학습자의 독립성을 키우는 것이 어렵다는 것을 알게 되었습니다. 임상 학습 상황에서 참가자들은 환자의 안전을 보장하기 위해 학생의 독립성을 중단해야 했습니다. '어느 단계에서 시간이 부족해지면 학생에게 사과하고 시간이 부족하다고 말해야 합니다. 그들은 [임상의가] 대신해야 할 것입니다'(P15). The primacy of patient care meant that, at times, clinical educators found it challenging to foster learner independence. In a clinical learning context, participants were required to suspend students' independence in order to ensure patient safety: ‘And at some stage you run out of time and you need to apologize to the student and say, look, we're running out of time. They're [the clinician] going to have to take over’ (P15).
3.3 고립 대 협업 3.3 Isolation versus collaboration
숨겨진 커리큘럼의 운영은 일부 참가자들이 의료 서비스를 제공할 때 느꼈던 협업과 대조적으로 교사로서 고립감을 느낀 이유를 설명할 수 있습니다. 교사로서 역할을 수행하면서 참가자들은 협업의 장벽과 학생의 필요나 진행 상황에 대한 제한된 정보로 인해 고립감을 느낀다고 설명했습니다. The operation of a hidden curriculum can explain why some participants felt isolated as teachers in contrast to the collaboration they felt when providing health care. In their roles as teachers, participants described feelings of isolation due to barriers to collaboration and limited information available about student needs or progress.
참가자들은 협업 부족으로 인해 다른 교육자들로부터 배울 수 있는 기회가 제한되고 이용 가능한 지원이 부족하다고 인식되어 고립감을 느꼈다고 설명했습니다. 참가자들은 동료 교사로부터 배우고 관찰하고 싶지만 그럴 기회가 없었다고 입을 모았습니다: '다른 사람이 어떻게 가르치는지 실제로 관찰하는 것은 제가 경험해 본 적이 없는 일입니다'(P6). 참가자들은 '고립되어 있고, 주변에 팀이 없으니'(P9) 외로움을 느꼈고, 이러한 상황에 대해 '조금 굳어졌다'(P1)고 느끼며 동료들의 지원이 부족하다고 체념했습니다. 참가자들이 여러 역할을 수행하다 보니 교육과 학습에 대한 지원을 받기가 어려웠습니다: Participants described how a lack of collaboration resulted in isolation through limited opportunities to learn from other educators and a perceived lack of available support. Participants shared a desire to learn from and observe their peers teach but did not have the opportunity to do so: ‘Actually observing how somebody else teaches is not something I've had the pleasure of observing’ (P6). Participants felt alone: ‘You're isolated, you [have] not got the team around you’ (P9) and resigned to a lack of collegial support by feeling ‘a little bit hardened’ (P1) to the situation. The multiple roles performed by participants meant that support for teaching and learning was difficult to obtain:
4년차 프로그램에서 서로 다른 로테이션으로 튜토리얼을 운영하고 센터 간 물류를 조율하는 것의 모든 의미를 이해하는 사람은 극소수입니다. 그래서 많은 사람들에게 도움을 요청할 수는 없었어요. (P16) There's a very small number of people who understand all the implications of running a tutorial like that in the fourth-year program during different rotations and trying to coordinate the logistics across centres. So, I can't really ask too many people for help that in many respects. (P16)
참가자들이 고립감을 극복하기 위해 시도한 한 가지 방법은 동료들과 공식적, 비공식적 관계를 구축하는 것이었습니다. 이러한 관계는 참가자들이 이용할 수 있는 지원을 파악하는 데 도움이 되었습니다. 참가자들은 '통제 불능 상태가 되는 것을 막기 위해 비공식적으로 연락을 취하거나'(P15), 도움을 받을 수 있는 동료를 찾는다고 설명했습니다: '옆 방에 강사로 일하는 정말 좋은 직장 동료가 있는데, 정말 좋은 조언을 해주었습니다'(P12). 마찬가지로 교육 고문과 같은 교수진과의 공식적인 관계는 참가자들이 전문성 개발을 위한 지원을 받을 수 있음을 의미했습니다. '[교육 고문]에게 연락해서 방금 진행한 워크숍이 정말 형편없어서 도움이 필요하다고 말했죠! 며칠 만에 우리는 회의를 조직하고 몇 가지 아이디어를 브레인스토밍했습니다. (P2). Oneway participants tried to combat isolation was to build formal and informal relationships with colleagues. These relationships helped participants identify supports available to them. Participants described ‘informal catch-ups to try and prevent things spiralling out of control’ (P15) or identifying colleagues on whom they could rely for support: ‘I have a really good, um, office mate next door who is a lecturer as well, who gave me some really good advice’ (P12). Similarly, formal connections with faculty, such as education advisors, meant that participants could access support for professional development: ‘So I actually contacted [an education advisor] and I was like, this workshop I just had totally sucked and we need some help! Within a couple of days, we'd organized a meeting and we'd brainstorm some ideas’. (P2).
참가자들이 고립감을 느끼는 데 기여한 또 다른 요인은 학생들에 대한 정보가 제한적으로 공유되어 교육에 영향을 미쳤다는 점입니다. 이러한 상황은 최상의 치료를 제공하기 위해 환자에 대한 정보가 일상적으로 공유되는 임상 실습과는 대조적입니다. 참가자들은 학생을 만나기 전에는 학생이 어려움을 겪고 있거나 추가 학습 지원이 필요하다는 사실을 알지 못했다고 설명했습니다: '... 학생들이 어려움을 겪고 있다는 사실을 알기 전까지는 정보를 얻지 못하거나 전혀 얻지 못하기 때문에 조금 어렵습니다'(P7). 이러한 격차로 인해 참가자들은 자신이 제공하는 강의의 질이 영향을 받는다고 느낄 수 있습니다. '미리 알았더라면 실제로 그것에 맞춰 강의를 조금 더 조정할 수 있었을 텐데'(P7). 고립감은 프로그램 기간 동안 또는 프로그램 기간 내에 교육자에게 전달되지 않는 학생 진도에 대한 단면적인 스냅샷을 제공하는 평가 프로세스 때문일 수 있습니다. 참가자들은 현재의 평가 관행이 학생의 진도에 대한 제한된 관점을 제공함으로써 학생의 능력에 대한 우려로 이어진다고 느낀다고 설명했습니다: '어떤 영역에서는 학생들이 충분히 제대로 평가받지 못한 것 같아서 논문을 작성하게 되었습니다'(P4). Another factor, which contributed to participants' feelings of isolation, was the limited information shared about their students, which affected their teaching. This situation contrasts with clinical practice, where information about patients is routinely shared to deliver the best possible care. Participants described being unaware that students were having difficulties or required extra learning support prior to meeting them: ‘… it's a bit hard because we don't necessarily get information about the fact that the students are struggling until, or we don't at all’ (P7). This gap could lead to participants feeling that the quality of teaching they delivered was impacted: ‘If I'd known that beforehand, I would have actually been able to adapt my teaching around it a bit’ (P7). A feeling of isolation may be due to assessment processes that provide cross-sectional snapshots of student progress that are not communicated to educators across, or within, years of the programme. Participants described how they felt that current assessment practices meant that a limited view of student progress was obtained, leading to concern about students' abilities: ‘I feel in some areas they haven't been assessed robustly enough and then they come to our paper’ (P4).
4 토론 4 DISCUSSION
우리는 보건 전문직 프로그램에서 교수진에게 숨겨진 커리큘럼이 어떻게 운영될 수 있는지 설명하는 세 가지 방법을 확인했습니다. 이러한 설명에는 다음 등이 포함됩니다.
교수 전문성이 어떻게 평가되고 이해되는지,
교육 기관의 관습이 교육 목표에 어떤 영향을 미치는지,
교수진이 의료 전문가로서 경험하는 동료애에 비해 교사로서 고립감을 어떻게 느끼는지
이러한 설명은 미래의 의료 전문가를 교육하는 교사와 안전한 환자 치료를 제공하는 의료 전문가라는 두 가지 역할을 동시에 수행하려는 교수진에게 숨겨진 커리큘럼이 어떻게 운영될 수 있는지를 보여줍니다. 교수진 교육에 영향을 미칠 수 있는 요인을 파악할 수 있도록 교수진을 위한 숨겨진 교육과정 모델의 네 가지 영역14 과 관련하여 세 가지 주요 연구 결과를 논의합니다. 숨겨진 교육과정의 모든 영역이 작동할 가능성이 있지만, 각 결과에 대한 논의와 가장 관련성이 높은 영역만 명시적으로 언급한다는 점에 유의하는 것이 중요합니다. We identified three ways to explain how a hidden curriculum can operate for faculty in health professions programmes. These explanations involve
how teaching expertise is valued and understood,
how institutional conventions impact on teaching goals and
how faculty feel isolated as teachers compared to the collegiality they experience as health care professionals.
These explanations illustrate how a hidden curriculum can operate for faculty as they attempt to perform two roles simultaneously: as teachers who are educating future health care professionals and as health professionals who are ensuring the provision of safe patient care. We discuss the three main findings in relation to the four domains of the model of hidden curriculum for faculty14so that possible factors influencing faculty teaching can be identified. It is important to note that although all domains of the hidden curriculum are likely operating, we will only explicitly name domains that are most relevant to our discussion of each finding.
교수진을 위한 숨겨진 커리큘럼이 작동하는 것으로 보이는 한 가지 방법은 교육 전문 지식의 중요성이 저평가될 때입니다.숨겨진 교육과정의 동기-심리 및 제도-조직 영역과 관련된 요인은 특히 임상 업무 또는 연구 결과와 비교할 때 보건 전문직 교육자가 소속 기관에서 자신의 교육이 저평가되었다고 느끼는 다른 맥락의 결과와 이 결과를 이해하는 데 도움이 될 수 있습니다.4-6, 21, 22
참가자들이 설명했듯이, 교수진은 관련 교육 전문성 없이 교육 역할을 할당받을 수 있으며,23, 24 이는 자신의 진료 범위를 벗어난 임상 역할을 수행하지 않는 것과 대조될 수 있는 관행입니다. 교육 내용 지식의 개념은 교육과 관련된 지식과 실습을 식별합니다.25 교육 내용 지식은 교수 역할에 익숙하지 않은 교수진이 어려움을 겪는 이유를 이해하고 교수로서의 역량을 개발하기 위해 어떻게 지원할 수 있는지 파악하는 데 사용되었습니다.26
마찬가지로, 임상적 통찰력을 교육 전문성과 동일시하는 대학 정책 및 절차에 따라 교수진에게 전달되는 가정은 교수진이 취약성을 느끼고 자신의 역량을 의심하며 자신이 제공하는 교육의 질에 의문을 제기하게 할 수 있습니다. 이러한 상황은 보건 전문직 교육 전반에 걸쳐 나타납니다.27
One way a hidden curriculum for faculty appears to operate is when the importance of having teaching expertise is undervalued. Factors related to the motivational–psychological and institutional–organisational domains of the hidden curriculum can assist us to understand this finding and those from other contexts about health professions educators feeling that their teaching is undervalued by their institution, especially when compared to clinical work or research outputs.4-6,21,22
As our participants described, faculty may be allocated teaching roles without relevant teaching expertise,23, 24a practice, which may contrast with not being expected to undertake clinical roles outside one's scope of practice. The concept of Pedagogical Content Knowledgeidentifies knowledge and practice specific to teaching.25Pedagogical Content Knowledgehas been used to understand why faculty may struggle when new to a teaching role and identify how they can be assisted to develop competency as a teacher.26
Likewise, assumptions conveyed to faculty by university policies and procedures that equate clinical acumen with teaching expertise may lead faculty to feel vulnerable, doubt their capabilities and question the quality of teaching they provide. This situation appears across health professions education.27
교수진이 행동할 능력이 부족하다고 인식하면교육 기관에서 자신의 가시성에 의문을 제기할 수 있습니다.28 교육 목표를 훼손하는 영향은 숨겨진 커리큘럼의 문화적 맥락 영역에서도 식별할 수 있습니다. 예를 들어, 직장 학습 환경의 맥락에서 교육보다 건강 관리가 우선시되는 경우가 있는데, 이를 인정하지 않을 경우 교수진에게 필요한 교육 전문성을 약화시킬 수 있습니다. 교육보다 건강 관리를 우선시하는 것은 교직원과 학생에게 구조적인 장벽으로 작용할 수 있습니다. 현장 학습에 대한 구조적 장벽은 학생의 역량을 키우는 것을 더욱 어렵게 만들 수 있습니다.29 숨겨진 커리큘럼의 문화적 맥락적 경계에서 영향을 인식하면 직장 문화에 따라 교수진이 자신의 역할과 전문성을 어떻게 인식할 수 있는지 설명하는 데 도움이 될 수 있습니다. 교수진이 교육 관행을 개발하거나 변경하는 데 부서나 동료의 관성이 있다고 느끼는 경우, 기관의 정책과 절차에 도전할 자율성이 부족하다고 느낄 수도 있습니다. If faculty members perceive, they lack ability to act, then they may question their visibility in the institution.28Influences that undermine teaching goals can also be identified within the cultural–contextual domain of the hidden curriculum. An example is how health care is prioritised over teaching in workplace learning environments contexts, however, and when unacknowledged, it can undermine the teaching expertise required by faculty. Prioritising health care over teaching can act as a structural barrier for faculty and students. Structural barriers to on-the-job learning can make it more difficult to foster students' capabilities.29Awareness of influences in the cultural–contextual boundary of the hidden curriculum can assist us to account for how faculty may perceive their role and expertise are valued based on the workplace culture. When faculty feel there is inertia from departments or colleagues to develop or change teaching practice, they may also feel a lack of autonomy to challenge institutional policies and procedures.
교수진을 위한 숨겨진 커리큘럼이 운영되는 두 번째 방식은 교육 목표가 훼손되는 경우입니다. 교수진은 학생들이 의료 전문가로서 협동 실습을 할 수 있도록 준비시킨다는 교육기관의 목표에도 불구하고 학생의 참여와 협업을 제한하는 시간표와 커리큘럼 구조로 인해 어려움을 겪을 수 있습니다. 교육기관의 정책과 절차는 동료와 학생의 비전문직업적 행동을 방치할 수 있습니다. 숨겨진 커리큘럼의 제도적-조직적 및 동기-심리적 영역과 관련된 영향은 이러한 책무성과 책임감의 결여가 어떻게 수용 가능한 전문직업적 행동을 심어준다는 핵심 목표와 상충되는지 설명하는 데 사용될 수 있습니다. 이러한 연구 결과는 교수진을 위한 숨겨진 커리큘럼이 전문직업성 교육에 어떤 영향을 미칠 수 있는지 보여주는 연구에 추가됩니다.17 교수진을 위한 숨겨진 커리큘럼은 또한 우리의 행동이 비전문직업적 행동을 지속시키는 것과 같은 의도하지 않은 결과를 초래하는 방법을 더 고려할 수 있게 해줍니다. A second way a hidden curriculum for faculty appears to operate is when teaching goals are undermined. Faculty can be challenged by timetables and curriculum structures that limit student engagement and collaboration, despite the purported institutional goal of preparing students for collaborative practice as a health care professional. Institutional policies and procedures may allow unprofessional behaviours from colleagues and students to be left unchecked. Influences related to the institutional–organisational and the motivational–psychological domains of the hidden curriculum can be used to explain how this lack of responsibility and accountability is at odds with a core goal of instilling acceptable professional conduct. These findings add to work that shows how a hidden curriculum for faculty may influence the teaching of professionalism.17A hidden curriculum for faculty also allows us to further consider how our actions result in unintended consequences, such as perpetuating unprofessional behaviours.
교직원을 위한 숨겨진 커리큘럼이 작동하는 것으로 보이는 세 번째 방식은 교직원이 가르칠 때 고립을 보고하는 것입니다.이 발견은 교직원을 위한 숨겨진 커리큘럼의 동기-심리적, 대인관계-사회적, 상황-문화적 영역의 영향으로 설명할 수 있습니다. 종종 의료 전문가들은 최적의 환자 치료를 제공하기 위해 협력하고, 다양한 직종에 종사하는 개인의 전문성을 활용하여 환자의 경과를 모니터링하기 위한 정보를 공유합니다. 이러한 협업 관행은 교수진에게 교사로서의 역할에서도 유사한 협업과 정보 공유가 이루어질 것이라는 기대감을 심어줄 수 있습니다. 이러한 기대가 충족되지 않으면 교직원은 고립감을 느끼게 됩니다. 이러한 고립감은 고등 교육에서 학자들이 흔히 경험하는 것으로, 일반적으로 교사로서 우리는 '교실 문을 닫고 교육적 고독을 경험하는 반면, 학자로서의 삶에서는 활발한 커뮤니티의 일원'입니다.30 p6 임상의가 교사 역할을 맡으면 교사와 임상의로서의 경쟁 업무로 인해 다른 보건 전문 교육자로부터 배울 수 있는 기회와 교육 자원에 대한 접근성이 제한될 수 있습니다. 이러한 결과는 교수진에 대한 공동 지원과 관련된 연구에서 보고된 고립감과 지원의 필요성을 강화합니다.23 연구 참여자의 경우, 학생에 대한 정보가 교수진에게 제한적으로 제공되어 고립감이 악화될 수 있습니다. 학생 진도에 대한 단면적인 스냅샷은 교수진이 교사로서 자신이 생각하는 기준에 도달할 수 있도록 학생들에게 학습 기회를 제공하는 것을 어렵게 만들 수 있습니다.
A third way a hidden curriculum for faculty appears to operate encompasses the isolation faculty report when teaching. This finding can be explained by influences in the motivational–psychological, interpersonal–social and contextual–cultural domains of the hidden curriculum for faculty. Often, health professionals collaborate to provide optimal patient care and share information to monitor a patient's progress over time by drawing upon the expertise of individuals from different professions. This collaborative practice may set an expectation for faculty that there will be similar collaboration and information sharing in their role as teachers. When this expectation is not met, faculty feel isolated. This sense of isolation is a common experience of academics in higher education, more generally, where as teachers, we ‘close the classroom door and experience pedagogical solitude, whereas in our life as scholars, we are members of active communities’.30p6When clinicians take on the role of teacher, they may have limited access to educational resources and opportunities to learn from other health professional educators due to competing duties as teacher and clinician. These findings reinforce the isolation and need for support reported in a study involving collegial support for faculty.23For our participants, feeling isolated may be exacerbated by the limited information provided to faculty about their students. Cross-sectional snapshots of student progress can make it difficult for faculty to provide learning opportunities to their students that allows them to attain the standard they hold for themselves as teachers.
숨겨진 커리큘럼의 제도적-조직적 영역의 구조를 고려함으로써 교수진이 고립감을 완화할 수 있는 방법을 파악할 수 있었습니다. 교수진은 공식 및 비공식 동료 검토 및 멘토링에 대해 교수진 개발자에게 지침과 조언을 구하고 이러한 옵션을 교사로서 격려와 성장의 원천으로 활용할 수 있습니다. 비공식적인 동료 지원은 교사의 정체성 형성을 강화할 수 있지만23, 이러한 관행 자체도 숨겨진 커리큘럼의 적용을 받을 수 있습니다. 동료 지원은 또한 교사가 소속 기관으로부터 가치를 인정받는 데 도움이 될 수 있습니다.2,22 숨겨진 교육과정의 대인관계-사회적 영역에서 가능한 영향을 숙고함으로써 우리는 동료와 교류함으로써 고립감을 개선하려는 참가자들의 시도를 숨겨진 교육과정이 교사에 미치는 긍정적인 영향이라고 볼 수 있었습니다. 교수진이 자신의 고립감을 인식하고 지원을 구할 때, 그들은 자신의 상황을 개선하기 위해 숨겨진 커리큘럼의 측면을 해결하기 위해 제도적 구조를 사용할 수 있습니다. 교원은 '수동적인 졸이 아니라 교육기관 내에서 저항'31(2쪽)하는 행위를 통해 숨겨진 교육과정에 맞서 주체성을 행사하고 자신에게 가장 중요한 것을 드러낼 수 있다고 제안되었습니다.32 그러나 제도적 구조와 문화적 규범은 이러한 저항 행위에 대항하여31, 33 교원이 경험하는 고립을 지속하거나 심지어 강화할 수 있습니다. 교직원을 위한 숨겨진 커리큘럼의 동기-심리적 영역에 대해 생각하면 교직원에게 무엇이 중요한지 이해하고 이러한 이해를 활용하여 긍정적인 변화를 촉진할 수 있습니다. 향후 연구에서는 자기 결정 이론34과 같은 동기 부여 이론의 개념을 적용하여 교직원을 위한 숨겨진 커리큘럼의 개인적 동기 부여 영역을 보다 심층적으로 조사할 수 있습니다.
Considering structures in the institutional–organisational domain of the hidden curriculum allowed us to identify how faculty can mitigate their sense of isolation. Faculty may seek guidance and advice from faculty developers about formal and informal peer review and mentoring and use these options as sources of encouragement and growth as teachers. Informal peer support can strengthen teacher identity formation23; however, such practices themselves may also be subject to the hidden curriculum. Peer support can also help faculty to feel valued by their institution.2, 22By pondering possible influences from the interpersonal–social domain of the hidden curriculum, we were able to view our participants' attempts to ameliorate their isolation by engaging with colleagues as a positive impact of the hidden curriculum for faculty. When faculty recognise their isolation and seek supports, they may be using institutional structures to address aspects of the hidden curriculum to improve their situation. It has been suggested that faculty can exercise agency in the face of the hidden curriculum through acts of ‘resistance within education institutions rather than being passive pawns’31(p. 2)and reveal that which is most important to them.32Institutional structures and cultural norms, however, may counteract these acts of resistance,31, 33thereby perpetuating or even reinforcing the isolation experienced by faculty. Thinking about the motivational–psychological domain of the hidden curriculum for faculty allows us to understand what is important to faculty and use this understanding to promote positive change. A future study might apply concepts from a motivation theory, such as Self-Determination Theory34to probe more deeply into the personal–motivational domain of the hidden curriculum for faculty.
이 세 가지 주요 조사 결과를 종합해 보면, 숨겨진 교육과정이 교수진에 의해 상호 영향을 주고받으며 어떻게 경험될 수 있는지를 알 수 있습니다. 교수진이 교사로서의 역할이 저평가되고, 훼손되고, 고립되었다고 느끼는 것은 보건 전문직 교육에만 국한된 것이 아닙니다.22, 27 그러나 이러한 문제를 보건 전문직 교육에서 교수진을 위한 숨겨진 교육과정으로 구성하면 교사, 연구자 및 임상의로서의 역할을 수행하는 교수진에게 이러한 문제를 정당화하는 데 도움이 될 수 있습니다.4, 35-38 이 연구의 결과는 숨겨진 교육과정이 교수진이 교사로서의 역할을 수행하는 방식과 교사로서 자신을 보는 방식을 어떻게 형성하는지 이해하는 데 더 잘 사용될 수 있습니다. When these three main findings are viewed together, they illustrate how the hidden curriculum can be experienced as overlapping interacting influences by faculty. Faculty feeling that their role as teachers is undervalued, undermined and isolated is not unique to health professions education.22,27However, framing these issues as a hidden curriculum for faculty in health professions education might help legitimise these issues for faculty who take on roles as teachers, researchers and clinicians.4,35-38Findings from this study can be used to better understand how the hidden curriculum might shape how faculty enact their roles as teachers and how they view themselves as teachers.
연구 결과에는 교수진 개발자가 고려할 수 있는 몇 가지 시사점이 있습니다. 아마도 가장 유용한 인사이트는 교수진이 지금까지 '숨겨진' 것을 가시화할 수 있도록 지원하는 것과 관련이 있을 것입니다. '무언가를 '숨겨진 것'으로 분류하면 손댈 수 없거나 심지어 존재하지 않는 상태로 격상될 수 있습니다'12(528쪽)-우리는 이러한 결과를 피하고자 합니다. 우리는 숨겨진 것을 드러내어 가시화함으로써 의문을 제기하고 해결할 수 있도록 하고 있습니다.39 교수진 개발자는 숨겨진 교육과정의 네 가지 개념 영역을 사용하여 교육기관 맥락에서 운영되는 숨겨진 교육과정이 교수진에게 미치는 영향을 인식하고 시각화하는 데 도움을 받을 수 있습니다. 이 연구의 초점이 교육에 맞춰져 있으므로 향후 연구에서는 교수 역할의 다른 차원과 관련하여 숨겨진 커리큘럼을 조사할 수 있습니다. 교수진에게 숨겨진 커리큘럼이 어떻게 운영되는지 이해함으로써 교수진 개발자는 예를 들어 까다로운 교육 경험을 논의하기 위한 공통 언어를 개발하고 사용하는 등 보건 전문직 교육자가 임상 및 비임상 학습 환경에서 성공할 수 있도록 지원하는 도구를 더 잘 설계하고 공유할 수 있습니다. 향후 연구에서 탐구해야 할 한 가지 영역은 교수진이 교육 현장에서 직면한 문제를 해결하기 위해 '해결 방법'을 시작하고 유지하는 방법입니다. 이러한 해결 방법은 연구 결과에서 발견되었으며, 교수진이 문제나 이슈에 직접 직면하지 않고 해결책을 구현하는 방법을 나타냅니다. Our findings have several implications that faculty developers can consider. Perhaps the most useful insight involves assisting faculty to make the hitherto ‘hidden’ visible. ‘Labelling of something as “hidden” might elevate it to the status of untouchable or even non-existent’12(p. 528)—we want to avoid this outcome. We are uncovering the hidden to make it visible so that it can be questioned and addressed.39Faculty developers can use the four conceptual domains of the hidden curriculum to help recognise and visualise the influence of a hidden curriculum operating in their institutional contexts for their faculty. Given the focus of this study on teaching, a future study could examine the hidden curriculum in relation to other dimensions of the faculty role. By understanding how the hidden curriculum operates for faculty, faculty developers can design and share tools to better support health professions educators to thrive in clinical and nonclinical learning environments by, for example, developing and using a common language to discuss demanding teaching experiences. One area to explore in a future study is how faculty initiate and maintain ‘workarounds’ to address the challenges they faced in their teaching practice. These workarounds were present in our findings and represent the ways that faculty implemented a solution to resolve a problem or issue without confronting it directly.
이번 조사 결과는 스스로를 교사라고 밝힌 임상의에 국한됩니다. 향후 연구에서는 가르치지 않기로 선택했거나 스스로를 교사로 생각하지 않는 임상의의 관점을 조명할 수 있습니다. 참가자들에게 교수진에 대한 숨겨진 커리큘럼에 대한 인식을 직접 물었다면 연구 결과를 강화할 수 있었을 것입니다. 대신, 참가자들이 까다로운 교육 경험에 대한 이야기를 나눈 인터뷰 녹취록을 분석했습니다. 그러나 이러한 경험을 탐색하는 과정을 통해 교수들이 거주하는 '의학교육이라는 삶의 공간'9(404쪽)에 대해 깊이 이해할 수 있었고, 이러한 관점을 숨겨진 교육과정에 대한 이해를 통해 설명할 수 있었다고 생각합니다. 우리의 연구 결과가 현재 문헌에 추가되어 더 많은 논의와 확장을 촉진할 수 있기를 바랍니다. Our findings are limited to clinicians who self-identify as teachers. A future study may shed light on the views of clinicians who choose not to teach or who do not view themselves as teachers. Asking participants directly about their perceptions of the hidden curriculum for faculty may have strengthened our research findings. Instead, we analysed interview transcripts where participants shared stories of demanding teaching experiences. Through the process of exploring these experiences, however, we feel that we were able to gain a deep understanding of the ‘life-space we call medical education’9(p404)which faculty inhabit and were able to explain these perspectives through our understanding of the hidden curriculum. It is hoped that our results can add to the current literature and prompt further discussion and expansion.
5 결론 5 CONCLUSION
우리는 보건 전문직 프로그램에서 교수진을 위해 숨겨진 커리큘럼이 어떻게 운영될 수 있는지 설명하는 세 가지 방법을 확인했습니다. 이러한 설명에는 교육 전문 지식의 중요성이 어떻게 저평가되는지, 교육 목표가 어떻게 훼손되는지, 교수진이 의료 전문가로서 경험하는 동료애에 비해 교사로서 어떻게 고립감을 느끼는지 등이 포함됩니다. 교수진을 위한 숨겨진 커리큘럼은 교육에 대한 가정, 기대 및 행동을 확립하고 유지하는 구조, 규범 및 관행에 의해 강화되는 것으로 보입니다. 연구 결과는 숨겨진 커리큘럼이 여러 겹치는 영역에서 작동하는 것으로 시각화되어 교수진이 자신과 자신의 역할을 보는 방식을 어떻게 형성할 수 있는지 보여줍니다. 이러한 인사이트는 교수진 개발자가 숨겨진 커리큘럼을 가시화하여 보건 전문직 교육자를 지원하는 데 사용할 수 있습니다. We identified three ways to explain how a hidden curriculum can operate for faculty in health professions programmes. These explanations involve how the importance of teaching expertise is undervalued, how teaching goals are undermined and how faculty feel isolated as teachers compared to the collegiality they experience as health care professionals. The hidden curriculum for faculty appears to be reinforced by structures, norms and practices that establish and maintain assumptions, expectations and behaviours about education. Our results show how the hidden curriculum can be visualised as operating in multiple, overlapping domains and shape how faculty see themselves and their roles. These insights may be used by faculty developers to help make the hidden curriculum visible, and, thereby, support health professions educators.
Med Educ. 2023 Aug;57(8):761-769.doi: 10.1111/medu.15026.Epub 2023 Feb 14.
Revealing the impact of the hidden curriculum on faculty teaching: A qualitative study
Introduction:In health professions education, faculty may feel frustrated or challenged by aspects of their teaching. The concept of a hidden curriculum for students describes the expectations and assumptions enacted in educational programmes that tacitly impact students' learning experiences. A hidden curriculum has been suggested as a possible influence on faculty but has not been well explored. The aim of this study was to explain how a hidden curriculum might operate for faculty in health professions education.
Methods:An interpretivist perspective was used to frame this qualitative study that examined one-on-one interview data generated with 16 faculty members from six different health care professions. Participants were asked to describe teaching experiences that they perceived as demanding. Using a hidden curriculum framework, descriptions of demanding teaching experiences were analysed inductively to identify relationships between a teacher's intended practice and what they could accomplish. These relationships were interpreted as the possible ways that a hidden curriculum was operating for faculty.
Results:A hidden curriculum for faculty was found to operate in three ways by undervaluing the importance of having teaching expertise, undermining teaching goals through institutional conventions and perpetuating feelings of isolation.
Discussion:A hidden curriculum for faculty can be represented as multiple overlapping domains and shape how faculty experience their teaching roles. The results provide examples that reveal how a hidden curriculum may operate for faculty. Faculty developers may find the insights provided by this study useful to make the hidden curriculum visible and help their faculty make sense of and navigate demanding teaching experiences.
강의평가는 가르침의 질 저하와 성적 인플레이션을 조장한다: 이론적 및 실증적 분석(BASIC AND APPLIED SOCIAL PSYCHOLOGY, 2020) Student Evaluations of Teaching Encourages Poor Teaching and Contributes to Grade Inflation: A Theoretical and Empirical Analysis Wolfgang Stroebe
학생 교수 평가(SET)는 1920년대에 퍼듀 대학교의 교육 심리학자 Herman H. Remmers(예: Remmers & Brandenburg, 1927)와 워싱턴 대학교의 학습 심리학자 Edwin R. Guthrie(예: Guthrie, 1953)에 의해 독자적으로 개발되었습니다. Remmers와 Guthrie는 대학 교사에게 자신의 강의가 학생들에게 어떻게 인식되고 있는지에 대한 정보를 제공하여 필요한 경우 개선하는 데 도움을 주고자 했습니다. 그들은 이러한 강의 평가에 대한 접근 권한을 강의 교사에게만 제한하려고 했습니다. 1953년 거스리는 "이 정보를 궁극적인 능력의 척도로 받아들이는 것은 심각한 오용이 될 것"(221쪽)이라고 경고했지만, SET는 곧 대학 관리자들에게 중요한 정보원이 되었고, 이들은 이를 능력 향상 및 승진에 대한 결정의 근거로 사용했습니다. Student Evaluations of Teaching (SETs) were independently developed in the 1920s by the educational psychologist Herman H. Remmers at Purdue University (e.g., Remmers & Brandenburg,1927) and the learning psychologist Edwin R. Guthrie (e.g., Guthrie,1953) at the University of Washington. Remmers and Guthrie wanted to provide university teachers with information about how their teaching was perceived by students and thus help them to make improvements, where necessary. They intended to limit access to these course evaluations to course teachers. Even though Guthrie warned in 1953 that “it would be a serious misuse of this information to accept it as ultimate measure of merit” (p. 221), SETs soon became valued sources of information for university administrators, who used them as a basis for decisions about merit increases and promotion.
일반적인 SET는
학생들에게 코스 교사에 대한 인식을 묻는 양식으로 구성되며,
보통 매우 동의함부터 매우 동의하지 않음까지 5점 리커트 척도로 평가하도록 되어 있습니다
. 학생은 교수자와 코스에 대한 전반적인 평점을 매기도록 요청받습니다.
또한 강사의 특정 특성(예: 지식, 공정성, 도움됨)과 코스의 특정 특성(예: 조직, 난이도, 유익함)을 평가하도록 요청받습니다.
그런 다음 모든 학생과 각 평가 항목 및 모든 평가 항목에 대해 평균 평점이 계산됩니다.
이러한 평균 평가는 종종 학과 또는 학부의 다른 교수들이 받은 평가와 비교하여 교수의 교육 효과를 평가하는 데 사용됩니다(Uttl 외., 2017).
The typical SET
consists of forms that ask students to rate their perception of course teachers,
often on 5-point Likert scales, ranging fromstrongly agreetostrongly disagree.
Students are asked to give overall ratings of both their instructor and their course.
In addition, they are asked to rate specific characteristics of the instructor (e.g., knowledge, fairness, helpfulness) and of the course (e.g., organization, difficulty, informative).
Mean ratings are then computed across all students and for each rated item, as well as across all rated items.
These mean ratings are often used to evaluate a professor’s teaching effectiveness by comparing them with ratings received by other professors in the department or in the faculty (Uttl et al.,2017).
1973년에는 29%의 대학만이 SET를 수집했지만, 1983년에는 68%, 1993년에는 86%로 증가했습니다(Seldin, 1998). 2010년에 실시된 설문조사에 따르면 94%의 대학에서 SET를 수집하고 있으며, 거의 모든 학장이 강의실 수업이 교수진 성과 평가의 주요 부분이라고 답했으며, 일반적으로 강의실 수업의 질에 대한 주요 정보 출처는 SET라고 답했습니다(Miller & Seldin, 2014). Whereas in 1973 only 29% of colleges collected SETs, this practice increased to 68% in 1983 and to 86% in 1993 (Seldin,1998). A survey conducted in 2010 indicated that SETs were collected in 94% of colleges, that nearly all deans declared that classroom teaching was a major part of the performance evaluation of their faculty, and that SETs were usually their main source of information about the quality of classroom teaching (Miller & Seldin,2014).
승진 및 임기 결정의 근거로 SET를 사용하는 것은 SET가 교수 효과와 학생 학습의 유효한 척도인 경우에만 정당화됩니다. 그러나 그렇지 않은 경우도 있습니다(예: Boring et al., 2016; Uttl et al., 2017). 이는 코스에 대한 학생의 만족도를 반영하는 것일 가능성이 높으며, 이는 교육 효과와 무관한 여러 요인에 의해 영향을 받을 수 있습니다(Freishtat, 2016). 이 글의
첫 번째 섹션에서는 SET가 학생 학습의 유효한 척도가 아니라는 증거를 제시합니다.
두 번째 섹션에서는 SET가 어떻게 부실한 교수를 조장하고 성적 인플레이션을 유발하는지 보여주는 프로세스 모델을 제안합니다.
세 번째 섹션에서는 과정 모델에서 가정하는 과정에 대한 증거를 검토합니다.
네 번째 섹션에서는 성적 인플레이션의 정도를 설명하고 이러한 인플레이션 과정의 어두운 측면에 대해 논의합니다.
마지막으로, SET의 책임감 있는 사용에 대한 결론을 논의합니다.
The use of SETs as a basis for decisions on promotion and tenure is justified only if SETs are a valid measure of teaching effectiveness and student learning. But they are not (e.g., Boring et al.,2016; Uttl et al.,2017). They are most likely a reflection of students’ satisfaction with a course, which can be influenced by many factors that are unrelated to teaching effectiveness (Freishtat,2016).
In the first section of this article, evidence is presented that SETs are not a valid measure of student learning.
In the second section a process model is proposed, showing how SETs encourage poor teaching and cause grade inflation.
The third section reviews evidence for the processes assumed by the process model.
The fourth section illustrates the extent of grade inflation and discusses the dark side of this inflationary process.
Finally, conclusions about a responsible use of SETs are discussed.
교수에 대한 학생 평가의 타당성에 대해 On the validity of student evaluations of teaching
SET는 안면 타당성이 매우 높습니다. 결국, 학생들은 많은 코스를 수강하므로 특정 강사가 효과적인 강사인지 판단할 수 있어야 합니다. 이러한 가정을 뒷받침하는 증거는 학생의 코스 평가가 해당 코스에서 받은 성적과 양의 상관관계가 있다는 것입니다. 다음의 가정을 하면 이 가정을 뒷받침하는 것으로 해석할 수 있습니다.
(a) 학생은 좋은 교사로부터 더 잘 배울 것이다
(b) 코스 성적은 학습의 좋은 척도이다
(c) 학생은 강사의 강의 품질을 평가할 수 있다.
그러나 한 수업의 모든 학생이 동일한 강사에게 노출되기 때문에 더 많이 배우는 학생이 그 강사를 더 나은 교사로 인식하는지에 대해 의문을 가질 수 있습니다. 또 다른 근본적인 비판은 학생의 코스 성적과 교수자에 대한 평가 사이의 상관관계가 편견을 반영할 수 있다는 것입니다. 학생은 코스 종료 시점에 코스 성적을 받지만, 일반적으로 이미 예상되는 성적을 잘 알고 있습니다. 편향 해석은 좋은 성적을 받을 것으로 예상하는 학생이 나쁜 성적을 받을 것으로 예상하는 학생보다 교사를 더 긍정적으로 평가한다고 가정할 수 있습니다.
SETs have a great deal of face validity. After all, students take many courses and should therefore be able to judge whether a particular instructor is an effective teacher. Supporting this assumption is the evidence that students’ course evaluations are positively correlated with the grades they received in those courses. This can be interpreted as supportive if we make the following assumptions:
(a) Students learn more from good teachers,
(b) course grades are a good measure of learning, and
(c) students are able to evaluate the quality of the teaching of their instructor.
However, because all students in a class are exposed to the same instructor, one could wonder if students who learn more also perceive him or her as a better teacher. Another more fundamental critique is that the correlation between students’ course grades and their evaluation of a teacher might merely reflect bias. Although students receive their course grades at the end of a course, they typically already have a good idea what to expect. A bias interpretation would assume that students who expect to receive a good grade evaluate a teacher more positively than students who expect to receive a poor grade.
교수에 대한 학생 평가에 대한 여러 섹션 연구 Multisection studies of student evaluations of teaching
이 두 가지 해석을 구분하는 한 가지 방법은 한 수업 집합의 평균 SET 점수가 해당 수업의 평점 평균(GPA)과 상관관계가 있는 경우 코스 성적과 SET 간의 관계가 유지되는지 테스트하는 것입니다. SET가 편향성이 아닌 교수 효과를 반영하고 코스 성적이 학습을 반영하는 경우, 수업 집합의 평균 SET는 해당 수업의 평균 GPA와 양의 상관관계를 가져야 합니다. 이 예측은 다중 섹션 코스에서 테스트되었습니다.다중 섹션 코스는 각각 다른 교수자가 가르치는 여러 개의 병렬 섹션으로 분할된 코스입니다. 최적의 다중 섹션 코스는 다음 요구 사항을 충족해야 합니다:
(a) 동일한 자료를 가르치는 여러 섹션이 있어야 하고,
(b) 각 섹션은 다른 교수자가 가르쳐야 하며,
(c) 학생이 스스로 선택하지 않도록 섹션에 무작위로 배정되어야 하고,
(d) 모든 섹션은 동일한 중앙 관리 시험으로 평가되어야 하며,
(e) 시험 직전 또는 시험과 함께 SET를 시행해야 합니다.
One way to distinguish between these two interpretations is to test whether the relationship between course grades and SETs would be maintained if the correlation of the average SET scores of a set of classes were correlated with the grade point average (GPA) of those classes. If SETs reflect teaching effectiveness rather than bias, and if course grades reflect learning, then the average SET of a set of classes should be positively correlated with the average GPA of these classes. This prediction has been tested withmultisection courses.These are courses that are split into a number of parallel sections, each taught by a different instructor. An optimal multisection course should meet the following requirements:
(a) It should have many sections in which the same material is being taught,
(b) each section should be taught by a different instructor,
(c) students should be randomly assigned to these sections to avoid self-selection,
(d) all sections should be assessed with the same centrally administered exam, and
(e) SETs should be administered either just before or with the exam.
나중에 설명할 Boring 등(2016)의 연구에서 모든 1학년 학생들은 동일한 필수 과목을 수강했습니다. 각 과목에서 한 명의 교수가 약 900명의 학생을 대상으로 주요 강의를 진행했습니다. 과목은 10~24명의 학생으로 구성된 섹션으로 나뉘어 강사가 가르쳤습니다. 모든 학생이 치르는 기말 시험은 코스 교수가 출제했습니다. 학생들이 학습한 양이 많은 섹션을 학습한 양이 적은 섹션보다 더 긍정적으로 평가한 경우(그리고 시험이 학생 학습의 유효한 척도인 경우), 섹션 평균 세트는 섹션 평균 성적(GPA)과 양의 상관관계가 있어야 합니다. 학생을 무작위로 섹션에 배정하는 것이 불가능한 경우가 많으므로 일부 다섹션 연구에서는 사전 학습 또는 능력의 지표(예: 전체 GPA, SAT 점수)에 따라 최종 성적을 보정합니다. 다중 섹션 설계는 SET의 유효성에 대한 연구에서 가장 표준적인 방법으로 간주됩니다(예: Abrami et al., 1990; Cohen, 1981, 1983; Feldman, 1989). In a study by Boring et al. (2016) to be described later, all 1st-year students took the same mandatory courses. In each course, main lectures were given by a professor to approximately 900 students. Courses were divided into sections of 10–24 students taught by instructors. The final exam, taken by all students, was written by the course professor. If students rated sections in which they learned a great deal more positively than sections in which they learned little (and if the exam was a valid measure of student learning), average-section SETs should correlate positively with average-section grades (GPA). As it is often impossible to assign students randomly to sections, some multisection studies correct final grades by indicators of prior learning or ability (e.g., overall GPA, SAT scores). The multisection design is considered the gold standard in research on the validity of SETs (e.g., Abrami et al.,1990; Cohen,1981,1983; Feldman,1989).
이러한 다중 섹션 연구에 대한 초기 메타 분석(예: Cohen, 1981; Feldman, 1989)에서는 SET 평균과 GPA 사이에 중간 정도의 양의 상관관계가 있다는 결론을 내렸습니다. 가장 영향력 있는 메타 분석은 68개의 다중 섹션 연구를 기반으로 한 Cohen의 메타 분석으로, 이 중 67개 연구에서 유용한 데이터를 제공했습니다. 전체 강사 평점과 GPA 간의 평균 상관관계는 r = .43으로, 중간 정도의 큰 효과를 보였습니다. Cohen(1981)의 메타 분석과 이후 Feldman(1989)의 메타 분석에 대한 비판에서 Uttl 등(2017)은 대부분의 다중 섹션 연구에 포함된 섹션 수가 다소 적고 이러한 소규모 연구는 종종 상관관계가 매우 높았다고 지적했습니다. 예를 들어, 코헨의 다중 섹션 연구 중 1/3 이상이 섹션 수가 10개 이하였습니다(Uttl 외, 2017). 이러한 저자들이 표본 크기를 보정했다면 이 문제는 덜 심각했을 것입니다. 그러나 Uttl 등(2017)이 비판한 것처럼, 이러한 메타 분석은 표본의 크기와 관계없이 모든 연구에 동일한 가중치를 부여했습니다. Cohen(1981)은 최소 20개 이상의 섹션을 사용한 연구를 분석한 결과 평균 상관관계가 .37로 더 낮았다고 보고했지만, 이것이 문제가 될 수 있다고 부인했습니다. Uttl 등(2017)은 30개 이상의 섹션을 사용한 다중 섹션 연구만을 기준으로 분석할 경우 상관관계는 r = .27로 감소한다고 덧붙였습니다. Early meta-analyses of such multisection studies (e.g., Cohen,1981; Feldman,1989) concluded that there was a moderately positive correlation between SET averages and GPAs. Most influential was the meta-analysis of Cohen, which was based on 68 multisection studies of which 67 provided useful data. The average correlation between overall instructor ratings and GPA wasr= .43, a moderately large effect. In a critique of Cohen’s (1981) meta-analysis, as well as the later meta-analysis by Feldman (1989), Uttl et al. (2017) pointed out that the number of sections included in most of their multisection studies was rather small and that these small studies often had extremely high correlations. For example, more than one third of Cohen’s multisection studies had 10 or fewer sections (Uttl et al.,2017). This would have been less of a problem if these authors had corrected for sample size. However, as Uttl et al. (2017) criticized, these meta-analyses gave the same weight to all studies, independent of their sample size. Cohen (1981) denied that this could be a problem, even though he reported that an analysis of studies that used at least 20 or more sections resulted in a lower average correlation ofr= .37. As Uttl et al. (2017) added, the correlation is reduced tor= .27 if one bases one’s analysis only on multisection studies with 30 or more sections.
Clayson(2009)의 최근 메타 분석에 따르면 SET와 학습 간의 가중치 없는 평균 상관관계는 r = .33인 반면, 표본 크기에 따라 가중치를 둔 상관관계는 r = .13에 불과하다고 보고했습니다. 흥미롭게도 클레이슨은 SET-학습 상관관계와 출판 연도 간에 r = .48의 상관관계가 있으며, 초기 연구에서 효과가 가장 높다고 보고했습니다. 또한 그는 섹션 수와 SET 학습 상관관계 사이의 상관관계는 r = -.37이었으며, 섹션 수가 적은 연구에서 상관관계가 더 높았다는 사실을 발견했습니다. 그러나 클레이슨의 메타 분석은 SET-학습 상관관계가 r = .41이고 섹션 수가 35개인 코헨의 메타 분석을 다중 섹션 연구 중 하나로 포함했기 때문에 문제가 있습니다. Uttl 등(2017)이 언급했듯이, "메타분석에서 추정된 r을 다 중 섹션 연구의 r과 혼합하여 다중 섹션 r에 대한 또 다른 메타분석을 수행할 이유를 생각할 수 없습니다."(31페이지). A more recent meta-analysis by Clayson (2009) reported that the unweighted average correlation between SETs and learning wasr= .33, whereas the correlation weighted by sample size was onlyr= .13. Of interest, Clayson also reported a correlation ofr= .48 between the SET–learning correlation and the year of publication, with effects being highest in early studies. He also found that the correlation between number of sections and the SET–learning correlation wasr= −.37, with studies having few sections achieving higher correlations. However, Clayson’s meta-analysis is problematic, because he included Cohen’s meta-analysis as one of his multisection studies with a SET–learning correlation ofr= .41 and 35 sections. As Uttl et al. (2017) remarked, “We cannot think of any reason mixing the meta-analysis estimatedrwith multisection studies’rto conduct another meta-analysis of multi-sectionrs” (p. 31).
Uttl 등(2017)은 체계적인 문헌 검색을 통해 51개 논문에서 보고된 97개의 다중 섹션 연구를 기반으로 대규모 메타분석을 수행했습니다. 다시 말하지만, 섹션 수가 적은 연구는 종종 매우 높은 상관관계를 보고했습니다.
실제로 섹션 수와 SET 학습 상관관계의 상관계수는 r = -.35였습니다.
소규모 연구 효과를 통제했을 때 추정된 SET-학습 상관관계는 r = .12였습니다.
사전 지식/능력을 통제한 연구만 포함하면 SET-학습 상관관계는 r = -.06으로 감소했습니다.
Uttl 외(2017)는 "여러 섹션의 연구는 학생들이 높은 평가를 받은 교수로부터 더 많이 배운다는 주장을 뒷받침하지 않는다"고 결론지었습니다(35페이지). Uttl et al. (2017) conducted a larger meta-analysis based on 97 multisection studies reported in 51 articles, which they identified after a systematic literature search. Again, studies with few sections often reported extremely high correlations.
In fact, the correlation between number of sections and SET–learning correlation was r = −.35.
When they controlled for small study effects, the estimated SET–learning correlation was r = .12.
Including only studies that controlled for prior knowledge/ability reduced the SET–learning correlations to r = −.06.
Uttl et al. (2017) concluded that “multisection studies do not support the claims that students learn more from highly rated professors” (p. 35).
Web of Science 및 Scopus(검색어: "학생의 교수 평가")에서 문헌을 검색한 결과, Uttl 등(2017)이 문헌 검색을 중단한 이후에 발표된 최근의 다중 섹션 연구는 단 한 건뿐이었습니다(Boring 등, 2016; Boring, 2017에서도 논의됨). 이 연구는 유럽(즉, 프랑스) 학생의 데이터를 사용하며 379명의 강사가 가르치는 1,177개 섹션의 1학년 학생 4,423명의 23,000세트에 기반합니다. 이 데이터는 특히 흥미로운데, 섹션에 대한 자율 선택이 없었고 SET에 대한 응답이 의무적이었기 때문에 응답률이 거의 100%에 달했습니다. SET와 최종 시험 점수 간의 평균 상관관계는 r = .04였습니다. A literature search on Web of Science and Scopus (search term: “student evaluation of teaching”) revealed only one recent multisection study published after Uttl et al., (2017) stopped their literature search (Boring et al.,2016; also discussed in Boring,2017). This study uses data from European (i.e., French) students and is based on 23,000 SETs from 4,423 first-year students in 1,177 sections taught by 379 instructors. The data are particularly interesting because there was no self-selection into sections and responses to SETs were compulsory so that there was a near 100% response rate. The average correlation between SETs and final exam scores wasr=.04.
SET가 학생의 학습과 관련이 없다는 사실을 발견하는 데 40년이 걸렸다는 것이 어떻게 가능한 일인가요? 한 가지 이유는 대부분의 연구가 1981년 이전에 수행되었기 때문일 수 있습니다. Clayson(2009)이 보고한 바와 같이, SET-학습 상관관계의 크기는 출판 연도와 밀접한 상관관계가 있었습니다. Uttl 등(2019)이 이 연관성을 자세히 살펴본 결과, 1981년 이전에 발표된 69개 연구의 평균 상관계수는 .31인 반면, 1981년 이후에 발표된 28개 연구의 평균 상관계수는 .06으로 나타났습니다. How is it possible that it took 40 years to discover that SETs are unrelated to student learning? One reason could be that the majority of studies had been conducted before 1981. As Clayson (2009) reported, the size of SET–learning correlations were strongly correlated with year of publication. When Uttl et al. (2019) looked in more detail at this association, they found that the 69 studies published prior to 1981 yielded an average correlation ofr= .31, whereas the 28 studies published in or after 1981 had an average correlation ofr= .06.
이는 상당한 차이이며, 이러한 차이를 어떻게 설명할 수 있을지 궁금해집니다. Uttl 등(2019)은 이해 상충(COI)을 설명으로 제시했습니다: 초기 연구의 대부분은 SET 시스템을 판매하는 기업에서 근무하거나 소유한 연구자들이 발표했으며, 따라서 상당한 SET-학습 상관관계를 찾는 데 (재정적) 이해관계가 있었습니다. 제약 연구에서도 자금 출처가 연구 결과에 영향을 미친다는 충분한 증거가 있습니다(예: Bekelman et al., 2003; Lundh et al., 2018). Vartanian 등(2007)은 설탕 함유 청량음료가 체중에 미치는 영향에 대한 연구 결과가 자금 출처의 영향을 받았다고 보고하기도 했습니다: 설탕 함유 청량음료는 중립적인 출처가 아닌 생산자가 연구 비용을 지불했을 때 체중에 미치는 영향이 적었습니다. This is a substantial difference, and one wonders how such a difference can be explained. Uttl et al. (2019) offered conflict of interest (COI) as an explanation: Many of the early studies were published by researchers who either worked for or owned corporations that sell SET systems and thus had a (financial) interest in finding substantial SET–learning correlations. There is ample evidence from pharmaceutical research that funding sources influence research outcomes (e.g., Bekelman et al.,2003; Lundh et al.,2018). Vartanian et al. (2007) even reported that findings of the effects of sugar-containing soft drinks on body weight were influenced by the funding source: Sugar-containing soft drinks had less impact on weight when the study was paid for by the producer rather than a neutral source.
이러한 COI의 영향은 잘 알려져 있지만, COI가 교육의 질을 측정하는 척도인 SET의 효과에 대한 연구에도 영향을 미친다는 사실은 새로운 발견입니다. 그러나 이는 놀라운 일이 아닙니다. 결국, SET 시스템을 판매하는 회사에서 일하거나 소유하고 있는 연구자는 SET와 교육 효과 사이의 상관관계가 낮기보다는 높기를 선호할 것이라고 가정할 수 있습니다. 업튼 싱클레어(1934/1940)는 "어떤 사람이 무언가를 이해하지 못해야 월급을 받는 상황에서, 그 사람이 무언가를 이해하도록 하는 것은 어렵다"(109쪽)고 말한 적이 있습니다. Uttl 등(2019)이 제시한 증거는 설득력이 있습니다. 그들은 연구 저자 중 적어도 한 명 이상이 SET 기업과 연관된 경우 SET-학습 상관관계가 훨씬 더 크다는 것을 발견했습니다. 기업 COI가 있는 15개 연구의 상관관계는 r = .58인 반면, 기업 이해관계가 없는 저자의 82개 연구의 상관관계는 r = .18이었습니다(그림 1). Although these effects of COI are well known, the finding that COI also influenced research on the effectiveness of SETs as measure of teaching quality is new. However, it is not surprising. After all, it can be assumed that a researcher who either works for or owns a firm that sells SET systems would prefer to find a high rather than a low correlation between SET and teaching effectiveness. As Upton Sinclair (1934/1940) once wrote, “It is difficult to get a man to understand something, when his salary depends on his not understanding it” (p. 109). The evidence presented by Uttl et al. (2019) is persuasive. They found that SET–learning correlations were much larger when at least one author of a study was associated with an SET corporation. Whereas the correlation wasr= .58 for the 15 studies with a corporate COI, the correlation wasr= .18 for 82 studies of authors without corporate interests (Figure 1).
시스몬도(2008)는 제약 연구 결과에 대한 COI의 영향 분석에서 이러한 갈등이 의식적인 수준에서는 작동하지 않을 수 있지만, 업계로부터 자금을 받으면 연구자와 의뢰자 사이에 선물 관계가 형성되어 의뢰자가 보답해야 할 필요성을 느낄 수 있다고 제안했습니다. 심리학 연구에서는 COI로 인한 연구자의 동기가 알게 모르게 연구 결과에 영향을 미칠 수 있는 미묘한 방식이 있습니다. 연구자는 일관성이 없는 연구 결과보다 자신의 가설을 뒷받침하는 결과를 면밀히 조사할 동기가 떨어질 수 있으며, 따라서 가설을 뒷받침하는 결과를 면밀히 조사할 가능성이 낮아질 수 있습니다. 불일치를 면밀히 조사하려는 동기가 부족하다는 것을 보여주는 예로, Uttl 외(2017)이 언급한 Abrami 외(1988)의 논문을 들 수 있습니다. 이 저자들은 초기 메타분석을 비교하면서 Cohen(1981)과 McCallum(1984)이 같은 연구에서 추출한 데이터 간의 불일치를 관찰했지만 이를 추적하지는 않았습니다. Uttl 등(2017)은 추출된 데이터의 정확성을 확인하기 위해 원래 연구에서 추출한 데이터를 점검한 결과, McCallum 데이터의 상당 부분이 단순히 부정확하다는 사실을 발견했습니다. In an analysis of the effect of COI on outcome of pharmaceutical research, Sismondo (2008) suggested that such conflicts might not operate on a conscious level but that accepting funds from industry creates a gift relationship between the investigator and the sponsor, in which the sponsor might feel a need to reciprocate. In psychological research, there are subtle ways in which a researcher’s motivation due to COI can unknowingly influence study findings. Researchers may be less motivated—and therefore less likely—to scrutinize results that support their hypotheses than findings that are inconsistent. An example that suggests lack of motivation to scrutinize inconsistencies—mentioned by Uttl et al. (2017)—is in an article by Abrami et al. (1988). In comparing early meta-analyses, these authors observed disagreements between data extracted by Cohen (1981) and McCallum (1984) from the same studies but did not follow this up. When Uttl et al. (2017) checked the extracted data for accuracy in the original studies, they discovered that a large proportion of the McCallum data was simply incorrect.
교수와 무관한 요인이 학생의 교수 평가에 미치는 영향 The influence of teaching-irrelevant factors on student evaluations of teaching
SET는 성별, 인종 등 교육 효과와 무관한 수많은 변수의 영향을 받습니다. 교수자의 호감도와 같이 교수 효과와 관련이 없어 보이는 다른 변수도 효과와 관련이 있을 수 있습니다. 예를 들어, 강사가 학생에게 접근하기 쉽고 도움이 되기 때문에 호감을 가질 수 있습니다. 안타깝게도 이러한 특성에 대한 연구는 주로 코스 평점 또는 강사 평점과의 (직접적인) 관계를 입증하는 데만 집중되어 왔습니다. 이러한 요소와 강사 또는 코스의 전반적인 평가 사이의 연관성을 매개할 수 있는 이론적으로 그럴듯한 변수를 평가하려고 시도한 연구자는 거의 없었습니다. 코스 교사는 커뮤니케이터이므로 커뮤니케이터의 효율성을 높이는 것으로 알려진 변수(예: 인지된 전문성, 호감도, 권력)는 강사의 교수 효과를 높일 가능성이 높습니다. 따라서 교수 효과와 직접적인 관계가 없어 보이는 특성도 교수 효과와 관련된 프로세스를 통해 간접적인 영향을 미칠 수 있습니다. SETs are influenced by numerous variables that are unrelated to teaching effectiveness, such as gender and race. Other variables, such as likeability of an instructor—which seem to be irrelevant—could be related to effectiveness. For example, the instructor may be liked because he or she is accessible and helpful to students. Unfortunately, research on these characteristics has exclusively focused on demonstrating the (direct) relationship with course ratings or instructor ratings. Rarely have researchers tried to assess theoretically plausible variables that might mediate the association between such factors and overall ratings of instructors or courses. Because course teachers are communicators, variables known to increase the effectiveness of a communicator (e.g., perceived expertise, likeability, power) are likely to increase an instructor’s teaching effectiveness. Thus, characteristics that seem to have no direct relationship with teaching effectiveness might have indirect effects through related processes that are associated with teaching effectiveness.
SET와 강한 연관성이 있는 것으로 반복적으로 밝혀진 가장 노골적으로 관련성이 없는 특성 중 하나는 강사의 신체적 매력입니다. 교육기관 SET에서는 신체적 매력을 평가하지 않기 때문에, 매력이 교수자에 대한 학생의 평가에 영향을 미친다는 대부분의 증거는 RateMyProfessors.com(RMP) 웹사이트를 사용한 연구에서 제공되었습니다. RMP의 또 다른 장점은 기관별 SET와 달리 이 정보를 공개적으로 이용할 수 있다는 것입니다. RMP 평점과 기관별 SET의 일치 여부에 대한 의문이 종종 제기되어 왔기 때문에(예: Legg & Wilson, 2012; Murray & Zdravkovic, 2016), 몇 가지 RMP 결과를 검토하기 전에 이 문제를 먼저 논의합니다. One of the most blatantly irrelevant characteristics that has been repeatedly shown to be strongly associated with SETs is the physical attractiveness of instructors. Because institutional SETs do not assess physical attractiveness, most of the evidence that attractiveness influences students’ evaluation of teachers has been provided by studies using the RateMyProfessors.com (RMP) website. An added advantage of RMP is that, unlike institutional SETs, this information is publicly available. Because the correspondence of RMP ratings to institutional SETs has often been questioned (e.g., Legg & Wilson,2012; Murray & Zdravkovic,2016), I discuss this issue before reviewing some RMP findings.
RMP 등급과 기관 SET의 대응 관계 The correspondence of RMP ratings to institutional SETs
1999년에 설립된 RMP는 학생이 교수를 유용성, 명확성, Easiness 및 "인기도"의 네 가지 측면에서 평가할 수 있는 인기 있는 웹사이트입니다. 유용성과 명확성은 강의의 질을 나타내는 지표로 결합됩니다.1 RMP의 교수자 평가와 교육기관 SET를 비교한 대부분의 연구에서 상당한 상관관계가 발견되었으며(예: Brown et al., 2009; Colardarci & Kornfield, 2007; Sonntag et al., 2009; Timmerman, 2008), 이는 상당한 수준의 동등성이 있음을 시사합니다. 예를 들어,
캘리포니아 대학교 샌디에이고의 1,002명의 교수를 대상으로 RMP 및 SET 등급을 모두 받은 Timmerman(2008)은 강사를 추천할 학생의 비율과 전반적인 품질에 대한 RMP 등급 간의 상관관계가 r = .66임을 확인했습니다. RMP 전반적인 품질과 학생의 수업 추천 비율 간의 상관관계는 r = .51이었고, RMP와 자기 보고 학습 간의 상관관계는 r = .57이었습니다.
Sonntag 등(2009)은 랜더 대학교 교수 104명의 RMP 평점을 바탕으로 비슷한 결과를 보고했습니다. 사용된 SET 평가는 5점 척도로 교수와 수업에 대해 우수하다고 평가한 것입니다. RMP 전체 품질 평가와 교수자 우수성에 대한 SET 평가의 상관관계는 r = .69, 수업 우수성과의 상관관계는 r = .60이었습니다.
Brown 등(2009)은 312명의 Brooklyn College 강사를 대상으로 한 연구에서, Colardarci와 Kornfield(2007)는 메인 대학의 283명의 강사를 대상으로 한 연구에서 유사한 상관관계를 보고했습니다.
이러한 상관관계의 크기는 일반적으로 RMP 평가가 SET 평가에 참여한 학생보다 훨씬 적은 수의 학생을 대상으로 한다는 점을 고려하면 특히 놀랍습니다. Established in 1999, RMP is a popular website where students can evaluate their professors on four dimensions: helpfulness, clarity, easiness, and “hotness.” Helpfulness and clarity are combined into an indicator of quality of teaching.1Most studies comparing evaluations of instructors on RMP to institutional SETs have found substantial correlations (e.g., Brown et al.,2009; Colardarci & Kornfield,2007; Sonntag et al.,2009; Timmerman,2008) suggesting a fair degree of equivalence. For example,
Timmerman (2008), who identified 1,002 professors at the University of California, San Diego, with both RMP and SET ratings, found a correlation ofr=.66 between the percentage of students who would recommend an instructor and RMP ratings of overall quality. The correlation between RMP overall quality and the percentage of students’ recommending a class wasr=.51 and between RMP and self-reported learning wasr=.57. S
imilar findings were reported by Sonntag et al. (2009) based on RMP ratings of 104 Lander University professors. The SET ratings used were ratings of professors and of classes as excellent on 5-point scales. The correlation of RMP overall quality ratings with SET ratings of instructor excellence wasr=.69 and with class excellence wasr=.60.
Similar correlations were reported by Brown et al. (2009) in a study based on 312 Brooklyn College instructors and by Colardarci and Kornfield (2007) in a study based on 283 instructors at the University of Maine.
The size of these correlations is particularly surprising, if one considers that RMP ratings are typically based on much smaller numbers of students than those who participated in the SET evaluations.
레그와 윌슨(2012)이 "RateMyProfessors.com은 편향된 평가를 제공한다"라는 자극적인 제목의 논문을 발표했으므로, 그들의 연구를 간략히 검토해 볼 필요가 있습니다. 이들은 연구에 기꺼이 참여한 25명의 교수에 대한 세 세트의 RMP 평점을 수집했습니다. 첫 번째 세트는 해당 교수의 이전 수업에 대한 평가로 구성되었습니다. 두 번째 세트는 수업 중에 시행된 세트에 포함된 RMP 항목에 대한 평가로 구성되었습니다. 이 학생들은 나중에(아마도 학기 말에) RMP에서 수업을 평가하도록 요청받았습니다. 주요 결과는 수업 중 및 학기말에 평가한 명확성 평가가 이전 수업에서 수집한 명확성 평가보다 약 0.5점 정도 더 높았다는 것입니다. 또한 교수들은 연구 전에 진행된 수업에서 덜 도움이 되고 더 쉬웠다고 평가했습니다. 이러한 차이에 대한 한 가지 설명은 이러한 교수자가 연구 기간 동안 최상의 컨디션을 유지하고 있었기 때문일 수 있습니다. Since Legg and Wilson (2012) published a paper with the suggestive title “RateMyProfessors.com Offers Biased Evaluations,” a brief review of their study is warranted. They collected three sets of RMP ratings of 25 professors willing to participate in the study. The first set comprised ratings of previous classes given by those professors. The second comprised ratings of RMP items embedded in an SET administered during classes. These students were later (probably at the end of the semester) asked to rate the class on RMP. The main finding was that in-class and end-of-semester evaluations of clarity were slightly higher (by approximately 0.5 points) than clarity ratings collected on previous classes. Professors were also rated less helpful and easier in classes given before the study. One explanation for these differences could be that these instructors were on their best behavior during the study.
Murray와 즈드라브코비치(2016)의 비판적 연구도 마찬가지로 설득력이 떨어집니다. 이 저자들은 교수자의 RMP 등급을 12개 항목으로 구성된 척도로 비교했습니다. A critical study by Murray and Zdravkovic (2016) is similarly unconvincing. These authors compared RMP ratings of instructors with a 12-item scale that
교수자가 (a) 가르치는 것을 즐기는지, (b) 잘 정리되어 있는지, (c) 친절하고 학생을 배려하는지, (d) 도전적인 과제를 내주는지, (e) 추가 도움을 제공할 수 있는지, (f) 강의 자료에 열정적인지 여부와 관련된 교수자 및 코스 측면을 다루었습니다. (p. 141) addressed instructor and course aspects related to whether the professor (a) enjoys teaching, (b) is well organized, (c) is friendly and considerate of students, (d) makes challenging assignments, (e) is available to provide extra help and (f) is enthusiastic about the course material. (p. 141)
이러한 항목은 각 연구 참여자가 인지한 중요도에 따라 개별적으로 가중치를 부여했습니다. 저자들은 RMP 척도(M = 3.56)가 아닌 6항목 척도로 측정했을 때 강의에 대한 평가가 더 높았다(M = 3.80)고 보고했습니다. 저자들은 그들의 복합 지수가 RMP보다 더 유효한 교수 효과 척도라는 증거를 제시하지 않았습니다. 또한, 다소 복잡한 척도와 단순한 RMP 평가의 차이도 미미합니다. These items were individually weighed by each study participant according to perceived importance. The authors reported that the evaluation of teaching was higher (M=3.80) when measured with the six-item scale rather than the RMP scale (M=3.56). The authors present no evidence that their complex index constituted a more valid measure of teaching effectiveness than the RMP. Furthermore, the difference between their rather complex measure and the simple RMP ratings is minor.
신체적 매력 Physical attractiveness
신체적으로 매력적인("섹시한") 강사는 덜 매력적인 동료 강사보다 더 긍정적인 교수 평가를 받았습니다(예: Boehmer & Wood, 2017; Felton 외., 2008; Fisher 외., 2019; Freng & Webber, 2009; Hamermesh & Parker, 2005); Johnson & Crews, 2013; Riniolo 외., 2006; Rosen, 2018; Wolbring & Riordan, 2016). 학생 평가가 20개 이상인 미국과 캐나다의 모든 교수(369개 기관의 교수 6,851명)에 대한 데이터를 사용한 초기 RMP 연구에서 Felton 등(2008)은 "인기도"와 "품질" 간의 상관관계가 r = .64로 나타났다고 보고했습니다. Physically attractive (i.e., “hot”) instructors receive more positive teaching ratings than their less attractive colleagues (e.g., Boehmer & Wood,2017; Felton et al.,2008; Fisher et al.,2019; Freng & Webber,2009; Hamermesh & Parker,2005); Johnson & Crews,2013; Riniolo et al.,2006; Rosen,2018; Wolbring & Riordan,2016). In an early RMP study that used data for all the professors in the United States and Canada who had at least 20 student ratings (6,851 professors from 369 institutions), Felton et al. (2008) reported a correlation ofr=.64 between “hotness” and “quality.”
미국 4522개 대학의 190,006명의 교수에 대한 7,882,980개의 평가(최소 20개 평가)를 기반으로 한 Rosen(2018)의 최근 RMP 연구에서도 인기도와 자질 간의 강력한 연관성이 반복적으로 나타났습니다. 품질 평가가 2.5점 미만인 교수는 거의 없었으며, 품질 평가가 만점인 교수의 70%가 인기 있는 교수로 간주되었습니다. Riniolo 외(2006)의 연구에서도 이와 비슷한 강력한 효과가 보고되었습니다. 다른 RMP 연구에서는 이보다 약한 연관성을 발견했습니다. 예를 들어, Freng과 Webber(2009)는 r = .37의 상관관계를, Johnson과 Crews(2013)는 r = .16의 상관관계를 보고했습니다. A more recent RMP study by Rosen (2018), which was based on 7,882,980 ratings of 190,006 professors from 4522U.S. colleges and universities, who had a minimum of 20 ratings, replicated the strong association between hotness and quality. Hardly any professor with a quality rating below 2.5 was considered hot, compared to 70% of professors with a perfect quality rating. Similarly strong effects were reported by Riniolo et al. (2006). Other RMP studies found weaker associations. For example, Freng and Webber (2009) reported a correlation ofr=.37 and Johnson and Crews (2013) ofr=.16.
이러한 신체적 매력의 영향이 RMP 평가에만 국한되지 않는다는 사실은 강사의 인지된 매력(웹사이트의 사진 평가에 기반)과 학기말 SET를 연관시킨 두 가지 연구에서 입증되었습니다.
94명의 강사를 대상으로 한 연구에서 Hamermesh와 Parker(2005)는 "표본에서 가장 외모가 좋지 않은 강사와 가장 외모가 좋은 강사 간에 강의 평가가 거의 두 표준 편차만큼 차이가 났다"고 보고했습니다(372페이지).
독일에서 125명의 강사를 대상으로 실시한 연구에서 Wolbring과 Riordan(2016)은 신체적 매력과 SET의 연관성이 다소 약하다는 것을 발견했습니다.
그러나 SET 등급은 수업 결석률도 예측했습니다: 학생들은 신체적으로 매력적인 강사의 수업에 결석하는 횟수가 약간 적었습니다. 학생과 강사의 성별이 동성인지 이성인지는 아무런 차이가 없었습니다. The fact that these effects of physical attractiveness are not limited to RMP ratings has been demonstrated in two studies that related perceived attractiveness of instructors (based on ratings of photographs from websites) to their end-of-semester SETs.
Based on a study of 94 instructors, Hamermesh and Parker (2005) reported that “the instructional rating varies by nearly two standard deviations between the worst- and best-looking instructors in the sample” (p. 372).
In a study conducted in Germany with 125 instructors, Wolbring and Riordan (2016) found a somewhat weaker association of physical attractiveness with SETs.
However, SET ratings also predicted absenteeism from class: Students missed slightly fewer classes of physically attractive instructors. It made no difference whether students and instructors were of the same or opposite sex.
Wolbring과 Riordan(2016)은 학생들이 매력적인 남성 또는 다소 덜 매력적인 남성 또는 여성의 사진(이력서에 첨부)에 노출되는 실험 연구를 통해 신체적 매력과 교수 평가의 연관성을 재현했습니다. 그런 다음 학생들은 이 자극을 준 사람이 하는 것으로 가정한 강의를 듣고 평가해야 했습니다. 다시 말하지만, 신체적 매력은 강의의 질에 대한 평가에 영향을 미쳤습니다. 마지막으로 Ambady와 Rosenthal(1993)은 두 명의 여대생이 13명의 대학 교수의 신체적 매력에 대해 평가(30초 무성 영화 클립 기준)한 결과, 해당 강사가 가르친 강의의 질에 대한 학생들의 학기말 평가와 상관계수가 r = .32로 나타났다고 보고했습니다. Wolbring and Riordan (2016) replicated their association of physical attractiveness and teaching evaluation in an experimental study in which students were exposed to pictures (attached to a CV) of either an attractive or a somewhat less attractive man or woman. Students then had to listen to—and evaluate—a lecture supposedly given by this stimulus person. Again, physical attractiveness influenced ratings of the quality of that lecture. Finally, Ambady and Rosenthal (1993) reported that ratings (based on a 30-s silent film clip) of the physical attractiveness of 13 college teachers by two female undergraduates correlatedr=.32 with students’ end-of-term ratings of the quality of courses taught by these instructors.
강사에 대한 호감도 Likeability of instructor
신체적 매력이 강사의 인지된 효과를 높일 수 있는 한 가지 방법은 호감도와의 연관성을 통해서입니다. 호감도는 더 넓은 개념이지만, 신체적 매력은 호감도를 결정하는 주요 요인입니다. 미국 대학의 학생 861명을 대상으로 현재 수강 중인 수업의 두 강사의 신체적 매력을 평가하도록 한 연구에 따르면 호감도와 r = .47의 상관관계가 있는 것으로 나타났습니다(Gurung & Vespia, 2007). 강사에 대한 호감도와 수업의 즐거움 사이의 상관관계는 r = .80이었습니다. 출석과의 상관관계도 양의 상관관계(r = .30)를 보였는데, 이는 학생이 강사를 좋아하면 수업에 더 자주 출석한다는 것을 의미합니다. One way that physical attractiveness might increase the perceived effectiveness of an instructor is through its association with likeability. Although likeability is a broader concept, physical attractiveness is a major determinant of likeability. A study that asked 861 students from a U.S. university to rate the physical attractiveness of two instructors of classes they were currently taking reported a correlation ofr=.47 with liking (Gurung & Vespia,2007). The correlation between liking their instructor and enjoyment of the class wasr=.80. The correlation with attendance was also positive (r=.30), suggesting that students will attend a class more regularly if they like an instructor.
Feistauer와 Richter(2018)는 독일 대학에서 심리학 강의 또는 세미나를 가르친 26명의 강사를 평가한 260명의 학생 표본을 바탕으로 비슷한 결과를 보고했습니다. Feistauer와 Richter는 학생들이 수강한 심리학 세미나 또는 강의의 강사에 대한 평가와 호감도의 연관성을 연구했습니다. 호감도는 첫 번째 세션의 첫 10분 동안과 학기가 끝나기 전에 단일 항목 측정으로 두 번 평가했습니다. 강사의 전반적인 성과는 학기 말에 단일 항목 척도로 평가했습니다. 두 가지 호감도 평가는 중간 정도의 상관관계(.55-.58)를 보였습니다. 학기 초에 측정된 '좋아요'는 강의에 대한 강사 전체 평점의 총 분산 중 9.4%를 차지했으며, 세미나에 대한 평점의 총 분산 중 20.5%를 차지했습니다. 학기 말(즉, 평가 시점)의 호감도는 강의의 경우 36.5%, 세미나의 경우 54.7%의 분산을 차지했습니다. Similar findings were reported by Feistauer and Richter (2018) based on a sample of 260 students rating 26 instructors who taught psychology lectures or seminars at a German university. Feistauer and Richter studied the association of likeability with the evaluation of instructors, whose seminars or lectures on psychology the students had attended. Likeability was rated twice with a single-item measure administered during the first 10min of the first session and before the end of the semester. The overall performance of instructors was assessed with a single-item scale toward the end of the semester. The two liking ratings were moderately correlated (.55–.58). Liking measured at the beginning of the semester accounted for 9.4% of the total variance in overall ratings of the instructor for lectures and 20.5% of the variance for seminars. Liking at the end of the semester (i.e., at the time of the evaluation) accounted for 36.5% of the variance for lectures and 54.7% for seminars.
Delucchi(2000)의 연구는 호감도에 영향을 미치는 강사의 특성에 대해 몇 가지 시사점을 제공합니다. Delucchi는 SET 평가에 대한 요인 분석을 기반으로 다음과 같은 평가로 구성된 호감도 지수를 확인했습니다. 호감 가는 강사는 학생들과 좋은 관계를 맺고, 대화하기 쉬우며, 주제에 대해 열정적으로 보이고, 학생들 사이에 공동체 의식을 형성하는 것으로 나타났습니다. 이러한 결과는 단일 항목 측정의 타당성을 입증하기 위해 시간 1에서 Reysen(2005) 호감도 척도를 시행한 Feistauer와 Richter(2018)가 보고한 결과와 일치합니다. 레이센 척도는 학생이 강사를 친근하고, 호감이 가고, 마음이 따뜻하고, 접근하기 쉽고, 지식이 풍부하고, 신체적으로 매력적이며, 자신과 비슷하다고 인식하는지를 평가했습니다. 레이센 척도는 강의에서 r = .98, 세미나에서 r = .89의 상관관계를 보였으며, 같은 시기에 주어진 단일 항목 측정과 학기 말에 주어진 단일 항목 측정의 상관관계는 r = .46, r = .45였습니다. 첫 수업 모임의 첫 10분 동안 평가된 호감도는 주로 외모에 기반할 가능성이 높기 때문에, 이러한 (초기) 높은 상관관계는 레이센 척도가 사람들이 신체적으로 매력적인 타인에 대해 가지고 있는 고정관념을 완벽하게 포착하고 있음을 시사합니다. 초기 호감도 평가가 학기 말 호감도와 중간 정도의 상관관계만 있고, 학기 말 강사에 대한 전체 평가에서 초기 호감도가 후기 호감도보다 훨씬 적은 변수를 차지한다는 결과는 개인이 개별적인 정보를 받을 때 그 효과가 약해진다는 매력 고정관념에 대한 고전적인 메타 분석의 결론과 일치합니다(Eagly et al., 1991). 한 학기가 진행되는 동안 학생들은 강사가 첫인상을 바탕으로 기대했던 것만큼 따뜻하고 친근하며 지식이 풍부하지 않다는 사실을 발견했을 수 있습니다. A study by Delucchi (2000) provides some indications about the characteristics of instructors that influence likability. Based on a factor analysis of SET ratings, Delucchi identified a likeability index that consisted of some of the following evaluations. A likeable instructor had good rapport with students, was easy to talk to, seemed enthusiastic about the subject matter, and created a feeling of community among students. These findings are consistent with findings reported by Feistauer and Richter (2018), who had also administered the Reysen (2005) Likability Scale at Time 1 to establish the validity of their single-item measure. The Reysen scale assessed whether the instructor is perceived by students as friendly, likeable, warmhearted, approachable, knowledgeable, physically attractive, and similar to them. The Reysen scale correlatedr=.98 in lectures andr=.89 in seminars with the single-item measure given at the same time andr=.46 andr=.45 with the single-item measure given at the end of the semester. Because likability assessed during the first 10 min of the first class meeting is likely to be mainly based on physical appearance, these (initially) high correlations suggest that the Reysen scale perfectly captures the stereotype people hold of physically attractive others. The finding that initial ratings of liking were only moderately correlated with liking at the end of the semester and that initial liking accounted for much less variance than later liking in the end-of-semester overall rating of instructors is consistent with the conclusions of the classic meta-analysis of the attractiveness stereotype that the effect is weakened when individuals receive individuating information (Eagly et al.,1991). In the course of the semesters, students might have discovered that their instructors were not quite as warmhearted, approachable, and knowledgeable as they had expected them to be based on their first impression.
호감도는 접근성, 친근함, 지식과 같이 좋은 강의의 일부인 특성의 결과인 것으로 보입니다.신체적 매력이 이러한 특성과 상관관계가 있다는 발견은 후광 효과의 가능성을 시사합니다: 학생들은 신체적으로 매력적인 강사가 이러한 특성도 가지고 있다고 가정합니다. 이러한 해석은 신체적 매력이 수업 출석과 관련이 있는 이유 또는 RMP 연구에서 '섹시함'이 항상 인지된 도움과 높은 상관관계가 있는 이유를 설명할 수 있습니다. 마지막으로 Feistauer와 Richter(2018)의 연구에서 학생들이 10분간 친분을 쌓은 후 강사가 따뜻하고 친근하며 지식이 풍부하고 자신과 비슷하다고 판단한 이유를 설명할 수 있습니다. Likeability appears to be the result of characteristics that are certainly part of good teaching, such as approachability, friendliness, and knowledgeableness. The finding that physical attractiveness is correlated with these characteristics suggests the possibility of a halo effect: Students assume that a physically attractive instructor also possesses these traits. This interpretation would explain why physical attractiveness is related to class attendance, or why “hotness” in RMP studies is always highly correlated with perceived helpfulness. It would finally explain why, in the study of Feistauer and Richter (2018), students decided after being acquainted for 10min that their instructor was warmhearted, approachable, knowledgeable, and similar to them.
사전 과목 관심도 Prior subject interest
학생들은 관심이 적은 과목보다 관심이 있는 과목의 강의를 더 긍정적으로 평가할 것이라고 예상할 수 있습니다. 놀랍게도 증거는 엇갈립니다. Olivares(2001)는 첫 수업 모임이 시작될 때 측정한 사전 관심도는 코스에 대한 전반적인 평가와 관련이 없다는 사실을 발견했습니다. 이와는 대조적으로 Griffin(2004)은 초기 관심도와 교사 평가 간에 중간 정도의 상관관계(r = .37)가 있으며 코스 평가와는 훨씬 더 높은 상관관계(r = .50)가 있다고 보고했습니다. Feistauer와 Richter(2018)도 약하지만 통계적으로 신뢰할 수 있는 연관성을 보고했습니다. One would expect that students rate courses on topics in which they are interested more positively than courses of little interest. Surprisingly the evidence is mixed. Olivares (2001) found prior interest—measured at the beginning of the first class meeting—unrelated to global rating the course. In contrast, Griffin (2004) reported a moderate correlation between initial interest and teacher ratings (r=.37) and an even higher correlation with ratings of a course (r=.50). Feistauer and Richter (2018) also reported a weak but statistically reliable association.
학생은 종종 코스 콘텐츠와 자료가 자신에게 얼마나 흥미로울지에 대해 잘못된 기대를 갖게 됩니다. 특히 심리학 과목에서 이러한 현상이 두드러지게 나타나는데, 심리학을 처음 배우는 학생들은 학습 내용에 대해 비현실적인 기대를 하는 경우가 많습니다. 많은 사람들이 사람들을 아는 방법과 그들을 돕는 방법을 배울 것이라고 기대하지만, 이론과 통계 학습에 노출되는 것을 발견합니다. 따라서 강사 평가와 관련된 초기 관심도를 찾지 못한 Olivares(2001)가 학기 말에 평가한 관심도 변화가 강사에 대한 학생 평가와 중간 정도의 상관관계가 있다는 것을 발견한 것은 흥미롭습니다(r = .42). 초기 관심도와 관심도 변화 간의 상관관계가 r = .21에 불과한 것으로 보아 이 수업에서는 상당한 변화가 있었을 것입니다. 강의 내용에 대한 관심이 강의의 즐거움에 영향을 미치고, 따라서 강사에 대한 평가에도 영향을 미친다는 것은 그럴듯해 보입니다. 코스에 전혀 관심이 없는 학생은 강사에 대해 매우 긍정적인 평가를 내릴 가능성이 낮습니다. 가르치는 과목에 대한 학생의 흥미를 불러일으키는 것은 분명 교수 능력의 특징입니다. 불행히도 통계학보다는 사회 심리학을 가르치는 것이 더 쉽습니다. Students will often have false expectations about the content of a course and how interesting the material will be to them. This is particularly likely in psychology courses, in which beginning students often have unrealistic expectations of what they will learn. Although many expect that they will learn how to know people and how to help them, they find themselves exposed to learning theories and statistics. It is therefore interesting that Olivares (2001), who failed to find initial interest related to instructor ratings, found that interest change assessed at the end of the semester moderately correlated with student ratings of their instructors (r=.42). There must have been quite a bit of change happening in these classes, as the correlation between initial interest and interest change was onlyr=.21. It seems plausible that interest in the content of a course influences enjoyment of the course and therefore also ratings of the instructor. Students who are totally uninterested in a course are unlikely to give an instructor very positive ratings. Arousing students’ interest in the subject that one is teaching is certainly a characteristic of teaching ability. Unfortunately, it is easier if one teaches social psychology rather than statistics.
소수자 지위 Minority status
소수 집단에 속하는 교사가 일반적으로 다수 집단에 속하는 교사보다 능력이 떨어진다는 것은 믿을 수 없으므로, 소수 집단에 속하는 교사의 지위는 SET에 영향을 미치지 않아야 합니다. 그럼에도 불구하고 대부분의 연구에 따르면 비백인 강사는 백인 동료 강사보다 낮은 SET 등급을 받습니다(예: McPherson & Jewell, 2007; Reid, 2010; Smith, 2007). 22명의 강사가 가르친 280개의 대학원 수업으로 구성된 24개 학기 연속 데이터를 기반으로 한 연구에서 백인 강사는 비백인 동료보다 더 높은 SET 점수를 받았습니다(McPherson & Jewell, 2007). 미국 남부에 위치한 한 교육대학의 소수 교수진 표본을 대상으로 한 Smith(2007)의 연구에서도 비슷한 결과가 보고되었습니다. 역시 흑인 교수진은 백인 교수진보다 교수 효과성에 대해 낮은 평가를 받았으며, 다른 소수계 교수진(라틴계, 아시아계, 아메리카 원주민)의 평가는 그 사이에 머물렀습니다. Hamermesh와 Parker(2005)도 소수 교수진과 영어가 모국어가 아닌 교수진이 다수 교수진과 영어가 모국어인 교수진보다 훨씬 낮은 강의 평가를 받았다고 보고했습니다. Because it is implausible that teachers belonging to a minority are generally less able instructors than majority teachers, minority status should have no impact on SETs. And yet, most studies show that non-White instructors receive SET ratings that are lower than that of their White colleagues (e.g., McPherson & Jewell,2007; Reid,2010; Smith,2007). In a study based on data from 24 consecutive semesters, comprising 280 graduate classes taught by 22 instructors, White instructors received higher SET scores than their non-White colleagues (McPherson & Jewell,2007). Similar results were reported by Smith (2007) based on a much larger sample of minority faculty members from a college of education situated in the southern United States. Again, Black faculty members received lower evaluations of teaching effectiveness than their White colleagues, with ratings of other minority faculty (Latinos, Asians, Native Americans) falling in between. Hamermesh and Parker (2005) also reported that minority faculty members and non-native English speakers received substantially lower teaching ratings than majority faculty members and native English speakers.
5,630개 인문대학 교수진에 대한 평가를 기반으로 한 RMP 연구에서도 비슷한 패턴이 나타났습니다(Reid, 2010). RMP에는 교수진의 인종이 기재되어 있지 않기 때문에 Reid는 다인종 학생 그룹에게 교수진의 사진을 보고 인종을 결정하도록 했습니다. 소수 인종 교수진은 백인 교수진에 비해 강의의 질, 유용성, 명확성에서 덜 호의적인 평가를 받았습니다. 그러나 Easiness에서는 더 긍정적인 평가를 받았습니다. 이러한 차이는 주로 흑인 교수진의 품질 평가가 낮았기 때문이었습니다. 소수자 신분인 교사가 낮은 평점을 받은 가장 큰 요인은 편견입니다. 편견을 가진 사람들은 소수자 교직원을 덜 똑똑하고 전문성이 떨어진다고 인식하는 경향이 있습니다. A similar pattern emerged from an RMP study based on ratings of 5,630 faculties of liberal arts colleges (Reid,2010). Because RMP does not list race of instructors, Reid had a multiracial group of students decide on race based on photographs of these faculty members. Racial minority faculty members were rated less favorably than White faculty members on quality, helpfulness, and clarity. However, they received more positive ratings on easiness. These differences were mainly due to lower quality ratings received by Black faculty members. The most likely determinant of the lower ratings received by minority status teachers is prejudice. Prejudiced individuals would tend to perceive minority faculty members as less intelligent and possessing less expertise.
성별 Gender
성별 차이에 대한 증거는 일관성이 떨어집니다. 그러나 성별 차이가 발견되는 경우 대부분 여성 강사가 강의 품질에 대해 더 낮은 평가를 받았습니다. Rosen(2018)의 RMP 연구에 따르면 여성은 강의의 질에서 약간 낮은 점수를 받았습니다. 이러한 성별 차이는 Boehmer와 Wood(2017)의 RMP 연구와 Arceo-Gomez와 Campos-Vazquez(2019)의 멕시코 인터넷 사이트(MisProfesores.com)를 기반으로 한 연구에서도 보고되었지만 Reid(2010)와 Stuber 외(2009)의 RMP 연구에서는 나타나지 않았습니다. Evidence for gender differences is less consistent. However, if gender differences are found, it is mostly female instructors, who receive lower ratings on teaching quality. The RMP study of Rosen (2018) found that women received slightly lower scores on quality. Such gender differences were also reported in an RMP study of Boehmer and Wood (2017) and by Arceo-Gomez and Campos-Vazquez (2019) in a study based on a Mexican internet site (MisProfesores.com) but not in RMP studies of Reid (2010) and Stuber et al. (2009).
기관 SET를 기반으로 한 세 개의 대규모 다집단 연구에서도 남성에 유리한 성별 차이가 보고되었습니다(Boring, 2017; Hamermesh & Parker, 2005; Mengel et al., 2019). 앞서 설명한 Boring 등(2016)의 데이터 세트를 사용하여 Boring(2017)은 남학생과 여학생 모두 전반적인 만족도에서 남교수에게 약간 더 높은 점수를 주었으며, 여학생의 경우 그 차이가 다소 덜 두드러진다는 것을 발견했습니다. 그러나 이러한 차이는 미미했습니다. 이와는 대조적으로 Hamermesh와 Parker(2005)는 여성 강사가 남성 동료보다 거의 절반 표준편차 낮은 평가를 받았다고 보고했습니다. 마지막으로 네덜란드 마스트리흐트 대학교 경영경제학부에서 실시한 약 20,000명의 학생 평가를 기반으로 한 연구에서 Mengel 등(2019)은 성적이나 학생의 학습 시간이 강사의 성별에 영향을 받지 않았음에도 불구하고 여성이 남성 동료보다 체계적으로 낮은 평가를 받는다는 사실을 발견했습니다. 이러한 성별 차이는 특히 수학적 내용이 포함된 강의에서 두드러졌습니다. Three large multisection studies based on institutional SETs also reported gender differences favoring men (Boring,2017; Hamermesh & Parker,2005; Mengel et al.,2019). Using the dataset of Boring et al. (2016) described earlier, Boring (2017) found that both male and female students gave male professors slightly higher ratings on overall satisfaction, with the difference somewhat less marked for female students. However, these differences were minimal. In contrast, Hamermesh and Parker (2005) reported that female instructors received ratings that were nearly half a standard deviation lower than those of their male colleagues. Finally, in a study based on nearly 20,000 student evaluations conducted at the School of Business and Economics of Maastricht University (Netherlands), Mengel et al. (2019) found that women received systematically lower ratings than their male colleagues, even though neither grades nor students’ study hours were affected by the gender of their instructor. These gender differences were particularly marked for courses with mathematical content.
이 마지막 결과는 학문 분야(예: 과학 대 인문학)에 따라 성별 차이가 조정될 수 있다는 가능성을 제기합니다. 그러나 증거는 일관성이 없습니다. 피셔 외(2019)의 RMP 연구에 따르면 영어, 역사, 철학보다 공학, 경영/경제학, 컴퓨터 과학과 같은 분야에서 성차별이 더 많이 발견되었으며, 이러한 부서의 여성 직원 비율을 통제한 경우에도 마찬가지였습니다. 그러나 Stuber 등(2009)은 이러한 차이를 발견하지 못했습니다. 이 연구자들은 하드 과학, 공학, 수학, 경영을 전통적으로 남성의 영역으로, 예술과 인문학은 전통적으로 여성의 영역으로 정의했습니다. 이들은 전통적으로 남성 분야 교수자가 인문이나 예술을 가르치는 교수자보다 더 부정적인 평가를 받는다는 일반적인 결과를 반복했지만, 성별에 따른 상호작용은 발견되지 않았습니다: 여성이 남성보다 더 많은 불이익을 받지 않았습니다. This last finding raises the possibility that gender differences could be moderated by discipline (e.g., science vs. humanities). However, the evidence is inconsistent. An RMP study by Fisher et al. (2019) found more gender discrimination in fields such as engineering, business/economics, and computer science than in English, history, and philosophy—even when they controlled for percentage of female staff in these departments. However, Stuber et al. (2009) did not find such differences. These authors defined the hard sciences, engineering, mathematics, and business as traditionally male areas and arts and humanities as traditionally female. Although they replicated the typical finding that instructors teaching in those traditionally male fields were rated more negatively than those teaching humanities or arts, there was no interaction with gender: Women were not more penalized than men.
여성 강사가 일반적으로 더 낮은 평가를 받는 것은 교수 능력이 낮기 때문일까요?많은 인용을 받은 MacNell 등(2015)의 연구는 이러한 해석을 배제하는 것으로 보입니다. 이 연구자들은 강사의 인지된 성별을 조작하는 실험을 실시했습니다. 온라인 수업에 두 명의 보조 강사(남성 1명, 여성 1명)가 각각 다른 두 가지 성 정체성으로 활동했습니다. 실제 성별에 관계없이 남성 정체성을 가진 강사가 전문성, 신속성, 공정성, 존중, 칭찬, 열정에서 더 높은 평가를 받았습니다. 그러나 Uttl과 Violo(2020)는 여러 가지 측면에서 이러한 결과에 의문을 제기했습니다: 그들은 두 사람만을 대상으로 한 조사 결과를 모든 남성 또는 여성 강사에게 일반화하기 어렵다고 주장했습니다. 또한 각 조건의 학생 표본이 8명에서 12명으로 다소 적었습니다. 그러나 가장 중요한 것은 세 가지 이상값이 있었는데, 두 명의 여성 조건에서 모든 세트 항목에서 가장 낮은 평점을 받았다는 점입니다. 이러한 이상값을 제거하면 성별 차이가 사라졌습니다. 대신 학생들은 인지된 성별에 관계없이 실제 여성 강사를 남성 강사보다 더 높게 평가했습니다. Could the lower ratings typically received by female instructors reflect lower teaching ability? A highly-cited study by MacNell et al. (2015) appeared to rule out this interpretation. These authors conducted an experiment in which they manipulated theperceivedgender of instructors. Two assistant instructors (one male and one female) in an online class each operated under two different gender identities. Regardless of actual gender, male-identity teachers received higher evaluation on professionalism, promptness, fairness, respectfulness, giving praise, and enthusiasm. However, Uttl and Violo (2020) questioned these findings on several accounts: They argued that one could hardly generalize to all male or female instructors based on findings with only two individuals. Furthermore, the sample of students in each condition was rather small, ranging from eight to 12 individuals. But most critically, there were three outliers; they gave the lowest ratings on all SET items in the two female conditions. If one removed these outliers, the gender difference disappeared. Instead, students rated the actual female instructor higher than the male instructor, regardless of perceived gender.
성별에 따른 또 다른 연구는 Mitchell과 Martin(2018)에 의해 수행되었습니다. 서로 다른 대학의 교수진인 크리스티나 미첼 박사와 조나단 마틴 박사가 각자의 대학에서 동일한 내용의 온라인 강의를 진행했습니다.2 이 강의는 여성 강사가 아닌 남성 강사가 맡았을 때 더 긍정적인 평가를 받았습니다. 각기 다른 학생 집단에게 강의가 제공되었기 때문에 강사의 성별이 강의에 대한 학생 집단의 평가와 혼동을 일으켰습니다. 또한 미첼 박사와 마틴 박사는 학생들에게 잘 알려져 있었을 가능성이 높았기 때문에 단순한 성별 정보보다는 강사에 대한 기존의 태도가 이러한 평가에 영향을 미쳤을 가능성이 있습니다. 이 가설을 배제할 수 없다고 해서 이 가설이 타당하다는 의미는 아니라는 점을 서둘러 덧붙이고 싶습니다.
Another study that varied gender was conducted by Mitchell and Martin (2018). Dr. Kristina Mitchell or Dr. Jonathan Martin, who are faculty members at different colleges, gave an online course of identical content at their respective colleges.2The course was rated more positively when attributed to a male instructor rather than a female instructor. Because the courses were given to different student populations, gender of instructor was confounded with the student population rating the courses. Furthermore, because Drs. Mitchell and Martin were likely to be known to their students, it seems possible that preexisting attitudes toward these instructors rather than mere gender information could have influenced these ratings. I hasten to add that the fact that we cannot rule out this hypothesis does not mean that it is plausible.
훈련 Discipline
신체적 매력, 인종, 성별에 대해서는 선택의 여지가 없는 반면, 전공 분야는 일반적으로 선택할 수 있습니다.가르치는 것에 대해 긍정적인 평가를 받고 싶다면 수학, 공학 또는 컴퓨터 과학보다는 인문학이나 언어를 선택해야 한다는 충분한 증거가 있습니다. Centra(2009)는 238,471개 학급의 교육 시험 서비스 데이터를 사용하여 인문학(영어, 역사, 언어) 학급에 비해 자연과학(수학, 공학, 컴퓨터 과학) 학급이 0.30 표준편차 더 낮은 평가를 받았다는 사실을 발견했습니다. 이와 일관되게 Felton 등(2008)은 RMP 연구에서 가장 높은 평가를 받은 학과는 언어학, 사회학, 정치학이었고 공학, 컴퓨터 과학, 화학이 가장 낮은 평가를 받은 학과였다고 보고했습니다. 뉴욕대학교의 영어 및 수학 수업의 SET를 비교한 Uttl과 Smibert(2017)의 연구에서도 비슷한 차이가 발견되었습니다. 영어 수업의 평균 SET는 4.29, 수학 수업의 평균은 3.68이었습니다. SET가 인사 결정에 사용된다는 사실과 일관되게, Uttl과 Smibert(2017)는 정량적 과목을 가르치는 교수가 영어과 동료 교수보다 종신 재직, 승진 또는 성과급을 받을 가능성이 낮다는 사실을 발견했습니다. Whereas people have no choice regarding their physical attractiveness, race, or gender, they typically can choose their discipline. There is ample evidence that if they want to receive positive ratings for their teaching, they should choose humanities or languages rather than mathematics, engineering, or computer science. Using Educational Testing Service data from 238,471 classes, Centra (2009) found that compared with classes in humanities (English, history, languages), natural science classes (mathematics, engineering, and computer science) were rated 0.30 standard deviations lower. Consistent with this, Felton et al. (2008) reported from their RMP study that the departments with the highest quality ratings were languages, sociology, and political science, with engineering, computer science, and chemistry as the lowest ranking departments. A similar difference was found by Uttl and Smibert (2017) in a comparison of SETs of English and Math classes at New York University. The average SET of English classes was 4.29; the math average was 3.68. Consistent with the fact that SETs are used for personnel decisions, Uttl and Smibert (2017) found that professors teaching quantitative courses were also less likely than their colleagues in English departments to be tenured, promoted, or given merit pay.
결론 Conclusion
강의에 대한 학생 평가는 강의 효과를 측정하지 않습니다. 또한 강사의 소수자 여부, 외국 억양 및 성별, 가르치는 분야 등 강의의 질과 무관한 여러 요인에 의해 영향을 받습니다. 따라서 대학 관리자가 채용, 급여 인상 및 승진에 관한 결정에 이러한 요소를 사용하는 것은 불공정하고 잠재적으로 불법일 수 있습니다. 실제로 최근 캐나다 라이어슨 대학교와 교수 협회 간의 갈등에 관한 중재 결정(Ryerson University v Ryerson 교수 협회, 2018, CanLII 58446)에서 한 중재인은 "교육 효과성 평가에 관한 한, 특히 임기 및 승진에 관한 한-SET는 기껏해야 불완전하고 최악의 경우 완전히 편향되어 신뢰할 수 없다"고 주장했습니다. 그는 대학이 더 이상 승진 및 임기 결정에서 교수 효과성의 척도로 SET를 사용해서는 안 된다고 선언했습니다. Student evaluations of teaching do not measure teaching effectiveness. Furthermore, they are influenced by several factors unrelated to teaching quality such as minority status, foreign accent and gender of instructors, and the discipline they are teaching. This makes their use by university administrators in decisions about hiring, salary increases, and promotions unfair and potentially illegal. In fact, in a recent arbitration decision regarding a conflict between the Canadian Ryerson University and its faculty association (Ryerson University v Ryerson Faculty Association,2018, CanLII 58446), an arbitrator argued that “insofar as assessing teaching effectiveness is concerned – especially in the context of tenure and promotion—SETs are imperfect at best and downright biased and unreliable at worst.” He decreed that the university should no longer use SETs as a measure of teaching effectiveness in promotion and tenure decisions.
교수에 대한 학생 평가의 편향 효과: 프로세스 모델 The biasing effects of student evaluations of teaching: a process model
이 섹션에서는 채용, 급여 인상, 승진 결정에 SET를 오용하는 것이 부실 교육과 성적 인플레이션의 원인이 될 수 있다고 주장합니다. 대학 관리자는 좋은 SET를 매우 중요하게 생각하기 때문에 교수자에게는 좋은 SET를 얻는 것이 매우 중요합니다. 이는 학생에게 자신이 받는 강의 유형에 영향을 미칠 수 있는 효과적인 도구를 제공합니다. SET가 교육 효과의 유효한 지표이고 학생들이 학습에 대한 필요성에 의해서만 동기를 부여받는다면 이는 문제가 되지 않을 것입니다. 그러나 SET는 교수 효과와 관련이 없고, 앞서 살펴본 바와 같이 상당수의 학생이 열심히 공부하고 많은 것을 배우려는 동기가 없는 것으로 보이며(예: Chiu 외, 2019; Felton 외, 2008; Rosen, 2018), 쉬운 코스와 관대한 채점을 선호하기 때문에 이러한 피드백을 수용하면 교육의 질이 떨어질 가능성이 높습니다. 이 과정을 설명하기 위해 대다수 학생의 동기에 대한 경험적으로 뒷받침되는 가정을 기반으로 한 모델을 제시합니다. 모델을 제시한 후에는 모델에서 가정하는 각 과정을 뒷받침하는 증거를 검토합니다. In this section, I argue that this misuse of SETs in decision about hiring, salary increases, and promotions could be the cause of bad teaching and grade inflation. University administrators place great emphasis on good SETs, which makes getting good SETs highly important for instructors. This provides students with an effective tool to influence the type of teaching they receive. This would be no problem if SETs were a valid indicator of teaching effectiveness and if students were motivated only by a need to learn. However, because SETs are unrelated to teaching effectiveness and because—as I show—a sizeable proportion of students does not seem motivated to work hard and to learn a great deal (e.g., Chiu et al.,2019; Felton et al.,2008; Rosen,2018) and prefers easy courses and lenient grading, their feedback—if accepted—is likely to reduce the quality of teaching. To describe this process, a model is presented that is based on empirically supported assumptions about the motivation of a majority of students. After presenting the model, I review evidence that supports each of the processes assumed by the model.
이 분석은 모든 학생이 좋은 코스 성적을 받는 것을 좋아한다는 가정에서 시작합니다. 또한 이러한 학생들 중 다수는 읽기, 쓰기 및 기타 수업 준비에 너무 많은 시간을 소비하지 않기를 원합니다(그림 2, Chiu 외., 2019, Felton 외., 2008, Rosen, 2018). 일반적으로 상충되는 이러한 목표를 달성하는 한 가지 방법은 채점을 관대하게 하고 과제를 너무 많이 요구하지 않는 것으로 알려진 교사와 함께 수업을 듣는 것입니다(Johnson, 2003; Sabot & Wakeman-Linn, 1991). 그 결과, 많은 학생들이 노력이 필요하고 좋은 성적이 확실하지 않은 도전적인 과목보다 좋은 성적이 보장되는 쉬운 수업을 선호합니다(예: Bar et al., 2009; Johnson, 2003; Sabot & Wakeman-Linn, 1991). 따라서 학생은 관대하게 채점하고(예: Anderson et al., 1975; Greenwald & Gillmore, 1997a; Griffin, 2004; Olivares, 2001) 너무 많은 노력을 요구하지 않는 교사에게 좋은 SET의 보상을 제공합니다(예: Felton et al., 2008; Rosen, 2018).
This analysis starts with the assumption that all students like getting good course grades. Many of these students would also prefer not to spend too much time on reading, writing, and other class preparation (Figure 2; Chiu et al.,2019; Felton et al.,2008; Rosen,2018). One way to achieve these normally conflicting goals is to take classes with teachers who are known to grade leniently and not require too much coursework (Johnson,2003; Sabot & Wakeman-Linn,1991). As a result, many students prefer easy classes that promise good grades to challenging courses, where hard work is required and good grades are not a certainty (e.g., Bar et al.,2009; Johnson,2003; Sabot & Wakeman-Linn,1991). The students therefore give the reward of good SETs to teachers who grade leniently (e.g., Anderson et al.,1975; Greenwald & Gillmore,1997a; Griffin,2004; Olivares,2001) and do not require too much work (e.g., Felton et al.,2008; Rosen,2018).
교사는 자신의 코스에서 좋은 점수를 받기를 원할 뿐만 아니라 좋은 점수가 승진 및 성과급 상승에 중요하다는 것을 알고 있기 때문에 쉬운 코스를 제공하고 관대하게 채점하려는 인센티브가 생깁니다(Birnbaum, 2000; Keng, 2018; Moore & Trahan, 1998; Ryan et al., 1980; Simpson & Siguaw, 2000). 인센티브가 강할수록 부서에서 사용하는 비교 수준이 더 엄격해집니다(예: 강사는 부서 평균 이상의 점수를 받아야 하는가, 아니면 70번째 백분위수 이상의 점수를 받아야 하는가?). 비교 그룹은 학과입니까, 교수진입니까, 아니면 대학 전체입니까?). 이 과정의 가장 근거리적인 결과는 SET가 종종 부실한 강의와 관대한 채점에 대해 보상한다는 것입니다. 이러한 하위권 경쟁의 보다 원초적인 효과는 성적 인플레이션입니다. Teachers not only like their courses to receive good SETs but also know that good SETs are important for promotion and merit increases, which creates an incentive to offer easy courses and to grade leniently (Birnbaum,2000; Keng,2018; Moore & Trahan,1998; Ryan et al.,1980; Simpson & Siguaw,2000). The stronger the incentive, the stricter the comparison levels used in a department (e.g., Are instructors required to score above the mean of the department, or even above the 70th percentile? Is the comparison group the department, the faculty, or the whole university?). The most proximal result of this process is that SETs often reward poor teaching and lenient grading. The more distal effect of this race to the bottom is grade inflation.
이 모델은 미국 대학교육의 가장 큰 역설, 즉 GPA는 수십 년 동안 증가했지만(Rojstaczer, 2015) 대학생들이 더 열심히 일하거나 대학에 더 적합한 자격을 갖추지 못했다는 사실에 대한 설명을 제공합니다.3 반대로 SAT 점수는 하락 추세를 보이고 있으며(예: Adams, 2015; Washington Post, 2015) 오늘날 학생들은 수십 년 전보다 학업에 더 적은 시간을 소비하고 있습니다(예: Arum & Roksa, 2011; Babcock & Marks, 2011). 심지어 대학 교육이 수십 년 전보다 오늘날 비판적 사고, 복잡한 추론, 작문 능력의 향상을 저해한다는 증거도 있습니다(Arum & Roksa, 2011; Pascarella 외., 2011). 여기에 제시된 간단한 프로세스 모델에 따르면, SET의 광범위한 사용은 이러한 효과의 주요 원인입니다. This model offers an explanation for the great paradox of American university education—namely, that GPAs have increased for decades (Rojstaczer,2015), yet university students have not become more hardworking or better qualified for college.3On the contrary, SAT scores show a downward trend (e.g., Adams,2015; Washington Post,2015), and students spend less time on academic pursuits today than they did a few decades ago (e.g., Arum & Roksa,2011; Babcock & Marks,2011). There is even evidence to suggest that a college education results in a lower gain in critical thinking, complex reasoning, and writing skills today than it did several decades ago (Arum & Roksa,2011; Pascarella et al.,2011). According to the simple process model suggested here, the widespread use of SETs is a major cause of these effects.
편향의 원인: 증거 Causes of bias: the evidence
이 섹션에서는 좋은 성적과 쉬운 코스에 대한 학생의 선호가 어떻게 SET를 편향시키고 코스 선택에 영향을 미치는지에 대해 설명합니다. Stroebe(2016)의 연구를 바탕으로 다음의 네 가지 명제에 대한 증거가 제시됩니다.
(a) 학생은 좋은 성적에 긍정적인 SET를 보상한다,
(b) 학생은 쉬운 코스에 긍정적인 SET를 보상한다,
(c) 학생은 좋은 성적을 약속하는 코스를 선택한다,
(d) 교수자는 좋은 SET를 원한다(필요로 한다)
This section discusses how students’ preference for good grades and easy courses biases SETs and influences course choices. Building on Stroebe (2016), evidence for four propositions is presented:
(a) Students reward good grades with positive SETs,
(b) students reward easy courses with positive SETs,
(c) students choose courses that promise good grades, and
(d) instructors want (need) good SETs.
학생은 좋은 성적에 대해 긍정적인 SET로 보상합니다. Students reward good grades with positive SETs
Anderson 등(1975)은 간단한 연구를 통해 이러한 편향을 입증했습니다. 그들은 한 수업에서 두 번, 즉 수업의 첫 번째 세션이 끝날 때와 마지막 세션이 끝날 때, 그리고 기말 시험 전에 기대 성적과 SET를 모두 평가했습니다. 그런 다음 참가자들을 성적 기대치가 더 나빠진 그룹, 좋아진 그룹, 동일하게 유지된 그룹으로 나누었습니다. 편향 해석을 뒷받침하는 결과, 강사와 코스에 대한 전반적인 평가는 성적 기대치가 높아질수록 향상되었고, 성적 기대치가 낮아질수록 크게 감소했습니다. 학부 경영학 과정 학생 499명을 대상으로 한 Clayson 등(2006)의 연구에서도 동일한 패턴이 보고되었습니다. 10주차에 그리고 16주차에 학생들은 강사와 기대 성적을 평가하도록 요청받았습니다. Anderson 등의 연구 결과와 마찬가지로, Clayson 등은 기대 성적의 변화가 강사에 대한 학생의 평가 변화와 연관되어 있음을 발견했습니다. Anderson et al. (1975) demonstrated this bias with a simple study. They assessed both grade expectations and SET twice in a class, once at the end of the first session of a class and again in the last session, but before the final exam. They then divided their participants into those whose grade expectations became worse, improved, or remained the same. In support of a bias interpretation, the overall ratings of instructor and course improved with improving grade expectations and decreased substantially with decreasing grade expectations. The same pattern was reported by Clayson et al. (2006) in a study of 499 students of undergraduate business courses. At Week 10 and again at Week 16, students were asked to evaluate their instructors and their expected grades. In line with the findings of Anderson et al., Clayson et al. found changes in expected grades to be associated with corresponding changes in students’ evaluation of their instructor.
웰슬리 대학이 관대한 학점을 부여하는 학과에 성적 상한선을 도입했을 때도 비슷한 패턴이 관찰되었습니다(Butcher 외., 2014). 2000년대 초, 웰슬리의 교수진과 행정부는 성적 인플레이션으로 인해 학교의 신뢰도가 위협받고 있다고 판단했습니다. 일반적으로 학점 인플레이션은 주로 인문사회과학 분야에서 문제가 되었지만 이공계 학과에는 영향을 미치지 않았습니다. 이 대학은 입문 및 중급 과정에서 평균 학점이 B+(3.33)를 넘지 않아야 한다는 규칙을 제정했습니다. 성적 상한제는 평균 학점을 낮추는 데는 효과적이었지만 교수 평가도 낮아지는 예상치 못한 부작용을 낳았습니다. 교수를 강력 추천하는 학생의 비율이 5% 감소하고, 중립 및 추천하지 않음 항목이 증가했습니다. Butcher 등(2014)은 "채점 정책으로 인해 평균 학점이 낮아지자 학생들이 교수에 대한 만족도가 낮아졌다는 결과가 강력하게 나타납니다."(200페이지)라고 결론지었습니다. 2019년에 이 대학은 이 채점 정책을 폐지했습니다 (https://www.wellesley.edu/registrar/grading/grading_policy).
A similar pattern was observed when Wellesley College introduced a grade ceiling for lenient-grading departments (Butcher et al.,2014). In the early 2000s, the faculty and administration at Wellesley decided that the credibility of the institution was threatened by grade inflation. As is generally the case, grade inflation was mainly a problem in the humanities and social sciences but did not affect science departments. The college instituted the rule that the average grade must not exceed a B+ (3.33) in introductory and intermediate courses. Although the grade ceiling was effective in lowering average grades, it had the unexpected side effect that it also lowered faculty ratings. The percentage of students strongly recommending their professor decreased by 5%, and there was an increase inneutralanddo not recommendcategories. As Butcher et al. (2014) concluded, “The results strongly indicate that students were less pleased with their instructors, when the grading policy lowered average grades” (p. 200). In 2019, the college rescinded this grading policy (https://www.wellesley.edu/registrar/grading/grading_policy).
경영대학원 필수 수업에 성적 상한선을 도입한 한 대형 주립대학에서 실시한 연구에서도 비슷한 결과가 보고되었습니다(Gorry, 2017). 성적 상한선은 입문 과정에서는 2.8점, 중급 과정에서는 3.2점으로 설정되었습니다. 두 상한선 모두 평균 성적을 낮추는 데 효과적이었습니다. 그러나 상한선을 2.8로 설정하면 코스 평가가 크게 낮아지고 자퇴 횟수도 증가한 반면, 상한선을 높게 설정하면 코스 평가에 미치는 영향은 훨씬 작았습니다. Similar findings were reported from a study conducted at a large state university where grade ceilings were introduced in required business school classes (Gorry,2017). The grade ceiling was set at 2.8 in introductory courses and at 3.2 in intermediate courses. Both ceilings were effective in lowering average grades. But while the 2.8 ceiling significantly lowered course evaluations and also increased the number of withdrawals, the effect of the higher ceiling on course evaluation was much smaller.
SET가 성적 기대치에 의해 편향된다는 가설에 대한 추가 지원은 Greenwald와 Gillmore(1997a)의 연구에서 나옵니다. 이 연구자들은 교수의 질과는 관련이 없는 세 가지 항목을 SET에 추가했습니다. 학생들은 강사의 필체의 가독성, 목소리의 명료성, 강의실 시설의 질을 평가해야 했습니다. 편향 해석에 따라 연구진은 기대 성적과 이러한 항목에 대한 평가의 긍정성 간에 양의 상관관계가 있음을 발견했습니다. 모든 학생이 같은 목소리를 듣고, 같은 글을 읽고, 같은 교실에서 수업을 들었기 때문에 이러한 학급 내 상관관계가 발견되었다는 것은 성적에 대한 기대치가 이러한 평가에 편향성을 가졌음을 시사합니다. 또한 학급 간 분석에서는 이러한 상관관계를 관찰할 수 없었으며, 이는 이러한 자질이 교수 효과와 관련이 없다는 가정을 더욱 뒷받침합니다. Further support for the hypothesis that SETs are biased by grade expectations comes from a study by Greenwald and Gillmore (1997a). These researchers added three items to an SET that were fairly unrelated to teaching quality. Students had to rate the legibility of the instructor’s handwriting, the audibility of his or her voice, and the quality of classroom facilities. In line with a bias interpretation, they found a positive correlation between expected grades and the positiveness of ratings on these items. Because all students heard the same voice, read the same writing, and worked in the same classroom, the finding of this within-class correlation suggests that grade expectations biased these evaluations. Furthermore, this correlation could not be observed for between-class analyses, which further supports the assumption that these qualities were unrelated to teaching effectiveness.
편향성 설명에 대한 보다 직접적인 증거는 올리바레스(2001)에 의해 제공되었는데, 그는 채점에 대한 관대함을 SET와 연관시켰습니다. 149명의 학생과 동일한 강사가 가르치는 두 학부 과정의 7개 섹션을 대상으로 한 연구에서 다음과 같은 질문을 통해 인식된 채점 관대함을 직접 측정했습니다: "지금까지 수강한 다른 모든 대학 강사와 비교했을 때, 이 강사의 채점을 어떻게 평가하시겠습니까?" 응답 척도는 매우 엄격함/엄격함부터 매우 쉬움/관대함까지 다양했습니다. 학기 말에 실시한 측정에서 채점 관용도는 교수자의 전체 평점(r = .45)과 여러 항목으로 구성된 SET 척도(r = .45) 모두와 상관관계가 있는 것으로 나타났습니다. 그리핀(2004)은 39개 교육 과정에 등록한 754명의 학부생을 대상으로 한 연구에서 이보다 다소 낮은 상관관계를 보고했습니다. 채점 관대함은 "이 교수자는 관대하거나 쉬운 채점자이다(매우 동의함부터 매우 동의하지 않음까지)"라는 문항으로 평가되었습니다. 모든 SET 평점의 평균과의 상관관계는 r = .23으로 Olivares(2001)의 연구보다 낮았습니다. 그러나 두 연구에서 모두 채점에 대한 관대함이 교수자 평가와 양의 상관관계를 보였으며, 이는 교수자가 관대하게 채점함으로써 강의 평가를 개선할 수 있어야 함을 시사합니다. Even more direct evidence for a bias explanation has been provided by Olivares (2001), who related perceived grading leniency to SETs. In a study based on 149 students and seven sections of two undergraduate courses taught by the same instructor, perceived grading leniency was measured directly with the following question: “Compared to all other college instructors you have had, how would you rate this instructor’s grading?” The response scale ranged frommuch harder/strict gradertomuch easier/lenient grader. In measures taken at the end of the semester, grading leniency correlated with both the global rating of the instructor (r=.45) and the multiple-items SET scale (r=.45). A somewhat lower correlation was reported by Griffin (2004) in a study based on 754 undergraduate students enrolled in 39 education courses. Grading leniency was assessed with the statement, “This instructor is a lenient/easy grader (strongly agreetostrongly disagree).” The correlation with the average of all SET ratings wasr=.23 and thus lower than in the study of Olivares (2001). However, in both studies, perceived grading leniency was positively correlated with instructor evaluation, suggesting that instructors should be able to improve their teaching ratings by grading leniently.
교수자가 관대하게 채점하거나 코스 요구 사항을 낮추고 싶지 않은 경우 다른 전략을 사용하여 SET를 개선할 수 있습니다. Youmans와 Jee(2007)의 연구에 따르면, 한 세트의 수업 중 절반은 세트에 응답해야 하는 날 초콜릿 바를 받았습니다. 초콜릿 바를 제공한 사람은 수업 강사와는 무관한 사람으로, 다른 기능에서 초콜릿 바를 가져온 것으로 추정됩니다. 초콜릿을 받은 학급의 평균 SET 점수가 더 높았습니다(4.07점 대 3.85점). 수업의 절반에게 첫 번째 세션에서 쿠키를 제공한 후 해당 세션의 강의 품질을 평가하도록 한 연구에서도 비슷한 평가 차이가 관찰되었습니다(Hessler et al., 2018). If instructors do not want to grade leniently or lower their course requirements, they can use other strategies to improve their SETs. In a study by Youmans and Jee (2007), half of a set of classes were treated with chocolate bars on the day they had to respond to the SET. The person giving the chocolate bars was independent of the class instructor and (allegedly) had these bars over from another function. The average SET score was higher for the classes receiving chocolate (4.07 vs. 3.85). A similar difference in ratings was observed in a study where half of the classes were given cookies during a first session and then had to evaluate the teaching quality of that session (Hessler et al.,2018).
학생들은 쉬운 코스에 좋은 SET로 보상 Students reward easy courses with good SETs
이 제안에 대한 지지는 주로 앞서 설명한 RMP 웹사이트의 연구에서 비롯됩니다. 이 웹사이트에서는 관대한 채점이라는 측면에서 '쉬움'이 명확하게 정의되어 있습니다. 학생들은 스스로에게 "이 교수가 가르치는 수업이 얼마나 쉬운가? 많은 노력 없이도 A를 받을 수 있는가?"라고 질문하도록 되어 있습니다. Easiness은 RMP 연구에서 교수 효과 평가의 강력한 예측 인자로 일관되게 밝혀졌습니다(Boehmer & Wood, 2017; Felton et al., 2008; Johnson & Crews, 2013; Rosen, 2018). 앞서 설명한 Felton 등(2008)의 연구에서 품질과 Easiness은 r = .62의 상관관계를 보였습니다. 학생들은 많은 노력 없이도 우수한 성적을 받을 수 있는 코스를 많은 시간과 노력이 필요한 코스보다 더 긍정적으로 평가했습니다. 뛰어난 교사가 아무리 어려운 내용도 쉽게 이해할 수 있도록 가르친다면 난이도가 교육의 질에 따른 결과일 수 있다고 주장할 수도 있지만, 이러한 해석은 난이도를 정의하는 방식과 일치하지 않을 수 있습니다. 또한 RMP에서는 학생이 교수에 대한 코멘트를 작성하여 자신의 평가를 정당화할 수 있으며, "'Easiness' 점수가 높은 교수는 일반적으로 업무량이 적고 학점이 높다는 코멘트를 받았습니다."(Felton 외., 2008, 40쪽). 이러한 결과는 Rosen(2018)에 의해 전반적인 품질과 Easiness 간의 상관관계가 r = .61로 나타나 펠튼 등이 보고한 상관관계와 거의 동일하게 재현되었습니다. Boehmer와 Wood(2017)와 Johnson과 Crews(2013)의 RMP 연구에서도 유사한 상관관계(각각 .66 및 .62)가 보고되었습니다. 앞서 설명한 RMP 연구에서 Timmerman(2008)이 보고한 난이도 평가와 교수자를 추천하는 학생의 비율 간의 상관관계는 r = .35로 다소 낮았습니다. Support for this proposition comes mainly from studies of the RMP website described earlier. On that website, easiness is clearly defined in terms of lenient grading. Students are instructed to ask themselves, “How easy are the classes this professor teaches? Is it possible to get an A without much work”? Easiness is consistently found to be a strong predictor of the evaluation of teaching effectiveness in RMP studies (Boehmer & Wood,2017; Felton et al.,2008; Johnson & Crews,2013; Rosen,2018). In the study by Felton et al. (2008), described earlier, quality and easiness correlated atr= .62. Students rated courses that enabled them to get excellent grades without doing much work more positively than courses that required a great deal of time and effort. Although one could argue that easiness might be a consequence of quality, with brilliant teachers making even the most difficult material easy to understand, this interpretation would be inconsistent with the way easiness is defined. Furthermore, RMP allows students to write comments about a professor to justify their ratings and “professors with high ‘Easiness’ scores usually received comments regarding a low workload and high grades” (Felton et al.,2008, p. 40). These findings were replicated by Rosen (2018) with a correlation between overall quality and easiness ofr= .61 that is practically identical to the correlation reported by Felton et al. RMP studies by Boehmer and Wood (2017) and Johnson and Crews (2013) reported similar correlations (.66 and .62, respectively). A somewhat lower correlation ofr=.35 between easiness ratings and the percentage of students recommending an instructor was reported by Timmerman (2008) in the RMP study described earlier.
3,799개 대학의 교수 85,306명의 데이터를 사용한 또 다른 RMP 연구에서는 상위권 대학에서 Easiness과 품질 간의 상관관계가 다소 약한 것으로 나타났습니다(Chiu et al., 2019). 이 연구자들은 2016년 Forbes의 미국 상위 200개 대학 분류(http://www.forbes.com/top-colleges)를 사용하여 표본의 대학을 상위 또는 비상위 기관으로 분류했습니다. 연구진은 쉬운 코스가 더 높은 수준으로 평가된다는 강력한 주 효과를 재현했지만, 대학 분류와 상호작용하기 쉬운 정도도 발견했습니다: 상위권 대학의 학생들은 비 상위권 대학의 학생들보다 쉬운 코스의 질에 대해 약간 덜 긍정적으로 평가했지만(각각 4.0점 대 4.13점), 어려운 코스는 약간 더 긍정적으로 평가했습니다(각각 3.37점 대 3.27점). 이러한 (소소한) 효과에 대한 가장 그럴듯한 해석은 상위권 대학이 더 열심히 노력하려는 학생들을 끌어들여 더 어려운 과목에 더 잘 대처할 수 있게 한다는 것입니다. The association between easiness and quality was found to be somewhat weaker at top universities in another RMP study using data of 85,306 professors from 3,799 colleges and universities (Chiu et al.,2019). These researchers used the 2016 Forbes classification of top 200 U.S. colleges and universities (http://www.forbes.com/top-colleges) to classify the colleges and universities of their sample into top or nontop institutions. Although they replicated the strong main effect that easy courses were rated as having a higher quality, they also found easiness to interact with their college classification: Students at top colleges evaluated easy courses slightly less positively on quality than students from nontop colleges (4.0 vs. 4.13, respectively) but rated difficult courses slightly more positively (3.37 vs. 3.27, respectively). The most plausible interpretation of these (minor) effects is that top colleges attract students who are more willing to work hard, which enables them to cope better with more difficult courses.
일부 연구자들은 RMP 등급이 대학 SET 등급과 동등한지 의심하기 때문에(예: Legg & Wilson, 2012; Murray & Zdravkovic, 2016), 이러한 동등성이 여기에 제시된 주장에 필수적인 것은 아니라는 점에 유의하는 것이 중요합니다. 학생 평가에서 'Easiness'이 코스의 '품질'에 대한 평가와 높은 상관관계가 있는 것으로 나타났다는 사실은 이 두 가지 차원이 학생들의 마음속에 밀접하고 긍정적으로 연관되어 있다는 충분한 증거입니다. Because some researchers doubt that RMP ratings are equivalent to ratings on university SETs (e.g., Legg & Wilson,2012; Murray & Zdravkovic,2016), it is important to note that this equivalence is not essential for the argument presented here. The fact that “easiness” has been found to be highly correlated with evaluations of the “quality” of a course in students’ ratings is sufficient evidence that the two dimensions are closely and positively associated in the minds of these students.
학생들은 좋은 성적을 약속하는 코스를 선택합니다. Students choose courses that promise good grades
경제학자 새뮤얼슨(1948)이 개척한 공개 선호 이론에 따르면 소비자의 선호도는 구매 행동으로 드러날 수 있습니다. 이 이론은 코스 선택에도 적용되어야 하므로, 관대하게 채점하는 교사의 코스에 대한 학생의 선호도는 코스 선택을 통해 드러나야 합니다. 초기 연구에서 Sabot과 Wakeman-Linn(1991)은 학생들이 한 학과에서 두 번째 과목을 수강할 가능성을 첫 번째 과목에서 받은 성적의 함수로 평가했습니다. 경제학을 전공할 의향이 없었지만 해당 학과의 과목을 수강한 적이 있는 학생 중 경제학 입문 과목에서 A가 아닌 B를 받은 경우 두 번째 과목을 수강할 확률이 18% 낮았고, C를 받은 경우 28% 낮았습니다. According to the revealed preference theory pioneered by the economist Samuelson (1948), the preferences of consumers can be revealed by their purchasing behavior. Because this theory should also apply to course choices, the preference of students for courses of teachers who grade leniently should be revealed by their course choice. In an early study, Sabot and Wakeman-Linn (1991) assessed the likelihood that students took a second course in a department as a function of the grades they received in their first course. Of students who did not intend to major in economics but had taken a course in that department, the probability of taking a second course was 18% lower if they received a B rather than an A and 28% lower if they received a C in an introductory course in economics.
마찬가지로 Johnson(2003)은 이전 학기에 수강한 과목의 평균 성적에 대한 정보를 제공한 종단 연구에서 이러한 정보가 학생의 향후 선택에 영향을 미친다는 사실을 발견했습니다. 한 학생이 두 명의 강사가 가르치는 과목 중 한 과목의 평균 학점이 A-이고 다른 과목의 평균 학점이 B인 경우, 학생이 두 번째 과목보다 첫 번째 과목을 선택할 확률은 2대 1이었습니다. 마지막으로, 물리 및 생명 과학 분야의 졸업에 대한 지속성에 대한 연구에서 Ost(2010)는 과학 과목보다 비과학 과목에서 더 높은 성적을 받은 학생이 선택한 과학 분야에서 더 높은 성적을 받은 학생보다 과학을 전과할 가능성이 더 높다는 것을 발견했습니다. Similarly, in a longitudinal study that provided information about the extent to which students informed themselves about the average grade of courses taught in the previous semesters, Johnson (2003) found that this information influenced students’ future choices. If a student had a choice between courses taught by two instructors, one course having a GPA of A– and the other having a GPA of B, the odds that a student would choose the first course over the second were 2 to 1. Finally, in a study of persistence toward graduating in the physical and life sciences, Ost (2010) found that students who received higher grades in their nonscience courses than their science courses were more likely to transfer out of the sciences than were students who received higher grades in their chosen science field.
관대하게 채점된 코스에 대한 학생들의 "드러난 선호도"에 대한 추가 증거는 코넬 대학교의 연구에서 나옵니다(Bar 외., 2009). 이 대학은 1998년부터 모든 과목의 중간 성적을 웹사이트에 게시하고 학생의 성적표에 이를 기재하기로 결정했습니다. 이 대학은 "성과에 대한 정확한 인식을 통해 학생들이 중간 성적이 상대적으로 낮은 과목을 수강하도록 장려할 수 있을 것"이라고 기대했습니다(94페이지). 하지만 이 희망은 실현되지 않았습니다. 실제로 이 웹사이트를 도입한 후 중앙값이 A인 과목의 비율이 16% 증가했습니다. 그러나 더욱 놀라운 것은 이러한 강좌에 등록한 학생의 비율이 42% 증가했다는 것입니다. 그러나 이러한 증가는 주로 평균 이하의 학생들 때문이었습니다. SAT 점수 기준 상위 20%에 해당하는 고능력 학생은 이러한 관대한 채점 방식의 강좌에 매력을 느끼지 못했습니다. Further evidence for students’ “revealed preference” for leniently graded courses comes from a study at Cornell University (Bar et al.,2009). This university decided as of 1998 to publish median grades for all courses on a website and to mention them in students’ transcripts. The university hoped that a more “accurate recognition of performance may encourage students to take courses in which the median grade is relatively low” (p. 94). This hope was not supported. In fact, the proportion of courses with an A median increased by 16% after the introduction of this website. But even more striking, the proportion of students who enrolled in such courses increased by 42%. However, this increase was mainly due to students of average or lower ability. High-ability students—in the top 20% according to their SAT scores—were less attracted by these leniently graded courses.
교수자가 좋은 SET 점수를 원한(필요로 한)다 Instructors want (need) good SETs
좋은 성적과 적은 학습량을 약속하는 코스에 대한 학생의 선호가 코스 성적에 영향을 미치려면 교수자가 이러한 선호를 채택하여 교수자의 선호로 전환해야 합니다. 앞서 언급했듯이 이러한 전환의 매개체는 바로 SET입니다. 학생과 교수진은 암묵적인 협상 상황에 놓여 있으며, 양측 모두 상대방에게 가치 있는 '좋은 것'을 가지고 있습니다.교수진은 좋은 성적과 쉬운 코스를 제공할 수 있고, 학생은 긍정적인 SET를 제공할 수 있습니다.교육의 질은 교수 평가의 중요한 측면이며, 앞서 언급했듯이 SET는 종종 교육의 질을 나타내는 주요 지표로 사용됩니다. 학생들이 좋아하고 많은 것을 배울 수 있는 코스를 만들기 위해 최선을 다했을 가능성이 높은 교사에게 낮은 평가를 받는 것은 불쾌한 경험이 될 수 있습니다. 낮은 SET는 교사의 종신 재직 또는 성과급 인상 기회를 감소시킬 수 있다는 사실 때문에 이러한 경험을 더욱 불쾌하게 만듭니다. 따라서 바람직한 행동에 대한 보상과 바람직하지 않은 행동에 대한 처벌이라는 SET의 분배 권한은 학생들이 교사의 행동을 형성할 수 있도록 합니다. For students’ preferences of courses that promise good grades and low workloads to influence course grades, these preferences must be adopted by faculty members andtransformedinto faculty preferences. As mentioned earlier, the medium of this transfer is the SET. Students and faculty are in an implicit negotiation situation, where each side has a “good” that is valuable to the other side. Faculty can provide good grades and easy courses, and students can provide positive SETs. Teaching quality is an important aspect of faculty evaluation and, as mentioned earlier, SETs are often used as major indicator of teaching quality. Receiving poor ratings is an unpleasant experience for teachers who are likely to have done their best to produce courses that students enjoy and in which they learn a great deal. The fact that poor SETs might decrease a teacher’s chance of tenure or of a merit salary increase makes this experience even more unpleasant. Thus, thepowerof dispensing SETs—to reward desirable and to punish undesirable behavior—enables students to shape faculty behavior.
불안정한 지위에 있는 교수진(예: 젊은 테뉴어 트랙 교수진)은 특히 관대한 채점을 통해 자신의 강의에 대한 평점을 개선하려는 동기를 갖게 된다는 증거가 있습니다. 한 중형 주립대학의 연구에 따르면 종신직과 비종신직이 가르치는 수업의 평점 차이는 0.5점 정도였으며, 비종신직이 더 좋은 성적을 받은 것으로 나타났습니다(Moore & Trahan, 1998). 대만 대학에서 실시한 연구에서 Keng(2018)도 비슷한 결과를 보고했습니다. There is evidence that faculty members in precarious positions (e.g., young tenure track faculty) will be particularly motivated to improve the ratings they receive for their course by grading leniently. A study at a medium-sized state university showed a difference in the GPA of classes taught by tenured versus untenured staff of half a grade point, with untenured staff giving better grades (Moore & Trahan,1998). Similar results were reported by Keng (2018) in a study conducted at a Taiwan university.
긍정적인 SET에 대한 교수진의 선호도는 의도적 경로와 비의도적 경로라는 두 가지 경로를 통해 교수자의 교육에 영향을 미칠 수 있습니다. 교수자를 대상으로 한 설문조사에 따르면 많은 교수자가 학생들이 관대하게 채점되고 쉬운 코스를 선호한다는 사실을 알고 있습니다(예: Birnbaum, 2000; Ryan et al., 1980; Simpson & Siguaw, 2000). 예를 들어, 캘리포니아 주립대 풀러턴 캠퍼스에서 Birnbaum(2000)이 실시한 소규모 설문조사에 응답한 교수진의 65%는 기준을 높이고 내용을 늘리면 교수 평가가 낮아진다고 생각했지만, 45%는 학생 학습이 향상될 것이라고 생각했습니다. 심지어 일부는 SET를 개선하기 위해 전략적으로 업무량을 줄이고 채점에 관대함을 사용했다고 인정했습니다. 72%는 SET를 사용하면 교수진이 강의 내용을 축소할 것이라고 생각했습니다. Faculty preference for positive SETs can influence faculty teaching by two routes—namely, a deliberate and a nondeliberate route. Surveys of instructors indicate that many teachers are aware of students’ preference for leniently graded, easy courses (e.g., Birnbaum,2000; Ryan et al.,1980; Simpson & Siguaw,2000). For example, 65% of the faculty members who responded to a small survey conducted by Birnbaum (2000) at the California State University, Fullerton, believed that raising standards and increasing content lowered teaching evaluation, even though 45% thought that it would increase student learning. Some even admitted using strategic workload reduction and grading leniency to improve their SETs. Seventy-two percent believed that the use of SETs would encourage faculty members to water down the content of their course.
실제로 위스콘신대학교 라크로스 캠퍼스에서 실시한 소규모 설문조사에 응답한 교수진의 22%는 SET의 도입으로 인해 코스에서 다루는 자료의 양을 줄이게 되었다고 답했으며, 38%는 난이도를 낮췄다고 인정했습니다(Ryan et al., 1980). 마지막으로, 안타깝게도 응답률이 매우 낮았던 마케팅 과학 아카데미 회원을 대상으로 한 웹 기반 설문조사에서는 응답자에게 동료가 SET에 영향을 미치기 위해 사용한 전략의 이름을 말하도록 요청했습니다. 가장 자주 언급된 전략은 관대한 채점이었습니다. 시험 당일에 쿠키, 스낵, 피자를 제공하는 것도 자주 언급되었습니다.앞서 설명한 것처럼 이러한 전략은 모두 효과적일 가능성이 높습니다. 교사들이 자신의 평가를 높일 수 있는 기법을 충분히 알고 있다면, 특히 낮은 평가를 받은 교사들 중 일부는 이러한 전략을 채택하고 싶은 유혹을 받을 것입니다. In fact, 22% of faculty respondents to a small survey conducted at the University of Wisconsin–La Crosse indicated that the introduction of SETs had induced them to decrease the amount of material covered in their course, and 38% admitted to lowering the difficulty level (Ryan et al.,1980). Finally, a web-based survey of members of the Academy of Marketing Science, which unfortunately had an extremely low response rate, asked respondents to name strategies that their colleagues had used to influence SETs. The most frequently mentioned strategy was grading leniency. Another frequently mentioned technique was serving cookies, snacks, or pizza on the day of the exam. As discussed earlier, all of these strategies are likely to be effective. If teachers are fully aware of techniques that could raise their evaluations, some of those receiving poor evaluations will be tempted to adopt these strategies, particularly if they are still untenured.
또한 학생은 교수자와 학생 중 어느 한쪽이 완전히 인식하지 못하는 사이에 원하는 방향으로 교수자의 행동을 변화시킬 수 있습니다.
코스에 대한 낮은 평가를 받은 교수자는 평가를 개선하기 위해 어떻게 해야 하는지 몇 명의 학생에게 물어볼 수 있습니다. 학생은 너무 많은 자료가 제시되고 토론 시간이 너무 짧았다고 불평할 수 있습니다. 또한 수강 중인 다른 수업에 비해 이 특정 코스에 너무 많은 독서가 필요하다고 언급할 수도 있습니다.
교수진은 '올해의 교사상'을 받은 동료가 이론과 연구 결과를 생생하게 보여주기 위해 몇 편의 영화를 보여준다는 사실을 더 알아차릴 수도 있습니다. 따라서 교수진은 자신의 SET를 개선하기 위해 강의에 제시되는 자료를 줄여 토론 시간을 만들고, 읽기 요구 사항을 줄이며, 강의를 더 매력적으로 만들기 위해 영화를 상영하기로 결정할 수 있습니다.
이러한 모든 변화는 학생들의 작업량을 상당히 줄여주고 훨씬 적은 양의 자료를 다루는 시험에서 좋은 성적을 거둘 가능성을 높여줍니다. Students can also shape the behavior of faculty members in a desired direction without either side being fully aware of doing so.
After receiving poor evaluations for a course, a faculty member might ask a few students what he or she should do to improve ratings. Students might complain that too much material was presented and there was too little time for discussion. They might also mention that too much reading was required for this particular course compared with other classes they were taking.
The faculty member might further realize that colleagues who receive “Teacher of the Year” awards show a few films to bring theories and findings to life. To improve his or her SETs, the faculty member might therefore decide to reduce the material presented in lectures to create time for discussion, to reduce reading requirements, and to show films to make lectures more attractive.
All of these changes will considerably reduce students’ workload and increase the chances that they will do well in exams that will cover much less material.
Uttl 등(2017)이 논의한 것처럼, 실제로 일부 SET 지지자들이 염두에 두고 있던 것이 바로 이 점이라는 점이 흥미롭습니다. 아브라미와 아폴로니아(1990)가 주장했듯이, It is interesting to note that, as Uttl et al. (2017) discussed, this is actually what some proponents of SETs had in mind. As Abrami and Apolonia (1990) argued,
너무 높은 학업 기준은 너무 낮은 학업 기준만큼이나 학생의 학습에 해로울 수 있습니다. 좋은 교수법의 과학적 기술은 학생들이 배울 수 있는 것과 학생들이 기대할 수 있는 것 사이의 균형을 찾는 것입니다. 평가는 이를 잘 수행하는 강사를 식별하는 데 도움이 된다고 믿습니다. (p. 520) academic standards that are too high may be as detrimental to the learning of students as academic standards that are too low. The art of science of good teaching is finding the balance between what students might learn and what students are capable of leaning. We believe that ratings help identify those instructors who do this well. (p. 520)
따라서 한 과목에서 가르쳐야 할 양을 결정해야 하는 것은 대학의 학문적 수준이나 학문을 습득하는 데 필요한 지식이 아니라 학생들이 과목에 기꺼이 노력을 투자하려는 의지와 그 내용을 습득할 수 있는 능력입니다. 그리고 이러한 지침을 기꺼이 따르는 교사만이 좋은 교수 평가를 받을 수 있습니다. So it is not the academic standard of a university or the knowledge that is required for mastering a discipline that should determine the amount that needs to be taught in a course but students’ willingness to invest effort in a course and their ability to master the material. And only teachers, who are willing and able to follow these guidelines will be rewarded with good teaching evaluations.
성적 인플레이션: 증거 Grade inflation: the evidence
대규모 사립 및 공립 대학 표본의 GPA 변화에 대한 광범위한 연구에서 Rojstaczer(2015; Rojstaczer & Healy, 2010)는 1930년대와 1940년대 이후 성적이 서서히 상승하고 있다는 사실을 발견했습니다. 그러나 1960년대에 가파른 상승세를 보이다가 1970년대에 평준화되었습니다(그림 3). 이러한 증가는 베트남 전쟁과 성적이 저조한 학생들이 징집되지 않도록 보호하고자 하는 바람 때문인 경우가 많았습니다(Rojstaczer & Healy, 2010). 1980년대에는 SET가 교수 평가의 주요 정보원이 되면서(Seldin, 1998), 10년에 0.10~0.15점의 비율로 성적이 다시 상승하기 시작했습니다. 이러한 증가는 공립 대학보다 사립 대학에서 훨씬 더 가파르게 나타났습니다. 로이스타처는 이러한 증가의 원인을 세 가지로 꼽았습니다:
(a) 수업에 대한 학생 평가가 의무화되었고,
(b) 학생들이 점점 더 진로에 집중하게 되었으며,
(c) 등록금 상승률이 가계 소득을 앞질렀습니다.
In an extensive study of changes in GPAs of a large sample of private and public universities, Rojstaczer (2015; Rojstaczer & Healy,2010) found that grades have been slowly rising since the 1930s and 1940s. However, there was a steep increase in the 1960s that leveled off in the 1970s (Figure 3). This increase has often been attributed to the Vietnam War and the wish to protect poorly performing students from being drafted (Rojstaczer & Healy,2010). In the 1980s, the time when SETs became major information sources in faculty evaluations (Seldin,1998), grades began to rise again at a rate of 0.10 to 0.15 GPA points per decade. These increases were much steeper for private than for public universities. Rojstaczer attributed this increase to three factors:
(a) Student evaluation of classes became mandatory,
(b) students became increasingly career focused, and
(c) tuition rises outpaced family incomes.
학생들은 고객이 되었고, (돈을 지불하는) 고객으로서 좋은 최종 결과물, 즉 취업 시장에서 경쟁력을 갖출 수 있는 성적을 받은 기말고사를 기대했습니다. 이러한 해석은 높은 등록금을 부과하는 유럽 국가 중 하나인 영국에서 고등 교육에 성적 인플레이션이 발생하는 이유도 설명할 수 있습니다(Bachan, 2017). Students became customers and, as (paying) customers, expected a good end product—namely, a final exam with a grade that would allow them to be competitive on the job market. This interpretation would also explain why there is grade inflation in higher education in the United Kingdom (Bachan,2017), the one European country that charges high tuition rates.
최근 수십 년 동안 학생들이 더 똑똑해지거나 더 열심히 일하게 되었다는 증거는 없습니다. 오히려 증거는 반대 방향을 가리키고 있습니다. 1969년과 1993년 사이에 SAT 평균 총점은 5% 감소했습니다(Rosovsky & Harley, 2002). 이러한 추세가 계속되고 있다는 것은 워싱턴 포스트(2015)에 실린 SAT 점수의 하락 추세가 계속되고 있다는 보고서에 의해 시사됩니다. 또한 학생들이 공부하는 데 더 많은 시간을 소비한다는 증거도 없습니다. 오히려 1960년에는 학생들이 학업에 주당 40시간을 투자했지만, 2003년에는 27시간, 2008년에는 15시간을 투자했습니다. 공부하는 시간, 실험실 시간, 수업 시간을 모두 합쳐도 오늘날 학생들은 학업에 보내는 시간은 16%에 불과합니다(Arum et al., 2011).
There is no evidence that students have become more intelligent or hardworking in recent decades. If anything, the evidence points in the opposite direction. Between 1969 and 1993, the average combined score on the SAT declined by 5% (Rosovsky & Harley,2002). That this trend has continued is suggested by a report in theWashington Post(2015) that SAT scores had continued their downward trend. There is also no evidence that students spend more time studying. On the contrary, whereas students spent 40hr per week on academic work in 1960, they devoted 27hr in 2003 and 15hr in 2008. Combining time for studying, for labs, and in classes, students today spend only 16% of their time on academic pursuits (Arum et al.,2011).
금전적 인플레이션에 비해 성적 인플레이션의 문제점은 성적이 5점 응답 척도로 표시된다는 점입니다. 성적이 상향 평준화되면 곧 상위권으로 쏠림 현상이 심해집니다.성적 인플레이션은 주로 A의 증가에 의해 주도되었습니다.2006년에는 전체 문자 성적 중 43%가 A였으며, 이는 1960년 이후 28% 포인트, 1988년 이후 12% 포인트 증가한 수치입니다(Rojstaczer & Healy, 2010). 성적 인플레이션의 가장 강력한 영향은 사립 대학에서 발생했으며, 사립 대학은 공립 대학보다 A와 B가 훨씬 더 많았습니다. 하버드 대학교에서는 학부 과정의 A 비율이 1966년 22%에서 1996-1997년 46%로 증가했습니다(B.P. Wilson, 1998). 가장 놀라운 점은 2013년에는 학부생의 평균 학점이 A-가 되었다는 점입니다(Bernhard, 2014). The problem with grade inflation as compared with monetary inflation is that grades are expressed on a 5-point response scale. With the upward shift in grading, it soon becomes very crowded at the top. The grade inflation was mainly driven by an increase in As. In 2006, 43% of all letter grades were As, an increase of 28 percentage points since 1960 and of 12 percentage points since 1988 (Rojstaczer & Healy,2010). The strongest effect of grade inflation occurred for private universities, where As and Bs became even more prevalent than at public universities. At Harvard, the percentage of As for undergraduate courses increased from 22% in 1966 to 46% in 1996–1997 (B.P. Wilson,1998). Most striking, by 2013, A– had become the median grade for undergraduates (Bernhard,2014).
성적 인플레이션은 주로 인문학과 사회과학(경제학 제외)에 영향을 미친 것으로 보입니다. 물리학, 화학, 수학에서는 성적 인플레이션이 훨씬 적은 것으로 보입니다. 그 이유는 명확하지 않습니다. 앞서 보고된 바와 같이, 이러한 "어려운 과학" 분야의 학생들이 좋은 성적을 받는 데 관심이 없다는 징후는 확실히 없습니다(Uttl & Smibert, 2017). 그렇다면 왜 이러한 교수들은 코스 부하를 완화하고 더 관대하게 채점하지 않을까요? 한 가지 설명은 어려운 과학과 수학 수업의 교육 목표가 훨씬 더 명확하게 정의되어 있기 때문일 수 있습니다. Lodahl과 Gordon(1972)은 이러한 차이를 설명하기 위해 Kuhn(1964)의 패러다임 개념을 사용합니다: "패러다임 개념의 본질은 이론, 방법론, 기술 및 문제에 대한 과학 분야 내 신념의 합의 또는 공유 정도입니다."(Lodahl & Gordon, 1972, 58쪽). 따라서 패러다임이 높은 분야일수록 코스 내용에 대한 합의가 더 높습니다. 교수자는 심리학 입문 수업에서 학생의 학습량을 자유롭게 결정할 수 있지만 수학, 물리학 또는 화학을 가르치는 수업에서는 그렇지 않을 수 있습니다. Grade inflation appears to have mainly affected the humanities and social sciences (with the exception of economics). There appears to be much less grade inflation in physics, chemistry, and mathematics. It is not clear why this is the case. As reported earlier, there certainly is no indication that students in those “hard science” areas are uninterested in receiving good grades (Uttl & Smibert,2017). So why do these professors not ease course loads and grade more leniently? One explanation could be that classes in hard sciences and mathematics have much more clearly defined teaching goals. Lodahl and Gordon (1972) use Kuhn’s (1964) concept of paradigm to describe this difference: “The essence of a paradigm concept is the degree of consensus or sharing of beliefs within a scientific field about theory, methodology, techniques and problems” (Lodahl & Gordon,1972, p. 58). High paradigm fields will therefore have greater agreement about the content of a course. Whereas instructors have a great deal of freedom in deciding how much a student has to learn in an introductory psychology class, this might not be the case in a class teaching mathematics, physics, or chemistry.
성적 인플레이션의 어두운 면 The dark side of grade inflation
학점 인플레이션이 서로 윈윈하는 상황이라고 주장할 수도 있습니다. 학생은 좋은 성적을 받고 강사는 좋은 SET를 받으니 모두가 만족할 수 있습니다. 안타깝게도 성적 인플레이션에는 어두운 면이 있으며 실제 효과는 훨씬 덜 긍정적입니다.성적 인플레이션은 우수한 성과를 내거나 합리적으로 열심히 일하려는 인센티브를 감소시킵니다. 모두가 A를 받는다면 학생이 왜 수업에 많은 시간을 투자해야 할까요? 따라서 성적이 관대하게 매겨진 수업에서 학생들이 덜 열심히 노력하는 것으로 밝혀진 것은 놀라운 일이 아닙니다(Babcock, 2010; Greenwald & Gillmore, 1997b). One could argue that grade inflation is a win-win situation. Students receive good grades and instructors receive good SETs and everybody is happy. Unfortunately, there is a dark side to grade inflation and the actual effects are much less positive. Grade inflation reduces the incentive to excel, or even to work reasonably hard. Why should a student invest a great deal of time in working for a class, if everybody gets an A? It is therefore not surprising that students have been found to work less hard in leniently graded classes (Babcock,2010; Greenwald & Gillmore,1997b).
예를 들어, Greenwald와 Gillmore(1997b)는 표준 SET에 코스에서 예상되는 성적과 작업량(학생이 코스에 투자한 시간 수)에 관한 질문을 추가했습니다. 학생이 코스에서 좋은 성적을 기대하는 경우 더 열심히 노력할 것이라고 생각할 수 있지만, 이러한 성적 기대가 채점 관용에 대한 지식에 기반한 것이라면 이는 적용되지 않을 것입니다. 이 후자의 가설과 일치하는 Greenwald와 Gillmore(1997b)의 연구에 따르면 작업량과 기대 성적 간에 음의 상관관계가 있는 것으로 나타났습니다. 이 효과는 상대적 기대 성적을 상관관계로 사용했을 때 더욱 강해졌습니다. 학생들이 평소 성적과 비교하여 현재 코스에서 더 나은 성적을 기대할수록 코스 활동에 투자하는 시간이 줄어드는 것으로 나타났습니다. 이 결과는 2003년부터 2007년까지 약 8,000개의 수업을 대상으로 한 Babcock(2010)에 의해 재현되었습니다. Babcock은 기대 성적이 1점 상승하면 주당 학습 시간이 0.94시간 감소할 것으로 추정했습니다. For example, Greenwald and Gillmore (1997b) added questions about expected grades in a course and about workload (numbers of hours students spent on a course) to a standard SET. Whereas one would think that students would work harder if they expected a good grade in a course, this should not apply if this grade expectation is based on knowledge about grading leniency. Consistent with this latter hypothesis, Greenwald and Gillmore (1997b) found a negative correlation between workload and expected grades. This effect became even stronger when relative expected grade was used as a correlate. The better students expected to do in the present course compared with their usual performance, the less time they invested in coursework. This finding was replicated by Babcock (2010) with nearly 8,000 classes covering the years 2003 to 2007. Babcock estimated that a 1-point increase in expected grade would reduce weekly study time by 0.94hr.
학생들이 성적이 관대할수록 과목을 더 긍정적으로 평가하지만(예: Griffin, 2004; Olivares, 2001), 동시에 그러한 과목에서 더 적게 학습한다면, 학생들이 더 긍정적으로 평가하는 과목에서 더 적게 학습할 것으로 예상할 수 있습니다. 이는 적어도 '나쁜 강의'를 학생이 많이 배우지 못하는 강의로 정의한다면 좋은 강의 평가가 실제로는 나쁜 강의에 대한 보상일 수 있음을 시사합니다(Stroebe, 2016). 코스 성적이 더 이상 학습의 유효한 지표로 간주될 수 없다는 사실은 교수 효과를 측정할 수 없게 만듭니다. Johnson(2003)은 후속 과정에서의 학생의 성과를 학습의 척도로 삼는 훌륭하지만 간단한 해결책을 제안했습니다. 즉, 학생들이 통계 입문 과목에서 학습한 양은 입문 과목에서 습득한 지식을 기반으로 하는 고급 통계 과목에서 받는 성적과 관련이 있어야 한다는 것입니다. If students evaluate a course more positively the more leniently they are graded (e.g., Griffin,2004; Olivares,2001), but at the same time work less in such courses, one could expect that students learn less in their more positively evaluated courses. This would suggest that good teaching evaluations may, in fact, reward bad teaching, at least if one defines “bad teaching” as courses in which students do not learn a great deal (Stroebe,2016). The fact that course grades can no longer be considered a valid indicator of learning leaves us without a measure of teaching effectiveness. Johnson (2003) suggested the brilliant but simple solution to take students’ performance in follow-up courses as a measure of learning. Thus, the amount students learned in an introductory statistics course should be related to the grades they receive in an advanced statistics course that builds on the knowledge acquired in the introduction.
이 패러다임을 사용한 6개의 연구가 수행되었습니다(Braga et al., 2014; Carrell & West, 2010; Johnson, 2003; Keng, 2018; Weinberg et al., 2009; Yunker & Yunker, 2003). 대부분은 많은 수의 코스 섹션에 의존할 수 있습니다. 이는 SET가 익명으로 처리되고 개별 학생에 대한 평가가 알려지지 않기 때문에 중요합니다. 따라서 SET와 동시 코스의 성적 간의 연관성은 일반적으로 한 섹션의 평균 SET와 해당 섹션의 평균 성적의 상관관계로 계산됩니다. Yunker와 Yunker(2003)의 연구는 12명의 교수자가 가르치는 46개 섹션만을 대상으로 한 것이지만, 미국 공군사관학교에서 수행된 Carrell과 West(2010)의 보다 일반적인 연구는 421명의 교수자가 2,820개의 개별 코스 섹션에서 가르치는 10,534명의 학생을 대상으로 표본 크기를 설정했습니다. 이 연구와 Braga 등(2014)의 연구 역시 학생들이 무작위로 섹션에 배정되었다는 장점이 있습니다. 6개의 연구 모두에서 SET는 동시 수강한 과목의 학생 성적과 양의 상관관계가 있었습니다. 그러나 후속 심화 과정의 성적을 기준으로 삼았을 때 5개의 연구에서 코스 평가는 음의 상관관계를 보였습니다(Braga et al., 2014; Carrell & West, 2010; Johnson, 2003; Keng, 2018; Yunker & Yunker, 2003).4 Weinberg 등(2009)의 연구에서는 현재 코스에 대한 학생 평가가 후속 코스에서의 성과와 무관한 것으로 나타났습니다. Six studies that used this paradigm have been conducted (Braga et al.,2014; Carrell & West,2010; Johnson,2003; Keng,2018; Weinberg et al.,2009; Yunker & Yunker,2003). Most of them could rely on large numbers of course sections. This is important, because SETs are anonymous and ratings are not known for individual students. Therefore, the association of SETs to grades in concurrent courses is typically computed as correlation of the average SET of a section with the average grades of that section. Although the study by Yunker and Yunker (2003) is based on only 46 sections taught by 12 faculty members, the more typical study of Carrell and West (2010)—conducted at the U.S. Air Force Academy—had a sample size of 10,534 students taught in 2,820 separate course sections by 421 faculty members. This study and the study by Braga et al. (2014) also have the advantage that students were randomly assigned to sections. In all six studies, SETs were positively correlated with students’ grades in the concurrent course. However, when performance in subsequent—more advanced—courses was used as criterion, course ratings were negatively correlated in five of the studies (Braga et al.,2014; Carrell & West,2010; Johnson,2003; Keng,2018; Yunker & Yunker,2003).4In the Weinberg et al. (2009) study, student evaluations of the current course were found unrelated to the performance in a subsequent course.
요약하면, Weinberg 등(2009)의 연구를 제외하고 이 연구들은 학생들이 많은 것을 배우지 못한 코스를 더 긍정적으로 평가하는 경향이 있다는 증거를 제시합니다. 또는 Braga 등(2014)의 결론처럼 "미래의 성과를 촉진하는 데 더 효과적인 교사가 학생들로부터 더 나쁜 평가를 받는다"(81쪽)는 결론을 내릴 수도 있습니다. In summary, then, with the exception of the study by Weinberg et al. (2009), these studies present evidence that students tend to evaluate more positively the courses in which they did not learn a great deal. Or, as Braga et al. (2014) concluded, “teachers, who are more effective in promoting future performance receive worse evaluations from their students” (p. 81).
일반적인 결론 General conclusion
이 글에서 검토한 증거를 통해 도출할 수 있는 주요 결론은 SET가 교수 효과성의 유효한 측정 기준이 아니므로 학장이나 학과장이 교수진을 평가하는 데 사용해서는 안 된다는 것입니다. 여전히 SET의 증거에 근거하여 인사 결정을 내리는 대학 관리자는 법정에서 자신의 결정에 이의를 제기할 수 있는 위험을 감수해야 합니다. 교수 효과성의 척도로서 SET가 무효라는 증거가 있고, Ryerson 대학의 사례에서 알 수 있듯이 이러한 법정 소송에서 승소할 가능성은 그리 높지 않습니다. The main conclusion to be derived from the evidence reviewed in this article is that SETs are not valid measures of teaching effectiveness and should therefore not be used by deans or chairpersons to evaluate faculty members. University administrators, who still base personnel decisions on evidence from SETs, run the risk that their decisions could be challenged in court. Given the evidence that SETs are invalid as measures of teaching effectiveness—and as the example of Ryerson University suggests—the chances of winning such court cases are not very good.
교수 능력은 성과급 인상이나 승진에 대한 결정에 중요한 요소이므로 대학 관리자는 다른 정보원을 사용할 수 있습니다. SET를 사용하는 대신 교사에게 강의 개발 방법과 강조하는 문제에 대한 자세한 설명을 담은 강의 포트폴리오를 작성하도록 요청할 수 있으며, 포트폴리오에는 권장 도서 목록과 시험 문제도 포함되어야 합니다. 이렇게 하면 적어도 특정 영역에 대한 강좌가 해당 영역의 핵심으로 간주되는 콘텐츠(예: 이론, 연구)를 다루고 최신 문헌에 기반하고 있음을 보장할 수 있습니다. 또한 이러한 포트폴리오에는 일부 주요 강의의 파워포인트 프레젠테이션이 포함될 수 있습니다(예: Goss & Bernstein, 2015). 테뉴어 결정의 경우, 선배 동료의 평가를 위해 몇 개의 강의를 비디오로 녹화할 수 있습니다. 강의에 대한 결정은 매우 저조한 성과를 확인하는 것만 포함하므로 이러한 평가에서 합의에 도달할 수 있어야 합니다. Because teaching ability is an important factor in decisions about merit increases or promotions, university administrators could use alternative sources of information. Instead of using SETs, they could ask teachers to compile teaching portfolios in which they give detailed descriptions of how they develop their courses and which issues they emphasize; the portfolio should also contain lists of recommended reading and exam questions. This would at least ensure that a course on a given area covers the content (i.e., theories, research) considered central to that area and is based on up-to-date literature. In addition, such a portfolio could include the PowerPoint presentations of some of the main lectures (e.g., Goss & Bernstein,2015). In the case of tenure decisions, one could video record a few lectures for evaluation by senior colleagues. Because the decision about teaching would only involve identifying a very poor performance, it should be possible to reach agreement in such evaluations.
SET 정보는 평가를 받는 교수자에게만 제공되어야 합니다. 이렇게 하면 교수자가 SET에서 높은 점수를 받아야 한다는 압박을 크게 줄일 수 있습니다(예: 기준을 낮추고 채점을 관대하게 함). SET가 편향되어 있기는 하지만, 이를 완전히 폐지하면 학생뿐만 아니라 교수자가 유용하게 활용할 수 있는 정보를 얻을 수 있는 기회를 박탈당하게 됩니다. 그러나 교수자는 SET에 영향을 미치는 다양한 편향의 원인을 인식하고 자신의 강의 평가를 평가할 때 이를 고려해야 합니다. 채점을 까다롭게 하고, 많은 독서를 요구하며, 학생에게 열심히 노력하는 모습을 보이는데도 최고 평점을 받는 영감을 주는 교사가 있습니다. 그러나 대부분의 교수자에게 이러한 전략은 적어도 학부 과정을 가르칠 때는 일반적으로 최적의 세트에 미치지 못하는 결과를 초래합니다. 그러나 대학 캠퍼스의 학부 학습에 대한 대규모 연구를 바탕으로 Arum과 Roksa(2011)는 "상당한 양의 읽기(일주일에 40페이지 이상)와 쓰기(한 학기 동안 20페이지 이상)가 모두 필요한 과목을 수강한 학생들의 학습률이 더 높았다"(205페이지)고 결론지었습니다. SET information should be provided only to the instructors who are evaluated. This would substantially reduce the pressure on faculty members to receive top SET scores (e.g., by lowering standards and lenient grading). Although SETs are biased, totally abandoning them would deprive not only students of their voice with regard to teaching quality but also instructors of information they might find useful. However, instructors should be aware of the various sources of bias that affect SETs and take them into account when assessing the evaluation of their own teaching. There are some inspired teachers who receive top ratings even though they are tough graders, require a lot of reading, look for hard work from their students. However, for most instructors such strategies will typically result in less-than-optimal SETs, at least when they teach undergraduate courses. Yet, based on a large study of undergraduate learning at college campuses, Arum and Roksa (2011) concluded “that students, who took courses requiring both significant reading (more than 40 pages a week) and writing (more than 20 pages over the course of the semester) had higher rates of learning” (p. 205).
적어도 사회과학과 인문학에서는 학생들이 좋은 학점을 받는 데 익숙해져 있기 때문에 학점 인플레이션을 없애기 위해서는 근본적인 대책이 필요합니다. 성적 상한제 도입은 효과적인 전략 중 하나입니다(Butcher et al., 2014; Gorry, 2017). 안타깝게도 학점 상한제는 이 정책을 시행하는 대학 학생들의 경쟁력을 떨어뜨린다는 단점이 있습니다.고용주들은 프린스턴의 학점 상한제를 알지 못할 수도 있기 때문에, B+가 A-보다 취득하기 더 어려웠을지라도 프린스턴 졸업생보다 A-를 받은 하버드 졸업생을 선호할 수 있습니다. 이것이 프린스턴이 2014년에 이 제도를 폐지한 이유일 것입니다(Windemuth, 2014). 그리고 웰슬리 칼리지가 2019년에 이 제도를 폐지한 이유일 것입니다. 따라서 성적 상한제는 사립 및 공립 대학의 전체 시스템에 도입되는 경우에만 허용될 수 있습니다. 미국에서는 그런 일이 일어날 가능성이 거의 없습니다. 대신, 일반적으로 도입될 수 있고 잠재적 고용주에게 더 많은 정보를 제공할 수 있는 덜 야심 찬 조치는 성적표에 학생의 개별 성적과 함께 수업의 중간 성적을 표시하는 것입니다. 그러나 대학 교사에게 자신의 강의가 학생들에게 어떻게 인식되었는지에 대한 정보를 제공하여 개선에 도움을 주기 위한 SET가 성적 인플레이션뿐만 아니라 교육의 질 저하를 초래한 것은 아이러니한 일입니다. Because students have become used to getting good grades, at least in the social sciences and humanities, radical measures would be needed to eliminate grade inflation. The introduction of grade ceilings is one effective strategy (Butcher et al.,2014; Gorry,2017). Unfortunately, grade ceilings have the disadvantage of lowering the competitiveness of students from universities practicing this policy. Because employers might not be aware of the Princeton grade ceiling, they might prefer a Harvard graduate with an A– to a Princeton graduate with a B+, even if the B+ might have been more difficult to get than the A–. This is probably the reason why Princeton dropped this measure in 2014 (Windemuth,2014), and why Wellesley College dropped it in 2019. Thus, grade ceilings would be acceptable only if they were introduced by the whole system of private and public universities. In the United States, something that is unlikely to happen. Instead, a less ambitious measure that could generally be instituted and would make grades more informative for potential employers would be to indicate the median grade of a class with students’ individual grades on their transcripts. It is ironic, though, that SETs intended to provide university teachers with information about how their teaching was perceived by students and thus help them to make improvements resulted not only in grade inflation but also in a deterioration of teaching quality.
참고 Notes
1 2016년 5월에 RateMyProfessors.com은 평가 방식을 변경했습니다. 명확성 및 유용성 점수를 삭제하고 이제 학생들에게 교수의 전반적인 질을 명시적으로 평가하도록 요청했습니다. 2018년 6월에는 성차별적이라는 불만에 대응하여 인기도 평가도 삭제했습니다. 1 In May 2016, RateMyProfessors.com changed their rating scheme. They dropped the clarity and helpfulness scores and now ask students to explicitly rate the overall quality of professors. In June 2018 they also dropped the hotness ratings, responding to complaints that it was sexist.
2 이 기사의 연구에 대한 설명이 완전히 명확하지 않습니다. 저자들은 보충 자료를 언급하고 있지만 제가 접근할 수 없었습니다. 기사에 제공된 보충 자료 주소는 항상 기사만 불러올 뿐 자료는 불러오지 않았습니다. 미첼 박사에게 보낸 이메일에는 답변이 없었습니다. 2 The description of the study in the article is not totally clear. The authors refer tosupplementary material, which I was unable to access. The address forsupplementary materialgiven in the article always brought up the article but not the material. An email to Dr. Mitchell was not answered.
3 이러한 역설은 미국만의 현상은 아닐 수 있습니다. 영국에서도 성적 인플레이션에 대한 증거가 있습니다(Adams, 2019; Bachan, 2017; Stroebe, 2016). 그러나 근본적인 과정에 대한 연구는 훨씬 적습니다. 3 This paradox may not be a uniquely American phenomenon. There is also evidence of grade inflation in Great Britain (Adams,2019; Bachan,2017; Stroebe,2016). However, there is much less research about underlying processes.
4 학생의 성적은 능력 요인에도 크게 영향을 받기 때문에 Yunker와 Yunker(2003)는 전체 GPA와 ACT 점수를 대조군으로 사용했습니다. Weinberg 등(2009)은 현재 수강 중인 과목의 성적을 통제했는데, 이는 문제가 있습니다. 4 Because students’ grades are also strongly influenced by ability factors, Yunker and Yunker (2003) used the overall GPA as well as the ACT score as controls. Weinberg et al. (2009) controlled for grades in the current course, which is problematic.
Abstract
Student Evaluations of Teaching (SETs) do not measure teaching effectiveness, and their widespread use by university administrators in decisions about faculty hiring, promotions, and merit increases encourages poor teaching and causes grade inflation. Students need to get good grades, and faculty members need to get good SETs. Therefore, SETs empower students to shape faculty behavior. This power can be used to reward lenient-grading instructors who require little work and to punish strict-grading instructors. This article reviews research that shows that students (a) reward teachers who grade leniently with positive SETs, (b) reward easy courses with positive SETs, and (c) choose courses that promise good grades. The study also shows that instructors want (and need) good SETs.
모듈에서 MOOCs로: 온라인 교육과정 개발의 여섯-단계 접근법(Acad Med, 2019) From Modules to MOOCs: Application of the Six-Step Approach to Online Curriculum Development for Medical Education Belinda Y. Chen, MD, David E. Kern, MD, MPH, Robert M. Kearns, MSEd, Patricia A. Thomas, MD, Mark T. Hughes, MD, MA, and Sean Tackett, MD, MPH
온라인 커리큘럼은 중요한 온라인 상호작용이 포함된 계획된 교육 경험입니다. 온라인 커리큘럼은 기관, 지리적, 시간적 경계를 넘나들며 교수 및 학습 효율성을 높이고 교육 학술활동을 구성할 수 있습니다. 대부분의 보건 전문직 학위 및 교육 프로그램에서 온라인 학습 버전을 채택하고 있습니다.1-3 Online curricula are planned educational experiences with significant online interactions. Online curricula can span institutional, geographic, and temporal boundaries; increase teaching and learning efficiency; and constitute educational scholarship. Versions of online learning have been adopted by most health professions degree and training programs.1–3
많은 교수진이 교육적 책임을 다하기 위해 온라인 커리큘럼 개발(CD)에 참여하고 있습니다. 커리큘럼 결과에 대한 책임을 지는 경우가 많지만, 교수진은 온라인 CD에 참여할 준비가 되어 있지 않을 수 있습니다. 이로 인해 교수진의 불만, 비효율적인 리소스 사용, 비효율적인 커리큘럼이 발생할 수 있습니다.2,4-6 Many faculty participate in online curriculum development (CD)to fulfill their educational responsibilities. Although often held accountable for curricular outcomes, faculty may be unprepared to engage in online CD. This can result in faculty frustration, inefficient resource use, and ineffective curricula.2,4–6
보건 전문직 커리큘럼은 대중의 건강 관리 요구를 충족해야 할 책임이 있기 때문에 건전한 CD 프로세스를 요구합니다. 온라인 교육 과정은 많은 청중에게 도달할 수 있기 때문에 온라인 CD는 특히 이러한 요구에 대한 책임이 있습니다. 이 글에서는 의료 교육용 CD에 대해 널리 받아들여지고 있는 체계적인 접근 방식7,8인 의학교육용 커리큘럼 개발을 위한 6단계 접근 방식을 온라인 CD에 어떻게 적용할 수 있는지 설명합니다. Health professions curricula demand sound CD processes because of their responsibility to meet the health care needs of the public. Online CD is particularly accountable to these demands because online curricula can reach large audiences. We describe how a widely accepted, systematic approach to CD for health care education7,8—the Six-Step Approach for Curriculum Development for Medical Education—can be applied to online CD.
이 글에서는 현재 널리 사용되는 네 가지 온라인 커리큘럼 형식을 설명하고 비교하며, 그 차이점이 온라인 CD에 실질적인 영향을 미칩니다(표 1): In this article we describe and compare four currently popular online curricular formats whose differences have practical implications for online CD (Table 1):
온라인 커리큘럼의 네 가지 일반적인 형식 비교 Comparisons of Four Common Formats of Online Curriculaa
혼합형 커리큘럼: 온라인과 대면 세션이 결합된 형태로, '플립형 강의실'은 혼합형 학습의 한 버전입니다. Blended curricula: Online and face-to-face sessions are combined; the “flipped classroom” is a version of blended learning.
교수자가 주도하는 완전 온라인 커리큘럼: 모든 커리큘럼 콘텐츠가 온라인으로 제공되며 교수진과 정의된 학습자 그룹 간에 온라인 상호 작용이 이루어집니다. Instructor-led fully online curricula: All curricular content is online, and online interaction occurs between faculty and a defined group of learners.
자기 주도형 모듈: 학습자가 커리큘럼을 시작하고 주도하며, 학습자가 학습하는 동안 교수자의 추가 입력이 필요하지 않습니다. Self-paced modules: The curriculum is initiated and directed by the learner, with no additional faculty input during the learner’s experience.
대규모 공개 온라인 코스(MOOC): 이 커리큘럼은 대규모의 쌍방향 참여를 목표로 하며 인터넷에 접속할 수 있는 사람이라면 누구나 참여할 수 있습니다. Massive open online courses (MOOCs): The curriculum aims for large-scale interactive participation and is open to anyone with Internet access.
의학 커리큘럼에서 사용되는 교육 방법, 평가 방법 및 리소스 유형에 대한 표준화된 용어도 만들어졌습니다.9 Standardized terminologies have also been created for the instructional methods, assessment methods, and resource types used within medical curricula.9
개요 Overview
6단계 접근법은 커리큘럼을 "계획된 교육 경험"으로 정의하며, 단기 교육 세션 또는 다년간의 프로그램에 적용할 수 있습니다. CD는 순차적으로 제시되지만 연속적이고 순환적인 프로세스이며 모든 단계는 서로 영향을 미칩니다(그림 1). 특정 교육 방법(4단계)을 고려하는 것으로 시작할 수 있지만, 실행을 위한 리소스 및 관리 요구 사항(5단계), 해당 방법이 대상 학습자의 요구 사항과 일치하는지 여부(2단계), 교육 목표(3단계), 학습자 및 프로그램 평가 계획(6단계) 등도 고려해야 합니다. 그림 1의 상단에 있는 1단계는 모든 보건 전문직 CD가 보건의료 문제를 해결하는 것을 목표로 한다는 점을 강조합니다. 아래에서는 각 단계의 기본 사항을 요약하고 온라인 CD의 각 단계에 대한 특별한 고려 사항을 설명합니다. The Six-Step Approach defines curriculum as any “planned educational experience” and can be applied to short educational sessions or multiyear programs. Though presented sequentially, CD is a continuous, cyclical process, and all steps influence each other (Figure 1). One might begin by considering a specific educational method (Step 4), but must also consider resource and administrative requirements for implementation (Step 5) and the method’s congruency with targeted learners’ needs (Step 2), as well as educational objectives (Step 3) and both learner and program evaluation plans (Step 6). Step 1 is at the top ofFigure 1to emphasize that all health professions CD aims to address a health care problem. Below, we summarize the fundamentals of each step and describe special considerations for each step in online CD.
1단계: 문제 식별 및 일반적인 요구 사항 평가 Step 1: Problem Identification and General Needs Assessment
일반 원칙 General principles
1단계에서 교육자는 교육 개입으로 해결할 의료 문제를 파악하고 지역적 수준에서 국제적 수준까지 그 중요성(예: 유병률, 이환율, 비용)을 특성화합니다. 이는 일반적으로 이용 가능한 데이터(예: 출판된 문헌, 공중 보건 통계)를 검토하고 새로운 데이터(예: 전문가 자문)를 수집하여 수행합니다. In Step 1, the educator identifies the health care problem that the educational intervention will address and, on a regional to international level, characterizes its importance (e.g., prevalence, morbidity, cost). This is typically done by a review of available data (e.g., published literature, public health statistics) and collection of new data (e.g., expert consultation).
일반적 요구도 평가는 환자, 사회, 보건의료 교육자, 보건의료 전문가가 파악한 문제에 대한 이상적인 접근 방식과 현재 접근 방식 사이의 격차를 정의합니다. 1단계는 대규모로 수행하거나10 소규모 CD 팀에 의해 수행될 수 있습니다. 1단계가 끝나면 교육자는 계획된 교육 활동을 통해 보건의료 전문직 교육생이 미래 환자의 요구를 충족할 수 있도록 준비하는 방법을 명확히 설명할 수 있습니다. The general needs assessment defines the gap between the ideal and current approaches to the identified problem by patients, society, health care educators, and health care professionals. Step 1 may be conducted on a large scale10or by smaller CD teams. By the end of Step 1, educators can articulate how planned educational activities will prepare health professions trainees to meet the needs of future patients.
특별 고려사항 Special considerations
온라인 CD의 1단계는 기존 CD와 유사한 경우가 많지만, 온라인 CD에서는 기존 온라인 커리큘럼을 검색하는 데 더 많은 노력이 필요합니다. 동료 검토를 거친 온라인 커리큘럼 저장소(예: http://www.mededportal.org)를 검색하고 교육기관 및 전문 학회 웹사이트(예: http://www.POGOe.org)8를 검토하면 결과를 얻을 수 있습니다. 교육자들과 네트워킹하거나 의학 사서와 상담하면 비슷한 문제를 해결하기 위한 다른 커리큘럼을 파악하는 데 도움이 될 수 있습니다. Often, Step 1 for online CD is similar to traditional CD, although more effort is required in online CD to search for existing online curricula. Searching online peer-reviewed curriculum repositories (e.g.,www.mededportal.org) and reviewing websites of institutions and professional and specialty societies (e.g.,www.POGOe.org)8can yield results. Networking with educators or consulting with medical librarians can help identify other curricula that aim to solve similar problems.
다음은 1단계가 결핵(TB) 치료를 개선하기 위해 온라인 CD에 어떤 영향을 미쳤는지 보여주는 예시입니다.
결핵은 효과적인 치료 옵션이 있음에도 불구하고 저소득 및 중간 소득 국가(LMIC)에서 이환율과 사망률의 주요 원인으로 확인되었습니다. 사례 발견 및 치료 권고에 관한 의료진의 지식 격차가 중요한 장벽으로 밝혀져 교육적 개입이 결핵 치료에 도움이 될 수 있습니다. 기존 커리큘럼은 대면 교육으로 진행되었기 때문에 출장 비용과 일정 관리 등의 문제로 인해 접근성이 제한적이었습니다. 이러한 단점을 해결하기 위해 "글로벌 결핵 임상 관리 및 연구"라는 제목의 MOOC를 개발하여 LMIC의 의료진에게 마케팅하여 7,800명의 학습자에게 성공적으로 도달했으며, 이 중 87%는 결핵 유병률이 높은 환경에서 근무하는 사람들이었습니다.11
Here is an illustration of how Step 1 influenced online CD to improve tuberculosis (TB) care.
TB was identified as a leading cause of morbidity and mortality in low- and middle-income countries (LMICs) despite the existence of effective treatment options. Provider knowledge gaps regarding case-finding and treatment recommendations were found to be an important barrier, making TB care amenable to an educational intervention. Existing curricula were face-to-face, which limited their reach because of travel costs and scheduling logistics. To address these shortcomings, a MOOC titled “Global Tuberculosis Clinical Management and Research” was developed and marketed to providers in LMICs, successfully reaching 7,800 learners, 87% of whom were in settings with high TB prevalence.11
단순히 온라인으로 커리큘럼을 제공하는 것만으로는 보건 요구 사항을 해결하지 못할 수 있습니다. 일반적인 MOOC 데이터에 따르면 가장 필요한 사람들에게 도달하지 못하는 경우가 많습니다.12,13 커리큘럼의 목적을 명확히 하면 커리큘럼 개발자가 교육 효과를 극대화하는 결정을 내리는 데 도움이 됩니다. Simply making a curriculum available online may not address health needs. General MOOC data indicate that many may not reach those who need them most.12,13Clarifying one’s curricular purpose helps the curriculum developer make decisions to maximize educational impact.
2단계: 목표 요구 사항 평가 Step 2: Targeted Needs Assessment
일반 원칙 General principles
2단계에서는 대상 학습자의 요구 사항과 학습 환경에 초점을 맞춥니다. 목표 요구 사항 평가에는 대상 학습자 및 이해 관계자의 특성, 요구 사항, 선호도, 학습자 환경에서 사용 가능한 리소스 등의 데이터 수집이 포함됩니다. Step 2 focuses on the needs of one’s targeted learners and their learning environments. The targeted needs assessment involves the collection of data, such as the characteristics, needs, and preferences of the targeted learners and stakeholders, and available resources in the learners’ environments.
특별 고려 사항 Special considerations
온라인 CD의 목표 요구 사항 평가는 범위와 복잡성이 다양할 수 있습니다. "강의실 뒤집기"14는 교수자가 청중을 알고 있기 때문에 비교적 간단할 수 있습니다. 자기 주도형 모듈 또는 MOOC는 지리적으로 분산된 다양한 학습자 그룹을 대상으로 하기 때문에 복잡할 수 있습니다. Targeted needs assessments for online CD can vary in scope and complexity. “Flipping the classroom”14may be relatively simple because the instructor knows the audience. Self-paced modules or MOOCs can be complex because they target diverse groups of geographically dispersed learners.
온라인 커리큘럼은 낮은 사회적 참여도, 낮은 관련성 인식, 부적절한 자기 조절 행동과 관련하여 중도 탈락률이 높을 수 있으므로,15,16 학습자의 요구, 선호도, 동기, 온라인 학습에 대한 과거의 긍정적 및 부정적 경험17을 이해하는 것이 참여도를 유지하는 데 중요합니다.
학습자의 언어 능력,
문화,
선호하는 콘텐츠 액세스 모드(예: 노트북, 태블릿, 모바일 장치),
학습 경험에 사용할 수 있는 시간,
동기식 세션의 가용성(예: 지역사회 건강 결과 커리큘럼 연장에 참여하는 의료 제공자18),
학점의 필요성(예: 계속 의학 교육[CME], 자격증 유지),
액세스 또는 수료 인정에 대한 지불 의향
...도 온라인 교육 과정의 수용에 영향을 줄 수 있습니다. Online curricula can have high dropout rates related to low social engagement, low perceived relevance, and inadequate self-regulatory behaviors,15,16so understanding learner needs, preferences, motivations, and past positive and negative experiences with online learning17is important for maintaining engagement.
Learners’ language skills,
cultures,
preferred modes of accessing content (e.g., laptop, tablet, mobile device),
time available for the learning experience,
availability for synchronous sessions (e.g., practicing providers to participate in extension for community health outcomes curricula18),
the need for credit (e.g., continuing medical education [CME], maintenance of certification), and
the willingness to pay for access or recognition of completion
...may also affect the uptake of an online curriculum.
평가해야 할 환경적 요인으로는 인터넷 접속의 가용성 및 품질, 현지 테크놀로지 지원 등이 있습니다. 국제 커리큘럼의 경우, 미디어 공유(예: YouTube) 및 소셜 미디어(예: Facebook) 플랫폼에 대한 접근 제한과 같은 법률 및 규정이 커리큘럼 콘텐츠 제공 또는 커뮤니케이션을 위해 어떤 사이트를 선택할지에 영향을 미칠 수 있습니다. Environmental factors to evaluate include the availability and quality of Internet access and local technical support. For international curricula, laws and regulations, such as restricted access to media-sharing (e.g., YouTube) and social media (e.g., Facebook) platforms, can affect which sites are chosen for curricular content delivery or communication.
학습자와 학습자의 환경을 사전에 완전히 평가할 수 없는 경우, 목표 요구 사항 평가의 일부를 온라인 커리큘럼에 포함시킬 수 있습니다. 예를 들어, 커리큘럼을 진행하는 동안 학습자의 피드백을 의도적으로 수집하면 혼란스러운 용어나 문화적으로 민감한 이미지 중 수정이 필요한 부분을 파악할 수 있습니다. When learners and their environments cannot be fully assessed in advance, parts of a targeted needs assessment can be embedded in online curricula. For example, intentionally gathering feedback from learners during the curriculum can identify confusing terminology or culturally sensitive images needing revision.
3단계: 목표 및 목적 Step 3: Goals and Objectives
일반 원칙 General principles
요구 사항 평가를 기반으로 3단계에서 목적과 목표를 정의합니다.
목적goals은 방향을 제시하고 커리큘럼의 경계를 설정합니다.
목표objectives는 학습자의 인지, 정서 및 정신 운동 성취도에 대한 구체적이고 측정 가능한 기대치를 설명합니다.
목표objectives는 건강 관리에 미칠 것으로 예상되는 영향을 명확히 설명할 수 있습니다.
교육 목적과 목표는 이후 단계에서 교육 및 평가 전략의 선택을 안내합니다.
Based on the needs assessments, goals and objectives are defined in Step 3.
Goals provide direction and set curricular boundaries.
Objectives describe specific and measurable expectations for learners’ cognitive, affective, and psychomotor achievements.
Objectives can also articulate the anticipated impact on health care.
Goals and objectives guide the selection of educational and evaluation strategies in later steps.
특별 고려 사항 Special considerations
교직원은 새로운 교육 테크놀로지의 '화려한' 기능을 시험해 보고 싶은 유혹을 받을 수 있습니다. 그러나 1단계에서 설명한 의료 요구 사항과 2단계의 목표 요구 사항 평가를 기반으로 목표를 작성하면 기존 테크놀로지 및 새로운 테크놀로지를 보다 신중하게 사용할 수 있습니다.
블렌디드 커리큘럼은 라이브 세션 중에 실습과 피드백을 통합하여 의사소통 및 절차적 스킬에서 고차원적인 목표를 달성하는 데 도움이 될 수 있습니다.
MOOC와 자기 주도형 모듈은 더 많은 학습자에게 정보를 전달할 수 있지만, 현재 학습자의 심리 운동 스킬을 개발하거나 학습자의 행동을 변화시키는 데는 한계가 있습니다.
앞으로는 복잡한 분기 로직이 포함된 시뮬레이션 사례 시나리오와 가상 환경과 같은 새로운 테크놀로지를 통해 학습자가 고차원적인 인지적 사고, 절차, 심지어 팀워크와 커뮤니케이션 스킬까지 연습할 수 있게 될 것입니다.
일반적으로 고차원적인 목표19,20를 설정하고 그에 따라 테크놀로지를 선택해야 합니다. 또한 테크놀로지가 허용하는 경우 학습자가 직접 목표를 설정하는 데 참여해야 합니다.21 Faculty may be tempted to try out the “bells and whistles” of new educational technologies. However, writing objectives based on the health care need delineated in Step 1 and the targeted needs assessment in Step 2 can direct more thoughtful use of established and emerging technologies.
Blended curricula can help achieve higher-order objectives in communication and procedural skills by integrating practice and feedback during live sessions.
MOOCs and self-paced modules may convey information to a larger number of learners, but are currently limited in their ability to develop learners’ psychomotor skills or change learners’ behaviors.
In the future, new technologies such as simulated case scenarios with complex branching logic and virtual environments may allow learners to practice higher-order cognitive thinking, procedures, and even teamwork and communication skills.
Generally, one should aim for higher-order objectives19,20and select technologies accordingly. Also, when technology permits, learners should be engaged in setting their own objectives.21
4단계: 교육 전략 Step 4: Educational Strategies
일반 원칙 General principles
4단계는 교육 목표 달성을 촉진하기 위해 실현 가능한 교육 전략과 콘텐츠를 선택하는 단계입니다. 교육 목표에 부합하는 여러 교육 방법을 사용하면 학습을 강화하고 학습자 선호도의 차이를 해결할 수 있습니다. Step 4 involves selecting feasible educational strategies and content to facilitate achievement of educational objectives. Using multiple educational methods congruent with educational objectives reinforces learning and addresses differences in learner preferences.
특별 고려 사항 Special considerations
온라인 커리큘럼은 멀티미디어, 상호 작용 및 가상 소셜 구성 요소를 통합하여 기존의 교실 기반 모델보다 더 유연하고 접근 가능하며 개별화된 학습을 가능하게 할 수 있습니다. 최적의 온라인 학습을 위한 공식은 없지만,22,23 교육 전략의 선택을 안내하는 증거와 원칙이 존재합니다. 예를 들어,
연구에 따르면 연습 문제, 간격을 둔 반복, 피드백, 사회적 존재감이 고차원적인 학습자 목표를 달성하는 데 가장 효과적이라고 합니다.6,24
콘텐츠 레이아웃 및 멀티미디어 통합 지침25,26에서는 정보를 '청크'하고 그래픽과 단어를 결합하여 청각과 시각 경로를 동시에 자극하는 것을 권장합니다.
연구와 전문가 지침이 불충분한 경우 일반적인 교육 과학과 이론이 교육 전략을 안내할 수 있습니다.
Online curricula can incorporate multimedia, interactivity, and virtual social components to allow for more flexible, accessible, and individualized learning than traditional classroom-based models. Although there is no formula for optimal online learning,22,23evidence and principles exist to guide selection of educational strategies. For example,
studies have suggested that practice exercises, spaced repetition, feedback, and a social presence are most effective for achieving higher-order learner objectives.6,24
Guidelines for content layout and incorporating multimedia25,26endorse “chunking” information, combining graphics and words, and simultaneously stimulating auditory and visual pathways.
When studies and expert guidelines are insufficient, general educational science and theory can guide educational strategies.
대부분의 온라인 커리큘럼은 커리큘럼 콘텐츠를 저장 및 전달하고 평가 및 평가를 용이하게 하는 소프트웨어인 학습 관리 시스템(LMS)을 통해 전달됩니다. 많은 교육기관이 이미 LMS 공급업체와 계약을 맺었지만 일부 LMS는 오픈 액세스 방식입니다. LMS는 테크놀로지 지원을 제공할 수 있지만 커리큘럼 옵션을 제한할 수도 있습니다. 새로운 테크놀로지는 인터넷 접속이 원활하지 않은 환경에서도 '온라인 커리큘럼'에 접근할 수 있게 해주며,27 이러한 테크놀로지가 LMS와 어떻게 연동되는지에 따라 교육 전략에 더 많은 영향을 미칠 수 있습니다. 커리큘럼 내에서 LMS 선택 및 교육 설계를 결정할 때는 LMS 옵션의 특성을 파악하는 것이 중요합니다. Most online curricula are delivered through learning management systems (LMSs), software that stores and delivers curricular content and facilitates assessment and evaluation. Some LMSs are open-access, although many institutions have already contracted with LMS vendors. LMSs can offer technical support but may also constrain curricular options. New technologies make it possible to access “online curricula” despite poor Internet access,27and how these interface with LMSs may further influence educational strategies. Knowing characteristics of one’s LMS options is important for LMS selection and instructional design decisions within the curriculum.
기존 커리큘럼을 온라인 형식으로 전환하면 교수진과 학습자 간의 동기식상호 작용을 유지하면서 더 많은 청중에게 다가갈 수 있고 강의실 공간의 제약을 극복할 수 있습니다. 웹 회의 소프트웨어를 사용하는 라이브 세션이 포함된 완전 온라인 커리큘럼과 같은 온라인 동기식 세션을 사용하면 기존의 대면 방식을 간단하게 조정할 수 있습니다. 특수 온라인 미디어 룸을 사용하면 강사가 학습자의 표정과 몸짓을 관찰하는 등 실시간으로 학습자를 볼 수 있으므로 기존 강의실을 시뮬레이션할 수 있습니다. 학습자의 유연성을 높이기 위해 기존 방식을 비동기식온라인 형식에 적용하는 것은 쉽지 않지만, 유사한 방식이 존재하고(표 2) 대부분의 LMS와 호환되는 경우가 많습니다. Converting a traditional curriculum to an online format can allow faculty to reach a larger audience and overcome classroom space limitations while maintaining synchronous interactions between faculty and learners. Adapting traditional face-to-face methods can be made straightforward by using online synchronous sessions, such as fully online curricula with live sessions that use web conferencing software. Use of special online media rooms can simulate traditional classrooms as an instructor can view learners in real time, including observing facial expressions and body language. Adapting traditional methods to asynchronous online formats, often to increase learner flexibility, is less straightforward, although analogous methods exist (Table 2) and are compatible with most LMSs.
저작권 및 공정 사용 원칙은 온라인 커리큘럼에 사용할 콘텐츠를 선택할 때 고려해야 할 주요 사항입니다.
저작권은 원본 콘텐츠의 제작자가 배포를 승인할 수 있는 법적 권리입니다.
공정 사용은 저작권이 있는 저작물을 교육 목적으로 제한적으로 사용하는 경우에 적용됩니다. 그러나 자료가 온라인으로 널리 배포되거나 온라인 커리큘럼에 대한 요금이 부과되는 경우에는 공정 사용 원칙이 더 이상 적용되지 않을 수 있으며, 법률 상담이 필요할 수 있습니다.
저작권법은 국가마다 다르며무엇이 공정 사용으로 간주되는지는 해석에 따라 달라질 수 있습니다.28 저작권 규정을 위반하지 않으려면 공개적으로 이용 가능한 콘텐츠 또는 크리에이티브 커먼즈 라이선스(적절한 저작자 표시를 통해 원본 저작물의 공유를 허용하는 라이선스)가 있는 콘텐츠를 사용하는 것이 좋습니다.29
Principles of copyright and fair use are major considerations when choosing the content for online curricula.
Copyright is the legal right of a creator of original content to authorize its distribution.
Fair use applies to limited use of a copyrighted work for educational purposes. However, when material is widely distributed online or there is a charge for online curricula, the principle of fair use may no longer apply, and legal consultation may be needed.
Copyright laws vary internationally, and what is considered fair use is subject to interpretation.28To avoid violating copyright regulations, consider using publicly available content or content with a Creative Commons license (which permits sharing of an original work with appropriate author attribution).29
마지막으로 예산은 방법 선택에 영향을 미칩니다. 텍스트와 기성 그래픽은 일반적으로 비용이 저렴하지만, 맞춤형 그래픽과 전문 동영상은 제작 비용이 수백 또는 수천 달러에 달할 수 있습니다. 먼저 목표에 부합하는 여러 전략을 파악한 다음 사용 가능한 리소스에 따라 선택하는 것이 좋습니다. Finally, budgets influence choice of methods. Text and ready-made graphics are typically inexpensive, whereas custom graphics and professional videos can cost hundreds or thousands of dollars to produce. We recommend first identifying multiple strategies congruent with one’s objectives, and then selecting based on available resources.
5단계: 구현 Step 5: Implementation
일반 원칙 General principles
5단계에서는 교육과정을 실행하기 위한 자원(예: 인력, 시간, 공간 및 자료, 자금), 정치적 지원, 행정 메커니즘을 식별, 조달, 적절히 사용하는 것이 포함됩니다. 파일럿은 정식 시행에 앞서 학습자의 경험을 바탕으로 교육과정을 수정할 수 있는 기회를 제공합니다. 커리큘럼이 혁신적이거나 학습자가 회의적인 경우에는 우호적인 청중을 대상으로 파일럿을 실시하는 것이 현명합니다. 복잡한 커리큘럼은 리소스를 집중하고 초기 성공 가능성을 극대화하며 더 많은 수요를 창출하기 위해 별도의 세그먼트로 단계적으로 도입할 수 있습니다. Step 5 involves the identification, procurement, and appropriate use of resources (e.g., personnel, time, space and materials, funding), political support, and administrative mechanisms to implement the curriculum. Piloting provides an opportunity to revise a curriculum, based on learner experience, prior to full implementation. When the curriculum is innovative or learners are skeptical, piloting on a friendly audience is wise. Complicated curricula may be phased in as separate segments to focus resources, maximize the likelihood of initial success, and create demand for more.
특별 고려 사항 Special considerations
온라인 커리큘럼은 더 많은 인력과 재정적 요구 사항, 다양한 대상에게 배포해야 하는 어려움, 학습자와 참여 교수진 모두 온라인 교육에 익숙해져야 하기 때문에 기존 커리큘럼보다 구현이 더 복잡한 경우가 많습니다30. 교육기관마다 테크놀로지에 투자하는 방식은 다르지만,31 온라인 CD를 교육기관의 우선순위에 맞게 조정하면 복잡성을 관리하고 CD를 간소화하는 데 필수적인 리소스에 접근할 수 있습니다. Implementation for online curricula is often more complex than for traditional curricula30because of greater personnel and financial requirements; challenges of disseminating to large, diverse audiences; and the need to familiarize both learners and participating faculty with online instruction. Although academic centers vary in how they invest in technology,31aligning online CD with institutional priorities can provide access to essential resources to manage complexities and streamline CD.
온라인 커리큘럼을 탐색하는 것이 간단해 보이는 경우에도 학습자와 교수진에게 지침과 데모를 제공하는 것이 필요한 경우가 많습니다. 일부 교육기관에서는 LMS 탐색을 도입하는 온라인 커리큘럼을 필수로 제공합니다. 온라인 커리큘럼에는 처음에 탐색을 위한 간단한 지침이 포함될 수도 있습니다. 커리큘럼을 진행하는 동안 문제를 해결하기 위한 지속적인 테크놀로지 지원이 필요한 경우가 많습니다. LMS 공급업체에서 테크놀로지 지원을 제공하지 않거나 여러 시스템을 사용하는 경우, 교육기관 또는 후원 조직에서 테크놀로지 지원을 제공하여 교직원의 중요한 리소스가 테크놀로지 문제 해결에 전용되지 않도록 해야 합니다. Providing instructions and demonstrations for learners and faculty is often necessary even when navigating online curricula seems straightforward. Some institutions have prerequisite online curricula that introduce LMS navigation. Online curricula can also include brief instructions for navigation at the outset. Ongoing technical support to troubleshoot issues during the curriculum is often necessary. If the LMS vendor does not provide technical support or if multiple systems are used, the institution or sponsoring organization will need to provide technical assistance to avoid diverting significant faculty resources to overcoming technical issues.
교수진은 혼합형 커리큘럼을 개발할 때 온라인 요소를 독립적으로 통합할 수 있지만, 일반적으로 온라인 CD의 다양한 측면에 익숙한 팀원과 협력하는 것이 좋습니다(표 3). 교수는 일반적으로 교수 설계자, 프로젝트 관리자 및/또는 미디어 테크놀로지자(예: 비디오그래퍼, 그래픽 디자이너)와 협력하여 주제별 전문가(SME)의 역할을 수행합니다. 부록 디지털 부록 1(https://links.lww.com/ACADMED/A625)은 온라인 CD 팀에서 사용할 수 있는 일반적인 용어에 대한 가이드를 제공합니다. Although faculty can independently incorporate online elements when developing blended curricula, one should generally seek to work with team members familiar with different aspects of online CD (Table 3). Faculty usually serve as subject matter experts (SMEs) in collaboration with instructional designers, project managers, and/or media technicians (e.g., videographers, graphic designers). Supplemental Digital Appendix 1, available athttps://links.lww.com/ACADMED/A625, provides a guide to common terminology that can be used by online CD teams.
리소스 생성 및 커리큘럼 설계에 소요되는 선행 시간은 상당한 경우가 많습니다. 중소기업에서 요구하는 시간은 계획된 커리큘럼의 복잡성과 다른 CD 팀원의 가용성, 경험 및 스킬에 따라 달라집니다.32 Delgaty는 강사 주도의 완전 온라인 커리큘럼을 개발한 경험을 바탕으로 커리큘럼 활동 1시간당 7시간의 교수 시간4을 제안합니다.33 커리큘럼 중 토론 게시판 진행과 같은 활동에는 많은 시간이 소요될 수 있으며 Delgaty4는 학생 활동 1시간당 4시간의 교수 시간이 필요하다고 추산합니다. 교수진이 정기적인 커리큘럼 주기에 참여할 수 없을 것 같으면 자기 주도형 커리큘럼을 선택하는 것이 현명한 선택일 수 있습니다. 이러한 커리큘럼은 생성 후 교수진의 지속적인 입력이 필요하지 않지만, 훨씬 더 많은 교수자의 사전 시간이 필요합니다. 프로젝트 관리자 없이 새로운 LMS에서 3시간짜리 자기 주도형 모듈 시리즈를 개발하기 위해 3명의 교수진으로 구성된 저희 팀은 각 커리큘럼 활동의 각 시간에 대해 25시간 이상 계획하고 피드백하는 데 투자했습니다. 중소기업과 개발 팀의 다른 사람들이 사용 가능한 시간을 파악하면 온라인 커리큘럼 옵션 중에서 적절한 선택을 하고 지속 가능성을 보장할 수 있습니다(표 1). Upfront time for resource creation and curricular design is often substantial. Time demanded from SMEs depends on the complexity of the planned curriculum and the availability, experience, and skills of other CD team members.32Delgaty proposes an estimate of 7 hours of faculty time for each 1 hour of curricular activity4based on her experience developing an instructor-led fully online curriculum.33Activities such as moderating discussion boards during the curriculum can be time-consuming; Delgaty4estimates that 4 hours of faculty time per hour of student activity was necessary. If faculty are unlikely to be available for regular cycles of the curriculum, self-paced curricula may be a prudent choice. Such curricula require no ongoing faculty input after creation, but require much more upfront faculty time. To develop a 3-hour series of self-paced modules in a new LMS without a project manager, our team of 3 faculty each devoted more than 25 hours of planning and feedback for each hour of curricular activity. Having a sense of the time available to SMEs and others on the development team allows one to make appropriate selections among online curricular options and ensure sustainability (Table 1).
온라인 커리큘럼의 개방적인 특성으로 인해 기밀 유지 및 접근성에 관한 규정에 주의를 기울여야 합니다. 미국 의학교육의 예로는 다음 등이 있습니다.
개인 건강 정보를 보호해야 하는 의료보험 이동성 및 책임에 관한 법률(HIPAA),
학생 정보를 기밀로 유지해야 하는 가족교육권 및 개인정보 보호법(FERPA),
장애인(청각 또는 시각 장애를 포함하되 이에 국한되지 않음)이 교육 과정에 접근할 수 있도록 요구하는 미국 장애인법(ADA)
대부분의 교육기관 LMS는 이미 기밀 유지 요구 사항을 충족하고 있으므로, CD 팀은 일반적으로 비디오 콘텐츠에 캡션을 추가하고 '대체 태그'(시각 장애인을 위해 이미지 대신 표시되는 문구)를 제공함으로써 접근성 요구 사항에 집중할 수 있습니다. The open nature of online curricula requires attention to regulations governing confidentiality and accessibility. U.S. medical education examples include
the Health Insurance Portability and Accountability Act (HIPAA), which requires that personal health information be protected;
the Family Educational Rights and Privacy Act (FERPA), which requires that student information be kept confidential; and
the Americans with Disabilities Act (ADA), which requires that individuals with disabilities (including, but not limited to, hearing or vision impairment) have access to the curriculum.
Because most institutional LMSs already ensure that confidentiality requirements are met, the CD team can usually focus on accessibility requirements by captioning video content and providing “alt tags” (wording that appears in place of images for the visually impaired).
온라인 커리큘럼 예산은 상당히 다양하며(표 1) 개발, 구현 및 유지 관리 비용을 포함해야 합니다. 일부 교수진은 사용 가능한 리소스에 맞게 목표와 목적을 축소하는 반면, 다른 교수진은 1단계와 2단계에서 파악한 문제와 요구 사항의 강도에 따라 추가 리소스를 성공적으로 확보할 수 있습니다. Online curricular budgets range considerably (Table 1) and should include the cost of development, implementation, and maintenance. Some faculty scale back goals and objectives to fit available resources, while others may successfully garner additional resources based on the strength of the problem identification and needs demonstrated during Steps 1 and 2.
온라인 커리큘럼은 무료 개방형 접근 방식, 유료 접근 방식, 하이브리드 접근 방식(예: 누구나 접근할 수 있지만 교육 학점을 받으려면 비용을 지불해야 함) 중 하나를 채택할 수 있습니다. 온라인 커리큘럼은 가장 많이 사용되는 CME 활동 유형으로, 2016년에 13억 달러의 등록비가 발생했습니다.34 MOOC는 보통 자격증에 25달러에서 50달러를 청구하며, 인기 있는 MOOC는 직접 수익으로 상당한 수익을 창출할 수 있습니다. 독립적으로 수익성이 없는 온라인 커리큘럼은 보완적인 학업 프로그램 등록을 위한 광고로서 가치가 있을 수 있습니다. Online curricula can be free and open-access, require payment for access, or adopt a hybrid approach (e.g., anyone may access, but receiving educational credit requires payment). Online curricula are the most-used type of CME activity, which generated $1.3 billion in registration fees in 2016.34MOOCs often charge $25 to $50 for a certificate; popular MOOCs can generate significant returns as direct revenue. Online curricula that are not independently profitable may be valuable as advertising for enrollment in complementary academic programs.
수강료를 부과하면 커리큘럼 수정 및 유지 관리에 도움이 될 수 있지만 온라인 커리큘럼의 활용도와 영향력을 제한할 수 있습니다. 수강료를 부과할 계획이라면 추가 요소를 고려해야 합니다:
온라인 커리큘럼을 결제 포털과 어떻게 통합할 것인가?
개인 또는 교육기관이 수수료를 지불할 것인가?
개별 커리큘럼 구성 요소를 기준으로 수수료를 부과할 것인가, 아니면 시간 제한을 기준으로 부과할 것인가?
커리큘럼 교수진, 해당 부서 또는 학과, 교육기관 간에 수익이 어떻게 배분됩니까?
Charging fees can support curriculum revision and maintenance, but may limit the uptake and impact of an online curriculum. If planning to charge fees, one must consider additional factors:
How will the online curriculum integrate with a payment portal?
Will fees be paid by individuals or institutions?
Will fees be based on individual curricular components or on a time-limited basis?
How will revenue be distributed among curriculum faculty, their divisions or departments, and the institution?
커리큘럼을 광범위하게 배포하려는 교수진은 브랜딩 문제(조직의 이름 또는 로고 사용에 관한 정책)도 고려해야 하며, 지적 재산권 소유권도 고려해야 할 수 있습니다. 또한 커리큘럼 개발자는 커리큘럼의 일부가 통제 범위를 벗어나 원치 않는 사용, 변경 또는 배포되지 않도록 보호하고자 할 수 있으며, 우려되는 경우 법률 자문을 구해야 합니다. Faculty seeking to disseminate curricula broadly must also consider issues of branding—the policies governing use of an organization’s name or logo—and may need to consider intellectual property ownership. Curriculum developers may also wish to protect parts of their curricula from undesired use, alteration, or dissemination beyond their control and, where concerns exist, should seek legal advice.
6단계: 평가 및 피드백 Step 6: Evaluation and Feedback
일반 원칙 General principles
6단계에서는 커리큘럼이 성공적인지, 어떻게 개선할 수 있는지 평가합니다. 여기에는 다음의 10가지 작업이 포함됩니다.
평가 사용자 식별,
사용자 요구 사항 명시,
평가 질문의 우선순위 지정,
평가 설계(예: 사후 시험만, 사전/사후 시험, 비교 그룹) 선택,
평가 방법 선택,
도구 구성,
윤리적 문제(예: 기밀성) 해결,
데이터 수집,
데이터 분석,
결과 보고 등
6단계에는 개별 참가자에 대한 평가와 프로그램의 구조, 프로세스 및 결과에 대한 평가가 포함됩니다. 정성적 및 정량적 데이터는 형성적 및 종합적 목적으로 수집되어야 합니다. 평가 방법론은 실현 가능하고 교육 목표와 일치해야 합니다. Step 6 evaluates whether the curriculum was successful and how it can be improved. It includes 10 tasks:
Step 6 includes assessment of individual participants and evaluation of the program’s structures, processes, and outcomes. Qualitative and quantitative data should be collected for formative and summative purposes. Evaluation methodology must be feasible and congruent with educational objectives.
특별 고려 사항 Special considerations
혼합형 커리큘럼은 대면 세션을 포함하므로 기존 커리큘럼과 동일한 평가 옵션을 제공합니다.
완전 온라인 커리큘럼에서도 교수자는 LMS를 통해 업로드된 문서 및 멀티미디어 파일을 검토하고 온라인 토론에 대한 참여를 추적할 수 있습니다.
자기 주도형 모듈과 MOOC는 일반적으로 자동 채점이 필요하므로 평가 옵션이 가장 적습니다.
MOOC는 동료 채점도 제공하지만, 이는 타당성을 보장하고 학습자의 참여를 높이기 위해 신중하게 설계되어야 하며, 비슷한 배경을 가진 등록자를 짝지어 동료 평가의 품질을 교수자의 평가와 비교하여 보정하고 가중치를 부여하는 것이 유용할 수 있습니다.35
Blended curricula offer the same assessment options as traditional curricula because they include face-to-face sessions.
Even in fully online curricula, instructors can review uploaded documents and multimedia files through an LMS and track participation in online discussions.
Self-paced modules and MOOCs have the fewest assessment options as both typically require automated grading.
MOOCs also offer peer grading, although this must be thoughtfully designed to ensure validity and enhance learner engagement; pairing enrollees of similar backgrounds and calibrating and weighting the quality of peer assessments against the instructor’s may be beneficial.35
온라인 형성 평가의 경우 모바일 장치를 사용하면 언제 어디서나 평가를 수행할 수 있습니다. 학습 대시보드는 학습자에게 자신의 응답이 다른 사람과 어떻게 비교되는지 실시간으로 보여줄 수 있습니다. 게임화 기능은 학습자의 노력과 집중력을 높여 학습 효과를 높일 수 있습니다.36,37 온라인 총괄 평가의 경우 시험 보안 및 무결성을 위한 안전장치가 필요한 경우가 많습니다. For online formative assessments, mobile devices can allow assessments to occur at any time and in any location. Learning dashboards can show learners how their responses compare to others in real time. Gamification features can help learners increase effort and focus to enhance learning.36,37For online summative assessments, safeguards for exam security and integrity are often necessary.
온라인 커리큘럼의 평가에는 일반적으로 다음이 포함되어야 합니다.38
사용성, 재사용 가능성, 지속 가능성, 학습자 경험, 테크놀로지에 대한 만족도 등 비전통적 요소를 평가
프로세스/구현에 대한 보다 강력한 평가
온라인 커리큘럼은 또한 신속한 평가 및 조정을 위해 두 가지 대안을 비교하는 "A/B 테스트"를 수행할 수 있는 기회를 제공합니다. 학습자가 커리큘럼에 참여하는 동안 데이터를 전자적으로 수집해야 하는 경우가 많기 때문에 비교 그룹(식별 및 접근이 어려울 수 있음)을 사용하거나 종단적 추적 관찰이 필요한 평가(학습자가 분산되어 있어 응답률이 낮을 수 있음)와 같은 특정 평가 설계가 어려울 수 있습니다. Evaluation of online curricula should generally include
a more robust evaluation of process/implementation,
assessing nontraditional factors such as usability, reusability, sustainability, learner experience, and satisfaction with the technology.38
Online curricula also offer the opportunity to conduct “A/B testing,” where two alternatives are compared with rapid evaluation and adjustment. Because data often must be collected electronically during learners’ participation in the curriculum, certain evaluation designs might be challenging, such as those using a comparison group (which might be difficult to identify and access) or those requiring longitudinal follow-up (where response rates might be low because learners are dispersed).
온라인 커리큘럼 평가 및 평가는 교육과 학습의 과학을 발전시킬 수 있는 새로운 기회를 제공합니다. 예를 들어, 대부분의 플랫폼은 학습자의 위치 및 커리큘럼 참여 시간과 같은 변수를 자동으로 추적합니다. 비교적 새로운 분야인 학습 분석은 온라인 학습 데이터를 사용하여 예측 모델을 만들고 학습자를 실시간으로 안내합니다. 많은 학습자의 평가를 자동으로 대조하여 코호트 전체와 시간 경과에 따른 성과를 추적할 수 있습니다. 위치 및 시간 정보와 빈번하고 반복적인 평가를 결합하여 생성된 "빅 데이터"39를 활용하면 학습이 발생하는 방식을 더욱 세분화할 수 있습니다.40,41 Online curricular assessments and evaluations provide new opportunities to advance the science of teaching and learning. For example, most platforms automatically track variables such as the locations of learners and time spent engaging in the curriculum. The relatively new field of learning analytics uses data from online learning to create predictive models and guide learners in real time. Assessments can be automatically collated for large numbers of learners to track performance across cohorts and over time. Harnessing the “big data”39generated by combining location and time information with frequent and repeated assessments has the potential to provide greater granularity for how learning occurs.40,41
유지 관리 및 개선 Maintenance and Enhancement
일반 원칙 General principles
완벽한 커리큘럼은 없습니다. 교육과정을 완전히 시행한 후에는 6단계의 모든 요소를 재검토하여 필요한 리소스와 지원이 확보되어 있는지 확인하고 교육과정을 지속적으로 갱신해야 합니다. 커리큘럼 콘텐츠와 디자인은 최신 상태로 유지되어야 하며 중요한 의료 요구사항에 맞춰 조정되어야 합니다. 리소스 제약을 고려하여 개정의 우선순위를 정하고 관리하는 프로세스를 수립해야 합니다. No curriculum is perfect. After full curriculum implementation, all elements of the Six Steps should be revisited to ensure that necessary resources and support remain secure and that the curriculum undergoes continuous renewal. Curricular content and design should remain up-to-date and aligned with important health care needs. One needs to establish processes for prioritizing and managing revisions, given resource constraints.
특별 고려 사항 Special considerations
온라인 커리큘럼에서는 커리큘럼 팀에 대한 재정적 지원을 유지하는 것 외에도 연간 LMS 사용료를 지불하고 지속적인 테크놀로지 지원을 위한 자금을 마련해야 하는 경우가 많습니다. In online curricula, in addition to maintaining financial support for the curricular team, it is often necessary to pay annual LMS fees and fund ongoing technical support.
많은 온라인 커리큘럼이 전통적인 학사 일정을 따르지 않으므로 커리큘럼 콘텐츠 및 방법의 수정은 시기, 콘텐츠 유형, 학습자의 기대치, 온라인 CD 팀의 가용성 및 예산에 따라 달라집니다. 콘텐츠와 교육 방법을 최신 상태로 유지하는 것은 이러한 변화를 구현하는 데 필요한 리소스와 균형을 이루어야 합니다. Because many online curricula do not conform to a traditional academic calendar, the revision of curricular content and methods will depend on timing, type of content, learner expectations, availability of the online CD team, and budget. Keeping content and educational methods on the cutting edge must be balanced with the resources required to implement such changes.
학술활동으로서의 온라인 커리큘럼 Online Curricula as Scholarship
일반 원칙 General principles
일부 교육기관에서는 학술활동에 대한 정의의 변화를 인정하고 있지만,39,42,43 대부분의 교육기관은 6단계(각 단계마다 학술활동 기회를 제공)를 진행함으로써 충족할 수 있는 Glassick의44 잘 알려진 기준을 지지합니다.45
1단계와 2단계에서는 적절한 준비와 명확한 목표를,
3단계에서는 이러한 목표를 명확히 하고 적절한 방법을(4단계와 5단계),
6단계에서는 중요한 결과와 반성적인 비평을 도출합니다.
대부분의 전통적인 커리큘럼이 진정한 학술활동이 되기에는 부족한 부분은 효과적인 프레젠테이션의 영역이며, 이 영역에서는 동료 검토를 위한 배포와 가용성이 필요합니다. Although some institutions have recognized changing definitions of scholarship,39,42,43most endorse Glassick’s44well-accepted criteria, which can be satisfied by proceeding through the Six Steps (with each step offering opportunities for scholarship).45
Steps 1 and 2 ensure adequate preparation and clear goals,
Step 3 articulates those goals and leads to appropriate methods (Steps 4 and 5), and
Step 6 yields significant results and reflective critique.
Where most traditional curricula fall short of becoming true scholarship is in the realm of effective presentation, which requires dissemination and availability for peer review.
특별 고려사항 Special considerations
전파는 실제 커리큘럼이 소속 교육기관을 넘어 확산되거나 커리큘럼 관련 작업의 발표 또는 출판을 통해 발생할 수 있습니다.4 MedEdPORTAL과 같은 일부 커리큘럼 저장소에서는 자료를 온라인에 게시하기 전에 동료 검토를 요구합니다. MOOC 또는 자기 주도형 모듈과 같은 온라인 커리큘럼은 많은 청중에게 제공되므로 정의상 "배포"된 것으로 간주되며, 이러한 커리큘럼에 대한 동료 검토는 평가를 통해 이루어질 수 있습니다. 온라인 커리큘럼의 평가를 공유하면 대상 그룹의 지식 또는 스킬에 대한 지역, 국가 또는 국제적인 정보를 제공할 수도 있습니다.46,47 Dissemination can occur by the spread of the actual curriculum beyond one’s home institution or by presentation or publication of curriculum-related work.4Some curriculum repositories, such as MedEdPORTAL, require peer review before materials are placed online. Online curricula such as MOOCs or self-paced modules are by definition “disseminated” as they are made available to large audiences; peer review of these curricula can occur through their evaluations. Sharing evaluations from online curricula can also provide regional, national, or international information on the knowledge or skills of targeted groups.46,47
혼합형 및 교수자 주도형 커리큘럼에는 이미지, 사례 연구, 도표 또는 다른 환경에서 공유하고 재사용할 수 있는 평가와 같은 구성 요소인 재사용 가능한 학습 객체(RLO)가 포함되어 있는 경우가 많습니다. 엄격한 개발 및 평가를 거친 RLO는 학술활동으로 인정받을 수 있습니다. Blended and instructor-led curricula often contain reusable learning objects (RLOs)—components such as images, case studies, diagrams, or assessments that can be shared and reused for other settings. RLOs that have undergone rigorous development and evaluation can qualify as scholarship.
보건 전문직 교수진도 온라인 학습과 관련된 교육 학술활동에 참여할 수 있는 기회를 모색할 수 있습니다. 체계적인 CD 프로세스를 적용하여 생성된 정보는 학습을 표준화 및 개별화하는 방법에 대한 이해를 발전시킵니다. 커리큘럼과 커리큘럼 구성 요소를 공유하면 노력의 중복을 줄이고, 각 작업의 영향을 받는 학습자의 수를 확대하며, 전문성 향상을 촉진할 수 있습니다. Health professions faculty can also pursue opportunities to engage in educational scholarship around online learning. Information generated from applying a methodical CD process advances our understanding of how to both standardize and individualize learning. Sharing curricula and curricular components will reduce duplication of effort, expand the number of learners influenced by each work, and promote professional advancement.
결론적 관찰 Concluding Observations
의료 교육에 대한 온라인 접근 방식은 중복되는 CD 노력을 줄이고, 커리큘럼의 질을 높이며, 많은 학습자의 성취도를 문서화할 수 있습니다. 이러한 접근 방식은 정도의 차이는 있지만 비동기적이고 자기 주도적일 수 있으며, 학습자와 교육자에게 더 개인화되고 시간 효율적일 수 있습니다. 비교적 많은 초기 리소스 투자가 필요할 수 있지만, 교육 및 평가의 이점, 지리적 및 제도적 경계를 넘어서는 도달 범위, 의료 결과에 영향을 미칠 수 있는 잠재력을 고려하면 이러한 노력을 정당화할 수 있습니다. 6단계 접근법을 온라인 CD의 특수한 요소에 대한 이해와 함께 적용하면 보다 효과적이고 학술적인 교육 프로그램 개발로 이어질 수 있습니다. Online approaches to health care education can reduce duplicative CD efforts, increase the quality of curricula, and document achievement by a large number of learners. They can be, to varying degrees, asynchronous and self-paced, and potentially more personalized and time-efficient for learners and educators. Although they may require a relatively large upfront investment of resources, their instructional and assessment advantages, their reach across geographical and institutional boundaries, and their potential to affect health care outcomes can justify the effort. Applying the Six-Step Approach with an understanding of factors particular to online CD can lead to more effective and scholarly educational program development.
1B.Y. Chen is director, Faculty Development Programs in Curriculum Development, Johns Hopkins University School of Medicine, and assistant professor, Division of General Internal Medicine, Johns Hopkins Bayview Medical Center, Baltimore, Maryland; ORCID: http://orcid.org/0000-0002-9905-6180. D.E. Kern is emeritus professor of medicine, past director, Faculty Development Programs in Curriculum Development, Johns Hopkins University School of Medicine, and past director, Division of General Internal Medicine, Johns Hopkins Bayview Medical Center, Baltimore, Maryland; ORCID: http://orcid.org/0000-0002-9327-6190. R.M. Kearns is director, Online Education, Johns Hopkins University School of Medicine, Baltimore, Maryland. P.A. Thomas is professor of medicine and vice dean for medical education, Case Western Reserve University School of Medicine, Cleveland, Ohio. M.T. Hughes is assistant professor of medicine, Division of General Internal Medicine, and coeditor, Johns Hopkins Internal Medicine Ambulatory Care Curriculum on PEAC: Physician Education and Assessment Center, Johns Hopkins School of Medicine, Baltimore, Maryland. S. Tackett is assistant professor of medicine and international medical education director, Division of General Internal Medicine, Johns Hopkins Bayview Medical Center, Baltimore, Maryland; ORCID: http://orcid.org/0000-0001-5369-7225.
Online curricula can make high-quality health professions education accessible in virtually any setting. They can enhance teaching and learning by both standardizing curricular resources and individualizing curricular experiences. Despite growing demand for and institutional interest in online curricula for medical education, many medical educators lack a framework for online curriculum development. Without rigorous and thoughtful development, online curricula can waste opportunity and resources by leading to education that is inferior to traditional methods. In this article, the authors describe a systematic approach to online curriculum development based on the Six-Step Approach for Curriculum Development for Medical Education, a widely used method that has led to successful implementation of a variety of traditional and online curricula. In each step, special considerations for curricula with larger and more diverse learner audiences-characteristic of many online curricula-are highlighted. Four common online curricular formats are also discussed: blended curricula, instructor-led fully online curricula, self-paced modules, and massive open online courses (MOOCs). The authors emphasize factors that differentiate one online format from another, including the budgetary, technical, and human resource requirements for each. The article concludes by urging medical educators to pursue opportunities to study and disseminate online curricular work.
미국 의과대학생의 장애, 프로그램 접근성, 공감, 번아웃: 전국단위 연구(Med Educ, 2022) Disability, program access, empathy and burnout in US medical students: A national study Lisa M. Meeks1 | Karina Pereira-Lima2 | Melissa Plegue3 | Neera R. Jain4 | Erene Stergiopoulos5 | Catherine Stauffer6 | Zoie Sheets7 | Bonnelin K. Swenor8 | Nichole Taylor9 | Amy N. Addams10 | Christopher J. Moreland11
1 서론 1 INTRODUCTION
의학교육에서 장애에 대한 이해를 높여야 할 필요성은 전 세계 장애인이 겪는 의료 격차에 대한 글로벌 보건 데이터1와 여러 국가의 의사들이 장애 환자에게 양질의 진료를 제공할 수 있는 능력에 대해 우려를 표명하는 연구 결과를 통해 입증되었습니다.2-5 이러한 필요를 해결하는 한 가지 메커니즘은 장애에 대한 일반적인 고정관념을 줄이면서 의학을 더 잘 알릴 수 있는 장애 의대생을 포용하고 지원하는 것입니다.6, 7 실제로 점점 더 많은 연구가 다양한 의료 인력이 모든 의사, 수련의, 환자에게 혜택을 줄 수 있다고 제안합니다.8-10 그러나 의학교육에서 장애 수련의가 직면하는 잠재적 기여와 과제에 대한 연구는 아직 부족합니다.11 The need for a greater understanding of disability in medical education is evidenced by global health data on health care disparities encountered by people with disabilities worldwide1and by research showing that physicians from different countries report concerns about their ability to provide quality care for disabled patients.2-5One mechanism of addressing this need is through the inclusion and support of medical students with disabilities, who may better inform medicine while reducing prevailing stereotypes of disability.6,7Indeed, a growing body of research suggests that a more diverse medical workforce can benefit all physicians, trainees and patients.8-10However, research on potential contributions and challenges faced by disabled trainees in medical education is still scarce.11
장애 환자는 학대,1,12,13 차별14-19 및 의사소통의 어려움17,20-24을 경험하는 비율이 높으며, 이는 장애 환자가 직면한 건강 불평등의 잠재적 원인으로 의료진의 공감 능력 저하를 지적합니다. 반대로, 일화 보고와 질적 연구에 따르면 장애를 가진 의사와 의대생이 의료계에 기여하는 가치 있는 기여 중 하나는 환자 치료에 접근하는 고도의 공감 능력입니다.25-30 실제로 선행 연구에 따르면 장애를 가진 환자와 그렇지 않은 환자 모두 장애를 가진 의사가 더 공감 능력이 뛰어나다고 생각하는 것으로 나타났습니다.31, 32 Patients with disabilities encounter high rates of mistreatment,1,12,13discrimination14-19and communication difficulties17,20-24that point to diminished provider empathy as a potential contributor to health inequities faced by this population. Conversely, anecdotal reports and qualitative research suggest that one of the valuable contributions that physicians and medical students with disabilities bring to the medical workforce is the highly empathic way they approach patient care.25-30Indeed, prior studies have found that patients with and without disabilities report believing that disabled physicians are more empathic.31,32
문헌에는 의사의 공감에 대한 다양한 정의가 있지만, 주로 환자의 관점을 이해하고 존중하는 인지적 역량으로 정의되는 경우가 많습니다.33-36 의사의 공감은 다른 문화권의 환자들에게 높은 평가를 받고 있으며37 환자의 불안 감소, 환자 만족도 및 치료 순응도 증가, 더 나은 환자 결과와 관련이 있습니다33, 35, 38 그러나 공감은 의과대학 과정에서 감소할 수 있으며39-41 번아웃 수준은 증가하는 것으로 나타납니다.42 공감은 환자 치료를 개선하는 것으로 알려져 있지만, 소진은 전문성 저하,43 환자 만족도 감소44, 45 및 의료 오류 증가와 관련이 있습니다.46, 47 또한 선행 연구에 따르면 공감과 소진은 서로 연결되어 있으며, 의대생의 높은 소진 수준은 낮은 공감 점수와 관련이 있습니다.48, 49 While the literature contains multiple definitions of physician empathy, it is most often defined as a predominately cognitive competency of understanding and respecting the patient perspective.33-36Physician empathy is highly valued by patients from different cultures37and has been associated with decreased patient anxiety, increased patient satisfaction and adherence to treatment, and better patient outcomes33,35,38However, empathy may decline over the course of medical school,39-41whereas levels of burnout appear to increase.42While empathy is known to improve patient care, burnout is associated with lower professionalism,43diminished patient satisfaction44,45and increased medical errors.46,47In addition, prior studies suggest that empathy and burnout are connected, with higher levels of burnout associated with lower empathy scores in medical students.48,49
스스로 장애가 있다고 식별한 경우, 수련 중 상당한 구조적 장벽26, 29, 50, 51이 소진을 증가시키고, 이는 다시 공감 능력 저하로 이어질 수 있습니다. 실제로 선행 연구에 따르면 장애를 가진 학생들은 의과대학에서 더 높은 수준의 고통을 경험하며52, 장애를 경험한 의사가 의학교육에 더 많이 참여해야 한다는 전 세계적인 지지에도 불구하고 장애 수련의들은 의학교육에 동등하게 접근하지 못하고 있습니다.1, 26, 53, 54 의과대학 중퇴에 대한 생각과의 연관성을 고려할 때,55 장애 의대생들의 소진은 이들을 더 높은 이탈 위험에 처하게 하여 의학 분야에서 중요하지만 대표되지 않는 이 그룹의 대표성을 떨어뜨릴 수 있습니다. 마찬가지로, 소진과 공감 사이의 반비례 관계로 인해,48,49 장애 의대생이 보여준 높은 가치의 공감 능력이 이 집단의 소진 수준 증가로 인해 위협을 받을 수 있습니다. 현재까지 장애 의대생의 번아웃 및 공감 능력 약화와 관련된 잠재적 요인을 조사한 연구는 없습니다. 효과적이고 합리적인 편의시설에 대한 접근성 부족이 그러한 요인 중 하나입니다. For those who self-identify with a disability, substantial structural barriers during training26,29,50,51may contribute to increased burnout, which may, in turn, lead to decreased empathy. Indeed, prior research suggests that students with disabilities experience higher levels of distress during medical school52and that disabled trainees are denied equal access to medical education despite global endorsements about the benefits of a larger representation of physicians with lived experience of disability.1,26,53,54Given its associations with thoughts of dropping out of medical school,55burnout among medical students with disabilities may place them at higher risk for attrition, reducing the representation of this valuable and underrepresented group in medicine. Similarly, due to the inverse associations between burnout and empathy,48,49it is possible that the highly valued empathy demonstrated by disabled medical students could be threatened by increased levels of burnout in this population. To our knowledge, no studies have investigated potential factors associated with the development of burnout and erosion of empathy among medical students with disabilities. Lack of access to effective reasonable accommodations presents one such factor.
장애가 있는 학습자의 경우, 프로그램 접근성(접근성 요구가 이미 충족된 환경으로 인해 편의를 제공받거나 편의가 필요하지 않은 경우로 정의)은 웰빙 및 성과 결과 개선과 긍정적인 관련이 있는 것으로 나타났습니다. 특히, 1년차 레지던트를 대상으로 한 연구에 따르면
[장애를 스스로 보고하고 프로그램 접근성이 부족한 레지던트]는 장애가 없는 동료보다 인턴 기간 동안 우울 증상이 나타날 위험이 더 높았으며, 장애가 없는 레지던트와 프로그램 접근성이 있는 장애인 레지던트 모두보다 의료 과실을 스스로 보고할 가능성이 더 높은 것으로 나타났습니다.
반대로 [장애와 프로그램 접근성을 스스로 보고한 레지던트]는 우울 증상이나 의료 오류 보고의 증가 측면에서 장애를 스스로 보고하지 않은 레지던트와 차이가 없었습니다.56
의료 전문가 학생과 수련의를 대상으로 한 또 다른 연구에서는 편의 제공에 대한 만족도가 높을수록 우울증 위험에 대해 양성 판정을 받을 가능성이 낮아지고, 일부의 경우 취업 가능성이 높아지는 것과 관련이 있었습니다.57 필요한 합리적인 편의에 대한 접근성 부족은 장애 의대생의 표준화된 시험 점수 저하 및 학생 진급 지연과도 관련이 있습니다.58, 59 For learners with disability, program access, defined as access to accommodations or not needing accommodations due to an environment where access needs are already met,56has been positively associated with improved well-being and performance outcomes. Specifically, a study of first-year medical residents demonstrated that
residents with self-reported disability and lack of program access were at a higher risk for developing depressive symptoms during internship than their peers without disabilities and were more likely to self-report medical errors than both residents without disabilities and disabled residents with program access.
Conversely, residents who self-reported disability and program access did not differ from residents without self-reported disabilities in terms of increase in depressive symptoms or reports of medical errors.56
In another study of health care professional students and trainees, higher satisfaction with accommodations was associated with lower likelihood of screening positive for the risk of depression and, for a subset, increased likelihood of obtaining employment.57Lack of access to needed reasonable accommodations has also been associated with lower scores in standardised exams and delayed student progression among medical students with disabilities.58,59
장애를 가진 의사는 건강 형평성 증진을 위한 다각적인 접근 방식에서 중요한 부분을 차지할 수 있지만, 장애를 가진 의대생의 공감 능력과 소진 정도를 조사하는 연구는 부족합니다. 이 데이터를 체계적으로 평가하면 장애 학생의 경험을 보다 미묘하게 이해하고 추가 지원의 잠재적 필요성을 발견할 수 있습니다. 또한 프로그램 접근성이 장애 수련의의 복지 및 성과와 밀접하게 연관되어 있다는 이전의 증거와56-59 국제 권고안에서 장애 접근성을 강조하는 점을 고려할 때,1, 26, 53, 54 [프로그램 접근성, 소진, 공감, 자가 보고 장애 사이의 연관성에 대한 연구]는 다양하고 소중한 인구의 복지와 성과를 더 잘 지원하기 위한 가능한 개입 대상을 식별할 수 있는 잠재력을 가지고 있습니다. While physicians with disabilities may be a critical part of a multifaceted approach to advancing health equity, there is a dearth of research that examines empathy and burnout measures for medical students with disabilities. Systematically assessing this data will allow for a more nuanced understanding of the experiences of students with disabilities and uncover the potential need for additional support. In addition, given prior evidence that program access is closely linked with the wellbeing and performance of disabled trainees,56-59and the emphasis on disability access across international recommendations,1,26,53,54research on the associations between program access, burnout, empathy and self-reported disabilities has the potential to identify possible targets of intervention to better support the well-being and performance of this diverse and valued population.
이 연구는 [장애를 스스로 밝힌 의대생]과 [장애가 없는 의대생]의 소진 및 공감 지표를 비교하고, 미국 의대생의 두 국가 코호트에서 스스로 밝힌 장애와 보고된 프로그램 접근성 부족이 공감 및 소진 측정과 관련이 있는지 조사하여 장애 의대생의 웰빙과 공감에 관한 문헌의 격차를 해소하는 것을 목표로 했습니다. This study aimed to characterise indicators of burnout and empathy among medical students with self-disclosed disabilities, compared with those without disabilities, and to investigate whether self-disclosed disability and reported lack of program access are associated with measures of empathy and burnout in two national cohorts of US medical students, addressing the gap in literature about the well-being and empathy among medical students with disabilities.
2 연구 방법 2 METHODS
2.1 연구 환경 및 참여자 2.1 Study setting and participants
우리는 미국 의과대학협회(AAMC)의 2학년 설문조사(Y2Q)에 응답한 의과대학 2학년 학생 두 코호트(2019년과 2020년)로부터 비식별화된 데이터를 확보했습니다. Y2Q는 미국 동종요법 의과대학에 재학 중인 모든 2학년 의대생을 대상으로 매년 실시하는 익명의 온라인 설문조사입니다. 전체 데이터 세트에는 2개 연도 코호트의 의대생 27,009명(2019년 코호트의 경우 151개 의대 13,967명, 2020년 코호트의 경우 153개 의대 13,042명, 2019년[21,917명] 및 2020년[22,138명] 적격 의대생 수 기준 전체 응답률 61.3%)이 포함되었습니다. 이 중 2만 3,898명(88.5%)이 '귀하는 장애(예: ADHD, 학습, 심리, 만성 건강, 이동, 청각, 시각 등)가 있습니까'라는 질문에 예 또는 아니오로 응답하여 분석에 포함되었습니다(496명[1.8%]은 '모름'이라고 응답하여 제외됨). 최종 표본은 2019년과 2020년 미국 의대 2학년 학생의 54.2%를 차지합니다. 수집된 데이터에는 인구통계학적 특성(성별, 연령대, 성적 지향, 인종/민족, 코호트 연도 등), 장애 관련 질문과 함께 개인 관련 변수, 학습 환경, 소진 및 공감에 대한 측정이 포함되었습니다. 모든 데이터는 의대생이나 의과대학에 대한 식별 정보 없이 인구 수준에서 수집되었기 때문에 이 연구는 콜로라도대학교 의과대학 기관윤리심의위원회에서 면제된 것으로 간주되었으며, 역학 관찰 연구 보고 강화(STROBE) 보고 가이드라인을 따랐습니다. We obtained de-identified data from two cohorts (2019 and 2020) of second-year medical students who replied to the Association of American Medical Colleges (AAMC) Year 2 Questionnaires (Y2Q). The Y2Q is an anonymous online survey that is administered annually to all second-year medical students actively enrolled in US-allopathic medical schools. The complete dataset included 27 009 medical students from two yearly cohorts (13 967 from 151 medical schools for the 2019 cohort and 13 042 from 153 medical schools for the 2020 cohort; overall response rate of 61.3% based on the number of eligible second-year medical students in 2019 [21 917] and 2020 [22 138]). Of those, 23 898 (88.5%) provided a yes or no response to the question ‘Are you a person with a disability (e.g., ADHD, learning, psychological, chronic health, mobility, hearing, vision, etc.)?’ and were included in the analyses (496 [1.8%] replied ‘I don't know’ and were excluded). The final sample represents 54.2% of second-year US medical students in 2019 and 2020. Obtained data included demographic characteristics (i.e. sex, age group, sexual orientation, race/ethnicity and cohort year), disability-related questions, along with measures of personal-related variables, learning environment, burnout and empathy. Given that all data were obtained on a population-level without any identifying information about medical students or their medical schools, the study was deemed exempt by the University of Colorado Medical School Institutional Review Board and followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
2.2 조치 2.2 Measures
2.2.1 장애 관련 질문 2.2.1 Disability-related questions
장애 상태 및 유형 Disability status and type
의대생의 장애 상태는 '장애(예: ADHD, 학습, 심리, 만성 건강, 이동성, 청각, 시각 등)가 있는 사람입니까?"라는 질문에 대한 응답을 통해 평가되었습니다. 장애 상태 질문에 대한 가능한 응답에는 '예', '아니오' 또는 '모르겠다'가 포함되었습니다. 장애 유형은 '다음 중 귀하의 장애를 가장 잘 설명하는 것은 무엇입니까?"라는 질문을 사용하여 결정되었습니다. 장애 유형이 두 가지 이상인 경우 해당되는 항목을 모두 선택하세요'. 이 질문에는 '주의력 결핍/과잉 행동 장애(ADHD)', '만성 건강 장애', '청각 장애 또는 난청', '학습 장애', '이동 장애', '심리적 장애', '시각 장애' 또는 '기타' 등의 응답이 가능했습니다. Medical students' disability status was assessed through their responses to the question ‘Are you a person with a disability (e.g., ADHD, learning, psychological, chronic health, mobility, hearing, vision, etc.)?’ Possible responses to the disability-status question included ‘yes’, ‘no’, or ‘I don't know’. Disability type was determined using the question ‘Which of the following best describes your disability? If you have more than one type, select all that apply’. Available responses to this question included ‘attention deficit/hyperactivity disorder (ADHD)’, ‘chronic health disability’, ‘deaf or hard of hearing’, ‘learning disability’, ‘mobility disability’, ‘psychological disability’, ‘visual disability’ or ‘other’.
프로그램 접근성 Program access
장애가 있는 학생에게 의과대학에서 장애에 대한 편의를 제공했는지 여부를 물었습니다(예/아니오). '아니오'라고 답한 응답자에게는 "다음 중 의과대학에서 편의를 제공하지 않았거나 제공하지 않은 이유를 가장 잘 설명하는 것은 무엇입니까?"라는 추가 질문이 주어졌습니다. 응답은 다음과 같습니다: '편의 요청이 거부됨', '편의 요청이 검토 중임', '편의가 필요하지 않다고 생각하여 편의 요청을 하지 않음', '기타 이유로 편의 요청을 하지 않음'. 이전 연구56, 60에 따라 프로그램 접근성을 코딩하여 편의를 제공받았거나 편의가 필요하지 않다고 응답한 학생을 포함했습니다. 그 외의 모든 응답은 프로그램 접근성 부족으로 코딩했습니다. Students with disabilities were asked whether their medical school provided accommodations for their disabilities (yes/no). Those who replied ‘no’ were further asked the question ‘Which of the following best describes why your medical school did not or has not provided accommodations?’ Responses included: ‘my request for accommodations was denied’, ‘my request for accommodations is under review’, ‘I have not requested accommodations because I feel I do not need accommodations’ and ‘I have not requested accommodations for other reasons’. In keeping with previous studies,56,60we coded program access to include students reporting receiving accommodations or not needing accommodations. All other responses were coded as lack of program access.
2.2.2 번아웃 2.2.2 Burnout
번아웃 증상은 의대생용 올덴버그 번아웃 인벤토리(OLBI-MS)61,62 를 사용하여 측정하였는데, 이는 Oldenburg 번아웃 인벤토리(OLBI)를 수정 및 단축한 버전입니다.61 OLBI-MS는 번아웃의 두 가지 차원인 탈진(8개 항목, 본 연구 표본에서 크론바흐 알파 = 0.8)과 이완(8개 항목, 본 연구 표본에서 크론바흐 알파 = 0.8)을 측정하는 16개 항목으로 구성됩니다. Demerouti와 Bakker에 따르면,61 소진은 '격렬한 신체적, 정서적, 인지적 긴장의 결과, 즉 특정 직무 요구에 장기간 노출된 장기적인 결과'로 정의되며, OLBI의 disengagement 항목은 개인과 업무의 관계, 특히 '업무와의 동일시 및 같은 직업을 계속할 의지와 관련하여'61 개인과 업무의 관계에 관한 것입니다.62 OLBI의 의대생 버전(OLBI-MS)에서는 모든 항목에서 '업무'라는 단어를 '학습'로 대체합니다. 각 하위 척도는 0-3점 척도로 측정되는 각 항목의 합산으로 계산됩니다. 점수가 높을수록 번아웃 수준이 높음을 나타냅니다. 전체 의대생 인구의 번아웃 수준이 높고,42 심리측정 특성이 우수함에도 불구하고 OLBI가 번아웃에 대한 임상적 컷오프를 제공하지 않는다는 점을 감안하여,63 Y2Q에 응시한 전체 의대생 표본에 대한 특정 하위 그룹 점수 범위에 임상적 의미를 부여하기 위해 사분위수를 사용했습니다. 따라서 의료 전문가64 및 의대생의 소진을 평가하기 위해 OLBI 및 OLBI-MS를 사용한 선행 연구의 절차에 따라,65 각 OLBI-MS 하위 척도에서 학생들의 점수는 75번째 백분위수 이상에서 높은 것으로 분류되었습니다(즉, 전체 Y2Q 표본에서 높은 탈진 14 이상, 높은 몰입도 12 이상 [N = 27 009]). Burnout symptoms were measured using the Oldenburg Burnout Inventory for Medical Students (OLBI-MS),61,62which is a modified and shortened version of the Oldenburg Burnout Inventory (OLBI).61The OLBI-MS consists of 16 items measuring two dimensions of burnout—exhaustion (8 items, Cronbach's alpha = 0.8 in the present study sample) and disengagement (8 items, Cronbach's alpha = 0.8 in the present study sample). According to Demerouti and Bakker,61exhaustion is defined as ‘a consequence of intense physical, affective and cognitive strain, i.e. as a long-term consequence of prolonged exposure to certain job demands’, and the disengagement items from the OLBI concern the relationship of individuals with their work, ‘particularly with respect to identification with work and willingness to continue in the same occupation’.61In the medical student version (OLBI-MS) of the OLBI, the word ‘work’ is substituted by ‘studies’ on every item.62Each subscale is calculated by summing across its items, which are measured on a 0–3 point scale. Higher scores indicate higher levels of burnout. Given the high levels of burnout among the overall population of medical students,42and that despite having good psychometric properties, the OLBI does not provide clinical cutoffs for burnout,63quartiles were used to provide clinical meaning to the ranges of specific subgroup scores relative to the total sample of medical students who took the Y2Q. Therefore, following the procedures of prior studies that used the OLBI and OLBI-MS to assess burnout among health professionals64and medical students,65students' scores in each OLBI-MS subscale were categorised as high at the 75th percentile and above (i.e. high exhaustion ≥ 14 and high disengagement ≥ 12 in the complete Y2Q sample [N = 27 009]).
2.2.3 공감 2.2.3 Empathy
공감은 대인관계 반응성 지수(IRI)의 관점 취하기 및 공감적 관심 하위 척도에서 파생된 8개 항목을 사용하여 측정했습니다.66, 67 IRI 점수는 0-4점 척도로 측정되는 8개 항목의 합산으로 계산됩니다. 가능한 점수 범위는 0~32점이며, 점수가 높을수록 공감 수준이 높음을 나타냅니다. 본 연구에서 IRI의 크론바흐 알파는 0.8이었습니다. 공감 능력의 저하가 환자 치료 결과의 저하와 관련이 있다는 점을 감안하여, 의대생 전체 인구와 비교하여 자가 보고 장애가 낮은 공감 능력과 관련이 있는지 평가하기 위해 전체 Y2Q 표본에서 25번째 백분위수 이하의 IRI 점수(IRI ≤ 22)를 낮은 공감 능력으로 분류했습니다. Empathy was measured using eight items derived from the perspective taking and empathic concern subscales of the Interpersonal Reactivity Index (IRI).66,67The IRI scores are calculated by summing across the 8 items, which are measured on a 0–4 point scale. The possible range of scores is 0–32, with higher scores indicating higher levels of empathy. The Cronbach's alpha for the IRI in the present study was 0.8. Given that reduced empathy is associated with poorer patient care outcomes, IRI scores at the 25th percentile or below in the complete Y2Q sample (IRI ≤ 22) were categorised as low empathy in order to assess whether self-reported disability is associated with a higher or lower risk of presenting low empathy in relation to the overall population of medical students.
2.2.4 개인 관련 조치 2.2.4 Personal-related measures
모호성에 대한 내성은 7항목으로 구성된 모호성에 대한 내성 척도(TFA)를 사용하여 측정했습니다.68 TFA는 불확실한 상황에 대처하는 개인의 능력을 측정하기 위해 고안되었으며 1~6점 척도로 측정되는 7가지 항목으로 구성되어 있습니다. TFA 점수는 7개 항목의 점수를 모두 합산하여 계산되며, 총점 범위는 7-42점입니다. TFA 점수가 높을수록 모호성에 대한 내성이 높다는 것을 의미합니다. 본 연구 샘플의 TFA에 대한 크론바흐 알파는 0.8이었습니다. Tolerance for ambiguity was measured using the 7-item Tolerance for Ambiguity Scale (TFA).68The TFA is designed to measure the individual's ability to cope with situations of uncertainty and includes seven items measured on a 1–6 point scale. TFA scores are calculated by summing scores across all seven items, with a possible total score range of 7–42. Higher scores on the TFA indicate higher tolerance for ambiguity. The Cronbach's alpha for TFA in the present study sample was 0.8.
현재 인식하는 삶의 질에 대한 결과를 통제하기 위해 전반적인 삶의 질, 정신적, 육체적, 정서적, 사회적, 영적 웰빙 등 삶의 6가지 측면에 대한 응답자의 인식을 측정하는 6항목 선형 아날로그 자기 평가 척도(LASA-6)를 포함시켰습니다. LASA-6 점수는 0~10점 척도로 평가되는 각 항목의 점수를 합산하여 계산됩니다(본 연구 표본의 경우 크론바흐 알파 = 0.9). 총 점수의 가능한 범위는 0-60점이며, 점수가 높을수록 삶의 질이 높다는 것을 나타냅니다. To control the results for current perceived quality of life, we included the 6-item Linear Analogue Self-Assessment Scale (LASA-6), which measures respondents' perceptions about the following six aspects of life: overall quality of life, mental, physical, emotional, social and spiritual well-being. LASA-6 scores are calculated by summing across its items, which are rated on a 0–10 point scale (Cronbach's alpha = 0.9 in the present study sample). The possible range of the total score is 0–60, with higher scores indicating higher perceived quality of life.
2.2.5 학습 환경 측정 2.2.5 Learning environment measures
학습 환경에 대한 학생들의 인식은 의과대학 학습 환경 설문조사(MSLES)를 통해 측정되었습니다.69 MSLES는 정서적 분위기(3개 항목), 교수 상호작용(4개 항목), 학생-학생 상호작용(4개 항목) 등 학습 환경의 세 가지 차원을 측정하는 11개 항목으로 구성되어 있습니다. 각 하위 척도는 0~5점 척도로 측정되는 개별 항목의 합산으로 계산됩니다. MSLES 하위 척도의 점수가 높을수록 학습 환경에 대해 더 긍정적으로 인식하고 있음을 나타냅니다. MSLES 하위 척도의 크론바흐 알파 값은 정서적 분위기에서 0.9, 교수진 상호작용에서 0.8, 학생-학생 상호작용에서 0.8이었습니다. Students' perceptions regarding their learning environment were measured through the Medical School Learning Environment Survey (MSLES).69The MSLES consists of 11 items measuring three dimensions of the learning environment: emotional climate (3 items), faculty interactions (4 items) and student–student interactions (4 items). Each subscale is calculated by summing across the individual items, which are measured on a 0–5 point scale. Higher scores on MSLES subscales indicate a more positive perception of the learning environment. Cronbach's alpha values for the MSLES subscales were 0.9 for emotional climate, 0.8 for faculty interactions and 0.8 for student–student interactions.
2.3 통계 분석 2.3 Statistical analyses
2.3.1 장애 상태, 공감 및 번아웃 간의 연관성 2.3.1 Associations between disability status, empathy and burnout
전체 샘플에 대한 기술 요약 통계를 계산하고 장애 상태(즉, 장애가 있는 학생과 없는 학생)에 따라 계층화했습니다. 장애 학생과 비장애 학생 간의 인구통계학적 특성의 차이는 카이제곱 테스트를 사용하여 평가했습니다. 성별, 성적 지향, 연령대, 인종/민족, 코호트 연도, TFA 점수, LASA-6 점수, MSLES 하위 척도 점수 등 인구통계학적, 개인 관련 및 학습 환경 공변수를 고려한 조정되지 않은 오즈비(OR)와 다변량 로지스틱 회귀 모델을 사용하여 장애 유무와 높은 소진, 높은 참여도 및 낮은 공감 지표 간의 연관성을 조사했습니다. 이전 연구에 따르면 높은 소진이 공감에 해롭다는 사실이 밝혀졌기 때문에,41, 48, 70, 71 낮은 공감에 대한 다변량 모델에는 높은 소진과 높은 참여도도 독립 공변량으로 포함되었습니다. 또한 장애 상태, 공감, 소진 사이의 관찰된 연관성에서 특정 장애 유형이 미치는 영향에 대한 통찰력을 얻기 위해 높은 소진, 높은 참여도, 낮은 공감의 다변량 모델에서 각 개별 장애 유형을 순차적으로 제외하여 민감도 분석을 수행했습니다. We calculated descriptive summary statistics for the overall sample and stratified by disability status (i.e. students with and without disabilities). Differences in demographic characteristics among students with and without disabilities were assessed using chi-squared tests. We examined for the associations between the presence of disabilities and indicators of high exhaustion, high disengagement and low empathy using unadjusted odds ratio (OR) and multivariable logistic regression models accounting for the following demographic, personal-related and learning environment covariates: sex, sexual orientation, age group, race/ethnicity, cohort year, TFA score, LASA-6 score and MSLES subscale scores. Because previous studies suggest that high burnout is detrimental to empathy,41,48,70,71multivariable models for low empathy also included high exhaustion and high disengagement as independent covariates. Additionally, to gain insight into the influence of specific types of disability in any observed associations between disability status, empathy and burnout, we performed sensitivity analyses by serially excluding each individual disability type from our multivariable models of high exhaustion, high disengagement, and low empathy.
2.3.2 프로그램 접근, 공감, 소진 사이의 연관성 분석 2.3.2 Associations between program access, empathy and burnout
의대생의 소진 및 공감 지표와 프로그램 접근성 간의 연관성을 확인하기 위해 2단계 2차 분석을 실시했습니다: 먼저, 조정되지 않은 OR을 사용하여 장애가 보고된 학생의 하위 집합 내에서 프로그램 접근성 부족과 높은 소진, 높은 참여도 및 낮은 공감 지표의 존재 사이의 연관성을 조사했습니다. 그 후, 인구통계학적, 개인 관련, 학습 환경 및 소진 측정을 고려하면서 높은 소진, 높은 참여도, 낮은 공감도 지표가 장애 상태 및 프로그램 접근과 관련이 있는지 여부를 조사하는 다변량 로지스틱 분석을 수행했습니다. 번아웃 측정치는 공감에 대한 다변량 모델에서 독립 공변량으로만 포함되었습니다. To identify possible associations of program access with indicators of burnout and empathy among medical students, we performed a two-step secondary analysis: First, we examined for associations between lack of program access with the presence of indicators of high exhaustion, high disengagement and low empathy within the subset of students with reported disabilities using unadjusted OR. Subsequently, we performed multivariable logistic analyses examining whether indicators of high exhaustion, high disengagement and low empathy associated with disability status and program access while accounting for demographic, personal-related, learning environment and burnout measures. Burnout measures were only included as independent covariates in multivariable models for empathy.
모든 통계 분석에서 양변량 p < .05는 통계적으로 유의미한 것으로 간주되었습니다. 모든 분석은 SPSS-21(IBM Corp)을 사용하여 수행되었습니다. A two-sided p < .05 was considered statistically significant for all statistical analyses. All analyses were conducted using SPSS–21 (IBM Corp).
3 결과 3 FINDINGS
본 연구에 포함된 2학년 의대생 2만 3,898명(2019년과 2020년 미국 의대생 2학년의 54.2%) 중 2438명(10.2%)이 장애가 있다고 스스로 밝혔습니다. 장애를 보고하지 않은 학생에 비해 장애가 있는 학생은 여성(χ2 = 8.1, df = 1, p = .004), 나이가 많거나(χ2 = 212.5, df = 1, p < . 0001), 레즈비언, 게이 또는 양성애자(χ2 = 353.9, p < .0001), 의학계에서 소외된 인종 및 민족 그룹(χ2 = 31.9, df = 1, p < .0001) 및 2020년 코호트(χ2 = 12.8, df = 1, p < .0001) 출신일 가능성이 높았습니다(표 1). Of the 23 898 second-year medical students included in the present study (54.2% of second-year US medical students in 2019 and 2020), 2438 (10.2%) self-identified as having a disability. Compared with students who did not report a disability, students with disabilities were more likely to be women (χ2 = 8.1, df = 1, p = .004), older (χ2 = 212.5, df = 1, p < .0001), lesbian, gay or bisexual (χ2 = 353.9, p < .0001), from racial and ethnical groups underrepresented in medicine (χ2 = 31.9, df = 1, p < .0001) and from the 2020 cohort (χ2 = 12.8, df = 1, p < .0001) (Table 1).
3.1 장애를 보고한 학생과 보고하지 않은 학생의 소진 및 공감 능력 3.1 Burnout and empathy among students with and without reported disabilities
장애를 보고한 학생은 장애가 없는 학생에 비해 높은 소진(1181명 [49.3%] 대 6433명 [30.6%], OR 2.21 [95% CI, 2.01-2.40])과 높은 이탈disengagement(979명 [40.7%] 대 6291명 [29.9%], OR 2.21 [95% CI, 2.01-2.40])를 보고할 가능성이 훨씬 더 높았습니다(장애가 없는 학생에 비해 장애를 보고한 학생의 소진 점수가 유의하게 높았음). 공감 점수의 경우, 장애가 없는 동료보다 장애가 있는 동료가 낮은 공감을 나타낼 가능성이 현저히 낮았습니다(608 [25.5%] 대 6531 [31.1%], OR 0.76, 95% CI [0.69-0.83]). Compared with students without disabilities, students who reported disabilities were significantly more likely to report high exhaustion (1181 [49.3%] vs. 6433 [30.6%], OR 2.21 [95% CI, 2.01–2.40]) and high disengagement (979 [40.7%] vs. 6291 [29.9%], OR 2.21 [95% CI, 2.01–2.40]). With respect to empathy scores, SWD were significantly less likely to present low empathy than their colleagues without disabilities (608 [25.5%] vs. 6531 [31.1%], OR 0.76, 95% CI [0.69–0.83]).
인구통계학적, 개인 관련 및 학습 환경 특성을 고려한 다변량 모델에서 스스로 보고한 장애의 존재는 높은 소진(OR 1.60 [95% CI, 1.43-1.79]) 및 높은 이탈(OR 1.11 [95% CI, 1.001-1.24])의 확률을 높이고, 낮은 공감(OR .74 [95% CI, 0.66-0.82]) 확률을 낮추는 것과 유의미한 연관성을 보였습니다(표 2). 다변량 모델에서 개별 장애 유형을 순차적으로 제외한 민감도 분석 결과, 장애 학생은 단일 장애 유형을 제거하더라도 높은 소진(1.42 [95% CI, 1.21-1.67] ~ 1.63 [95% CI, 1.44-1.83]) 확률이 유의하게 높았고 낮은 공감(.65 [95% CI 0.55-0.76] ~ 0.80 [95% CI, 0.71-0.90]) 확률은 유의하게 낮은 것으로 나타났습니다. 이와는 달리, 다변량 모델에서 만성 건강, 청각 또는 심리적 장애가 있는 학생을 제거했을 때 장애가 있는 학생의 높은 이탈disengagement 확률이 더 이상 높지 않았습니다(1.09 [95% CI, 0.97-1.23]에서 1.19 [95% CI, 1.02-1.40])(그림 S1).
In multivariable models accounting for demographic, personal-related and learning environment characteristics, the presence of a self-reported disability was significantly associated with increased odds of high exhaustion (OR 1.60 [95% CI, 1.43–1.79]) and high disengagement (OR 1.11 [95% CI, 1.001–1.24]) and lower odds of presenting low empathy (OR .74 [95% CI, 0.66–0.82]) (Table 2). Sensitivity analyses serially excluding each individual disability type from multivariable models demonstrated that disabled students continued to present significantly higher odds for high exhaustion (from 1.42 [95% CI, 1.21–1.67] to 1.63 [95% CI, 1.44–1.83]) and significantly lower odds for low empathy (from .65 [95% CI 0.55–0.76] to 0.80 [95% CI, 0.71–0.90]) regardless the removal of any single disability type. Differently, students with disability were no longer more likely to present higher odds for high disengagement when either students with chronic health, hearing or psychological disabilities were removed from multivariable models (from 1.09 [95% CI, 0.97–1.23] to 1.19 [95% CI, 1.02–1.40]) (Figure S1).
3.2 프로그램 접근과 소진 및 공감 지표의 연관성 3.2 Associations of program access with indicators of burnout and empathy
프로그램 접근성이 있는 SWD와 비교했을 때, 프로그램 접근성이 없다고 답한 SWD는 높은 소진(229 [67.4%] 대 931 [46.4%], OR 2.39, 95% CI [1.87-3.04]) 및 높은 이탈(193 [56.4%] 대 771 [38.4%], OR 2.08, 95% CI [1.65-2.63])를 보일 가능성이 유의미하게 높았습니다. 반면, 낮은 공감과 프로그램 접근성 부족 사이에는 유의미한 연관성이 확인되지 않았습니다(93 [27.5%] 대 505 [25.3%], OR 1.12, 95% CI [0.86-1.45])(그림 1).
Compared with SWD with program access, SWD who reported not having program access were significantly more likely to present high exhaustion (229 [67.4%] vs. 931 [46.4%], OR 2.39, 95% CI [1.87–3.04]) and high disengagement (193 [56.4%] vs. 771 [38.4%], OR 2.08, 95% CI [1.65–2.63]). In contrast, no significant associations were identified between low empathy and lack of program access among SWD (93 [27.5%] vs. 505 [25.3%], OR 1.12, 95% CI [0.86–1.45]) (Figure 1).
인구통계학적, 개인 관련 및 학습 환경 공변량을 고려한 다변량 모델에서 장애 학생은 프로그램 접근 여부에 관계없이 장애가 없는 학생보다 높은 소진 지표를 나타낼 가능성이 더 높았습니다(접근 요구 충족, OR 1.50 [95% CI, 1.34-1.69]; 접근 부족 OR 2.59 [95% CI, 1.93-3.49]). 또한, 프로그램 접근이 가능한 장애 학생은 프로그램 접근이 부족한 학생보다 높은 소진 증상을 보일 가능성이 낮았습니다(프로그램 접근이 가능한 장애 학생과 그렇지 않은 학생 비교, OR 0.58 [95% CI, 0.42-0.79]). 반면, 프로그램 접근성이 부족하다고 보고한 장애 학생은 비장애 학생보다 높은 소진 지표를 나타낼 가능성이 훨씬 더 높았지만(OR 1.43 [95% CI, 1.09-1.87]), 프로그램 접근성이 있는 SWD는 그렇지 않았습니다(OR 1.09 [95% CI, 0.97-1.22]). 유의하지는 않았지만, 프로그램 접근 권한이 있는 SWD는 프로그램 접근 권한이 없는 SWD보다 높은 참여도를 보일 가능성이 낮은 경향을 보였습니다(OR 0.76 [95% CI, 0.57-1.01]; p = .06). 공감과 관련하여, 두 그룹 모두 장애가 없는 또래보다 낮은 공감 지표를 나타낼 가능성이 낮았습니다(접근 요구 충족, OR 0.75 [95% CI, 0.67-0.85]; 접근 부족, OR 0.68 [95% CI, 0.52-0.90]). 프로그램 액세스가 있는 경우와 없는 경우의 낮은 공감 확률에 유의미한 차이가 없었기 때문에 프로그램 액세스는 공감에 영향을 미치지 않는 것으로 나타났습니다(OR 1.10 [95% CI, 0.82-1.48])(표 3).
In multivariable models accounting for demographic, personal-related and learning environment covariates, disabled students were more likely to present indicators of high exhaustion than students without disabilities regardless of program access (access needs met, OR 1.50 [95% CI, 1.34–1.69]; lack of access OR 2.59 [95% CI, 1.93–3.49]). Further, SWD with program access were less likely to present high exhaustion than their counterparts reporting lack of program access (SWD with program access vs. without, OR 0.58 [95% CI, 0.42–0.79]). In contrast, whereas students with disabilities reporting lack of program access were significantly more likely than students without disabilities to present indicators of high disengagement (OR 1.43 [95% CI, 1.09–1.87]), SWD with program access were not (OR 1.09 [95% CI, 0.97–1.22]). Although not significant, SWD with program access showed a tendency towards being less likely to present high disengagement than SWD without program access (OR 0.76 [95% CI, 0.57–1.01]; p = .06). With respect to empathy, both groups of SWD were less likely than their peers without disabilities to present indicators of low empathy (access needs met, OR 0.75 [95% CI, 0.67–0.85]; lack of access, OR 0.68 [95% CI, 0.52–0.90]). Program access did not seem to impact empathy as there was not a significant difference in low empathy odds between SWD with and without access (OR 1.10 [95% CI, 0.82–1.48]) (Table 3).
4 토론 4 DISCUSSION
저희가 아는 한, 의대생들의 공감 능력, 소진, 프로그램 접근성, 장애 사이의 연관성을 체계적으로 조사한 연구는 이번이 처음입니다. 미국 의대생의 전국 표본 데이터를 사용하여 장애 학생의 번아웃 증상 빈도가 높음에도 불구하고, 장애 학생이 비장애 학생에 비해 공감 능력이 낮을 가능성이 유의하게 낮다는 사실을 확인했습니다. 중요한 점은 프로그램 접근성을 고려한 후에도 [프로그램 접근성이 있는 장애 학생]은 [비장애 학생]과 높은 이탈 측면에서 차이가 없었으며, 프로그램 접근성과 관계없이 공감도가 낮다고 보고하지 않았다는 점입니다. 이러한 데이터는 이 집단이 공감 능력이 뛰어난 인력과의 관련성을 강조하고 장애 의대생의 복지와 유지를 위해프로그램 접근성이 중요한 역할을 한다는 점을 강조합니다. To our knowledge, this is the first study to systematically investigate the association between empathy, burnout, program access and disability among medical students. With the use of data from a national sample of US medical students, we identified that despite the high frequency of burnout symptoms among disabled students, this population was significantly less likely to present low empathy than their peers without disabilities. Importantly, after accounting for program access, disabled students who had program access did not differ from students without disabilities in terms of high disengagement and did not report low empathy regardless of program access. These data highlight the relevance of this population to a more empathic workforce and underscore the critical role of program access to the well-being and retention of medical students with disabilities.
이전 연구에 따르면 공감 점수가 높을수록 인구통계학적 요인(예: 여성 성별,39, 72-74 고령,72, 73 소외된 인종/민족75 및 성적 소수자76), 모호성에 대한 높은 내성,77 더 나은 삶의 질,74 학습 환경에 대한 더 긍정적인 인식72 및 낮은 참여도72, 74, 78, 79 우리의 연구 결과는 장애와 높은 공감 사이의 연관성이 의대생의 공감과 관련된 이러한 잘 알려진 요인들을 고려한 후에도 지속된다는 사실을 입증함으로써 문헌에 추가되었습니다. 특히 프로그램 접근성을 고려한 다변량 모델에서는 프로그램 접근성이 있는 장애 학생과 없는 장애 학생 모두 비장애 학생에 비해 공감 능력이 낮을 가능성이 적었으며, 이는 프로그램 접근성이 제공되지 않는 상황에서도 공감 능력이 유지된다는 것을 시사합니다. 이러한 결과를 종합해 볼 때, 장애에 대한 생생한 경험이 장애 의대생의 공감 능력을 향상시키는 강력한 보호 요인이 될 수 있음을 시사합니다. Prior studies demonstrate that higher empathy scores are associated with demographic factors (e.g. female sex,39,72-74older age,72,73underrepresented race/ethnicity75and sexual minorities76), higher tolerance for ambiguity,77better quality of life,74more positive perceptions of the learning environment72and lower disengagement.72,74,78,79Our study results add to the literature by demonstrating that the associations between disability and higher empathy persisted even after accounting for these well-established factors associated with empathy among medical students. Notably, multivariable models accounting for program access identified that both disabled students with and without program access were less likely to present low empathy than their peers without disabilities, suggesting that even in situations where program access is not provided, empathy remains preserved. Taken together, these results suggest that lived experience of disability25,26,28may be a robust protective factor, leading to increased empathy among medical students with disabilities.
수련 의사를 대상으로 한 최근 연구에 따르면 프로그램 접근성이 장애 학습자의 웰빙과 성과에 매우 중요하다고 합니다.56, 58 본 연구 결과는 프로그램 접근성이 장애 의대생의 낮은 소진 및 낮은 이탈과 관련이 있으며, 장애와 프로그램 접근성을 스스로 보고하는 학생과 비장애 동료의 이탈 지표가 다르지 않음을 보여줌으로써 이러한 지식을 뒷받침합니다. 소진exhaustion이 탈진burnout의 스트레스 요소로 이해되고 이탈disengagement이 학업에 대한 부정적인 태도와 같은 직업을 계속 유지하지 않으려는 태도와 관련이 있다는 점을 고려할 때,61,80 본 연구 결과는 장애 의대생의 복지와 유지에 있어 프로그램 접근성이 중요한 역할을 한다는 것을 시사합니다. 이는 의과대학별로 장애 접근성을 알리는 전문 지식의 수준이 다양하다는 일화 보고서에서 특히 주목할 만합니다.26 2021년 연구에 따르면 미국 의과대학의 35%가 AAMC 고려사항에 따라 장애 공개 시스템을 유지하지 않는 것으로 나타났습니다.50 이와 동시에 의과대학에 장애 전문 인력을 배치하여 장애 학생 집단을 위한 효과적인 편의를 개선하고 지원을 전달할 수 있는 이점이 있다는 여러 요구가 있었습니다.26, 51, 81 우리의 연구 결과는 이러한 권고사항과 장애 공개 및 편의 요청에 대한 구조적 장벽을 제거할 필요성을 뒷받침합니다.50, 82 일반적으로 보고된 구조적 장벽에는 장애 공개 과정에서의 이해 상충(예: 학생의 평가 또는 승진에 역할을 맡은 개인이 학생의 편의 요청 검토에 관여하는 경우),25, 29, 81 장애 자원 전문가들의 편의에 대한 전문 지식 및 지식 부족26, 50 모범 사례 및 관련 장애 및 판례법에 의해 알려지지 않은 장애 공개 시스템이 포함되나 이에 한정되지는 않습니다.81
Recent studies with training physicians suggest that program access is critical to the well-being and performance of learners with disabilities.56,58Our results endorse this body of knowledge by demonstrating that program access was associated with lower exhaustion and disengagement among medical students with disabilities and that students self-reporting disabilities and program access did not differ from their colleagues without disabilities in terms of disengagement indicators. Given that exhaustion is understood as the stress component of burnout and disengagement is associated with negative attitudes toward one's studies and unwillingness to continue in the same profession,61,80our findings suggest a critical role of program access to the well-being and retention of medical students with disabilities. This is particularly noteworthy as anecdotal reports suggest varying levels of expertise informing disability access across medical schools.26A 2021 study demonstrated that 35% of US medical schools did not maintain disability disclosure systems in alignment with AAMC considerations.50In parallel, multiple calls support the benefit of having specialised disability personnel for the medical school to enhance effective accommodations and communicate support for the population of students with disabilities.26,51,81Our findings support these recommendations and the need to remove structural barriers to disability disclosure and accommodation request.50,82Commonly reported structural barriers include, but are not limited to, conflicts of interest in the disability disclosure process (e.g. when individuals who hold a role in students' assessment or promotion are involved in the review of students' requests for accommodations),25,29,81lack of expertise and knowledge about accommodations among disability resource professionals26,50and disability disclosure systems that are not informed by best practices and relevant disability and case law.81
이 연구에는 한계가 있습니다.
첫째, 횡단면 설계로 인해 인과관계나 확인된 연관성의 방향에 대한 명확한 결론을 내릴 수 없습니다.
둘째, 표본 규모가 크고 응답률이 높지만 의대 2학년생에 초점을 맞춘 데이터이기 때문에 의대 교육 전반에 걸친 공감의 안정성에 대해 보고할 수 있는 능력이 제한됩니다.
셋째, 본 연구 측정의 자기보고적 특성은 장애 및 정신 건강 공개에 대한 학생들의 기밀성 우려를 줄이는 데 중요하지만, 이러한 측정은 낙인, 편견 및 공식 평가에 대한 접근성에 영향을 받을 수 있는 학생들의 공개 결정에 의해 제한될 수 있습니다.26
넷째, 우수한 심리측정 특성에도 불구하고61 OLBI는 선별 도구이며 번아웃에 대한 임상 평가가 아닙니다.
다섯째, 본 분석에는 의대생의 소진 및 공감과 관련이 있을 수 있는 몇 가지 인구통계학적, 개인 관련 및 학습 환경 요인이 포함되었지만, 의료 시스템에 대한 개인적인 경험, 이전 학업 환경에서의 장애 공개 및 프로그램 이용과 같은 잠재적으로 관련성이 있는 다른 요인은 설문조사에 포함되지 않았습니다.
여섯째, 민감도 분석 결과 단일 장애 유형이 스스로 공개한 장애와 소진 및 공감 지표 간의 연관성과 관련된 전반적인 결과에 큰 영향을 미치지 않는 것으로 나타났지만, 특정 유형의 장애를 보고한 학생 수가 적어 각 장애 유형에 따른 다변량 분석을 수행할 수 없었습니다.
마지막으로, 본 연구에서는 필요한 경우 스스로 보고한 편의 제공 부족을 통해 프로그램 접근성 부족을 파악하고자 했지만, 장애 접근성은 편의 제공을 넘어 낙인찍는 태도와 편견 등 환경과 포용성을 형성하는 추가적인 장벽을 포함하는 다요인적 구조입니다.
This study has limitations.
First, its cross-sectional design does not allow definitive conclusions about causality or the direction of the identified associations.
Second, despite the large sample size and high response rate, the data focus on second-year medical students, reducing our ability to report on the stability of empathy across the medical education continuum.
Third, although the self-reported nature of our study measures is critical to reducing students' confidentiality concerns regarding disability and mental health disclosures, these measures may be limited by students' decision to disclose, which can be influenced by stigma, bias and access to formal evaluation.26
Fourth, despite its good psychometric properties,61the OLBI is a screening instrument and not a clinical assessment of burnout.
Fifth, although our analyses included several demographic, personal-related and learning environment factors that are likely relevant for burnout and empathy among medical students, the survey does not include other potentially relevant factors such as personal experiences with health care systems and with disability disclosure and program access in previous academic settings.
Sixth, while our sensitivity analyses suggest that no single type of disability played a large impact on the overall outcomes related to the associations between self-disclosed disability and indicators of burnout and empathy, the small number of students reporting certain types of disabilities did not allow us to perform multivariable analyses specific to each disability type.
Finally, although we aimed to capture the lack of program access through self-reported lack of accommodations when needed, disability access is a multifactorial construct that extends beyond accommodation and includes additional barriers, including stigmatising attitudes and biases that shape climate and inclusion.
이러한 한계에도 불구하고 이 연구는 대규모의 전국적인 학생 표본을 사용하여 연구 결과를 강화했습니다. 장애 학생의 소진과 공감을 유발하는 추가적인 잠재적 요인을 파악하기 위해서는 추가적인 연구가 필요합니다. 또한, 의대생들의 장애, 공감, 웰빙 사이의 연관성을 조사하는 종단 연구를 통해 확인된 연관성을 더 잘 이해하고 의대생들의 공감 능력이 의과대학 내내 유지되는지 여부를 파악할 필요가 있습니다. 미국 의대생의 장애, 프로그램 접근성, 공감 및 소진에 대한 이 대규모 전국 연구는 [장애가 없는 학생]에 비해 [장애 학생]이 프로그램 접근성이나 소진에 관계없이 공감 능력이 떨어질 위험이 낮으며, 프로그램 접근성이 이 집단의 소진과 이탈을 줄이는 데 중요한 요인이 될 수 있음을 시사합니다. 이러한 연구 결과는 의학 분야에서 장애 학생의 강점에 대한 이해를 더하고 다양한 학생 집단을 모집하고 지원하는 데 시사점을 제공합니다.
Despite these limitations, this study uses a large, national sample of students, strengthening our findings. Further research is needed to identify additional potential drivers of burnout and empathy among students with disabilities. Moreover, longitudinal studies investigating the associations between disability, empathy and well-being among medical students are needed to better understand the identified associations and to determine whether empathy is maintained throughout medical school for this population. This large national study of disability, program access, empathy and burnout among US medical students suggests that, compared with students without disabilities, disabled students are at lower risk for low empathy regardless of program access or burnout and that program access may be a critical factor in reducing exhaustion and disengagement in this population. These findings also add to our understanding of the strengths of students with disabilities in medicine and have implications for recruiting and supporting this diverse population of students.
Med Educ. 2023 Jun;57(6):523-534.doi: 10.1111/medu.14995.Epub 2022 Dec 14.
Disability, program access, empathy and burnout in US medical students: A national study
Objective:The objective of this study is to investigate whether self-disclosed disability and self-reported program access are associated with measures of empathy and burnout in a national sample of US medical students.
Methods:The authors obtained data from students who responded to the Association of Medical Colleges (AAMC) Year 2 Questionnaire (Y2Q) in 2019 and 2020. Data included demographic characteristics, personal variables, learning environment indicators, measures of burnout (Oldenburg Burnout Inventory for Medical Students), empathy (Interpersonal Reactivity Index) and disability-related questions, including self-reported disability, disability category and program access. Associations between disability status, program access, empathy and burnout were assessed using multivariable logistic regression models accounting for YQ2 demographic, personal-related and learning environment measures.
Results:Overall, 23 898 (54.2%) provided disability data and were included. Of those, 2438 (10.2%) self-reported a disability. Most medical students with disabilities (SWD) self-reported having program access through accommodations (1215 [49.8%]) or that accommodations were not required for access (824 [33.8%]). Multivariable models identified that compared with students without disabilities, SWD with and without program access presented higher odds of high exhaustion (1.50 [95% CI, 1.34-1.69] and 2.59 [95% CI, 1.93-3.49], respectively) and lower odds of low empathy (0.75 [95% CI, 0.67-.85] and 0.68 [95% CI, 0.52-0.90], respectively). In contrast, multivariable models for disengagement identified that SWD reporting lack of program access presented higher odds of high disengagement compared to students without disabilities (1.43 [95% CI, 1.09-1.87], whereas SWD with program access did not (1.09 [95% CI, 0.97-1.22]).
Conclusions:Despite higher odds of high exhaustion, SWD were less likely to present low empathy regardless of program access, and SWD with program access did not differ from students without disabilities in terms of disengagement. These findings add to our understanding of the characteristics and experiences of SWD including their contributions as empathic future physicians.
의학교육에서 장애 표용: 질향상 접근을 향하여 (Med Educ, 2022) Disability inclusion in medical education: Towards a quality improvement approach Satendra Singh1 | Lisa M. Meeks2
1 서론 1 INTRODUCTION
장애를 가진 의사를 포함한 보다 다양한 인력으로 초점을 전환하는 것은 국제적으로 상당한 주목을 받고 있습니다.1,2 실제로 장애 포용은 의학교육에서 르네상스를 경험하고 있습니다. 전 세계의 의학교육 협회, 규제 기관 및 프로그램은 장애 포용의 가치를 지지하며 자격을 갖춘 장애 수련의에 대한 제도적 장벽을 제거하고 포용적 관행을 강화하는 등 시스템 변화를 촉구하고 있습니다.3-7 The shift in focus to a more diverse workforce that includes physicians with disabilities has gained considerable international traction.1,2Indeed, disability inclusion is experiencing a renaissance in medical education. Across the globe, medical education associations, regulating bodies and programmes espouse the value of disability inclusion and are calling for systems change, including removing systemic barriers to qualified trainees with disabilities and strengthening inclusive practices.3-7
2 의료 협회 지침 2 MEDICAL ASSOCIATION GUIDANCE
최근 몇 년 동안 5개 의학 협회는 다음과 같이 의학교육에서 직접적으로 행동을 촉구하는 중요한 지침 문서를 제공했습니다:
의학교육에서의 접근성, 포용성 및 행동: 장애를 가진 학습자 및 의사의 생생한 경험(미국의과대학협회, 2018),3
환영 및 가치 인정: 의학 교육 및 훈련에서 장애인 학습자 지원(영국의학위원회, 2018),4
포용적 의학 교육: 장애가 있는 의대 프로그램 지원자 및 학생에 대한 지침(호주 및 뉴질랜드 의과대학 학장협회, 2021),5
장애가 있는 수련의를 위한 의학교육 장벽 평가 연구(미국의사협회, 의학교육위원회, 2022)6
의료계에서의 장애(영국의사협회, 2020).7
이러한 간행물은 장애 포용성 강화를 촉구하는 동시에 의학교육 전반에 걸쳐 자격 있는 수련의가 직면한 글로벌 장벽과 지속적인 과제를 드러내기도 합니다. In recent years, five medical associations have provided significant guiding documents that directly call for action in medical education including:
Accessibility, Inclusion, and Action in Medical Education: Lived Experiences of Learners and Physicians With Disabilities (Association of American Medical College, 2018),3
Welcomed and Valued: Supporting disabled learners in medical education and training (General Medical Council, UK, 2018),4
Inclusive Medical Education: Guidance on medical programme applicants and students with a disability (Medical Deans Australia and New Zealand Inc, 2021),5
A Study to Evaluate Barriers to Medical Education for Trainees with Disabilities (American Medical Association, Council on Medical Education, 2022)6 and
Disability in the Medical Profession (British Medical Association, 2020).7
While these publications call for greater disability inclusion, they also unveil global barriers and ongoing challenges for qualified trainees across the medical education continuum.
3 규제 부족 3 LACK OF REGULATION
알려진 장벽에도 불구하고 장애가 있는 수련의를 보호하기 위한 규제는 거의 존재하지 않습니다. 일반적으로 수련의 지원을 규제하는 인증 기관은 차별 금지 및 합리적 편의 제공에 대한 법적 요건 외에 장애 포용에 대한 지침을 거의 제공하지 않습니다.8 장애에 초점을 맞춘 규정은 없지만 일부 인증 기관은 학교가 질 개선(QI) 노력에 참여하도록 요구하고 있습니다.9, 10 Despite known barriers, little regulation exists to protect trainees with disabilities. Accrediting bodies, which usually regulate trainee support, offer little guidance on disability inclusion beyond legal requirements for non-discrimination and reasonable accommodation.8While disability-focused regulations are absent, some accreditation bodies do require schools to engage in Quality Improvement (QI) efforts.9,10
의료 협회의 장애 포용에 대한 요구3-7와 규제의 부재를 고려할 때, 질 개선 모델은 장애 포용 및 서비스 노력을 유도하는 데 중요한 이점을 제공할 수 있습니다. 이 논평에서는 의학교육의 질 향상을 위한 고려사항을 제시하며, 이는 전 세계적으로 개정된 세계의학교육연맹(WFME)의 교육(기초의학교육, BME), 수련(의학전문대학원 교육, PME), 실무(지속적 전문성 개발, CPD)의 세 가지 수준 모두에서의 QI 표준 3부작을 다룹니다(표 1). 우리는 조직의 실천과 행동을 안내하기 위해 고안된 데밍의 질 관리를 위한 핵심 사항을 사용하여 시스템 기반의 장애 포용적이고 접근 가능하며 공평한 의학교육의 비전을 제안합니다.11 Given the calls for disability inclusion by medical associations,3-7coupled with the prevailing lack of regulation, models of quality improvement may hold material benefits for guiding disability inclusion and service efforts. In this commentary, we offer considerations for quality improvement in medical education that address the globally revised trilogy of World Federation for Medical Education (WFME) standards of QI at all three levels of education (Basic Medical Education, BME), training (Postgraduate Medical Education, PME) and practice (Continuing Professional Development, CPD) (Table 1). We propose a vision of systems-based disability-inclusive, accessible and equitable medical education using key points from Deming's Points for Quality Management, designed to guide organisational practice and behaviour.11
TABLE 1. Deming's points for quality management applied to disability inclusion
W. Edwards Deming's 14 points
Where applicable in medical education
1.
Create constancy of purposetowards improvement
BME/PME/CPD
Recommendation: Build long-range disability inclusion QI into the institutional planning.
2.
Adopt the new philosophy.
BME/PME
Recommendation: Adopt a new philosophy that disability diversity results in stronger, more capable and innovative systems and that physicians with disabilities add value to health care and should be celebrated.
3.
Cease dependence on inspection to achieve quality.
BME/PME
Recommendation: Build quality into the system by removing barriers to access found in physical space, curriculum, policy, technical standards, disability service, licensure and accommodation request.
4.
Move towards a single supplier for any one item. (Standards to minimise variation/interpretation)
BME/PME
Recommendation: Provide specialised disability resource providers to assist with disability inclusion and regulate the requirement for this position.
5.
Improve constantly and forever every process for planning, production, and service
BME/PME/CPD
Recommendation: Develop a task force to consistently and quickly respond to new disability related barriers and to proactively recommend changes that improve access for all.
6.
Institute training on the job.
BME/PME/CPD
Recommendation: Provide staff and faculty training on disability justice, disability competency and consciousness.
7.
Adopt and institute leadership.
BME/PME
Recommendation: Leadership must communicate the commitment to disability inclusion and must create actionable steps to reach their goals.
8.
Drive out fear.
BME/PME
Recommendation: Fear must be driven out through two mechanisms; creating a safe place for trainees to disclose and educating institutional stakeholders about the success of physicians with disabilities.
14.
The transformation is everybody's job.
BME/PME/CPD
Recommendation: Communicate to the training community that access is an organisational commitment and that each stakeholder has a specific role.
Abbreviations: BME: Basic Medical Education; CPD: Continuing Professional Development; PME: Postgraduate Medical Education.
품질 관리를 위한 데밍의 포인트 4 DEMING'S POINTS FOR QUALITY MANAGEMENT
데밍의 모델은 처음에는 산업을 위해 고안되었지만 의학교육 분야에도 적용되었습니다.12, 13 데밍의 모델은 특히 장애 포용이라는 주제에 적용할 수 있습니다.
첫째, 데밍의 개선 접근 방식은 개인이 아닌 시스템에 초점을 맞추고 있습니다. 역사적으로 장애 포용은 시스템에 대한 검토 없이 개인의 문제로 간주되어 왔으며,14 개인을 문제시해 왔습니다.
둘째, 데밍의 모델은 결함이 있는 시스템을 계속 사용하면 기업의 성장이 저해된다는 점을 인식하고, 장애 포용에 초점을 맞춘 연구자들이 지지하는 접근 방식인 업무 수행 방식에 대한 역사적 이론을 버리고 조직이 근본적인 변화를 겪을 것을 촉구합니다.15
다음으로, 데밍의 이론은 사람들이 서비스 품질 개선을 위한 새로운 통찰력과 아이디어를 창출할 수 있는 기회를 만들기 위해 조직적, 직업적 장벽을 허물어야 한다고 주장합니다.
마지막으로 데밍은 리더에게 서비스 실행의 불확실성과 변동성을 최소화할 것을 요구하는데, 이는 문헌에서 지지하는 필요성입니다.3, 8, 16
여기서는 데밍의 14가지 품질 관리 이론 중 9가지를 적용하여 장애인을 의료 교육에 포함할 수 있도록 개선합니다. Although initially designed for industry, Deming's models have been applied to the field of medical education.12,13Deming's model is especially applicable to the subject of disability inclusion.
First, Deming's approach to improvement is specific to the system versus the individual. Disability inclusion has historically been viewed as an individual issue, problematizing the person,14 without review of the system.
Second, Deming's model recognises that the continued use of a flawed system will hinder a company's growth and calls for organisations to undergo fundamental change, throwing out historical theories of how work is accomplished, an approach supported by researchers focused on disability inclusion.15
Next, Deming's theory calls for us to break down organisational and professional barriers as a necessary move for creating opportunities for people to generate new insights and ideas for improving service quality.
Finally, Deming calls on leaders to minimise uncertainty and variability in executing service, a need endorsed in the literature.3, 8, 16
Here, we apply 9 of Deming's 14-point quality management theory to improve the inclusion of individuals with disabilities in medical education.
장애 포용에 적용되는 데밍의 포인트 5 DEMING'S POINTS AS APPLIED TO DISABILITY INCLUSION
5.1 데밍의 포인트 1: 개선을 향한 목적의 일관성 만들기 5.1 Deming point 1: Create constancy of purpose towards improvement
알바니즈(1999)는 데밍의 요점 1을 사용하여 의학교육이 장애 포용의 핵심 아이디어인 학습 환경의 지속적인 개선에 중점을 두고 장기적인 관점을 통합하는 제도적 문화를 조성할 것을 촉구했습니다.13 실제로 의학교육에서 장애 포용 작업은 정책, 실무 및 커리큘럼에서 장애 포용을 옹호하는 한 두 명의 챔피언이 주도하는 학교별 작업인 경우가 많습니다. '챔피언' 모델을 고려할 때, 교수진이 바뀌면 장애 포용 업무가 축소되거나 완전히 없어질 수 있습니다. 또는 전체 의학교육 기업이 지속적인 개선 모델에 전념하는 경우, 교수진이나 리더십의 변화와 관계없이 장애 포용은 기업의 우선 순위로 유지됩니다. Using Deming's point 1, Albanese (1999) called for medical education to create an institutional culture that incorporates the long-range perspective with a focus on continual improvement of the learning environment—a key idea for disability inclusion.13Indeed, disability inclusion work in medical education is often school specific, spearheaded by one or two champions who advocate for disability inclusion in policy, practice and curricula. Given the ‘champion’ model, a change in faculty may result in a reduction in—or complete elimination of—disability inclusion work. Alternatively, if the entire medical education enterprise commits to a continuous improvement model, then disability inclusion remains a priority of the enterprise, regardless of changes in faculty or leadership.
5.2 데밍 포인트 2: 새로운 철학의 채택 5.2 Deming point 2: Adopt the new philosophy
데밍은 품질 개선을 위해 새로운 철학을 채택할 것을 제안했습니다. 역사적으로 장애인 포용은 소송 위험을 완화하는 것을 주요 목표로 하는 규정 준수 문제로 간주되어 왔습니다. 교육 환경마다 장애 포용에 대한 접근 방식은 다양하지만, 모든 측면에서 다양성을 증진하려는 노력을 포함하는 사회 정의적 관점은 장애와 관련하여 종종 잊혀졌습니다. 장애 포용에 관한 연구에서 Jain은 장애를 인간 다양성의 정상적인 부분이자 가치 있는 사회적 정체성으로 간주하는 의도적 포용의 원칙에 따라 '변혁적' 접근 방식을 요구합니다.17 이러한 접근 방식에 따라 교육 환경은 모든 교육생을 포함하도록 의도적으로 설계되고 시스템에 보편적 설계와 유연성이 내장된 환경으로 전환됩니다.17, 18 변화는 모든 훈련생을 위한 환경을 개선하고 여러 가지 다양한 경로를 통해 역량을 달성하는 것을 목표로 하는 지속적인 과정(데밍 포인트 5 참조)입니다.17 따라서 새로운 철학은 장애 다양성이 더 강력하고 유능하며 혁신적인 시스템으로 이어진다고 말할 수 있습니다. 이 철학의 지배적인 사고방식은 장애가 있는 수련생은 의료서비스에 가치를 더하며, 따라서 축하받아야 한다는 것입니다. Deming suggestedadopting a new philosophyfor quality improvement. Historically, disability inclusion has been viewed as a compliance issue, with the primary goal of mitigating litigation risk. While training environments vary in their approach to disability inclusion, the social justice lens, which includes an avowed commitment to increasing diversity in all respects, is oft-forgotten when it comes to disability. In her work on disability inclusion, Jain calls for a ‘transformative’ approach, guided by the principles of intentional inclusion, where disability is viewed as a normal part of human variation and a valued social identity.17Under this approach, the training environment shifts to one that is intentionally designed to include all trainees, with universal designand flexibility built into the system.17,18Change is an ongoing process (see Deming point 5), with the goal of improving the environment for all trainees and the achievement of competency through multiple and diverse pathways.17Thus, a new philosophy would state that disability-diversity results in stronger, more capable and innovative systems. The prevailing mindset under this philosophy is that trainees with disabilities add value to health care and, therefore, should be celebrated.
5.3 데밍의 요점 3: 검사에 대한 의존을 중단하고 처음부터 제품에 품질을 구축하여 품질을 달성해야 합니다. 5.3 Deming's point 3: Cease dependence on inspection to achieve quality by building quality into the product in the first place
Albenese(1999)는 데밍의 3단계를 의학교육에 적용할 때, 평가는 양질의 교육과 조기 문제 발견에 중점을 두고 학생들이 개선해야 할 부분을 파악하여 교정이 적용될 수 있도록 돕기 위한 목적이어야 한다고 주장했습니다.13 그러나 장애가 있는 능력주의 환경에서는 양질의 수련생 평가가 이루어지지 않을 수 있습니다.15 Albenese (1999) argued that in applying Deming's step 3 to medical education, assessment should be for the purpose of helping students identify where they need to improve with the focus on high-quality education and early problem detection so that remediation can be applied.13However, high-quality trainee assessment may be absent when it occurs within a barrier-laden, ableist environment.15
의학교육 내에서 장애는 종종 시스템에 대한 위협으로 문제시됩니다.14 실제로 의료화medicalization, 즉 '의료기관이 [다양하고 비합치적non-conforming 인간의 상태와 행동]을 [생의학 지식의 영역에 들어오는 문제]로 취급하는 경향'은 자주 보고되는 문제입니다.19 장애 포용의 '상태'는 접근에 대한 시스템적 장벽으로 측정할 수 있으며, 이는 비장애 동료와 비교하여 장애인 수련생에게 불균등한 결과를 초래합니다.20 이러한 장벽은 다음을 포함한 여러 영역에 존재합니다.24, 25
입학,3, 21, 22 교육,18 과정,16 의학 교육 및 면허 시험에서의 편의 제공,23, 24 합리적이고 적절한 편의/조정에 관한 지식 부족3, 16 및 의사 면허를 위한 차별적 관행
Within medical education, disability is often problematized as a threat to the system.14Indeed,medicalization, or the ‘tendency of a medical institution to deal with diverse, non-conforming human conditions and behaviors entering the realm of biomedical knowledge’ asproblemsto be cured, is an oft-report issue.19The ‘State’ of disability inclusion can be measured by systemic barriers to access, which lead to disparate outcomes for trainees with disabilities compared to their non-disabled peers.20These barriers are present in several domains, including:
admissions,3, 21, 22 instruction,18 process,16 access to accommodation in medical training and licensure exams,23, 24 lack of knowledge regarding reasonable and appropriate accommodation/adjustments3, 16 and discriminatory practices for physician licensure.24, 25
능력주의적이고 역사적으로 적대적인 환경의 맥락에서, 장애를 스스로 확인해야 하는 상황은 또한 장애를 과소 보고하는 결과를 낳고, 수련생들은 묵묵히 고통받으며 프로그램을 충분히 이용하지 못하고 의료계에 소속감을 느끼는 혜택을 누리지 못합니다.25 미국에서는 수련생이 주도하는 공개 및 요청에 대한 정책 지원이 부분적으로 법에 근거하고 있습니다.26 이 경우 기관이나 단체가 장애인이라고 선제적으로pre-emptively판단하고 편의를 제공하는 것을 금지하고 있습니다. 사전 문의pre-inquiry에 대한 법적 제한에도 불구하고, 기관은 유니버설 교수 설계Universal Design of Instruction의 메커니즘을 활용하여 가능한 한 모든 교육생을 위해 설계된 교수 학습 제품을 만들어 모든 학습자가 학습 환경에 접근할 수 있도록 하는 사전 접근proactive 방식을 취할 수 있고 또 취해야 합니다.18 현재까지 장애 포용에 대한 장벽을 제거하기 위한 시스템 전반의 요구 사항은 존재하지 않으므로 데밍의 포인트 4로 이어집니다. In the context of an ableist and historically hostile environment.15The need to self-identify a disability will also result in an underreporting of disability and a cadre of trainees who are silently suffering, never truly having full access to our programmes and never reaping the benefits of feeling included in the medical community.25The policy support for US-based trainee-driven disclosure and request is partially informed by the law.26In this case, it prohibits institutions or organisations from pre-emptively determining that a person is disabled and offering accommodation. Despite legal restrictions on pre-inquiry, organisations can and should engage in proactive approaches to access by utilising mechanisms of Universal Design of Instruction, making the learning environment accessible to all learners through the creation of teaching and learning products that are designed for all trainees to the fullest extent possible.18To date, no system-wide requirement to remove barriers to disability inclusion exist, leading us to Deming's point 4.
5.4 데밍 포인트 4: 하나의 품목에 대해 단일 공급자로 이동(변형/해석을 최소화하는 표준) 5.4 Deming point 4: Move towards a single supplier for any one item (standards to minimise variation/interpretation)
데밍은 제조업체가 단일 공급업체와의 관계를 발전시킬 것을 강력히 촉구합니다.11 원래 목표는 제조업체로 들어오는 재료의 품질을 높이고 변동성을 줄이는 것입니다. 의학교육에서는 장애를 공개한 후 수련의를 지원하는 일관된 프로세스가 없습니다.8 실제로 대부분의 수련의는 규제되지 않고 정보가 부족한 시스템에 들어가게 되며, 의사가 될 수 있는 능력에 대한 지속적인 믿음과 전문적 지원 부족으로 인한 과소 수용 또는 노골적인 거부에 취약해집니다.16 장애 포용 노력은 모범 사례나 규정 없이 개별 기관에 맡겨져 일관되지 않은 의사 결정과 매우 다양한 수련의 경험으로 이어지곤 합니다.16 편견을 줄이고, 이해 상충을 피하며, 과정에 대한 근접성과 전문성을 향상시키기 위해 설계된 '구조'가 존재하지만3 이러한 구조적 권장 사항은 규제되지 않습니다.16 Deming strongly urges manufacturers to develop a relationship with a single supplier.11The original goal is to raise the quality and reduce the variability of the materials that come to the manufacturer. In medical education, there is no consistent process for supporting a trainee once a disability disclosure is made.8Indeed, most will enter an unregulated, uninformed system leaving them vulnerable to persistent ableist beliefs about their ability to become physicians and under-accommodation or outright denial of accommodation due to lack of specialised support.16Disability inclusion efforts are often left to the individual institutions, sans best practice or regulation, leading to inconsistent decision-making and highly varied trainee experiences.16While suggested ‘structures’ exist3and are designed to reduce bias, avoid conflicts of interest and enhance proximity and expertise to the process, these structural recommendations are not regulated.16
문헌에는 [접근성access을 위한 전문가 접점expert touch point]으로서 [전문 장애 자원 전문가]를 갖출 것에 대한 요구가 다수 존재한다.3, 6, 8, 16 이 '단일 공급자' 접근법은 [장애 지원 제공자]를 한 명으로 하여 장애 수련의가 의료 교육에서 장애 포함 및 편의에 대한 전문 지식을 갖춘 비-평가적인 지도자에게 비밀리에 접근하는 모범 사례를 가리킵니다. 이러한 '단일 공급자'는 시스템 전반에 걸쳐 여러 번의 협상의 필요성을 줄이고, 민감한 장애 관련 문서를 보관할 수 있는 중앙 집중식 기밀 공간을 제공하며, 편의 제공에 대한 해석이 필요한 교수진이나 관리자를 지원합니다.16 또한 평가자가 장애에 기반한 편견을 인식하지 못할 때 발생할 수 있는 차별적 대우를 줄여줍니다. 규제 기관이 정신건강 서비스 제공자에게 요구하는 것과 유사하게 의과대학 전반에 걸쳐 이러한 역할을 요구한다면 의학교육이 데밍의 요점 4에 더 가까워지고 변형/해석을 최소화할 수 있을 것입니다.8 The literature consists of multiple calls for a specialised disability resource professional as an expert touch point for access.3,6,8,16This‘single supplier’approach points towards the best practice of having a single disability resource provider so that trainees with disabilities have access to a confidential, non-evaluative leader with expertise in disability inclusion and accommodation in medical training. This ‘single supplier’ reduces the need for multiple negotiations across the system, allows for a centralised and confidential space for holding sensitive disability documentation and provides support to faculty or administrators who require interpretation of an accommodation.16It also reduces disparate treatment that can sometimes occur when evaluators are unaware of their disability-based biases. If regulating bodies were to require this role across medical schools, similar to how they require mental health providers, medical education would move closer to Deming's point 4 andminimise variation/interpretation.8
5.5 데밍의 요점 5: 계획, 생산 및 서비스를 위한 모든 프로세스를 지속적으로 그리고 영원히 개선해야 합니다. 5.5 Deming's point 5: Improve constantly and forever every process for planning, production and service
데밍은 증가하는 요구사항에 진정으로 대응하기 위해서는 조직이 지속적인 개선에 집중해야 한다고 강조했습니다. 더 많은 장애인 교육생이 시스템에 들어와 정보를 제공함에 따라 새로운 장벽이 식별되고 더 큰 포용의 기회가 발견될 것입니다. 지속적인 개선을 위한 노력은 시스템을 민첩하게 만들고, 장벽을 파악하고, 신속하게 대응할 수 있게 해주며, 유니버설 디자인, 커리큘럼 변경 또는 비표준 시간 내에 의학 학위를 이수할 수 있도록 시스템 내 유연성 강화를 통해 많은 교육생의 요구를 충족하도록 시스템을 발전시킬 수 있습니다. Deming highlighted that to be truly responsive to growing needs, an organisation must focus on continuous improvement. As more trainees with disabilities enter and inform the system, new barriers will be identified and opportunities for greater inclusion uncovered. A constant commitment to improving allows the system to be nimble, identify barriers, and respond quickly, evolving the system to meet the needs of many trainees through universal design, curricular changes or enhanced flexibility within a system to allow for completion of a medical degree in non-standard time.
5.6 데밍의 요점 6: 직무에 대한 교육 실시 5.6 Deming's point 6: Institute training on the job
의학교육의 사회적 책무는 국가적, 세계적 차원에서 환자와 의료 시스템의 요구사항에 대응하기 위한 노력과 능력을 의미합니다.27 2006년 장애인 권리 협약과 2011년 세계 장애 보고서에서 인권 원칙에 기반한 장애 교육을 보장하기 위한 제도를 강조했음에도 불구하고, 원칙적으로 정착되지 않았습니다.28-31 Medical education's social accountability implies a commitment and ability to respond to the requirements of patients and health care systems on a national and global scale.27Despite the Convention on the Rights of Persons with Disabilities in 2006, and the World Report on Disability in 2011 emphasising institutions to ensure disability training based on human rights principles, it has not percolated down in principle.28-31
의사들이 장애는 사회적 구성물이며, 교육이나 진료에서 장애를 인권의 부정이나 제한을 위한 정당한 근거로 삼아서는 안 된다는 점을 인식해야 할 필요성이 커지고 있습니다. 이러한 이유로 연구자들은 정의와 자율성을 구현하기 위해 의료 환경 내에서 장애 문화적 역량을 구현할 것을 요구해 왔으며, 인증 기관에 서한을 보내 BME와 PME에 이를 의무적으로 포함하도록 요청해 왔습니다. 그러나 장애 역량이 의학교육의 필수적인 부분이 되도록 사법 운동을 통해 변화를 이끌어내는 것은 소수의 열정적인 장애 인권 운동가들에게 달려 있는 경우가 많습니다.32-37 데밍의 institute training on the job 철학을 실현하고 법적 의무를 이행하기 위해서는 장애 역량으로서 장애 권리에 대한 의학교육자의 의무적인 교육과 더불어 장애 의식을 가르치려는 열망,38 데밍의 포인트 5와 6을 바탕으로 맥락 내에서의 장애에 대한 이해를 일관되고 지속적으로 성장시키는 것을 목표로 삼아야 합니다. 또한 장애를 '극복'한 것으로 간주하는 장애 포용 철학에서 교육기관이 장애 교육생을 다양한 학습자 커뮤니티의 일원으로 예상하고 정상화하는 철학으로 조정되어야 합니다. There is a growing need for physicians to realise that disability is a social construct, and be it in teaching or practice, disabilities must not be taken as a legitimate ground for the denial or restriction of human rights. On this account, researchers have been calling for disability cultural competencies within health care settings to implement justice and autonomy and statutory bodies writing to accreditation bodies to mandatory include it in the BME and PME. Yet, more often than not, the onus lies on a few passionate disability rights activists to bring change through judicial activism to ensure disability competencies are a mandatory part of medical education.32-37To realise Deming's philosophy ofinstitute training on the job, and to fulfil legal obligations, there must be mandatory training of medical educators on disability rights as disability competencies as well as an aspiration to teach disability consciousness,38which draws on Deming's Points 5 and 6; to consistently and continually aim to grow in our understanding of disability in context. In addition, the philosophy of disability inclusion must be adjusted from one where disabled trainees are viewed as having ‘overcome’ disability to one where institutions anticipate and normalise disabled trainees as part of the community of diverse learners.
5.7 데밍의 요점 7: 리더십 채택 및 제도화 5.7 Deming's point 7: Adopt and institute leadership
의학계 전반에 걸쳐 장애 포용에 대한 행동 촉구에도 불구하고, 이러한 요구를 실행 가능한 조치로 전환하고 장애인 인구의 성장을 환영하고 지원하며 촉진하는 환경을 조성하는 데 실패하고 있습니다. 실제로 교육 접근성에 대한 지속적인 보고는 앞서 언급한 가이드라인이 널리 채택되지 않았다는 증거입니다.39-41 Despite calls to action on disability inclusion across medical associations, there exists a failure to translate these calls into actionable steps and to create environments that welcome, support and foster growth in the disabled population. Indeed, continued reports of inaccessibility in training stand as evidence that the aforementioned guidelines are not widely adopted.39-41
연구자들은 사명 선언문을 뛰어넘는 모범 사례를 제안했습니다.3, 42 장애 포용에 성공하려면 시스템의 모든 이해관계자, 특히 리더십이 목적에 전념해야 합니다. 데밍의 기관 리더십 철학은 기관이 조직 전반에 걸쳐 양질의 포용성을 수용하고 최고 수준의 리더십이 장애 커뮤니티의 정보를 바탕으로 측정 가능한 변화를 가져오는 데 전념할 때만 달성할 수 있습니다. 그들은 '우리 없이는 아무것도 없다'는 장애 포용의 모토에 따라 행동해야 하며, 대의에 대한 헌신과 목표 달성을 위한 실행 가능한 계획을 커뮤니티에 전달해야 합니다. Researchers have suggested best practices to move beyond mission statements.3,42If we are to excel at disability inclusion, all stakeholders in the system must be committed to the purpose, especially leadership. Deming's philosophy ofinstitute leadershipcan only be achieved; however, if institutions embrace quality inclusion throughout the organisation and where the highest levels of leadership are committed to bringing about measurable change, informed by the disability community. They must act in line with the disability inclusion mantra, ‘nothing about us, without us’ and communicate to the community their commitment to the cause and an actionable plan to reach the goal.
5.8 데밍의 요점 8: 두려움을 몰아내세요 5.8 Deming's point 8: Drive out fear
의대 교육자 및 지도자, 학생에게 두려움은 장애 포용을 방해할 수 있습니다. 수련의 관점에서 볼 때 의과대학 입학 지원 절차는 좋은 지원자에 대한 제한적인 시각을 유지합니다. 수련생들은 의대 프로그램이 좋은 의사를 몸이 불편하지 않은 사람으로 간주한다고 보고합니다. 이상적인 의대 지원자이자 미래의 의대 수련의는 '엄격한 학업 요구와 적극적인 사회적 헌신을 병행하면서 우수한 평가를 유지하는 사람'입니다.41 의대 입학의 경쟁적 특성을 고려할 때, 많은 수련의는 공개에 대한 두려움에 시달리며 장애와 같이 결점으로 간주될 수 있는 정보를 공유하지 않도록 권장될 수 있습니다. 접근하기 어려운 지원서 양식, 의과대학 입학 시험에서 편의 제공 부족, 의사 섀도잉에 대한 불공평한 접근, 입학 위원회에 대한 반장애인주의 교육 부족 등 입학 절차 자체가 부담스러울 수 있습니다.15, 21, 22 For medical educators and leaders, and students, fear may stall disability inclusion. From the trainee perspective, the application process for medical school entry retains restrictive views of a good applicant. Trainees report that their programmes view the good doctor as someone who is not unwell. The ideal medical applicant and future medical trainee is someone who ‘juggles rigorous academic demands with active social commitments while maintaining excellent evaluations’.41Given the competitive nature of medical school admissions, many trainees are driven by fear of disclosure and may be encouraged not to share information that might be considered a deficit, like a disability. The admissions process itself may prove burdensome, with inaccessible formats for application, lack of access to accommodation on medical school entry examinations, inequitable access to physician shadowing and lack of anti-ableist training for admissions committees.15,21,22
반대로, 입학 위원회, 교수진 및 관리자는 미지의 영역에 대한 두려움으로 장애인이 의학 분야에 적합하지 않다고 잘못 판단할 수 있습니다. 장애 포용을 장려하기 위해서는 프로그램이 장애를 공개하고 편의를 요청할 수 있는 안전한 공간이라는 신뢰와 명확한 이해를 통해 학습자의 두려움을 없애야 합니다. 교육 프로그램에서 장애를 가진 의사의 실제 성공 사례를 공유하면 두려움을 없애는 데 직접적인 도움이 될 수 있습니다. Conversely, admissions committees, faculty and administrators may fear the unknown, and may falsely believe that individuals with disabilities are not well suited for a career in medicine. In order to encourage disability inclusion, fear must be driven out of learners through trust and a clear understanding that the programme is a safe space to disclose and request accommodations. For training programmes, sharing success stories of physicians with disabilities in practice can help directly drive out fear.
5.9 데밍의 요점 14: 변화는 모두의 일이다 5.9 Deming's point 14: The transformation is everybody's job
행동 촉구에도 불구하고 의학교육에 장애를 포용하고 의학교육 내 장애 커리큘럼에 대한 글로벌 지침이 부족합니다. 교육 기관의 모든 구성원은 장애 접근성에서 각자의 역할을 수행하며, 자신이 교육 기관의 장애 접근성이라는 큰 그림에 어떻게 부합하는지 이해해야 합니다. 장애 접근은 또한 장애 정보를 제공해야 합니다. 장애인 수련의에 대한 동등한 접근은 환자와 의료 제공자 모두에서 세계에서 가장 큰 소수인 장애인의 요구를 해결하지 않는 한 달성할 수 없습니다. 데밍에 따르면 이러한 결함[오류]은 학습의 기회로 보아야 합니다. 변화는 우리 모두의 일이므로, 최근 의학교육에서의 장애 포용을 위한 국제위원회43 가 출범하고 국제적으로 장애 편의시설을 마련하기 위해 노력하는 것은 환영할 만한 움직임이며, 지침이 없는 국가에 다가갈 수 있도록 WFME 지역 협회의 적극적인 참여가 필요합니다.1, 2, 44 Despite calls to action, we lack global guidance on disability inclusion in medical education and disability curriculum within medical education. Each person in the institution plays a role in disability access and should understand how they fit into the larger picture of institutional access. Disability access must also be disability informed. Equal access for disabled trainees, will not be achieved until and unless we address the needs of the world's largest minority—people with disabilities—both as patients and providers. These deficiencies[errors]must beseen as learning opportunities, per Deming. Astransformation is everyone's job, the recent launch of the International Council for Disability Inclusion in Medical Education43and its work on producing disability accommodations internationally is a welcome move and needs active participation from the WFME regional associations to reach out to nations with no guidance.1,2,44
6 결론 6 CONCLUSION
WFME는 품질 개선을 위한 글로벌 표준 3부작을 제시했습니다. 우리는 장애 포용의 질을 개선하기 위해 QI 개입을 사용할 수 있는 여러 지점을 제공했습니다. 인권의 관점에서 장애를 바라보고, 합리적인 편의에 대한 표준화된 접근과 이해를 제공하고, 시스템의 모든 이해관계자에게 교육을 제공하면 장애 포용을 향한 문화와 분위기가 인간화될 수 있습니다. 보다 다양한 보건 전문 인력은 건강 결과를 개선하고, 건강 격차를 완화하며, 장애를 포용하고 접근 가능하며 공평한 보건 전문 교육, 훈련 및 실습으로 이어질 수 있습니다. WFME has given the trilogy of Global Standards for Quality Improvement. We provided multiple points where QI intervention can be used to improve the quality of disability inclusion. Viewing disability from the human rights perspective, providing standardised access and understanding of reasonable accommodation and providing training to all stakeholders in the system may result in humanising the culture and climate towards disability inclusion. A more diverse health professional workforce can improve health outcomes, mitigate health disparities and lead to disability-inclusive, accessible and equitable health profession education, training and practice.
Med Educ. 2023 Jan;57(1):102-107.doi: 10.1111/medu.14878.Epub 2022 Jul 24.
Disability inclusion in medical education: Towards a quality improvement approach
The issue:The shift to a more diverse workforce that includes physicians with disabilities has gained considerable international traction. Indeed, disability inclusion is experiencing a renaissance in medical education. However, the philosophy of disability inclusion must be adjusted from one where disabled trainees are viewed as problematic and having to 'overcome' disability to one where institutions anticipate and welcome disabled trainees as a normative part of a diverse community.
Observations:Most trainees with disabilities will enter an unregulated, uninformed system leaving them vulnerable to under-accommodation, systems barriers and lack of informed support. Further, the perception of the super human good doctor creates disincentives for candidates to disclose their disability, creating structural barriers that the system needs to address. A less often discussed contributor to health care inequities is the inadequate training of health professional educators on disability rights and disability competencies. Indeed, the lack of education, coupled with minimal exposure to disability outside of the hierarchical patient-provider relationship, perpetuates to stereotypes and biases that impact clinical care.
Approach:Disability inclusion has not been reviewed through the lens of quality improvement. To close this gap, we examine the state of the science through the lens of disability inclusion and offer considerations for a quality improvement approach in medical education that addresses the global revised trilogy of World Federation for Medical Education standards of quality improvement at all three levels of education, training and practice.
Conclusion:We propose a vision of systems-based disability-inclusive, accessible and equitable medical education using 9 of Deming's 14 points as applicable to medical education.
의학교육에서 장애 역량 훈련(Med Educ Online.2023) Disability competency training in medical education (Med Educ Online.2023) Danbi Leea,b, Samantha W. Pollackb, Tracy Mroza,b, Bianca K. Frognerb and Susan M. Skillmanb
소개 Introduction
장애인은 건강 상태와 의료 서비스에서 지속적인 격차를 경험합니다. [1,2,3] 적절한 의료 서비스를 가로막는 다단계 장벽의 핵심은 장애인의 다양한 경험과 필요에 대한 의료 서비스 제공자의 인식과 교육 부족, 부정적인 태도와 가정입니다[4,5]. 장애인은 접근하기 어려운 공간 및 장비, 의사소통 부족, 치료 결정 시 기존 장애 또는 기능적 상태를 고려하지 않는 등 의료 제공자의 장애 친화적 진료 부족으로 인해 양질의 의료 서비스를 이용하는 데 어려움을 겪고 있습니다[6-8]. 의사를 포함한 25,000명 이상의 의료 서비스 제공자를 대상으로 한 최근 연구에 따르면 60% 이상이 장애인에 대한 자신의 암묵적인 편견을 인식하지 못하고 있는 것으로 나타났습니다[9]. 그러나 문헌에 따르면 의료 서비스 제공자들은 장애에 대한 부정적인 태도와 특정 임상 및 접근 요구 사항을 포함한 장애인의 광범위한 의료 요구 사항을 다루는 제한된 교육만 받고 있습니다[10-13]. People with disabilities experience persistent disparities in health status and health care. [1,2,3] Central to the multilevel barriers to adequate health care are the lack of awareness and training among health care providers about the varied experiences and needs of individuals with disabilities, as well as negative attitudes and assumptions [4,5]. People with disabilities continue to experience challenges in accessing quality health care because of lack of disability-competent care by providers such as inaccessible space and equipment, poor communication, and not considering existing disability or functional status in making treatment decisions [6–8]. A recent study of over 25,000 health care providers, including physicians, found that more than 60% were unaware of their own implicit bias against people with disabilities [9]. Yet, literature shows that providers receive only limited training addressing negative attitudes towards disability and the wide range of health care needs of people with disabilities including specific clinical and access needs [10–13].
2017년에 발표된 미국 의과대학 장애 커리큘럼을 검토한 결과, 장애 역량을 통합하는 수준은 여전히 이질적이며 주로 노출에 기반한 것으로 나타났으며 종단적 모델을 제공하는 학교는 소수에 불과했습니다[12]. 여기에는 강의 및 단일 코스와 같은 교훈적인 방법부터 사무직 로테이션 중 표준화된 장애 환자 포함, 6주 통합 사무직 경험, 위의 모든 방식과 4년간의 장애 중심 선택적 사무직에 대한 옵션이 포함된 4년 통합 장애 커리큘럼에 이르기까지 다양합니다. 의학교육에서 장애에 대해 무엇을 가르쳐야 하는지에 대한 합의가 부족하기 때문에 장애 커리큘럼 제공의 다양성은 내용에도 영향을 미칩니다[14]. A review of published U.S. medical school disability curricula in 2017 found that the level of integrating disability competency remained to be heterogeneous and primarily exposure-based with only a few schools providing a longitudinal model [12]. These range from didactic methods like lectures and single courses, to the inclusion of standardized patients with disabilities during clerkship rotations; 6-week integrated clerkship experiences; and 4-year integrated disability curriculum that included all of the above modalities and the option of attending a 4th-year disability-focused elective clerkship. The variability in delivering disability curricula also extends to content as there has been lack of agreement on what to teach about disability in medical education [14].
이러한 격차를 인식하고 2019년에 보건의료 교육 장애 연합은 장애 관련 콘텐츠와 경험을 보건의료 교육 및 훈련 프로그램에 통합하는 것을 촉진하기 위해 보건의료 교육 장애에 관한 핵심 역량(핵심 역량)을 발표했습니다[15]. 다양한 보건의료 분야의 보건의료 교육자, 교수진 및 전문가로 구성된 연합 회원들은 역량 초안을 작성하고 140명의 장애 전문가 및 보건교육자로부터 두 차례에 걸친 반복적인 프로세스를 통해 피드백을 받았습니다. 2년에 걸친 이 과정을 통해 장애의 사회적, 환경적, 신체적 측면에 대한 보건의료 교육 표준을 제공하는 6개의 핵심 역량과 49개의 하위 역량(표 1)이 도출되었습니다[14,15]. 이러한 핵심 역량이 의학교육에서 다루어지고 있는지 여부와 그 방법을 조사한 연구는 아직 없습니다. 이 연구는 미국의 의학교육 프로그램에서 핵심역량이 어느 정도 다루어지고 있는지, 그리고 교과과정 통합을 확대하는 데 있어 촉진요인과 장벽이 무엇인지 살펴보는 것을 목표로 했습니다. Recognizing this gap, in 2019, the Alliance for Disability for Health Care Education published Core Competencies on Disability for Health Care Education (Core Competencies) to promote the integration of disability-related content and experiences into health care education and training programs [15]. Members of the alliance composed of health care educators, faculty and professionals across different health care disciplines drafted the competencies and received feedback through a two-wave iterative process from 140 disability experts and health educators. This two-year process resulted in six core competencies and 49 sub-competencies (Table 1) that provide health care education standards on social, environmental, and physical aspects of disability [14,15]. There has yet been a study that examined whether and how these Core Competencies are addressed in medical education. The study aimed to explore the extent the Core Competencies are addressed in medical education programs in the U.S. and the facilitators and barriers to expanding curricular integration.
이 연구는 순차적 혼합 방법 설계를 사용하여 온라인 설문조사에 이어 정성적 인터뷰를 진행했습니다. 문제에 대한 보다 심층적이고 완전한 이해를 제공하기 위해 양적 및 질적 데이터를 모두 수집했습니다[16]. 이 연구는 워싱턴대학교 기관생명윤리심의위원회(IRB# MOD00007591)에서 면제를 결정했습니다. The study used a sequential mixed-methods design, where an online survey was followed by qualitative interviews. Both quantitative and qualitative data were collected to provide a more in-depth and complete understanding of the problem [16]. This study was determined to be exempt by the University of Washington Institutional Review Board (IRB# MOD00007591).
설문지 Questionnaire
23개 항목으로 구성된 설문지는 장애 연구(DL), 의료 서비스(TM, BF, SS, SP), 의료 인력(DL, TM, BF, SS, SP) 연구 분야의 전문가로 구성된 다학제 프로젝트 팀에 의해 개발되었습니다. 객관식 질문은 현재 커리큘럼에서 어떤 핵심 역량이 다루어지고 있는지, 학교에서 장애 콘텐츠를 커리큘럼에 통합하는 데 있어 어떤 촉진자와 장벽이 있는지, 장애인이 어떻게 참여하고 있는지 파악하기 위해 사용되었습니다. 핵심 역량에 매핑된 학습 활동의 세부 사항(예: 이름, 내용/주제, 형식, 필수/선택 사항, 활동 시기)을 수집하기 위해 개방형 질문이 사용되었습니다. 예비 설문조사 문항은 장애 교육에 전문성을 갖춘 의과대학 교수진과 장애인의 공평한 의료 서비스를 옹호하는 장애인 단체의 장애인 전문가 등 6명의 전문가로 구성된 자문 패널에 의해 파일럿 테스트 및 검토를 거쳤습니다. 이후 이들의 피드백을 바탕으로 설문지를 수정했습니다. A 23-item questionnaire was developed by a multidisciplinary project team of experts in the research areas of disability studies (DL), health services (TM, BF, SS, SP), and health workforce (DL, TM, BF, SS, SP). Multiple-choice questions were used to identify which Core Competencies are currently addressed in the curriculum; what facilitators and barriers schools experience in to incorporating disability content into the curriculum; and how people with disabilities are involved. Open-ended questions were used to gather details of learning activities mapped to the Core Competencies (i.e., name, content/topic, format, required/optional, and timing of the activity). Preliminary survey questions were pilot-tested and reviewed by an advisory panel of six experts including faculty from medical schools with expertise in disability education and experts with disabilities from disability organizations advocating for equitable health care of people with disabilities. The survey was then revised based on their feedback.
설문조사는 2019학년도 현재 예비 또는 잠정 인증 상태를 유지하고 있는 프로그램을 포함하여 미국의 모든 동종요법 및 정골요법 의과대학(n = 196개)에 배포되었습니다. 2020년 2월부터 6월 사이에 커리큘럼 학장, 학부 교육 학장, 프로그램 디렉터에게 이메일 초대장과 6차례의 리마인더를 보냈습니다. 설문조사 응답의 데이터 수집에는 REDCap(Research Electronic Data Capture)이 사용되었습니다[17]. The survey was distributed to all allopathic and osteopathic medical schools in the U.S. (n = 196), including programs with preliminary or provisional accreditation status as of the 2019 academic year. Email invitations and six reminders were sent to curriculum deans, deans of undergraduate education, and program directors between February and June 2020. Research Electronic Data Capture (REDCap) was used for data collection of survey responses [17].
질적 인터뷰 Qualitative interviews
질적 인터뷰 대상자는 설문조사 응답자 중에서 다양한 지역의 의과대학을 대표할 수 있도록 의도적으로 선정되었습니다. 제1저자와 제2저자는 반구조화된 인터뷰 가이드를 사용하여 Zoom을 통해 30~60분간 개별 인터뷰를 진행했습니다. 설문조사 결과를 바탕으로 설문조사에 기술된 학습 활동과 장벽 및 지원 사항을 더 잘 이해할 수 있도록 설계된 인터뷰 가이드(표 2)를 작성했습니다. 인터뷰 가이드는 동일한 다학제 프로젝트 팀에서 개발했습니다. 인터뷰에 앞서 참가자들은 연구 참여에 대한 사전 동의를 제공했습니다. 동의한 참가자에게는 장애 콘텐츠가 포함된 학습 활동과 그것이 학생에게 미치는 영향, 학습 활동을 시작하고 유지하는 데 도움이 되는 요소, 더 많은 통합을 가로막는 장벽에 대해 설명해 달라는 요청을 받았습니다. 인터뷰는 허가를 받아 녹음되었습니다. Qualitative interviewees were purposefully selected from survey respondents to represent medical schools from different regions. Thirty to sixty-minute individual interviews were conducted by the first and second authors via Zoom using a semi-structured interview guide. Informed by the survey findings, the interview guide that was designed to better understand the learning activities and barriers and supports described in the survey (Table 2). The interview guide was developed by the same multidisciplinary project team. Prior to the interview, participants provided informed consent to their research participation. Consented participants were asked to describe learning activities with disability content and their impact on students, facilitators to initiating and maintaining learning activities, and barriers to integrating more. Interviews were recorded with permission.
데이터 분석 Data analysis
O'Cathain 외[18]가 제안한 데이터 삼각측량 프로토콜에 따라 데이터를 먼저 개별적으로 분석한 다음 해석 단계에서 통합했습니다. 먼저, 의과대학에서 어떤 핵심역량을 얼마나 많이 다루고 있는지, 장애인이 어떻게 참여하고 있는지, 어떤 지원과 장벽이 존재하는지 파악하기 위해 서술적 통계를 사용하여 설문조사 데이터를 분석했습니다. 개방형 질문에 기술된 학습 활동의 세부 사항(예: 학습 활동의 유형, 초점, 길이, 빈도)을 코딩하고 정성적, 정량적으로 요약했습니다. 그런 다음 개별 인터뷰의 메모와 녹취록을 주제 분석을 사용하여 분석했습니다[19]. 주제는 연구팀과 논의했습니다. 코딩-재코딩, 데이터 삼각측량, 데이터의 두꺼운 기술, 반성성(장애인으로서의 입장에 대한 끊임없는 성찰과 토론)을 통해 신뢰성, 전달성, 확인성을 확보했습니다. 마지막으로 해석의 깊이를 더하기 위해 양적 데이터와 질적 데이터의 결과를 비교하고 수렴성, 상호보완성, 불일치성을 검토했습니다[18].
Following the data triangulation protocol suggested by O’Cathain et al. [18], data were first analyzed separately then integrated at the interpretation stage. First, survey data were analyzed using descriptive statistics to identify which and how many Core Competencies were addressed in medical schools, how people with disabilities are involved, and what supports and barriers exist. Details of the learning activities described in the open-ended questions were coded (e.g., types, focus, length, and frequency of the learning activities) and summarized qualitatively and quantitatively. Then, notes and transcripts from the individual interviews were analyzed using thematic analysis [19]. Themes were discussed with the research team. Credibility, transferability, and confirmability were ensured through coding-recoding, data triangulation, thick description of data, and reflexivity (i.e., constant reflection and discussion regarding positionality as persons without disabilities). Finally, to add depth to the interpretation, results from quantitative and qualitative data were compared and examined for convergence, complementarity, and discrepancy [18].
결과 Results
참가자 Participants
총 14개 프로그램에서 설문조사를 완료했습니다. 대부분의 응답자는 대규모 코호트를 보유한 동종요법 공립 의과대학이었습니다(표 3). 5명의 의과대학 대표가 질적 인터뷰에 참여했습니다. 여기에는 미국의 4개 인구조사 지역을 대표하는 사립 의과대학 1개와 공립 의과대학 4개가 포함되었습니다. A total of 14 programs completed the survey. Most respondents were allopathic public medical schools with larger cohorts (Table 3). Five medical school representatives participated in the qualitative interview. This included one private and four public medical schools representing four U.S. census regions.
조사 결과 Findings
설문조사와 질적 인터뷰 결과를 통합하여 두 가지 주제 영역으로 분류했습니다:
1) 핵심 역량을 다루는 장애 역량 교육 현황,
2) 장애 역량 교육을 통합하는 데 있어 장벽과 촉진 요인.
특히 질적 데이터를 통해 다음에 대해 보다 심층적으로 이해할 수 있었습니다.
1) 커리큘럼 구조와 시간이 핵심역량 통합에 미치는 영향,
2) 자원과 챔피언의 중요한 역할
Integrated, the results from the survey and qualitative interviews were categorized into two topic areas: 1) status of disability competency training addressing the Core Competencies and 2) barriers and facilitators to integrating disability competency training. Qualitative data particularly provided more in-depth understanding on 1) the influence of curricular structure and time on integrating Core Competencies and 2) the crucial role of resources and champions.
핵심 역량을 다루는 장애 역량 교육 현황 Status of disability competency training addressing the Core Competencies
14개 학교 중 11개 학교가 교육과정에서 5~6개의 핵심 역량을 다루고 있다고 응답했습니다(표 4). 대부분의 학교(n=13)는 장애에 대한 맥락 및 개념적 프레임워크와 팀 및 시스템 기반 실무에 대해 다루고 있다고 답했습니다. 법적 의무와 책임에 관한 역량은 가장 적게 다루고 있었습니다(n = 6). Eleven out of 14 schools reported that their curriculum addresses five to six Core Competencies in their curriculum (Table 4). Most schools (n = 13) said that they address contextual and conceptual frameworks on disability and teams and systems-based practice. Competencies around legal obligations and responsibilities were least addressed (n = 6).
장애 역량 교육의 정도는 다양했습니다. 의과대학의 약 절반은 커리큘럼에 한두 가지 학습 활동이 있다고 답했고, 나머지 절반은 세 가지 이상의 학습 활동이 있다고 답했습니다. 대부분의 학습 활동은 일회성 환자 패널 또는 환자 시뮬레이션과 같이 45분~2시간의 단일 세션으로 제공되었습니다. 일부는 2년 이상의 통합 사례, 1년 이상의 주간 시뮬레이션, 4주간의 임상 로테이션 등 여러 과정과 장기간에 걸쳐 통합된 더 긴 학습 활동도 있었습니다. 고급 배치 또는 임상 로테이션과 같은 연장된 경험은 선택 사항이었지만 대부분의 학습 활동은 필수였습니다. 4학년의 임상 로테이션과 3학년의 몇 가지 환자 대면을 제외하고 보고된 모든 학습 활동은 의학교육의 첫 2년 동안 완료되었습니다. The extent of disability competency training varied. About half of the medical schools reported one or two learning activities within their curriculum; the other half described three or more learning activities. Most learning activities described were offered in single 45-minute to 2-hour sessions such as one-time patient panels or patient simulations. Some were longer and more integrated across different courses and extended time periods, including integrated cases over 2 years, weekly simulations over a year, and 4-week clinical rotations. The majority of learning activities were required although most of the extended experiences such as advanced placement or clinical rotations were optional. Except for the clinical rotations in year 4 and a few patient encounters in year 3, all learning activities reported were completed during the first two years of medical education.
학습 활동에는 강의, 사례 연구, 패널 토론, 소그룹 토론이 포함되었습니다. 많은 학교에서
장애에 대한 인식을 높이기 위해 다양한 장애 모델, 능력주의, 암묵적 편견과 같은 주제를 논의하고,
장애 에티켓과 임상 평가 또는 다학제 진료에서 장애인과 상호작용하는 방법을 다루었으며,
환자 패널을 통해 장애인의 생생한 경험에 대해 배울 수 있는 기회를 제공했습니다.
일부 학교에서는 재활의 맥락에서 의학적 상태로서의 장애에 대해 배우거나(예: 재활 현장 방문, PM&R 임상 로테이션) 의학적 맥락에서 장애 관련 진단(예: 뇌성마비, 치매)을 이해하는 데 중점을 둔 활동을 보고했습니다. 장애인 또는 표준화된 환자와의 일회성 만남 및 시뮬레이션이 더 일반적이었으며, 장애 커뮤니티와의 현장 프로젝트 또는 장애인과의 장기 임상 경험과 같은 몰입형 체험 학습 기회를 제공하는 학교는 더 적었습니다. 핵심 역량과 연계된 학습 활동의 구체적인 예는 표 4에 나와 있습니다. The learning activities included lectures, case studies, panel discussions, and small group discussions. Many
discussed topics such as different disability models, ableism, and implicit bias to raise awareness of disability;
addressed disability etiquette and how to interact with people with disabilities in clinical assessments or in interdisciplinary care; and
provided opportunities to learn about the lived experiences of people with disabilities through patient panels.
Some schools reported activities focused on learning about disability as a medical condition within the context of rehabilitation (e.g., visiting rehabilitation sites, clinical rotation in PM&R) or understanding disability-related diagnoses (e.g., cerebral palsy, dementia) in a medical context. One-time encounters and simulations with people with disabilities or standardized patients were more common, and less schools offered immersive experiential learning opportunities such as a field project with disability communities or extended clinical experiences with people with disabilities. Specific examples of learning activities linked to the Core Competencies are listed inTable 4.
의과대학 커리큘럼에서 신체적 장애를 가장 많이 다루고 있었으며(n = 13), 감각 장애에 대한 논의는 가장 적었습니다(n = 9). 또한 설문조사 결과에 따르면 장애인은 패널(n = 9) 또는 환자(n = 7)로서 학습 활동에 참여하는 경우가 많았으며, 교육(n = 4) 또는 커리큘럼 활동 계획(n = 4)에 참여하는 역할은 적었습니다. 3개 학교는 장애인이 전혀 참여하지 않았다고 보고했습니다. (표 5 참조) Most frequently, the medical school curricula addressed physical disability (n = 13) while sensory disabilities were least discussed (n = 9). The survey result also shows that people with disabilities were often engaged in learning activities as panelists (n = 9) or patients (n = 7) with less of a role in teaching (n = 4) or planning curricular activities (n = 4). Three schools reported no involvement of individuals with disabilities. (seeTable 5)
설문조사 결과와 유사하게, 주요 정보 제공자들과의 질적 인터뷰에서는 패널과 함께하는 짧은 독립 세션, 시뮬레이션 또는 특정 주제를 다루는 토론과 관련된 학습 활동이 많이 논의되었습니다. 인터뷰 참여자들은 패널과 환자와의 만남이 종종 학생들이 좋아하고 긍정적인 영향을 미친다고 언급했습니다. Similar to the survey results, in the qualitative interviews with key informants, many learning activities discussed involved short independent sessions with panels, simulations, or discussions that address particular topics. Interviewees noted that panels and patient encounters are often liked by students and have a positive impact.
... 학생들은 이러한 세션이 끝난 후 훨씬 더 자신감이 생겼다고 말했습니다... [장애] 환자와 함께 방에 들어가서 어떻게 행동해야 하는지 알고, 때로는 조금 어색할 수 있지만 괜찮습니다... 에티켓과 H&P(병력 및 신체 검사) 방법에 대해 염두에 두고 환자에게 물어보십시오. (CS1) … students have voiced that they feel a lot more confident after these sessions … going into the room with a patient with [disabilities], knowing how to act, and kind of owning that sometimes, yeah, you’re going to feel a little awkward, that’s ok … be mindful of etiquette and how you go about an H&P [history and physical examination], you know, ask the patient. (CS1)
그러나 이러한 교육은 일반적으로 커리큘럼 전체에 걸쳐 한 번만 제공되기 때문에 많은 인터뷰 대상자가 충분하지 않다고 설명했습니다. 일부 인터뷰 참여자들은 4년 동안 여러 곳에서 장애에 대해 이야기하는 것이 중요하다고 강조했습니다. '커리큘럼에 장애를 더 많이 포함시키는 더 좋은 방법은 장애인 사례를 곳곳에 배치하는 것이라고 생각합니다...' 몇몇은 다양성 및 건강 격차 논의에 장애 내용을 엮는 방법에 대해 언급했습니다. 한 학교는 3학년과 4학년 가정의학과 및 내과 실습에 다양성 및 의료 격차 스레드의 일부로 장애 관련 학습 이벤트 두 개를 포함했습니다. 또 다른 인터뷰 참여자는 다음과 같이 말했습니다, However, because they were typically offered only once throughout the curriculum, many interviewees described those as not enough. Some interviewees stressed the importance of talking about disability in multiple places throughout the four years: ‘I think a better way to get more disability into the curriculum would be to put more examples of people with disabilities…peppered throughout…’ A few mentioned how they weave disability content into the diversity and health disparities discussion. One school included two disability-related learning events as part of their diversity and health care disparities thread in their 3rdand 4thyear family medicine and internal medicine clerkships. Another interviewee shared,
우리는 ... 자폐증 패널과 모의 환자 만남을 ... 커리큘럼의 일부에서 집단 내 환자에 대해 이야기하고 있습니다 ... 저는 장애가 [건강의 사회적 결정 요인을 이해하는] 이 맥락에서 전적으로 적절하다는 사례를 만들 수 있었습니다... (CS2). We have … the autism panel and the simulated patient encounter … in a part of the curriculum where they’re talking about patients within populations … I was able to make the case that disability is totally appropriate in this context [of understanding social determinants of health] … (CS2)
처음 2년 동안만 학습 활동을 한 참가자들은 이후 임상에서 정보를 다시 연결시키는 반복적인 경험이 부족하다는 데 동의했습니다: '[T]3년차와 4년차에는 사람들이 반드시 모여서 첫 2년 동안 배운 내용을 되돌아볼 수 있는 기회가 없기 때문에... 완전히 적중하거나 놓치는 경우가 있습니다'(CS5). 또한 프로그램 구조가 장벽이 될 수 있다는 점을 인식했습니다. '[첫 18개월 이후에는] 학생들이 수백 개의 장소에 있기 때문에 교육 단계에서 지식을 쌓는 데 환자 경험을 활용할 수 없다고 생각합니다'(CS4). 하지만 이 참가자는 임상 실습 중에 장애 콘텐츠를 통합하기 위해 필수 온라인 강의를 사용할 수 있는 가능성을 제시했습니다. Participants who only had learning activities in their first two years agreed that an iterative experience tying back the information in later clinical years is missing: ‘[T]here’s nothing in the third and fourth year where people necessarily come together to think back on what they learned in the first two years … So it’s completely hit or miss what they get’ (CS5). They also recognized that program structure could be a barrier: ‘[after the first 18 months] I don’t think there is a capitalization on the patient experience to build their knowledge in their phases of training because [students] are in hundreds of locations’ (CS4). This participant yet expressed the potential of using required online lectures to integrate disability content during clerkships.
장애 역량 교육 통합의 장벽 및 촉진 요인 Barriers and facilitators to integrating disability competency training
표 6에서 볼 수 있듯이, 장애 역량 교육을 커리큘럼에 통합하는 데 가장 자주 확인된 촉진제는 교수진의 지지자(n = 11)였으며, 학술적 리더십의 지원(n = 8), 지역사회 기반 장애 단체와의 파트너십(n = 7)이 그 뒤를 이었습니다. 장애 학생, 교수진 또는 교직원이 프로그램에 참여하는 것도 장애 역량 교육의 통합에 긍정적인 영향을 미치는 것으로 보입니다. 가장 큰 장벽은 커리큘럼에 새로운 콘텐츠를 추가할 시간이 부족하다는 점(n = 10)이었으며, 리소스 부족(n = 5)이 그 뒤를 이었습니다. 일부 응답자는 촉진 요인(예: 교수진의 지지자, 장애인 단체와의 관계)의 부족도 장벽으로 보고했습니다. As seen inTable 6, the most frequently identified facilitator to incorporating disability competency training into curriculum was having a faculty champion (n = 11) followed by support of academic leadership (n = 8) and partnership with community-based disabilities organizations (n = 7). Having students, faculty, or staff with disabilities in the program also seems to positive affect the integration of disability competency training. An overwhelming barrier was lack oftime in the curriculum to add new content (n = 10), followed by inadequate resources (n = 5). Lack of factors identified as facilitators (e.g., faculty champion, relationship with disability organizations) was also reported as barriers by some respondents.
설문조사 결과와 일관되게, 모든 주요 정보 제공자들은 제한된 커리큘럼 시간을 확보하기 위한 경쟁이 더 많은 장애 역량 콘텐츠를 통합하는 데 가장 큰 어려움이라는 데 동의했습니다. 한 인터뷰 참여자는 '커리큘럼에서 발판을 마련하는 것이 정말 어렵습니다. 정말 어렵죠. 두 시간을 위해 싸워야 합니다. (CS5). 인터뷰에서는 장애 역량 교육을 커리큘럼에 통합하는 데 있어 교수진 또는 학생 챔피언이 있다는 점도 분명하게 드러났습니다. 챔피언은 대개 이 주제에 관심을 갖고 강의 자료를 개발하고 실행한 교수진이었습니다. 한 프로그램에서는 장애 형제가 있는 학생 챔피언이 학생들이 장애인 환자, 간병인 및 장애인과 함께 일하는 다른 의료 종사자들과 교류할 수 있는 선택 과목을 개설했습니다. 한 인터뷰 참여자는 휠체어를 사용하는 의사인 코스 디렉터가 의사로서 자신의 장애 경험에 대해 이야기해주기 때문에 '훌륭한 자산'이 되었다고 설명했습니다(CS1). Consistent with the survey result, all key informants agreed that competition for limited curriculum time is the biggest challenge to integrating more disability competency content. One interviewee said, ‘finding a foothold in the curriculum is huge. It’s really hard. You fight for your two hours.’ (CS5). In the interviews, it was also clear that having a faculty or student champion has been a force in integrating disability competency training into the curriculum. The champions were usually faculty members who were invested in this topic and who developed and carried out course materials. In one program, a student champion who has a sibling with a disability initiated an elective course where students have chances to interact with patients with disabilities, their caregivers, and other health care workers that work with people with disabilities. One interviewee described that having a course director who is a physician using a wheelchair has been a ‘wonderful asset’ because he would talk about his own disability experience as a physician (CS1).
질적 인터뷰를 통해 이러한 챔피언에 대한 지나친 의존이 얼마나 취약한지를 알 수 있었습니다. 휠체어 사용자인 의사의 은퇴가 다가오면 학생들이 그와 교류하고 배울 기회를 잃게 될 것이기 때문에 인터뷰 대상자는 이를 우려했습니다(CS1). 다른 사람들도 이러한 의견을 제시했습니다. 한 사람은 '[교수 챔피언이] 떠났을 때 재활의학과에 있는 누구와도 연결이 되지 않았습니다. 연락이 끊겼어요. (CS4). 한 인터뷰 대상자는 챔피언이 촉진자로 여겨지는 반면, 장애 역량 교육의 약점이라고 지적했습니다: 장애인 역량 교육 접근 방식이 항상 챔피언에 의존해 왔다는 점이 이 노력의 큰 약점이라고 생각합니다. 저는 그들[챔피언]이 할 수 있는 일에 대해 존경심을 가지고 있습니다... 하지만 지속 가능하지도 않고 확장 가능하지도 않습니다... 챔피언이 은퇴하자마자 콘텐츠와 커리큘럼에 판매 기한이 정해져 있는 것과 같습니다. 커리큘럼에 대한 수요의 힘을 견딜 수 없습니다. (CS2) The qualitative interviews also revealed the fragility of too much reliance on these champions. The upcoming retirement of the physician who is a wheelchair user was a concern of the interviewee because students would lose the opportunity to interact with and learn from him (CS1). This sentiment was also presented by others. One person said, ‘When [the faculty champion] left, I didn’t have a connection with anyone in rehabilitation. I lost those contacts.’ (CS4). While having a champion was seen as a facilitator, one interviewee pointed out how that is a weakness of disability competency training: I think that’s a huge weakness in this effort, that the disability training approach has always relied on champions. I have so much respect for what they [champions] are able to do … But, it’s not sustainable, and it’s not scalable … [A]s soon as the champion retires, there’s like a sell-by date on the content and the curriculum. It just cannot withstand the forces of the demands on the curriculum. (CS2)
인터뷰 참여자들은 또한 커리큘럼에 장애 콘텐츠를 통합하는 데 있어 기관의 지원과 리소스가 중요한 역할을 한다고 지적했습니다. 그들은 어떤 특정 리소스를 이용할 수 있고 어떻게 활용했는지에 대한 자세한 정보를 제공했습니다. 이러한 자원에는 다음 등이 포함되었습니다.
콘텐츠 개발을 위한 보호된 시간,
패널 또는 환자와의 만남 세션을 조정할 전담 직원,
패널 또는 표준화된 환자와 가족에게 지급할 자금,
환자 자원봉사자 모집을 위한 장애인 단체와의 연결
Interviewees also pointed to the critical role of institutional supports and resources in integrating disability content in the curriculum. They provided more information on what specific resources they had access to and how they utilized those. These resources included
protected time to develop content,
designated staff to coordinate panel or patient encounter sessions,
funds to pay panelists or standardized patients and families, and
connection to disability organizations to recruit patient volunteers.
환자와의 만남과 패널을 실행하는 데 필요한 리소스가 자주 지적되었습니다. 한 프로그램에서는 참가자의 접근성을 보장하기 위해 패널/시뮬레이션 세션을 지원하는 데 많은 직원이 참여했습니다(예: 자폐증 환자에게 적합한 환경, 시각 장애가 있는 환자 안내)(CS3). 일부의 경우, 리소스 부족으로 인해 모범 사례라고 생각했던 활동을 하지 못했습니다. '[문제 기반 학습]을 위해 퍼실리테이터를 위해 [장애인] 사람들을 모았는데...[제한된 리소스 때문에] 그 이후로 하지 못했습니다.'(CS5). (CS5). Resource needs for implementing patient encounters and panels have been frequently noted. One program had many of their staff involved in supporting the panel/simulation session to ensure accessibility of participants (e.g., appropriate environment for patients with autism, guiding patients with visual impairment) (CS3). For some, the lack of resources prevented activities they believed to be best practice: ‘I brought people [with disabilities] together for the facilitators for [problem-based learning]…[H]aven’t done it since because of limited resources.’ (CS5).
기대하는 효과에 적합한 패널리스트를 찾는 것은 때때로 어려운 일이었습니다. 일부 패널은 전달하고자 하는 다른 메시지(예: 총기 규제)를 가지고 있었기 때문에 한 참가자(CS4)는 '그들이 무슨 말을 할 지 모르겠다'고 말했습니다. 팬데믹으로 인해 패널 세션을 계획하는 데 시간을 내기가 어려워지자, 이 프로그램은 학생들이 장애인과 장애인 권리 운동의 생생한 경험을 접할 수 있는 방법으로 '크립 캠프' 다큐멘터리를 시청하고 성찰하는 것으로 대체했습니다. 인터뷰 대상자는 '잘 만들어진 영화가 메시지를 전달하는 데 더 효과적일 것 같다'고 말했습니다. Finding the right panelists for the hoped impact was sometimes a challenge. ‘I don’t know what they are going to say’ said one participant (CS4) as some panelists had other messages they wanted to communicate (e.g., gun control). When finding time for planning a panel session became a challenge due to the pandemic, this program replaced it with watching and reflecting on the ‘Crip Camp’ documentary, as a way to expose students to the lived experience of people with disabilities and the disability rights movement. The interviewee shared, ‘maybe a very well-done film will be more effective in bringing across the messages.’
일부 인터뷰 대상자는 장애인 단체 또는 다른 분야의 콘텐츠 전문가(예: 언어 병리학 및 물리 치료 교수진)와의 파트너십이 중요하다고 언급했는데, 이는 자신들이 이 주제에 대한 전문성을 갖추지 못했기 때문입니다. 그래서 그들[사무국장]은 그것[장애 콘텐츠]이 중요하다고 느꼈고... 아마도 [장애 단체]가 전문가이기 때문에 그들의 편에 서 있다는 것을 알고 훨씬 더 자신감을 느꼈을 것입니다. (CS1) Some interviewees mentioned the importance of having partnership with a disability organization or content experts from different disciplines (e.g., faculty from speech language pathology and physical therapy), as they did not have expertise in this topic. So they [clerkship directors] felt like it [disability content] was important and … probably felt a lot more confident knowing that [the disability organization] was in their corner, because they’re the experts. (CS1)
새로운 콘텐츠를 개발하기 위한 시간과 자원을 확보하기 위한 또 다른 방법으로 한 인터뷰 참여자는 외부 자금을 적극적으로 모색했습니다. 이 사람은 외부 지원금이 '첫 발을 내딛는 데' 도움이 된다고 말했습니다. 이 인터뷰 참여자는 콘텐츠가 개발되면 일반적으로 학생들에게 인기가 있고 보조금이 끝난 후에도 계속되는 경향이 있지만, 외부 자금이 없었다면 애초에 이러한 활동은 일어나지 않았을 것이라고 말했습니다: '큰 금액은 아니더라도 보조금을 제공하는 것은 의과대학의 협조를 구하는 측면과 실제로 콘텐츠를 개발하고 실행하는 측면에서 밤낮으로 힘든 일입니다.' (CS2) As another way to secure time and resources to develop new content, one interviewee actively sought external funding. This person reported that external grant helps ‘get a foot in the door.’ Once content is developed, those activities are typically popular with students and tend to continue after the grant ends, said this interviewee, but they would not happen in the first place without external funding: ‘Offering grants, even if it’s not a huge amount of money, is night and day in terms of getting cooperation from the medical school, and in terms of actually developing content and implementing.’ (CS2)
한 인터뷰 참여자는 핵심 역량을 의학교육 연락위원회(LCME) 인증 기준에 포함시키면 챔피언이나 자원이 없어도 장애 콘텐츠를 적극적으로 통합할 수 있다고 제안했습니다. One interviewee suggested that embedding the Core Competencies into the Liaison Committee on Medical Education (LCME) accreditation standards may lead to proactive integration of disability content even without a champion or resources.
토론 Discussion
이 연구에서는 의과대학이 커리큘럼에 핵심역량을 통합하는 정도와 통합을 방해하는 장벽 및 촉진 요인을 조사했습니다. 설문조사 응답에서 많은 학교가 대부분의 핵심 역량을 다루고 있다고 답했습니다. 장애 역량 교육의 정도는 의과대학 프로그램마다 차이가 있었으며, 대부분 장애에 대한 심도 있는 이해의 기회가 제한적인 것으로 나타났습니다. 대부분의 학교는 제한적이기는 하지만 장애인과 어느 정도 교류하고 있었습니다. 가장 빈번한 촉진자는 교수진이었으며, 더 많은 학습 활동을 통합하는 데 가장 큰 장벽은 커리큘럼 내 시간 부족이었습니다. 질적 인터뷰는 커리큘럼 구조와 시간의 영향, 교수진 챔피언과 자원의 중요성에 대한 더 많은 통찰력을 제공했습니다. The study explored the extent medical schools integrate the Core Competencies in their curriculum and the barriers and facilitators to the integration. In survey responses, many schools reported addressing most of the Core Competencies. The extent of disability competency training varied across medical programs with the majority showing limited opportunities for in-depth understanding of disability. Most schools had some, although limited, engagement with people with disabilities. Having faculty champions was the most frequent facilitator and lack of time in the curriculum was the most significant barrier to integrating more learning activities. Qualitative interviews provided more insight on the influence of the curricular structure and time and the importance of faculty champion and resources.
이전 문헌[11,12]과 일관되게, 의과대학에서 장애 역량 학습 활동의 형식과 기간은 다양했습니다. 이 연구에 참여한 대부분의 참가자들은 커리큘럼에서 여러 핵심 역량을 다루고 있다고 답했지만, 대부분의 역량이 한두 가지 학습 활동에서 다루어져 관련 주제에 대한 심도 있는 이해를 제공하지 못할 가능성이 높았습니다. 일회성 패널이나 환자와의 만남은 장애인과의 상호작용에 대한 학생의 자신감과 장애 경험에 대한 이해에 영향을 미칠 수 있지만, 이전 연구에 따르면 이러한 영향은 단기적이며[11,20] 장기적으로 장애인을 위한 임상 치료의 질 향상으로 이어지지는 않는 것으로 나타났습니다[16]. 특히 의료진의 암묵적인 편견이 장애인의 평등하고 질 높은 의료 서비스를 저해하는 요인이 될 수 있으므로 장애 문제에 대해 성찰하고 이를 접할 수 있는 기회를 자주 갖는 것이 중요합니다[9]. 또한 설문조사에 따르면 대부분의 활동이 첫 2년 동안 완료된 것으로 나타났습니다. 장애 관련 콘텐츠가 조기에 도입된 것은 긍정적이지만, 임상 진료와 관련된 역량은 학생들이 임상 상황에서 지식을 적용해야 하기 때문에 후반기에 주로 발생합니다. Consistent with previous literature [11,12], the format and length of disability competency learning activities in medical schools varied. Although most participants in this study reported that their curriculum addresses multiple Core Competencies, most competencies were addressed in one or two learning activities that is likely not providing an in-depth understanding of the related topics. While one-time panels or patient encounters can have an impact on student confidence in interacting with people with disabilities and their understanding of disability experiences, previous research found that this impact is short term [11,20] and does not translate into improved quality of clinical care for people with disabilities long term [16]. Especially, with health care provider’s implicit bias being a contributor to equal and quality healthcare for people with disabilities, frequent opportunities to reflect on and be exposed to disability issues are critical [9]. The survey also showed that most activities were completed in the first two years. It is positive that disability content was introduced early; however, competencies related to clinical care would require students to apply their knowledge in clinical context, which often occur in later years.
연구 참여자와 문헌에서 제안한 바와 같이, 오래 지속되는 혁신적 경험을 촉진하기 위해 의료 프로그램은 커리큘럼 전반에 걸쳐 종적, 반복적, 통합적 학습 활동을 고려해야 합니다[8,13,20]. 강의, 패널, 토론과 함께 몰입형 체험 학습 활동이 이상적입니다[8,21]. 그러나 제한된 자원과 시간 제약을 고려할 때, 기존 커리큘럼에 콘텐츠를 엮고 커리큘럼의 기존 사례를 수정하는 것이 장애 관련 내용을 전체적으로 통합하고 학생들의 장애 관련 임상 치료 역량을 촉진하는 데 더 현실적이고 효과적인 변화일 수 있습니다[20]. 사례 전반에 걸쳐 장애를 대표하고 다양성과 문화적 겸손의 맥락에서 장애에 대해 이야기하는 것을 일상화하면 미래의 의사들이 장애인과 함께 일할 때 명시적 및 암묵적 편견을 적극적으로 성찰하고 제거하는 데 도움이 될 수 있습니다[22]. 다양성 및 문화적 역량 논의에서 장애는 종종 누락됩니다[22]. 의학 프로그램이 장애 역량을 의학교육의 필수적인 부분으로 간주하고 커리큘럼 개선을 위한 투자를 하려면 LCME 표준에 장애를 문화적 역량의 일부로 명시적으로 포함하는 등 더 나은 제도화가 이루어져야 합니다[22]. As suggested by the study participants and literature, to promote long-lasting transformative experiences, medical programs should consider longitudinal, iterative, and integrated learning activities woven throughout the curriculum [8,13,20]. Along with lectures, panels, and discussions, immersive experiential learning activities would be ideal [8,21]. However, considering limited resources and time constraints, weaving content into existing curriculum and modifying existing cases in the curriculum may be more realistic and effective changes to make to integrate disability content throughout and to facilitate students’ competency in disability related clinical care [20]. Having disability representation throughout cases and normalizing talking about disability in context of diversity and cultural humility could help future physicians actively reflect on and work towards eliminating their explicit and implicit biases when working with people with disabilities [22]. Disability is often omitted from diversity and cultural competency discussions [22]. Better systemization, such as explicitly including disability as part the cultural competency in LCME standards, needs to be made for medical programs to view disability competency as an essential part of medical education and make the investment for improving curricular [22].
이 연구와 이전 출판물에서는 장애 역량 교육을 의학교육에 통합하기 위해 챔피언을 발굴해야 할 필요성을 강조했습니다[8,13]. 챔피언에 대한 의존도는 의과대학 전반에서 장애 교육의 다양성에 기여하는 요인으로 확인되었습니다[14]. 의과대학 전반에 걸쳐 장애학 전문 지식이나 실무 경험을 갖춘 교수진이 부족하다는 것은 강화된 LCME 표준이 적용되더라도 장애 역량을 가르치는 능력은 다양할 수 있기 때문에 문제가 됩니다. 비전문가도 쉽게 실행할 수 있는 수업 계획이나 리소스를 만들고 공유하는 데 더 많은 노력을 기울이면 이러한 다양성을 줄일 수 있습니다. 예를 들어, Borowsky 등은 능력주의, 장애의 사회적 모델, 장애의 역사와 문화, 건강 격차에 대해 논의하는 2시간짜리 참여형 수업 계획을 발표했습니다[23]. 필요한 모든 자료가 포함된 이 계획과 가이드는 지식이나 경험이 적은 사람들도 쉽게 실행할 수 있습니다. 그러나 가장 중요한 것은 장애 주제에 대한 대다수 교육자의 무능력과 옹호자의 부족은 장애인이 의료 교육과 진료에 더 쉽게 접근하고 포용할 수 있도록 인력을 다양화할 필요가 있음을 요구한다[22]. This study and previous publications have highlighted the need for identifying a champion to integrate disability competency training into medical education [8,13]. The dependency on champions has been identified as a contributor to variability in disability training across medical schools [14]. The lack of faculty with disability studies expertise or lived experiences across medical schools is problematic because even with a strengthened LCME standard, the ability to teach disability competency will vary. The variability may be reduced with more efforts in creating and sharing lesson plans or resources that can be easily implemented by non-experts. For example, Borowsky et al. published a participatory 2-hour lesson plan that discusses ableism, the social model of disability, disability history and culture, and health disparities [23]. With all materials needed, these plans and guides may be easy to implement for those with less knowledge or experience. Yet, most importantly, the incompetency of majority of educators in the topic of disability and lack of champions call for the critical need for diversifying the workforce by making medical education and practice more accessible and inclusive for individuals with disabilities [22].
이 연구에서 장애인은 주로 자문위원이나 강사가 아닌 패널리스트 또는 표준화 환자로 참여했습니다. 환자와의 만남은 표준화된 행위자보다 장애인과 그 가족을 통해 이루어지는 경우가 더 많았는데, 이는 장애인 커뮤니티에서 비판받는 접근 방식입니다[21]. 그러나 장애인 또는 장애인 커뮤니티의 참여에는 시간과 금전적, 인적 자원이 필요하기 때문에 종종 부담으로 인식되는 것으로 나타났습니다. 또한 지역 장애 커뮤니티와의 연결이 항상 챔피언 없이 구축되는 것은 아닙니다. 이 연구에 참여한 한 학교가 공유한 것처럼, 장애인의 직접적인 참여를 조정할 자원이 부족한 프로그램에서는 장애인 권리와 문화에 관한 다큐멘터리나 회고록을 활용하는 것이 좋은 대안이 될 수 있습니다[21]. 비전문가가 관계를 시작하는 데 관심이 있는 경우 장애 콘텐츠를 기획하고 가르치기 위해 지역 장애 단체를 찾고 참여하는 방법에 대한 자료도 출판되어 있습니다[24]. In this study, people with disabilities were primarily involved as panelists or standardized patients rather than advisory members or instructors. Patient encounters were more often completed with individuals with disabilities and their families than with standardized actors, an approach criticized by disability communities [21]. However, we found that engaging people with disabilities or the disability community requires time and monetary and human resources and thus is often perceived as burden. In addition, connections with local disability communities are not always established without a champion. Like one school in this study shared, using documentaries or memoirs about disability rights and culture could be good alternatives for programs lacking the resources to coordinate direct involvement of people with disabilities [21]. There are also published materials on how to find and engage with local disability organizations to plan and teach disability content if a non-expert is interested in initiating a relationship [24].
장애인이 자문위원이나 강사로 활동하는 학교는 소수에 불과했습니다. 전반적으로 교수진, 학생 및 자문위원의 장애 대표성을 개선하면 커리큘럼 결정에 장애인의 목소리가 반영될 수 있습니다[10]. 이는 의학계에서 장애를 가진 의사가 3.1%에 불과하고[25], 의대생의 4.5%만이 장애를 가지고 있다고 밝힌[26] 최근 연구 결과와도 일치합니다. 장애 역량 교육에 대한 많은 장벽과 필요성은 더 많은 학생, 교수진, 장애를 가진 의사가 현장에 투입되면 해결될 수 있습니다. 장애를 가진 사람들이 많아지면 더 많은 챔피언이 나올 것입니다. 또한 임상 환경에서 환자가 아닌 동료, 동료, 교사, 멘토로서 장애인을 대할 때 교수진과 학생은 장애가 아닌 그 사람을 바라보고 부정확한 가정과 불편함을 해소할 수 있습니다[27]. 이러한 변화는 의학교육의 정책과 관행에서 장벽을 제거하고 접근성과 포용성을 증진하려는 의도적인 노력을 통해서만 달성할 수 있습니다[22,28]. Only a few schools had a person with a disability serving as an advisory member or instructor. Overall, improving disability representation among faculty, students, and advisory members will ensure that curricular decisions reflect their voices [10]. This is consistent with recent studies that confirmed the underrepresentation of disability in Medicine as having only 3.1% of physicians [25] and 4.5% of medical students identify as disabled [26]. Many barriers and needs to disability competency training could be mended with more students, faculty, and physicians with disabilities in the field. With more individuals with disabilities, there will be more champions. In addition, the interaction with someone with a disability as a peer, colleague, teacher, and mentor, and not as a patient in a clinical setting, will allow faculty and students to see the person and not their disability and debunk inaccurate assumptions and discomfort [27]. These changes can only be achieved with intentional efforts to remove barriers and promote access and inclusion in policies and practices in medical education [22,28].
이 연구에는 몇 가지 한계가 있습니다. 모집 노력에도 불구하고 설문조사 응답률이 낮았던 것은 연구 기간 동안 의과대학과 의과대학장에게 영향을 미친 코로나19 팬데믹의 영향일 가능성이 높습니다. 이 주제에 더 많은 투자와 관심이 있는 학교일수록 설문조사에 응답할 가능성이 더 높았을 것입니다. 또한 이러한 역량을 직접적으로 다루지 않는 학교는 이러한 부족함을 드러내려고 하지 않았을 수도 있습니다. 따라서 이 연구 결과는 일반적으로 의과대학이 커리큘럼에서 장애 역량을 다루는 방식을 대표하지 않을 수 있습니다. This study has a few limitations. Despite efforts to recruit, the low response rate to the survey was likely influenced by the onset of the COVID-19 pandemic, which affected medical schools and directors during the study period. Schools who are more invested and interested in this topic may have been more likely to respond to the survey. In addition, schools that are not directly addressing these competencies may not have been as willing to reveal this deficit. Therefore, the study results may not represent how medical schools in general address disability competency in the curricula.
이러한 한계에도 불구하고 이번 연구 결과를 통해 시간이 제한된 의학교육 내에서 장애 역량 교육을 통합하기 위한 노력과 잠재력을 파악할 수 있었습니다. 또한 모든 의과대학에 이 연구에서 설명한 것과 같은 제도적 지원과 지지자가 있는 것은 아니라는 점도 중요합니다. 인터뷰 참여자 중 한 명이 권고한 바와 같이, 의과대학이 이 중요한 주제를 교육에 통합하도록 장려하기 위해 핵심역량을 LCME 인증 기준에 명시적으로 통합하는 것을 추가로 고려할 필요가 있으며, 이는 가능한 옹호자, 자원 및 지원과 관계없이 의과대학에 인센티브를 제공할 수 있습니다. 모든 의사가 장애인과 함께 일할 수 있도록 교육을 받도록 하는 것은 장애인의 건강 및 의료 서비스 격차를 줄이기 위한 중요한 단계가 될 것입니다.
Despite these limitations, the findings allowed for an understanding of efforts made and the potential for integrating disability competency training within time-restricted medical education. It is also important to note that not all medical schools have the institutional support and champions that this study described. As recommended by one of the interviewees, further consideration of explicitly integrating the Core Competencies into LCME accreditation standards may be needed so medical schools are incentivized to integrate this important topic in their education regardless of available champions, resources, and supports. Ensuring that all physicians are trained to work with people with disabilities would be a critical step towards reducing disparities in health care for and the health of people with disabilities.
Med Educ Online. 2023 Dec;28(1):2207773.doi: 10.1080/10872981.2023.2207773.
Disability competency training in medical education
Purpose:Lack of health care providers' knowledge about the experience and needs of individuals with disabilities contribute to health care disparities experienced by people with disabilities. Using the Core Competencies on Disability for Health Care Education, this mixed methods study aimed to explore the extent the Core Competencies are addressed in medical education programs and the facilitators and barriers to expanding curricular integration.
Method:Mixed-methods design with an online survey and individual qualitative interviews was used. An online survey was distributed to U.S. medical schools. Semi-structured qualitative interviews were conducted via Zoom with five key informants. Survey data were analyzed using descriptive statistics. Qualitative data were analyzed using thematic analysis.
Results:Fourteen medical schools responded to the survey. Many schools reported addressing most of the Core Competencies. The extent of disability competency training varied across medical programs with the majority showing limited opportunities for in depth understanding of disability. Most schools had some, although limited, engagement with people with disabilities. Having faculty champions was the most frequent facilitator and lack of time in the curriculum was the most significant barrier to integrating more learning activities. Qualitative interviews provided more insight on the influence of the curricular structure and time and the importance of faculty champion and resources.
Conclusions:Findings support the need for better integration of disability competency training woven throughout medical school curriculum to encourage in-depth understanding about disability. Formal inclusion of the Core Competencies into the Liaison Committee on Medical Education standards can help ensure that disability competency training does not rely on champions or resources.
Keywords:Disability competency; disability; diversity; health care education; medical education.
연구-바탕 교육과정 설계에서의 실제성 프레임워크 (TEACHING IN HIGHER EDUCATION, 2017) A framework for authenticity in designing a research-based curriculum Navé Wald and Tony Harland
소개 Introduction
저희는 뉴질랜드 오타고 대학교의 학부 생태학 커리큘럼을 살펴보던 중 고등 교육에서 진정성이라는 주제에 관심을 갖게 되었습니다(Harland, Wald, Randhawa, 곧 출간 예정). 이 프로그램에서 학생들은 연구를 통해 학습하며, '진정성'이라는 개념은 오랫동안 학습 활동 설계의 중심이 되어 왔습니다. 기본 아이디어는 학생들이 생태학을 공부할 때마다 어떤 형태로든 진정성 있는 연구에 참여해야 한다는 것입니다. 우리가 진정성이라고 생각하는 것을 달성하기 위해 교사는 전문적인 연구 활동을 사용하여 학생들을 안내합니다. 진정성을 갖추기 위해 교사-학생 관계는 대학원 감독과 호환되는 모델로 전환됩니다. 교육 및 커리큘럼에 대한 이러한 일반적인 접근 방식은 연구자로서 학생을 가르치기 위한 전략 2에서 Jenkins, Healey, Zetter(2007)에 의해 설명되었지만, 이 저자들은 진정성을 주장하지는 않습니다. 생태학에서는 이전에는 '진정성'의 정확한 의미를 고려하지 않았으며, 이 글에서는 이 용어의 사용과 관련된 담론적 수사를 이론 및 교육 실무와 관련하여 살펴볼 것입니다. 그런 다음 이러한 지식을 바탕으로 연구를 통해 교수의 진정성에 대한 프레임워크를 제시합니다. We became interested in the subject of authenticity in higher education while examining the undergraduate ecology curriculum at the University of Otago, New Zealand (Harland, Wald, and Randhawaforthcoming). In this programme, students learn by doing research and the concept of ‘authenticity’ has long been central to the design of learning activities. The basic idea is that anytime students are studying ecology, they should be engaged in some form of authentic research. In order to achieve what we consider as authenticity, teachers use their professional research activities to guide them. In order to be authentic, the teacher-student relationship shifts towards a model compatible with postgraduate supervision. This general approach to teaching and curriculum has been described by Jenkins, Healey, and Zetter (2007) in their Strategy 2 for teaching students as researchers, although these authors do not claim authenticity. In ecology, we had not previously considered the precise meaning of ‘authenticity’ and in this essay the discursive rhetoric around the use of the term will be examined in relation to theory and teaching practice. We then use this knowledge to offer a framework for authenticity in teaching through research.
우리는 연구자로서 학생들을 가르치는 다양한 모델에서 진정성에 대한 주장을 찾기 시작했지만(Hung and Chen 2007, Laursen 외. 2010, Sadler 외. 2010, Sadler and McKinney 2010), 고등 교육에서도 다양한 맥락에서 진정성이 사용된다는 사실을 발견했습니다. 여기에는 교수 및 학습(Cranton 2001, Cranton과 Carusetta 2004a, 2004b, Herrington과 Herrington 2006, Herrington, Reeves, Oliver 2014), 평가(Frey, Schmitt, and Allen 2012, Gulikers, Bastiaens, Kirschner 2004, Herrington과 Herrington 1998), 성취(Newmann 1996, Newmann과 Archbald 1992) 등이 포함됩니다. 거의 모든 경우에서 '진정성' 또는 '진정성 있는 행동'을 구성하는 요소의 의미는 완전히 설명되지 않았으며, 따라서 여전히 애매한 상태로 남아 있습니다. 고등 교육에서 진정성에 대한 연구는 결코 미지의 영역이 아니지만, 역사적 측면에서 보면 20세기 듀이주의 사상(Petraglia 1998)에 뿌리를 둔 비교적 최근의 아이디어이므로 교육의 진정성에 대한 탐구는 긴 궤적을 가지지 않습니다(Splitter 2009). Although we set out to find claims to authenticity in various models of teaching students as researchers (Hung and Chen2007; Laursen et al.2010; Sadler et al.2010; Sadler and McKinney2010), we discovered that it was also used in many different contexts in higher education. These include teaching and learning (Cranton2001; Cranton and Carusetta2004a,2004b; Herrington and Herrington2006; Herrington, Reeves, and Oliver2014), assessment (Frey, Schmitt, and Allen2012; Gulikers, Bastiaens, and Kirschner2004; Herrington and Herrington1998), and achievement (Newmann1996; Newmann and Archbald1992). In nearly all cases the meaning of what constitutes ‘being authentic’ or ‘doing something authentically’ is not fully explained and thus remains elusive. While the study of authenticity in higher education is by no means uncharted territory (for examples see Carusetta and Cranton2005; Cranton and Carusetta2004a,2004b; Kreber2013; Kreber et al.2007), in historical terms it is a relatively recent idea rooted in twentieth-century Deweyan thought (Petraglia1998), and thus inquiries into educational authenticity do not have a long trajectory (Splitter2009).
진정성의 복잡성을 이해하기 시작하려면 용어의 다양한 용도와 정의를 살펴보는 것부터 시작할 수 있습니다. 옥스퍼드 영어 사전(1989)은 '진위성'을 명사로, '진품'을 형용사이자 명사로 정의합니다. 주로 이러한 용어는 사람, 문서, 인공물, 아이디어, 행동, 정체성, 프로세스 등 어떤 것을 지칭합니다. - 진짜, 진품, 진실, 원본, 사실, 정확성, 유효성, 권위 등의 고유한 특성을 지닌 것으로 인식되는 것을 의미합니다. 정확한 의미는 구체적인 맥락에 따라 달라집니다. 사회학적 관점에서 '진정성은 존재의 상태가 아니라 과정이나 표현의 객관화, 즉 특정 시간과 장소의 사람들이 이상이나 모범을 대표한다고 동의하게 된 일련의 자질을 의미합니다'(Vannini and Williams 2009, 3). 따라서 진정성은 사회적으로 구성되므로 유동적이고 맥락에 따라 달라지며 논쟁의 대상이 될 수 있습니다. 따라서 진정성의 구성은 권력, 현실성, 권위, 그리고 궁극적으로는 우월성에 대한 내재적이고 암묵적인 아이디어를 암시합니다. 따라서 진정성은 다양한 의미와 가치가 담긴 키워드입니다(Williams 1976). To begin to appreciate the complexity of authenticity one can start by examining the term’s various uses and definitions.
The Oxford English Dictionary (1989) defines ‘authenticity’ as a noun and ‘authentic’ as both adjective and noun. Primarily, these terms refer to something – person, document, artefact, idea, behaviour, identity, process, etc. – having the perceived inherent quality of being real, genuine, true, original, factual, accurate, valid, authoritative, and so forth. The exact meaning will depend on the specific context at hand.
From a sociological perspective, ‘Authenticity is not so much a state of being as it is the objectification of a process or representation, that is, it refers to a set of qualities that people in a particular time and place have come to agree represent an ideal or exemplar’ (Vannini and Williams2009, 3).
Thus, authenticity is socially constructed and as such is fluid, highly contextual and may be contested. Constructions of authenticity, then, allude to inherent and implicit ideas of power, realness, authority and, ultimately, of superiority. Authenticity is, therefore, akeywordladen with a range of meanings and values (Williams1976).
연구를 통해 과학을 가르친다는 좁은 맥락에서조차도 실질적으로 다른 교육 모델과 관련하여 진정성에 대한 주장이 제기되는 것은 놀라운 일이 아닙니다. 그런 다음 우리는 '어떤 이유로 사건과 경험이 어떻게 해석되고 해석되어야 하는지에 대해 궁금증을 불러일으킬 때 철학을 해야 한다'고 주장한 맥신 그린(1973, 10)에서 힌트를 얻습니다. 달리 말하면, 그린은 우리가 파편화되고 의미가 거의 없는 그림에서 더 나은 일관성을 추구할 때 추상화로 전환할 것을 촉구합니다. 따라서 이 글에서는 이 용어의 사용과 관련된 담론적 수사를 살펴볼 것입니다. 진정성에 관한 문헌을 읽은 것은 연구를 통한 학습의 원리와 진정성 이론을 연결할 수 있는 중요한 아이디어를 발견하기 위한 목적으로 특별히 수행되었습니다. 본질적으로 우리는 '우리의 작업이 '진정성있다'라는 말을 이해하는 데 도움이 되는 매우 복잡한 현상에서 무엇을 취할 수 있을까'라는 연구 질문을 던졌습니다. 문헌 검토를 통해 새롭게 등장한 연관성을 바탕으로 교육과 학습, 그리고 진정성에 대한 현재의 논쟁에 정보를 제공하기 위해 설계된 프레임워크를 구축했습니다. 그 결과, 우리의 질문과 관련된 진정성을 이해하는 세 가지 방법을 확인할 수 있었습니다: It is of little surprise then that even within the narrower context of teaching science through research, claims for authenticity are made in relation to substantially different educational models. We then take a cue from Maxine Greene (1973, 10) who argued we ought to ‘philosophize when, for some reason, we are aroused to wonder about how events and experiences are interpreted and should be interpreted’. Put differently, Greene urges us to turn to abstraction when we seek better coherence from a picture otherwise fragmented and of little sense. In this article, therefore, the discursive rhetoric around the use of the term will be examined. Our reading of the literature on authenticity was done specifically with the purpose of discovering significant ideas that might connect the principles of learning through research with the theories of authenticity. Essentially we were asking the research question: ‘what can we take from a highly complex phenomenon that would help us understand our work as authentic?’ After our literature review, emerging associations were used to construct a framework designed to inform both teaching and learning and the current debates around authenticity. We were able to identify three ways of understanding authenticity that were relevant to our inquiry:
'실제 세계'와 관련된 진정성 Authenticity as relating to the ‘real-world’
실존적인 진정한 자아 The existential authentic self
의미의 정도 A degree of meaning
'현실 세계'와 관련된 진정성 Authenticity as relating to the ‘real world’
진정성을 과학교육과 연결하는 가장 일반적이고 응용적인 관점은 '실제 세계'를 반영하는 교육입니다. 간단히 말해, '진정성 있는 과학은 과학자들이 연구하는 방식과 밀접하게 일치하는 탐구 교육의 변형이며 전통적인 학교 과학 실험실 실습과는 다르다'(크로포드 2015, 113)고 할 수 있으며, 이 개념은 우리가 여기서 다루는 생태 프로그램의 커리큘럼 설계에 큰 지침이 되었습니다. 과학교육의 진정성에 대한 이러한 단순한 개념화는 '상응하는 관점'(Kreber 2013, Splitter 2009)으로도 알려져 있으며, 존 듀이와 진보주의 운동의 실용주의 교육적 신념과 강하게 공명합니다. 듀이는 엘리트주의-이상주의 교육과 직업-도제 교육 사이의 확립된 이분법을 거부했는데, 이는 '아이디어의 궁극적 중요성은 현실 세계에 적용될 때 그 결과에서 찾을 수 있다는 가정에 뿌리를 둔 거부'였습니다(Petraglia 1998, 26). 따라서 페트라글리아(1998)는 듀이가 교육과 '실제 삶' 사이의 벽을 허물고, 이를 통해 진정성에 대한 특정한 수사학을 확립한 영향력 있는 유산을 남겼다고 평가합니다. 듀이는 '학습은 학생들에게 '배울 것'이 아니라 '할 일'이 주어질 때 일어난다'고 믿었으며, 학생들이 하는 일은 '실제 삶'과 관련되어야 하며, 이것이 바로 이러한 접근 방식을 의미 있고 가치 있게 만드는 이유입니다(Greene 1973, 158, 원문에서 강조). The most common and applied perspective that links authenticity with science education is teaching that mirrors the ‘real world.’ Put simply, ‘Authentic science is a variation of inquiry teaching that aligns closely with how scientists do their work and differs from traditional school science laboratory exercises’ (Crawford2015, 113), and this concept has largely guided the curriculum design of the ecology programme that we address here. This simple conceptualisation of authenticity in science education, also known as the ‘corresponding view’ (Kreber2013; Splitter2009), strongly resonates with the pragmatist pedagogical beliefs of John Dewey and the Progressivist movement. Dewey rejected the established dichotomy between an elitist-idealist education and vocational-apprenticeship training, a rejection that ‘was rooted in the assumption that the ultimate significance of an idea is to be found in its consequences when applied in the real world’ (Petraglia1998, 26). Thus, Petraglia (1998) attributes to Dewey the influential legacy of dismantling the wall between education and ‘real life,’ by which a particular rhetoric of authenticity was established. Dewey believed that ‘learning takes place when students are given something todorather than something to learn,’ and what they do should relate to ‘real life,’ which is what renders this approach significant and worthwhile (Greene1973, 158, emphasis in original).
예를 들어, 헤링턴, 리브스, 올리버(2014, 401)는 '진정성 있는 학습은 학습 과제를 미래의 사용 맥락에 위치시키는 교육학적 접근 방식'이라고 주장합니다. 따라서 진정한 학습의 모델은 지식이 실제 생활에서 그리고 나중에 어떻게 활용될지를 반영하도록 설계됩니다. 이 접근 방식에 따르면 학생들은 졸업 후 자신이 선택한 직업과 분야에서 지식을 창출하고 혁신을 이룰 수 있는 지식과 기술을 습득해야 합니다. 따라서 진정성은 전문적인 환경에서 지식이 어떻게 생산되고 전달되는지를 반영합니다(Herrington 및 Herrington 2006). 이러한 교육적 접근 방식은 지식이 적용될 맥락에서 의미 있는 학습이 설정된다는 Brown, Collins, Duguid(1989)의 상황적 학습 또는 상황적 인지 이론에 뿌리를 두고 있습니다(Herrington, Reeves, Oliver 2010).
Herrington, Reeves, and Oliver (2014, 401), for example, maintain that ‘Authentic learning is a pedagogical approach that situates learning tasks in the context of future use.’ Models of authentic learning are thus designed to reflect how knowledge will be utilised in real life and at a later time. Accoㄴrding to this approach, students should acquire knowledge and skills that would allow them, after graduation, to create knowledge and innovate in their chosen professions and fields. Therefore, authenticity reflects how knowledge is produced and communicated in professional settings (Herrington and Herrington2006). This pedagogical approach is rooted in Brown, Collins, and Duguid’s (1989) theory of situated learning or cognition in which meaningful learning is set in the context within which the knowledge will be applied (Herrington, Reeves, and Oliver2010).
그러나 Hung과 Chen(2007)은 학교 공동체와 전문직 공동체 모두 그 자체로 진정성이 있다고 주장합니다. 그들은 이 두 커뮤니티 간의 관계를 맥락-프로세스 프레임워크 내에서 분석해야 한다고 제안합니다. 이 프레임워크에서 진정성에 대한 접근 방식은 주로 유동적이고 다면적인 정체성 개념과 학교 공동체와 전문직 공동체 사이의 전환과 관련된 정체성의 문화화, 형성 및 변화에 초점을 맞추고 있습니다. Hung과 Chen(2007, 162-3)은 '진정성의 문제를 현실 세계의 실천과 학문에만 국한시켜서는 안 되며, 맥락과 과정 차원을 모두 만족시킬 때 진정성 있는 학습이 가능하다'고 말했는데, 여기서 전자는 실천 공동체를, 후자는 정체성 함양과 변형을 의미합니다. 이와는 대조적으로 Splitter(2009, 139)는 '교실 밖의 세계'에서 일어나는 일이 우리가 진정성이 의미하는 바, 또는 의미할 수 있는 바에 대한 표준을 제공한다는 가정에 의문을 제기합니다. 이 저자는 교실에서 이루어지는 일과 '실제 세계'에서 이루어지는 일 사이의 단순한 관계에 반대합니다. 대신, 스플리터에게 진정성은 과업의 의미, 성취도 또는 가치에 뿌리를 두고 있기 때문에 '실제'에 있는 것은 실제보다 덜 중요하다고 말합니다. 이 개념은 진정성에 대한 주장이 이상화된 관행에 대한 주관적인 가치 판단에 근거한다는 것을 의미합니다(Splitter 2009). However, Hung and Chen (2007) argue that both what they call school community and professional community are authentic in their own right. They propose that the relationships between these two communities should be analysed within a context-process framework. In this framework, approaches to authenticity focus predominantly on the fluid and multi-faceted notion of identity, and its enculturation, formation and transformation within and in relation to the transition between the school community and the professional community. For Hung and Chen (2007, 162-3) ‘the issue of authenticity should not be constrained to real world practices and disciplines, but authentic learning should be possible when we satisfy both context and process dimensions,’ where the former refers to the practice community and the latter to identity enculturation and transformation. In contrast, Splitter (2009, 139) questions ‘the presumption that what happens in “the world beyond the classroom” offers a standard for what we mean, or might mean, by authenticity.’ This author argues against a simple relationship between what is done in the classroom and what is being done in the ‘real world.’ Instead, for Splitter authenticity is rooted in a task’s degree of meaning, fulfilment or worthiness, and therefore what is ‘out there’ is less important than what ought to be. This idea means that assertions of authenticity are based on subjective value judgments about idealised practices (Splitter2009).
수학적 모델링을 가르치는 맥락에서 Vos(2011)는 '교육-현실 세계'의 연결고리에 대한 다른 관점을 제시합니다. Vos는 진정성의 개념이 사회적으로 구성되는 것으로 인식하고 특정 맥락에서 진정성을 형성하는 데 신중을 기할 것을 촉구합니다.
먼저, 진정성이 사본과 시뮬레이션을 지칭할 수 있는지, 아니면 무조건적인 원본을 지칭할 수 있는지 결정해야 합니다.
두 번째 고려 사항은 진위가 예/아니오의 이진법인지, 아니면 어느 정도 서수적 품질을 갖는지에 관한 것입니다.
보스는 진위성의 정의는 이분법적이어야 하며 원본만을 지칭해야 한다고 주장합니다. 따라서 교육 과제는 전체적으로 진정성이 있는 것이 아니라, 진정성 있는 측면을 포함할 수 있습니다. 또한 과제에 진정성 요소가 있으려면 학교 밖 전문가가 인증 할 수있는 학교 밖에서 유래 한 널리 인식 할 수있는 품질이 있어야하며, 이는 '실제로 ... 진정성을 구현'해야합니다 (Vos 2011, 720). Writing within the context of teaching mathematical modelling, Vos (2011) provides a different view on the ‘teaching-real world’ nexus. Vos recognises the concept of authenticity as being socially constructed and urges its formation in a particular context to be done thoughtfully.
First, a decision should be made as to whether authenticity can refer to copies and simulations or to unconditional originals.
The second consideration concerns whether authenticity is a yes/no binary or has an ordinal more-or-less quality.
Vos argues that a definition of authenticity should be a binary and refer only to originals. Consequently, an educational task will never be authentic as a whole; rather, it may contain authentic aspects. In addition, for a task to have authentic elements it must have a widely recognisable quality that has an out-of-school origin certifiable by out-of-school experts, which ‘in fact … embody the authenticity’ (Vos2011, 720).
실존적 진정성 자아 The existential authentic self
교육에서 진정성의 또 다른 중요한 측면은 실존 철학과 자아 및 존재 감각과 관련이 있습니다. 교육 문헌에서는 교사의 행동 및 가치관, 교사-학생 관계와 관련하여 진정성의 이러한 측면을 논의하는 경향이 있지만, 여기서는 연구를 통해 교육이라는 주제와도 연결하고자 합니다. Another important facet of authenticity in education is linked to existential philosophy and to a sense of self and of being. Whereas the education literature tends to discuss this aspect of authenticity in relation to teachers’ behaviour and values and to teacher-student relations, here we also wish to link it to the theme of teaching through research.
철학적 관점에서 볼 때, 일부 진정성은 '현대 서구 세계의 문화적 구성물이며 ... [그리고] 개인에 대한 서구의 개념과 밀접하게 연관되어 있다'(Handler 1986, 2). 테일러(1991)의 『진정성의 윤리』에서 그는 이러한 개인주의가 현대 사회의 업적이면서 동시에 그 폐해라고 말하며, 개인주의가 사람들의 의미와 존재감에 미친 결과에 대해 우려하고 있습니다. '진정성'이란 사회적 관습과 압력에도 불구하고 자기 자신에 대해 독창적이고 진실한 것을 의미합니다. 트릴링(1972, 93)은 진정성이 '불길한 의미를 지닌 단어'이며, '이 단어가 우리 시대의 도덕적 속어의 일부가 된 것은 타락한 상태의 특이한 본질, 존재와 개인 존재의 신뢰성에 대한 불안을 가리킨다'고 지적합니다. 기든스(1991)도 자아 정체성, 대인 관계, 도덕성 또는 도덕적 지지와 관련하여 진정성에 대해 논의합니다. 그에 따르면 '진정성 있는 사람은 자신을 알고 그 지식을 담론적으로 그리고 행동 영역에서 상대방에게 드러낼 수 있는 사람'입니다(Giddens 1991, 186-7). 따라서 진정성은 사람들 간의 신뢰와 도덕적 지원을 강화하기 위해 자아의 무결성을 활용하는 데 매우 중요합니다. From a philosophical standpoint, for some authenticity is ‘a cultural construct of the modern Western world … [and is] closely tied to Western notions of the individual’ (Handler1986, 2). In Taylor’s (1991)Ethics of Authenticity, this individualism is both an achievement of modern society and its malaise, and he is concerned with the consequences it has had for people’s sense of meaning and being. Being ‘authentic’ means being original and true to one’s self in spite of societal conventions and pressure. Trilling (1972, 93) notes that authenticity ‘is a word of ominous import’ and that this ‘word has become part of the moral slang of our day points to the peculiar nature of our fallen condition, our anxiety over the credibility of existence and of individual existences.’ Giddens (1991) also discusses authenticity in relation to self-identity, interpersonal relationships and morality, or moral support. For him, ‘the authentic person is one who knows herself and is able to reveal that knowledge to the other, discursively and in the behavioural sphere’ (Giddens1991, 186-7). Authenticity, then, is crucial for harnessing the integrity of the self for enhancing trust and moral support among people.
따라서 진정성은 일반적으로 긍정적인 의미를 지니며, 포터(2010, 6)가 '모성어'라고 부르는 '커뮤니티', '지속 가능성', '자연'과 같은 유사한 강력한 용어 그룹에 속한다고 볼 수 있습니다. 서구 사회는 진정성에 대한 추구에 사로잡혀 있으며, 포터는 현대 생활에서 의미를 찾기 위해 자기 성취와 발견을 추구하는 개인주의적 추구로 이해합니다. 그러나 포터에게 진정성이란 특권의 본질은 누구나 가질 수 있는 것이 아니기 때문에 특권을 구성하는 관계적이고 주관적인 속성인 허구입니다. 따라서 진정성에 대한 열망은 현대 사회의 문제에서 벗어나기보다는 근대 이전의 삶에 대한 잘못된 낭만적 관념을 조장합니다(Potter 2010). 치커링(2006)도 진정성의 일반적인 긍정적 속성과 함께 진정성이 나쁠 수 있는 가능성에 주목합니다. 그에게 진정성은 개념적으로 간단합니다. '진정성이 있다는 것은 보이는 것이 곧 얻는 것임을 의미합니다. 내가 믿는 것, 내가 말하는 것, 내가 행동하는 것이 일관성이 있다는 것입니다'(Chickering 2006, 8). 그러나 내적 일관성은 진정으로 선하거나 악한 사람에게도 똑같이 적용될 수 있습니다. Thus, authenticity usually carries positive connotations and arguably belongs to a group of similarly powerful terms like ‘community,’ ‘sustainability’ and ‘natural;’ what Potter (2010, 6) calls ‘motherhood words.’ Western society is possessed by a quest for authenticity, which Potter understands as an individualistic pursuit after self-fulfilment and discovery in order to find meaning in modern life. For Potter, however, authenticity is a hoax, a relational and subjective attribute that constructs privilege, because the very nature of privilege is that not everybody can have it. So rather than escaping the malaises of modern society, the aspiration to authenticity promotes ill-informed romantic notions of pre-modern life (Potter2010). Chickering (2006) also notes the usual positive attribute of authenticity alongside the possibility for authenticity to be bad. For him, authenticity is conceptually straightforward: ‘Being authentic means that what you see is what you get. What I believe, what I say, and what I do are consistent’ (Chickering2006, 8). Internal consistency, however, can be equally ascribed to someone who is authentically good or evil.
Kreber (2013)와 Kreber 외(2007)가 교육과 학문적 실천에서 진정성을 조사했을 때, 하이데거의 실존철학과 '죽음을 향한 진정한 존재의 존재론적 가능성'과 관련하여 '일상성', '진정성', '비진정성' 사이의 구별에 상당한 주의를 기울였습니다(Heidegger 1962, 304).
여기서 일상성이란 자신의 행동과 신념이 타인의 행동과 신념에 의해 지시되는 순응주의를 의미합니다. 이 상태는 '부(un)진정성'으로 간주되는 반면,
'비(in)진정성'은 사람이 자신의 예정된 죽음을 받아들이거나 깨닫지 못하여 자신의 삶을 비판적으로 검토하지 않는 상태입니다.
따라서 진정성은 개인이 자신의 유한한 존재를 인식하고 성찰하는 삶을 살도록 요구합니다. '하이데거의 작업에서 [돌본다는 것은] 세속적인 일과 자신의 존재에 대해 '관심을 갖는 것'을 의미하기 때문에'(Kreber 외, 2007, 32, 원문 강조) 돌봄의 개념은 이러한 성찰적 삶의 핵심입니다.
When Kreber (2013) and Kreber et al. (2007) examined authenticity in teaching and academic practice, considerable attention was paid to Heidegger’s existential philosophy and his distinction between ‘everydayness,’ ‘authenticity,’ and ‘inauthenticity’ in relation to the ‘ontological possibility of an authentic Being-towards-death’ (Heidegger1962, 304).
Here, everydayness denotes conformism, where one’s actions and beliefs are directed by those of others. This state is deemed ‘unauthentic,’
whereas ‘inauthenticity’ is when persons do not come to terms with or realise their own predetermined demise and therefore do not critically examine their lives.
Authenticity, then, requires individuals to appreciate their finite existence and live examined lives. The notion of care is central to such examined life; for ‘in Heidegger’s work, [to care] means “to be concerned”about worldly affairs and one’s own existence’ (Kreber et al.2007, 32, emphasis in original).
하이데거의 존재 방식은 무엇보다도 자신의 유한한 경력을 고려하고 이 시기에 무엇을 성취하고 싶은지, 성취해야 하는지를 고민해야 하는 교사의 직업적 삶과 관련이 있습니다.
일상성이라는 선택지는 교사가 다른 모든 사람들이 하는 것처럼 보이는 일을 하는 길을 의미합니다.
반대로 진정성이란 교육자로서 자신의 제한된 선택지를 인식하는 동시에 가르치는 것에 대해 성찰하고 반성하며, 자신이 가르치는 대상과 영향력에 대해 진정으로 관심을 갖는 것을 의미합니다.
Kreber 등(2007)에 따르면 비진정성은 가르치기를 꺼려하고 이기적인 이유만으로 가르치는 것을 의미합니다.
이러한 진정성 개념화의 초점은 주로 자기 자신에 맞춰져 있지만, 크레버와 동료들은 개인이 생활하고 행동하는 사회적 맥락의 중요성을 강조한 아도르노(1973)의 비판에도 주목합니다. 개인의 결정, 신념, 행동이 환경의 영향을 받는다는 점에서 아도르노의 진정성에 대한 관점은 보다 구조주의적입니다. 이를 깨닫기 위해서는 비판적 의식이 필요합니다. Heidegger’s modes of Being are relevant to the professional lives of teachers, who first and foremost should consider their own finite careers and ponder what they wish or ought to achieve in this time.
The option of everydayness implies a path where a teacher does what everybody else seems to be doing.
In contrast, being authentic means to be cognisant of one’s limited options as an educator but also to be reflective and reflexive towards teaching, and to genuinely care about one’s subject and impact.
Inauthenticity, for Kreber et al. (2007), implies being reluctant to teach and doing so only for selfish reasons.
The focus of this conceptualisation of authenticity is devoted primarily to one’s self, but Kreber and colleagues also note Adorno’s (1973) critique that emphasises the importance of the social context within which individuals live and act. Adorno’s view of authenticity is more structuralist as an individual’s decisions, beliefs and actions are influenced by their environment. Realising this requires a critical consciousness.
의식이라는 개념은 실존주의와 진정성에 관한 사르트르의 저술에서도 핵심적인 개념입니다. 사르트르에게 있어 사람의 존재는 본질보다 우선합니다. 이것은 '인간은 무엇보다도 먼저 존재하고, 자신을 만나고, 세계로 솟구쳐 오르고, 그 후에 자신을 정의한다'는 것을 의미합니다(Sartre 2001, 29). 이는 무엇보다도 인간이 되는 데에 미리 정해진 목적이 없으며, 인간은 자신의 실존적 존재를 구성할 책임과 자유가 있다는 것을 의미합니다(카코리 및 후투넨 2012). 그러나 자신의 존재에 의미를 부여하는 자유와 책임은 내면적으로만, 고립적으로만 일어나는 것이 아니라 '존재는 본질에 선행하기 때문에 자신이 무엇이며 타인을 위해 무엇을 하는지에 대해 도덕적으로 책임이 있다. 사람은 자신에 대해서만 책임지는 것이 아니라 모든 인간에 대해 책임을 져야 한다'(카코리와 후투넨 2012, 355). 따라서 자신의 선택에 대한 책임감은 사르트르(1957)의 실존주의 사상의 핵심입니다. 또한, 선택의 자유와 능력은 아무리 제약이 있더라도 '의식의 존재와 그 자체에 대한 의식을 수반한다'(Priest 2001, 107)고 말합니다. The idea of consciousness is also central in Sartre’s writings on existentialism and authenticity. For Sartre, a person’s existence comes before essence. This means ‘that man first of all exists, encounters himself, surges up in the world – and defines himself afterwards’ (Sartre2001, 29). This means,inter alia, no predetermined purpose for being human as well as humans’ responsibility and freedom to construct their own existential being (Kakkori and Huttunen2012). The freedom and responsibility for giving meaning to one’s being, however, does not happen only internally, in isolation; but rather, ‘Because existence precedes essence, one is morally responsible for what one is and what one does for others. One is not responsible for only oneself but instead for all humans’ (Kakkori and Huttunen2012, 355). This sense of responsibility for one’s own choices, then, is key in Sartre’s (1957) existential ideas. Moreover, one’s freedom and capacity of making choices, however constrained, ‘entails the existence of consciousness, and consciousness of itself’ (Priest2001, 107).
사르트르의 실존주의는 하이데거의 실존주의에 비해 고등 교육 분야에 덜 영향을 미쳤지만, 존재와 자아에 대한 그의 사상은 어느 정도 구매력이 있었습니다. 예를 들어, Barnett(2007)은 사르트르의 사상을 고등 교육에서 학생들이 (자신의 행동에 대한 책임을 지는 것과 같이) 자신의 존재를 변화시키는 여정과 연결시킵니다. Barnett(2007, 61)은 '고등 교육은 학생이 진정성을 갖게 될 때 정점에 도달한다'고 말하며, 여기서 하이데거의 작품에서도 발견할 수 있는 '소유권'이라는 개념이 중추적인 역할을 한다고 말합니다. 책임감과 소유권이라는 실존적 개념은 개인이 독립적인 학습자가 되는 데 중요하며, 이러한 학습은 답을 찾는 것뿐만 아니라 질문하는 사람이 됨으로써 이루어집니다(Greene 1973). Sartre’s existentialism has had less impact on the field of higher education, compared with Heidegger’s, but his ideas of being and self did have some purchase. Barnett (2007), for example, links Sartre’s ideas to the journey students undergo in higher education, where they transform their being by, among other things, assuming responsibility for their actions. For Barnett (2007, 61), ‘Higher education achieves its apogee when the student becomes authentic,’ where the idea of ‘ownership,’ which he also finds in Heidegger’s work, is pivotal. These existential ideas of responsibility and ownership are important for individuals’ ability to become independent learners, and this learning happens by means of not only finding answers but also being the ones asking the questions (Greene1973).
Brook(2009)도 하이데거의 실존 철학과 진정성 개념을 통해 교수법을 검토합니다. 다시 말하지만, 하이데거의 실존적 의미의 진정성은 진정한 인간이 되는 것을 필요로 합니다. 이것은 자기 자신이 되고, 타인을 돌보고, 자신의 필멸성과 따라서 시간성을 깨닫는 것을 포함합니다. 인간은 진정성 있는 존재로 태어나지 않으며, 평생을 진정성 있는 존재가 되지 못한 채 살아갈 수도 있기 때문에 진정성 있는 존재가 되고 변화한다는 개념이 중요합니다. 따라서 인간은 진정한 존재가 될 수 있으며, '하이데거는 교육을 진정한 의미에서 진정성의 형성으로 공식화한다'(Brook 2009, 51, 강조 추가)고 말합니다. 이러한 맥락에서 크레버(2013, 45)는 교사와 학생 모두의 진정성을 증진하는 것이 '고등교육의 주요 목적 또는 보편적 목표가 되어야 한다'고 주장합니다. 그녀에게 고등 교육에서 그리고 고등 교육을 통해 진정성을 형성하는 것은 궁극적으로 사람들이 더 비판적이고, 인식하고, 동정심을 갖고, 연결되는 더 공정하고 풍요로운 세상을 촉진하는 것을 목표로합니다. Jarvis(1992)에 따르면 교사는 관련된 모든 사람의 개인적 발전과 성장을 촉진하려고 노력할 때 진정성 있게 행동합니다. 이 과정에서 학습은 일방적인 것이 아니라 교사와 학생이 대화를 통해 학습하고 상호 성장을 위한 책임을 공유한다는 Paulo Freire(2000)의 아이디어를 따릅니다. Brook (2009) also turns to Heidegger’s existential philosophy and notions of authenticity for examining teaching. Again, Heidegger’s existential meaning of authenticity necessitates becoming truly human. This constitutes being one’s self, caring for others and realising one’s own mortality and hence temporality. This notion of becoming, of transforming, is key because humans are not born authentic and may live their entire lives without being authentically themselves. Thus, they can become authentic beings, and ‘Heidegger formulates education in its proper sense as theformationof authenticity’ (Brook2009, 51, emphasis added). In this vein, Kreber (2013, 45) argues that promoting the authenticity of both teachers and students ‘should be a chief purpose or universal aim of higher education.’ For her, the formation of authenticity in and through higher education ultimately aims to promote a fairer and more enriched world, where people are more critical, aware, compassionate and connected. For Jarvis (1992), teachers act authentically when they attempt to nurture the personal development and growth of everybody involved. In this process, learning is not uni-directional; but rather, it follows Paulo Freire’s (2000) ideas around teachers and students learning in dialogue and sharing responsibilities for mutual growth.
프레이레(2000)는 그의 대표작인 '억압받는 자의 교육학'에서 진정성을 언급하거나 '진정성'이라는 용어를 다양한 방식으로 사용했습니다. 주로 '진실성' 또는 '진정성'을 의미하며, 예를 들어 혁명(지도자가 민중과 소통하는 것)과 권위(권력이 위임되고 공유되는 것)와 관련해서도 사용됩니다. 프레이레는 연대, 자유, 진정성을 함께 연결하며, 이러한 결합은 양방향 소통의 교육학에 달려 있습니다. '진정한 교육은 'A'가 'B'를 위해 또는 'A'가 'B'에 대해 수행하는 것이 아니라, 'A'와 'B'가 (세계, 즉 양 당사자에게 감동을 주고 도전하며 그에 대한 견해나 의견을 제시하는) 세계를 매개로 수행됩니다'(Freire 2000, 93, 원문에서 강조 표시). 교사의 사고는 학생의 사고에 의해 인증되어야 하며, 프레이레에 따르면 이는 학생이 자신의 비진정적이고 억압된 존재를 확인하고 그 사고를 해방하기 위해 행동하지 않는 한 일어날 수 없습니다. 이러한 억압을 내면화하는 상태는 본질적으로 하이데거(1962)가 말한 일상성, 즉 현실을 수동적으로 받아들이고 독창적이고 비판적인 사고가 결여된 상태입니다. In his seminal workPedagogy of the Oppressed, Freire (2000) refers to authenticity or uses the term ‘authentic’ in various ways. It primarily denotes ‘truthfulness’ or ‘genuineness,’ for instance in relation to revolution (where leaders communicate with the people) and authority (where power is delegated and shared). Freire links together solidarity, freedom and authenticity, whose combination depends on a pedagogy of bidirectional communication, ‘Authentic education is not carried on by “A”for “B” or by “A”about “B,” but rather by “A”with “B,” mediated by the world – a world which impresses and challenges both parties, giving rise to views or opinions about it’ (Freire2000, 93, emphasis in original). The teacher’s thinking must be authenticated by student thinking and, for Freire, this cannot occur unless the students are able to identify their inauthentic and oppressed being and act to liberate their thought. Such a state of internalising oppression is essentially Heidegger’s (1962) everydayness: a passive acceptance of reality and lack of original and critical thinking.
크레버(2013, 11)는 '진정성은 적어도 세 가지의 광범위한 철학적 전통, 즉 실존주의, 비판주의, 공동체주의에 의해 뒷받침되는 다차원적 개념'이라고 말합니다.
실존적 관점에서 진정성은 자신의 가능성과 삶의 목적에 대한 자기 인식과 내면의 견해에 대한 헌신으로 이해됩니다.
비판적 관점에서 실존적 진정성을 포함한 진정성은 자신의 지식, 가치, 신념에 대한 반성적 비판을 전제로 합니다. 이러한 비판은 이러한 것들이 어떻게 무비판적으로 동화되어 왔으며, 때로는 당연한 것으로 받아들여졌는지를 고려합니다.
공동체주의적 관점은 개인의 진정성에 영향을 미치는 사회적 맥락의 중요성을 지적함으로써 비판적 관점과 관련이 있습니다.
진정성은 종종 자기 자신을 발견하고 진실해지는 것과 관련이 있지만, 사람들은 고립되어 살지 않으며 공동체주의 관점은 관계의 중요성과 사람들의 상호 연결성을 강조합니다. Kreber (2013, 11) notes that ‘Authenticity is a multidimensional concept underpinned by at least three broad philosophical traditions: the existential, the critical and the communitarian.’
From an existential perspective authenticity is understood as self-awareness of one’s own possibilities and purpose in life, and commitment to one’s inner views.
From a critical perspective, authenticity, including existential authenticity, is contingent on reflective critique of one’s own knowledge, values and beliefs. This critique would take account of how these have been uncritically assimilated and, at least sometimes, taken for granted.
The communitarian perspective is related to the critical by pointing to the importance of social contexts in affecting an individual’s authenticity.
While authenticity is often associated with discovering and being true to one’s self, people do not live in isolation and the communitarian perspective stresses the importance of relationships and people’s interconnectedness.
의미의 정도 A degree of meaning
의미의 정도가 진정성의 가치를 구성한다는 생각은 두 가지 측면이 있습니다.
첫째, 서론에서 언급했듯이 진정성이라는 개념은 복잡하고 상황에 따라 달라지지만, 본질적으로 긍정적인 속성을 가지고 있습니다. 이런 의미에서 진정성이 있다고 평가받으려면 사람, 사물, 아이디어 또는 프로세스가 기본적으로 높은 수준의 의미를 가져야 합니다.
둘째, 교육학적 관점에서 볼 때 의미의 정도는 실존적 자아뿐만 아니라 해당 관점(Splitter 2009)의 중요한 속성입니다. 따라서 의미 정도라는 개념을 통해 진정성을 이해하는 것은 여기에서 확인된 진정성의 다른 가치에 내재되어 있기 때문에 의문을 제기할 수 있습니다.
그러나 우리는 고등 교육에서 그리고 고등 교육을 통해 진정성을 향상시키는 데 중요하기 때문에 이 아이디어를 별도로 다루었습니다(Kreber 2013 참조). 이를 별개의 가치로 다루는 것은 위에서 설명한 것처럼 의식, 책임, 소유권, 보살핌에 관한 실존적 아이디어의 중요성을 강조하는 데 도움이 됩니다. 이러한 의미에서 우리는 진정한 자아가 다소 개인적인 의미를 지닌 경험('현실 세계'에 해당하거나 그렇지 않은 경험)에 따라 다르게 영향을 받는다고 주장합니다. 개인적 의미를 지닌 경험은 부과된 과제와 필수 지식을 포함하는 교육 시스템에서 항상 제공되는 것은 아니며, 학생들은 학습 과제에서 주인의식과 책임감에 따라 의미를 찾을 가능성이 더 높습니다. The idea that a degree of meaning constitutes a value of authenticity is twofold.
First, as noted in the introduction, while the concept of authenticity is complex and context dependent, it has an inherent positive attribute. In this sense, to be regraded authentic, a person, an object, an idea or a process must by default have a high degree of meaning.
Second, from a pedagogical perspective, a degree of meaning is an important attribute of the corresponding view (Splitter 2009) as well as of the existential self. As such, understanding authenticity through the idea of a degree of meaning could be questioned because it is inherent to the other values of authenticity identified here.
However, we have treated this idea separately because of its importance for enhancing authenticity in and through higher education (see Kreber2013). Having this as a distinct value serves to emphasise the importance of existential ideas around consciousness, responsibility, ownership and care, as outlined above. In this sense, we argue that the authentic self is influenced differently by experiences (‘real world’ corresponding or otherwise) that have more or less personal meaning. Experiences that have personal meaning are not always available in a system of education that includes imposed tasks and required knowledge, and students are more likely to find meaning in a learning task depending on the sense of ownership and responsibility it animates in them.
학습이 학생에게 의미를 가져야 한다는 생각은 단순히 '암기식 학습'에 반대하여 '의미 있는 학습'을 경험하는 것에 관한 것이 아닙니다(Novak 2002; Ramsden 2003). 또한 의미 있는 지식은 학습자가 이미 알고 있고 할 수 있는 것을 기반으로 구축되어야 한다는 구성주의적 관점도 아닙니다. 여기서 우리가 관심을 두는 것은 학습 경험의 맥락에서 개인적 의미를 개발하는 것입니다(Rawson 2000). Rawson에 따르면, 개인적 의미는 학생이 스스로 지식을 탐색하고, 어느 정도의 자기 결정권과 주제와 맥락을 초월할 수 있는 잠재력을 제공하는 활동에 참여할 때 가장 잘 달성됩니다. 이러한 의미에서 의미 있다는 것은 학생이 중요하거나 가치 있다고 판단하는 경험을 의미하며, 결과적으로 다른 진정성 가치와도 잘 부합합니다. 또한 하이데거와 사르트르에 따르면 학습자 개개인은 항상 더 넓은 사회적 맥락에서 주체이며, 개인의 의미는 더 넓은 커뮤니티의 다른 사람들을 통해 구성되고 그들과 공유된다고 주장합니다. The idea that learning should have meaning for a student is not just about experiencing ‘meaningful learning’ as opposed to ‘rote learning’ (Novak2002; Ramsden2003). Neither is it about the constructivist view that to have meaning knowledge should be built on what the learner already knows and can do. What we are concerned about here is developing personal meaning in the context of the learning experience (Rawson2000). According to Rawson, personal meaning is best achieved when students are engaged in their own search for knowledge, an activity that offers a degree of self-determination and the potential to transcend both subject and context. Being meaningful in this sense is about an experience that the student determines to be significant or worthwhile, and as a consequence fits well with other authenticity values. In addition, following Heidegger and Sartre, we also argue that the individual learner is always a subject in a wider social context and that personal meaning is both constructed through, and shared with, others in a wider community.
'진정성 있는' 연구를 통한 학부생 교육 Teaching undergraduate students through ‘authentic’ research
우리는 진정성의 세 가지 렌즈를 사용하여 오타고 대학의 생태학 프로그램에서 진정성 있는 연구에 대한 우리의 주장을 재고했습니다. 이 작업을 돕기 위해 이론적 아이디어를 출발점으로 삼아 각 아이디어를 교육, 커리큘럼, 지식 및 학생 학습 결과에 대한 아이디어와 연결하는 프레임워크가 개발되었습니다. 이를 통해 우리는 생태학 분야의 진정한 학부 연구를 구성하는 요소에 대한 보다 자세한 설명을 만들었습니다(표 1). 이 표에는 생태학 프로그램의 현재 관행 중 일부가 진정성에 대한 요건을 충족한다고 주장할 수 있는 개념이 포함되어 있지만, 더 중요한 것은 이러한 개념이 현상에 대한 이해를 발전시키는 데 도움이 된다는 것입니다. 프레임워크를 설명한 후에는 연구를 통한 다른 형태의 학부 교육이 이 진정성 프레임워크와 어떻게 비교되는지 논의할 것입니다.
Using the three lenses of authenticity we have reconsidered our claim to authentic research in the ecology programme at the University of Otago. To help us in this task a framework was developed that took the theoretical ideas as a starting point and then connected each of these to ideas about teaching, curriculum and outcomes for knowledge and student learning. In doing so we have produced a fuller explanation of what we consider constitutes authentic undergraduate research in ecology (Table 1). The table includes concepts that allow us to claim that parts of the present practices in the ecology programme meet the requirements for authenticity, but more importantly, these concepts assist our developing understanding of the phenomenon. After explaining the framework, we will discuss how other forms of undergraduate teaching through research compare with respect to this framing of authenticity.
이 프레임워크는 특정 맥락에서 진정성의 핵심 가치로 간주되는 것을 통합합니다. 이러한 가치는 커리큘럼을 조정할 때 교사가 집중해야 하는 주요 개념과 일치합니다(Biggs and Tang 2011). 표 1에서 정렬은 커리큘럼 설계, 교수 전략 또는 특정 교수 철학의 채택을 통해 초점 포인트를 적용하는 것을 의미합니다. 따라서 우리는 '실제 세계'에서 과학이 수행되는 방식을 반영하는 보다 응용적 속성과 실존적 자아에 대한 철학적 요소를 함께 가져옵니다. 그러나 결정적으로, 진정성은 맥락에 따라 달라지고 사회적으로 구성되기 때문에 이 프레임워크는 진정성을 주장하는 데 필요한 의미의 정도를 전달합니다. 따라서 연구를 통한 진정성 있는 교육 모델은 학생에게 연구에 대한 주인의식을 고취시켜야 하며, 이는 학생에게 과제에 대한 책임과 동료에 대한 보살핌을 맡기고, 교사는 전문적인 지원을 제공함으로써 달성됩니다. 따라서 이 프레임워크는 이론적 요소뿐만 아니라 실제적 요소도 포함하고 있습니다. 언급된 결과 중 많은 부분이 측정하거나 평가하기 어려운 것은 사실이지만, 더 많은 경험적 테스트가 필요하지만 현재 연구를 통해 다양한 교육 모델과 비교하여 검토할 수 있습니다. The framework incorporates what we consider the core values of authenticity within our particular context. These values are then matched with the main concepts that teachers would need to focus on when aligning a curriculum (Biggs and Tang2011). InTable 1alignment refers to the application of focus points, either through curriculum design, teaching strategies or adopting specific teaching philosophies. As such we bring together the more applied attributes of mirroring how science is done in the ‘real world,’ and philosophical elements of the existential self. But crucially, since authenticity is context dependent and socially constructed, the framework conveys the degree of meaning necessary for claiming authenticity. Thus conceived, an authentic model of teaching through research should promote students’ sense of ownership over the research, which is achieved by entrusting them with the responsibility for the work and care for their peers, while teachers provide expert support. The framework therefore contains theoretical as well as practical elements. It is certainly the case that many of the outcomes noted will be difficult to measure or evaluate, but while more empirical testing is required, it is currently possible to examine it against different models of teaching through research.
이 프레임워크를 뒷받침하기 위해 Chinn과 Malhotra(2002)는 듀이(1938)가 사용한 용어인 '진정한 탐구'와 관련된 인지적 과정에 대한 포괄적인 개요를 제공합니다. 이러한 과정에는 자신의 연구 질문 생성, 복잡한 절차의 발명, 자신의 결과에 대한 의문 제기, 다양한 형태의 논증 사용, 이전 연구의 (때로는 상충되는) 결과의 사용 등이 포함됩니다. 이러한 과제는 학생의 주인의식과 고차원적인 학습 결과로 이어집니다. 그러나 일부 저자는 완전히 다른 패러다임과 관련하여 진정성을 주장하기도 했습니다. 따라서 진정한 탐구 또는 연구, 즉 '진짜 과학을 하는 것'에 대한 단순한 이해는 일반적으로 공유되지만, 우리의 프레임워크에서는 진정성이라는 하나의 가치로만 구성됩니다. 진정성에 대한 유일한 척도를 갖는 것과는 대조적으로, 이 프레임워크를 구성하는 일련의 가치들은 필연적으로 연구를 통해 근본적으로 일관된 형태의 교육을 초래할 것입니다. 이 주장을 받아들인다면, 생태학에 대한 우리의 주장을 포함하여 모든 주장이 그 자체로 진정성이 있을 수 있는지에 대한 의문이 제기됩니다. 우리는 대답은 '아니오'라고 제안하며, 여기에 제시된 프레임워크가 연구 모델을 통한 진정한 교육을 설계하는 데 어느 정도 유연성을 허용하지만, 적절하고 인식 가능한 경계를 설정하기 때문에 충분히 제약적이라는 점에 유의해야 합니다. In support of the framework, Chinn and Malhotra (2002) provide a comprehensive overview of the cognitive processes implicated in what they call ‘authentic inquiry,’ a term also used by Dewey (1938). These processes include the generation of one’s own research questions, the invention of complex procedures, the questioning of one’s own results, the employment of multiple forms of argument, the use of (sometimes conflicting) results from previous studies, and more. These tasks lead to both ownership and higher-order learning outcomes for students. However, some authors have made claims for authenticity in relation to quite different paradigms. Therefore, while the simple understanding of authentic inquiry or research – namely ‘doing real science’ – is commonly shared, in our framework it constitutes only one value of authenticity. In contrast to having a sole measure for authenticity, the set of values constituting this framework will inevitably result in a fundamentally consistent form of teaching through research. If this argument is accepted, then it brings into question whether all claims can be authentic in their own right (including our own for ecology). We suggest the answer is no, and further note that although the framework offered here allows for some flexibility in designing an authentic teaching through research model, it is also sufficiently constraining because it sets adequate and recognisable boundaries.
이를 '실제 세계'의 가치와 관련하여 설명하기 위해 Laursen 외(2010, 2)에 따르면 '실제 연구란 질문, 방법, 일상적인 작업 방식이 해당 분야에 진정성 있는 연구'라고 합니다. 따라서 학부 연구는 진정성에 대한 해당 관점을 주요 특징으로 삼고, 프로그램의 가치나 효과를 평가할 수 있는 기준으로 삼습니다. 같은 저자들은 또한 진정성이 교직원과 학생 모두에게 유익한 것으로 보고 있으며 다음과 같은 점에 주목합니다: To illustrate this with reference to the ‘real world’ value, according to Laursen et al. (2010, 2), ‘real research is an investigation whose questions, methods, and everyday ways of working are authentic to the field.’ Undergraduate research, therefore, privileges the corresponding view of authenticity as a key feature, and positions it as a benchmark according to which the value or effectiveness of a programme could be evaluated. The same authors also see authenticity as being beneficial to both staff and students and note that:
지도교수는 답을 알 수 없지만 자신과 자신의 학문에 관심이 있고, 그 답에 기득권을 가지고 있기 때문에 진짜인 연구 질문에서 시작합니다. 그들은 그 질문의 범위를 정의하고, 제한된 시간 내에 초보 연구자에게 적절한 규모의 프로젝트를 제공하는 접근 방식을 고안한 다음, 의도적으로 가르칠 수 있는 순간을 활용합니다. (Laursen 외. 2010, 205) Advisors begin with a research question that is real because its answer is unknown but of interest to them and their discipline; they have vested interest in its answer. They define the scope of that question and devise approaches to it that offer a right-sized project to a novice researcher with a limited time frame, then purposefully exploits its teachable moments. (Laursen et al. 2010, 205)
그러나 진정성 있는 연구에 대한 이러한 관점에도 문제가 없는 것은 아닙니다. 이러한 연구 프로젝트는 교실을 넘어서는 관련성이 있고 독창적이라는 측면에서 진정성이 있을 수 있지만, 학생들의 독창성, 창의성 및 아이디어와 관련된 측면에서는 그렇지 않을 수 있습니다. 또한 Hung과 Chen(2007)의 말을 빌리자면, 이 모델은 과학자로서의 정체성을 형성하고 교양을 쌓는 진정한 학습의 과정 차원에서는 부적절할 수 있습니다. 마찬가지로, 우리의 프레임워크를 사용하면 이러한 모델이 '실제' '지식 결과' 기준의 일부 요소를 충족할 수 있지만 학생의 기여도를 완전히 인정받지 못할 수도 있습니다. 또한 학생이 연구 설계 및 수행에 대한 책임이 있다는 의미에서 프로젝트를 소유하지 않기 때문에 세 가지 가치 범주에 걸친 학생의 성과가 실현될 가능성이 낮습니다. This view of authentic research, however, is not without problems. Such a research project could be authentic in terms of having relevance beyond the classroom and being original, but not so much in relation to students’ originality, creativity and ideas. And, borrowing from Hung and Chen (2007), this model may be inadequate for the process dimension of authentic learning, where identity formation and enculturation as scientists are developed. Similarly, using our framework, whereas such a model may satisfy some elements of the ‘real-world’ ‘knowledge outcomes’ criterion, the contribution of the student may not be fully recognised. In addition, student outcomes across the three value categories are unlikely to materialise because the student does not own the project in the sense of having the responsibility for designing and performing the research.
다른 학생 연구 모델도 있으며, 미국에서는 학부생이 기존 과학 연구팀에서 견습생으로 일할 수도 있습니다(Laursen 외. 2010). Grabowski, Healy, Brindley(2008)는 학부생이 교수진의 연구 프로젝트와 매칭되어 구직 지원과 유사한 과정을 거치는 프로그램을 조사했습니다. 오버하우저와 르분(2012)은 학부생이 시민 과학이라는 더 넓은 틀 안에서 연구에 참여하는 약간 다른 사례를 조사합니다. 이 모델에서 학생들은 연구 설계, 프로토콜 테스트, 데이터 수집, 출판물 공동 저술과 같은 다양한 연구 과제를 수행했으며, 이 모든 과제는 진정성 있는 것으로 간주되었습니다. 그러나 이 연구의 대부분이 여름 방학 동안 이루어졌고, 얼마나 많은 학생이 프로젝트에 참여했는지 명확하지 않았으며, 학생들이 다른 실제 하위 과제에 참여했을 수 있기 때문에 전체 연구 과정을 경험했는지 또는 얼마나 많은 학생이 경험했는지는 확실하지 않습니다. There are other models of student research and in the United States, undergraduates may work as apprentices in an established scientific research team (Laursen et al.2010). Grabowski, Healy, and Brindley (2008) examine a programme where undergraduate students are matched with faculty members’ research projects in a process that resembles a job application. Oberhauser and LeBuhn (2012) examine a slightly different example whereby undergraduate students engage in research within a broader framework of citizen science. In this model students performed different research tasks such as study design, protocol testing, data collection and co-authoring publications, all of which were deemed authentic. It seems, however, that much of this research was done over summer breaks, it was not clear how many students were involved in the project, and because students may have been involved in different authentic sub-tasks it is not certain if or how many experienced the complete research process.
학부 연구에 대한 접근 방식에 대한 간략한 논의에서 Harvey와 Thompson(2009, 13)은 진정한 학부 연구 경험이란 '발표 및 출판을 목표로 연구를 수행하는 지적 동료로서 한 명 이상의 학생을 참여시키는 교수 주도 프로젝트'라고 주장합니다. 저자들이 인정하듯이 이 접근 방식에는 소수의 선별된 학생만 참여할 수 있고 교수의 연구 관심사에 치우칠 수 있지만, 지속 가능한 모델이 될 수 있습니다. 결정적으로, 학생의 참여는 인지적으로나 인식론적으로 유의미해야 하며, 의미 있는 협업으로 이어져야 하는데, 이는 위에서 언급한 다른 견습 모델보다 더 중요한 요건일 수 있습니다. 그러나 저자들이 이 견습 모델이 지속 가능한 상생 모델이라는 보다 명시적인 주장과 '실제 과학을 하는 것'이라는 암묵적인 주장 외에 왜 이 모델이 진정성 있는 것으로 간주되는지는 명확하지 않습니다. In their brief discussion of approaches to undergraduate research, Harvey and Thompson (2009, 13) maintain that an authentic undergraduate research experience is ‘a faculty-led project [that] engages one or more students as intellectual colleagues who conduct research directed toward presentation and publication.’ This approach would include, as the authors admit, only a small and selective number of students and would lean towards the teacher’s research interest, but this would make it a sustainable model. Crucially, students’ involvement should be cognitively and epistemically significant, resulting in a meaningful collaboration, a requirement that perhaps goes further than some of the other apprenticeship models mentioned above. It is not entirely clear, however, why this apprenticeship model is deemed authentic by the authors, beyond the more explicit claim that it is a win-win sustainable model and the implicit claim that it is about ‘doing real science.’
연구 견습생 관련 문헌을 검토한 새들러와 맥키니(2010)는 여러 연구에서 이러한 직책을 맡은 학부생이 지식과 기술 수준이 향상되었다는 증거를 발견했다고 언급했습니다. 그러나 이 저자들은 '이러한 경험이 데이터 분석, 질문 제기, 가설 세우기 등 인식론적으로 더 까다로운 관행을 포함하도록 발전하지 않으면 고차원적인 결과에 대한 학습 이득이 제한될 수 있다'는 우려를 표명합니다(Sadler and McKinney 2010, 48). 따라서 학생들이 '실제' 연구에 참여할 수는 있지만, 어떤 역할이나 과제를 수행해야 하는지, 주인의식, 책임감, 관심을 통해 의미를 가질 수 있을 만큼 연구 과정을 충분히 경험할 수 있는지 여부가 항상 명확하지는 않습니다. In a review of the research apprentice literature, Sadler and McKinney (2010) noted that several studies found evidence that undergraduate students that held such positions improved their level of knowledge and skills. However, these authors express a concern that ‘if these experiences do not evolve to include more epistemically demanding practices, such as data analysis, question posing, and hypothesizing, then learning gains on higher-order outcomes will likely be limited’ (Sadler and McKinney2010, 48). Thus, students may be involved in ‘real-world’ research but it is not always clear what roles or tasks they are required to perform and whether or not they get to experience enough of the research process for it to have meaning through a sense of ownership, responsibility and care.
또한, 도제식 모델에서 '실제' 연구를 통한 학습이 대중 고등 교육에 적합한 전략인지에 대한 적절한 의문이 제기되고 있습니다. 소수의 재능 있는 학생을 선별하여 연구 기회를 제공하는 것과 모든 능력을 갖춘 다수의 학생이 독창적인 연구를 수행하여 학습하는 것은 결코 같을 수 없기 때문에 이 질문은 중요합니다. 예를 들어, Gardner 등(2015)은 '떠오르는 대학 신입생'(62명)을 포함한 견습생 연구 프로그램을 연구했는데, 그 수는 공개되지 않았지만 8명의 학생이 연구 참여에 동의했습니다. 따라서 이 프로그램은 상대적으로 소수의 뛰어난 능력을 가진 학생들을 대상으로 한 것으로 보입니다. 반면, 우리의 프레임워크는 연구를 통한 진정한 교육을 학급의 모든 학생을 위한 커리큘럼에 통합할 수 있는 지침을 제공하는 것을 목표로 합니다. Moreover, there is a pertinent question as to whether learning through ‘real-world’ research in an apprenticeship model is a viable strategy for mass higher education. This question is important since selectively identifying a small number of talented students for research opportunities is by no means the same as getting a large number of students of all abilities to learn by carrying out original research. Gardner et al. (2015), for instance, studied an apprenticeship programme of research that included what they describe as ‘rising college freshmen’ (62), and while their number was not disclosed, eight student agreed to take part in the study. It seems, therefore, that this programme was targeted at relatively small number of exceptionally capable students. In contrast, our framework aims to provide guidance for the incorporation of authentic teaching through research into a curriculum for all students in a class.
2000년대 초 오타고 대학교의 생태학 프로그램이 재설계되었을 때 주요 목표 중 하나는 비판적 사고 능력을 개발하는 것이었습니다. 과학자가 되는 법을 배우는 것도 우선 순위가 높았지만 이는 대부분 비판적 사고의 범주에 속했습니다. 그러나 이 두 가지 모두 학생들이 진정한 연구에 참여하게 함으로써 달성할 수 있는 목표였습니다(Spronken-Smith 외. 2011). Spronken-Smith 외(2011, 732)는 '생태학 프로그램의 탐구는 학생에게 새로운 지식을 창출하고 궁극적으로 과학에 새로운 지식을 제공할 수 있는 모든 기회가 있어야 한다는 의미에서 진정성이 있었다'고 말합니다... [프로그램의 3년 동안의] 모든 연구 활동은 생태학자의 작업 측면을 다루기 때문에 이런 의미에서 모두 진정성이 있다'고 설명합니다. 앞서 언급한 '실제 세계'에 상응하는 진정성에 대한 주장은 좀 더 심도 있는 설명이 필요합니다. When the ecology programme at the University of Otago was redesigned in the early 2000s one of the main aims was to develop critical thinking skills. Learning to be a scientist also featured high as a priority, but this largely fell within the parameters of critical thinking. Both, however, were to be achieved through getting students engaged in authentic research (Spronken-Smith et al.2011). Spronken-Smith et al. (2011, 732) note that ‘the inquiry in the ecology programme was authentic in the sense that there had to be every chance of new knowledge being created for the student and eventually new knowledge to science … All research activities [over three-years of the programme] cover aspects of an ecologist’s work so, in this sense, they are all authentic.’ This earlier claim to ‘real world’ corresponding authenticity requires some more in-depth explanation.
커리큘럼은 모든 학생이 대학에 처음 입학할 때부터 연구자로서의 훈련을 받도록 설계되어 3년 동안의 경험 중 일부는 연구를 통해 배우는 데 중점을 두어 연구를 수행하도록 합니다. 연구 활동은 학생들의 현재 능력에 맞게 조정되며, 프로그램이 진행됨에 따라 기대되는 연구 수준이 높아져 결국에는 고급 대학원생이나 심지어 학부 교사의 작업과 비슷해집니다(Harland 2016). 이 프로그램은 학생들이 완전히 설계하고 주도하는 캡스톤 연구 프로젝트로 마무리됩니다. 이 연구 프로젝트의 준비는 프로그램에 참여한 교사들이 연구를 수행하는 방식을 면밀히 따릅니다. 학생들은 짝을 이루어 2학년 때 짧은 현장 학습을 통해 다양한 생태계를 탐험한 후, 3학년 프로젝트에 대한 연구 제안서와 함께 보조금 신청서를 작성합니다. 이 보조금 신청서는 교직원과 학생이 모두 참여하는 이중 맹검 동료 검토 과정을 거치며, 피드백은 연구 설계를 개선하는 데 사용됩니다. 프로그램 3년차에는 학생들이 연구 프로젝트를 수행하고 보고서를 작성합니다. 이러한 프로젝트에서 생성된 지식은 해당 분야에 새로운 지식일 가능성이 높으며, 지난 몇 년 동안 일부는 기존 학술지(Harland, Wald, Randhawa 곧 출간 예정)에 연구를 발표하기도 했습니다. 그러나 이 프로그램은 미래의 학자를 양성하는 것이 목적이 아니라 학생 연구자로서의 작업을 통해 모든 학생의 개인적 성장을 촉진하고자 합니다(Harland 2016). The curriculum is designed so that all students are trained as researchers from when they first start at university so that a part of their experiences over three years focuses on learning through research by learning to do research. Research activities are aligned to students’ current abilities and as they progress in the programme, the expected level of research increases so that eventually their work resembles that of more advanced postgraduate students or even of their academic teachers (Harland2016). The programme concludes with a capstone research project that isfully designed and led by the students. The preparation of this research project follows closely how the teachers in the programme do research. Working in pairs, and following a short fieldtrip in second-year where students explore a number of different ecosystems, students write a grant application with a research proposal for the third-year project. This grant application goes through a double-blind peer-review process involving both staff and students, and the feedback is then used to improve the research design. In the third year of the programme, students conduct their research projects and write their reports. The knowledge generated in these projects has every chance of being new to the discipline and in past years some have published their research in established journals (Harland, Wald, and Randhawa forthcoming). The programme, however, does not aim to train future academics; instead, it wishes to promote the personal growth of all students through their work as student-researchers (Harland2016).
이 모델에는 '실제 과학 수행'이라는 익숙한 형태로 '실제 세계'와의 대응이 포함될 수 있지만, 우리는 더 이상 이것만으로는 '진짜authentic'라고 부르기에 충분하다고 주장하지 않습니다.오히려 연구를 통한 교육이 진정성을 가지려면 학생들이 자신이 선택한 학문 분야에서 학습자이자 연구자로서, 그리고 교실 밖에서도 자아를 긍정적이고 의미 있게 발전시킬 수 있어야 한다는 것이 우리의 견해입니다. 진정성 있는 학습자는 자신의 가치와 행동에 대한 지식을 얻고 이것이 자신과 타인에게 어떤 영향을 미치는지 알게 됩니다. 학생들의 의식에 대한 이러한 실존적 효과는 학생들이 더 큰 책임감을 갖도록 장려하고 연구를 결정할 수 있는 더 많은 자유를 부여하는 커리큘럼을 통해 달성됩니다. 이 주장을 받아들인다면, 이러한 교육 모델에서 연구는 독창적일 뿐만 아니라 대부분 학생이 주도해야 한다는 결론이 나옵니다. 표 2는 생태학 프로그램의 캡스톤 프로젝트에서 학생과 교사가 책임져야 하는 '실제' 과제를 세분화하여 보여줍니다. The ‘real-world’ correspondence may be embedded in this model in the familiar form of ‘doing real science,’ but we would no longer claim that this in itself is sufficient for calling it ‘authentic.’ Rather, it is our view that for teaching through research to be authentic, it should positively and meaningfully enable students to develop their sense of self, both within their chosen discipline as learners and researchers, and beyond the classroom. The authentic learner gains knowledge about his or her values and actions and how these impact on self and others. This existential effect on students’ consciousness is achieved by a curriculum that encourages them to assume greater responsibility and that gives them more freedom to determine their research. If this argument is accepted, then it follows that in such a pedagogical model research should be not only original but also largely student-led.Table 2breaks down ‘real-world’ corresponding tasks and shows what students and teachers assume responsibility for in the capstone project of the ecology programme.
이러한 책임은 진정한 자아의 일부이지만, 이것이 프로젝트 주인의식을 전제로 하는 개인적으로 의미 있는 경험과 어떻게 관련될지 예측하기는 더 어려워 보입니다. 학생에게 책임감을 부여하고 프로젝트를 설계하도록 요구할 수는 있지만, 진정성에 대한 우리의 관점에서 진정으로 느껴야 하는 소유권을 부여할 수는 없습니다(Barnett 2007). 지금까지는 코스 평가에서 주인의식이 특히 학습자이자 연구자로서 자신감을 키우는 데 매우 중요하다는 사실이 일관되게 밝혀졌다는 사실 외에 이러한 경험이 학생들에게 어떤 의미를 갖는지는 명확하지 않았습니다. 진정성의 맥락에서 우리는 진정성 있는 학습 경험에 어느 정도의 개인적 의미가 필요한지 묻고 있습니다. 우리가 결정해야 할 것은 의미가 학습자이자 생태학자가 되는 데, 그리고 궁극적으로 한 사람의 존재와 자아가 되는 데 어떤 영향을 미치는지입니다(Barnett 2007). 그런 다음 이것이 공동 연구 커뮤니티 내에서 일하는 것과 어떤 관련이 있는지, 그리고 나중에 학생들이 사회에 더 광범위하게 기여하는 방법과 어떤 관련이 있는지 확인해야 합니다.
Such responsibility is part of the authentic-self but it seems more difficult to predict how this might relate to personally meaningful experiences that are predicated on the idea of project ownership. Students may be given responsibility and be required to design a project, but they cannot be given ownership, which has to be genuinely felt (Barnett2007) in our view of authenticity. To date it has not been clear what the experiences have meant to students, beyond the fact that course evaluations have consistently shown that ownership has been very important, particularly with respect to students growing in confidence as both learners and developing researchers. In the context of authenticity we are asking whatdegreeof personal meaning is required for an authentic learning experience. What we need to determine is how meaning impacts on becoming a learner and an ecologist, and ultimately on being and becoming one’s own person (Barnett2007). We then need to ascertain how this relates to working within a collaborative research community and perhaps later how students contribute to society more broadly.
전반적으로, 그리고 보다 실용적인 측면에서 볼 때, 연구를 통한 진정한 교육 모델은 대학원 및 학부 연구자들이 지식을 학습하고 생성하는 방식을 최대한 가깝게 따르는 모델이며, 여기에는 여러 가지 기술적 작업뿐만 아니라 연구에 만연한 복잡성, 불확실성, 정치성을 다루어야 하는 것도 포함됩니다. 이 개념에서 학부생은 마치 대학원생처럼 일하기 때문에 일반적으로 이 수준에서 기대할 수 있는 것보다 훨씬 더 큰 학습 책임을 지는 동시에 교수와 훨씬 더 긴밀하고 협력적인 관계를 구축합니다(Harland 2016). 이러한 새로운 관계는 고차원적인 학습 성과와 인식론적으로 까다로운 관행에 대한 요구의 결과입니다. 우리 중 한 명은 수년 동안 이 프로그램에 참여해 왔고 오랫동안 학생들을 연구자로 가르치는 것을 지지해 왔지만, 연구를 통한 교육에서 진정성을 위한 프레임워크의 정교화는 프로그램 개발에서 거의 고려되지 않았던 기술적 과제와 가치를 모두 강조했습니다. 이는 대부분 실존적인 진정한 자아와 의미의 정도와 관련이 있습니다. 이 프레임워크를 통해 우리는 이러한 형태의 교육학, 무엇에 집중해야 하는지, 우리의 가치를 실천과 어떻게 일치시킬 수 있는지 재고할 수 있었습니다. '현실 세계'에 해당하는 과제는 비교적 쉽게 연계할 수 있는 것처럼 보이지만, '존중', '소속감', '풍요로움'과 같은 가치는 학생의 학습 결과에 대한 광범위한 토론에서 거의 주목을 받지 못했으며, Barnett(2007)의 '되기'는 더더욱 그러했습니다. 그러나 우리는 이러한 요소들이 모두 진정한 연구를 통해 학습의 필수적인 부분이라고 주장할 수 있습니다. Overall, and in more pragmatic terms, an authentic model of teaching through research is one that follows as closely as possible how postgraduate and academic researchers learn and generate knowledge, which includes a number of technical tasks as well as having to deal with the complexities, uncertainties and politics that are omnipresent in research. In this conception, undergraduate students work as if they were postgraduate students and so have a far greater responsibility over their learning than might typically be expected at this level, while establishing a much closer and more collaborative relationship with their teachers (Harland2016). These new relationships are a consequence of the drive for higher-order learning outcomes and epistemologically demanding practises. Although one of us has been involved in this programme for many years, and has long been an advocate of teaching students to be researchers, the elaboration of a framework for authenticity in teaching though research has highlighted both technical challenges and values that have received little consideration in the development of the programme. These are mostly related to the existential authentic self and degree of meaning. The framework has allowed us to reconsider this form of pedagogy, what to focus on and how to align our values with practice. Although the ‘real world’ corresponding tasks seem relatively straightforward to align, values such as ‘respect’, ‘belonging’ and ‘enrichment’ have received little attention in wider debates on student learning outcomes; Barnett’s (2007) ‘Becoming,’ even less so. Yet we would argue that they are all an essential part of learning through authentic research.
결론 Conclusions
이 논문은 학부 생태학 프로그램에서 연구를 통한 교육과 관련하여 무엇이 진정성을 구성하는지에 대한 논의에서 시작되었습니다. 과학 교육에서 진정성이란 일반적으로 과학자들이 교실에서 생각하고 작업하는 방식을 그대로 재현하는 것을 의미합니다(Crawford 2015). 그러나 우리의 토론은 진정성에 대해 더 미묘하고 정보에 입각 한 조사를 수행하도록 자극하는 여러 가지 질문을 제기했습니다. 학부생들이 독창적인 연구를 통해 새로운 지식을 창출하는 데 참여하도록 하는 아이디어는 연구를 통한 교수법에서 중추적인 역할을 하며, 진정성은 일반적으로 소위 '실제 세계'와 '대응하는 관점'으로 알려진 것과 관련하여 프레임워크가 구성됩니다(Splitter 2009). This paper was conceived out of a discussion about what constitutes authenticity in relation to teaching through research in an undergraduate ecology programme. The common use of authenticity in science teaching refers to replicating the way in which scientists think and work in the classroom (Crawford2015). Our discussion, however, raised a number of questions that prompted us to carry out a more nuanced and informed inquiry into authenticity. The idea of getting undergraduate students involved in generating new knowledge through original research is pivotal in pedagogies of teaching through research and authenticity is commonly framed in relation to the so-called ‘real world,’ and what has become known as the ‘corresponding view’ (Splitter2009).
그러나 여기에 제시된 진정성에 대한 제안된 프레임워크는 연구를 통한 교육에서 진정성을 구성하는 요소에 대한 보다 복잡한 이해를 제공합니다. 이는 일반적으로 사용되는 '현실 세계'에 해당하는 관점에 진정성의 다른 두 가지 핵심 가치, 즉 실존적 진정한 자아와 의미의 정도를 추가함으로써 그렇게합니다. 하이데거, 아도르노, 사르트르와 같은 실존 철학자들의 연구, 특히 의식, 책임, 소유권, 보살핌과 관련된 진정성에 대한 그들의 분석은 고등 교육 분야의 학자들에 의해 확인되고 사용되어 왔습니다. 그러나 여기서 우리의 주요 기여는 이러한 아이디어를 연구를 통해 교육 맥락에서 '현실 세계'에 대한 상대적으로 더 일반적인 아이디어와 결합하는 것입니다. 실존주의와 밀접한 관련이 있는 의미의 정도는 진정성과 관련된 주로 긍정적인 의미를 반영하며, 이는 다시 우수한 모범의 표현이라는 개념의 더 일반적인 의미를 반영합니다. 이러한 가치들을 종합하면 교사가 주요 초점 포인트와 이러한 포인트가 다양한 결과와 어떻게 연계되는지를 안내하는 프레임워크가 구성됩니다. 이 프레임워크는 커리큘럼을 설계할 때 어느 정도 유연성을 허용하는 동시에 연구를 통해 과학 교육의 맥락에서 우리가 진정성이 있다고 인식하는 것에 대한 명확한 지침과 경계를 제공합니다. The proposed framework for authenticity presented here, however, offers a more complex understanding of what constitutes authenticity in teaching through research. It does so by adding to the commonly used ‘real world’ corresponding view two other core values of authenticity; namely, the existential authentic self and a degree of meaning. The work of existential philosophers such as Heidegger, Adorno and Sartre, and more specifically their analyses of authenticity in relation to consciousness, responsibility, ownership and care, have been identified and used by scholars in higher education. But our main contribution here is joining these ideas together with the relatively more common ideas about the ‘real world’ within the context of teaching through research. A degree of meaning, which is also closely related to existentialism, reflects the predominantly positive connotation associated with authenticity, which in turn echoes the concept’s more common meanings as a representation of a superior exemplar. Put together, these values constitute a framework that directs teachers towards key focus points and how these align with different outcomes. It allows for some flexibility in designing a curriculum while at the same time provides clearer guidance and boundaries for what we perceive to be authentic in the context of science teaching through research.
따라서 제안된 프레임워크는 주로 연구를 통한 진정한 교육 모델이 어떻게 학생들의 개인적, 심지어 직업적 발달에 긍정적이고 의미 있으며 장기적인 효과를 가져올 수 있는지에 초점을 맞추고 있습니다. 프레임워크의 '학생'과 '지식 결과'에는 교육자로서 학생들이 갖추기를 바라는 몇 가지 핵심 가치와 기술이 포함되어 있습니다. 프레임워크의 '초점' 및 '정렬' 구성 요소는 커리큘럼이 이러한 가치와 기타 결과를 심어줄 수 있는 방법에 대한 지침 역할을 합니다. 원하는 결과를 달성하기 위한 이러한 수단은 주로 학생이 주도하고 책임감, 주인의식, 파트너십 및 배려의 개념을 키우는 학습 환경에 의해 조정되는 '실제 세계'에 해당하는 과제에 달려 있습니다. 하지만 이 프레임워크 내에서 '실제 세계' 측면에 대한 몇 가지 좋은 증거가 있지만, 실존과 의미 속성에 대해서는 더 많은 조사가 필요합니다. The proposed framework is thus mainly concerned with how an authentic model of teaching through research could lead to positive, meaningful and long-lasting effects on the personal, and perhaps even professional, development of students. The ‘student’ and ‘knowledge outcomes’ in the framework include some key values and skills that we as educators wish our students to have. The ‘focus’ and ‘alignment’ components in the framework serve as guidance for ways in which a curriculum could instil those values and other outcomes. These means for achieving the desired outcomes predominantly rests on ‘real world’ corresponding tasks that are student-led and moderated by a learning environment that fosters notions of responsibility, ownership, partnership and care. And yet, while we have some good evidence for the ‘real world’ aspects within this framework, the existential and meaning attributes require further inquiry.
ABSTRACT
This conceptual paper is concerned with the discursive and applied attributes of ‘authenticity’ in higher education, with a particular focus on teaching science through student research. Authenticity has been mentioned in passing, claimed or discussed by scholars in relation to different aspects of higher education, including teaching, learning, assessment and achievement. However, it is our position that in spite of the growing appeal of authenticity, the use of the term is often vague and uncritical. The notion of authenticity is complex, has a range of meanings and is sometimes contested. Therefore, we propose here a practice-oriented and theoretically-informed framework for what constitutes authenticity within the context of teaching through research. This framework brings together aspects of the ‘real world,’ existential self, and embedded meaning, and aligns them with different outcomes relating to knowledge and to students. Different models of teaching through research with conflicting claims to authenticity are used to illustrate the framework.
연구-바탕 학습이 효과적인가? 사회과학에서 사전-사후 분석(STUDIES IN HIGHER EDUCATION, 2021) Is research-based learning effective? Evidence from a pre–post analysis in the social sciences Insa Wessels a,b, Julia Rueßa, Christopher Gessa, Wolfgang Deickea and Matthias Zieglerb
소개 Introduction
교육과 연구는 잘 정의된 다양한 교육 형식을 통해 연결될 수 있습니다. 그 중 하나는 학생이 지도 교수자의 도움을 받아 스스로 연구를 수행하는 연구 기반 학습(RBL)입니다. RBL은 현재 의미 있는 학습 경험의 부족과 자극적인 교육 형식의 필요성 등 고등 교육 분야의 다양한 요구를 해결하기 위한 만병통치약으로 여겨지고 있습니다. 따라서 몇몇 저자와 기관은 모든 학문적 연구 프로그램은 아니더라도 많은 학문적 연구 프로그램의 커리큘럼에 RBL을 통합해야 한다고 주장합니다(예: Healey와 Jenkins 2009). 실제로 미국 국립과학재단의 REU 프로그램과 같이 다양한 학문 분야와 형태로 RBL을 구현하려는 프로그램이 점점 더 많이 시도되고 있습니다. 이러한 노력의 주요 목표는 학생들에게 연구 참여를 경험할 수 있는 기회를 제공하는 것입니다.과학, 기술, 공학 및 수학(STEM) 분야에서는 RBL이 실제로 그 약속에 부응하고 효과적인 학습 경험을 구성한다는 증거가 있습니다(Linn 외. 2015). 그러나 STEM 분야 외의 분야에서는 RBL이 어떤 연구 성향을 촉진하는지는 아직 불분명합니다. 따라서 본 연구는 다양한 인지적, 정의적 동기부여적 연구 성향의 습득에 관한 RBL의 효과를 사회과학 분야로 일반화할 수 있는지 살펴보고자 합니다. Teaching and research can be linked through a variety of well-defined instructional formats. One of these is research-based learning (RBL), in which students conduct their own research with the help of a supervisor. RBL is currently seen as a panacea for addressing a range of demands within higher education, e.g. a lack of meaningful learning experiences and the need for stimulating instructional formats. Accordingly, several authors and institutions claim that RBL should be incorporated into the curriculum of many if not every academic study programme (e.g. Healey and Jenkins2009). Indeed, a growing number of programmes have attempted to implement RBL in a range of disciplines and forms, e.g. the REU programme by the US National Science Foundation. The main goal of these endeavours is to provide students with an opportunity to experience participation in research. In science, technology, engineering, and mathematics (STEM) disciplines, there is evidence that RBL does indeed live up to its promises and constitutes an effective learning experience (Linn et al.2015). However, outside the STEM disciplines, it is still unclear which research dispositions RBL fosters. Thus, this study aims to examine whether RBL’s effectiveness regarding the acquisition of various cognitive and affective-motivational research dispositions can be generalised to the social sciences.
이론적 배경 Theoretical background
다른 형태의 연구 관련 교육과 관련하여 연구 기반 학습의 포지셔닝 Positioning research-based learning in relation to other forms of research-related teaching
교육과 연구는 다양한 방식으로 연결될 수 있습니다. 널리 사용되는 모델에서 Healey와 Jenkins(2009)는 두 가지 축을 따라 학생을 연구에 참여시키기 위한 다양한 교육 형식을 구분합니다.
첫 번째 축은 연구 결과 또는 연구 과정 중 어느 쪽을 강조하는지를 설명합니다.
다른 축은 학생이 참여자로서 능동적인 역할을 맡는지, 아니면 청중으로서 수동적인 역할을 맡는지를 설명합니다.
이 두 축은 네 가지 형식으로 결합할 수 있습니다: 연구-지도형, 연구 주도형, 연구 중심형, 연구 기반 학습입니다. RBL에서는 교수자가 연구 과정에 초점을 맞추고 학생은 능동적으로 연구와 탐구를 수행합니다. 그러나 이러한 설명은 학생의 연구 참여의 정확한 본질을 설명하지 못합니다. Huber(2014)는 RBL을 학생이 자신의 연구 질문에 따라 자율적인 방식으로 전체 연구 과정을 진행하는 교육 형식으로 정의합니다. 교수자는 촉진자 역할을 맡습니다. 이론적으로 도출된 이 정의는 연구 관련 형식의 경험적 분류(Rueß, Gess, Deicke 2016)에서 재현되었으며, 현재 연구에서 RBL의 기본 정의로 사용됩니다.각주1 Teaching and research can be linked in different ways. In a popular model, Healey and Jenkins (2009) distinguish among different instructional formats for engaging students in research along two axes. The first axis describes whether the research results or the research process is emphasised. The other axis describes whether students take on an active role as participants or a passive role as audience. These two axes can be combined into four different formats: research-tutored, research-led, research-oriented and research-based learning. In RBL, teaching focuses on the research process, and students actively conduct research and inquiry. However, this description fails to describe the exact nature of students’ involvement in research. Huber (2014) further defines RBL as an instructional format in which students work through the entire research process in a self-regulated manner, guided by their own research questions. The instructor takes on a facilitating role. This theoretically derived definition was replicated in an empirical classification of research-related formats (Rueß, Gess, and Deicke2016) and serves as the underlying definition of RBL in the current study.Footnote1
연구 기반 학습의 효과 The effectiveness of research-based learning
자신의 연구 프로젝트를 수행하는 것은 다양한 인지적, 행동적, 정서적 경험을 수반하며(Lopatto, 2009, 29), 이는 결과적으로 RBL과 관련된 다양한 이점으로 이어집니다. Conducting one’s own research project involves various cognitive, behavioural, and affective experiences (Lopatto,2009, 29), which in turn lead to a wide range of benefits associated with RBL.
RBL은 과학적 커리어를 육성할 수 있기 때문에 장기적인 사회적 혜택과 관련이 있습니다: RBL에 참여한 학생들은 대학원 교육 또는 박사 학위 취득에 더 큰 관심을 보였으며(Lopatto 2007; Russell, Hancock, McCullough 2007), 졸업 후 6년 후에도 과학 관련 직업에 종사할 가능성이 더 높았습니다(Hernandez et al. 2018). RBL is associated with long-term societal benefits because it can foster scientific careers: Students participating in RBL reported a greater interest in pursuing postgraduate education or PhDs (Lopatto2007; Russell, Hancock, and McCullough2007) and were more likely to be engaged in scientific careers six years after graduation (Hernandez et al.2018).
또한 RBL은 학계 밖의 직업에도 필요한 연구 기술을 육성합니다(British Academy 2012). RBL은 데이터나 상황을 객관적으로 검토하고 문제 해결의 즐거움을 찾는 능력, 즉 '연구자적 사고방식'을 개발하는 데 도움이 된다고 합니다(Wood 2003). 연구자의 사고방식은 다양한 직업 활동에서 효과적일 수 있습니다. 예를 들어 심리 치료 분야에서 치료사는 연구 지식을 활용하여 새로운 치료 접근법에 대한 증거를 참조할 수 있습니다(Levant 외. 2006). 따라서 연구 관련 지식과 기술을 습득하는 것은 과학 및 비과학 분야 모두에서 성공적으로 커리어를 쌓기 위한 전제 조건이며, 이는 이 글의 적절한 초점입니다. In addition, RBL fosters research skills that are also necessary for occupations outside academia (British Academy2012). RBL is said to facilitate the development of a ‘researcher’s mindset’ – the ability to objectively examine data or a situation and finding enjoyment in solving problems (Wood2003). A researcher’s mindset can be effective in a wide range of professional activities. For example, in the field of psychotherapy, therapists could draw upon their research knowledge to consult evidence on new therapeutic approaches (Levant et al.2006). Hence, the acquisition of research-related knowledge and skills is a prerequisite for successfully engaging in both scientific and non-scientific careers – making it an appropriate focus for our article.
과제를 성공적으로 수행하려면 지식과 같은 인지적 성향과 이러한 지식을 실천에 옮기기 위한 정서적 동기 부여 성향이 모두 필요합니다(Blömeke, Gustafsson, Shavelson 2015). 성향은 특정 상황에서 개인이 일반적으로 어떻게 행동할지를 결정하는 다양한 잠재적, 개인적 자원(예: 태도, 특성 및 능력)을 나타내는 포괄적인 용어입니다(Schmidt-Atzert와 Amelang 2012, 63). 따라서 연구 영역에서 유능한 성과를 내기 위해서는 다양한 인지적(예: 지식) 및 정서적-동기적(예: 흥미) 연구 성향이 필요합니다. RBL이 다양한 인지적 및 정의적-동기적 연구 성향의 개발을 촉진하는 데 효과적인지 여부는 이전 연구의 초점이었습니다. 기존 증거는 다음 섹션에서 소개합니다. Successfully engaging in a task requires both cognitive dispositions, such as knowledge, and affective-motivational dispositions to put this knowledge into practice (Blömeke, Gustafsson, and Shavelson2015).Dispositionserves as an umbrella term to denote a range of latent, personal resources (e.g. attitudes, traits and abilities) that determine how an individual will normally act in a certain situation (Schmidt-Atzert and Amelang2012, 63). Accordingly, competent performance in the research domain requires various cognitive (e.g. knowledge) and affective-motivational (e.g. interest) research dispositions. Whether RBL is effective at facilitating the development of different cognitive and affective-motivational research dispositions has been the focus of previous studies. The existing evidence will be introduced in the following sections.
인지적 이득 Cognitive gains
RBL의 효과에 대한 대부분의 경험적 연구는 인지적 연구 성향에 초점을 맞추고 있습니다. 그러나 이러한 연구의 대부분은 STEM 학생을 평가했으며(예: Linn 외. 2015; Seymour 외. 2004), 사회과학 분야에서 RBL의 효과를 조사한 연구는 소수에 불과합니다. 사회복지학 분야의 한 연구에서 학생들은 영역 전반의 연구 지식을 습득했습니다(Whipple, Hughes, Bowden 2015). 타라반과 로그(2012)는 심리학 학생들이 연구에 참여함으로써 연구 방법 기술 향상과 같은 다양한 인지적 이점을 얻을 수 있다는 증거를 발견했습니다. RBL에 참여하면 과학적 과정 전반에 대한 이해도도 높아질 수 있습니다(Lloyd, Shanks, Lopatto 2019). Most empirical studies on the effectiveness of RBL focus on cognitive research dispositions. However, the majority of these studies assessed STEM students (e.g. Linn et al.2015; Seymour et al.2004), with only a few studies investigating the effect of RBL in the social sciences. In a study from the field of social work, students gained domain-general research knowledge (Whipple, Hughes, and Bowden2015). Taraban and Logue (2012) found evidence for a range of cognitive benefits of psychology students’ participation in research, such as improved research methods skills. Participation in RBL can also lead to increased understanding of the scientific process as a whole (Lloyd, Shanks, and Lopatto2019).
다른 연구자들은 개별 연구 단계와 관련된 특정 기술, 예를 들어 통계 소프트웨어 사용 능력(Whipple, Hughes, Bowden 2015), 연구 결과의 전달 및 발표 능력(Stanford 외. 2017)을 조사했습니다. 또한 RBL은 비판적 사고(Hunter, Laursen, Seymour 2007; Kilgo, Ezell Sheets, Pascarella 2015)와 독립적으로 작업하는 능력(Stanford 외. 2017)과 같은 보다 일반적인 인지적 성향을 촉진하는 것으로 보입니다. Other researchers have examined specific skills pertaining to individual research steps, e.g. the ability to use statistics software (Whipple, Hughes, and Bowden2015) and communicating and presenting one’s research (Stanford et al.2017). RBL also seems to facilitate more general cognitive dispositions like critical thinking (Hunter, Laursen, and Seymour2007; Kilgo, Ezell Sheets, and Pascarella2015) and the ability to work independently (Stanford et al.2017).
따라서 사회과학에서 RBL은 다양한 인지적 성향을 촉진하는 데 효과적인 것으로 보이지만, 이러한 결과는 예비적 증거로만 사용될 수 있습니다. 이 분야의 이러한 연구와 다른 연구들의 해석 가능성과 관련된 문제는 방법론적 설계에 있습니다: 대부분의 기존 연구는 주관적인 사후 평가와 스스로 평가한 기술 향상에 초점을 맞추고 있습니다(예: 스탠포드 외. 2017). 그러나 자기 평가는 종종 성격(John and Robins 1994) 또는 기술 수준 자체(숙련되지 않은 학생은 자신의 능력을 과대평가함, Kruger와 Dunning 1999 참조)에 의해 왜곡될 수 있습니다. 객관적인 척도를 사용한 대규모 조사는 보다 실질적인 결론을 제공하지만, 지금까지는 STEM 학생을 대상으로만 완료되었습니다(예: Russell, Hancock, McCullough 2007). Linn 등(2015)은 RBL의 효과를 객관적으로 조사할 수 있는 유효한 척도가 부족하다는 것이 근본적인 문제라고 지적합니다. 이 문제를 해결하기 위해 사회과학 분야의 인지적 연구 성향을 객관적으로 측정하는 사회과학 연구 역량 테스트가 Gess와 동료들에 의해 개발되었습니다(Gess, 가이거, 지글러 2018; Gess, 웨셀스, 블뢰메케 2017). 이 도구는 연구 과정의 중요한 단계를 수행하는 데 필요한 다양한 연구 지식 영역의 일관된 모델을 기반으로 합니다(부록 1, 온라인 보충 데이터 참조). 검증 연구에서 이 도구는 사회과학 연구 교육을 평가하는 데 적합한 것으로 나타났으며 RBL의 인지적 이점을 객관적으로 측정할 수 있는 도구로 사용될 수 있습니다. Thus, while RBL in the social sciences seems to be effective at facilitating a range of different cognitive dispositions, these results can only serve as preliminary evidence. A problem concerning the interpretability of these and other studies in the field lies in their methodological designs: Most existing studies focus on subjective ex-post assessments and self-evaluated skill gains (e.g. Stanford et al.2017). However, self-assessments are often distorted by personality (John and Robins1994) or skill levels themselves (unskilled students overestimate their abilities, see Kruger and Dunning1999). Large-scale investigations using objective measures provide more substantial conclusions, but have so far only been completed for STEM students (e.g. Russell, Hancock, and McCullough2007). Linn et al. (2015) note that the underlying problem is a lack of valid measures to objectively investigate the effectiveness of RBL. To address this problem, theSocial-scientific Research Competency Test, an objective measure of cognitive research dispositions in the social sciences, was developed by Gess and colleagues (Gess, Geiger, and Ziegler2018; Gess, Wessels, and Blömeke2017). The instrument is based on a coherent model of different areas of research knowledge necessary to conduct critical steps in the research process (see Appendix 1, online supplemental data). In validation studies, the instrument has been shown to be suitable for evaluating social-scientific research education and could serve as an objective measure of the cognitive benefits of RBL.
정서적 동기 부여 효과 Affective-motivational gains
고등 교육 연구에서 학습에 대한 정서적 동기 부여 측면의 중요성을 점점 더 인정하고 있습니다(예: Postareff와 Lindblom-Ylänne 2011). 이러한 일반적인 추세를 반영하여 RBL에 대한 연구에서도 정서적 동기 부여에 대한 관심이 높아지고 있습니다. Higher education research is increasingly acknowledging the importance of affective-motivational aspectsfor learning (e.g. Postareff and Lindblom-Ylänne2011). Reflecting this general trend, affective-motivational gains have also drawn increased attention in research on RBL.
RBL이 정서적 동기 부여 연구 성향을 변화시킬 수 있다는 증거는 여러 분야의 표본을 대상으로 한 연구에서 종종 발견됩니다. 연구 자기 효능감 향상(Deicke, Gess, Rueß 2014; Whipple, Hughes, Bowden 2015), 지적 호기심 증가(Bauer, Bennett 2003), 연구 과정의 장애물에 대한 높은 내성(Lloyd, Shanks, Lopatto 2019) 등의 이점이 입증되었습니다. 또한 STEM 학생을 대상으로 한 연구에서는 학습에 대한 열망이 더 크고 모호한 문제를 해결하려는 성향이 증가하는 것으로 나타났습니다(Ward, Bennett, Bauer 2003). Evidence on RBL’s potential to alter affective-motivational research dispositions often stems from studies with multidisciplinary samples. Demonstrated benefits include higher research self-efficacy (Deicke, Gess, and Rueß2014; Whipple, Hughes, and Bowden2015), increased intellectual curiosity (Bauer and Bennett2003) and a higher tolerance for obstacles in the research process (Lloyd, Shanks, and Lopatto2019). Furthermore, a study with STEM students demonstrated a greater desire to learn and an increased disposition towards working with ambiguity (Ward, Bennett, and Bauer2003).
기존의 몇몇 연구는 모두 개인의 정서적-동기적 연구 성향을 조사했으며, 주로 탐색적인 방식으로 진행되었습니다. 그러나 연구를 수행하는 것은 학생들이 불확실성과 다양한 좌절을 처리해야 하는 특히 까다로운 작업입니다(John and Creighton 2011). 따라서 연구를 성공적으로 수행하려면 연구 과정의 어려움에 대처할 수 있는 다양한 정서적-동기적 성향이 필요하다고 가정할 수 있습니다. 사회과학 분야의 학생 연구에 필요한 정서적-동기적 연구 성향에 대한 일관되고 경험적으로 근거한 모델이 최근에 개발되었습니다(Wessels 외. 2018). 예를 들어, 연구 과정을 시작하고 유지하는 데 필요한 성향은 연구 흥미가 필요하며, 연구 과정을 지속하려면 불가피한 좌절에 대처할 수 있는 좌절 내성이 필요합니다. RBL이 이러한 연구 성향을 개발하는 데 효과적인지 여부는 불분명합니다. The few existing studies all examine individual affective-motivational research dispositions, often in an exploratory manner. However, conducting research is an especially demanding task that requires students to handle uncertainties and manifold frustrations (John and Creighton2011). Thus, it can be assumed that successfully conducting research requires a range of different affective-motivational dispositions to cope with the challenges of the research process. A coherent, empirically grounded model of the affective-motivational research dispositions necessary for student research in the social sciences has been recently developed (Wessels et al.2018). It encompasses dispositions that are necessary to begin and to sustain the research process: for example, research interest is needed to initiate a research process, while sustaining it requires frustration tolerance to cope with inevitable setbacks. It is unclear whether RBL is effective in developing these research dispositions.
전반적으로 사회과학에서 RBL의 본질과 효과에 대한 연구는 다른 분야의 연구와 달리 일반적으로 부족하고 취약한 방법론적 설계에 기반하는 경우가 많습니다. 그러나 STEM 학생을 대상으로 한 연구에서 얻은 증거가 사회과학에 쉽게 적용된다고 가정할 수는 없습니다.
첫째, 연구는 사회과학보다 자연과학 분야의 대학 프로그램에서 더 중요해 보입니다(Taraban and Logue 2012 참조).
둘째, STEM 분야의 연구 경험은 대부분 교육적 문화가 다를 수 있는 구조화된 실험실 환경에서 이루어집니다(Rand 2016).
셋째, 학문 분야별 결과 변수를 조사하려면 해당 학문 분야에서 연구를 수행해야 합니다.
Overall, studies on the nature and effectiveness of RBL in the social sciences are generally scarce and often based on weak methodological designs – in contrast to studies from other disciplines. However, one cannot assume that the evidence gained in studies with STEM students easily translates to the social sciences.
First, research seems more important to university programmes in the natural sciences than in the social sciences (cf. Taraban and Logue 2012).
Second, most research experiences within STEM disciplines occur in structured lab environments that might have a different pedagogical culture (Rand 2016).
Third, if discipline-specific outcome variables are to be investigated, a study needs to be conducted in that specific discipline.
또 다른 미해결 질문은 사회과학에서 RBL이 다양한 연구 성향의 변화에 영향을 미치는 과정에 관한 것입니다. STEM 학생을 대상으로 한 연구에서 학습 향상에 대한 주요 예측 변수는 연구 경험의 기간과 강도입니다. 연구 경험이 오래 지속되고 강도가 높을수록 기술 수준이 더 크게 향상됩니다(Bauer와 Bennett 2003). 또 다른 연구에 따르면 연구 과정에서 자율성(예: 스스로 방법론을 결정할 수 있는 자율성)이 높은 학생일수록 학습 성과가 더 높은 것으로 나타났습니다(Gilmore 외. 2015). 그러나 사회과학에서 RBL 과정의 어떤 특성이 다양한 연구 성향의 변화에 영향을 미치는지는 아직 연구되지 않았습니다. Another open question pertains to the processes by which RBL in the social sciences affects changes in different research dispositions. In studies with STEM students, the main predictors of learning gains are the duration and intensity of the research experience: longer-lasting and more intense research experiences lead to stronger increases in skill levels (Bauer and Bennett2003). Another study found that students with higher levels of autonomy in the research process, e.g. the autonomy to make their own methodological decisions, showed stronger learning gains (Gilmore et al.2015). However, which characteristics of RBL courses in the social sciences affect changes in different research dispositions has not been studied yet.
연구 질문 및 가설 Research questions and hypotheses
이 백서의 목적은 사회과학에서 RBL 과정의 효과를 분석하는 것입니다.
(1) 연구 기반 학습이 인지적 및 정의적-동기적 연구 성향에 긍정적인 영향을 미치는가?
(2) 다양한 코스 특성이 이러한 연구 성향의 변화와 어떤 관련이 있는가?
The objective of this paper is to analyse the effectiveness of RBL courses in the social sciences. Two main research questions guided our work:
(1) Does research-based learning have a positive effect on cognitive and affective-motivational research dispositions?
(2) How do different course characteristics relate to changes in these research dispositions?
첫 번째 연구 질문과 관련하여 다음과 같은 가설을 테스트했습니다: Pertaining to the first research question, the following hypotheses were tested:
가설 1a: 이전 연구에서 학생의 연구 경험과 자기 평가 지식 습득 간의 연관성이 발견되었으므로(Taraban and Logue 2012), 연구 지식(방법 지식, 방법론 지식, 연구 과정 지식)에 대한 사전 시험 점수보다 사후 시험 점수가 유의미하게 높을 것으로 예측합니다. Hypothesis 1a:As previous studies have found associations between student research experiences and self-evaluated knowledge gains (Taraban and Logue2012), we predict that students will have significantly higher post-test scores than pre-test scores for research knowledge (knowledge of methods, knowledge of methodologies and research process knowledge).
가설 1b: 이전 연구에서 학생의 연구 경험과 연구 과정의 장애물에 대한 높은 내성(Lloyd, Shanks, and Lopatto 2019)과 모호성을 다루는 능력 증가(Ward, Bennett, and Bauer 2003) 사이의 연관성이 발견되었으므로, 우리는 학생들이 정서적 동기 연구 성향에 대해 사전 테스트 점수보다 사후 테스트 점수가 유의하게 높을 것으로 예측합니다. Hypothesis 1b:As previous studies have found associations between student research experiences and a higher tolerance for obstacles in the research process (Lloyd, Shanks, and Lopatto2019) as well as an increased ability to work with ambiguity (Ward, Bennett, and Bauer2003), we predict that students will have significantly higher post-test scores than pre-test scores for affective-motivational research dispositions.
두 번째 연구 질문과 관련하여 다음과 같은 가설을 테스트했습니다: Pertaining to the second research question, the following hypotheses were tested:
가설 2a: STEM 분야의 연구에서 더 길고 강도 높은 연구 경험(Bauer와 Bennett 2003)이 RBL 참여 효과에 긍정적인 영향을 미친다는 사실이 입증되었으므로, 연구 경험의 강도, 즉 수행한 연구 단계의 수가 연구 지식의 변화에 영향을 미칠 것으로 예측합니다. Hypothesis 2a:Since studies in STEM disciplines have demonstrated that longer and more intense research experiences (Bauer and Bennett2003) have a positive influence on the effect of participation in RBL, we predict that the intensity of the research experience, i.e. the number of research steps performed, will influence changes in research knowledge.
가설 2b: 연구 과정에서의 자율성이 높을수록 RBL 참여 효과에 긍정적인 영향을 미친다는 연구 결과(Gilmore 외. 2015)가 있으므로, 학생들의 자율성, 즉 연구 질문과 연구 방법을 자유롭게 선택할 수 있는 능력은 정서적-동기적 연구 성향의 변화에 긍정적인 영향을 미칠 것으로 예측합니다. Hypothesis 2b:Since studies in STEM disciplines have demonstrated that higher levels of autonomy in the research process (Gilmore et al.2015) positively impact the effect of participation in RBL, we predict that students’ autonomy, i.e. ability to freely choose a research question and a research method, will positively affect changes in affective-motivational research dispositions.
가설 2c: 학생들의 자기 효능감, 자신이 '진짜 연구'를 하고 있다는 지각, 학생들의 과제에 대한 교수자의 관심, 향후 진로에 대한 RBL의 유용성 지각 등 다양한 동기 부여 요인이 정의적-동기적 성향의 변화에 긍정적인 영향을 미칠 것이라고 예측합니다. Hypothesis 2c:We predict that different motivating factors, e.g. students’ self-efficacy, the perception that they are doing ‘real research’, perceived instructor interest in the students’ work, and the perceived usefulness of RBL for their later career will positively affect changes in affective-motivational dispositions.
연구 방법 Methods
연구 질문에 답하기 위해 10개 대학에서 다양한 사회과학 분야에서 제공되는 RBL 과정의 시작과 종료 시점에 종이 기반 측정을 실시했습니다. To answer our research questions, paper-based measurements were conducted at the beginning and the end of RBL courses offered in different social scientific disciplines at 10 different universities.
절차 Procedure
사회과학 분야의 비교 가능한 RBL 과정을 연구하는 것이 목적이었기 때문에 경험적 사회과학 연구 방법을 사용하는 학습 프로그램의 커리큘럼만 고려했습니다. 여기에는 사회학, 정치학, 심리학, 교육학이 포함되었습니다(Gess, Wessels, Blömeke 2017 참조). As the objective was to study comparable RBL courses in the social sciences, only the curricula of study programmes employing empirical social science research methods were considered. These included sociology, political science, psychology, and education science (see also Gess, Wessels, and Blömeke2017).
적합한 RBL 코스는 코스 설명을 통해 확인했습니다. RBL의 정의에 따라 학생들이 자율적인 방식으로 전체 연구 주기를 경험할 수 있는 코스만 고려했습니다. 146개 코스의 강사에게 이메일을 통해 연락하여 연구 참여를 요청했으며, 65명이 참여에 동의했고 50명은 주로 강의 시간 제약으로 인해 참여를 원하지 않았으며 나머지 31명의 강사는 응답하지 않았습니다. 사전 테스트는 과정의 첫 2주 동안, 사후 테스트는 과정의 마지막 2주 동안 예정되어 있었습니다. Suitable RBL courses were identified via their course descriptions. Only courses that allowed students to experience a full research cycle in a self-regulated manner were considered, in line with our definition of RBL. The instructors of 146 courses were contacted via email and asked to participate in the study; 65 agreed to participate, 50 did not wish to participate, mostly due to time constraints in the course, and the remaining 31 instructors did not respond. Pre-tests were scheduled for the first two weeks of the course, and post-tests for the last two weeks of the course.
사전 및 사후 측정은 독일 전역의 10개 대학에서 총 70개의 RBL 코스에서 실시되었습니다. 실험에 참여한 모든 대학은 다양한 분야의 학위를 제공하는 10,000~50,000명의 학생을 보유한 국공립 대학이었습니다. Altogether, pre- and post-measurements were conducted inN = 70 RBL courses at 10 universities across Germany. All universities included were state-funded public universities with 10,000-50,000 students offering degrees in a wide range of disciplines.
테스트는 이 기사의 저자 중 한 명이 수업 시간에 진행했으며, 그는 연구의 절차 및 일반적인 목적을 설명했습니다. 설문지는 인쇄된 소책자 형태로 배포되었습니다. 생일 월 등 민감하지 않은 정보를 기반으로 한 개인 6자리 코드를 사용하여 익명성을 보장하면서 사전 및 사후 설문지를 일치시켰습니다. 설문지를 작성하는 데 약 25분 정도 소요되었습니다. 사후 테스트도 동일한 절차를 따랐습니다. 또한 코스 강의의 특성에 대한 간단한 강사 설문조사도 실시했습니다. The testing itself was conducted during class time by one of the authors of this article, who explained the procedure and general purpose of the study. The questionnaires were administered in the form of printed booklets. A personal 6-digit code based on non-sensitive information, e.g. birthday month, was used to match pre- and post-test questionnaires while granting anonymity. Filling in the questionnaire took approximately 25 min. The post-test followed the same procedure. Additionally, a brief instructor survey on characteristics of the course instruction was administered.
샘플 Sample
표본은 총 952명의 학생(여성 74.1%, 남성 23.5%)으로 구성되었으며, 이 중 881명이 1차 측정에, 539명이 2차 측정에 참여했습니다. 첫 번째 측정 시점의 참여율이 더 높았던 이유는 학기 초에 코스 출석률이 높았기 때문입니다. The sample encompassedN = 952 students (74.1% female, 23.5% male), of which 881 participated in the first measurement and 539 participated in the second measurement. Higher participation rates at the first measurement point were due to higher course attendance at the beginning of the semester.
참여 학생의 평균 연령은 M = 24.38세(SD = 4.79)였습니다. 학생의 61.6%는 학사 과정에 재학 중이었고 29.5%는 석사 과정에 재학 중이었습니다. 50명의 학생은 전통적인 독일 대학 졸업장과 같은 다른 학습 프로그램에 등록했으며, 학습 진도에 따라 학사 또는 석사 과정 학생으로 분류되었습니다. 학사 과정 학생들은 평균적으로 2학년이 거의 끝날 무렵이었으며, 이수한 학기 수는 평균 3.33학점(SD = 1.67)이었습니다. 석사 과정 학생들은 평균적으로 석사 2학년 초에 재학 중이었으며, 평균 이수 학기는 M = 2.57 (SD = 1.63) 학기였습니다. The mean age of the participating students wasM = 24.38 years (SD= 4.79). 61.6% of the students were enrolled in a bachelor’s programme, while 29.5% were enrolled in a master’s programme. Fifty students were enrolled in other study programmes, such as the traditional German university diploma, and were treated as either bachelor’s or master’s students depending on their study progress. Bachelor’s students were near the end of their second year of study on average; the mean number of semesters completed wasM = 3.33 (SD= 1.67). Master’s students were at the beginning of their second year of master’s studies on average, withM = 2.57 (SD= 1.63) semesters of the degree completed on average.
학생들은 교육학(31.4%), 심리학(22.4%), 사회학(10.3%), 커뮤니케이션학(8.6%), 정치학(5.5%) 등 다양한 전공 분야에 등록했으며 나머지 학생들은 미디어 연구와 같은 보다 구체적인 사회과학 과목을 공부하고 있었습니다. The students were enrolled in different fields of study, namely educational science (31.4% of the students), psychology (22.4%), sociology (10.3%), communication science (8.6%), and political science (5.5%) The remaining students were studying other, more specific social scientific subjects (i.e. media studies).
학생들은 70개의 RBL 과정 중 하나에 등록했습니다. 참여는 종종 학생들의 학습 프로그램에서 필수적인 부분이었습니다: 41.8%의 학생들은 이 특정 과정에 의무적으로 등록해야 했고, 35.7%는 다른 RBL 과정을 선택할 수 있었으며, 17.6%만이 RBL 교육 형식이 포함되지 않은 과정을 선택할 수 있었습니다. 코스당 평균 참가자 수는 M = 13.54명(SD = 12.62명)이었습니다. 대부분의 학생은 한 학기 코스에 등록했으며(77.7%), 22.3%의 학생은 두 학기 코스에 등록했습니다. 65명의 강사 또는 공동 교수진이 강의를 진행했습니다. 이 중 52명의 강사가 코스 종료 시 강사 설문조사에 참여했습니다. The students were enrolled in one of 70 RBL courses. Participation was often a mandatory part of the students’ study programmes: 41.8% of the students were required to enrol in this specific course; an additional 35.7% could have chosen a different RBL course, while only 17.6% could have chosen a course not involving the instructional format of RBL. The average number of participants per course wasM = 13.54 (SD = 12.62). The majority of students were enrolled in one-semester courses (77.7%); 22.3% of the students were enrolled in two-semester courses. The courses were led by 65 different instructors or co-teaching teams. Fifty two of these instructors participated in the instructors’ survey at the end of the course.
측정 항목 Measures
연구 지식 Research knowledge
사회과학 분야의 연구 지식을 평가하기 위해 Gess, Wessels, Blömeke(2017)의 9개 항목으로 구성된 사회과학 연구 역량 측정의 짧은 버전이 사용되었습니다. 이 테스트는 양적 연구와 질적 연구에 관한 문항으로 연구 방법에 대한 지식, 방법론에 대한 지식, 연구 과정 지식을 평가합니다. 이 시험은 다양한 연구 문제에 대한 객관식 문항과 함께 짧은 비네팅을 사용합니다(부록 1, 온라인 보충 데이터의 샘플 문항 참조). 이 도구는 여러 검증 연구를 거쳤으며 학사 및 석사 학위 프로그램에서 사회과학 연구 과정을 평가하는 데 적합합니다(Gess, Geiger, Ziegler 2018; Gess, Wessels, Blömeke 2017). 27개 문항으로 구성된 전체 측정은 완료하는 데 35분이 걸리고 수업 시간이 부족하기 때문에 변별 변인, 문항 난이도, 신뢰도, 장문 버전과의 상관관계를 바탕으로 내용 영역 측면에서 원래 시험의 전체 범위를 반영하는 9개 문항으로 구성된 짧은 버전이 개발되었습니다. 짧은 버전의 개인별 점수와 긴 버전의 개인별 점수의 상관관계는 r = 0.86으로, 두 버전이 유사한 구성을 측정한다는 것을 나타냅니다. 그러나 짧은 버전의 테스트는 긴 버전과 동일한 검증 절차를 거치지 않았다는 점에 유의해야 합니다. 학생들의 답변은 정답(1) 또는 오답(0)으로 코딩되어 최종 데이터는 9개의 이분법적 항목으로 구성되었습니다. 신뢰도는 가중 오메가 h = 0.69로 수용 가능한 수준이었습니다(표 1 참조).
A 9-item short version of the social-scientific research competence measure by Gess, Wessels, and Blömeke (2017) was used to assess research knowledge in the social sciences. This test assesses knowledge of research methods, knowledge of methodologies and research process knowledge with items referring to both quantitative and qualitative research. The test uses short vignettes coupled with multiple choice questions on different research problems (see sample item in Appendix 1, online supplemental data). The instrument has gone through several validation studies and is suitable for the evaluation of research courses in the social sciences in both bachelor’s and master’s degree programmes (Gess, Geiger, and Ziegler2018; Gess, Wessels, and Blömeke2017). Since the full 27-item measure takes 35 min to complete and in-class time was sparse, a 9-item short version reflecting the full breadth of the original test in terms of content areas was developed based on the discrimination parameters, item difficulty, reliability and correlation with the long version. The correlation of the person scores for the short version and the person scores for the long version isr = 0.86, which indicates that the two versions measure a similar construct. However, it must be noted that the short version of the test has not undergone the same validation procedure as the long version. The students’ answers were coded as either correct (1) or incorrect (0), such that the final data consisted of 9 dichotomous items. The reliability was acceptable, with weighted omegah = 0.69 (seeTable 1).
정서적-동기적 연구 성향 모델(Wessels 등, 2018)은 사회과학 연구를 수행하는 데 필요한 9가지 성향을 포괄하며, 이 중 4가지 성향을 본 연구에서 조사 대상으로 선정했습니다.
(1) 연구에 대한 가치 관련 관심은 연구의 유용성에 대한 신념을 포함합니다.
(2) 연구 수행의 즐거움은 다양한 연구 활동과 관련하여 경험하는 즐거움을 의미합니다.
(3) 연구 관련 불확실성 내성은 연구 과정의 불확실성에 대처하는 성향을 의미합니다.
(4) 연구 관련 좌절 내성은 연구 과정에서 좌절을 견딜 수 있는 성향을 의미합니다.
The model of affective-motivational research dispositions (Wessels et al.2018) encompasses nine necessary dispositions for pursuing research in the social sciences, of which four were selected to be investigated in the present study.
(1)Value-related interest in researchsubsumes beliefs about the usefulness of research.
(2)Finding joy in conducting researchdenotes the joy experienced with respect to different research activities.
(3) Research-relateduncertainty toleranceis the disposition to handle uncertainties in the research process.
(4) Research-relatedfrustration toleranceis the disposition to endure setbacks in the research process.
자기 평가 척도(샘플 항목과 기본 설명 데이터는 표 1에서 확인할 수 있음)는 연역적 및 귀납적 검사 구성 절차에 따라 다단계 프로세스로 개발되었습니다(Burisch 1984). 먼저, 고정된 이론 중심의 구성 원칙에 따라 각 성향별로 최소 20개의 문항을 구성했습니다(Wilson 2005). 문항은 사회과학과 학생 250명을 대상으로 한 파일럿 연구를 바탕으로 선정 및 개선되었습니다. 최종 도구는 각 성향당 4~5개 문항으로 구성되었으며, 보통 또는 양호한 신뢰도를 보였습니다(가중 오메가 h = 0.68-0.82). 모든 정서적 동기 부여 측정의 응답 형식은 1점(전혀 동의하지 않음)에서 5점(전혀 동의함)까지의 5점 리커트 척도입니다. Self-assessment scales (sample items and basic descriptive data can be found inTable 1) were developed in a multistep process following deductive and inductive test construction procedures (Burisch1984). First, at least 20 items per disposition were constructed according to fixed theory-driven construction principles(Wilson2005). The items were selected and refined based on a pilot study withN = 250 students from the social sciences. The final instruments encompass 4 or 5 items per disposition and exhibit acceptable or good reliabilities (weighted omegah = 0.68–0.82). The response format for all affective-motivational measures was a five-point Likert scale ranging from 1 (completely disagree) to 5 (completely agree).
교수자 및 코스 특성 Instructor and course characteristics
학생 설문 조사 Student survey
사전 및 사후 테스트 중에 학생에게 추가 정보를 요청했습니다. 사전 테스트에서는 학생들이 스스로 평가한 연구 자기 효능감(5점 척도 6개 항목, 예: '주요 변수를 조작하기 어렵더라도 정량적 연구에 적합한 평가 도구를 찾을 수 있다고 확신한다')이 포함되었습니다. 사후 테스트에서 학생들은 지금까지 수행한 연구 단계(예: 관련 문헌 검색), 연구 프로젝트에 대한 강사의 관심도, '실제' 연구를 하고 있는지에 대한 인식, 향후 커리어에 대한 이 과정의 유용성에 대해 질문했습니다(모두 5점 척도로 각 항목 1개씩 측정). During the pre- and post-test, students were asked for additional information. At pre-test, this included their self-assessed research self-efficacy (6 items on a 5-point scale, e.g. ‘I am sure I can find suitable assessment tools for a quantitative study, even if the main variable is difficult to operationalize’). At post-test, students were asked about the research steps (e.g. searching for relevant literature) they had completed so far, their perception of the instructor’s interest in their research project, their perception of whether they were doing ‘real’ research, and the perceived usefulness of the course for their later career (all measured with one item each on a 5-point scale).
강사 설문조사 Instructor survey
사후 테스트는 강사의 관점에서 강좌의 교육 개념에 대한 정보를 수집하는 데에도 사용되었습니다. 강사에게 배포된 5분 분량의 설문지를 통해 학생들이 연구 질문과 방법을 자율적으로 선택할 수 있는지에 대해 질문했습니다(5점 척도 2개 항목). The post-test was also used to gather information about the course’s instructional concept from the instructor’s perspective. A 5-minute questionnaire distributed to the instructors asked about students’ autonomy in choosing their own research question and method (two items on a five-point scale).
통계 분석 Statistical analysis
첫 번째 단계로, 학생들의 사전 및 사후 테스트 데이터는 개인 6자리 코드를 통해 매칭되었습니다. SPSS 23을 사용하여 데이터 확인 및 매니페스트 변수에 대한 설명적 분석을 수행했습니다. 시간 경과에 따른 다양한 변수의 변화를 조사하기 위해 잠재 변화 점수 모델링(McArdle 2009, LCM)과 다중 회귀 분석을 사용했습니다. LCM과 필요한 모든 선행 분석은 Mplus 버전 8(Muthén and Muthén 2017)을 사용하여 수행했습니다. 다음 세 단계가 수행되었습니다: In a first step, students’ pre- and post-test data were matched via their personal six-digit code. We used SPSS 23 to conduct data checks and descriptive analyses of the manifest variables. To investigate changes in the different variables over time, we employed latent change score modelling (McArdle2009; LCM) and multiple regressions. LCM and all necessary preceding analyses were performed with Mplus version 8 (Muthén and Muthén2017). The following three steps were performed:
차원성 테스트 Dimensionality tests
가정된 요인 구조를 확인하고 데이터의 의미 있는 해석을 위해 모든 변수에 대해 확인적 요인 분석을 실시했습니다(부록 2, 온라인 보충 데이터 참조). 거의 모든 변수에 대해 단차원 모형이 더 나은 모델 적합도를 보였습니다. 유일한 예외는 '연구 수행의 즐거움 찾기' 변수였는데, 이 변수는 1차원 모형과 3차원 모형 모두에서 부적합한 모델 적합도를 나타냈습니다. 따라서 데이터의 의미 있는 해석을 위해 이 구성요소를 두 가지 요인으로 분리하여 후속 분석을 실시했습니다.
첫 번째 요인은 '과학 문헌 작업의 즐거움'을,
두 번째 요인은 '경험적 데이터 작업의 즐거움'을 설명합니다.
To confirm the assumed factor structures and allow for a meaningful interpretation of the data, we conducted confirmatory factor analyses on all variables (see Appendix 2, online supplemental data). For almost all variables, the unidimensional model exhibited better model fit. The only exception was the variable ‘Finding joy in conducting research’, which exhibited inadequate model fits in both the unidimensional and the three-dimensional solution. Hence, subsequent analyses were conducted with two separate factors for this construct to ensure a meaningful interpretation of the data. The first factor describes ‘joy in working with scientific literature’, while the second describes ‘joy in working with empirical data’.
측정값 불변성 테스트 Measurement invariance tests
잠재 변화 점수 모델링의 전제 조건은 강력한 요인 불변성입니다(McArdle 2009). 강력한 요인 불변성이 주어져야만 모든 요인 적재량과 절편이 모든 측정 지점에 대해 동일한 값으로 고정될 수 있습니다. Meredith와 Horn(2001)에 따라 점점 더 제약이 많은 모델의 CFI 값을 비교했습니다(부록 3, 온라인 보충 데이터 참조). 모든 변수에 대해 강력한 요인 불변성 또는 부분 측정 불변성이 확립되었으며, 이는 후속 분석이 의미 있게 해석될 수 있음을 의미합니다. A prerequisite for latent change score modelling is strong factorial invariance (McArdle2009). Only if strong factorial invariance is given can all factor loadings and intercepts be fixed to the same values for all measurement points. Following Meredith and Horn (2001), the CFI values of increasingly constrained models were compared (see Appendix 3, online supplemental data). For all variables, either strong factorial invariance or partial measurement invariance was established, meaning that the subsequent analyses can be meaningfully interpreted.
잠재 변화 점수 모델링 Latent change score modelling
그런 다음 시간에 따른 변수의 변화를 조사하기 위해 잠재 변화 점수 모델링(LCM)을 사용했습니다. LCM에서 변화는 두 개 이상의 측정 지점에서의 변화를 표현하는 잠재 차이 변수로 모델링됩니다(그림 1 참조). 이 접근 방식을 통해 측정 오류 없이 개인 내 변화의 개인 간 차이를 관찰할 수 있습니다(McArdle 2009). We then employed LCMs to examine changes in our variables over time. In LCM, change is modelled with latent difference variables that express the change across two or more measurement points (seeFigure 1). This approach enables us to observe interindividual differences in intraindividual change free from measurement error (McArdle2009).
LCM 분석은 두 단계로 수행되었습니다:
첫 번째 단계에서는 각 변수에 대해 단변량 LCM(두 개의 측정 지점, T1 및 T2 포함)을 지정했습니다. 잠재 변화 변수는 T1에서 T2까지의 개인 내 변화를 나타냅니다. 따라서 이 변수는 가설 H1a 및 H1b(효과)를 테스트하기 위해 해석되었습니다. 잠재 변화 변수의 분산은 개인 간 차이, 즉 학생의 연구 성향이 다른 방식으로 발전하는지 여부를 나타냅니다.
유의미한 개인 간 차이가 발견되면 두 번째 단계로 잠재 변화 변수를 6가지 코스 특성에 따라 회귀 분석했습니다. 그런 다음 회귀 계수를 해석하여 가설 H2a, H2b 및 H2c(코스 특성의 영향)를 테스트했습니다.
LCM analyses were performed in two steps:
In the first step, we specified univariate LCMs (with two measurement points, T1 and T2) for each variable. The latent change variable indicates intraindividual changes from T1 to T2. Therefore, this variable was interpreted to test hypotheses H1a and H1b (effectiveness). The variance of the latent change variable indicates interindividual differences, i.e. whether students’ research dispositions develop in different ways.
When significant interindividual differences were found, in a second step, the latent change variable was regressed on six different course characteristics. The regression coefficients were then interpreted to test hypotheses H2a, H2b and H2c (impact of course characteristics).
데이터의 중첩된 구조(70개 코스에 중첩된 952명의 학생)를 설명하기 위해 Mplus 명령 TYPE = COMPLEX를 사용하여 코스를 클러스터 변수로 사용했습니다. 또한 두 측정 지점에서 동일한 항목을 사용하여 발생하는 방법 분산을 설명하기 위해 자동 상관 오류를 포함했습니다. 누락된 데이터는 전체 정보 최대 가능성 추정(FIML)을 사용하여 처리했습니다. 양호한 모델 적합도를 결정하기 위한 기준으로는 Hu와 Bentler(1999)가 제시한 기준을 사용했으며, CFI가 0.95 이상이고 RMSEA가 0.06 미만인 모델을 적절한 적합도를 가진 것으로 간주했습니다. To account for the nested structure of the data (N = 952 students nested in 70 courses), we used the course as a cluster variable with the Mplus command TYPE = COMPLEX. Additionally, auto-correlated errors were included to account for method variance resulting from the use of the same items over the two measurement points. Missing data were handled using full-information maximum likelihood estimation (FIML). The criteria suggested by Hu and Bentler (1999) were used as a reference point for determining good model fit: models with a CFI > 0.95 and a RMSEA < 0.06 were considered to have adequate fit.
결과 Results
단변량 잠재 변화 점수 모델: 시간에 따른 개인의 인지 및 정서적-동기적 연구 성향의 변화(가설 H1a 및 H1b) Univariate latent change score models: changes in individual cognitive and affective-motivational research dispositions over time (hypotheses H1a and H1b)
연구 지식 Research knowledge
연구 지식에 대한 LCM은 양호한 모델 적합도를 보였습니다(표 2 참조). 변화 변수의 평균은 작지만 유의미했으며(ΔM = 0.04, p < .01), 이는 T1에서 T2로 유의미한 변화가 있었음을 나타냅니다. 즉, RBL 과정을 수강한 후 학생들은 T1보다 평균 0.45개 문항(9개 문항 중)을 더 많이 정답으로 맞힐 수 있었습니다. 따라서 데이터는 가설 H1a를 지지했습니다. 변화 변수의 분산은 매우 작고 유의하지 않았으며(σ2 = 0.001, p = .8), 이는 개인 간 차이가 없음을 나타냅니다. The LCM for research knowledge exhibited good model fit (seeTable 2). The mean of the change variable was small but significant (ΔM = 0.04,p < .01), indicating a significant change from T1 to T2. This means that after taking the RBL course, students were able to correctly answer 0.45 questions more on average (out of nine questions) than at T1. Thus, the data supported hypothesis H1a. The variance of the change variable was very small and not significant (σ2 = 0.001,p = .8), indicating that there were no interindividual differences.
모든 정서적 동기 부여 성향에 대한 단변량 LCM은 매우 우수한 모델 적합도를 보였습니다(표 2 참조). 이러한 성향은 T1에서 T2로 발전하는 과정에서 차이가 있었습니다: The univariate LCMs for all affective-motivational dispositions had very good model fits (seeTable 2). The dispositions differed in their development from T1 to T2:
연구에 대한 가치 관련 관심 Value-related interest in research
그 결과 T1에서 T2로 넘어갈수록 유의미한 감소가 나타났습니다(ΔM = -0.14, p < .01). 변화 변수의 유의미한 분산(σ2 = 0.33, p < .01)은 관심도 변화에 개인 간 차이가 있음을 나타냅니다. The results revealed a significant decrease from T1 to T2 (ΔM = −0.14,p < .01). The significant variance of the change variable (σ2 = 0.33,p < .01) indicates the presence of interindividual differences in changes in interest.
연구 활동과 관련된 기쁨 Joy with respect to research activities
위에서 설명한 바와 같이 이 변수는 두 가지 요인으로 구성되어 있으며, 각 요인의 발달을 개별적으로 조사했습니다.
그 결과, '과학 문헌 작업의 즐거움'이 T1에서 T2로 넘어가면서 유의미하게 감소한 것으로 나타났습니다(ΔM = -0.17, p < .01). 변화 변수의 유의미한 분산(σ2 = 0.36, p < .01)은 학생들의 궤적에 차이가 있었음을 나타냅니다.
두 번째 요인인 '경험적 데이터 작업의 즐거움'에서는 유의미한 변화가 관찰되지 않았습니다(ΔM = -0.05, p = .25). 유의미한 분산은 학생의 궤적에 개인 간 차이가 있음을 나타냅니다(σ2 = 0.15, p < .01).
As described above, this variable consisted of two distinct factors whose development was examined individually. The results suggest a significant decrease in ‘joy in working with scientific literature’ from T1 to T2 (ΔM = −0.17,p < .01). The significant variance of the change variable (σ2 = 0.36,p < .01) indicates that there were differences in students’ trajectories. No significant change was observed for the second factor, ‘joy in working with empirical data’ (ΔM = −0.05,p = .25). The significant variance indicates the presence of interindividual differences in students’ trajectories (σ2 = 0.15,p < .01).
불확실성 내성 Uncertainty tolerance
결과는 T1에서 T2로 유의미한 증가를 시사합니다(ΔM = 0.12, p < .01). 유의미한 분산(σ2 = 0.38, p < .01)은 학생의 궤적에 상당한 개인 간 차이가 있음을 나타냅니다. The results suggest a significant increase from T1 to T2 (ΔM = 0.12,p < .01). The significant variance (σ2 = 0.38,p < .01) indicates that there were substantial interindividual differences in students’ trajectories.
좌절감 내성 Frustration tolerance
결과에 따르면 좌절감 내성은 T1에서 T2로 크게 변하지 않았습니다(ΔM = 0.03, p = .24). 유의미한 차이는 개인 간 차이를 나타냅니다(σ2 = 0.12, p < .01). The results show that frustration tolerance did not change significantly from T1 to T2 (ΔM = 0.03,p = .24). The significant variance was indicative of interindividual differences (σ2 = 0.12,p < .01).
따라서 이 데이터는 불확실성 내성에 대해서만 가설 H1b를 지지합니다. 연구에 대한 가치 관련 흥미와 과학 문헌 작업에 대한 즐거움의 경우 유의미한 감소가 발견되었습니다. Therefore, the data supports hypothesis H1b only with respect to uncertainty tolerance. For value-related interest in research and joy in working with scientific literature, significant decreases were found.
시간 경과에 따른 다양한 연구 성향의 변화에 대한 다른 변수의 영향(가설 H2a, H2b 및 H2c) Influence of other variables on changes in different research dispositions over time (hypotheses H2a, H2b and H2c)
다음으로, 단변량 LCM에서 개인 간 차이의 증거가 있는 연구 성향에 대해 변화 변수의 예측 변수를 분석했습니다. 연구에 대한 가치 관련 관심, 과학 문헌 작업에 대한 즐거움, 불확실성에 대한 내성이 그 예입니다. Next, predictors of the change variable were analysed for the research dispositions for which the univariate LCMs showed evidence of interindividual differences. This was the case for value-related interest for research, joy in working with scientific literature and uncertainty tolerance.
연구에 대한 가치 관련 관심 Value-related interest for research
다중 회귀 분석 결과 연구에 대한 가치 관련 관심의 잠재적 변화에 대한 두 가지 유의미하고 긍정적인 예측 변수가 밝혀졌는데, 바로 나중에 커리어에 대한 강의의 유용성과 학생의 작업에 대한 교수자의 관심도였습니다. 이 회귀 모델로 설명된 전체 분산은 10%였습니다(표 3 참조). The multiple regression revealed two significant and positive predictors of the latent change in value-related interest in research: the perceived usefulness of the course for one’s later career and the instructor’s perceived interest in the students’ work. The overall variance explained by this regression model was 10% (seeTable 3).
과학 문헌 작업의 즐거움 Joy in working with scientific literature
이 과정의 유용성은 T1에서 T2로의 기쁨의 잠재적 변화에 대한 중요한 예측 변수로 작용했습니다. 이 과정이 나중에 커리어에 유용하다고 인식한 학생은 과학 문헌을 다루는 기쁨이 더 크게 증가했습니다. 전체 회귀 모델은 기쁨 변화의 분산 중 5%를 설명했습니다(표 3 참조). The perceived usefulness of the course served as a significant predictor of the latent change in joy from T1 to T2. Students who perceived the course as useful for their later career experienced greater increases in joy in working with scientific literature. The full regression model explained 5% of the variance in the change in joy (seeTable 3).
불확실성 내성 Uncertainty tolerance
불확실성 내성은 T1에서 연구 자기효능감에 의해 유의미하게 예측되었습니다. 자기효능감은 음의 예측 변수로 작용했는데, 학생의 자기효능감이 높을수록 불확실성 내성이 더 많이 감소하거나 덜 증가했습니다. 이 회귀 모델로 설명된 전체 분산은 6%였습니다(표 3 참조). Uncertainty tolerance was significantly predicted by research self-efficacy at T1. Self-efficacy served as a negative predictor: the higher a student’s self-efficacy, the more uncertainty tolerance decreased or the less it increased. The overall variance explained by this regression model was 6% (seeTable 3).
이러한 결과는 추가적인 동기 부여 요인의 영향을 조사한 가설 H2c와 일치합니다. 가설 H2a와 H2b는 지지되지 않았습니다. These findings are in line with hypothesis H2c, which examined the influence of additional motivating factors. Hypotheses H2a and H2b were not supported.
토론 및 시사점 Discussion and implications
본 연구에서는 사회과학 분야에서 RBL의 효과를 조사했습니다. 70개 코스에서 사전-사후 측정을 적용하여 RBL 참여를 통한 다양한 인지적 및 정의적-동기적 연구 성향의 변화를 조사했습니다. 연구 지식은 유의미하게 증가했지만, 추가 조사가 필요한 개인 간 차이는 관찰되지 않았습니다. 연구 관련 불확실성 내성은 증가한 반면, 연구 흥미와 과학 문헌 작업에 대한 즐거움은 RBL 참여 기간 동안 감소했습니다. 후속 회귀 분석 결과, 불확실성 내성의 변화는 연구 자기 효능감에 의해 유의미하게 예측되는 것으로 나타났습니다. 흥미와 즐거움의 변화는 향후 커리어에 대한 강좌의 유용성 지각에 의해 예측되었으며, 흥미의 변화는 강사가 학생의 과제에 대해 지각한 관심도에 의해 예측되기도 했습니다. Our study examined the effectiveness of RBL in the social sciences. By applying pre–post measurements in 70 courses, we examined changes in different cognitive and affective-motivational research dispositions through participation in RBL. Research knowledge increased significantly, but no interindividual differences were observed that could be further investigated. Research-related uncertainty tolerance increased, whereas research interest and joy in working with scientific literature decreased over the course of RBL participation. Subsequent regression analyses showed that the change in uncertainty tolerance was significantly predicted by research self-efficacy. The changes in interest and joy were predicted by the perceived usefulness of the course for one’s later career, while the change in interest was also predicted by the instructor’s perceived interest in the students’ work.
예상과는 달리, RBL을 경험하는 동안 수행한 연구 단계의 수와 학생들에게 주어진 자율성은 정서적-동기적 연구 성향의 변화에 영향을 미치지 않았습니다. Contrary to our expectations, the number of research steps performed and the autonomy students were given during the RBL experience did not have an effect on changes to any of the affective-motivational research dispositions.
연구 지식 Research knowledge
전반적으로 RBL에 참여하는 동안 연구 지식이 크게 증가했습니다(가설 1a 참조). 개별 사회과학 분야의 학생을 대상으로 한 이전 연구에서도 비슷한 결과가 보고된 바 있습니다(예: 타라반과 로그 2012). 우리는 연구 지식의 세 가지 하위 영역인 방법 지식, 방법론 지식, 사회과학 연구 과정 지식을 평가하는 객관적인 테스트 도구를 사용하여 이러한 결과를 확인할 수 있었습니다. Overall, research knowledge increased significantly over the course of RBL participation (see hypothesis 1a). Previous studies with students from individual social scientific disciplines have reported comparable results (e.g. Taraban and Logue2012). We were able to confirm these findings using an objective test instrument assessing three sub-areas of research knowledge: knowledge of methods, knowledge of methodologies and research process knowledge in the social sciences.
그러나 표본에 포함된 학생들은 향상도에서 상당한 개인 간 차이를 보이지 않았으며, 다른 변수와 관련하여 관찰된 변화의 차이를 설명하기 위한 추가 분석을 수행할 수 없었습니다. 이러한 개인 간 차이가 나타나지 않은 것은 지식 항목의 답안 패턴이 비슷했기 때문일 수 있습니다. 저희는 9개 항목으로 구성된 짧은 버전의 긴 테스트를 사용했기 때문에 학생들 간의 실질적인 차이를 파악하기에 충분하지 않았을 수 있습니다. 향후 프로젝트에서는 27개 문항으로 구성된 테스트 양식이나 학생들의 답변에 더 많은 변수가 있는 다른 객관적인 측정을 사용할 것을 권장합니다. However, the students in our sample did not exhibit substantial interindividual differences in their improvement and no further analyses could be conducted to explain differences in the observed change with reference to other variables. This lack of interindividual differences might have been due to similar answering patterns on the knowledge items. We used a 9-item short version of a longer test, which might not have been sufficient to identify substantial differences between students. In future projects, we would recommend using the 27-item test form or another objective measurement that yields more variance in students’ answers.
정서적 동기 부여 연구 성향 Affective-motivational research dispositions
조사된 네 가지 정서적-동기적 연구 성향 중 세 가지에서 첫 번째 측정 시점과 두 번째 측정 시점 사이에 유의미한 변화가 발견되었습니다. A significant change from the first to the second measurement point was found for three out of the four affective-motivational research dispositions examined.
우리의 예상(가설 1b 참조)에 따라 RBL에 참여하는 동안 불확실성 내성이 증가했습니다. 이러한 불확실성 내성의 변화는 연구 자기 효능감에 의해 유의미하게 예측되었습니다(가설 2c 참조). 그러나 자기효능감은 음의 예측 변수로 작용하여 학생의 자기효능감이 높을수록 불확실성 내성의 긍정적인 변화는 더 작았습니다. 연구 자기효능감이 낮은 학생은 연구 경험이 적기 때문에 불확실성 내성이 더 크게 증가할 수 있으며, 따라서 RBL에 참여함으로써 더 큰 혜택을 받을 수 있습니다. 높은 수준의 불확실성 내성은 연구 과정의 예측할 수 없는 특성에 대처하는 데 중요합니다. 불확실성 내성은 연구 수행뿐만 아니라 점점 더 복잡해지는 세상과 마주하는 데에도 필수적이라는 주장도 있습니다(Brew 2010). 이러한 의미에서 불확실성 내성은 학생들이 과학 경력을 쌓는 데 도움이 될 뿐만 아니라 다른 직업을 준비하는 데도 도움이 됩니다. 학생들의 불확실성 내성을 어떻게 변화시킬 수 있는지는 현재 여러 분야에서 논쟁의 대상이 되고 있습니다. 보건 과학 분야에서는 불확실성과 관련된 감정 과정을 모니터링하고 통제함으로써 의대생의 불확실성 내성을 향상시킬 수 있다는 제안이 있었습니다(Iannello 외. 2017). 이 권고를 사회과학 연구에 적용하면, 연구 과정에서 불확실성과 관련된 경험적 감정에 대한 안내를 통합하는 것이 좋습니다. 이를 위한 한 가지 방법은 반성적 학습 일기를 사용하는 것입니다(Nevalainen, Mantyranta, Pitkala 2010). 하지만 저희는 표본에서 불확실성과 관련된 반성적 과정을 테스트하지 않았습니다. 일부 강사가 연구와 관련된 불확실성에 대해 반성하고 논의했다고만 추정할 수 있습니다. 보다 포괄적인 결론을 도출하기 위해서는 RBL 과정에서의 불확실성 내성 발달에 대한 안내된 성찰 과정의 영향을 조사하는 추가 연구가 필요합니다. In line with our expectations (see hypothesis 1b), uncertainty tolerance increased over the course of RBL participation. This change in uncertainty tolerance was significantly predicted by research self-efficacy (see hypothesis 2c). However, self-efficacy served as a negative predictor: the higher a student’s self-efficacy, the smaller the positive change in uncertainty tolerance. Students with low levels of research self-efficacy might exhibit stronger increases in uncertainty tolerance because these students have less research experience and thus benefit more strongly from participation in RBL. A high level of uncertainty tolerance is important for coping with the unpredictable nature of the research process. Some claim that uncertainty tolerance is vital not only for conducting research but also for facing an increasingly complex world in general (Brew2010). In this sense, uncertainty tolerance not only assists students in pursuing scientific careers but also prepares students for other professions. How students’ uncertainty tolerance can be changed is currently a subject of debate in several fields. In the health sciences, it has been suggested that medical students’ uncertainty tolerance can be enhanced by monitoring and controlling emotional processes related to uncertainty (Iannello et al.2017). Translating this recommendation to research in the social sciences, we suggest integrating guided reflections on experienced emotions related to uncertainty in the research process. One way of doing so would be to use reflective learning diaries (Nevalainen, Mantyranta, and Pitkala2010). However, we did not test for reflective processes related to uncertainty in our sample. We can only assume that some instructors reflected on and discussed research-related uncertainties. Further research investigating the influence of guided reflection processes on the development of uncertainty tolerance in RBL courses would be necessary to come to a more comprehensive conclusion.
연구에 대한 흥미와 즐거움은 사전 및 사후 테스트 모두에서 높은 평균값을 보였으며, 이는 참여 학생들이 일반적으로 연구 및 관련 활동을 매우 좋아한다는 것을 나타냅니다. 그러나 불확실성 내성과는 달리 흥미와 즐거움은 RBL에 참여하는 동안 감소했습니다(가설 1b 참조). 이에 대한 몇 가지 가능한 설명이 있습니다. 아마도 학생들은 과정을 진행하는 동안 연구가 무엇인지에 대해 보다 현실적인 아이디어를 얻었을 것입니다. 연구를 시작할 때 학생들의 연구 개념은 해당 사회의 지배적인 연구 관점의 영향을 받을 수 있습니다. 독일에서는 대중이 연구를 흥미롭고 신뢰할 수 있는 것으로 인식하고 있습니다(Wissenschaft im Dialog 2018). 따라서 단일 연구 프로젝트의 설명력이 얼마나 작은지 깨닫는 것은 좌절감이나 환멸을 줄 수 있습니다. 연구의 본질과 실제에 대한 보다 현실적인 이해는 연구에 대한 관심이나 기쁨을 감소시키는 동시에 다른 사람들이 '과학자가 되는 것'이라고 부르는 것의 지표가 될 수 있습니다(Hunter, Laursen, Seymour 2007). Interest and joy in research exhibited high mean values during both the pre- and post-test, indicating that the participating students are generally very fond of research and related activities. However, unlike uncertainty tolerance, interest and joy decreased over the course of RBL participation (see hypothesis 1b). There are several possible explanations for this. Perhaps students gain a more realistic idea of what research is during the course. At the beginning of their studies, students’ conceptions of research might be influenced by the predominant view of research in their society: in Germany, the public perceives research as interesting and trustworthy (Wissenschaft im Dialog2018). Thus, realising how small the explanatory power of a single research project is might be frustrating or disillusioning. Gaining a more realistic understanding of the nature and practice of research might lead to decreased interest or joy in research, while simultaneously serves as an indication of what others have termed ‘becoming a scientist’ (Hunter, Laursen, and Seymour2007).
회귀 분석 결과 특정 코스 변수가 유의미한 예측 변수로 작용하는 것으로 나타났습니다(가설 2c 참조). 즉, 학생의 연구에 대한 관심의 변화는 교수자가 학생의 연구에 대해 가지는 관심도와 학생이 평가한 해당 코스의 향후 경력에 대한 유용성에 의해 유의미하게 예측되었습니다. 강사가 자신의 연구에 관심이 있다고 지각하는 것은 학생에게 동기를 부여하고 연구에 대한 관심을 높일 수 있습니다. 실용적인 의미로, 교수자가 학생의 작업에 관심이 있는 척해야 한다는 의미는 아닙니다. 교수자가 진정으로 관심 있는 주제(예: 자신의 연구 주제)를 RBL 코스의 주제로 선택하는 것만으로도 충분할 수 있습니다. 자신의 연구 주제를 강의실에 가져와서 교육과 연구를 결합하는 것은 종종 교수자에게 유용한 관행으로 권장되어 왔습니다(Vicens and Bourne 2009). 이에 대한 주요 주장 중 하나는 교육과 연구 모두에 관여하는 강사의 귀중한 시간을 절약할 수 있다는 것입니다. 또한 연구 결과에 따르면 교육과 연구를 병행하면 교수자의 주제에 대한 관심에 더 많은 동기를 부여받는 학생에게도 이점이 있는 것으로 나타났습니다. The regression analyses showed that certain course variables served as significant predictors (see hypothesis 2c): changes in students’ interest in research were significantly predicted by the instructor’s perceived interest in the students’ research and the perceived usefulness of the course for their later career (both rated by the students). Perceiving that the instructor is interested in their work might be motivating for students and increase their own interest in research. As a practical implication, this does not mean that instructors shouldpretendto be interested in students’ work. It could suffice for instructors to choose topics for RBL courses that are of genuine interest to them – for example, their own research topics. Bringing one’s own research topics into the classroom, thereby combining one’s teaching and research, has often been recommended as a useful practice for instructors (Vicens and Bourne2009). One of the main arguments for this is that it saves valuable time for instructors involved in both teaching and research. Our results additionally suggest that combining teaching and research comes with benefits for students, who feel more motivated by their instructors’ interest in the topic.
즐거움의 변화는 학생들의 향후 커리어에 대한 강좌의 유용성에 따라 유의미하게 예측되었습니다. 강좌가 향후 커리어에 유용하다고 인식한 학생들은 연구에 더 많은 즐거움을 얻었습니다. 학문적 커리어를 목표로 하지 않는 학생의 경우, 비학문적 커리어에 관심이 있는 연구 주제를 선택하거나 서비스 학습을 적용하는 등 학계 밖에서의 유용성을 강조하거나 강화하는 것이 도움이 될 수 있습니다(Potter, Caffrey, Plante 2003). 이러한 방식으로 더 많은 학생들이 자신의 연구 프로젝트를 수행하는 것이 학계 밖의 경력에 유용하다고 인식하여 연구하는 데 더 큰 즐거움을 찾을 수 있습니다. Changes in joy were significantly predicted by the perceived usefulness of the course for students’ later careers: those students who perceived the course as useful for their future career gained more joy in research. For students who do not aspire to academic careers, it might be beneficial to emphasise or enhance the course’s usefulness for outside academia, e.g. by choosing research topics that are of interest in non-academic careers or applying service learning (Potter, Caffrey, and Plante2003). In this way, more students might perceive conducting their own research projects as useful for careers outside academia and therefore find greater joy in doing research.
예상과는 달리, RBL을 경험하는 동안 수행한 연구 단계의 수와 학생들에게 주어진 자율성은 정서적-동기적 연구 성향의 변화에 영향을 미치지 않았습니다(가설 2a 및 2b 참조). 이는 미리 정의된 연구 문제를 해결하거나 제한된 양의 연구 단계만 완료해도 학생들에게 긍정적인 영향을 미친다는 것을 나타냅니다. Contrary to our expectations, the number of research steps performed and the autonomy students were given during the RBL experience did not have an effect on changes to any of the affective-motivational research dispositions (see hypothesis 2a and 2b). This indicates that even working on pre-defined research problems or completing only a limited amount of research steps has a positive effect on students.
전반적으로 다양한 정서적 동기 변수의 변화를 예측하는 데 사용된 회귀 모델은 잠재적 변화 변수의 분산 중 5%(과학 문헌 작업의 즐거움), 6%(불확실성 허용), 10%(연구 흥미)를 차지했습니다. 이러한 효과 크기는 작은 것으로 분류될 수 있지만(Cohen 1988), 학생들이 예측 변수에 대한 설문지에 응답하는 데 1~2분밖에 걸리지 않았다는 점을 고려할 때 이러한 회귀 분석의 비용 대비 가치 비율은 매우 긍정적인 것으로 간주할 수 있습니다. 보다 근본적인 관점에서 볼 때, 정서적 동기 부여 성향은 현재의 기분이나 개인적인 삶의 사건과 같은 다양한 외부 변수의 영향을 받는 복잡하고 다차원적인 현상이라는 점에 유의해야 합니다. 이 연구에서 조사한 변수(예: 학생의 자율성, 교수자의 관심도)는 전체 코스에 걸쳐 다양한 정서적 동기 부여 연구 성향의 변화를 정확하게 예측하기에 충분하지 않습니다. 그러나 부분적으로 중요한 예측 변수로 작용하여 RBL 코스 설계에 실용적인 새로운 아이디어를 제공했습니다. Overall, the regression models used to predict changes in different affective-motivational variables accounted for 5% (joy in working with scientific literature), 6% (uncertainty tolerance) and 10% (research interest) of the latent change variable’s variance. While these effect sizes can be classified as small (Cohen1988), it is important to put these values into perspective: given that answering the questionnaires on the predictor variables took students only 1–2 min, the cost-value ratio of these regression analyses can be considered very positive. From a more fundamental perspective, it must be noted that affective-motivational dispositions are complex, multidimensional phenomena that are influenced by a range of external variables, such as current mood or personal life events. The variables examined in this study (e.g. student autonomy, instructors’ interest) are not sufficient to accurately predict changes in different affective-motivational research dispositions over an entire course. However, they did partially serve as significant predictors and thus provide practical new ideas for designing RBL courses.
향후 연구를 위한 한계와 시사점 Limitations and implications for future research
본 연구와 이 분야의 다른 연구의 문제점은 대조군이 없다는 점입니다(Lopatto 2004 참조). 적절한 비교 그룹이 없으면 연구 경험 자체가 효과적인지 또는 RBL 코스에 참여하는 학생의 유형이 효과적인지 여부가 불분명합니다(Linn 외. 2015). 일부 저자들은 RBL 과정을 찾는 학생들이 애초에 다른 학생들보다 학업 능력이 더 높고 동기 부여가 더 강하다고 주장합니다(Carter 외. 2016). 우리 표본에서는 RBL 과정 참여가 학생들의 학습 프로그램에서 필수적인 부분인 경우가 많았기 때문에 표본에서 강한 자기 선택 편향이 있을 가능성을 배제할 수 없습니다. 그럼에도 불구하고 RBL의 효과에 대한 최종 결론을 도출하기 위해서는 의미 있고 일치하는 대조군이 필요합니다(예: RBL 과정 대기자 명단이 있는 학습 프로그램을 조사하는 등). A problem with our and other studies in the field is the lack of a control group (cf. Lopatto2004). Without an adequate comparison group, it remains unclear whether the research experience itself is effective or whether it is the type of student who participates in RBL courses (Linn et al.2015). Some authors claim that students who seek out RBL courses have higher academic abilities and are more motivated than other students in the first place (Carter et al.2016). In our sample, participation in the RBL course was often a mandatory part of the students’ study programme; thus, a strong self-selection bias in our sample can be ruled out. Nevertheless, a meaningful, matched control group is still necessary to draw final conclusions on the effectiveness of RBL, e.g. by examining study programmes with a waiting list for RBL courses.
또 다른 한계는 테스트 시점과 관련이 있습니다. 사후 측정은 강의가 끝날 무렵 강의실에서 실시되었기 때문에 최종 논문 작성이나 연구 결과 발표의 효과를 반영하지 못했습니다. 그러나 자신의 연구에 대해 공개적으로 발표하는 것은 학생들에게 특히 동기를 부여하는 것으로 묘사되어 왔으며(Cuthbert, Arunachalam, Licina 2012), 따라서 RBL과 관련된 학습 결과에 영향을 미칠 수 있습니다. 향후 연구에서는 추후 또는 후속 측정을 통해 최종 과제의 효과를 통합해야 합니다. Another limitation concerns the testing time point. Since the post-measurement was conducted in the classroom towards the end of the course, our results do not reflect the effect of writing final papers or presenting research results. However, giving a public presentation on one’s research has been described as particularly motivating by students (Cuthbert, Arunachalam, and Licina2012) and thus might influence the learning outcomes associated with RBL. Future research should incorporate the effects of final assignments by using later or follow-up measurements.
본 연구의 정량적 설정은 연구 프로젝트에 대한 학생들의 개인적인 관점, 연구 과정의 어려움에 대한 개별적인 반응, 교수자의 행동에 대한 추가적인 생각을 다룰 수 없음을 의미했습니다. 향후 프로젝트에서는 심층 인터뷰를 통해 학생들의 관점을 통합하여 본 연구의 예비 결과와 그에 따른 시사점을 추가로 탐색하고 검증할 수 있습니다. Our study’s quantitative set-up meant that the students’ personal perspectives on their research projects, individual reactions to challenges in the research process and additional thoughts on their instructors’ behaviour could not be addressed. A future project could further explore and validate the preliminary findings of this study and the resulting implications by incorporating students’ perspectives via in-depth interviews.
이 연구의 목적은 인지적 및 정서적 동기부여 연구 성향을 향상시키기 위한 사회과학 분야의 RBL 과정의 효과를 조사하는 것이었습니다. 연구 결과에 따르면 RBL은 연구 지식과 연구 관련 불확실성 내성을 향상시키는 데 효과적인 교육 형식이라는 결론을 내릴 수 있습니다. 특히 학생들이 RBL 경험이 향후 커리어에 도움이 될 것이라고 생각할 때 RBL 과정이 효과적이라는 것이 입증되었습니다. The aim of this study was to examine the effectiveness of RBL courses in the social sciences for enhancing cognitive and affective-motivational research dispositions. Based on the results, we can conclude that RBL is an effective instructional format for enhancing research knowledge and research-related uncertainty tolerance. RBL courses proved especially effective when students thought the RBL experience was useful for their later career.
RBL이 효과적인 교육 형식인지에 대한 질문은 지금까지 STEM 분야의 연구에서 주로 다루어져 왔으며, 사회과학 분야의 증거는 아직 부족합니다. 본 연구에서는 사전-사후 설계를 사용하여 다양한 사회과학 분야의 학생들을 대상으로 RBL의 효과에 대한 체계적인 설명을 제공함으로써 학문별 측정치를 향상시키고자 했습니다. 선택한 절차는 해당 분야의 기존 증거를 확장하는 데 적합했지만, 추가 연구 노력에서 해결해야 할 다양한 미해결 질문이 남아 있습니다.
The question of whether RBL is an effective instructional format has so far been dominated by studies from the field of STEM, while evidence from the social sciences remains scarce. Our study sought to provide a systematic account of the effectiveness of RBL among students from different social scientific disciplines for enhancing discipline-specific measures using a pre–post design. While the chosen procedure was suitable for extending existing evidence in the field, a range of open questions remain that should be addressed in further research endeavours.
ABSTRACT
Research-based learning (RBL) is regarded as a panacea when it comes to effective instructional formats in higher education settings. It is said to improve a wide set of research-related skills and is a recommended learning experience for students. However, whether RBL in the social sciences is indeed as effective as has been postulated for other disciplines has not yet been systematically examined. We thus administered a pre–post-test study toN = 952 students enrolled in 70 RBL courses at 10 German universities and examined potential changes in cognitive and affective-motivational research dispositions. Latent change score modelling indicated that students increased their cognitive research dispositions, whereas most affective-motivational research dispositions decreased. The instructors’ interest in the students’ work served as a significant predictor of changes in research interest and joy. Practical implications for designing RBL environments can be inferred from the results.
의학교육커리큘럼에서 인공지능의 필요성, 도전, 적용(JMIR Med Educ.2022) Needs, Challenges, and Applications of Artificial Intelligence in Medical Education Curriculum Joel Grunhut1*, BA; Oge Marques2,3*, PhD; Adam T M Wyatt4*, PhD
소개 Introduction
인공지능(AI)과 그 응용 분야는 진단, 진단 촉진, 의사 결정, 빅데이터 분석, 관리 등 의료 분야의 많은 글로벌 문제를 해결할 수 있는 큰 가능성을 가지고 있습니다[1,2]. AI는 전 세계 의사 부족 문제를 해결하고 전 세계 오지에 의료 서비스를 제공할 수 있는 잠재력을 가지고 있습니다[2]. Artificial intelligence (AI) and its applications hold great promise for solving many of health care’s global issues including making diagnoses, facilitating diagnostics, decision-making, big-data analytics, and administration [1,2]. AI has the potential to solve the global doctor shortage and bring access to health care to remote areas of the world [2].
이미 많은 의료 분야에서 AI의 실제 적용을 통해 혜택을 보고 있습니다. 예를 들어 심방세동, 간질 발작, 저혈당증을 감지하거나 조직 병리 검사 또는 의료 영상에 기반한 질병 진단 등이 있습니다[3]. AI의 사용은 영상의학이나 병리학 분야에 국한된 것이 아니라, 1차 진료부터 긴급한 중환자 결정에 이르기까지 다양한 분야를 아우르는 단일 데이터 형태인 이미지 인식에 대한 AI의 힘을 보여주는 지표입니다. 최근 데이터에 따르면 의학의 모든 전문 분야에서 의사를 보조하는 데 AI를 활용하는 방안을 모색하고 있습니다[4]. 딥러닝 알고리즘은 다양한 의료 분야에서 웨어러블, 스마트폰 및 기타 모바일 모니터링 센서를 통해 개인이 매일 사용하는 데이터의 양이 증가함에 따라 이를 기능적으로 이해할 수 있습니다[3]. AI는 대부분의 데이터 형태에 대해 분석을 수행하고 지능적인 실행 가능한 권장 사항을 제공하는 기능을 지속적으로 개선할 것입니다[5]. 향후 AI의 발전은 의료의 모든 측면에 스며들 것으로 예상됩니다[6]. Many fields of medicine have already seen benefit from the practical application of AI. Examples include the detection of atrial fibrillation, epilepsy seizures, and hypoglycemia, or the diagnosis of disease based on histopathological examination or medical imaging [3]. The use of AI is not limited to the fields of radiology or pathology; rather, those fields are indicators of the power of AI for image recognition, a singular form of data that transverses many fields spanning from primary care practice to urgent midsurgical decisions. Recent data show that every specialty in medicine is exploring the use of AI in assisting physicians [4]. Deep learning algorithms can make functional sense of increasing amounts of data used by individuals daily through wearables, smartphones, and other mobile monitoring sensors in different areas of medicine [3]. AI will continue to improve its capabilities to perform analysis and provide intelligent actionable recommendations on most forms of data [5]. It is expected that the future advancements in AI will permeate all aspects of medicine [6].
파괴적 혁신 Disruption
AI가 의료 분야에서 계속 발전하고 있지만 도전 과제가 없는 것은 아닙니다. AI는 이러한 임상 진료의 진화에 대비하지 못한 의사들의 저항에 직면해 있습니다[3]. 의사들은 AI의 발전으로 혜택을 받을 가능성이 높지만, 대체에 대한 두려움으로 인해 이러한 기회를 놓칠 수 있습니다. 또한 AI에 대한 지식이 부족하면 머신러닝 예측의 신뢰성에 대한 회의론이 생길 수 있습니다. 이러한 반발로 인해 다른 전문 분야에서는 AI 솔루션을 사용하여 산업을 발전시키는데 반해 의료 부문의 상당 부분이 AI에 적응하지 못하고 있을 수 있습니다[3]. As AI continues to make advancements in health care, it is not without challenges. AI is met with resistance from physicians ill-equipped for such an evolution of clinical practice [3]. It is likely that physicians would benefit from the advancements of AI, but an understandable fear of replacement may prevent these opportunities. Furthermore, a lack of knowledge in AI can create skepticism in the trustworthiness of a machine learning prediction. This pushback may be preventing a large part of the health care sector from adapting to AI as other professional sectors continue to use AI solutions to advance their industries [3].
AI는 기존의 임상의사-환자 양자 구도를 훨씬 더 윤리적이고 감정적으로 복잡한 임상의사-AI-환자 삼자 구도로 변화시킬 것입니다. 이는 윤리적, 법적, 재정적 영향과 함께 신뢰와 책임 측면을 극적으로 변화시킬 것입니다[7]. 의사는 이러한 큰 변화에 대비해야 합니다[8]. AI will change the dynamics of the traditional clinician-patient dyad to a much more ethically and emotionally complex clinician-AI-patient triad. This will dramatically alter the trust and accountability aspects with ethical, legal, and financial implications [7]. Physicians must be prepared for this great change [8].
AI와 같은 신흥 기술은 전통적인 교육 프로그램을 통해 유지되는 노동 시장을 혼란에 빠뜨릴 잠재력을 가지고 있습니다. 이러한 시장 혼란에 탄력적으로 대응하기 위해서는 의사 교육 프로그램에 변화가 필요합니다[9]. 현재의 학부 의학교육(UME) 커리큘럼은 진화하는 기술의 새로운 요구사항에 점점 더 부합하지 못하고 있습니다. 대부분의 의과대학이 변화를 수용하고 의학 커리큘럼의 구성 요소를 정기적으로 업데이트하기 위해 노력하고 있지만, 대대적인 개편은 달성하기 어렵고 커리큘럼에서 AI를 구현하는 데 방해가 될 수 있습니다. 깊이 내재된 가치와 인증 과정 등 다양한 요인으로 인해 중요한 커리큘럼 개혁을 달성하기는 어렵습니다[10]. Emerging technologies such as AI have the potential to disrupt labor markets maintained through traditional education programs. In order to be resilient to these market disruptions, physician training programs will require change [9]. The current undergraduate medical education (UME) curriculum is increasingly out of sync with the new needs of an evolving technology. Although most medical schools embrace change and strive to regularly update the components of the medical curriculum, a major overhaul is difficult to achieve and may be a hindrance to the implementation of AI in the curriculum. The path to significant curricular reform is difficult because of a variety of factors, including deeply embedded values and the accreditation process [10].
UME는 미래를 맞이하고 학생들에게 AI를 통해 더 넓은 범위의 의료 서비스에 대한 접근성을 제공해야 합니다. [데이터 과학에 대한 지식, 알고리즘 품질 평가, 다양한 AI 제품 간 변별]은 의학교육의 필수 구성 요소이며, 교수진은 이를 통합하기 시작해야 합니다. 의과대학은 의사가 미래에 대체할 수 없는 역할을 확립하기 위해 컴퓨터보다 경쟁 우위를 점할 수 있는 고유한 인간 능력을 가르치고 육성하기 시작해야 합니다[9]. UME must begin to welcome the future and provide students access to a broader scope of health care through AI. Knowledge on data science, assessing algorithmic quality, and differentiating among different AI products are necessary components of medical education, which faculty must begin to incorporate. Medical schools must begin to teach and nurture unique human abilities that give physicians a competitive advantage over computers to establish an irreplaceable role in the future [9].
의사에게는 어떤 기술이 필요할까요? What skills Do Physicians Need?
의료계는 임상 의사 결정을 개선하기 위한 데이터 사용이 증가하면서 숙련된 의사와 기계의 상호 작용이 필요한 AI 시대에 접어들고 있습니다[11]. 차세대 의사에게 올바른 기술과 AI에 대한 적응력을 교육하면 이 새로운 데이터 과학 혁명의 일원이 될 수 있습니다[8]. 현재 의사가 AI와 함께할 수 있는 접근 방식은 다양합니다. 데이터 과학 과정을 수강하는 의사, 펠로우십 기회를 얻는 의사, 의학교육 프로그램에 참여하는 데이터 과학자 등이 있습니다. 이들은 전체 의사 인구의 극히 일부에 불과하므로 UME에서 보다 통합적이고 전향적인 접근 방식이 필요합니다. The practice of medicine is entering the age of AI in which the use of data to improve clinical decision-making will grow, bringing forth the need for skillful medicine-machine interaction [11]. Educating the next generation of physicians with the right techniques and adaptations to AI will enable them to become part of this emerging data science revolution [8]. Currently, there are different approaches for physicians to become accompanied to AI. There are physicians taking courses in data science, fellowship opportunities, and data scientists entering medical education programs. These represent a small fraction of the total physician population, and therefore a more integrative and forward approach in UME is necessary.
의료 전문가들은 AI의 장점과 비용 절감, 품질 향상, 의료 서비스 접근성 확대 등의 잠재력에 대해 충분히 교육받아야 합니다. 마찬가지로 중요한 것은 의사가 투명성 및 책임과 같은 AI의 단점에 대해 잘 알고 있어야 한다는 것입니다. 이러한 목표를 달성하기 위해서는 커리큘럼의 여러 측면에 걸쳐 AI를 원활하게 통합해야 합니다[11]. Medical professionals need to be sufficiently trained in AI, its advantages, and its potential to lower cost, improve quality, and expand access to health care. Of equal importance, physicians should be knowledgeable in its shortfalls such as transparency and liability. AI needs to be seamlessly integrated across the different aspects of the curriculum to achieve these goals [11].
AI 솔루션의 권장 사항을 환자의 치료 과정에 통합할 때 의사는 환자가 가질 수 있는 모든 우려에 답할 수 있어야 합니다. 더 중요한 것은 의사가 AI가 환자 치료에 도움이 되는 기술이 되고 해를 끼치는 기술이 되지 않도록 할 책임이 있다는 것입니다. 기술 혁명은 의료 분야에서 AI 기반 구현에 대한 윤리적 고려 사항과 관련하여 많은 과제를 제기합니다. 데이터베이스의 소수자 배제, 법적 보호 문제, 인본주의적 터치의 감소 등 여러 윤리적 문제들이 의료 분야에 AI를 적용하는 데 있어 우려를 불러일으킵니다. 이러한 이유로 인해 미래의 의사에게 매우 중요한 의무인 AI에 대한 충분한 지식과 경험 습득의 중요성이 부각되고 있습니다[12]. When incorporating recommendations from AI solutions to a patient’s course of treatment, physicians should be capable to answer any concerns that patients may have. Perhaps even more importantly, physicians are responsible for ensuring that AI becomes a technology beneficial for patient care and not possibly a cause of harm. The technological revolution raises many challenges with regards to ethical considerations of AI-based implementation in health care. Minority exclusions in databases, issues with legal protections, and a decrease in humanistic touch, among other ethical issues, raise concern for an adaptation of AI in health care. These reasons bring forth the importance of acquiring sufficient knowledge and experience about AI, an obligation of high importance for future physicians [12].
의과대학은 학생들에게 데이터 과학, 생물 통계학, AI의 생명윤리적 영향, 근거 기반 의학 등과 함께 기초 및 임상 의학에 대한 폭넓은 지식을 교육하는 데 필요한 조치를 취해야 합니다. 의대생 교육에는 [올바른 정보와 수사를 구별하는 능력]과 [환자와 대중을 위해 철저하게 검증되고 신뢰할 수 있는 정보를 만들고 배포하는 방법을 이해하는 능력] 개발이 포함되어야 합니다[12]. Medical schools should take necessary steps to educate students with widespread knowledge of basic and clinical medicines along with data science, biostatistics, bioethical implications of AI, and evidence-based medicine. Part of a medical student’s training should include developing the abilities to distinguish correct information from rhetoric and to understand how to create and disseminate thoroughly validated, trustworthy information for patients and the public [12].
제안 단계 Suggested Steps
현재 의학교육에서 인공지능은 초기 단계에 있으며 추측 단계에 머물러 있습니다[13-16]. 이전에 우리는 이 주제에 대해 발표된 대부분의 문헌이 학부 의학교육의 변화를 요구하고 있으며 커리큘럼 변화를 뒷받침하기 위한 연구가 필요하다는 것을 보여주었습니다[17]. 그럼에도 불구하고 이러한 변화를 만들기 위해 취해야 할 단계에 대해 고민한 사람은 거의 없습니다. 이는 주요 커리큘럼 개편을 실행하는 데 어려움이 있기 때문에 예상되는 일입니다. 여기에서는 인식되는 어려움에 대한 개요를 제공하고 이러한 문제를 해결하기 위한 해결책을 제시합니다(표 1). Currently, the state of AI in medical education is in its infancy and speculative stages [13-16]. Previously, we have shown that the majority of published literature on the topic call for change in undergraduate medical education and that research is necessary to support curricular changes [17]. Even so, few have given thought to the steps that must be taken to create this change. This is expected because of the difficulty in implementing major curricular changes. Here, we provide an outline of the perceived difficulties and offer solutions to resolve these challenges (Table 1).
의과대학 커리큘럼 변경은 변화에 대한 저항으로 인해 실행하기 어렵습니다. 이러한 저항은 변화를 통합하는 방법에 대한 합의가 부족하고 이미 바쁜 커리큘럼으로 인해 정당화됩니다. 이러한 이유로 추가 교과목이나 업무량을 제안하면 의대생에게 최선의 이익이 되는 의학교육 교수진의 비판에 직면할 가능성이 높습니다. 국가 인프라 수준에서 이러한 문제는 의학교육 및 기관의 리더가 지원할 수 있습니다. 이러한 인식은 연례 미국 의과대학 졸업 설문조사에 1~3개의 질문을 추가하여 학생들의 관심도와 능력을 측정함으로써 쉽게 명확히 할 수 있습니다. 예를 들어, 설문지에는 UME 기간 동안 AI를 가르쳐야 하는지, 몇 학년도에 가르쳐야 하는지, 어떻게 통합해야 하는지에 대한 동의를 구할 수 있습니다. 이러한 의견은 인증 요건으로 전환되어 변화를 촉진할 수 있습니다. Medical school curricular changes are difficult to implement due to resistance to change. This resistance is justified through a lack of consensus on how to incorporate change and an already busy curriculum. For this reason, proposing additional courses or workload will likely be met with criticism from medical education faculty in the best interest of medical students. On a level of national infrastructure, these issues can be supported by leaders of medical education and organizations. These perceptions can be clarified easily through the addition of 1-3 questions on the annual Association of American Medical Colleges Graduation Questionnaire to gauge interest and ability over time from students. For example, the questionnaire can ask for agreement on whether AI should be taught during UME, what year of training it should be taught in, and how it should be incorporated. These can translate into accreditation requirements and drive change forward.
Table 1. Multitiered solutions to include AIin the medical education curriculum.
Levels and target areas of improvement
Examples
National infrastructure
AAMCb
Questionnaire, materials, and guidance
LCMEc
Minimal requirements and expert panels
Multi-institutional research
Longitudinal research on attitudes and quality improvements
Individual school
Faculty expansion
Bioethics, bioinformatics, and medical AI experience
Basic knowledge lessons
Introductory courses, benefits and pitfalls of AI, and ethics of AI
Case-based learning
Multispecialty implications in previous cases and biostatistical implications
Student specific
Journal clubs or reading groups
Specialty-specific journals, health care systems journals, and AI in health care journals
Use of AI in clinical setting
Tumor board, radiology rotation, and point of care ultrasound
aAI: artificial intelligence.
bAAMC: Association of American Medical Colleges.
cLCME: Liaison Committee on Medical Education.
더 중요한 질문은 학부 의학교육자들이 어떻게 연합하여 커리큘럼에 AI를 통합하는 것에 대한 수준 높은 연구를 수행할 수 있는가 하는 것입니다. 연구와 프로토콜의 기준이 서로 다른 개별 학교의 보고서가 모든 학부 의학교육에 필요한 변화를 정의할 수 있을까요? 여러 의과대학의 공동 및 연합 연구 노력은 이 문제에 대한 다각적이고 다양한 의견을 제공할 수 있으며, 이는 반드시 필요합니다. A more overarching question is how undergraduate medical educators can unite to perform high-quality research on the incorporation of AI in the curriculum. Would individual school reports with differing standards in research and protocol do justice to a necessary change across all undergraduate medical education? A joint and united research effort from multiple medical schools would provide a multifaceted and diverse input on the issue and is necessary.
개별 학교 차원에서는 커리큘럼을 개선하기 위한 자원 투자가 필요할 것입니다. 시간 및 내용 제약 문제를 해결하기 위해 UME 전반에 걸친 종단적 AI 스레드를 옹호해야 합니다. 근거 기반 의학을 가르치는 과정에는 AI의 입력을 평가하는 추가적인 관점을 통합해야 합니다. 의과대학 교수진은 근거 기반 의학에서 AI의 역할에 대한 질문에 답하거나 토론할 준비가 되어 있지 않을 수 있습니다. 따라서 의과대학 교수진에 다른 학교의 임상의학 데이터 과학자나 컴퓨터 과학 및 공학 교수진을 추가하는 것이 필수적입니다. On an individual school level, investments of resources will be necessary to create improvements in the curriculum. A longitudinal AI thread throughout the UME should be advocated to solve time and content constraint issues. Courses teaching evidence-based medicine should incorporate an additional perspective of evaluating the input of AI. Medical school faculty may not be equipped to answer questions or discuss the role of AI in evidence-based medicine. Therefore, it is imperative to add clinician data scientists or computer science and engineering faculty from other schools to medical school teaching faculty.
공중 보건 과학을 배우는 학생들은 AI가 미래의 연구와 진료에서 무엇을 할 수 있고 무엇을 할 수 없는지 알기 위해 AI에 대한 배경 지식을 습득해야 합니다. 의과대학 커리큘럼에서 AI의 전체 과정을 가르치는 것은 너무 어렵습니다. 의학에서 AI에 대한 입문 강의는 반드시 필요하고 옹호되어야 합니다. 대부분의 학교에서는 강사가 데이터 과학자일 가능성이 높지만, 강사가 강의 경험이 있고 의대생에게 친숙하며 의학에서 AI의 역할에 대해 잘 알고 있는 사람이어야 합니다. 강사는 이전에 컴퓨터 과학 과목에서 의학에서 AI의 역할에 대해 이미 가르친 적이 있는 것이 좋습니다. 가장 중요한 것은 강사가 AI가 의료 분야에 가져온 광범위한 윤리적 문제를 다룰 수 있는 수준의 생명윤리 역량을 갖추고 있어야 한다는 것입니다. Students learning public health sciences must be introduced to a background in AI in order to know what AI can and cannot do for their future research and practices. It is far too difficult to teach entire courses of AI in a medical school curriculum. An introductory lecture to AI in medicine is a necessity and should be advocated for. In most schools, the instructor will likely be a data scientist, but it is important that the instructor has teaching experience, is familiar with medical students, and is conversant with the role of AI in medicine. Preferably, the instructor will have already taught about the role of AI in medicine previously in a computer science course. Most importantly, instructors should have levels of competency in bioethics to address the expansive ethical issues AI has brought to health care.
사례 기반 학습과 시뮬레이션 학습은 임상 시나리오에 AI 기반 권장 사항을 통합할 수도 있습니다. 사례와 시뮬레이션에 AI를 통합함으로써 학생들은 AI 기반 솔루션을 접하고 친숙해질 수 있습니다. AI 애플리케이션을 협업하고 관리하려면 의대생이 확률적 추론에 대한 깊은 이해와 윤리적 고려가 필요합니다[10]. 이러한 수업은 AI 추천의 정확성과 해석에 대한 지식을 갖춘 교수진이 가르쳐야 합니다. 의과대학은 의학 콘텐츠에서 양질의 AI를 제공하기 위해 이 분야의 교수진을 추가로 채용해야 할 가능성이 높습니다. Case-based learning and simulation learning can also incorporate AI-based recommendations in clinical scenarios. By integrating AI into cases and simulations, students can have exposure and familiarity with AI-based solutions. Collaborating and managing AI applications will require a deep understanding of probabilistic reasoning and ethical consideration from medical students [10]. These lessons should be taught from faculty with knowledge about the accuracy and interpretations of AI recommendations. It is likely that medical schools will need to hire additional faculty in this field to ensure quality delivery of AI in medicine content.
또 다른 제안은 다른 기관에서 만든 웹 기반 의료 프로그램(예: 스탠포드 대학의 의료 분야의 인공 지능 전문가 프로그램)에서 AI에 대한 액세스를 제공하는 것입니다. 이러한 프로그램은 의료와 AI의 접점에서 세계적으로 유명한 전문가인 교수진이 가르치며, 의대생은 비용을 지불하고 프로그램을 이용할 수 있습니다. 프로그램에 대한 액세스를 제공함으로써 의과대학은 다른 방법으로는 제공할 수 없었던 새로운 지식을 커리큘럼에 주입할 수 있습니다. Another suggestion is for institutions to offer access to AI in web-based health care programs created at other institutions (eg, Stanford University’s Artificial Intelligence in Healthcare professional program). These programs are taught by faculty who are world-renowned experts at the interface of health care and AI, and the programs are available to medical students with a cost. Providing access to a program will enable medical schools to infuse new knowledge in a curriculum that could not be provided otherwise.
학생 개개인의 차원에서는 학생들이 AI에 능동적으로 참여함으로써 교육의 변화를 주도할 수 있습니다. 앞서 의대생이 AI 도구를 코딩하고 만드는 방법을 배울 필요는 없지만,AI의 작동 방식과 한계는 이해해야 한다는 데 대부분의 최신 문헌이 동의하고 있음을 살펴봤습니다[17]. 학생들은 의학 저널에서 의료 분야의 AI 발전에 대해 읽을 수 있습니다. 의료 AI를 주제로 한 저널을 포함하여 많은 주요 저널에서 AI 연구가 활발히 진행되고 있습니다. 의료 분야 AI의 최신 동향을 읽음으로써 학생들은 의료의 미래에 대한 정보를 얻고 준비할 수 있습니다. 의과대학에서 증거 기반 의학 학습과 결합하면 학생들은 AI 연구의 무결성을 평가할 수 있습니다. On an individual student level, students can help drive change in their education with a proactive engagement with AI. Previously, we have shown that most of the current literature agrees that medical students do not need to learn how to code and create AI tools, but they should understand how AI works and its limitations [17]. Students can read about AI advancements in health care in medical journals. AI research has a strong appearance in many leading journals, including medical AI-themed journals. Reading the current trends in AI in health care will inform and prepare students for the future of health care. When combined with evidence-based medicine learning at medical school, students will be able to assess the integrity of AI research.
학생들은 임상 환경에서도 AI를 접할 수 있습니다. 이미 AI 기반 소프트웨어가 탑재된 개별 휴대용 초음파를 통해 학생들이 교육에 도움을 받았다는 보고가 있습니다[18,19]. 학생들은 방사선과 로테이션에서 AI 애플리케이션을 보고 AI 애플리케이션의 영향을 받는 환자 치료에 관여하는 여러 전문 분야의 방사선과 전문의 및 임상의와 임상 의사 결정에서 AI의 역할에 대해 토론할 수 있습니다. AI 통합은 전문 분야에 따라 다르겠지만, 의료 서비스 전반에 걸쳐 AI가 도입될 가능성이 높습니다. 예를 들어 방사선과 전문의, 병리학자, 종양 전문의, 외과의로 구성된 종양 위원회는 AI 애플리케이션의 영향을 받습니다. 학생들은 관심 있는 분야에 대한 노출을 맞춤화할 수 있습니다. 위의 제안은 의학교육 전반에 적용되며 일반 의학교육의 중요성과 개선의 여지를 강조합니다. 전문 분야에 특화된 AI 주제는 UME에는 필요하지 않을 수 있지만 레지던트 과정과 그 이후에는 필요할 수 있습니다. 그럼에도 불구하고 의과대학은 AI에 대한 종단적 커리큘럼을 통해 학생들이 AI를 사용하여 다양한 전문 분야를 접할 수 있도록 할 수 있습니다. Students can expose themselves to AI in the clinical setting as well. There are already reports of students receiving individual portable ultrasounds with AI-driven software to help advance their education [18,19]. Students can see AI applications in their radiology rotations and discuss its role in clinical decision-making with radiologists and clinicians across different specialties involved in patient care impacted by AI applications. AI integration will be specialty specific, but AI as a whole will likely be present across health care. For example, a tumor board, consisting of radiologists, pathologists, oncologists, and surgeons, is impacted by AI applications. Students can tailor their exposure toward fields of interests. The suggestions above apply to medical education as a whole and highlight the importance and room for improvement in general medical education. Specialty-specific AI topics would not be necessary for UME but perhaps in residency and beyond. Nevertheless, through a longitudinal curricular thread in AI, medical schools can expose their students to a wide variety of specialties using AI.
AI를 통한 의사 결정의 교훈은 도시와 농촌을 막론하고 의료 서비스의 전 영역에 걸쳐 개인에게 적용될 것입니다. AI는 의료 서비스에 대한 접근성을 확대할 수 있는 잠재력을 가지고 있기 때문에 다양한 의료 환경에 침투할 것으로 예상됩니다. 따라서 학생 개개인은 어떤 의료 분야를 선택하든 AI에 대해 학습하여 대비해야 합니다. Lessons in decision-making with AI will apply to individuals across the spectrum of health care, both in city and rural settings. It is expected that AI will permeate various health care settings because of its potential to expand access to health care. Therefore, individual students should be prepared by learning about AI no matter what area of medicine they choose.
방법론적 접근 A Methodological Approach
새로운 의학 커리큘럼의 변화는 의대생에게 긍정적이거나 부정적인 영향을 미칠 수 있습니다. 또한 완전히 새로운 주제를 도입하는 것과 같은 커리큘럼의 변화는 어려운 작업입니다. 따라서 여러 지역의 의학교육 전문가들이 함께 협력하여 시행된 변화를 만들고 평가하는 것이 중요합니다. 교육 연구는 다양한 커리큘럼 개혁의 효과를 평가하는 데 필수적입니다[20]. 이러한 성공을 달성하기 위한 한 가지 제안은 커리큘럼에서 다양한 AI 구현의 결과를 측정하기 위한 장기 연구를 시작하는 것입니다. New medical curricular changes can have tremendous positive and negative impacts on medical students. Additionally, a change in curriculum such as the introduction of an entire novel topic is a difficult task. Therefore, it is important that medical education specialists across different regions work in unison to create and assess the implemented changes. Educational research is vital to assessing the effectiveness of different curricular reforms [20]. One suggestion to achieving such success is to begin a long-term study to measure the outcomes of different implementations of AI in the curriculum.
학생과 교수진의 태도, 기술 수준, UME에서 AI에 대한 구체적인 요구 사항을 측정하는 연구는 현 시점에서 매우 중요하고 시급한 과제입니다. 이러한 제안을 통합하기 위한 추가 노력은 측정 가능하고 해석 가능한 데이터를 확보하여 UME에서 AI 구현을 발전시켜야 합니다. 이러한 목표를 달성하기 위해서는 여러 기관이 공동으로 연구하는 것이 논리적인 접근 방식입니다. Research measuring student and faculty attitudes, skill level, and specific needs of AI in UME is crucial and urgent at this point in time. Further efforts to incorporate these suggestions should be measurable and have interpretable data to advance the implementation of AI in UME. A concerted multi-institutional study is a logical approach in order to achieve these goals.
의과대학 학장들이 모여 AI 커리큘럼 개혁을 논의하고 계획해야 합니다. 조직 차원에서 의학교육 관리 기관은 이러한 변화를 제정하고 촉진해야 합니다. 의학교육 연락 위원회는 특별 위원회를 통해 AI를 의학교육에 가장 잘 통합하는 방법에 대한 제안과 지침을 제공해야 합니다. Medical education deans need to gather to discuss and plan AI curricular reform. At the organizational level, medical education governing bodies must enact and promote these changes. The Liaison Committee on Medical Education should provide suggestions and guidelines of how to best incorporate AI to medical education through special committees.
2018년에 미국의학협회는 "의학교육에서 AI 교육이 학습 및 임상 결과에 미치는 효과에 관한 연구"를 촉구했습니다[21]. 3년이 지난 지금, 이용 가능한 문헌에 따르면 UME는 이 요청에 대해 느리게 대응하고 있습니다[17]. 따라서 이 원래의 요청을 실천으로 옮기기 위해 더 많은 노력을 기울여야 합니다. In 2018, the American Medical Association called for “Research regarding the effectiveness of AI instruction in medical education on learning and clinical outcomes” [21]. Three years later, the available literature suggests UME has been slow to address this call [17]. Thus, further efforts should be made to advance this original call into practice.
결론 Conclusion
현재와 미래의 의학 분야 AI의 발전으로 인해 학부 의학교육자들은 커리큘럼에 AI를 도입하고 구현해야 합니다. 이러한 커리큘럼 변화를 가장 효과적으로 달성하는 방법을 효과적으로 연구하기 위해서는 종단적 연구 계획이 필요합니다. 의학교육 관리 기관, 의학교육 학장, 의학교육 연구자들은 학부 의학교육 커리큘럼에 AI를 구현하기 시작해야 합니다. 이러한 기관의 집단적 합의를 통해 앞으로 나아간다면 미래의 의사인 재학생들이 적절한 AI 노출을 받을 수 있을 것입니다. The current and future advancements of AI in medicine oblige undergraduate medical educators to act and implement AI in the curriculum. Longitudinal research plans are necessary to effectively study how to best achieve these curricular changes. Medical education governing bodies, medical education deans, and medical education researchers should begin to implement AI in the undergraduate medical education curriculum. Moving forward with collective agreement from these entities will ensure current students—our future physicians—receive adequate AI exposure.
JMIR Med Educ. 2022 Jun 7;8(2):e35587.doi: 10.2196/35587.
Needs, Challenges, and Applications of Artificial Intelligence in Medical Education Curriculum
1Schmidt College of Medicine, Florida Atlantic University, Boca Raton, FL, United States.
2Department of Electrical Engineering and Computer Science, College of Engineering and Computer Science, Florida Atlantic University, Boca Raton, FL, United States.
3Department of Biomedical Sciences, Schmidt College of Medicine, Florida Atlantic University, Boca Raton, FL, United States.
4Department of Population Health and Social Medicine, Schmidt College of Medicine, Florida Atlantic University, Boca Raton, FL, United States.
Artificial intelligence (AI) is on course to become a mainstay in the patient's room, physician's office, and the surgical suite. Current advancements in health care technology might put future physicians in an insufficiently equipped position to deal with the advancements and challenges brought about by AI and machine learning solutions. Physicians will be tasked regularly with clinical decision-making with the assistance of AI-driven predictions. Present-day physicians are not trained to incorporate the suggestions of such predictions on a regular basis nor are they knowledgeable in an ethical approach to incorporating AI in their practice and evolving standards of care. Medical schools do not currently incorporate AI in their curriculum due to several factors, including the lack of faculty expertise, the lack of evidence to support the growing desire by students to learn about AI, or the lack of Liaison Committee on Medical Education's guidance on AI in medical education. Medical schools should incorporate AI in the curriculum as a longitudinal thread in current subjects. Current students should understand the breadth of AI tools, the framework of engineering and designing AI solutions to clinical issues, and the role of data in the development of AI innovations. Study cases in the curriculum should include an AI recommendation that may present critical decision-making challenges. Finally, the ethical implications of AI in medicine must be at the forefront of any comprehensive medical education.
Keywords:AI; artificial intelligence; medical education; medical student.
의학교육에서 인공지능 훈련 도입하기 (JMIR Med Educ.2019) Introducing Artificial Intelligence Training in Medical Education Ketan Paranjape1*, MS, MBA; Michiel Schinkel2*, MD; Rishi Nannan Panday3, MD; Josip Car4, MD, PhD, FRCP; Prabath Nanayakkara2, MD, PhD, FRCP
의료 서비스 트렌드 Trends in Health Care
전 세계 의료 서비스 지출은 2017년 7조 7,000억 달러에서 2022년 10조 달러로 5.4%의 비율로 증가할 것으로 예상됩니다[1]. 이는 선진국의 경우 국내총생산에서 의료비가 차지하는 비중이 평균 9%에 달한다는 것을 의미합니다[2,3]. 의료 서비스 접근성 및 경제성 확대에 영향을 미칠 수 있는 미국의 세제 개혁 및 정책 변화(건강보험개혁법)[4], 유럽연합 탈퇴 결정에 따른 영국의 의료 서비스 지출에 대한 영향[5] 등이 주요 글로벌 동향으로 꼽힙니다, 중국과 인도의 인구 증가와 부의 증가[6-8], 러시아의 의료 서비스를 위한 사회경제 정책 개혁 시행[9], 아르헨티나의 보편적 의료 서비스를 효과적으로 만들기 위한 시도[10], 아프리카의 전자 의료 및 원격 의료에 대한 대대적인 추진[11], 전 세계적으로 전례 없는 인구 고령화 속도의 영향[12] 등이 있습니다. Global health care expenditure has been projected to grow from US $7.7 trillion in 2017 to US $10 trillion in 2022 at a rate of 5.4% [1]. This translates into health care being an average of 9% of gross domestic product among developed countries [2,3]. Some key global trends that have led to this include tax reform and policy changes in the United States that could impact the expansion of health care access and affordability (Affordable Care Act) [4], implications on the United Kingdom’s health care spend based on the decision to leave the European Union [5], population growth and rise in wealth in both China and India [6-8], implementation of socioeconomic policy reform for health care in Russia [9], attempts to make universal health care effective in Argentina [10], massive push for electronic health and telemedicine in Africa [11], and the impact of an unprecedented pace of population aging around the world [12].
임상의의 관점에서 볼 때 의료 정보의 증가는 놀라울 정도로 의료 서비스 제공 방식에 영향을 미치는 중요한 트렌드가 많이 있습니다. 1950년에 의료 정보가 두 배로 늘어나는 데 50년이 걸렸습니다. 1980년에는 7년이 걸렸습니다. 2010년에는 3.5년이 걸렸고 2020년에는 73일 만에 두 배가 될 것으로 예상됩니다[13]. 이러한 성장은 의료 전문가들이 의료 정보를 보유하고 이를 효과적으로 진료에 활용해야 하는 과제를 안겨주고 있습니다. From clinicians’ perspective there are many important trends that are affecting the way they deliver care of which the growth in medical information is alarming. It took 50 years for medical information to double in 1950. In 1980, it took 7 years. In 2010, it was 3.5 years and is now projected to double in 73 days by 2020 [13]. This growth is posing a challenge to health care professionals to both retain and use it effectively to practice medicine.
의료 분야에서 인공지능의 부상 Rise of Artificial Intelligence in Health Care
의료 분야의 인공 지능 Artificial Intelligence in Health Care
인공 지능(AI)은 일반적으로 인간의 특성인 작업을 수행할 수 있는 컴퓨터 알고리즘을 이해하고 만드는 데 중점을 둔 과학 분야입니다[14]. AI는 이제 의료 분야에서 탄력을 받고 있습니다. "기계가 생각할 수 있는가?"라는 질문을 제기한 튜링의 중요한 논문인 컴퓨팅 기계와 지능[15]에 뿌리를 둔 AI는 먼 길을 걸어왔습니다. 자연어 처리(NLP)[16], 음성 인식[17], 가상 에이전트[18], 의사 결정 관리[19], 머신 러닝[20], 딥 러닝[21], 로봇 프로세스 자동화[22] 등이 AI의 발전 사례로 꼽힙니다. Artificial intelligence (AI) is a scientific discipline that focuses on understanding and creating computer algorithms that can perform tasks that are usually characteristics of humans [14]. AI is now gaining momentum in health care. From its early roots in Turing’s seminal paper, Computing Machinery and Intelligence [15], where he proposed the question “Can machines think?”, AI has come a long way. Examples of advances in AI include natural language processing (NLP) [16], speech recognition [17], virtual agents [18], decision management [19], machine learning [20], deep learning [21], and robotic process automation [22].
오늘날 AI는 의료 분야에서 더 빠르고 정확한 진단을 위해[23], 영상의학을 보강하고[24], 사람의 피로로 인한 오류를 줄이고, 의료 비용을 절감하고[25], 지루하고 반복적이며 노동 집약적인 작업을 보조 및 대체하고[26], 최소 침습 수술[27], 사망률을 줄이기 위해[28] 시범적으로 도입되고 있습니다. Today, AI is being piloted in health care [23] for faster and accurate diagnosis, to augment radiology [24], reduce errors due to human fatigue, decrease medical costs [25], assist and replace dull, repetitive, and labor-intensive tasks [26], minimally invasive surgery [27], and reduce mortality rates [28].
인공 지능의 도전 과제 Challenges With Artificial Intelligence
의료 분야에서 인공지능이 부상하고 일상적인 임상 진료에 통합되는 것은 어려운 과제가 될 것입니다. 의사의 기존 업무 방식 변화와 함께 블랙박스 문제[29]와 책임 문제[30]가 가장 예상되는 과제 중 하나입니다. The rise of AI in health care and its integration into routine clinical practice is going to be a challenge. Along with changing the conventional ways physician work, theblack box problem[29] and liability issues[30] are some of the most anticipated challenges.
블랙박스 Black Box
마운트 사이나이 병원의 연구원들은 70만 명의 환자 데이터로 학습된 딥러닝 알고리즘을 개발했습니다. 이 알고리즘은 정신분열증과 같은 질병의 발병을 높은 정확도로 예측할 수 있었습니다[31]. 이 질환은 전문가도 진단하기 어렵다는 사실을 고려하면 더욱 인상적입니다. 이 알고리즘의 가장 큰 문제점은 시스템이 어떻게 이러한 예측을 생성했는지, 어떤 요소를 고려했는지 알 수 없다는 것입니다. 이러한 현상을 블랙박스 현상이라고 합니다. 의학에서는 전례가 없는 일이지만, 시스템이 어떻게 작동하는지에 대한 이해가 없는 경우 시스템을 신뢰하기는 어렵습니다. 의사는 입력과 알고리즘을 이해하고 AI가 제안한 진단을 해석하여 오류가 없는지 확인해야 합니다. 또한 표준 치료법에 비해 좋은 결과를 입증할 수 있는 경우에도 블랙박스 의학의 결과 또는 의도하지 않은 부작용이 무엇인지 이해해야 합니다. Researchers at Mount Sinai Hospital have created a deep learning algorithm that was trained on the data of 700,000 patients. This algorithm was able to predict onset of a disease such as schizophrenia with high accuracy [31]. This is even more impressive considering the fact that this condition is difficult to diagnose even for experts. The main problem with this algorithm is that there is no way to know how the system created this prediction and what factors were taken into consideration. This phenomenon is called theblack boxphenomenon. It would not be a precedent in medicine, nevertheless it is difficult to trust a system when there is no understanding on how it works. The physician needs to understand the inputs and the algorithm and interpret the AI-proposed diagnosis to ensure no errors are made. We also need to understand what the consequences or unintended side effects are of black box medicine, even when good outcomes can be demonstrated against a standard of care.
마지막으로, 많은 AI 시스템이 인간과 동물의 중추 신경계의 측면을 모방하려고 시도하지만, 이는 여전히 블랙박스에 가깝습니다. 최근 논문에서 자도르[32]는 동물의 뇌에서 이 현상을 이해하기 위해 더 많은 것을 배울 수 있다고 주장했습니다. Finally, many of the AI systems attempt to mimic aspects of human and animal central nervous systems that are, at large, still a black box. In a recent paper, Zador [32] argued that we have much more to learn from animal brains to unravel this phenomenon.
개인정보 보호 및 데이터 제어 Privacy and Control Over Data
AI 알고리즘을 개발하려면 거의 대부분 많은 환자의 데이터가 필요합니다. 예를 들어, Google은 2개 병원에서 11년 동안 총 216,221명의 성인 비식별 데이터에서 수집한 460억 개의 데이터 포인트를 사용하여 입원 환자의 결과를 예측하고 있습니다[33,34]. 이는 환자 개인정보 보호 및 통제와 관련하여 많은 우려를 불러일으킵니다. 환자가 자신의 정보가 알고리즘 개발에 사용되는 연구에 참여하기를 원하지 않는다면 어떻게 될까요? 유럽연합에서는 잊혀질 권리에 따라 환자가 동의를 철회한 경우 개인 데이터를 삭제할 수 있습니다[35]. 환자 데이터가 제한적인 상황에서 알고리즘 개발자는 합성 데이터 또는 가상의 데이터로 모델을 학습시키므로 안전하지 않고 잘못된 치료 권장 사항을 생성할 위험이 있습니다[36]. 마지막으로, AI 시스템은 알고리즘이 의료 정보를 잘못 분류할 수 있는 사이버 보안 공격에도 취약합니다[37]. The development of AI algorithms almost as a rule requires data from a large number of patients. Google, for example, is using 46 billion data points collected from 216,221 adults’ deidentified data over 11 combined years from 2 hospitals to predict the outcomes of hospitalized patients [33,34]. This raises many concerns including relating to patient privacy and control. What happens if a patient does not want to participate in a study where their information is used in algorithm development? In the European Union, the Right to be Forgotten would allow personal data to be erased when the patient has withdrawn their consent [35]. In situations where patient data are limited, algorithm developers train the models on synthetic or hypothetical data, with the risk of generating unsafe and incorrect treatment recommendations [36]. Finally, AI systems are also vulnerable to cybersecurity attacks that could cause the algorithm to misclassify medical information [37].
환자 치료 및 책임에 대한 인공지능 사용 기준의 부재 Lack of Standards for Use of Artificial Intelligence in Patient Care and Liability
의료 분야에서 인공지능의 사용과 관련하여 해결되지 않은 또 다른 문제는 알고리즘의 예측에 대한 책임입니다. 부정확한 예측으로 인해 환자가 심각한 피해를 입었을 때 누가 책임을 져야 하는지 불분명합니다. 의사, 병원, 소프트웨어를 개발한 회사, 소프트웨어를 개발한 사람, 심지어 데이터를 제공한 사람 등 모든 관련 당사자가 책임을 져야 한다고 주장할 수 있습니다. 의료 분야에서 AI를 사용하기 위한 표준은 여전히 개발 중입니다[38,39]. 임상 치료, 품질, 안전, 의료 과실, 커뮤니케이션 가이드라인에 대한 새로운 표준을 개발하여 AI를 더 많이 사용할 수 있도록 해야 합니다. 최근 출시된 당뇨망막병증의 자율 감지를 위한 AI 시스템은 의료 과실 및 책임 보험에 가입되어 있습니다[40,41]. Another unresolved question related to the use of AI in health care is liability for the predictions of an algorithm. It is unclear who is liable when a patient experiences serious harm because of an inaccurate prediction. One could argue for any of the involved parties: the physician, the hospital, the company that developed the software, the person who developed the software, or even the person who delivered the data. Standards for use of AI in health care are still being developed [38,39]. New standards for clinical care, quality, safety, malpractice, and communication guidelines have to be developed to allow for greater use of AI. A recently launched AI system for autonomous detection of diabetic retinopathy carries medical malpractice and liability insurance [40,41].
AI 사용과 챗봇[42]과 같은 도구의 적극적인 사용이 증가함에 따라 의사와 환자는 이러한 기술의 강점과 한계를 인식하고 효과적이고 안전하게 사용하는 방법에 대한 교육을 받아야 합니다[43,44]. As use of AI and proactive use of tools such as chatbots [42] increases, physicians and patients will need to be aware of strengths and limitations of such technologies and be trained in how to effectively and safely use them [43,44].
인공지능은 오늘날 의사의 과제를 어떻게 해결할 수 있을까요? How Can Artificial Intelligence Address Today’s Physician Challenges?
의료 정보가 빠른 속도로 증가함에 따라 의사들은 이를 따라잡는 데 어려움을 겪고 있습니다. 이로 인해 정보 과부하가 발생하고 레지던트 자격을 얻기 위해 미국 의사 면허 시험(USMLE)을 통과하기 위해 이 모든 내용을 암기해야 한다는 압박감이 커지고 있습니다. 오늘날 의사들은 의료 비용이 증가하고 규제로 인해 행정 절차에 추가적인 부담이 가중되는 복잡한 질환과 동반 질환이 있는 고령화 사회에서 더 긴 시간 동안 일하고 있으며[45,46] 조정된 치료를 제공해야 할 것으로 예상됩니다. With medical information growing at a breakneck speed, physicians are having trouble keeping up. This is leading to information overload and creates pressure to memorize all this content to pass the United States Medical Licensing Examinations (USMLE) to qualify for residency positions. Physicians today are working longer hours and are also expected to deliver coordinated care [45,46] in an aging society with complex conditions and comorbidities where health care costs are increasing and regulations are putting an additional burden on administrative processes.
AI는 대량의 데이터를 통합하고 의사 결정 과정을 보완하여 진단을 식별하고 치료법을 추천함으로써 의사를 도울 수 있습니다. 의사는 결과를 해석하고 환자에게 권장 사항을 전달할 수 있는 능력이 필요합니다.
또한 AI는 일상적인 업무 수행에 대한 의사의 부담을 덜어줌으로써 영향을 미칠 수 있습니다[47].
음성 인식은 키보드 사용을 대체하여 정보를 입력하고 검색하는 데 도움이 될 수 있습니다[48].
의사 결정 관리는 방대한 양의 데이터를 선별하고 의사가 정보에 입각하여 의미 있는 결정을 내리는 데 도움이 될 수 있습니다[49,50].
자동화 도구는 의료 접근성 보호법과 같은 규제 요건을 관리하는 데 도움이 될 수 있으며 의사가 비용 결정을 내리기 전에 적절한 기준을 검토할 수 있도록 지원합니다[51].
마지막으로, 의료 전문가의 심각한 부족 문제를 해결하기 위해 가상 에이전트는 향후 환자 치료의 일부 측면을 지원하고 환자를 위한 신뢰할 수 있는 정보원이 될 수 있습니다[52].
AI could help physicians by amalgamating large amounts of data and complementing their decision-making process to identify diagnosis and recommend treatments. Physicians in turn need the ability to interpret the results and communicate a recommendation to the patient.
In addition, AI could have an impact by alleviating the burden from physicians for performing day-to-day tasks [47].
Speech recognitioncould help with replacing the use of keyboards to enter and retrieve information [48].
Decision managementcan help with sifting enormous amounts of data and enable the physician to make an informed and meaningful decision [49,50].
Automation toolscan help with managing regulatory requirements such as Protecting Access to Medicare Act and enable physicians to review the appropriate criteria before making a cost decision [51].
Finally, to help with the acute shortage of health care professionals, virtual agents could, in the future, help with some aspects of patient care and become a trusted source of information for patients [52].
의학교육에서의 인공 지능 교육 Artificial Intelligence Training in Medical Education
오늘날 의학교육의 현황 State of Medical Education Today
의사는 전문의가 되기까지 오랜 기간의 수련 과정을 거칩니다. 의학은 지난 수십 년 동안 큰 변화를 겪었지만, 의학교육은 여전히 전통적인 커리큘럼을 기반으로 하고 있습니다[53]. 구체적인 교육 기간은 국가마다 다르지만 이러한 커리큘럼의 핵심 역량은 전 세계적으로 유사합니다[54]. 전임상 교육의 핵심 단계 이후 교육은 대부분 실습 기반 학습을 중심으로 이루어집니다[53]. 의학교육은 환자 치료, 의학 지식, 대인관계 및 의사소통 기술, 실습 기반 학습 및 개선, 전문성, 시스템 기반 실습 등 6가지 영역을 기반으로 하는 경우가 많습니다[55]. 이러한 영역은 의학 교육 졸업 인증 위원회(ACGME)에 의해 도입되었습니다. 의료 교육의 대부분은 가능한 한 많은 정보를 소비하고 이 지식을 환자 치료에 적용하는 방법을 배우는 데 중점을 둡니다. 이 과정은 여전히 대부분 암기 위주입니다[56]. 의대생이나 레지던트들이 AI, 모바일 의료 애플리케이션, 원격 의료와 같은 새로운 기술에 익숙해지는 데 소요되는 시간은 적습니다[53,55,56]. 미국에서는 USMLE에서 이러한 주제에 대한 시험을 치르지 않습니다[57]. 그러나 2018년 미국 의학 협회(AMA) 연례 회의에서 증강 지능에 대한 AMA의 첫 번째 정책이 채택되어 의학교육에서 AI를 어떻게 다뤄야 하는지에 대한 연구가 장려된 이후 변화는 불가피한 것으로 보입니다[58]. 표 1에는 AMA에서 제시한 의학교육에 AI를 통합하기 위한 몇 가지 이니셔티브가 나와 있습니다[58].
Physicians go through extensive periods of training before they can eventually register as specialists. Although medicine has seen major changes over the last decades, medical education is still largely based on traditional curricula [53]. The specific length of training differs between countries, but the core competencies of these curricula are globally similar [54]. After a core phase of preclinical didactics, training is mostly centered around practice-based learning [53]. Medical education is often based on 6 domains: patient care, medical knowledge, interpersonal and communication skills, practice-based learning and improvement, professionalism, and systems-based practice [55]. These fields were introduced by the Accreditation Council for Graduating Medical Education (ACGME). A large part of medical training focuses on consuming as much information as possible and learning how to apply this knowledge to patient care. This process is still largely memorization based [56]. Less time is spent on familiarizing medical students or residents with new technologies such as AI, mobile health care applications, and telemedicine [53,55,56]. In the United States, USMLE does not test on these subjects [57]. However, change seems inevitable since the 2018 annual meeting of the American Medical Association (AMA) saw the adoption of AMA’s first policy on augmented intelligence, encouraging research into how AI should be addressed in medical education [58]. InTable 1, several initiatives for incorporating AI in medical education are shown, as presented by the AMA [58].
Table 1. Initiatives for artificial intelligence in medical education.
Institution
Project
Duke Institute for Health Innovation
Medical students work together with data experts to develop care-enhanced technologies made for physicians
University of Florida
Radiology residents work with a technology-based company to develop computer-aided detection for mammography
Carle Illinois College of Medicine
Offers a course by a scientist, clinical scientist, and engineer to learn about new technologies
Sharon Lund Medical Intelligence and Innovation Institute
Organizes a summer course on all new technologies in health care, open to medical students
Stanford University Center for Artificial Intelligence in Medicine and Imaging
Involves graduate and postgraduate students in solving heath care problems with the use of machine learning
University of Virginia Center for Engineering in Medicine
Involves medical students in the engineering labs to create innovative ideas in health care
AMA는 의사와 수련 중인 의사를 위한 AI 교육 모듈 개발 장려, 환자 치료에 영향을 미칠 수 있는 AI 교육 격차 해소, 의사가 AI 교육 자료 개발 및 실행에 참여하도록 보장하는 등 의학교육에 AI를 통합하기 위한 정책을 채택했습니다. 이러한 새로운 정책의 결과로 AMA는 다음과 같이 장려할 것입니다: The AMA adopted policies on integrating AI into medical education, which include encouraging the development of AI education modules for physicians and physicians-in-training, addressing disparities in AI education that could impact patient care, and ensuring that physicians are involved in the development and implementation of educational materials on AI. As a result of these new policies, the AMA will encourage:
인증 및 면허 기관은 인증 및 면허 기준에서 AI를 가장 적절하게 다루는 방법을 연구해야 합니다.
의료 전문 학회 및 이사회는 AI와 관련된 전문 분야별 교육 모듈 제작을 고려합니다.
의학교육에서 AI 교육이 학습 및 임상 결과에 미치는 효과에 관한 연구.
교육기관과 프로그램은 AI 보조 기술을 언제 가르쳐야 하는지 결정할 때 신중해야 하며, 여기에는 확립된 근거 기반 치료법을 고려하고 새로운 교육 모듈을 수용하기 위해 제거해야 할 다른 커리큘럼에 대한 고려가 포함됩니다.
이해관계자는 학습자가 AI 시스템에 내재되어 있을 수 있는 편견이 의도치 않게 전파되는 것을 방지하는 데 도움이 되는 교육 자료를 제공해야 합니다.
AI에 대한 기관별 접근성의 차이가 자원이 적고 AI 기술에 대한 접근성이 낮은 학교의 학생 교육 격차에 어떤 영향을 미칠 수 있는지에 대한 연구.
환자 치료에서 데이터의 평가, 이해 및 적용에 관한 의학교육 전반에 걸친 교육 강화.
AI 교육 자원의 격차가 자원이 부족하고 AI 기술에 대한 접근성이 낮은 지역사회의 환자들의 의료 서비스 격차에 어떤 영향을 미칠 수 있는지에 대한 연구.
교육 기관의 리더와 학장은 학습자의 AI 이해와 사용을 돕기 위해 데이터 과학자 및 엔지니어와 같은 비임상의를 교수진 명단에 포함시키는 것을 적극적으로 추진해야 합니다.
AI 애플리케이션 개발 시 임상의사와 긴밀히 협력하고 감독합니다.
Accrediting and licensing bodies to study how AI should be most appropriately addressed in accrediting and licensing standards.
Medical specialty societies and boards to consider production of specialty-specific educational modules related to AI.
Research regarding the effectiveness of AI instruction in medical education on learning and clinical outcomes.
Institutions and programs to be deliberative in the determination of when AI-assisted technologies should be taught, including consideration of established evidence-based treatments, and including consideration regarding what other curricula may need to be eliminated in order to accommodate new training modules.
Stakeholders to provide educational materials to help learners guard against inadvertent dissemination of bias that may be inherent in AI systems.
The study of how differences in institutional access to AI may impact disparities in education for students at schools with fewer resources and less access to AI technologies.
Enhanced training across the continuum of medical education regarding assessment, understanding, and application of data in the care of patients.
The study of how disparities in AI educational resources may impact health care disparities for patients in communities with fewer resources and less access to AI technologies.
Institutional leaders and academic deans to proactively accelerate the inclusion of non-clinicians, such as data scientists and engineers, onto their faculty rosters in order to assist learners in their understanding and use of AI.
Close collaboration with and oversight by practicing physicians in the development of AI applications.
의료 교육에서 종종 간과되는 또 다른 중요한 기술 관련 측면은 전자 건강 기록(EHR)을 사용하는 것입니다. EHR은 환자 안전 개선과 같은 많은 이점을 제공할 뿐만 아니라 의료 서비스에서 AI를 구현하는 데도 도움이 됩니다. AI 알고리즘은 EHR의 정보를 사용하므로 편향되지 않은 데이터를 EHR에 입력하는 방법에 대한 지식이 필수적입니다. 그렇지 않으면 AI 알고리즘도 편향될 가능성이 높습니다[59]. 현재 의대생과 의사를 대상으로 한 EHR 사용 교육은 의료 커리큘럼에 일반적으로 포함되지 않아[60], 의료 전문가가 이 기술의 진정한 잠재력을 이해하지 못한 채 종이로 정보를 캡처하는 대체 수단으로 EHR을 사용하고 있습니다[61]. EHR 사용에 대한 교육은 일반적으로 병원 시스템을 실제로 사용하기 위한 기본 기술만 가르치는 임시 임시 입문 과정으로 구성됩니다. 데이터의 품질과 컴퓨터가 환자-의사 관계에 미치는 영향에 대한 우려는 거의 다루어지지 않으며[60], USMLE에서도 이러한 주제에 대해 테스트하지 않습니다[57]. Another important technology-related aspect that is often overlooked in medical training is working with electronic health records (EHRs). EHRs have many benefits, such as improved patient safety, but also assist the implementation of AI in health care. AI algorithms use information from the EHR, and therefore, the knowledge on how to input unbiased data into the EHR is essential. Otherwise, the AI algorithm will likely be biased as well [59]. At present, training on use of EHRs for medical students and physicians is not commonly incorporated in the medical curriculum [60], resulting in the medical professional using the EHR as a replacement to capture information on paper without understanding the true potential of this technology [61]. Training on the use of EHRs usually consists of ad hoc brief introductory courses that just teach the basic skills to use the hospital’s system in practice. Quality of data and concerns on the impact of the computer on the patient-physician relationship are rarely addressed [60] and the USMLE does not test on these subjects either [57].
임상의료행위의 변화 How Clinical Practice Is Changing
의료 서비스의 급속한 디지털화로 인해 EHR은 정보에 입각한 결정을 내리는 데 사용할 수 있는 귀중한 정보를 획득하고 처리하는 새로운 방법을 촉진합니다[62]. 이러한 발전과 정보화 시대에서 AI 시대로의 전환[56]은 임상 진료와 환자 치료 결과를 더 나은 방향으로 변화시킵니다. 미래의 의사들은 데이터 관리, AI 도구 감독, 정보에 입각한 의사 결정을 내리기 위한 AI 애플리케이션 사용 등 다양한 기술과 역량을 갖춰야 할 것입니다. With the rapid digitization of health care, EHRs facilitate new ways to acquire and process valuable information that can be used to make an informed decision [62]. These advances and transitioning from an information age to the age of AI [56] change clinical practice and patient outcomes for the better. Physicians of the future will have to add to the armory of their skills and competencies, the ability to manage data, supervise AI tools, and use AI applications to make informed decisions.
의사는 이러한 도구 중 어떤 것이 환자에게 가장 적합한지 결정하는 데 중요한 역할을 하게 될 것입니다. 이는 결국 의사와 환자의 관계를 변화시킬 가능성이 높습니다[63]. 정보 처리가 주로 컴퓨터에 의해 이루어지면 의사가 환자를 돌보고 소통하는 데 더 집중할 수 있다는 점에서 의료 분야에서 AI의 주요 이점 중 하나가 부각됩니다[64]. 마지막으로, AI 시대에는 "의사는 내러티브, 기계론적, 수학적 사고를 훈련에 결합하고, 환자를 중심에 두고 질병의 생체-사회적 모델을 고려해야 한다"고 말합니다. "컴퓨터는 인간의 강점과 한계, 그리고 정보 과부하가 특징인 환경을 인식하는 자기 성찰적인 의료 전문가를 결코 대체할 수 없습니다."[65,66]. Physicians will have a crucial role in deciding which of these tools is best for their patients. In turn, this will likely change the physician-patient relationship [63]. When information processing is done mainly by computers, this highlights one of the major benefits of AI in medicine: it allows the physician to focus more on caring for and communicating with patients [64]. Finally, in the age of AI, “the physician should combine narrative, mechanistic and mathematical thinking in their training and consider the biopsycho-social model of the disease with the patient at its center.” “Computers will never substitute for self-reflective medical expert who is aware of the strengths and limitations of human beings and of an environment characterized by information overload” [65,66].
미래에는 의사에게 무엇을 요구할까요? What Will Be Asked From Physicians in the Future?
미래의 의사들은 임상에서 AI를 적절히 활용하기 위해 광범위한 기술을 필요로 할 것입니다. 의사는 의학의 원리를 이해하는 것 외에도 수학적 개념, AI 기초, 데이터 과학 및 관련 윤리적, 법적 문제에 대한 충분한 지식을 습득해야 할 것입니다. 이러한 기술은 다양한 출처의 데이터를 사용하고, AI 도구를 감독하며, 알고리즘이 예상보다 정확하지 않을 수 있는 경우를 인식하는 데 도움이 됩니다[67]. 또한, AI 기반 시스템이 환자의 신체적, 정서적 상태를 모두 고려할 수 없기 때문에 커뮤니케이션 및 리더십 기술과 감성 지능이 그 어느 때보다 중요해질 것입니다[56]. 이러한 특성은 컴퓨터가 습득하기 어렵기 때문에 AI 시대에 훌륭한 의사의 특징이 될 것입니다. Future physicians will need a broad range of skills to adequately use AI in clinical practice. Besides understanding the principles of medicine, physicians will also need to acquire satisfactory knowledge of mathematical concepts, AI fundamentals, data science, and corresponding ethical and legal issues. These skills will help them to use data from a broad array of sources, supervise AI tools, and recognize cases where algorithms might not be as accurate as expected [67]. Furthermore, communication and leadership skills as well as emotional intelligence will be more important than ever as AI-based systems will not be able to consider all the physical and emotional states of the patient [56]. These traits are hard to master for computers and will characterize a great physician in the age of AI.
실용적인 고려 사항 Practical Considerations
의료 정보를 암기하는 데 소요되던 시간 중 일부는 이제 다른 기술에 투자해야 할 것입니다. 이는 학생과 레지던트가 수련을 경험하는 방식에 큰 영향을 미칠 것입니다. 더 이상 사실적 지식이 아닌 의사소통 능력, 감성 지능, 컴퓨터 사용법에 대한 지식으로 역량을 판단하는 방식으로 시스템이 바뀌어야 합니다. Some of the time that was originally spent on memorizing medical information will now have to be devoted to other skills. This will have a major impact on the way students and residents will experience their training. The system has to change in such a way that competence will no longer be judged based on factual knowledge but rather on communication skills, emotional intelligence, and knowledge on how to use computers.
2016년 AMA의 설문조사에 따르면 의사의 85%가 새로운 디지털 도구의 이점을 인식하고 있지만[58], 커리큘럼이 지나치게 많기 때문에 새로운 주제를 채택하는 데 관심이 제한되어 있습니다[68]. AI 중심 교육을 의료 커리큘럼에 통합하는 것은 기술이 발전함에 따라 시간이 걸릴 것입니다. 학습을 위한 새로운 인프라를 도입해야 하며 컴퓨터 과학, 수학, 민족지학, 경제학 등의 분야에서 새로운 교육자를 채용해야 합니다. 현재 이러한 과목은 ACGME의 핵심 역량에 포함되지도 않지만 이러한 역량은 "변화하는 지식에 적응할 수 있을 만큼 충분히 견고합니다"[69]. With an overfull curriculum, there is limited interest in adopting new topics [68], although a 2016 survey by AMA shows that 85% of physicians perceive benefits from new digital tools [58]. The integration of AI-oriented education into the medical curriculum will take time as the technology evolves. A new infrastructure for learning has to be introduced, and new educators from disciplines such as computer sciences, mathematics, ethnography, and economics will need to be hired. At the moment, these subjects are not even covered by the core competencies of ACGME, but these competencies “are robust enough to adapt to changing knowledge” [69].
커리큘럼의 변화를 이루기 위해서는 많은 정치적, 관료적 장애물을 극복해야 합니다. 새로운 학습 성과를 창출하기 위해서는 교육 시스템, 프로그램 구조, 목표가 바뀌어야 합니다[70]. 변화는 많은 양의 증거가 생성될 때만 실행될 수 있습니다. 우리는 아직 인공지능을 위한 변화를 구현할 단계에 이르지 못했습니다. 또한 의학 내 다른 많은 분야에서도 마땅히 받아야 할 관심을 받지 못했다고 주장합니다[71,72]. AI는 그 이점을 증명해야 하며, 현재 적절한 의학 교육이 부족한 다른 중요한 과목보다 의학 커리큘럼의 중요한 주제라는 점을 정당화해야 합니다. To achieve a change in curriculum, many political and bureaucratic hurdles have to be overcome.Educational systems, program structures,andobjectiveshave to change to create new learning outcomes [70]. A change can only be implemented when large amount of evidence is generated. We have not reached that stage of implementing changes for AI. Furthermore, many other fields within medicine argue that they have not received the attention they deserve [71,72]. AI needs to prove its benefits and also justify that it is an important topic for medical curriculum over other important subjects that lack adequate medical training at present.
그러나 의학교육에서 AI 교육을 실시해야 한다는 가장 설득력 있는 주장 중 하나는 이 교육이 기존 교과 과정을 대체하기보다는 기존 교과 과정을 보강할 수 있다는 것입니다. 학생들이 AI 도구 사용법을 교육받을 때는 도구 사용법에 대한 기본 지식을 습득하는 것에서 기본 원리에 대한 기본적인 이해로 초점을 옮겨야 합니다. 이렇게 하면 학생들은 현재 도구가 구식이 되고 새로운 도구가 도입되었을 때 이러한 기본 지식을 활용할 수 있습니다. However, one of the most compelling arguments for the implementation of AI training in medical education is that this training will augment existing curriculum rather than replace existing coursework. When students are trained to use AI tools, focus should shift from acquiring basic knowledge on how to use the tool to a basic understanding of the underlying principles. This will enable the students to use this fundamental knowledge when current tools get outdated and new tools are introduced.
또 다른 현실적인 문제는 기존의 의료 교육이 주로 주치의와 레지던트 또는 의대생 간의 상호작용을 중심으로 이루어졌다는 점입니다. AI가 임상 진료에 점점 더 많이 도입되면 문제가 될 수 있습니다. 많은 시니어 의사들은 AI에 대한 경험이 거의 없거나 전혀 없습니다. AI 교육은 평생 의학 교육(CME) 프로그램을 통해 제공될 수 있으며, 의료계 외부의 교육자에게도 교육을 받아야 할 수 있습니다. 예를 들어, AI와 임상 진료의 미래에 관한 2학점짜리 CME 과정은 전산 생물학자와 비즈니스 경제학자가 제공합니다[73]. Another practical problem is that traditional medical training revolves mainly around the interactions between an attending physician and the residents or medical students. When AI is increasingly introduced into clinical practice, this could be problematic. Many senior physicians have little to no experience with AI. AI training could be delivered via Continuing Medical Education (CME) programs and might need to be also taught by educators from outside the medical community. For example, a 2-credit CME course on AI and the Future of Clinical Practice is delivered by a computational biologist and business economists [73].
권장 사항 Recommendations
프레임워크 Framework
암기 위주의 전통적인 의학 커리큘럼은 정보화 시대에서 AI 시대로의 전환을 따라야 합니다. 미래의 의사들은 점점 더 다양한 출처의 정보를 효과적으로 통합하고 활용할 수 있는 역량을 배워야 합니다[56]. 이러한 지식을 의학에 포함시키기 위해서는 교육 초기부터 이러한 개념을 도입하는 것이 필수적입니다. 많은 국가에서 의과대학에 입학하기 위해서는 의과대학 입학시험(MCAT)을 치러야 합니다. 예를 들어, 현재 미국 MCAT 시험은 생물학, 화학, 물리학, 심리학, 사회학 및 추론에 중점을 둡니다 [78]. 이러한 시험은 선형 대수 및 미적분의 기초와 같은 수학적 개념에 대한 테스트를 시작할 수 있습니다. 이러한 개념은 AI에 대한 기초적인 이해에 필수적이며 나머지 커리큘럼의 분위기를 조성합니다. The traditional medical curriculum, which is mostly memorization based, must follow the transition from the information age to the age of AI. Future physicians have to be taughtcompetence in the effective integration and utilization of information from a growing array of sources[56]. To embed this knowledge into medicine, it is of the essence to start introducing these concepts from the beginning of training. In many countries, a Medical College Admission Test (MCAT) has to be taken to be admitted into medical school. The current US MCAT exam, for example, focuses on biology, chemistry, physics, psychology, sociology, and reasoning [78]. These exams could start testing on mathematical concepts such as basis of linear algebra and calculus. These concepts are vital to the elementary understanding of AI and will set the tone for the rest of the curriculum.
전임상 교육 과정의 핵심 단계에서는 의료 데이터 큐레이션 및 품질[79], 출처[80], 통합[81], 거버넌스, EHR[60], AI 기초, AI의 윤리 및 법적 문제[82,83]를 다루는 데 시간을 할애해야 합니다. AI 및 로봇 기술에 대한 비판적 평가와 통계적 해석에 대한 교과목도 중요합니다[84].
첫째, 이러한 과목은 현재 응용 프로그램이 구식이 된 후에도 사용할 수있는 이러한 과목의 기초에 대해 가르치기 위해 독립된 과정으로 가르 칠 수 있습니다 [68]. 이러한 독립적인 과목은 현재 커리큘럼에서 의료 정보학 및 통계학 과목을 대체하고 보완할 수 있습니다.
둘째, 임상 과정에서도 반복하여 학생들이 AI의 임상 적용에 익숙해지고 다양한 환경에서 EHR과 함께 작업할 수 있도록 해야 합니다[68].
In the core phase of preclinical didactics, time should be devoted to working with health data curation and quality [79], provenance [80], integration [81], and governance, working with EHRs [60], AI fundamentals, and ethics and legal issues with AI [82,83]. Course work in critical appraisal and statistical interpretation of AI and robotic technologies is also important [84].
First, these subjects could be taught in self-contained courses to teach about the fundamentals of these subjects that can be used even after current applications become outdated [68]. These self-contained courses could potentially replace and augment courses on medical informatics and statistics in the current curriculum.
Second, they should also recur in clinical courses to familiarize students with the clinical applications of AI and work with EHRs in diverse settings [68].
AI를 도입하는 한 가지 접근 방식은 근거 기반 의학[85]과 같은 과목에서 이 기술을 통합하는 것입니다. 학생은 PubMed와 같은 데이터베이스나 진단 테스트 또는 체계적 문헌고찰을 통해 증거를 평가하는 방법을 배우게 되는데, 이 과정은 데이터 과학의 개념을 적용하고 NLP와 같은 AI 기술을 적용하고 시나리오를 분석하여 윤리 및 책임 문제에 대해 테스트함으로써 강화될 수 있습니다[86]. 또한, 학생들은 컴퓨터 및 소프트웨어 공학의 기초에 대한 교육을 받아 실제 AI 애플리케이션의 의미를 이해해야 합니다. 예를 들어, 하드웨어 및 소프트웨어 개발과 사용자 경험 설계의 기초도 유용할 수 있습니다. An approach to introducing AI could be to incorporate this technology during courses such as Evidence Based Medicine [85]. As the student is taught to appraise evidence through databases such as PubMed or diagnostic tests or systematic reviews, this process could be augmented by applying concepts from data sciences, applying AI technologies such as NLP and analyzing scenarios to test them on questions of ethics and liability [86]. In addition, the students should also be trained in the fundamentals of computer and software engineering to understand the semantics behind real-world AI applications. For example, basics of hardware and software development and user experience design may also be valuable.
임상 로테이션과 레지던트 기간 동안에는 AI를 실제로 적용하는 데 초점을 맞춰야 합니다. 디지털 바이오마커[87]와 디지털 치료법[88]이 발전함에 따라 학생들도 AI에 의존하는 이러한 기술에 대한 교육을 받아야 합니다. 이러한 기술은 가까운 미래에 가정 내 환경에서 대규모 진단과 치료를 가능하게 할 잠재력을 가지고 있습니다[89]. 교육이 끝나면 USMLE는 최종 시험에 데이터 과학 및 AI 기초에 관한 상당수의 문제를 포함시켜야 합니다. 의료 전문가들이 최신 개발 동향을 파악할 수 있도록 의료 AI 관련 컨퍼런스에 참석하도록 인센티브를 제공할 수 있습니다. 참석하는 의사를 위해 AI 및 데이터 과학에 대한 광범위한 과정이 CME의 일부가 되어야 합니다. 자세한 내용은 표 2를 참조하십시오.
During clinical rotations and residency, focus should shift toward relevant applications of AI in practice. With advancements in digital biomarkers [87] and digital therapeutics [88], students should also be trained in these technologies as they rely on AI. They have the potential to enable large-scale diagnostics and treatments in in-home environments in the near future [89]. At the end of training, the USMLE should include a substantial number of questions on data science and AI fundamentals in their final exams. Attendance of conferences on health care AI could be incentivized, so that health care professionals stay up-to-date with the latest developments. For attending physicians, extensive courses on AI and data science should be part of CME. SeeTable 2for more details.
Table 2. List of Continuing Medical Education programs on artificial intelligence in health care.
Program
Faculty; organization
Number of Continuing Medical Education credits
Artificial Intelligence and the Future of Clinical Practice [73]
Computational biologist, Business economist; Massachusetts Medical Society
2.0
Intro to AI and Machine Learning: Why All the Buzz [74]
Medical Informatics, Radiology; The Radiological Society of North America
1.0
Current Applications and Future of Cardiology [75]
Healthcare Technologists, Bioinformatics, Cardiology; Mayo Clinic
10.0
Artificial Intelligence and Machine Learning: Application in the Care of Children [76]
Pediatric Medicine; University of Pittsburgh School of Medicine
1.0
Artificial Intelligence in Healthcare: The Hope, The Hype, The Promise, The Peril [77]
Medical Informatics, Business Administration; Stanford University School of Medicine
6.0
보다 균형 잡힌 미래의 의사를 양성하기 위해 AI 기술은 비분석 및 사람 중심의 의료 측면과도 균형을 이루어야 합니다. 의사 소통, 공감, 공동 의사 결정, 리더십, 팀 구축, 창의성과 같은 다른 기술도 의사에게 계속 중요해질 기술입니다. 텍사스 대학교 오스틴 캠퍼스의 Dell 의과 대학에서는 리더십, 창의성, 커뮤니케이션과 같은 소프트 스킬 교육에 집중하기 위해 기초 과학 커리큘럼의 기간을 단축했습니다[63]. AI skills must also be balanced with nonanalytics and person-centered aspects of medicine to develop a more rounded doctor of the future. Other skills such ascommunications, empathy, shared decision making, leadership, team building, and creativity are all skills that will continue to gain importance for physicians. At the Dell Medical School at the University of Texas, Austin, the curriculum in basic sciences has been reduced in duration to accommodate training in soft skills such as leadership, creativity, and communication [63].
임상의가 혁신적으로 사고하고 기술 기반 치료 모델을 만들 수 있도록 하려면 구현 과학, 운영 및 임상 정보학에 대한 다학제적 교육이 필요합니다. 스탠포드 의과대학은 대학원 의학교육에 인간 중심의 설계 접근 방식을 도입하여 디지털 미래를 위한 임상의사 혁신가를 양성하는 프로그램을 만들었습니다[90]. 보스턴 매사추세츠 종합병원의 헬스케어 혁신 연구소에서는 레지던트 수련생에게 데이터 과학, 머신러닝, 의료 운영, 서비스, 디자인 사고, 지적 재산권, 기업가 정신 등의 주제를 다루는 의료 혁신 분야의 1년 펠로우십을 제공합니다[91]. 이러한 프로젝트는 새로운 개발이며 의학교육에 AI를 도입하기 위해 취한 첫 번째 단계입니다. To enable clinicians to think innovatively and create technology-enabled care models, multidisciplinary training is needed in implementation science, operations, and clinical informatics. The Stanford medical school has created such a program to train clinician-innovators for the digital future by introducing a human-centered design approach to graduate medical education [90]. At the Healthcare Transformation Laboratory at Massachusetts General Hospital in Boston, a 1-year fellowship is offered in health care innovation exposing resident trainees to topics in data sciences, machine learning, health care operations, services, design thinking, intellectual property, and entrepreneurship [91]. These projects are new developments and are the first steps taken to introduce AI in medical education.
첫 단계 First Steps
이러한 모든 개입을 동시에 도입할 수는 없으므로 향후 몇 년 동안의 토대를 마련할 몇 가지 첫 단계를 제안합니다. 먼저 의학전문대학원입학자격시험의 수학 영역과 유사한 수학적 개념에 관한 문제를 MCAT에 도입하는 것부터 시작할 것을 제안합니다. 의학교육의 핵심 단계에서 데이터 과학 및 AI 기초에 대한 고품질 웹 기반 강좌를 자유롭게 제공해야 합니다. 이를 통해 학생들은 다음 수련 과정에서 자연스럽게 이러한 과목을 응용하는 데 집중할 수 있습니다. As not all of these interventions can be introduced simultaneously, we suggest a few first steps that will lay the foundation for the upcoming years. We suggest to start off by introducing questions on mathematical concepts into the MCAT similar to the mathematics section in the Graduate Record Examination. High quality Web-based courses on data sciences and AI fundamentals should be freely offered in the core phase of medical education. This might lead to students focusing on applications of these subjects more naturally in following years of training.
이미 이 교육 단계를 마친 레지던트와 의대생에게는 남은 의학교육 기간 동안 기초 과목에 대한 강좌가 제공되고 필수로 이수해야 합니다. 새로운 기술을 활용한 진료 모델을 만드는 데 관심이 있는 학생의 경우,임상 기간 중 또는 레지던트 졸업 후 갭이어 기간 동안 의료 혁신에 대한 전문 교육을 받을 수 있도록 장려해야 합니다. 현직 의사를 위한 입문 과정과 재교육 과정도 제공되어야 합니다. 특히 이 그룹은 향후 의대생과 레지던트에게 이러한 주제에 대해 교육하는 임무를 부분적으로 다시 맡을 수 있도록 광범위한 교육이 필요합니다. 표 3에는 의학교육의 다양한 단계에 추가할 수 있는 권장 콘텐츠가 나열되어 있습니다. 표 4에는 의사와 수련의가 이 기술과 의료 분야에서의 적용에 대해 자세히 알아보기 위해 참석할 수 있는 의료 컨퍼런스에서 빠르게 진화하는 AI의 일부가 나열되어 있습니다. For residents and medical students who have already finished this phase of training, courses on the fundamental subjects should be available and mandatory throughout the remaining part of their medical education. For students interested in creating new technology-enabled care models, dedicated training in health care innovation during a gap year during the clinical years or after residency should be encouraged. For attending physicians, introductory courses and refresher courses should also be made available. Extensive training is especially necessary for this group so that they can partly take back the task of educating medical students and residents on these subjects in the future.Table 3lists suggested content that can be added to the various phases of medical education.Table 4lists a small subset of rapidly evolving AI in health care conferences that physicians and trainees can attend to learn more about this technology and its applications in health care.
결론 Conclusions
의사와 기계의 협업은 임상 의사 결정과 환자 건강 결과를 개선할 수 있는 가장 큰 잠재력을 가지고 있습니다[114]. AI는 의료 기록, 유전자 보고서, 약국 기록, 환경 데이터 등 더 많은 데이터를 큐레이션하고 처리하여 더 많은 의료 정보를 보유, 액세스, 분석할 수 있습니다. 그러나 돌봄의 기술을 대체할 수는 없습니다. AI와 그 응용이 의료 분야에서 주류가 되면서 의대생, 레지던트, 펠로우, 개업의는 AI, 데이터 과학, EHR 기본 사항, AI와 관련된 윤리 및 법적 문제에 대한 지식을 갖춰야 합니다. 의과대학은 이러한 내용을 커리큘럼의 일부로 포함시켜야 합니다. 의대생이 의사가 되기까지 단계적으로 교육하는 것이 좋습니다. Physicians and machines working in combination have the greatest potential to improve clinical decision making and patient health outcomes [114]. AI can curate and process more data such as medical records, genetic reports, pharmacy notes, and environment data and in turn retain, access, and analyze more medical information. However, it cannot replace the art of caring. As AI and its application become mainstream in health care, medical students, residents, fellows, and practicing physicians need to have knowledge of AI, data sciences, EHR fundamentals, and ethics and legal issues concerning AI. Medical schools will need to include them as part of the curriculum. A staged approach to educating the medical student through their journey is recommended.
AI는 더 빠르고 정확한 진단을 가능하게 하고, 영상의학을 보강하며, 인간의 피로로 인한 오류를 줄이고, 의료 비용을 절감하며, 지루하고 반복적이며 노동 집약적인 작업을 보조 및 대체하고, 최소 침습 수술을 가능하게 하며, 사망률을 감소시킬 것입니다. AI will enable faster and accurate diagnosis, augment radiology, reduce errors due to human fatigue, decrease medical costs, assist and replace dull, repetitive, and labor-intensive tasks, minimally invasive surgery, and reduce mortality rates.
2022년까지 전 세계 의료비 지출이 미화 10조 달러에 달할 것으로 예상되는 가운데, AI는 환자 경험 향상, 인구 건강 개선, 비용 절감, 의료진 경험 개선이라는 의료 분야의 네 가지 목표를 달성할 수 있는 귀중한 잠재력을 가지고 있습니다[115,116]. With the global health care expenditure projected to reach US $10 trillion by 2022, AI has the invaluable potential to advance the quadruple aim in health care—enhance the patient experience, improve population health, reduce costs, and improve the provider experience [115,116].
JMIR Med Educ. 2019 Dec 3;5(2):e16048.doi: 10.2196/16048.
Introducing Artificial Intelligence Training in Medical Education
Health care is evolving and with it the need to reform medical education. As the practice of medicine enters the age of artificial intelligence (AI), the use of data to improve clinical decision making will grow, pushing the need for skillful medicine-machine interaction. As the rate of medical knowledge grows, technologies such as AI are needed to enable health care professionals to effectively use this knowledge to practice medicine. Medical professionals need to be adequately trained in this new technology, its advantages to improve cost, quality, and access to health care, and its shortfalls such as transparency and liability. AI needs to be seamlessly integrated across different aspects of the curriculum. In this paper, we have addressed the state of medical education at present and have recommended a framework on how to evolve the medical education curriculum to include AI.
Keywords:algorithm; artificial intelligence; black box; continuing education; curriculum; data sciences; deep learning; machine learning; medical education.
인공지능이 의학교육에 갖는 함의 (Lancet Digit Health.2020) Implications of artificial intelligence for medical education
Vanessa Rampton 1, Michael Mittelman 2, Jörg Goldhahn 3
디지털 헬스1는 의학에 큰 변화를 가져왔지만, 이로 인해 야기되는 문제는 아직 의학교육 전반에 걸쳐 교육과 학습에 통합되지 않았습니다. 이 문제는 의료 디지털화의 구체적인 사례로 논의되는 인공지능(AI) 시스템의 부상이 교육의 근본적인 패러다임 변화와 연관되어 있다는 점에서 더욱 시급한 문제입니다. 20세기 의학교육 모델은 실험 결과가 공인된 표준으로 발전하여 교과서 교육에 영향을 미치는 것에 의존했지만, 오늘날에는 더 이상 이러한 순서가 적용되지 않습니다. 새로운 의료 AI 기술이 개발되고, 임상에 도입되고, 환자들이 사용하는 속도가 빨라지면서 의사들은 아직 일반적으로 받아들여지는 지식의 일부가 되지 않은 실험 기법을 적절히 다룰 수 있는 역량을 갖춰야 합니다. 어떤 치료법이 환자에게 가장 큰 혜택을 줄 수 있는지에 대한 민첩한 교육과 교육받은 추측이 의사들이 [단순히 기술에 반응하지 않고 이러한 기술의 도입을 주도할 수 있도록] 하는 데 매우 중요합니다. Although digital health1 has occasioned huge changes for medicine, the issues it provokes have yet to be integrated into teaching and learning across the medical education continuum. This question is all the more pressing given that the rise of artificial intelligence (AI) systems, discussed here as a specific example of healthcare's digitalisation, are associated with a fundamental paradigm shift in teaching. Whereas 20th-century medical education models relied on experimental results evolving into a recognised standard that then informed textbook teaching, today this sequencing no longer holds. The speed at which new health AI technologies are developing, being introduced into clinical practice, and being used by patients requires equipping doctors to deal appropriately with experimental techniques that have not yet become part of a generally accepted body of knowledge. Agile teaching and educated guesswork about which treatments will benefit patients the most are crucial for enabling physicians to lead the introduction of such technologies without simply being forced to react to them.
당면 과제 중 하나는 기존의 교육 프레임워크를 21세기 현실을 고려하여 현실적으로 업데이트할 수 있는 방법을 모색하는 것입니다. 일반적으로 의학교육자들은 역량 프레임워크를 사용하는데, 이 프레임워크에는 여러 가지 경쟁 모델이 존재하며, 이 중 한 가지 역량은 여러 전문적 역할을 적절히 수행할 수 있는 것으로 간주될 수 있습니다. 엘러웨이에 따르면 이러한 프레임워크는 "이상을 집합적으로 정의하는 일련의 명제와 관계"를 설명하는 이론으로 간주하므로 지속적으로 테스트하고 도전해야 한다고 생각합니다.2 오늘날 의사가 환자의 의료 요구를 적절히 충족하는 데 필요한 다양한 능력은 모두 AI 지원 시스템의 영향을 받습니다.3 Part of the task at hand is to ask how existing educational frameworks can be realistically updated to take into account 21st-century realities. As a rule, medical educators work with competency frameworks, of which several competing models exist, whereby a competence can be considered the suitable performance of several professional roles. Following Ellaway, we view such frameworks as theories outlining “a series of propositions and relationships that collectively define an ideal”, and therefore consider that they must be continuously tested and challenged.2 Today, the various abilities that physicians require to adequately meet patients' health-care needs are all affected by AI-enabled systems.3
기술이 앞으로 어떻게 발전할지는 아무도 예측할 수 없지만, 의학은 환자의 웰빙을 증진하고 모든 사람이 적절한 의료 서비스를 이용할 수 있도록 하는 등 [인류 공통의 요구]에 부응합니다.4 한편, 우리는 환자가 자신의 치료와 관련하여 무엇을 원하고 필요로 하는지, 그리고 환자의 선호도가 의학 교육에 어떻게 더 잘 통합될 수 있는지 잘 파악하고 있습니다. 일부 환자 옹호자들이 쓴 것처럼, 여기에는 의학교육자가 환자를 완전한 가치의 파트너로 간주하는 것뿐만 아니라 "의사가 환자가 겪고 있는 일에 진정으로 관심을 갖고 진정으로 돕고 싶어 한다는 것을 느끼는 것"과 "환자의 가치, 희망, 선호도를 완전히 맥락화하고 이해할 수 있는 능력"이 포함됩니다. 5 치료가 환자와 그 가족이 치료에 중요한 역할을 하는 파트너십으로 진화함에 따라 의사는 환자와 협력하여 환자와의 관계를 발전시키고 이해해야 하며, 이는 매우 다양할 수 있는 AI 및 빅 데이터와의 관계를 발전시켜야 합니다. 또한 다양한 배경을 가진 환자와 협력하여 사회 정의 문제와 전문가 시스템 중심의 솔루션에 대한 민감성을 개발해야 합니다. No one can predict the future ways in which technology will develop, but medicine serves common human needs, such as promoting patient well-being and making adequate health care available to all.4 Meanwhile, we have a good picture of what patients want and need with regard to their own care, and how their preferences could be better integrated into medical education. As some patient advocates have written, this includes being considered full-value partners by medical educators, as well as “sensing that your doctor truly cares about what you are going through, and really does want to help”, and has the ability to “fully contextualise and appreciate the patient's values, wishes, and preferences”.5 As care has evolved to become more of a partnership, in which patients and their families have a key role to play in their treatment, physicians ought to collaborate with patients to develop and understand the patient's own relationship with AI and big data, which can vary dramatically. Moreover, they must work with patients from different backgrounds to develop sensitivities to problems of social justice and expert systems-driven solutions.
존경받고 널리 사용되는 도구 중 하나인 캐나다 전문의 의학교육 지침(CanMEDS) 의사 역량 프레임워크는 변화를 위한 실용적이고 효과적인 지렛대라는 장점이 있습니다.6 또한, CanMEDS에 묘사된 많은 역할이 미국의 의학전문대학원 교육 인증위원회(ACGME)와 같은 다른 프레임워크에서 재현되고 있어 우리가 관찰하는 것이 더 중요하다는 것을 강조합니다. 또한 의사소통자, 협력자, 리더, 건강 옹호자, 학자, 전문가, 의료 전문가 등 의사의 역할은 정의상 비기술적non-technical이며, 합리적이거나 객관적인 기준으로 환원할 수 없기not reducible to rational or objective criteria 때문에 [기계에 의해 (완전히) 대체될 위험이 없다는 점]에서 CanMEDS는 매력적인 이론적 프레임워크입니다. 이 중 6개는 개념적으로 사회과학과 인문학에 기반을 두고 있으며, 의료 전문가의 역할은 나머지 6개, 즉 연결성과 함께 속한 것에 대한 지식을 통합하는 것으로, 기계는 부분적으로만 수행할 가능성이 높습니다.7 By way of illustration, take one respected and widely used instrument, the Canadian Medical Education Directives for Specialists (CanMEDS) Physician Competency Framework, which has the advantage of being a practical and effective lever for change.6 Moreover, many of the roles depicted in CanMEDS are reproduced in other frameworks, such as the Accreditation Council for Graduate Medical Education (ACGME) in the USA, which underscores the broader importance of our observations. CanMEDS is also an appealing theoretical framework because none of the physician roles it describes—communicator, collaborator, leader, health advocate, scholar, professional, and medical expert—are at risk of being (entirely) replaced by machines, because they are non-technical by definition, and not reducible to rational or objective criteria. Of the roles, six are conceptually based in the social sciences and humanities, and the role of medical expert is to integrate the remaining six, that is to have knowledge of connectedness and what belongs together, something machines are likely to accomplish only partially.7
동시에 AI가 가져온 변화는 모든 의사의 역할에 영향을 미칩니다.8 At the same time, changes brought about by AI affect all physicians' roles.8
의사 소통자의 역할과 전통적인 의사와 환자의 만남이"컴퓨터를 진료실에 도입함으로써 삼자 관계로 바뀌었다"는 사실을 고려하십시오.9 의사는 개인 정보 보호에 대한 우려, 권한 박탈, 모든 것을 알고 싶은 욕구 부족을 포함하여 빅 데이터 및 AI 지원 대상에 대한 환자의 다양한 반응을 인정해야 합니다. Take the role of communicator, and the fact that the traditional physician–patient encounter has “been altered into a triadic relationship by introducing the computer into the examination room”.9 Physicians need to acknowledge the large variety of patients' responses to big data and AI-supported objects, including concerns regarding privacy, disempowerment, and a lack of desire to know everything
협력자로서 의사는 의료 AI 기술과 지식의 폭넓은 접근성이 다른 의료 전문직(예: 심리학자, 물리치료사, 간호사)은 물론 환자들에게도 힘을 실어준다empowers는 사실을 받아들이고 이를 바탕으로 배타적 지식 보유자로서의 의사의 기존 지위에 의문을 제기하도록 교육받아야 합니다. As a collaborator, physicians should be taught to accept and build on the fact that health AI technology and the wider accessibility of knowledge empowers some other health professions (eg, psychologists, physiotherapists, and nurses), as well as patients themselves, questioning physicians' previous status as holders of exclusive knowledge.
리더로서 의사는 환자와 협력하여 AI 기술을 투명하고 책임감 있게 구현하고, 디지털 기술을 개발하고 옹호하는 것에 대해 상업적 및 기타 이해관계를 명확히 하는 문화에 기여해야 합니다. As a leader, physicians must work with patients to make the implementation of AI technologies transparent and accountable, contributing to a culture that makes explicit the commercial and other interests of those developing and advocating for digital technologies.
건강 옹호자로서 의사는 환자 및 취약 계층과 협력하여 로봇 간병인과 같은 전문가 시스템의 사용이 권한이 부여된 선택인지 아니면 더 광범위한 사회경제적 접근 문제와 관련이 있는지를 확인할 수 있습니다. 이러한 환경에서 보다 다양한 팀을 옹호함으로써 교육과 임상 실습을 개선해야 하며, 이러한 팀은 AI 솔루션이 더 큰 시스템적 문제를 가리는 사례를 더 잘 식별할 수 있기 때문입니다. As a health advocate, physicians can work with patients and disadvantaged groups to establish whether the use of expert systems—such as robot carers—is an empowered choice or rather related to broader socioeconomic access problems. They ought to improve education and clinical practice by advocating for more diverse teams in those settings, as these are better able to identify instances in which AI solutions mask larger systemic problems.
학자로서 의사는 디지털 리터러시 향상과 AI, 수학적 모델링, 의사 결정 이론 등에 대한 지속적인 학습을 통해 이점을 얻을 수 있습니다. 이는 데이터의 편향성에 대한 인식, 그리고 이러한 편향성이 AI 모델이 객관적이고 중립적인 결과를 도출할 수 있다는 주장을 어떻게 약화시키는지에 대한 인식과 관련이 있습니다. 의사는 질병의 주관적인 측면을 포함하여 다양한 현실과 지식의 종류를 더 잘 이해하기 위해 환자 학자들의 연구를 활용해야 합니다. As a scholar, physicians will benefit from improved digital literacy and continuous learning about AI, mathematical modelling, decision theory, and so on. This is linked to an awareness of biases in data, and how these undermine any claims about how AI models are able to produce objective, neutral results. They should draw on the work of patient scholars to understand better different realities and kinds of knowledge, including the subjective aspect of illness.
전문직으로서 의사는 공학, 데이터 및 정보 과학의 도구를 자신의 기술에 통합해야 하는 직업 정체성의 근본적인 변화를 받아들여야 합니다. 한편, 의사는 e헬스 진료가 환자에게 도움이 되는지 여부에 대한 최종 결정권은 환자에게 있으며, 의사는 환자의 결정을 지원하는 데 필요한 지침과 조언을 제공할 책임이 있다는 점도 인정해야 합니다. As a professional, physicians should accept a fundamental change in professional identity which requires them to incorporate tools from engineering, data, and information sciences into their skill sets. Meanwhile, physicians should also acknowledge that patients have the final say in whether an eHealth practice benefits them, whereas physicians have a responsibility to provide the necessary guidance and advice to support patients' decisions.
의료 전문가로서 의사는 환자와 협력하여 통합 지식의 중요성, 즉 함께 속한 것, 사회적 관계, 질병이 환자의 삶과 어떻게 관련되어 있는지에 대한 (기계가 접근할 수 없는) 지식을 창출하고 해석할 수 있어야 합니다.10 As medical experts, physicians must be able to work together with patients to create and translate the importance of integrated knowledge, that is knowledge of what belongs together, social relationships, and how illness relates to a patient's life, something that is inaccessible to machines.10
AI 의료 기술의 급증으로 가장 큰 혜택을 받는 것은 환자임을 확인하는 것은 앞으로 몇 년 동안 핵심 과제로 남을 것이며, 의사의 디지털 리터러시를 개선하고 환자의 관점을 더 잘 통합하는 의학교육의 새로운 접근 방식이 중요해질 것입니다. AI 기반 혁신에는 일반적으로 느리고 점진적으로 임상 진료에 대한 근거 기반의 표준을 생성하는 기존 모델을 뛰어넘는 것이 포함되기 때문에 이러한 접근 방식이 더욱 필요합니다. 즉, 환자의 희망사항은 AI 기술이 환자의 건강과 웰빙에 어떻게 기여할지 예측하는 데 중요한 척도가 됩니다. Making sure that it is patients who benefit the most from the surge of AI health technology will remain a key challenge in years to come, and new approaches in medical education that improve the digital literacy of physicians and better integrate patients' views will be crucial. This is all the more necessary since AI-driven transformations involve going beyond previously accepted models of the usually slow and gradual process of generating evidence-based gold standards for clinical practice. In turn, this means that patients' wishes are a crucial measure for anticipating how AI technologies contribute to their health and well-being.
1McGill University, Institute for Health and Social Policy & Department of Philosophy, Montreal, Quebec H3A 1A3, Canada. Electronic address: vanessa.rampton@mcgill.ca.
2American Living Organ Donor Fund, Philadelphia, PA 19103, USA.
3Institute for Translational Medicine, ETH Zurich, Switzerland.
의학교육은 정보시대에서 인공지능시대로 옮겨가야 한다(Acad Med, 2018) Medical Education Must Move From the Information Age to the Age of Artificial Intelligence Steven A. Wartman, MD, PhD, and C. Donald Combs, PhD
윌리엄 오슬러는 의학은 불확실성의 과학이자 확률의 예술이라고 말한 것으로 알려져 있습니다. 하지만 오늘날 이 오랜 관점은 도전받지는 않더라도 개선되고 있습니다. 의료계의 변화하는 모습과 의사들이 현대 의료 현장에 보다 효과적으로 진입할 수 있도록 하는 의학교육 개혁은 백서와 뉴스 기사에서 자주 등장하는 주제입니다. 일반적인 개혁 주제에는 커뮤니케이션, 팀워크, 위험 관리 및 환자 안전에 대한 새로운 강조가 포함됩니다. 이러한 개혁은 중요하지만 충분하지 않다고 생각합니다. 가장 근본적인 변화, 즉 정보화 시대에서 인공지능 시대로 빠르게 전환되고 있는 의료계의 현실을 해결하는 데 더 많은 관심을 기울여야 합니다. 이러한 변화의 결과는 심대하며 학부 의학교육 프로그램의 개혁을 요구합니다. 이러한 개편의 기본 원칙은 학생들이 "정보"와 "인공 지능"의 차이를 이해하고 관리해야 한다는 것입니다. William Osler is reported to have said that medicine is a science of uncertainty and an art of probability. Yet today, this time-honored perspective is being refined, if not challenged. The changing state of the medical profession and the medical education reforms that will enable physicians to more effectively enter contemporary practice are frequent topics of white papers and news stories. Common reform themes include a renewed emphasis on communication, teamwork, risk management, and patient safety. We believe that these reforms are important but insufficient. More attention needs to be given to addressing the most fundamental change of all—the practice of medicine is rapidly transitioning from the information age to the age of artificial intelligence. The consequences of this transition are profound and demand the reformulation of undergraduate medical education programs. A fundamental principle of this reformulation is that students must understand and manage the difference between “information” and “artificial intelligence.”
정보 대 인공 지능 Information Versus Artificial Intelligence
정보 시대(대략 1970년대부터 2010년대 기계 학습 도구가 등장하기 전까지)에는 정확하고 시의적절하며, 목적에 맞게 구체적이고 체계적으로 정리되고, 의미와 관련성을 부여하는 맥락 내에서 제시된 데이터를 사용하여 이해도를 높이고 불확실성을 줄이는 것이 특징이었습니다.1 이 시기 의사의 주요 과제는 [유효성을 판단]하고, [사용 가능한 정보를 효과적으로 사용하는 방법을 찾는 것]이었습니다. The information age (roughly from the 1970s to the emergence of machine learning tools during the 2010s) featured the use of data that were accurate and timely, specific and organized for a purpose, and presented within a context that gave them meaning and relevance, as well as led to an increase in understanding and decrease in uncertainty.1The primary challenges for physicians during this time were determining validity and how to effectively use the available information.
인공 지능(또는 컴퓨터가 인간의 인지를 모방하는 것)은 한때 미래적인 비전으로만 여겨졌습니다. 이제 컴퓨터나 컴퓨터로 제어되는 로봇이 지능적인 존재와 관련된 작업을 수행하는 능력은 널리 받아들여지고 있습니다. 더 중요한 것은 "인공 지능"이라는 용어가 [추론, 의미 발견, 일반화 및 경험으로부터 학습하는 능력]과 같은 인간의 특징적인 지적 과정을 부여받은 시스템의 개발에 적용된다는 점입니다.2 인공 지능의 응용 프로그램을 사용한 데이터 조작은 의학교육에 중요한 영향을 미칩니다. 암기 위주의 현행 커리큘럼은 점점 더 다양한 출처의 정보를 효과적으로 통합하고 활용할 수 있는 역량을 가르치는 커리큘럼으로 전환해야 합니다. Artificial intelligence—or the mimicking of human cognition by computers—was once only a futuristic vision. Now, the ability of a computer or a computer-controlled robot to perform tasks commonly associated with intelligent beings is widely accepted. More important, the term “artificial intelligence” applies to the development of systems that are endowed with the intellectual processes characteristic of humans, such as the ability to reason, discover meaning, generalize, and/or learn from experience.2The manipulation of data using applications of artificial intelligence has significant implications for medical education. The current, largely memorization-based curriculum must transition to one that teaches competence in the effective integration and utilization of information from a growing array of sources.
예를 들어, 인체 안팎에서 사용 가능한 센서의 수와 유형이 기하급수적으로 증가하고 개인 및 조직 정보 인프라에 연결되는 것을 관리하는 것은 인공지능 시대에 떠오르는 과제 중 하나에 불과합니다. 의사와 환자 모두가 이용할 수 있는 대규모 데이터 모음, 점점 더 정교해지는 머신러닝(예: 왓슨 및 알파고) 사용, 의사와 환자 간의 지식 격차 축소 등 빅 데이터 사용의 의미는 현재의 의료 교육 모델에도 상당한 도전 과제를 안겨주고 있습니다. 의사가 신뢰할 수 있는 인공지능 기반의 의사결정 지원 소프트웨어를 사용하든, (병원, 환자 가정 또는 인체 내에) 배치된 로봇을 관리하든, 의사는 이 새로운 패러다임에 대한 교육을 받아야 할 것입니다. For example, managing the exponential growth in the number and type of available sensors, both within and outside the human body, and their connectivity to personal and organizational information infrastructures, is just one of the challenges emerging in the age of artificial intelligence. The implications of using big data, including large compilations of data that are available to both physicians and their patients, increasingly sophisticated uses of machine learning (e.g., Watson and Alpha Go), and the narrowing of the knowledge differential between physicians and patients, also pose substantial challenges to the current medical education model. Whether physicians use decision support software based on reliable artificial intelligence or manage robots deployed in hospitals, patients’ homes, or within the human body, they will need to be educated in this new paradigm.
20세기에 주로 집중된 의학교육 개혁 Medical Education Reform Has Largely Focused on the 20th Century
재단과 정부 기관이 자금을 지원하는 국가 보고서의 연구 결과를 바탕으로 의학교육을 개혁하려는 노력은 1910년 아브라함 플렉스너의 보고서 이후 일상화되어 몇 년마다 발표되고 있습니다. 미국의사협회는 2000년부터 2015년까지 의학교육 개혁을 촉구하는 국가 보고서가 15건 발표되었다고 언급했습니다.3 이러한 개혁안은 만성 질환 관리 및 진료 조정, 시스템 기반 진료, 진료 기반 개선, 효과적인 커뮤니케이션 등 이전에 확인된 개혁 분야와 많은 부분이 일치합니다. 전통, 인증 문제, 변화에 대한 교수진의 저항, 학생들이 국가 시험에서 좋은 성적을 거둘 수 있도록 준비시켜야 할 필요성 등이 일반적으로 필요한 개혁을 방해하는 주요 요인으로 간주됩니다. 미국의학협회의 수잔 스코첼락은 다음과 같이 주장합니다:
"[이러한 개혁에서] 빠진 것은 의료 서비스 전달의 과학입니다. 만성 질환을 어떻게 관리할까요? 예방과 건강에 어떻게 집중하나요? 어떻게 팀으로 일할 것인가?"3
Efforts to reform medical education, largely based on the findings in national reports funded by foundations and government agencies, have become routine and have been rolled out every few years since Abraham Flexner’s 1910 report. The American Medical Association noted that from 2000 to 2015 there were 15 national reports calling for medical education reform.3These proposed reforms paralleled many of the previously identified areas for reform, including the management of chronic conditions and care coordination, systems-based practice, practice-based improvement, and effective communication. Tradition, accreditation concerns, faculty resistance to change, and the need to prepare students to perform well on national board exams are generally considered the major factors impeding needed reform. Susan Skochelak of the American Medical Association argued:
“What’s been missing [from these reforms] is the science of health-care delivery. How do you manage chronic disease? How do you focus on prevention and wellness? How do you work in a team?”3
2016년 강연에서 워트먼은 의학교육의 "재부팅"을 주장하면서 현재 확인된 많은 개혁이 21세기 의학교육에 필요하지만 충분하지 않다고 지적했습니다.4 그는 또한 의학교육 개혁의 실적을 보면 의미 있는 변화를 받아들이는 데 더딘 산업을 묘사한다고 지적했습니다. 21세기형 의료 기술을 습득하기 위해서는 의학교육의 보다 근본적인 변화가 필요하다고 생각합니다. "한 번 보고, 한 번 하고, 한 번 가르친다"는 격언이 과거 의사의 임상 술기 학습 방식을 특징지었을지 모르지만, 이제 교육이 효과적이려면 모든 수준의 학습자가 자신의 성과를 표준과 비교하고 역량을 갖출 때까지 계속 연습할 기회를 가져야 한다는 것이 분명해졌습니다.5 의료의 질 저하와 지속 불가능한 비용 증가로 고민하는 리더, 외부 이해관계자, 대중의 압박으로, 의사들은 학습 목표를 보다 나은 치료 제공 및 책무성 강화 조치와 더욱 긴밀하게 연계하는 이니셔티브를 설계하는 데 더 엄격한 과제에 직면해 있습니다.6 In a 2016 lecture, Wartman advocated a “reboot” of medical education, noting that many of the current reforms that have been identified are necessary but not sufficient for 21st-century medical education.4He also noted that the track record of medical education reform depicts an industry that is slow to adopt meaningful change. The acquisition of 21st-century skills for medical practice requires, in our opinion, a more radical transformation of medical education. Although the dictum “see one, do one, teach one” may have characterized the way physicians learned clinical skills in the past, it is now clear that, for training to be effective, learners at all levels must have the opportunity to compare their performance against a standard and to continue to practice until competence is achieved.5Pressed by their leaders, external stakeholders, and a public troubled by lapses in quality of care and unsustainable cost increases, physicians are facing stiffer challenges in designing initiatives that more closely link the goals of learning with both the delivery of better care and measures of greater accountability.6
고용주들은 학부, 대학원 및 평생 의학 교육을 더욱 긴밀하게 통합해야 한다는 설득력 있는 주장을 펼치고 있습니다. 이들은 면허를 취득한 후 다른 의료 팀원들과 함께 일하고, 의료 전문직과 치료 연속체를 아우르는 지식을 갖추고, 스마트폰, 소셜 미디어 및 기타 장치를 사용하여 데이터 플랫폼을 활용하고, 고객 서비스를 포함한 결과 분석과 성과 개선에 집중하는 의사를 필요로 합니다.7 Employers are making a compelling case for a tighter integration of undergraduate, graduate, and continuing medical education. They need physicians who work at the top of their license with other members of the health care team; have knowledge that spans the breadth of the health professions and care continuum; leverage data platforms by using smartphones, social media, and other devices; and focus on analyzing outcomes and improving performance, including customer service.7
의학교육의 의미 있는 변화에 대해 아브라함 플렉스너만큼 큰 소리로 환호하는 사람은 없을 것입니다. 변화에 대한 유연성과 자유, 그리고 변화의 의무는 그의 메시지의 일부였습니다. 그는 의심할 여지없이 오늘날 필요한 의학교육의 근본적인 구조조정을 지지할 것입니다. 그렇다면 문제는 다음과 같습니다:
20세기의 지배적인 모델에서 21세기의 새로운 과제, 특히 빅데이터와 인공 지능의 전문 진료 분야 적용 증가에 대응할 수 있는 의학교육으로 어떻게 개혁할 수 있을까요?
No one would cheer more loudly for meaningful change in medical education than Abraham Flexner. The flexibility and freedom to change—indeed, the mandate to do so—were part of his message. He would undoubtedly support the fundamental restructuring of medical education that is needed today. So, the question becomes:
How do we reform medical education from the dominant 20th-century model into one that can address the emerging challenges of the 21st century, especially the increasing application of big data and artificial intelligence in professional practice?
21세기를 위한 의학교육 리부트 A Medical Education Reboot for the 21st Century
우리는 의학교육 재부팅의 토대는 미래의 의료 행위가 [의사, 다른 의료 전문가, 기계(소프트웨어와 하드웨어 모두 포함), 환자] 간의 명백한 파트너십이 될 것이라는 공동체의 인식에 있다고 믿습니다. 미래의 의료 행위는 의사의 기본 규칙을 변화시키는 네 가지 특징을 갖게 될 것입니다. We believe that the foundation for a medical education reboot lies in the community’s recognition that future medical practice will be an explicit partnership among physicians, other health care professionals, machines (which includes both software and hardware), and patients. Future medical practice will have four characteristics that change the ground rules for physicians.
첫째, 다양한 장소에서 진료가 제공될 것입니다. 기술은 환자와 함께, 그리고 환자 내부로 이동하며 지속적인 데이터 흐름을 제공할 것입니다. 대용량 데이터 저장 및 처리 인프라에 실시간으로 더 쉽게 액세스할 수 있게 될 것입니다. 환자, 보험사, 규제 당국은 편의성과 입증 가능한 결과를 요구할 것입니다. First, care will be provided in many locations. Technology will move with and inside patients, providing a continuous flow of data. Large data storing and processing infrastructures will become more readily accessible in real time. Patients, insurers, and regulators will insist on convenience and demonstrable results.
둘째, 의료 서비스는 새롭게 구성된 의료팀에 의해 제공될 것입니다.[신성하게 여겨져왔던 일대일 의사-환자 관계]는 환자와 여러 의료 제공자(예: 간호사, 사회복지사, 물리 및 작업 치료사, 케어 매니저, 가정 건강 보조원, 사회적 지원 그룹, 가족, 아직 정의되지 않은 새로운 종류의 의료 제공자)와의 관계로 대체될 것이며, 환자의 거주지와는 무관하게 이루어집니다. 의사나 팀 리더 역할을 하는 다른 사람들은 팀 치료에서 최대한의 가치를 얻는 방법을 배워야 합니다. 이를 위해서는 새로운 진료 방식에 맞춰 팀원들의 진료 범위를 신중하게 재설계해야 할 것입니다. 그 결과 현재의 면허 제약에 대한 도전과 수정이 이루어질 것으로 예상됩니다. Second, care will be provided by newly constituted health care teams. The sacrosanct one-to-one doctor–patient relationship will be replaced by patient relationships with multiple health providers (e.g., nurses, social workers, physical and occupational therapists, care managers, home health aides, social support groups, family members, and new kinds of health care providers yet to be defined, without regard to where patients live). Physicians or others who serve as team leaders will need to learn how to gain the most value from team care. Such practice will necessitate the careful redesign of the scopes of practice of team members to align with new practice modalities. As a result, we believe that current licensure constraints will be challenged and modified.
셋째, 다양한 출처의 데이터, 접근 가능한 대규모 데이터 세트, 인공 지능을 기반으로 진료가 제공될 것입니다. 방대한 메타 데이터 세트에 대한 기계 기반 분석의 통합이 환자 치료의 표준이 되어 각 환자를 지속적으로 모니터링할 수 있게 될 것입니다. 데이터를 관리하고 방대한 양의 정보에 대한 유효한 평가를 제공하기 위해 새로운 해석 및 기능적 진료 인프라가 시간이 지남에 따라 개발될 것입니다. 의사는 환자와 그 가족, 기계, 점점 더 다양해지는 의료 전문가들의 복잡한 교차점 속에서 의사결정이 이루어지는 환경에서 진료를 하게 될 것입니다. Third, care will be delivered based on a growing array of data from multiple sources, accessible large data sets, and artificial intelligence. The incorporation of machine-based analysis of huge meta-data sets will become standard for patient care, leading to continuous monitoring of each patient. A new interpretive and functional practice infrastructure will be developed over time both to manage the data and to provide valid assessments of the expanding volume of information. Physicians will practice in an environment where decision making takes place within the complex intersection of patients and their families, machines, and an expanding variety of health professionals.
넷째, 마지막으로 의학과 기계 간의 인터페이스를 능숙하게 관리해야 할 것입니다.기계는 많은 분야에서 더 많은 것을 알게 되고 전통적으로 의사가 수행하던 더 많은 작업을 수행할 수 있게 될 것입니다. 따라서 돌봄제공자는 기계가 점점 더 인지적, 육체적으로 인간을 능가할 것이라는 사실을 받아들여야 합니다. Fourth, and finally, the interface between medicine and machines will need to be skillfully managed. Machines will know more in many areas and be able to perform more tasks that traditionally have been performed by physicians. Thus, caregivers will need to come to terms with the fact that devices increasingly will outperform humans, both cognitively and physically.
미래 실무에 필요한 기술 Necessary Skills for Future Practice
인지 심리학의 연구 결과를 더 잘 활용하고, 교육에서 인간과 기계를 더 긴밀하게 연계하며, 치료 전달에 기계를 통합하고 환자를 치료의 적극적인 협력자로 보는 데 초점을 맞춘 시뮬레이션을 강화하는 등 인공지능 시대로 이동함에 따라 새로운 기술과 전문성이 요구될 것입니다. New skills and expertise will be required as we move to an age of artificial intelligence, including better use of the findings of cognitive psychology, closer alignment of humans and machines in education, and enhanced use of simulations focused on the integration of machines in care delivery and on patients as active collaborators in their care.
인지 심리학은 사실과 개념이 사용될 맥락에서 가르치고, 연습하고, 평가할 때 가장 잘 기억되고 활용된다는 사실을 입증했습니다. 임상 전문 지식에 대한 수십 년간의 연구를 통해 징후와 증상을 평가하고, 진단 검사를 선택 및 해석하고, 데이터를 종합하여 임상 평가 및 치료 계획을 개발하는 의사의 사고가 밝혀졌습니다.8 한 관찰자는 "기술이 변화하고 데이터 안개가 짙어짐에 따라 교육 표준을 새로 고치고, 개선하고, 개선해야 합니다."9 Cognitive psychology has demonstrated that facts and concepts are best recalled and put into service when they are taught, practiced, and assessed in the context in which they will be used. Several decades of research on clinical expertise have elucidated the thinking of physicians as they evaluate signs and symptoms, select and interpret diagnostic tests, and synthesize data to develop clinical assessments and care plans.8As noted by one observer, “Educational standards need to be refreshed, refined and improved as technology changes and the data fog thickens.”9
생물의학에 대한 근본적인 이해와 임상 지식 및 실무 전문 지식과의 상호 연결성이 의학교육의 중심이 되어야 한다는 데에는 이견이 없습니다. 그러나 21세기 커리큘럼에는 인공지능이 지원하는 풍부한 데이터 환경에서 의사가 보다 정밀하게 진료할 수 있는 역량을 강화하는 요소도 포함되어야 합니다. 한 가지 예로, 학습자는 의사 결정의 맥락에서 빅 데이터에 노출되어야 합니다. 학습자는 빅데이터의 네 가지 V에 대한 확실한 이해를 키워야 합니다.
볼륨(과거의 데이터 양에 비해 오늘날의 데이터 양은 방대함),
다양성(데이터는 다양한 유효성을 가진 다양한 소스에서 제공됨),
속도(데이터는 매우 빠르게 생성되고 있으며 그 속도가 증가하고 있음),
진실성(생성되는 데이터의 품질을 평가해야 함)
There is no disagreement that a fundamental understanding of the biomedical sciences and their interconnectedness with clinical knowledge and expertise in practice should remain central to medical education. However, the 21st-century curriculum also should include components to strengthen physicians’ capacity to practice with more precision in a data-rich environment supported by artificial intelligence. As one example, learners must be exposed to big data in the context of decision making. They must develop a solid understanding of the four Vs of big data:
volume (the amount of data today is vast compared with the amount in the past);
variety (data come from many different sources of varying validity);
velocity (data are being generated very fast, and momentum is increasing); and
veracity (the quality of the data being generated needs to be assessed).
또한 학습자는 인공 지능 애플리케이션을 통해 의료 서비스 제공에서 데이터가 어떻게 집계, 분석되고 궁극적으로 개인화되는지에 대한 기본적인 이해를 개발해야 합니다. 또한 의사 결정 지원 소프트웨어, 로봇 또는 보다 정교한 소셜 미디어 애플리케이션에 구현된 다양한 애플리케이션을 관리하는 방법에 대해 폭넓게 생각할 수 있어야 합니다. 양과 벨트리10는 "가장 중요한 과제는 의료 데이터를 정밀 의학, 예방 의학, 예측 모델링을 위한 부가 가치로 변환하는 방법입니다."라고 지적했습니다. Learners also will need to develop a basic understanding of how data are being aggregated, analyzed, and ultimately personalized in health care delivery through artificial intelligence applications. They will need to be able to think broadly about how to manage the variety of applications, whether embodied in decision support software, robots, or more sophisticated social media applications. As Yang and Veltri10noted, “The most critical challenge is how we can transform the health care data into additional values for precision medicine, preventive medicine, and predictive modeling.”
결론 Conclusion
의대생들이 인공지능 애플리케이션으로 변화된 의료 환경에서 성공적으로 실습할 수 있도록 가르치는 방법은 오늘날 커리큘럼 개혁의 중심이 되어야 합니다. 이를 위해서는 인증 기관의 전폭적인 지원이 필요합니다.
혁신과 실험에 기꺼이 개방적이고,
학생들의 미래 진료와 무관한 사실 기반 암기와 임상 실습에 중점을 두는 기존 모델을 훨씬 뛰어넘을 수 있도록
미래의 의대 졸업생들이 면허를 취득하고 가치 기반 재정 시스템에 적응하려면 새로운 방식의 평생 교육에 참여해야 합니다. 이들은 다음을 강화해야 할 것입니다.
진료 연속체 전반에 걸쳐 의료 전문가의 역량에 대한 확실한 이해를 통합
전문 진료에서 팀워크를 강화
정보 플랫폼 및 인텔리전스 도구에 대한 편안한 지식을 보유
고객 서비스 기술을 강화
성과와 결과를 개선하기 위해 정보 및 인텔리전스의 효과적인 사용
이러한 전문적 특성의 토대는 학부 의학교육 커리큘럼에 포함되어야 합니다. How to teach medical students to practice successfully in a health care environment transformed by artificial intelligence applications should be a central focus of curricular reform today. It requires the whole-hearted support of accreditors who are
willing to be more open to innovation and experimentation and
able to move far beyond the old model with its emphasis on fact-based memorization and clinical clerkships that are often unrelated to students’ future practice.
Future medical school graduates will need to participate in new modalities of lifelong education if they are to perform at the top of their license and adapt to a value-based financing system. They will need to
incorporate a solid understanding of the capabilities of health professionals across the care continuum,
enhance teamwork in their professional practice,
possess a comfortable knowledge of information platforms and intelligence tools,
strengthen their customer service skills, and
reinforce the effective use of information and intelligence to improve performance and outcomes.
The foundation for these professional attributes must be embedded in undergraduate medical education curricula.
또한 커리큘럼 전반에 걸쳐 두 가지 추가 기술(새로운 기술, 기존 기술)을 강조하고 전달해야 합니다.
첫 번째는 의사가 데이터 플랫폼에서 생성된 확률의 의미를 인간 특유의 복잡성에 직면한 환자에게 전달할 수 있는 능력을 향상시키는 통계적 전문 지식을 습득하는 것입니다.
두 번째는 진정으로 자비로운 의료인이 되기 위한 지속적인 교육과 평가이며, 이는 의학이 점점 더 첨단화되는 상황에서 간과해서는 안 되는 부분입니다.
Two additional skills, one new, one old, also must be emphasized and carried throughout the curriculum.
The first is the mastering of statistical expertise that enhances the ability of the physician to communicate the meaning of the probabilities generated by data platforms to patients in the face of their uniquely human complexity.
The second involves constant training and evaluation toward being a truly compassionate provider, something that must not be overlooked as medicine becomes increasingly high tech.
즉, 의학교육은 기초적인 생의학 및 임상 과학을 넘어 새로운 진단 및 치료 트렌드에 대한 최신 정보를 제공해야 합니다. 다양한 의료 전문가들 간의 전문적 노력의 조직화, 기계 학습 및 로봇과 같은 정보 및 인텔리전스 도구의 사용, 성과 및 결과 개선에 대한 끊임없는 집중, 환자와의 자비로운 소통의 숙달을 보장하는 체계적인 커리큘럼으로 발전해야 합니다. In other words, medical education will need to move beyond the foundational biomedical and clinical sciences and updates on emerging diagnostic and therapeutic trends. It will need to evolve to include systematic curricular attention to the organization of professional effort among a variety of health professionals, the use of information and intelligence tools such as machine learning and robots, a relentless focus on improving performance and outcomes, and ensuring the mastery of compassionate communication with patients.
1S.A. Wartman is president and CEO, Association of Academic Health Centers, Washington, DC. C.D. Combs is vice president and dean, School of Health Professions, Eastern Virginia Medical School, Norfolk, Virginia.
Noteworthy changes coming to the practice of medicine require significant medical education reforms. While proposals for such reforms abound, they are insufficient because they do not adequately address the most fundamental change-the practice of medicine is rapidly transitioning from the information age to the age of artificial intelligence. Increasingly, future medical practice will be characterized by: the delivery of care wherever the patient happens to be; the provision of care by newly constituted health care teams; the use of a growing array of data from multiple sources and artificial intelligence applications; and the skillful management of the interface between medicine and machines. To be effective in this environment, physicians must work at the top of their license, have knowledge spanning the health professions and care continuum, effectively leverage data platforms, focus on analyzing outcomes and improving performance, and communicate the meaning of the probabilities generated by massive amounts of data to patients, given their unique human complexities. The authors believe that a "reboot" of medical education is required that makes better use of the findings of cognitive psychology and pays more attention to the alignment of humans and machines in education and practice. Medical education needs to move beyond the foundational biomedical and clinical sciences. Systematic curricular attention must focus on the organization of professional effort among health professionals, the use of intelligence tools involving large data sets, and machine learning and robots, all the while assuring the mastery of compassionate care.