관리추론과 환자-의사 상호작용: 공동 의사결정과 모의 외래환자로부터의 통찰(Med Teach, 2023)
Management reasoning and patient-clinician interactions: Insights from shared decision-making and simulated outpatient encounters (Med Teach. 2023)
David A. Cooka , Ian G. Hargravesb , Christopher R. Stephensonc and Steven J. Durningd
소개
Introduction
의학은 환자의 상태를 진단하는 것보다 환자의 필요를 관리하는 것이 더 중요하지만, 방대한 임상 추론 문헌은 대부분 관리를 무시하여 환자 치료에 해를 끼칩니다(Cook 외. 2018). 최근 연구에서는 환자-임상의 상호작용의 중요한 역할을 포함하여 관리 추론의 중요한 특징이 강조되었습니다(Cook 외. 2018, 2019, 2022b). 실제로 관리 추론은 '전적으로 특정 임상의 내부가 아닌 개인 간의 공간에서' 이루어집니다. (Cook 외. 2022b) 그러나 관리 추론의 이러한 상호 작용 및 의사소통 측면에 대한 우리의 이해는 아직 불완전하게 개발되어 있습니다. 이 연구의 목적은 [관리 추론에서 환자-임상의 상호 작용]에 대한 이해를 넓히는 것입니다.
Medicine is more about managing patient needs than diagnosing their conditions, but the vast clinical reasoning literature largely ignores management, to the detriment of patient care (Cook et al. 2018). Recent work has highlighted important characteristics of management reasoning (Cook et al. 2018, 2019, 2022b), including the crucial role of patient-clinician interactions. Indeed, management reasoning takes place substantially ‘in the space between individuals rather than entirely within a given clinician.’ (Cook et al. 2022b) However, our understanding of this interactional and communicative aspect of management reasoning remains incompletely developed. The purpose of this study is to expand our understanding of patient-clinician interactions in management reasoning.
관리 추론이 진단 추론보다 더 중요하다는 것은 틀림없는 사실이지만, 현재까지 거의 모든 임상 추론 연구와 이론은 후자에 초점을 맞추고 있습니다(Elstein 외. 1978; Eva and Norman, 2005; Norman, 2005; Norman 외. 2007, 2017). 최근에야 관리 추론이 명시적으로 구분되고 논의되기 시작했습니다(Cook et al. 2018, 2019). [관리 추론]은 '임상의가 임상 정보(병력, 검사 결과, 검사 결과), 선호도, 의학 지식, 맥락(상황) 요소를 통합하여 치료, 추가 검사, 후속 진료, 제한된 자원의 할당 등 개별 환자의 관리에 대한 결정을 내리는 인지적 과정'으로 정의되었습니다(Cook 외. 2019).
Management reasoning is arguably more important than diagnostic reasoning, yet nearly all clinical reasoning research and theory to-date have focused on the latter (Elstein et al. 1978; Eva and Norman, 2005; Norman, 2005; Norman et al. 2007, 2017). Only recently has management reasoning been explicitly distinguished and discussed (Cook et al. 2018, 2019). Management reasoning has been defined as ‘the cognitive processes by which clinicians integrate clinical information (history, exam findings, and test results), preferences, medical knowledge, and contextual (situational) factors to make decisions about the management of an individual patient, including decisions about treatment, further testing, follow-up encounters, and allocation of limited resources’ (Cook et al. 2019).
[임상적 추론]은 일반적으로 개별 임상의의 인지적 활동으로 해석됩니다. 이는 진단 추론의 경우 대부분 사실일 수 있지만, 관리 추론은 [공유된 숙고 과정]을 수반합니다(Cook 외. 2019). 최근의 경험적 연구에서 우리는 관리 추론의 주요 특징을 파악하기 위해 의사-환자 간 만남을 시뮬레이션한 동영상을 검토했으며(Cook 외. 2022b), 관리 추론이 한 사람 내에서만 발생하는 것이 아니라 [사람들이 상호 작용할 때 발생]한다는 사실을 확인했습니다. 그러나 우리는 관리 추론에서 환자-임상의 상호 작용에 대한 이해가 불완전하다는 것을 인식하고 있으며, 이 현상에 대한 이해를 심화시키고 교육, 평가, 임상 실습 및 향후 연구에 대한 시사점을 식별해야한다고 느낍니다. 저희는 공유 의사결정(SDM)이 이 문제를 밝히는 데 도움이 될 수 있다고 가정합니다. 공유 의사결정은 환자와 임상의가 함께 협력적으로 의사결정 또는 추론하는 방법에 대한 이론적, 실제적 프레임워크를 제공하기 때문입니다.
Clinical reasoning is commonly construed as a cognitive activity within individual clinicians. While this may be largely true of diagnostic reasoning, management reasoning entails a shared deliberative process (Cook et al. 2019). In a recent empirical study we reviewed videos of simulated physician-patient encounters to identify key features of management reasoning (Cook et al. 2022b), and confirmed that management reasoning occurs as people interact rather than solely within one person. We recognize, however, our incomplete comprehension of patient-clinician interactions in management reasoning, and feel prompted to deepen our understanding of this phenomenon and identify implications for teaching, assessment, clinical practice, and future research. We postulate that shared decision-making (SDM) could help illuminate this issue, as SDM offers theoretical and practical frameworks about how patients and clinicians collaboratively make decisions, or reason, together.
SDM은 [환자의 자율성]과 [환자 중심 치료]를 강화하기 위해 널리 장려되고 있습니다. SDM의 다양한 모델은 환자-임상의 상호 작용의 다양한 측면을 강조합니다. 대부분의 모델은 치료 옵션 중에서 선택할 때와 같이 의사 결정에 환자를 참여시키는 데 중점을 둡니다(Makoul and Clayman, 2006; Bomhof-Roordink 외. 2019).
- 미국 의료 연구 및 품질 관리국 'SHARE' 모델은 임상의가
- 명시적으로 환자의 참여를 구하고,
- 옵션을 탐색하도록 돕고,
- 환자의 가치와 선호도를 평가하고,
- 결정에 도달하고,
- 결정을 평가할 것을 권장합니다(미국 의료 연구 및 품질 관리국, 2020).
- 이와 유사하게, 엘윈의 '세 가지 대화' 모델은 다음을 강조합니다(엘윈 외. 2012, 2017).
- 환자를 의사 결정에 참여시키고(팀 대화),
- 각 옵션에 대해 논의하며(옵션 대화),
- 선호도를 통합하는 것(결정 대화)
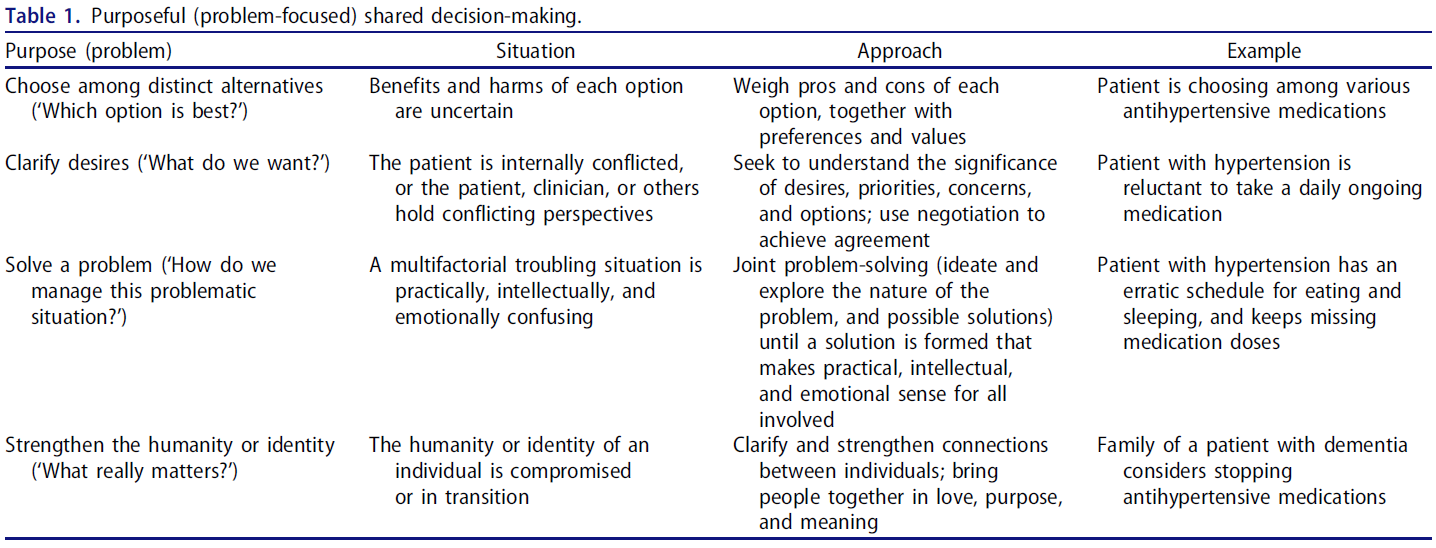
- 최근에는 많은 임상 상황에서 욕구를 명확히 하거나, 문제를 해결하거나, 인간성과 정체성의 실존적 문제를 해결하는 것만큼 옵션 중에서 선택하는 것이 중요하지 않다는 점을 인식한 '목적 지향적 SDM'(Purposeful SDM)이라는 새로운 SDM 모델이 제안되었습니다(표 1)(Hargraves et al. 2019).
SDM is widely promoted to enhance patient autonomy and patient-centered care. Different models of SDM emphasize different aspects of patient-clinician interactions. Most models focus on involving patients in decision-making (Makoul and Clayman, 2006; Bomhof-Roordink et al. 2019), as when choosing among treatment options.
- The Agency for Healthcare Research and Quality ‘SHARE’ model encourages clinicians to
- explicitly Seek the patient’s participation;
- Help them explore options;
- Assess their values and preferences;
- Reach a decision; and
- Evaluate the decision (Agency for Healthcare Research and Quality, 2020).
- Similarly, Elwyn’s ‘Three Talk’ model emphasizes engaging patients in decision-making (team talk), discussing each option (option talk), and integrating preferences (decision talk) (Elwyn et al. 2012, 2017).
- Recently, a new model of SDM has been proposed—‘Purposeful SDM’ (Hargraves et al. 2019)—that recognizes that many clinical situations do not entail choosing among options so much as clarifying desires, solving problems, or addressing existential issues of humanity and identity (Table 1) (Hargraves et al. 2019).
이러한 관점에서 볼 때, [SDM의 주요 목적]은 환자를 의사 결정에 '참여'시키는 것이 아니라, [환자의 특정 문제에 적합한 협력 방법을 수립하는 것]입니다. [목적 지향적 SDM]은 [참여 중심]이 아닌 [문제 중심]입니다.
Viewed through this lens, the primary purpose of SDM is not to “involve” patients in decision-making, but to establish methods for working together that are appropriate for this patient’s particular problems. Purposeful SDM is problem-focused rather than involvement-focused.
이 연구에서는 이러한 SDM 모델('참여 중심', '문제 중심')과 함께 환자와 임상의가 함께 관리 결정을 내리는 시뮬레이션 동영상을 활용하여 성공적인 또는 실패한 관리 추론에 기여하는 환자-임상의 상호 작용 요소를 조명했습니다.
In this study we drew on videos of simulated patients and clinicians as they made management decisions together, along with these SDM models (‘involvement-focused,’ ‘problem-focused’), to illuminate elements of patient-clinician interactions that contribute to successful or unsuccessful management reasoning.
방법
Method
저희는 환자와 임상의의 모의 만남을 담은 10개의 비디오를 검토하고 [두 가지 개념적 렌즈]를 통해 관찰한 내용을 체계적으로 해석했습니다. 이 동영상은 이전 연구(Cook 외. 2022b)에서 사용한 것과 동일한 동영상이지만, 새롭게 수집한 데이터와 새로운 프레임워크를 사용하여 고유한 스토리를 전달했습니다.
We reviewed 10 videos of simulated patient-clinician encounters and systematically interpreted our observations through two distinct conceptual lenses. These were the same videos used in our previous study (Cook et al. 2022b), but we used newly-collected data and novel frameworks to tell a unique story.
비디오 선택 및 코딩
Video selection and coding
각 비디오(45초~7분 길이)는 [레지던트 의사와 환자 간의 모의 외래 환자 추적 관찰]을 묘사했습니다. 평가자 교육 연구에 사용된 비디오 라이브러리에서 5가지 의학적 문제(고혈압, 고지혈증, 섬유근육통, 당뇨병, 유두상 갑상선암)에 대해 각각 2개의 비디오를 선택했습니다(Cook et al. 2009, Cook and Beckman, 2009). 이러한 경험을 통해 학습을 극대화하기 위해 52명의 내과 의사('극단적인 그룹'의 의도적 표본 추출)의 미니 CEX '상담' 평점을 기준으로 각 문제별로 가장 낮은 점수와 가장 높은 점수를 받은 동영상을 선정했습니다.
- 3개 문제(6개 동영상)의 경우 레지던트-배우가 열악한 연기와 우수한 연기를 번갈아 연기하도록 코칭을 받았고, 환자-배우에게는 대본 없이 진정성 있는 답변을 하도록 지시했습니다.
- 나머지 4개의 비디오는 대본이 작성되었습니다.
Each video (45 s to 7 min long) portrayed a simulated outpatient follow-up encounter between a resident physician and a patient. From a library of videos used in a study of rater training (Cook et al. 2009; Cook and Beckman, 2009) we selected 2 videos for each of 5 medical problems (hypertension, hyperlipidemia, fibromyalgia, diabetes mellitus, and papillary thyroid cancer). To maximize our learning from these encounters, we selected the lowest-scoring and highest-scoring videos for each problem, based on mini-CEX ‘counseling’ ratings from 52 internal medicine physicians (‘extreme groups’ purposive sampling).
- For 3 problems (6 videos) the resident-actor was coached to alternately portray poor or superior performance, and the patient-actor was instructed to respond authentically; there was no written script.
- The other 4 videos were scripted.
비디오는 2단계에 걸쳐 검토되었습니다. 1단계(2020년 11월)에서는 4명의 연구자(DAC, CRS, SJD, LDG)가 개방형 프롬프트가 포함된 코딩 양식(부록 1, 보충 자료)을 사용하여 각 비디오를 최소 2회 독립적으로 검토했습니다:
- '이 만남에서 관리 추론의 어떤 특징이 분명하게 드러나는가? [환자, 제공자, 시스템 선호도, 제약, 가치의 우선순위, 의사소통 및 공유된 의사결정(환자 선호도 확인, 통합) 등 5가지 특징 목록]'을 포함한 5가지 특징 목록으로 구성했습니다.
논의는 2021년 10월부터 2022년 1월까지 계속되었습니다.
We reviewed videos in 2 phases. In phase 1 (November 2020), 4 investigators (DAC, CRS, SJD, LDG) independently reviewed each video at least twice using a coding form with open-ended prompts (Appendix 1, Supplementary material), including:
- ‘What features of management reasoning are evident in this encounter? [list of 5 features including Prioritization of patient, provider, and system preferences, constraints, and values; and Communication and shared decision-making (ascertainment of, integration with patient preferences)].’
Discussions continued October 2021 to January 2022.
데이터 분석 중에 커뮤니케이션과 SDM은 추가 조사가 필요한 것으로 나타났으며, 2단계(2022년 2월)에서 이를 추진했습니다. 먼저 Purposeful SDM 모델의 주요 개발자를 포함하여 SDM에 대한 폭넓은 경험을 가진 조사자(IGH)를 팀에 추가했습니다(Hargraves 외. 2019). 그는 처음에는 1단계 조사 결과에 대한 지식 없이 독립적으로 동일한 동영상을 검토한 다음, 조사자 DAC 및 SJD와 함께 동일한 동영상을 검토했습니다. 이 조사자들은 처음에는 독립적으로, 그다음에는 그룹으로 각 비디오를 검토하면서 참여 중심 모델과 문제 중심 모델을 차례로 명시적으로 고려했습니다. 각 영상에 대해 각 모델의 주요 특징이 반영되었는지 여부를 코딩했습니다(부록 2, 보충 자료). 참여 중심 모델의 주요 특징은 쓰리 토크 모델(OPTION-5(Barr 외. 2015))에 기반한 도구와 최근 검토(Bomhof-Roordink 외. 2019)를 통해 확인했습니다. 문제 중심 모델의 경우, 목적 중심 SDM(Hargraves et al. 2019)의 개념을 사용했습니다(표 1). 개방형 프롬프트를 사용하여 추가 관찰 사항을 문서화했습니다.
During data analysis, communication and SDM stood out as warranting further investigation, which we pursued in phase 2 (February 2022). We first added to our team an investigator (IGH) with extensive experience in SDM including being a principal developer of the Purposeful SDM model (Hargraves et al. 2019). He reviewed the same videos, first independently and without knowledge of the phase 1 findings, and then in conjunction with investigators DAC and SJD. These investigators reviewed each video, first independently and then as a group, explicitly considering in turn the involvement-focused and problem-focused models of SDM. For each video we coded whether key features of each model were reflected in the encounter (Appendix 2, Supplementary material). We identified key features of the involvement-focused model from an instrument grounded in the Three Talk model (the OPTION-5 (Barr et al. 2015)) and from a recent review (Bomhof-Roordink et al. 2019). For the problem-focused model we used concepts from Purposeful SDM (Hargraves et al. 2019) (Table 1). We documented additional observations using open-ended prompts.
데이터 분석 및 모델 구축
Data analysis and model building
우리는 4단계로 진행되는 지속적인 비교 질적 분석 접근법(Glaser, 1965)을 사용했습니다.
- 1단계에서는 모든 원시 관찰을 요약하고 검토하여 1단계의 초기 관찰을 분석했습니다(특정 SDM 모델 없음). 그런 다음 여러 차례의 음성 및 전자 매개 대화를 통해 중복을 해결하고 이러한 관찰을 반복적으로 재구성, 재개념화, 정교화 및 구체화했습니다.
We used a constant comparative qualitative analysis approach (Glaser, 1965), proceeding in 4 stages. In stage 1, we analyzed the initial observations from phase 1 (no specific SDM model) by summarizing and reviewing all raw observations. We then engaged in multiple voice and electronic-mediated conversations to resolve redundancies and iteratively reorganize, reconceptualize, elaborate, and refine these observations. - 환자-임상의 상호작용에 대한 추가 인사이트를 얻을 수 있는 기회를 인식하고 풍부한 새로운 데이터를 수집했습니다(위의 2단계, IGH의 독립 검토 및 그룹의 공동 검토 포함). 이러한 데이터를 분석하는 동안(2단계) 우리는 각 비디오에 대해 차례로 논의하면서 개별 코딩을 공유하고 각 모델의 렌즈를 통해 이러한 결과를 해석하면서 추가 인사이트를 공동으로 정교화했습니다.
Recognizing the opportunity to glean further insights regarding patient-clinician interactions, we collected abundant new data (phase 2 above, including IGH's independent review and the group’s conjoint review). During analysis of these data (stage 2) we discussed each video in turn, sharing our individual codings and jointly elaborating further insights as we interpreted these findings through the lens of each respective model. - 다음 단계(3단계)에서는 관리 추론과 환자-임상의 상호작용 간의 연관성을 명시적으로 탐색했습니다. 1단계와 2단계에서 얻은 결과를 사용하여 이전에 보고된 12가지 관리 추론 기능(Cook 외. 2022b) 각각과 참여 중심 및 문제 중심 SDM 모델 간의 상호 영향을 체계적으로 고려했습니다.
Next (stage 3) we explicitly explored the connections between management reasoning and patient-clinician interactions. Using our findings from stages 1 and 2, we systematically considered the reciprocal implications between each of 12 previously-reported management reasoning features (Cook et al. 2022b) and the involvement-focused and problem-focused SDM models. - 마지막으로 4단계에서는 축 분석을 통해 다양한 기능과 모델을 비교하여 몇 가지 잠정적인 모범 사례를 식별했습니다.
Finally, in stage 4 we used axial analysis to cut across the various features and models, to identify several tentative best practices.
모든 검토자가 주요 결과에 대해 완전한 합의를 도출했습니다. 부록 1~3에는 모든 관찰 및 분석에 대한 자세한 문서 추적이 포함되어 있습니다(보충 자료).
All reviewers came to full consensus on key findings. Appendices 1–3 contain a detailed paper trail of all observations and analyses (Supplementary material).
반사성
Reflexivity
우리의 배경은 관찰과 분석에 분명 영향을 미쳤습니다. 세 명의 조사자(DAC, SJD, CRS)는 현직 의사(일반 내과 전문의)이며, 두 명의 조사자는 교육/인지(SJD) 및 디자인, 커뮤니케이션, SDM(IGH) 분야의 박사 학위를 보유하고 있습니다. 세 명의 연구자(DAC, SJD, CRS)가 12가지 기능의 경영 추론 모델을 설명하는 데 협력했으며, 한 명(IGH)은 목적 지향적 SDM 모델을 개발했습니다(Hargraves et al. 2019).
Our background surely influenced our observations and analyses. Three investigators (DAC, SJD, CRS) are practicing physicians (general internists) and 2 have PhDs with backgrounds in education/cognition (SJD) and design, communication, and SDM (IGH). Three investigators (DAC, SJD, CRS) collaborated in describing the 12-feature model of management reasoning and one (IGH) developed the purposeful SDM model (Hargraves et al. 2019).
결과
Results
개념적 모델 없이 관찰(1단계)
Observations without conceptual model (stage 1)
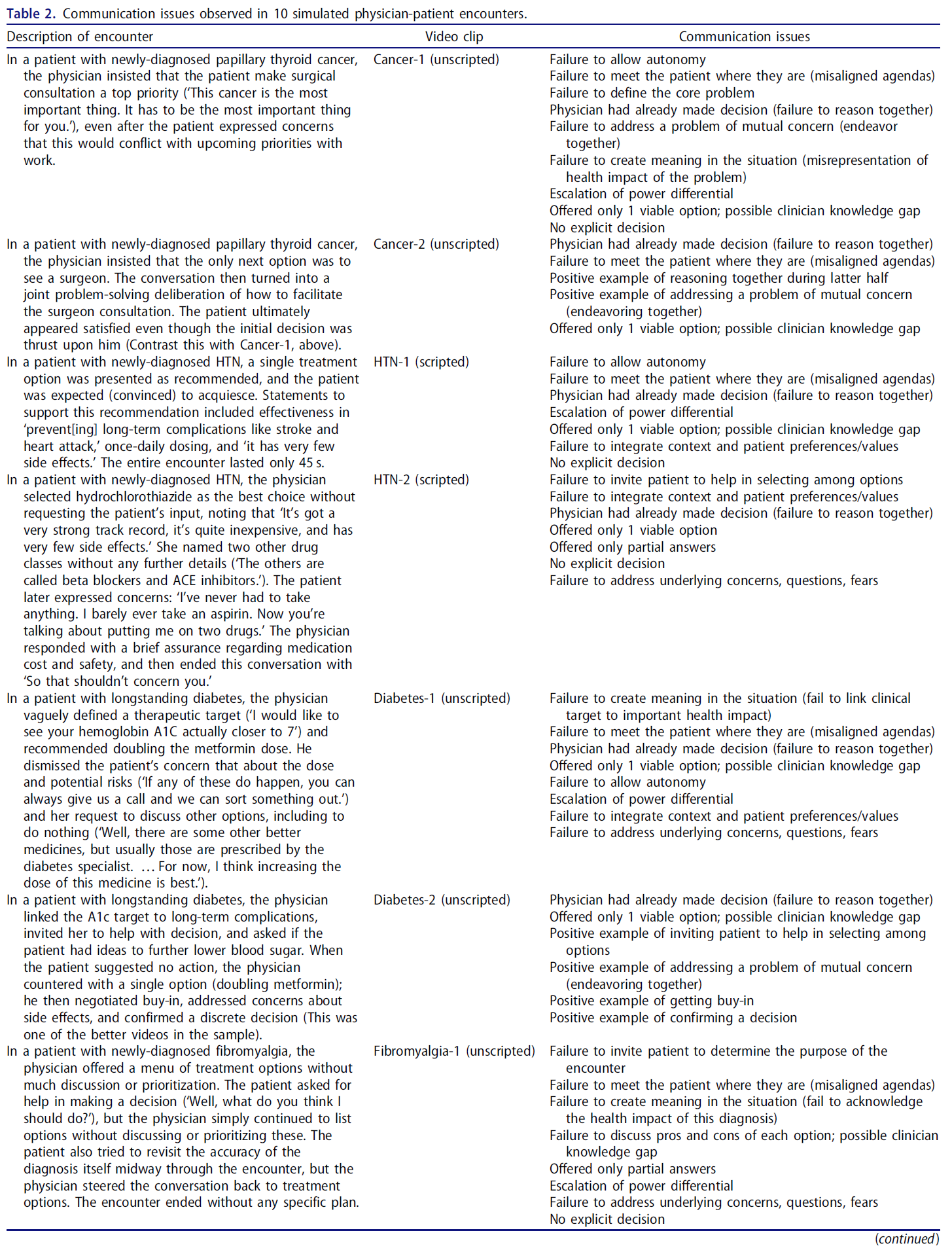
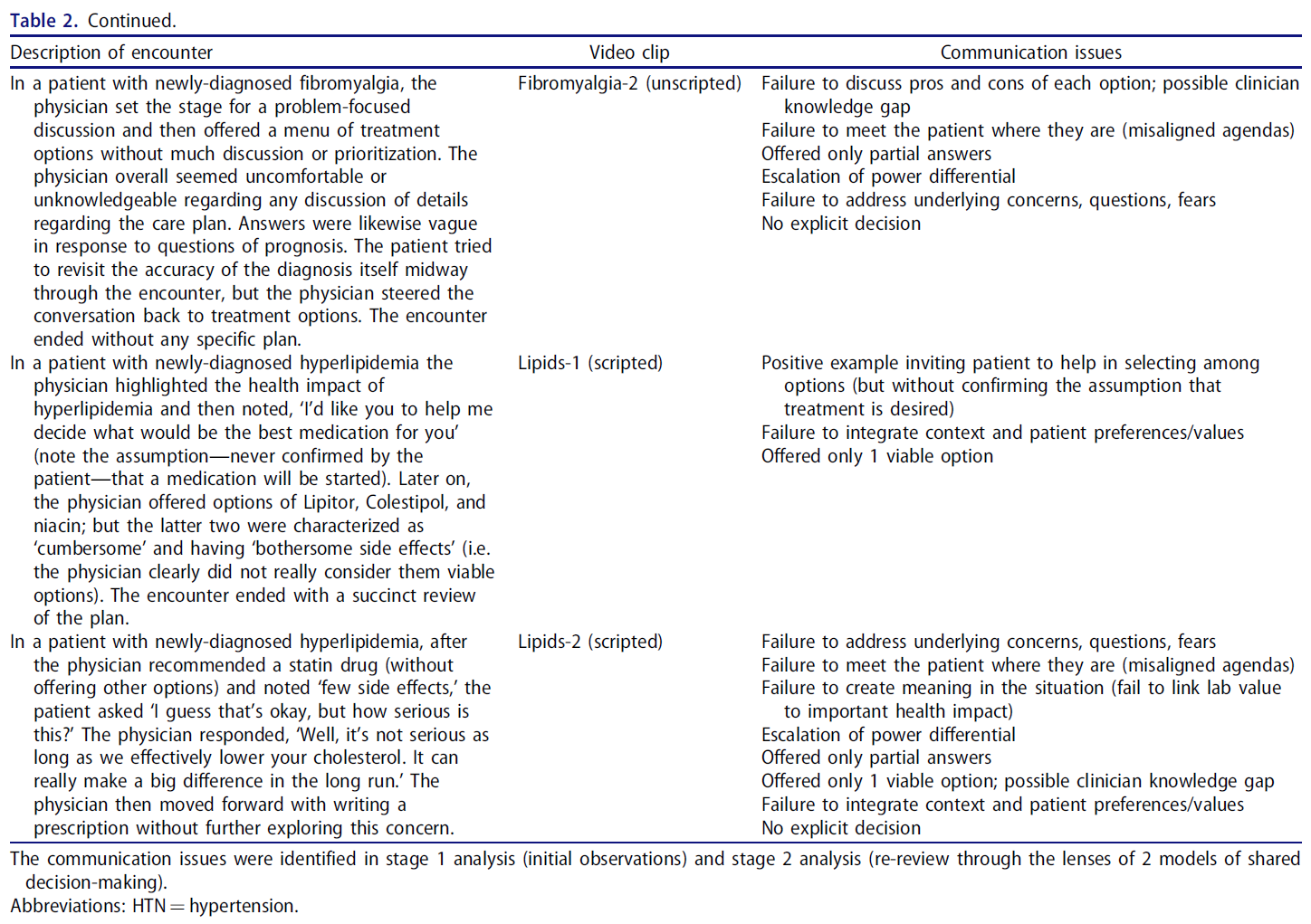
먼저 특정 개념적 모델 없이 관찰한 내용을 보고하고, 환자-임상의 상호작용의 질이 특히 낮거나 추론 과정 또는 치료 계획에 해로운 것으로 보이는 사례(및 그에 따른 시사점, 결과 또는 문제)를 강조했습니다. 또한, 아무리 우수한 동영상이라도 평범한 수준에 불과하다고 판단되는 경우라도 우수한 성과를 보인 사례도 찾았습니다. 표 2에는 각 비디오와 눈에 띄는 인상이 설명되어 있으며, 부록 1에는 관찰 및 분석에 대한 자세한 내용이 나와 있습니다(보충 자료).
We first report observations made without a specific conceptual model, highlighting instances (and corresponding implications, consequences, or problems) in which the patient-clinician interaction was of particularly poor quality or seemed detrimental to the reasoning process or care plan. We also sought instances of superior performance, although in our judgment even the best videos were only mediocre. Table 2 describes each video and salient impressions; Appendix 1 details our observations and analyses (Supplementary Material).
의사는 환자의 자율성이나 선택을 허용하거나 장려하지 않는 경우가 많았습니다. 이는 대놓고 드러나는 경우는 거의 없었습니다(예: 단 하나의 옵션만 제시된 동영상은 단 한 편뿐이었음). 그러나 [미묘한 표현]으로 자율성을 침해하는 경우가 종종 있었습니다. 한 조사자는 의사들이 '환자의 의사를 뭉겠다'고 썼습니다. 예를 들어, 새로 갑상선 유두암 진단을 받은 환자에게 의사는 환자에게 수술 상담을 최우선 순위로 삼으라고 주장했습니다('이 암은 가장 중요한 암입니다. 이 암은 당신에게 가장 중요한 것이어야 합니다'), 환자가 업무 마감일과 충돌할 수 있다는 우려를 표명했음에도 불구하고. 고혈압, 고지혈증, 당뇨병에 대한 약물 치료 시작을 보여주는 동영상에서는 일반적으로 한 가지 치료 옵션이 권장되는 것으로 제시되고 환자는 이에 동의할 것으로 예상(설득)되었습니다. 이러한 문제는 치료 옵션을 식별할 때뿐만 아니라 치료 목표를 정의할 때도 나타났습니다. 예를 들어, 당뇨병 환자의 경우 의사는 국가 가이드라인에 정의된 치료 목표를 선언했지만 환자에게 이러한 목표에 동의하는지 묻지 않았습니다.
Physicians often failed to allow or encourage patient autonomy or choice. This was rarely overt (i.e. there was only one video in which only a single option was presented). However, subtle statements frequently subverted autonomy. As one investigator wrote, physicians ‘steamrolled over the patient’s wishes.’ For example, with a patient with newly-diagnosed papillary thyroid cancer, the physician insisted that the patient make surgical consultation a top priority (‘This cancer is the most important thing. It has to be the most important thing for you’), even after the patient expressed concerns that this would conflict with work deadlines. In videos showing initiation of drugs for hypertension, hyperlipidemia, or diabetes, a single treatment option was typically presented as recommended, and the patient was expected (convinced) to acquiesce. This problem appeared not only in identifying treatment options; it also showed up in defining goals of care. For example, in a patient with diabetes, the physician declared treatment targets as defined by national guidelines, but never asked the patient if she agreed with these targets.
의사는 일반적으로 환자에게 관리 옵션 목록을 제공했지만, 환자에게 이러한 옵션 중 하나를 선택하도록 명시적으로 권유하는 경우는 드물었습니다. 상담의 여러 단계에서 어려움이 드러났습니다.
- 상담의 목표(해결해야 할 문제)를 정의할 때 새로 섬유근육통을 진단받은 환자는 진단의 정확성을 다시 확인하고자 했지만, 의사는 곧바로 치료 옵션으로 대화를 이끌었습니다.
- 고혈압에 대한 초기 약물 치료를 논의할 때 환자에게 세 가지 옵션이 주어졌지만 의사는 환자의 의견을 묻지 않고 환자의 의학적 문제에 맞춰 가장 적합한 옵션을 선택했습니다.
- 치료 목표를 고려할 때 의사는 가이드라인에 따른 당화혈색소(A1c) 목표치를 제시하고 그보다 조금 더 높은 목표를 제시하는 환자의 제안을 무시했습니다.
이와 대조적으로 한 동영상에서는 의사가 고지혈증 환자에게 "어떤 약이 가장 좋을지 결정할 수 있도록 도와달라"고 요청했습니다.
Although physicians usually offered patients a list of management options, only infrequently did they explicitly invite patients to participate in choosing among these options. Difficulties surfaced at various stages in the encounter.
- When defining the goal of the encounter (problem to be addressed), a patient with newly-diagnosed fibromyalgia wanted to revisit the accuracy of the diagnosis, yet the physician steered the conversation immediately to treatment options.
- When discussing initial drug treatment for hypertension, a patient was given three options but the physician selected her top choice (tailored to the patient’s medical problems) without soliciting the patient’s input.
- When considering goals of therapy, a physician invoked a guideline-aligned A1c target and subsequently brushed aside the patient’s suggestion of a slightly higher target.
By contrast, in one video the physician invited a patient with hyperlipidemia, ‘I’d like you to help me decide what would be the best medication for you.’
의사는 종종 그 만남에서 [해결해야 할 핵심 문제를 정의하는 데 실패]했습니다. 위의 갑상선암과 섬유근육통의 예는 이 점을 잘 보여줍니다. 환자를 참여시키지 않음으로써 환자에게 가장 중요한 문제(상충되는 개인적 우선순위 또는 진단의 정확성에 대한 우려)를 고려하지 않고 궁극적으로 의사에게 가장 중요한 문제(치료)에 집중하게 됩니다. 이 문제는 치료 옵션을 논의할 때 다른 만남에서도 나타났습니다. 예를 들어, 의사는 일반적으로 치료 효과에 초점을 맞추는 반면 환자는 부작용과 비용에 대해 인내심을 발휘했습니다.
Physicians often fell short in defining the core problem to be addressed in the encounter. The examples above of thyroid cancer and fibromyalgia illustrate this point: By failing to involve the patient, they ultimately focused on the problem most salient to the physician (treatment) without considering the problem most salient to the patient (juggling conflicting personal priorities or concerns about the accuracy of diagnosis). This issue surfaced in other encounters when discussing treatment options. For example, physicians commonly focused on treatment efficacy while patients perseverated on side effects and cost.
의사들은 때때로 [근본적인 우려, 두려움, 질문]을 탐색하고 해결하지 못했습니다.
- 한 고혈압 환자는 '약을 먹어본 적이 없어요. 아스피린도 거의 먹지 않아요. 그런데 이제 두 가지 약을 먹으라고 하네요'라고 말했습니다. 의사는 약이 저렴하고 매우 안전하다고 짧게 대답한 후 '그러니 걱정하지 않으셔도 됩니다'라고 말하며 대화를 끝냈습니다.
- 고지혈증 환자에게 의사는 다른 옵션은 제시하지 않고 스타틴 계열의 약을 추천하면서 '부작용이 거의 없다'고 언급했습니다. 환자가 '괜찮지만 얼마나 심각한가요?"라고 묻자 의사는 "콜레스테롤을 효과적으로 낮추는 한 심각하지 않습니다."라고 대답했습니다. 장기적으로는 정말 큰 차이를 만들 수 있습니다."라고 대답했습니다. 그 후 의사는 이 문제에 대해 더 자세히 알아보지 않고 처방전을 작성했습니다.
Physicians occasionally failed to explore and address underlying concerns, fears, and questions.
- A patient with hypertension expressed, ‘I’ve never had to take anything. I barely ever take an aspirin. Now you’re talking about putting me on two drugs.’ The physician responded with a brief assurance that the medication was inexpensive and quite safe, and then terminated the conversation with, ‘So that shouldn’t concern you.’
- For a patient with hyperlipidemia the physician recommended a statin drug (without offering other options) and noted ‘few side effects.’ When the patient asked, ‘I guess that’s okay, but how serious is this?’ the physician responded, ‘Well, it’s not serious as long as we effectively lower your cholesterol. It can really make a big difference in the long run.’ The physician then moved forward with writing a prescription without further exploring this concern.
의사 결정의 [맥락을 적절히 탐색하지 않는 것]은 어디에나 있었습니다. 의사들은 환자에게 선호도, 가치관, 자원, 제약 조건에 대해 직접 질문하는 경우가 거의 없었으며, 설령 질문을 하더라도 짧고 피상적인 수준에 그쳤습니다. 의사들은 상황을 완전히 파악하기 위해 추가 질문을 하는 경우는 거의 없었습니다. 의료팀이나 시스템의 자원과 제약을 탐색하는 의사의 사례는 훨씬 더 적었습니다.
Failure to adequately explore the context of decision-making was ubiquitous. Physicians rarely asked the patients directly about their preferences, values, resources, and constraints, and when they did the inquiry was brief and superficial. Physicians never followed with additional probing questions to fully explore the situation. We saw even fewer examples of physicians exploring the resources and constraints of the health care team or system.
좀 더 넓게 보면, 이러한 실패와 다른 실패는 환자가 있는 곳에서 환자를 만나지 못하는 것, 즉 의사의 의제와 환자의 의제 사이의 단절로 통합됩니다. 위의 예 외에도 당뇨병 환자의 다른 동영상에서 의사는 약물 치료를 강화하라는 권고를 완화할 수 있는 생활 습관 조치에 관한 과거의 논의를 기억하지 못했습니다.
Viewed more broadly, these and other failures coalesce into a failure to meet the patient where they are—a disconnect between the physician’s agenda and the patient’s. In addition to the examples above, in a different video of a patient with diabetes, the physician failed to remember past discussions regarding lifestyle measures that might have mitigated recommendations to intensify drug treatment.
거의 모든 동영상에서 의사는 [환자와 함께 환자의 욕구, 우선순위, 동반 질환, 자원 등을 통합하는 데 실패]했습니다. 많은 동영상에서 의사는 매우 제한된 범위의 옵션을 제시했습니다. 다른 영상에서는 의사가 여러 가지 옵션을 제시했지만 환자의 고유한 요구 사항을 고려하여 명시적으로 우선순위를 정하지 않았습니다. 이러한 행동은 비개인적인(맞춤화되지 않은 일반적인) 계획으로 이어졌습니다.
In nearly every video, the physician failed to work jointly with the patient to integrate their desires, priorities, comorbidities, resources, etc. In many videos the physician presented a very limited range of options. In others, the physician offered several options but did not explicitly prioritize these considering the patient’s unique needs. Such actions resulted in an impersonal (untailored, generic) plan.
마지막으로, 임상의와 환자 간의 [관계를 구축하는 데 전반적으로 실패]한 것으로 나타났습니다. 어떤 경우에는 '증기 압연' 욕구와 잊혀진 대화의 경우처럼 의도하지는 않았지만 적극적으로 (비록 의도하지는 않았지만) 이러한 관계가 훼손되었습니다. 다른 영상에서는 서두르는 대화, 고민을 털어놓지 않거나 무시하는 말투 등 좀 더 미묘했습니다. 이는 관계에 상처를 입혔다기보다는 소홀히 한 것을 반영합니다.
Finally, we noted a general failure to build the clinician-patient relationship. In some instances, this relationship was actively (albeit unintentionally) undermined—as in the cases of ‘steamrolled’ desires and forgotten conversations. In other videos it was more subtle—a hurried conversation, failure to explore concerns, or dismissive tone of voice. These reflect a neglect of rather than injury to the relationship.
SDM의 렌즈를 통한 조사(2단계)
Examination through lens of SDM (stage 2)
위의 결과를 바탕으로 상호 보완적인 인사이트를 발견하기 위해 두 가지 SDM 렌즈(모델)를 사용하여 이러한 동영상을 체계적으로 재검토했습니다(표 2). 부록 2에는 방법, 관찰 및 분석에 대한 자세한 내용이 나와 있습니다(보충 자료).
Building on the above results, we systematically re-examined these videos (Table 2) using 2 lenses (models) of SDM in hope of discovering complementary insights; Appendix 2 details our methods, observations, and analyses (Supplementary Material).
참여 중심 모델
Involvement-focused model
[참여 중심 모델]은 [SDM의 전통적인 개념]으로, 환자가 의사 결정에 적절히 참여하여 자율성을 존중하고 가치에 기반한 의사 결정을 내릴 수 있도록 돕는 것이 SDM의 주된 이유입니다. 이러한 접근 방식의 대표적 모델인 [Three Talk 모델](Elwyn 외. 2017)은 SDM 회의에서 환자가 [팀 토크, 옵션 토크, 결정 토크]의 3단계 대화에 참여하도록 합니다. 우리는 이 모델을 사용하여 참여 중심 렌즈를 통해 해석된 관찰을 구조화했습니다.
The involvement-focused model represents a traditional concept of SDM wherein the predominant reason for SDM is to ensure that patients are adequately involved in decision-making, to respect their autonomy and help them make value-informed decisions. Representative of this approach, the Three Talk model (Elwyn et al. 2017) involves patients at 3 stages of conversation in SDM encounters: team talk, option talk, and decision talk. We used this model to structure observations interpreted through the involvement-focused lens.
Issues related to team talk
[팀 대화]는 환자를 의사 결정에 참여하도록 유도하고 협력 관계를 구축합니다. 위에서 언급한 바와 같이, 의사들이 환자를 의사 결정에 참여시키고 동등하게 협력하도록 초대하는 경우는 거의 없었습니다. 또한, 많은 경우 대화가 오히려 [환자의 자율성을 떨어]뜨리고 [의사와 환자 간의 권력 차이를 확대]하는 것으로 나타났습니다. 갑상선암 환자(환자에게 즉시 외과 의사를 만나라고 주장), 섬유근육통 환자(진단 재검토 요청 무시), 당뇨병 환자(치료 강화를 연기하자는 환자의 제안 묵살) 등이 그 예입니다.
Team talk invites the patient to participate in decision-making and establishes a collaborative relationship. As noted above, only rarely did physicians invite patients to engage in decision-making and collaborate as equals. Moreover, we noted that in many instances the conversation actually diminished patient autonomy and escalated the power differential between physician and patient. Examples include the patients with thyroid cancer (insisting the patient see a surgeon immediately), fibromyalgia (ignoring requests to revisit the diagnosis), and diabetes (dismissing the patient’s proposal to defer treatment intensification).
Issues related to option talk
옵션 대화에서는 의사가 제시한 옵션의 장단점에 대해 논의합니다. 거의 모든 만남에서 의사는 거의 옵션을 제공하지 않았으며 각 옵션에 대한 정보도 제한적으로만 제공했습니다(위 및 표 2 참조).
Option talk discusses the pros and cons of the options identified by the physician. In nearly every encounter, physicians offered very few options and provided only limited information about each option (see above and Table 2).
또한 의사들은 [아무것도 하지 않는 옵션]을 제공한 적이 없었습니다. 그들은 항상 환자에게 조치가 필요하고 환자가 원한다고 가정했습니다.
Moreover, physicians never offered the option of doing nothing. They always assumed action was needed and desired by patient.
이러한 [제한된 옵션 목록]은 대안, 부작용, 비용, 일반적으로 차선책이 선호되는 상황(예: 비용 또는 편의성 기준) 또는 즉각적인 조치가 없을 때의 실제 위험에 대한 불완전한 지식 등 [임상의의 지식 격차]를 반영하는 것일 수 있다는 것을 감지했습니다. 지식 격차는 또한 환자의 질문에 대한 불완전한 답변(부분적인 답변 또는 질문과 관련이 있지만 직접적으로 다루지 않는 답변)의 기저에 있는 것으로 보였습니다. 지식 격차가 흔해 보였지만, 실제 지식 오류는 이 동영상에서 드물게 나타났습니다.
We sensed that such constrained option lists could reflect clinician knowledge gaps—incomplete knowledge of alternatives, side effects, costs, situations in which a typically-suboptimal option might emerge as preferred (e.g. based on cost or convenience), or the true risk of no immediate action. Knowledge gaps also seemed to underlie incomplete responses to patient questions (partial answers or answers related to but not directly addressing the question). Although knowledge gaps seemed common, actual knowledge errors were infrequent in these videos.
Issues related to decision talk
[의사 결정 대화]는 환자의 선호도를 파악하고 통합하여 결정을 내리는 과정입니다. 의사는 일반적으로 환자의 선호도를 구하거나 환자를 진지하게 대하지 않았습니다. 예를 들어 당화혈색소(A1c)가 목표치보다 약간 높은 당뇨병 환자에게 메트포르민 용량을 늘려야 하며 생활습관 개선만으로는 충분하지 않다는 말을 들었다면, 이는 목표 설정과 치료 결정 모두에 환자가 관여하는 것에 위배됩니다. 마찬가지로, 유두상 갑상선암 환자는 우려를 표명했지만 대놓고 무시당했습니다.
Decision talk identifies and integrates the patient’s preferences culminating in a decision. Physicians typically did not seek the patient’s preferences or earnestly entertain them. For example, a patient with diabetes and an A1c slightly above goal was told she needed to increase the dose of metformin and that lifestyle measures would be inadequate; this violates involvement in both establishing targets and deciding on treatment. Likewise, the patient with papillary thyroid cancer expressed concerns that were overtly brushed aside.
문제 중심 모델
Problem-focused model
[문제 중심 모델](목적 중심 SDM, 표 1)에서 SDM의 목적은 [환자가 겪고 있는 문제(좁게 또는 넓게 정의)를 해결]하기 위한 것입니다.
- 참여 중심 모델이 대화 유형과 자율성에 중점을 두는 반면,
- 문제 중심 접근 방식은 환자와 의사가 이 문제에 대한 적절한 대응책을 함께 발견할 수 있는 방법에 중점을 둡니다. 이러한 단계에는 다음이 포함됩니다.
- 문제 특성 파악,
- 가능한 해결책 제안,
- 여러 가능성 중 판단 방법 결정,
- 치료 계획 개발
이러한 요소(문제, 가능성, 판단 접근 방식, 치료 계획) 중 어느 것도 대화 전에 완전히 정의된 것은 없습니다. 대화의 목적은 각 요소를 발견하고, 활용하고, 조정하여 잘 형성된 대응 가능한 문제 해결책을 만들기 위해 '함께 노력'하는 것입니다. 이와 대조적으로, 많은 [참여 중심 모델]은 문제와 가능성(옵션)을 미리 알고 있다고 가정합니다. 우리는 문제 중심 렌즈를 통해 관찰한 내용을 해석하면서 추가적인 인사이트를 발견했습니다.
In the problem-focused model (Purposeful SDM, Table 1), the reason for SDM is to address a problem (narrowly or broadly defined) that the patient is experiencing.
- Whereas the involvement-focused model concentrates on types of talk and autonomy,
- a problem-focused approach concentrates on how the patient and physician can discover together an appropriate response to this problem. These steps include:
- characterize the problem,
- propose possible solutions,
- determine how to judge among the possibilities, and
- develop a care plan.
None of these elements (the problem, possibilities, judgement approach, or care plan) are fully defined prior to the conversation. The purpose of conversation is to ‘endeavor together’ to discover, use, and adapt each element to craft a well-formed, responsive problem resolution. By contrast, many involvement-focused models assume that the problem and possibilities (options) are known up-front. We identified additional insights as we interpreted our observations through the problem-focused lens.
Issues related to characterizing problems
환자와 임상의 사이의 숙의 과정에는 [문제 상황의 인간적 의미를 이해]하는 것이 포함됩니다. 이 동영상에서 의사들은 일반적으로 문제에 대한 매우 좁은 개념을 전달했으며, 종종 '높은 LDL = 스타틴' 또는 '갑상선암 = 수술 상담'과 같은 특정 해결책과 연결시켰습니다. 환자나 상황보다는 검사 결과, 조직 검사 또는 질병을 관리하는 경향이 있었습니다.
Part of deliberation between patient and clinician involves developing an understanding of the human significance of the problematic situation. In these videos, physicians typically conveyed a very narrow conception of the problem, often linking it with a specific solution: ‘high LDL = statin’ or ‘thyroid cancer = surgical consultation.’ They tended to manage the test result, biopsy, or disease, rather than the patient or situation.
이 과정에서 [상황의 진정한 의미], 즉 문제와 잠재적 해결책이 [환자의 건강과 삶 전반에 미치는 영향]을 전달하지 못했습니다. 이러한 실패에는 건강에 미치는 영향보다는 다음이 포함될 수 있습니다.
- 중간 목표(예: 심혈관 질환 위험보다는 당화혈색소 또는 혈압 목표)에 초점을 맞추거나,
- 질병의 영향을 최소화하거나 과장하거나,
- 문제와 해결책이 불일치하는 경우(예: 심각한 문제와 사소한 해결책 또는 그 반대의 경우)
예를 들어, 유두상 갑상선암은 비교적 무해하여 몇 주만 지연해도 문제가 거의 발생하지 않는데도 의사는 긴급한 수술 의뢰를 고집했습니다. 이러한 실패는 의사(및 상황에 대한 잘못된 이해)나 대화 중 잘못된 단계로 인해 발생할 수 있습니다. 결론적으로, 대부분의 '공유' 의사 결정은 공식적이고 의사의 치료 목표에 초점을 맞춘 것이었습니다.
In doing so, they failed to convey the true meaning of the situation—the impact (of both the problem and potential solutions) on the patient’s health and life in general. This failure could involve
- focusing on interim objectives rather than health impact (e.g. A1c or blood pressure targets rather than risk of cardiovascular events),
- minimizing or overstating the impact of illness, or
- mismatching the problem and solution (e.g. a serious problem and a trifling solution, or vice versa).
For example, papillary thyroid cancer is relatively innocuous, such that a few-week delay would rarely cause problems, yet the physician insisted on urgent surgical referral. Such failures can arise within the physician (and their [mis]understanding of the situation), or from mis-steps in the conversation. As a corollary, most ‘shared’ decision-making was formulaic and focused on physician goals of care.
예외적으로, 의사와 환자가 합의된 관심사(예: 문제)를 해결하기 위해 함께 노력한 몇 가지 사례를 확인했습니다. 예를 들어, 다른 갑상선암 동영상에서 의사는 환자가 외과 의사를 만나야 한다는 일방적인 결정을 내렸지만, 환자가 스케줄에 대한 상충을 명확히 밝히자 대화는 외과 의사와의 상담을 촉진하는 방법을 모색하는 공동 문제 해결 심의 과정으로 전환되었습니다. 환자는 초기 결정이 내려졌음에도 불구하고 궁극적으로 만족하는 모습을 보였습니다. 이는 공동 심의를 거치지 않은 '동일한' 시나리오에서 의제와 우선순위가 충돌한 것과는 극명한 대조를 이룹니다.
As an exception, we identified a few instances in which the physician and patient worked together to address an area of agreed-upon concern (i.e. a problem). For example, in the other thyroid cancer video the physician made a unilateral decision that the patient needed to see a surgeon, but when the patient articulated scheduling conflicts the conversation transformed into a joint problem-solving deliberation exploring how to facilitate the surgeon consultation. The patient ultimately appeared satisfied even though the initial decision was thrust upon him. This contrasts sharply with the ‘same’ scenario without joint deliberation that led to a clash of agendas and priorities.
Issues related to proposing possibilities
심의의 또 다른 측면은 문제에 대한 [가능한 대응을 식별]하는 것입니다. 환자와 의사는 함께 협력하여 [가능한 해결책을 제안하거나, 만들거나, 발견]할 수 있습니다. 위에서 언급한 바와 같이, 이 동영상에서 의사들은 거의 항상 하나의 실행 가능한 옵션을 제시하고 다른 대안(있는 경우)은 열등한 것으로 묘사했습니다. 까다로운 수술 상담을 해결한 대화(위)는 공동으로 협력하여 대안을 찾아낸 좋은 예입니다.
Another aspect of deliberation involves identifying possible responses to a problem. Working together, patients and physicians may propose, create, or discover possible solutions. As noted above, in these videos physicians nearly always offered a single viable option, portraying alternatives (if any) as inferior. The conversation that resolved the challenging surgical consultation (above) is a good example of working jointly to identify alternative possibilities.
가능성 판단과 관련된 문제
Issues related to judging possibilities
가능성이 발생하면 그 중에서 [판단하는 방법(예: 옵션 비교, 협상, 문제 해결, 통찰력 개발)을 수립]해야 합니다. 이상적으로는 환자와 의사가 함께 이 작업을 수행합니다. 이 비디오에서 의사가 환자와 적극적으로 협력하여 서로의 관심사를 해결하는 경우는 드물었습니다. 오히려 거의 항상 의사가 진료실에 들어가기 전에 결정을 내린 다음 환자가 이 계획에 동의하도록 설득하는 데 시간을 소비하는 것처럼 보였습니다. 이러한 계획은 대개 합리적이며 가이드라인에 부합하는 것이었지만 환자의 의견은 반영되지 않았습니다. 한 조사자는 '추론은 임상의의 머릿속이 아닌 교과서에서 일어났다'고 기록했습니다.
As possibilities arise, methods of judging among them (e.g. weighing options, negotiating, problem solving, developing insight) should be established. Ideally, patients and physicians do this together. In these videos, physicians infrequently worked actively with patients to solve a problem of mutual concern. Rather, it nearly always appeared that the physician had made the decision before walking into the room, and then spent time convincing the patient to agree with this plan. Such plans were usually well-reasoned and in alignment with guidelines, but devoid of patient input. As one investigator documented, ‘Reasoning happened in the textbook (not in the clinician’s head).’
우리는 치료 목표(예: 의사가 당뇨병, 고지혈증 또는 고혈압에 대한 가이드라인 기반 치료 목표에 대해 논의하지 않고 선택)와 치료 접근 방식(예: 약물, 약물 용량, 수술 상담)에 대한 대화에서 이러한 단점을 인식했습니다. 또한 의사가 섬유근육통 진단에 대한 환자의 불확실성을 무시하고 치료 계획의 윤곽을 미리 제시하는 경우와 같이 진료 흐름에서도 이러한 문제를 확인할 수 있었습니다. 이러한 행동은 거의 항상 의사와 환자 사이에 마찰을 일으켰고, 의사는 자신의 해결책이 좋다고 환자를 설득하려고 노력했습니다.
We recognized this shortcoming in conversations about both goals of treatment (e.g. the physician selecting [rather than discussing] guideline-based treatment targets for diabetes, hyperlipidemia, or hypertension) and treatment approach (e.g. drug, drug dose, surgical consultation). We also saw this in the encounter flow, as when the physician ignored the patient’s uncertainty with her diagnosis of fibromyalgia and forged ahead to outline a care plan. Such actions nearly always resulted in friction between physician and patient, with the physician trying to convince the patient that their solution was good.
Issues related to developing care plans
공유된 심의 프로세스는 문제에 대응하고 지적, 실제적, 정서적으로 [합당한 치료 계획을 수립]하기 위해 노력합니다. 지적, 실용적, 정서적 일관성을 갖춘 대응 계획의 예는 거의 없었습니다. 대신 일반적으로 치료 계획 내에서 [단절] 또는 [잔류 갈등]이 관찰되었습니다.
- 갑상선암 동영상은 문제의 심각성(상담의 시급성이 낮음)과 제안된 해결책의 영향(환자의 삶에 큰 지장을 초래함) 사이의 갈등을 보여줍니다.
- 두 섬유근육통 동영상의 치료 계획은 체계적이지 않고 불완전하며 환자의 경험과 단절되어 있어 환자가 실질적인 다음 단계에 대해 당황하고 좌절하며 방향을 잃게 만들었습니다.
- 다른 영상에서는 환자의 질문에 대한 답변이 없거나 치료 목표가 강요될 때 지적 단절이 빈번하게 발생하고, 환자의 우려를 무시하거나 자율성을 무시할 때 감정적 갈등이 발생하는 것을 볼 수 있었습니다.
The shared deliberative process works towards a care plan that responds to the problem and makes sense intellectually, practically, and emotionally. We saw few examples of responsive plans with intellectual, practical, and emotional coherence. Instead, we typically observed a disconnect or residual conflict within the care plan.
- The thyroid cancer video illustrates a conflict between the severity of the problem (low urgency for consultation) and the impact of the proposed solution (large disruption of the patient’s life).
- The care plans in both fibromyalgia videos were poorly organized, incomplete, and disconnected from the patient’s experience, leaving the patient perplexed, frustrated, and disoriented regarding practical next steps.
- In other videos we saw frequent intellectual disconnects when patient questions remained unanswered or treatment targets were imposed, and emotional conflicts when patient concerns were brushed aside or autonomy had been disregarded.
또한 [명시적인 결정이 없는 경우]도 많이 보았습니다. 의사는 일반적으로 여러 가지 제안을 하고 선호하는 옵션을 언급하기도 했지만, 환자에게 이 계획에 대한 동의를 요청하거나 받지 않았습니다. 이러한 실패는 단순히 의사 소통 능력이 부족해서일 수도 있지만, 일부 영상에서는 의사가 환자의 동의를 얻지 못했다는 인식 때문에 의도적으로 동의를 구하지 않는 것처럼 보이기도 했습니다. 그 외에는 최선의 접근 방식에 대한 불확실성 때문인 경우가 더 많았습니다.
Additionally, we saw many instances in which there was no explicit decision. The physician had typically made a number of suggestions, and might have even stated a preferred option, but never asked for or received agreement for this plan from the patient. Although such failures could reflect merely poor communication skills, in some videos the physician seemed to deliberately avoid asking for agreement, due perhaps to awareness that the conversation had failed to garner the patient’s buy-in. Less often, vacillation seemed due to uncertainty in the best approach.
환자-임상의 상호 작용 및 관리 추론 통합(3단계)
Integrating patient-clinician interactions and management reasoning (stage 3)
마지막으로, 관리 추론에서 커뮤니케이션과 환자-임상의 상호작용의 역할을 이해하고자 하는 본 연구의 목표를 달성하기 위해, 이전에 확인된 관리 추론의 12가지 특징(Cook 외. 2022b)과 두 SDM 모델 간의 상호 영향을 체계적으로 고려함으로써 2단계 결과와 관리 추론의 틀을 통합했습니다(부록 3에서는 관찰 및 분석에 대한 자세한 내용(보충 자료)을 확인할 수 있습니다). 이 분석에서 얻은 수많은 인사이트(표 3) 중 주목할 만한 결과는 다음과 같습니다:
Finally, to achieve our study’s goal of understanding the role of communication and patient-clinician interaction in management reasoning, we integrated stage 2 findings and the framework of management reasoning by systematically contemplating the reciprocal implications between 12 previously-identified features of management reasoning (Cook et al. 2022b) and the two SDM models; Appendix 3 details our observations and analyses (Supplementary Material). Among the numerous insights from this analysis (Table 3), notable findings include:
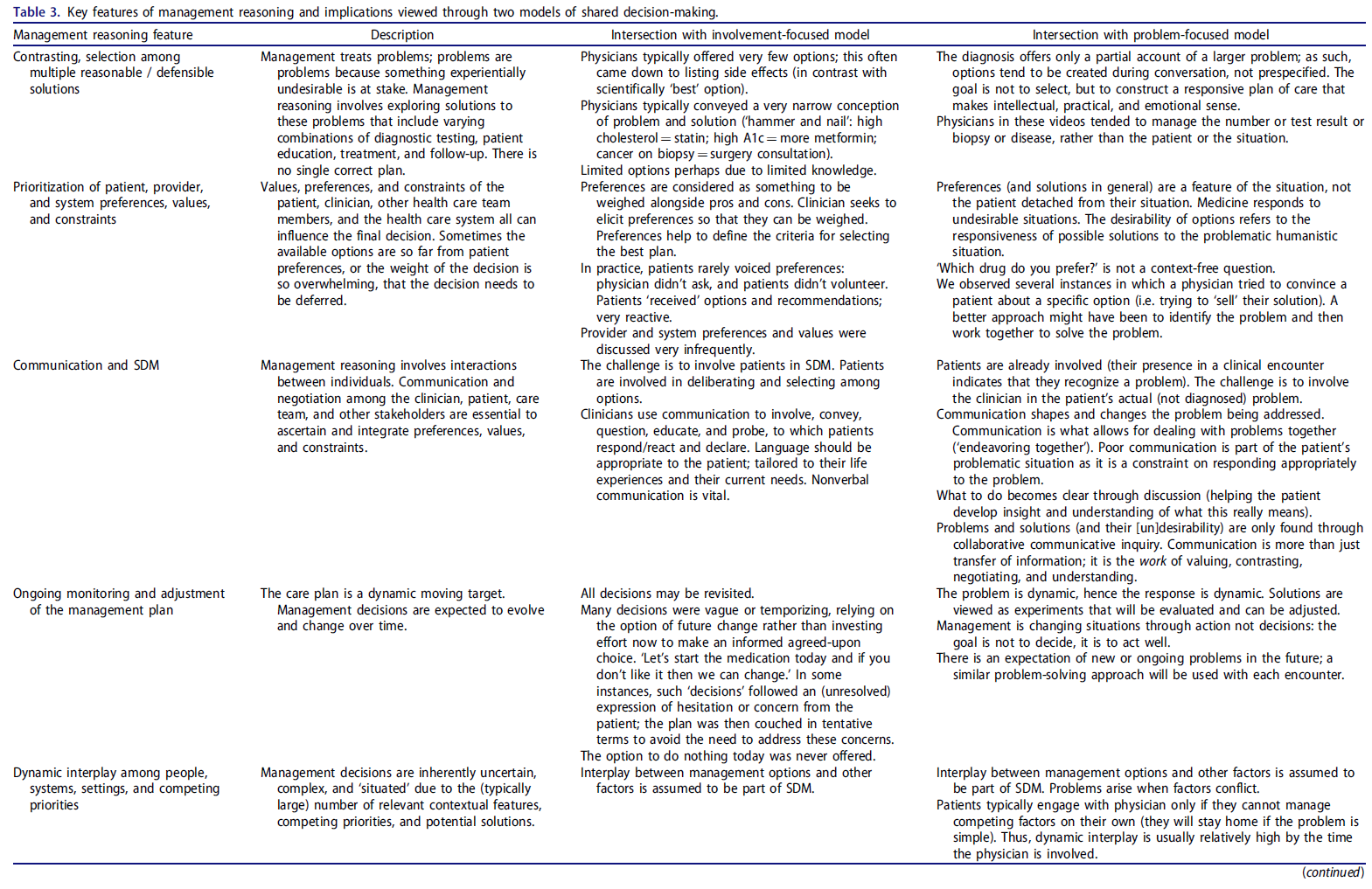
- [문제 중심 모델]에서 선호도는 환자가 아닌 [상황의 특징]입니다. 문제가 있는 상황은 바람직하지 않으며, 가능한 해결책은 다양한 제약 조건 내에서 인간의 범위 내에서 상황에 대응하는 성공 여부에 따라 바람직(선호) 또는 그렇지 않은 것으로 결정됩니다. [관리 추론]은 문제 상황에 대한 바람직한 해결책을 모색합니다.
- In the problem-focused model, preferences are a feature of the situation not the patient. Problematic situations are undesirable, and possible solutions are desirable (preferred) or otherwise according to their success in responding to the human scope of the situation within various constraints. Management reasoning seeks a preferred solution to a problematic situation.
- [환자, 의사, 상황적 제약 사이의 역동적인 상호 작용]은 거의 모든 대면 진료에서 보통 또는 높은 수준입니다. 문제가 쉽게 파악되거나 쉽게 해결될 수 있었다면 환자는 집에 머물렀을 것입니다. 임상의는 [일이 예상대로 진행되지 않을 때 개입]합니다.
- The dynamic interplay among patient, physician, and situational constraints is moderate or high for virtually all face-to-face encounters. If the problem were readily characterized or easily resolved, the patient would have stayed home. Clinicians get involved when things do not go as expected.
- 의사들은 [충분한 정보를 바탕으로 상호 합의]하여 선택하기보다는 [잠정적이거나 임시적인 용어('일단 약을 시작하고 마음에 들지 않으면 바꾸면 된다')로 '결정']을 내리는 경우가 많습니다. 물론 '관리 계획의 지속적인 모니터링과 조정'은 관리 추론의 핵심 기능이지만(Cook et al., 2019), 의사들은 종종 [질문을 미루고, 우려를 제쳐두고, 대립을 피하기] 위해 이러한 [전제에 지나치게 의존]하는 것처럼 보였습니다('캔을 걷어차 버리자').
- Physicians often couched “decisions” in tentative or temporary terms (‘Let’s start the medication and if you don’t like it then we can change’) rather than mutually agreeing upon a well-informed choice. Of course, ‘ongoing monitoring and adjustment of the management plan’ is a key feature of management reasoning (Cook et al., 2019); but physicians often seemed to rely excessively on this premise to defer questions, brush aside concerns, and avoid confrontation (‘kick the can down the road’).
- [언어]는 [미묘하지만 중요한 방식으로 문제를 형성하고 변화]시킬 수 있습니다. 예를 들어, 고지혈증을 'LDL을 낮춰야 한다' 또는 '심장마비 위험을 줄여야 한다'는 식으로 표현하면 문제의 성격과 해결책을 협상하는 방식이 크게 달라질 수 있습니다.
- Language can shape and change the problem in subtle but important ways. For example, framing hyperlipidemia as needing to ‘lower your LDL’ or ‘reduce your risk of a heart attack’ could lead to dramatically different problem characterizations and solution negotiations.
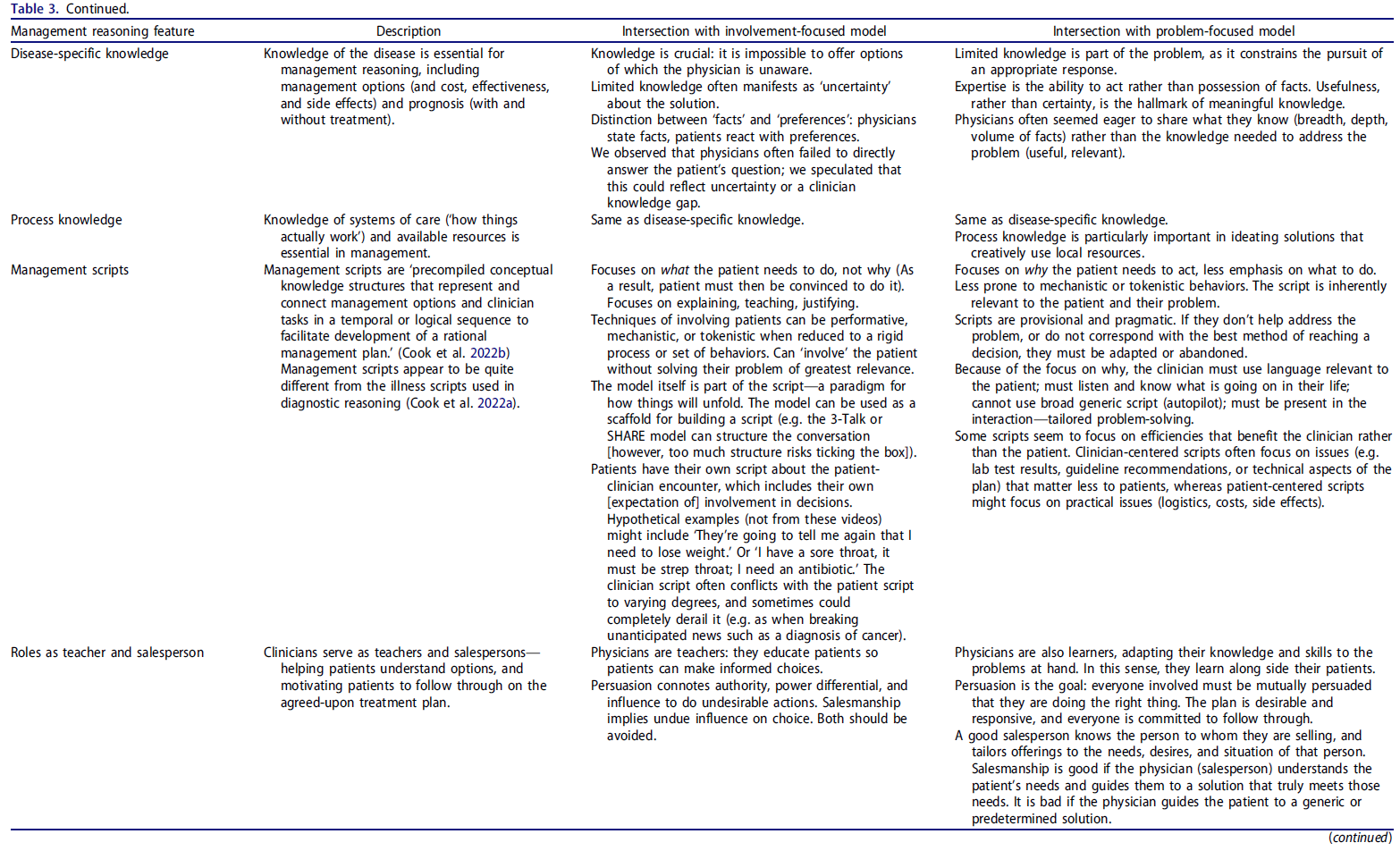
- 우리는 이전에 정의한 관리 스크립트('합리적인 관리 계획의 개발을 용이하게 하기 위해 관리 옵션과 임상의 업무를 시간적 또는 논리적 순서로 표현하고 연결하는 사전 편집된 개념적 지식 구조'(Cook et al., 2022b))와 관련된 [두 가지 새로운 인사이트]에 주목하고 나중에 자세히 설명했습니다(Cook et al., 2022a).
- We noted 2 novel insights related to management scripts, which we previously defined (‘precompiled conceptual knowledge structures that represent and connect management options and clinician tasks in a temporal or logical sequence to facilitate development of a rational management plan’ (Cook et al., 2022b)) and later elaborated in detail (Cook et al., 2022a).
- 첫째, 의사의 [관리 스크립트]는 [의사의 요구](예: 효율적인 만남 또는 신속한 결정 촉진)와 [환자의 요구](문제 이해, 질문에 대한 답변, 개별화된 결정 지원)의 [우선순위]에 따라 연속체를 따라 달라집니다.
- First, physicians’ management scripts vary along a continuum in prioritizing physician needs (e.g. promoting an efficient encounter or expedited decision) vs patient needs (understanding problems, answering questions, supporting individualized decisions).
- 둘째, [환자]는 의사와의 상호작용을 안내하는 [자신만의 인지적 스크립트]를 가지고 있습니다. 환자와 의사의 스크립트는 모두 유사한 범주(문제, 옵션, 선호도, 교육 요구, 대인관계, 진료 흐름(Cook et al., 2022a))로 구성될 가능성이 높지만, 각 범주에 대해 인스턴스화된 세부 사항은 상당히 다를 수 있습니다.
- Second, patients have their own cognitive script that guides their interactions with the physician. Both patient and physician scripts likely comprise similar categories (problems, options, preferences, education needs, interpersonal interactions, and encounter flow (Cook et al., 2022a)); but the details instantiated for each category could differ substantially.
- 문제를 해결할 때 의사는 [일반적으로 이미 알고 있는 지식에 의존]하게 되는데, 이 지식이 당면한 문제를 해결하는 데 항상 적절하거나 충분하지 않을 수 있습니다. 부주의적이든(모르는 것을 알기 어렵기 때문) 의도적이든(지식 격차를 인정하거나 추가 정보를 찾는 것을 피하기 위해서) 이러한 지식 격차는 문제 중심 SDM을 방해합니다.
- When grappling with a problem, physicians will typically rely on what they already know—which may not always be relevant or sufficient to resolve the problem at hand. Whether inadvertent (it is difficult to know what one does not know) or conscious (to avoid admitting a knowledge gap or seeking additional information), such knowledge gaps will interfere with problem-focused SDM.
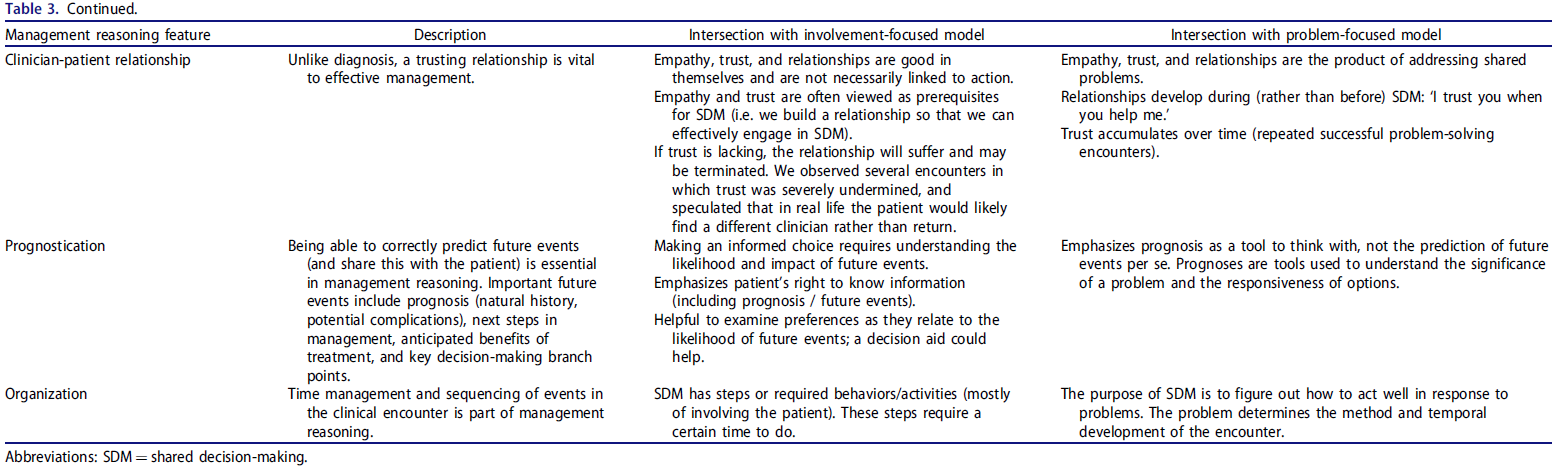
- 환자-의사 관계의 특성은 모델에 따라 다릅니다.
- [참여 중심 모델]에서는 공감과 신뢰의 효과적인 관계가 효과적인 SDM의 매개체(전구체)입니다. 이와 대조적으로
- [문제 중심 모델]에서는 효과적인 관계가 SDM의 산물입니다(즉, 의사와 환자가 문제를 해결하기 위해 함께 노력하면서 관계가 발전합니다).
- The nature of patient-physician relationships differs by model.
- In the involvement-focused model an effective relationship of empathy and trust is a mediator of (precursor to) effective SDM. By contrast,
- in the problem-focused model an effective relationship is the product of SDM (i.e. the relationship develops as the physician and patient work together to solve problems).
- [설득]도 모델에 따라 다르게 볼 수 있습니다.
- [참여 중심 모델]에서는 설득은 [나쁜 것으로 간주]된다. 권위, 권력 차이, 바람직하지 않은 행동을 하도록 영향력을 행사하는 것이고, 이러한 위험 때문에 환자를 의사 결정에 참여시켜 자율성을 보존해야 한다고 생각합니다.
- [문제 중심 모델]에서 설득은 좋은 것이고, 사실상 목표이다. 모든 이해관계자가 이 상황에서 최선의 행동 방침을 상호 설득할 때까지 함께 노력하는 것이지만, 과도한 권력 기반 설득은 이 방법을 왜곡하는 것입니다.
- Persuasion can also be viewed differently, depending on the model.
- In the involvement-focused model, persuasion is bad, connoting authority, power differential, and influence to do (undesirable) actions; this risk drives the need to preserve autonomy by involving patients in decision-making.
- In the problem-focused model, persuasion is good—indeed, the goal: stakeholders work together until all are mutually persuaded that a course of action is best in this circumstance; undue power-based persuasion is a corruption of this method.
제안된 모범 사례(4단계)
Proposed best practices (stage 4)
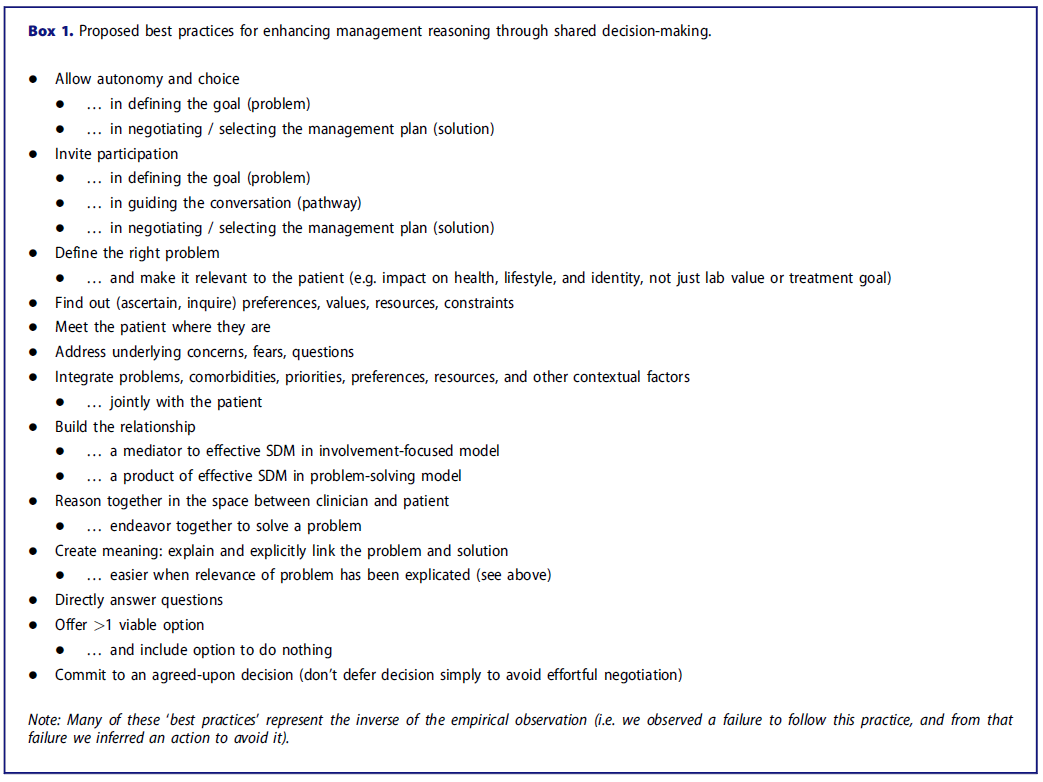
이러한 결과를 바탕으로 우리는 관리 추론에서 환자-임상의 상호작용에 대한 몇 가지 잠정적인 모범 사례를 확인했으며, 이는 상자 1에 나열되어 있습니다.
Drawing on these findings we identified several tentative best practices for patient-clinician interactions in management reasoning, listed in Box 1.
토론
Discussion
이 연구는 관리 추론이 전적으로 [임상의의 머릿속]이 아닌 [개인 사이의 공간]에서 발생한다는 이전 연구(Cook 외. 2022b)의 관찰을 더욱 입증합니다. 두 가지 다른 SDM 렌즈를 통해 시뮬레이션된 환자-임상의 만남을 분석하여 관리 추론에서 의사소통과 환자-임상의 상호 작용의 상호 보완적인 측면을 조명했습니다. SDM의 [참여 중심 모델]은 환자의 자율성을 보호하고, 정보를 명확하게 교환하며, 최종 결정이 환자의 선호도에 부합하도록 관리 추론에 환자를 참여시키는 것이 중요하다는 점을 강조했습니다. [문제 중심 모델]은 공동의 노력에서 소통과 상호 작용이 어떻게 올바른 의사 결정을 촉진하는 데 도움이 되는지 밝혀냈습니다.
This study further probes the observation from an earlier study (Cook et al. 2022b) that management reasoning occurs in the space between individuals and not entirely in the clinician’s head. Analysis of simulated patient-clinician encounters through 2 distinct SDM lenses illuminated complementary aspects of communication and patient-clinician interaction in management reasoning. The involvement-focused model of SDM highlighted the importance of involving patients in management reasoning so that patient autonomy is preserved, information is clearly exchanged, and final decisions align with the patient’s preferences. The problem-focused model revealed how communication and interaction in a shared endeavor serve to facilitate well-formed decisions.
이러한 모델을 함께 사용하면 [커뮤니케이션 실패에 대한 순진한(분석 1단계) 관찰을 이해]하는 데 도움이 됩니다. 예를 들어, 의사가 환자를 만나지 못했거나 선택권을 제공하지 않은 경우, 모델에 따라 다른 이유로 인해 특히 중요하다는 것을 이제 알 수 있습니다.
- [참여 중심 관점]에서 볼 때, 이는
- 환자와 임상의 사이의 거리를 악화시키고,
- 종종 의사소통을 차단하고,
- 불신을 키우고,
- 자율성을 무시하고,
- 만남을 의지의 대결로 바꾸고,
- 환자를 복종적인 역할로 강요하고,
- 지속적인 관리에 필요한 파트너십을 해치고,
- 환자가 임상의의 조언을 따라야 한다는 확신을 갖지 못하게 만들었습니다.
- [문제 중심의 관점]에서 볼 때, 이와 같은 관찰된 실패는 임상의가 다음과 같은 것을 의미합니다.
- 문제가 있는 곳에서 환자를 직접 만나지 않았기 때문에 문제의 중요성/의미에 대해 자세히 설명하거나 해결하지 못했습니다,
- 문제를 해결하기 위해 환자-임상의 팀의 잠재력을 충분히 개발하지 못했습니다,
- 임상의가 선험적으로 결정한 것보다 상황에 더 잘 대응할 수 있는 심의 옵션을 제시하지 않았습니다,
- 종종 만남에서 모든 심의를 제거했습니다 (옵션이 논의되지 않을 때 얼마나 많은 '추론'또는 '의사 결정'이 발생하는지에 대한 의문을 제기합니다).
- 불확실한 가치의 치료 계획을 초래했습니다.
- 문제가 있는 곳에서 환자를 직접 만나지 않았기 때문에 문제의 중요성/의미에 대해 자세히 설명하거나 해결하지 못했습니다,
Together, these models help make sense of the naïve (analysis stage 1) observations of communicative failures. For instance, we now recognize that when physicians failed to meet the patient where they were or offered no choices, this was especially significant—for reasons that differed depending on the model.
- From the involvement-focused perspective this
- exacerbated the distance between patient and clinicians, and
- often shut down communication,
- bred mistrust,
- disrespected autonomy,
- turned the encounter into a contest of wills,
- forced the patient into a subservient role,
- harmed the partnership needed for ongoing management, and
- left the patient unconvinced that they should follow the clinician’s advice.
- From the problem-focused perspective these same observed failures meant that the clinician
- didn’t meet the patient where their problem lay (and hence the full significance/meaning of the problem was never elaborated or addressed),
- didn’t develop the full potential of the patient-clinician team to address the problem,
- didn’t bring forward options for deliberation that might better respond to the situation than those determined by the clinician a priori,
- often removed all deliberation from the encounter (raising the question of how much ‘reasoning’ or ‘decision-making’ occurs when no options are discussed), and
- resulted in a care plan of uncertain value.
제한 사항
Limitations
이 연구에는 한계가 있습니다.
- 첫째, 우리가 관찰한 동영상은 실제와 같이 보이도록 의도되었지만 실제 임상의와 환자 간의 상호작용은 하나도 없었고 4편은 대본으로 제작되었습니다. 이는 동영상의 맥락(성인 외래 환자 일차 진료만), 수행 수준(절반은 의도적으로 열악한 것으로 선택되었고 모범적인 것은 없음), 원래 목적(평가자 교육 연구(Cook 외. 2009; Cook 및 Beckman, 2009)) 및 총 수와 함께 임상적 다양성을 종합적으로 제한했습니다. 현재의 결론이 적절히 뒷받침된다고 생각하지만, 다른 관점(예: 대본에 없는, 다른 임상 상황, 다른 수준의 임상의 수행 또는 교육)을 제공하는 다른 사례에 대한 분석을 통해 추가적인 인사이트가 나올 수 있을 것으로 예상합니다. 일부 독자는 다른 목적으로 제작된 동영상의 용도 변경을 무시할 수도 있지만, 이미 언급한 맥락적 제약에 비추어 볼 때 이는 사소한 문제라고 생각합니다.
- 둘째, 많은 추론은 실패한 사례나 바람직한 행동을 취하지 않은 채 방치된 사례에 대한 관찰을 바탕으로 이루어졌으며, 이러한 추론은 당연히 관찰자의 관점에 따라 달라질 수 있습니다.
- 셋째, 본 연구의 저자들은 기본 개념 프레임워크의 개발자(Cook 외. 2018; Hargraves 외. 2019)이자 관찰자 및 분석가로서 본 연구의 관찰자 및 분석가로서 참여했으며, 이는 강점이지만 확증 편향의 위험도 있습니다. 또 다른 강점으로는 이러한 동영상을 사용하여 이전에 발표한 연구를 확장하면서
- (a) SDM 및 정성적 데이터 분석에 상당한 전문성을 갖춘 새로운 연구자(IGH)를 팀에 추가하고,
- (b) 모든 동영상을 개별적으로 또는 그룹으로 재검토하여 풍부하고 새로운 데이터를 수집하고,
- (c) 상호 보완적인 개념적 렌즈를 사용하여 이러한 데이터를 분석하고,
- (d) 이러한 분석을 지속하여 SDM과 경영 추론을 통찰력 있게 통합하고 여러 모범 사례를 식별했다는 점을 들 수 있습니다.
- 요컨대, 이러한 강점은 제안된 결론을 충분히 뒷받침하지만, 이러한 한계는 추가적인 인사이트를 발견해야 함을 시사합니다.
This study has limitations.
- First, the videos we observed were intended to be realistic, but none were actual clinician-patient interactions and 4 were scripted. This, together with the videos’ context (only adult outpatient primary care), performance levels (half were intentionally selected as poor, and none were exemplary), original purpose (a study of rater training (Cook et al. 2009; Cook and Beckman, 2009)), and total number, collectively constrained the clinical variation. While we believe the present conclusions are appropriately supported, we surmise that additional insights could emerge from analysis of other encounters offering alternative perspectives (e.g. unscripted, different clinical contexts, or different levels of clinician performance or training). Some readers might also discount the repurposing of videos created for another purpose, however we believe this constitutes a minor concern relative to the contextual constraints already noted.
- Second, many inferences were based on observations of failures or presumably desirable actions left undone; such inferences naturally depend on the perspectives of those observing.
- Third, we authors were both the developers of the guiding conceptual frameworks (Cook et al. 2018; Hargraves et al. 2019) and the observers and analyzers in this study; while this is a strength, there is some risk of confirmation bias. Additional strengths include that as we extended our previously-published work using these videos, we
- (a) added to our team a new investigator (IGH) with substantial expertise in SDM and qualitative data analysis;
- (b) collected abundant, rich new data by re-reviewing all videos both independently and as a group;
- (c) analyzed these data using complementary conceptual lenses; and
- (d) continued this analysis to a achieve an insightful integration of SDM with management reasoning and identify several best practices.
- In short, these strengths provide ample support for the conclusions proposed, but these limitations suggest that additional insights remain to be discovered.
시사점
Implications
이번 연구 결과는 교육, 임상 실무 및 향후 연구에 중요한 [시사점]을 제공합니다. 가장 중요한 것은 관리 추론이 임상의의 머릿속이 아닌 [개인 간의 공간에서 일어나는 의도적인 상호 작용]을 포함한다는 점입니다. [환자와 임상의]는 [서로 다른 관점, 지식 기반, 경험, 우선순위에서 '추론'을 하지만, 한 팀으로서 '추론']을 해야 합니다. 이는 관리 추론을 가르치고 평가하는 방식에 중요한 시사점을 줍니다. 관리 추론의
- [일부 요소]는 [임상의 내부]에서 발생하는 것처럼 가르치고 평가할 수 있지만,
- [환자와 임상의의 상호 작용]도 가르치고 평가해야 하며,
- [어느 시점에는 전체 전체를 종합]해야 합니다.
Our findings have important implications for education, clinical practice, and future research. Most importantly, we affirm that management reasoning involves a deliberative interaction occurring in the space between individuals and not within a clinician’s mind. Both the patient and clinician are ‘reasoning’—from different perspectives, knowledge bases, experiences, and priorities, but hopefully as a team. This has notable implications for how we teach and assess management reasoning.
- While some elements of management reasoning can be taught and assessed as though occurring within the clinician,
- the patient-clinician interaction must also be taught and assessed;
- and at some point the entire whole must be assembled.
관리 추론과 SDM은 모두 [상호 합의된 공유 문제], 예를 들어 진단 라벨이나 목표치를 벗어난 검사실 수치보다는 [생명이나 건강에 대한 상호 위협에 초점]을 맞출 때 가장 효과적입니다. [공유된 문제]는
- 공동의 문제 해결('함께 노력하기')을 유도하고,
- 사회적 조정과 협력(의사소통적 행동)을 촉진하며,
- 갈등과 과도한 설득의 필요성을 피할 수 있습니다.
이러한 관점에서 볼 때 관리 추론은 문제 해결을 위해 고심하는 것입니다.
Management reasoning and SDM both work best when focused on a shared, mutually-agreed problem—a mutual threat to life or health rather than, for example, a diagnostic label or off-target lab value. A shared problem
- engenders joint problem-solving (‘endeavoring together’),
- promotes social coordination and cooperation (communicative action (Bohman and Rehg 2017)), and
- avoids conflict and the need for undue persuasion.
Viewed this way, management reasoning is deliberating to resolve the problem.
우리는 임상의와 환자라는 [두 가지 관리 스크립트]가 작용한다는 새로운 통찰력을 강조합니다. 우리는 이전에 [임상의의 관리 스크립트]에 대해 자세히 설명했습니다. (Cook 외. 2022a) [관리 추론의 환자 측면]은 지금까지 무시되어 왔습니다. 또한 일부 스크립트는 주로 임상의에게 도움이 되는 반면(즉, 진료 효율 개선), 다른 스크립트는 환자의 대응 결정을 돕는 데 더 중점을 둡니다(연속선상에 있음). 대부분의 스크립트는 의식적인 생각 없이 자발적으로 개발되며(Custers 2015), [환자 중심 스크립트를 촉진하는 방법]은 아직 불분명합니다. SDM과 관련된 관리 스크립트에 대한 추가 연구가 필요합니다.
We underscore the novel insight that there are two management scripts in play—the clinician’s and the patient’s. We previously elaborated on the clinician’s management script; (Cook et al. 2022a) the patient’s side of management reasoning has thus-far been neglected. We also note that some scripts primarily help the clinician (i.e. to improve encounter efficiency), while others (along a continuum) are more directed at helping the patient make a responsive decision. Most scripts develop spontaneously (Custers 2015)—without conscious thought—and it remains unclear how to promote patient-centered scripts. Further research on management scripts as they relate to SDM is needed.
특히 SDM과 관련된 관리 추론에 대한 연구가 초기 단계에 있다는 점을 강조합니다. 위에서 언급한 것 외에도 이 연구에서 제기된 중요한 질문은 다음과 같습니다: 공유된 숙고 과정으로서 관리 추론을 어떻게 평가할 수 있는가? (임상 진단 추론을 평가하기 위한 수많은 도구가 존재하지만, 관리 추론에 초점을 맞춘 도구는 없습니다(Daniel 외. 2019). 마찬가지로, [참여 중심의 SDM]을 평가하기 위한 수많은 도구가 존재하지만, [대응적 문제 해결]에 초점을 맞춘 도구는 없습니다(Hartasanchez 외. 2021)). '좋은' 의학적 결정이란 무엇인가요? (보편적인 정의는 없으며, 환자 대 임상의, 임상 지침 대 실제 경험, 전문의 대 일차 진료, 참여 중심 SDM 대 문제 중심 SDM 등 다양한 관점에 따라 답이 달라지며, 이는 교육 및 평가에 중요한 영향을 미칩니다).
We emphasize the nascent state of research in management reasoning, especially in relation to SDM. Important questions emerging from this study, beyond those noted above, include: How can we assess management reasoning as a shared deliberative process? (Numerous tools exist to assess clinical diagnostic reasoning; none focus on management reasoning (Daniel et al. 2019). Similarly, numerous tools exist to assess involvement-focused SDM; none focus on responsive problem-solving (Hartasanchez et al. 2021)). What is a ‘good’ medical decision? (There is no universal definition; the answer varies for different perspectives—patient vs clinician, clinical guideline vs practical experience, specialist vs primary care, involvement-focused SDM vs problem-focused SDM, etc.—with important implications for training and assessment).
마지막으로, 연구 결과에 따르면 [좋은 의사소통]은 [단순히 좋은 매너]가 아니며, [명목상 환자를 '참여'시키는 암기식 행동]이 최선의 결정에 도달하는 데 적합하지도 않습니다. 의사소통에는 목적이 있으며, 대화가 의사소통의 목적과 동떨어져 있거나 관련된 사람들이 서로 다른 목표를 추구한다면 추론과 의사 결정에 상당한 장애가 발생할 것입니다(Hargraves 외. 2019; Bohman and Rehg 2017). 임상의는 [환자와 임상의가 함께 할 수 있는 의사소통]이 무엇인지 인식하고, 진료 목적에 따른 잠재력을 깨닫고, 환자별 및 상황별 요구에 민첩하게 부응할 수 있도록 의사소통의 내용과 방법을 조정해야 합니다.
Finally, our findings suggest that good communication is not simply good manners, nor that rote behaviors to nominally ‘involve’ patients are adequate for reaching the best decision. Communication serves a purpose, and if talking is detached from the purpose of communication, or if those involved seek disparate goals, then reasoning and decision-making will be significantly impaired (Hargraves et al. 2019; Bohman and Rehg 2017). Clinicians must (learn to) recognize what communication enables patients and clinicians to do together, realize that potential in achieving an encounter-specific purpose, and adjust what and how they communicate to nimbly meet patient-specific and situation-specific demands.
Management reasoning and patient-clinician interactions: Insights from shared decision-making and simulated outpatient encounters
PMID: 36763491
Abstract
Purpose: To expand understanding of patient-clinician interactions in management reasoning.
Methods: We reviewed 10 videos of simulated patient-clinician encounters to identify instances of problematic and successful communication, then reviewed the videos again through the lens of two models of shared decision-making (SDM): an 'involvement-focused' model and a 'problem-focused' model. Using constant comparative qualitative analysis we explored the connections between these patient-clinician interactions and management reasoning.
Results: Problems in patient-clinician interactions included failures to: encourage patient autonomy; invite the patient's involvement in decision-making; convey the health impact of the problem; explore and address concerns and questions; explore the context of decision-making (including patient preferences); meet the patient where they are; integrate situational preferences and priorities; offer >1 viable option; work with the patient to solve a problem of mutual concern; explicitly agree to a final care plan; and build the patient-clinician relationship. Clinicians' 'management scripts' varied along a continuum of prioritizing clinician vs patient needs. Patients also have their own cognitive scripts that guide their interactions with clinicians. The involvement-focused and problem-focused SDM models illuminated distinct, complementary issues.
Conclusions: Management reasoning is a deliberative interaction occurring in the space between individuals. Juxtaposing management reasoning alongside SDM generated numerous insights.
Keywords: Decision Making; clinical decision-making; communication; diagnostic reasoning; shared; therapeutic reasoning.