역량중심의학교육 도입: 앞으로 나아가기(Med Teach, 2017)
Implementing competency-based medical education: Moving forward
Jason R. Franka,b, Linda Snella,c, Robert Englanderd and Eric S. Holmboee; on behalf of the ICBME Collaborators

배경
Background
큰 혁신은 갑자기 가능한 것이 절실히 필요한 것과 만날 때 일어납니다.
Big breakthroughs happen when what is suddenly possible meets what is desperately necessary.
토마스 프리드먼 (2012)
Thomas Friedman (2012)
2010년 Medical Teacher 특별호에서 국제 CBME 협력자들은 역량 기반 의학교육(CBME)을 "의학교육 프로그램의 설계, 실행, 평가 및 평가에 대한 성과 기반 접근법으로, 역량에 대한 조직화된 프레임워크를 사용"하며(Frank 외. 2010b, 641쪽) "근본적으로 졸업생의 성과 능력을 지향하고 사회 및 환자 요구 분석에서 도출된 역량을 중심으로 구성된 의사 실습 준비에 대한 접근법"으로 정의했습니다. 이는 시간 기반 교육을 강조하지 않고 더 큰 책임감, 유연성, 학습자 중심성을 약속합니다."(Frank 외, 2010a, 636쪽).
In a special issue of Medical Teacher in 2010, competency-based medical education (CBME) was defined by the International CBME Collaborators as “[a]n outcomes-based approach to the design, implementation, assessment, and evaluation of medical education programs, using an organizing framework of competencies” (Frank et al. 2010b, p. 641) and as “an approach to preparing physicians for practice that is fundamentally oriented to graduate outcome abilities and organized around competencies derived from an analysis of societal and patient needs. It de-emphasizes time-based training and promises greater accountability, flexibility, and learner-centredness” (Frank et al. 2010a, p. 636).
2009년에 결성되어 여러 의학교육 기관의 후원을 받는 국제 CBME 협력체는 차세대 의료 전문가를 준비시키기 위한 역량 기반 접근법을 탐구, 개발 및 향상시키는 데 관심이 있는 회원들이 모인 학술 네트워크입니다. CBME는 현대 의학 커리큘럼 설계 모델에서 발생하는 특정 과제와 단점을 해결할 수 있는 유망한 수단으로 인정받고 있습니다. 보다 구체적으로, CBME 모델의 개발은 다음에 대한 대응입니다.
Formed in 2009 and sponsored by several medical education organizations, the International CBME Collaborators are a scholarly network whose members are interested in exploring, developing, and enhancing competency-based approaches to preparing the next generation of health professionals. CBME is recognized as a promising means of addressing certain challenges and shortcomings attributed to contemporary models of medical curriculum design. More specifically, the development of the CBME model is a response to
- 환자, 인구, 의료 전문직 교육 프로그램과 관련된 결과에 더 큰 책임을 지고 더 집중해야 한다는 요구(Frenk 외. 2010);
- 의학 교육 후 졸업생 능력의 용납할 수 없는 변동성을 줄여야 할 필요성(Langdale 외. 2003; Raymond 외. 2011);
- 일부 졸업생이 안전하고 효과적인 진료를 할 준비가 되어 있지 않다는 증거;
- 의료 시스템에서 최선이 아닌 아닌 환자 치료 결과의 패턴(예: IOM 2000, 2001; OECD 2000-2015a, 2000-2015b, 2000-2015c);
- 21세기 실무와의 관련성을 보장하기 위해 커리큘럼 내용을 근본적으로 재검토할 것을 요구합니다. 여기에는 전문 의료 지식을 넘어 의사소통, 협업, 전문성 및 전문적 정체성 형성, 시스템적 사고, 평생 학습, 인구 건강, 지속적 개선에 대한 역량을 포함하도록 교육의 바람직한 성과에 대한 확장된 비전이 포함됩니다;
- 교육에 소요된 시간이 역량의 대리 지표가 되는 교육 모델은 더 이상 바람직하지도 방어할 수도 없다는 우려.
- calls for greater accountability and a greater focus on outcomes relating to patients, populations, and health professions education programs (Frenk et al. 2010);
- the need to reduce unacceptable variability in graduate abilities after medical training (Langdale et al. 2003; Raymond et al. 2011);
- evidence that some graduates are not prepared for safe and effective practice;
- patterns of suboptimal patient outcomes in health care systems (e.g. IOM 2000, 2001; OECD 2000–2015a, 2000–2015b, 2000–2015c);
- calls for a fundamental re-examination of curriculum content to ensure relevance to the twenty-first century practice. This includes an expanded vision of the desired outcomes of training, such that they go beyond expert medical knowledge to include competencies in communication, collaboration, professionalism and professional identity formation, systems thinking, lifelong learning, population heath, and continuous improvement;
- concerns that models of education in which time spent in training is a surrogate marker of competence are no longer desirable or defensible.
CBME의 진화
The evolution of CBME
CBME는 2009년에 시작된 것이 아닙니다. 그 역사는 ten Cate(2014)에 의해 기술되었으며, 획기적인 발전은 표 1에 요약되어 있습니다. 미국에서 역량 기반 교육에 대한 아이디어는 거의 한 세기 전에 특정 성과와 행동에 초점을 맞춘 산업 및 비즈니스 모델에서 처음 등장했습니다. 1960년대에는 보다 관련성 있고 성과에 초점을 맞춘 교육에 대한 요구에 따라 교사 교육에 역량 기반 교육 훈련이 도입되었습니다(Houston 1973; Burke 1999).
CBME did not begin in 2009. Its history has been described by ten Cate (2014), and landmark developments are summarized in Table 1. In the United States, the idea of competency-based training first surfaced almost a century ago within industrial and business models that focused on specific outcomes and behaviors. In the 1960s, competency-based education training was introduced in teacher education in response to demands for more relevant and outcomes-focused training (Houston 1973; Burke 1999).

20세기 내내 보건 전문직 교육자들은 커리큘럼 개발에서 수많은 잠정적인 혁신을 고려했습니다.
- 1978년, 세계보건기구를 위한 비전 보고서에서 맥개히 등은 보건 전문직 교육이 지역 및 지역 인구 보건 요구를 진정으로 충족할 수 있도록 전 세계적으로 CBME를 채택할 것을 촉구했습니다.
- 사실, 60년 이상 동안 역량 기반 교육은 여러 관할 구역과 사회복지(Menefee & Thompson 1994), 카이로프랙틱 의학(Wangler 2009), 약학(Marshall 외. 1997) 등 여러 직종에서 교육 접근법으로 사용되거나 제안되어 왔습니다.
- 1990년대에 많은 관할권에서 역량 프레임워크를 교육 및 훈련의 핵심 요소로 사용하는 '결과 지향적 접근법'이 등장했습니다.
- 오늘날 가장 널리 알려진 세 가지 역량 기반 프레임워크는 영국의 굿 메디컬 프랙티스 표준(General Medical Council 2013), 미국의 의학전문대학원 교육 인증 위원회의 아웃컴 프로젝트(Swing 2007), 캐나다 왕립 의사 및 외과의사 대학의 CanMEDS 역량 프레임워크(Frank 외. 2015)입니다.
- 2010년, 메디컬 티처는 이 새로운 역량 기반 패러다임을 문서화, 정교화, 개발 및 보급하는 데 전념하는 국제 CBME 협력자들이 널리 인용된 일련의 논문을 발표했습니다(Campbell 외 2010; Dath 외 2010; Frank 외 2010a, 2010b; Harris 외 2010; Holmboe 외 2010; Iobst 외 2010; Snell & Frank 2010; Swing 외 2010; Taber 외 2010; ten Cate 외 2010).
Throughout the twentieth century, health professions educators considered numerous tentative innovations in curriculum development.
- In 1978, in a visionary report for the World Health Organization, McGaghie et al. called for the worldwide adoption of CBME to ensure that health professions education could truly meet local and regional population health needs.
- In fact, for more than 60 years competency-based education has been used, or suggested, as an approach to education in multiple jurisdictions and across multiple professions, including social work (Menefee & Thompson 1994), chiropractic medicine (Wangler 2009), and pharmacy (Marshall et al. 1997).
- In the 1990s, many jurisdictions witnessed the emergence of “outcomes-oriented approaches” that used competency frameworks as a key component of education and training.
- Today, the three most widely known competency-based frameworks are the Good Medical Practice standard in the United Kingdom (General Medical Council 2013), the Outcomes Project of the Accreditation Council for Graduate Medical Education in the United States (Swing 2007), and the CanMEDS Competency Framework of the Royal College of Physicians and Surgeons of Canada (Frank et al. 2015).
- In 2010, Medical Teacher published a series of widely cited papers from the International CBME Collaborators dedicated to documenting, elaborating, developing and disseminating this emerging competency-based paradigm (Campbell et al. 2010; Dath et al. 2010; Frank et al. 2010a, 2010b; Harris et al. 2010; Holmboe et al. 2010; Iobst et al. 2010; Snell & Frank 2010; Swing et al. 2010; Taber et al. 2010; ten Cate et al. 2010).
시리즈 II
Series II
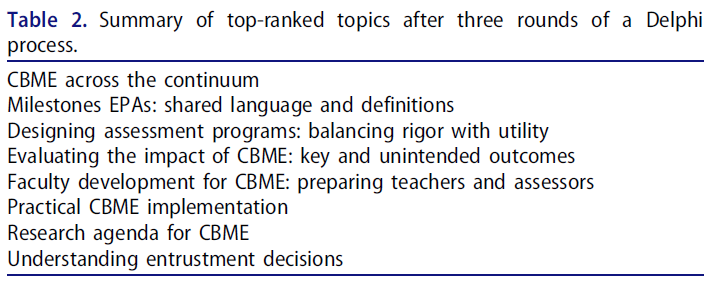
CBME는 관련자들이 이 접근법의 이론, 원리 및 실습에 대해 배우고 경험을 쌓으면서 흥미로운 방식으로 계속 발전하고 있습니다. 지난 10년 동안 CBME와 전 세계 교육자 네트워크는 비약적으로 성장했으며, 이번 메디컬 티처에서는 CBME의 개념과 논쟁뿐만 아니라 CBME의 실행에 초점을 맞춘 두 번째 논문 시리즈를 제공하게 되어 기쁘게 생각합니다. 국제 CBME 협력자들은 2013년과 2016년에 추가로 서밋을 개최했습니다. 참가자들의 관심 주제와 이슈는 델파이 프로세스를 통해 우선순위를 정했고(표 2 참조), 그 결과 논의된 내용을 이 시리즈 논문으로 정리했습니다.
CBME continues to evolve in exciting ways as those involved learn and gain experience in the theories, principles, and practices of this approach. Both CBME and our global network of educators have grown dramatically in the last decade, and in this issue of Medical Teacher, we are pleased to offer a second series of papers focused not just on CBME concepts and controversies, but also on the implementation of CBME. The International CBME Collaborators held further summits in 2013 and 2016. Topics and issues of interest to the participants were prioritized using a Delphi process (see Table 2), and the resulting discussions were distilled into this series of articles.
입문 논문에서 홀름보에와 동료들은 주요 국제 운동으로서 CBME의 성장에 대해 논의하고 이 모델에 대해 제기된 몇 가지 비판을 다룹니다(홀름보에 외. 2017). 잉글랜드와 공동 저자들은 한 걸음 더 나아가 의학교육자들이 의학교육의 이러한 적응적 변화에 필요한 공유 언어를 향해 나아감에 따라 공통의 정의를 개발하고 특정 핵심 개념 간의 관계를 파악하기 위한 국제 CBME 협력자들의 노력을 제시합니다(잉글랜드 외 2017).
In an introductory paper, Holmboe and colleagues discuss the growth of CBME as a major international movement and address some of the criticisms that have been leveled against the model (Holmboe et al. 2017). Englander and coauthors take a further step, presenting the efforts of the International CBME Collaborators to develop common definitions and to identify the relationships between certain core concepts, as medical educators move toward a shared language necessary for this adaptive change in medical education (Englander et al. 2017).
실행은 많은 사람들에게 현재 문제이기 때문에, CBME를 실행하는 데 있어 가장 중요한 과제는 Caverzagie 외. (2017)에서 논의합니다. (2017)은 CBME로의 전환을 지원하는 데 필요한 구조적 변화를 탐구함으로써 구현 주제를 이어갑니다. 퍼거슨 외(2017)는 의료 전문가 교육을 둘러싼 직업적, 제도적, 조직적 문화에 필요한 변화를 더 깊이 파고듭니다. 이들은 현재 의학교육 문화에서 CBME의 수용을 가로막는 주요 장벽을 파악하고 이를 해결하기 위한 방법을 제안합니다.
Because implementation is a current issue for many, overarching challenges to implementing CBME are discussed by Caverzagie et al. (2017). Nousiainen et al. (2017) continue the implementation theme by exploring the structural changes needed to support the transition to CBME. Ferguson et al. (2017) delve deeper to consider changes needed in the professional, institutional, and organizational cultures surrounding the training of medical professionals. They identify key barriers to the acceptance of CBME within the current culture of medical education and propose ways to address them.
평가는 원칙과 실무의 관점에서 여전히 어려운 과제로 남아 있습니다. Harris 등(2017)은 CBME 평가의 최근 발전을 살펴보고, 2013년 CBME에 관한 초청 서밋에서 논의된 평가와 관련된 주요 이슈를 설명합니다. CBME 평가의 핵심 원칙은 Lockyer 외(2017b)에 의해 설명되어 있으며, 이들은 평가 프로그램의 효과를 보장하는 방법도 검토합니다.
Assessment remains a challenge from the perspective of principles and practice. Harris et al. (2017) explore recent developments in CBME assessment, describing key issues regarding assessment as discussed at the 2013 invitational summit on CBME. Core principles of assessment in CBME are described by Lockyer et al. (2017b), who also examine ways to ensure the effectiveness of assessment programs.
협력자들은 미래를 내다보기도 했습니다. Lockyer 외(2017a)는 CBME의 원칙이 아직까지 지속적 전문성 개발(CPD)에 널리 채택되지는 않았지만, 레지던트 이후에도 대학원 수련 기간만큼이나 중요하며, 개업의가 경력 전반에 걸쳐 역량을 유지할 수 있도록 CPD 접근 방식에 상당한 변화가 필요하다고 제안합니다. 이 논문에서는 CPD 개혁의 근거를 살펴보고, CBME-CPD 프레임워크로의 전환을 촉진하는 핵심 요소와 직장 내 역량 및 성과 평가를 위한 확장된 역할을 고려하며, CBME 환경에서 CPD를 지원하기 위한 교육 활동을 제안하고, 다양한 이해관계자에 대한 시사점을 강조합니다. 마지막으로, 그루펜 외(2017)는 CBME의 맥락에서 연구가 필요한 다양한 이론적, 실제적 질문을 제시합니다. 저자들은 CBME 실행의 결과와 모범 사례에 대한 증거를 수집하는 데 있어 해결해야 할 방법론적 문제를 추가로 탐구합니다.
The Collaborators also looked to the future. Although the principles of CBME have yet to be widely adopted in continuing professional development (CPD), Lockyer et al. (2017a) suggest that they are just as important after residency as they are during postgraduate training, and that significant changes are needed in the approach to CPD to ensure that practicing physicians maintain competence throughout their careers. Their paper explores the rationale for CPD reform; considers the key elements that would facilitate a transition to a CBME–CPD framework and an expanded role for the assessment of competence and performance in the workplace; suggests educational activities to support CPD in a CBME environment; and highlights the implications for different stakeholders. Finally, Gruppen et al. (2017) present a range of questions, both theoretical and practical, that require research in the context of CBME. The authors further explore methodological issues that will need to be addressed in gathering evidence about outcomes and best practices in implementing CBME.
가장 최근에 열린 두 차례의 국제 CBME 협력자 서밋을 통해 다른 저널에 게재된 논문이 추가로 발표되었습니다. 카라치오 외(2016)가 작성한 임상의사-교육자를 위한 헌장에는 의학교육이 사회의 필요에 기반해야 하고, 구조나 과정이 아닌 결과에 초점을 맞춰야 하며, 초기 의대생부터 시니어 개원의까지 전 과정에 걸쳐 원활하게 이루어져야 한다는 CBME의 세 가지 기본 원칙이 명시되어 있습니다. 그런 다음 헌장은 효과적인 실행을 보장하기 위해 9가지 약속을 제안합니다. 위탁 의사 결정에 관한 논문에서 ten Cate 등(2016)은 임상 수련에서 위임 의사 결정을 내리는 과정을 설명하고, 다양한 신뢰 방식을 개괄하며, 위탁으로 이어지는 요인에 대해 논의합니다. 이 논문은 CBME에서 이루어지는 평가 결정의 토대를 마련합니다. Van Melle 등(2016)은 CBME 프로그램을 평가하고 그 영향을 이해하기 위한 엄격한 접근법으로 기여도 분석을 사용할 것을 제안합니다.
The two most recent summits of the International CBME Collaborators resulted in additional papers that have been published in other journals. A charter for clinician–educators framed by Carraccio et al. (2016) outlines three basic tenets of CBME: medical education must be based on the needs of society; it must focus on outcomes, not structure or process; and it must be seamless across the continuum from early medical student to senior practitioner. The Charter then proposes nine commitments to ensure that implementation is effective. In a paper on entrustment decision-making, ten Cate et al. (2016) describe the process of making entrustment decisions in clinical training, outline varied modes of trust, and discuss the factors that lead to entrustment. This paper lays a foundation for the assessment decisions made in CBME. Van Melle et al. (2016) propose using contribution analysis as a rigorous approach to evaluate CBME programs and understand its impact.
가까운 미래
The near future
역량 기반의 성과 중심 교육은 현재 여러 관할권에서 시행되고 있습니다. 이는 일련의 열망, 혁신, 개념, 실험에서 수많은 보건 전문직 교육 기관의 체계적이고 지지받는 방향으로 변모했습니다. 많은 일이 있었지만 아직 해야 할 일이 많이 남아 있습니다. 도전과제는 여전히 남아 있고 자원은 무한하지 않지만, 의학교육 및 수련 시스템을 개선할 수 있는 기회가 존재하며, 역량 기반 프레임워크로의 전환은 미래 의사들의 더 나은 교육을 통해 개별 환자와 사회의 건강에 상당한 긍정적 영향을 미칠 것이라고 확신합니다. 시간만을 기준으로 한 수련은 이제 끝날 때가 되었습니다.
Competency-based, outcomes-focused education is now implemented in a number of jurisdictions. It has been transformed from a set of aspirations, innovations, concepts, and experiments into the systematic and espoused directions of numerous institutions of health professions education. Although much has happened, much remains to be done. Challenges remain, and resources are not limitless, but we are certain the opportunities for improvement in our medical education and training systems exist, and that the move to a competency-based framework will have a significant positive impact on the health of individual patients and society through the better education of future physicians. The end of training based only on time is now … and it is about time.
Implementing competency-based medical education: Moving forward
Affiliations collapse
PMID: 28598743
Abstract
For more than 60 years, competency-based education has been proposed as an approach to education in many disciplines. In medical education, interest in CBME has grown dramatically in the last decade. This editorial introduces a series of papers that resulted from summits held in 2013 and 2016 by the International CBME Collaborators, a scholarly network whose members are interested in developing competency-based approaches to preparing the next generation of health professionals. An overview of the papers is given, as well as a summary of landmarks in the conceptual evolution and implementation of CBME. This series follows on a first collection of papers published by the International CBME Collaborators in Medical Teacher in 2010.
'Articles (Medical Education) > 교육과정 개발&평가' 카테고리의 다른 글
| 졸업후의학교육에서 공유의사결정을 위한 EPA 식별하기: 국가 델파이 연구(Acad Med, 2021) (0) | 2024.01.02 |
|---|---|
| 학부의학교육에서 지속적 질 개선의 문화 만들기(Acad Med, 2020) (0) | 2023.12.06 |
| 적응적 의과대학 교육과정: 지속적 개선을 위한 모델(Med Teach, 2018) (0) | 2023.11.30 |
| 미국 의료시스템과학 교육의 한국 도입과 그 비판(Korean J Med Hist, 2022) (0) | 2023.11.16 |
| 모든 이해관계자를 위한 핵심 역량 평가 프로그램 만들기: 선박 설계와 건조에서 얻을 수 있는 것( Adv Health Sci Educ Theory Pract. 2020) (0) | 2023.11.10 |