"정말 곤란하게 만들어요", 중국 전공의의 전문직업성 딜레마(Adv Health Sci Educ Theory Pract. 2023)
“It really puts me in a bind”, professionalism dilemmas reported by Chinese residents
Xinzhi Song1 · Nan Jiang1 · Ning Ding1 · Honghe Li1 · Chunyu Xin1 · Ruoyi Qu1 · Deliang Wen1

소개
Introduction
전문직업성은 시대와 문화에 따라 달라지는 복잡하고 다차원적이며 통합적인 구성 요소이며(Hodges et al., 2011), 사회에서 의사에게 기대하는 행동과 속성으로 볼 수 있습니다(Cruess et al., 2009). 전문직업성 연구 분야에서는 덕목 기반, 행동 기반, 정체성 형성 등 세 가지 주요 유형의 프레임워크가 발전해 왔습니다(Irby & Hamstra, 2016). 각 프레임워크는 서로를 보완하고 더 큰 전체에 기여하는 강점과 한계를 가지고 있습니다.
- 미덕 기반 프레임워크는 인성을 강조하고 의사의 내적 습관, 도덕적 추론, 인문학적 자질에 중점을 둡니다.
- 전문직 정체성 형성은 개인과 집단 모두를 포함하며, 정체성 개발과 실무 커뮤니티로의 사회화에 중점을 둡니다.
- 이 두 가지 유형의 프레임워크 모두 학습자에게 동기를 부여하는 데 도움이 되지만, 덕성 기반 프레임워크의 경우 인성 및 도덕적 추론을 평가하기 어렵고, 전문직 정체성 형성을 설명, 해석 및 평가하기는 더욱 어렵습니다(Barnhoorn et al., 2019; Irby & Hamstra, 2016).
- 위의 두 가지 프레임워크의 문제점에 비해 행동 기반 프레임워크는 행동이 내면의 정신 모델을 반영할 수 있다는 전제하에 관찰 가능한 행동의 측정을 강조합니다. 통합된 작업이나 활동의 여러 구성 요소를 개별 행동으로 분리할 수 있지만, 관찰 가능한 행동을 평가하는 것이 통일성과 객관성을 확보하는 데 가장 용이할 수 있습니다(Barnhoorn & van Mook, 2015). 실제로 이러한 행동은 종종 개별 전문가와 환자의 수준을 넘어 동료 및 의료 시스템과의 상호 작용을 포함합니다(Irby & Hamstra, 2016; Lesser et al., 2010). Lesser 등이 제안한 바와 같이 관찰 가능한 행동의 렌즈를 통해 전문직업성을 바라보는 것은 전문직업성이 다차원적이라는 개념을 강화하고 의사가 실제로 발휘해야 하는 판단과 기술의 범위를 지적합니다(Lesser 등, 2010).
Professionalism is a complex, multidimensional, and integrated construct that varies across time and culture (Hodges et al., 2011) and can be viewed as the behaviors and attributes expected of a doctor by society (Cruess et al., 2009). In the field of professionalism research, three dominant types of frameworks have evolved, namely virtue-based, behavior-based, and identity formation (Irby & Hamstra, 2016). Each framework has strengths and limitations that complement each other and contribute to the larger whole.
- The virtue-based framework emphasizes character and focuses on the inner habits of the heart, moral reasoning, and humanistic qualities of the physician.
- Professional identity formation involves both the person and the group, focusing on identity development and socialization into a community of practice.
- Against the challenges of the above two frameworks, the behavior-based framework emphasizes measurement of observable behaviors, with the premise that behaviors may reflect inner mental models. Though it may separate different components of integrated tasks or activities into discrete behaviors, assessment of observable behaviors may be easiest to achieve uniformity and objectivity (Barnhoorn & van Mook, 2015). In fact, these behaviors often go beyond levels of the individual professional and the patient to include interactions with colleagues and with the health care system (Irby & Hamstra, 2016; Lesser et al., 2010). As proposed by Lesser et al., viewing professionalism through the lens of observable behaviors reinforces the notion that professionalism is multidimensional and points to the range of judgment and skills physicians need to exhibit in practice (Lesser et al., 2010).
전문직업성은 의사의 경력 전반에 걸쳐 배양되고 평가되어야 하며, 학부 및 대학원 환경에서 전문직업성 원칙을 확립하기 위해서는 조기 교육이 매우 중요합니다(O'Sullivan 외., 2012). 레지던트 기간은 의사가 수련과 경험을 통해 전문직업성 행동을 개발하는 중추적인 시기입니다. 이를 인식한 미국의학전문대학원교육인증위원회(ACGME)는 레지던트가 레지던트를 졸업하기 전에 갖춰야 할 6가지 일반 역량 중 하나로 '전문직업성'을 우선적으로 꼽았습니다(미국의학전문대학원교육인증위원회, 2021). 수련 중인 레지던트는 의대생과 달리 훨씬 더 많은 수의 환자에 노출되고 업무의 복잡성이 높으며 단순한 관찰이 아닌 환자 진료에 대한 감독 책임을 져야 합니다(Levinson et al., 2014). 그 결과, 전공의들은 임상 수련 과정에서 전문직업성과 관련하여 많은 어려움에 직면하게 됩니다(Kinoshita et al., 2015; McArthur & Moore, 1997). 예를 들어, 전공의는 제한된 시간 내에 임상 지식과 기술을 향상시켜야 한다는 압박감을 느낄 수 있으며, 이로 인해 전문직업성 문제보다는 생산성과 효율성에 더 많은 관심을 갖게 됩니다(Brainard & Brislen, 2007; Chang et al., 2017). 또한 비윤리적이거나 비전문직업적이라고 생각되는 임상 활동을 목격하거나 참여할 수도 있습니다(Christakis & Feudtner, 1993; Kinoshita et al., 2015). 그러나 병원 위계질서의 숨겨진 커리큘럼 하에서는 전공의가 선배 의사의 결정이나 명령에 반대하기 어렵기 때문에 침묵해야 할 의무를 느낄 수 있으며(Martinez et al., 2015), 이로 인해 전공의는 전문직업성 딜레마에 빠지게 됩니다(Monrouxe & Rees, 2012).
Professionalism should be cultivated and assessed throughout the physician’s career, and early education is critical for establishing professionalism principles in both undergraduate and postgraduate settings (O’Sullivan et al., 2012). Residency is a pivotal period for physicians to develop their professionalism behaviors with training and experience. Recognizing this, the Accreditation Council for Graduate Medical Education (ACGME) has preferentially listed “professionalism” as one of the six general competencies that residents must possess before graduating from residency (Accreditation Council for Graduate Medical Education, 2021). Different from medical students, residents-in-training are exposed to a significantly increased number of patients, have higher work complexity, and need to take supervised responsibility for patient care instead of mere observation (Levinson et al., 2014). As a result, residents encounter many challenges with regard to professionalism in their clinical training (Kinoshita et al., 2015; McArthur & Moore, 1997). For example, they may feel pressured to improve clinical knowledge and skills within a limited time, which makes them more concerned about productivity and efficiency than about professionalism issues (Brainard & Brislen, 2007; Chang et al., 2017). They may also witness or participate in clinical activities which they believe to be unethical or unprofessional (Christakis & Feudtner, 1993; Kinoshita et al., 2015). However, under the hidden curriculum of hospital hierarchy, it is difficult for residents to stand against senior physicians’ decisions or orders, and so they might feel obligated to keep silent (Martinez et al., 2015), thus causing residents to fall into professionalism dilemmas (Monrouxe & Rees, 2012).
실제로 레지던트들은 종종 전문직업성 딜레마를 경험하는데, 이는 전문직업적으로 또는 전문직업성 기준에 따라 행동하는 방법을 알고 있지만 제도적, 위계적 또는 사회문화적 제약으로 인해 행동할 수 없거나 어렵다고 느끼는 갈등 상황을 말합니다(Cuban, 2001; Wiggleton 외., 2010). 윤리적 또는 전문직업적 행동을 반복적으로 수행하지 못할 때,
- 일부 레지던트는 시간이 지남에 따라 이러한 부정적인 사건을 경험하면서 괴로워하는 반면,
- 일부 레지던트는 임상 역할 모델의 규범적 행동과 태도를 집단적이고 수동적으로 흡수하고 채택하여 특정 비전문직업적 행동이 용인되고 "바뀌지 않음" 문화가 강화됩니다
또한 전문직업성 딜레마는 전문직업적 태도, 행동 및 전문직업적 정체성 형성에 부정적인 영향을 미친다는 증거도 있습니다(Kushner & Thomasma, 2001). 오늘날의 레지던트들은 미래의 레지던트를 교육하는 사람들이 될 것입니다. 전문직업성 딜레마가 적시에 적절하게 해결되지 않으면 의사(예: 연민 피로 및 소진)와 의료 서비스 전체(예: 환자 치료의 질 저하, 심지어 환자 안전 위협)에 여러 가지 심각한 결과가 나타날 수 있습니다(Monrouxe et al., 2015).
Indeed, residents often experience professionalism dilemmas, which refer to conflictual situations when one knows how to behave professionally or in accordance with the standards of professionalism but instead feels unable or difficult to act due to institutional, hierarchical, or sociocultural constraints (Cuban, 2001; Wiggleton et al., 2010). When repeatedly failing to perform ethical or professional behaviors,
- some residents become distressed when experiencing these negative events over time, while
- others collectively and passively absorb and adopt normative behaviors and attitudes from their clinical role models, resulting in certain unprofessional behaviors becoming acceptable and reinforcing a “no change” culture (Caldicott & Faber-Langendoen, 2005; Kelly & Nisker, 2009).
Evidence also showed that professionalism dilemmas negatively impact the development of professional attitudes, behaviors, and professional identity formation (Kushner & Thomasma, 2001). Today’s residents will be the ones who train residents in the future. If professionalism dilemmas are not appropriately addressed in a timely manner, a number of serious consequences may emerge for both physicians (e.g., compassion fatigue and burnout) and the whole of healthcare (e.g., decreasing the quality of patient care, even threatening patient safety) (Monrouxe et al., 2015).
중국의 의료 및 의학 교육
Health care and medical education in China
중국은 전 세계 인구의 약 5분의 1(14억 명 이상)이 의료비를 부담하고 있으며, 복잡한 의료 및 건강보험 시스템을 갖추고 있습니다. 중국의 병원은 기능과 업무에 따라 1차, 2차, 3차 병원의 세 가지 계층으로 분류됩니다. 이 분류에 따라 각 계층에 속하는 병원은 다시 A, B, C 등급으로 세분화되며, 가장 전문화된 병원을 위한 특별 등급인 3AAA 병원이 추가로 지정됩니다. 따라서 중국 병원 분류 시스템을 3단계 10등급 시스템이라고 합니다(중화인민공화국 보건부, 1989).
- 이 시스템 내에서 일차 병원은 서구의 진료소, 지역 병원 및 1차 진료 기관과 유사합니다. 일반적으로 병상 수가 100개 미만이며 예방 치료, 재활 치료 및 기타 기본적인 의료 서비스를 제공합니다.
- 2차 병원은 서양의 지역 병원 또는 지방 병원과 유사하며 일반적으로 100~500개의 병상을 보유하고 종합적인 의료 서비스를 제공하며 지역 의료 연구 및 교육을 수행합니다.
- 3차 병원은 서양의 진료 의뢰 병원과 동등한 수준으로 간주되며 시, 도 또는 국가 차원의 종합적인 대형 병원입니다. 3차 병원은 주변 지역의 의료 허브 역할을 하며 1, 2차 병원의 진료뿐만 아니라 전문 의료 서비스도 제공합니다. 따라서 3차 병원은 가장 많은 병상(500개 이상)을 보유하고 있으며 의학 교육과 과학 연구 분야에서 훨씬 더 큰 역할을 담당합니다.
China bears the health burden of nearly one-fifth of the world’s population (more than 1.4 billion) and is home to a complex health care and health insurance system. Hospitals in China are classified by function and tasks into three tiers, namely primary, secondary, and tertiary hospitals. On top of this classification, hospitals within each tier are then sub-graded into A, B, and C levels, with an additional special level—the 3AAA hospital—reserved for the most specialized hospitals. Therefore, the Chinese hospital classification system is referred to as the 3-tier 10-level system (Ministry of Health of the People’s Republic of China, 1989).
- Within this system, primary hospitals are similar to medical clinics, community hospitals, and primary care institutions in the West. They usually contain less than one hundred beds and fulfill preventive care, rehabilitative care, and other basic medical care needs.
- Secondary hospitals, similar to Western regional or district hospitals, usually have between one hundred and five hundred beds, provide comprehensive health services, and conduct regional medical research and education.
- Tertiary hospitals are regarded as equivalents to referral hospitals in the West and are comprehensive large-scale hospitals at the municipal, provincial, or national level. Tertiary hospitals act as medical hubs for their surrounding areas and provide both specialist health services as well as consultations for primary and secondary hospitals. As such, tertiary hospitals have the highest bed capacities (over five hundred) and play a much larger role in medical education and scientific research.
2020년 기준 중국 인구의 95% 이상이 최소 기본 의료 보험에 가입했습니다(중화인민공화국 국가의료보장국, 2021). 중국의 기본 의료 보험에는 도시 직장인 기본 의료 보험(UEBMI), 도시 전공의 기본 의료 보험(URBMI), 신농촌 협동 의료 제도(NRCMS) 등 세 가지 주요 유형이 있습니다. 대부분의 국가에서 기본 의료 보험이 제공되지만, 공공 의료 보험은 일반적으로 의료비의 절반 정도만 보장하며 만성 질환의 경우 보장 범위가 더 낮을 수 있습니다. 또한 보험 유형에 관계없이 병원 등급이 높아질수록 환급률이 감소한다는 사실도 있습니다(예: NRCMS의 환급률은 1차 병원에서 60%의 보장률을 유지하지만 3차 병원에서는 약 30%에 불과합니다). 환자들은 길고 지루한 진료 의뢰 절차를 거쳐 여러 기관을 거치는 것을 선택할 수도 있고, 환자가 하위 병원에 대한 신뢰가 부족한 경우처럼 직접 상위 병원으로 이동하는 것을 선택할 수도 있습니다(Wang, 2019). 2020 보건 통계 보고서에 따르면 병상 가동률은 1차 병원에서 54.7%, 2차 병원에서 81.6%인 반면 3차 병원에서는 97.5%였습니다(중화인민공화국 국가위생건강위원회, 2021a). 이처럼 3차 병원의 높은 점유율은 환자 대 의사 비율 증가, 의사-환자 관계의 긴장감 증가, 3차 병원의 의료 서비스 제공자 및 의료진의 과중한 업무 부담 등의 문제를 야기합니다(Wen et al., 2016).
As of 2020, more than 95% of the Chinese population had at least basic health insurance coverage (National Healthcare Security Administration of the People’s Republic of China, 2021). China’s basic medical insurance scheme includes three main types: the Urban Employee Basic Medical Insurance (UEBMI), the Urban Residents Basic Medical Insurance (URBMI), and the New Rural Co-operative Medical Scheme (NRCMS). Despite most of the country having basic medical coverage, public health insurance usually only covers about half of medical expenses, and this coverage may be even lower for chronic illnesses. Additionally, regardless of the type of insurance, all come with the fact that reimbursement rates decrease as hospital ranking increases (e.g., the reimbursement rate of NRCMS maintains 60 percent coverage in primary hospitals but only about 30 percent in tertiary hospitals). Patients can choose to undergo the long and tedious referral process up the chain of institutions, or patients can choose to jump the line and personally go directly to higher-level hospitals, as is often the case when patients lack trust in lower-level hospitals (Wang, 2019). According to the 2020 Health Statistics Report, bed utilization rates were 54.7% in primary hospitals and 81.6% in secondary hospitals, while the rate was 97.5% in tertiary hospitals (National Health Commission of the People’s Republic of China 2021a). This marked higher occupancy in tertiary hospitals also brings about problems such as higher patient-physician ratios, increased tensions in physician–patient relationships, and overburdening of healthcare providers and medical staff at tertiary hospitals (Wen et al., 2016).
중국의 국가 표준 레지던트 교육 시스템은 2014년에 설립되었습니다(국가보건가족계획위원회, 2014). 레지던트 프로그램은 전공과목에 관계없이 3년으로 정해졌으며, 임상에서 일하고자 하는 모든 의대 졸업생은 먼저 표준화된 레지던트 교육을 이수해야 합니다. 다른 많은 국가(예: 일본, 브라질, 네덜란드, 영국)와 유사한 의료 수련 모델을 가지고 있음에도 불구하고(Wijnen-Meijer 외, 2013), 중국의 레지던트 수련 시스템은 모든 레지던트가 일반적으로 최고 수준의 병원 기관이자 가장 바쁜 3차 A급 병원에서 수련을 받도록 요구합니다(중화인민공화국 국가위생건강위원회 2021b). 이러한 수련 환경에서 중국인 전공의는 과도한 업무량, 긴 근무 시간, 수면 부족, 근무 시간 외의 지속적인 당직 등으로 고통받고 있습니다(Bai et al., 2021). 또한 중국 전공의들은 개인적인 이익보다 대인 관계와 사회적 조화를 중시하는 중국 집단주의 사회의 문화적 영향과 요구와 함께 숨겨진 커리큘럼의 어려움에도 직면합니다. 따라서 서구의 전형적인 일과 삶의 분리는 개인적 관계와 직업적 관계 사이에 명확한 이분법이 없는 중국 환경에서는 달성하기가 훨씬 더 어렵습니다(Bedford, 2022). 그러나 현재까지 중국 전공의가 직면할 수 있는 전문직업성 딜레마와 도전 과제에 대해 조명한 연구는 거의 없습니다.
A system for national standardized residency training in China was established in 2014 (National Health & Family Planning Commission, 2014). Residency programs were set at three years in duration regardless of specialty, and all medical graduates looking for work in a clinical capacity must first complete standardized residency training. Despite having similar models of medical training to many other countries (e.g., Japan, Brazil, Netherlands, UK) (Wijnen-Meijer et al., 2013), the resident training system in China requires all residents to be trained in tertiary A-grade hospitals, which are usually the highest-level hospital institution and also the busiest (National Health Commission of the People’s Republic of China 2021b). In this kind of training environment, Chinese residents suffer from an excessive workload, longer working hours, sleep deprivation, and consistently being on call outside of working hours (Bai et al., 2021). In addition, Chinese residents also face the challenges of the hidden curriculum, along with cultural influences and demands of China’s collectivist society, where interpersonal relationships and social harmony are valued above personal interests. As such, the typical work-life separation in the West is much harder to achieve in the Chinese setting, where there is not necessarily a clear dichotomy between personal and professional relations (Bedford, 2022). However, to date, few studies have shed light on some of the professionalism dilemmas and challenges that Chinese residents may face.
전문직업성 딜레마에 대한 포괄적인 목록은 병원 관리자와 의료 교육자 모두에게 많은 이점을 제공할 것입니다. 예를 들어, 병원은 이 목록을 체크리스트로 사용하여 기존의 전문직업성 문제를 평가하고 레지던트를 위한 목표 개선안을 마련할 수 있으며(Cullen et al., 2017), 병원 관리자는 이 종합 목록을 사용하여 제도적 변화를 구현할 수 있는지 평가할 수 있습니다. 임상 교수진과 레지던트 프로그램 디렉터는 이 체크리스트의 단일 또는 여러 딜레마를 기반으로 교육 사례를 설계할 수 있으며, 이 체크리스트를 사용하여 이러한 전문직업성 딜레마로 인해 심각한 문제를 겪고 있는 레지던트를 선별하고 체크리스트에 제시된 구체적이고 관찰 가능한 행동 관련 문제에 따라 교정을 시행할 수 있습니다(Cullen 등, 2017; Hawkins 등, 2009). 따라서 본 연구는 행동 기반 전문직업성 프레임워크에 기반한 전문직업성 딜레마 체크리스트를 개발하고, 중국 전공의가 듣거나 목격하거나 경험한 전문직업성 딜레마의 범위와 비율을 조사하고, 전문직업성 딜레마에 직면했을 때 전공의의 관점을 이해하는 것을 목표로 합니다.
A comprehensive list of professionalism dilemmas would provide many benefits for both hospital administration as well as medical educators. For example, hospitals can use this as a checklist to assess existing professionalism challenges and to create targeted remediation for their residents (Cullen et al., 2017); on the institutional side, hospital administrators can also use this comprehensive list to assess whether institutional changes can be implemented. Clinical faculty and residency program directors can design teaching cases based on single or multiple dilemmas from this checklist and can also use this checklist to screen residents who may be deeply troubled by these professionalism dilemmas and implement remediation, guided by the specific, observable behavior-related challenges presented in the checklist (Cullen et al., 2017; Hawkins et al., 2009). Therefore, our research aims to develop a checklist of professionalism dilemmas based on a behavior-based professionalism framework, to examine the range and proportion of professionalism dilemmas heard of, witnessed, or experienced by Chinese residents, and to gain understanding of residents’ perspectives when faced with professionalism dilemmas.
연구 방법
Methods
연구 설계
Study design
본 연구는 정성적(문서 분석 및 포커스 그룹 인터뷰)과 정량적(소규모 설문조사) 데이터로 구성된 혼합 방법 연구였습니다. 문서 분석은 이전에 발표된 논문에서 전문직업성 딜레마 항목을 요약하여 후속 포커스 그룹 인터뷰를 위한 전체적인 개요와 가이드를 제공했습니다. 포커스 그룹 인터뷰에서는 전문직업성 딜레마 항목에 대한 참가자들의 경험과 인식을 탐색하고 이해하기 위해 내러티브 탐구(Monrouxe & Rees, 2012; Wang & Ho, 2020)를 사용했습니다. 질적 연구 결과를 보고할 때는 질적 연구 보고 기준(SQRQ)을 따랐습니다(O'Brien et al., 2014). 각 포커스 그룹에서 소규모 설문조사를 실시하여 참가자들이 들어본 적이 있거나 목격하거나 경험했다고 답한 전문직업성 딜레마 항목의 비율을 조사했습니다.
Our study was a mixed methods study consisting of qualitative (document analysis and focus group interviews) and quantitative (a small-scale questionnaire survey) data. Document analysis summarized professionalism dilemma items from previously published papers, providing an overall outline and guide for subsequent focus group interviews. For focus group interviews, we used narrative inquiry (Monrouxe & Rees, 2012; Wang & Ho, 2020) to explore and make sense of participants’ experiences and perceptions of professionalism dilemma items. When reporting qualitative results, we followed the Standards for Reporting Qualitative Research (SQRQ) (O’Brien et al., 2014). A small-scale questionnaire survey was conducted during each focus group to investigate the proportion of professionalism dilemma items that participants reported to have heard of, witnessed, or experienced.
모집 및 샘플링
Recruitment and sampling
2021년 3월과 4월 사이에 랴오닝성 선양에 위치한 종합 3차 A급 병원의 대학원 수련부 공고를 통해 6개월 이상 수련을 받은 레지던트를 대상으로 의도적 표본 추출(Moser & Korstjens, 2018)을 실시했습니다. 이 레지던트들은 이미 임상 경험이 어느 정도 있고 연구에 충분하고 유용한 정보를 제공할 수 있기 때문에 선발되었습니다. 또한 성별, 수련 기간, 전공이 다른 레지던트들을 의도적 표본 추출에 포함시켜 참여자 특성의 다양성을 확대했습니다. 참가자들을 전문 분야에 따라 여러 포커스 그룹으로 분류했습니다. 그런 다음 각 포커스 그룹 인터뷰 라운드마다 각 전문화 그룹에 대한 인터뷰를 연속적으로 진행했으며 주제별 포화 상태에 도달하면 모집을 중단했습니다. 연구 참여는 자발적으로 이루어졌으며 모든 참가자는 서면 동의서에 서명했으며 어떠한 보상도 받지 않았습니다.
Between March and April 2021, we conducted purposive sampling (Moser & Korstjens, 2018) of residents who have undergone at least 6 months of training through announcements made by the Postgraduate Training Department of a comprehensive tertiary A-grade hospital in Shenyang, Liaoning province. These residents were selected because they already have some clinical experience and can provide sufficient and useful information for our research. Also, residents of different sex, duration of training completed, and specialization were selected in the purposive sampling to expand the diversity of participant characteristics. We grouped the participants into different focus groups according to their specialization. Then, for each round of focus group interviews, we conducted interviews with each specialization group in consecutive order and stopped recruiting when we reached thematic saturation. Participation in the study was voluntary, and all participants signed written informed consent forms and did not receive any compensation.
데이터 수집
Data collection
먼저 검색 주제를 '전문직업성 딜레마', '전문직업성 도전', '전문직업성 과실'로 설정하고 검색 대상을 '의사', '레지던트', '의대생'으로 설정한 논문에 대해 Web of Science에서 문헌 검색을 실시했습니다. 논문은 특정 시나리오를 설명하거나 특정 행동을 나열한 경우 포함할 수 있었습니다. 자세한 검색 전략은 보충 정보 부록 A에서 확인할 수 있습니다. 등록된 모든 논문에 기술된 딜레마, 도전 과제 또는 비전문직업적 행동은 Monrouxe와 Rees(2012)가 구성한 전문직업성 딜레마 주제 목록을 참조하여 추출 및 요약하여 전문직업성 딜레마 항목 풀을 생성했습니다. 그런 다음 템플릿 분석(King, 1998)을 사용하여 모든 항목을 Li 등(Li, 2017)의 중국 의사를 위한 기존 행동 기반 전문직업성 프레임워크에 매핑하여 네 가지 영역으로 구성했습니다. 이 과정은 두 명의 연구자(XZS, NJ)가 개별적으로 수행했으며, 이견이 있는 문항은 다른 세 명의 저자(ND, HHL, RYQ)와 함께 그룹 토론을 통해 해결했습니다. 그 결과 체크리스트의 첫 번째 버전이 만들어졌고, 이 체크리스트는 포커스 그룹의 첫 번째 라운드에서 사용되었습니다.
We first conducted a literature search on Web of Science for papers with retrieval themes focused on “professionalism dilemma”, “professionalism challenge”, and “professionalism lapse” and the retrieval population focused on “physician”, “resident”, and “medical student”. Papers were eligible for inclusion if they described specific scenarios or listed specific behaviors. The detailed search strategy can be found in Supplementary information Appendix A. We extracted and summarized the dilemmas, challenges, or unprofessional behaviors described in all the enrolled papers with reference to the list of professionalism dilemma themes constructed by Monrouxe and Rees (2012) and generated an item pool of professionalism dilemmas. Using template analysis (King, 1998), all items were then mapped to an existing behavior-based professionalism framework for Chinese physicians by Li et al., comprising four domains (Li, 2017). This process was performed individually by two researchers (XZS and NJ), and disputes were settled by group discussion with three other authors (ND, HHL, and RYQ). The result was the first version of the checklist, to be used in the initial round of focus groups.
그 후 포커스 그룹 인터뷰를 반복적으로 실시했습니다. 모든 인터뷰는 허가를 받아 오디오로 녹음하고 익명으로 처리했습니다.
- 각 인터뷰 세션이 시작될 때 그룹 진행자(XZS)는 참가자들에게 전문직업성의 개념을 소개했습니다.
- 의사 헌장(ABIM 재단, 2002)의 기본 원칙,
- ACGME(의학전문대학원 교육 인증위원회, 2021)에서 제안한 전문직업성의 속성,
- Li 등의 전문직업성 프레임워크(Li, 2017)
- 그런 다음 참가자들에게 전문직업성 딜레마에 대한 첫 번째 버전 체크리스트를 가이드로 제공하고 첫 번째 하위 영역의 각 항목을 읽고 해당 항목에 대해 들어본 적이 있는지, 목격한 적이 있는지, 경험한 적이 있는지 선택하도록 요청했습니다(체크박스에 체크).
- 모든 참가자가 하위 영역을 완료한 후, 그룹 진행자는 참가자들에게 차례로 자신이 들었거나 목격했거나 경험한 구체적인 시나리오를 구두로 설명하고 개인적인 태도와 느낌을 공유하도록 요청했습니다.
- 첫 번째 하위 영역의 기존 항목에 대해 논의한 후, 그룹 진행자는 참가자들에게 하위 영역에 나열되지 않은 다른 시나리오를 경험한 적이 있는지 설명해 달라고 요청했습니다. 이후 각 하위 영역에서도 동일한 형식이 이어졌습니다.
- 연구원들은 각 포커스 그룹 인터뷰의 데이터를 분석하여 체크리스트의 업데이트 버전을 작성했으며, 이 체크리스트는 첫 번째 라운드와 동일한 형식의 후속 포커스 그룹에서 사용되었습니다.
- 새로운 항목이 보고되지 않으면 데이터 수집이 종료되었습니다.
We then conducted iterative rounds of focus group interviews. All interviews were audio recorded with permission and anonymized.
- At the beginning of each interview session, the group facilitator (XZS) introduced participants to the concept of professionalism, including
- Participants were then given the first version checklist on professionalism dilemmas as a guide and were asked to read each item in the first sub-domain and select (by checking the box) whether they had heard of, witnessed, or experienced the given item.
- After everyone had completed a sub-domain, the group facilitator invited participants to, in turn, verbally describe the specific scenarios they had heard of, witnessed, or experienced and share some of their personal attitudes and feelings.
- After discussing existing items in the first sub-domain, the group facilitator then asked participants to describe if they had experienced any other scenario not listed within the sub-domain. The same format continued for each subsequent sub-domain.
- Researchers analyzed data from each round of focus group interviews to compile an updated version of the checklist, which was then used in the subsequent round of focus groups that followed the same format as the first round.
- Data collection ended when no new items were reported.
데이터 분석
Data analysis
Li 등의 행동 기반 전문직업성 프레임워크는 연구자가 코드를 추가, 수정 또는 삭제하는 등 데이터를 해석하는 동안 조정할 수 있는 사전 정의된 템플릿을 제공했습니다(King, 2004). 강력하고 잘 정의된 선험적 템플릿을 사용하면 주제를 미리 설정할 수 있는 동시에 연구자에게 어느 정도 유연성을 제공할 수 있었습니다(Brooks et al., 2015). 포커스 그룹 인터뷰의 첫 번째 라운드가 끝난 후, 모든 인터뷰 오디오 파일을 전사하고 비식별화했습니다. 녹음된 인터뷰는 NVivo 12(QSR International Pty Ltd., Doncaster, VC, Australia)를 사용하여 코딩했습니다. 두 명의 연구자(XZS와 CYX)가 모든 참가자의 녹취록을 독립적으로 검토하여 각 항목과 관련된 인용문을 식별했습니다. 두 연구자가 이견이 있는 시나리오와 체크리스트의 각 하위 영역 끝에 새로 제안된 시나리오에 대해서는 5명의 연구자(XZS, NJ, HHL, ND, CYX)가 모여 전문직업성 딜레마로 분류할 수 있는지 논의하고, 분류할 수 있다면 체크리스트 하위 영역의 기존 항목에 속할지 아니면 새로운 항목으로 추가할지에 대해 협의했습니다. 참가자들의 이야기를 바탕으로 체크리스트 초판의 기존 항목의 문구를 수정하여 중국 전공의에게도 적용 가능하도록 수정했습니다.
The behavior-based professionalism framework by Li et al. provided a predefined template from which researchers could make adjustments during interpretation of data, including adding, modifying, or deleting codes (King, 2004). Using a strong, well-defined a priori template allowed for themes to be established in advance while also providing some flexibility for researchers (Brooks et al., 2015). After the first round of focus group interviews, all interview audio files were transcribed and de-identified. We coded the recorded interviews using NVivo 12 (QSR International Pty Ltd., Doncaster, VC, Australia). Two researchers (XZS and CYX) independently reviewed all the participants’ transcripts to identify quotes related to each of the items. For any scenario where the two researchers had disputes on and for any newly proposed scenario at the end of each subdomain of the checklist, five researchers (XZS, NJ, HHL, ND, and CYX) met to discuss whether it can be classified as a professionalism dilemma and, if so, conferred on whether it belonged to an existing item in the checklist subdomain or to add this scenario as a new item. From participant narratives, we revised the wording of the original items in the first version of the checklist to make it applicable to Chinese residents.
각 포커스 그룹 인터뷰가 끝난 후 데이터 분석을 수행한 후 체크리스트의 업데이트 버전을 작성하여 다음 라운드에 사용했습니다. 연구자들은 새로운 코드가 나오지 않을 때 주제별 포화 상태가 충족되었다고 동의했고, 그 이후에는 새로운 포커스 그룹 인터뷰를 진행하지 않았습니다. 이 시점에서 모든 항목이 체크리스트의 최종 버전으로 확정되었고 각 항목과 관련된 모든 인용문이 확인되었습니다. 그런 다음 모든 연구원이 모여 질적 편집 분석 프로토콜(Miller & Crabtree, 1992)을 사용하여 각 항목을 가장 대표할 수 있는 인용문을 선정했습니다. 그런 다음 대표 인용문을 영어로 번역했습니다. 분석이 진행되는 동안 코딩이 진행됨에 따라 연구자의 성찰을 기록하기 위해 메모를 작성했습니다.
Data analysis was performed after each round of focus group interviews, following which we compiled an updated version of the checklist and used it for the next round. Researchers agreed that thematic saturation had been met when no new codes emerged, following which no new rounds of focus group interviews were conducted. At this point, all the items were finalized into the final version of the checklist and all quotes related to each of the items were identified. Then, all researchers convened to select quotes that were most representative of each item using a qualitative editing analysis protocol (Miller & Crabtree, 1992). Representative quotes were then translated into English. Throughout the analysis, memos were created to serve as records of researchers’ reflections as the coding progressed.
두 차례의 포커스 그룹 인터뷰를 통해 50명의 참가자 전원이 작성한 체크리스트 설문지를 바탕으로 참가자들이 보고한 전문직업성 딜레마 항목의 비율을 해당 항목에 대해 들어본 적이 있는지, 목격한 적이 있는지, 경험한 적이 있는지에 따라 계층화하여 계산했습니다.
Based on checklist questionnaires filled out by all 50 participants during two rounds of focus group interviews, we calculated the proportion of professionalism dilemma items as reported by participants, stratified by whether they had heard of, witnessed, or experienced the item.
반사성
Reflexivity
연구팀은 데이터 수집 및 분석 과정에서 각 구성원의 이전 경험, 역할, 동기가 데이터 해석에 영향을 미칠 수 있음을 이해했습니다. 따라서 정기적으로 회의를 통해 각자의 개인적인 관찰과 관점, 그리고 그것이 데이터 분석 및 결과 적용과 어느 정도 관련성이 있는지에 대해 논의함으로써 반성적 사고를 실천했습니다. 또한 데이터 분석 중에 메모를 작성하여 코딩하는 동안 연구자의 반성을 기록했습니다.
Throughout the data collection and analysis, the research team understood that each member’s prior experiences, roles, and motivations may influence the interpretation of the data. Therefore, we practiced reflexivity by regularly meeting to discuss our personal observations and perspectives and the extent to which they may be relevant to the data analysis and to the application of our results. Memos were also created during data analysis to record researcher reflections during coding.
연구팀의 모든 구성원은 질적 연구 및 의료 전문직업성 연구에 대한 교육이나 배경 지식을 갖추고 있습니다. 또한 XZS와 HHL은 의료 정보학에 대한 배경 지식이 있습니다. NJ는 영어 원어민으로 MBBS 학위를 보유하고 있으며 중국에서 임상 교육 경험이 있습니다. XZS와 CYX는 데이터 수집 당시 의학교육학 박사 과정 중이었습니다. ND, HHL, RYQ는 학부 및 대학원 전문직업성 과정의 교수진 및 과정 개발자였으며, XZS는 조교였습니다. DLW는 소아과 과장을 역임했으며 현재는 의학교육과 교수로 재직 중입니다. 각자의 고유한 배경과 경험을 바탕으로 각 멤버는 그룹 토론에 풍부하고 건설적인 피드백을 더했습니다.
All members of the research team have some training or background in qualitative research and in medical professionalism research. Additionally, XZS and HHL have backgrounds in medical informatics. NJ is a native English speaker who holds an MBBS degree and has clinical training experience in China. XZS and CYX were PhD candidates in medical education at the time of data collection. ND, HHL, and RYQ are teaching faculty and course developers for undergraduate and graduate professionalism courses; XZS is the teaching assistant. DLW was a chief of pediatrics and is now a professor of medical education. Based on their own unique backgrounds and experiences, each member added richness and constructive feedback to the group discussions.
결과
Results
검색 전략에 따라 1차 검색에서 총 613개의 출판물이 검색되었습니다. 적격성 기준에 따라 55개의 출판물이 최종 연구에 등록되었습니다. 그런 다음 등록된 출판물에서 전문직업성 딜레마에 관한 53개 항목을 수집, 분석, 요약하여 Li 등이 제시한 전문직업성 프레임워크의 10개 하위 영역에 매핑했습니다. 등록된 모든 출판물, 딜레마 또는 도전과 비전문직업적 행동에 대한 특정 시나리오, 문서 분석의 1차 버전 체크리스트는 부록 정보 부록 B에 나와 있습니다.
Following our search strategy, a total of 613 publications were retrieved in the initial search. Based on eligibility criteria, 55 publications were enrolled in the final study. We then compiled, analyzed, and summarized 53 items on professionalism dilemmas from these enrolled publications and mapped them to the 10 sub-domains of the professionalism framework by Li et al. All enrolled publications, corresponding specific scenarios on dilemmas or challenges and unprofessional behaviors, and the first version checklist from document analysis are shown in Supplementary information Appendix B.
총 두 차례의 포커스 그룹 인터뷰(1라운드에서는 3개 그룹, 2라운드에서는 2개 그룹)를 진행했으며, 50명의 전공의가 참여했습니다. 표 1에는 참가자의 인구통계학적 특성이 요약되어 있습니다. 1차 포커스 그룹 인터뷰에서는 5개의 새로운 항목이 생성되었으며, 2차 인터뷰에서는 새로운 항목이 나타나지 않았습니다. 문서 분석과 두 차례의 포커스 그룹 인터뷰를 거쳐 최종 58개 항목의 전문직업성 딜레마 체크리스트(문서 분석에서 53개 항목, 포커스 그룹 인터뷰에서 5개 항목)가 생성되었습니다(표 2 참조). 58개 항목은 4개의 영역과 10개의 하위 영역으로 나뉘며, 각 영역의 명칭과 포함된 항목 수는 다음과 같다.
- 연민(2),
- 존중(6),
- 의사소통(6),
- 협업(7),
- 성실성(9),
- 의무(5),
- 우수성 추구(8),
- 의료 자원의 공정한 관리(4),
- 환자 기밀성(4),
- 사전 동의(7) .
각 전문직업성 딜레마 항목에 해당하는 발췌문은 보충 정보 부록 C에 나와 있습니다.
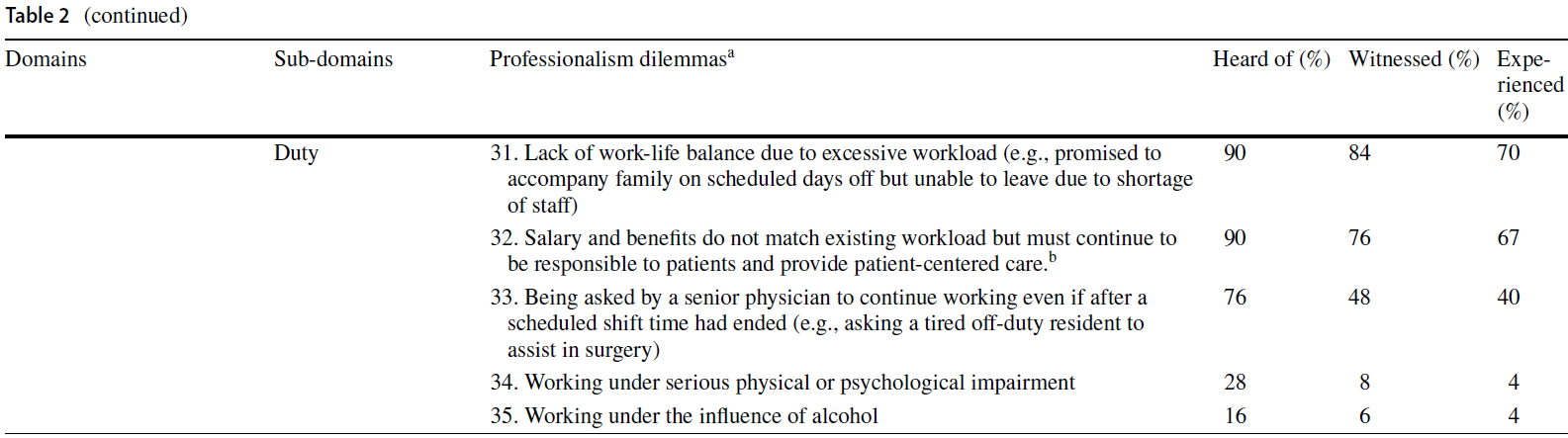
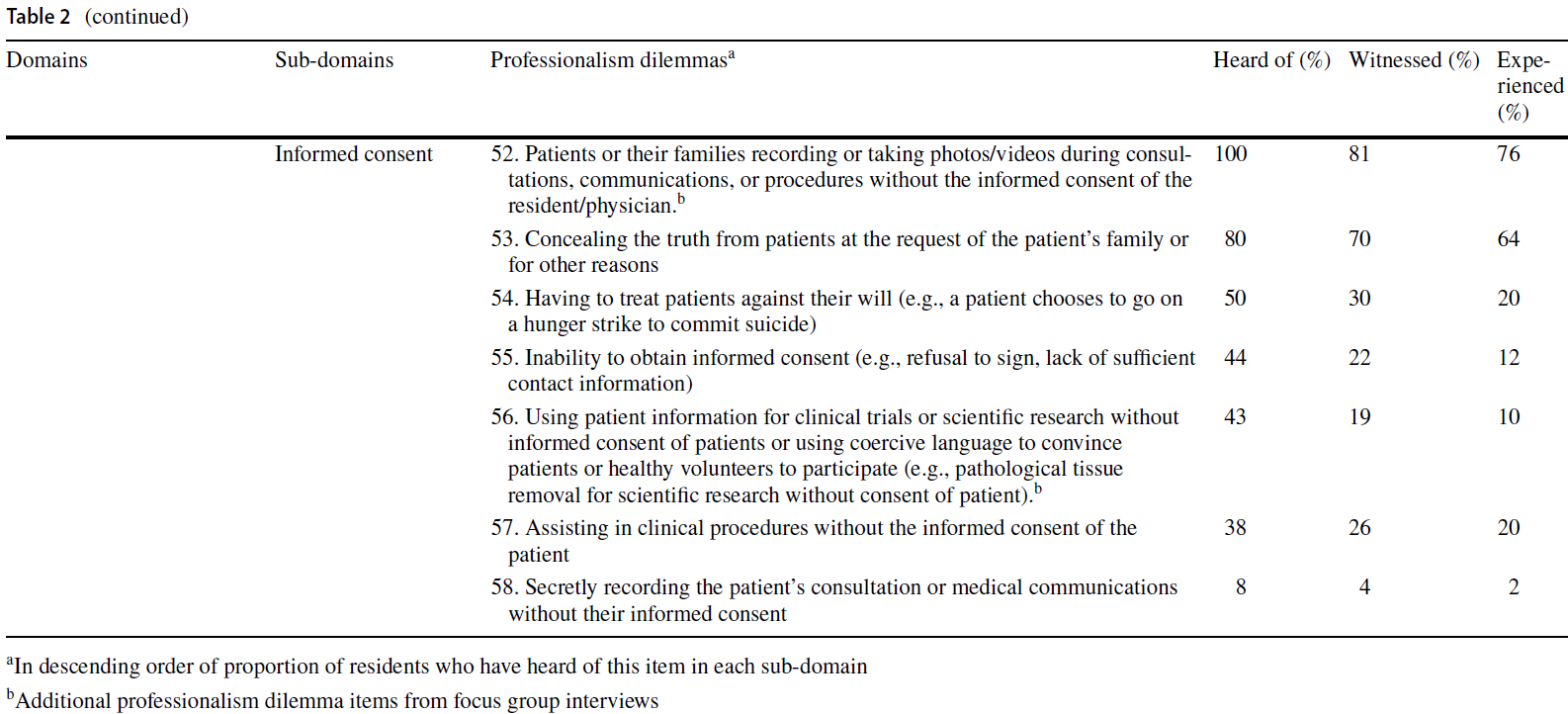
In total, we conducted two rounds of focus group interviews—three groups in round one, and two groups in round two—involving 50 residents. Table 1 summarizes the demographic characteristics of the participants. Five new items were generated in the first round of focus group interviews, and no new items emerged in the second round. After document analysis and two rounds of focus group interviews, a final 58-item checklist of professionalism dilemmas was generated—53 items from document analysis and five items from focus group interviews (see Table 2). These 58 items were distributed in four domains and 10 sub-domains, whose names and the number of contained items were:
- compassion (2),
- respect (6),
- communication (6),
- collaboration (7),
- integrity (9),
- duty (5),
- pursuit of excellence (8),
- fair stewardship of health care resources (4),
- patient confidentiality (4), and
- informed consent (7).
Excerpts corresponding to each professionalism dilemma item are shown in Supplementary information Appendix C.






전문직업성 딜레마 테마
Professionalism dilemma themes
연민 딜레마
Compassion dilemmas
이 테마에는 환자에 대한 연민과 공감과 관련하여 레지던트들이 겪는 어려움을 반영하는 두 가지 딜레마 항목이 포함되어 있습니다. 가장 자주 보고된 딜레마 항목은 연민을 느끼지만 환자를 도울 힘이 없다고 느끼는 경우로, 레지던트의 38%가 경험한 적이 있으며, 이 항목에서 가장 자주 언급된 시나리오는 환자가 높은 의료비 때문에 치료를 포기해야 하는 경우였습니다. 한 참가자는 이러한 딜레마를 다음과 같이 설명했습니다:
This theme contained two dilemma items, reflecting challenges that residents encountered relating to compassion and empathy for patients. The more frequently reported dilemma item was Showing compassion but feeling powerless to help patients, with 38% of residents having experienced it, and the most frequently mentioned scenario within this item was Patients were forced to give up treatment because of high medical expenses. One participant described this dilemma as follows:
가정 경제적인 이유로 치료를 포기하는 환자들이 많은데, 이는 매우 안타까운 일입니다. 솔직히 일부 환자들은 조기에 치료를 받으면 생명을 연장할 수 있는 가능성이 있지만, 가정 형편 때문에 포기하고 집에 가서 병의 자연스러운 진행을 기다려야 합니다. 그들을 도울 수 없다는 것이 안타깝습니다. (A6, 산부인과)
Due to family financial reasons, there are a lot of patients who give up treatment, which is very unfortunate. To be honest, some patients may have the possibility to prolong their lives if they are treated as early as possible, but they give up because of family conditions and have to go home to wait for the natural progression of the disease. It’s a pity that I am unable to help them. (A6, Obstetrics and Gynaecology)
이 항목에서 흔히 보고된 또 다른 시나리오는 기존의 의료 기술로 효과적인 치료를 제공하거나 환자의 고통을 완화할 수 없다는 것이었습니다:
Another common reported scenario within this item was Existing medical techniques cannot offer effective treatment or alleviate patient suffering, as described by one of the participants:
수술 병동에서 한 환자를 만난 적이 있습니다. 그는 나이가 많았고 장암이 재발한 상태였습니다. 수술이 금기인 데다 현재의 기술로는 통증을 해결할 수 없었기 때문에 치료를 포기하고 남은 여생을 집에서 보내기로 결정했습니다. 이런 환자를 만나면 어떻게 해야 할지 모르겠고 아무것도 도와줄 수 없는 것 같아 마음이 아픕니다. (E8, 외과)
I once met a patient in the surgery wards. He was up in age and his bowel cancer had recurred. Because he was contraindicated for surgery and the current technology was not able to resolve his pain, he gave up treatment and chose to spend the rest of his days at home. When I encounter this kind of patient, I feel like I don’t know what to do and can’t do anything to help. (E8, Surgery)
존중 딜레마
Respect dilemmas
이 주제는 환자, 선배 의사, 동료 및 기타 의료 전문가와의 상호존중에 대한 레지던트들의 어려움을 반영하여 6개의 딜레마 항목으로 구성되었습니다. 가장 흔하게 보고된 딜레마는 환자로부터의 직간접적인 언어적 또는 신체적 굴욕감으로, 레지던트의 44%가 이를 경험한 적이 있다고 답했습니다. 레지던트들은 환자로부터 모욕감을 당해도 별다른 조치를 취할 수 없었으며 최대한 참고 견디려고 노력했다고 설명했습니다.
This theme consisted of six dilemma items, reflecting residents’ challenges on mutual respect with patients, senior physicians, peers, and other health care professionals. The most common reported dilemma was Direct or indirect verbal or physical humiliation from patients, with 44% of residents having experienced it. Residents described they could not do much about being humiliated by their patients and tried to just endure and bear with it as much as possible.
환자로부터의 굴욕감은 흔한 일입니다. 예를 들어, 류마티스 질환과 함께 종양이 진행된 한 환자는 정신 건강이 매우 좋지 않았습니다. 그는 진통제를 많이 복용했는데, 류머티즘 약과 함께 "죽여버릴 거야"와 같은 말을 하며 언어적 공격성을 보이기도 했습니다. 무엇이 환자의 행동을 유발했는지는 모르겠지만 그는 우리의 생명을 언어적으로 위협하고 있었습니다. (B7, 내과)
Humiliation from patients is common. For example, a patient with advanced stage tumor combined with rheumatic disease displayed very poor mental health. He would take a lot of pain medication, which, along with the rheumatism medication, led to some verbal aggression, saying words like “I’m going to kill you”. I don’t know what drove the behavior of the patient, but he was verbally threatening our lives. (B7, Internal medicine)
또 다른 흔하게 보고된 딜레마는 선배 의사로부터의 부적절한 비판, 굴욕감 또는 처벌이었습니다. 전공의들은 선배 의사로부터 비판을 받거나 모욕을 당했을 때 선배 의사의 행동을 이해할 수 있지만, 선배 의사가 전공의의 감정을 배려해 환자 앞에서 심하게 말하지 않기를 바란다고 답했습니다.
Another common reported dilemma was Inappropriate criticisms, humiliation, or punishments from senior physicians. When criticized or even humiliated by senior physicians, residents said they could understand senior physicians’ behaviors, but hoped that senior physicians would consider their feelings and try not to speak harshly of them in front of patients.
첫 부서인 신생아 병동으로 로테이션을 갔을 때가 기억납니다. 주치의 선생님은 정말 엄격하셨어요. 처음 갔을 때 많은 사람들 앞에서 제가 잘못한 것을 지적하는 경우가 많았고, 거칠게 들리는 말을 하셔서 기분이 정말 불편했어요. (D6, 소아과)
I remembered when I rotated to my first department, which was the neonatal ward. The senior physician was so strict. When I first got there, she often pointed out what I did wrong in front of a lot of people, and she would say something that sounds harsh, which made me feel really uncomfortable. (D6, Pediatrics)
커뮤니케이션 딜레마
Communication dilemmas
이 주제는 전공의들이 환자와 소통하는 과정에서 겪는 어려움을 반영하여 총 6개의 딜레마 항목으로 구성되었습니다. 6개 딜레마 항목 중 4개 항목에 대해 레지던트의 50% 이상이 해당 항목과 관련된 경험을 보고했습니다. 가장 흔하게 보고된 딜레마는 환자가 개인 연락처 정보를 끈질기게 요구하는 경우로, 레지던트의 90%가 이 문제를 경험한 것으로 나타났습니다. WeChat은 중국에서 인스턴트 메시징, 소셜 미디어, 모바일 결제에 사용되는 주요 독립형 앱입니다. 많은 레지던트들이 개인 생활과 직장 생활 모두에서 이러한 환자들의 반복적인 방해를 경험한 후 더 이상 환자들과 위챗이나 개인 연락처 정보를 공유하지 않겠다고 밝혔습니다.
This theme included six dilemma items, reflecting the challenges that residents encountered in the process of communicating with patients. For four of the six dilemma items, at least 50% of residents reported experiences related to the item. The most common reported dilemma was Patients being persistent for personal contact information, with 90% of residents having experienced it. WeChat is the major standalone app used for instant messaging, social media, and mobile payment in China. Many residents expressed that they would no longer share their WeChat or personal contact information with patients after they had experienced repeated interruptions by these patients in both their personal and work lives.
일반적으로 환자가 제 위챗을 요청하면 검사지를 보낼 수 있도록 알려줍니다. 하지만 환자가 제가 어떻게 대답해야 할지 모르거나 너무 바빠서 제 시간에 응답하지 못하면 환자는 저를 비난합니다. 개인 연락처를 알려줘야 할지 말아야 할지 고민할 때도 있어요. (B6, 내과)
Generally, when the patient asks for my WeChat, I will give him so that I can send him test sheets. But if the patient asks me something I don’t know how to answer or I am too busy to respond in time, he will blame me. Sometimes I struggle with whether or not I should give out my personal contact information. (B6, Internal medicine)환자의 가족은 좋은 사람들이기 때문에 제가 할 수 있는 한 최선을 다해 도와야겠다고 생각하곤 합니다. 하지만 좋은 의도가 실제로 좋은 결과를 가져오는 것은 아니며, 가족들이 더 압박을 받는다는 것을 알게 될 때가 있어요. 그들은 온갖 종류의 질문을 하고 사소한 것까지 물어보곤 했죠. 지금은 환자 가족들에게 제 개인 위챗 정보를 제공하지 않습니다. 감당하기 너무 힘들거든요. 아무리 좋은 환자 가족이라도 나중에 이렇게 골칫거리가 될 수도 있어요. (D10, 소아과)
I may find that my patient’s family members are nice people, so I think to myself that I’d do as much as I can to help them out. But then sometimes I found out that good intentions don’t actually have good results, and the family members will become more pressing. They would ask all kinds of questions and ask about every little thing. I don’t give out my personal WeChat info to patient family members now. It’s too difficult to handle. The nicest family members of patients may still become this troublesome some ways down the road. (D10, Pediatrics)
치료에 협조하지 않는 환자나 가족, 의사소통 및 언어 장벽, 어리거나 경험이 없다고 무시하는 환자도 레지던트들이 흔히 겪는 딜레마였습니다. 레지던트들은 의사소통의 딜레마를 겪을 때 일반적으로 환자와 적극적으로 소통한다고 답했습니다. 그래도 효과가 없을 경우 일부 레지던트는 문제를 보고하고 상사에게 도움을 요청하기도 했습니다.
Patients or their families refusing to cooperate with treatment, Communication and language barriers, and Patients dismissing them as young or inexperienced were also dilemmas commonly reported by residents. Residents said when experiencing communication dilemmas, they would generally actively communicate with patients. If it remained ineffective, some of them would report the problem and turn to their superiors for help.
협업 딜레마
Collaboration dilemmas
이 주제에는 레지던트들이 동료, 선배 의사 및 기타 의료 전문가와 협력하는 과정에서 겪는 어려움을 반영하는 7가지 딜레마 항목이 포함되었습니다. 가장 많이 보고된 딜레마는 다른 의료 전문가와의 협력에 대한 어려움으로, 52%의 레지던트가 이를 경험한 적이 있다고 답했습니다. 한 레지던트는 전문가 간 협업에 대한 불만을 표하기도 했습니다.
This theme included seven dilemma items, reflecting the challenges that residents encountered in the process of cooperating with peers, senior physicians, and other healthcare professionals. The most common reported dilemma was Difficulty in cooperating with other healthcare professionals, with 52% of residents having experienced it. One resident also expressed some displeasure in interprofessional collaboration.
요즘은 의사와 간호사가 동등하다고 하지만, 실제로는 간호사가 우리 레지던트보다 더 높은 지위를 가지고 있다고 느낍니다. 저희가 진료 지시를 내리면 실행은 간호사가 담당하는데, 가끔 급하게 대응해야 하는 경우가 있어서 간호사에게 서둘러 달라고 요청하곤 했어요. 하지만 간호사는 제가 서너 번을 요청할 때까지는 그렇게 하지 않았는데, 나중에 알고 보니 곧 점심시간이 되기 때문이었습니다. 전에도 이런 식으로 동료 전공의를 꾸짖고 울게 만드는 간호사를 본 적이 있습니다. (D1, 산부인과)
Although it’s said that physicians and nurses are equal nowadays, I feel that nurses actually have a higher status than us residents. After we put in a medical order, nurses would be responsible for executing it, but sometimes the order would require an urgent response, so I would ask the nurse to rush it. But the nurse wouldn’t do it until I have asked three or four times, which I found out was because it was going to be her lunch break soon. I have witnessed nurses scolding my peer like this before and sending her crying. (D1, Obstetrics and Gynaecology)
또 다른 일반적인 딜레마는 책임과 업무를 다른 사람에게 미루는 것이었습니다. 한 참가자는 자신의 불만 경험을 이야기했습니다. 하지만 그 상황에서도 상대방의 기분을 상하게 하거나 갈등이나 불편을 초래하고 싶지 않아서인지, 그는 동료에게 자신이 해야 할 일을 계속해달라고 요청하지 않았습니다.
Another common reported dilemma was Pushing responsibilities and work tasks off to others. One participant recounted his experience with grievance. However, even in his situation, possibly out of consideration for not wanting to offend or cause conflict or inconveniences, he did not reach out to ask his peer to continue the work she was supposed to do.
제 앞의 레지던트는 저에게 많은 일을 맡겼습니다. 저는 그런 분들을 만났습니다. 한 아이가 30일 이상 입원해 있었습니다. 단계별 요약과 사례 논의가 필요했습니다. 이 환자를 담당했던 제 동료는 아무것도 쓰지 않았습니다. 결국 저는 어느 날 밤 거의 5시간 동안 혼자서 모든 정보를 작성했습니다. 전화도 하지 않았어요. (D10, 소아과)
The resident before me left a lot of work to me. I have met such kinds of people. A child had been hospitalized for more than 30 days. There needed to be a phased summary and case discussion. My peer, who was responsible for this patient, didn’t write anything. Finally, I spent nearly five hours one night and filled in all the information by myself. I didn’t call her either. (D10, Pediatrics)
무결성 딜레마
Integrity dilemmas
이 주제에는 금전적 이득, 의사와 환자 또는 의료 대리인 간의 관계 등 레지던트들이 정의 또는 정직에 대한 인식을 위반할 수 있는 어려움을 반영하는 9가지 딜레마 항목이 포함되었습니다. 가장 흔하게 보고된 딜레마는 환자로부터의 선물 수락이었으며, 60%의 레지던트가 이를 경험한 것으로 나타났습니다. 레지던트들은 과일과 꽃은 허용되는 선물이지만 빨간 봉투(현금 선물)와 기프트 카드는 반환해야 한다고 생각했으며, 직접 반환할 수 없는 경우 환자의 병원 계좌로 입금해야 한다고 답했습니다. 또한 전공의들은 환자가 방금 입원했는지, 퇴원했는지에 따라 선물의 의미를 다르게 인식했습니다. 퇴원을 앞둔 환자들은 환자 치료가 잘 안 될까 봐 의사의 비위를 맞추기 위해 억지로 선물을 주기보다는 레지던트들의 노고에 감사하는 마음에서 진심으로 선물을 준다고 인식하고 있었습니다.
This theme included nine dilemma items, reflecting the challenges that residents encountered that may violate their perceptions of justice or honesty, including financial gains and relationships between physicians and patients or medical representatives. The most common reported dilemma was Accepting gifts from patients, with 60% of residents having experienced it. Residents thought that fruits and flowers were acceptable gifts, but red envelopes (cash gifts) and gift cards should be returned, including crediting the patient’s hospital account when the money could not be returned in person. Residents also viewed the meaning of gifts differently depending on whether patients were just admitted to hospital or after they had been discharged. Residents perceived that patients who are about to be discharged from hospital give gifts due to their appreciation of the residents’ work and from a place of real gratitude, rather than because they are forced to please the doctors for fear of poor patient care.
사실 선물은 아주 흔한 일이라고 생각합니다. 환자가 돈 대신 무언가를 줄 수 있다는 것은 의사에게 마음에서 우러나오는 감사의 표시이자, 의사와 환자 간의 화합을 도모할 수 있는 방법이기도 합니다. 과일뿐만 아니라 지역 특산품도 선물하는 환자분들을 많이 봤습니다. (C7, 외과)
I think gift-giving is actually quite common. When a patient can give something instead of money, it shows that he is grateful to the physician from his heart, and it is also a way to promote harmony between doctors and patients. I see that patients not only give fruits but also local specialties. (C7, Surgery)
또 다른 공통된 딜레마는 가족이나 친구에게 연고주의를 보이는 것으로, 36%의 레지던트가 경험한 적이 있다고 답했습니다. 전공의들은 주로 사회적 관계 역학 관계에 따라 이러한 행동을 이해할 수 있다고 생각했습니다. 한 참가자는 자신의 진료 예약일 경우 친한 의사에게 도움을 요청하기 위해 줄을 서는 경우도 있다고 답했습니다.
Another common reported dilemma was Showing nepotism for family and friends, with 36% residents having experienced it. Residents believed this kind of behavior to be understandable, mainly out of adherence to social relationship dynamics. One participant reported that he would even jump the queue to seek help from a familiar physician if it was his own medical appointment.
저는 제 진료를 위해 대기열을 건너뛰고 주치의가 여의치 않으면 무료 진찰을 해줄 수도 있습니다. 예를 들어, 동료의 가족이 입원해야 하는 경우, 주치의는 실제로 기꺼이 도움을 주고 외래 진료실이나 입원 병동을 배정하는 등 일반적으로 거절하지 않는 것을 보았습니다. (B2, 내과)
I would jump the queue for my own medical treatment, then the senior physician may provide me with a free examination if convenient. I have seen that, for example, if a peer’s family members needed to be hospitalized, the senior physician would in fact be willing to provide help and would generally not refuse, such as arranging an outpatient clinic or inpatient ward for them. (B2, Internal medicine)
지각이나 결근 시 서명을 위조하거나 동료에게 대신 서명을 부탁하는 것도 흔한 딜레마로 보고되었습니다. 레지던트들은 임상 업무와 의학 강의 참석의 균형을 맞추는 것이 어렵다고 보고했습니다. 한 참가자는 다른 사람이 의학 강의에 로그인하는 것을 도와주는데 거절하는 방법을 모른다고 말했습니다.
Forging signatures or asking peers to sign on one’s behalf when late or absent was also a common reported dilemma. Residents reported finding it difficult to balance clinical work with medical lecture attendance. One participant reported he would help others sign in for medical lectures and did not know how to refuse.
다른 사람을 위해 로그인했다가 행정 직원에게 발각되어 경고를 받았습니다. 동료가 저에게 대신 로그인해 달라고 요청하면 "강의는 들으러 가겠지만 대신 로그인해 줄 수 없습니다"라고 말할 수 없을 것 같습니다. (C10, 외과)
I signed in for others and was found and warned by the administrative staff. If a peer asked me to sign in for him, I don’t think I could say something like “I will go to the lecture, but I cannot sign in for you”. (C10, Surgery)
의무 딜레마
Duty dilemmas
이 주제에는 전공의들이 직무를 수행하면서 직면하는 어려움을 반영하는 5가지 딜레마 항목이 포함되었습니다. 가장 많이 보고된 딜레마는 과도한 업무량으로 인한 일과 삶의 균형 부족으로, 70%의 전공의가 이를 경험한 적이 있다고 답했습니다. 레지던트들은 과중한 업무량으로 인해 휴일에도 초과 근무를 하는 것이 일반적이라고 생각했습니다. 특히 외과 전공의와 산부인과 전공의는 수술의 복잡성이나 양이 많아 밤늦게까지 일하는 경우가 많다고 답했습니다.
This theme included five dilemma items, reflecting the challenges that residents faced in fulfilling their professional duties. The most common reported dilemma was Lack of work-life balance due to excessive workload, with 70% of residents having experienced it. Residents believed it to be common to work overtime due to heavy workloads, even during holidays. In particular, surgery residents and obstetrics and gynecology residents said that they often worked late at night because of the complexity or volume of operations.
외과에서 과중한 업무량은 매우 흔한 일이라고 생각합니다. 일과 삶의 균형을 맞추기 어려운 것은 어쩔 수 없는 일입니다. 그것은 우리가 감당할 수 있는 일이 아닙니다. 환자에게 수술이 필요하거나 수술이 매우 복잡합니다. 이런 상황에서는 어떻게 해야 할까요? (C1, 외과)
I think the heavy workload in surgery is extremely common. It is inevitable that it is difficult to balance work and life. It’s not something that we can deal with. The patient needs an operation or the operation is very complex. What can anyone do in this situation? (C1, Surgery)
또 다른 일반적인 딜레마는 급여와 복리후생이 기존 업무량과 일치하지 않는 것으로, 67%의 레지던트가 이를 경험한 적이 있다고 답했습니다. 레지던트들은 의사와 마찬가지로 환자 중심의 자세를 가져야 하지만, 낮은 급여와 발생하는 특정 문제를 해결할 수 없는 현실에 괴로워하며 성과에 기반한 공정한 임금 분배를 요구했습니다.
Another common reported dilemma was Salary and benefits do not match existing workload, with 67% of residents having experienced it. Residents should hold the same patient-centered attitude as physicians, but plagued by low salary and the inability to resolve certain problems that arise, they called for performance-based fair distribution of wages.
우리는 매우 바쁘고 거의 모든 일을 하고 있습니다. 우리 사이에는 "일할 때는 의사이지만 돈을 계산할 때는 학생이다"라는 속담이 있습니다. 모두가 잘 알고 있는 말입니다. (E7, 외과)
It’s obvious that we are very busy, and we do almost everything. There is a very popular saying between us, which is, “you are a doctor when you work, and you are a student when they count money”. Everyone knows this well. (E7, Surgery)
레지던트의 40%는 과중한 업무량과 낮은 급여의 어려움 외에도, 매우 피곤한 상황에서도 예정된 근무 시간이 끝난 후에도 선배 의사로부터 계속 일해달라는 요청을 받은 경험이 있다고 답했습니다. 레지던트들은 육체적, 정신적으로 피곤한 상태에서 환자를 수술하는 것이 환자 안전을 위협할 수 있다고 생각했지만 위계적인 구조 때문에 용기를 내어 거절하지 못했습니다.
In addition to the challenges of heavy workload and low pay, 40% of residents experienced Being asked by a senior physician to continue working even after a scheduled shift time had ended, even when they were very tired. Residents thought that performing surgery on patients when they were physically and mentally fatigued would threaten patient safety, but due to the hierarchical structure, they were not brave enough to say no.
일이 너무 많다고 생각해요. 산부인과에서 야간 당직을 서고 있었는데, 밤새도록 일하다 보니 거의 하루 종일 쉬지 않고 밤낮으로 일했죠. 그런데 야간 근무를 마치고 퇴근할 때 선배 의사에게 수술이 있다고 연락이 왔어요. 그 당시 저는 이미 매우 졸려서 수술실에서 선배 의사에게 기계적으로 협조하고 있었어요. 저에게는 매우 고통스러웠고, 만약 문제가 생기면 환자에게 책임질 수 없다고 생각했습니다. (D3, 산부인과)
I think it’s too much work. I was on a night shift in obstetrics, and I had been up all night, which was basically a day and a night without a break. However, when I was leaving the night shift, I was pulled in by the senior physician for a surgery. I was already very sleepy at that time, just mechanically cooperating with the senior physician in the OR. It was very excruciating for me, and I don’t think we were being responsible to the patient if something goes wrong. (D3, Obstetrics and Gynaecology)
우수성 딜레마
Excellence dilemmas
이 주제는 전공의들이 임상술기 향상이나 과학적 지식 습득 등 탁월함이나 자기계발을 추구하는 과정에서 겪는 어려움과 도전을 반영하여 총 8개의 딜레마 항목으로 구성되었습니다. 가장 많이 보고된 딜레마는 '과학 연구, 시험, 임상 업무의 압력 사이에서 균형을 맞추기 어려움'이었으며, 전공의의 58%가 이를 경험한 적이 있다고 답했습니다. 레지던트들은 연구 성과가 승진을 위한 필수 요건임에도 불구하고 퇴근 후를 제외하고는 낮에 과학 연구를 할 수 있는 시간이 매우 제한적이라고 언급했습니다. 심지어 시험이 있는 날에도 선배 의사들은 전공의들이 퇴근하는 것을 꺼려했습니다.
This theme included eight dilemma items, reflecting the difficulties and challenges that residents encountered in the process of pursuing excellence or self-improvement, such as improving clinical skills or acquiring scientific knowledge. The most common reported dilemma was Difficulty balancing pressures from scientific research, examinations, and clinical work, with 58% of residents having experienced it. Residents mentioned that there was very limited time for scientific research during the day, except after work, despite research achievements being a requirement for promotion. Even in the face of exams, senior physicians were reluctant to let them off work.
예를 들어, 시험이 다가오는데 상사는 제가 교육을 받으러 왔다고 생각해서 계속 일해야 한다고 생각하죠. 시험 준비를 위한 휴가를 주지 않았고, 제가 휴가를 요청해도 승인하는 것을 매우 꺼려했습니다. (E3, 내과)
For example, there would be an exam coming up, but the superior would think that I am here for training, so I have to work for him. He wouldn’t give me leave to prepare for my exams, and he would be very reluctant to approve any leave when I ask. (E3, Internal medicine)
레지던트들은 때때로 임상 진료 표준을 준수하지 않는 정상화 실패를 보고했습니다. 한 참가자는 전공의의 표준 이하의 의료 행위를 언급했고, 그 영향을 받아 레지던트도 같은 행동을 하기 시작했습니다.
Residents sometimes reported Normalizing failures to adhere to clinical practice standards. One participant mentioned substandard medical practices by the senior physician, and under his influence, the resident began to do the same.
제 선배 의사는 임상 능력이 뛰어납니다. 하지만 그는 항상 장갑 없이 드레싱을 갈아입고, 환자를 진찰할 때도 장갑을 사용하지 않습니다. 하지만 그는 매우 유능한 의사였고, 모든 사람들이 우리 부서장보다 훨씬 더 숙련되었다고 말했습니다. 그러다 보니 저도 익숙해져서 장갑을 끼지 않는 경우가 많아요. (C5, 외과)
My senior physician has excellent clinical competence. However, he always changes dressings without gloves and also doesn’t use gloves when examining patients. But he is a very capable doctor, with everyone commenting that he is even more skilled than our department director. Then I got used to it as well, so I often don’t wear gloves either. (C5, Surgery)
또 다른 딜레마는 자신의 능력을 넘어서는 의료 업무를 독립적으로 완수하도록 부탁받는 것입니다. 레지던트의 10%만이 이러한 경험을 했다고 답했지만, 이러한 행동의 결과는 심각할 수 있으며 잠재적으로 환자 안전을 위협할 수 있습니다. 한 참가자는 자신이 겪은 위태로운 경험을 보고했지만 결과는 긍정적이었습니다.
Another dilemma was Being asked to independently complete medical tasks beyond one’s ability. Although only 10% of residents reported they experienced this, the consequences of this behavior can be serious and may potentially threaten patient safety. One participant reported a precarious experience he had, though the outcome was positive.
한 번은 선배 의사가 근무를 마치고 집으로 돌아갔고, 저도 퇴근 후 집에 가야 했는데 환자의 배액관이 떨어졌습니다. 이때 어떻게 해야 할지 몰라 선배 의사에게 전화를 걸어 상황을 사진으로 찍어 보내 어떻게 해야 할지 물어봤어요. 그는 저에게 혼자서 처리하라고 했습니다. 저는 망설였지만 시키는 대로 했습니다. 시술 도중에 환자가 고통스러워 비명을 지르기 시작했고, 저는 튜브가 복막에 닿았을지도 모른다고 생각했습니다. 저는 배액관을 빼서 소독하고 다시 시술을 진행했고, 두 번째 시술은 순조롭게 진행되었습니다. 수술 내내 침착해 보였지만 속으로는 많이 긴장했어요! (C1, 외과)
Once my senior physician went home after his shift, and I was supposed to go home after work, but a patient’s drainage tube fell off. At this point, I did not know what to do, so I called my senior physician and sent photos of the situation to ask what to do. He told me to take care of it alone. I hesitated but did as he asked. Halfway through the procedure, the patient started to scream in pain, so I thought the tube might have touched his peritoneum. I withdrew the drain to sterilize and performed the procedure again, which worked out smoothly the second time. I looked calm the whole time, but I was very nervous inside! (C1, Surgery)
의료 자원의 공정한 관리에 대한 딜레마
Dilemmas on the fair stewardship of health care resources
이 주제에는 의료 자원의 불공정한 관리를 다룰 때 전공의들이 겪는 어려움을 반영하는 네 가지 딜레마 항목이 포함되었습니다. 가장 흔하게 보고된 딜레마는 불필요한 의료 서비스나 처방을 계속 요구하는 환자로, 66%의 전공의가 이를 경험한 적이 있다고 답했습니다. 병원에 입원한 일부 환자는 의료 보험이 입원 환자 검사에 대해서만 환급을 해준다는 이유로 질병과 관련 없는 추가 의료 검사를 요구한다고 언급했습니다. 또한 일부 환자는 기대만큼 효과가 없을지라도 회복을 앞당기기 위해 의사에게 더 높은 등급의 항생제나 더 비싼 약을 처방해달라고 요청했습니다.
This theme included four dilemma items, reflecting the challenges that residents encountered when dealing with unfair stewardship of health care resources. The most common reported dilemma was Patients persisting to ask for unnecessary medical services or prescriptions, with 66% of residents having experienced it. Residents mentioned that some patients admitted to the hospital asked for additional medical tests not related to their disease because their medical insurance would only reimburse them for inpatient tests. Some patients also asked physicians to prescribe higher-grade antibiotics or more expensive drugs to accelerate their recovery, even if these drugs would not be as effective as they expect.
환자는 약간의 사소한 문제가 있었고 치질로 병원에 왔습니다. 그런 다음 그는 그것을 전체 검진으로 취급하고 모든 것을 확인하고 싶어했습니다. 저는 그에게 단순한 치질이라고 설명했지만 그는 제가 거짓말을한다고 생각했고 심지어 게으르다고 비난했습니다. 이런 환자에게 뭐라고 말해야 할지 모르겠어요. (C3, 외과)
The patient had some minor problems and came to the hospital for hemorrhoids. Then he treated it as a full checkup and wanted to check everything. I explained that it was simple hemorrhoids to him, but he thought I was lying to him and even accused me of being lazy. I don’t know what to say to patients like this. (C3, Surgery)
전공의들은 선배 의사들의 과잉진료를 목격했다고 보고했습니다. 그러나 일부 전공의는 의학 지식이 부족해 선배 의사의 과잉진료 여부를 판단할 수 없었다고 답했다.
Residents reported that they witnessed Overtreatment by senior physicians. However, some residents also expressed that their medical knowledge was limited, so they could not judge whether the senior physicians were indeed overtreating.
저는 과잉진료에 대해 듣고 목격한 적이 있습니다. 한 번은 주치의가 적응증과 가이드라인을 초과하는 약물과 용량을 조합하여 사용한 적이 있습니다. 그에게는 이유가 있었어요. 더 안전하고 원활하게 치료하고 싶었을 뿐이었죠. 그래서 주치의에게 물어봤고, 주치의는 괜찮다고 대답했지만 여전히 기존 임상 지침에 부합하지 않는다고 생각했습니다. (C10, 외과)
I did hear about and witness excessive medical treatment. Once, my attending physician used drugs and dosages in combinations that exceeded the indications and guidelines. He had his reasons; he just wanted to make it safer and smoother. So, I asked him about it, he answered me, and I thought it was ok, but it still didn’t meet the existing clinical guidelines. (C10, Surgery)
환자 기밀 유지에 대한 딜레마
Dilemmas on patient confidentiality
이 주제는 전공의들이 환자 비밀을 지키는 데 겪는 어려움과 과제를 반영하여 4개의 딜레마 항목으로 구성되었습니다. 한 참가자는 동료 레지던트들이 환자의 개인정보나 신원과 관련된 정보를 소셜 미디어에 게시하는 것을 목격했다고 공유했습니다. 그녀는 이러한 행동이 비전문직업적이라고 생각했지만, 이에 대해 아무런 조치를 취하지 않았습니다.
This theme included four dilemma items, reflecting the difficulties and challenges that residents encountered in keeping patient confidentiality. One participant shared that her peers were involved in Posting information related to a patient’s privacy or identification on social media. Though she thought the behavior was unprofessional, she did not take any action on it.
다른 사람들이 정말 귀여운 아이들의 사진이나 동영상을 찍어 모자이크 없이 WeChat이나 웨이보에 게시하는 것을 본 적이 있습니다. 나쁜 의도는 없었다고 생각하지만 여전히 좋은 행동은 아닌 것 같아요. (D8, 소아과)
I have seen others take photos or videos of really cute kids and then post them on WeChat or Weibo without mosaics. I don’t think they had any ill intentions, but it’s still not a very good thing to do. (D8, Pediatrics)
사전 동의에 관한 딜레마
Dilemmas on informed consent
이 주제에는 환자와 의사 모두 사전 동의 위반 시 레지던트들이 겪는 어려움을 반영하는 7가지 딜레마 항목이 포함되었습니다. 가장 흔하게 보고된 딜레마는 환자 가족의 요청이나 다른 이유로 환자에게 진실을 숨기는 것이었습니다. 레지던트들은 환자가 자신의 질병에 대해 알 권리가 있다고 믿지만, 문화적 전통과 부작용에 대한 두려움 때문에 환자의 상태를 가족에게 먼저 알리는 것을 우선순위로 삼았습니다.
This theme included seven dilemma items, reflecting the challenges that residents encountered in violations of informed consent, for both patients and physicians. The most common reported dilemma was Concealing the truth from patients at the request of the patient’s family or for other reasons. Even though residents believed that patients had the right to know about their illness, due to cultural traditions and fear of adverse consequences, they still made it a priority to inform the family member first about the patient’s condition.
악성 종양에 걸린 환자가 있었는데 아들이 그 사실을 숨겼습니다. 제가 그 환자라면 저도 제 병에 대해 알 권리가 있다고 생각했습니다. 시간이 얼마 남지 않았더라도 앞으로 어떻게 해야 할지 알고 후회하지 않아야 한다고 생각했습니다. 하지만 환자가 정신적으로 무너지고 살 시간이 줄어들지 않도록 숨기는 것이 좋을 수도 있습니다. 하지만 그래도 환자에게 알려야 한다고 생각해요. (A1, 산부인과)
I had a patient who had a malignant tumor that she didn’t know about, and her son kept it from her. I thought if I was that patient, I should have the right to know my illness. Even if I don’t have much time left, I would want to know what I should do next and have no regrets. But maybe it’s good for him to keep it from her, lest she break down mentally and have less time to live. But I still think the patient should be told. (A1, Obstetrics and Gynaecology)악성 종양을 가진 일부 환자의 경우 가족들이 의사에게 "아직 환자에게 말하지 말아주세요"라고 말합니다. 중국인의 눈에는 환자에게 말하면 환자가 소식을 견딜 수 없을 수도 있습니다. (B1, 내과)
For some patients with malignant tumors, their families will say to the doctor, “Please don’t tell the patient yet.” In the eyes of Chinese people, if you tell the patient, he may not be able to bear the news. (B1, Internal medicine)
전공의들은 사전 동의를 받을 수 없는 상황에 대해 불만과 무력감을 표했습니다. 법과 정책에 따라 사전 동의서에 서명하지 않으면 환자는 수술이나 처방과 같은 특정 의료 서비스를 제공받을 수 없습니다.
Residents expressed frustration and helplessness when it came to Inability to obtain informed consent. Due to laws and policies, without signing informed consent, patients cannot be provided certain medical services, such as surgeries or prescriptions.
저희 내과에서는 큰 수술은 하지 않지만 스텐트 삽입과 같은 최소 침습적 시술은 시행합니다. 동맥이 막혀 스텐트 삽입이 필요한 위독한 상태의 환자가 있었습니다. 하지만 가족들은 반대했습니다. 가족들은 특정 종교적 신념이 있는 것 같았고 동의서에 서명하기를 거부했습니다. 시술을 진행하기 위해 서명을 강요할 수 없었기 때문에 환자의 의료 기록에 무슨 일이 있었는지 기록할 수밖에 없었습니다. (E6, 내과)
We don’t do major surgical procedures in our internal medicine department, but we do perform some minimally invasive procedures like stenting. I had a patient who was in a critical condition and had a blocked artery and needed stenting. But his family members disagreed. They seemed to have certain religious beliefs and refused to sign the consent form. Well, then we could only make a note of what happened in the patient’s medical record, because we couldn’t force them to sign anything for the procedure to go ahead. (E6, Internal medicine)
첫 번째 인터뷰 라운드에서 새로운 딜레마 항목이 등장했습니다: 환자나 그 가족이 오디오 녹음을 하거나 사진/비디오를 찍는 것이었습니다. 레지던트들은 이러한 행동이 의사의 사전 동의를 위반하는 것으로 인식했지만, 이를 막거나 그냥 넘어가는 등 서로 다른 반응을 보였습니다.
During the first round of interviews, a new dilemma item emerged: Patients or their families making audio recordings or taking photos/videos. Residents perceived such a behavior as a violation of informed consent for the physician but reacted differently toward it, either stopping it or letting it go.
토론
Discussion
문서 분석과 포커스 그룹 인터뷰를 통해 행동 기반 관점에서 전문직업성 딜레마 체크리스트를 개발했습니다. 체크리스트에는 4개 영역에 걸쳐 58개 항목과 10개 하위 영역이 포함되어 있습니다. 문서 분석은 수많은 기존 출판물을 바탕으로 이루어졌기 때문에 체크리스트에 포함된 대부분의 전문직업성 딜레마는 국제 사회에도 적용될 수 있습니다(보충 정보 부록 B 참조). 예를 들어, 레지던트가 전문직업성 결여와 문제를 목격하거나 직접적으로 관련된 선행 연구에서 보고된 것(예: 환자에 대한 차별적이고 무례한 대우, 환자 대상화 및 표준 이하의 진료, 자신의 능력 이상의 수행 요구, 환자에게 공개적으로 모욕당함)이 이에 해당합니다. 또한 중국 문화에 고유한 전문직업성 딜레마, 특히 문화 간 전문직업성 딜레마에 대해 Ho 등이 보고한 내용을 정리했으며(Ho 등, 2017), 이러한 딜레마의 각각의 근거를 지적하고 원칙, 의미, 영향 및 문화적 규범을 언급했습니다(Ho 등, 2012).
Through document analysis and focus group interviews, we developed a checklist of professionalism dilemmas from a behavior-based perspective. The checklist included 58 items over four domains, with 10 sub-domains. Since document analysis drew from a plethora of existing publications, most of the professionalism dilemmas in our checklist would be applicable to the international community (see Supplementary information Appendix B), such as those reported by previous studies on residents observing or being directly involved in professionalism lapses and challenges (e.g., discriminatory and disrespectful treatment of patients, objectification of patients and substandard practice, being asked to perform beyond their capability, being openly humiliated by patients). We also collated some professionalism dilemmas that are unique to the Chinese culture, especially intercultural professionalism dilemmas reported by Ho et al. (Ho et al., 2017), who also pointed out these dilemmas’ respective rationales, referencing principles, implications, affects, and cultural norms (Ho et al., 2012).
본 연구에서 전문직업성 딜레마의 중요한 원인은 "거절하기 어려움"에 기인할 수 있습니다. 중국인과 미국인의 거절 전략에 대한 비교 연구에 따르면 미국인은 중국인보다 직접 거절을 훨씬 더 자주 사용하며(Cai, 2009), 중국인의 개인적 경계에 대한 내재적 장애물인 미안지(얼굴)를 발견했습니다. Mianzi는 중국인들은 체면을 잃는 것에 큰 불쾌감을 느끼며 체면이 손상되는 상황을 피하기 위해 항상 노력한다는 점에서 중국 문화에 깊이 뿌리내린 심리사회적 구조입니다. 레지던트가 상사에게 거절하는 것은 이미 전 세계적으로 공통적으로 발생하는 병원 위계질서와 의료 시스템의 숨겨진 커리큘럼으로 인해 어려운 일입니다(Chang et al., 2017; Komaromy et al., 1993). 이는 때때로 전공의가 자신의 능력을 넘어서는 의료 업무를 수행하도록 요구받거나(우수성-43) 과도한 육체적, 정신적 피로에도 불구하고 초과 근무를 해야 하는 경우(의무-33)와 같이 환자 안전을 위험에 빠뜨리기도 합니다. 특히 레지던트가 자신의 진료 수준을 저하시킬 수 있는 업무에 직면했을 때 자유롭게 의견을 말할 수 있도록 제도적 차원에서 보다 전문직업적인 업무 문화를 장려하기 위해 모든 노력을 기울여야 합니다.
An important source of professionalism dilemmas in our study could be attributed to “difficulty saying no”. A comparative study of Chinese and American refusal strategies found that Americans use direct refusal far more frequently than the Chinese (Cai, 2009), with mianzi (face) being an inherent obstacle to personal boundaries for Chinese. The psychosocial construct of mianzi is deeply rooted in Chinese culture in that people take great offense at any loss of face, and efforts are always made to avoid face-risking situations. It is already difficult for residents to say no to their superiors owing to hospital hierarchy and the hidden curriculum of the health care system, which is a common occurrence throughout the world (Chang et al., 2017; Komaromy et al., 1993). This may sometimes even place patient safety at risk, such as when residents are required to perform medical tasks beyond their ability (Excellence-43) or when they are required to work overtime despite excessive physical and mental fatigue (Duty-33). Every effort should be made to encourage a more professional work culture, especially at a systemic level, so that residents can have the freedom to speak up when they are faced with tasks that may compromise their level of care.
친구나 동료와 같은 지인의 부탁을 거절하기는 어렵지만, 특히 중국인 전공의의 경우 더욱 그러할 것으로 보입니다. 전공의들은 친구가 우선 의료 예약을 요청하거나(청렴성-23) 동료를 위해 로그인해 달라는 요청(청렴성-24)과 같은 특정 행동이 연고주의이며 도덕적 청렴성의 기본 원칙에 위배된다는 것을 이해하지만, 대부분은 여전히 이러한 요청에 '예'라고 답합니다. 중국 문화에서 이러한 행동은 사회의 조화로운 균형에 중요한 역할을 하는 렌칭renqing의 교환(Chen, 2005; Wang & Pak, 2015)에 기인할 수 있습니다. 지인이 이러한 문제를 해결하도록 돕는 것은 전공의들에게 체면을 세워줄 수 있지만, 도움을 거부하면 지인의 관계적 기대에 위배될 뿐만 아니라 유교 윤리에 기반한 더 넓은 사회적 규범에 위배되어 양측 모두 체면을 잃게 되는 경우가 많습니다(Bedford, 2022). 신뢰의 감소는 지인 네트워크 내에서 화합이라는 가장 중요한 사회적 가치를 상쇄했다는 것을 의미할 수 있습니다.
While it is difficult for residents to say no to their acquaintances, such as friends or peers, this seems to especially be the case for Chinese residents. Although residents understand that certain behaviors, such as when friends request priority medical bookings (Integrity-23) or when they are asked to sign-in for peers (Integrity-24), are nepotic and violate basic principles of moral integrity, most will still choose to say yes to these requests. In Chinese culture, this kind of behavior can be attributed to an exchange of renqing (Chen, 2005; Wang & Pak, 2015), which is crucial to the harmonious balance of society. Helping acquaintances resolve these troubles would add much face for the residents, but if they refuse to help, it would not only violate the relational expectations of the acquaintance, it would also violate a wider social norm grounded in Confucian ethics, often resulting in both parties losing face (Bedford, 2022). The reduction in trust may imply that you have offset the paramount social value of harmony within this network of acquaintances.
중국인들은 또한 일부 어려운 환자의 요청을 거절하는 데 어려움을 겪고 있다고 보고했습니다. 전공의의 나이가 젊어 보인다는 이유만으로 전공의가 잘 할 수 있는 시술을 더 높은 수준의 의사에게 의뢰하거나(의사소통-10, 12), 환자가 불필요하거나 과한 의료 서비스를 요구하는 경우(의료 자원의 공정한 관리-44) 등 불합리해 보이는 요청에도 환자의 고집에 타협하는 경우가 있다고 합니다. 이제 막 입사한 레지던트가 환자의 요청에 따라 개인 연락처를 알려주는 데 동의하는 현상도 있습니다(커뮤니케이션-9). 레지던트들은 학부 의학교육 과정에서 배운 이타주의의 강한 영향력을 "내가 할 수 있는 한 많이 도와야 한다"와 같은 말로 간접적으로 자주 언급했습니다. 이타주의는 조화로운 의사-환자 관계를 구축하려는 궁극적인 목표와 함께 강조되는 핵심 요소일 수 있습니다(Luo et al., 2017). 그러나 이러한 바람직한 결과를 달성하기 위해서는 좋은 이타적 의도와 적절한 전문직업성 교육 및 제도적 지원이 병행되어야 합니다. 중국에서는 위챗이 주요 커뮤니케이션 앱으로 성장했으며, 일부 중국 의사들은 지속적인 진료를 제공하기 위해 위챗에 자체 환자 그룹을 개설하기도 합니다(Zhang, 2017). 그러나 의사들은 WeChat 연락처를 가진 환자로부터 지속적으로 압박을 받거나 심지어 괴롭힘을 당한다고 보고했으며, 이로 인해 의사들은 환자에게 개인 연락처 정보를 제공할지 여부를 놓고 고민하고 있습니다. 이러한 상황이 만연해 있으므로 레지던트는 임상 로테이션을 시작하기 전에 사적인 채널을 통해 환자와 소통할 경우 어떤 결과가 초래될 수 있는지 알려야 합니다. 여기에는 일과 휴식 사이의 뚜렷한 이분법 부족, 비공식적인 상담으로 인한 잠재적 오진 및 위험 등이 포함될 수 있지만 이에 국한되지는 않습니다(Hu, 2020). 이 모든 것은 중국의 의료 교육에 개인정보 보호 및 정보 관리 교육이 포함되어야 함을 시사하며, 이는 현재 아직 개발 중입니다. 일부 중국 의료진이 사적인 채널을 통해 환자와 소통하는 이유에 대해서는 병원 내 공개 커뮤니케이션 채널의 활용도가 낮고(Liu, 2017) 미국, 영국, 호주 등 국가에서 이미 시행 중인 전문직업성에 대한 통일된 소셜 미디어 가이드라인이 없기 때문이며(DeJong, 2018), 중국 의료기관은 일반적인 권고 사항(예: 사적인 채널을 통해 진단이나 치료를 해서는 안 된다)만 제시하고 비공식 커뮤니케이션 채널에 대한 명확한 제한을 설정하지 않았기 때문이라고 설명합니다. 이와 같은 의사들의 딜레마를 해결하기 위해서는 전문직업성 교육이 무엇보다 중요하지만, 국가 차원에서 소셜 미디어 가이드라인을 마련하고, 병원은 공개 및 내부 커뮤니케이션 시스템을 강화하며, 지역사회 차원에서 이러한 주제에 대한 환자 교육을 실시할 것을 권장합니다.
Chinese residents also reported difficulty saying no to the requests of some difficult patients. Even if requests seem unreasonable, the resident may compromise at the patient’s insistence, such as when patients request a higher-level physician for a procedure the resident can well take care of simply because the resident appears young in age (Communication-10 & 12) or when patients request unnecessary or over-the-top medical services (Fair stewardship of health care resources-44). A phenomenon is that some residents who are just entering the workplace would agree to give patients their personal contact information at the patient’s request (Communication-9). Residents have frequently, and sometimes indirectly, referenced the strong influence of altruism taught during their undergraduate medical education, with statements such as, “helping as much as I can”. Altruism may be a key factor here, emphasized with the ultimate goal to build a harmonious physician–patient relationship (Luo et al., 2017). However, to achieve this desired outcome, good altruistic intentions would need to be paired with appropriate professionalism training and institutional support. In China, WeChat has grown to become the primary communications app, and some Chinese physicians establish their own patient groups on WeChat to provide continuation of care (Zhang, 2017). However, residents have reported being constantly pressed or even harassed by patients who have their WeChat contact, which leaves residents struggling with whether to give patients their personal contact information. Given the pervasiveness of these situations, residents should be informed the consequences of communicating with patients through private channels prior to the start of their clinical rotations. These may include but are not limited to lack of a distinct dichotomy between work and rest and potential misdiagnoses and risks arising from informal consultations (Hu, 2020). All of this suggest that medical education in China should include privacy and information management training, which is currently still under development. As for why some Chinese medical staff continue to communicate with patients through private channels, it comes down to poorly utilized public communication channels in hospitals (Liu, 2017) and the lack of unified social media guidelines on professionalism, such as those already in effect in countries such as the US, UK, and Australia (DeJong, 2018), and Chinese medical institutions have only provided general recommendations (e.g., diagnoses or treatment should not be done via private channels) but have not established clear restrictions on unofficial communication channels. While professionalism education is paramount in the wake of this type of dilemma for residents, we also recommend that social media guidelines be set at a national level, hospitals strengthen their public and internal communication systems, and patient education on these topics be provided at the community level.
한 레지던트는 동료가 모자이크(프라이버시 보호를 위해 사진을 디지털 픽셀로 처리한 것) 처리 없이 소아 환자의 사진을 WeChat 모멘트에 게시하는 것을 목격했다고 언급했습니다(환자 기밀-50). 의사나 레지던트가 의도적이든 의도적이지 않든 위챗과 같은 소셜 미디어 앱에 환자 정보를 공개하는 경우가 있기 때문에, 이러한 사례는 비단 한 사람에게만 국한된 것은 아닙니다. WeChat은 이제 중국에서 없어서는 안 될 올인원 앱으로, 메시징 앱으로 기능하고, 공식 계정을 호스팅하고, 대화형 소셜 피드 플랫폼(WeChat 모멘트)을 지원하고, 디지털 결제 서비스(WeChat Pay)를 제공하고, 미니 프로그램이나 비디오 채널을 제공합니다(CMI 미디어 그룹, 2020). 의료 전문가들도 WeChat을 사용하여 앱 내에서 의료용 애플릿에 액세스하고 WeChat 모멘트에서 업무 및 생활 업데이트를 공유합니다(오슬로 대학교 인문학부, 2020). 이 레지던트는 환자 사진을 소셜 미디어에 공유하는 것이 비전문직업적이라고 생각했지만, 숨겨진 커리큘럼이나 사회 규범 위반에 대한 두려움 때문에 동료에게 이 문제를 제기하거나 상사에게 보고하지 않았습니다. 그럼에도 불구하고 중국 법률은 의사가 환자의 사생활을 공개하는 것을 명시적으로 금지하고 있으며, 이로 인한 부작용에 따라 경고, 벌금, 의사 면허 정지 또는 취소에 이르는 처벌이 부과될 수 있습니다(중화인민공화국 국무원, 2021). 그러나 현실적으로 의료기관이 직원들이 소셜 미디어에서 공유하는 모든 정보를 모니터링하기는 어렵기 때문에 의사와 레지던트에 대한 처벌은 환자 개인의 불만부터 병원 경영에 이르기까지 사안별로 발생할 가능성이 높습니다. 환자의 프라이버시와 의사의 전문직업성을 모두 보호한다는 관점에서, 의료 전문가에게 환자 프라이버시 침해로 간주되는 행동을 명확하게 알리는 프로그램과 가이드라인을 시행하는 것도 마찬가지로 중요합니다.
One resident mentioned witnessing colleagues post photos of child patients without mosaic (digital pixelation of photos to protect privacy) on WeChat moments (Patient confidentiality-50). This may not be an isolated singular scenario, since at times, physicians or residents may intentionally or unintentionally disclose patient information on social media apps such as WeChat. WeChat is now an indispensable all-in-one app in China, functioning as a messaging app, hosting official accounts, supporting an interactive social feeds platform (WeChat Moments), providing digital payment services (WeChat Pay), and featuring mini programs or video channels (CMI Media Group, 2020). Health professionals also use WeChat to access medical applets within the app and to share work and life updates in WeChat Moments (Faculty of Humanities of University of Oslo, 2020). For this resident, even though she believed sharing photos of patients to social media was unprofessional, she did not confront her colleagues about this or report it to her superiors, possibly for fear of the hidden curriculum or violating social constructs. Nevertheless, Chinese law explicitly prohibits physicians from disclosing patients’ privacy, and punishments ranging from warnings, fines, suspension or even revocation of physicians’ licenses can be imposed depending on the adverse consequences caused (The State Council of the People’s Republic of China, 2021). However, in actuality, it may be difficult for medical institutions to monitor all information shared by its employees on social media, so consequences against physicians and residents are more likely to crop up on a per-case basis from patients’ individual complaints to hospital management. In view of protecting both patient privacy and physician professionalism, it is equally important to implement programs and guidelines to clearly inform health professionals of behaviors that are indicative of a breach of patient privacy.
환자의 가족은 임상적 의사 결정에 중요한 역할을 하는데(Weng et al., 2011), 이는 환자 가족의 요청에 따라 환자에게 진실을 숨기는 경우(사전 동의-53), 가족의 서명 거부로 사전 동의를 받을 수 없는 경우(사전 동의-55) 등의 딜레마가 발생하는 이유를 설명해 줍니다. 중국에서는 문화적, 사회적, 법적 요인이 환자에게 질병 상태를 완전히 공개하지 않는 데 근본적인 역할을 합니다. 예를 들어, 환자가 암 진단을 받으면 의사는 환자의 가족에게 먼저 알리고, 가족은 환자가 질병에 대해 어느 정도 알아야 하는지 결정합니다(Tang et al., 2006). 의사가 암 진단에 대한 정보를 가족에게 먼저 제공하도록 선택할 수 있다는 것은 중국 법률에 의해 뒷받침됩니다(중화인민공화국 국무원, 2021). 많은 중국인에게 죽음에 대한 논의는 금기시되기 때문에(Ho et al., 2017), 가족 구성원은 환자가 감당하기 힘들고 정서적 붕괴로 이어져 환자의 죽음을 앞당길 수 있다는 두려움 때문에 환자에게 진실을 밝히기 위해 숨기거나 점진적인 접근 방식을 취하는 경향이 있습니다(Weng et al., 2011). 또한 중국의 집단주의 문화에서는 환자를 별도의 개인으로 간주하지 않고 가족의 구성원으로 간주합니다(Ho et al., 2012). 따라서 자연스럽게 임상적 결정과 정서적 부담 모두 환자의 가족 전체가 공유합니다. Su 등은 암 진단을 통보받은 직후에는 환자에게 불안과 고통을 유발할 수 있지만, 암 진단을 완전히 공개하는 것이 장기적으로 환자에게 도움이 된다고 제안합니다(Su 등., 2020). 우리는 집단주의 문화권에서 가족의 역할은 환자에게 중대한 질병을 숨기는 것이 아니라 환자에게 알린 후 환자가 정서적 부담을 감당할 수 있도록 돕는 것으로 구체화되어야 한다고 믿습니다.
Family members of patients play an important role in clinical decision-making (Weng et al., 2011), which explains why there are dilemmas such as Concealing the truth from patients at the request of the patient’s family (Informed consent-53) and Inability to obtain informed consent owing to the family’s refusal to sign (Informed consent-55). In China, cultural, social, and legal factors play a fundamental role in not fully revealing disease status to patients. For example, when a patient is diagnosed with cancer, the physician would often first inform the patient’s family members, who would then determine how much the patient should know about the condition (Tang et al., 2006). It is supported by Chinese law that physicians may choose to give information about cancer diagnoses to family members first (The State Council of the People’s Republic of China, 2021). For many Chinese, discussions of death are taboo (Ho et al., 2017), so family members tend to conceal or take more gradual approaches to disclose the truth to the patient because they fear it would be too much for the patient to bear and would lead to an emotional breakdown that would accelerate the patient’s death (Weng et al., 2011). Additionally, under the Chinese collectivist culture, the patient is not considered to be a separate individual but rather a component of the family (Ho et al., 2012). Therefore, naturally, both clinical decisions and emotional burdens are shared by the patient’s entire family. Su et al. suggest that although it may cause anxiety and distress in patients immediately after being informed of their diagnosis, the complete disclosure of cancer diagnoses benefits patients in the long term (Su et al., 2020). We believe that in collectivist cultures, the role of the family should be embodied in helping patients bear the emotional burden after informing patients rather than concealing critical illnesses from patients.
우리의 연구 결과는 집단주의와 관계주의가 중국인이 직면하는 전문직업성 딜레마를 분석하는 데 큰 설명력을 가지고 있음을 시사하는 것 같습니다.
- 집단주의는 상호 의존적인 사회적 지향을 나타내며, 이는 자아를 중요한 관계를 포괄하는 상호 연결된 존재로 보는 관점과 관련이 있습니다(Grossmann & Na, 2014). 집단주의 사회는 조화, 관련성, 사회적 연결에 중점을 두는 경향이 있습니다(Oyserman & Lee, 2008). 또한 토착 심리학자들은 유교 문화의 영향을 강조하며 유교 사회에서 개인을 고립된 존재가 아닌 사회적 관계의 관점에서 이해할 것을 제안하며, 렌칭, 꽌시, 면지는 사회적 관계와 개인 행동을 이해하는 데 중요한 개념입니다(Wang & Pak, 2015). 이러한 관점에서 볼 때, 중국인들이 자기 자신에 대한 영향에 대해서는 덜 합리화하지만 자신의 행동이 가능한 모든 팀원과의 관계, 환자 및 가족과의 관계에 미치는 파급 효과에 대해서는 광범위하게 고려하는 것은 놀라운 일이 아닙니다(Ho et al., 2012). 이는 한국, 일본, 싱가포르와 같이 유교의 영향을 받은 사회에 문화적 뿌리를 둔 의사들을 만날 때 특히 주목해야 할 현상입니다.
- 관계주의는 유교 사회에서 더 두드러지지만, 복종과 충성의 원칙을 인정하지 않는 등 개인주의가 더 뚜렷한 사회에서도 관계에 대한 관심이 없는 것은 아닙니다(Lingard et al., 2001). 아마도 전 세계의 레지던트들을 위해 의학교육자들은 현재 개인 수준에서 적용되는 원칙을 강조하는 것에서 나아가 임상 환경에서 관계의 균형을 잡을 수 있도록 명시적으로 도와야 할 것입니다.
Our results seem to suggest that collectivism and relationalism have great explanatory power in the analyses of professionalism dilemmas encountered by Chinese residents.
- Collectivism represents an interdependent social orientation, which is associated with a view of the self as interconnected, encompassing important relationships (Grossmann & Na, 2014). Collectivist societies tend to focus on harmony, relatedness, and social connection (Oyserman & Lee, 2008). Also, indigenous psychologists highlight the influence of Confucian culture and propose to understand the individual in Confucian societies not in isolation but in terms of social relationships, and renqing, guanxi, and mianzi are important concepts in understanding social relationships and personal behaviors (Wang & Pak, 2015). From this perspective, it is not surprising that Chinese residents rationalised less frequently about implications for self but extensively considered the rippling effects of their behaviors on their relationships with all possible team members and with patients and their families (Ho et al., 2012). It is a phenomenon to which we should pay special attention when we encounter physicians with cultural roots in Confucius-influenced societies, such as those of Korea, Japan, and Singapore.
- Although relationalism is more pronounced in Confucian societies, attention to relationships is not absent in societies in which individualism is more evident, such as in unavowed principles of obedience and allegiance (Lingard et al., 2001). Perhaps, for residents all over the world, medical educators should move beyond the current emphasis on principles that apply at the individual level and explicitly help them to balance relationships in clinical settings.
집단주의와 관계주의는 타인에 대한 친절, 이타심, 연대, 상호 도움, 신뢰, 지원, 개선을 옹호하며(Wang, 2006), 깊은 상호의존 관계, 사회적 조화와 안정, 사회의 균형을 가져다줍니다(Oyserman et al., 2002). 그러나 이러한 긍정적인 효과에도 불구하고, 본 연구 결과와 앞선 논의에서 살펴본 바와 같이 강한 집단주의 사회의 문화적 증상은 뚜렷한 개인적 경계가 없는 것과 같은 문제점을 야기하기도 합니다. 따라서 우리가 작성한 전문직업성 딜레마 체크리스트는 이러한 전문직업성 문제를 해결하기 위한 초기 도구로 사용될 수 있습니다. 체크리스트에 제시된 항목과 주제는 향후 사례 연구 및 평가 루브릭을 위한 기반을 마련하여 다양한 개입 또는 개선 접근법을 알려줄 수 있습니다. 이를 바탕으로 전문직업성 교육은 레지던트들이 전문직업적으로 행동하고 임상에서 전문직업성 딜레마와 도전에 대처하는 데 필요한 대처 기술을 연마하고 보건 시스템 및 병원 관리 원칙과 지침을 개선하는 데 도움이 될 것입니다. 이 연구 결과의 또 다른 이점은 체크리스트에서 제기된 사항을 바탕으로 의학 지식의 대중화, 의료진 존중, 의료 시스템 탐색 등 개선이 필요한 영역을 다룰 수 있는 환자 교육에서의 역할이 될 것입니다.
Collectivism and relationalism advocate kindness to others, selflessness, solidarity, and mutual help, trust, support, and improvement (Wang, 2006) and bring about deeply interdependent relationships, social harmony and stability, and a balance to society (Oyserman et al., 2002). However, despite these positive effects, cultural symptoms of a strongly collectivist society also pose its own challenges, such as a lack of distinct personal boundaries, as demonstrated in the results of this study and in the previous discussion. As such, the checklist of professionalism dilemmas we have compiled may serve as an initial tool to begin tackling these professionalism challenges. The items and themes presented in the checklist would pave the way for future case studies and evaluation rubrics that could inform a variety of interventions or remedial approaches. Based on these, professionalism training would equip residents to conduct themselves professionally and also hone the necessary coping skills to deal with professionalism dilemmas and challenges in clinical practice and aid in improving health system and hospital management principles and guidelines. An added benefit of the results of this study would be its role in patient education, where areas that require improvement, such as popularizing medical knowledge, respect for healthcare providers, and navigating the health care system, can be addressed based on points raised within the checklist.
본 연구에는 몇 가지 한계가 있습니다. 이 연구에서 인터뷰 대상자를 의도적으로 샘플링했기 때문에 편향된 대표성을 나타낼 수 있습니다(Tongco, 2007). 포커스 그룹은 단일 병원에서 실시되었기 때문에 다른 기관에서 근무하는 레지던트의 경험과 관찰을 반영하지 못할 수 있으므로 연구 결과를 더 많은 집단에 일반화하는 데 한계가 있습니다. 또한 레지던트 수련 기간이 길수록 각 전문직업성 딜레마에 대해 듣고, 목격하고, 경험한 레지던트의 비율이 더 높을 가능성이 높았습니다. 이 연구에서는 수련 기간이 다른 레지던트들을 포함했지만, 모집된 참가자 중 52%가 수련 기간이 6개월밖에 되지 않은 레지던트였기 때문에 전문직업성 딜레마에 대한 전반적인 보고율이 낮을 수 있습니다. 향후 대규모 표본 추출을 통해 레지던트를 폭넓게 대표하는 정량적 연구에서는 잠재적 편향에 대한 우려를 최소화하기 위해 전공과, 경력 수준, 사회인구학적 배경에 따라 레지던트들이 보고한 전문직업성 딜레마의 범위를 비교해야 합니다. 이 버전의 전문직업성 딜레마 체크리스트가 완전한 것은 아니며 향후 임상 분야, 기관 및 지역 전반에 걸쳐 의견을 폭넓게 수렴하려는 노력이 필요하다는 점에 유의할 필요가 있습니다. 이 연구의 주요 목적은 전문직업성 딜레마 체크리스트를 구성하는 것이었지만, 이 체크리스트가 실행된다면 심리측정 특성에 대한 추가 테스트를 통해 이러한 전문직업성 딜레마가 레지던트의 복지 및 제공되는 의료 서비스의 질과 어떤 관련이 있는지 밝혀낼 수 있을 것입니다.
Our study has several limitations. The purposive sampling of interviewees in this study could have led to a biased representation (Tongco, 2007). Focus groups were conducted at a single hospital and may not reflect the experiences and observations of residents at other institutions, so generalization of research findings to the larger population is limited. In addition, longer residency training was more likely to increase the proportion of residents who have heard of, witnessed, and experienced each of the professionalism dilemmas. In this study, although we included residents with different training years, 52% of the recruited participants were residents who had only been in training for 6 months, which may lower the overall reporting rates of professionalism dilemmas. Future quantitative studies of a wide representation of residents through large-scale sampling should compare the range of professionalism dilemmas reported by residents across specialties, experience levels, and sociodemographic backgrounds in order to minimize concern for potential bias. It is worth noting that this version of the professionalism dilemma checklist is not inexhaustible and would benefit from future efforts to broaden input across clinical disciplines, institutions, and regions. Although the main aim of this study was to construct a checklist of professionalism dilemmas, if this checklist is to be implemented, further testing of its psychometric properties would shed light on how these professionalism dilemmas relate to resident wellbeing and quality of health care provided.
"It really puts me in a bind", professionalism dilemmas reported by Chinese residents
PMID: 36595184
Abstract
Residents play a pivotal role in the healthcare system. However, few tools have systematically revealed the dilemmas and challenges faced by residents. This study aimed to develop a checklist for professionalism dilemmas based on a behavior-based professionalism framework and to examine the range and proportion of professionalism dilemmas heard of, witnessed, or experienced by Chinese residents. Mixed methods were used, comprising qualitative (document analysis and focus group interviews) and quantitative (a small-scale questionnaire survey) data. Document analysis summarized professionalism dilemma items from previous publications. For focus group interviews, we used narrative inquiry to explore and make sense of residents' experiences and perceptions of professionalism dilemmas. A small-scale questionnaire survey was conducted during each focus group to investigate the proportion of professionalism dilemma items that residents reported to have heard of, witnessed, or experienced. Through document analysis and focus group interviews, we developed a checklist of professionalism dilemmas based on a behavior-based professionalism framework. The checklist included 58 items over four domains, with 10 sub-domains (compassion, respect, communication, collaboration, integrity, duty, pursuit of excellence, fair stewardship of health care resources, patient confidentiality, and informed consent). We also sought a preliminarily subjective impression by exploring the proportion of residents who have heard of, witnessed, and experienced each of the professionalism dilemma items and residents' perspectives when faced with professionalism dilemmas. Residents inevitably encounter or experience a diverse range of professionalism dilemmas. This checklist of professionalism dilemmas that was developed could prove to be a significant reference for targeted professionalism education, both for the resident as well as for faculty. It can also act as a helpful tool for improving hospital management guidelines and patient education.
Keywords: Document analysis; Narrative inquiry; Professionalism; Professionalism dilemma; Resident.
© 2023. The Author(s), under exclusive licence to Springer Nature B.V.
'Articles (Medical Education) > 전문직업성(Professionalism)' 카테고리의 다른 글
| 행복은 무엇인가? 의학교육을 위한 비판적 내러티브 리뷰(Perspect Med Educ. 2023) (0) | 2023.09.19 |
|---|---|
| 역량있는 건강 애드보커시에 대한 환자와 의사의 관점 탐색(Med Educ, 2020) (0) | 2023.09.15 |
| '너의 모든 형태로서의 너 자신': 의과대학생의 정체성 안정에 대한 근거이론 탐색(Med Educ, 2023) (0) | 2023.08.31 |
| 테크니컬 어려움: 테크놀로지에 대한 비판적 철학적 지향 가르치기(Teach Learn Med, 2023) (0) | 2023.08.30 |
| 언어, 철학, 그리고 의학교육 (Teach Learn Med, 2021) (0) | 2023.08.09 |