중국의 2021년 의료전문직 면허법 수정: 코멘터리(Health Syst Reform. 2022)
Amending the Law for Licensing Medical Practitioners of China in 2021: A Commentary
Chengxiang Tanga,b, Jiayi Jiangb,c, Yuanyuan Gua, and Gordon Liub
소개
Introduction
다양한 의료 서비스 제공자 중 의사는 의료 시장에서 가장 중요한 부분을 차지하고 있으며, 의사의 자질은 의료 시스템에서 결정적인 역할을 합니다. 의사 면허 시험은 의사의 질과 그에 따른 의료 서비스를 보장하는 데 매우 중요한 의미를 갖습니다. 1950년대 이후 중국 의료 시스템의 주요 임무는 절박한 의료 인력 부족 문제를 해결하고 증가하는 의료 수요를 충족하는 것이었습니다.1 이 문제를 해결하기 위해 중국은 의사를 양성하기 위해 다단계 의학교육 시스템을 도입했고, 그 결과 일부 현직 의사들은 3차 학위 중심의 의학교육을 받지 못했습니다.2
Among the various health service providers, physicians are the most important part of the health care market, and their quality plays a determining role in the health system. The licensing examination for medical practitioners is of great significance to guarantee the quality of physicians and consequent health care services. Since the 1950s, the primary job of the health care system in China is to address a desperate shortage in the health workforce and satisfy the increasing demand for health care.1 To address this problem, China adopted a multi-tiered medical education system to train doctors, which resulted in a part of the practicing physicians receiving no tertiary degree-oriented medical education.2
의학교육 개혁의 발전과 함께 중국은 1999년에 처음으로 개업의에 관한 법률을 제정하여 중등직업학위(SVD)을 가진 '의대생'만이 의사 자격시험에 응시하여 개업의가 될 수 있도록 허용했습니다. 2002년 기준으로 중국에서는 개업 의사의 41%가 SVD만 가지고 있었습니다.
With the development of medical education reform, China enacted its first Law for Practicing Medical Practitioners since 1999, which allowed “medical students” with only a secondary vocational diploma (SVD) to take the medical examination and therefore become practicing physicians. As of 2002, 41% of practicing physicians only had an SVD in China.
2021년 1월, 전국인민대표대회 상무위원회는 의사의 질과 의료 시장의 형평성을 개선하기 위해 1999년 시행 이후 처음으로 '의료인 면허법'을 개정했습니다. 주요 개정 내용은 다음과 같습니다:
- (1) 전문직 규제에 관한 다른 법률과의 일관성을 유지하기 위해 현행 "개업의사"라는 명칭을 "의사"로 단순 대체합니다.
- (2) 개정안은 의사의 의무와 의무, 의사의 법적 권리 및 보수를 더욱 명확히 규정합니다. 개정안은 또한 의료 시설과 시장을 교란하는 행위에 대한 형사 책임을 규정하고 있습니다.
- (3) 면허시험의 최소 학력 수준을 종전의 중등 전문학사 학위에서 개정안에서는 전문학사 또는 전문대졸 수준으로 재설정합니다. 또한 개정안은 시험 등록에 관한 사항을 개선합니다.
- (4) 1차 의료 제공자, 특히 일반의에 대한 교육이 강화됩니다.
- (5) 개정안에는 SARS-COV-19의 예방 및 통제 전략에 대한 교훈과 경험이 포함됩니다.
In January 2021, the Committee meeting of the National People’s Congress amended the “The Law for Licensing Medical Practitioner” for the first time since its implementation in 1999, aiming to improve the quality of physicians and equity in the health care market. The major amendments include:
- (1) In order to be consistent with other legislations on professional regulation, the current title “Practicing Physician” is simply replaced by “Physician.”
- (2) The amendments further clarify the physicians’ duties and obligations, as well as the legal rights and remuneration of physicians. The amendments also stipulate the criminal liability for disrupting health care facility and the market.
- (3) The minimum education-level of the licensing examination is re-set to a vocational diploma or junior college level in the amendment, rather than a secondary vocational diploma previously. In addition, the amendments make improvements on the registration of the examination.
- (4) The training of primary care providers, in particular the general practitioners, will be strengthened.
- (5) The amendments include the lessons and experiences of the prevention and controlling strategy of SARS-COV-19.
우리는 의사 자격 면허 시험의 최소 교육 수준을 학사 학위로 설정해야한다고 생각하는 것을 제외하고는 이러한 개정안을지지합니다. 다음 섹션에서는 먼저 중국 보건통계연감의 데이터를 기반으로 중국 내 의사들의 교육 수준 구조와 분포를 제시합니다. 그런 다음 의사 자격 시험의 문턱을 학사 수준으로 설정해야 하는 여러 가지 이유를 설명합니다.3
We endorse these amendments except that we believe the minimum education-level of the licensing examination of physicians’ qualifications should be set to a bachelor degree. In the following sections, we first present the structure and distribution of practicing physicians’ educational level in China based on the data from the Health Statistical Yearbook of China. We then give a number of reasons to explain why the threshold for the physician qualification examination should be set at the bachelor level.3
의사 의학교육의 구조와 분포
The Structure and Distribution of Physicians’ Medical Education
다단계 의학교육 체계에서 비롯된 현재의 의학교육 의사 구성은 보건의료체계의 질적 발전을 저해할 것입니다. 그림 1은 2002년부터 2019년까지 중국 내 의사 교육 분포의 연도별 변화를 보여줍니다. 일반적으로 학사 학위 이상의 의사의 비율은 수년에 걸쳐 증가해 왔으며, 전문학사 및 SVD 이하의 의사의 비율은 감소했지만, 이러한 '부적절한' 의학교육 파이프라인은 여전히 교육 시스템에서 사소하다고 볼 수 없는 요소로 남아있었습니다. 2019년에도 전문대 졸업장 이하의 학력을 가진 개업 의사의 비율은 여전히 34%에 달했습니다.
The current physician mix in medical education originating from a multi-tiered medical education system will inhibit quality development of a health care system. Figure 1 illustrates the annual changes of physicians’ educational distribution in China from 2002 to 2019. In general, the proportion of physicians with a bachelor degrees or above had been increasing over the years, and the share of physicians with vocational diploma and SVD or below has decreased, even though this “inappropriate” pipeline of medical education remained as a non-trivial component of the training system. There were still 34% of practicing physicians with vocational college diplomas or below in 2019.

중국에서는 의대 입학 경쟁이 치열하며, 의대 입학은 국가 대학입학자격시험(NCEE) 점수에 따라 결정됩니다. 중국 교육부는 의학 학사 프로그램의 입학 점수를 전문 의과대학의 전문학사 프로그램보다 훨씬 높게 책정하고 있습니다. 이 두 프로그램 간의 학업 성취도로 표시되는 입학 학생의 질은 크게 다릅니다. 2018년 학부 입학률은 43.3%로, 이는 단기 의과 대학에 입학한 학생들이 NCEE를 응시한 상위 43.3% 학생들보다 낮은 순위를 차지했음을 의미합니다.4
Admission to medical school is highly competitive in China and is based on the students’ scores in the national college entrance examination (NCEE). The National Education Department sets the enrollment scores for medical bachelor programs much higher than vocational diploma programs at junior medical colleges. The quality of admitted students, indicated by their academic performance, between these two programs are significantly different. In 2018, the undergraduate admission rate was 43.3%, which implies that those students admitted into junior medical colleges were ranked below the top 43.3% students taking the NCEE.4
또한 두 의학 프로그램 간에는 교육의 질과 자원에 현저한 차이가 있습니다. 의과 대학 3학년 학생은 3년 동안만 공부해야 하며 실습은 매우 제한적입니다. 특히 이러한 학생들은 고등학교 과정을 통해 학문적 기초가 탄탄하지 않을 수 있다는 점을 고려할 때 의료 교육이 불충분할 수 있습니다. 반면, 의학 학사 프로그램의 학생은 일반적으로 실험실 및 임상 환경에서 보다 엄격한 교육을 포함하여 약 5년의 의학 교육을 받아야 하며, 학위 요건의 일부로 논문을 작성해야 합니다.
There are also remarkable differences in the teaching quality and resources between two streams of medical programs. A junior medical college student needs to take only 3 years of study, with very limited practical training. This may result in insufficient medical training, especially given the fact that these students may not have solid academic foundations through their high school study. By contrast, a student in a medical bachelor program usually needs to take around 5 years of medical training, including more rigorous training in laboratory and clinical settings, and needs to complete a thesis as the partial fulfillment of the requirements for the degree.
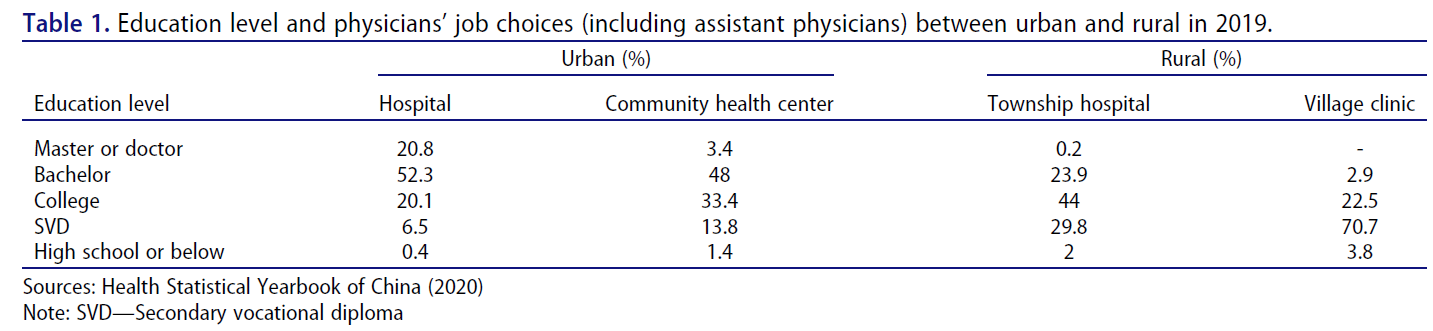
의대생들의 학력 이질성이 높기 때문에 중국 내 개업 의사의 질과 분포에 상당한 이질성이 존재합니다. 예를 들어, 중국에서는 개업 의사의 질과 양이 도시와 농촌 간에 불균등하게 분포되어 있으며,2,5,6 고급 의사(학사 학위 이상)는 도시 지역에 집중되어 있습니다. 표 1은 중국 도시와 농촌의 교육 수준과 의사의 직업 선택(보조 의사 포함) 간의 관계를 보여줍니다.
- 도시 지역에서는 2019년 병원에서 근무하는 의사의 27%, 지역 보건소에서 근무하는 의사의 48.6%가 전문학사 이하의 학력을 가지고 있었습니다.
- 농촌 지역에서는 향진 병원에서 근무하는 의사의 75.8%, 지역 보건 센터에서 근무하는 의사의 97%가 전문학사 이하의 학력을 가지고 있었습니다.
학사 학위 이상을 소지한 개원의는 도시 병원에 더 집중되어 있었습니다. 따라서 농촌 지역 주민들은 도시 지역 주민들과 동등하게 양질의 서비스를 제공받지 못할 수 있습니다.
The high heterogeneity in educational background of medical students has led to significant heterogeneity in quality and distribution of practicing physicians in China. For example, the quality and quantity of practicing physicians are unequally distributed between urban and rural areas in China,2,5,6 and high-quality physicians (with a bachelor degree or above) are concentrated in urban areas. Table 1 shows the relationship between education levels and physicians’ job choices (including assistant physicians) between urban and rural areas in China.
- In urban areas, 27% of the practicing physicians at hospitals and 48.6% at community health centers had vocational diplomas or below in 2019.
- In rural areas, 75.8% of the practicing physicians at township hospitals and 97% at community health centers had vocational diplomas or below.
Practicing physicians with a bachelor degree or above were more concentrated in urban hospitals. Therefore, residents in rural areas may not have equal access to quality services as those in urban areas.
학사 수준의 일차 의료 교육 통합
Unifying Primary Medical Education at Bachelor-level
중국 전국인민대표대회 상무위원회는 의사 자격 시험 응시 자격을 중등 교육에서 비학사 고등 교육으로 상향 조정하는 의사법 개정안을 통과시켰습니다. 그러나 의료 기준 설정에 있어 이러한 점진적 접근 방식은 장기적으로 실수를 누적시키고 경제적, 보건적 비용을 증가시킬 뿐입니다. 현재 의료 서비스의 복잡성과 의학교육 및 기술의 급속한 발전을 고려할 때, 우리는 가능한 한 빨리 의학교육을 학사 수준으로 통합하는 것이 합리적이라고 강력히 주장합니다. 다음 섹션에서 그 이유를 설명합니다.
The review conference of China’s Congress amended the Law for Practicing Physicians to upgrade the eligibility for the examination of physician qualification from secondary education to non-bachelor tertiary education. However, this incremental approach in a medical standards setting will only accumulate long-term mistakes, and aggregate economic and health costs. Given the complexity of health care at present and rapid development in medical education and technology, we strongly argue that it is reasonable to unify medical education at a bachelor level as soon as possible. We present our reasons in the following sections.
전 세계 의사를 위한 입문 수준 기준
Entry-level Standards for Physicians around the World
국가마다 의학교육과 훈련에 큰 차이가 있지만, 초급 의학교육의 최소 기준은 학사 학위 교육을 요구합니다.
- 호주, 필리핀, 미국 등 일부 국가에서는 의대생이 의학전문대학원 수준의 의학 프로그램에 입학해야 면허 시험에 응시할 수 있습니다.7
- 미국의 경우 미국 의사 면허 시험(USMLE)에 응시하려면 학사 학위(4년)와 의과대학 4년 졸업 학위가 필요합니다.8 공인된 레지던트 프로그램(3~7년)을 마친 후 의료 행위가 허용됩니다. 따라서 미국에서 주치의가 되기 위해서는 약 11년, 외과의사가 되기 위해서는 13년 이상의 수련 기간이 소요됩니다.
Although there are large variations in medical education and training across countries, the minimum standards for entry-level medical education require bachelor-degree training.
- Some countries, such as Australia, Philippines, and the USA, even require medical student to enter the graduate-level medical program before they can attend the licensing examinations.7
- In the US, in order to be eligible for the United States Medical Licensing Examination (USMLE), candidates require a bachelor degree (4 years), and a four-year graduate degree from medical schools.8 Medical practice is allowed after completing an accredited residency program (3–7 years). Therefore, it takes around 11 years of training to become a primary care physician and over 13 years to become a surgeon in the United States.
개발도상국인 태국의 경우 반세기 전에 학사 수준의 교육으로 입문 의학교육이 시작되었습니다.9
- 태국의 학부 의학교육(입문 의학교육)은 6년이 걸리며 보통 1학년은 기초 교육, 2~3학년은 기초 의학 교육, 4~6학년은 임상 교육으로 3단계로 나뉩니다.9,10
- 태국보다 선진국인 중국이 왜 이런 이상한 의학교육 시스템을 유지하면서 교육 기간과 재능이 다른 모든 졸업생을 의사가 될 수 있도록 하는지 의문이 들 수밖에 없습니다. 의료 인력 부족과 인구 건강 개선의 시급한 필요성이 이러한 의료 교육 및 훈련 시스템을 개발하게 된 초기 이유였지만, 오늘날 중국이 직면하고 있는 주요 문제는 더 이상 아닙니다.
In Thailand, a developing country, the entry-level medical education was set at bachelor-level training a half-century ago.9
- The Thai undergraduate medical program (entry-level medical education) takes 6 years to finish and is usually divided into three stages: the first year for basic education, the 2nd-3rd years for basic medical education, and the 4th-6th years for clinical training.9,10
- This raises a question why China, a country more developed than Thailand, would keep such an odd medical education system and allow all graduates with different training periods and different talents to become doctors. The shortage of health workforce and urgent need to improve population health were the initial reasons for developing this system of medical education and training, but they are no longer the main issues China is facing today.
의대생 공급 과잉
Oversupply of Medical Students
중국은 세계에서 가장 큰 규모의 의료 인력 교육 시스템을 갖추고 있습니다. 2014년부터 2018년까지 의과대학 통계에 따르면 중국의 의대 졸업생 수는 총 560만 명 증가했지만, 의료 인력 규모는 210만 명 증가에 그쳤습니다. 일정 비율의 인력 감소가 있더라도 전체 시장에서 의대 졸업생의 공급과 고용 사이의 큰 격차를 설명하기는 여전히 어렵습니다. 한 가지 가능한 설명은 일부 저학력 의대생이 보건 분야에 진출하지 않아 의대 졸업생 공급 과잉을 초래했다는 것입니다.
China has the largest education system for health workforce in the world. According to the statistics of medical schools from 2014 to 2018, the number of medical graduates in China increased by 5.6 million in total, but the size of the health workforce increased by only 2.1 million. Even though there is a certain proportion of workforce attrition, it is still difficult to explain the huge gap of the whole market between supply and employment of medical graduates. One possible explanation is that some less-educated medical students did not enter into the health sector and created an oversupply of medical graduates.
또한, 매년 전문 의과대학 및 중등 의과대학에 등록하는 의대생 수는 의학 학사 이상 프로그램에 등록하는 학생 수보다 훨씬 더 많았습니다.
- 예를 들어, 2018년에 고등 의과대학에 등록한 의대생 수는 85만 5,000명이었으며, 이 중 61만 1,000명이 전문대학 학사 학위 프로그램에 등록했습니다. 또한 전문학사 학위 프로그램에 등록한 학생은 39만 명에 달했습니다.
이러한 공급 패턴은 의학교육의 질에 영향을 미칠 뿐만 아니라 보건 인력 수급의 불균형을 심화시켰습니다.11 중등 직업 교육 및 직업 교육 졸업생의 과잉 공급은 전문과목 혼합의 왜곡(잘 훈련된 일차 진료 의사의 부족)과 의사 시장에서 의대 졸업생 간의 치열한 경쟁을 심화시키는 결과를 초래했습니다.
Moreover, the number of medical students enrolled each year at junior medical colleges and secondary schools was much higher than that at medical bachelor programs or above.
- For example, in 2018, the number of medical students enrolled in tertiary medical schools was 855,000, of which 611,000 were enrolled in vocational college diploma programs. In addition, there were 390,000 students enrolled in SVD programs.
This supply pattern not only affected the quality of medical education but also led to an increasing imbalance in the supply and demand of health workforce.11 The oversupply of graduates with secondary vocational education and vocational education further resulted in the distortion of specialty mix (inadequate numbers of well-trained primary care physicians) and increased intensive competition among medical graduates in physicians’ market.
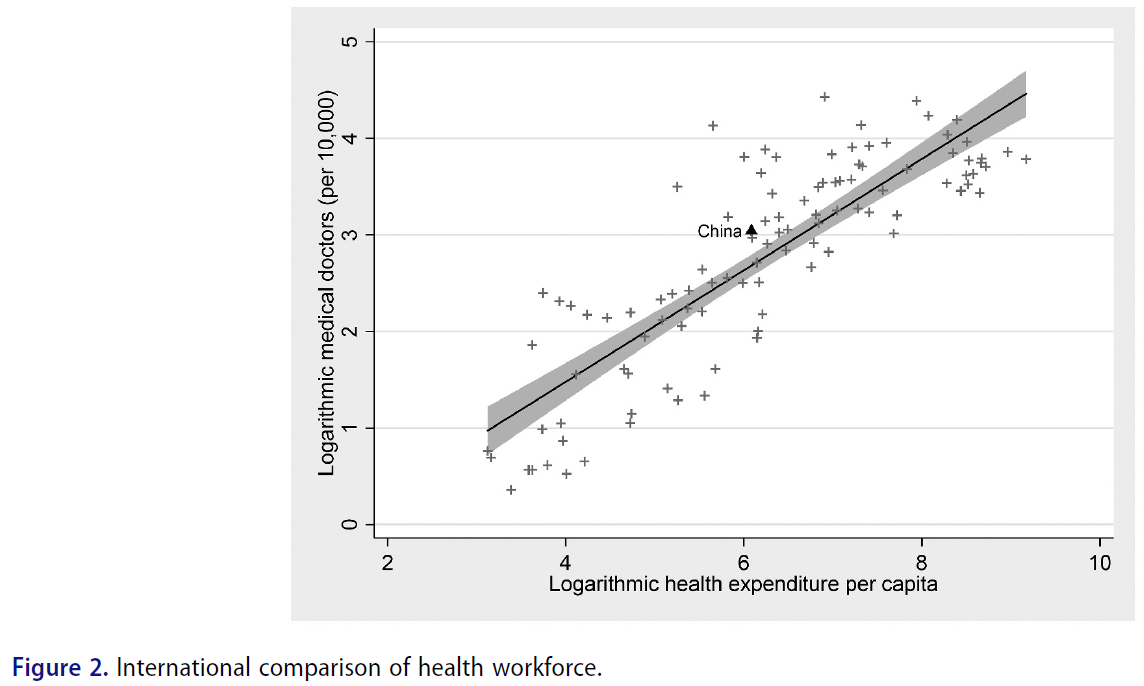
같은 규모로 볼 때 중국의 개업 의사 수는 더 이상 다른 비교 대상 국가보다 적다고 볼 근거가 없습니다. 1인당 의료비 지출과 인구 10,000명당 의사 수 사이에는 양의 상관관계가 있는 것으로 알려져 있는데, 이는 의료비 지출이 의료 시스템에서 고용하는 직원 수와 관련이 있다는 사실을 반영하는 것입니다. WHO 데이터를 기반으로 국제 비교 관점에서 중국의 의사 수를 조사했습니다.12 그림 2에 따르면 중국의 의사 공급은 모든 국가 중에서 상대적으로 적절한 수준입니다.
We have reasons to believe that, on the same scale, the stock of practicing physicians in China is no longer less than that in any other comparable countries. There is a known positive association between health expenditure per capita and the number of medical doctors per 10,000 people, which reflects the fact that how much you spend is related to how many employees the system hires. We examined the number of physicians in China from the perspective of international comparison based on the WHO data.12 Figure 2 suggests that the provision of practicing physician in China is relatively adequate among all nations.
다단계 의료 교육 시스템이 의료 시장에 미치는 장기적 비용
The Long-term Costs of Multi-tiered Medical Education System on Healthcare Market
2019년 Hsieh & Tang의 논문에 따르면, 의사들의 학력 차이가 현저한 의료 시장은 환자 입장에서 더 나은 서비스를 제공할 수 있는 양질의 의사를 찾는 데 추가적인 탐색 및 정보 비용을 부과합니다.2 학력이 높은 의사는 도시 지역에서 진료하는 경향이 있기 때문에 대형 병원에 고용될 가능성도 높습니다. 이로 인해 농촌 지역과 1차 의료 기관의 인적 자원이 악화되고 있습니다. 1970년대에 아켈로프가 개발한 모델에 따르면13 의사의 능력은 관찰할 수 없으며, 이는 의사의 보수가 그들이 제공하는 서비스의 질에 따라 달라지지 않는다는 것을 의미합니다. 규제 시장regulated market에서는 모든 의사에게 평균 수준의 임금을 지급하므로 우수한 의대생이 더 나은 보수를 기대하기 때문에 의료 시장에 진입할 동기가 부족합니다. 또한 의사들은 추가 의료 교육을 받거나 인적 자본에 투자할 인센티브가 적습니다. 장기적으로 다단계 의학교육 시스템은 의료 시장의 형평성과 효율성 측면에서 두 가지 해악을 초래할 것입니다.
According to Hsieh & Tang’s paper in 2019, the health care market in which physicians have remarkable differences in their education, imposes additional searching and information costs to the seeking of quality doctors who can provide better services from patients’ perspective.2 As doctors with higher educational background tend to practice in urban areas, they are also more likely to be employed by larger hospitals. This has caused a deterioration of human resources in rural areas and at primary health care facilities. Based on the model developed by Akerlof in the 1970s,13 physicians’ ability cannot be observed, which means physicians’ remuneration does not depend on the quality of services they provide. The regulated market pays all the doctors an average level of wage, so there is a lack of motivation for high-quality medical students to enter the health care market since they would expect better payments. Doctors would also have less incentives to receive further medical education and to invest in their human capital. In the long run, a multi-tiered medical education system will contribute to twofold harms in both equity and efficiency of the health care market.
법 개정 및 시행의 어려움
Difficulties in Amending and Implementing the Law
일반적으로 법률과 사법 제도는 그 시행을 위해 비교적 안정적인 기대치를 필요로 합니다. 안정성을 유지하기 위해서는 일단 의사에 대한 법률이 시행된 후 사회적 상황이 크게 변화하기 전에 자의적으로 폐지하거나 개정할 수 없습니다. 따라서 법 개정은 법안 제출부터 법안 심사, 의결 및 채택, 공포 및 시행에 이르기까지 엄격한 절차를 거쳐야 하므로 시간이 걸립니다. 예를 들어, 중화인민공화국 의사 개업에 관한 법률은 1998년에 국회 위원회에서 통과되었지만 23년 후인 2021년에 첫 번째 개정이 이루어졌습니다. 이 기간 동안 중국의 경제 발전은 눈부신 성과를 거두어 지난 20년 동안 GDP가 7조 9,700억 위안에서 82조 7,122억 위안으로 약 937% 증가했으며,14 이에 따라 의료 수요와 의료 시장에도 큰 변화가 일어났습니다. 법 개정 과정이 더디더라도 의학교육 체계 정상화를 위한 법 개정이 시급한 상황입니다.
Generally speaking, legislation and the judicial system require a relatively stable set of expectations of the law for its implementation. In order to maintain stability, it cannot be abrogated or amended discretionarily before the social contexts change significantly once the law for physicians goes into effect. Therefore, any amendment of the law must follow a rigorous procedure, from submission to the consideration of the draft law, then to the vote and adoption, and to the promulgation and implementation of the law, which will take time. For example, the law for practicing physicians of the People’s Republic of China was passed by the Committee of the Congress in 1998, while its first amendment came twenty-three years later in 2021. The economic development of China has made extraordinary achievements during this period, with its GDP growing from 7.97 trillion yuan to 82.7122 trillion yuan in the last two decades and an increase of about 937%,14 and thus significant changes have taken place in health demands and health care market. There is an urgency to amend the law to normalize the medical education system even though the process of amendment will be slow.
2021년 개정안 제정 및 시행을 위한 장애물도 존재합니다. 2019년 중국 보건 통계 연감의 데이터에 따르면15 현재 전문 학사 학위 대학에 재학 중인 의대생은 100만 명이 넘습니다. 이러한 의대생의 경력 개발과 전환, 교수진 및 관련 인력에 미치는 영향을 신중하게 고려해야 하며, 그렇지 않으면 모든 개혁이 그들의 이익에 대한 비용으로 간주되어 저항을 받게 될 것입니다.
There are also obstacles for the enactment and implementation of the 2021 amendment. According to data from the Health Statistical Yearbook of China in 2019,15 there are over one million medical students currently enrolled in vocational diploma colleges. The career development and transition for these medical students and the impact on their faculties and related personnel need to be carefully considered, otherwise any reforms will be seen as costs of their interests and thus resisted.
결론
Conclusion
우리는 중국 의회가 오랜만에 마침내 최근 의사법 개정을 추진한 것을 기쁘게 생각합니다. 그러나 우리는 중국의 의사 자격 시험에 대한 교육 자격이 여전히 국제 표준에 훨씬 못 미친다고 주장합니다. 중앙은행이 과도한 유동성을 흡수할 수 있기 때문에 통화(자본) 완화는 쉬운 반면, 이미 의료 시장에서 형성된 의사들의 인적 자본을 되돌리기는 거의 불가능합니다. 따라서 우리는 중국이 최근 개정안과 같이 의사 자격 시험의 문턱을 전문대 수준이 아닌 학사 수준으로 설정하는 것을 의미하는 초급 의학교육 기준을 개선할 것을 강력히 권고합니다. 이는 의사의 자질을 향상시킬 뿐만 아니라 중국 의료 시장의 형평성과 효율성 문제를 해결하는 데 도움이 될 것입니다.
We are delighted to see that the Congress in China finally promoted the recent amendments on the Legislation of Practicing Physician after a long time. However, we argue that the educational eligibility for examination of the physicians’ qualification in China is still far below the international standard. It is easy to do monetary (capital) easing because the central bank can soak up excessive liquidity, while it is hardly possible to take back human capital of physicians already formed in a health care market. Therefore, we highly recommend that China improve the entry-level medical education standards, which implies setting the threshold at bachelor level for the examination of physician’s qualification, instead of junior college level as in the recent amendment. This will not only improve the quality of the physicians but also will help to address equity and efficiency issues in the health care market in China.
Health Syst Reform. 2022 Jan 1;8(1):e2048438. doi: 10.1080/23288604.2022.2048438.
Amending the Law for Licensing Medical Practitioners of China in 2021: A Commentary
PMID: 35416752
Abstract
The Law for Licensing Medical Practitioners of the People's Republic of China, enacted in 1999, was amended in 2021. This commentary reviews the key points of the amendment and raises doubts as to one of its points. Specifically, we argue that the minimum education level required to take the physicians' licensing examination should be set to completion of a bachelor degree, instead of a vocational diploma or junior college graduation as in the 2021 amendment. China adopted a system of multi-tiered medical education more than 70 years ago. This policy has resulted in a threshold of entry-level medical education far below the global standards. The highly heterogeneous education background of physicians in China has led to low standards of practicing physicians, which in turn have significantly negative impacts on the health care market. We illustrate changes over time in the educational distribution and regional distribution of practicing physicians in China, and present reasons to improve entry-level educational standards, by setting the physician licensing threshold at an appropriate level. This will not only improve the overall quality of physicians but will also help address equity and efficiency issues in the health care market.
Keywords: China; licensing; medical education; physician supply.
'Articles (Medical Education) > 세계화, 다양한 국가' 카테고리의 다른 글
| 졸업후의학교육을 위한 인증 시스템: 다섯 개 국가의 비교(Adv Health Sci Educ Theory Pract. 2019) (0) | 2023.12.17 |
|---|---|
| 인도네시아의 의사국가면허시험: 학생, 교수, 대학의 관점(© 2018 The University of Leeds and Rachmadya Nur Hidayah) (0) | 2023.11.19 |
| 베트남의 의사면허시험에 대한 코멘터리(MedEdPublish, 2023) (0) | 2023.11.19 |
| 베트남 의학교육의 혁신(BMJ Innov 2021) (0) | 2023.11.19 |
| 동남아시아의 면허시험: 교육정책의 변화에서 찾아낸 교훈( Asia Pacific Sch, 2019) (0) | 2023.11.19 |