보건의료에서 목소리 높히기의 최신지견 문헌고찰(Adv Health Sci Educ Theory Pract. 2022)
A state‑of‑the‑art review of speaking up in healthcare
Efrem Violato1
서론
Introduction
교육을 포함한 의료 분야에서는 [목소리를 높이는 것]을 지원하고 사람들이 [목소리를 높이는 데] 참여하도록 훈련할 책임과 필요가 있다. [목소리를 높이는 것]은 [다른 사람들이 환자 관리 및 안전과 관련된 우려를 인식하도록 하기 위한 우려 또는 다른 의견을 말하는 것]입니다. 현재 의료 시스템 전반에 걸쳐 [많은 실무자]에게 [환자 안전, 관리 및 위험에 대한 우려를 제기하는 방법]에 대한 인식된 능력(지식과 기술과 함께)은 충분하지 못하다. 목소리를 낼 수 없거나 목소리를 낼 수 없는 것은 환자의 안전, 교육, 전문성 발달 및 전문적 정체성에 부정적인 영향을 미칠 수 있다. 개인적, 대인적, 전문적, 그리고 조직적인 요인을 포함하여, 말을 하는 것을 어렵게 하고 심지어 직업적으로 그리고 개인적으로 위험하게 만드는 수많은 도전들이 존재한다. 일레인 브로밀리는 그러한 요인들의 합체 때문에 죽었다. 여러 자격을 갖춘 전문가들이 방안에 모여 '삽관이 산소를 공급할 수 없는' 상황을 겪은 후 [건강한 사람이 사망한 것]은 [사람들이 목소리를 내지 않거나 내지 못할 때 일어날 수 있는 일]을 상징적으로 보여준다. 대조적으로 팀이 약물과 전달 방법을 선택하도록 유도하는 것과 같이 직접적이고 지속적으로 목소리를 높이는 것은 잠재적으로 치명적인 오류를 피할 수 있다.
In healthcare, including education, there is a responsibility and need to support speaking up and train people to engage in speaking up (Milligan et al., 2017). Speaking up is voicing concern or a differing opinion to make others aware of a concern related to patient care and safety (Okuyama et al., 2014). Currently, for many practitioners across healthcare systems the perceived ability along with knowledge and skills of how to raise concern about patient safety, care, and risk is suboptimal (Jones et al., 2021; Kim et al., 2020; Milligan et al., 2017; Morrow et al., 2016). The absence of, or inability to, speak up can negatively impact patient safety, education, professional development, and professional identity (Bickhoff et al., 2017). Numerous challenges exist that make speaking up difficult and even professionally and personally risky including individual, interpersonal, professional, and organizational factors (Jones et al., 2021; Kim et al., 2020). Elaine Bromiley died because of the confluence of such factors. The death of a healthy person after a ‘can’t intubate can’t oxygenate’ situation with multiple qualified professionals in the room is emblematic of what can happen when people do not or can not speak up (Harmer, 2005). In contrast, directly and persistently speaking up, such as by questioning a team leads choice of drug and delivery method, can avoid potentially fatal errors (Calhoun et al., 2014).
한동안 존재했지만, [목소리를 높이는 것]에 대한 세계적으로 인정된 도전이 지난 10년 동안 표면화되었다. 문제에 대한 접근 방식은 다양한 관점을 통합했으며 그 결과 지식을 수집하고 문헌을 요약하는 다양한 형식의 리뷰 기사가 있었다.
While extant for some time, the globally recognized challenge of speaking up has come to the fore in the last ten years (Jones et al., 2021; Peadon et al., 2020). Approaches to the problem have incorporated different perspectives (Holmes et al., 2014; Kohn et al., 1999) and as a result there have been multiple review articles of different formats compiling knowledge and summarizing the literature.
리뷰 기사의 발표로, 말하기에 대한 문헌과 지식의 요약은 분류되고 다른 지식 흐름에 걸쳐 확산될 수 있다. 이미 목소리를 높이는 연구는 기존 증거에 대한 연속성과 연관성이 부족하며 새로운 연구는 이전의 결함을 수정하거나 이전의 발견을 기반으로 하지 않는다. 의료 분야에서 목소리를 높이는 연구는 비교적 초기 단계이기 때문에, 발전을 촉진하고 확산을 방지하기 위해 기존의 지식을 하나의 포괄적인 소스로 통합하는 것이 필수적이다. 이 기사는 목소리를 높이는 연구를 계획하는 연구자, 목소리를 높이는 방법에 대한 정책 입안자, 목소리를 높이는 교육자를 돕기 위해 현재의 "최첨단"을 대표하는 통일된 진술서를 만들고자 한다. 이 목적을 해결하기 위해 다음과 같은 유도 연구 질문이 개발되었다:
With the promulgation of review articles, summations of the literature and knowledge about speaking up may become fractionated and diffuse across different knowledge streams. Already, research on speaking up lacks continuity and connection to existing evidence and new research does not correct prior flaws or build on previous findings (Jones et al., 2021). Research on speaking up in healthcare is relatively nascent so it is imperative to bring together existing knowledge in a single comprehensive source to promote forward development and prevent diffusion. The present article seeks to create a unified statement representing the current "State of the Art" for speaking up to assist researchers planning studies on speaking up, policymakers deciding on how to improve speaking up, and educators developing curriculum and course material for speaking up. To address this purpose, a guiding research question was developed:
말을 하는 것에 관한 문헌 전반에 걸쳐 공통적인 발견을 식별하고 합성하여, 의료 분야에서 [목소리를 높이는 것]에 대한 연구와 지식의 현재 상태를 통일적으로 이해할 수 있는가?
Can common findings across the literature on speaking up be identified and synthesized to produce a unified understanding of the current state of research and knowledge about speaking up in healthcare?
방법들
Methods
최신 리뷰를 통합하여 향후 조사를 위한 현재 지식과 우선순위에 대한 종합적인 앤솔로지anthology를 효율적으로 구축하는 방식으로 최첨단 검토를 수행하였다. 최첨단 리뷰는 일차 연구의 공식적인 품질 평가를 포함하지 않고 더 높은 수준의 합성을 통해 지식을 병합하기 위한 리뷰를 수집하는 데 초점을 맞춘다. 검토 형식의 다양성은 이차 수준의 공식 평가의 가능성을 배제한다.
A State-of-the-Art review was conducted by amalgamating recent reviews to efficiently create a comprehensive anthology of the current knowledge and priorities for future investigation (Grant & Booth, 2009). A State-of-the-Art review does not include formal quality assessment of primary research but focuses on collating reviews to merge knowledge through higher-level synthesis. The diversity of review formats precludes the possibility of secondary level formal assessment (Fusar-Poli & Radua, 2018; Grant & Booth, 2009).
검색 전략
Search strategy
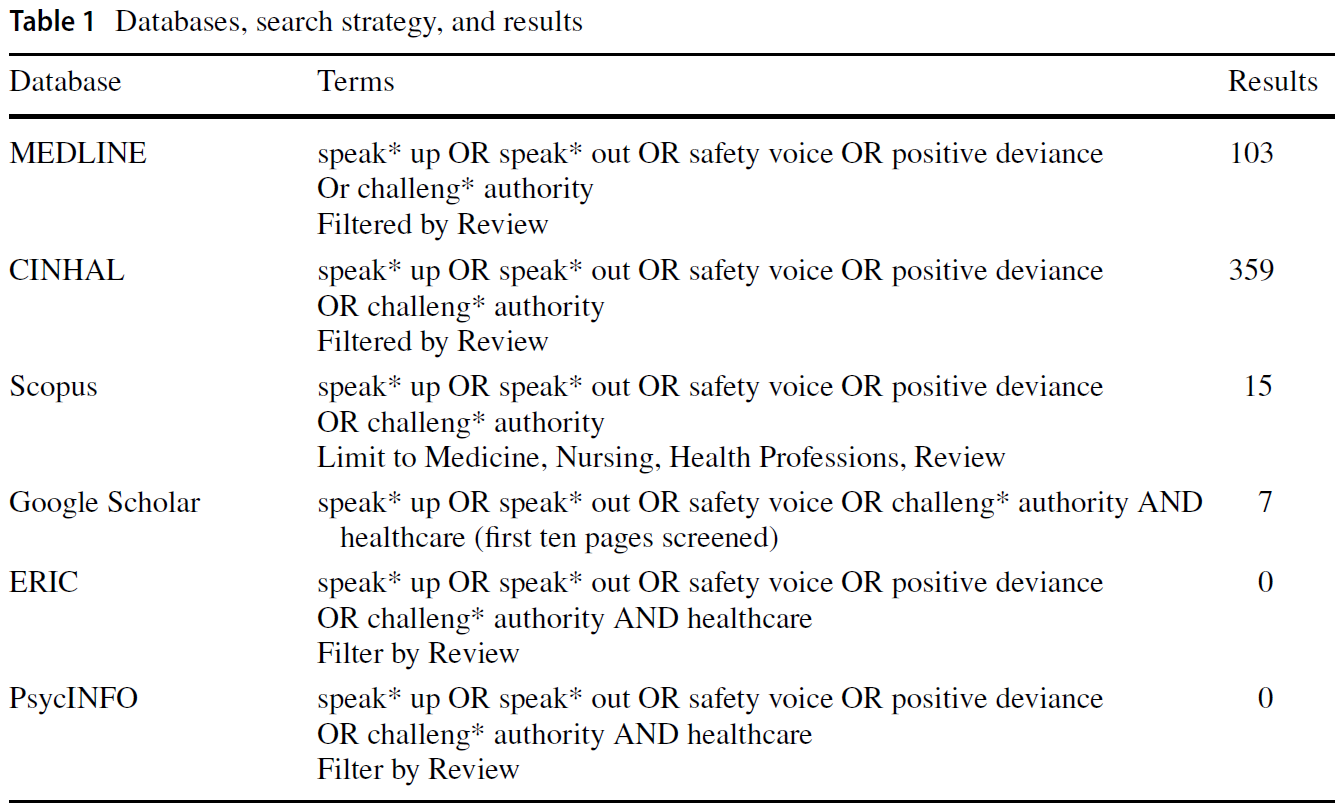
문헌은 MEDLINE, CINHAL, Scopus, Google Scholar, PsycINFO, ERIC를 사용하여 소스되었다. 수색은 2020년 10월에 처음 실시되었고 2021년 2월과 9월에 다시 실시되었다. 표 1은 검색어와 결과를 보여줍니다. 말하기 및 기타 출판물에 대한 연구를 위한 참조 목록을 손으로 검색했습니다.
Literature was sourced using MEDLINE, CINHAL, Scopus, Google Scholar, PsycINFO, and ERIC. The search was initially conducted in October 2020 and again in February and September 2021, with no year limits. Table 1 shows search terms and results. Reference lists for studies on speaking up and other publications were hand-searched (e.g., Mannion et al., 2018).
추출.
Extraction
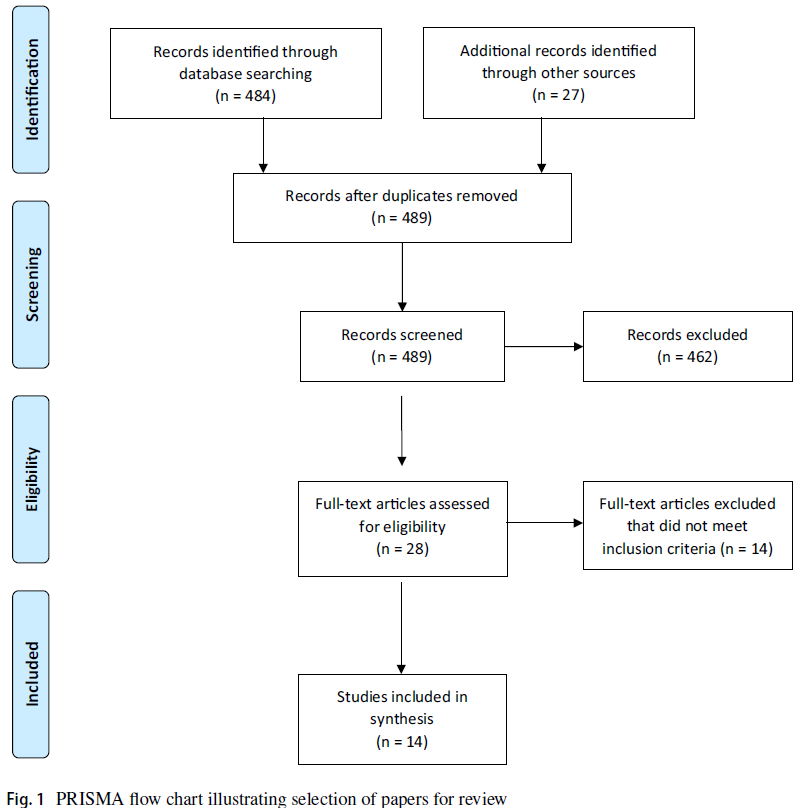
검색 및 검토 프로세스는 체계적 검토 및 메타 분석(PRSMA)을 위한 선호 보고 항목 형식을 따랐다(그림 1). 중복제거 후 주 조사관이 보다 면밀하게 검토할 수 있도록 제목과 요약을 포함하도록 선별했다.
- 포함 기준: 목소리를 높이고, 안전한 목소리를 내고, 권위에 도전하는 것에 관한 기사를 검토한다; 모든 검토 유형 및 방법.
- 제외 기준 : 비검토 기사, 예를 들어, 1차 소스 연구, 내부 고발에 대한 문헌, 일반적인 환자 옹호 및 환자 안전과 관련 없는 측면.
추가 기록은 전문가 간 교육 및 협업을 위한 자료와 팀 커뮤니케이션과 같은 다른 출처의 직접 검색을 통해 확인되었다.
The search and review process followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) format (Fig. 1) (Moher et al., 2009). After de-duplication, titles and abstracts were screened for inclusion for closer review by the principal investigator.
- Inclusion criteria: review articles on speaking up, safety voice, and challenging authority; all review types and methods.
- Exclusion criteria: non-review articles, e.g., primary source research, literature on whistleblowing, patient advocacy in general, and unrelated aspects of patient safety.
Additional records were identified through a hand search of other sources such as resources for interprofessional education and collaboration and team communication.
분석.
Analysis
연구 질문, 결과, 한계 및 결론과 같은 공통점을 식별하는 데 초점을 맞춘 상수 비교 분석(American Psychological Association, n.d.)의 반복 과정을 사용하였다. PI는 모든 기사를 읽고 요약하여 내용에 대한 개요와 일반적인 이해를 발전시켰다. 그런 다음 기사를 다시 읽고 각 검토의 결과를 추출했다. 연구 결과가 나오자 최종 합성이 가능할 때까지 모든 논문을 검토하여 새로운 연구 결과와의 일치성을 확인했다.
An iterative process of constant comparative analysis (American Psychological Association, n.d.), focused on identifying commonalities such as research questions, outcomes, limitations, and conclusions was used. All articles were read and summarized by the PI to develop a compendium and general understanding of the content. Articles were then re-read, and the findings of each review were extracted. As findings emerged, all articles were reviewed to determine concordance with the emergent findings until a final synthesis was possible.
결과.
Results
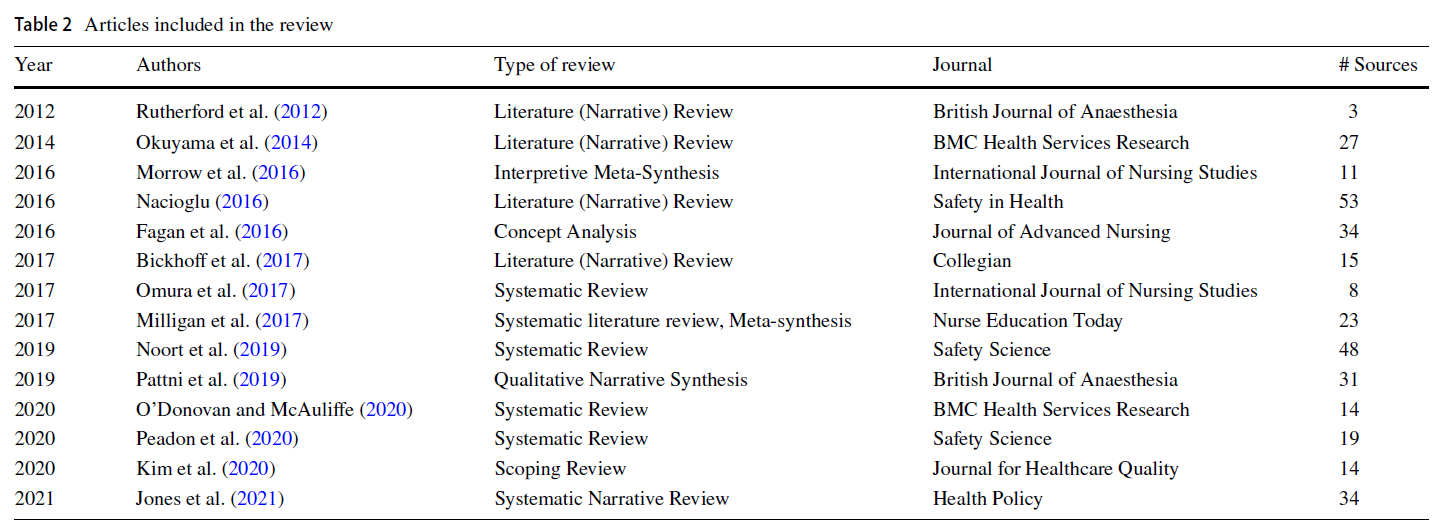
14개의 리뷰 기사를 분석하였다(표 2). 14개의 리뷰는 양적, 질적, 혼합적 방법 연구, 논평, 이론 논문 등 335개의 기사를 다루었다. 335개의 기사 중 51개는 150개의 복제 기사와 236개의 고유 기사에 대한 다중 리뷰를 포함했다(모든 기사에 대해서는 보충 자료 참조). 가장 자주 검토된 논문은 Pian-Smith 외 연구진(2009)(검토 8배), Raemer 외 연구진(2016)(검토 7배), Schwapach and Gerrick(2014)(검토 6배), Johnson and Kimsey(2012)(검토 6배), Sayre 외 연구진(2012)(검토 6배), Barzo Salazar et al(2014)(검토 5배)이다. 이 기사 세트는 반복적으로 인용되는 기사의 29%를 차지했다.
Fourteen review articles were analyzed (Table 2). The 14 reviews covered 335 articles, including quantitative, qualitative, mixed methods research, commentaries, and theoretical papers. Fifty-one of the 335 articles included multiple reviews, for 150 replications and 236 unique articles (for all articles, see the supplemental material). The articles most frequently reviewed were: Pian-Smith et al (2009) (reviewed 8×), Raemer et al (2016) (reviewed 7×), Schwappach and Gehrig (2014) (reviewed 6×), Johnson and Kimsey (2012) (reviewed 6×), O’Connor et al. (2013) (reviewed 6×), Sayre et al (2012) (reviewed 6×), Barzallo Salazar et al. (2014) (reviewed 5×). This set of articles accounted for 29% of repeatedly cited articles.
주요 소스는 여러 글로벌 지역의 데이터를 나타냅니다: 아시아(홍콩, 일본, 한국, 네팔, 대만), 아프리카(동아프리카, 케냐), 유럽(불가리아, 키프로스, 핀란드, 아일랜드, 이탈리아, 스웨덴, 스위스), 중동(이란, 이스라엘)이다. 가장 빈번하게 제공된 기사는 호주와 뉴질랜드, 캐나다, 미국, 영국에서 왔다. 대부분의 문헌은 학생들을 포함한 의사와 간호사들에 초점을 맞추었다. 소수의 문헌은 연합된 보건 전문가, 행정, 약사, 환자를 조사했다(보조 자료 참조).
The primary sources represented data from multiple global regions: Asia (Hong Kong, Japan, Korea, Nepal, Taiwan), Africa (East Africa, Kenya), Europe (Bulgaria, Cyprus, Finland, Ireland, Italy, Sweden, Switzerland), and the Middle East (Iran, Israel). The articles most frequently sourced were from Australia and New Zealand, Canada, the United States, and the United Kingdom. Most of the literature focused on physicians and nurses, including students. A minority of the literature examined allied health professionals, administration, pharmacists, and patients (see supplemental material).
현상의 정의
Definition of the phenomena
모든 기사들은 [목소리를 높이는 것]을 정의했다. Okuyama 외 연구진(2014)은 Leonard 외 연구진(2004)과 Lyndon 외 연구진(2012)에서 파생된 간결하고 포괄적인 정의를 제공했다: "목소리 높이기"는 병원 환경에서 [의료 팀 내의 다른 사람들의 위험하거나 부족한 행동]을 인식하거나 인지할 때, 환자 안전과 의료 품질의 이점에 대한 의료 전문가들의 [우려를 제기]하는 것으로 정의된다
All articles defined speaking up similarly. Okuyama et al. (2014) provided a concise and comprehensive definition, derived from Leonard et al. (2004) and Lyndon et al. (2012), that encompassed the definitions used by all the reviews: “Speaking up' is defined as the raising of concerns by healthcare professionals for the benefit of patient safety and care quality upon recognising or becoming aware of the risky or deficient actions of others within healthcare teams in a hospital environment.”
14개 리뷰에 걸쳐 목소리를 높이기 위한 세 가지 맥락이 조사되었다:
- (1) 훈련을 포함한 팀 상황;
- (2) 의료 계층 내의 일반적인 맥락
- (3) 주로 간호학과 학생들에 초점을 맞춘 전문 그룹들 사이의 차이.
모리슨의 '직원 목소리' 모델을 변형한 위험한 상황에서 목소리를 높이는 행위인 '안전 목소리'는 대중적인 해석 프레임워크였다.
- [직원 목소리]는 더 높은 조직 위치에 있는 누군가에게 관심, 제안, 정보 또는 업무 관련 의견을 자발적으로 전달하는 것입니다.
- [안전 목소리]은 개념적으로 직원 목소리와 유사하지만, 내용과 메시지가 안전에 초점을 맞추고, 맥락이 안전-중시 조직과 관련되어 있으며, 조치가 법적으로 요구될 수 있으며, 조치가 조직(예: 내부 고발)을 넘어 확장될 수 있다는 점에서 다르다.
Across the 14 reviews, three contexts for speaking up were examined:
- (1) team situations, including training;
- (2) general contexts within the hierarchies of healthcare; and
- (3) differences amongst professional groups, focused primarily on nursing and students.
‘Safety voice’, the act of speaking up in hazardous situations adapted from Morrison's model of ‘employee voice’ (Morrison, 2011; Noort et al., 2019) was a popular interpretive framework.
- Employee voice is voluntary communication of concerns, suggestions, information, or work-related opinions to someone in a higher organizational position (Morrison, 2014).
- Safety voice is conceptually similar to employee voice though differs in that the content and message are focused on safety, the context relates to safety–critical organizations, action may be legally required, and the action can extend beyond the organization e.g., whistleblowing (Noort et al., 2019).
용어 및 언어
Terms and language
도전적인 권위를 정의하고 논의하기 위한 공통 언어는 다음을 포함한다: "Speaking Up", "Hierarchies", "Psychological Safety", "Safety Voice", "Challengeing Authority", "Communication"
Common language to define and discuss challenging authority, included:
- "Speaking Up,"
- "Hierarchies,"
- "Psychological Safety,"
- "Safety Voice,"
- "Challenging Authority," and
- "Communication."
'엘리트에 의한 불경', '돌봄 전문가의 춤', '순환 위계', '불도덕성', '청렴의 의무', '수평적 폭력', '불건전한 순종' 등 다양한 용어가 등장했다
Variable language and unique terms arose including
- "Incivility by Elites” (Morrow et al., 2016),
- "Dance of Caring Professionals (Morrow et al., 2016),"
- "Circular Hierarchy (Morrow et al., 2016),"
- "Immorality (Okuyama et al., 2014),"
- "Duty of Candor (Milligan et al., 2017),"
- "Lateral [Horizontal] Violence (Milligan et al., 2017)," and
- "Unwholesome Submissiveness (Peadon et al., 2020)."
연구 질문 및 검토 결과
Research questions and findings of the reviews
각각의 리뷰는 독특한 연구 질문으로 문헌에 대한 독특한 조사를 제안했다. 모든 검토에서 조사 결과를 정리할 수 있는 5가지 공통 질문이 존재했다:
- (1) 어떤 개입/훈련이 사용되었으며 얼마나 효과적입니까?;
- (2) 어떤 메커니즘이 목소리를 높이는 데 영향을 미칩니까? ;
- (3) 목소리를 높이는 것에 대한 사람들의 인식과 경험은 무엇인가? ;
- (4) 사람들은 어떻게 말합니까?;
- (5) 목소리를 높이는 것이 얼마나 효과적인가?
Each review proposed to be a unique investigation of the literature with unique research questions. Across all reviews five common questions existed under which findings can be organized:
- (1) what interventions/training have been used and how effective are they? (Jones et al., 2021; Kim et al., 2020; Milligan et al., 2017; Nacioglu, 2016; O’Donovan & McAuliffe, 2020; Okuyama et al., 2014; Omura et al., 2017);
- (2) what mechanisms (inhibitors/enablers) influence speaking up? (Bickhoff et al., 2017; Nacioglu, 2016; Okuyama et al., 2014; Peadon et al., 2020);
- (3) what are people's perceptions and experiences of speaking up? (Fagan et al., 2016; Morrow et al., 2016; Noort et al., 2019; Pattni et al., 2019);
- (4) how do people speak up? (Bickhoff et al., 2017; Morrow et al., 2016; Pattni et al., 2019; Rutherford et al., 2012);
- (5) how effective is speaking up? (Milligan et al., 2017; Nacioglu, 2016; Okuyama et al., 2014).
어떤 개입/훈련이 사용되었으며, 얼마나 효과적입니까?
What interventions/training have been used, and how effective are they?
[목소리 높이기]는 보건 전문가 교육의 필수적인 부분으로 간주되지만 말하기/주장 훈련/갈등 훈련에 대한 커리큘럼과 체계적인 훈련이 부족하여 교육 격차가 존재한다. 5가지 형태가 확인되었다.
- 교육 및 시뮬레이션,
- 교육 및 리더십 비디오,
- 교육 및 사례 연구,
- 교육 워크샵
- 비교육적 개입 (포럼 놀이, 전체론적 촉진 및 행동 연구 회의로 구성)
Speaking up is considered an essential part of health professionals' education, yet an educational gap exists with a lack of curriculum and systematic training on speaking up/assertiveness training/conflict training (O’Donovan & McAuliffe, 2020; Omura et al., 2017; Pattni et al., 2019). Five forms of intervention have been identified:
- education and simulation,
- education and leadership videos,
- education and case studies,
- educational workshops, and
- non-educational interventions, comprising forum play, holistic facilitation, and action research meetings (Jones et al., 2021; Kim et al., 2020; O’Donovan & McAuliffe, 2020; Okuyama et al., 2014; Omura et al., 2017).
목소리를 높이기 위한 훈련과 개입에 대한 연구는 비교적 새로운 것으로 [효능 증거는 제한적이다]. 일반적으로, 목소리를 높이기 위한 교육적 개입은 [태도와 자신감]에 대한 짧은 지속적인 긍정적 영향을, [행동]에 대한 영향은 미미하거나 결여되어 있다. [팀 훈련]과 [적극적인 의사소통]에 대한 개입은 어느 정도 효과적이지만, [코칭 기반의 훈련]은 효과적이지 않은 것으로 보인다. 항공, 특히 [CRM(Crew/Crisis Resource Management)]에서 적용된 팀 기술 훈련 및 커뮤니케이션 기법이 긍정적으로 평가되었으며, 태도, 자신감 및 행동에 가장 강력한 긍정적 효과를 보였다. 개입의 구체적인 특징은 일관된 긍정적 효과를 보여주지 않는다.
Research on training and interventions for speaking up is relatively new with limited efficacy evidence. Generally, educational interventions for speaking up have weak short lasting positive effects on attitudes and confidence with effects on behaviour being minimal or absent. Interventions for team training and assertive communication are somewhat effective, coaching based training does not appear to be effective. Team skills training and communication techniques adapted from aviation, specifically Crew/Crisis Resource Management (CRM) were positively evaluated, and showed the strongest positive effects on attitudes, confidence, and behaviour (Fagan et al., 2016; Jones et al., 2021; Kim et al., 2020; Milligan et al., 2017; Nacioglu, 2016; O’Donovan & McAuliffe, 2020; Okuyama et al., 2014; Omura et al., 2017; Pattni et al., 2019; Peadon et al., 2020). No specific characteristics of interventions show consistent positive effects.
어떤 메커니즘(활성화/억제제)이 목소리를 높이는 데 영향을 미칩니까?
What mechanisms (enablers/inhibitors) influence speaking up?
많은 선행 사례들이 목소리를 높이는 것을 억제하거나 가능하게 하는 것으로 확인되었지만, [소수의 메커니즘]만이 억제, 가능 또는 둘 다로 일관되게 확인되었다.
Numerous antecedents have been identified as inhibiting or enabling speaking up, though only a few mechanisms were consistently identified as inhibitory, enabling, or both (Bickhoff et al., 2017; Fagan et al., 2016; Jones et al., 2021; Kim et al., 2020; Morrow et al., 2016; Noort et al., 2019; Omura et al., 2017; Pattni et al., 2019; Peadon et al., 2020).
Inhibitors of speaking up
확인된 [주요 억제 메커니즘]은 [위계 구조]와 [권력 역학]이었지만, 실험 조건에서 위계 구조를 평탄화하는 것이 지속적으로 목소리 높이기를 개선하지는 않았다. [위계 구조]는 간호사와 학생 간호사 사이와 같은 [Intraprofessional]한 것과, 마취사와 호흡기 치료사 사이와 같은 [Interprofessional]한 것이 있다. [Inter 및 Intra professional한 위계]의 장벽과 수행자 직업 문화는 종종 [하위 계층, 특히 학생들에 의해 극복될 수 없는 것]으로 여겨지나, [고위 의사를 포함하여 더 상급 위치에 있는 사람들에게도 극복될 수 없는 것]으로 여겨졌다. 위계와 문화가 [극복할 수 없을 정도로 명백한 것]은 종종 목소리를 높이려고 노력하는 것조차 허무감을 만들어낸다.
- [위계구조]와 [권력 역학]은 역할, 책임, 직업적 고정관념에 대한 기대감을 조성하고 뒷받침함으로써 목소리를 높이는 것을 제약하는 것으로 확인되었다.
- [고정관념]은 목소리를 높이는 것에 대한 수용, 목소리를 높이는 인식 능력, 목소리를 높이는 것에 대한 책임감을 감소시키고 계층의 제약에 도전하는 것을 피하게 할 수 있다.
The primary inhibitory mechanism identified was hierarchies and power dynamics, though in experimental conditions flattening hierarchies does not consistently improve speaking up (Bould et al., 2015; Friedman et al., 2015; Sydor et al., 2013). Hierarchies are both
- intraprofessional, such as between a charge nurse and a student nurse, and
- interprofessional such as between an anesthetist and a respiratory therapist.
Inter and intra professional hierarchical barriers and attendant professional cultures are often seen to be insurmountable by those lower in hierarchies, in particular students, but also by those in more advanced positions including senior medical doctors (Peadon et al., 2020). The apparent insurmountably of hierarchy and culture often create a sense of futility in even trying to speak up (Morrow et al., 2016).
- Hierarchies and power dynamics were identified as constraining speaking up by creating and supporting expectations about roles, responsibilities, and professional stereotypes.
- Stereotypes can inhibit acceptance of speaking up, perceived ability to speak up, diminish responsibility for speaking up, and lead to avoidance of challenging the constraints of hierarchy.
- [심리적 안전성]의 부족은, 인식이든 실제이든, [보복, 갈등, 괴롭힘, 괴롭힘 등 부정적인 결과에 대한 두려움] 및 [다른 사람들의 능력에 의문을 제기하는 것에 대한 우려]를 유발하여 목소리를 높이는 것을 억제한다.
- [부정적인 결과에 대한 두려움]은 상황에 따라 달라질 수 있다;
- 학생은 부정적인 평가를 두려워할 수 있는 반면,
- 상급 전문가는 동료의 능력에 의문을 제기하는 것처럼 보임으로써 동료의 기분을 상하게 하고 싶지 않을 수 있다.
- [일관성 없는 언어 및 훈련], 그리고 [목소리 높이기의 구성요소에 대한 이해의 불화]도 억제적이다.
- A lack of psychological safety, perceived or actual, inhibits speaking up through fear of negative consequences, including reprisal, conflict, bullying and harassment, and concerns about questioning others' competency.
- Fear of negative consequences can be context-dependent;
- a student may fear a negative evaluation,
- while a senior professional may not want to offend a colleague by appearing to question the colleague's competency.
- Inconsistent language, training, and discordant understandings about what constitutes speaking up are inhibitory.
Enablers of speaking up
["안전한 목소리"]를 갖는 것은 목소리를 높이는 것을 가능하게 한다; 그러나 안전 음성의 의미는 "분해되고 초기disintegrated and nascent"이다. 가장 일관성 있게 파악된 지지 요인은 [관리적 및 행정적 지원을 통한 조직적 지원]이었습니다.
- [조직적 지원]에는 리더십 직책에 있는 사람들이 모델, 멘토링, 격려 및 목소리를 높이는 행동을 받아들이는 것이 포함됩니다.
- [시스템 지원]은 주로 접근 가능한 보고 시스템과 "내부고발"에 대한 지원으로 식별되었다.
[서포트가 필요하다는 인식]은 [조직적 지원을 만들어내는 데] 필요하다. 이 때 [하향식 지원]을 동반함으로써, [목소리를 낼 수 있다고 느끼게 임파워링empowerng]하면서 [심리적으로 안전한 조직이나 환경]을 만들어낼 수 있다.
Having "safety voice" is an enabler of speaking up; however, the meaning of safety voice is "disintegrated and nascent" (Noort et al., 2019). The most consistently identified enabler was organizational support through managerial and administrative support.
- Organizational support includes those in leadership positions modeling, mentoring, encouraging, and accepting speaking up behaviour.
- System supports were mainly identified as accessible reporting systems and support for “whistleblowing” (Fagan et al., 2016).
Awareness of the need to provide support is required to create organizational support, with top-down support necessary to create an empowering and psychologically safe organization or environment where a person feels it is possible to have a voice (Morrow et al., 2016; O’Donovan & McAuliffe, 2020).
- [목소리를 높이는 것에 대한 지원]은 또한 환자 중심성, 환자 안전 및 전문적인 원칙 보호와 같은 [전문직업적 의무(예: 환자 옹호자가 되는 것)]로부터 온다.
- [임상 및 안전 관련 경험과 지식]은 모두 도움이 됩니다.
- 목소리를 높이는 부정적인 방향의 enabler는 "감정적 빌드업"이다; 사람들은 목소리를 내지 않는 것이 불가능하다는 것을 발견하는 "감정적 빌드업"의 수준에 도달하곤 한다.
- Support for speaking up also comes from professional mandates such as patient-centeredness, patient safety, and safeguarding professional principles, e.g., being a patient advocate (Bickhoff et al., 2017).
- Experience and knowledge, both clinical and safety-related, are supportive (Fagan et al., 2016; Okuyama et al., 2014).
- A negatively oriented enabler of speaking up is “emotional buildup”; people reach a level of “emotional buildup” where they find it impossible not to speak up (Morrow et al., 2016).
Inhibitor/enabler of speaking up
- [위계 구조]는 주요 억제 메커니즘이지만, [상급 위치에 있는 사람들이 목소리를 높이고, 조언하고, 가능하게 하고, 받아들일 때], 목소리를 높이는 것을 긍정적으로 지원할 수 있는 의료의 필수적인 측면으로 간주된다;
- 예를 들어, 개별 [간호사 관리자]들은 학생들이나 그들 이하의 다른 사람들이 목소리를 높이는지 여부에 긍정적 또는 부정적인 영향을 미칠 수 있다.
- [상호 존중의 긍정적인 멘토-멘티 관계]의 경우, 너무 많은 존중이 의사소통을 방해하는 반면, 부정적인 관계는 의사소통을 방해할 수 있지만, 목소리를 높이는 것을 지지할 수 있다.
- [개인적 요소](문화적, 세대적 배경, 태도, 성격, 성별, 경험, 자신감 등)도 억제하거나 가능하게 할 수 있다. 이러한 개별 특성이 어떻게 기능하는지는 상황에 따라 달라질 수 있습니다.
- [학생]은 조직적인 지원, 임상 지식, 안전에 대한 헌신, 그리고 목소리를 낼 수 있는 자신감을 갖기 위한 [기술과 도구가] 필요할 수 있다.
- 반면 [경험이 많은 동료]는 조직 지원이나 의견 표명을 위한 [도구의 필요성을 느끼지 못할 수도] 있습니다.
- While being the primary inhibitory mechanism, hierarchy is also seen as a necessary aspect of healthcare that can positively support speaking up when those in advanced positions model, mentor, enable and accept speaking up; e.g., individual nurse managers can have a positive or negative effect on whether students or others below them speak up (Morrow et al., 2016).
- A positive mentor–mentee relationship of mutual respect can support speaking up, though too much respect may prevent speaking up, while a negative relationship impedes communication.
- Individual factors like cultural and generational background, attitudes, personality, sex, experience, and confidence could be inhibitory or enabling. How these individual characteristics function is developing and can vary based on context.
- A student may need organizational support, clinical knowledge, a commitment to safety, and the skills and tools for speaking up to have the confidence to speak up.
- Simultaneously, a more experienced colleague may not feel a need for organizational support or tools for speaking up.
관련성은 불분명하지만 [문화적 고려]가 중요하다.
- [위계적 구배]가 의료 문화에 너무 깊이 뿌리박혀 있어서, 그 효과가 국가 문화적 영향을 대체할 수도 있지만,
- 반대로 [국가 문화]가 너무 강해서 직업적 변화와 개입을 무시할 수도 있다.
Cultural considerations are important though the relevance is unclear (Jones et al., 2021).
- Hierarchy gradients may be so ingrained in medical culture that the effects supersede national cultural influences (Kobayashi et al., 2006),
- or alternatively, national culture is so strong it overrides professional changes and intervention (Roh et al., 2015).
목소리를 높이는 것에 대한 사람들의 인식과 경험은 무엇인가?
What are people's perceptions and experiences of speaking up?
전반적으로, [목소리 높이기]에 대한 인식과 경험은 부정적이며, 이것이 [목소리 높이기]를 억제하는 메커니즘이 될 수 있다. 개인과 조직은 종종 [목소리를 높이는 것]이 가치가 있지만, [적극적으로 장려되지는 않는다]고 말한다. 목소리를 높이고 공개적인 의사소통은 효과적이지 않고, 직업적으로 안전하지 않은 [고-위험, 저-보상 행동]으로 간주되며, 학대와 같은 다른 [부정적인 결과에 대한 두려움]을 수반한다. 게다가, 말하는 행동은 종종 [무시]되고, [언제 목소리를 높여야 하는지, 무엇에 대해 높여야 하는지가 불분명]한 경우가 많다. 사람들은 목소리를 높이는 것이 동료들과 [동료들에게 굴욕감을 줄 것]이라고 생각할지도 모른다. 부정적인 결과에 대한 학생들의 우려는 주로 [(자신에 대한) 부정적인 평가]와 [미래의 연습practice에 대한 영향]과 관련이 있다. 안전하지 않은 상황과 환자에 대한 우려를 개선하는 것이 목소리를 높이는 주된 이유입니다. 목소리를 높이는 것은 [감정적인 부담]을 수반할 수 있으며, 조직, 고위직 동료, 동료들의 지원과 함께 [용기가 필요]하다.
Overall, perceptions and experiences of speaking up are negative and can be inhibitory mechanisms on speaking up. Individuals and organizations frequently indicate speaking up is valued but is not actively encouraged. Speaking up and open communication is viewed as a high-risk, low reward behaviour that is ineffective and professionally unsafe, carrying a fear of abuse and other negative consequences. Further, speaking up behaviour is often ignored, and it is often unclear when to speak up and what speaking up entails. People may think speaking up will humiliate peers and colleagues. Student concerns over negative consequences primarily relate to negative assessment and impacts on future practice. Improving unsafe situations and concern for the patient is the primary reason for speaking up. Speaking up may carry an emotional burden, and courage along with support from organizations, colleagues of senior status, and peers is required (Bickhoff et al., 2017; Fagan et al., 2016; Milligan et al., 2017; Morrow et al., 2016; Nacioglu, 2016; Noort et al., 2019; Okuyama et al., 2014; Peadon et al., 2020).
사람들은 어떻게 목소리를 높일까요?
How do people speak up?
사람들이 실제로 어떻게 목소리를 높이는지에 대한 연구가 부족하다. 종종 사람들은
- 질문이나 제안을 위한 [매니퓰레이팅 발화]같은 [간접적 방법]을 사용하거나
- [행동을 피하고], [오더를 넣치 않는 것]과 같은 [하극상subversion]을 사용하는 [부정적이거나 침묵적인 방법]을 사용한다.
- [긍정적인 방법]은 사실을 수집하고, 목소리를 높이려는 의도를 보여주고, 언제 어디서 목소리를 내야 하는지에 대한 구체적인 대상을 파악하는 것이다.
There is a paucity of research on how people speak up in practice (Bickhoff et al., 2017; Milligan et al., 2017; Morrow et al., 2016; Noort et al., 2019; Okuyama et al., 2014; Rutherford et al., 2012). Often people
- engage in indirect methods by manipulating speech to use questions or suggestions or
- use negative or silent methods by avoiding action and using subversion, such as not filling an order.
- Positive methods include collecting facts, showing an intent to speak up, and identifying specific targets for when and where to speak up.
[목소리 높이기 행동]에 대한 많은 증거는 학생에 관한 것이다. 학생들은 언제 누구에게 걱정을 보고해야 할지 모른다. 목소리를 높이는 것을 생각할 때, 사람들은 [결과에 대한 효용과 기대를 저울질하고 평가]한다. 전문가 간의 연구와 행동 등급 척도와 같은 객관적인 척도의 부재로 인해 목소리를 높이는 데 있어 전문적인 차이에 대한 경험적 증거가 부족하다.
Much of the evidence on speaking-up behaviour is for students, who often do not know when and to whom to report concerns. When considering speaking up people weigh and evaluate the utility and expectations about outcomes. Empirical evidence for professional differences in speaking up is lacking due to an absence of cross-professional research and objective measures like behavioural rating scales.
목소리를 높이는 것은 얼마나 효과적인가?
How effective is speaking up?
연구 부족으로 인해 실제로 목소리를 높이는 것의 효과는 알려져 있지 않다. 연구와 증거의 우세는 교육 개입과 훈련의 효과에 초점을 맞추고, 목소리를 높이면서 스스로 보고한 경험에 초점을 맞춘다. 환자의 목소리를 높이는 것이 환자의 목소리를 높이는 것이 잘 받아들여지지 않는다는 것을 발견한 연구는 거의 없다.
In practice effectiveness of speaking up is unknown due to a lack of research. The preponderance of research and evidence focuses on the effectiveness of educational interventions and training and self-reported experiences with speaking up. Very few studies have investigated patient speaking up those that have found patient speaking up is not well received (Nacioglu, 2016).
시뮬레이션의 중요성
The importance of simulation
시뮬레이션은 교육 및 훈련을 조사하는 데 중요한 것으로 간주된다; 그러나 시뮬레이션 기반 연구는 부족하다. 14개 리뷰에 걸쳐 17개의 시뮬레이션 기반 연구가 명시적으로 식별되었다(추가 자료 참조). Patni 외 연구진(2019)은 시뮬레이션 연구와 대조적으로 자기 보고서 연구가 널리 퍼져 있다고 확인했다. 시뮬레이션 기반 연구의 [세 가지 유형]이 확인되었다:
- 교육 검증
- 장벽의 효과(예: 엄격한 계층) 검증
- 목소리를 높이기 위한 방법 검증(예: 2단계 규칙).
시뮬레이션 연구의 논의는 [효용, 과제, 개선]의 세 가지 영역에 초점을 맞추었다.
Simulation is considered important for investigating education and training; however, there is a dearth of simulation-based research. Across the fourteen reviews, seventeen simulation-based studies were explicitly identified (see supplemental material). Pattni et al. (2019) identified self-report studies were pervasive contra to simulation studies. Three types of simulation-based studies were identified:
- testing education,
- testing effects of barriers (e.g., strict hierarchy), and
- testing methods to speak up (e.g., two-challenge rule).
The discussion of simulation research focused on three areas: utility, challenges, and improvement (Fagan et al., 2016; Kim et al., 2020; Morrow et al., 2016; Noort et al., 2019; O’Donovan & McAuliffe, 2020; Okuyama et al., 2014; Omura et al., 2017; Pattni et al., 2019; Peadon et al., 2020).
시뮬레이션의 효용
Utility of simulation
[시뮬레이션]은 [목소리 높이기와 관련된 교육, 훈련 및 개념을 검증]하기 위한 유망한 방법으로 간주된다. 주요 효용은 [성과와 행동의 객관적인 측정을 얻는 것]으로 간주된다. 또한 시뮬레이션은 개별 요인(예: 태도, 성격, 의사소통 능력) 및 수식자와 장벽(예: 평평한 팀 대 계층 구조 팀)의 영향을 측정하는 데 유용하다. 시뮬레이션은 또한 사람들이 기술을 연습하고 교훈적으로 전달된 지식을 통합할 수 있게 하며 시나리오 기반 학습에 대한 학생들의 욕구를 충족시키며 새로운 말하기 방법을 테스트하고 개발하는 환경으로 사용될 수 있다.
Simulation is viewed as a promising modality for education, training, and testing concepts related to speaking up (Fagan et al., 2016; Noort et al., 2019; O’Donovan & McAuliffe, 2020; Okuyama et al., 2014; Omura et al., 2017; Pattni et al., 2019; Peadon et al., 2020). The primary utility is seen as obtaining objective measurements of performance and behaviour. Additionally, simulation is useful in measuring the effects of individual factors (e.g., attitudes, personality, communication skills) and the impact of modifiers and barriers (e.g., flat vs. hierarchically structured teams). Simulation can also allow people to practice skills and incorporate knowledge delivered didactically and fulfills students' desire for scenario-based learning and can be used as an environment to test and develop new speaking up methods.
시뮬레이션 과제
Challenges of simulation
[거의 모든 리뷰는 시뮬레이션을 비판]했으며, [시뮬레이션 기반 연구는 한계로 간주]되었다. [일차적인 비판]은 시뮬레이션이 임상 환경과 일치하지 않으며, 시뮬레이션에 의존하는 개입의 효과가 부족한 원인이 된다는 것이었다. 시뮬레이션 중에 참가자로부터 인식된 [책임과 긴급성이 결여]되어 있다고 가정한다. 흥미롭게도 [저 위험 설정]으로 간주되는 시뮬레이션 연구와 참가자들이 훈련을 받은 후에, 목소리를 높이는 [효과가 모든 곳에서 발생하지는 않았다]. 참가자에게 생소한 시나리오와 맥락, 시간 압축, 종단적 연구 부족 등 [시뮬레이션 방법에 초점을 맞춘 추가 비평]이 이어졌다. 시뮬레이션 동안 [사용된 평가의 신뢰성]은 부적절한 척도와 일관성 없는 관찰자/평가자 훈련으로 인해 제한된 것으로 간주되었다. 확인된 유일한 무작위 대조군 시험은 시뮬레이션 연구였지만, 전반적인 품질은 낮았다.
Nearly every review critiqued simulation, with simulation-based research being considered a limitation. The primary critique was that simulation does not match the clinical environment and the lack of verisimilitude is a cause of the lack of effectiveness of interventions that rely on simulation. It is assumed there is a lack of perceived responsibility and urgency from participants during simulation. Interestingly across simulation studies, which are considered low risk settings, and after participants received training, speaking up was not ubiquitous (O’Donovan & McAuliffe, 2020; Omura et al., 2017; Pattni et al., 2019; Peadon et al., 2020). Additional critique focused on simulation methods, including scenarios and contexts unfamiliar to participants, time compression, and lack of longitudinal study (Omura et al., 2017). The reliability of assessments used during simulation was considered limited due to inadequate measures and inconsistent observer/rater training. While the only Randomized Control Trials identified were simulation studies, the overall quality was low (Omura et al., 2017).
시뮬레이션 개선
Improvement to simulation
오무라 외 연구진(2017)에 따르면 한계에도 불구하고 시뮬레이션은 유리하고 중요하며 계속 사용되어야 한다. "…시뮬레이션을 사용한 관찰자 기반 결과 측정은 반응, 지식 및 태도뿐만 아니라 행동 변화도 평가할 수 있음이 분명하다."
리뷰 전반에 걸쳐 [시뮬레이션 개선]은 다음과 같은 6가지 제안에 초점을 맞추고 있다:
- (1) 시뮬레이션에서 행동 결과를 자주 측정하고, 행동을 평가하는 더 나은 방법을 개발한다;
- (2) 실제 시나리오, 텍스트, 언어 및 대화를 사용하여 실제 관측에서 역방향으로 시뮬레이션을 설계함으로써 생태학적 대응성이 향상된 시뮬레이션을 설계;
- (3) 실험 방법과 사전 테스트 방법을 사용하여 [목소리 높이기의 원인 메커니즘과 장벽을 이해]한다;
- (4) 학습을 촉진하고 신뢰를 유지하기 위해 좋은 디브리핑 전략을 사용한다(특히 속임수를 사용할 때에)
- (5) 시뮬레이션에서 교육 및 훈련의 효과를 실무 결과와 연결하기 위해 종단 연구를 사용한다;
- (6) 시뮬레이션 교육을 위해 멀티미디어 및 확장 현실을 사용하여 탐색합니다.
Despite the limitations, simulation is viewed as advantageous, important and should continue to be used, according to Omura et al. (2017), "…it is evident that observer-based outcome measures with simulation can evaluate not only, reaction, knowledge and attitudes, but also behaviour change". Across the reviews, improvements to simulation focus on six suggestions (Fagan et al., 2016; Kim et al., 2020; Morrow et al., 2016; Noort et al., 2019; O’Donovan & McAuliffe, 2020; Okuyama et al., 2014; Omura et al., 2017; Pattni et al., 2019; Peadon et al., 2020):
- (1) Frequently measure behavioural outcomes in simulation and develop better methods of assessing behaviour;
- (2) Design simulations with better ecological correspondence by designing simulations backward from real-world observations using real scenarios, text, language, and conversation;
- (3) Use experimental methods and pre-test measures to understand causative mechanisms and barriers of speaking up;
- (4) Use good debriefing strategies to facilitate learning and maintain trust, especially when deception is used;
- (5) Use longitudinal studies to connect the effects of education and training in simulation to practice outcomes;
- (6) Explore using multi-media and extended reality for simulation training.
검토한 리뷰에서 의견을 제시하는 능력을 향상시키기 위한 권장 사항
Recommendations in the reviewed reviews to improve speaking up
다음과 같은 다섯 가지 공통 권고안이 제시되었다:
- (1) 조직 지원 및 문화 변화;
- (2) 목소리를 높이는 연구를 개선
- (3) 원인 메커니즘에 대한 더 나은 이해 개발
- (4) 교육 및 훈련 개선;
- (5) 외부 지식을 통합하는 것.
Five common recommendations arose:
- (1) organizational support and culture change;
- (2) improving the research on speaking up;
- (3) developing a better understanding of causative mechanisms;
- (4) improving education and training;
- (5) incorporating outside knowledge.
조직 지원 및 문화 변화
Organizational support and culture change
[조직의 지원과 문화적 변화]는 심리적 안전, 시민의식, 그리고 모든 수준의 의료 전문가들에 걸친 파트너십을 통해 정당한 문화를 만들어낼 수 있다. 하향식 조직 및 문화 변화는 목소리를 낼 수 있는 [제도적 장벽과 요인]에 초점을 맞춰야 하고 이것은 대체로 바뀔 수 있다. 목소리를 높이는 것은 [경영진과 행정부를 포함]한 [모든 직원들의 지지]를 받아야 하며, 조직들은 [위계질서와 직업적 긴장]을 포함하여 기존의 불리한 직장 문화를 해결해야 한다. [지도적 위치]에 있는 사람들과 직업과 팀의 고위 구성원들은 모델링, 멘토링, 격려 및 말하기 행동을 수용함으로써 변화를 창출할 수 있다. 이러한 기술과 행동에 대한 [교육, 훈련, 격려 및 지원이 지도직에 제공]되어야 한다; 행동을 강요하는 것이 필요할지도 모른다. 또한 조직변화를 구현하고자 할 때는 구현장소에 고유한 국가문화, 사회경제적 맥락, 정치적 맥락 등을 고려할 필요가 있다.
Organizational support and cultural change can create just cultures through psychological safety, civility, and partnership across all levels of healthcare professionals. Top-down organizational and cultural change should focus on institutional barriers and enablers to speaking up that are mostly modifiable (Bickhoff et al., 2017; Fagan et al., 2016; Kim et al., 2020; Morrow et al., 2016; Noort et al., 2019; Omura et al., 2017; Pattni et al., 2019). Speaking up must be supported by all staff members, including management and administration, and organizations must address existing adverse workplace cultures, including hierarchy and professional tension. Those in leadership positions and senior members of professions and teams can create change through modeling, mentoring, encouraging, and accepting speaking-up behaviour. Education, training, encouragement, and support for these skills and behaviours should be provided to leadership positions; mandating the behaviours may be necessary. Additionally, when attempting to implement organizational change, it is necessary to consider national culture, socio-economic contexts, and political contexts endemic to the location of implementation.
목소리를 높이는 연구 개선
Improve research on speaking up
말하기가 어떻게 발생하는지 더 잘 이해하고 교육과 훈련을 개선하기 위해서는 더 엄격한 연구가 필요하다. 7가지 개선점이 확인되었다:
- (1) 교육 및 훈련 중 평가를 포함하여 보다 객관적인 측정 및 평가를 사용하여 말하기 평가 방법을 개선합니다;
- (2) 사람들이 목소리를 높이는 방법, 목소리를 높이는 결과 및 목소리를 높이는 방법에 대한 이해를 향상시키기 위해 생태학적 관찰이 필요하다;
- (3) 연구는 병원 밖, 의학과 간호 외의 직업, 다른 직장과 국가 문화, 그리고 문화적으로 다양한 팀에서 필요하다. 연구는 초국가적 및 국가적 정책의 효과를 이해하기 위해 지역적 이행을 넘어서야 한다;
- (4) 실험 방법 및 시뮬레이션을 사용하여 목소리 높이기의 원인 메커니즘, 활성화 요인 및 억제 요인을 테스트한다;
- (5) 교육에 보다 현실적인 시뮬레이션을 사용한다;
- (6) 시행 격차를 해소하고 교육 및 훈련의 장기적 효과와 개인 및 조직의 변화가 어떻게 발생하는지 이해하기 위해 다양한 맥락에서 종단적 연구를 수행한다;
- (7) 연구에 대한 이해관계자의 참여를 높이고 더 많은 자금 및 리소스를 포함하여 목소리를 높이는 데 연구의 우선순위를 지정합니다.
More rigorous research is required to better understand how speaking up occurs and to improve education and training (Bickhoff et al., 2017; Jones et al., 2021; Nacioglu, 2016; Omura et al., 2017; Rutherford et al., 2012). Seven improvements were identified:
- (1) Improve how speaking up is measured by using more objective measures and assessments, including assessment during education and training;
- (2) Ecological observation is required to improve understanding about how people speak up, outcomes of speaking up, and how speaking up is received;
- (3) Research is needed in contexts outside of hospitals, with professions outside of medicine and nursing, in different workplace and national cultures, and with culturally diverse teams. Research should move beyond local implementation to understand the effects of transnational and national policies;
- (4) Using experimental methods and simulation, to test causative mechanisms, enablers, and inhibitors of speaking up;
- (5) Use more situationally realistic simulation for training;
- (6) Conduct longitudinal research in multiple contexts to bridge the implementation gap and understand the long-term effects of education and training and how change occurs in individuals and organizations;
- (7) Increase stakeholder involvement in research and prioritize research on speaking up, including more funding and resources.
원인 메커니즘에 대한 더 나은 이해 개발
Developing a better understanding of causative mechanisms
[원인 메커니즘에 대한 더 나은 이해]는 연구를 개선하는 것과 동시에 이루어진다. 특정 선행사례들은 업무량, 말하기 수용성, 말하기에 대한 인식된 가치, 환자에게 피해를 주지 않으려는 욕구, 협박, 괴롭힘, 괴롭힘과 같은 부정적 결과의 영향을 통해 말하기를 억제하는 것을 포함하여 적절한 양의 연구를 하는 것으로 확인되었다. 개인의 차이와 성격, 그리고 직장, 직업, 문화적 맥락의 영향을 포함하지 않고 사람들이 목소리를 높이도록 이끄는 사회적, 심리적 과정에 대한 더 많은 지식이 필요하다. 다양한 교육 모드의 효과와 조직 변화에 대한 적용된 시도가 목소리를 높이는 데 어떻게 영향을 미치는지에 대한 더 나은 이해가 필요하다.
A better understanding of causative mechanism is concurrent with improving research (Jones et al., 2021; Kim et al., 2020; Milligan et al., 2017; Noort et al., 2019; Omura et al., 2017; Peadon et al., 2020). Certain antecedents were identified as having an adequate amount of research including workload, receptiveness to speaking up, perceived value in speaking up, the desire to avoid patient harm, and the inhibition of speaking up through the effect of negative consequences such as intimidation, bullying, and harassment. More knowledge is required about the social and psychological processes that lead people to speak up or not including individual differences and personality, and effects of workplace, professional, and cultural contexts. Better understanding of the effectiveness of different modes of training and how applied attempts at organizational change affect speaking up is necessary.
[목소리 높이기]는 일반적으로 [사회적으로 구성된 현상]으로 간주되어 왔으며, [목소리 높이기]가 왜 이뤄지지 않는지에 대한 가정, 추론, 의미의 속성이 만들어졌다. [일어나지 않은 일]을 평가하고 부재를 추리에 의해서 해석하는 것은 동일한 결과에 대해 반대되거나 상충되는 해석을 만들 수 있다. [목소리를 높이는 것]을 [본질적으로 의미 있고 사회적으로 내재된 현상]으로 보고 [경험적 접근법]을 사용하면 목소리를 높이는 것에 대한 보다 구체적인 이해로 이어질 수 있다.
Speaking up has typically been viewed as a socially constructed phenomenon, and assumptions, inferences, and attributions of meaning are made about the absence of speaking up. Assessing things that have not happened and interpreting absence inferentially can create opposing or conflicting interpretations of the same outcomes. Viewing speaking up as an inherently meaningful and socially embedded phenomenon and using an empirical approach can lead to a more concrete understanding of speaking up (Noort et al., 2019).
교육 및 훈련 개선
Improvement to education and training
모든 의료 수준에서 목소리를 높이는 것에 대한 [더 많은 교육과 훈련]이 필요하다. 학습자는 더 많은 교육과 훈련을 통해 목소리를 높일 수 있는 더 많은 지원을 원합니다. 교육과 훈련은 학부 수준에서 시작되어야 하며, 대학원 이후의 훈련과 지속적인 교육에서 계속되어야 한다. [목소리를 높이는 것]에 대한 교육과 훈련의 효과에 대한 의구심이 있으며, [개입의 맞춤형 및 이질적 특성]은 일관된 훈련 효과의 부족에 기여할 가능성이 있다. 목소리를 높이는 [도구와 기법에 대한 표준화된 훈련과 표준화된 평가 조치]는 개인의 경력 전반에 걸쳐 그리고 교육 및 훈련 자체에 대한 지속적인 개선 프로세스를 창출할 수 있다. 교육 및 훈련은 대면 및 기타 전달 방법을 사용하여 주로 [CRM과 같은 높은 효율성을 가진 방법]에 초점을 맞춰야 한다.
More and better education and training on speaking up is needed at all levels of healthcare (Fagan et al., 2016; Kim et al., 2020; Morrow et al., 2016; Noort et al., 2019; O’Donovan & McAuliffe, 2020; Okuyama et al., 2014; Omura et al., 2017; Pattni et al., 2019). Learners want more support for speaking up through more education and training. Education and training should begin at the undergraduate level and continue in post-graduate training and continuing education. Education and training on speaking up have questionable efficacy, with the bespoke and heterogenous nature of interventions likely contributing to the lack of consistent training effects. Standardized training for the tools and techniques of speaking up and standardized assessment measures can create continuous improvement processes for individuals throughout their career and for education and training itself. Education and training should focus on methods with high efficacy, primarily CRM, using face-to-face and other delivery methods.
다양한 직업의 특정 상황과 작업 환경에 맞춘 [시뮬레이션과 개입을 통한 경험적 시나리오 기반 학습]은 교육과 훈련을 개선할 수 있다. 학습자부터 고위 경영진까지 [모두가 참여하는 교육훈련] 설계 단계 중 [다층적 조직적 투입]이 필요하다. 교육 및 훈련 개선은 복잡하고 연구, 전략 계획 및 조직 변화를 통한 [하향식 노력의 얽힘]이 필요하다. 교육의 개선과 목소리를 높이기 위한 개입이 발생함에 따라 [새로운 세대]에게 더 나은 훈련이 제공될 수 있다. [목소리 높이기를 격려 및 수용하고, 행동을 모델링하고, 신입생들을 멘토링]하는 새로운 세대의 전문가들을 만들어 냄으로써 [광범위한 문화 변화]가 일어날 수 있다. [다양한 사고 방식과 실천 방식을 가진 새로운 전문가들]이 의료 시스템으로 이동하기 시작함에 따라, 기존 시스템과 실무자를 개선하기 위한 노력을 통해 발생하는 [하향식 조직 변화를 반영하는 상향식 변화가 발생]할 것이다.
Experiential scenario-based learning through simulation and interventions tailored to different professions' specific contexts and work environments may improve education and training. Multilevel organizational input during the design phase of education and training that includes everyone from learners to senior management is needed. Improving education and training is complex and requires the intertwining of top-down efforts through research, strategic planning, and organizational change. As improvements to education and interventions for speaking up occur better training can be provided to new generations. By creating a new generation of professionals who encourage and accept speaking up, model the behaviour, and mentor new students widespread culture change can occur. As new professionals with different ways of thinking and practicing begin moving into the healthcare system bottom-up change will occur to mirror the top-down organizational changes occurring through efforts to improve existing systems and practitioners.
외부 지식 통합
Incorporating outside knowledge
[의료 외 분야, 특히 의학 외 분야의 지식]은 교육과 훈련을 개선하고 말하기 이해에 대한 연구를 가속화함으로써 말하기 문제를 해결하는 데 도움이 될 수 있다. 가장 가치 있는 것으로 확인된 두 가지 주요 지식 분야는 [조직 행동 연구]를 포함하여 [심리학]과 [비즈니스]이다. [복잡성]과 [시스템 이론]도 도움이 될 수 있다. 의료 외의 관련 연구는 일반적으로 통합되지 않고 활용되지 않는다.
Knowledge from areas outside of healthcare, particularly outside of medicine, can help address the problem of speaking by improving education and training and accelerating research on understanding speaking up (Jones et al., 2021; Nacioglu, 2016; Noort et al., 2019; Peadon et al., 2020). The two main knowledge areas identified as being most valuable are psychology and business, including organizational behavioural research. Complexity and systems theories could also prove helpful. The large amounts of relevant research outside of healthcare are generally not incorporated and utilized.
목소리를 높이는 것에 대한 기존 지식의 종합
Synthesis of the existing knowledge on speaking up
[목소리를 높이는 것]은 주로 [위계 구조, 영향에 대한 두려움, 조직 지원의 부족]을 포함하는 [깊이 뿌리박힌 장벽] 때문에 효과적이지 못한 것으로 인식된다. [리더십과 선배 동료들의 지원, 환자에 대한 관심, 개인의 특성]이 목소리를 높이는 것을 지원한다. 목소리를 높이는 원인 메커니즘, 촉진자 및 억제자의 영향은 복잡한 상호작용에 존재한다. [원인 메커니즘]의 진정한 효과는 잘 이해되지 않으며, 그 효과를 명확하게 말할 수 없다. [목소리 높이기]를 더 잘 이해하기 위해서는 더 나은 평가, 실험, 종적 연구, 생태 관찰을 포함한 개선된 연구 방법이 필요하다. [상향식 조직 변화와 상향식 교육 및 훈련]은 원활한 목소리 내기에 필수적이다. 현재, 교육과 훈련은 충분히 자주 제공되지 않으며 일관적이거나 적절하게 효과적이지 않다; 개선이 필수적이다. 시뮬레이션은 교육, 훈련 및 연구에서 중요한 역할을 할 수 있지만 또한 개선이 필요하다. 현재 목소리를 높이는 것과 관련된 지식과 연구가 대두되고 있으며, 단점을 해결하고 질문을 명확히 하고 개선할 수 있는 방법을 찾을 수 있는 기회가 많다.
Speaking up is perceived to be ineffective due to deeply ingrained barriers that primarily include hierarchy, fear of repercussions, and a lack of organizational support. Support from leadership and senior colleagues, concern for the patient, and individual characteristics support speaking up. The influence of causative mechanisms, facilitators and inhibitors of speaking up exist in complex interactions. Causative mechanisms' true effects are not well understood, and effects cannot be stated definitively. Improved research methods including better assessment, experiment, longitudinal study, and ecological observation are needed to better understand speaking up. Top-down organizational change and bottom-up education and training are essential to facilitate speaking up. Currently, education and training are not delivered frequently enough and are not consistently or adequately effective; improvement is essential. Simulation can have an important role in education, training, and research, but also requires improvement. Currently, knowledge and research related to speaking up is emergent, with many opportunities to address shortcomings, clarify questions, and identify avenues for improvement.
논의
Discussion
의료 분야에서 목소리를 높이는 것에 대한 지식의 현재 상태에 대한 통합된 이해를 개발하기 위해 14개의 리뷰를 합성했다. 목소리를 높이는 것은 전 세계적으로 관련된 의료 문제입니다. 국가와 의료 시스템 전반에 걸쳐 목소리를 높이는 것이 문제라는 공통된 이해가 있지만, 문제를 효과적으로 해결하는 방법에 대한 지식은 제한적이다.
Fourteen reviews were synthesized to develop a unified understanding of the current state of knowledge on speaking up in healthcare. Improving speaking up is a globally relevant healthcare issue. Across countries and healthcare systems there is a shared understanding that difficulty in speaking up is a problem, however, knowledge about how to effectively address the problem is limited.
최신 검토를 기반으로 한 권장 사항
Recommendations based on the state-of-the-art review
언어의 일관된 사용
Consistent use of language
[목소리 높이기]를 조사하기 위해서는 일관된 언어가 필요하다. Okuyama 외 연구진(2014)은 모든 검토에 반영된 간결하고 구체적인 정의를 제공하며 적용 가능성을 확대하기 위해 "병원 환경"을 제거하는 경우 합의된 정의를 위해 충분히 일반적이다:
- "말하기"는 의료 전문가들이 의료 팀 내 다른 사람들의 [위험하거나 부족한 행동을 인식하거나 인지]할 때, 환자의 안전과 의료 품질의 이점에 대한 우려를 제기하는 것으로 정의된다
Consistent language is necessary to investigate speaking up. Okuyama et al (2014) provide a concise, concrete definition, reflected in all the reviews and sufficiently general for a consensus definition if "hospital environment" is removed to broaden applicability:
- "Speaking up' is defined as the raising of concerns by healthcare professionals for the benefit of patient safety and care quality upon recognizing or becoming aware of the risky or deficient actions of others within healthcare teams."
'스피킹 업'은 '안전 보이스'보다 장점이 있는데, 이는 [안전 보이스]가 수동적이고 정의적으로 '분해되고 초기'이기 때문이다. 모리슨의 프레임워크 내에서 [안전 목소리]는 미래의 이해를 지원할 수 있지만, 지식은 창발적이고, 더 간단한 개념화가 권장된다.
'Speaking up' is advantageous over 'safety voice' as speaking up is actionable and precise while safety voice is passive and definitionally "disintegrated and nascent" (Noort et al., 2019). Safety voice within Morrison's framework may support future understandings; however, knowledge is emergent, and a simpler conceptualization is recommended.
명확하고 객관적인 언어는 목소리를 높이고 토론하고 연구하는 데 사용되어야 한다. "엘리트의 무례함"과 "불건전한 복종" 등의 용어는 모호하고 비난적이다. [Value-laden terms]를 통해 [책임, 죄책감 및 보복의 필요성]을 명시적으로 할당하는 것은 [개방적 의사소통과 책임 없는 문화의 기본적인 환자 안전 원칙을 훼손]한다. 최적의 환자 치료를 제공하기 위해 목소리를 높이도록 장려하고 지원하는 대학 팀과 조직을 만드는 것은 개인이나 그룹을 권력 투쟁과 자연스러운 갈등 상태에 있다고 보는 데서 오는 것이 아니다.
Clear, objective language should be used for discussing and researching speaking up. Terms such as "incivility of elites” and "unwholesome submissiveness” etc., are ambiguous and accusatory. Explicitly assigning blame, guilt, and the need for reprisal through value-laden terms undermines fundamental patient safety principles of open communication and blame-free cultures (Helmreich et al., 1999; Kohn et al., 1999). Creating collegial teams and organizations that encourage and support speaking up to provide optimal patient care does not come from viewing individuals or groups as being in a power struggle and natural state of conflict.
연구 방향
Research directions
말하기를 이해하기 위한 [기본 질문]을 설정할 수 있습니다. 말하기에서 가장 큰 차이를 설명하는 변수와 공분산은 무엇입니까? 여기서 변수는 발화의 단일 행동 결과를 억제하거나 가능하게 하는 원인 메커니즘 또는 선행 요소로 정의될 수 있다. 단순화된 접근 방식은 목소리를 높이기 위한 변수의 복잡한 상호 작용에 대한 인과 관계 조사를 지원한다. 1차 활성화 또는 억제 변수에 대한 지식이 증가함에 따라, 데이터 수집은 구조 방정식 모델링(SEM)을 사용하여 경험에 기반한 말하기 모델을 개발하기 위해 더 효율적으로 초점을 맞출 수 있다. SEM을 활용한 초기 시도는 부분적으로 engagement에 의해 매개된 "음성"을 촉진하는 지원 및 제어의 이중 요인 모델을 확인했다. 단순화된 개념화와 경험적으로 파생된 모델은 연구, 행동 관찰 및 평가를 지원할 것이다.
A foundational question for understanding speaking up can be set: which variables account for the most variance in speaking up, and what are their covariance? Here variables can be defined as the causative mechanisms or antecedents that inhibit or enable the single behavioral outcome of speaking up. A simplified approach supports causal investigation of the complex interactions of the variables for speaking up. As knowledge about the primary enabling or inhibitory variables increases, data collection can be more efficiently focused to develop an empirically based model of speaking up using Structural Equation Modelling (SEM) (Kenny, 2019). An early attempt utilizing SEM identified a bifactorial model of support and control promoting “voice” that was partially mediated by engagement (Voogt et al., 2019). Simplified conceptualization and an empirically derived model would support research, behavioural observation, and assessment.
[심리학의 지식]을 연구와 교육, 특히 사회심리학의 준법, 권위에 대한 복종, 순응에 대한 방대한 연구와 함께 통합하면 분야를 가속화할 수 있다. 심리학은 치료의 대인 관계를 포함한 의료 제공의 많은 영역과 교차하는 과학이다. 맥락은 중요하지만, 인간 행동과 인지의 원칙은 일반적으로 보편적이며, 이미 알려진 것을 재발견할 필요는 없다.
Incorporating knowledge from psychology in research and education, specifically social psychology with its vast research on compliance, obedience to authority, and conformity (Cialdini & Griskevicius, 2010; Cialdini & Trost, 1998) can accelerate the field. Psychology is a science that intersects with many areas of healthcare delivery, including the interpersonal aspects of care. Context is important; however, the principles of human behaviour and cognition are generally universal (Ariely, 2008; Olsson-Collentine et al., 2020), and it is not necessary to rediscover what is already known (Avorn, 2018; Croskerry et al., 2017).
연구에서 도출된 추론을 개선하기 위해서는 수행되는 연구의 양과 질을 개선하는 것이 필요하다. 두 측면 모두에서 지속적인 개선은 말하기를 촉진하는 교육과 방법을 만들고 신뢰성과 타당성이 좋은 객관적 관찰 평가에 의해 안내되는 효과적인 표준화된 개입을 개발하는 데 도움이 될 수 있다.
Improvements to the quantity as well as quality of research being conducted is necessary to improve the inferences drawn from the research (Vazire et al., 2022). Continuous improvement in both aspects can help create education and methods to promote speaking up and develop effective standardized interventions with long-lasting effects guided by objective observational assessments with good reliability and validity.
시뮬레이션 향상
Enhancement of simulation
연구와 교육을 위한 시뮬레이션에 대한 인식 전환이 필요하다. 시뮬레이션의 한계는 모달리티 자체에 내포되어 있습니다. 제한으로 간주되기보다는, 시뮬레이션을 목소리를 높이기 위한 훈련과 원인 메커니즘을 실험적으로 조사할 수 있는 풍부한 가능성을 제공하는 [생태학적/외부적 타당성이 높은 시험장]으로 보아야 한다. 임상 연구 및 관찰 시뮬레이션과 함께 이론 개발, 실험, 교육 및 평가를 위한 주요 이점이다. 예를 들어, [목소리 높이기] 예측 모델은 임상 및 조직 수준에서 조사로 이동하기 전에 시뮬레이션에서 평가할 수 있다. 임상 환경으로 발전하는 과정에서 시뮬레이션은 목소리를 높이는 기술을 연습하는 매개체가 될 수 있다. 구현 과학의 통합은 시뮬레이션에서 임상 공간에 이르는 학습을 전파하고 임상의, 교육자 및 행정부의 새로운 지식과 관행을 활용하는 데 도움이 될 수 있다.
A shift in the perception of simulation for research and education is necessary. Simulation’s limitations are implied in the modality itself. Rather than being seen as a limitation simulation should be viewed as a testing ground with high ecological/external validity that provides abundant possibilities to experimentally examine training and causative mechanisms for speaking up (Friedman et al., 2015). In conjunction with clinical research and observation simulation is a major boon for theory development, experimentation, education, and assessment. For example, predictive models of speaking up can be evaluated in simulation before moving to investigation at the clinical and organizational level. In the progression to the clinical environment, simulation can be an intermediary to practice the skill of speaking up. The incorporation of implementation science can help to disseminate the learnings from simulation to the clinical space and uptake of new knowledge and practices by clinicians, educators, and administration.
현재 검토의 한계
Limitations of the present review
- (1) 관련 문헌이 누락되었을 가능성이 높다. 최근의 특정 기사와 관련 기사들은 어떤 리뷰에도 포함되지 않았다.
- (2) 현재 검토는 사용된 검토의 검색, 분석 및 보고에 따라 결정된다. 검토 방법론적 품질의 평가는 현재 방법론적 검토가 반드시 관련이 있는 것은 아니기 때문에 수행되지 않았다. 검색에서 메타 분석이 확인되지 않았으며, 이는 해당 분야가 개발 단계에 있음을 나타낸다. 많은 변수와 여러 검토 유형에 걸쳐 다양한 효과 크기가 분산되어 있기 때문에 현재 체계적인 평가가 불가능하다.
- (3) 본 검토는 환자 치료의 맥락에서 목소리를 높이는 데 초점을 맞췄다. 개인의 존엄성을 지지하기 위해 목소리를 높이는 것이 필요한 다른 교육적이고 전문적인 맥락이 존재하며 고려되어야 한다.
- (1) Relevant literature was likely missed. Certain recent and relevant articles were not included in any of the reviews (Calhoun et al., 2014; Daly Guris et al., 2019; Fisher & Kiernan, 2019; Kaba et al., 2016; Kuo et al., 2020; Oner et al., 2018; Shanks et al., 2020).
- (2) The present review is contingent on the search, analysis, and reporting of the reviews used. An assessment of the reviews methodological quality was not conducted as, at present, a methodological review is not necessarily relevant. No meta-analyses were identified in the search, indicating the field is in a developmental stage. With numerous effect sizes spread over many variables and multiple review types at this time systematic evaluation is not possible (Noort et al., 2019).
- (3) The present review focused on speaking up in the context of patient care. Other educational and professional contexts exist, and should be considered, where speaking up is necessary to support individual dignity (Gianakos et al., 2022).
결론
Conclusion
환자 위해 문제가 지속되고 환자 안전을 발전시키고 지속적으로 개선할 필요가 있는 상황에서, 그 임무를 추진하기 위한 공동의 노력이 필요하다. 행동의 명백한 단순성에도 불구하고, 목소리를 높이는 것은 잘 이해되지 않고, 연구는 초기 단계에 있으며, 교육과 훈련에 대한 개선이 필요하며, 외부의 견해가 필요하다. 초기 분야의 리뷰는 중복성을 줄이고 현재 지식의 포괄적인 통합을 제공하기 위해 단일의 포괄적인 문서를 작성할 필요성을 뒷받침한다. 현재의 합성은 통일된 이해를 촉진하고, 기존의 지식을 명확하게 하며, 향후 연구의 공통된 출발점으로 기능하고자 한다.
With the persistent issue of patient harm and the need to advance and continuously improve patient safety, a concerted effort is needed to carry the mission forward (Cohen & Patel, 2020). Despite the apparent simplicity of the behaviour, speaking up is not well understood, research is in early stages, improvements to education and training are required, and outside views are needed. The plethora of reviews in an incipient field supports the need to create a single comprehensive document to reduce redundancy and provide a comprehensive synthesis of the current knowledge. The current synthesis intends to foster a unified understanding, clarify existing knowledge, and function as a common starting point for future research.
A state-of-the-art review of speaking up in healthcare
PMID: 35666354
Abstract
Throughout healthcare, including education, the need for voicing of concern by speaking up is a globally recognized issue that has come to the fore in the last ten years. There has been a rapid growth in the number of review articles on the topic. To prevent diffusion of knowledge and support future research it is necessary to gather the existing knowledge in a single place. The purpose of the present article is to bring together the existing reviews on speaking up to create a source of unified knowledge representing the current "State of the Art" to advance future research and practice. A State-of-the-Art review was conducted to synthesize the existing knowledge on speaking up. Six databases were searched. Fourteen review articles spanning 2012 to 2021 were identified. Five main research questions have been investigated in the literature and five common recommendations for improvement are made, the knowledge across all reviews related to the research questions and recommendations was synthesized. Additionally, simulation-based research was frequently identified as an important though limited method. Further issues in the literature are identified and recommendations for improvement are made. A synthesis was successfully developed: knowledge about speaking up and research related to speaking up is in an emergent state with more shortcomings, questions, and avenues for improvement than certitude. The whys and how of speaking up remain open questions.
Keywords: Challenging authority; Healthcare professional; Healthcare student; Interprofessional; Patient safety; Safety voice; Speaking up.
© 2022. The Author(s), under exclusive licence to Springer Nature B.V.
'Articles (Medical Education) > 전문직업성(Professionalism)' 카테고리의 다른 글
| 의과대학생의 전문직정체성 형성: 위계적, 집단적 문화에서의 혼합연구(BMC Med Educ, 2022) (0) | 2023.01.28 |
|---|---|
| 어떻게 전문직 정체성을 기를 것인가?: 의학교육분야의 철학적 정원 가꾸기(Persepctives on Medical Education, 2023) (0) | 2023.01.28 |
| "요즘 애들": 밀레니얼 학습자에 대한 우리의 대화 다시 생각하기 (Med Educ, 2019) (0) | 2023.01.13 |
| 세대적 상황성: 보건의료전문직에서 세대적 고정관념에 도전하기 (Med Teach, 2022) (0) | 2023.01.10 |
| 뒤를 돌아보고 앞으로 나아가기: 의과대학 1학년의 포트폴리오 글쓰기에 대한 메타-성찰(Acad Med, 2018) (0) | 2022.12.15 |