학부의학교육에서 적극적 환자 참여의 역할: 체계적 문헌고찰(BMJ Open. 2020)
Role of active patient involvement in undergraduate medical education: a systematic review
Stijntje Willemijn Dijk ,1 Edwin Johan Duijzer,2 Matthias Wienold3
소개 및 근거
Introduction and rationale
최근 수십 년 동안 의학교육에 환자의 참여가 점점 더 많이 주장되어 왔으며, 의학교육 개혁가들이 채택하는 일반적인 관행이 되었습니다.1 환자와 환자의 이야기는 더 이상 임상 교육에서 '학습 자료'의 대상으로만 사용되는 것이 아닙니다. Towle 등은 교육, 평가 및 커리큘럼 개발에서 환자 교사로서 지속적인 참여와 더불어 의학 커리큘럼의 코드 설계자로서 기관 차원의 참여까지 다양한 수준의 참여를 확인했습니다.1-4 이제 의학교육자들은 의대생과 환자 및 그 가족, 지역사회를 연결하여 종적 관계의 중요성을 인식하고, 학생들의 사회적 상호작용 기술을 향상시키고, 실제 세계에서 질병에 대처하는 학습을 촉진하는 것의 가치를 깨닫고 있습니다.5 6
In recent decades, the involvement of patients in medical education has been advocated for increasingly and has become common practice adopted by reformers of medical education.1 Patients and their narratives are no longer just used as subjects for ‘learning material’ in clinical training. Towle et al identified different levels of involvement, from paper-based involvement to involvement at the institutional level as codesigners of the medical curriculum in addition to sustained involvement as patient teachers in education, evaluation and curriculum development.1–4 Medical educators are now seeing the value of linking medical students with patients and their families and communities to foster awareness of the importance of longitudinal relationships, to improve students’ social interaction skills and to facilitate learning of coping with illness in the real world.5 6
의학교육에서 환자의 협력적 역할이 점점 더 커지고 있지만, 이를 어떻게 포함시킬지, 모든 수준의 의학교육에서 환자 참여를 계획하기 위한 체계적이고 기관 차원의 접근법을 개발하는 방법에 대해 배워야 할 것이 많습니다.3 7 임상 의사 결정과 환자 중심 치료에서 보다 동등한 파트너십을 향한 노력은, 국내 및 국제 지침에 힘입어, 의학교육에서 파트너십이 표준이 되는 문화를 개발하기 위한 노력의 확대를 촉진하고 있습니다.3 5-15
Despite an increasingly collaborative role of patients in medical education, there is much to be learnt about how to embed it, and how to develop systematic, institution-wide approaches to planning patient involvement in all levels of medical education.3 7 The drive towards a more equal partnership in clinical decision-making and patient-centred care, fuelled by national and international guidelines, promotes the expansion of the efforts towards developing a culture where partnership in medical education becomes the norm.3 5–15
연구자들은 의학교육에서 환자의 적극적인 참여에 대한 다양한 정의를 사용함에 따라 문헌 검색에서 다양한 포함 기준을 사용했습니다. 이로 인해 포함된 논문이 중복되고 공통된 이론적 틀과 용어가 생성되는 데 한계가 있었습니다.3 16 이전 연구에서는 장단기 학습 결과, 윤리적 문제, 심리적 영향 및 모집, 선발, 준비와 같은 주요 절차적 기여자와 관련된 지식 기반에 큰 격차가 있는 것으로 확인되었습니다. 또한 적극적인 환자 참여의 비용 효율성에 대한 정보도 제한적입니다.
As researchers have used varying definitions of active patient involvement in medical education, they have used varying inclusion criteria in their literature searches. This has resulted in overlap of included papers, and limited the generation of a common theoretical framework and terminology.3 16 Previous studies have identified major gaps in the knowledge base relating to short and long-term learning outcomes, ethical issues, psychological impact and key procedural contributors like recruitment, selection and preparation. There is also limited information of the cost-effectiveness of active patient involvement.
의학교육에서의 환자 참여에 대한 체계적 문헌고찰1 17-19 및 비체계적 문헌고찰2 8 20이 발표된 이후, 많은 새로운 연구가 발표되었습니다. 이전 리뷰에서는 환자 교사 역할만 다루거나,1 특정 술기(친밀한 검사)를 가르치고 평가하거나,17 모의 환자를 포함하거나,17 대학원 의학교육을 포함하거나18 모든 의료 전문직을 다루었습니다.2 17 20 최근의 체계적 고찰에서는 주로 학습자의 관점에서 환자 참여, 결과 및 참여 이유에 대한 포괄적인 개요를 제공했습니다.19
Since the publication of the last systematic reviews1 17–19 and non-systematic reviews2 8 20 of patient involvement in medical education, many new studies have been published. Previous reviews addressed only the patient teacher role,1 teaching and assessing one specific skill (intimate examination),17 included simulated patients,17 included postgraduate medical education18 or addressed all healthcare professions.2 17 20 A recent systematic review provided a comprehensive overview of the involvement, outcome and reason behind involvement mainly from learner’s perspective.19
본 논문에서는 학부 의학교육의 모든 분야 또는 환경에서 단순히 우발적인 수동적 참여를 넘어서는 모든 형태의 참여를 포함하는 환자 참여에 대한 광범위한 정의를 사용하여 가장 최근의 문헌을 검토하고 요약합니다. 이 정의를 채택함으로써 우리는 연구 데이터의 범위와 양을 확장하여 적극적인 환자 참여에 대한 실질적인 지식 기반을 늘리고 개선된 이론적 틀과 공통 용어의 근거를 마련할 수 있습니다. 본 연구는 주로 환자의 참여에 대한 환자의 관점에 초점을 맞춘 새로운 접근 방식을 취합니다.
Our paper reviews and summarises the most recent literature using a broad definition of patient involvement consisting of any form of involvement that is beyond merely incidental passive involvement, in any field or setting of undergraduate medical education. By adopting this definition we are able to extend the scope and amount of research data in order to increase the practical knowledge base on active patient involvement and in order to give ground to an improved theoretical framework and common terminology. Our study takes a novel approach by focusing primarily on the patients’ perspective on their involvement.
방법
Methods
설계
Design
문헌 검색은 [의대생 학부 교육의 개발, 전달 또는 평가에 실제 환자 및 지역사회 구성원이 직접 참여하는 것]으로 정의되는 [의학교육에 대한 적극적인 환자 참여]를 찾기 위해 체계적인 검토 방법을 사용했습니다.
Our literature search employed a systematic review method looking for active patient involvement in medical education defined as the direct involvement of real patients and community members in the development, delivery or evaluation of undergraduate education of medical students.
검색 전략
Search strategy
저자들은 2018년 7월 12일에 PubMed를 통해 검색을 수행했습니다. 검색어에는 환자*, 커뮤니티*, 참여, 참여*, 협력*, 협력*, 대표*, 의학교육, 커리큘럼, 의대생* 등이 단독으로 또는 조합하여 사용되었습니다. 검색 기준은 병원 정보 전문가가 검토했습니다. 전체 검색 전략은 온라인 부록 파일 1에서 확인할 수 있습니다.
The authors performed a search through PubMed on 12 July 2018. The search terms used on their own and in combination included: patient*, communit*, involvement, engag*, cooperat*, collaborat*, represent*, medical education, curriculum, medical student*. Search criteria were reviewed by a hospital information specialist. The full search strategy can be found in online supplementary file 1.
2003년 1월 1일부터 2018년 7월 12일 사이에 영어로 출판되고 학부 의학교육에 환자의 적극적인 참여를 다룬 1차 경험적 연구를 보고한 모든 논문을 포함할 수 있었습니다. 모의 환자 또는 배우, 검사만 받은 환자 또는 병동에서 관찰만 받은 환자를 대상으로 한 연구는 검토 대상에서 제외되었습니다.
All articles published in English between 1 January 2003 and 12 July 2018 and reporting primary empirical research that addressed the active participation of patients in undergraduate medical education were eligible for inclusion. Studies with simulated patients or actors, patients solely undergoing examinations or patients who were only being observed in wards were excluded from the review.
1차에서는 제목과 초록을 기준으로, 2차에서는 전문을 기준으로 논문을 평가했습니다. 포함된 모든 논문의 참고문헌을 분석하여 원래 포함 기준에 부합하는 추가 연구가 있는지 확인했습니다. 포함 기준을 준수한 모든 리뷰는 관련 참고 문헌에 대해 추가적으로 평가되었습니다. 최종 분석에는 원저 연구 논문만 포함되었습니다.
We assessed articles based on title and abstract in the first round, and in a second round based on full text. References of all included articles were analysed for additional studies that matched the original inclusion criteria. All reviews that complied with the inclusion criteria were additionally assessed for relevant references. Only original research articles were included in the final analysis.
포함된 연구의 질 평가
Quality assessment of included studies
질적, 양적 및 혼합 방법 설계의 논문이 포함되었으므로 두 명의 저자(SWD 및 ED)가 혼합 방법 평가 도구를 적용하여 연구의 방법론적 품질을 평가했습니다(온라인 보충 파일 2).21 평가된 방법론적 품질에 따라 연구는 제외되지 않았습니다.
As our review included papers of qualitative, quantitative and mixed methods designs, two authors (SWD and ED) applied the Mixed Methods Appraisal Tool to assess the methodological quality of studies (online supplementary file 2).21 Studies were not excluded based on assessed methodological quality.
데이터 추출 및 합성
Data extraction and synthesis
모든 저자(SWD, ED, MW)는 포함된 연구에서 데이터를 추출하기 위해 미리 준비된 표준화된 양식을 사용했습니다. 두 번째 저자는 추출된 데이터가 정확한지 확인했으며, 불일치하는 부분은 토론을 통해 해결했습니다. 저자, 출판 연도, 저널, 개입 국가, 연구 유형, 초록, 연구 환경, 보고된 재정적 측면, 개입 환자 수, 개입 학생 수, 환자 특성, 환자 참여 동기, 모집 관행, 교육 및 준비 관행, 환자 단체의 역할, 환자 참여 유형, 결과 측정, 지속 가능성에 대한 조직의 언급 및 추구한 학습 결과 등의 데이터가 기록되었습니다. 이러한 학습 결과의 범위를 탐색하기 위해 의과대학에서 일반적으로 적용되는 역량 프레임워크인 CanMEDS 프레임워크에 따라 의도된 학습 결과를 분류했습니다.22 추출된 데이터를 관련 테마로 구성하여 데이터 요소 간의 연결과 불일치를 탐색했습니다. 환자가 맡을 수 있는 잠재적 역할을 그룹화할 때 기존의 프레임워크를 사용하지 않기로 결정했습니다. 토론 섹션에서는 역할의 다양성에 대한 우리의 연구 결과를 Towle 등의 기존 분류체계와 비교합니다.2
All authors (SWD, ED, MW) used a prepiloted standardised form to extract data from included studies. A second author checked if the extracted data were accurate, and discrepancies were resolved through discussion. The following data were recorded: authors, year of publication, journal, country intervention, study type, abstract, study setting, financial aspects reported, number of patients in intervention, number of students in intervention, patient characteristics, patient motivations to join, recruitment practices, training and preparation practices, role of patient organisations, type of patient involvement, outcome measurement, organisational remarks on sustainability and pursued learning outcomes. To explore this range of learning outcomes, we categorised intended learning outcomes according to the CanMEDS framework as a commonly applied competency framework within medical schools.22 We organised extracted data in related themes to explore connections and discrepancies between data elements. We opted not to use any of the existing frameworks for grouping potential roles patients take on. In the Discussion section, we compare our findings of the diversity of roles with the existing taxonomy by Towle et al.2
환자 및 대중 참여 성명서
Patient and public involvement statement
이 연구 이니셔티브의 초기 동기는 국제환자단체연합(IAPO)과 국제의대생협회연맹(IFMSA)의 회원인 저자들 간의 협력에 따른 것입니다. 환자 대표이자 공동 저자인 MW는 프로젝트 시작, 연구 설계, 데이터 분석, 토론 및 논문 작성 등 연구 프로젝트의 모든 단계에 동등한 파트너로서 참여했습니다. 이 논문의 초안은 2019 유럽 환자 포럼에서 300명의 환자 대표들이 참석한 가운데 본회의에서 발표되고 논의되었으며, 그 피드백이 최종 논문에 반영되었습니다.
The initial impulse for this study initiative followed a collaboration between the authors as members of the International Alliance of Patients’ Organizations (IAPO) and the International Federation of Medical Students' Associations (IFMSA). MW, patient representative and co-author, was involved as an equal partner in all stages of the research project including project initiation, study design, data analysis, discussion and writing of the paper. The initial draft of this paper was presented and discussed at the European Patient Forum 2019 in a plenary session with 300 patient representatives present, feedback from which has been incorporated into the final paper.
결과
Results
연구 선택
Study selection
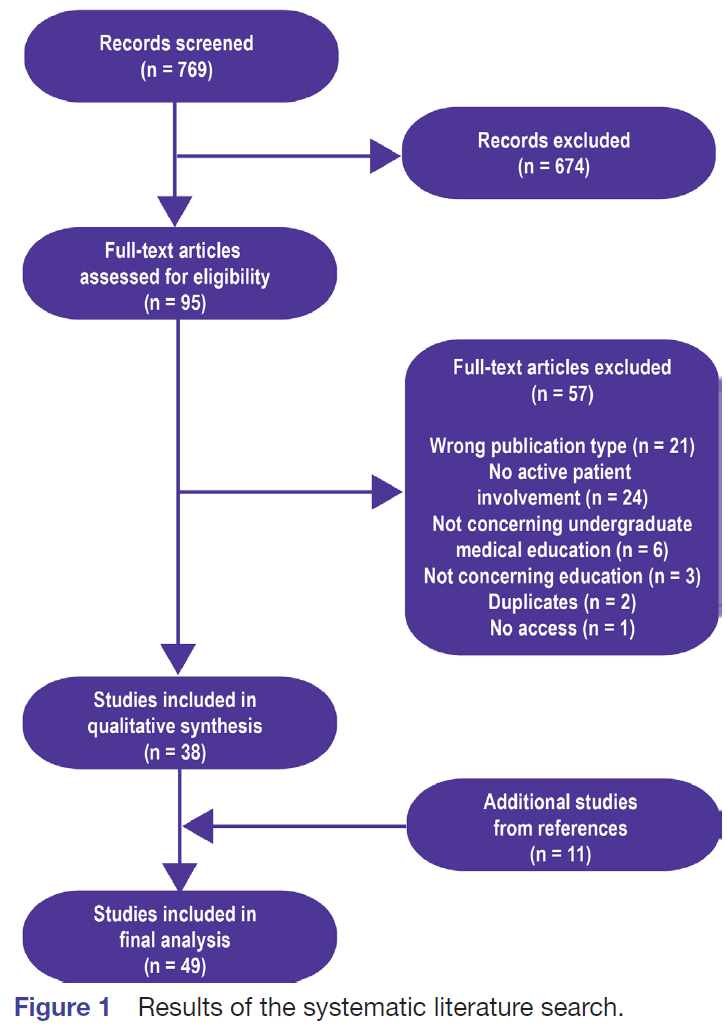
초기 검색 결과 769개의 논문이 검색되었으며, 이 중 제목 및/또는 초록을 기준으로 95개의 논문이 추가 검토 대상으로 선정되었습니다. 이 95개 논문은 두 명의 저자(SWD 및 ED)가 독립적으로 읽었으며 지정된 기준에 따라 포함되었습니다. 검토자 간의 합의율은 91.2%였습니다. 나머지 논문은 짧은 토론 후 합의에 따라 포함되었습니다. 주요 제외 사유는 논문 유형이 잘못된 경우(학회 초록 또는 논평), 환자의 적극적인 참여와 관련이 없는 연구였습니다. 참고문헌 검토 결과 11편의 논문이 추가로 포함되었습니다. 포함 기준을 충족한 49개 연구의 특징은 그림 1과 온라인 부록 파일 3에 제시되어 있습니다.
The initial search resulted in 769 articles, of which 95 were selected for further review based on the title and/or abstract. These 95 articles were independently read by two authors (SWD and ED) and included based on the specified criteria. Consensus between reviewers was 91.2%. The remaining articles were included based on consensus after a short discussion. Main reasons for exclusion where wrong article type (conference abstracts or commentaries) and studies that did not concern active participation of patients. The review of references resulted in 11 additional articles for inclusion. The characteristics of the 49 studies that met inclusion criteria are presented in figure 1 and online supplementary file 3.
포함된 연구에서 추출한 데이터를 사용하여 다음 하위 섹션의 증거를 종합했습니다:
We used the extracted data from included studies to synthesise the evidence in the following subsections:
- 환자를 의학교육에 참여시키는 근거.
- 환자 모집 및 선정.
- 의학 교육에 참여하기 위한 환자의 준비 과정.
- 의학 교육에서 환자가 수행하는 역할.
- 환자 참여를 통해 추구하는 학습 목표.
- 환자 참여에 대한 우려 사항.
- 환자 참여의 영향에 대한 환자들의 견해.
- 환자 참여의 재정적 영향.
- 환자 단체의 역할.
- 환자 참여의 지속 가능성을 보장하기 위한 조치.
- Rationale for involving patients in medical education.
- Patient recruitment and selection.
- Patients’ preparation to participate in medical education.
- Roles patients take on in medical education.
- Learning objectives pursued through patient involvement.
- Concerns about the involvement of patients.
- Patients’ views on the impact of their involvement.
- Financial implications of patient involvement.
- Roles of patient organisations.
- Measures to ensure the sustainability of patient involvement.
의학 교육에 환자를 참여시키는 근거
Rationale for involving patients in medical education
몇몇 저자는 의학교육에 환자 참여를 의무화하는 정부 정책, 즉 영국 보건부 및 영국 일반의학회,16 23 24 호주 의학회25 및 WHO5 를 환자 참여 이니셔티브의 근거로 언급했습니다. 이러한 정치적 동인 외에도
- 학생들에게 환자 중심 및 전문가 간 치료를 가르치기 위해24 26-28,
- 학생들에게 만성 질환 치료를 소개하기 위해29-31,
- 다문화 학습 환경을 조성하기 위해,
- 사회적 책임과 포용 의제를 실천하기 위해32-37,
- 교육을 더욱 매력적이고 강력하며 혁신적으로 만들기 위해38,
- 환자에게 권한을 부여하기 위해39
환자들은 미래의 의료 인력을 양성하고24 32 의료 시스템을 개선한다는 점에서 더 광범위한 커뮤니티에 대한 책임감을 느낀다고 언급했습니다.24 33 40
Several authors referred to government policy mandating patient participation in medical education, namely the UK Department of Health and the UK General Medical Council,16 23 24 the Australian Medical Council25 and the WHO5 as a rationale for their patient involvement initiatives. Besides these political drivers, cited rationales were:
- to teach students patient-centred and interprofessional care24 26–28;
- to introduce students to chronic illness care29–31;
- to create a multicultural learning environment;
- to practise social accountability and an inclusion agenda32–37;
- to make education more engaging, powerful and transformative38; and
- to empower patients.39
Patients mentioned that they felt a sense of responsibility to the broader community in shaping the future health workforce24 32 and improving the healthcare system.24 33 40
환자 모집 및 선택
Patient recruitment and selection
가장 자주 보고된 환자 모집 방법은
- 기존 대학 파트너십 및 기존 프로그램,28 33 41-46
- 언론 또는 소셜 미디어를 통한 광고 또는 보건 시설에 게시,26 34-36 47 48
- 지역사회 및 환자 단체,
- 개인적 인맥 및 이전 참가자,32 38 49-51 및
- 보건 전문가를 통하여 52-55
학생들이 만성 질환 환자를 섀도잉하는 한 프로젝트에서는 학생들이 직접 환자를 모집하도록 요청받았습니다.30
The most frequently reported methods to recruit patients were through
- existing university partnerships and existing programmes,28 33 41–46
- advertisements through press or social media or posted in health facilities,26 34–36 47 48
- through community and patient organisations,
- through personal connections and previous participants,32 38 49–51 and
- through health professionals.52–55
In one project, where students shadowed a patient with a chronic condition, students were asked to recruit patients themselves.30
선발 기준은 일반적으로 광범위하게 설정되어 모든 환자 또는 지역사회 구성원을 초대했습니다. 환자 교육자의 일반적인 기준에는 다음 등이 포함되었습니다.
- 좋은 의사소통 능력,
- 교육에 대한 선호,
- 추가 학습에 대한 적성,
- 열정,
- 연구에 전념할 수 있는 시간,
- 완전히 움직일 수 있고 반복적인 신체 검사에 대처할 수 있는 능력 48 54 56
어떤 경우에는 환자에게 질병의 대표적인 신체적 징후가 요구되기도 했습니다.53 54 56 57
Selection criteria were generally set up broadly, inviting any patient or community member. General criteria for patient educators included
- good communication skills,
- affinity for teaching,
- aptitude for further learning,
- enthusiasm,
- time to commit to the study, as well as
- being fully mobile and being able to cope with repeated physical examinations.48 54 56
In some cases patients were required to have representative physical signs of their disease.53 54 56 57
의료 교육에 참여하기 위한 환자의 준비 과정
Patients’ preparations to participate in medical education
20개의 논문에서 환자 교사의 준비에 대해 언급하고 있습니다. 준비 기간은 총 100시간의 상당한 교육 세션42 에서부터 서면 정보만 제공하거나 1~1.5 시간의 단일 오리엔테이션 세션이 대부분이었습니다.24 30 32 39 43 49 52 57 근골격계(MSK) 술기를 교육하는 환자 대상 교육 프로그램이 가장 광범위했으며 의료 또는 교육 전문가가 제공했습니다.42 47 54 56 58 59 다른 준비 세션은 덜 형식적이며 교수진 교육 전문가, 학생 또는 동료에 의해 진행되었습니다.
Twenty articles mention preparation of patient teachers. The duration of the preparation ranged from substantial training sessions of 100 hours in total42 to the majority of programmes providing solely written information or a single orientation session of 1–1.5 hours.24 30 32 39 43 49 52 57 Training programmes for patients in teaching musculoskeletal (MSK) skills were the most extensive and were delivered by medical or educational experts.42 47 54 56 58 59 Other preparatory sessions were less formal and were facilitated by faculty educational experts, students or peers.
준비 프로그램의 주요 목표는 다양했습니다. 한 연구에서는 학생의 학습 결과를 보호하기 위해 환자 교육자가 코스 목표를 인식하는 것이 중요하다고 강조했습니다.53 다른 연구에서는 환자들의 자신감 향상, 기술 훈련 제공57, 교육 과정과 관련된 지식 제공을 목표로 언급했습니다.23 39 48 60 이러한 세션에서는 문제 기반 학습, 프레젠테이션 전달 방법, 코퍼실리테이션 방법, 효과적인 피드백 제공 방법과 같은 접근법을 다루었습니다. 또한 준비 과정은 코칭, 감독 및 디브리핑 방법을 사용하여 갈등, 감정, 충족되지 않은 기대와 같은 [이점과 과제를 예측할 수 있는 기회]를 제공했습니다.40 61
The primary aims of the preparatory programmes varied. One study underscored the importance of patient educators being aware of the course goals in order to safeguard student learning outcomes.53 Others mentioned aiming to serve the needs of patients in building their confidence, providing skills training57 and providing knowledge related to the educational process.23 39 48 60 These sessions addressed approaches such as problem-based learning, how to deliver a presentation, cofacilitation methods and how to provide effective feedback. Preparation also provided opportunities for anticipating benefits and challenges such as conflicts, emotions, unmet expectations, using methods of coaching, supervision and debriefing.40 61
한 논문에서는 평가 도구로 짧은 퀴즈를 통해 환자 교육자의 준비를 마무리하고 교육을 시작하기 전에 졸업 세션을 갖는 것을 언급했습니다.28 또 다른 논문에서는 환자 교육자가 교육할 준비가 되었는지 확인하기 위해 교육 후 만족도 설문지를 사용하는 것을 설명합니다.47 대부분의 논문에서는 환자 교육자가 역할을 수행하기 전에 환자를 평가하는 것에 대해 다루지 않았습니다.
One article mentions finishing the preparation of patient educators with a short quiz as an assessment tool and having a graduation session before starting to teach.28 Another article describes the use of a post-training satisfaction questionnaire to help ensure that patient educators felt ready to teach.47 The majority of papers did not address assessing patients prior to them taking on their roles.
Towle 등은 [환자 교육자의 준비성]과 [교육의 형식과 내용의 실제성authenticity] 사이의 긴장에 대해 논의했습니다.49 이들은 [학계]와 [지역사회]라는 두 문화 사이에서 중개자 역할을 할 수 있는 지역사회 조직 대표의 중요한 역할을 강조합니다. 한 논문에서는 환자 교육자가 명시적으로 교육을 받지 않았기 때문에 학생과 환자의 만남이 가능한 한 진정성 있게 이루어질 수 있다고 설명합니다.53 또 다른 논문에서는 환자와 교육자 간의 협업을 통해 진정한 환자 관점을 잃지 않고 상호 학습이 가능하다고 설명합니다.39
Towle et al discussed the tension between preparedness of patient educators and authenticity of education in both form and content.49 They highlight the critical role of the community organisation representatives who can be brokers between the two cultures of academia and community. One article describes an intervention in which the patient educators explicitly have not received training, so the student–patient encounters would be as authentic as possible.53 Another article described that the collaboration between patients and educators allows for mutual learning without an authentic patient perspective being lost.39
의학 교육에서 환자가 맡는 역할
Roles patients take on in medical education
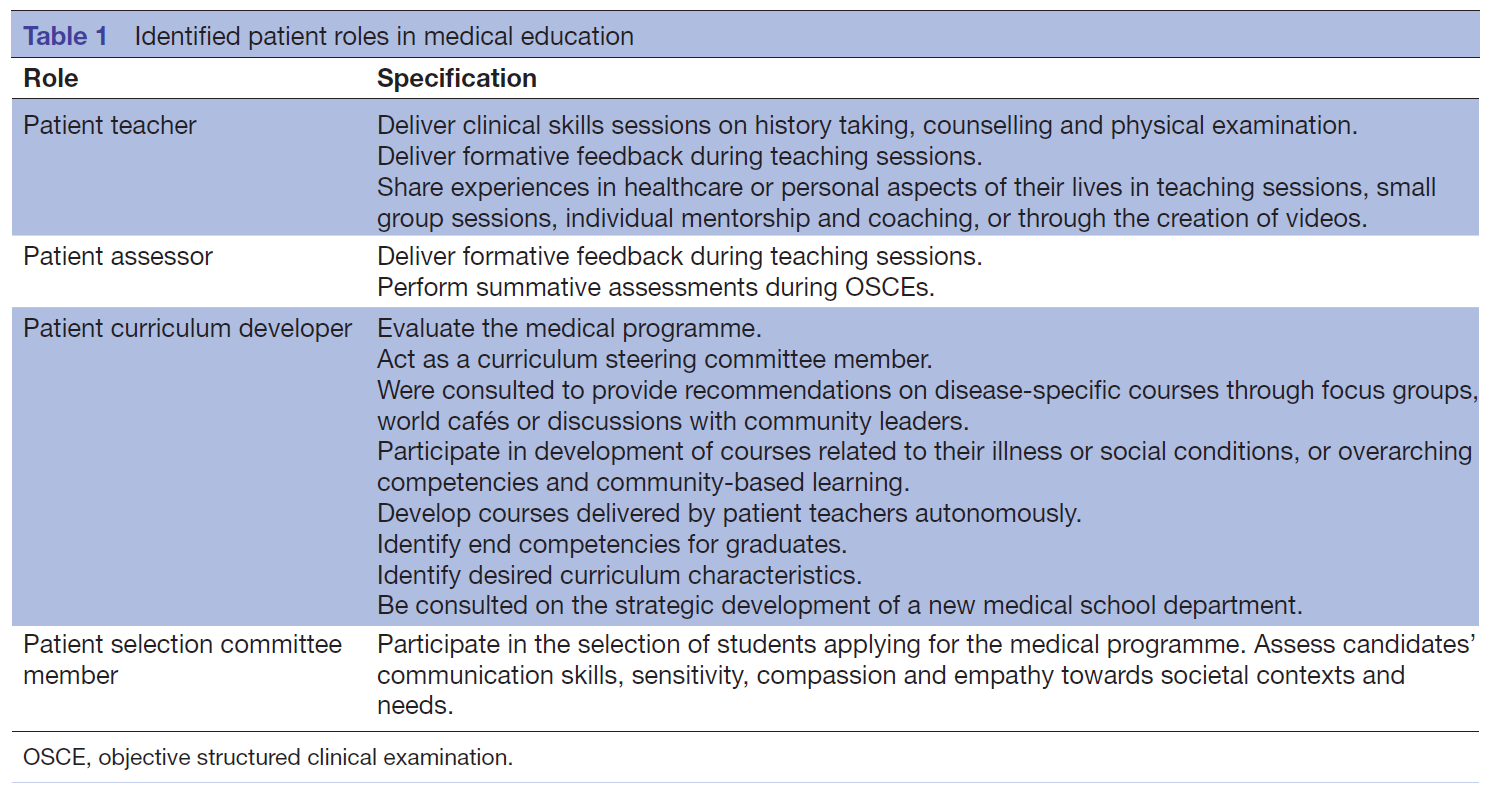
우리가 확인한 주요 역할 범주는 교사, 평가자, 커리큘럼 개발자 및 학생 선발자로서의 환자 영역으로 나뉩니다(표 1).
The main categories of roles that we identified are divided in the areas of a patient as a teacher, an assessor, a curriculum developer and a student selector (table 1).
교사로서의 환자
Patient as teacher
교사의 역할이 가장 많이 언급되었습니다. 환자 교사들은 다발성 경화증과 같은 자신의 질환에 대한 병력 청취 및 신체 검사 세션에 대한 임상 기술 실습을 진행했습니다.42 47 54 56 58 59 62 환자 교사들은 학생들에게 기술을 가르치고 즉각적인 피드백을 제공하여 추가 학습을 촉진하도록 훈련받았습니다.56
The role of a teacher was cited most frequently. Patient teachers gave clinical skills practicals on history taking and physical examination sessions on their own condition such as MSK disorders.42 47 54 56 58 59 62 They were trained to teach students skills and deliver immediate feedback, which stimulated further learning.56
장애인 환자 교사로 활동하는 여러 장애인 환자 그룹이 의사소통 기술과 병력 청취에 대한 실습을 진행했습니다.48 53 57 HIV 감염인이 교사로 참여하여 학생들이 상담을 제공하는 모의 임상 상황에 참여했습니다.60
Several groups of patients with disabilities acting as patient teachers with disabilities gave practicals on communication skills and history taking.48 53 57 People living with HIV participated as teachers during a simulated clinical encounter in which students provided counselling.60
환자들은 임상 기술 외에도 전반적인 치료 관리 경험과 삶의 개인적인 측면에 대해 학생들에게 가르쳤습니다. 여기에는 실제적인 신체적, 가정적 적응부터 자신과 가족에게 영향을 미치는 심리적, 사회적, 행동적 문제까지 다양한 내용이 포함되었습니다. 교육은 패널 토론과 소그룹 세션24 43 63뿐만 아니라 지역사회와 환자 가정 방문을 통해 이루어졌습니다.31 52 만성 질환을 가진 환자 교사가 멘토 역할을 하고 학생들과 정기적으로 만났습니다.27 29 환자들은 학생들에게 환자 중심주의와 전문직 간 전문성,23 24 31 38 49 지역사회 중심주의, 문화적 역량 및 윤리를 가르쳤습니다.33 64 환자들은 자신의 이야기를 들려주고 성찰을 자극하는 등 자신의 교육 방법을 선택할 수 있었습니다.38 지적 및 발달 장애가 있는 환자 그룹도 자신의 관점과 이야기를 공유하는 비디오를 통해 학습 자료 제작에 참여했습니다.65
In addition to clinical skills, patients taught students about their experiences of overall management of care, and the personal aspects of their lives. These ranged from practical physical and home adjustments, to psychological, social and behavioural issues impacting them and their family. Teaching was done through panel discussions and small group sessions24 43 63 as well as visits to the community and patients’ homes.31 52 Patient teachers with chronic conditions acted as mentors, and met regularly with students.27 29 Patients taught students patient-centredness and interprofessionalism,23 24 31 38 49 community-centredness, cultural competence and ethics.33 64 Patients could choose their own teaching method, such as telling their stories and stimulating reflection.38 A group of patients living with intellectual and developmental disabilities also participated in the creation of learning materials, through videos sharing their perspectives and stories.65
Jackson 등의 연구에 참여한 대부분의 환자는 자신을 가르치는 것이 아니라 파트너십을 맺고 질병의 특정 측면을 설명하고 공유하는 역할을 한다고 생각했습니다.52
Most patients in the study by Jackson et al considered themselves not as teaching, but having a role of partnership, explanation and sharing certain aspects of their illness.52
학생의 역량 평가자로서의 환자
Patient as assessor of students’ competence
교육 세션 중 피드백과 같은 형성적 학생 평가 외에도 환자는 학년 말 객관적 구조화 임상시험(OSCE)과 같은 고부담 총괄 평가에 참여했습니다.39 환자는 공식 평가에 사용되는 학생 에세이에 대한 서면 피드백도 제공했습니다.39 환자는 학생 수행의 대부분 비인지 영역을 평가했습니다.35 46 Jha 등이 인터뷰한 의학교육자들은 학생들이 편안하게 느끼는지, 학생들이 올바른 질문을 했는지 평가하는 데 환자의 역할이 있다고 생각했습니다.66 Raj 등의 연구에 참여한 환자와 의학교육자들은 환자의 평가를 칭찬했지만, 학생들은 환자가 임상 기술을 신뢰할 수 있는지 또는 너무 관대할 수 있는지에 대해 우려를 표명했습니다.54
In addition to formative student assessment, such as feedback during teaching sessions, patients participated in high stakes summative assessments, such as the final year objective structured clinical examination (OSCE).39 Patients also provided written feedback to student essays, which were used for formal assessment.39 Patients assessed mostly non-cognitive domains of student performance.35 46 Medical educators interviewed by Jha et al believed there was a role for patients in assessing whether students made them feel at ease and whether students asked the right questions.66 While patients and medical educators in the study by Raj et al54 praised patients’ assessments, students expressed their concerns whether patients could reliably assess clinical skills or whether they were likely to be too lenient.54
커리큘럼 개발에서 환자의 역할
Patient role in curriculum development
커뮤니티 구성원들은 커리큘럼 개발에 참여하고자 하는 동기가 있었습니다.35 의료 전문가로 간주되지는 않았지만, 자신과 가족을 위한 최적의 의료 서비스를 보장하는 데 관심이 있었습니다.26
Community members were motivated to participate in curriculum development.35 While they were not seen as medical experts, they did have an interest in ensuring optimal healthcare for themselves and their families.26
지역사회 구성원은 교육 프로그램의 계획, 실행 및 평가에 적극적으로 참여했습니다.46 49 환자 교사는 계획 단계부터 교육 전달 단계까지 자율성을 가졌습니다.43 67 여러 환자가 정신과 교육과정28 및 전문직 간 교육 교육과정의 운영위원회 위원으로 활동했습니다.49
Community members actively participated in the planning, implementation and evaluation of the educational programme.46 49 Patient teachers had autonomy from the stage of planning to the stage of delivery of teaching.43 67 Several patients were members of the steering committee for the psychiatry curriculum28 and the interprofessional education curriculum.49
환자들은 자신의 질병 또는 사회적 상태와 관련된 교육과정 개발에 참여했습니다.35 원주민 대표들은 원주민 건강 교육과정 개발 및 지역사회 배치에 대한 권장 사항을 제공했습니다.33 44 하와이 원주민과의 포커스 그룹 회의는 문화적 역량 및 건강 격차 교육과정을 정의하기 위해 열렸습니다.37 트랜스젠더 건강 교육과정에 대한 월드 카페 토론도 마찬가지로 열렸습니다.36 소수자 커뮤니티 회원들은 교육과정 설계, 특히 암 격차 교육과정의 내용에 대한 의견을 제공했습니다.35
Patients were involved in the development of courses related to their illness or social conditions.35 Aboriginal delegates provided recommendations for the development of an Aboriginal health curriculum and community placement.33 44 Focus group meetings with Native Hawaiians were held to define a cultural competencies and health disparities curriculum.37 A world café discussion was similarly held to inform the curriculum on transgender health.36 Minority community members provided input on curricular design, especially on the content of the cancer disparities curriculum.35
질병 또는 역량별 교육과정 외에도 이해관계자와의 자문 회의에 참여하여 바람직한 특성, 졸업생의 역량, 지역사회 기반 학습 환경 개발을 파악했습니다.45 환자들도 교육과정의 바람직한 특성에 대해 자문을 구했습니다.68 한 의과대학에서는 포커스 그룹을 통해 신설 의과대학의 인구보건학과의 전략적 발전을 위한 의견을 구했습니다.69
Beyond the disease or competency-specific courses, patients were involved in consultative meetings with stakeholders to identify desirable attributes, competencies of graduates and development of a community-based learning environment.45 Patients were also consulted on the desired characteristics of the curriculum.68 One medical school sought input for the strategic development of the department of population health in a new medical school through focus groups.69
의과대학 학생 선발에서 환자의 역할
Patient role in selection of students to medical schools
커뮤니티 구성원은 임상의사 및 교수진과 함께 의학전문대학원 입학 프로그램에 지원하는 학생을 선발하는 패널에 초대되었습니다.32 커뮤니티 구성원은 특히 지원자의 의사소통 능력과 사회적 맥락 및 사회적 요구에 대한 민감성, 연민, 공감 능력을 평가하는 학생 선발 과정 및 팀의 일원으로 초대되었습니다.45
Community members were invited to join a panel together with clinicians and academic staff members to select students applying for the Graduate Entry Medical Program.32 Members of the community were invited to be a part of the student selection process and team, especially in assessing candidates’ communication skills as well as sensitivity, compassion and empathy towards social contexts and societal needs.45
교수진과 환자 간의 협력
Collaboration between faculty and patients
환자 교사와의 협업에서 교수진의 역할은 다양했습니다. 일부 환자 교사는 임상 프리셉터의 감독 하에 일했습니다.60 다른 세션에서는 환자가 실무자와 공동 촉진자 역할을 했습니다.23 워크샵은 환자 교사가 주도하고 교수진이 진행했지만 통제하지는 않았습니다. 교수진의 역할은 학생과 멘토 간의 직접적인 학습을 지원하는 것이었습니다.49 교수진은 회의에 항상 참석하지는 않았지만 토론을 위한 광범위한 주제 설정과 같은 배경 지원을 제공할 수 있었습니다.46 환자 교사들은 프로그램 지원이 참여에 필수적이며, 개별 메시지를 가르치는 것에서 보편적인 수업을 가르치는 것으로 전환할 수 있게 해준다고 말했습니다.43
The role of faculty members in the collaboration with patient teachers varied. Some patient teachers worked under the supervision of a clinical preceptor.60 In other sessions, patients were cofacilitators with practitioners.23 Workshops were led by patient teachers and facilitated, but not controlled, by faculty. The faculty member’s role was to support the direct learning between students and mentors.49 Faculty was not always present in meetings but could provide background support, such as setting broad topics for discussions.46 Patient teachers stated that programme support was essential for participation, allowing them to transform from teaching individual messages to teaching universal lessons.43
한 연구에 참여한 일반인 참가자들은 일반인 관점의 중요성을 인정하기 위해 커리큘럼 소유권 공유가 필요하다고 생각한 반면, 교수진 참가자들은 커리큘럼 개발의 소유권을 추정했습니다.26 Jha 등의 연구에 참여한 [교수진]은 평가 또는 코스 개발에 환자를 더 많이 참여시키는 방법에 대해 명확하지 않았고, 그렇게 하는 것이 적절하다고 확신하지도 못했습니다. 일부 교수진은 환자 평가자 및 코스 개발자와 함께 일한 경험을 토큰주의적이라고 표현했습니다.66
Lay participants of one study regarded sharing of curriculum ownership as necessary to acknowledge the importance of lay perspectives, whereas faculty participants presumed ownership of curriculum development.26 Faculty in the study by Jha et al were not clear on how to involve patients more fully in assessments or course development, nor were they convinced of the appropriateness of doing so. Some faculty members expressed their experiences of working with patient assessors and course developers as tokenistic.66
환자의 적극적인 참여를 통한 학습 목표 달성
Learning objectives pursued through active patient involvement
환자 참여의 학습 결과는 4건의 무작위 대조 실험42 47 54 62 과 2건의 추가 연구에서 MSK 검사 기술을 주제로 정량적으로 평가되었습니다.56 59 훈련된 환자 교육자가 제공한 세션과 류마티스내과 직원이 수동적으로 검사를 받는 환자와 함께 제공한 세션54 62 및 비 MSK 전문 의사와의 세션을 비교했을 때 구조화된 임상 검사(OSCE) 점수 증가에 차이가 관찰되지 않았습니다.42 Humphrey-Murto 등의 실험에서 교수진이 가르친 학생은 환자 교육자가 가르친 학생(30명 중 5명)보다 낙제한 학생이 훨씬 적었습니다(32명 중 0명).62 학생들은 환자 교육자보다 교수진 교육자를 더 높게 평가했습니다(5점 리커트 척도에서 4.13점 대 3.58점).62
Learning outcomes of patient participation were quantitatively assessed on the subject of MSK examination skills in four randomised controlled experiments42 47 54 62 and two further studies.56 59 No difference was observed in increased structured clinical examination (OSCE) scores when comparing sessions delivered by trained patient educators with sessions delivered by rheumatology staff together with a passive patient undergoing examination54 62 and sessions with a non-MSK specialist physician.42 In the experiment by Humphrey-Murto et al, significantly fewer faculty-taught students failed (0 out of 32) than patient educator-taught students (5 out of 30).62 Students rated faculty educators higher than patient educators (4.13 vs 3.58 on a 5-point Likert scale).62
교수진이 주도하는 정규 세션 외에 환자 교사의 교육을 받은 학생은 정규 커리큘럼에 참여한 학생에 비해 OSCE 점수가 더 많이 상승했습니다.47 de Boer 등59 의 중재는 학생들에게 전임상 MSK 장애 블록에서 두 번의 비의무적 실제 환자 학습 세션에 참여할 기회를 제공했습니다.59 참여한 학생들은 블록 종료 테스트에서 훨씬 더 높은 점수를 얻었습니다
When students were taught by a patient teacher in addition to the regular faculty-led sessions, their OSCE scores increased more compared with students participating in the regular curriculum.47 An intervention by de Boer et al59 offered students the opportunity to participate in two non-obligatory real patient learning sessions in the preclinical MSK disorders block.59 Students who participated scored significantly higher at the end-of-block test.
오스왈드 등은 MSK 신체 검사 술기를 가르칠 때 환자 교육자와 의사 교육자 간에 교육 방식이 어떻게 다른지 조사했습니다.58 비디오 녹화에 따르면 교육을 받은 환자 교육자는 모든 주요 관절을 일관되게 다룸으로써 내용과 스타일이 더 일관된 것으로 나타났습니다. Bokken 등53 은 실제 환자와 시뮬레이션 환자의 교육 효과에 대한 학생의 관점을 평가했습니다.53 전반적으로 교육 효과가 높은 것으로 나타났습니다. 학생들은 실제 환자를 더 현실감 있고 신체 검사 실습에 더 유용하다고 생각했습니다.
Oswald et al examined how teaching was different between patient educators and physician educators when teaching MSK physical examination skills.58 Video recordings show that trained patient educators were more consistent in content and style by consistently covering all major joints. Bokken et al53 assessed student’s perspectives on instructiveness of real patients versus simulated patients.53 Overall instructiveness was marked high. Students regarded real patients as more authentic and the encounters more useful in practising physical examination.
Jaworksy 등의 중재 연구에서는 의대생이 환자 강사에게 HIV 검사 상담을 제공했습니다.60 검증된 의료진 HIV/AIDS 낙인 척도70의 중재 전 및 중재 후 점수는 유의미한 감소(68.74점 대 61.81점)를 보여주었습니다. 학생들은 HIV 관련 치료를 제공할 때 편안함이 증가했다고 보고했습니다(10.24점 대 18.06점). 마찬가지로 신체적 또는 정신적 장애를 가진 환자 교사를 대상으로 한 중재 연구에 참여한 학생들은 태도 개선,28 의사소통의 편안함 증가,57 자기 효능감과 자신감 증가,63 모든 인터뷰 스테이션에서 평균 수행 점수가 대조군에 비해 높은 것으로 나타났습니다.65
In the intervention study by Jaworksy et al, medical students provided HIV test counselling to patient instructors.60 Preintervention and postintervention scores of the validated Health Care Provider HIV/AIDS Stigma Scale70 demonstrated a significant decrease (68.74 vs 61.81). Students reported increased comfort in providing HIV-related care (10.24 vs 18.06). Similarly, students in intervention studies with patient teachers living with physical or mental disabilities demonstrated an improved attitude,28 increased levels of comfort in communication,57 increased levels of self-efficacy and confidence,63 65 and higher mean performance scores across all interview stations when compared with a control group.65
Rees 등의 연구에 참여한 학생들은 교과서 학습에 비해 환자와의 만남이 더 동기 부여가 되었다고 설명했습니다.71
Students in the study by Rees et al described the encounters with patients as more motivating compared with textbook learning.71
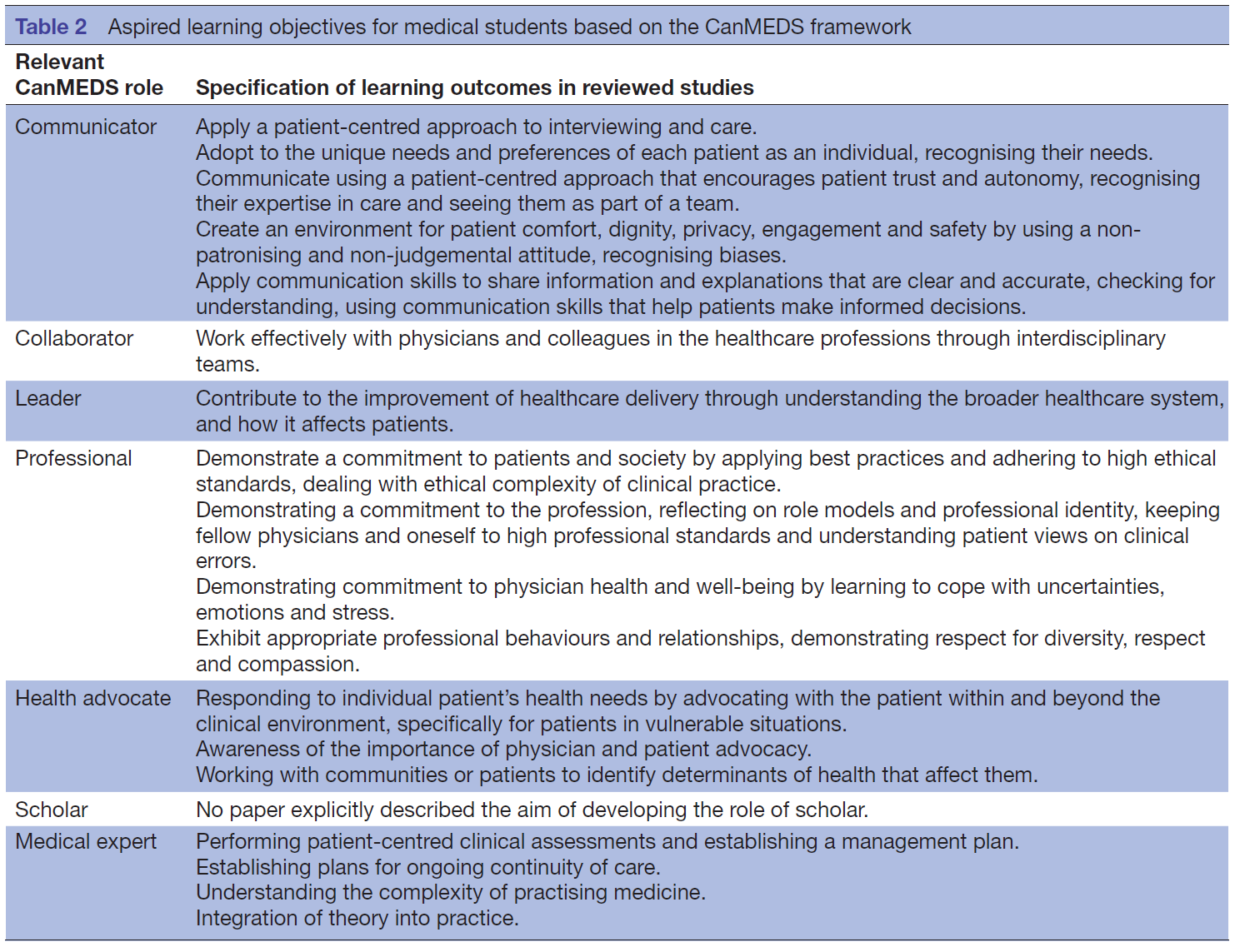
이 검토에서 확인된 질적 연구에서는 환자 참여 교육의 광범위한 학습 성과가 언급되었습니다. 이러한 다양한 결과를 탐색하기 위해 캐나다 왕립 의사 및 외과의사 대학에서 개발한 CanMEDS 프레임워크에 따라 분류를 사용했습니다22(표 2).
Wide ranges of learning outcomes of education with patient participation were mentioned in the qualitative studies identified by this review. To explore this range of outcomes a categorisation is used according to the CanMEDS framework, developed by the Royal College of Physicians and Surgeons of Canada22 (table 2).
커뮤니케이터
Communicator
몇몇 저자는 환자 참여 교육의 주요 성과로 환자 중심 진료를 언급했습니다.23 27 29 49 67 환자 중심에는 다음이 포함되었습니다.
- 환자 멘토를 개인으로 보는 능력,27
- 치료에서 환자 자율성과 전문성의 중요성,64
- 동정적이지 않고 판단하지 않는 태도,55
- 환자의 필요를 인식하고41
- 환자를 팀의 유능한 일부로 보는 것41
Jha 등은 적극적인 환자 참여 자체가 동등한 파트너십을 보여준다고 지적했으며66 Rees 등은 이 접근법이 학생들이 의료에 대한 총체적인 시각을 개발하는 데 도움이 된다고 결론을 내렸습니다.71
Several authors mentioned patient-centred care as the main outcome of education involving patients.23 27 29 49 67 Patient-centredness included
- the ability to see patient mentors as individuals,27
- the importance of patient autonomy and expertise in care,64
- adopting a non-patronising and non-judgemental attitude,55
- recognising patients’ needs41 and
- seeing the patient as a capable part of the team.41
Jha et al pointed out that active patient involvement by itself demonstrates an equal partnership66 and Rees et al concluded that this approach helps students to develop a holistic perspective of healthcare.71
보다 일반적으로 환자 참여는 의사소통의 중요성에 대한 이해 증가,27 29 의사소통 기술 구축 및 향상,55 71 공감, 경청 기술 및 존중과 관련이 있습니다.71
More generally, patient participation was associated with increased understanding of the importance of communication,27 29 building and improving communication skills,55 71 empathy, listening skills and respect.71
협력자
Collaborator
McKinlay 등은 학생들이 만성 질환을 앓고 있는 환자의 가정 방문을 수행하는 교육 프로그램을 설명했는데,31 학생들은 반성적 평가에서 만성 질환 관리에서 다학제간 팀에 대한 이해가 높아진 것으로 나타났습니다. 4명의 저자가 환자가 참여하는 전문가 간 교육 프로그램을 설명했습니다.23 27 44 49
McKinlay et al described an education programme in which students undertake a home visit to a patient with a chronic condition,31 where students demonstrated increased understanding of interdisciplinary teams in management of chronic conditions in their reflective assays. Four authors described interprofessional education programmes in which patients are involved.23 27 44 49
리더
Leader
의학, 물리치료, 작업치료, 간호학, 약학 학생이 환자 멘토와 팀을 이룬 종단적 멘토 프로그램에서 학생들은 의료 시스템에 대해 더 깊이 이해했다고 보고했습니다.27 1년 동안 진행된 학생 멘토 프로그램은 학생들에게 치료의 연속성에 대한 경험과 인식을 제공했습니다.55
In a longitudinal mentor programme with medical, physical therapy, occupational therapy, nursing and pharmacy students teaming up with a patient mentor students reported a deeper understanding of the healthcare system.27 A yearlong student mentor programme gave students an experience in and appreciation of continuity of care.55
전문가
Professional
다양한 질적 연구에 따르면 환자 참여는 임상 실무의 윤리적 복잡성과 임상의 오류에 대한 환자의 관점을 다루고64 반성적 기술을 개발하는 데 기여할 수 있다고 합니다.29 48 55 역할 모델에 대한 고찰 일부 저자는 의료인의 역할에 대한 이해의 폭을 넓히고,27 개인적 이상향에 관하여 알려주는 뛰어난 임상의의 자질,64 미래의 전문직 모델55 및 전문직 정체성을 만드는 것을 언급했습니다.71 실제 환자 교육자와의 만남 경험도 불확실성, 감정 및 스트레스에 대처하는 데 도움이 될 수 있습니다.71
Various qualitative studies suggested that patient involvement can attribute to dealing with ethical complexity in clinical practice and patients’ perspectives on clinician error64 and developing reflective skills.29 48 55 Reflecting on role models some authors referred to broadening understanding of the role of the healthcare provider,27 qualities of remarkable clinicians that inform personal ideals,64 creating a future professional model55 and professional identity.71 Experiences with real patient educator encounters could also help in coping with uncertainties, emotions and stress.71
특정 환자 또는 소수자 그룹의 환자 교육자에 대한 노출은 학생들이 만성 질환과 노인,27 31 정신 건강 문제29 또는 장애를 가진 환자에 대한 긍정적인 태도를 높이는 데 도움이 되었습니다.48
Exposure to patient educators from within specific patient or minority groups helped students increase positive attitude towards chronic conditions and elderly,27 31 patients with mental health problems29 or disabilities.48
건강 옹호자
Health advocate
환자 멘토와의 윤리 및 전문성 모듈 경험에 대한 연구에서 학생들은 일상적인 실무에서 환자 옹호의 중요성에 대해 성찰했습니다.64 보다 구체적으로, 학생들은 취약한 상황에 처한 환자를 옹호할 수 있는 역량을 갖추게 되었습니다. 사켓쿠 등이 설명한 교육 프로그램의 목표 중 하나는 특히 장애인의 맥락에서 의사 옹호의 영향에 대한 인식을 개발하는 것이었습니다.63 사전 테스트와 사후 테스트에 따르면 이 프로그램을 통해 이러한 인식이 크게 증가한 것으로 나타났습니다.
Students reflected on the importance of patient advocacy in day-to-day practice in a study on experiences within an ethics and professionalism module with patient mentors.64 More specifically, students were empowered to advocate for patients when they are in vulnerable situations. One of the aims of the education programme described by Saketkoo et al was to develop an awareness of the impact of physician advocacy, specifically in the context of people with disabilities.63 A pretest and post-test showed that this awareness increased significantly with the programme.
학자Scholar
학자 역량 개발의 목표를 명시적으로 설명한 프로그램은 없습니다.
No programmes have explicitly described the aim of developing the competency of scholar.
의료 전문가
Medical expert
의료 전문가의 역할은 환자 중심의 고품질의 안전한 진료를 제공하기 위해 의학 지식, 임상 기술 및 전문적 가치를 적용함으로써 다른 모든 역할을 통합하는 것입니다. 두 논문에서는 환자 참여가 의학 실습의 복잡성을 인식함으로써 학생의 학습을 지원한다고 언급했습니다.41 48 Jha 등은 환자가 실습에서 이론의 예시를 제공함으로써 학생의 이해와 기억을 향상시킨다고 설명했습니다.66
The role of medical expert integrates all other roles by applying medical knowledge, clinical skills and professional values in the provision of high-quality and safe patient-centred care. Two articles mentioned that patient participation supports students’ learning by recognising the complexity of practising medicine.41 48 Jha et al described the patient as providing an illustration of the theory in practice, thus enhancing students’ understanding and recall.66
환자 참여에 대한 우려
Concerns about the involvement of patients
여러 저자들은 의학교육에 환자를 교사로 참여시킬 때 우려를 제기하기도 했습니다. 일부 교수진 교육자들은 환자의 이야기가 너무 충격적이어서 학생들이 그로 인한 감정을 다루기 위해 지원이나 디브리핑이 필요할 수 있다고 우려했습니다.66 71 질적 연구에서 학생들은 서비스 사용자가 임상의에게 물어보지 않고 정보와 조언을 요청하거나 서비스 사용자가 임상의에게 말하지 않은 정보를 학생들에게 누설할 때 '압박'을 느꼈습니다.71 학생들은 환자에게 잘못된 정보를 제공할까 봐 걱정했습니다.
Various authors have also raised concerns when involving patients as teachers in medical education. Some faculty educators were concerned that patient stories might be so traumatic that students would require support or debriefings to deal with the resulting emotions.66 71 In a qualitative study, students felt ‘pressured’ by service users asking them for information and advice, rather than asking their clinicians, or when service users divulged information to students that they had not told their clinicians.71 Students worried about giving incorrect information to patients.
학생들은 한 사람의 관점만 보게 되어 편향된 시각을 갖게 될 수 있다는 우려를 표명했습니다.23 학생들은 또한 환자들이 좋은 퍼포먼스와 안 좋은 퍼포먼스를 구별하기 어렵고, 피드백이나 평가에 너무 관대할 수 있다는 점을 우려했습니다.54 Henriksen과 Ringsted67 의 연구에 참여한 학생들은 환자의 지식에 대해 회의적인 태도를 보였으며67 환자가 교육 환경을 계획하고 전달하는 데 자율성을 갖는 맥락에서 구조화되지 않은 체험 학습에 대해 우려를 표명했습니다.67 다른 연구에서 직원들은 동일한 환자가 동일한 프로그램에 너무 자주 참여하면 환자 경험의 영향이 감소될 수 있다는 우려를 표명했습니다.66
Students expressed reservations that they were only getting the view of one person, which could lead to a biased perspective.23 Students were also concerned that patients might have difficulty discriminating between poor and good performance, and are likely to be too lenient in feedback or assessment.54 Students in the study by Henriksen and Ringsted67 expressed scepticism about patients’ knowledge67 and expressed concerns about unstructured experiential learning in a context where patients had autonomy in both planning and delivering the teaching encounter.67 In a different study, staff members expressed the concern that the impact of the patient experience might be reduced if the same patient was involved in the same programme too often.66
환자 참여의 영향에 대한 환자들의 견해
Patients’ views of the impact of their involvement
환자들은 환자 중심주의를 가르치고,24 72 자신의 몸과 진정성을 제공하고, 학생들의 자신감을 강화하며,72 더 넓은 지역사회에 대한 책임을 다하고,24 32 의료 시스템을 개선하기 때문에 의미 있는 기여와 개인적인 성취감을 느낀다고 설명했습니다.24 33 40
Patients described a strong sense of having a meaningful contribution and personal fulfilment, because they were teaching patient-centredness,24 72 offering their body and authenticity, bolstering students’ confidence,72 fulfilling their responsibility to the broader community24 32 and improving the healthcare system.24 33 40
환자들은 개인적 차원에서 물질적, 직업적, 개인적, 정서적 혜택을 설명했습니다. 물질적 혜택에는 선물과 같은 유형의 보상43 을 받고 전체 건강 검진을 받은 것이 포함되었습니다.40 의대생 교육에 참여한 요통 환자 교육자들은 참여로 인해 자신의 요통 관리가 개선되었고, 의사와의 상담에서 자신의 요구를 표현하는 데 자신감이 향상되었다고 말했습니다.47 일부 환자들은 교육할 때 의료 전문가로부터 더 많은 시간과 관심을 받았다고 느꼈습니다.71
On an individual level patients described material, professional, personal and emotional benefits. Material benefits included receiving tangible rewards such as gifts43 and receiving a full medical check-up.40 Patient educators with back pain involved in teaching medical students stated their participation improved the management of their own back pain, and improved confidence in voicing their needs in consultations with physicians.47 Some patients felt that they received more time and attention from their healthcare professionals when they were teaching.71
환자들은 학생 선발 과정에 참여함으로써 직업적 성장과 개인적 성취감을 느꼈다고 설명했습니다.32 하템 등은 의료 서비스 제공자를 더 찾는 것을 더 잘 하게 되었다거나, 자신의 건강 상태에 대한 지식이 증가하는 등 환자에게 실질적인 이점이 있다고 보고했습니다.43
Patients described professional growth and personal fulfilment from being involved in the selection process of students.32 Hatem et al reported practical benefits for patients including getting better at finding healthcare providers and increased knowledge of their medical condition.43
환자가 의료 교육에 참여하는 것과 관련된 단점과 위험에는 낙인찍는 가정, 자기 공개에 대한 취약성 및 자발적인 질의응답 교환에 직면하는 것이 포함됩니다. 예를 들어, HIV를 주제로 강의하는 한 환자 교육자는 한 남성이 질병에 대한 지식 부족과 무지로 인해 매우 좌절했던 경험을 설명했습니다. 환자들은 또한 예상치 못한 질병의 진행이 교육 능력에 영향을 미친다는 사실에 주목했습니다. 어떤 경우에는 이로 인해 교사로서의 헌신에서 손을 떼는 경우도 있었는데, 이는 환자 교육자들 사이에서 불가피한 손실이었습니다.43 환자들은 또한 학생들의 부정적이고 인정하지 않는 반응에 대한 취약성을 설명했습니다.40 47 멘토들은 초기에 일반적으로 자신이 공유하는 내용이 학생들에게 도움이 되는지에 대해 불안하고 확신하지 못했습니다.29 사회경제적으로 열악한 지역에서 지역사회 기반 개입에 참여한 환자의 절반은 인터뷰 전에 불안, 걱정 또는 긴장감을 표현했지만, 모든 경우에서 환자는 이것이 정상이라고 느꼈습니다.52 환자들은 '취약하다'는 단어 외에도 임상 교육 환경 내에서 서비스 이용자의 감정을 강조하기 위해 '노출', '두려움', '피곤함', '스트레스' 및 '괴로움'과 같은 용어를 사용했습니다.71 일부는 정신건강 서비스 이용자가 자신의 이야기를 반복적으로 말하는 것이 트라우마틱하다고 설명하기도 했습니다.71
The drawbacks and risks associated with patient involvement in medical education included being confronted with stigmatising assumptions, vulnerability of self-disclosure and spontaneous question-answer exchanges. A patient educator teaching on the subject of HIV, for example, described the experience of being very frustrated with one man’s lack of knowledge and ignorance about the disease. Patients also drew attention to the fact that unanticipated disease progression had an impact on their ability to teach. In some cases, this resulted in them pulling out of their commitment as teachers, an inevitable loss among patient educators.43 Patients also described a sense of vulnerability to negative and non-appreciative reactions from students.40 47 Initially, mentors were commonly anxious and unsure about whether what they shared was of benefit to students.29 Half of the patients involved in the community-based intervention in a socioeconomic-deprived area expressed feelings of anxiety, apprehension or nervousness prior to the interview, although in all cases patients felt that this was normal.52 In addition to the word ‘vulnerable’, patients employed terms like ‘exposed’, ‘frightened’, ‘tired’, ‘stressed’ and ‘harrowing’ to emphasise service users’ feelings within the clinical education environment.71 Some even described it as traumatic for mental health service users to repeatedly tell their stories.71
의학 교육에 대한 환자 참여의 재정적 영향
Financial implications of patient involvement in medical education
19편의 논문에서 환자 비용 상환, 사례금 지급, 조직 비용 또는 비용에 대한 인식 등 개입의 재정적 측면에 대해 언급했습니다. 그러나 경제적 및 재정적 자원은 체계적으로 비교할 수 있는 방식으로 조사되지 않았습니다. 보고된 재정적 비용에는 장애 기술 워크숍에 800달러,63 신체 검사 교육에 800파운드54, 전체 환자 파트너 프로그램에 2640파운드가 포함되었습니다.47 10개의 연구에서 참여 환자에게 시간당 8유로에서 하루 350파운드43 53 54 또는 불특정 금액의 보수를 제공했습니다.28 35 39 48 50 57 4개의 연구에서 여행, 전화 또는 우편 비용과 같은 환자 비용을 환급했습니다.24 34 47 65 일부 직원은 환자가 다과나 대중교통에 지출해야 하는 현금이 참여에 장벽이 될 것을 두려워했습니다.73
Nineteen articles commented on any financial aspect of the interventions, ranging from reimbursement of patients’ expenses, payments of honoraria, organisational costs or perceptions of cost. Economic and financial resources, however, have not been explored in a way that they can be systematically compared. Reported financial costs included $800 for a disability skills workshop,63 £800 for a physical examination training54 and £2640 for the overall Patient Partners programme.47 Ten studies offered participating patients remuneration through honoraria between €8 per hour and £350 per day43 53 54 or an unspecified amount.28 35 39 48 50 57 Four studies offered reimbursement of patient expenses such as travel, phone or mail costs.24 34 47 65 Some staff feared that cash patients needed to spend on refreshments or public transport would be a barrier for their participation.73
의학교육자들은 환자 참여가 재정적 투자와 직원 시간 모두에서 비용이 많이 드는 노력이라고 제안했습니다.71 비용 효과성에 대해 언급한 논문은 한 편뿐으로, 환자 주도 교육이 의사 주도 교육에 비해 비용 효율적인 방법이라고 언급했지만 경제적 평가는 제공하지 않았습니다.54 비용 효과성 또는 비용 편익 분석을 제공한 논문은 없었습니다.
Medical educators suggested that patient involvement was a costly endeavour, both in financial investment as well as staff time.71 Only one article commented on cost-effectiveness, noting that patient-led teaching is a cost-effective method compared with physician-led teaching, but did not provide an economic evaluation.54 No paper provided a cost-effectiveness or cost-benefit analysis.
환자 단체의 역할
Roles of patient organisations
환자 단체와 의료진 간의 가장 많이 언급된 상호작용은 개별 환자를 지역사회 구성원 또는 질환별 지원 그룹의 구성원으로 모집하기 위해 환자 단체와 네트워크를 활용하는 것이었습니다.24 28 29 36 49 55 56 60 69 Baral 등의 논문에서는 의과대학 운영위원회가 보건과학 아카데미 교육과정 개발을 위해 농촌 지역사회 및 소비자 단체의 대표들에게 자문을 구했습니다.45 지역사회에 기반을 둔 환자 옹호 및 지원 단체의 대표들이 Towle과 Godolphin의 연구에서 중재 자문 그룹에 참여했습니다.49 이러한 환자 단체의 대표들이 모두 환자 본인이었던 것은 아닙니다. 이들은 학계와 지역사회라는 두 문화 사이의 중개자 역할을 수행했습니다.
The most cited interaction between patient organisations and medical faculties was the use of patient organisations and their networks for the recruitment of individual patients as community members or members of condition-specific support groups.24 28 29 36 49 55 56 60 69 In the paper by Baral et al, representatives from rural communities and consumer groups were consulted by the medical school steering committee for the development of the Academy of Health Sciences curriculum.45 Representatives of community-based patient advocacy and support organisations took part in the advisory group of the intervention in the study by Towle and Godolphin.49 Not all of these representatives of patient organisations were patients themselves. They were described as brokers between two cultures of academia and community.
리즈 대학교는 자신의 경험을 바탕으로 교사와 연구자로서의 역할을 알리는 일반인들로 구성된 '환자 목소리 그룹'이라는 내부 환자 전담 그룹과 협력했습니다. 이 그룹은 형성 평가와 종합 평가에 참여했습니다. 또한 학교 내에 지속적인 지원을 제공하는 환자 및 대중 참여 관리자가 배정되었습니다.39
The University of Leeds worked with a dedicated internal patient group named ‘The Patient Voice Group’, consisting of lay people who use their experiences to inform their roles as teachers and researchers. This group was involved in formative and summative assessment. Additionally, a patient and public involvement manager who provided ongoing support was assigned within the school.39
일부 의학교육자들은 정치적인 단체와 협력하는 것에 대한 두려움 때문에 환자 단체와 협력하지 않기로 명시적으로 선택했습니다.71 그들은 토큰주의에 대한 비판을 방지하기 위해 다양한 목소리를 들을 수 있도록 여러 환자 그룹을 포함시키기로 결정했습니다. 환자들은 그룹에 참여함으로써 동료들로부터 지지와 우정을 얻을 수 있었다고 말했습니다.71
Some medical educators made the explicit choice not to collaborate with patient organisations, due to a fear of working with politicised groups.71 They did make a decision to include groups of patients to allow multiple voices to be heard in order to prevent criticisms of tokenism. Patients stated that participating in groups gave them support and companionship from their peers.71
의료 교육에 참여하고자 하는 환자 단체는 상자 1 에 설명된 몇 가지 실용적인 사항을 고려할 수 있습니다.
Patient organisations wishing to engage in medical education may wish to consider some of the practical points as described in box 1 .
박스 1. 의료 교육에 참여하고자 하는 환자 단체를 위한 실용적인 사항
Box 1. Practical points for patient organisations wishing to engage in medical education
환자 단체를 위한 실용적인 포인트
Practical points for patient organisations
- 회원들에게 의학교육 참여의 잠재적 이점을 강조하고 공통된 동기에 부응합니다.
- 의학교육에 참여하는 환자들 간에 동료 지원 네트워크를 활성화합니다.
- 해당 지역의 교육 기관에 환자 및 대중의 참여를 위한 기존 프레임워크가 있는지, 환자 및 대중의 참여를 명시적으로 약속했는지, 환자 및 대중의 참여를 전담하는 임원을 임명하여 협력의 시작점을 제공할 수 있는지 조사합니다.
- 의료진 내에 환자 위원회 또는 자문 그룹을 구성하여 교육 과정에 구조적으로 환자의 의견을 반영하고 보호할 수 있도록 요청합니다.
- 교육 과정의 어느 단계가 목표에 가장 적합한지 결정합니다. 학교의 사명과 비전, 학습 목표, 교육 전략, 교수법, 학습자 평가 또는 코스 평가에 노력을 집중할 수 있습니다.
- 모든 의미 있는 개입이 전체 교수진 수준에서 이루어져야 하는 것은 아니며, 하나의 학습 목표 또는 특정 질병 관련 코스와 같은 특정 영역에 집중할 수도 있습니다.
- 대학과의 성공적인 협업과 모범 사례를 더 많은 환자 및 학계 커뮤니티에 소개하세요.
- Highlight potential benefits of involvement in medical education to members and respond to common motivations.
- Facilitate peer support networks among patients involved in medical education.
- Investigate whether teaching facilities in your area have existing frameworks for patient and public involvement, have made explicit commitments to patient and public involvement and/or have appointed officers specifically assigned to patient and public involvement that could provide you with a starting point for collaboration.
- Call for the creation of a patient committee or advisory group within a medical faculty to enable and safeguard structural input into the educational process.
- Determine which step of the educational process is best suited for your goals. You might choose to focus your efforts on the mission and vision of the school, learning objectives, educational strategies, teaching, assessment of learners or the evaluation of the course.
- Not every meaningful intervention has to be at an overall faculty level, they may also be on specific areas such as one learning objective or a disease-specific course.
- Showcase successful collaborations with universities and best practices to the wider patient and academic communities.
환자 참여의 지속 가능성을 보장하기 위한 조치
Measures to ensure the sustainability of patient involvement
환자 참여를 유지하는 데 있어 핵심 요소로 확인된 것은
- 적절한 자원 지원 제공,
- 일반인 기여의 가치에 대한 공식적인 인정,
- 일반인 의견에 따른 변화에 대한 교수진의 명확한 약속이었습니다.26
The key factors identified in sustaining patient involvement were
- the provision of adequate resource support,
- formal acknowledgement of the value of lay contributions and
- a clear faculty commitment to change following lay input.26
환자와 지역사회 참여를 보장하기 위해 대학의 사명과 비전 선언문 또는 전략 계획에 사회적 책임 또는 환자 중심 교육과 의료를 기관 전체에 통합하는 것이 여러 논문에서 인용되었습니다. 저자들은 환자 참여 프로그램의 자원 집약도가 높기 때문에 대학이 지속 가능하려면 [환자 중심의 토대]를 중시해야 한다고 강조했습니다.26 44 45 61 커리큘럼에 지속적인 모듈로 이니셔티브를 통합하면 산발적인 환자 참여가 아닌 지속 가능한 환자 참여를 달성할 수 있습니다.53 63
Institution-wide incorporation of social accountability or patient-centred education and medicine in the university’s mission and vision statement or strategic plan was cited in several papers to ensure patient and community involvement. The authors emphasised that the resource intensity of a patient involvement programme requires the university to value its patient-centred underpinnings in order to be sustainable.26 44 45 61 The incorporation of initiatives as ongoing modules in the curriculum achieved sustainable patient involvement rather than sporadic involvement.53 63
리즈대학에서는 기관에 [상설 환자 의견 그룹]이 설립되었습니다.39 이 기관은 환자 및 대중 참여 관리자를 임명하여 지속적인 지원을 제공했습니다. 일부 이니셔티브는 기존 기관과 협력하거나, 학교 전체 수준에서 시행하거나45 관절염과 같은 한 가지 질환에 초점을 맞추었습니다.58 Gaver 등55 은 환자 참여의 지속 가능성을 위한 핵심 과제로 자원봉사 조직과 가족 간의 약속을 수립하는 과정을 확인했습니다.55
In the University of Leeds, a permanent patient voice group was incorporated in the institution.39 The institution appointed a patient and public involvement manager to provide ongoing support. Some initiatives chose to work in partnership with existing institutions, implemented at a school-wide level45 or focused on one condition such as arthritis.58 Gaver et al55 identified the process of establishing commitment among volunteering organisations and families as a key challenge to the sustainability of patient involvement.55
의학교육자들은 환자 교육자가 급여를 받고 의과대학의 직원으로 간주된다면, 그들은 더 진지하게 역할을 수행하고 더 신뢰할 수 있을 뿐만 아니라 교육 팀의 존경받는 일부로 여겨질 수 있다고 언급했다.66
Medical educators commented that if patient educators were paid and seen as an employee of the medical school, they might take on the role more seriously and become more reliable, as well as being seen as a respected part of the educational team.66
토론
Discussion
이 검토는 49개의 주요 경험적 연구를 체계적으로 평가했으며, 의대 학부 교육에서 환자의 적극적인 참여의 역할과 영향에 대한 업데이트된 통합 증거를 제공하는 것을 목표로 했습니다. 새로운 경험적 증거는 학부 의학교육에서 환자가 적극적으로 참여하는 학습 목표와 교육 환경의 범위가 점점 더 넓어지고 있음을 보여줍니다.
This review systematically evaluated 49 primary empirical studies and was aimed at providing updated integrated evidence on the role and impact of the active involvement of patients in medical undergraduate education. The new body of empirical evidence shows the increasing range of learning objectives and educational settings in which patients play an active part in undergraduate medical education.
우리 연구에 따르면 환자들은 의학교육에 참여함으로써 물질적, 전문적, 개인적, 정서적 이점을 얻었다고 설명했습니다. 기대되는 혜택 외에도 여러 저자는 환자 참여 프로그램을 시작해야 하는 근거로 정책적 의무를 언급했습니다. 그러나 몇몇 연구에서는 낙인찍힘에 대한 두려움, 토큰주의 또는 교육 세션의 구조 부족과 같은 잠재적인 피해와 부정적인 경험에 대해 보고했습니다. 학생, 교수진, 환자 스스로가 제기하는 환자 참여와 관련된 우려는 체계적인 방식으로 면밀히 모니터링하고 적절하게 해결해야 합니다.
Our study found that patients described material, professional, personal and emotional benefits of participating in medical education. In addition to expected benefits, several authors mentioned policy mandates as rationale for initialising patient involvement programmes. Several studies however reported on the potential harms and negative experiences, such as fear of stigmatisation, tokenism or lacking structure of teaching session. Concerns related to patient involvement coming from students, faculty and patients themselves should remain closely monitored in a systematic manner and addressed appropriately.
포함된 논문은 다양한 유형의 환자 역할을 설명했지만, 이전 검토와 유사하게 대부분의 논문에서 환자 교사의 역할을 언급했습니다.1 17-19 최근 논문에서는 환자가 커리큘럼 개발에 점점 더 많이 관여하고 있음을 시사합니다. 이러한 이니셔티브의 대부분은 부수적인 것이었으며 제도적 통합과 장기적인 참여가 부족했습니다.
Included papers described various types of roles for patients, but the vast majority of papers cited the role of a patient teacher, similarly to previous reviews.1 17–19 More recent papers suggest that patients are increasingly involved in curriculum development. Most of these initiatives were incidental and were lacking institutional incorporation and longitudinal involvement.
이 검토에서 확인된 환자의 역할은 주로 Towle 외2(상자 2)의 검토에서 제안한 스펙트럼의 3~6단계와 일치합니다. 또한 이 스펙트럼에서 특정 레벨로 분류할 수 없는 새로운 역할도 추가로 확인했습니다. 한 역할에서 환자는 커리큘럼 개발에서 동등한 역할을 수행했지만, 전체 커리큘럼이 아닌 특정 코스에 대해서만 역할을 수행했으며, 이는 Towle의 레벨 4와 5 사이에 속했습니다. 또 다른 역할에서는 환자가 특정 과정을 넘어 교육기관 차원의 주제와 커리큘럼 개발에 대해 자문을 받았지만, 동등한 파트너라기보다는 교수진이 주도하는 이니셔티브에서 자문을 받아 Towle의 레벨 4, 5, 6.2의 부분적인 요소를 나타냈습니다.
The patients’ roles identified in this review are largely in accordance with levels 3–6 of the spectrum proposed in the review by Towle et al2 (box 2). We additionally identified new roles that could not be ascribed to one specific level on this spectrum. In one role, patients did take on roles as equal in curriculum development, but only to specific courses rather than the curriculum as a whole, falling between Towle’s levels 4 and 5. In another role, patients were consulted in institution-level topics and curriculum development beyond specific courses, but rather than being equal partners, they were consulted in a faculty-driven initiative, displaying partial elements of Towle’s levels 4, 5 and 6.2
박스 2. Towle 등이 정의한 의학교육에 대한 환자 참여의 스펙트럼2
Box 2. Spectrum of patient involvement in medical education by Towle et al2
Towle 등이 정의한 의학교육에서의 환자 참여 수준2
Levels of patient involvement in medical education as defined by Towle et al2
- 종이 기반 또는 전자 사례의 초점으로서의 환자.
- 임상 환경에서 표준화되거나 자원한 환자.
- 교수진이 주도하는 커리큘럼에서 학생들과 자신의 경험을 공유하는 환자.
- 학생을 가르치거나 평가하는 데 관여하는 환자 교사.
- 학생 교육, 평가 및 커리큘럼 개발에서 특정 과정을 넘어 커리큘럼 전체에 대한 동등한 파트너로서의 환자 교사.
- 교육, 평가 및 커리큘럼 개발에 환자 교사로서 지속적으로 참여하는 것 외에도 기관 차원에서 참여하는 환자.
- Patients as focus of a paper-based or electronic case.
- Standardised or volunteer patients in clinical settings.
- Patients sharing their experiences with students in a faculty-directed curriculum.
- Patient teachers involved in teaching or evaluating students.
- Patient teachers as equal partners in student education, evaluation and curriculum development beyond specific courses, to the curriculum as a whole.
- Patients involved at the institutional level in addition to sustained involvement as patient teachers in education, evaluation and curriculum development.
이 검토에서 확인된 학습 목표는 미래의 의사를 위한 CanMEDS의 역할 중 한 가지를 제외하고 모두 포함되었습니다. 이는 환자의 참여가 의료 커리큘럼의 다양한 측면에 지속적으로 더 큰 영향을 미치고 있음을 보여줍니다.
The learning objectives identified in this review encompassed all but one of the CanMEDS roles for future physicians. This demonstrates that patient’s involvement is continuing to gain a larger influence on a diverse range of aspects of the medical curriculum.
[지속 가능한 환자 참여를 지원하기 위한 조치]에는 다음 등이 포함되었습니다.
- 장기적인 기관 통합,
- 환자 모집 및 교육,
- 자원 지원,
- 교수진의 명확한 약속
학생, 교수진, 환자 모두 환자 참여의 중요성과 이점을 강조했지만, 기관은 환자와 학생에게 발생할 수 있는 잠재적 피해를 완화하기 위해 지속적으로 고려하고 모니터링하며 조치를 취해야 합니다. 환자 참여와 관련된 재정적 측면에 대해 보고한 논문은 소수에 불과했으며, 이는 타당성을 뒷받침하기 위해 추가 조사가 필요합니다.
Measures to support sustainable patient involvement included
- longitudinal institutional incorporation,
- patient recruitment and/or training,
- resource support and
- clear commitment by faculty.
The importance and advantages of patient involvement were highlighted by students, faculty and patients themselves; however, organisations must continue to consider, monitor and take steps to mitigate any potential harms to patients and students. Only few papers reported on the financial aspects related to patient involvement, which should be further investigated to help support feasibility.
중요한 한계는 기존 문헌에 공통된 용어가 없어 관련 논문이 누락될 위험이 높다는 점이며, 이는 이전에 다른 검토 저자들이 한계로 보고한 바 있습니다.2
An important limitation was the lack of common terminology in the existing literature, potentiating the risk of missing relevant articles, which has been previously reported as a limitation by other review authors.2
저희의 체계적 문헌고찰에는 동료 심사를 거친 저널의 원저 문헌만 포함되었습니다. 환자가 의학교육 참여에 대해 쓴 많은 논문은 블로그 게시물, 학회 성명서, 환자 단체 뉴스레터 등 회색문헌에서만 찾을 수 있으므로, 이 리뷰는 이 주제에 대한 환자 관점의 중요한 측면을 놓칠 수 있는 위험이 있습니다. 또한 영어로 작성된 연구만 포함되었기 때문에 선정된 논문이 편향되었을 수 있습니다. 포함된 논문의 대부분은 북미(n=23), 유럽(n=17), 호주 및 뉴질랜드(n=7)에서 수행되었습니다.
Our systematic review included only original literature from peer-reviewed journals. As many articles written by patients on their involvement in medical education may only be found in grey literature, including blog posts, conference statements and patient organisation newsletters, this review runs a risk of having missed important aspects of patient views on this topic. Additionally, only studies written in English were included, which may have led to bias in selected papers. The majority of included papers were from North America (n=23), Europe (n=17) and Australia and New Zealand (n=7).
포함된 연구의 대부분은 질적 연구(n=38)였으며, 그 외에는 혼합 방법(n=5) 또는 질적 연구(n=6)였습니다. 포함된 논문 중 대조군을 사용한 논문은 소수에 불과했습니다(n=7). 대부분의 경우 학생과 환자가 자발적으로 중재에 참여했기 때문에 연구 결과를 더 많은 인구에 일반화하기에는 한계가 있을 수 있습니다. 편견을 유발했을 수 있는 또 다른 중요한 요인은 대부분의 연구가 익명화되지 않았거나(익명화가 불가능) 학생 평가의 일부였기 때문에 응답에 사회적 선호 편향이 적용될 위험이 있다는 점입니다.
The majority of included studies were qualitative (n=38), others were mixed methods (n=5) or qualitative (n=6). Only few of the included papers used control groups (n=7). In most cases, students and patients participated in interventions on a voluntary basis, which may limit the generalisability of findings to the wider population. Another important factor that may have introduced bias is that most studies were not (possible to be) anonymised, or were part of student assessments, which introduces a risk of responses being subject to social desirability bias.
향후 연구는 환자, 학생, 의료 시스템에 대한 장기적인 영향, 특히 환자 중심주의와 공동 의사 결정에 대한 주제에 초점을 맞춰야 합니다. 이러한 연구 격차로 인해 현재 문헌에 기반한 권장 사항은 제한적입니다. 또한 교육 정책의 의사 결정자에게 중요한 요소일 수 있는 환자 참여에 대한 경제적 평가를 수행한 논문은 없습니다. 마지막으로, 환자 참여에 대한 기존 프레임워크를 의학교육에서 새롭게 확인된 환자의 역할과 필요에 맞게 업데이트하려면 더 많은 연구가 필요합니다.
Future research should focus on the long-term effects for patients, students and the healthcare system, especially on the subjects of patient-centredness and shared decision-making. This gap in research limits recommendations that can be made based on current literature. Additionally, no paper performed an economic evaluation of patient involvement, which may be a critical factor for decision makers in educational policy. Finally, more research is needed to update existing frameworks for patient involvement to the newly identified roles and needs patients have in medical education.
결론Conclusion
의학교육에서의 환자 참여에 관한 첫 번째 논문이 발표된 지 40년이 넘었습니다. 오늘날 의학교육계와 환자 커뮤니티는 모두 환자 중심주의를 촉진하기 위한 움직임에 함께 동참하고 있습니다. 이 체계적 문헌고찰은 교육기관에 적극적인 환자 참여를 지속적으로 통합하고자 하는 커리큘럼 개발자와 의학교육에 참여하고자 하는 환자 단체에 도움이 될 수 있는 지식과 실질적인 고려사항을 제공합니다.
It has been over 40 years since the first article on patient involvement in medical education was published. Today, both the medical education community and the patient community have joined together in the movement to promote patient-centredness. This systematic review provides knowledge and practical considerations that can aid curriculum developers who wish to sustainably incorporate active patient involvement in their institutions, and patient organisations wishing to engage in medical education.
Role of active patient involvement in undergraduate medical education: a systematic review
PMID: 32718925
PMCID: PMC7389514
DOI: 10.1136/bmjopen-2020-037217
Free PMC article
Abstract
Objectives: To identify the scope of active patient involvement in medical education, addressing the current knowledge gaps relating to rationale and motivation for involvement, recruitment and preparation, roles, learning outcomes and key procedural contributors.
Methods: The authors performed a systematic search of the PubMed database of publications between 2003 and 2018. Original studies in which patients take on active roles in the development, delivery or evaluation of undergraduate medical education and written in English were eligible for inclusion. Included studies' references were searched for additional articles. Quality of papers was assessed using the Mixed Methods Appraisal Tool.
Results: 49 articles were included in the review. Drivers for patient involvement included policy requirements and patients' own motivations to contribute to society and learning. Patients were engaged in a variety of educational settings in and outside of the hospital. The vast majority of studies describe patients taking on the role of a patient teacher and formative assessor. More recent studies suggest that patients are increasingly involved in course and curriculum development, student selection and summative assessment. The new body of empirical evidence shows the wide range of learning objectives was pursued through patient participation, including competencies as professional, communicator, collaborator, leader and health advocate, but not scholar. Measures to support sustainable patient involvement included longitudinal institutional incorporation, patient recruitment and/or training, resource support and clear commitment by faculty. The importance and advantages of patient involvement were highlighted by students, faculty and patients themselves; however, organisations must continue to consider, monitor and take steps to mitigate any potential harms to patients and students.
Discussion: This systematic review provides new knowledge and practical insights to physicians and faculty on how to incorporate active patient involvement in their institutions and daily practice, and provides suggested action points to patient organisations wishing to engage in medical education.
Keywords: education & training (see medical education & training); health services administration & management; medical education & training.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
'Articles (Medical Education) > 교육과정 개발&평가' 카테고리의 다른 글
| 의학교육의 문턱개념: 스코핑 리뷰(Med Educ, 2022) (0) | 2023.05.04 |
|---|---|
| 멀고 숨겨진 존재: 환자를 EPA의 개발, 내용, 도입의 전면에 두기(Acad Med, 2021) (0) | 2023.04.13 |
| 대표성의 딜레마: 보건전문직교육의 환자참여(Acad Med, 2018) (0) | 2023.04.09 |
| 의학교육에 환자와 공공의 참여를 향하여 (Med Educ, 2016) (0) | 2023.04.08 |
| 가정의학 전공의교육 및 CPD에서 역량중심의학교육 용어의 개념화: 스코핑 리뷰(Acad Med, 2020) (1) | 2023.02.28 |