활동이론을 활용하여 의학 업무와 학습을 변혁하기 (Med Teach, 2021)
Using activity theory to transform medical work and learning
Yrj€o Engestr€oma and Eeva Py€or€al€ab

소개
Introduction
의사는 의료 기관의 복잡한 사회 시스템에서 필수적인 구성원으로 일합니다. 역량 기반 교육 프레임워크는 미래의 의사가 시스템 기반 진료, 옹호 및 협업을 개발할 수 있도록 의료 교육을 요구합니다(Orsino and Ng 2019). 동시에 의료의 전반적인 대상, 즉 환자가 겪고 있고 치료를 원하는 건강 문제의 스펙트럼에 근본적인 변화가 일어나고 있습니다. 장기 치료가 필요한 노인과 만성 질환 환자의 비율이 증가하고 있습니다. 두 가지 이상의 만성 질환을 앓고 있는 다질환 환자는 의료 자원의 상당 부분을 확대하고 활용하고 있습니다(Barnett et al. 2012; Braithwaite 2018). 동시에 의료 전문가들은 빈곤과 열악한 건강이 밀접하게 연관되어 있으며 사회경제적으로 박탈당한 사람들은 의료 서비스에 대한 접근성이 제한되어 있다는 사실을 점점 더 많이 인식하고 있습니다.
Physicians work as integral members of the complex social systems of healthcare organizations. Competency-based education frameworks require that medical training develop future physicians’ systems-based practice, advocacy, and collaboration (Orsino and Ng 2019). At the same time, a foundational change is going on in the overall object of medicine, namely the spectrum of health problems patients are suffering from and seeking care for. The proportion of elderly people and patients with chronic conditions requiring long-term care is increasing. Patients with multimorbidity, i.e. suffering from two or more chronic conditions, are expanding and utilizing a significant portion of health care resources (Barnett et al. 2012; Braithwaite 2018). At the same time, medical professionals are becoming increasingly aware that poverty and poor health go hand in hand and the socio-economically deprived have limited access to health care.
환자 치료의 파편화는 의료계의 주요 과제입니다. 의료 시스템은 주로 복잡한 장기 질환과 만성 질환, 정신 장애, 빈곤의 동시 발생보다는 환자의 단일 증상과 질병을 치료하도록 설계되어 있습니다(Walker and Druss 2017).
Fragmentation of patient care is a major challenge for healthcare practice. Healthcare systems are largely designed to treat patients’ single symptoms and diseases rather than complicated long-term disorders and the co-occurrence of chronic conditions, mental disorders, and poverty (Walker and Druss 2017).
다질환과 치료의 파편화에 관한 연구에 따르면 의료 교육은 환자에게 의료 부서 간, 그리고 치료 중인 환자와의 연속성, 조정 및 협업을 제공하는 접근 방식을 채택해야 합니다(Barnett 외. 2012; Braithwaite 2018; Engeström 2018). 그럼에도 불구하고 대부분의 의학 연구는 포괄적인 환자 치료와 1차 의료와 전문의 진료 간의 협력을 희생하면서 질병 중심의 전문의 관점에 초점을 맞추고 있습니다.
Studies on multimorbidity and fragmentation of care call for medical education to adopt an approach that provides patients with continuity, coordination, and collaboration across healthcare units and with patients under their care (Barnett et al. 2012; Braithwaite 2018; Engeström 2018). Still, most medical studies focus on disease-centred specialist perspectives at the expense of comprehensive patient care and collaboration between primary healthcare and specialist care.
동시에 의료 시스템은 빠른 이직률과 단기적인 수익을 선호하는 시장 중심의 비즈니스 계산과 경영주의에 의해 점점 더 침투하고 있습니다. 의료의 도구는 합리화, 표준화, 상품화라는 측면에서 틀이 잡히고 있으며, 이러한 개념은 수평적으로 공동 구성된 치료 궤적과 장기적인 사회적 영향보다는 선형적이고 미리 포장된 하향식 프로세스와 절차를 선호합니다. 이러한 힘은 의료 대상의 필요한 확장을 매우 어렵게 만듭니다.
Concurrently, systems of healthcare are increasingly penetrated by market-oriented business calculations and managerialism that favor rapid turnover and short-term profits. The instruments of medicine are becoming framed in terms of rationalization, standardization, and commoditization, notions that favor linear and pre-packaged top-down processes and procedures rather than horizontally co-constructed care trajectories and long-term societal impact. These forces make the needed expansion of the object of medicine very difficult.
환자 치료와 의학교육의 파편화와 장기 질환 및 동반 질환을 가진 환자의 증가로 인해 의료의 대상에 대한 근본적인 확장, 즉 더 긴 시간의 관점, 더 광범위한 협업 및 학제 간 접근 방식, 의료인과 그 조직의 혁신적 에이전시가 필요합니다. 따라서 우리는 변화, 교란, 논쟁을 조사하기 위해 고안된 이론적, 방법론적 접근이 필요합니다.
Fragmentation of patient care and medical education as well as the increasing number of patients with long term conditions and comorbidities require a radical expansion of the object of medicine: longer time perspectives, broader collaborative and interdisciplinary approaches, and transformative agency from medical practitioners and their organizations. Therefore, we need a theoretical and methodological approach designed to investigate transformation, disturbances, and controversy.
문화-역사적 활동 이론(CHAT)은 역사적으로 형성된 체계적 모순을 분석의 출발점으로 삼습니다. 그림 1은 활동 시스템의 일반 모델(Engeström 2015, 63쪽)을 사용하여 의료 업무에 만연한 모순에 대한 작업 가설을 구성하는 방법을 보여줍니다.
Cultural–historical activity theory (CHAT) takes historically formed systemic contradictions as the starting point of the analysis. Figure 1 shows how the general model of an activity system (Engeström 2015, p. 63) can be used to construct a working hypothesis of the pervasive contradictions of medical work.
모순은 일상적인 의료 업무에서 혼란과 갈등을 야기합니다. 다른 한편으로는 일상적인 혁신과 지역적 변화를 촉진하기도 합니다(Martin et al. 2017). 따라서 의료 사회 시스템이 복잡성을 이해하고 관리하며, 모순의 역학을 파악하고, 이를 해방적 변화에 활용하도록 도전합니다.
Contradictions generate disturbances and conflicts in everyday medical work. On the other hand, they also stimulate everyday innovation and local change (Martin et al. 2017). Thus, they challenge the medical social system to understand and manage complexity, to identify the dynamics of contradictions, and to utilize them in emancipatory transformations.
이 글에서는 CHAT의 주요 개념과 확장적 학습 이론을 소개합니다(Engeström과 Sannino 2010, Engeström 2015, 2018). 확장적 학습은 이론, 경험적 연구, 형성적 개입 사이에 강한 연관성이 있는 연구 전통입니다. 따라서 우리는 의료 전문가와 환자가 치료의 파편화와 의료 활동 시스템의 모순을 해결하기 위해 의료 서비스 맥락에서 구현 된 형성적 개입의 구체적인 사례를 통해 활동 이론을 논의합니다.
This article introduces key concepts of CHAT and the theory of expansive learning (Engeström and Sannino 2010; Engeström 2015, 2018). Expansive learning is a research tradition with strong links between theory, empirical research, and formative interventions. Therefore, we discuss activity theory with the help of concrete examples of formative interventions implemented in the context of healthcare where healthcare professionals and patients tackled fragmentation of care and contradictions in the activity systems of medical work.
의료 업무의 근접 개발 영역: 협력적이고 변혁적인 전문성
The zone of proximal development of medical work: Collaborative and transformative expertise
활동 이론에서 변화는 미리 정해진 종점을 향한 선형적인 움직임으로 간주되지 않습니다. 이는 근위 발달 영역으로 이해됩니다. 이 개념은 원래 비고츠키(1978, 86쪽)가 개인 학습의 맥락에서 제시했습니다. Engeström(2015, 138쪽)은 집단 활동 수준에서 학습과 발달을 다루기 위해 이 개념을 재정의했습니다. 근접 발달 영역은 현재와 미래 사이의 가능성의 지형으로, 당면한 모순에 대한 해결책으로 활동을 집단적으로 변화시킬 수 있습니다.
In the activity theory, transformations are not seen as linear moves toward pre-fixed end points. They are understood as zones of proximal development. This concept was originally presented by Vygotsky (1978, p. 86) in the context of individual learning. Engeström (2015, p. 138) redefined the concept to address learning and development at the level of collective activities. Zones of proximal development are terrains of possibilities between the present and the future where activities can be collectively transformed as a solution to the contradictions at hand.
의료 업무와 같은 활동의 근접 발전 영역을 묘사하려면 역사적 변화와 발전의 주요 차원을 파악해야 합니다. 그림 2에서는 의료 전문성의 근위 발전 영역을 개인 전문성과 집단 전문성(수직적 차원), 안정을 위한 학습과 변화를 위한 학습(수평적 차원)이라는 두 가지 차원을 통해 설명합니다. 이 두 가지 차원이 합쳐져 네 가지 영역이 형성되는데, 왼쪽 아래에는 역사적으로 가장 오래된 기술 전문 지식이, 오른쪽 위에는 아직 미지의 영역인 협업 및 혁신 전문 지식이 위치합니다.
To portray a zone of proximal development of an activity such as medical work, we need to identify the key dimensions of historical change and development. In Figure 2, the zone of proximal development of medical expertise is illustrated with the help of two dimensions: namely, between an individual and a collective locus of expertise (the vertical dimension), and between learning for stability and learning for change (the horizontal dimension). Together, these two dimensions form a fourfold field in which the historically earliest craft expertise is located in the lower-left section and the largely uncharted collaborative and transformative expertise is located in the upper right section.
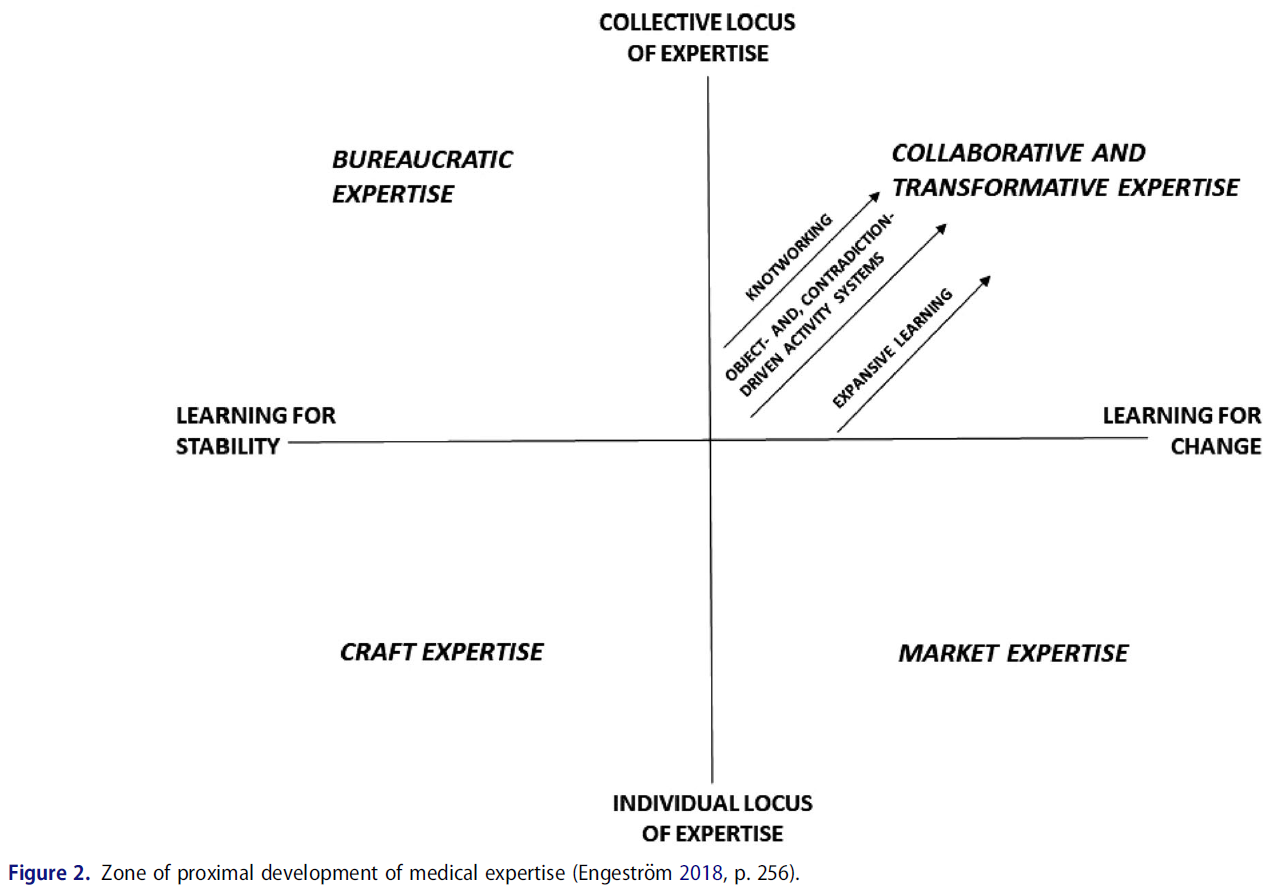
협력적이고 변혁적인 전문성은 의료진이 지속적인 시스템 변화 노력에 참여한다는 것을 의미합니다. 이는 의료진 간의 협업과 의료기관, 환자 및 대상 지역사회, 기타 사회 주체 간의 연합 구축을 통해서만 달성할 수 있습니다. 그림 2에서 설명한 바와 같이, 협력적이고 혁신적인 전문성을 향한 세 가지 선봉은 다음과 같다.
- (1) 전문성을 목적 지향적이고 모순에 기반한 활동 시스템으로 재개념화하기,
- (2) 전문성을 협상된 매듭으로 추구하기,
- (3) 확장적 학습으로 전문성 구축하기
다음 섹션에서는 이 세 가지 선봉에 대해 소개합니다.
Collaborative and transformative expertise implies that medical practitioners are involved in ongoing systemic change efforts. This can only be accomplished by means of collaboration among healthcare practitioners and coalition-building between healthcare units, their patients and target communities, and other societal actors. As described in Figure 2, we may identify three spearheads toward collaborative and transformative expertise:
- (1) reconceptualizing expertise as object-oriented and contradiction-driven activity systems,
- (2) pursuing expertise as negotiated knotworking, and
- (3) building expertise as expansive learning.
We will introduce these three spearheads in the following sections.
객체 지향 활동 시스템으로서의 전문성
Expertise as object-oriented activity systems
CHAT의 기본 아이디어 중 하나는 수명이 짧고 목표 지향적인 활동actions과 지속적이고 집단적인 활동activities을 구분하는 것입니다(Leont'ev 1978). 활동activity은 행동을 생성하는 협력적이고 총체적인 시스템으로 이해됩니다. 활동 시스템은 대상object을 지향합니다. 대상은 활동의 장기적인 목적을 구현하여 가능한 행동의 지평을 생성합니다. 의료 서비스에서 일반적인 대상은 건강과 질병이지만, 특정 불만을 가진 각각의 특정 환자는 대상의 구체적인 표현입니다.
One of the foundational ideas of CHAT is the distinction between short-lived, goal-directed actions and durable and collective activities (Leont’ev 1978). An activity is understood as a collaborative and holistic system that generates actions. An activity system is oriented toward an object. The object embodies the long-term purpose of the activity, generating horizons for possible actions. In healthcare, the general object is health and illness, whereas each specific patient with a specific complaint is a situated manifestation of the object.
의료와 같은 복잡한 사회 제도에는 각 활동 시스템의 노드 내부와 노드 간, 그리고 상호 연결된 활동 시스템 간에 역사적으로 축적된 체계적 모순이 존재합니다. 오늘날 의료 업무의 주요 과제 중 하나는 진료의 파편화, 또는 활동 이론적 용어로 대상의 파편화이며, 특히 여러 만성 질환을 가진 환자를 진료할 때 두드러집니다(Kerosuo and Engeström 2003; Engeström 2018; Meijer 외. 2020, 언론 보도 중). 그림 3은 핀란드 헬싱키시의 의료 시스템에서 여러 의료 전문 분야와 진료소 사이를 떠돌던 한 환자의 치료가 파편화되는 과정을 보여줍니다.
In complex social institutions such as healthcare, there are historically accumulated systemic contradictions within and between the nodes of each activity system, and among interconnected activity systems. One of the major challenges in medical work today is the fragmentation of care, or in activity-theoretical terms, the fragmentation of the object, especially salient in the care of patients with multiple chronic conditions (Kerosuo and Engeström 2003; Engeström 2018; Meijer et al. 2020, in press). Figure 3 portrays the fragmentation of the care of a patient who drifted between several medical specialties and clinics in the health care system of the city of Helsinki in Finland.
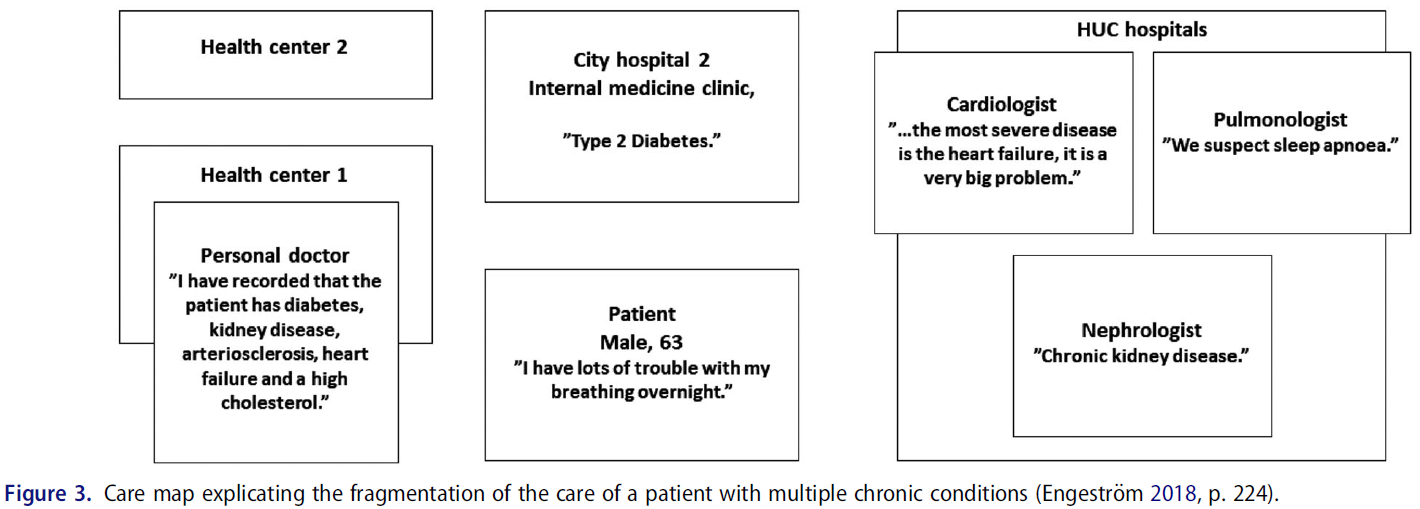
파편화는 다음의 경우에 나타났습니다.
- (a) 서로 다른 전문 간병인이 자신의 제한된 책임과 역량 영역에 '속하는' 증상과 치료에만 집중하고,
- (b) 서로 다른 간병인 사이에 공통 언어나 이해가 없으며,
- (c) 환자 치료에 관여하는 여러 당사자 간의 조정, 협력 및 의사소통을 보장하는 효율적인 메커니즘이 없을 때
파편화는 발췌문 1에 예시된 바와 같이 치료의 공백과 중단 위험을 초래했습니다.
Fragmentation emerged when
- (a) the different specialist caregivers concentrated exclusively on the symptoms and care that ‘belonged’ to their own restricted areas of responsibility and competence,
- (b) there was neither common language nor understanding between the different caregivers, and
- (c) there was no efficient mechanism that guaranteed coordination, cooperation, and communication between the different parties involved in the patient’s care.
Fragmentation led to gaps and risks of disruption in the care, as exemplified in Excerpt 1.
발췌문 1
Excerpt 1
환자: 남편은 암으로 사망했고 딸은 이제 열여섯 살이 되었습니다. 우리 둘만 남았기 때문에 딸을 성인이 되도록 키우기 위해 가능한 모든 수단을 동원해 살아남고 신장을 보호해야 한다고 생각합니다. 그래서 그것이 저에게 스트레스를 주는 원인이죠.
Patient: My husband died of cancer and my daughter is now sixteen. Being just the two of us, I feel I have to stay alive and protect my kidney by all possible means, to bring her up into adulthood. So that’s what causes stress for me.
연구원: 그래서 문제는 급성 상황에서 정보가 한 의사에서 다른 의사로 전달되었는지 여부에 대한 불확실성입니다....
Researcher: So the problem is uncertainty in acute situations, whether or not information has been passed from one doctor to the other…
환자: 네, 최근에 있었던 특정 상황처럼 제가 직접 정보를 전달할 수 없는 경우입니다. 제 상황을 설명할 수 없었어요. 그것은 제가 여러 번 생각했던 것입니다...
Patient: Yes, if I cannot convey the information myself, like it was in that particular situation recently. I was not able to explain my situation. That’s something I have thought about many times…
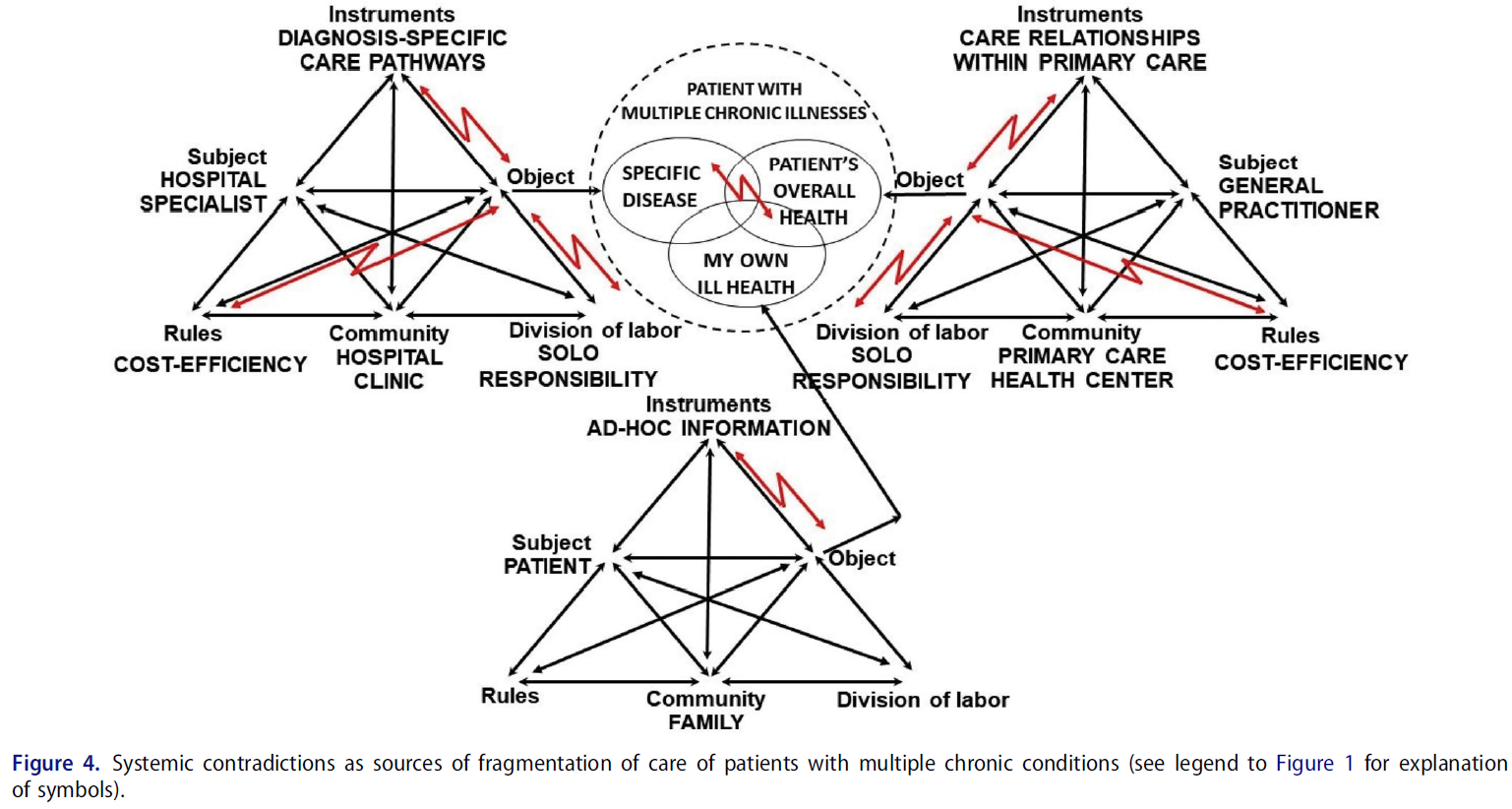
치료의 파편화는 활동 시스템 간 및 활동 시스템 내부의 모순으로 인해 발생했습니다. 병원의 전문 진료, 일차 의료의 일반 진료, 아픈 환자 자신의 삶이라는 활동 체계는 각각 다른 대상을 가지고 있었고, 이 대상들은 자주 충돌하고 거의 만나지 못했습니다. 분업은 각 의사의 단독 책임을 강조하여 전문의와 일반의의 책임을 효과적으로 캡슐화했습니다. 또한, 여러 만성 질환을 앓고 있는 환자에게는 공유된 도구가 필요했을 텐데, 이 두 가지 활동 체계는 특정한 별도의 도구로 운영되었습니다. 게다가 시장 경제 규칙에 따라 의료 기관은 단기적인 비용 효율성을 우선시해야 했습니다. 이러한 긴장이 가득한 상황은 그림 4에 개략적으로 설명되어 있습니다.
The fragmentation of care was generated by contradictions between and within activity systems. The activity systems of specialist care in the hospital, general practice in primary health care, and the patient’s own life with ill health each had a different object, and these objects frequently collided and rarely met. The division of labor emphasized solo responsibility of each practitioner, effectively encapsulating the responsibilities of the specialist and the general practitioner. Moreover, these two activity systems operated with specific, separate instruments, whereas a patient with multiple chronic conditions would have needed shared instruments. Furthermore, the market economy rules guided the health care units to prioritize short-term cost-efficiency. This tension-laden constellation is schematically illustrated in Figure 4.
매듭을 짓는 전문성
Expertise as knotworking
의료 업무의 근접 개발 영역을 향한 두 번째 선봉은 매듭짓기입니다. 매듭짓기의 개념은 파편화를 극복하기 위한 일련의 개입에서 개발되었습니다(Engeström 외. 1999; Engeström 2008). 학습 과제는 의사와 환자가 간병인 조직 간에 협력하고 환자의 치료를 공동으로 계획 및 모니터링할 수 있는 새로운 방법을 모색하고 확립하는 것이었습니다. 의료 분야에서 영구적인 팀은 당면한 문제에 대응하는 유동적인 전문 지식의 조합, 즉 '매듭'으로 점점 더 대체되고 있습니다(Engeström 2008, Bleakley 2014, Hurlock-Chorostecki 외. 2015, Larsen 외. 2017, Varpio and Teunissen 2020, 보도 중).
The second spearhead toward the zone of proximal development of medical work is knotworking. The concept of knotworking was developed in a series of interventions aimed at overcoming fragmentation (Engeström et al. 1999; Engeström 2008). The learning challenge was to seek and establish a new way for practitioners and patients to work between the caregiver organizations and collaboratively plan and monitor a patient’s care. In healthcare, permanent teams are increasingly replaced by fluid combinations of expertise, ‘knots’ that correspond to the problem at hand (Engeström 2008; Bleakley 2014; Hurlock-Chorostecki et al. 2015; Larsen et al. 2017; Varpio and Teunissen 2020, in press).
매듭이라는 개념은 느슨하게 연결된 행위자 및 활동 시스템 간의 협업 성과가 빠르게 맥동하고 부분적으로 즉흥적으로 오케스트레이션되는 것을 의미합니다(Engeström 외. 1999). 매듭은 빠른 즉흥성과 장기적인 관점의 계획 및 후속 조치를 모두 포함하는 분리된 활동과 전문 지식의 실타래를 묶고 다시 묶는 방식으로 작동합니다. 의료 분야에서 매듭짓기의 구체적인 도구성은 고객 또는 환자를 협상과 유연한 합의의 동등한 당사자로 간주하는 것과 관련이 있습니다. 이를 위해서는 참여 주체 간에 공유된 언어와 대상이 필요합니다.
The notion of a knot refers to a rapidly pulsating and partially improvised orchestration of collaborative performance between otherwise loosely connected actors and activity systems (Engeström et al. 1999). Knots operate by tying and retying together otherwise separate threads of activity and expertise, involving both rapid improvisation and a long-term perspective of planning and following up. The specific instrumentality of knotworking in healthcare is related to clients or patients as being equal parties in the negotiations and flexible agreements. This requires a shared language and object between the participating actors.
매듭짓기는 대상의 파편화를 극복하기 위한 모델입니다. 환자 치료에 관여하는 여러 전문 분야와 기관의 의료진은 치료 궤적의 다양한 지점에서 환자를 위해 각자의 전문성을 협상, 조정, 결합하는 방법을 모색합니다. 매듭짓기의 한 예로 여러 부서에서 환자의 치료에 관한 모든 관련 정보가 포함된 치료 합의서라는 도구를 공동으로 개발하고 실행하는 것을 들 수 있습니다(Engeström 2018). 발췌문 2는 발췌문 1에 제시된 파편화된 환자 치료를 개선하기 위한 다자간 치료 합의서 협상의 예를 보여줍니다.
Knotworking is a model for overcoming fragmentation of the object. Practitioners from different specialties and organizations involved in the care of a patient seek ways to negotiate, coordinate, and combine their expertise for the best of the patient in various points of the care trajectory. An example of knotworking is the collaborative development and implementation of an instrument called care agreement that contained all relevant information about the patient’s care in different units (Engeström 2018). Excerpt 2 gives an example of negotiation of the multi-party care agreement to improve the fragmented care of the patient presented in Excerpt 1.
발췌 2
Excerpt 2
주치의[환자 앞에 있는 문서를 가리키며]: 그럼, 1차 진료 보건소에서 환자를 담당하고 있는 의사로서 [환자의 개인 주치의]가 먼저 작성하시겠습니까? 그리고 나서...
Chief physician [pointing at a document in front of her]: So, will you [the patient’s personal GP] be first, as the physician responsible for her at the primary care health center? And then we will add…
자문 의사: 여기서는 이미 마련되어 있는 것을 문서화하는 것이지만, 이러한 연락처가 아직 만들어지지 않은 유사한 사례가 있다면 다른 환자들이 혜택을 볼 수 있는 일종의 모델이 될 것입니다.
Consulting physician: Here we are kind of documenting what is already in place, but if we had a similar case where these contacts had not yet been created, this would serve as sort of a model from which other patients could benefit.
주치의: 환자의 주치의가 바뀌고 이전 주치의가 휴가를 떠난 후 다음 주치의가 반년 동안 진료하는 상황이 발생하면 매우 중요할 것입니다. 이런 경우 의사가 알 수 있도록 하는 것이 매우 중요합니다.
Chief physician: It would be very important if we had a situation where the patient’s personal physician is changed, the previous doctor would go on leave, and the next doctor would come for half a year. In such cases this has great importance, so that the doctor knows…
주치의: 이왕이면 환자도 서명하게 해주세요. .... 서명을 보면 여러 사람이 관련되어 있음을 알 수 있습니다....
Chief physician: Please let the patient also sign it, while you are at it. …. From the signatures one sees that there are several people involved….
협상된 매듭을 짓는 것은 의료 서비스에서 협상된 치료와 협업을 위한 새로운 도구를 만드는 데 있어 까다로운 단계입니다. 이러한 시도는 잠재적으로 환자를 배제하는 전통적인 형태의 전문가 간 의사소통 및 조정으로 쉽게 돌아갈 수 있습니다. 발췌문 2에서 주치의는 다른 의사들에게 치료 동의서에 환자의 서명이 필요하다는 점을 상기시켜야 했습니다.
Engaging in negotiated knotworking is a demanding step in the creation of new tools for negotiated care and collaboration in healthcare. Attempts easily slip back to the traditional forms of communication and coordination among professionals potentially excluding the patient. In Excerpt 2, the chief physician had to remind the other practitioners that also the patient’s signature was needed in the care agreement.
폭넓은 학습으로서의 전문성
Expertise as expansive learning
확장 학습은 변화를 위한 학습을 분석하고 촉진하는 독특한 방법을 제공합니다. 확장 학습 이론은 아직 존재하지 않는 새로운 활동 패턴을 학습하는 데 중점을 두며, 설계된 대로 학습합니다(Engeström 2015, 2016). 확장적 학습의 대상은 다양한 관점 사이에서 갈등하고, 협상하고, 혼성화하며, '야생에서' 개념을 종합적으로 형성하는 다중 목소리 학습 과정에 참여합니다(Engeström과 Sannino 2012).
Expansive learning provides a unique way of analyzing and promoting learning for change. The theory of expansive learning focuses on learning of new patterns of activity that are not yet there; they are learned as they are designed (Engeström 2015, 2016). The subjects of expansive learning are involved in a multi-voiced learning process in which they struggle, negotiate, and hybridize between the alternative perspectives and collectively form concepts ‘in the wild’ (Engeström and Sannino 2012).
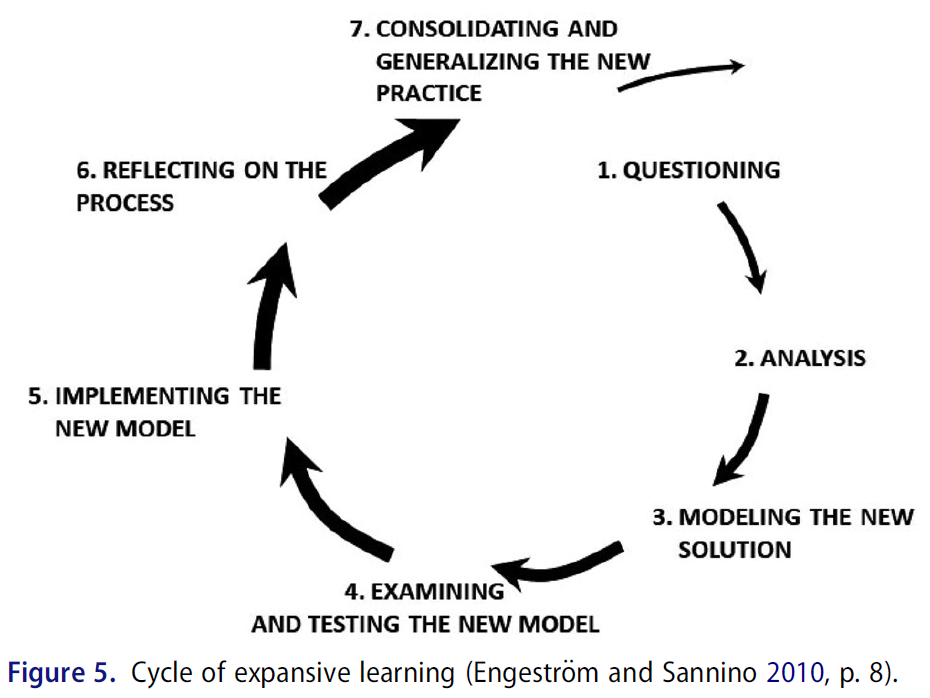
확장적 학습은 확장적 학습의 주기를 형성하는 학습 행동을 통해 진행됩니다(그림 5). 그림에서 굵어진 화살표는 프로세스에 참여하는 참여자의 수와 헌신적인 노력의 측면에서 증가하는 모멘텀을 나타냅니다. 확장 학습의 주기는 의도적인 개입 없이도 가끔 발생하지만, 이는 드문 경우입니다. 확장적 학습의 주기를 촉발하고, 지원하고, 분석하기 위해 형성적 개입 방법론이 개발되었습니다(Engeström 외. 2014).
Expansive learning proceeds by means of learning actions that form cycles of expansive learning (Figure 5). The thickening arrows in the figure indicate increasing momentum in terms of numbers and commitment of participants involved in the process. Cycles of expansive learning sometimes occur without deliberate intervention, but this is rare. A methodology of formative interventions has been developed to trigger, support, and analyze cycles of expansive learning (Engeström et al. 2014).
변화 실험실이라는 형성적 개입 방법은 1990년대에 주요 변화에 직면한 조직과 직장을 연구하기 위해 개발되었습니다(Engeström 외. 1996, Engeström과 Sannino 2010, Virkkunen과 Newnham 2012, Sannino와 Engeström 2017). 변화 실험실은 광범위한 학습을 촉발하고 지원하는 것을 목표로 합니다. 변화 실험실은 클리닉과 같은 지역 단위에 초점을 맞출 수도 있고, 더 큰 규모의 모순과 긴장을 해결하기 위해 여러 활동 시스템을 한데 모을 수도 있습니다.
A formative intervention method called Change Laboratory was developed in the 1990s for studying organizations and workplaces facing major transformations (Engeström et al. 1996; Engeström and Sannino 2010; Virkkunen and Newnham 2012; Sannino and Engeström 2017). Change Laboratory is aimed at triggering and supporting expansive learning. A Change Laboratory may focus on a local unit, such as a clinic, or bring together multiple activity systems to resolve larger-scale contradictions and tensions.
변화 실험실 방법을 사용하려면 연구자가 실제 업무 환경에서 인터뷰, 관찰, 비디오 녹화 등 경험적 자료를 수집해야 합니다. 이 자료에는 연구자가 새로운 활동 패턴을 모색하고 설계하기 위해 변화 실험실 세션 참가자들의 참여, 분석 및 협력 노력을 자극하기 위해 '거울'로 삼을 수 있는 중요한 사건, 장애 및 문제가 포함되어 있으며, 연구자는 이 중에서 발췌하여 제공합니다.
The Change Laboratory method requires that the researchers collect empirical material, e.g. interviews, observation, and video-recordings, from authentic workplace contexts. The material includes critical incidents, disturbances, and problems of which the researcher selects and provides extracts for a ‘mirror’ to stimulate involvement, analysis, and collaborative efforts among participants in Change Laboratory sessions to seek and design new patterns of activity.
일반적인 체인지 랩 개입은 6~10개의 세션으로 진행됩니다.
- 참가자는 먼저 연구자가 선정한 비디오 발췌본을 시청하여 기존 활동 방식에 의문을 제기하는 학습 행동을 유도합니다.
- 그런 다음 참가자들은 역사적, 경험적 분석을 통해 문제와 그 체계적 원인, 가능한 해결책 또는 해결책을 논의합니다. 문제, 원인 및 제안된 해결책은 필자가 화이트보드나 플립 차트에 기록합니다.
- 그런 다음 참가자들은 모델링 학습 활동에 참여하여 근위 개발 영역과 새로운 활동 모델을 공동으로 초안을 작성합니다.
- 새로운 모델의 목표와 내용을 논의하고 모델을 검토하고 테스트하는 활동에 해당하는 세부적인 변경 및 개선 제안이 이루어집니다.
- 참가자는 모델을 실행하는 학습 행동에 해당하는, 활동의 실질적인 변화를 계획하고 실행합니다.
- 프로세스는 프로세스를 반성하는 행동으로 수행한 작업을 검토하여 평가합니다.
- 결과의 통합 및 일반화는 변화 실험실 개입이 끝날 무렵에 시작되며 일반적으로 그 이후에도 계속됩니다.
A typical Change Laboratory intervention proceeds through 6–10 sessions.
- Participants first view video excerpts selected by the researchers to elicit the learning action of questioning the existing mode of activity.
- Next, participants discuss the problems, their systemic causes, and possible remedies or solutions – performing historical and empirical analysis. Problems, causes, and suggested solutions are written up on whiteboards or flip charts by a scribe.
- Then, participants engage in the learning action of modeling, jointly drafting a zone of proximal development and a new model for their activity.
- The aims and contents of the new model are discussed, and detailed changes and improvement suggestions are made, corresponding to the action of examining and testing the model.
- Participants plan and execute practical changes in the activity, corresponding to the learning action of implementing the model.
- The process is assessed by examining the work accomplished in an action of reflecting on the process.
- Consolidation and generalization of the outcomes are initiated toward the end of a Change Laboratory intervention and typically continue after it.
헬싱키에서 일차 의료와 전문 병원 진료 간의 협상된 업무 방식 개발에 관한 핀란드 연구(Engeström 외. 2003; Engeström 2018)는 의료 환경에서 변화 실험실을 성공적으로 구현한 풍부한 설명을 제공합니다. 실제 상황에서 일차 진료와 이차 진료 사이의 환자 치료의 세분화에 대한 데이터를 수집하고, 9번의 Change Laboratory 세션을 진행했으며, 환자 및 환자 치료에 관여하는 실무자와 함께 10개의 환자 사례를 연속적으로 분석했습니다.
A Finnish study on the development of a negotiated way of working between primary health care and specialized hospital care in Helsinki (Engeström et al. 2003; Engeström 2018) provides a rich description of a successful implementation of Change Laboratory in healthcare settings. Data were gathered on the fragmentation of patient care between primary and secondary care in the real-life contexts, nine Change Laboratory sessions were conducted and ten patient cases were jointly analyzed in successive sessions with the patients and the practitioners involved in their care.
여러 차례에 걸친 확장적 학습을 통해 의사와 환자는 여러 만성 질환을 앓고 있는 환자를 치료하는 과정에서 파편화를 발견한 한 의사가 시작한 치료 계약이라는 새로운 도구를 만들어냈습니다(Kerosuo와 Engeström 2003). 계약서의 첫 번째 초안은 시작 의사와 환자 간에 협상이 이루어졌습니다. 그런 다음 초안을 환자의 치료에 관여하는 다른 의료진에게 보내 당사자 간의 협상을 거쳤습니다. 치료 합의서에는 여러 대상자의 진단과 주요 관심사가 요약되어 있고 치료 계획이 설명되어 있습니다. 또한 새로운 상황이 발생하고 변경 사항이 있을 때 서로에게 최신 정보를 제공하는 방법도 설명했습니다. 치료 동의서는 환자를 포함한 주요 당사자가 서명했습니다. 치료 동의서 도구에서 중요한 두 가지 도구, 즉 치료 지도와 환자의 치료 달력이 추가로 개발되었습니다. 두 가지 모두 의사와 환자가 공동으로 작성하고 협상했습니다.
In multiple cycles of expansive learning, practitioners and patients generated a new instrument called the care agreement initiated by a physician who noticed fragmentation in the care of a patient with multiple chronic illnesses (Kerosuo and Engeström 2003). The first draft of the agreement was negotiated between the initiating physician and the patient. The draft was then sent to other healthcare practitioners involved in the patient’s care and negotiated among the parties. The care agreement summarized the diagnoses and key concerns of the different subjects and outlined their plans of care. It also explicated the ways they kept each other up-to-date when new developments occurred and changes were made. The care agreement was signed by the key parties, including the patient. Two additional instruments, important in the care agreement instrumentality were developed, namely that of a care map and a care calendar of the patient. Both were collaboratively constructed and negotiated by the physicians and the patients.
확장적 학습 주기는 세 가지 수준에서 식별되고 지원될 수 있습니다.
- 환자 치료에서 상호 연결된 활동 시스템 간에 새로운 기본 모델을 생성하고 구현하는 데는 일반적으로 몇 년이 걸립니다(예: Engeström 외. 2007).
- 중간 수준은 변화 실험실 개입의 도움을 받아 집중적인 지역적 변화로 구성되며, 몇 개월이 소요됩니다(예: Engeström 외. 2013).
- 가장 작은 규모의 확장 학습 미니 사이클은 단일 개입 세션 또는 이와 유사한 제한된 에피소드로 구성됩니다(예: 누미조키 외. 2018).
Expansive learning cycles may be identified and supported at three levels.
- To generate and implement a new foundational model between interconnected activity systems in patient care typically takes several years (e.g. Engeström et al. 2007).
- An intermediate level consists of a focused local transformation with the help of a Change Laboratory intervention, requiring several months (e.g. Engeström et al. 2013).
- The smallest scale of mini-cycles of expansive learning consists of single intervention sessions or similar restricted episodes (e.g. Nummijoki et al. 2018).
변화 실험실 중재는 핀란드(Engeström 2018), 덴마크(Skipper 외. 2016), 브라질(Vilela 외. 2020; Grilo Diniz 외. 2020, 보도 중), 영국(Reid 외. 2015; Morris 외. 2020, 보도 중)의 다양한 의료 환경에서 수행 및 보고되었습니다.
Change Laboratory interventions have been carried out and reported in various medical settings in Finland (Engeström 2018), Denmark (Skipper et al. 2016), Brazil (Vilela et al. 2020; Grilo Diniz et al. 2020, in press), and the United Kingdom (Reid et al. 2015; Morris et al. 2020, in press).
의학교육을 위한 교훈
Lessons for medical education
이 글에서는 의학교육의 맥락에서 활동 이론과 확장적 학습 이론을 소개합니다(Engeström 2015, 2018). 확장적 학습은 의료 시스템의 복잡성과 모순을 분석하기 위한 개념적 프레임워크와 다양한 의료 부서와 환자가 함께 협력하여, 그들이 직면한 긴장과 장애물에 대한 새롭고 창의적인 해결책을 찾는 형성적 개입 방법을 제공합니다. 이러한 유형의 접근 방식은 특히 의료계가 직면한 문제를 탐구하는 데 적합합니다(Barnett 외. 2012; Braithwaite 2018; Engeström 2018; Bleakley 2020, 보도 중).
This article introduces activity theory and the theory of expansive learning in the context of medical education (Engeström 2015, 2018). Expansive learning provides a conceptual framework for analyzing the complexities and contradictions of systems of health care and methods for formative interventions where the participants in different healthcare units and patients work together to find new, creative solutions to the tensions and obstacles they face. This type of approach is particularly well suited for exploring the challenges healthcare is facing (Barnett et al. 2012; Braithwaite 2018; Engeström 2018; Bleakley 2020, in press).
협력적이고 혁신적인 전문 지식으로 전환하는 환경에서 의학교육은 미래의 의료 관행을 형성하는 데 공동의 책임이 있습니다. 의료 행위는 그것이 운영되는 더 넓은 커뮤니티의 요구에 부응할 때만 발전할 수 있습니다. 의대생들은 강의실을 넘어 환자를 포괄적으로 치료하고 의사가 환자의 전인적 치료를 옹호하는 실제 의료 환경에서 교육을 받는 경우가 점점 더 많아져야 합니다. 이에 따라 일터에서 일하는 모든 의료인은 의료 교육자가 되어야 합니다. 이는 의료, 고객 커뮤니티, 의학교육이라는 상호 연결된 활동 시스템 간의 협업과 소통을 강화해야만 달성할 수 있습니다.
In the landscape of transition toward collaborative and transformative expertise, medical education becomes co-responsible for shaping future medical practice. Medical practice can only evolve in response to the needs of the broader communities within which it operates. Beyond classrooms, medical students should increasingly receive education in authentic healthcare settings where patients are treated comprehensively and practitioners advocate for their holistic care. Correspondingly, all medical practitioners in workplaces become medical educators. This can only be achieved by intensifying collaboration and communication between the interconnected activity systems of healthcare, its client communities, and medical education.
의학교육의 새로운 원형과 패러다임, 즉 대상 지역사회, 의료기관, 의과대학, 학생, 의료 전문가, 환자 및 기타 이해관계자 간의 변화 연합이 등장할 것입니다(Coburn and Penuel 2016; Sannino 2020). 형성적 개입의 방법론, 특히 변화 실험실 방법은 이러한 변화 연합을 구축하고 분석하는 데 중요한 자원이 될 수 있습니다(Sannino 외. 2016). 이러한 새로운 형태의 의학교육에 대한 중재주의적 연구가 시급히 필요합니다.
A new prototype and paradigm of medical education will emerge, namely a transformation coalition between target communities, healthcare organizations, medical schools, students, healthcare professionals, patients, and other stakeholders (Coburn and Penuel 2016; Sannino 2020). The methodology of formative interventions, especially the Change Laboratory method, may serve as an important resource for building and analyzing such transformation coalitions (Sannino et al. 2016). Interventionist research in these new forms of medical education is urgently needed.
Using activity theory to transform medical work and learning
PMID: 32715847
Abstract
This article introduces key concepts of activity theory and expansive learning. Expansive learning builds on the foundational ideas of the cultural-historical activity theory (CHAT). It is a research approach designed for studying the complexities and contradictions in authentic workplace environments. Change Laboratory is a formative intervention method developed for studying workplaces in transition and for stimulating collaborative efforts to design improved patterns of activity. We present concrete examples of formative interventions in healthcare, where good patient care was compromised by the fragmentation of care and disturbances in collaboration between the healthcare experts. This implies that physicians are challenged to develop collaborative and transformative expertise. We present three spearheads into a zone of proximal development, representing opportunities for change of medical expertise: (1) reconceptualizing expertise as object-oriented and contradiction-driven activity systems, (2) pursuing expertise as negotiated knotworking, and (3) building expertise as expansive learning. While medical expertise needs to expand, medical education must also look for ways to evolve and meet the challenges of the surrounding society. We call for adopting an interventionist approach for developing medical education and intensifying collaboration with the practitioners in healthcare units, their patients, and target communities.
Keywords: Activity theory; change laboratory; expansive learning; formative intervention; healthcare; medical education.
'Articles (Medical Education) > 교육이론' 카테고리의 다른 글
| 분산된 인지: 보건의료전문직교육에 이론적 통찰과 실용적 적용: AMEE Guide No. 159 (Med Teach, 2023) (0) | 2023.10.10 |
|---|---|
| 마스터의 집 해체하기: HPE에서 형평성과 사회적 정의의 앎의 새로운 방식 (Adv Health Sci Educ Theory Pract. 2020) (0) | 2023.08.01 |
| 보건 전문가를 위한 교육학으로서의 변혁적 학습: 스코핑 리뷰(Med Educ, 2019) (0) | 2023.05.04 |
| 임상추론의 생태학적 설명(Acad Med, 2022) (0) | 2023.02.03 |
| 사회인지진로이론(Social Cognitive Career Theory) (0) | 2023.01.07 |