테크놀로지 강화 학습 (Understanding Medical Education Ch10)
Technology‐enhanced Learning
Rachel H. Ellaway
Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Alberta, Canada

소개
Introduction
의학 교육에는 오랜 역사를 지닌 많은 테크놀로지(예: 교과서, 모형, 삽화)가 있지만, 현대에 '테크놀로지'라는 용어는 일반적으로 디지털 도구 및 시스템을 지칭하는 것으로 이해됩니다. 실제로 최근 몇 년 동안 개인용 디지털 기기가 급증하면서 미래의 의사를 양성하는 데 있어 (디지털) 테크놀로지는 거의 유비쿼터스에 가까운 존재가 되었습니다. 독자들이 이 장을 디지털 테크놀로지뿐만 아니라 의학교육에서 사용되는 모든 테크놀로지의 맥락에서 생각해 보시기 바랍니다. 테크놀로지 사용과 의학교육 관행 사이의 다양한 교차점을 완전히 다루는 것은 한 장의 범위를 넘어서는 것이므로 이 책 전체에 제시된 자료에 반영된 테크놀로지 사용을 고려하는 것도 독자들에게 권장합니다.
While there are many technologies (such as textbooks, models, and illustrations) that have a long pedigree in medical education, the contemporary use of the term ‘technology’ is generally understood as referring to digital tools and systems. Indeed, there has been a proliferation of personal digital devices in recent years, to the point that (digital) technologies have become a near‐ubiquitous presence in the training of tomorrow’s doctors. I invite readers to consider this chapter in the context of all technology use in medical education, not just digital technologies. To fully address the multitude of intersections between technology use and medical education practices is beyond the scope of a single chapter so I would also encourage readers to consider technology use as it is reflected in the material presented throughout this volume.
저는 'e-러닝'이라는 보다 대중적이지만 다소 문제가 있는 개념보다는 '테크놀로지 강화 학습'(TEL)이라는 용어를 주요 참조 프레임으로 사용합니다. TEL 개념의 핵심은 테크놀로지의 매개 역할에 초점을 맞추는 것입니다. 교사는 가르치고 학습자는 배우며, 테크놀로지를 사용함으로써 변화되는 것은 바로 이러한 일을 수행하는 방법과 그 이후의 과정입니다. 이 주제를 탐구하면서 저는 의학교육에서 테크놀로지 사용을 평가하기 위한 다양한 이론적 틀을 고려하고, 이를 바탕으로 의학교육에서 테크놀로지 강화 학습을 개발, 사용 및 평가하기 위한 일련의 기법을 제시할 것입니다. 이를 통해 현대 의학교육에서 테크놀로지 사용과 관련된 입장, 관행, 기회 및 과제에 대한 비판적 검토를 제공하는 것이 저의 목표입니다.
I use the term ‘technology‐enhanced learning’ (TEL) as my main frame of reference rather than the more popular but rather problematic concept of ‘e‐learning’. Central to the concept of TEL is a focus on the mediating role of technology. Teachers teach and learners learn; it is how they do these things (and what follows) that is changed by their use of technology. In exploring this topic, I will consider a range of theoretical frames for appraising the use of technology in medical education, and from these I will set out a series of techniques for developing, using, and evaluating technology‐enhanced learning in medical education. My goal in doing so is to provide a critical review of the positions, practices, opportunities, and challenges associated with using technology in contemporary medical education.
의학교육에서의 테크놀로지 사용
Technology Use in Medical Education
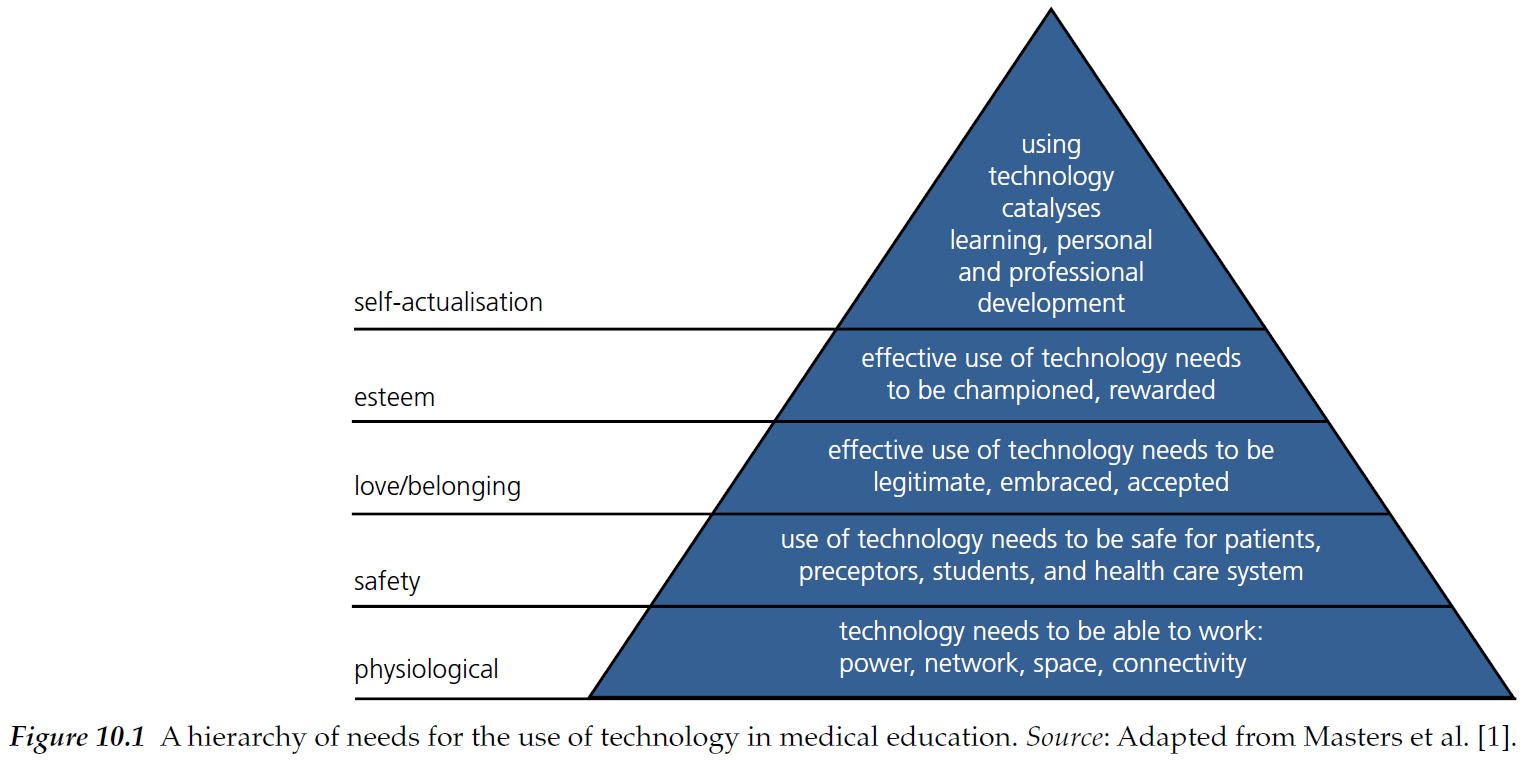
현대 의학교육에는 장치(노트북 컴퓨터, 태블릿, 모바일 장치 등) 및 주변 장치(프린터, 카메라, 키보드 등), 소프트웨어(이 장을 작성하는 데 사용한 워드 프로세싱 및 일러스트레이션 도구 등) 및 앱(모바일 장치 및 태블릿용), 서비스(Google 및 Skype에서 제공하는 것 등), 디지털 콘텐츠(YouTube 및 Wikipedia에서 제공하는 것 등), 소셜 미디어(Twitter 및 Facebook 등) 등 매우 많은 테크놀로지가 사용되고 있습니다. 이러한 테크놀로지 중 일부는 의료 교육 기관에서 제공하지만(예: 학습 관리 시스템), 대부분은 학습자(예: 노트북 및 모바일 장치)가 제공하거나 의료 교육과 직접적인 관련이 거의 또는 전혀 없는 제3자(예: Google 및 Wikipedia)가 제공합니다. 따라서 테크놀로지를 의학교육 또는 의학교육자에게 특정한 것으로 논의하는 것은 어려울 수 있으며, 다양한 출처를 고려할 때 평가하거나 지시하기 어려울 수 있습니다. 학생 또는 교수진의 노트북이나 모바일 기기는 교육 및 학습 목적으로 사용될 수 있지만, 다른 많은 목적과 다양한 맥락에서 사용됩니다. 의료 교육의 맥락에서 이러한 교차성에 대해 생각해 보는 것이 중요한데, 예를 들어 교사와 학습자가 소셜 미디어를 사용할 때 사회적 및 교육적 이점이 다소 모호해질 수 있습니다. 우리는 직접적으로 상호작용하는 테크놀로지에 더 많은 주의를 기울이는 경향이 있으며, 이러한 테크놀로지에 의존하는 많은 지원 테크놀로지의 중요한 역할은 종종 잊어버립니다. 네트워크 및 전력의 가용성, 보안 및 로그인 서비스 제공, 강력한 방식으로 시스템을 호스팅할 수 있는 능력 등은 의학교육에서 테크놀로지를 사용하기 위한 기반을 제공하는 데 필수적인 요소입니다. 비용, 분쟁, 자연재해 등의 이유로 이러한 기반 테크놀로지를 쉽게 사용할 수 없는 의과대학은 테크놀로지를 더 임시적으로 사용하는 경향이 있습니다. 매슬로우의 욕구위계설에 따라 의료 교사와 학습자의 테크놀로지에 대한 의존도를 '욕구 계층'(그림 10.1)[1]의 관점에서 이해할 수 있습니다. 여기서 중요한 교훈은 의존적 요소가 불확실하거나 부재할 경우 의료 교육에서 테크놀로지 사용이 손상되거나 약화될 수 있다는 것입니다. 여기에는 기능 및 안전 요소뿐만 아니라 의학교육에서 테크놀로지 사용의 정당성 및 수용 가능성(또는 학생이 침대 옆에서 스마트폰을 사용하는 것과 같은 특정 테크놀로지 사용)에도 달려 있습니다.
There are a great many technologies being used in contemporary medical education, including devices (such as laptop computers, tablets, and mobile devices) and their peripherals (such as printers, cameras, and keyboards), software (such as the word processing and illustration tools that I used to write this chapter) and apps (for mobile devices and tablets), services (such as those offered by Google and Skype), digital content (such as that offered by YouTube and Wikipedia), and social media (such as Twitter and Facebook). While some of these technologies are provided by institutions of medical education (such as learning management systems), many are provided by learners (such as laptops and mobile devices), or by third parties with little or no direct focus on medical education (such as Google and Wikipedia). It can therefore be challenging to discuss technology as something specific to medical education or medical educators, and difficult to appraise or direct given its diverse provenance. Although a student or faculty laptop or mobile device can be used for teaching and learning purposes, it is also used for many other purposes and in many other contexts. It is important to think about this intersectionality in the context of medical education, exemplified for instance by teacher and learner use of social media where the social and instructional benefits can become rather blurred. We tend to pay more attention to the technologies with which we interact directly and often oblivious to the critical role of the many supporting technologies they depend on. Essential if unexciting factors such as availability of networks and electrical power, the provision of security and sign‐ in services, and the ability to host systems in a robust way are necessary to provide a foundation for the use of technology in medical education. Medical schools that do not have these foundational technologies readily available (for instance because of cost, conflict, or natural disasters) tend to make more tentative use of technologies. Drawing loosely from Maslow, the dependence of medical teachers and learners on their technologies can be understood in terms of a ‘hierarchy of needs’ (Figure 10.1) [1]. The key lesson here is that the use of technology in medical education can be compromised or undermined if its dependent factors are uncertain or absent. Not only does this include functional and safety factors, it also depends on the legitimacy and acceptability of using technology, (or particular uses of technology such as students having smartphones at the bedside) in medical education.
의학 교육에서 테크놀로지 사용에 관한 분업에 유의하는 것도 중요합니다. 일부 테크놀로지는 학습자와 교수자 모두가 사용하지만 사용 방식이 다릅니다. 예를 들어, 온라인 포트폴리오와 학습 관리 시스템은 사용자 역할에 따라 서로 다른 도구와 보기를 제공합니다. 다른 테크놀로지들은 학습자 또는 교사에게 어느 정도 특화된 경향이 있습니다. 예를 들어, 교사는 PowerPoint와 같은 도구를 광범위하게 사용하는 반면, 학습자는 참고 자료를 훨씬 더 많이 사용하는 경향이 있습니다.
It is also important to note the division of labour regarding the use of technology in medical education. Some technologies are used by both learners and teachers but in different ways. For instance, online portfolios and learning management systems present different tools and views depending on the user role. Other technologies tend to be more or less learner, or teacher, specific. For instance, teachers may make extensive use of tools like PowerPoint, while learners tend to make much greater use of reference materials.
이러한 예비 관찰 결과를 종합해 보면 의학교육의 맥락에서 테크놀로지 사용이 절대적으로 효과적이거나 그렇지 않다고 말할 수 없다는 것이 분명해집니다. 그 유용성은 과제, 테크놀로지, 개인 및 상황에 따라 달라집니다. 따라서 의학교육에서 사용되는 테크놀로지와 그 활용의 다양성을 고려할 때 간결하고 일반화할 수 있는 방식으로 실습을 안내하는 것은 압도적인 작업처럼 보일 수 있습니다. 그러나 의학교육에서 테크놀로지 사용과 관련된 문제에 대한 포괄적인 모델을 설정하기 위해 활용할 수 있는 몇 가지 이론적 프레임워크가 있습니다.
Drawing these preliminary observations together, it becomes clear that we cannot say that technology use is, or is not, effective in any absolute way in the context of medical education. Its utility depends on the task, the technology, the individual, and their circumstances. Given the plurality and diversity of technologies and their uses in medical education it may therefore seem like an overwhelming task to guide practice in both a succinct and generalisable way. However, there are several theoretical frames we can draw on to set out an inclusive model of issues in and around technology use in medical education.
학습을 위한 테크놀로지
Technologies for Learning
의학교육은 상호 연결된 일련의 활동(예: 강의, 술기 실습, 문제 기반 학습, 시험, 침상 학습 등)으로 이해할 수 있습니다. 활동 이론[2]의 개념을 사용하여 이러한 활동을 분석할 수 있는데, 이 이론의 핵심은 활동은 매개되며, 활동은 그것을 매개하는 인공물에 의존하고, 그것에 의해 형성된다는 것입니다. 예를 들어,
- 10여 년 전만 해도 많은 의과대학에서 강의, 실습 및 기타 학습 세션에서 학습자에게 종이 유인물을 제공하는 것이 일반적인 관행이었지만, 이제는 전자적으로 노트를 제공하거나 심지어 노트 없이 교사의 PowerPoint 슬라이드에 액세스하는 것이 훨씬 더 일반적입니다.
- 한때 주석이 달린 유인물과 종이 메모로 가득했던 링 바인더는 대부분 전자 파일과 문서로 대체되었습니다.
따라서 이제 컴퓨터와 컴퓨터가 지원하는 다양한 도구가 학습자의 개인 지식 기반 생성 및 사용을 매개한다고 말할 수 있습니다.
Medical education can be understood as sequences of interconnected activities (e.g. lectures, skills labs, problem‐based learning, exams, bedside learning, etc.). We can analyse these activities using concepts from activity theory [2], a central tenet of which is that activities are mediated; they both depend on mediating artefacts and are shaped by them. For example, whereas 10 or more years ago it was normal practice for many medical schools to provide their learners with paper handouts for lectures, labs, and other learning sessions, it is now much more common for notes to be provided electronically or even that there are no notes, simply access to the teacher’s PowerPoint slides. The once ubiquitous ring binder full of annotated handouts and paper notes has been largely replaced by electronic files and documents. We can say, therefore, that computers and the various tools they support now mediate learners’ creation and use of their personal knowledgebase.
의학교육의 모든 활동을 나열하고 각각의 활동을 매개하는 특정 테크놀로지를 설명하는 대신, 의학교육에서의 기능적 역할과 이와 관련된 다양한 매개 테크놀로지의 관점에서 다양한 유형의 활동을 고려할 수 있습니다. 상자 10.1을 참조하십시오.
Rather than listing all activities in medical education and describing specific mediating technologies within each, we can instead consider different types of activity in terms of their functional role in medical education and different mediating technologies associated with them. See Box 10.1.

의학교육에는 분명히 많은 활동 유형과 이를 중재하는 데 사용할 수 있는 많은 테크놀로지가 있습니다. 또한 일부 테크놀로지(예: 학습 관리 시스템)은 두 가지 이상의 활동을 중재하는 데 사용될 수 있으며, 특정 세션(수업, 로테이션, 실습 등)에는 여러 활동 유형이 사용되며 여러 테크놀로지가 중재할 수 있습니다. 따라서 우리는 단일 활동과 매개 테크놀로지에만 관심을 가져서는 안 되며, 의학교육의 표준인 활동과 매개 테크놀로지가 얽혀 있는 클러스터도 고려해야 합니다. 이를 통해 테크놀로지 매개가 다른 종류의 매개와 얽혀 있는 '블렌디드 러닝'이라는 개념으로 이어집니다. 예를 들어, 디지털 테크놀로지를 사용하여 대면 수업 환경에서 자료를 찾거나 자료를 만드는 것입니다. 블렌디드 학습은 학습 자체가 아니라 학습을 지원하기 위해 다양한 매개 요소를 사용하는 것임을 분명히 해야 합니다. TEL을 단독으로 사용하는 것보다 혼합하여 사용하는 것이 TEL을 단독으로 사용하는 것보다 더 나은 학습 결과를 가져온다는 증거가 있습니다[4].
Clearly there are many activity types in medical education and many technologies that can be used to mediate them. Moreover, some technologies can be used to mediate more than one kind of activity (such as learning management systems), and any given session (class, rotation, lab, etc.) may employ many activity types and be mediated by many technologies. We should not therefore be concerned solely with single instants of activity plus mediating technology, we should also consider the entangled clusters of activities and mediating technologies that are the norm in medical education. This leads us to the concept of ‘blended learning’ where technology mediation is entangled with other kinds of mediation. For instance, using digital technologies to look things up or create materials within a face‐to‐face class setting. We should be clear that it is not the learning that is blended, rather it is the use of different mediating components in support of learning that is blended. There is evidence to suggest that blended uses of TEL rather than isolated uses of TEL lead to better learning outcomes than using TEL on its own [4].
기기는 일반적으로 한 번에 한 사람만 사용하도록 설계되지만, 테크놀로지 사용은 사회적 맥락에서 이루어지며 상황에 따라 다른 사람이 보고 해석합니다. 따라서 학습자 및 실무자의 테크놀로지 사용은 전문적인 행동으로 볼 수 있습니다. 실제로 학습자의 컴퓨터, 태블릿, 스마트폰 사용은 학습자가 강의실이나 침대 옆에서 기기를 사용하도록 허용하거나 장려해야 하는지에 대한 논쟁에서 전문직업성에 대한 우려의 초점이 되어 왔습니다. 강의에서 테크놀로지를 사용하는 것은 이제 보편화되었지만, 학습자가 침대 옆에서 디지털 테크놀로지를 사용하는 것은 여전히 논쟁의 여지가 있습니다. TEL과 전문성 사이의 교차점은 '디지털 전문직업성'의 문제로 간주할 수 있습니다[5]. 이는 테크놀로지를 어디에서 사용해야 하고 사용하지 말아야 하는지에 대한 문제일 뿐만 아니라, 테크놀로지가 어떻게 사용되는지, 그리고 테크놀로지의 사용이 개인의 삶에서 개인적 측면과 직업적 측면을 어떻게 모호하게 만들 수 있는지에 초점을 맞추고 있습니다. 대표적인 예로 학습자와 실무자의 소셜 미디어 사용을 들 수 있습니다. 페이스북이나 트위터와 같은 도구는 다른 사람들과 소통할 수 있는 비할 데 없는 능력을 제공하지만, 개인, 특히 전문가로서 비공개로 유지되어야 할 삶의 측면을 공개함으로써 실수를 범할 수 있는 수단을 제공하기도 합니다. 기밀 정보 공개, 잠재적으로 위험한 상황에 처한 자신 또는 타인의 이미지 공유, 비전문적인 의견과 의견 공유 등, 디지털 미디어를 전문적으로 사용하는 능력은 미래의 의사를 양성하는 데 있어 필수적인 요소가 되었습니다. 박스 10.2를 참조하십시오.
Although devices are usually designed to be used by one person at a time, technology use is enacted in a social context; it is seen and interpreted by others according to circumstance. Learner and practitioner uses of technologies can therefore be seen as professional behaviours. Indeed, learner use of computers, tablets, and smartphones has been a focus of professionalism concerns reflected in debates over whether learners should be allowed or encouraged to use their devices in lectures or at the bedside. While the use of technology in lectures is now commonplace, learners’ use of digital technologies at the bedside is still a matter of contention. The intersections between TEL and professionalism can be considered as a matter of ‘digital professionalism’ [5]. This is not just about where technologies should and should not be used, it also focuses on how technologies are used and how the use of technologies can blur personal and professional aspects of individuals’ lives. A key example of this is learner and practitioner use of social media. Tools such as Facebook and Twitter afford an unparalleled ability to communicate with others, but they also create the means by which individuals can misstep by making aspects of their lives public, particularly as professionals, that should have been kept private. Whether concerned with disclosing confidential information, sharing images of oneself or others in potentially compromising situations, or sharing unprofessional opinions and comments, the ability to use digital media in a professional way has become part of the training of tomorrow’s doctors. See Box 10.2.
상자 10.2 중점 사항: 디지털 전문직업성
BOX 10.2 FOCUS ON: Digital professionalism
보건 전문직 학습자, 교사, 실무자는 디지털 테크놀로지 사용을 통해 새로운 기회와 위험에 노출됩니다.
- 기회에는 전문 네트워크를 형성하고 유지할 수 있는 능력과 필요에 따라 정보에 액세스하고 공유할 수 있는 능력이 포함됩니다.
- 위험에는 개인과 직업의 경계가 모호해지고 직업적 평판에 대한 위협에 더 많이 노출되는 것이 포함됩니다.
제도적 대응은 종종 테크놀로지 사용을 금지하거나 제한하는 것이었는데, 이는 테크놀로지 사용의 이점뿐만 아니라 위험도 제한합니다. 디지털 전문직업성은 의료 전문직업성 의 원칙에 기반하여 테크놀로지 사용을 보다 공평한 관점에서 바라봅니다:
Health professional learners, teachers, and practitioners are exposed to new opportunities and risks through their use of digital technologies.
- Opportunities include the ability to form and sustain professional networks and the ability to access and share information on demand.
- Risks include a blurring of personal and professional boundaries and a greater exposure to threats to professional reputations.
The institutional response has often been to proscribe or limit the use of technologies, which limits the benefits of technology use as well as the risks. Digital professionalism builds on the principles of medical professionalism to frame technology use in a more equable light:
디지털 미디어는 의료 전문직업성에 대한 본질적인 위협이 아닙니다. 전문가는 환자 치료, 연민, 이타주의, 신뢰성의 원칙을 지지하는 방식으로 긍정적인 목적으로 디지털 미디어를 사용해야 합니다. 전문가는 디지털 미디어와의 관계가 형성되는 특성을 인식하고 신중하고 윤리적이며 책임감 있게 진료할 수 있는 역량을 유지해야 합니다. [5]
Digital media are not an intrinsic threat to medical professionalism. Professionals should use digital media for positive purposes in ways that support principles of patient care, compassion, altruism, and trustworthiness. Professionals should be aware of the shaping nature of their relationships with digital media and they should maintain the capacity for deliberate, ethical, and accountable practice. [5]
디지털 전문직업성은 다음 사항에 주의를 기울여 가르치고, 모델링하고, 평가할 수 있습니다:
- 숙련도: 테크놀로지를 효과적이고 안전하며 책임감 있게 사용할 수 있는 능력.
- 평판: 자신의 행동과 다른 사람의 행동에 대한 대응을 통해 자신의 직업적 평판을 유지할 수 있는 능력.
- 책임감: 전문적으로 건전한 테크놀로지 사용 방법을 개발 및 유지하고, 다른 사람들에게 이를 가르치고, 모델링하고, 장려하는 능력입니다.
Digital professionalism can be taught, modelled, and assessed by attending to:
- Proficiency: the ability to use technologies effectively, safely, and responsibly.
- Reputation: the ability to maintain one’s professional reputation both through their own actions and in responding to the actions of others.
- Responsibility: developing and sustaining professionally sound ways of using technologies, and teaching, modelling, and encouraging this in others.
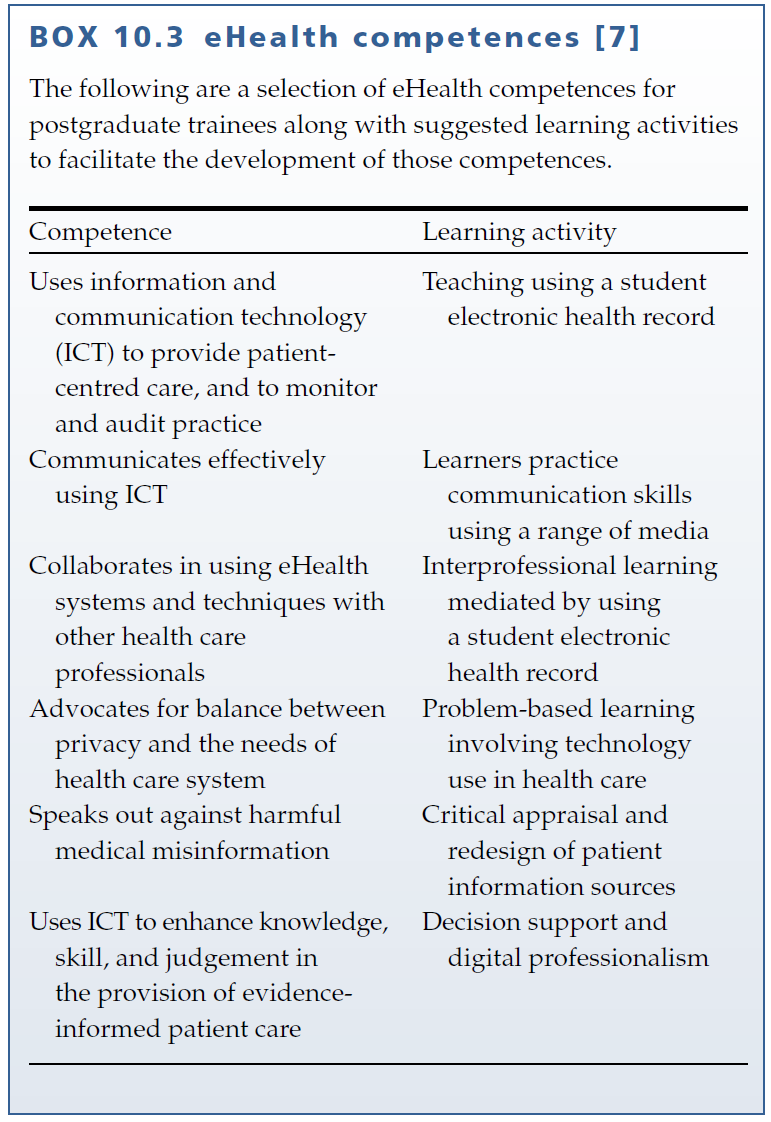
디지털 전문직업성은 우리가 고려해야 할 테크놀로지, 의료 교육 및 진료의 유일한 교차점은 아닙니다. 전자 의료 기록, 의료 영상 보관 및 통신 시스템(PACS), 처방전 및 주문 입력 시스템과 같은 디지털 테크놀로지가 점점 더 의료 행위를 매개하고 있으며, 이는 학습자가 디지털 환경에서 실습할 수 있도록 준비하는 것이 의학교육에서 점점 더 중요한 과제가 되고 있음을 의미합니다. 이러한 테크놀로지는 임상 의료행위뿐만 아니라 학습을 매개할 수 있으며, 이를 위해 '메시지로서 매개하는 테크놀로지'라고 부릅니다. [6] 의학교육에 대한 시사점은 이러한 테크놀로지를 학습을 매개하는 데 사용하는 스킬을 개발하는 것과 함께 이러한 테크놀로지를 사용하는 스킬을 개발해야 한다는 것입니다. 명확히 말하자면, 이는 운영자 테크놀로지를 개발하는 것이 아니라 임상 활동 및 워크플로우 내에서 디지털 도구와 정보를 사용하는 원리를 이해하는 것입니다. 상자 10.3을 참조하십시오.
Digital professionalism is not the only intersection of technology, medical education, and practice that we need to consider. Digital technologies such as electronic health records, picture archiving and communication systems (PACS), formularies, and order entry systems are increasingly mediating the practice of medicine, which means that preparing learners to practice in a digital environment is a growing issue for medical education. These technologies can mediate learning as well as clinical practice, and to that end, have called them ‘medium‐as‐message technologies’. [6] The implication for medical education is that developing skills in the use of these technologies needs to be combined with their use for mediating learning. To be clear, this is more than developing operator skills, but rather about understanding the principles of using digital tools and information within clinical activities and workflows. See Box 10.3.
이 섹션을 마무리하기 전에, 현대 학습자들이 모두 학습에 테크놀로지를 사용하는 데 열중한다는 널리 퍼진 가정에 대해 한 마디 주의를 기울일 필요가 있습니다. '넷 세대' 및 '디지털 네이티브'와 같은 용어는 디지털 시대의 학습자 및 학습의 본질적인 변화를 암시하기 위해 만들어졌습니다[8]. 그러나 학습자 자체에 큰 차이가 있다는 증거는 거의 없으며, 오히려 학습자와 교사 등 다른 사람들이 사용하는 테크놀로지의 변화로 인한 기회와 위험에 대한 증거가 더 많습니다. 특정 집단이나 학급에는 다양한 사람들이 존재한다는 것이 현실입니다.
- 학습을 위해 테크놀로지를 사용하고 탐구하는 데 관심이 있는 사람,
- 인쇄물이나 필기 자료와 같은 전통적인 미디어를 선호하는 사람,
- 일부 테크놀로지는 좋아하지만 다른 테크놀로지는 사용하지 않는 사람, 또는
- 학습에 사용하는 미디어에 무관심한 사람 등
테크놀로지에 대한 학습자의 다양한 태도와 학습자가 다양한 테크놀로지를 다양하게 활용할 수 있다는 점을 고려해야 합니다.
Before closing this section, it is important to add a word of caution regarding the widespread assumption that contemporary learners are all keen on using technology in their studies. Terms such as the ‘Net Generation’ and ‘digital natives’ have been coined to allude to some intrinsic change in the nature of learners and learning in the digital age [8]. There is, however, little evidence that there are significant differences in the learners themselves but rather in the opportunities and risks afforded by the changing range of technologies that they and others, such as their teachers, use. The reality is that, in any given cohort or class, there will be
- those who are interested in using and exploring technologies for learning,
- those who would rather use traditional media such as print and hand‐written resources, and
- many who like some technologies but prefer not to use others, or
- those who are indifferent to the media with which they are using to learn.
TEL practices need to encompass the diversity of learner attitudes to technology as well as the diverse uses they may make of different technologies.
교육용 테크놀로지
Technologies for Teaching
학습자가 여전히 학습을 하는 것과 마찬가지로 교사는 여전히 가르치는 사람입니다. 의료 교육에서 테크놀로지를 사용하는 것은 단순히 학습을 매개하는 것뿐만 아니라 가르침을 매개하는 것이기도 합니다. 예를 들어, 이제
- 강의를 준비한다는 것은 파워포인트 프레젠테이션을 만드는 것을 의미하고,
- 강의를 한다는 것은 일반적으로 파워포인트 슬라이드와 대화하거나 그 주변에서 이야기하는 것을 의미하며,
- 강의실은 일반적으로 파워포인트 프레젠테이션을 보여주는 데 필요한 스크린과 데이터 프로젝터를 중심으로 구성되고,
- 학습자는 강사의 파워포인트 슬라이드를 다운로드하고 검토하는 방식으로 후속 조치를 취합니다.
따라서 PowerPoint(및 관련 테크놀로지)의 사용은 현대 강의와 관련된 많은 활동을 매개한다고 말할 수 있습니다.
In the same way that learners are still the ones doing the learning, teachers still teach. Using technologies in medical education is not just about mediating learning, it is also about mediating teaching. For example,
- preparing a lecture now means building a PowerPoint presentation,
- giving a lecture usually means talking to or around one’s PowerPoint slides,
- lecture theatres are typically configured around the screens and data projectors needed to show PowerPoint presentations, and
- learners follow up by downloading and reviewing their lecturers’ PowerPoint slides.
We can say therefore that the use of PowerPoint (and its associated technologies) mediates many of the activities associated with the contemporary lecture.
다양한 교수 활동은 다양한 방식으로 매개될 수 있습니다. 상자 10.1에 요약된 활동 유형을 기반으로 교수 활동 유형과 관련 매개 테크놀로지를 고려할 수 있습니다. 상자 10.4를 참조하세요.
Different teaching activities may be mediated in different ways. We can build on the activity types outlined in Box 10.1 to consider teaching activity types and their associated mediating technologies. See Box 10.4.

테크놀로지가 학습자의 학습을 대신하지는 않지만, 일부 테크놀로지는 교사의 교육 방식을 매개합니다. 예를 들어, 멀티미디어 교육 리소스나 YouTube 동영상을 사용하여 임상 절차를 수행하는 방법을 배우는 것은 인간 교사의 지시를 받는 것이 아니라 교사의 교육 방식을 매개합니다. 이는 TEL에 교사가 존재하지 않는다는 뜻이 아니라 교사가 TEL의 사용에 의하여 매개된다는 의미입니다. 따라서 우리는 TEL에서 가르침의 존재감이라는 개념을 고려할 수 있습니다. 최소한의 중재에서 완전한 중재에 이르는 교사 존재감의 연속체를 다음과 같이 고려할 수 있습니다:
Although technologies do not do the learning for learners, some technologies mediate how teachers teach, for instance using a multimedia teaching resource or a YouTube video to learn how to execute a clinical procedure rather than being instructed by a human teacher. This is not to say that there is no teacher present in TEL, only that the teacher is mediated by the use of TEL. We can therefore consider the concept of teaching presence in TEL. We can consider a continuum of teacher presence from minimally mediated to fully mediated as follows:
- 최소한의 중재: 디지털 테크놀로지는 교사와의 구체화된 상호작용을 보강합니다. 예를 들어, 문제 기반 학습 그룹의 학습자는 온라인에서 자료를 조사하고 참조하여 대면 토론을 촉진하는 데 기여할 수 있습니다.
• Minimal mediation: digital technologies augment embodied interactions with teachers. For instance, learners in a problem‐based learning group may research and reference materials online to contribute to their facilitated in‐person discussions. - 동기식 중재: 교사는 학습자와 함께 참여하지는 않지만 하나 이상의 테크놀로지를 사용하여 학습자와 상호 작용합니다. 예를 들어, 교사가 웹 세미나 또는 대규모 공개 온라인 코스(MOOC)에서 그룹에 프레젠테이션을 하고 모든 참가자가 컴퓨터를 통해 상호 작용하는 경우를 들 수 있습니다. 원격 회의, 웹 회의, 가상 세계와 같은 다양한 테크놀로지를 통해 동기식 중재를 다양하게 활용할 수 있습니다.
• Synchronous mediation: the teacher is not co‐present with their learners but interacts with them using one or more technologies. For instance, a teacher presenting to a group in a webinar or massive open online course (MOOC) with all participants interacting through their computers. A range of technologies, such as teleconferencing, web‐conferencing, and virtual worlds, can all afford variations on synchronous mediation. - 비동기식 중재: 교사가 학습자와 상호 작용하지만 실시간은 아닙니다. 예를 들어, 교사가 토론 게시판이나 공유 블로그를 사용하여 전문성 개발의 개념적 문제에 대해 토론하는 경우입니다. 토론 게시판, 이메일, 소셜 미디어, 위키 및 블로그와 같은 테크놀로지는 모두 비동기식 중재를 다양하게 활용할 수 있습니다.
• Asynchronous mediation: the teacher interacts with their learners but not in real time. For instance, a teacher uses a discussion board or a shared blog to discuss conceptual issues in professional development. Technologies such as discussion boards, email, social media, wikis, and blogs can all afford variations on asynchronous mediation. - 완전 중재: 교사와 학습자 간의 상호작용이 테크놀로지와 학습자 간의 상호작용으로 대체되는 경우로, 학습자가 비디오를 보거나 멀티미디어 교육 패키지를 사용하거나 온라인 교과서를 사용하는 경우를 예로 들 수 있습니다. 이 경우 교사(또는 적어도 교사 한 명)는 학습자가 사용하는 자료의 디자인에 대한 지침을 기록해 두었습니다. 학습자가 교사와 직접 상호작용할 수 없다는 점을 고려할 때, 이러한 자료의 교육적 유용성은 부분적으로 이러한 테크놀로지에 내장된 교육적 상호 작용에 달려 있습니다. TEL의 맥락에서 상호 작용은 상호 작용할 대상이 있느냐의 문제가 아니라 학습자가 중개된 교수자 존재와 상호 작용할 수 있는 방법의 문제입니다.
• Full mediation: interactions between a teacher and their learners are replaced by interactions between technologies and learners; for example learners view videos, use multimedia teaching packages, or even online textbooks. In this case the teacher (or at least a teacher) has recorded their instruction in the design of the materials the learners use. Given that the learners cannot interact directly with a teacher, the instructional utility of these materials is in part dependent on the instructional interactivity built in to these technologies. Interactivity in the context of TEL is not so much a matter of having things to interact with but rather how learners can interact with a mediated teaching presence.
교육에 사용되는 일부 형태의 테크놀로지는 타사 온라인 참고 자료를 사용하여 사실을 검색하는 것과 같이 상당히 자연스럽게 배포할 수 있지만, 대부분의 경우 효과적이기 위해서는 신중한 설계와 구성이 필요합니다. 따라서 '디자인'은 교육에 테크놀로지를 사용하는 데 있어 핵심적인 문제입니다. 교육용 테크놀로지 사용에는 설계가 필요한 다양한 측면이 있습니다.
- 콘텐츠(프레젠테이션, 강의 자료),
- 활동(시뮬레이션, 시나리오, 실습),
- 커뮤니케이션(토론, 협업),
- 교육 및 지원(가이드 및 매뉴얼) 등
Some forms of technology used for teaching can be deployed fairly spontaneously (such as looking up facts using third‐party online reference materials), but most need careful design and configuration to be effective. ‘Design’ then is a key issue in using technologies for teaching. There are many different aspects of technology use for teaching that need to be designed:
- content (presentations, course materials),
- activities (simulations, scenarios, labs),
- communication (discussion, collaboration), and
- training and support (guides and manuals).
의료 교사가 이러한 설계 작업을 직접 수행할 수도 있지만, 학교에서는 교사의 설계 활동을 지원하기 위해 교육 디자이너를 전문가로 고용하는 경우가 많습니다. 교수 설계에 관한 풍부한 문헌[9, 10]이 있어 교사가 수업에서 테크놀로지를 사용하는 데 도움이 됩니다. 예를 들어, Mayer의 '멀티미디어 원칙'은 테크놀로지 매개 교육 자료 설계를 위한 증거 기반 지침을 제시합니다(상자 10.5)[11]. 교육 설계에 영향을 주는 다른 관련 교육 원칙은 이 책의 다른 곳에서 논의됩니다(예: 6장).
Although medical teachers may undertake these design tasks themselves, schools often engage instructional designers as specialists to support teachers in their design activities. There is a rich literature on instructional design [9, 10] to support teachers in using technology in their teaching. For instance, Mayer’s ‘multimedia principles’ sets out evidence‐based guidance for designing technology‐mediated teaching materials (Box 10.5) [11]. Other relevant educational principles informing instructional design are discussed elsewhere in this book (e.g. Chapter 6).

테크놀로지 매개 교육 활동의 설계에 정보를 제공하는 데 사용할 수 있는 강력한 연역적 원칙이 있지만, 교육을 지원하는 테크놀로지 설계 및 사용의 대부분은 교사가 사용할 수 있는 테크놀로지와 같이 교사가 직면하는 실질적인 제약에 의해 형성됩니다. 예를 들어, 대학과 의과 대학에서는 교수자가 사용해야 하는 Blackboard 또는 Moodle과 같은 단일 교육기관용 온라인 학습 플랫폼이 있는 것이 일반적입니다. 보다 유연한 태도를 가진 학교의 경우에도 여러 시스템을 지원하는 프로그램에 대한 비용 및 기타 위험은 지속 불가능한 것으로 판명될 수 있습니다. 교육 디자이너와 함께 일하든 아니든, 의료 교사는 교육에 대해 다음을 알아야 합니다[12].
- 어떤 테크놀로지를 사용할 수 있고 사용해야 하는지,
- 어떤 테크놀로지를 사용할 수 있는지,
- 어떤 테크놀로지가 예상되는 특정 상황에서 가장 효과적일지,
- 테크놀로지를 어떻게 구성하고 제시해야 하는지
또한 현지의 테크놀로지 사용 문화(허용되는 테크놀로지 사용과 허용되지 않는 테크놀로지 사용 등)와 참가자의 역량(경험 정도, 사용할 수 있는 도구 및 장치 등)을 이해해야 합니다.
Although there are robust deductive principles that can be used to inform the design of technology‐mediated teaching activities, much of the design and use of technology in support of teaching is shaped by the practical constraints that teachers face, such as what technologies are available to them. For instance, it is common for universities and medical schools to have single institutional elearning platforms, such as Blackboard or Moodle, which instructors are required to use. Even for schools with a more flexible posture, the costs and other risks for a programme supporting multiple systems will likely to prove unsustainable. Whether or not they are working with instructional designers, medical teachers need to know
- what technologies can and should be used in their teaching,
- what technologies are available to them,
- what technologies would work best in the particular situation envisaged, and
- how the technology should be configured and presented [12].
They should also appreciate the local culture of technology use (what technology use is and is not acceptable or popular, etc.), and the capabilities of the participants (how experienced they are, what tools and devices they have available to them, etc.).
분명히 의학 교육에 테크놀로지를 사용하는 것은 풍부하고 때로는 복잡한 작업이 될 수 있으며, 이러한 복잡성은 일부 교사에게는 흥미를 유발하고 다른 교사에게는 불쾌감을 줄 수 있습니다. 학습자와 마찬가지로, 특정 교사 그룹에는 다양한 교사 가 있을 수 있습니다.
- 다양한 테크놀로지를 사용하고 싶어 하는 교사,
- 어떤 종류의 테크놀로지도 사용하는 것을 좋아하지 않는 교사,
- 어떤 테크놀로지는 좋아하지만 다른 테크놀로지는 사용하지 않는 교사
테크놀로지 사용과 관련하여 교사와 학습자의 선호도를 일치시키는 것은 협상하기 어려울 수 있으며, 특정 의료 교육 활동에서 테크놀로지 사용의 정도를 어느 정도 유연하게 조정하는 것이 바람직합니다.
Clearly the use of technologies for teaching in medicine can be a rich and at times complex undertaking, and this complexity may be intriguing to some teachers and off‐putting to others. As with learners, for any given group of teachers there are likely to be
- those who are keen to use different technologies,
- those who do not like using technologies of any kind, and
- those who like using some technologies but not others.
Matching teacher and learner preferences as regards technology use can be difficult to negotiate and some flexibility in how much technology use is involved in any given medical education activity is advisable.
평가를 위한 테크놀로지
Technologies for Assessment
학습 및 교수를 위한 테크놀로지를 살펴보았으므로 이제 평가를 위한 테크놀로지를 살펴보겠습니다. 일반적인 평가와 마찬가지로 학습자 관점에서의 테크놀로지 사용은 형성적 평가와 총괄적 평가로 구분되는 경향이 있습니다.
Having considered technologies for learning and teaching, we turn now to technologies for assessment. As with assessment in general, uses of technologies from a learner point of view tend to fall into formative and summative.
형성 평가 목적의 테크놀로지 사용은 온라인 시험, 퀴즈 및 현재 지식을 측정하고 격차나 약점을 파악하는 기타 방법에 중점을 두는 경향이 있습니다. 이러한 시험은 독립형 시험(예: 스마트폰용 시험 준비 앱)일 수도 있고 멀티미디어 교재에 포함될 수도 있습니다. 어느 쪽이든 테크놀로지를 통해 시험을 출제, 자동화 및 채점할 수 있지만, 문제나 시험의 가치는 여전히 좋은 평가 자료를 작성하는 교사의 스킬에 달려 있습니다. 테크놀로지가 형성 평가를 매개할 수는 있지만 그 자체로 더 나은 평가가 되는 것은 아닙니다.
Formative uses of technology tend to focus on online tests, quizzes, and other ways of gauging current knowledge and identifying gaps or weaknesses. These may be standalone tests (such as exam preparation Apps for smartphones) or they may be embedded in multimedia teaching materials. Either way, although technologies allow for the presentation, automation, and scoring of tests, the value of a question or test still depends on teachers’ skills in writing good assessment materials: technologies can mediate formative assessments but they do not in and of themselves make for better assessment.
총괄 평가 목적으로 테크놀로지를 사용하는 예로는 종이 기반 형식이 아닌 온라인으로 시험을 출제하거나 지속적인 의료 교육 활동에 대한 보고(예: 일종의 e-포트폴리오 시스템 사용)가 있습니다.
Uses of technology for summative assessment purposes include presenting exams online (rather than in a paper‐based format), and reporting on continuing medical education activities (such as using some kind of e‐portfolio system).
평가 테크놀로지 자체는 형성형 또는 총괄형 프로세스를 지원하도록 설계될 수 있지만, 많은 평가 테크놀로지가 두 가지 용도로 모두 사용될 수 있습니다. 질문은 질문이고, 시험은 시험이며, 포트폴리오는 포트폴리오입니다. 차이를 만드는 것은 의도와 관련된 절차적 엄격성입니다. 총점 평가 목적의 테크놀로지, 특히 고부담 평가 활동을 위한 테크놀로지는 더 높은 수준의 접근 제어 및 보안과 더 큰 로딩 용량이 필요합니다. 감독(감독) 컴퓨터 매개 고부담 시험은 부정행위와 허위 진술로부터 안전해야 하며 동시 대량 시스템 액세스를 처리할 수 있어야 합니다.
Assessment technologies themselves may be designed to support either formative or summative processes but many of them can be used for both purposes. A question is a question, a test is a test, and a portfolio is a portfolio: it is the intent and the procedural rigour involved that makes the difference. Technologies for summative assessment purposes, particularly for high stakes assessment activities, need higher levels of access control and security, and greater loading capacity: a proctored (supervised) computer‐ mediated high stakes examination must be secure against cheating and misrepresentation and be able to handle simultaneous mass system access.
테크놀로지는 형성적 평가와 총괄적 평가 활동을 중재하는 데 유용할 수 있지만, 평가를 지원하는 테크놀로지 사용은 평가 관리 및 배포, 평가 데이터 분석과 관련된 물류 및 워크플로우에 가장 큰 영향을 미쳤으며 가장 많이 활용되고 있습니다. 예를 들어, 전 세계 의과대학에서는 대량의 문제를 관리하고 평가해야 하는 프로그램 때문에 평가 구축 및 관리를 위한 온라인 시스템(예: ExamSoft 및 Respondus)을 사용하는 것이 점점 더 보편화되고 있습니다. 이러한 시스템의 데이터베이스에서 제공하는 문제 은행은 시험 시행 전에 문제를 조합하고 다듬을 수 있으며, 이전 문제 사용 내역과 성과 지표를 추적하여 시험 설계자가 시험을 조합하는 데 도움을 줍니다. 또한 이러한 시스템은 종이 기반 시스템보다 훨씬 빠르게 시험에서 학습자의 성과를 처리하고 보고할 수 있습니다. 그러나 이러한 시스템이 모든 형태의 평가를 지원하는 데에는 한계가 있습니다. 예를 들어, 이러한 시스템은 에세이나 장답형 시험 문제와 같은 서술형 답안을 처리하는 데는 한계가 있으며, 객관식 문제나 응답 그리드(OSCE의 평가자 양식 등)와 같은 표 형식 또는 구조화된 답안을 처리하는 데는 강점이 있습니다. 따라서 테크놀로지가 평가 프로세스를 중재하고 지원하는 역할을 할 수 있지만, 의학교육을 지원하는 강력한 평가를 제공하기 위해서는 여전히 교수진 및 평가에 관련된 다른 사람들의 핵심 스킬과 역할이 필수적입니다.
As much as technologies can be useful in mediating formative and summative assessment activities, technology use in support of assessment has arguably had the greatest uptake and the greatest impact on the logistics and workflows associated with managing and deploying assessments, and analysing assessment data. For instance, the use of online systems for building and managing assessments (such as ExamSoft and Respondus) is increasingly common in medical schools around the world, not least because programmes have to manage and evaluate large quantities of questions. The question banks that databases in these systems offer, from which exams can be assembled and refined before delivery, track previous uses of questions and their performance metrics to support exam designers’ in assembling exams. These systems can often also process and report on learner performance in exams much faster than paper‐based systems can. However, there are also limitations to the ability of these systems to support all forms of assessment. For instance, these systems tend to be limited in their ability to deal with written answers (such as essays or long‐answer test questions), their strength is in handling tabulated or structured responses such as multiple‐ choice questions or response grids (such as assessor forms in OSCEs). Thus, while technologies can play a role in mediating and supporting assessment processes, the core skills and roles of faculty and others involved in assessment are still an essential part of delivering robust assessments in support of medical education.
평가 중재는 학습자의 시험 결과를 손상시킬 수 있는 인공물을 도입할 수도 있습니다. 예를 들어, 테크놀로지 사용 경험이 많은 학습자(예: 컴퓨터 사용 또는 화면상의 물체 조작 능력)에게 유리한 시험이 있다면, 시험은 어느 정도 이러한 능력을 측정하고 보고할 것입니다. 학습자의 테크놀로지 사용 태도와 능력을 완전히 균질화normalize하는 것은 비현실적이므로, 테크놀로지 매개 시험 및 평가는 테크놀로지 매개로 인해 발생하는 인공물이 평가 프로세스 및 데이터에 침입하는 것을 최소화하도록 설계되어야 합니다.
Mediation of assessment can also introduce artefacts that can compromise the results of testing learners. For instance, if a test favours learners with more experience using technology (such as being able to use a computer or to manipulate onscreen objects) then the test will to some extent measure and report on this ability. Given that complete normalisation of learner attitudes and capabilities in using technology is unrealistic, technology‐mediated tests and assessments should be designed to minimalise the intrusion of artefacts arising from technology‐mediation in to assessment processes and data.
효과적인 평가 설계의 원칙은 제20장 및 제18장에서 고려한 전자 포트폴리오 관련 문제에 설명되어 있지만, 테크놀로지 활용 평가(TEA)의 일반적인 사용과 관련하여 Amin 등[13]이 유용한 지침을 제공합니다(상자 10.6).
Principles of effective assessment design are described in Chapter 20 and issues concerning e‐portfolios considered in Chapter 18, but in relation to the general use of technology‐enabled assessment (TEA), Amin et al. [13] provide helpful guidance (Box 10.6).
상자 10.6 사용 방법: 테크놀로지 지원 평가 사용
BOX 10.6 HOW TO: Use technology‐enabled assessment
테크놀로지 지원 평가(TEA) 사용 지침[13].
Guidelines for the use of technology‐enabled assessment (TEA) [13].
- TEA의 참신성에도 불구하고 여전히 강력한 일반 평가 원칙을 따라야 한다.
- 학교는 분명한 이점이 있는 경우에만 TEA를 사용해야 합니다.
- 학교는 특히 중요한 목적을 위해 TEA를 사용할 때 강점, 약점, 기회 및 위협을 평가해야 합니다.
- TEA를 위한 테크놀로지는 프로그램 수준의 평가 시스템 및 관행에 통합되어야 합니다.
- TEA에는 특별한 테크놀로지 및 평가 전문 지식이 필요하며, 이는 프로그램 내에서 구축되고 유지되어야 합니다.
- 시험 개발자는 TEA의 타당성, 특히 측정되는 구성 요소의 타당성을 보장해야 합니다.
- Despite the novelty of TEA, it is still dependent on robust general assessment principles.
- Schools should only use TEA where it confers a clear advantage.
- Schools should appraise the strengths, weaknesses, opportunities, and threats of using TEA, particularly for highstakes purposes.
- Technologies for TEA should be integrated within programme‐level assessment systems and practices.
- TEA requires particular technical and assessment expertise, which should be built and sustained within the programme.
- Test developers should ensure the validity of TEA, in particular the constructs being measured.
의학교육 관리를 위한 테크놀로지
Technologies for Managing Medical Education
평가 테크놀로지의 많은 가치가 평가 프로세스의 관리에서 찾을 수 있다는 관찰을 바탕으로, 의학교육에서 테크놀로지의 마지막 주요 적용 분야는 의학교육 시스템(프로그램, 코스 등) 지원, 일반적으로 시스템 내 활동을 관리, 추적 및 보고하는 역할에 사용되는 테크놀로지입니다. 다른 정보 관리 시스템과 마찬가지로 그 가치는 종종 규모의 경제에 따라 달라집니다. 단기간에 걸쳐 소수의 학습자의 진도를 추적하는 것은 직접적인 상호작용과 관찰을 통해 더 잘 이루어질 수 있지만, 다년간의 학습 프로그램에 걸쳐 수백 명의 학습자의 진도를 추적하려면 강력한 정보 추적 및 관리 시스템이 필요합니다. 이제 학습 프로그램에서는 온라인 지원 시스템으로 가상 학습 환경(VLE)이라고도 하는 학습 관리 시스템을 사용하는 것이 일반적인 관행이 되었습니다. 이러한 시스템은 일반적인 시스템(예: Moodle 및 Blackboard)과 의학 전용 시스템(예: Entrada) 모두 학습자, 교사 및 프로그램 관리자를 위한 통합된 도구를 제공합니다. 이러한 시스템은 일반적으로 학습자와 교사가 시스템에서 수행한 작업을 모니터링, 추적, 기록 및 보고하기 위한 도구를 제공하므로 이러한 시스템을 사용하여 가장 큰 이점을 얻을 수 있는 그룹은 후자의 그룹입니다. 따라서 활동 로깅은 이러한 도구의 핵심 기능입니다. 일부 활동 로그는 로그인, 파일 다운로드 또는 토론 게시판 참여와 같이 자동으로 생성되는 반면, 다른 활동 로그는 보다 명시적으로 활동을 추적하고 보고하기 위한 것입니다(예: 임상 만남 추적).
Building on the observation that much of the value of assessment technologies is to be found in the management of assessment processes, the last major area of application for technologies in medical education we will consider is their use in support of systems of medical education (programmes, courses, etc.), typically in the role of managing, tracking, and reporting on activities within those systems. As with any other information management system, their value often depends on economies of scale. While tracking the progress of a few learners over a short period of time may be better done through direct interaction and observation, tracking the progress of hundreds of learners over multi‐year programmes of study requires robust information tracking and management systems. It is now common practice for programmes of study to make use of learning management systems, also sometimes called Virtual Learning Environments (VLEs), as an online support system. These systems, both generic (e.g. Moodle and Blackboard) and medicine specific (e.g. Entrada), provide an integrated array of tools for learners, teachers, and programme managers. It is the latter group who may benefit the most from using these systems as these systems usually provide tools for monitoring, tracking, recording, and reporting on what learners and teachers have done in the system. Activity logging is therefore a key function of these tools. Some activity logs are generated automatically (such as logins, downloading files, or contributing to discussion boards) while others are more explicitly about tracking and reporting on activity (such as clinical encounter tracking).
로그 데이터는 그 자체로는 내재적 가치가 없으며, 이를 분석하고 이 분석을 통해 결론과 추론을 도출해야만 유용하게 사용할 수 있습니다. 이를 위해 학습 분석은 고등 교육과 의학 교육에서 점점 더 많은 관심을 받고 있는 분야입니다. 예를 들어, 역량 기반 의학교육(CBME)의 채택은 부분적으로 종단적 연속 평가와 개별 학습자의 진행 상황을 예상되는 발달 이정표와 비교하는 것을 기반으로 하며, 이 두 가지 모두 온라인 추적 및 보고의 이점을 누릴 수 있고 실제로 필요할 수 있습니다. 마찬가지로, 평생 의료 교육 및 역량 유지 프로그램도 데이터의 양과 관련된 개인의 수를 고려할 때 통합 시스템이 필요합니다.
Log data has no intrinsic value in and of itself, it needs to be analysed and conclusions and inferences drawn from this analysis for it to become useful. To this end, learning analytics is a growing area of interest in higher education and in medical education. For instance, the adoption of competency‐based medical education (CBME) is in part based on longitudinal continuous assessment and the comparison of individual learner progress with expected developmental milestones, both of which can benefit from, and may indeed require, online tracking and reporting. Similarly, continuing medical education and maintenance of competence programmes also require integrated systems given the quantities of data and number of individuals involved.
그러나 러닝 애널리틱스에는 여러 가지 과제와 한계가 있으며, 그 중 가장 중요한 것은 수집할 수 있는 데이터와 이러한 데이터가 무엇을 나타내는가 하는 점입니다.
- 전자 시스템은 주로 마우스 클릭(또는 트랙패드 탭) 및 키 누름과 같이 시스템 내에서 수행된 전자 이벤트만 기록할 수 있습니다.
- 이러한 이벤트는 일반적으로 다음과 연관됩니다.
- 특정 사람(사용자),
- 특정 컨텍스트(이 페이지 또는 이 시스템 내),
- 특정 날짜 및 시간
- 이러한 시스템에서는 다음은 기록하지 않습니다.
- 이벤트가 발생한 이유,
- 시스템상의 신원이 실제로 이벤트를 일으킨 개인과 동일한지 여부,
- 해당 이벤트가 해당 개인에게 미친 영향(예: 해당 이벤트의 결과로 학습한 내용)
- 사용자가 페이지를 로드하고 다음 페이지로 이동하기까지의 시간과 같은 측정값은 사용자가 자료를 읽었는지 또는 숙고했는지 여부를 반영할 수 있지만, 사용자가 동시에 다른 일을 하고 있었는지 또는 학습의 질과 관련이 없는 다른 많은 요인에 따라 달라질 수도 있습니다[14].
However, learning analytics does have a number of challenges and limitations, not least of which are what data can be collected and what these data represent.
- Electronic systems can only record electronic events undertaken within them, primarily mouse clicks (or trackpad taps), and keypresses.
- These are usually associated with
- a particular person (user),
- particular context (on this page or in this system), and
- a particular date and time.
- These systems do not record
- why the event took place,
- whether the identity of the person in the system is the same as the individual actually causing the events, or
- what impact those events had on that individual (such as what they learned as a result of this event.
- Measures such as the time between a user loading a page and moving to the next page may reflect whether or not they read or reflected on the material, but they could also depend on whether the user was doing something else at the same time, or many other factors not associated with the quality of learning [14].
학습 분석의 유용성은 기록할 수 있는 이벤트와 해당 이벤트가 의미하는 의미의 정확성에 의해 제한됩니다. 또한 의료 교육 시스템은 학습자의 행동뿐만 아니라 교사의 행동도 추적하는 데 사용될 수 있다는 점에 유의해야 합니다. 모든 사용자를 관찰하고 면밀히 조사하여 그들에 대한 가치 판단을 유추할 수 있는 이러한 파놉틱 기능은 (종종 관련자가 이러한 조사를 인지하지 못한 채) 윤리적 및 숨겨진 커리큘럼에 미치는 영향을 신중하게 고려해야 합니다[15].
The utility of learning analytics is limited by the events that can be recorded and the semantic precision of what those events mean. It should also be noted that medical education systems may be used to track teacher behaviours as well as those of their learners. This panoptic ability to observe and scrutinise all users and to infer value judgments about them (often without the individuals concerned being aware of this scrutiny) requires careful consideration of the ethical and hidden curriculum implications of doing so [15].
규모의 경제 원칙은 커리큘럼 매핑 도구 및 시스템의 사용으로 예시되는 교육 프로그램 관리에 테크놀로지가 사용되는 방식에도 반영됩니다. 커리큘럼 매핑에 대한 표준 접근 방식은 없지만, 모든 세션, 목표, 시험, 결과 및 기타 커리큘럼 구성 요소에 대한 포괄적이고 질문 가능한 데이터베이스는 의학교육 커리큘럼을 관리, 수정 및 보고하는 데 귀중한 자산이 될 수 있습니다. 평가 및 연구를 위해 커리큘럼 맵을 집계하고 비교할 수 있다면 더 많은 이점이 발생할 수 있습니다[16]. 그러나 일반적으로 커리큘럼 매핑 데이터베이스를 설정하고 유지하는 데 필요한 시간과 노력으로 인해 의과대학에서 이러한 종류의 도구를 사용하는 데 한계가 있는 경향이 있습니다. 실제로 경제성과 투자 수익률은 의학교육 시스템 관리를 위한 테크놀로지 사용에 있어 중요한 제한 요소입니다.
The principle of economies of scale also reflects how technologies are used in managing educational programmes, exemplified by the use of curriculum mapping tools and systems. Although there is no standard approach to curriculum mapping, a comprehensive and interrogatable database of all the sessions, objectives, tests, outcomes, and other curriculum components can be an invaluable asset in managing, revising, and reporting on medical education curricula. Further benefits can accrue when curriculum maps can be aggregated and compared in the interests of evaluation and research [16]. However, the time and effort typically required to set up and maintain curriculum mapping databases tends to limit medical schools’ commitment to using tools of this kind. Indeed, economics and return on investment is a critical limiting factor in the use of technologies for managing medical education systems.
교육용 보철물로서의 테크놀로지
Technologies as Educational Prostheses
주로 의료 교육 활동의 매개체로서 테크놀로지를 고려했다면, 저는 테크놀로지를 '교육적 보철물'로도 생각해보고 싶습니다. 이는 테크놀로지를 활용한 의학교육의 활용과 관련하여 중요한 역설 중 하나를 제기하는데, 가장 효과적인 교육 및 학습 접근 방식에는 일반적으로 매개 테크놀로지가 거의 포함되지 않는다는 것입니다. 실제로 교실과 병상 모두에서 교사와 학습자 간의 일대일 대면 상호작용은 양쪽 모두 경험할 수 있는 가장 효과적이고 가치 있는 상호작용입니다. 이러한 상호작용을 테크놀로지를 통해 다시 중재하는 것은 종종 친밀감과 즉각성을 떨어뜨리는 결과를 낳습니다. TEL을 사용하는 것이 최적의 개별 교육 접근 방식인 경우는 거의 없습니다. 그러나 상황이 항상 최적인 것은 아니며, 테크놀로지는 차선책으로 최적의 조건을 보완하는 보조 수단으로 사용될 수 있습니다.
Having primarily considered technology as a medium for medical education activities, I would also like to consider technologies as ‘educational prostheses’. This raises one of the key paradoxes around the use of technologyenhanced medical education, which is that approaches to teaching and learning that work best typically involve little mediating technology. Indeed, one‐to‐one in-person interactions between teachers and learners, both in the classroom and at the bedside are some of the most effective and valuable either party can experience. To re-mediate these interactions through technology is often to diminish their intimacy and immediacy. Using TEL is rarely the optimal individual instructional approach to take. But circumstances are rarely optimal, and technologies can work as prostheses to compensate for suboptimal conditions.
테크놀로지는 학습자를 대신하여 학습하지는 않지만, 다음을 통해 학습을 강화할 수 있습니다.
- 학습자가 지식을 찾고, 기록하고, 조직화하고, 구조화하고, 기억하도록 돕고,
- 사물을 상기시키고, 시간을 정리하도록 돕고,
- 다른 사람과 연결시켜주고,
- 학습을 연습하고, 테스트하고, 분석하고, 보고하도록 도와줌으로써
따라서 테크놀로지는 학습자가 학습하고 주변 세계와 상호 작용하는 방식을 확장하고, 구조화하고, 지원하는 학습 보철물로 기능할 수 있습니다.
Although technologies do not learn for learners, they can augment learning
- by helping them to find, record, organise, structure, and recall knowledge,
- by reminding them of things and helping to organise their time,
- by connecting them with others, and
- by helping them to rehearse, test, analyse, and report on their learning.
Technologies can therefore function as learning prostheses; they can extend, structure, and support the ways in which learners learn and interact with the world around them.
또한 테크놀로지는 교사가 기록, 정리, 구조화, 기억, 상기, 연결, 찾기, 리허설, 테스트, 분석, 보고를 할 수 있도록 지원함으로써 교수 보조 도구의 역할을 할 수 있습니다. 디지털 테크놀로지가 우리의 행동과 상호작용 방식을 보강할 수 있는 몇 가지 방법은 상자 10.7에 나와 있습니다.
Technologies can also act as teaching prostheses by helping teachers to record, organise, structure, remember, remind, connect, find, rehearse, test, analyse, and report on their teaching. Some of the ways in which digital technologies can augment the way we act and interact are set out in Box 10.7.
박스 10.7 디지털 테크놀로지의 보조적 특성
BOX 10.7 Prosthetic properties of digital technologies
디지털 테크놀로지를 통해 교육과 학습을 강화할 수 있습니다:
Digital technologies can be used to augment teaching and learning through:
- 시간과 노력을 절약할 수 있습니다: 사용자가 작업을 기억하고, 반복하고, 찾고, 기록하고, 정리할 수 있도록 돕고, 다른 사람이나 새로운 사건에 행동하고 대응하는 속도를 가속화하여
- 물리적 한계를 뛰어넘을 수 있도록 지원합니다: 사용자가 데이터 집합 시각화와 같이 규모가 크거나(데이터 집합 시각화), 서로 다른 장소에 있는 사람들이 함께 작업할 수 있도록 하여 지리적 한계를 극복하거나, 비동기적으로 함께 작업할 수 있도록 하여 시간적 한계를 극복하는 등
- 다른 사람들과 조직하고 연결합니다: 사용자가 자료와 생각을 만들고, 방송하고, 공유하고, 댓글을 달고, 특정 아이디어와 입장을 지지하거나 반대하는 토론, 논쟁, 도전, 로비를 할 수 있도록 지원함으로써
- 사회적 관습을 변화, 모호화 또는 평탄화합니다: 대면 상호작용을 형성하는 사회 구조가 사용자의 능력을 저해하는 방식으로 행동하고 상호작용할 수 있도록 지원함으로써
- 개인과 개인의 행동에 대한 가시성과 책임성을 높입니다: 사용자가 자신 또는 타인의 행동과 말을 면밀히 조사하고, 기록하고, 추적할 수 있도록 지원함으로써
- Saving time and effort
- by helping their users to remember, repeat, find, record, and organise their work, and by accelerating the speed at which they can act and respond to others or emerging events.
- Going beyond physical limitations
- by helping their users to interact with things that are big (such as visualising datasets), far (such as defeating geography by allowing individuals in different places to work together), or time shifted (such as defeating temporality by allowing individuals to work together asynchronously).
- Organising and connecting with others
- by helping users to create, broadcast, share, and comment on materials and thoughts, and to discuss, debate, challenge, or lobby for or against particular ideas and positions.
- Changing, blurring, or flattening social conventions
- by helping their users to act and interact in ways where social structures that shape face to face interactions would have inhibited their ability to do so.
- Heightening the visibility and accountability of individuals and their actions
- by helping their users to scrutinise, record, and track what they or others do and say.
보철 테크놀로지를 통해 일상적인 의료 교육에서 직면하는 많은 실질적인 한계를 해결할 수 있습니다. 이러한 방식으로 '규칙'을 바꾸면 특정 이점을 얻을 수 있지만, 테크놀로지 중재는 중재 활동에 대한 인식과 가치관도 변화시키는 경향이 있습니다. 고든 그레이엄은 다음과 같이 말했습니다:
- '테크놀로지 혁신은 단순히 미리 선택된 목적을 위한 개선된 수단으로만 간주될 수 없으며, 일부 테크놀로지는 단순히 수정하는 반면 다른 테크놀로지는 변화시키기 때문입니다'[17, 168쪽].
Prosthetic technologies allow us to work around many of the practical limitations we face in day‐to‐day medical education practice. Changing the ‘rules’ in this way may confer certain advantages, but technology mediation tends also to shift perceptions and values around the mediated activities. As Gordon Graham observed:
- ‘technological innovation cannot and should not be regarded merely as an improved means to a pre‐selected end, because, while some technology merely modifies, other technology transforms’ [17, p. 168].
테크놀로지적 중재를 통한 증강은 종종 일련의 트레이드오프와 가치관의 변화를 수반합니다. 예를 들어,
- 온라인 토론 게시판의 사용은 학습자 간, 교사-학습자 간 상호작용이 영구적으로 기록된다는 것을 의미하며, 이는 다시 말해 온라인 토론 게시판이 등장하기 전에는 의학교육에서 불가능했던 평가 및 평가 목적의 데이터로 활용될 수 있다는 것을 의미합니다.
- 마찬가지로, 교사와 학습자의 상호작용이 다양한 방식으로 매개될 수 있게 되면서 이전에는 의료 전문가 교육에 적용되지 않았던 것에 대해 생각하기 시작했습니다.
- 존재의 경제(온라인 상호작용이 아닌 대면 상호작용의 가치)와
- 주의의 경제(학습자 또는 교사의 주의를 끌고 유지하는 능력)
Augmentation through technological mediation often involves a series of trade‐offs and a shifting of values. For instance, the use of online discussion boards means that intra‐learner and teacher–learner interactions are now permanently recorded, which in turn means that they can be used as data for evaluation and assessment purposes, something that had no place in medical education until it became possible. Similarly, when teacher and learner interactions can be mediated in many different ways we begin to think about economies of presence (the value of, say, face‐to‐face as opposed to online interactions) and economies of attention (the ability to attract and retain learner or teacher attention) in ways that previously had no place in the training of health professionals.
의학교육에서의 TEL 평가 및 연구
Evaluating and Researching TEL in Medical Education
의학교육의 모든 측면과 마찬가지로 효율적이고 효과적인 실습은 강력한 연구 및 평가 근거에 기반해야 합니다. 의학교육에서 테크놀로지 사용에 대한 연구가 부족하지는 않지만, 근거의 질과 그 통화 및 진료 지침과의 관련성은 다소 제한적입니다(상자 10.8).
As with any aspect of medical education practice, efficient and effective practice needs to be based on robust research and evaluation evidence. Although there has been no shortage of studies into technology use in medical education, the quality of the evidence and its currency and relevance to guiding practice is somewhat limited (Box 10.8).
상자 10.8 증거는 어디에 있는가? 테크놀로지 기반 학습
BOX 10.8 WHERE’S THE EVIDENCE: Technology‐enhanced learning
TEL이 효과가 있는지 없는지에 대한 체계적인 검토가 많이 이루어졌습니다. 예를 들어, 가장 큰 규모의 리뷰 중 하나(초등 및 중등 교육에 초점을 맞춘)에서는 테크놀로지가 혼합된 형태로 사용될 때 상당한 교육적 이점을 제공할 수 있다는 결론을 내렸습니다[4]. 그러나 의학교육에 사용되는 테크놀로지의 다양성과 다양한 사용 방식을 고려할 때 단순히 'TEL이 효과가 있는가'라고 묻는 것만으로는 결정적인 대답은 물론 의미 있는 대답도 할 수 없습니다. 대신 어떤 상황에서 어떤 종류의 TEL이 효과적일 수 있는지, TEL의 어떤 기능이 학습의 수준과 질을 달리할 수 있는지를 고려해야 합니다.
There have been a number of systematic reviews into whether TEL does or does not work. For instance, one of the largest reviews (focused on primary and secondary education) concluded that technology can confer significant educational advantage when used in a blended form [4]. However, given the diversity of technologies used in medical education and the many different ways in which they are used, simply asking ‘does TEL work?’ is impossible to answer meaningfully let alone conclusively. We should instead consider in what situations specific kinds of TEL can work and what features of TEL afford different levels and qualities of learning.
Cook과 동료 연구자들[18, 19]이 제기한 이러한 주장은 테크놀로지 매개 개입과 무중재 또는 테크놀로지 매개 개입과 비테크놀로지 개입을 비교한 수많은 연구 결과에 대응하는 것으로, 어느 쪽도 이 분야에 실질적인 도움이 되지 못합니다. 비용, 지속 가능성, 위험과 같은 다른 본질적인 요소는 거의 고려되지 않았습니다[20]. TEL의 효능 및 효과와 관련된 상황적 변수가 매우 많기 때문에 상황적 요인도 고려해야 합니다[14]. 그러나 부분적으로는 교육적 우월성보다는 물류 및 편의성, 부분적으로는 사회 전반의 디지털 테크놀로지로의 광범위한 전환에 따라 테크놀로지 중재가 이미 의학교육의 표준이 되고 있기 때문에 이 모든 것이 논쟁의 여지가 있을 수 있습니다. 실습과 혁신을 평가하고 안내하기 위해서는 더 많은 연구가 필요할 수 있지만, '테크놀로지를 전혀 사용해야 하는가'라는 질문은 얼마 전에 역을 떠났습니다.
This argument, advanced by Cook and colleagues [18, 19], responds to the large number of studies that have compared a technology‐mediated intervention to no intervention or a technology‐mediated intervention to a non‐technological intervention, neither of which substantially add to the field. Other germane factors such as cost, sustainability, and risk are seldom considered at all [20]. Contextual factors also need to be considered as there are so many circumstantial variables associated with the efficacy and effectiveness of TEL [14]. All of this may be moot, however, as technological mediation is already becoming the norm in medical education, partly for logistical and convenience reasons rather than for instructional superiority, and partly in response to the broader switch to digital technologies in society as a whole. More research may be needed to evaluate and guide practice and innovation, but the ‘should we use technology at all?’ train left the station some time ago.
테크놀로지를 매개로 한 의학교육의 측면은 (적어도 초기에는) 새롭고 낯선 경향이 있기 때문에 전통적인 접근 방식보다 더 높은 입증 부담, 회의론, 과도한 자신감에 직면하는 경우가 많습니다. 우리는
- 테크놀로지가 해야 할 일을 신뢰할 수 있고 일관된 방식으로 수행할 수 있는지 평가해야 할 뿐만 아니라,
- 테크놀로지가 사용될 맥락에서 효과가 있는지, 그리고
- 그 테크놀로지를 사용할 모든 사람들에게 일관되게 효과가 있는지도 고려해야 합니다.
TEL에 대한 평가와 연구에는 다음 등이 활용될 수 있습니다.
- 요구 분석과 환경 조사(해당 테크놀로지가 해결해야 할 필요나 기회는 무엇인가),
- (개발 및 적용에 대한) 문서화,
- 사용성(예상대로 작동하는가, 사용자가 쉽고 일관되게 사용할 수 있는가?),
- 구현 관찰(사람들이 실제로 사용하면 어떤 일이 일어나는가?),
- 참여자 경험 및 만족도(사용자에게 어떤가?),
- 학습 결과(테크놀로지 사용이 어떤 영향을 미치는가?),
- 비용, 재사용 가능성 및 지속가능성(테크놀로지 사용이 좋은 투자 수익률인가)[21]
Technology‐mediated aspects of medical education (at least initially) tend to be new and unfamiliar and as such they often face a higher burden of proof, scepticism, and over confidence than more traditional approaches. Not only do we need to appraise
- whether a technology can do what it is supposed to do in a reliable and consistent way, we also need to consider
- whether it will work in the contexts within which it is going to be used, and
- whether it will do so consistently for all of those who are going to use it.
Both evaluation and research into TEL may draw on
- needs analyses and environmental scans (what need or opportunity is the technology to address),
- documentation (of development and application),
- usability (does it function as expected, can its users use it easily and consistently?),
- observation of implementation (what happens when people do use it?),
- participant experience and satisfaction (what is it like for users),
- learning outcomes (what impacts does using technology have?), and
- cost, reusability, and sustainability (is using technology a good return on investment?) [21].
또한 연구가 어디에 초점을 두는지 명확히 할 필요가 있습니다.
- 테크놀로지 그 자체를 평가하는 데 초점을 맞추고 있는지('이 도구는 어떤 속성과 기능을 가지고 있는가?' 등),
- 테크놀로지를 사용하는 활동에 초점을 맞추고 있는지('온라인 PBL은 얼마나 잘 작동하는가?' 등),
- 특정 활동 내에서 테크놀로지를 사용하는 데 초점을 맞추고 있는지('모바일 장치 사용이 학습자-환자 상호작용에 어떤 영향을 미치는가?' 등)
요약하자면, 저는 TEL 안팎에서 무엇을 연구하고 평가해야 하는지에 대한 의제를 제안하기보다는 TEL을 연구하고 평가하는 방식에서 엄격함을 확립하고 유지하는 것이 더 중요하다고 주장합니다.
We also need clarity as to whether studies are focusing
- on evaluating the technologies themselves (such as ‘what properties and capabilities does this tool have?’),
- on activities that use technology (such as ‘how well does online PBL work?’), or
- on the use of technology within particular activities (such as ‘what impact does the use of mobile devices have on learner–patient interactions’?).
To summarise, rather than proposing an agenda regarding what we should research and evaluate in and around TEL, I argue that it is more important to establish and maintain rigour in the ways we research and evaluate TEL.
움직이는 목표
A Moving Target
영원한 것은 없으며 디지털 테크놀로지는 의학교육의 다른 측면보다 일시적인 경향이 있습니다. 'e-러닝 혁명'이 끝난 것처럼 보이지만[22] 테크놀로지는 계속 변화하고 있습니다. 일부 신테크놀로지는 주류 의학교육의 일부가 되기도 하고(예: PowerPoint), 다른 신테크놀로지는 시들해지기도 합니다. 어떤 테크놀로지가 성공할지 실패할지 예측하는 것은 매우 어렵습니다. 예를 들어, 의학 교육에서의 가상현실(VR)[23]은 VR 복강경 수술 시뮬레이터와 같은 일부 용도가 있기는 하지만, 적어도 지금까지는 주류 의학 교육에서 VR 테크놀로지의 사용은 주변적인 수준에 머물러 있습니다.
Nothing lasts for ever and digital technologies tend to be more transient than most other aspects of medical education. Although the ‘e‐learning revolution’ would seem to be over [22] technologies continue to change. Some new technologies become part of mainstream medical education (such as PowerPoint), others wither on the vine. Predicting which ones will succeed or fail is notoriously hard to predict. For instance, virtual reality (VR) in medical education [23] but, although there are some uses (such as VR laparoscopic surgery simulators), at least so far, the use of VR technologies remains peripheral to mainstream medical education.
디지털 전문성만이 의학교육에서 새롭게 떠오르는 관심 분야는 아니며, TEL을 사용할 때 고려해야 할 다른 법적, 평판 및 보안 문제도 있습니다. 의학 교사들이 가장 흔히 직면하는 문제 중 하나는 웹의 자료를 교육 및 학습에 사용하거나 재사용할 수 있는 대상과 방법입니다. 디지털 테크놀로지를 사용하면 자료를 '복사하여 붙여넣기'하거나 다운로드하고 다른 사람과 공유하는 것이 매우 쉬워집니다. 하지만 이렇게 하는 것이 아무리 쉬워도 이를 합법적으로 처리하는 것은 그리 간단하지 않습니다. 국가마다 교육 목적으로 타사 자료를 재사용하는 것에 관한 법률이 다르고 변화하는 경향이 있을 뿐만 아니라, 타인의 지적 재산 오용에 대한 책임에 관한 기준도 제각각이기 때문입니다. 이는 크리에이티브 커먼즈와 같은 라이선스 모델을 개발하게 된 주요 동인 중 하나였습니다. 상자 10.9를 참조하세요.
Digital professionalism is not the only emerging area of concern in medical education, there are other legal, reputational, and security issues to consider when using TEL. One of the most common challenges for medical teachers is what and how materials from the Web can be used or reused in teaching and learning. Digital technologies can make it very easy to ‘copy and paste’ or download materials and to share them with others. However easy it is to do this, the legality of doing so is rarely so simple. Not only do different countries tend to have different and shifting laws regarding the reuse of third‐party materials for educational purposes, there are differing standards regarding liability for misuse of someone else’s intellectual property. This was one of the main drivers behind the development of licensing models such as Creative Commons. See Box 10.9.
상자 10.9 중점 사항: 교육 및 학습을 위한 자료 재사용
BOX 10.9 FOCUS ON: Reusing materials for teaching and learning
타사 자료 사용에 대한 권리는 '퍼블릭 도메인'(사용에 제한이 없음)과 '모든 권리 보유'(저작권자의 허락 없이는 자료를 사용할 수 없음, 다른 약정이 없는 경우 기본값) 사이에 속하는 경향이 있습니다. 이 두 가지 극단 사이에서 라이선스는 자료 사용 방법에 대한 구체적인 조건을 명시합니다. 라이선스는 상업적(예: 퍼블리셔)이거나 오픈 소스(예: 크리에이티브 커먼즈)일 수 있습니다. 크리에이티브 커먼즈(http:// creativecommons.org)에서 개발한 라이선스 시스템은 다음에 관한 규정을 기반으로 합니다.
- 저작물의 창작자 인정 여부(저작자 표시),
- 다른 저작물의 일부로 포함될 수 있는지 또는 원본 저작물의 구성 요소를 재사용할 수 있는지 여부(각색),
- 저작물을 상업적 목적으로 재사용할 수 있는지 여부,
- 파생 저작물이 소스와 동일한 라이선스 모델을 따라야 하는지
Rights for using third‐party materials tend to fall between ‘public domain’ (no restrictions on use) and ‘all rights reserved’ (materials cannot be used without the copyright holder’s permission, the default in the absence of any other arrangement). Between these two extremes, licences set out the specific conditions as to how materials can be used. Licences may be commercial (such as with publishers), or open source, (such as Creative Commons). The licensing system developed by Creative Commons (http:// creativecommons.org) is based on statements regarding
- acknowledging the creator(s) of the work (attribution),
- whether it can be included as part of something else or whether components of the original work can be reused (adaptation),
- whether or not the work can be reused for commercial purposes, and
- whether any derivative works need to follow the same licensing model as the source.
크리에이티브 커먼즈 라이선스는 재사용 가능한 학습 객체(RLO), 오픈 코스웨어, 무료 오픈 액세스 교육(FOAM) 자료를 게시하는 데 사용되었으며, MedEdPortal(www. mededportal.org), MedEdWorld(http://www.mededworld.org), 위키미디어(commons.wikimedia.org) 등의 온라인 저장소에 있는 많은 리소스를 게시하는 데도 사용되었습니다. 명시적인 라이선스 계약이나 타인의 자료 사용에 대한 허가가 없는 경우, 항상 모든 권리가 유보되어 있으며 재사용할 수 없다고 가정해야 합니다. 저작권 침해는 공정 사용(미국) 또는 공정 거래(영국, 캐나다)에 명시된 원칙에 따라 (관할권에 따라) 방어할 수 있지만, 이는 권리라기보다는 방어권으로 표현되는 경향이 있습니다. 또한 타사 자료의 라이선스 없는 사용은 관련 개인과 기관에 위험할 뿐만 아니라 학습자와 동료에게 부적절한 전문성 메시지를 전달할 수 있다는 점에 유의해야 합니다. 퍼블릭 도메인 및 크리에이티브 커먼즈 라이선스 자료를 사용하면 이러한 문제를 해결하는 데 큰 도움이 될 수 있습니다.
Creative Commons licences have been used to publish Reusable Learning Objects (RLOs), OpenCourseware, and Free Open Access Meducation (FOAM) materials, as well as many of the resources in online repositories such as MedEdPortal (www. mededportal.org), MedEdWorld (www.mededworld.org), and Wikimedia (commons.wikimedia.org). In the absence of an explicit licensing agreement or permissions for the use of someone else’s material you should always assume that all rights are reserved and that you cannot reuse it. Copyright breaches may be defended (depending on jurisdiction) under principles set out in Fair Use (USA) or Fair Dealing (UK, Canada), but these tend to be expressed as a defence rather than a right. It should also be noted that not only is unlicensed use of third‐party materials risky for the individuals and institutions involved, it also sends inappropriate professionalism messages to their learners and colleagues. Using public domain and Creative Commons licensed materials can go a long way to addressing these issues.
신원 도용, 사이버 범죄 및 해킹의 증가로 인해 TEL을 사용하는 의료 교육자 및 학습자의 안전과 생존 가능성은 근본적으로 도전받고 있습니다. 전자 시스템의 보안을 보장하고 유지하는 것은 교육자가 거의 고려하지 않더라도 끊임없는 싸움입니다. 이 문제를 해결하는 한 가지 방법은 전자 시스템을 공격으로부터 강화하는 것이지만, 테크놀로지적 약점(예: 유출된 비밀번호)보다는 인적 약점이 더 큰 위협인 경우가 많으며, 사용자의 실수나 경범죄를 교육하고 단속하는 데는 많은 비용이 소요될 수 있습니다. 어느 정도 주목을 받고 있는 대안적이고 다소 급진적인 접근 방식은 프라이버시보다는 보안에 중점을 두고 모든 정보를 공개하는 '포스트 프라이버시 사회'라는 개념입니다[24]. 이 글을 쓰는 시점에서 이러한 문화적 변화가 임박했다는 전망은 없지만, 전 세계적으로 디지털 테크놀로지가 널리 보급되면서 의학과 교육 모두에 근본적인 수준의 영향을 미쳤고 그 결과 의학교육이 원하든 원치 않든 변화하고 있다는 것은 부인할 수 없는 사실입니다.
The safety and viability of medical educators and learners using TEL is fundamentally challenged by the growing problem of identity theft, cybercrime, and hacking. Assuring and maintaining the security of electronic systems is a constant battle, even if it is one that educators rarely consider. While one way of addressing this is to harden electronic systems against attack, human rather than technical weaknesses (such as compromised passwords) are often the bigger threat problem, and training and policing user mistakes and misdemeanours can be expensive. An alternative and somewhat radical approach that has been gaining a degree of traction is the concept of a ‘post privacy society’ where all information is made publicly available [24] with a focus on security rather than privacy. While, at the time of writing, there is no imminent prospect of such a major cultural shift, it is undeniable that the widespread uptake of digital technologies around the world has impacted both medicine and education at a fundamental level and that, as a result, medical education is changing – whether it wishes to or not.
의학교육자는 TEL을 어떤 용도로 사용하든 시스템 장애, 업그레이드, 교체 또는 요구 사항 변경 등 변화와 불안정성에 대비해야 합니다. 또한 사용하는 인프라(예: 네트워크 및 보안)에 대한 의존도를 염두에 두어야 하며, 테크놀로지 사용의 실행 가능성과 공격에 대한 복원력을 모니터링해야 합니다.
Whatever use they make of TEL, medical educators need to plan for change and instability including system failures, upgrades, replacements, or changing requirements. They need to be mindful of their dependence on the infrastructure they use (such as networks and security), and they need to monitor the viability of their technology use and its resilience in the face of attack.
결론
Conclusions
테크놀로지는 매우 빠르게 구식이 되기 때문에 이 장에서 언급된 테크놀로지 중 일부는 이 책이 출판될 때 이미 구식이 되었을 가능성이 높습니다. 따라서 저는 특정 시점에 의학교육에서 사용되고 있는 다소 일시적인 특정 테크놀로지를 초월해야 하는 원칙과 개념에 중점을 두었습니다. 그럼에도 불구하고 저의 주장을 설명하기 위해 구체적인 사례를 제시하려고 노력했습니다. 이러한 사례들은 필연적으로 시대에 뒤떨어질 수밖에 없지만, 그 사례들이 보여주는 원칙은 여전히 유효하기를 바랍니다. 따라서 독자들은 (역사적 호기심에 의한 경우를 제외하고는) 구체적인 내용에 초점을 맞추기보다는 이러한 원칙에 비추어 각자의 시대와 상황에 맞게 재해석할 것을 제안합니다.
Technologies go out of date so quickly; indeed, it is quite possible that some of the technologies mentioned in this chapter will have already become obsolete by the time this book is published. My focus has therefore been on principles and concepts that should transcend the specific and somewhat ephemeral technologies that are being used in medical education at any given time. Nevertheless, I have tried to provide concrete examples to illustrate my arguments. While these examples will inevitably become dated, I hope that the principles they illustrate will stand. I suggest therefore that readers reinterpret the specifics of their own time and circumstances in light of these principles rather than (except perhaps in the sense of historical curiosity) focusing on the specifics.
의학교육에서 TEL의 사용은 긍정적인 변화를 위한 조력자 또는 촉매제가 될 수도 있고, 혼란을 야기하고 주의를 산만하게 하며 책임이 될 수도 있습니다. 테크놀로지 사용의 가치는 순전히 교육적인 문제에 기반하는 경우는 드물고 편의성, 중재 및 증강의 문제로 귀결되는 경향이 있습니다. 따라서 TEL 사용에 대한 찬반 논쟁은 교육적 효과보다는 교육 경제성에 관한 것이 대부분입니다. 문제는 더 효율적이고 편리한 교육 및 학습 방법을 찾는 것이며, 여기에는 테크놀로지 사용이 포함될 수도 있고 포함되지 않을 수도 있습니다. TEL은 또한 사용 가능한 것의 제약을 받습니다. 교사와 학습자는 현재 사용 가능한 테크놀로지의 어포던스를 활용하고 이에 적응하는 경향이 있습니다. 또한 테크놀로지는 기존 관행을 대체하기보다는 부가적인 방식으로 사용되는 경향이 있습니다. 대체는 한 테크놀로지의 편리함과 유용성이 다른 테크놀로지를 압도하여 효과적으로 시들어 버릴 때만 발생합니다.
The use of TEL in medical education can be an enabler or a catalyst for positive change, and it can also be a disruptor, a distractor, and a liability. The value of technology use is rarely based on purely educational issues and tends instead to be a matter of convenience, mediation, and augmentation. To that extent, arguments for and against the use of TEL are as much, if not more, about educational economics rather than instruction. The challenge is to find more efficient and convenient ways to teach and learn, and these may or may not involve the use of technologies. TEL is also constrained by what is available. Teachers and learners tend to make do with and adapt to the affordances of the technologies they have at hand. Moreover, technologies tend to be used in an additive way rather than displacing existing practices. Displacement only happens when the convenience and utility of one technique so outweighs the other that it effectively withers away.
학습과 교수의 질은 많은 요소(학습 대상, 학습 내용, 학습 장소, 학습에 투입할 수 있는 시간과 노력 등)에 따라 달라진다는 점을 고려할 때, 특정 학습 테크놀로지가 대안(테크놀로지적 또는 기타)보다 나은지 나쁜지를 묻기보다는, 특정 학습자와 교사의 특정 요구 사항을 특정 장소와 시간에 지원하는 데 유용하고 효과적인지를 물어야 합니다. 따라서 저는 이 장에서 반복되는 주제, 즉 의료 교육의 테크놀로지적 중재가 빠르게 표준이 되고 있으며, 따라서 교육자들은 테크놀로지적 문제와 교육적 문제의 교차성을 둘 중 하나만 따로 고려하지 말고 함께 고려해야 한다는 주제로 돌아갑니다. 따라서 이 장에서 제시하는 아이디어와 원칙은 이 책의 다른 모든 장에서 제시하는 아이디어와 원칙과 교차하고 정보를 제공하는 것으로 이해해야 합니다. 테크놀로지가 의학에서 교육과 학습을 중재하고 보강하는 것과 마찬가지로, TEL 개념은 모든 다양한 형태와 관행에서 의학교육을 중재하고 보강하는 것으로 간주되어야 합니다.
Given that the quality of learning and teaching depends on so many things (considerations such as who is involved, what they are learning, where they are learning, and how much time and effort can they put into their learning and so on), then, rather than asking whether a particular learning technology is better or worse than an alternative (technological or otherwise), we should ask whether it is useful and effective in supporting particular needs of particular learners and teachers in a particular place and time. I therefore return to a recurring theme in this chapter; that technological mediation of medical education is rapidly becoming the norm and as such educators should consider the intersectionalities of technical and educational issues rather than one or the other in isolation. The ideas and principles I have set out in this chapter should therefore be understood as intersecting with and informing the ideas and principles set out in every other chapter in this book. In the same way that technologies mediate and augment teaching and learning in medicine, TEL concepts should be seen as mediating and augmenting medical education in all its many forms and practices.
Summary
Technology-enhanced learning (TEL) fully address the multitude of intersections between technology use and medical education practices. Central to the concept of TEL is a focus on the mediating role of technology. Teachers teach and learners learn; it is how they do these things (and what follows) that is changed by their use of technology. This chapter considers a range of theoretical frames for appraising the use of technology in medical education, and from these sets out a series of techniques for developing, using, and evaluating technology-enhanced learning in medical education. It provides a critical review of the positions, practices, opportunities, and challenges associated with using technology in contemporary medical education. The intersections between TEL and professionalism can be considered as a matter of 'digital professionalism'. Technologies can work as prostheses to compensate for suboptimal conditions.