건강의 사회적 결정요인과 관련한 환자돌봄의 관찰가능한 프로세스 정의 (Med Educ, 2022)
Defining the observable processes of patient care related to social determinants of health
Junki Mizumoto | Toshichika Mitsuyama | Satoshi Kondo | Masashi Izumiya | Shoko Horita | Masato Eto

1 소개
1 INTRODUCTION
건강의 사회적 결정요인(SDH)은 '사람들이 태어나고, 성장하고, 생활하고, 일하고, 노화하는 조건으로... 글로벌, 국가 및 지역 수준에서 돈, 권력 및 자원의 분배에 의해 형성된다'으로 정의됩니다.1 SDH는 인구 건강 결과에 상당한 기여를 합니다. 의료 전문가는 건강 결과에 영향을 미치는 사회 구조를 인식하는 능력(구조적 역량이라고 함)을 훈련하고2 환자에게 개별화된 치료를 제공하고 공중 보건을 개선해야 하지만3 환자의 사회적 요구에 항상 부응하는 것은 아닙니다.4, 5 일부 연구에 따르면 의사는 사회적 어려움을 가진 환자를 돌보는 데 장벽을 경험한다고 보고했습니다.6-11
Social determinants of health (SDHs) are defined as ‘the conditions in which people are born, grow, live, work and age … shaped by the distribution of money, power and resources at global, national and local levels’.1 SDH makes a substantial contribution to population health outcomes. Although health care professionals are expected to train the ability to recognise social structure to influence health outcomes (as is called structural competency)2 and to deliver individualised care to patients and improve public health, 3 they do not always respond to patients' social needs.4, 5 Some studies have reported that physicians experience barriers in caring for patients with social difficulties.6-11
[사회적 불평등이 건강 상태에 미치는 영향]은 임상 수련 전문가들에 의해 종종 무시되어 왔습니다.12 예를 들어, 의학전문대학원 교육인증위원회는 레지던트 및 펠로우십 프로그램에서 수련의가 사회적 결정 요인을 식별 및 해결하고 환자의 건강 결과에 미치는 영향을 최적화하도록 준비시킬 수 있는 프로그램은 거의 없다고 보고했습니다.13 그럼에도 불구하고, SDH의 대학원 교육은 독특한 이점을 제공할 수 있을 것입니다. 레지던트는 환자의 건강 요구를 효과적으로 해결하는 기술을 개발하고 지역사회에 보다 생산적으로 참여함으로써 자기 효능감과 만족감을 경험할 수 있습니다.3 환자 건강에 영향을 미치는 사회적 결정 요인에 대해 학습하면 레지던트가 환자의 상황에 집중하고 환자-의사 관계를 강화하며 의료 팀 기반 파트너십을 구축하는 데 도움이 될 수 있습니다.13 이러한 학습은 어려운 상황에 있는 환자를 치료할 때 특히 중요합니다.3, 14 이러한 긍정적인 결과를 고려할 때 건강과 건강 관리를 개선하려면 SDH에 대한 의학 교육의 중요성을 강조하고 보다 효과적인 교육 전략을 개발하는 것이 중요해야 합니다.15
The effects of social inequity on health conditions have often been ignored by clinical training experts.12 For example, the Accreditation Council for Graduate Medical Education reported that few residency and fellowship programmes can prepare trainees to identify and address social determinants and optimise their effects on patients' health outcomes.13 Nevertheless, postgraduate education in SDH would provide unique benefits. Residents would experience self-efficacy and satisfaction by developing skills to effectively address patients' health needs and engaging more productively with their communities.3 Learning about social determinants that affect patient health could help residents focus on patients' contexts, strengthen patient–physician relationships and build health care team-based partnerships.13 Such learning is particularly important when residents deliver care for patients in difficult situations.3, 14 Considering these positive outcomes, emphasising the importance of medical education about SDH and developing a more effective educational strategy should be important to improve health and health care.15
SDH는 의학교육과 수련의 중요한 부분이지만, 전통적인 접근 방식으로는 SDH 역량을 문서화하기 어렵습니다.16 교육과정에서 비의료 교육 주제를 제시하는 것은 종종 모호한 목표와 불명확한 평가 기준을 특징으로 합니다.17 모호한 교육과정은 수련의에게 이러한 주제가 저평가되고 임상 학습과 단절되어 있다는 인상을 주고 환자 치료와 수련의의 전문적인 성장 모두에 해를 끼칠 수 있습니다.17 또한 SDH와 관련된 커리큘럼 기준이 부족하면 레지던트가 사회적 어려움을 가진 환자에 대한 편견과 오해를 조장할 수 있습니다.18 또한 대부분의 지도전문의는 자연스럽게 생물의학적 및 기술적 기술의 습득에 높은 가치를 두고 수련의의 사회적 책임과 윤리의식 함양에 소홀히 하는 경향이 있습니다.19
Although SDH is an important part of medical education and training, SDH competence is difficult to document using traditional approaches.16 Presentation of non-medical educational topics in the curriculum is often characterised by vague objectives and unclear assessment criteria.17 An ambiguous curriculum gives trainees the impression that these topics are undervalued and disconnected from clinical learning and may harm both patient care and the professional growth of trainees.17 Lack of curriculum criteria related to SDH may also foster residents' prejudices and misconceptions about patients with social difficulties.18 Additionally, most supervisors naturally place a high value on the acquisition of biomedical and technical skills and tend to neglect the development of social responsibility and ethics in trainees.19
전공의가 SDH 교육을 통해 무엇을 성취해야 하는지에 대한 명시적인 문서화가 중요합니다. 소외 계층에 대한 의료 서비스 제공과 같은 일부 역량은 자체적으로 위탁 가능한 전문 활동(EPA)을 수행할 가치가 있는 것으로 간주됩니다.20 예를 들어, 미국의과대학협회는 병력 청취와 관련된 EPA 하위 항목 중 하나는 SDH에 주의를 기울이는 환자 중심 면담을 수행하는 기술을 입증하는 것이라고 명시하고 있습니다.21 관찰 가능한 실습 활동(OPA)의 위탁 및 매핑은 레지던트 커리큘럼 및 평가 시스템에서 레지던트를 평가하는 데 사용할 수 있습니다.22, 23 OPA는 '위탁 결정을 내리기 위해 일상적인 실습에서 관찰해야 하는 학습 목표/활동의 모음'으로 정의됩니다.22 OPA는 두 가지 범주로 나뉩니다.
- 내용 OPA는 '호중구감소성 발열에 대한 항생제 치료 선택'과 같이 각 로테이션마다 다른 특정 활동입니다.
- 과정 OPA는 '정확하고 관련성 있는 병력 획득'과 같이 로테이션에 걸쳐 공통적으로 적용되는 활동입니다.22 과정 OPA의 개념은 모호한 역량 용어나 광범위한 EPA 대신 공동 의사 결정과 같은 특정 상황에서 의료 전문가가 따라야 하는 정확한 과정과 의료 절차를 설명하는 데 사용됩니다.24
Explicit documentation about what residents should achieve from SDH education is important. Some competencies, such as providing medical care for underserved populations, are considered worthy of their own entrustable professional activities (EPAs).20 For example, the Association of American Medical Colleges states that one of the EPA sub-items related to history taking is to demonstrate the skills to conduct patient-centred interviews that are attentive to SDH.21 Entrustment and mapping of observable practice activities (OPAs) can be used in residency curriculum and assessment systems to assess residents.22, 23 OPA is defined as ‘a collection of learning objectives/activities that must be observed in daily practice to form entrustment decisions’.22 There are two categories of OPA.
- Content OPAs are specific activities that differ for each rotation, such as ‘choose antibiotic therapy for neutropenic fever’.
- Process OPAs are activities that are conserved across rotations, such as ‘acquire accurate and relevant history’.22 The concept of process OPA is used to describe the precise process and medical procedures that medical professionals are expected to follow in specific situations, such as shared decision making,24 instead of using ambiguous competency terms or broad EPA.22
일차 의료 또는 포괄적인 일상 건강 관리에서 사회적 결정 요인에 대한 개입을 설명하는 여러 임상 프레임워크가 보고되었습니다. 이러한 개입은 세 가지 수준으로 나뉩니다.15, 25-28
- 일반적으로 개별 환자를 위한 미시적 수준,
- 의료 기관 및 지역사회를 위한 중시적 수준,
- 의료 시스템 및 행정 부서를 포함한 광범위한 인구를 위한 거시적 수준
이러한 프레임워크는 SDH를 의료 시스템에 통합하기 위한 청사진을 제공하지만, 의사가 [실제로 환자 치료를 제공하는 과정]은 자세히 설명되어 있지 않습니다. 또한 이러한 프레임워크의 대부분은 체계적인 합의 그룹 방법을 사용하여 개발되지 않았습니다. 임상 환경에서 의사가 하는 일을 자세히 설명하지 못하면 SDH 교육의 가치가 떨어집니다. 따라서 환자의 사회적 맥락과 필요에 대한 이해를 바탕으로 환자를 돌보는 [과정 OPA]를 설명해야 합니다. 본 연구는 합의 집단 방법을 사용하여 일차 진료 환경에서 SDH와 관련된 환자 진료 [과정 OPA]를 체계화하는 것을 목표로 했습니다.
Several clinical frameworks have been reported that describe interventions for social determinants in primary health care or comprehensive day-to-day health care. These interventions are usually divided into three levels:
- microlevel for individual patients,
- mesolevel for medical institutions and communities and
- macrolevel for broader populations, including health care systems and administrative divisions.15, 25-28
Although such frameworks provide a blueprint for integrating SDH into health care systems, the processes by which physicians actually deliver patient care have not been described in detail. In addition, most of these frameworks have not been developed using systematic consensus group methods. Failure to describe in detail what physicians do in clinical settings reduces the value of SDH education. The process OPA for caring for patients based on an understanding of patients' social contexts and needs should therefore be explicated. This study aimed to codify the process OPA for patient care related to SDH in a primary care setting, using consensus group methods.
2 연구 방법
2 METHOD
연구 설계
Study design
일본에서 2022년 1월부터 2022년 2월까지 일차 진료 환경에서 SDH와 관련된 진료 프로세스에 대한 합의를 도출하기 위해 수정된 델파이 기법29 을 시행했습니다. 수정 델파이 연구에서는 연구자들이
- (i) 문헌 검토를 수행하거나 다른 학술적 방법을 사용하여 작성한 초기 목록을 배포하고,
- (ii) 전문가들로부터 의견을 추출하여 익명으로 반복적으로 피드백을 제공하며,
- (iii) 구조화된 방식으로 합의에 도달합니다.30
수정 델파이 기법은 전문가 합의를 도출하는 데 널리 사용되며,31-33 특히 다양한 이해관계자가 있고 익명으로 독립적인 의견 제공이 필요할 때 유용합니다.34, 35 본 연구는 델파이 연구 수행 및 보고 지침(CREDES)을 따랐습니다.36 모든 라운드에서 설문지는 웹 기반 설문조사 시스템(SurveyMonkey: Survey Monkey, Inc., San Mateo, CA, USA)을 통해 제공되었습니다. 이 연구에 대한 윤리적 승인은 도쿄대학교 의학전문대학원 및 의학부 연구윤리위원회로부터 받았습니다(제2020250NI호).
A modified Delphi technique29 was implemented from January 2022 to February 2022 in Japan to reach a consensus on the processes of medical care related to SDH in a primary care setting. In a modified Delphi study, researchers
- (i) distribute an initial list that is prepared by conducting a literature review or using other academic methods,
- (ii) extract opinions from the experts and give them anonymous feedback iteratively and
- (iii) reach a consensus in a structured way.30
The modified Delphi technique is widely used to create expert consensus,31-33 especially when there are diverse stakeholders and when anonymous and independent provision of their opinions is needed.34, 35 This study followed the Guidance on Conducting and Reporting Delphi Studies (CREDES.)36 In all rounds, questionnaires were provided via a web-based survey system (SurveyMonkey: Survey Monkey, Inc., San Mateo, CA, USA). Ethical approval for this study was obtained from the research ethics committee of the University of Tokyo Graduate School of Medicine and Faculty of Medicine (No. 2020250NI).
잠재적으로 중요한 요인 목록 작성
Compilation of a list of potentially important factors
잠재적으로 중요한 단계의 예비 목록을 작성하기 위해 2021년 9월에 제1저자가 세 개의 전자 데이터베이스(MEDLINE, CINAHL, PsycINFO)에서 문헌 검색을 수행했습니다. 검색 결과 중복을 제거한 후 447개의 논문이 확인되었습니다. 논문 제목과 초록을 기준으로 선별한 결과 110편의 논문이 선정되었습니다. 전체 텍스트 심사 후 27편의 논문이 선정되었습니다.2, 3, 12, 14, 20, 37-58 이 문헌 검색의 세부 사항은 표 S1에 나와 있습니다. 이 문헌 검색을 통해 연구자들은 '구조적 역량'이라는 용어가 자주 사용된다는 것을 재발견하고 검색 공식을 수정했습니다. 의견, 리뷰, 사설, 사례 보고서, 활동 보고서 등 다양한 종류의 논문이 포함되었습니다. SDH와 관련된 환자 치료 과정을 직접적으로 언급한 논문은 거의 없었습니다. 첫 번째 저자는 논문을 종합하여 잠정적인 목록을 작성했습니다. 두 번째, 네 번째, 다섯 번째, 여섯 번째 저자는 이 목록을 비판적으로 검토 및 분석하고 반복적인 토론을 거쳐 일부 수정을 가했습니다. 목록은 커뮤니케이션, 실천, 자기 관리, 옹호라는 네 가지 구성 요소로 나뉜 13개 항목으로 구성되었습니다(표 S2 참조).
To develop a preliminary list of potentially important steps, a literature search of three electronic databases (MEDLINE, CINAHL and PsycINFO) was conducted by the first author in September 2021. The search identified 447 articles after the removal of duplicates. The articles were screened by article titles and abstracts, and 110 articles were selected. After full-text screening, 27 articles were selected.2, 3, 12, 14, 20, 37-58 Details of this literature search are shown in Table S1. Through this literature search, researchers rediscovered that the term ‘structural competency’ was often used, and the search formula was modified. A wide range of articles was included (e.g. opinions, reviews, editorials, case reports and activity reports). Few articles directly referred to the processes of patient care related to SDH. The first author synthesised the articles and constructed a tentative list. The second, fourth, fifth and sixth authors critically reviewed and analysed the list, held iterative discussions and made some modifications. The list consisted of 13 items, which were divided into four components: communication, practice, self-management and advocacy (see Table S2).
참가자 모집
Participant recruitment
성별, 연령, 직업, 진료 환경 등 구성원의 다양성을 보장하기 위해 의도적인 샘플링 전략을 사용했습니다. 패널은 임상 전문가(의사, 간호사, 공중보건의, 사회복지사, 약사, 의료 사무원), 레지던트, 의대생, 연구자, 소외 계층 및 환자를 위한 지원 위원으로 구성되었습니다. 모집 대상을 결정한 이유는 다음과 같습니다.
- 첫째, SDoH와 관련된 일차 진료에는 의료 사무원을 포함한 여러 직종이 관여하고 있으며,59, 60 의사가 수행하는 과정을 다루는 연구에서도 다양한 의료 직종의 의견이 존중되어야 합니다.
- 둘째, 의학교육의 수요를 충족하기 위해 과정에 대한 명시적인 설명이 필요하며, 의학교육의 이해당사자인 전공의, 학생, 환자의 의견을 수렴해야 합니다.
- 셋째, SDoH와 관련된 환자 진료의 범위는 전 국민이었지만, 사회적 소외계층도 주요 이해관계자로서 본 연구에서 중요한 잠재적 의사결정권자로 고려되어야 합니다. 그러나 소외 계층을 모집하고 참여시키는 데 현실적인 어려움이 있어61, 62 연구자들은 이 연구에서 이들을 모집할 수 없었습니다. 따라서 연구자들은 공중보건간호사, 소외계층 지원위원, 사회복지사, 사회학 전문 연구자 등 소외계층의 옹호자로 간주될 수 있는 사람들에게 본 연구에 참여해 줄 것을 요청했습니다.63 연구자들은 소외계층의 의견을 물어볼 필요가 없다고 생각하지 않는다는 점을 강조해야 합니다.
A purposive sampling strategy was used to ensure member diversity, including gender, age, profession and practice setting. The panel consisted of clinical professionals (physicians, nurses, public health nurses, social workers, pharmacists and medical clerks), residents, medical students, researchers, support members for marginalised people and patients. The reasons for determining recruitment targets were as follows. First, multiple professions, including medical clerks, are involved in the primary care practice related to SDoH,59, 60 and, even in research dealing with processes undertaken by physicians, the opinions of various medical professions should be respected. Second, an explicit description of the processes was to meet the demands of medical education, and the opinions of residents, students and patients, all of whom were stakeholders in medical education, should be solicited. Third, although the scope of patient care related to SDoH was the entire population, the socially marginalised population should be considered a key stakeholder and thus an important potential decision maker in this study. However, due to practical difficulties in recruiting the marginalised population and their participation,61, 62 researchers could not recruit them in this study. Researchers thus asked public health nurses, support members for marginalised people, social workers and expert researchers in sociology, who could be considered advocators, to participate in this study.63 It should be emphasised that researchers do not believe that the opinions of marginalised people need not be asked.
우리는 SDH에 대한 깊은 이해와 상당한 실무 경험이 있는 임상 전문가, SDH에 대한 관심과 지식이 있는 레지던트 및 의대생, 만성 질환을 앓고 있고 제1저자가 근무하는 병원에 정기적으로 다니는 환자를 모집했습니다. 환자 모집 과정에서 환자의 사회적 배경과 상황은 고려하지 않았습니다. 일반 의학(일반 내과, 호스피탈리스트, 가정의학과), 소아과, 정신과, 응급의학과 의사와 간호사를 모집했는데, 이러한 전문 분야는 일반적으로 미분화 문제를 가진 환자를 진료하고 이전 연구에서 SDH를 다룰 필요가 있는 것으로 확인되었기 때문입니다.20, 39, 50, 64-67 보건의료 및 의학 교육 분야 연구자뿐만 아니라 소외된 사람들과 함께 일하는 사회학자도 모집했습니다. 소외된 사람들을 위한 지원 멤버는 비의대생 2명과 의사 및 정치인 1명으로 구성되었습니다. 이 세 명은 노숙자 및 기타 소외된 사람들을 위해 자발적으로 지원을 제공했습니다. 모든 참가자는 이 연구에 참여하기 위해 자발적으로 서면 동의를 제공했습니다. 참가자에게는 2000엔(약 15달러) 상당의 상품권으로 구성된 인센티브가 제공되었습니다.
We recruited clinical professionals who had a deep understanding and considerable practice of SDH, residents and medical students who had an interest in and some knowledge of SDH and patients who had chronic conditions and regularly attended the hospital in which the first author worked. The social backgrounds and contexts of the patients were not considered in the recruitment process. We recruited physicians and nurses in general medicine (general internal medicine, hospitalist and family medicine), paediatrics, psychiatry and emergency medicine because these specialties usually care for patients with undifferentiated problems and have been identified as needing to address SDH in previous studies.20, 39, 50, 64-67 We recruited not only researchers in health care and medical education but also sociologists working with marginalised populations. Support members for marginalised people consisted of two non-medical students and one physician and statesperson. These three members voluntarily provided support for people experiencing homelessness and other marginalised people. All participants voluntarily provided their written consent to participate in this study. An incentive comprising a gift certificate worth JPY 2000 (approximately US$ 15) was offered to participants.
데이터 수집 및 분석
Data collection and analysis
각 라운드에서 참가자들은 5점 리커트 척도(1점: 전혀 중요하지 않다 ~ 5점: 매우 중요하다)로 각 항목을 평가하도록 요청받았습니다. 또한 참가자들은 각 항목에 대한 수정 사항을 제안하고 SDH와 관련된 의료 측면에 적합하다고 생각되는 다른 단계를 추가하도록 요청받았습니다. 참가자들의 응답은 이전 검토33 및 기타 선행 연구를 바탕으로 사전 정의된 기준에 따라 분석 및 선정되었습니다.68, 69 구체적으로 (i) 평균 점수가 4점 이상, (ii) 표준편차가 1 미만, (iii) 패널의 75% 이상이 4점 또는 5점을 준 항목은 모두 통과했습니다. 참가자들은 각 설문지를 작성하는 데 2주의 시간이 주어졌습니다. 각 마감일 며칠 전에 리마인더 이메일이 발송되었습니다. 모든 저자는 모든 라운드에서 모든 서면 의견을 읽었습니다. 첫 번째, 두 번째, 세 번째 저자는 내용 분석을 사용하여 의견을 분석했습니다.70 코딩 데이터는 다른 연구자들과의 논의를 통해 축소되고 수정되었습니다. 다음 라운드가 시작될 때 이전 라운드의 익명 결과 요약본이 전문가들에게 제공되었습니다. 우리는 모든 진술이 가능한 한 높은 수준에서 합의에 도달할 수 있는 동등한 기회를 갖도록 하기 위해 일부 진술이 이미 합의에 도달했더라도 후속 라운드에서 모든 진술을 다시 포함시키기로 결정했습니다.71 각 델파이 단계는 일본어로 진행되었습니다. 결과는 연구원과 전문 번역가가 영어로 번역했습니다.
In each round, participants were asked to evaluate each item on a 5-point Likert scale (1: absolutely unimportant to 5: absolutely important). The participants were also asked to propose revisions for each item and add any other steps considered suitable for aspects of medical care related to SDH. Their responses were analysed and selected using a predefined standard based on a previous review33 and other previous studies.68, 69 Specifically, items that met all the following standards were passed: (i) a mean score of 4 or higher, (ii) a standard deviation of less than 1 and (iii) scores of 4 or 5 from 75% or more of the panellists. Participants were given 2 weeks to fill out each questionnaire. Reminder e-mails were sent a few days before each deadline. All authors read all written comments in every round. The first, second and third authors analysed the comments using content analysis.70 Coding data were collapsed and then modified through discussion with the other researchers. At the start of the subsequent round, a summary of anonymous results from the previous round was provided to the experts. We chose to include all statements again in the subsequent round (even though some had already reached consensus) to ensure that every statement had an equal chance of achieving consensus at the highest possible level.71 Each Delphi step was conducted in Japanese. The results were translated into English by the researchers and professional translators.
3 결과
3 RESULTS
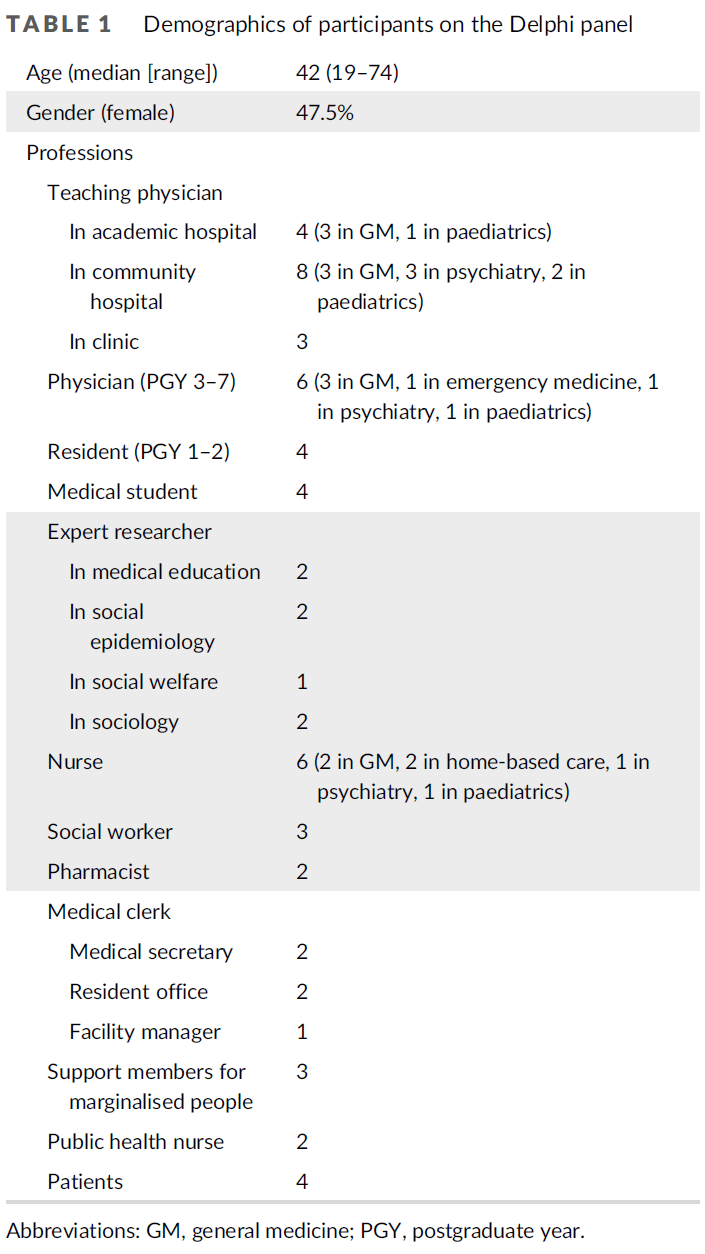
델파이 패널에는 총 63명이 모집되었으며, 이 중 61명이 참여했습니다. 2명은 업무 부담으로 인해 참여를 거부했습니다. 인구통계학적 데이터는 표 1에 나와 있습니다. 모든 참가자가 델파이 라운드를 완료했습니다.
A total of 63 people were recruited to the Delphi panel, of which 61 participated. Two declined participation because of work pressure. The demographic data are shown in Table 1. All participants completed the Delphi rounds.
1라운드에서는 초기 목록에서 탈락한 항목이 없었습니다. 동의 수준, 평균 및 표준편차는 표 S3에 나와 있습니다. 참가자들의 의견에 대한 내용 분석을 바탕으로 12개 항목이 수정되었습니다. 분석 결과에 따라 전문가 간 팀 기반 성찰에 대한 단계가 하나 추가되었고, 이에 따라 세 번째 구성 요소인 '자기 관리'를 '유지 관리'로 변경했습니다. 또한 모든 단계가 지속적인 환자-의사 관계 내에서 다른 전문가 및 이해관계자와 협력하여 수행되어야 한다는 서문을 추가했습니다(표 S4 참조).
In Round 1, no items were eliminated from the initial lists. The agreement levels, means and standard deviations are shown in Table S3. Twelve items were modified based on the content analysis of the participants' comments. According to the analysis, we drafted one new step about interprofessional team-based reflection and accordingly changed the third component ‘self-management’ to ‘maintenance’. We also developed a preface that stated that all steps should be conducted within an ongoing patient–physician relationship and in collaboration with other professionals and stakeholders (see Table S4).
2라운드 이후, 수정된 모든 항목이 긍정적인 합의 기준을 충족하는 것으로 확인되었습니다(표 S5 참조). 일부 사소한 수정이 이루어졌으며 모든 참가자의 승인을 받았습니다. 3라운드는 진행되지 않았습니다. 최종 버전의 목록은 14개 항목으로 구성되었으며, 이는 4개의 구성 요소로 나뉩니다(표 2).
After Round 2, all modified items were confirmed to meet the positive consensus standard (see Table S5). Some minor revisions were made and were approved by all participants. Round 3 was not performed. The final version of the list consisted of 14 items, which were divided into four components (Table 2).

4 토론
4 DISCUSSION
이 연구에서는 SDH와 관련된 환자 치료의 OPA 프로세스를 확인했습니다. 프로세스는 커뮤니케이션, 진료, 유지 관리, 옹호라는 네 가지 구성 요소로 분류되었습니다. 각 구성 요소는 서로 밀접한 관련이 있습니다. 커뮤니케이션은 좋은 진료에 기여합니다. 의사 자신과 팀원을 위한 유지 관리는 좋은 의사 소통과 진료의 기본입니다. 커뮤니케이션, 진료, 유지보수에 대한 경험은 옹호에 동기를 부여할 수 있습니다. 이 커뮤니케이션-실무-유지-옹호(CPMA) 프레임워크(그림 1 참조)는 이전에 보고된 접근 방식과 몇 가지 요소를 공유합니다. 예를 들어, 빈곤 아동 간호와 관련된 역량은 환자 간호, 대인관계 및 의사소통 기술, 전문성, 시스템 기반 실무 영역과 관련이 있습니다.39, 72 또한 간호 교육 전문가들은 환자의 기저질환을 변화시키고 건강 형평성을 증진하기 위해 비판적 돌봄 접근법과 세심한 권한 부여 간호 제공을 제안해 왔습니다.55, 73
This study identified the process OPA for patient care related to SDH. The processes were classified into four components: communication, practice, maintenance and advocacy. Each component is closely related to each other. Communication contributes to good practice. Maintenance for physicians themselves and team members is the base of good communication and practice. Experience about communication, practice and maintenance may motivate advocacy. This Communication–Practice–Maintenance–Advocacy (CPMA) framework (see Figure 1) shares some elements with previously reported approaches. For example, the competency relevant to the care of children in poverty is related to the domains of patient care, interpersonal and communication skills, professionalism and system-based practice.39, 72 In addition, professionals in nursing education have proposed a critical caring approach and provision of sensitive empowering care to change patients' underlying conditions and promote health equity.55, 73

CPMA 프레임워크에는 몇 가지 독특한 장점이 있습니다.
- 첫째, 전문가 패널은 다양한 이해관계자로 구성됩니다. 환자, 사회학자, 소외된 사람들을 위한 지원 단체의 참여로 패널의 다양성이 증가했습니다.
- 둘째, 프레임워크는 환자 치료 과정을 상세하게 설명하여 의학교육에 대한 활용도를 높였습니다.
[생물 의학 및 기술 중심의 지배적인 커리큘럼 패러다임]은 정답을 얻고 문제를 해결하는 데 중점을 둡니다. 이 패러다임에서 학습자는 SDH와 같이 확실성이 낮은 문제에 직면할 때 불편함을 느낄 수 있습니다.74, 75 문제를 해결하는 과정을 명시하면 이러한 불편함을 줄일 수 있습니다.17, 20 이 프레임워크는 잠재적으로 학습자에게 명확한 지표를 제공하고 임상 실습 및 현장 기반 평가에 반영하는 데 적용될 수 있습니다.
The CPMA framework has some unique advantages.
- First, the expert panel consisted of various stakeholders. The participation of patients, sociologists and support members for marginalised people increased panel diversity.
- Second, the framework clearly described in detail the patient care processes to increase its availability for medical education.
The dominant curriculum paradigm, which is centred on biomedicine and technology, focuses on obtaining correct answers and solving problems. In this paradigm, learners may feel uncomfortable when facing challenges with low levels of certainty, such as SDH.74, 75 Making explicit the process of tackling challenges could potentially reduce this discomfort.17, 20 This framework potentially provides learners with a clear indication and could be applied to reflection on their clinical practice and workplace-based assessment.
의사소통
Communication
이 구성 요소에는 환자와의 커뮤니케이션과 다른 전문가 및 이해관계자와의 커뮤니케이션이 모두 포함됩니다. 델파이 라운드에서는 환자에 대한 의사의 편견과 태도에 대한 의견이 나왔습니다. 예를 들어, 패널리스트들은 첫 번째 목록의 일부 항목('의사는 공동 의사 결정을 수행한다', '의사는 환자가 자신의 건강 상태에 대처할 수 있도록 적절한 설명과 지원을 제공한다')에 가부장적인 측면이 포함되어 있다고 지적했습니다. 일부 패널리스트는 의사 자신의 편견과 편견에 대한 의사의 인식이 언급되어야 한다고 제안했습니다. 이러한 편견과 태도는 항상 관찰할 수 있는 것은 아니지만, 환자 중심주의,49 다른 전문가와의 협력76 및 환자 결과를 저해할 수 있으므로76-78 의사소통 관련 교육 및 실습에서 심각하게 고려해야 합니다. 이 구성 요소는 의사소통에 대한 자세한 내용을 설명하며 효과적인 교육 및 평가에 기여할 수 있습니다.
This component includes both communications with patients and communications with other professionals and stakeholders. The Delphi rounds revealed opinions about physicians' biases and attitudes towards patients. For example, panellists pointed out that some of the items in the first list (‘The physician performs shared decision making’ and ‘The physician provides adequate explanation and support to help the patient deal with their health condition’) included some paternalistic aspects. Some panellists suggested that physicians' awareness of their own prejudice and biases should be mentioned. Although these biases and attitudes are not always observable, they may impair patient-centredness,49 collaboration with other professionals76 and patient outcomes76-78 and should thus be seriously considered in communication-related education and practice. This component illustrates detailed content about communication and may contribute to effective education and assessment.
실습
Practice
이 구성 요소는 의사가 환자 진료를 위해 진료실에서 실제로 하는 일을 설명합니다. 목록의 각 단계는 의사가 수행하는 활동의 관점에서 설명되었습니다. 이는 의사가 특권적인 위치에 있다는 것을 의미하지는 않습니다. 델파이 라운드에서 두 가지 관련 의견이 발견되었습니다.
- 첫째, 사회적 요구가 충족되지 않은 환자를 진료할 때 환자 중심 진료를 고려하는 것이 특히 중요합니다. 의사는 지시적이고 억압적인 방식으로 말함으로써 그러한 환자의 권한을 박탈하는 경향이 있기 때문에 이 점을 강조해야 합니다.79-81
- 둘째, 의사가 환자의 사회적 상황에 혼자 대처할 수 없으므로 다학제 간 협업의 중요성을 강조해야 합니다. 이러한 의견은 의료 시스템에서 일어나는 일은 환자에게 일어나는 일의 일부에 불과하다는 사실을 강조합니다.54 이러한 전문가들의 견해에 따라 이 구성 요소는 종단적이고 포괄적이며 팀 기반의 접근 방식이 필요하다고 주장합니다. 사회적 어려움을 포함한 복잡한 문제는 단기간에 해결되는 경우가 드물고 안정화가 더 적절한 목표인 경우가 많기 때문에 문제 해결을 요구하지 않습니다.82
This component illustrates what physicians actually do in the office for patient care. Each step on the list was described in terms of the activities performed by physicians. This does not imply that physicians are in a privileged position. The Delphi rounds uncovered two related opinions.
- First, it is particularly important to consider patient-centred care when seeing patients with unmet social needs. This should be emphasised because physicians tend to disempower such patients by speaking in a directive and oppressive manner.79-81
- Second, a physician cannot cope alone with patients' social circumstances, and the importance of interdisciplinary collaboration should be emphasised. These opinions underlined the fact that what happens in the health care system is only part of what happens to the patient.54 Under these expert views, this component insists that a longitudinal, comprehensive and team-based approach is needed. It does not ask for problem solving because complex problems, including social difficulties, are rarely resolved over a short period, and stabilisation is often a more appropriate goal.82
유지 관리
Maintenance
이 구성 요소는 전문가의 소진을 완화하고 환자 치료의 질을 유지 및 개선하기 위해 의사가 진료실 밖에서 하는 일을 보여줍니다. 환자의 사회적 요구 해결과 관련된 소진83-85은 자가 모니터링38 및 팀 빌딩을 통해 줄일 수 있습니다.86, 87 이 구성 요소는 다른 공개된 프레임워크와 비교하여 독특하며 수련의와 임상 감독자에게 새롭고 필수적인 통찰력을 제공할 수 있습니다.
This component illustrates what physicians do outside their office to mitigate professionals' burnout and then maintain and improve the quality of patient care. Burnout associated with addressing patients' social needs83-85 can be reduced by self-monitoring38 and team building.86, 87 This component is unique compared with other published frameworks and may give novel and essential insights to trainees and clinical supervisors.
옹호
Advocacy
의료 전문가들 사이에서 윤리적 가치와 인권에 대한 존중 부족은 건강 형평성에 대한 도전이며,88 건강 옹호는 의사에게 중요한 역량으로 간주되어야 합니다.89 그러나 건강 옹호에 대한 정의가 불분명하여 이 영역을 가르치고 평가하기 어려운 경우가 있습니다.90 [미시적 수준과 거시적 수준의 사회적 책임]에 대한 강조가 증가하고 있지만,91 일부 의사들은 옹호를 [사회 시스템의 개선이 아닌 개별 환자에게 적절한 치료를 제공하는 것]으로 생각했습니다.92,93 델파이 라운드에서는 개별 의사가 실행하는 옹호의 실현 가능성에 대한 몇 가지 의문이 제기되었습니다. 예를 들어, 사회 및 지역사회 구조의 변화는 개별 의사의 범위를 벗어난 것으로 판단되었습니다. 일부 전문가들은 일부 수련의, 특히 초심자들이 시스템 차원의 문제를 지나치게 강조하는 것에 대해 거부감을 나타낼 수 있다고 주장했습니다. 의대생을 대상으로 한 이전 연구에서도 비슷한 질문이 제기되었습니다: 학생들은 의사가 개별 환자를 옹호해야 한다는 데는 반대하지 않았지만, 옹호와 관련된 어려움을 예상했습니다.94 본 연구는 의사가 임상 환경에서 실천할 수 있고 실천해야 하는 옹호의 구체적인 측면에 대한 합의를 보여주었습니다. 예를 들어, 의료 시스템 내에서 접근성을 저해하는 요인을 파악하는 것은 일차 진료에 종사하는 모든 의사가 수용할 수 있는 것으로 판단되었습니다.
A lack of respect for ethical values and human rights among health professionals is a challenge for health equity,88 and health advocacy should be considered an important competency for physicians.89 However, definitions of health advocacy are sometimes unclear, which makes it difficult to teach and assess this domain.90 Although an increasing emphasis on mesolevels and macrolevels of social accountabilities has been put,91 some physicians thought of advocacy as the delivery of appropriate care for individual patients rather than an improvement in social systems.92, 93 The Delphi rounds generated some questions about the feasibility of advocacy as practised by individual physicians. For example, changing social and community structures was judged to be beyond the scope of individual physicians. Some experts insisted that some trainees, especially novices, may express a refusal of excessive emphasis on system-level challenges. A previous study of medical students raised similar questions: Although students did not disagree that physicians should advocate for individual patients, they anticipated challenges related to advocacy.94 The present study demonstrated a consensus on the specific aspects of advocacy that physicians can and should practise in clinical settings. For example, identifying factors that impede access within their health care system was judged to be acceptable for all physicians in primary care.
이 연구에는 몇 가지 한계가 있었습니다.
- 첫째, 모든 저자와 참여자가 일본에 거주하고 일하고 있습니다. 일본 상황과 관련된 환자 치료 측면에만 초점을 맞추지 않았기 때문에 이러한 연구 결과를 다른 국가에 일반화할 수 있을지는 불확실합니다. 일본은 보편적 의료 서비스와 잘 발달된 사회 보장 시스템으로 유명하지만, 사회 및 건강 불평등이 여전히 존재합니다.95 예를 들어, 일본의 상대적 빈곤층 비율은 2016년에 16%로 경제협력개발기구 평균인 11%보다 높았습니다.95 한부모 가구의 비율은 2013년에 50.8%로 가장 높았습니다.96 이러한 사회 경제적 불평등은 건강 결과를 손상시킵니다.98-101 본 연구 결과는 고소득 국가에서도 SDH 해결이 중요하다는 점을 강조합니다. 또한 일본에는 다양한 인종과 민족 정체성을 가진 사람들이 살고 있지만 대다수는 같은 인종과 민족입니다. 연구자들은 패널리스트의 인종 및 민족 정체성에 대해 묻지 않았지만, 아마도 거의 모든 패널리스트가 아시아인이었을 것으로 추정됩니다. 이 결과를 다른 문화와 국가에 적용할 때는 이러한 사실에 유의해야 합니다.
- 둘째, 각 라운드의 찬성률이 일관되게 높았다는 점입니다. 이는 임상에서 SDoH를 다루는 것이 정치적으로나 윤리적으로 옳은 것처럼 보이기 때문일 수 있으며, 참가자들은 제안된 항목을 거부하거나 거부하지 않으려는 경향이 있었습니다. 패널들의 의견에 대한 질적 분석은 상호보완적으로 작용하여 연구자들이 참가자들의 중요한 아이디어를 연구 결과에 반영하는 데 도움이 되었습니다.
- 셋째, 돌봄의 과정을 항목화하는 데에는 불가피한 한계가 있습니다. 일련의 과정이 미리 정해져 있고 불변하며 엄격하게 따라야 한다는 것은 오해입니다. 모든 환자는 고유한 사회적 맥락을 가지고 있으며, 의사와 이해관계자는 복잡한 사회적 결정 요인을 시급히 해결하기 위해 비판적이고 창의적인 사고의 중요성을 인식해야 합니다.
- 40 넷째, 이 연구는 치료 과정에서 관찰 가능한 단계만을 조사했습니다. SDH를 충분히 다루기 위해서는 전문가가 자신의 편견을 인식하는 능력과 같이 관찰할 수 없는 진료의 측면을 조사할 필요가 있습니다.40, 42, 45, 50, 77
- 다섯째, 이 연구에 참여한 환자 수가 적었습니다. 다른 전문가와 동등한 수준의 연구 참여에 대한 부담감이 환자 참여에 장애가 될 수 있습니다. 환자의 참여와 파트너십이 촉진되어야 하며,102, 103 새로 개발된 프레임워크는 보다 현실적이고 실질적인 방식으로 환자의 의견을 수렴하는 추가 연구를 통해 개선되어야 합니다.104 특히 소외된 환자들의 의견을 반영할 수 있는 잘 설계된 연구가 필요합니다.105, 106
This study had several limitations.
- First, all authors and participants live and work in Japan. Although we did not focus only on aspects of patient care specific to the Japanese situation, it is uncertain whether these findings can be generalised to other countries. Although Japan is known for its universal health care and well-developed social security systems, social and health inequities still exist.95 For example, the proportion of people with relative poverty in Japan was 16% in 2016, higher than that of the Organization for Economic Co-operation and Development average of 11%.95 This proportion among single-parent households was 50.8% in 2013,96 which was the highest.97 These socio-economic inequities impair health outcomes.98-101 The present findings highlight the importance of addressing SDH even in high-income countries. In addition, although people with various racial and ethnic identities live in Japan, the majority are of the same race and ethnicity. Researchers did not ask about panellists' racial and ethnic identities, but, presumably, almost all of the panellists were Asian. These facts should be noted when adapting the result to other cultures and countries.
- Second, the approval rates of each round were consistently high. It may be that addressing SDoH in clinical practice sounds politically and ethically correct, and participants tended to avoid denying and refusing proposed items. Qualitative analysis of the panellists' comments functioned complementarily, and it helped researchers to reflect participants' important ideas to the result.
- Third, there are inevitable limitations in itemising the process of care. It is a misapprehension that a series of processes is predetermined and immutable and should be strictly followed. Every patient has a unique social context, and physicians and stakeholders must be aware of the importance of critical and creative thinking to urgently address complex social determinants.40
- Fourth, this study examined only observable steps in the processes of care. To fully address SDH, it is necessary to investigate unobservable aspects of care, such as professionals' ability to recognise their own biases.40, 42, 45, 50, 77
- Fifth, the number of patients who participated in this study was a few. The burden of participating in research, which was equivalent to other professionals, might be a barrier to patient participation. Patient involvement and partnerships should be promoted,102, 103 and this newly developed framework should be refined by further research that gathers patient feedback in a more realistic and practical manner.104 In particular, well-designed research to reflect the opinions of marginalised patients is needed.105, 106
저희는 OPA 과정을 설명하는 것이 SDH에 대한 대학원 교육을 개선하는 데 중요한 단계라고 생각합니다. 이러한 연구 결과는 몇 가지 임상적 함의를 가지고 있습니다.
- 첫째, 건강 상태 불평등의 근원은 부와 권력의 불평등한 분배에 있지만, 많은 개입이 불평등 문제를 개인화하여 개인의 행동을 주요 해결책으로 삼고 있습니다. 이러한 접근 방식은 '판타지적 패러다임'이라는 비판을 받아야 합니다.107 이 연구는 의사가 개별 환자와 관련된 SDH를 해결하는 방법에 중점을 두었지만, 우리는 이러한 문제의 상위 원인을 이해하는 것이 중요하다는 것을 인식하고 있습니다. SDH의 상류 측면을 고려하는 것은 맥락화된 진료에 필수적입니다.3
- 둘째, CPMA 프레임워크는 일차 진료에 종사하는 모든 의사의 기본 요구 사항을 설명합니다. 전문 진료를 위해서는 보다 전문화된 역량이 필요합니다.108-111 의사는 특히 소외된 인구에게 진료를 제공할 때 이 목록 이상의 것을 목표로 해야 합니다.112-114
We believe that describing process OPA is an important step towards improving postgraduate education about SDH. These findings have several clinical implications.
- First, although the root of health status inequity is in the unequal distribution of wealth and power, many interventions personalise the problem of inequality and target individual behaviour as the main solution. This approach should be criticised as a ‘fantasy paradigm’.107 Although this study focused on how physicians address SDH related to individual patients, we recognise the importance of understanding upstream causes of these problems. A consideration of the upstream aspects of SDH is essential to contextualised care.3
- Second, the CPMA framework describes basic requirements for all physicians in primary care. More specialised competency is needed for expert practice.108-111 Physicians should aim beyond the list, especially when delivering care to marginalised populations.112-114
OPA는 수련의 평가 계획에 적절하게 매핑되어 있다면 평가할 수 있습니다.22 따라서 CPMA 프레임워크를 사용하는 평가 방법은 다른 맥락에서 개발 및 검증되어야 합니다. 이 프레임워크 실행의 교육 효과는 환자가 보고한 결과를 사용하여 평가해야 합니다. 또한, 이 프레임워크가 공유된 의사결정 및 환자 중심주의를 포함한 다른 환자 치료 영역과의 연관성을 확인해야 합니다.
OPA can be assessed if they are appropriately mapped in a trainee assessment plan.22 Thus, assessment methods using the CPMA framework should be developed and validated in other contexts. The educational effectiveness of implementing this framework should be evaluated using patient-reported outcomes. Additionally, the association of this framework with other realms of patient care, including shared decision making and patient-centredness, should be confirmed.
5 결론 5 CONCLUSION
수정된 델파이 기법을 사용하여 SDH와 관련된 환자 치료를 위한 프로세스 OPA를 설명했습니다. CPMA 프레임워크는 SDH 관련 의료 교육을 개선하는 데 도움이 될 수 있습니다. 다른 맥락에서 추가 검증, 구현 및 탐색을 위해서는 추가 연구가 필요합니다.
Using the modified Delphi technique, the process OPA for patient care related to SDH was described. The CPMA framework could help to improve medical education in SDH. Further research is needed for further validation, implementation and exploration in other contexts.
Defining the observable processes of patient care related to social determinants of health
Affiliations collapse
PMID: 35953461
DOI: 10.1111/medu.14915
Abstract
Introduction: An understanding of social determinants of health (SDH) and patients' social circumstances is recommended to deliver contextualised care. However, the processes of patient care related to SDH in clinical settings have not been described in detail. Observable practice activities (OPAs) are a collection of learning objectives and activities that must be observed in daily practice and can be used to describe the precise processes for professionals to follow in specific situations (process OPA.) METHODS: We used a modified Delphi technique to generate expert consensus about the process OPA for patient care related to SDH in primary care settings. To reflect the opinions of various stakeholders, the expert panel comprised clinical professionals (physicians, nurses, public health nurses, social workers, pharmacists and medical clerks), residents, medical students, researchers (medical education, health care, sociology of marginalised people), support members for marginalised people and patients. The Delphi rounds were conducted online. In Round 1, a list of potentially important steps in the processes of care was distributed to panellists. The list was modified, and one new step was added. In Round 2, all steps were acknowledged with few modifications.
Results: Of 63 experts recruited, 61 participated, and all participants completed the Delphi rounds. A total of 14 observable steps were identified, which were divided into four components: communication, practice, maintenance and advocacy. The importance of ongoing patient-physician relationships and collaboration with professionals and stakeholders was emphasised for the whole process of care.
Discussion: This study presents the consensus of a variety of experts on the process OPA for patient care related to SDHs. Further research is warranted to investigate how this Communication-Practice-Maintenance-Advocacy framework could affect medical education, quality of patient care, and patient outcomes.
© 2022 Association for the Study of Medical Education and John Wiley & Sons Ltd.
'Articles (Medical Education) > 교육과정 개발&평가' 카테고리의 다른 글
| 의학교육은 정보시대에서 인공지능시대로 옮겨가야 한다(Acad Med, 2018) (0) | 2023.07.07 |
|---|---|
| 사회적 책무성 프레임워크와 그것이 의학교육과 프로그램 평가에 갖는 함의: 내러티브 리뷰(Acad Med, 2020) (0) | 2023.07.07 |
| 보건의료전문직이 인공지능-기반 도구를 사용하기 위한 역량(Acad Med, 2023) (0) | 2023.05.25 |
| 필요하지만 충분하지 않고, 어쩌면 반생산적인 것: 강의평가의 복잡한 문제(Acad Med, 2023) (0) | 2023.05.14 |
| 의학교육의 문턱개념: 스코핑 리뷰(Med Educ, 2022) (0) | 2023.05.04 |