실패하는 것이 인간이다: 의학교육의 재교육을 재교육(Perspect Med Educ, 2017)
To fail is human: remediating remediation in medical education
Adina Kalet1 · Calvin L. Chou2 · Rachel H. Ellaway3

도입
Introduction
실패한 학습자에게 교정조치는 의료 교육의 필수적인 부분이지만 교정조치자, 교정조치자, 일반적으로 보건 및 교육 시스템에 부담을 줄 수 있다[1]. 의료 교육 문헌[2]에서 교정조치에 대한 관심이 증가하고 있지만, 교정조치의 메커니즘이나 적절한 절차와 방어의 문제에 초점을 맞추는 경향이 있었다.
Remediating failing learners is an essential part of medical education but one that can be taxing to the remediated, their remediators, and to health and educational systems in general [1]. Although there has been a growing focus on remediation in the medical education literature [2], it has tended to be on the mechanics of remediation or on matters of due process and defensibility.
첫 번째 논문에서 우리는 교정조치가 의료 교육에서 연습의 영역으로서 각각 자신의 규칙과 기대를 가지고 다른 연습 영역과 나란히 놓인 특별한 규칙과 기대를 가지고 모델링했다[3].
in our first paper we modelled remediation as a zone of practice in medical education with particular rules and expectations that sit alongside other zones of practice, each with its own rules and expectations [3].
의학교육의 교정조치는 '의사가 되기 위한 여정을 시작하였으나 진로를 벗어난 수련생에 대한 교정을 촉진하는 행위'[4]이다. 교정조치는 어려운 학습자를 위한 것뿐만 아니라 의사 인력의 질을 보장하기 위한 방법으로서 의료 교육의 필수적인 구성요소이다.
Remediation in medical education is ‘the act of facilitating a correction for trainees who started out on the journey toward becoming a physician but have moved off course’ [4]. Remediation is a necessary component of medical education, not only for the sake of struggling learners, but also as a way of assuring the quality of the physician workforce.
우리는 적자deficit가 복합화되고 고부담일 때보다는, 교육 프로그램에서 deficit를 조기에 감지하고 수정해야 한다는 것을 알고 있습니다 [9]. 우리는 또한 교정조치가 대개 효과가 있다는 것을 안다. 교육의 종료 시점이 되면, remediated 학습자는 non-remediated 동료와 구별되지 않는(차이가 없는) 경우가 많다[10, 11].
We know that we need to detect and correct deficits earlier in training programs, rather than later when deficits have compounded and the stakes are higher [9]. We also know that remediation usually works: learners who have been remediated are often indistinguishable from their non-remediated peers by the end of their training [10, 11].
많은 프로그램들은 종종 법적 보복의 두려움이나 교수진이 그들이 멘토링하고 있는 학습자들을 판단하는 것을 꺼리는 것에 대한 두려움 때문에 학습자들을 보호관찰하거나 그들을 해고하는 데 어려움을 겪는다. 교수진이 어려움을 겪고 있는 학습자를 보고하려고 할 때에도, 기관의 장벽과 공통된 정의와 행동의 부족은 실패한 학습자를 식별하고 해고하는 것을 어렵게 만들 수 있습니다 [15].
many programs have difficulty placing learners on probation or dismissing them, often because of the fear of legal reprisal or faculty reluctance to judge the learners that they have been mentoring. Even when faculty are willing to report struggling learners, institutional barriers and a lack of common definitions and actions can make it difficult to identify and dismiss failing learners [15].
교정조치는 일반적으로 교정조치자, 교정조치자 또는 교정조치자, 또는 양쪽 모두의 관점에서 검토되어 왔다. 그러나 교정조치는 본질적으로 위치하며 항상 맥락에 있으며, 그러한 맥락은 좋고 나쁨을 위해 교정조치의 관행을 형성하고 지시할 수 있다.
Remediation has typically been considered fromthe perspective of the individuals involved, either the remediator or the remediated, or both. However, remediation is intrinsically situated, it is always in context, and that context can shape and direct remediation practices both for good and ill.
다양한 훈련 컨텍스트는 성공하거나 실패하거나 교정할 수 있는 다양한 수준의 기회를 제공하며, 이러한 상황적 요인은 교정조치의 설계와 수행에도 정보를 제공해야 한다[17].
Different training contexts afford different levels and forms of opportunity to succeed or fail as well as to remediate, and these contextual factors should also inform the design and conduct of remediation [17].
비그넷 1: 샐리의 이야기
Vignette 1: Sally’s story
교정조치는 상황에 따라 형성될 뿐만 아니라, 상황도 교정조치에 의해 형성된다. 교정조치와 관련된 추가적인 노력과 잠재적 문제, 그리고 특정 학습자 결손을 식별하고 이를 효과적으로 해결하기 위한 어려움은 일반적으로 교정조치가 실제적이고 감정적인 부담으로 간주된다. 교정조치는 특히 다중 및/또는 심각한 문제, 심각한 학습자 부채 또는 기타 어려움을 겪는 학습자의 경우 비용이 많이 들고 시간이 많이 소요되는 경향이 있다. 이는 다시 자원의 가용성과 교육자의 헌신을 왜곡시킬 수 있다. 그것은 또한 상충되는 역할과 책임의 숨겨진 커리큘럼을 세울 수 있다.
Not only is remediation shaped by context, context is also shaped by remediation. The additional effort and potential distress associated with remediation, and the challenges in identifying specific learner deficits and effectively addressing them, typically position remediation as a burden, both practical and emotional. Remediation tends to be expensive and time-consuming, particularly for learners with multiple and/or severe challenges, significant learner debt, or other hardships. This can in turn skew the availability of resources and the commitment of educators. It can also establish a hidden curriculum of conflicted roles and responsibilities.
교정조치에 대한 시스템 이론에 대해
Towards a systems theory of remediation
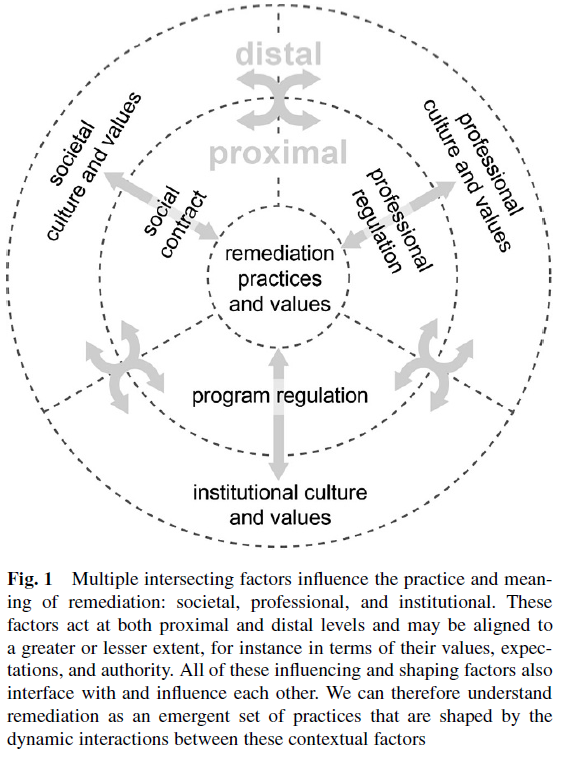
우리는 사회, 전문가, 기관의 영향력과 책임 측면에서 정의된 교정조치에 대한 시스템 수준 분석을 제안한다(그림 1).
We propose a system-level analysis of remediation, definedin terms of societal, professional, and institutional influ-ences and accountabilities (Fig. 1)
사회
Society
의료 교육과의 사회적 계약은 높은 품질과 안전 관리를 제공할 수 있고 이 의무를 무엇보다도 우선시하는 신뢰할 수 있는 의사의 일관되고 효과적인 양성을 요구한다. 그 대가로, 의료 교육자들은 자신의 역량 표준과 능력을 평가하는 표준을 정의하고 유지할 수 있는 상당한 자율성을 가진다 [18].
The social contract with medical education requires a consistent and effective production of trustworthy physicians who can deliver high quality and safe care, and who place this obligation above all others. In return, medical educators have significant autonomy to define and maintain their own standards of competence and the standards by which competence is assessed [18].
일부 가치(예: 기본 전문 표준)는 국제 통화를 가지고 있지만, 다른 가치(보상, 실행 범위, 위험과 모호성의 수용성, 의료 서비스에 대한 환자의 접근성, 개별 책임과 자율성 등)는 주, 주, 주, 주, 주, 주(州) 및 주 간에(심지어는 그 안에서도) 크게 다를 수 있다.[19]. 이러한 차이는 무엇이 허용 가능하고 허용할 수 없는 실무 표준을 구성하는지, 그리고 이러한 프로세스가 어떻게 수행되고 규제되는지 측면에서 교정조치 프로그램의 설계에 정보를 제공할 수 있다. 따라서 우리는 교정조치가 점점 더 세계화되는 세계에서도 표준화되고 규범화되어야 한다고 가정해서는 안 된다. 실제로, 사회적 맥락은 교정조치의 가치와 관행에 강하게 영향을 미칠 것이다.
Although some values (such as basic professional standards) have international currency, other values (such as rewards, scope of practice, acceptability of risk and ambiguity, access of patients to healthcare services, and individual accountability and autonomy) can vary significantly between states, provinces, and countries (and sometimes even within them) [19]. These differences can inform the design of remediation programs in terms of what constitutes acceptable and unacceptable standards of practice, and how these processes are conducted and regulated. We should not therefore assume that remediation is (or should be) a standardized and normative undertaking, even in an increasingly globalized world. Indeed, social contexts will strongly influence the values and practices of remediation.
점점 더 많은 의과대학들이 사회적 의무를 이행하고 의료계 종사자를 소송으로부터 보호하는 방법으로서 점점 더 높은 수준의 책무를 수용하고 있다. [의료 전문가]가 의료 오류에 대한 사회적 압력에 대응하여 [품질과 안전에 대한 주의]를 높인 것과 같은 방식으로[20, 21], 우리는 [의학 교육]에서 remediation을 유사하게 개념화함으로써 직업에 대한 신뢰 증가를 정당화할 것이라고 주장한다.
A growing number of medical schools have embraced increasing levels of accountability, both as a way to meet their social obligations and to protect the medical profession from litigation. In the same way that the medical profession has increased its attention to quality and safety in response to societal pressures about medical errors [20, 21], we argue that a similar conceptualization of remediation in medical education will justify an increase in trust in the profession.
또한, 교육 프로그램은 낙제 학습자에 의한 소송이 있어도 신중한 문서화만 되어있으면 성공하는 경우는 거의 없다는 것을 기억해야 하며, 이는 실패에 대해서 각 기관이 방어적인 입장을 갖을 필요가 없음obviate을 보여준다.
In addition, training programs must remember that litigation by failing learners rarely succeeds in the context of careful documentation [1], which should substantially obviate a defensive institutional stance towards failure.
직업
Profession
의료 직업의 규제는 전문직 학회, 비정부 조직, 입법자들 사이의 복잡한 상호 작용을 포함한다. 그러나 의료업계가 자율적으로 규제할 수 있는 범위도 관할권에 따라 크게 다르다 [22, 23]. 실제로, 서로 다른 조직과 기관이 서로 다른 의제를 보유하고 있지만, 학습자 성격의 중요한 결함을 확인할 때를 제외하고는 교정조치는 대부분 규제되지 않는다unregulated.
The regulation of the medical profession involves a complex interplay among professional societies, non-government organizations, and legislators. However, the extent to which the medical profession can self-regulate also varies greatly by jurisdiction [22, 23]. Indeed, although different organizations and agencies harbour different agendas, remediation is largely unregulated, except when it identifies critical flaws in learners’ characters.
예를 들어, 미국에서 교정조치는 학부 및 대학원 의학 교육의 인증 표준에서 약간 언급된다[24]. 이와는 대조적으로, 캐나다의 온타리오 대학(CPSO)은 공공 의료 등록부에 포함시키기 위해 학부 및 대학원 교정조치에 대한 선언을 요구한다[25]. 더욱이 교정조치의 일반적인 관행이 제안된 바 있고, 일부 [26, 27]에 의해 채택되었지만, 의학 교육 전반에 교정조치에 대한 규범적인 표준과 실천요강이 있다고 가정하기 보다는, 지역적으로 적절하고 대응적인 실천locally relevant and responsive practice과 균형을 이루어야 한다.
For instance, in the United States, remediation is mentioned sparingly in the accreditation standards for undergraduate and postgraduate medical education [24]. By contrast, in Canada, the College of Physicians and Surgeons of Ontario (CPSO) requires declaration of undergraduate and postgraduate remediation episodes for inclusion in their public physician register [25]. Moreover, although common practices in remediation have been proposed [5] and embraced by some [26, 27], assumptions that there are normative standards and practices for remediation across medical education, as a whole must balance with locally relevant and responsive practices.
제도
Institution
교정조치에 관한 사회적 및 전문적 지침이 제한적임을 고려할 때, 교정조치가 통제, 자원 및 구현되는 방법을 정의하는 것은 개별 의료 교육 프로그램에 해당된다. 또한 교정 조치와 관련된 많은 문제를 관리해야 합니다. 예를 들어 커리큘럼, 평가 및 교정 작업이 여러 가지 방법으로 잘못 조정되거나 잘못 조정될 수 있습니다. 예를 들어, 커리큘럼 유연성이 부족하면 (모듈 간 휴식 시간, 임상실습 사이 시간 및 평가 주) 상당한 중단disruption 없이는 remediation을 하기 어렵다. 다소 지독스러운unforgiving 이 구조는 학습 통합을 위한 공간이 거의 없이 전진하는 것으로, 어려움을 겪고 있는 학습자들에게 특히 어렵고 지속적인 실패 가능성을 증가시킬 수 있다.
Given the limited societal and professional guidance around remediation, it falls to individual medical education programs to define the ways in which remediation is governed, resourced, and implemented. They also have to manage the many challenges associated with remediation. For instance, curriculum, assessment, and remediation can be or become misaligned in many ways. Lack of curricular flexibility, for example, may dictate that remediation cannot occur without significant disruption (in the absence of breaks between modules, intersessions between clerkships, and assessment weeks). This somewhat unforgiving structure, inexorably marching forward with little space for consolidation of learning, is particularly difficult for struggling learners and can increase the likelihood of ongoing failure.
구조적으로 다양한 평가 프로그램(예: 객관식 시험, 서면 에세이, 시뮬레이션, 객관적인 구조화된 임상 평가), 형성적 방향, 타이밍 또는 맥락에 따라 그리고 훈련 받은 개인이 전체적으로 판단하는 프로그램은 약한 학습자에게 보다 효과적인 비계를 제공할 수 있다[5, 9, 29]. 게다가 평가가 학습을 주도한다고 종종 말하지만, 그 반대도 사실인 것처럼 보인다. 예를 들어, 최소 또는 암묵적으로 평가된 커리큘럼 요소(전문직업성 또는 시스템 기반 관행 등)는, 여기에 대해 어려움을 겪고 있는 학습자에게 적절한 조기 감지early detection를 제공하지 않으며, 학습자가 해당 역량이 요구되는 컨텍스트로 이동한 뒤에야 교정조치 '위기crisis'로 이어질 수 있다.
A program of assessment that varies in structure (e. g., multiple choice tests, written essays, simulations, objective structured clinical evaluations), formative orientation, timing, or context, and judged holistically by trained individuals, can provide more effective scaffolding for weaker learners [5, 9, 29]. Furthermore, although it is often said that assessment drives learning, the reverse also appears true. For instance, minimally or tacitly assessed curricular elements (such as professionalism or systems-based practice) do not provide adequate early detection for struggling learners and could lead to a remediation ‘crisis’ once the learner moves into a context where that competence is required.
교정조치 관행은 또한 기관 문화를 반영한다[31, 32].
Remediation practice also reflects institutional culture [31, 32].
- 실패의 문화적 차원은 개인이 실패하는지, 언제, 그리고 왜 실패하는지에 관한 가정과 믿음에서 생긴다.
- 여기에는 실패와 정상적인 성능 분산 사이의 임계값, 차선의 성능 차원이 어느 정도 중요한지, 실패가 교정될 수 있는지 여부, 실패의 사고를 영구적으로 기록해야 하는지 여부, 그리고 어려움을 겪고 있는 학습자에 대한 정보를 '앞으로 공급feed forward' 또는 엄격히 비밀로 유지해야 하는지 여부가 포함된다.
- 학교에서 어떤 교정조치도 허용할 수 있도록 하는 것은, 실패가 회복될 수 있다는 집단적 믿음과 합격과 해고 사이에 영역이 있다는 것을 재확인하는 것이다[33]. 막반 데르 보센 외. 의과대학 교수진이 시스템 수준 개입으로 전문성 교정조치에 대한 낙관론을 강화함으로써 고군분투하는 학생들을 낙제시키려는 의지를 증가시켰다[34].
- A cultural dimension of failure arises from assumptions and beliefs regarding whether, when, and why individuals fail.
- This includes the thresholds between failure and normal variance in performance, what dimensions of suboptimal performance are more or less important, whether failure can and should be remediated, whether incidents of failure should be permanently recorded, and whether information about a struggling learner should be ‘fed forward’ or kept strictly confidential [33].
- For a school to allow for any remediation at all reifies a collective belief that failure can be recovered from, and that there is a zone between passing and dismissal [33]. Mak-van der Vossen et al. have increased the willingness of medical school faculty to fail struggling students by enhancing their optimism about professionalism remediation with a systemslevel intervention [34].
- 책임의 문화적 차원은 학교의 임무, 기능, 목표, 책임 및 교정조치가 이러한 영역과 일치하는 방법에 관한 가정과 믿음에 의해 형성된다. 예를 들어,
- 사회, 직업, 교수진, 환자 및 기타 이해 관계자에 대한 프로그램의 책임과 학습자에 대한 책임(교정 실무에 반영됨)이 얼마나 균형을 이루는가?
- 이러한 우선 순위는 교정조치의 설계 및 실행에 어떤 영향을 미칩니까?
- '나쁜 사과'를 배제하는 것이 더 중요한가, 아니면 프로그램을 복구하고 완성하기 위해 발을 헛디딘 사람들을 돕는 것이 더 중요한가?
- 교정조치 시 학습자의 책임은 무엇입니까?
- 학교는 소수의 상환이나 다수의 성공에 어느 정도까지 그들의 자원을 목표로 해야 하는가?
- A cultural dimension of responsibility is shaped by assumptions and beliefs regarding the mission of the school, its function, its goals, its accountabilities, and the way remediation aligns with these domains. For example,
- how much do a program’s responsibilities to society, its profession, its faculty, their patients, and other stakeholders balance with its responsibilities to their learners (as reflected in remediation practice)?
- How does this prioritization affect the design and practice of remediation?
- Is it more important to exclude ‘bad apples’ or to help those who misstep to recover and complete the program?
- What are learners’ responsibilities in remediation?
- To what extent should schools target their resources on the redemption of a few or on the successes of the many?
고찰 Discussion
우리의 첫 번째 단계는 보다 광범위한 의료 교육 시스템 내에서 교정조치의 위치를 정하고 교정조치가 다른 관행과 다른 방법 및 그러한 차이의 영향을 명확하게 정의하는 것이었다[3]. 본 논문에서, 우리는 사회적, 전문적 및 제도적 맥락에서 교정조치에 대해 고려하도록 시야를 넓혔다.
Our first step was to situate remediation within the broader systems of medical education and to clearly define the ways in which remediation differs from other practices and the implications of those differences [3]. In this paper, we have expanded our gaze to consider remediation in societal, professional and institutional contexts.
더욱이 교정조치는 종종 학습자가 의사가 될 수 있다고 판단되는 [변곡점inflection]을 표시하기 때문에, 성공과 실패 사이의 한계 공간liminal space을 구성하고, 그것은 [자신의 역할과 의무, 거기서 거래되는 것의 의미와 관련된] 모든 사람에게 복잡한 메시지를 보낸다.
Moreover, because remediation often marks the inflection point at which a learner is either judged to be capable of becoming a physician or not, it constitutes a liminal space between success and failure that sends complex messages to all concerned about their roles and obligations and the meaning of what is transacted there.
역설은 종종 교정조치의 맥락에서 발생한다. 훈련의 후반 단계에서 문제가 있다고 간주되는 특성은 부분적으로 훈련 프로세스에서 역동적으로 창발하거나, 심지어 훈련의 초기 단계에서는 강점으로 간주될 수 있기 때문에 초기에 감지되지 않을 수 있다[36].
Paradoxes often arise in the context of remediation. Characteristics considered problematic in later stages of training may be undetectable early on, in part because they can emerge dynamically from the training process or could even be considered a strength in earlier phases of their training [36].
예를 들어, 자신의 개별 성과에 대한 일편단심, 고도로 훈련된 학습자는 의대 입학 위원회에서 높은 평가를 받을 수 있지만 복잡한 전문가 간 팀워크가 필요한 레지던트 교육에서 복잡한 임상 상황을 만났을 때 극복할 수 없는 어려움을 보여준다. [입학을 개선하는 것만으로 후속 교정조치의 필요성을 줄일 수 있다]고 가정하기보다는, 오히려 교정조치로 이어지는 결함이 의료 교육 과정과 시스템에서 실제로 나타날 수 있다는 점을 인식해야 한다.
For instance, a learner with a single-minded, highly disciplined dedication to their own individual performance may rate highly with medical school admissions committees but show insurmountable difficulties when encountering complex clinical situations in residency training that require intricate interprofessional teamwork. Rather than assuming that improving admissions alone will reduce the need for subsequent remediation, we should instead acknowledge that flaws leading to remediation could actually emerge from medical education processes and systems.
Vignette 2: Vin의 이야기
Vignette 2: Vin’s story
투명하고 명확한 교정조치 정책의 결여와 프로세스의 필요한 호출에 대한 책임감이 불충분하면 성과가 저조한 동료와 그들과 상호작용하는 교수진에게 소름 끼치는 영향을 미칠 수 있다. 유능하거나 전문적이지 못한 학습자를 '아직' 참는 것은 불충분한 제도적 지원을 우려하여 동료나 교수진이 개입하려는 동기를 감소시킨다. 이 과정은 또한 사회가 그 직업을 부여하는 자율규제를 약화시킨다. 최악의 경우, (암묵적으로 또는 명시적으로) 일부 학습자가 적절한 지원 없이 고군분투하도록 놔둬버리면, 도움이 필요한 다른 학습자가 스스로 확인self-identify할 가능성이 줄어든다. 비벌칙적이고 신뢰할 수 있으며 투명한 교정 프로세스는 모든 학습자가 자신과 서로를 최고 수준의 표준으로 유지할 수 있는 문화를 지원합니다.
The lack of a transparent and articulated remediation policy, combined with insufficient accountability for necessary invocation of the process, can produce a chilling effect on the peers of those who are underperforming and the faculty who interact with them. Tolerating ‘not yet’ competent or unprofessional learners diminishes the motivation of peers or faculty to intervene for fear of insufficient institutional support. This process also undermines the self-regulation that society grants the profession. In the worst case, implicitly or explicitly allowing some learners to struggle without adequate support diminishes the chances that others who need help will self-identify. A non-punitive, reliable and transparent remediation process supports a culture where all learners can hold themselves and each other to the very highest standards.
만약 우리가 교정조치가 의학 교육의 자연스러운, 어쩌면 바람직한 요소라는 것을 받아들인다면, 우리는 [모든 개별 학습자들의 성공]을 [교육과 교수진의 효과에 대한 암묵적인 판단]과 분리해야 한다. 이를 위해, 우리는 의료 교육에서 교정조치 원칙의 조정과 시스템 수준의 명확성을 위해 노력해야 한다. 이러한 원칙은 의사가 될 개인의 현재 및 미래 역량에 대한 방어 가능하고 미묘한 판단을 촉진해야 한다.
If we accept that remediation is a natural, perhaps even desirable, component of medical education, then we must disconnect the tacit judgment about the effectiveness of the curriculum and faculty from the success of every individual learner. To that end, we need to work towards systems-level clarity and alignment of remediation principles in medical education. These principles should foster defensible and nuanced judgments about the current and future competence of individuals who will become physicians.
그럼에도 불구하고 시스템 수준 접근법이 필요하며 이를 위해 다음과 같은 여러 가지 권장사항을 제시한다.
Nevertheless, a systems-level approach is required and, to that end, we make a number of recommendations:
교정조치 원칙과 실천은 의료교육 시스템이 위치한 곳situated에 맞춰져야 한다. 현재 교정조치는 강압에 시달리며 종종 모든 참가자가 꺼리는 '외부' 활동인 경향이 있다. 이는 프로세스를 저해하는 '불량' 행동을 조장할 수 있으며, 개별 프로세스를 사회적 또는 직업적 요구로부터 더욱 분리할 수 있습니다. 예를 들어, 교정조치의 시작을 위한 명시적 요건을 명명하면 학습자를 포함한 모든 이해 관계자가 수용할 수 있는 품질 개선 프로세스를 촉진할 수 있다. '건설적 정렬'의 이 원칙[41]은 교정조치의 장벽을 높이고 개선에 초점을 맞추도록 보장한다.
Remediation principles and practices should align with the medical education systems where they are situated. Currently, remediation tends to be an ‘outside’ activity, undertaken under duress and often unwillingly by all participants. This can encourage ‘rogue’ behaviour that undermines the process and can further separate the individual process fromsocietal or professional needs. For instance, naming explicit requirements for initiation of remediation can facilitate a quality improvement process that all stakeholders, including learners, can embrace. This principle of ‘constructive alignment’ [41]lowers rather than raises barriers to remediation and ensures that the focus is on improvement.
우리는 오늘날 의학교육의 [일상적 개선]에서부터 [제적으로 끝날 수 있는 고도로 구조화된 에피소드]에 이르기까지 일련의 교정 조치를 가능하게 하고 지원해야 한다. 앞에서 주장했듯이, 교정조치 연속체는 구조, 형평성, 문서화 및 폐쇄를 포함하여 [교정조치의 여러가지 정도와 형태]에 대한 비례적 관리proportional management를 포함해야 한다[3].
We must enable and support a continuum of remediation, ranging from individual improvements in day-to-day medical education, to highly structured episodes that may end with dismissal. As we have previously argued, the remediation continuum should encompass proportional management of different degrees and forms of remediation, including structure, equity, documentation, and closure [3].
교정조치는 처벌과 오명의 문제에서 벗어나, (대부분은 아니더라도), 많은 사람들이 어느 시점에서 필요로 하고 이익을 얻을 수 있는 훈련의 형태로 재구성되어야 한다. 실패한 교정조치 프로세스가 훈련에서 해고dismissal를 필요로 하는 경우, 동정적 시스템은 이미 실행 가능한 대체 경력 경로 또는 부채 용서를 제공하는 것을 고려했을 것이다.
Remediation should be reframed from a matter of punishment and stigma to a form of training that many, if not most, will need and benefit from at some point. If failed remediation processes necessitate dismissal from training, compassionate systems would have already considered providing viable alternative career pathways or debt forgiveness.
이상적으로, 기관은 필요한 전문지식을 포함하는 [교정조치 실천공동체]를 개발해야 한다. 여기에는
- 표준 역량 곡선 이하로 떨어진 학습자를 인식하고 참조할 수 있는 모든 강사, 임상 교사 및 감독자
- 어려운 학습자를 지원하고 교정 과정을 관리하기 위해 감사 코칭 기법과 학습 계획 개발을 사용하는 교정조치 팀
- 프로그램 또는 코스 감독, 학장 등으로 대표되는 최종 결정권자는 교정조치 과정의 결과에 대한 최종 판단을 알리기 위해 다른 두 그룹과 협의한다.
Optimally, institutions should develop a community of remediation practice, which contains the needed expertise. This should include
- all tutors, clinical preceptors, and supervisors who are able to recognize and refer learners who fall below a standard competence curve;
- a team of remediators, who use appreciative coaching techniques and the development of learning plans to support struggling learners and manage the remediation process; and
- an ultimate arbiter, represented by a programor course director, dean, etc., who consults with the other two groups to inform their final judgment about the outcomes of the remediation process.
결론
Conclusion
교정조치는 그림 1에서와 같이 의료 교육 시스템에 의해 형성되고 형성되는 복잡한 교육 및 평가 시스템의 일부이다. 교정조치는 알고리즘이나 정책에 얽매인 대응이 아니라 교육 생태계 내에서 사회적으로 구성되며, 학습, 지원, 평가, 규제, 프로세스, 정체성 등의 특성에 대한 메시지를 의료교육의 특정 시스템에 전달한다. 따라서 교정조치는 학교, 프로그램 및 교수진을 다소 대립적이고 적대적인 시각으로 캐스팅할 수 있다.
Remediation is part of a complex system of teaching and assessment that both shapes and is shaped by systems of medical education, as depicted in Fig. 1. Rather than an algorithmic or policy-bound response, remediation is socially constructed within educational ecosystems, and it sends messages about the nature of learning, support, assessment, regulation, process, identity, and so on, in and of a particular system of medical education. Remediation can thereby cast schools, programs, and faculty in a more or less confrontational and adversarial light.
그러므로, 학교의 교정문화는 그것의 전반적인 문화에 대해 많은 것을 말할 수 있다; 실제로, 그것은 제도문화를 정의(또는 재정의)하는 대표적인 행동들 중 하나일 수 있다. 교정조치는 사후생각afterthought나 불편한것inconvenience이 아니라, 우리가 최선을 다하거나 최악의 상황을 보는 문제가 되어야 한다. 의료 오류와 마찬가지로 교정조치는 개인의 고장이 아니라, 의료 훈련의 복잡한 시스템의 불가피한 측면으로 추구될pursue 수 있다.
Therefore, a school’s culture of remediation can say much about its overall culture; indeed, it might be one of the signature acts that defines (or redefines) the institutional culture. Far from being an afterthought or an inconvenience, remediation should be a matter of seeing us at our best, or our worst. Like medical error, remediation could be pursued as an inevitable aspect of the complex system of medical training, not a failure of an individual.
품질개선 운동을 통해 알 수 있듯, 문제를 미리 예상하고 대비해서 얻는 것이 숨기는 것보다 훨씬 많다. 따라서 의료 교육에서 [교정조치의 실천을 교정하는 것]이 더 중요하거나 실용적이었던 적은 없다. 그러나, 모든 교정조치가 그렇듯이, 우리는 우리의 노력에 성공하거나 실패할 수 있다. 우리가 성공했는지를 알 수 있는 기준은 의료 교육 전반에서 교정조치에 완전히 align하는 능력에서 비롯된다.
As is evident from the Quality Improvement movement, there is much more to be gained from anticipating the problemand preparing for it than hiding it. Remediating remediation practice in medical education has therefore never been more important or practical. However, as with all remediation, we may succeed or may fail in our efforts. The standard by which we will know whether we have succeeded flows from our ability to fully align remediation within medical education as a whole.
3. Ellaway RH, Chou CL, Kalet AL. Situating remediation: accommodating success and failure in medical education systems. Acad Med. 2017; https://doi.org/10.1097/ACM.0000000000001855.
Perspect Med Educ
. 2017 Dec;6(6):418-424.
doi: 10.1007/s40037-017-0385-6.
To fail is human: remediating remediation in medical education
Adina Kalet 1, Calvin L Chou 2, Rachel H Ellaway 3
Affiliations collapse
Affiliations
-
1Program on Medical Education Innovation and Scholarship, New York University School of Medicine, New York, USA. Adina.Kalet@nyumc.org.
-
2Department of Clinical Medicine, Academy of Medical Educators University of California, San Francisco, USA.
-
3Office of Health and Medical Education Scholarship at the Cumming School of Medicine, University of Calgary, Calgary, Canada.
-
PMID: 29071550
-
PMCID: PMC5732108
Free PMC article
Abstract
Introduction: Remediating failing medical learners has traditionally been a craft activity responding to individual learner and remediator circumstances. Although there have been moves towards more systematic approaches to remediation (at least at the institutional level), these changes have tended to focus on due process and defensibility rather than on educational principles. As remediation practice evolves, there is a growing need for common theoretical and systems-based perspectives to guide this work.
Methods: This paper steps back from the practicalities of remediation practice to take a critical systems perspective on remediation in contemporary medical education. In doing so, the authors acknowledge the complex interactions between institutional, professional, and societal forces that are both facilitators of and barriers to effective remediation practices.
Results: The authors propose a model that situates remediation within the contexts of society as a whole, the medical profession, and medical education institutions. They also outline a number of recommendations to constructively align remediation principles and practices, support a continuum of remediation practices, destigmatize remediation, and develop institutional communities of practice in remediation.
Discussion: Medical educators must embrace a responsible and accountable systems-level approach to remediation if they are to meet their obligations to provide a safe and effective physician workforce.
Keywords: Competency based medical education; Medical education; Remediation.
'Articles (Medical Education) > 교육과정 개발&평가' 카테고리의 다른 글
| 영국 기본의학교육에서 핵심 의사소통 커리큘럼의 합의문(Patient Educ Couns. 2018) (0) | 2021.02.05 |
|---|---|
| 학부의학교육에서 의사소통 교육과정의 내용에 대한 합의문(Med Educ, 2008) (0) | 2021.01.30 |
| 의학교육에서 수직통합: 포괄적 관점(BMC Med Educ, 2020) (0) | 2020.12.20 |
| CBME의 도입: 우려와 도전을 해결하고 있는가? (Med Educ, 2015) (0) | 2020.12.20 |
| 교육의 퀄리티와 카파시티 증가: 21세기의 도전(Med Educ, 2011) (0) | 2020.12.19 |