만약 우리가 하던대로 한다면, 얻던대로 얻을 것이다: 아카데믹 메디신 다시 생각하기 (Med Teach, 2018)
If we keep doing what we’re doing we’ll keep getting what we’re getting: A need to rethink “academic” medicine
Michael Wilkesa, Christine Casselb and Marc Klaub
캔자스에서는 활강 스키를 가르치지 않을 것이다.
You wouldn’t teach downhill skiing in Kansas
(브루스 블룸버그 2015, 퍼스널 커뮤니케이션)
(Bruce Blumberg 2015, Personal Communication)
의술
The practice of medicine
미국의 의료행위는 큰 스트레스를 받고 있다: 비용 상승과 변제 감소, 생산성, 관리 품질, 남용, 이해 상충, 다양한 전문 분야와 의료 전문가 간의 영역 다툼, 방해적이고 도움이 되지 않는 전자 기록 시스템, 그리고 미래의 의사들을 가르치기 위해 의사들을 연습함으로써 시간과 헌신을 줄이는 것의 조합. 의학교육은 이러한 스트레스를 공유하는 것에 더해서, 다음과 같은 문제들에 대한 스트레스, 논쟁, 토론을 가지고 있다: 온라인 학습의 역할 확대, 콘텐츠 대 개별화된 학습 스타일, 전통적인 "2 + 2" 커리큘럼을 변경하라는 압력(기초과학 2년 및 임상 교육 2년), USMLE 시험에 배치되는 필요성, 역할 및 강조,
전문직 간 교육의 역할, 임상 환경에서 연속성의 중요성과 교수진의 가용성과 기술, 그리고 보건 시스템의 새로운 "기초 과학"의 진입.
The practice of medicine in US is under great stress: a combination of rising costs and declining reimbursements, questions about productivity, quality of care, overuse, conflicts of interest, turf battles between various specialties and health care professions, intrusive and unhelpful electronic record systems, and decreasing time and commitment by practicing doctors to teach tomorrow’s doctors. Medical education shares these and has its own additional points of stress, controversy, and debate around such issues as the expanding role of online learning, focus on content versus individualized styles of learning, pressures to change the traditional “2 + 2” curriculum (two years of basic science and two years of clinical training), the need, role and emphasis placed on USMLE exams, the role of inter-professional education, the importance of continuity and the availability and skills of faculty in clinical settings, and the entry of a new “basic science” of health systems.
교육 문헌에는 교실-기반 기초 과학 교육(Hirsch and Ogur 2007)의 사일로에서 벗어날 필요성 및 임상 과학 변화와 더 많은 통합에 대한 불만이 가득하지만, 여전히 변화는 매우 느리다. [생명윤리, 웰니스/회복력 훈련, 사회적 결정 요인 및 건강 시스템 과학을 추가하라는 새로운 압력]은 현재 커리큘럼이 학생들에게 필요한 자료를 제공하고 그들이 배운 것을 유용하게 유지할 수 있는 방법에 대한 정밀한 조사scrutiny를 증가시킬 뿐이다. 의료 교육에서 임상 업무와 연구가 많은 학제 간 융합, 협업 및 학제 간 학습을 말하지만, 의과대학은 분열과 분리의 권력 구조를 유지하고 보상하는 "교실departments"라는 구시대적인 개념을 기반으로 사일로 속에 조직되어 있다. 학술의료센터AMC는, 다수의 그리고 종종 상충되는 인센티브의 세계에 살고 있기 때문에, 많은 문헌에서 요구되는 급진적인 변화에 관여하지engaged in 않았다. 아이러니하지만, 학술 의학에서 교육이 주된 사명이 되는 곳은 거의 없다.
While the education literature is rife with complaints about the need to get away from the silos of departmentally based basic science teaching (Hirsch and Ogur 2007) and the need to promote more integration with clinical science (Ioannidis et al. 2007; Frenk et al. 2010) change has been very slow. New pressures to add bioethics, wellness/resilience training, social determinants, and health systems science only increase scrutiny of whether the current curriculum presents material necessary to the students, and in a way that they can usefully retain what they learn. At a time when clinical work and research is heavily interdisciplinary in medical education we speak of integration, collaboration, and interdisciplinary learning but our schools are organized in silos based on outdated concepts of “departments” maintaining and rewarding power structures that divide and separate. Academic medical centers have not engaged in the radical change called for in so much of the literature (Frenk et al. 2010) because they are living in a world of multiple and often conflicting incentives. It is ironic, but almost nowhere in academic medicine is education the primary mission.
플렉스너의 도발적인 보고(1910년)에 따라 의학계는 [소규모의 독립적 견습생 기반 의과대학]에서 교수, 학습, 주택, 학사 학위 수여와 관련된 모든 물류를 제공할 수 있는 [대학에서 제공되는 과학 커리큘럼의 유럽 모델]로 옮겨갔다. 플렉스너는 "단순한" 실무의사가 아닌 [과학자인 교수진]을 명시적으로 옹호했다. 대학은 병원이나 의료 전달 시스템이 아니며, 공존할 때 자원, 권한, 임무 우선순위를 놓고 두 사람 사이에 경쟁이 벌어지는 경우가 많다. 실용적인 이유로, 우리 학술 병원은 급성 고강도의 치료를 제공하는 데 초점을 맞추고 있다. 이것이 마케팅, 자선사업, 연구뿐만 아니라 보상에 좋기 때문이다. 이러한 학술 병원에서 학생들은 보통 급성 문제에 초점을 맞춘 단일 학과 기반 팀(예: 내과 또는 외과)에 시간을 보내는 반면, 학생들은 퇴원 후 관리, 만성 질환, 예방 또는 환자 건강의 사회적 맥락에 대한 사전 예방적 관리에 거의 주의를 기울이지 않는다.
Following Flexner’s (1910) provocative report the medical community moved away from small, free-standing apprenticeship based medical schools toward a European model of scientific curriculum offered at a university which could provide all the logistics related to research, as well as teaching, learning, housing, and the awarding of academic degrees. Flexner explicitly advocated for faculty who were scientists, not “merely” practitioners. Universities are not hospitals or health care delivery systems, and when they co-exist there is often competition between the two over resources, authority, and mission priorities. For practical reasons, our academic hospitals are focused on providing acute high intensity care – after all that is the sweet spot for reimbursement, as well as marketing, philanthropy, and research. In these academic hospitals, students usually spend time on single discipline-based teams (e.g. internal medicine or surgery), focused on acute problems with little or no attention paid to management after discharge, proactive managing chronic disease, prevention, or the social context of patient wellness.
Academics에서는 발견discovery에 높은 가치를 둔다. 그리고 발견이란, "연구"의 성공이며, 이것은 환자나 인구 복지에 미치는 영향보다는 보조금, 출판물 및 인용 영향 요인에 의해 정의된다. Relman이 "의료-산업 복합체"(Relman 1980)라고 부른 것 내에서는
- 의료-산업 복합체에서 큰 가치가 부여되는 것은 다음과 같다: 기초과학 및 임상연구 활성화, 산업자금 지원, 이해충돌과 관계없이 특허와 파트너십을 통해 수익으로 이어지는 프로젝트.
- 반면 학생들을 [데이터 과학 및 성과 연구에 노출]시키고, [실무-기반 개선으로 이어질 수 있는 의료 시스템 과학]에 할애하는 시간과 리소스는 줄어든다. 이렇게 줄어드는 것에는 치료의 질, 의미 있는 환자 지향 결과, 기술 평가, 비용 효과, 리더십 또는 증거 기반 실무 지침 개발 등이 있다.
많은 학문적 환경은 후자의 활동이 합법적인 연구라고 거의 생각하지 않는다. [보건서비스 연구센터]가 있는 기관에서는 주로 의료 교육과정의 핵심이 아닌 독립비용센터로 연구가 운영되고 있다.
In academics a high value is place on discovery, with “research” success defined by grants, publications, and citation impact factors rather than on the impact on patient or population well-being. Within what Relman called “the medical-industrial complex” (Relman 1980)
- great value is placed on promoting basic science and clinical research, on industry funding, and on projects that lead to profit through patents and partnerships regardless of conflicts of interest (Angell 2000; Bekelman et al. 2003).
- Less time and resources are devoted to health systems science that would expose students to data science and outcomes research and lead to practice based improvements with a focus on quality of care, meaningful patient oriented outcomes, technology assessment, cost effectiveness, leadership, or the development of evidence-based practice guidelines.
Many academic environments barely consider such activities legitimate research. In institutions that have health services research centers, the research is largely run as an independent cost center that are not core to the medical curriculum.
미국 학술 의학에서 우리는 병원 환경에서 여러 세대의 의대 학생들을 훈련시켜 왔으며, 급성 질병에 초점을 맞추고, 종종 한 전문 분야가 다른 전문 분야와 경쟁하는 [학문분야-기반 사일로]에서 학습했습니다. 이곳은 대부분의 의사들이 결국 의료행위를 하는 곳이 아니다. 아레츠(2011)에 따르면, 우리에게 필요한 것은 적절한 장소에서, 적절한 제공자에 의해, 최고의 품질로 올바른 치료를 이끌기 위한 연구를 수행할 수 있는 새로운 세대의 의사들이다. 플렉스너는 의과대학이 인구나 그들이 앉아 있는 공동체의 건강에 대해 책임을 지라고 요구하지 않았지만, 규제 기준, 여론, 도덕적 책임은 적어도 이것에 대해 겸손한 주의를 기울이는 쪽으로 몰렸다. 실제로 미국에서 비과세 지위를 유지하기 위해서는 기관들이 상당한 '지역사회 혜택'을 제공해야 한다. 그러나 한두 개의 강의나 선택과목은 어떤 종류의 지역 사회 사명을 인정하겠지만, 이 임무 역시 핵심 커리큘럼에서 빠져 있다. 일부 학자들은 공동체의 건강에 기여할 뿐만 아니라 훈련생들이 공동체의 건강을 증진하는 데 필요한 분야에 진출하도록 자극하기 위해 [사회와의 묵시적인 '약속']이 있다고 믿는다. US News and World Reports와 같은 의대 순위는 [MCAT 및 Research 자금 지원]을 포함하지만, [지역사회 보건]이나 [학생 웰빙 또는 학생 성공]에 대한 척도는 없습니다(Report 2017).
In US academic medicine we have been training generations of medical students in a hospital environment, focused on acute illness, learning in disciplined based silo’s that often pit one specialty against another. This is not where most physicians will eventually practice. According to Aretz (2011), what we need are a new generation of doctors capable of doing research to drive the right treatments, at the right place, by the right providers, at the best quality. Flexner did not call on medical schools to be responsible for the health of populations or the communities in which they sit, and yet regulatory standards, public opinion, and moral responsibility have driven toward at least modest attention to this. Indeed, to maintain tax exempt status in the US, institutions are required to provide significant “community benefit”. But this mission, too, is missing from the core curriculum, although one or two lectures or electives will acknowledge some kind of community mission. Some scholars believe there is an implied “covenant” with society not only to contribute to the health of the community but to stimulate trainees to enter fields needed to promote health in communities (Coulter and Wilkes 1995). Medical school rankings such as the US News and World Reports count MCAT and Research funding but there is no measures of community health or for that matter student wellness or student success (Report 2017).
의학교육
Medical education
몇 세대 동안, 학부의학 교육, 졸업후의학 교육 및 지속적인 의학 교육 등 모든 수준의 의학 교육의 개혁이 필요하다고 경고해 왔다. 오늘날에는 목소리가 더 커지고(Cooke and Irby 2010), 필요성이 더 커지며(Macy 2008), 이전에는 볼 수 없었던 긴급성이 있습니다. 인구 통계는 극적으로 변화하고 있으며, 나이가 들수록 더 많은 수의 사람들이 더 활동적이고, 질병 부담이 증가하며, 더 많은 수의 사람들이 더 복잡한 치료를 필요로 한다. 65세 이상의 사람들의 수는 2030년까지 두 배가 될 것으로 예상되며 팔색조인은 가장 빠르게 성장하는 집단이다. 이것은 사회의 다른 부문들에 걸친 큰 건강 격차와 심지어 기본적인 건강 관리에 대한 접근성의 큰 차이로 인해 더욱 복잡해진다. 우리의 의료 시스템의 변화는 미래의 의사들이 다른 환경에서 일할 준비가 되어 있어야 한다는 것을 요구한다. 기술에 의한 우리 사회의 변혁은 2030년 의료의 실천이 오늘날과 전혀 다를 것이라는 것을 보장한다. 이러한 새로운 기술을 효율적이고 안전하게 사용해야 하는 필요성과 함께 의료 기술이 폭발적으로 성장하고 있습니다. 우리의 의료 시스템과 그 성장의 비용은 지속 가능하지 않다. 다음 세대의 의사들은 적절하고 필요한 치료를 제공함으로써 이러한 비용을 낮추고, 우리가 상상할 수 없는 도구와 소비자 관계를 통해 그렇게 해야 하는 도전을 받을 것이다. 우리는 미래의 의사들이 변화를 예측하고 수용하고 관리할 수 있도록 훈련시켜야 한다. 이를 위해서는 다른 환경에서, 종종 다른 교수진에 의해 다른 유형의 교육 모델, 다른 유형의 학습을 가져야 한다.
For generations (Frenk et al. 2010) sirens have warned of the need for reform of medical education at all levels – under graduate medical education, graduate medical education, and continuing medical education (Awasthi et al. 2005). Today the voices are louder (Cooke and Irby 2010), the need is greater (Macy 2008), and there is an urgency not seen before. Demographics are changing dramatically, with a larger number of people more active as they age, a greater number with an increased disease burden and more needing complex care. The numbers of people over 65 years of age are expected to double by 2030 and octogenarians are the fastest growing subgroup (Dall et al. 2013). This is complicated further by large health disparities across different sectors of society and large differences in access to even basic health care. The transformation of our health care system requires that tomorrow’s doctors must be prepared to work in different environments. The transformation of our society by technology guarantees that the practice of medicine in 2030 will be nothing like what it is today. There is the explosive growth in healthcare technology, with the need to use these new technologies efficiently and safely. The cost of our health care system and its growth is unsustainable. The next generation of physicians will be challenged to lower these cost by providing appropriate and necessary care, and to do so with tools and consumer relationships that we cannot imagine. We must train tomorrow’s doctors to anticipate, embrace, and manage change. To do this they must have a different type of educational model, a different type of learning, in different environments, often by different faculty.
교육과정에 새롭고 혁신적인 콘텐츠를 추가해야 한다는 요구 가운데 '인문주의, 공감, 대인관계 및 의사소통 능력'을 가르쳐야 한다는 요구도 있다. 이것 또한 대부분의 경우에 [높은 보상이나 보상을 받는 학술 영역이 아니기 때문에] 고통받고 있으며, 가르치는 임상의들은 환자 치료의 순간에 가장 원하는 속성을 발휘하기 어렵게 하는 바쁜 일정과 저글링 압력으로 우울증과 탈진증을 너무 자주 겪고 있다. 학생과 거주자 사이에서 우울증과 스트레스에 대한 관심이 높아짐에 따라, 이 과제를 해결하는 것은 [임상의가 실제로 진료을 즐기고 진정한 공감를 보여줄 수 있는 훈련 환경]을 찾는 것이 아니라, 이미 붐비는 커리큘럼(즉, 탄력성 훈련)에 추가하기 위한 추가 사항으로 간주되는 경우가 너무 많다. [휴머니즘에 대한 강의]는 아무리 잘해도 진짜 커리큘럼이 아니다; 학생들이 매일 진료실과 병동에서 경험하는 것은 진짜 커리큘럼이다.
Amidst the calls for adding new and innovative content to the curriculum is also a call to teach “humanism, empathy, and interpersonal and communication skills”. This too suffers as it is not a highly reimbursed or rewarded area of scholarship in most places, and clinicians who teach are too often themselves suffering from depression and burnout (Bunton et al. 2012), with rushed schedules and juggling pressures that make it difficult to exhibit the attributes most desired in the moment of patient care. As growing attention is paid now to depression and stress among students and residents, addressing this challenge is too often seen as one more additional thing to add to an already crowded curriculum (i.e. resilience training) rather than finding training environments where clinicians actually enjoy their practice and can demonstrate genuine empathy. A lecture on humanism – however well done – is not the real curriculum; what students experience every day in the clinic and on the wards is the real curriculum.
사회와 개인(졸업 당시 미국 의대 학생 평균 부채는 19만2000달러(AAMC 2017년)에 달하는 막대한 금액에도 불구하고, 우리의 노력은 여전히 부족하다. 의학 교육은 또한 그것이 어떻게 전달되는지에 대한 모델을 재고할 필요가 있다. 우리는 의학 학위 비용을 극적으로 줄이기 위해 기술과 혁신을 사용할 수 있어야 하며, 훨씬 더 다양한 그룹의 학생들이 이 교육을 더 쉽게 이용할 수 있도록 해야 한다. 미국은 우리가 지구상에서 가장 비싼 의료 시스템을 가지고 있다고 자랑할 수 있지만, 우리가 최고라고 주장할 수는 없다. 24개 이상의 국가의 의미 있는 건강 지표는 종종 실질적으로 우리의 건강 지표를 초과한다. 우리의 교육은 [서비스 남용의 원인이 되는 정확한 행동을 보상하는 환경]에서 교육생들에게 가르치고 있으며, 약간의 비용만으로도 가치가 입증된 예방과 같은 서비스를 과소평가하고 보상 시스템이 혜택을 거의 제공하지 않는 환경에 있다.
Despite the huge amount of money that society and individuals (average US medical student debt at graduation is $192,000 (AAMC 2017) expend on training doctors, our efforts are subpar. Medical education needs to also rethink the model of how it is delivered. We should be able to use technology and innovation to dramatically reduce the cost of the medical degree, making this education more accessible to a much more diverse group of students. The US can boast that we have the most expensive health care system on the planet but we cannot claim we have the best (Squires and Anderson 2015). Meaningful health indicators from more than two dozen nations exceed ours – often substantially (Squires and Anderson 2015). Our education teaches trainees in an environment where reimbursement systems reward the exact behaviors that contribute to overuse of services that offer little benefit and undervalues services such as prevention with proven value that may cost a fraction the price.
교육의 우선 순위
The priority of education
의학 교육에서 작은 변화가 기성 의과대학에서 자주 일어나고 있다. 확실히 소규모 그룹 교육, 새로운 종단적 입상실습, 고통스러울 정도로 느린 교육 기술 적응, 새로운 시뮬레이션 사용, 지원자를 보다 총체적으로 보려고 하는 의대 입학에 대한 새로운 접근법이 증가하고 있다. 미국에서는 지난 15년 정도 동안 기존 대학의 위신을 높이기 위해 12개 이상의 의과대학이 종종 신설되었습니다. 아마도 인증을 거부당하거나 동료들에 의해 심각하게 받아들여지지 않을까 하는 두려움 때문에, 이러한 새로운 학교들 중 진정으로 혁신적이고 전통적인 틀 밖에 서 있는 학교는 거의 없다. 오늘날 의과대학 지원자는 다양한 평판을 가진 학교에서 많은 선택권을 가지고 있지만, 교육의 우수성에 대한 척도에 대한 결정을 내릴 기회는 거의 없다. AMEE Aspire 상을 제외하고, 학생이 학교의 교육 혁신 수준, 학생 단체의 복지 또는 졸업생들의 질을 평가하는 데 사용할 수 있는 가이드는 거의 없습니다. 의과대학의 교육 프로그램에 대해 존재하는 정보는 종종 독점적이고 공개적이지 않다. 의과대학은 또한 학생들을 대상으로 한 마케팅에서 병원에서 제공되는 치료의 질에 대한 정보를 홍보하는 경우가 거의 없는데, 마치 그것이 커리큘럼과 관련이 있는 것이 아니라 잠재적 환자들에게만 해당되는 것처럼 말이다.
In medical education small changes are occurring often at establishment medical schools. Certainly there is a growth in small group teaching, new longitudinal clinical clerkships, the painfully slow adaption of educational technology, new uses of simulation, and new approaches to medical school admission that seek to look more holistically at the applicant. In the US, over the past 15 or so years, more than a dozen new medical schools have been created often to augment the prestige of an existing university. Perhaps out of fear of being denied accreditation or not being taken seriously by peers, few of these new schools are truly innovative and stand outside the traditional mold. An applicant to medical school today has many choices in schools with varying reputations, but little opportunity to base their decision on measures of educational excellence. With the exception of the AMEE Aspire award, there are few guides that a student can use to assess a school’s level of educational innovation, the wellbeing of the student body, or the quality of its graduates (https://amee.org/awards-prizes/aspire-award). What information does exist about medical school’s educational programs is often proprietary and not public. Medical schools also rarely promote information about the quality of care delivered at their hospitals in their marketing to students, as if that is not relevant to the curriculum but rather only to potential patients.
지난 한 세기 동안 많은 학교들이 학문분야-기반 커리큘럼에서 장기계통-기반 커리큘럼으로, 문제 또는 사례 기반 커리큘럼으로 발전했다. 그러나 의대는 성과와 시스템 기반 교육을 향한 여정을 이제 막 시작하고 있다. 여전히, 대부분의 면에서 2018년 훈련은 1988년과 비슷해 보인다. 학생들은 여전히 세 가지 R(읽기, 기억, 역류)에 집중해야 한다. 의사는 여전히 배의 선장이며, 임상 치료는 견습에 기반을 두고 있으며, 의사는 결과나 인구 건강보다는 그들이 하는 일에 따라 많은 보상을 받는다. 임상 실습은 "빅6" 분야(소아내과, 내과, 외과, 산부인과/산부인과, 정신의학과, 가정의학과)에 의해 지배되며, 따라서 우리는 학생들을 협업 의료 실습의 더 넓은 잠재적 영역과 새로운 분야에 노출시키지 못한다. 임상에서 학습에 대한 지배적인 접근법은 [견습 모델]이다. 우리의 임상 교수진은 "교사"로 불리지만, [교육 원리, 예상 역량, 평가 및 피드백, 또는 전체 의과대학 커리큘럼의 내용 또는 기본 철학]을 알고 있는 훈련된 교육자는 거의 없습니다.
Over the past century a number of schools have evolved from a science discipline-based curriculum, to organ-based curriculum to problem- or case-based curriculum. However, medical school are just beginning their journey toward outcomes and systems based education (Frenk et al. 2010). Still, in most ways training in 2018 looks much as it did in 1988. Students are still expected to focus on the three Rs (reading, remembering, and regurgitating). The physician is still the captain of the ship, clinical care is apprenticeship based, and physicians are heavily reimbursed based on what they do rather than on outcomes or the health a population. The clinical years are dominated by the “big six” disciplines (pediatrics, internal medicine, surgery, obstetrics/gynecology, psychiatry, and family medicine) and thus we fail to expose students to the broader potential areas of collaborative medical practice and to emerging disciplines. In the clinical years the dominate approach to learning is the apprenticeship model. Our clinical faculty are deputized as “teachers” but few are trained educators such that they are aware of educational principles, expected competencies, the skills of evaluation, and feedback, or the content or underlying philosophy of the overall medical school curriculum.
학술 의료 센터
The academic medical center
"교육 병원"의 개념은 적어도 1000년 전으로 거슬러 올라간다. 오늘날 우리는 "학술 의학"이 무엇을 의미하는지, 그리고 학술의료센터(AMC)가 무엇인지 물어보는 것이 타당하다. [학술 의학의 사회적 정의]는 공중의 건강을 증진시키는 것을 목표로 생각하고, 계획하고, 연구하고, 연구하고, 평가하고, 발견하고, 혁신하고, 가르치고, 배우는 의료 시스템의 능력을 포함할 것이다. [AMC에 의해 정의된 사명]과 [환자와 지역사회가 기대하는 사명] 사이에는 종종 불일치가 있다. 국제공동위원회(Joint Commission International)는 학술 의료센터를 의과대학과 행정적으로 통합되고 의과대학생 교육의 주요 현장이며 임상연구에 종사하고 있기 때문에 보다 실용적이다(JCI 2017). Academic centers 내에서는 학술원이 nonacademic centers보다 더 높은 수준의 의료 서비스를 제공한다는 암묵적인 가정이 있다. 그러나 학계에서는 전문화된 3차 진료, 고비용 진료 및 비병원 진료와 통합되지 않는 진료에 초점을 맞추고 있다. 학술 의학은 급성 3차 및 4차 치료에 중점을 두고 있지만, 재활, 만성 치료, 1차 치료, 건강, 예방 및 유지와 같은 분야에서 낮은 우선순위가 부여된다.
The concept of the “teaching hospital” dates back at least 1000 years (Aretz 2011). It is fair to ask today what do we mean by “academic medicine” and what is an academic medical center (AMC)? A social definition of academic medicine would include the ability of a health care system to think, plan, study, research, evaluate, discover, innovate, teach, and learn all with the goal of improving the health of the public. There is often a mismatch between the mission defined by the AMC and those expected by patients and communities. The Joint Commission International is more pragmatic as it defines an academic medical center as one that is administratively integrated with a medical school, is the principal site for the education of medical students, and is engaged in clinical research (JCI 2017). Within academic centers there is an unspoken assumption that academic centers also provide higher quality care than nonacademic centers. But academia also connotes a focus on specialized tertiary care, high cost care, and care that is often not integrated with non-hospital care (Cassel and Wilkes 2017). While academic medicine focuses on acute tertiary and quaternary care, there are areas such as rehabilitation, chronic care, primary care, wellness, prevention, and maintenance that are given low priority.
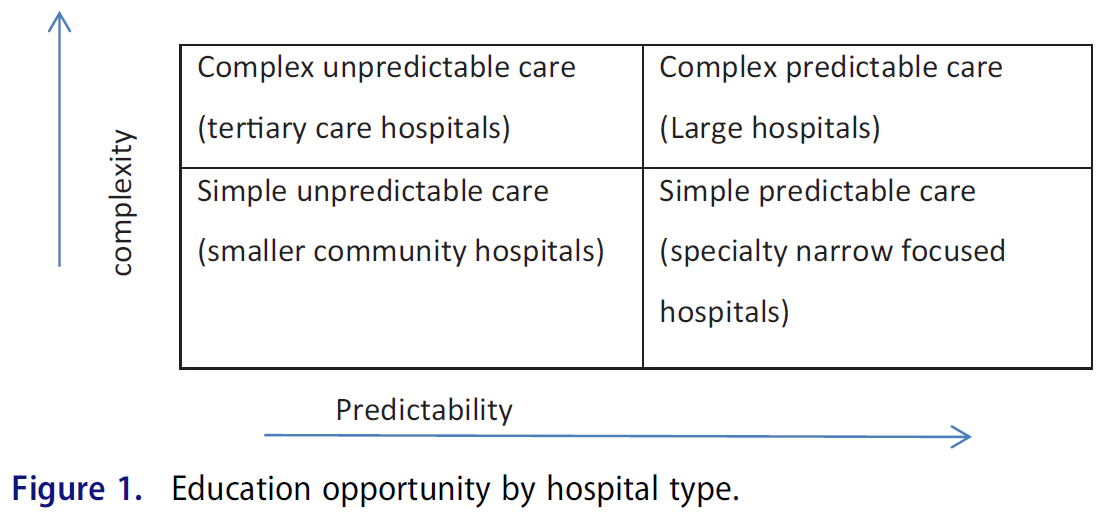
아레츠(개인 커뮤니케이션)는 [두 개의 연속체(예측가능성과 복잡성)]를 기반으로 의료의 4개 사분면(그림 1)을 설명한다. 통합 의료 시스템은 반드시 동일한 지리적 위치에 있는 것은 아니지만 이러한 각 영역에서 치료를 제공할 수 있다.
Aretz (personal communication) describes four quadrants (Figure 1) of health care based along two continua (predictability and complexity). An integrated health care system is capable of providing care in each of these areas although not necessarily at the same geographic location.
이러한 통합 시스템에서의 훈련은 많은 이점을 제공한다. 정보 기술 자원 저장소(Stuart and Triola 2015)가 점점 커지고 있기 때문에 교육적 관점에서 볼 때 더 이상 수십 개의 학과와 대규모 기초 과학 교수진이 있는 의대를 둘 필요가 없습니다. 사회가 필요로 하는 맥락에서 대학, 병원, 그리고 미래의 건강 제공자들의 훈련을 조사하는 새로운 표준이 필요하다. 정규 교육과정은 학생들이 무엇을 가르치고 전문적인 실습이 어떻게 모델링되고 강화되는지에 일관성이 있도록 비공식적인 숨겨진 교육과정과 동기화될 필요가 있다. 우리의 현재 시스템에서, 학생들은 신중하고 종종 (의식적인 고려 없이) 단순히 평가 연습에서 덜 가치가 있는 자료를 무시하면서 전략적으로 학습한다. 이와 같이 [윤리, 인구 의학, 의사소통 기술, 품질 향상, 전문직 간 협업, 임상 추론과 같은 내용]은 평가 점수에 작은 비율만 기여하므로 종종 학생들의 평가를 준비하는 집중 학습 자료로 무시된다.
Training in such an integrated system provides numerous advantages. Given the growing repository of information technology resources (Stuart and Triola 2015), from an educational perspective it is no longer necessary to have medical schools with dozens of departments and a large basic science faculty. There is a need for a new normal that examines the role of the university, the hospital, and the training of tomorrow’s health providers in the context of society’s needs. The formal curriculum needs to synchronize with the informal hidden curriculum (Hafferty 1998) so that there is consistency in what the students are taught and how professional practice is modeled and reinforced. In our current system, students are prudent and learn strategically, often (without conscious consideration) neglecting material that is simply worth less on assessment exercises. As such, content such as ethics, population medicine, communication skills, quality improvement, inter-professional collaboration, and clinical reasoning contribute only a small percentage to assessment scores and are thus often ignored as student focus learning material that will prepare them for their assessment.
"학술적"의 재정의
Redefining “academic”
미래의 의사를 훈련시키는 것은 올바른 내용, 올바른 교사, 올바른 환경을 올바른 학생들에게 제공해야 합니다. 하버드 경영학 교수인 Christensen은 ["파괴"]를 [시장을 크게 변화시키는, 덜 비싸고 더 효율적인 프로세스를 허용하는 새로운 접근법]으로 정의한다. 철강 제조, 휴대폰 또는 자동차 조립의 경우, 파괴의 이점이 분명했다. 그러나 의료 교육의 경우, 우리의 시스템(공장)은 노동력에 필요한 제품(공급자)을 생산하지 못하고 있습니다. 우리가 모래 속에 머리를 파묻고 있다면, 종국에는 [다른 사람들이 우리에게 변화를 강요]하거나, [다른 전문직들이 개입하여 새로운 역할을 맡길 것]이다. 또는, 우리는 (자발적으로) 새로운 교육 모델을 살펴볼 수 있습니다. 우리가 캔자스에서 활강 스키어들을 훈련시키는 것을 선택하지 않을 것처럼, 대학에서 의사들을 훈련시키는 것이 타당한지 생각해 볼 때이다. 환자, 다양한 지역사회, 의료 제공자, 지불자 및 의대 지원자를 포함한 이해관계자가 미래의 의사를 정의하는 고품질 전달 시스템에서 교육과 훈련을 연결하는 새로운 방법이 있는가?
Training tomorrow’s doctor’s needs to provide the right content, the right teachers, and the right environment, to the right students. Christensen, a Harvard Business Professor, defines “disruption” as a new approach that allows for less expensive and more efficient processes that significantly alter the market (Christensen 1997). In the case of steel manufacturing, cell phones, or automobile assembly the benefits of disruption have been clear. But in the case of medical education our system (factories) is not producing the products (providers) we need in the workforce. We can keep our heads in the sand and eventually either others will force change upon us or other professions will step in and assume new roles. Or, we can look at new models of education. Just as we would not opt to train downhill skiers in Kansas (sorry Kansas), it is time to think about whether training doctors in universities makes sense. Are there new ways of connecting education and training with the delivery of care in high quality delivery systems that engage stakeholders including patients, diverse communities, health care providers, payers, and medical school applicants in defining tomorrow’s doctors?
두 시스템(교육 및 의료)이 각각 최고의 의사 교육에 대한 강력한 기득권을 가지고 상호 작용하는 의료 제공 환경입니다. 고용주만이 잘 훈련된 인력 개발에 강한 관심을 가지고 있는 것은 아니다(그림 2).
It is in the health care delivery environment where the two systems (education and health care) interface each with a strong vested interest in the training the very best physicians. Employers are not the only ones with a strong interest in the development of a well trained workforce (Figure 2).

의료 시스템에 내장된 의과대학
A medical school embedded in a health care system
[카이저 퍼머넌트(KP)]가 국내 최고 기능 통합 건강 전달 시스템에 내장된 학습 실험실로 의대를 만들어 의료 분야에서 국가적 과제를 해결하고 의료 교육을 구체화하고자 하는 것도 이러한 맥락에서다. 학교의 궁극적인 목표는 KP를 위한 노동력을 훈련시키는 것이 아니라, KP 의료 제공의 성공을 활용하여 다음의 맥락에서 건강과 예방에 대한 헌신으로 새로운 훈련 모델을 개발하는 것이다.
- 의료 격차 완화,
- 증거 기반 관행의 개발 및 사용을 통한 의료 품질 개선
- 다양성과 포용성의 증가,
- 웰니스와 탄력성을 중시하고 강화하는 시스템 전반의 문화
It is in this context that Kaiser Permanente (KP) seeks to address national challenges in health care and shape medical education by creating a medical school as a learning laboratory embedded in one the nation’s highest functioning integrated health delivery system. The ultimate goal of the school is not to train a workforce for KP, but to leverage the success of KP health care delivery to develop new models of training with a commitment to health and prevention in the context of
- reducing health care disparities,
- improving health care quality through the development and use of evidence-based practice,
- increasing diversity and inclusion, and
- promoting a system wide culture that values and reinforces wellness and resilience.
KP는 건강플랜, 병원 및 기타 요양시설 시스템, 다중 전문 의료단체가 결합된 [미국에서 가장 큰 민간 통합 전달 시스템]이다. 급여 및 의료 제공 인센티브를 급여를 받는 의사와 연계하고, 시스템 기반 관행 및 예방에 중점과 연계함으로써, KP는 거의 모든 공개 신고 및 인증 시스템에서 높은 성과 점수를 획득할 수 있었으며, 지불 개혁과 품질 공개 보고를 통해 전달 시스템 전환의 모델이 되었습니다.
KP is the largest private integrated delivery system in the USA combining a health plan, a system of hospitals and other care facilities, and multi-specialty medical groups. With payment and health care delivery incentives aligned, with salaried physicians, and with a strong emphasis on system based practices and prevention KP has been able to achieve high performance scores on almost every public reporting and accreditation system (Leapfrog 2016; Quality 2016) and has become a model for delivery system transformation through payment reform and public reporting of quality.
KP는 의학 교육에서 새로운 것이 아니다; 그들은 현재 각각 30개 이상의 전문 분야에서 50개의 부속 대학 프로그램에서 900명 이상의 학생들을 훈련시키고 있다. 그러나, 이 교육생들은 다른 학교에서 온 방문객들이며, 제한된 기간 동안 KP에 있고 각각의 가정 기관에 책임을 지고 있기 때문에 혁신적인 교육을 어렵게 만들고 있다. 디스커버리호는 또한 연방 연구 자금 1억 달러, 1300개의 클리닉 추적, 3900만 달러의 KP 자금 지원 건강 결과 연구 및 140명의 상근 연구팀으로 구성된 KP 임무에 매우 중요하다. 임상 분야에서 KP 시스템은 단일 자금 출처, 글로벌 예산 및 서비스를 받는 인구의 건강으로 측정되는 궁극적인 책임을 가진 미니 국가 보건 시스템처럼 기능한다. KP는 보다 적극적인 치료로부터 이익을 얻기보다는 오히려 그 반대로 이익을 얻는다. 즉, 환자가 건강해질수록 환자와 시스템 모두에 더 많은 이점이 있다. 전문가들은 기업을 주도하지 않으며, 오히려 1차 진료와 특수 치료는 의료 팀의 일부로 기능하는 동등한 파트너입니다. 돌봄은 가정, 제공자 사무실, 병원, 숙련된 간호 시설(일명 "요양원") 및 호스피스로부터 연속해서 이루어진다. 마찬가지로, [질병disease뿐만 아니라 질환illness에도 초점을 맞추고 있다는 것]은, [1차 및 2차 예방, 진단, 치료, 만성 상태 관리 및 사후 관리, 지원 치료 및 완화 치료에 중점을 두고 있다는 것]을 의미한다. 환자 중심 치료는 시간이 지남에 따라 소규모 자발적 해약(연간 2% 미만)이 주어지면 긴 시간 범위와 통합된다.
KP is not new in medical education; they currently train over 900 students from 50 affiliated university programs each in more than 30 specialties. However, these trainees are visitors from different schools, at KP for limited period and each responsible to their home institution thus making innovative education difficult. Discovery is also crucial to the KP mission with over $100 million in federal research funding, 1300 clinic trails, $39 million in KP funded health outcomes research, and a team of 140 full time researchers (Kaiser-Permanente 2017). In the clinical arena, the KP system functions like a mini national health system with a single source of funding, a global budget, and the ultimate accountability measured by the health of the population served. Rather than profiting from more aggressive care, KP benefits from the reverse – the healthier it can keeps patients the more advantages there are to both patients and the system. The specialists do not drive the enterprise, rather primary care and specialty care are equal partners that function as part of care teams. Care covers a continuum from home, provider offices, hospital, skilled nursing facilities (aka “nursing homes”), and hospice. Similarly, the focus is not only on disease but on illnesses meaning that emphasis is placed on primary and secondary prevention, diagnosis, treatment, chronic condition management and follow-up, supportive care, and palliative care. Patient-centered care is integrated over time with a long time horizon given a small voluntary disenrollment (<2% per annum).
차별화 특성
Differentiating characteristics
의과대학은 기존 의과대학과는 크게 다를 것이다. 왜냐하면, KP의 차별화된 특성을 활용하여 사회적 사명을 지닌 예방 중심의 인구 기반 통합 돌봄 전달 모델로 활용하고, 이를 필요로 하는 회원들을 위한 세계적 수준의 전문 돌봄이 가능할 것이기 때문이다.
The School will be significantly different from traditional medical schools leveraging KP’s differentiating characteristics as a prevention-focused, population-based integrated care delivery model with a social mission, capable of world-class specialty care for the members who need it.
학교의 가장 중요한 차별화 요소는 카이저 퍼머넌트 메디컬 케어 프로그램의 일부가 된다는 것입니다. 카이저는 인구의 총체적 건강에 초점을 맞춘 치료와 자금 조달의 통합 모델입니다. Permanente Medicine으로 알려진 치료 모델은 증거 기반, 팀 제공, 기술 지원 및 문화적으로 책임 있는 것으로 가장 잘 특징지어집니다. 이러한 차이는 임상 치료, 교육, 연구/발견 및 사회적 사명으로 구분된다. 커뮤니티 건강, 발견 및 혁신, 다양성과 포용, 웰빙 등 여러 주제가 네 가지 영역에 모두 포함되어 있습니다.
The School’s most important differentiator is that it will be part of the Kaiser Permanente Medical Care Program, an integrated model of care and financing focused on the total health of populations. The model of care, known as Permanente Medicine best characterized as evidence-based, team delivered, technology enabled, and culturally responsible. These difference are broken down into clinical care, education, research/discovery, and social mission. Several themes – community health, discovery and innovation, diversity and inclusion, and wellness – are embedded in all four areas.
[다양성 채용 어젠다]는 의대 발전의 핵심 고려 사항이 될 것이다. KP의 현재 강력한 국가 프로그램을 기반으로, 건강 격차를 해결하고 특수 모집단에 관심이 있는 예비 학생들에게 독특한 임상 학습 기회를 제공할 것이다.
The diversity recruitment agenda will be a key consideration in the development of the medical school, building on KP’s current robust national programs that address health disparities and offer unique clinical learning opportunities for prospective students interested in special populations.
모든 미국의 의과대학과 마찬가지로 KP 의과대학은 오늘날 의과대학에서 대표성이 낮고 사회경제적으로 불리한 학생들을 포함하여 다양하고 포괄적인 학생 단체를 모집하는 데 상당한 도전에 직면할 것이다. 이 미션 크리티컬 다양성 목표를 달성하기 위해 학교는 KP가 다양한 인력을 창출하는 데 사용한 많은 측면을 활용할 필요가 있습니다.
Like all US medical schools, a KP medical school will face a significant challenge in recruiting a diverse and inclusive student body, including the underrepresented and socioeconomically disadvantaged students in medical schools today. To achieve this mission-critical diversity goal, the School will need to leverage many aspects that KP has used to create a diverse workforce.
많은 면에서 국가의 요구는 예방과 환자 권한 부여, 만성 질환의 효과적인 관리, 소득 극대화보다는 임상 증거와 환자에 중점을 두는 것, 통합 팀 간의 진료 조정, 보건 서비스 연구 등 KP가 뛰어난 동일한 분야이다.
In many ways, the needs of the nation are the same areas where KP excels, such as the emphasis placed on prevention and patient empowerment, effective management of chronic conditions, a focus on clinical evidence and the patient rather than on maximizing income, care coordination across an integrated team, and health services research.
올바른 내용, 올바른 교사, 올바른 환경을 파악하고 올바른 학생을 선발하는 것은 쉽지 않지만 우리가 수년간 academic center에서 배운 것이 있기에 가능하다. 환자, 직원 및 교수진과의 의미 있는 종단적 연결은 내일을 위한 리더를 훈련하는 데 매우 중요합니다. 교수진이 교수 전문성과 효과성을 가르칠 수 있는 시간을 제공하고, 급여를 지급하며, 지속적인 교수 개발을 제공하여 학습 커뮤니티를 최적화하고자 합니다.
Identifying the right content, the right teachers, and the right environment, and selecting the right students is not easy but is possible because of what we have learned from academic centers over the years. Meaningful longitudinal connections with patients, staff, and faculty are crucial to training leaders for tomorrow. By identifying unique approaches to student learning where faculty are provided time to teach, paid, and academically recognized for their teaching expertise and effectiveness, and provided ongoing faculty development to augment their skills we seek to optimize our learning community.
Academic medical centers는 전통적으로 환자와 지역 사회의 요구보다는 개별 교수진과 대학의 연구 요구를 충족시켜 왔다. KP는 현재 1,100만 명의 모든 회원에 대한 데이터를 제공하는 단일 전자 의료 기록에 초기에 투자하여 의료가 제공되는 모든 영역에서 유사한 환자 그룹에 걸친 의료 제공자 및 의료 품질에 대한 비교 데이터를 허용한다. 환자는 자신의 의료 정보에 대한 온라인 액세스, 예약 및 예약 변경, 담당 간호사나 의사에게 이메일 문의 전송, 특정 조건에 대한 건강 정보 및 코칭 등을 통해 권한을 부여받는다.
Academic medical centers have traditionally served the research needs of individual faculty and the University rather than the needs of patients and local communities. KP invested early in a single electronic medical record that now supplies data on all 11 million members, allowing comparative data on providers and quality of care across similar groups of patients in all arenas where care is delivered. Patients are empowered through access on-line to their own medical information, and to scheduling and changing appointment, sending email queries to their practice nurse or physicians, and receiving health information and coaching for specific conditions.
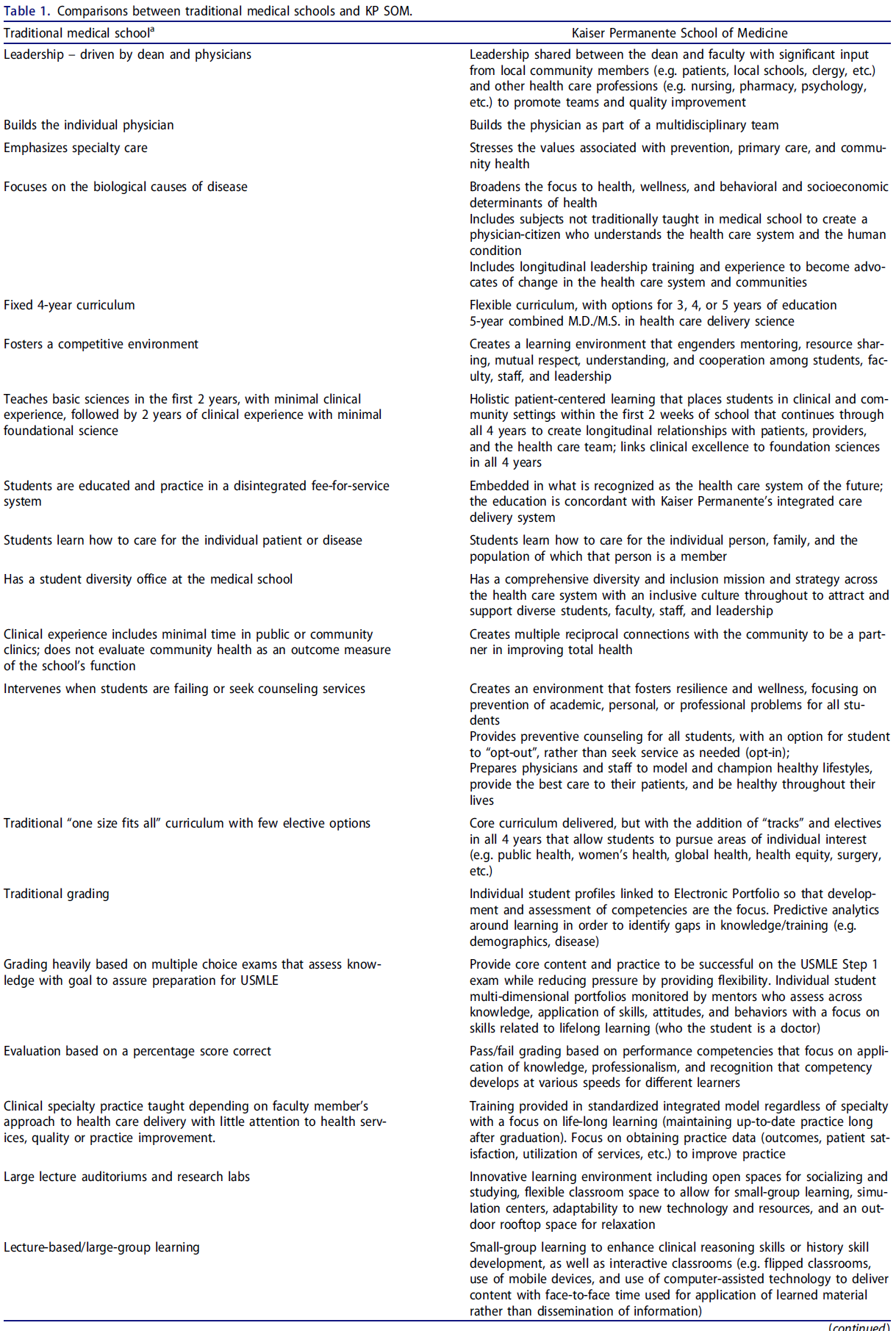
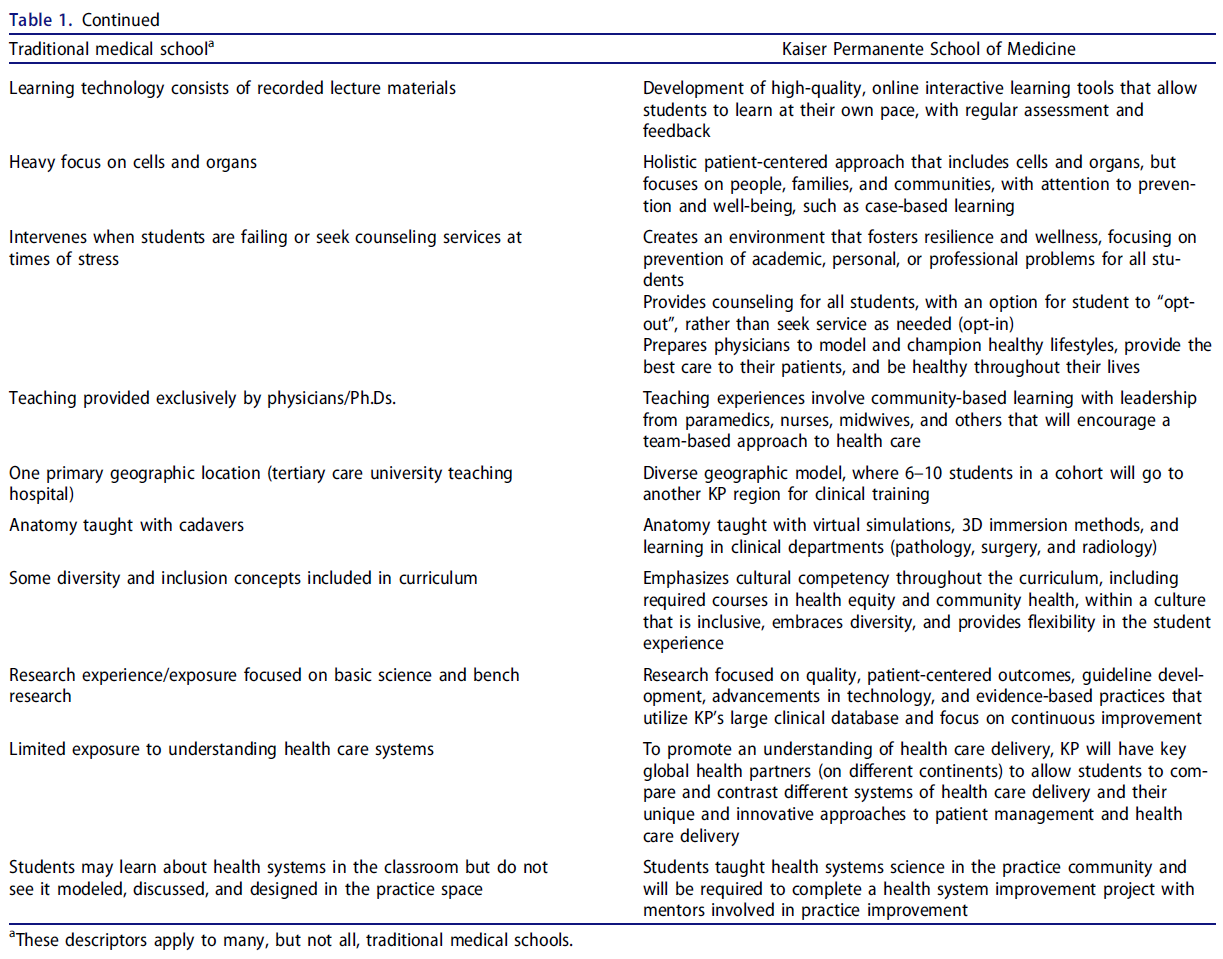
KP에서의 임무는 전통적인 학술 의과대학의 임무와 다르다(표 1). 학술 보건 센터는 두 축을 따라 네 개의 사분면(그림 2)으로 정렬하는 것처럼 보입니다.
The mission at KP is different from that of a traditional academic medical school (Table 1). Academic health centers seem to align themselves into four quadrants (Figure 2) along two axes.
Y축에는 사회적 사명 → 재정적 성공/성공에 대한 집중이 있습니다. x축에는 혁신적인 임상 실습과 제공 → 과학적 연구에 대한 헌신의 연속체가 있습니다. 완전히 사분면에 속하는 학교는 없지만, KPSOM은 사회적 임무와 임상 실습(사분면 1)에 더 중점을 두고 있다.
On the y-axis is a continuum from commitment to social mission → focus on financial success/prestige. On the x-axis is a continuum from commitment to innovative clinical practice and delivery → commitment to scientific research. While no school sits entirely within on quadrant, KPSOM is more focused on the social mission and clinical practice (quadrant 1).
의과대학의 스트레스는 4년 중 어느 시점에 학생들의 4분의 1이 심각한 우울증을 포함하여 정서적 행복의 감소를 초래하는 것으로 잘 입증되었다. 그 중 일부는 웰빙과 자존감을 손상시키고 회복력에 기여하지 않는 학습 환경 때문이다. 여기에다 자신들도 지쳐 있고 환경이 건강한 일과 삶의 균형에 도움이 되지 않는 교수진을 추가한다. KPSOM은 오랫동안 웰빙을 노동력으로 삼아온 인프라 지원과 리더십을 제공하는 시스템으로 소모가 적은 거대 퍼머넌트 의료단(2만2,000명 이상 의사)에서 선발해 업무에서 기쁨을 전하는 내과 교직원을 선발할 계획이다.
The stresses of medical school have been well documented to produce declines in emotional well-being, including serious depression among a quarter of students at some point in their four years (Dyrbye et al. 2010). Some of this is because of learning environments that impair wellbeing and self-esteem and do not contribute to resiliency (Cassel and Wilkes 2017). Add to this a faculty who are themselves burned out and the environment is not conducive to healthy work-life balance. KPSOM plans to select physician faculty who convey joy in their work, selected from the enormous Permanente medical group (more than 22,000 physicians) where burnout is lower as a result of a system that provides infrastructure support and leadership that has long made wellness a workforce a priority.
결론들
Conclusions
우리는 차세대 의사들을 훈련시키기 위한 이상적인 모델이 서비스되는 지역사회의 건강에 의해 결과가 정의되는 고기능 통합 의료 제공 시스템 내에 있다고 믿는다. 의대 설립 결정은 전통적인 학문적 의학 교육과 훈련이 의사가 트리플 목표(더 나은 의료, 더 건강한 인구, 더 현명한 지출)를 달성하기 위해 연습할 준비를 하지 못한다는 인식에서 영감을 받았다. KPSOM의 목표는 다른 의료 교육 기관들이 그들의 방법과 커리큘럼을 개선하고 강화하도록 고무시키는 촉매제 역할을 하는 것이다.
We believe an ideal model for training the next generation of physicians is within a high functioning, integrated health care delivery system where outcomes are defined by the health of the community served. The decision to initiate a medical school was inspired by the perception that traditional academic medical education and training does not prepare physicians to practice toward achieving the Triple Aim (better health care, healthier populations, and smarter spending). The goal at KPSOM is to act as a catalyst to inspire other medical education institutions to refine and strengthen their methods and curricula.
If we keep doing what we're doing we'll keep getting what we're getting: A need to rethink "academic" medicine
PMID: 29320901
Abstract
Purpose: For generations there have been warnings of the need to reform medical education at all levels. Today the voices pushing reform are louder, the need is greater, and there is an urgency not seen before. Approaches that have worked in the past to train physicians are no longer as relevant today as demographics, disease patterns, human resources, practice behaviors, technology, and attention to costs demand new collaborative approaches to clinical practice. To prepare for this practice tomorrow's doctors will need a different type of educational model, a different type of learning, in different environments, often taught by different faculty. This paper provides one innovative approach to redefine "academic medicine".
Methods: After reviewing current trends in medical education, this paper describes one approach being taken by a large nonprofit American health care system to move medical education and discovery (research) out of traditional academic universities and placing it within a health care delivery system.
Conclusions: The creation of a learning laboratory in a high functioning health care delivery system allows for leveraging the successes in quality health care delivery to transform medical education with a focus on prevention, improving health care quality, reducing disparities in health, and promoting practical evidence-based clinical and outcomes focused research.
'Articles (Medical Education) > 대학의학, 조직, 리더십' 카테고리의 다른 글
| 성과를 내는 리더십 (0) | 2022.10.11 |
|---|---|
| 리더를 만드는 것은 무엇인가? (0) | 2022.10.11 |
| 학부의학교육에 CBME와 개별화된 경로를 도입할 때 인프라와 조직문화의 결정적 역할(Med Teach, 2021) (0) | 2022.09.07 |
| 의학교육에서 사회적 정의: 포용으로는 충분하지 않다, 단지 첫 걸음일 뿐이다(Perspect Med Educ. 2022) (0) | 2022.08.31 |
| 어떻게 의학교육이 건강 형평성을 후퇴시키는가 (Lancet, 2022) (0) | 2022.08.31 |