CanMEDS 2025에서 형평성, 다양성, 포용성, 사회적 정의 (Can Med Educ J. 2023)
Equity, diversity, inclusion, and social justice in CanMEDS 2025
소개
Introduction
의료 분야의 사회 정의는 각 개인이 속한 다양한 공동체에 관계없이 건강, 복지, 기회 및 특권에 대한 권리가 다른 사람과 동일하다는 것을 지지합니다.1 사회 구조의 모든 측면에서 배제는 다수 인구의 권력을 확보하는 수단이 되어 왔으며, 의료 인력 구성2과 다양한 인구 및 지역사회의 환자에게 제공되는 치료의 가용성과 질 모두에 명백한 영향을 미쳤습니다.3,4 의사 인력은 성별 및 젠더, 원주민으로서의 정체성 또는 비주류 인종, 민족, 문화 또는 종교 집단에 속하는 경우, 다양한 능력, 가족의 사회경제적 지위 등 여러 인구집단을 과소 대표하고 있는 것으로 알려져 있습니다.5,6
Social justice in medicine upholds that each individual, regardless of the diverse communities to which they may belong, has the same right to health, wellbeing, opportunities and privilege as another.1 Exclusions in all aspects of societal structure have been a means to secure power for the majority population in Canada, and have unequivocally impacted medicine both through the composition of the medical workforce2 and the availability and quality of care provided to patients of diverse populations and communities.3,4 The physician workforce is recognized to have underrepresentation of several populations including those defined
- by their sex and gender;
- their identity as an Indigenous person or belonging to non-dominant racialized, ethnic, cultural or religious groups;
- by various abilities; and
- by familial socioeconomic status.5,6
이들 및 기타 억압받는 인구집단의 구성원들은 의학 교육 과정에서 불이익, 차별, 배제를 경험하고 있습니다7. 의학교육 시스템은 능력주의를 강화하고, 위계를 지지하며, 인구 집단 간의 차이를 영속화하고, 다른 지식을 배제하는 생물의학 모델을 장려하기 위해 구축되었습니다.8 캐나다 의료 시스템은 보편적 접근의 원칙에 기초하고 있지만, 의료 시스템에서 인종주의, 성차별, 젠더차별, 능력주의, 연령주의 등 여러 형태의 차별과 그 교차점9에서 겪는 피해에 대해 이용 가능한 치료를 받는 것의 이점을 반드시 평가해야 하는 환자들의 실제 경험과는 다른 경우가 많습니다. 이러한 환자들은 다른 환자들과 동일한 수준의 치료를 받지 못하며10 그 결과 더 나쁜 건강 결과를 겪습니다.11 일부 지역에서는 결과의 격차가 더 커지고 있습니다.11
The experiences of members of these and other oppressed populations throughout their medical training are of disadvantage, discrimination, and exclusion 7. Medical education systems have been constructed to reinforce meritocracy, support hierarchy, perpetuate differences between population groups, and promote the biomedical model to the exclusion of other knowledges.8 The Canadian health care system is founded on the principle of universal access, yet this is often not the lived experience of patients who necessarily assess the benefits of seeking available care against the harms of racism, sexism, genderism, ableism, and ageism among other forms of discrimination, and all their intersections,9 they suffer in the healthcare system. These patients are not afforded the same quality of care as others10 and suffer worse health outcomes as a result.11 In some areas, the gap in outcomes is widening.11
의료계의 변화에 대한 오랜 요구가 행동의 우선순위로 떠오른 지금,12 기존의 CanMEDS 의사 역량 프레임워크는 형평성, 다양성, 포용성, 사회 정의의 개념과 관련된 의사에 대한 기대치를 명시적으로 제시하는 방향으로 발전할 필요가 있습니다.13 우리는 여기서 이러한 개념을 검토하고, 의학교육(모든 저자), 연구(CB, ND, KOT), 임상 진료(모든 저자)에서 형평성 및 반인종주의 이니셔티브의 리더로서의 경험과 캐나다의 원주민(CB), 아프리카계 캐나다인(KOT), 소수 인종(JMM, SR, BMW), 의학계 여성(CB, ND), 장애인(ND)으로서 살아온 경험을 바탕으로 CanMEDS 의사 역량 프레임워크에 통합하기 위한 권고사항을 제시합니다. 독자들은 반인종주의에 대해 구체적으로 다룬 원고도 참고하시기 바랍니다.14,15
With the long call for changes in medicine now prioritized for action,12 the existing CanMEDS physician competency framework requires evolution with explicit statements for expectations of physicians related to concepts of equity, diversity, inclusion and social justice.13 We review these concepts here and provide recommendations for incorporating these in the CanMEDS physician competency framework drawn from our experiences as leaders in equity and anti-racism initiatives in medical education (all authors), research (CB,ND,KOT), and clinical practice (all authors) as well as our lived experiences as persons of Indigenous (CB), African-Canadian (KOT), and racial minorities in Canada (JMM, SR, BMW), women in medicine (CB, ND), and disabled (ND). We direct readers to also refer to the manuscripts that speaks specifically on the topic of anti-racism.14,15
형평성, 다양성, 포용성, 사회 정의란 무엇이며 의사의 역량에 중요한 이유는 무엇인가요?
What are equity, diversity, inclusion, and social justice and why are they important to physician competency?
형평성, 다양성, 포용성, 사회 정의는 차별을 해결한 결과로 간주되어야 합니다.
- (모든 사람에게 동일한 분배를 제공하는 평등equality과는 구별되는) 형평성equity은 개인이 한 집단 또는 다수의 집단에 속해 있다는 이유만으로 기회가 줄어들 뿐만 아니라 다른 구조적, 제도적 장벽에 직면하기 때문에 공정성fairness을 달성하는 데 필요한 행동에 차이가 있을 수밖에 없음을 인정합니다.16
- 다양성은 집단 내 모든 인구의 대표성을 높이고, 변화와 가능성이 무한하며, 다양한 지식과 경험에서 비롯된 관점과 혁신의 기회를 제공하는 것을 의미합니다.17
- 포용성은 집단 내 다양한 인구 구성원의 존재뿐만 아니라 그 경험의 성격을 말하며, 그들이 그 집단에서 지지받고 가치 있는 구성원이라고 평가하는 것을 말합니다.18
- 사회 정의는 각 개인이 다른 사람과 동일한 건강, 복지, 기회 및 특권을 가져야 한다는 권리 기반 접근 방식에서 개념화됩니다.1
Equity, diversity, inclusion, and social justice are to be considered outcomes of addressing discrimination.
- Distinct from equality (which is the same distribution for everyone), equity necessarily accepts there will be variations in actions required to attain fairness, as individuals encounter different structural and systemic barriers as well as reduced opportunities simply by virtue of their membership in a or many population(s).16
- Diversity refers to enhanced representation of persons from all populations in a collective, limitless in variations and possibilities, and yielding the opportunity for perspectives and innovations arising from multiple knowledges and experiences.17
- Inclusion speaks not only to the presence of but also the nature of the experience of members of diverse populations in a collective, and that they assess they are a supported and valued member of that collective.18
- Social justice is conceptualized from a rights-based approach, valuing that each individual should have the same health, wellbeing, opportunities and privilege as another.1
이러한 용어 및 관련 용어에 대한 간략한 정의는 표 1에서 확인할 수 있습니다.
Concise definitions of these and related terms are provided in Table 1.
| 용어 정의 Term |
Definition |
| Ableism | 에이블리즘 모든 형태의 장애(예: 신체적, 지적)를 가진 사람에 대한 차별 및/또는 편견. 장애를 가진 사람을 비장애인에 비해 열등한 존재로 규정하는 것입니다. Discrimination and/or prejudice against persons with any form of disability (e.g., physical, intellectual). Persons are defined by their disabilities, and are characterized as inferior to the non-disabled. |
| Ageism | 연령 차별 일반적으로 나이가 많은 사회 구성원에 대한 고정관념, 차별 및/또는 편견, 나이를 기준으로 한 사람에 대한 고정관념, 차별 및/또는 편견입니다. Stereotyping, discrimination and/or prejudice against persons on the basis of their age, typically against older members of society. |
| Accessibility | 접근성 참여의 장벽을 제거하여 모든 사람이 참여할 수 있는 환경을 조성하기 위한 편의 제공. Accommodations are made to remove barriers to participation, resulting in the ability for all to participate. |
| Anti-oppression | 반억압 억압 체제에 도전하는 전략, 이론, 행동 및 관행 The strategies, theories, actions, and practices that challenge systems of oppression |
| Cultural Safety | 문화적 안전 서비스 제공자와 조직이 불평등을 야기하는 편견과 장벽을 해소하는 성찰적이고 인식 있는 관행과 정책의 결과물입니다. 문화적 안전의 존재 여부를 결정하는 것은 서비스 제공자가 아니라 서비스를 받는 사람입니다. An outcome of reflective and aware practice and policy, where providers and organizations address bias and barriers contributing to inequities. It is the recipient of care, and not the provider, who determines if cultural safety is present or not. |
| Decolonization | 탈식민지화 사회 구조, 서비스 및 투자에 대한 자결권을 위한 고유한 권리와 권한을 회복합니다. Regaining inherent rights and power for self-determination of societal structure, services and investments. |
| Diversity | 다양성 집단 내에 가능한 한 다양한 속성이 존재합니다. The greatest possible representation of attributes are present within the collective. |
| Equity | 형평성 불균형이 해소된 공정성과 정의의 달성. Attainment of fairness and justice, with imbalances addressed. |
| Homophobia | 동성애 혐오 레즈비언, 게이, 퀴어 또는 양성애자라는 이유로 사람을 향한 고정관념, 차별 및/또는 편견. Stereotyping, discrimination and/or prejudice against persons on the basis of being lesbian, gay, queer or bisexual. |
| Inclusion | 포용성 모든 사람이 동등하게 환영받고, 지원받고, 가치를 인정받고, 존중받을 수 있도록 보장하는 행동과 접근 방식. Acts and approaches that ensure that all persons are equally welcomed, supported, valued and respected. |
| Intersectionality | 교차성 불평등에 직면한 여러 인구집단의 일원이 됨으로써 발생하는 상호 작용 또는 시너지 효과로 인해 독특한 경험을 할 수 있습니다. Interactions or synergies which arise from being a member of multiple populations facing inequities, and which results in a unique experience. |
| Meritocracy | 능력주의 능력과 성과에 따라 기회와 지위를 부여하지만 모든 사회 구성원의 기회를 제한하는 구조적 불평등을 인정하지 않는 시스템. System of awarding opportunities and status on the basis of ability and performance, but which neglects acknowledging structural inequities that limit opportunities for all members of society. |
| Racism | 인종차별 인종을 이유로 한 사람에 대한 고정관념, 차별 및/또는 편견. Stereotyping, discrimination and/or prejudice against persons on the basis of their race. |
| Sexism | 성차별 성별에 따른 고정관념, 차별 및/또는 편견 일반적으로 여성으로 식별되는 개인에 대한 편견. Stereotyping, discrimination and/or prejudice against persons on the basis of their sex typically against those individuals that identify as women. |
| Genderism | 젠더차별 젠더에 근거한 사람에 대한 고정관념, 차별 및/또는 편견. Stereotyping, discrimination and/or prejudice against persons on the basis of their gender. |
| Social justice | 사회 정의 각 개인이 경제적, 정치적, 사회적 권리와 기회를 모두 누릴 권리가 있다는 것을 장려하는 접근 방식. Approach promoting that each person has the right to the full spectrum of economic, political, and social rights and opportunities. |
의사 인력 및 다양한 배경을 가진 환자에게 제공되는 의료 서비스 모두에서 권력과 특권의 불균형에 대한 인식이 증가하고 있지만, 의사는 기존의 불평등을 식별하거나 사회 정의 목표를 향한 진전을 방해하는 복잡한 요인을 이해하도록 타고나지 않았다.19 의사는 의사 동료와 환자 모두를 위한 동맹allies으로서 정보에 기반한 근거 기반 조치를 취하는 데 필요한 기술을 개발해야 합니다.2
While there is increasing recognition of the power and privilege imbalances in both the physician workforce and the care provided to patients from diverse backgrounds, physicians are not intrinsically able to identify existing inequities, nor understand the complex contributors impeding progress towards social justice goals.19 Physicians need to develop the necessary skills to take informed and evidence-based action as allies for both physician colleagues and patients.2
형평성, 다양성, 포용성, 사회 정의는 2015 CanMEDS 역량 프레임워크에서 어떻게 표현됩니까?
How are equity, diversity, inclusion, and social justice represented in the 2015 CanMEDS competency framework?
CanMEDS 2015 의사 역량 프레임워크에는 의사 인력 및 환자 치료와 관련된 형평성, 다양성, 포용성 및 사회 정의와 관련된 추론이 있지만(표 2A 및 및2B),2B) 명시적으로 다루고 있는 경우는 드뭅니다. 특히, 이 역량들은 의료계, 더 넓게는 사회에 만연한 차별적 신념 및/또는 관행의 존재를 인정하지 않으며, 의사가 사회 정의를 증진하는 활동을 지원하거나 주도하는 데 유능해야 한다는 명시적인 기대치를 제시하지 않습니다. '리더' 및 '건강 옹호자' 측면의 기존 역량 중 적절하고 권한을 부여하는 의사 교육 및 근무 환경 유지와 관련된 내용은 없습니다. 이는 우리 직업에서 배제를 더욱 영속화하고, 다양하고 포용적인 의료 인력을 확보하기 위해 채용과 유지를 지원하는 데 형평성 이니셔티브가 필요하다는 점을 강조하지 않으며, 의학교육에 내재된 위계질서를 해체하는 데 기여하지도 않습니다.8
There are inferences relevant to equity, diversity, inclusion and social justice related to both the physician workforce and patient care in the CanMEDS 2015 physician competency framework (Table 2A and and2B),2B), but they are rarely explicitly addressed. Specifically, the competencies do not acknowledge the existence of discriminatory beliefs and/or practices rampant in medicine specifically and more broadly in society, and do not set out explicit expectations for physicians to be competent in supporting or leading activities that promote social justice. None of the existing competencies in ‘leader’ and ‘health advocate’ aspects related to upholding appropriate and empowering physician training and work environments. This further perpetuates exclusions in our profession and does not reinforce that equity initiatives are necessary to support recruitment and retention to achieve a diverse and inclusive medical workforce, nor contribute to dismantling the hierarchy inherent in medical education.8

이번 호 캐나다 의학교육 저널에 게재된 논문에서 Adam 외21는 CanMEDS 역할 설명 및 역량에서 '환자'라는 용어가 어떻게 언급되는지를 강조합니다. 역할 설명에서 환자를 치료의 파트너로 포지셔닝하는 경우가 많지만, 건강 옹호자 역량을 제외한 다른 역할의 핵심 및 활성화 역량에서는 환자를 정보와 치료의 수동적인 수신자로 포지셔닝합니다. 이러한 관점에서 볼 때, 이러한 역량은 지속적인 차별을 허용하는 방식으로 기존의 권력 불균형을 악화시키는 것으로 볼 수 있습니다.
In a paper published in this issue of the Canadian Medical Education Journal, Adam et al21 highlights how the term ‘patient’ is referenced in the CanMEDS role descriptions and competencies. While the role descriptions frequently position patients as partners in care, with the exception of the Health Advocate competencies, the key and enabling competencies of the other roles position patients as passive recipients of information and care. Viewed from this perspective, the competencies could be seen to exacerbate existing power-imbalances in a way that allows ongoing discrimination.
2025 CanMEDS 역량 프레임워크 내에서 형평성, 다양성, 포용성, 사회 정의를 어떻게 더 잘 표현할 수 있을까요?
How can equity, diversity, inclusion, and social justice be better represented within the 2025 CanMEDS competency framework?
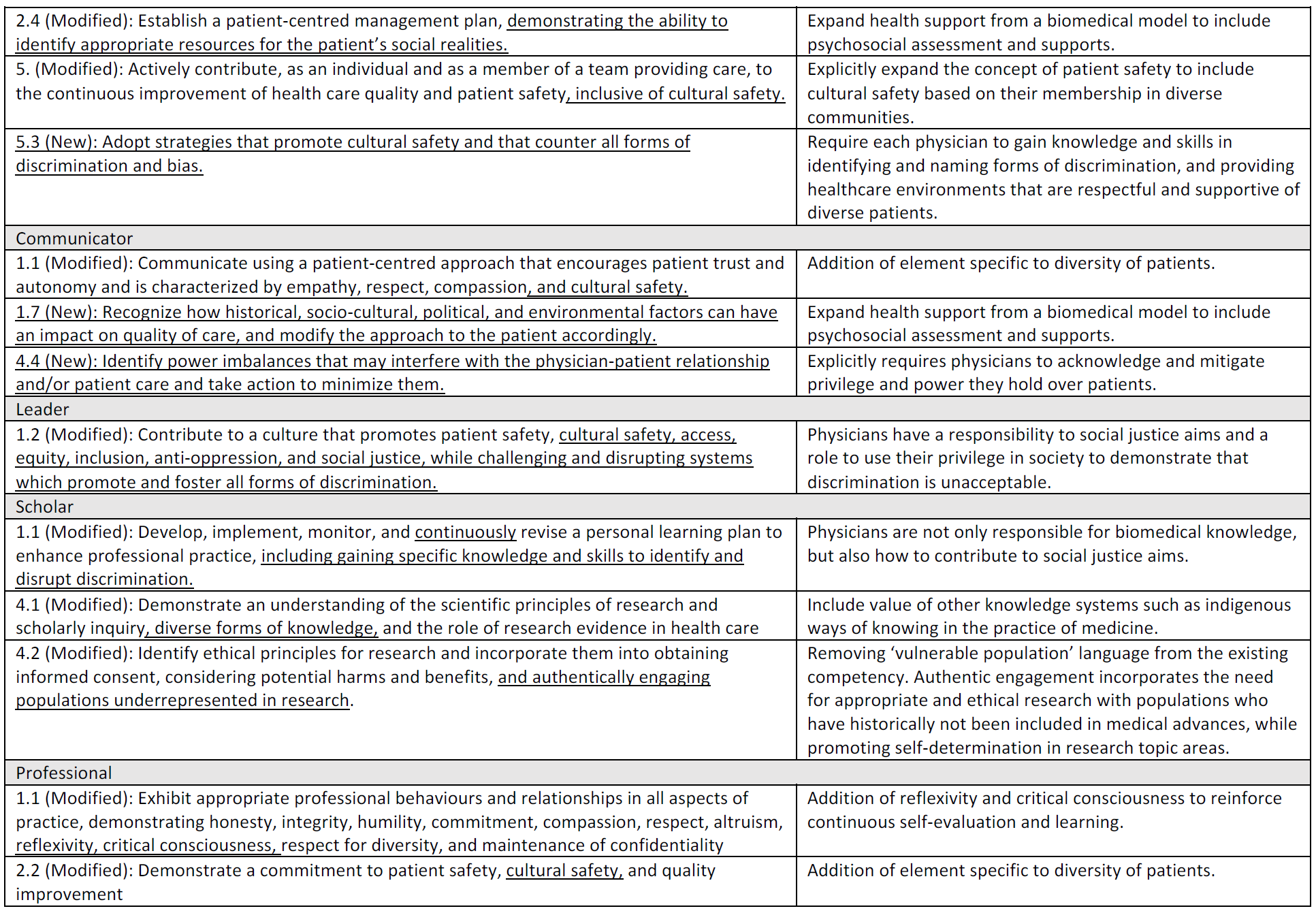
2025 CanMEDS 역량 프레임워크에 형평성, 다양성, 포용성 및 사회 정의와 관련된 역량을 명시적으로 포함할 것을 권장합니다. 이러한 역량을 포함하면 이 분야의 전문성 개발을 지원하여 의사가 불평등을 적극적으로 식별하고 대처하는 동시에 인력의 다양성과 포용성을 증진하는 데 도움이 될 것입니다. 또한 의사들이 형평성에 취약한 집단에 속하는 환자들과 효과적으로 소통할 수 있는 기술을 개발하여 의료 서비스 제공을 개선하고 체계적이고 구조적인 변화를 위한 옹호 활동을 지원할 수 있도록 하고자 합니다. 이러한 각 측면과 관련된 기존 CanMEDS 역량은 표 2A 및 및2B2B에 요약되어 있으며 표 2C 및 및2D2D에 수정이 제안되어 있습니다.
We recommend competencies explicitly related to equity, diversity, inclusion and social justice for the 2025 CanMEDS competency framework. Including such competencies will support professional development in this area that will help physicians to actively identify and combat inequities while promoting diversity and inclusion in the workforce. We also want to ensure physicians develop skills that allow them to effectively engage with patients belonging to equity-deserving groups to both improve the delivery of healthcare and assist in advocacy efforts for systemic and structural change. Existing CanMEDS competencies related to each of these aspects are outlined in Table 2A and and2B2B with suggested modifications in Table 2C and and2D2D.
의사 인력과 관련하여, 우리는 의사가 변화의 주체로 활동하여 인력의 다양성과 포용성을 지원한다는 기대를 강화하는 협력자 및 리더 역할에 새로운 역량을 추가할 것을 권장합니다. 건강 옹호자 역할에 새로 추가된 내용은 다양한 의사의 중요한 역할과 소외된 지역사회에 대한 의료 서비스 제공에 대한 증거를 반영합니다.22 학자 및 전문가 역할에 대한 수정 사항은 수련 중인 의사의 안전한 학습 환경과 의사 동료의 안전한 근무 환경을 보장하는 데 필요한 활동을 강화하는 한편, 의사가 학습자나 동료를 평가할 때 개인의 암묵적 편견을 인식하고 완화할 것을 촉구합니다.
Related to the physician workforce, we recommend new competencies under the Collaborator and Leader roles that reinforce the expectation that physicians act as agents of change to support diversity and inclusion in the workforce. A new addition to the Health Advocate role reflects evidence on the critical role of diverse physicians and care delivery to underserved communities.22 Modifications to the Scholar and Professional roles reinforce necessary activities to ensure safe learning environments for physicians in training and safe working environments for physician colleagues, while also calling on physicians to recognize and mitigate their personal implicit biases when assessing learners or peers.
또한 사회 정의를 위해 노력하는 의사의 책임을 강화하고 의료 서비스에서 공평하고 문화적으로 안전한23 환자 경험의 결과를 지원하는 전략을 제정하는 새로운 역량에 대한 권장 사항을 제시합니다. 특히, 우리는 심리사회적 평가와 건강의 사회적 결정요인 및 구조적 요인에 대한 불평등 해결을 포함하도록 치료 상호작용에서 의사의 책임을 확대하는 수정을 제안했습니다. 이를 위해서는 차별을 중단하고, 의사와 환자 간 상호작용에서 권력 불균형을 최소화하며, 지역사회 참여와 파트너십을 구축하고, 각 환자의 현실에 맞게 치료를 맥락화하기 위한 구체적인 기술 개발이 필요합니다. 마지막으로, 아담 외21가 설명한 유형의 의사-환자 상호작용의 틀을 해결하고 환자를 의료 서비스의 능동적 주체 및 파트너로 인식하는 언어를 통합하는 방향으로 전환하는 것이 중요합니다.
We also make recommendations for new competencies that reinforce the responsibility of physicians to strive for social justice and enact strategies that support outcomes of equitable and culturally safe23 patient experiences in healthcare. Specifically, we have suggested modifications that broaden the responsibility of physicians in care interactions to include psychosocial assessment and addressing inequities in the social determinants of health and structural factors. This will require specific skill development in interrupting discrimination, minimizing power imbalances in the physician-patient interaction, community engagement and partnership, and contextualizing care to the realities of each patient. Lastly, it will be important to address the framing of physician-patient interactions of the type described by Adam et al21 and shift towards incorporating languages that recognizes patients as active agents and partners in their healthcare.
형평성, 다양성, 포용성, 사회 정의를 증진하기 위해 기존 CanMEDS 프레임워크에 제안된 추가 및 수정 사항은 의학교육에 필요한 중요한 개선 사항을 다루는 것을 목표로 합니다. 이러한 변화는 의료 인력의 대표성을 강화하는 동시에 의료진에게 지원적이고 안전한 근무 환경을 제공하는 동시에 환자 치료에 도움이 되는 향상된 기술을 명시적으로 요구할 것입니다.
The proposed additions and revisions to the existing CanMEDS framework to promote equity, diversity, inclusion, and social justice aim to address critical improvements needed in medical education. These changes will strengthen representation in the medical workforce while providing a supportive and safe work environment for practitioners, while also explicitly requiring enhanced skills to benefit patient care.
Equity, diversity, inclusion, and social justice in CanMEDS 2025
PMID: 36998498
PMCID: PMC10042795
DOI: 10.36834/cmej.75845
'Articles (Medical Education) > 교육과정 개발&평가' 카테고리의 다른 글
| CanMEDS 2025의 데이터-기반 의학(Can Med Educ J. 2023 ) (0) | 2024.01.20 |
|---|---|
| CanMEDS 2025의 의사 휴머니즘(Can Med Educ J. 2023) (0) | 2024.01.20 |
| CanMEDS 의사 역량 프레임워크에서 새로 등장하는 개념들 (Can Med Educ J. 2023) (0) | 2024.01.20 |
| 졸업후의학교육에서 공유의사결정을 위한 EPA 식별하기: 국가 델파이 연구(Acad Med, 2021) (0) | 2024.01.02 |
| 학부의학교육에서 지속적 질 개선의 문화 만들기(Acad Med, 2020) (0) | 2023.12.06 |