관리추론: 핵심 특징과 개념 모델의 실증적 결정(Acad Med, 2023)
Management Reasoning: Empirical Determination of Key Features and a Conceptual Model
David A. Cook, MD, MHPE, Christopher R. Stephenson, MD, Larry D. Gruppen, PhD, and Steven J. Durning, MD, PhD
[관리 추론]은 임상 진료와 의학교육에서 매우 중요하지만 잘 연구되지 않은 현상입니다. 1,2 [진단 추론]과 관련된 임상 추론 프로세스는 상당한 연구를 통해 밝혀졌습니다. 3-6 반면, [환자 관리 결정]에 대한 추론과 관련된 프로세스에 대해서는 알려진 바가 훨씬 적습니다. 6,7 우리는 최근 관리 추론에 대한 개념적 프레임워크를 발표했습니다. 1,2 이 보고서에서 우리는 관리 추론을 "임상의가 임상 정보(병력, 검사 소견, 검사 결과), 선호도, 의학 지식, 맥락(상황) 요소를 통합하여 치료, 추가 검사, 후속 방문, 제한된 자원의 할당 등 개별 환자의 관리에 관한 결정을 내리는 인지적 과정"1으로 정의하고 5가지 주요 특징을 제안했습니다:
- 합리적이고 방어 가능한 여러 솔루션 간의 비교 및 선택,
- 환자, 임상의, 시스템 선호도, 제약, 가치의 우선순위 지정,
- 의사소통 및 공유된 의사 결정,
- 관리 계획의 지속적인 모니터링 및 조정,
- 사람, 시스템, 환경, 경쟁 우선순위 간의 역동적인 상호 작용(표 1).
우리 모델을 기반으로 최근 관리 스크립트의 개념을 설명하는 연구도 있습니다. 8
Management reasoning 1 is a critical yet understudied phenomenon in clinical practice and medical education. 1,2 Substantial research has illuminated the clinical reasoning processes involved in diagnostic reasoning. 3–6 By contrast, far less is known about the processes involved in reasoning about patient management decisions. 6,7 We recently published a conceptual framework for management reasoning. 1,2 In those reports, we defined management reasoning as “the cognitive processes by which clinicians integrate clinical information (history, exam findings, and test results), preferences, medical knowledge, and contextual (situational) factors to make decisions about the management of an individual patient, including decisions about treatment, further testing, follow-up visits, and allocation of limited resources,” 1 and proposed 5 key features:
- contrasting and selection among multiple reasonable and defensible solutions;
- prioritization of patient, clinician, and system preferences, constraints, and values;
- communication and shared decision making;
- ongoing monitoring and adjustment of the management plan; and
- dynamic interplay among people, systems, settings, and competing priorities (Table 1).
Others, building on our model, have recently described the concept of management scripts. 8

그러나 [관리 추론]에 대한 경험적 연구는 제한적입니다. 연구들은 종종 치료 결정을 결과로 사용하지만, 그러한 결정의 근간이 되는 관리 추론 프로세스에 초점을 맞춘 경우는 거의 없습니다. 9-11 한 그룹에서는 12개의 임상 추론 과제를 확인한 후 13개 24개의 임상 추론 과제를 확인했으며, 이 중 11개는 관리를 용이하게 합니다. [관리 추론의 현상]과 [진단 추론과의 차이점]을 더 명확하게 이해하면 이 분야의 미래 연구를 위한 발판을 마련하고 교육에 대한 잠재적 시사점을 파악할 수 있습니다. 이 연구에서는 귀납적(경험적)으로 시뮬레이션된 외래 환자-임상의사 면담에서 나타난 관리 추론의 주요 특징을 파악하고 관리 추론 과정을 설명하는 모델을 구축하고자 했습니다.
However, empirical research on management reasoning is limited. Studies often use treatment decisions as an outcome but only rarely have focused on the management reasoning processes that underlie such decisions. 9–11 One group identified 12 and subsequently confirmed 13 24 clinical reasoning tasks, of which 11 facilitate management. Greater clarity in understanding the phenomenon of management reasoning, and how it differs from diagnostic reasoning, will set the stage for future research in this field and identify potential implications for education. In this study, we sought to inductively (empirically) identify key features of management reasoning as manifested in simulated outpatient clinician–patient encounters and construct a model that describes the management reasoning process.
방법
Method
우리는 관리 추론의 특징을 파악하기 위해 모의 외래 환자 임상의와 환자 간의 만남을 담은 10개의 비디오 클립을 검토했습니다.
We reviewed 10 video clips of simulated outpatient clinician–patient encounters, to identify features of management reasoning.
비디오 클립
Video clips
비디오 클립은 이전에 발표된 [평가자 교육 연구]에서 사용되었습니다. 14,15
- 각 비디오는 레지던트 의사가 환자에게 의학적 상태(예: 고지혈증, 섬유근육통, 갑상선암)에 대해 상담하는 장면을 보여줍니다. 이 동영상은 레지던트의 실력이 미흡한 경우부터 우수한 경우까지 다양한 모습을 보여주기 위해 기획되었습니다.
- [6개의 비디오]는 저자 D.A.C.가 개발했으며, 마지막 해 또는 내과 전공의와 커뮤니티 풀의 표준화된 환자 간의 즉흥적인 대화로 구성되었습니다.
- 의사는 자신의 수행 능력(우수 또는 열악)을 변화시키도록 지시받았고, 표준화 환자는 일관적이되 적절하게 반응하도록 지시받았습니다.
- [4개의 비디오]는 미국 내과학회에서 개발했으며(미국 내과학회의 허가를 받아 사용), 서면 스크립트를 사용했습니다.
- [모든 비디오]는 52명의 메이요 클리닉 내과 의사가 미니 임상 평가 연습(Mini-CEX)을 사용하여 평가했습니다(이전 연구의 일부로 14,15). 15 사용 가능한 36개의 비디오 중에서 먼저 관리 상황을 가장 잘 나타내는 비디오(즉, 상담 중심)를 식별한 다음, Mini-CEX 상담 점수를 사용하여 가장 낮은 점수를 받은 5개와 가장 높은 점수를 받은 5개 비디오를 선정했습니다(다양한 성과를 풍부하게 표현하기 위해 극단적인 그룹을 의도적으로 선택).
- 최종적으로 선정된 5개의 동영상은 각각 2단계의 성과로 구성된 5개의 사례(새로운 고혈압 관리, 새로운 고지혈증, 새로운 섬유근육통, 최적 조절이 되지 않는 당뇨병, 암을 나타내는 갑상선 결절 생검)를 표현했습니다.
- 각 비디오는 트랜스크립션되었으며, 트랜스크립션은 비디오 검토 중 및 검토 후에 검토자가 참조할 수 있도록 제공되었습니다. 동영상 개발에 사용된 연구14,15는 메이요 클리닉 기관윤리심의위원회에서 면제 판정을 받았습니다. 이 연구에는 새로운 인간 피험자가 등록되지 않았습니다.
The video clips were used in a previously published study of rater training. 14,15
- Each video portrays a resident physician counseling a patient about a medical condition (e.g., hyperlipidemia, fibromyalgia, thyroid cancer). The videos were planned to show a range of resident performance varying from poor to superior.
- Six videos were developed by author D.A.C. and consisted of extemporaneous dialogues between a final-year or chief internal medicine resident physician and a standardized patient from our community pool.
- The physicians were instructed to vary their performance (superior or poor); the standardized patients were instructed to respond consistently but appropriately.
- Four videos were developed by the American Board of Internal Medicine (used with their permission) and used written scripts.
- All videos were rated (as part of the previous study 14,15) by 52 Mayo Clinic internal medicine physicians using the mini-clinical evaluation exercise (Mini-CEX). 15 From the 36 videos available, we first identified those that best represented management encounters (i.e., counseling focused) and then used the Mini-CEX counseling score to select the 5 lowest-scoring and 5 highest-scoring videos (extreme groups purposive selection to provide a rich representation of varying performances).
- The ultimately selected videos represented 5 encounters (management of new hypertension, new hyperlipidemia, new fibromyalgia, suboptimally controlled diabetes mellitus, and a thyroid nodule biopsy that indicated cancer), each at 2 levels of performance.
- Each video was transcribed, and transcripts were available to reviewers for reference during and after video review. The study used to develop videos 14,15 was judged exempt by the Mayo Clinic Institutional Review Board. No new human subjects were enrolled in this study.
관찰과 코딩의 만남
Encounter observation and coding
2020년 11월, 보드 인증 내과 의사 3명(D.A.C., C.R.S., S.J.D.)과 인지 심리학자 1명(L.D.G.)이 각 비디오를 최소 2회 이상 독립적으로 검토하고 추가로 여러 비디오를 짝을 지어 시청했습니다. 검토자들은 개방형 프롬프트가 있는 코딩 양식을 사용하여 치료(약물 및 비약물) 및 추가 진단 검사에 대한 결정, 공유된 의사 결정, 종단적 계획(예: 추적 관찰)에 대한 결정뿐만 아니라 이러한 작업을 자극, 중재, 형성 또는 영향을 미치는 추가 프로세스를 포함하되 이에 국한되지 않는 특정 관리 작업 및 프로세스를 식별하고 문서화했습니다. 우리는 이전에 구상한 모델 2를 출발점으로 삼아(즉, 여러 합리적인 옵션 중에서 선택, 환자 가치의 우선순위 결정, 공유된 의사 결정, 계획의 지속적인 조정, 사람과 시스템 간의 역동적인 상호 작용) [관리 추론의 추가 특징]을 모색했습니다. 개선할 수 있는 성과 측면(예: 레지던트에 대한 가상의 피드백)을 명시적으로 문서화했습니다. 또한 각 리뷰어는 동영상에 묘사된 경영 추론 활동을 넘어서는 새로운 인사이트, 주제, 연결점(깨달음)을 문서화했습니다.
In November 2020, 3 board-certified internal medicine physicians (D.A.C., C.R.S., and S.J.D.) and 1 cognitive psychologist (L.D.G.) independently reviewed each video at least twice and additionally viewed several videos in pairs. Using a coding form with open-ended prompts (see Supplemental Digital Appendix 1 at https://links.lww.com/ACADMED/B305), reviewers identified and documented specific management tasks and processes, including but not limited to decisions about therapy (drug and nondrug) and further diagnostic testing, shared decision making, and longitudinal planning (e.g., follow-up), as well as additional processes that stimulated, mediated, shaped, or were influenced by the tasks. We used our previously conceived model 2 as a starting point (i.e., selection among multiple reasonable options, prioritization of patient values, shared decision making, ongoing adjustment of the plan, and dynamic interplay among people and systems) and further sought additional features of management reasoning. We explicitly documented aspects of performance that could be improved (i.e., hypothetical feedback to the resident). In addition, each reviewer documented novel insights, themes, and connections (epiphanies) that extended beyond management reasoning activities portrayed in the video.
데이터 분석 및 모델 구축
Data analysis and model building
우리는 지속적인 비교 분석 접근법을 사용하여 진단적 추론에 대한 연구에서 주마와 골드스미트(Juma and Goldszmidt)13가 사용한 것과 유사한 방법을 채택했습니다. 16 우리 중 한 명(D.A.C.)은 모든 비디오에 대한 모든 조사자의 원시 관찰과 깨달음을 검토하고 이를 코딩 양식 프롬프트로 구성된 관리 작업, 프로세스 및 인사이트의 길고 포괄적인 목록으로 정리했습니다. 전체 검토팀은 음성 및 전자 매개 대화를 통해 이러한 아이디어를 반복적으로 재구성, 재개념화, 정교화, 구체화하여 [핵심 기능의 간결한 목록]으로 정리한 다음, [관리 추론 모델을 구축]하기 위해 일련의 토론을 진행했습니다. 이 분석에서는 공통 주제와 소주제(핵심 기능 및 과제)를 찾고, 높은 성과와 낮은 성과를 대조하고, 각 깨달음을 신중하게 탐색했습니다. 모든 검토자가 주요 특징과 최종 모델에 대해 완전히 합의했습니다.
We adopted a method similar to that used by Juma and Goldszmidt 13 in a study of diagnostic reasoning by using a constant comparative analysis approach. 16 One of us (D.A.C.) reviewed all investigators’ raw observations and epiphanies for all videos and organized these into a lengthy, comprehensive list of management tasks, processes, and insights organized by coding form prompts. The entire review team had a series of discussions (through voice and electronic-mediated conversations) to iteratively reorganize, reconceptualize, elaborate, and refine these ideas into a parsimonious list of key features and then construct a model of management reasoning. This analysis looked for common themes and subthemes (key features and tasks), contrasted high and low performances, and thoughtfully explored each epiphany. All reviewers came to full consensus on the key features and final model.
결과
Results
비디오를 관찰하는 동안 약 120페이지 분량의 한 칸 띄어쓰기 주석이 생성되었습니다. 이로부터 18페이지 분량의 관리 업무, 프로세스 및 인사이트 목록을 추출한 후 이를 핵심 기능 목록과 관리 추론 모델로 압축했습니다. 비디오 검토 과정에서 진화하고 단순한 관찰과 높은 수준의 인사이트가 혼합된 원시 내러티브를 직접 생성했기 때문에, 우리는 자신의 내러티브를 인용하거나 어떤 단계에서 인사이트가 도출되었는지 구분하기보다는 관찰과 인사이트를 전체적으로 요약하는 정제된 내러티브를 제시합니다.
We collectively generated approximately 120 pages of single-spaced typed comments during video observations. From this, we distilled an 18-page list of management tasks, processes, and insights, and subsequently condensed this into a list of key features and a model of management reasoning. Inasmuch as we generated the raw narratives ourselves, which evolved during video review and contained a mixture of simple observations and high-level insights, we present a refined narrative that summarizes our observations and insights as a whole, rather than quote our own narratives or attempt to discriminate at what stage an insight emerged.
관리 추론의 특징
Features of management reasoning
우리는 [관리 추론의 12가지 특징]을 확인했습니다(표 1). 이 중 5개는 이전에 비경험적 에세이에서 제안되고 기술된 바 있으며,1 관찰을 통해 확인되었습니다. 7가지 특징은 경험적 분석에서 새롭게 나타났으며 아래에서 설명합니다. 이 중 질병 관련 지식과 임상 경험의 조직화를 제외한 나머지는 진단적 추론과 달리 관리 추론에 고유한 특징입니다.
We identified 12 distinct features of management reasoning (Table 1). Five of these had been previously proposed and described in a nonempirical essay, 1 and they were confirmed in our observations. Seven emerged anew in our empirical analysis and are discussed below. Of these, all but illness-specific knowledge and organization of the clinical encounter are largely unique to management reasoning (in contrast to diagnostic reasoning).
질환-특이적 지식.
Illness-specific knowledge.
가장 눈에 띄는 인사이트 중 하나는 [관리 추론이 콘텐츠에 따라 다르다]는 점입니다. 거의 모든 다른 기능은 질병 자체에 대한 깊고 정확한 지식(질병별 지식) 또는 지역 의료 시스템 내에서 질병을 관리하는 방법(프로세스 지식, 아래 설명 참조)에 의존합니다.
One of the most salient insights was that management reasoning is content-specific. Nearly every other feature relies on deep, accurate knowledge of the illness itself (illness-specific knowledge) or how to manage the illness within the local health care system (process knowledge, described below).
[질환 특이적 지식]에는 [질병의 메커니즘, 병리, 자연사 또는 예후, 진단 및 치료 옵션(효과, 위험 및 비용 포함)]이 포함됩니다. 유능한 임상의는 [구체적인 근거 또는 가이드라인]을 간략하게 언급하여 이러한 요점을 뒷받침했습니다(예: "연구에 따르면 고혈압을 치료하면 심장병, 뇌졸중 및 신장 질환에 걸릴 확률이 줄어듭니다."). 관련 치료 옵션을 생략하거나, 치료 효과를 잘못 설명하거나, 중요한 부작용을 무시하거나, 추가 평가의 시급성을 부정확하게 전달하는 등의 [콘텐츠 지식 결함]이 저성과자(마이너 및 메이저 모두)에게서 빈번하게 관찰되었습니다.
Illness-specific knowledge includes the mechanism, pathology, natural history, or prognosis of disease, and diagnostic and treatment options (including effectiveness, risks, and costs). Effective clinicians supported many of these points with brief reference to specific evidence or guidelines (e.g., “Research shows that treating hypertension reduces your chance of heart disease, stroke, and kidney disease.”). We observed frequent content knowledge flaws in low performers (both minor and major), such as omitting relevant treatment options, misstating treatment effectiveness, neglecting important side effects, or inaccurately conveying the urgency of further evaluation.
프로세스 지식.
Process knowledge.
[프로세스 지식]은 [지역 의료 시스템에서 관리의 물류에 관한 운영적이고 실용적인 통찰력]("여기서 일이 어떻게 돌아가는지")을 포함합니다.
- [프로세스 지식의 격차]는 비약물 관리 옵션(예: 물리 치료, 전문가 상담, 후속 조치에 대한 모호한 계획)에 대한 불확실성 또는 사용 가능한 모든 자원을 활용하지 못하는 것으로 나타났습니다.
- [질병 특이적 지식 격차]에 비해 부정적 영향이 실질적이고 직접적이지 않을 수 있지만, 그럼에도 불구하고 [프로세스 지식 격차]는 환자에게 불확실성, 신뢰도 저하, 불만족을 남겼습니다.
- 요컨대, 의사가 [환자가 [임상의사 자신의 이해를 넘어서는 결정]을 내릴 수 있도록 가이드하는 것]은 불가능합니다.
Process knowledge encompasses operational, practical insights regarding the logistics of management in the local health care system (“how things work around here”).
- Process knowledge gaps manifested as uncertainty regarding nondrug management options (e.g., vague plans for physical therapy, specialist consultation, follow-up) or failure to draw on all available resources.
- Although their adverse effects were perhaps less substantial and direct than illness-specific knowledge gaps, process knowledge gaps nonetheless left the patient appearing uncertain, less trusting, and dissatisfied.
- In short, it is impossible for clinicians to guide patients in navigating a decision that exceeds their own understanding.
관리 스크립트.
Management scripts.
또 다른 중요한 인사이트는 관리 대면에서 [관리 스크립트]의 중요하고도 두드러진 역할이었습니다. [스크립트]는 일반적으로 다음과 같이 정의됩니다.
Another important insight was the prominent and critical role of management scripts in the management encounter. Scripts are defined generally as
[고수준]의 [사전 편집]된 [개념적 지식 구조] ... [이는] 개별 이벤트가 [시간적], 종종 [인과적] 또는 [계층적] 관계로 상호 연결되는 [일반적인 (고정관념화된) 이벤트 시퀀스]를 나타내며, 적절한 맥락에서 [통합된 전체]로 활성화될 수 있고, 실제 상황에 존재하는 정보로 [채워filled]지거나, 기억에서 검색되거나 맥락에서 [추론]할 수 있는 [변수와 슬롯]을 포함한다. 17(p457)
high-level, precompiled, conceptual knowledge structures … [that] represent general (stereotyped) event sequences, in which the individual events are interconnected by temporal and often also causal or hierarchical relationships; that can be activated as integral wholes in appropriate contexts [and] contain variables and slots that can be filled with information present in the actual situation, retrieved from memory, or inferred from the context. 17(p457)
[관리 스크립트]의 경우 [개별 이벤트]는 [진단 검사, 치료, 상담, 환자 교육, 공유 의사 결정, 모니터링 등]의 [관리 옵션]으로 구성됩니다. [스크립트]는 이러한 이벤트를 [합리적인 관리 계획]으로 연결합니다.
For management scripts, the individual events comprise management options, including diagnostic tests, treatments, consultations, patient education, shared decision making, and monitoring. Scripts link these events into a rational management plan.
우리는 [관리 스크립트]를 [합리적인 관리 계획의 개발]을 용이하게 하기 위해, [관리 옵션]과 [임상의 업무]를 [시간적 또는 논리적 순서]로 표현하고 연결하는 [미리 컴파일된 개념적 지식 구조]로 정의합니다(표 1).
We define management scripts as precompiled conceptual knowledge structures that represent and connect management options and clinician tasks in a temporal or logical sequence to facilitate development of a rational management plan (Table 1).
[관리 스크립트]는 [일관성 있고 유창하며 구조화된 내러티브]로서 이러한 만남에서 나타났습니다. 개별 요소는 특정 환자나 만남의 고유한 요구에 맞게 조정되었지만, 적어도 초기에는 예상치 못한 사건이나 정보(예: 환자의 저항이나 날카로운 질문)로 인해 중단되기 전까지는 스크립트 전체가 대체로 미리 결정된 것처럼 보였습니다.
- 저품질의 스크립트는 일관성이 없고, 구불구불하며, 반응적이고, 비인격적이며, 실망스러운 면담으로 이어져 결국 환자와 의료진 모두 불만족스러운 결과를 초래했습니다.
- 이와 대조적으로 고품질 스크립트는 환자의 질문을 미리 파악하고, 의사 결정을 공유하며, 신뢰와 확신을 불러일으키는 것으로 나타났습니다.
[스크립트의 품질]은 다음을 포함한 다각적인 요인으로 해석했습니다.
- 스크립트 내용(질환 특이적 및 일반적인 프로세스 지식),
- 시퀀스(자연스럽고 논리적인 시간적 전개),
- 유연성(환자의 배경, 동반 질환, 선호도, 제약 조건, 질문 및 이해도에 대한 대응),
- 유창성(전달의 용이성, 일관성 및 명확성)
Management scripts manifested in these encounters as coherent, fluent, structured narratives. Although individual elements were tailored to the unique needs of a given patient or encounter, the script as a whole seemed to be largely predetermined—at least initially and until disrupted by unexpected events or information (e.g., resistance or penetrating questions from the patient).
- Low-quality scripts led to encounters that appeared disjointed, meandering, reactive, impersonal, and dispiriting, and ultimately resulted in dissatisfaction for both patients and clinicians.
- By contrast, high-quality scripts seemed to preempt patient questions, facilitate shared decision-making, and engender trust and confidence.
We construed quality to be multifactorial, including
- script content (illness-specific and general process knowledge),
- sequence (natural, logical temporal evolution),
- flexibility (responsiveness to patient background, comorbidities, preferences, constraints, questions, and comprehension), and
- fluency (ease, coherence, and clarity of delivery).
스크립트의 일반성(즉, '나쁜 소식 전하기', '새로운 질환에 대한 치료 시작', '만성 질환에 대한 치료 강화' 등 콘텐츠 영역에서 반복될 수 있는 패턴을 준수하는 정도)도 다양했습니다. [가장 좋은 스크립트]는 [일반적인 틀에 기초]하며, [특정 질병과 환자 모두에게 맞춤화된 것]입니다.
Scripts also varied in the level of generality (i.e., adherence to a pattern that could be replicated across content areas, such as “breaking bad news,” “initiating treatment for a new condition,” and “intensifying treatment of a chronic condition”). The best scripts seem to be grounded in a general framework and then tailored to both the specific illness and the patient.
환자의 스승이자 영업사원으로서의 임상의 역할.
Clinician roles as patient teacher and salesperson.
우리는 공동 의사 결정의 개념과는 별개로 [환자에 대한 교사이자 영업사원으로서 임상의의 중요한 역할]을 확인했습니다. 효과적인 환자 교육은 공유 의사 결정
- 활동 전(의사 결정의 필요성을 입증하기 위해),
- 활동 중(옵션 간의 구별되는 특징을 강조하기 위해),
- 활동 후(관리 계획에서 환자의 개인적 책임을 알리기 위해)에 필수적입니다.
임상의는 이러한 환자 교육 요건에 대한 일차적인 책임이 있습니다.
We identified critical roles for the clinician as a teacher and salesperson to the patient that seemed distinct from the concept of shared decision making. Effective patient education is essential
- before (to substantiate the need to make a decision),
- during (to highlight distinguishing features among options), and
- after (to apprise patients of their personal responsibility in the management plan) the shared decision activity.
Clinicians have a primary responsibility in these patient teaching requirements.
마찬가지로 세일즈맨십, 즉 최종 결정에 대한 [환자의 완전한 동의를 얻는 역할도 중요]한 것으로 보입니다. 이 역할이 반드시 특정 치료 옵션을 '판매'하는 것을 의미하는 것은 아니며, 실제로 최고의 영업 담당자(임상의)는 먼저 구매자의 요구 사항을 확인한 다음, 이러한 요구 사항을 충족할 가능성이 가장 높은 옵션으로 구매자(환자)를 안내할 것입니다. 그럼에도 불구하고 결국에는 완전한 동의를 얻지 못하면 [차선의 결과(예: 낮은 순응도)]를 초래하게 됩니다. 또한 훌륭한 영업사원은 효과적으로 가르치고, 명확하고 공개적으로 소통하며, 신뢰 관계를 구축합니다(아래 설명 참조).
Likewise, there seems to be a strong role for salesmanship—that is, obtaining the patient’s full buy-in on the final decision. This role does not necessarily imply “selling” a specific treatment option; indeed, the best salesperson (clinician) would first ascertain the buyer’s needs and then steer the buyer (patient) toward the option(s) most likely to meet those needs. Nonetheless, in the end, anything but full buy-in will result in suboptimal results (e.g., poor adherence). A good salesperson also teaches effectively, communicates clearly and openly, and builds a relationship of trust (described below).
임상의와 환자의 관계.
Clinician–patient relationship.
우리는 임상의의 [미묘한 행동(예: 환자의 우려 사항을 효과적으로 해결하거나 무시하거나, 치료 옵션을 유창하게 또는 일관성 없이 설명하는 등)]이 환자의 신뢰를 구축하거나 약화시키는 여러 사례를 관찰했습니다. 신뢰가 없으면 대개 환자가 납득하지 못하고 불만족스러워합니다. 신뢰는 양방향입니다. 의료진도 환자를 신뢰해야 합니다(예: 환자가 진실하고 관리 계획에서 자신의 역할을 다할 것이라는 믿음). 대부분의 만남은 적당한 수준의 상호 신뢰에서 시작하여 후속 조치를 통해 강화되거나 약화되는 것으로 보였습니다.
We observed multiple instances in which subtle clinician actions (e.g., effectively addressing or neglecting a patient concern, or fluently or disjointedly describing treatment options) built or undermined the patient’s trust. Without trust, the encounter typically ended with an unconvinced and dissatisfied patient. Trust is bidirectional: the clinician must also trust the patient (e.g., that they are truthful and that they will fulfill their part in the management plan). Most encounters seemed to start with a moderate level of mutual trust that was strengthened and weakened through subsequent actions.
예후.
Prognostication.
많은 환자 질문은 다음과 관련된 향후 기대치와 관련이 있습니다.
- [질병]뿐만 아니라
- ("얼마나 빨리 나아질까요?")
- 특히 [관리 계획 자체]
- ("비용은 얼마나 드나요?", "이 약의 부작용은 무엇인가요?", "언제 외과의를 볼 수 있나요?", "언제 다시 볼 수 있나요?")
Many patient questions relate to future expectations regarding
- not only the illness
- (“How soon will I feel better?”)
- but also—perhaps especially—the management plan itself
- (“How much will this cost?”; “What are the side effects of this medication?”; “When will I see the surgeon?”; “When will I see you again?”).
임상의는 이러한 질문에 대한 답을 알고 있어야 미래의 상황을 정확하게 예측하거나 예상할 수 있습니다. 동영상에서 이러한 질문에 대한
- 모호한 답변은 신뢰를 약화시키고 환자가 걱정하고 좌절하는 것처럼 보이게 했습니다.
- 반면, 구체적인 답변을 제공할 수 있는 임상의는 환자의 신뢰, 확신, 헌신을 불러일으켰습니다.
효과적인 예후 예측에는 질병 관련 지식, 치료 과정 지식, 개인적 경험, 커뮤니케이션 기술, 효과적인 교육 등이 복합적으로 작용하는 것으로 나타났습니다. 가장 숙련된 임상의(스크립트가 잘 발달된 임상의)는 [질문이 나오기 전에 미리 예상하고 답변함]으로써 질문을 방지할 수 있었습니다.
Clinicians are expected to know these answers—accurately predicting or anticipating future events. In the videos, vague answers to these questions undermined trust and left patients appearing worried and frustrated. By contrast, clinicians who could provide specific answers engendered the patient’s trust, confidence, and commitment. Effective prognostication seemed to entail a combination of illness-specific knowledge, process knowledge, personal experience, communication skill, and effective teaching. The most skilled clinicians (those with well-developed scripts) were able to forestall questions by anticipating and answering questions before they were articulated.
임상 만남의 조직화(순서 및 시간 관리).
Organization of the clinical encounter (sequencing and time management).
마지막으로, 전체 관리 추론 활동에서 가장 중요한 것은 주어진 기간 동안 [추론 프로세스 자체를 조직(시퀀싱)하는 것]입니다(이 경우 외래 임상의와 환자 간 만남). 관리 추론은 환자 교육, 질문과 답변, 옵션 조사, 다른 팀원과의 커뮤니케이션, 의사 결정, 계획 실행과 같은 활동에 대한 선택, 순서 및 시간을 관리합니다. 조직은 다양한 수준의 의식적(의도적) 및 무의식적 추론을 반영합니다. 이러한 작업 시퀀스는 종종 관리 스크립트의 일부로 컴파일됩니다. 이 비디오에서 우리는 매우 짧은 만남(의료진이 환자를 의사 결정에 참여시키지 않음)과 매우 긴 만남(의료진이 잠재적인 문제를 예상하기보다는 허둥대고 우왕좌왕하며 반응하는 것처럼 보임) 모두에서 문제를 관찰했습니다. 그러나 주어진 만남은 치료의 한 지점에 불과하며, 즉각적인 관리 결정은 과거 만남에서 얻은 정보, 토론 및 결정을 통합하고 향후 만남을 예측해야 한다는 점을 인식하고 있습니다.
Finally, overarching the entire management reasoning activity is the organization (sequencing) of the reasoning process itself in a given period (in this case, an outpatient clinician–patient encounter). Management reasoning governs the choice, sequencing, and time spent on actions such as teaching patients, asking and answering questions, researching options, communicating with other team members, making decisions, and implementing the plan. Organization reflects varying degrees of conscious (deliberate) and unconscious reasoning. These action sequences are often compiled as part of the management script. In these videos, we observed problems with encounters that were both very short (the clinician failed to involve the patient in decision making) and very long (the clinician seemed to flounder, meander, and react rather than anticipate potential challenges). We recognize, however, that a given encounter represents only 1 point in care; immediate management decisions should integrate information, discussions, and decisions from past encounters and anticipate future encounters.
관리 추론의 함정
Pitfalls in management reasoning
또한 아래에 설명된 바와 같이 관리 추론에서 [몇 가지 실수]를 발견했습니다.
We also observed several missteps in management reasoning, as described below.
- 모호한 치료 계획: 임상의가 약물 투여 지침, 약물 부작용, 다음 관리 단계(예: 진단 검사, 전문의 상담, 물리 치료), 후속 조치 시기, 진행 중인 증상 관리 등 치료 계획에 대해 환자에게 세부 정보를 제공하거나 안심시키지 못했습니다. 환자는 당황하거나 좌절하거나 걱정하는 모습을 보였습니다.
- Vague care plans: Clinicians failed to provide details or reassurance to patients about the care plan, such as drug administration instructions, drug side effects, next steps in management (e.g., diagnostic testing, specialist consultation, physical therapy), timing of follow-up, and management of ongoing symptoms. The encounter ended with the patient appearing puzzled, frustrated, or worried.
- 제한된 치료 계획: 임상의는 한 가지 치료 옵션 또는 짧은 일반(이 환자에게 맞춤화되지 않은) 옵션 목록만 제시했습니다. 이러한 계획은 진단에 대한 반사적 반응(진단적 추론에서 조기 종결과 유사)으로 보이지만, 임상의가 열등하거나 실행 불가능하다고 판단되는 옵션을 의도적으로 피하면서 알려진 또는 가정된 선호도 및 제약 조건에 따라 최적의 계획을 신중하게 미리 선택한 것일 수도 있습니다.
- Restricted care plans: Clinicians presented only 1 treatment option or a short generic (not tailored to this patient) list of options. This plan seemed to be a reflexive response to the diagnosis (akin to premature closure in diagnostic reasoning); however, it could alternatively represent thoughtful preselection of an optimal plan based on known or assumed preferences and constraints, with the clinician intentionally avoiding options judged as inferior or infeasible.
- 환자 선호도를 확인하지 않은 경우: 임상의가 환자의 [선호도를 유도하거나 확인]하지 않고 계획을 제시했으며, 아마도 그러한 선호도에 대한 가정을 한 것으로 추정됩니다. 임상의가 환자와 오랜 기간 관계를 맺어온 경우에도 일반적으로 선호도를 확인하는 것이 필요합니다.
- Failure to ascertain patient preferences: Clinicians presented a plan without eliciting or confirming patient preferences, presumably by making assumptions about such preferences. Even when a clinician has a longstanding relationship with the patient, confirmation of preferences would typically seem warranted.
- 공유된 의사 결정의 부재: 임상의가 치료 계획을 수립하고 마무리할 때 [환자를 참여]시키지 않았습니다. 대안에 대한 사전 논의가 있든 없든 한 가지 옵션이 최선이라고 제시되었고, 환자는 이에 동의할 것으로 예상되었습니다. 일부 환자는 이러한 접근 방식을 받아들이는 것처럼 보였지만, 대부분은 불안해하거나 실망하거나 사기가 저하된 모습을 보였습니다.
- Absence of shared decision making: Clinicians failed to involve patients in formulating and finalizing the care plan. One option was proffered as optimal (with or without antecedent discussion of alternatives), and the patient was expected to acquiesce. Although some patients seemed to accept this approach, most appeared unsettled, disappointed, or demoralized.
- 단서를 따르지 않음: 임상의는 [우려, 질문, 의심을 암시하는 언어적 또는 비언어적 메시지를 해결]하지 못했습니다. 단서는 미묘한 것(표정이나 차분한 언어 표현)부터 명시적인 것(명확한 질문이나 우려 사항 진술)에 이르기까지 다양했습니다. 임상의의 반응에는 완전한 무시, 추가 논의 없이 피상적으로 인정, 짧은 논의 후 무시, 환자의 지속적인 우려에 대한 노골적인 무시(논의 없이 또는 논의 후)가 포함되었습니다. 환자는 항상 좌절하고 때때로 화를 내는 것처럼 보였습니다.
- Failure to follow cues: Clinicians failed to address verbal or nonverbal messages that suggested concerns, questions, and doubts. Cues ranged from subtle (facial expression or subdued verbal expressions) to explicit (clear question or statement of concern). Clinician responses included complete ignorance, cursory acknowledgment without further discussion, brief discussion followed by dismissal, and outright overruling of persistent patient concerns (without or after discussion). Patients always appeared frustrated and occasionally upset.
- 이해와 약속을 확인하지 않음: 임상의는 환자가 계획을 이해하고 동의했는지 확인하지 않았습니다.
- Failure to confirm understanding and commitment: Clinicians did not confirm that patients comprehended and agreed with the plan.
관리 추론의 모델
A model of management reasoning
임상의와 환자의 만남에 대한 경험적 분석을 바탕으로 [관리 추론의 모델]을 잠정적으로 제안합니다(그림 1). 이 모델은 주로 의료진과의 만남의 시간적 진화를 반영한 것으로, 이러한 진화가 임상의의 뇌에서 일어나는 실제 인지 과정이나 일련의 과정을 어느 정도 반영하는지는 확실하지 않습니다. 우리는 주어진 만남에서 단계가 반복되거나 동시에 진행되는 경우가 많다는 것을 인정합니다.
On the basis of our empirical analysis of clinician–patient encounters, we tentatively propose a model of management reasoning (Figure 1). This model largely reflects the temporal evolution of a management encounter; we are uncertain to what extent this evolution reflects the actual cognitive processes or sequence of processes that occur in the clinician’s brain. We acknowledge that steps are often repeated or concurrent in a given encounter.
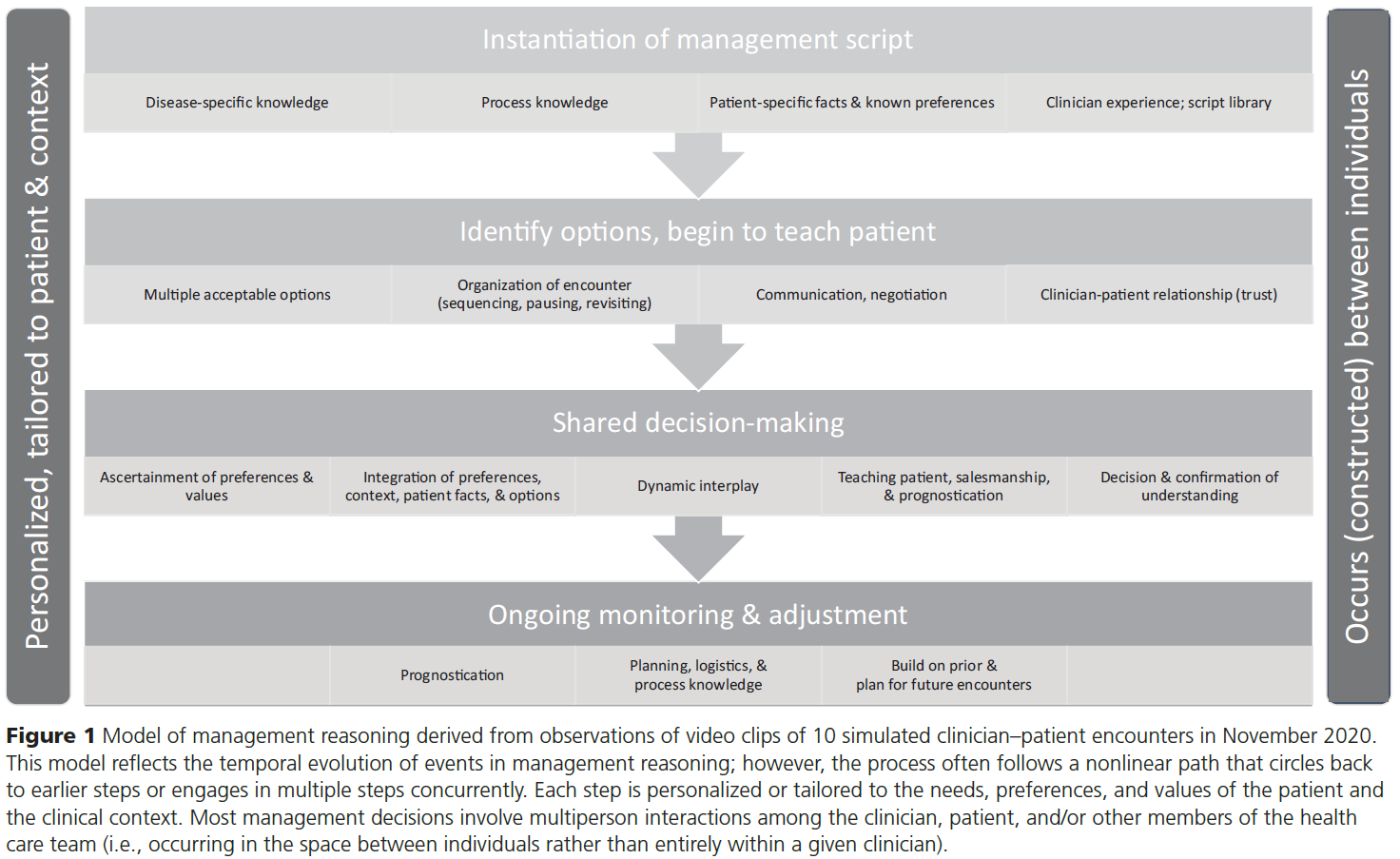
관리 추론의 첫 번째 단계는 관리 스크립트의 트리거(활성화), 선택 및 인스턴스화인 것으로 보입니다. 18 [스크립트 개념의 조작화]에는 다음의 조합이 반영됩니다.
- 질병별 지식,
- 프로세스 지식,
- 환자별 사실에 대한 지식(현재 및 과거 병력, 검사 결과, 검사 데이터 등)
- 임상의의 개인적 경험
[인스턴스화]는 [환자 및 상황별 요소를 통합]하여 [즉각적인 문제에 맞게 스크립트를 개인화]합니다. 스크립트에는 후속 진료에서 다룰 주요 문제(교육, 치료 옵션, 예후 등)가 코드화되어 있으며 추론 프로세스에서 중요한 의사 결정 시점을 강조합니다.
The first step in management reasoning seems to be the triggering (activation), selection, and instantiation of a management script. 18 Our operationalization of the script concept reflects a combination of
- illness-specific knowledge,
- process knowledge,
- knowledge of patient-specific facts (current and past history, examination findings, test data, etc.), and
- the clinician’s personal experience.
Instantiation integrates patient- and context-specific factors to personalize the script to the immediate problem. The script codifies the key issues (education, treatment options, prognosis, and so on) that will be addressed in the ensuing encounter and highlights critical decision points in the reasoning process.
관리 추론의 두 번째 단계에서는 [스크립트를 사용하여 이 환자와 상황에 적합한 잠재적 관리 솔루션을 식별한 다음 관련 문제(예: 의학적 상태, 관리 옵션)에 대해 환자에게 교육]합니다. 의식적이든 무의식적이든 이 단계에서 만남의 조직화(순서)가 시작됩니다.
The second step in management reasoning uses the script to identify potential management solutions appropriate to this patient and context, and then to educate the patient about relevant issues (e.g., the medical condition, management options). Organization (sequencing) of the encounter begins at this step, whether conscious or unconscious.
관리 추론의 세 번째 단계는 의사 결정을 공유하는 것입니다. 우리는 본질적으로 전혀 없음(즉, 환자의 동의를 전제로 한 치료 옵션 하나만 제시)에서 중간 정도(권장 접근법과 함께 여러 옵션을 제시하고 환자가 [동의]를 선택할 수 있도록 함)에 이르기까지 다양한 변형을 관찰했습니다. 이 동영상에서 모범적인 사례로 간주되는 사례는 없었지만, 누락된 부분과 단점(임상의가 개선해야 할 부분으로 문서화됨)은 [공동 의사 결정의 강력한 모델]을 충분히 강조했습니다. 이 모델에는 다음이 포함되었습니다.
- 환자의 선호도와 가치에 대한 명시적인 확인,
- 환자의 선호도와 가치를 다른 정보와 통합(질병별 지식, 환자별 정보, 프로세스 지식 포함)
- 향후 상황에 대한 예후 예측,
- 환자와 임상의 모두에게 잠정 결정이 실제로 최적이라는 확신을 주는 역동적인 상호 작용
The third step of management reasoning is shared decision making. We observed wide variation, ranging from essentially none (i.e., only 1 treatment option presented, with the patient’s acquiescence presumed) to moderate (presenting several options with a recommended approach, and allowing the patient to choose [concur]). Although these videos did not offer any encounters that we considered exemplary, the omissions and shortcomings (documented as areas for improvement for the clinician) amply highlighted a robust model of shared decision making. This model included
- explicit ascertainment or confirmation of patient preferences and values,
- integration of patient preferences and values with other information (including illness-specific knowledge, patient-specific information, and process knowledge),
- prognostication of future events, and
- a dynamic interplay that assured both patient and clinician that the tentative decision was in fact optimal.
우리는 [환자의 가치관을 통합하는 것]뿐만 아니라, 환자에게 [이러한 결정이 이루어졌다는 것을 명시적으로 전달하는 것]이 중요하다는 것을 관찰했습니다.
- 상황에 따라 의사 결정 과정에 참여하고, 생활 습관 개선 조치를 실행하고, 약을 복용하고, 다른 임상의와 상담하고, 후속 조치를 위해 재방문하는 등의 조치를 포함하여 환자가 치료 계획을 구매하도록 설득하는 데는 [교육과 세일즈맨십이 필수적]이었습니다.
- 이 동영상에는 설명되어 있지 않지만, [의사 결정 보조 도구]가 많은 경우에 도움이 되었을 것이라는 점에 주목했습니다.
- 또한 [다른 의료진과의 상호작용]을 보여주는 동영상은 없었지만, 이 단계에서 이러한 상호작용을 통해 의료진의 권장 사항, 우선순위, 가치, 물류 제약 사항을 확인하고 통합할 수 있을 것으로 예상됩니다.
- 공유 의사 결정 단계는 환자가 계획을 [이해하고 동의했음을 명시적으로 확인]하는 것으로 끝나는 것이 이상적입니다(일관성이 없더라도).
We observed that it was important not only to integrate the patient’s values but also to expressly convey to the patient that this had been done.
- Teaching and salesmanship were essential in persuading the patient to buy into the care plan, including (depending on the situation) actions such as engaging in the decision-making process, implementing lifestyle measures, taking a medication, consulting another clinician, and returning for follow-up.
- Although not illustrated in these videos, we noted that a decision aid would have been helpful in many instances.
- In addition, no video showed interaction with other members of the health care team, and we imagine such interactions at this step could ascertain and integrate their recommendations, priorities, values, and logistic constraints.
- The shared decision-making step ideally (albeit inconsistently) ended with explicit confirmation that the patient understood and subscribed to the plan.
관리 추론의 마지막 단계는 지속적인 모니터링과 관리 조정입니다. 이 모든 동영상은 이전 방문에 대한 후속 조치로 이루어졌기 때문에 장기간(경우에 따라 몇 년)에 걸친 관리 활동의 한 지점만 반영했습니다. 이러한 관점에서 볼 때 관리 추론은 반드시 이전 만남을 기반으로 하며 향후 후속 조치를 계획해야 합니다. 관리 스크립트는 [과거 정보(병력 및 치료에 대한 반응[이전 반응과의 변화])에 의해 맥락화된 새로운 정보(새로운 검사 결과 및 현재 임상 결과)]에 크게 영향을 받았습니다. 이 스크립트는 다시 제시된 관리 옵션과 임상의의 영업 피치의 테너를 결정했습니다. 또한 임상의는 이 상담에서 관리 범위(예: 당뇨병만 관리할지, 당뇨병과 혈압 및 니코틴 의존도까지 관리할지)에 대해 초기에 결정을 내렸습니다. 진료가 끝날 무렵에는 대개 후속 방문에 대한 계획이 수립되어 있었습니다(그렇지 않은 경우 환자는 대개 불확실하고 불만족스러워 보였습니다). 이러한 후속 계획은 약물 치료에 대한 반응 및 부작용 가능성, 수술의 그럴듯한 결과, 상담 일정의 예상 지연, 질병의 자연력 등 예상되는 또는 [필요한 사건(예후)을 예측하는 임상의의 능력]에 영향을 받습니다. 계획에는 ['이상적인' 후속 조치 계획]과 함께 [환자 및 상황적 요인(실제적인 물류)을 고려하는 것]이 이상적입니다.
The final step in management reasoning is ongoing monitoring and adjustment of management. All these videos were encounters in follow-up to an earlier visit and as such reflected only 1 point in a management activity spread over an extended period (in some cases, years). From this perspective, management reasoning necessarily builds on prior encounters and must plan for future follow-up. The management script was greatly influenced by new information (new test results and current clinical findings) contextualized by past information (medical history and response to treatment [change from prior response]). This script in turn dictated the management option(s) presented and the tenor of the clinician’s sales pitch. In addition, the clinician made decisions early on regarding the scope of management in this encounter (e.g., diabetes only vs diabetes and blood pressure and nicotine dependence). By the end of the encounter, plans were usually in place for a follow-up visit (and if not, the patient usually appeared uncertain and dissatisfied). These follow-up plans were influenced by the clinician’s ability to anticipate likely or necessary events (prognostication), such as likely response to and possible side effects of drug therapy, plausible outcomes of surgery, the expected delay in scheduling a consultation, or the natural history of the illness. Planning ideally included consideration of patient and contextual factors (practical logistics) married with “ideal” follow-up plans.
이러한 시간적 진화의 각 단계는 환자의 요구, 선호도 및 가치와 임상 상황에 따라 [개인화되거나 맞춤화]될 수 있으며, 맞춤화되어야 합니다. 예를 들어, '고혈압 신약'에 대한 관리 스크립트는
- 환자의 동반 질환 및 약물 알레르기, 보험 환급 및 상황(응급실 대 외래 진료소)을 고려해야 하며,
- [교육 및 세일즈맨십]은 환자의 사전 지식, 어휘 및 정보에 대한 욕구에 맞게 조정되어야 하고,
- [공유 의사 결정]에는 임상의가 제안한 계획에 대한 단순한 동의 이상의 것이 포함되어야 하며,
- [모니터링 및 조정]은 특정 치료, 질병의 심각도, 치료 반응, 환자 물류(예, 이동 비용 및 시간, 업무 공백 시간), 커뮤니케이션 옵션(예: 대면 방문이 아닌 전화 또는 화상 방문) 등을 고려해야 합니다.
임상의와 환자의 관계도 각 단계에서 강화되거나 약화될 것입니다.
We note that each step in this temporal evolution can and should be personalized or tailored to the needs, preferences, and values of the patient and the clinical context. For example, a management script for “new drug for hypertension” should take into account the patient’s comorbid conditions and drug allergies, insurance reimbursement, and context (emergency department vs outpatient clinic); teaching and salesmanship should be tailored to the patient’s prior knowledge, vocabulary, and desire for information; shared decision making should involve more than simple acquiescence to the clinician’s proposed plan; and monitoring and adjustment should take into account the specific treatment, severity of illness, treatment response, patient logistics (e.g., expense and time to travel, time away from work), and communication options (e.g., telephone or video visit rather than face-to-face visit). The clinician–patient relationship will also be strengthened or undermined at each step.
마지막으로, 이 동영상에서 관찰된 [관리 추론의 가장 중요한 특징]은 일반적으로 [임상의 내부의 인지적 연습]이 아니라 [임상의와 환자의 상호 작용으로 발생]한다는 것입니다. 물론 이러한 결과는 환자가 참석하지 않거나(예: 임상의가 혼자 또는 의료진과 함께 환자 데이터를 검토하는 경우) 의사 결정에 참여할 수 없는(예: 인공호흡기를 착용한 환자) 관리 상황을 반영하지 못하는 비디오 선택(즉, 대면)의 아티팩트일 수 있습니다. 그러나 대부분의 관리 결정은 궁극적으로 한 명의 임상의가 아닌 [여러 사람이 논의해야 한다]고 생각합니다. 이 동영상에는 나타나지 않지만 이러한 상호작용에는 의료진의 다른 사람(예: 학생, 간호사, 약사, 자문 의사)과 종단적, 비동기적, 간접적 상호작용(예: 의뢰 상담, 환자 인계, 공식적인 인계 없이 동료의 환자 진료)은 물론 동시적이고 직접적인 상호작용도 포함될 수 있습니다. 요컨대, 관리 추론은 전적으로 특정 임상의사 내에서가 아니라, 일반적으로 [개인 간의 공간]에서 발생한다고 추측할 수 있습니다.
Finally, an overarching feature of management reasoning as observed in these videos is that it commonly occurs as a clinician–patient interaction rather than as a cognitive exercise within the clinician. Naturally, this finding could be an artifact of the video selections (i.e., face-to-face encounters), which fail to reflect management situations in which the patient is not present (e.g., clinicians reviewing patient data alone or with the health care team) or unable to participate in decisions (e.g., patient on a ventilator). However, we believe that most management decisions ultimately involve multiperson discussions rather than a single clinician. Although not present in these videos, these interactions could involve others on the health care team (e.g., students, nurses, pharmacists, consulting physicians) and longitudinal, asynchronous, and indirect interactions (e.g., referral consultations, patient handovers, seeing a colleague’s patient without a formal handover) as well as concurrent, direct interactions. In short, it might be conjectured that management reasoning commonly occurs in the space between individuals rather than entirely within a given clinician.
토론
Discussion
이 연구는 시뮬레이션된 임상의와 환자의 만남을 담은 비디오에 대한 경험적 분석을 통해 이전에 설명한 관리 추론의 개념적 틀을 확장했습니다1,2.
- 이전에 생각했던 5가지 특징을 확인하는 것 외에도 관리 추론의 7가지 특징을 추가로 경험적으로 확인했습니다(표 1).
- 질병별 및 프로세스 지식의 중요성을 강조하고 관리 스크립트의 5가지 특징을 확인했습니다.
- (내용, 순서, 유연성, 유창성, 일반성)
- 또한 4단계의 시간적 진화와 개인 간 개인화 및 발생이라는 중요한 특징으로 구성된 관리 추론의 경험적 모델을 개발했습니다.
- (스크립트 인스턴스화, 옵션 식별 및 환자 교육, 공유된 의사 결정, 지속적인 모니터링 및 조정)
This study extended a previously described conceptual framework for management reasoning 1,2 through empirical analysis of videos of simulated clinician–patient encounters.
- In addition to confirming 5 previously conceived features, we empirically identified 7 additional features of management reasoning (Table 1).
- We highlighted the importance of illness-specific and process knowledge and identified 5 features of management scripts (content, sequence, flexibility, fluency, and generality).
- We developed an empirical model of management reasoning composed of 4 steps of temporal evolution (script instantiation, identifying options and teaching patients, shared decision making, and ongoing monitoring and adjustment) and overarching features of personalization and occurrence between individuals.
제한 사항
Limitations
이 연구에는 한계가 있습니다.
- 첫째, 관찰한 비디오는 사실적으로 제작되었지만 실제 임상의와 환자 간의 상호 작용이 아닙니다. 동영상은 원래 평가자 교육 연구를 위해 설계된 성인 외래 환자 1차 진료의 5개 질병으로 제한되었으며,14,15 최고 및 최악의 성과를 대표하도록 선택되었습니다. 10개의 비디오는 관리 추론 사례와 맥락의 제한된 샘플을 구성합니다. 따라서 본 연구 결과는 임상의가 모든 상황(예: 입원 환자, 전문의 또는 시술 환경)에서 관리에 대해 어떻게 추론하는지에 대한 표준적인 설명으로 해석될 수 없습니다.
- 둘째, 이번 연구 결과는 관찰 가능한 행동을 기반으로 합니다. 관찰된 행동은 다양한 원인에 의해 나타날 수 있습니다(예: 모호한 치료 계획은 불충분한 지식, 잘못된 추론 또는 잘못된 의사소통을 반영할 수 있음).
- 셋째, 저희는 이 연구에서 지침 개념 프레임워크 2의 개발자이면서 관찰자 및 분석자이기도 했으므로 확증 편향의 위험이 있습니다. 여섯 개의 비디오는 우리 중 한 명(박사)이 개발했으며, 이는 관찰의 객관성에 영향을 미칠 수 있습니다. 그러나 이러한 동영상 사례는 정해진 대본에 따르지 않고 즉흥적으로 제작되었으며 13년 전에 제작되었기 때문에 이러한 친숙도가 연구 결과에 큰 영향을 미치지는 않을 것으로 보입니다.
This study has limitations.
- First, the videos we observed were developed to be realistic, but they were not actual clinician–patient interactions. The videos were limited to 5 illnesses in adult outpatient primary care, originally designed for a study of rater training, 14,15 and selected to represent the best and worst performances. Ten videos constitute a limited sample of management reasoning instances and contexts. Our findings thus cannot be construed as canonical descriptions of how clinicians reason about management in all situations (e.g., inpatient, specialist, or procedural settings).
- Second, our findings are based on observable behaviors. We can speculate about but cannot confirm underlying cognitive processes; indeed, a given observed behavior could emerge from a variety of etiologies (e.g., a vague care plan could reflect inadequate knowledge, poor reasoning, or poor communication).
- Third, we were both the developers of the guiding conceptual framework 2 and the observers and analyzers in this study; therefore, there is some risk of confirmatory bias. Six videos were developed by one of us (D.A.C.), which could further influence the objectivity of observations. However, these video cases were extemporaneous (rather than adhering to a defined script) and moreover were created 13 years previously; therefore, it seems unlikely that this level of familiarity would significantly affect our findings.
이전 작업과의 통합
Integration with prior work
우리의 연구는 진단을 용이하게 하는 질병(질환, 병리학적 결함, 증상 및 징후)에 대한 지식 표현인 질병 스크립트에 대한 광범위한 문헌을 보완합니다. 17,19 이에 비해 관리 스크립트는 진단 검사, 치료, 상담, 환자 교육, 공유 의사 결정 및 모니터링과 같은 옵션과 임상의 업무를 연결하는 관리 계획 개발 경로에 대한 지식 표현입니다. 최근에 제안된 관리 스크립트 모델 중 하나는 시간적 진화를 강조했지만8 경험적 데이터에 기반하지 않고 임상의 내부의 활동(추론 및 의사 결정)에 초점을 맞추었습니다. 경험적 관찰에 기반한 저희 모델은 임상의, 환자 및 기타 의료진 구성원을 포함하며, [대인 커뮤니케이션]과 [공유 의사 결정]을 관리 스크립트의 핵심 기능으로 강조합니다.
Our work complements the extensive literature on illness scripts, which are knowledge representations of an illness (enabling conditions, pathological faults, and symptoms and signs) that facilitate diagnosis. 17,19 By contrast, management scripts are knowledge representations of the path to development of a management plan, linking options and clinician tasks, such as diagnostic tests, treatments, consultations, patient education, shared decision making, and monitoring. One recently proposed model of management scripts highlighted their temporal evolution 8 but was not based on empirical data and focused on activities (reasoning and decisions) within the clinician. Our model, grounded in empirical observations, includes clinicians, patients, and other members of the health care team, and highlights interpersonal communication and shared decision making as central features of the management script.
임상 추론의 한 모델에서는 11가지 관리 과제를 확인했습니다. 12,13 이 모든 것이 동적 상호 작용, 선호도 및 제약 조건의 우선순위 지정, 공유 의사 결정 및 모니터링이라는 특징 하에 우리 모델 안에 포함됩니다. 스크립트, 영업사원 역할, 임상의-환자 관계, 예후 및 조직과 같은 다른 기능도 고유합니다.
One model of clinical reasoning identified 11 management tasks. 12,13 All these are encompassed in our model under the features of dynamic interplay, prioritization of preferences and constraints, shared decision making, and monitoring. Other features in our model (such as scripts, salesperson role, clinician–patient relationship, prognostication, and organization) are unique.
또한 저희의 관리 추론 모델은 의료 의사 결정의 수학적 모델에 관한 방대한 문헌(예: 의사 결정 분석, 20-22 분석 계층 구조 프로세스, 23 관리 임계값, 24 및 선택의 경제 모델 25-27)을 보완합니다. 이러한 모델은 불확실성, 감정, 다양한 발생 확률 또는 시기, 경쟁하는 우선순위 등의 맥락에서 의사 결정에 관한 중요한 원칙을 설명해 왔습니다. 일반적인 수준에서 이러한 수학적 모델과 트위터의 경영 추론 모델에는 목표 정의, 옵션 식별, 혜택, 위험, 선호도에 따른 옵션 평가의 단계가 모두 포함되어 있다는 점에서 어느 정도 유사성이 있음을 인정할 수 있습니다. 그러나 수학적 모델은 이론을 발전시키거나 관리 지침 또는 의사결정 보조자료를 준비하는 등 연구 또는 배후에서 28 가장 유용해 보이는 반면, 트위터의 경영추론 모델은 병상에서의 상호작용을 강조합니다. 우리는 의사결정 모델과 관리 추론이 상호 근거를 마련하고, 입증하고, 서로를 조명할 수 있을 것으로 기대합니다.
Our model of management reasoning also complements the vast literature on mathematical models of medical decision making (such as decision analysis, 20–22 the analytical hierarchy process, 23 management thresholds, 24 and economic models of choice 25–27). Such models have elucidated important principles regarding decisions in the context of uncertainty, emotion, varying probability or timing of occurrence, and competing priorities. At a general level, we acknowledge some similarity between these mathematical models and our model of management reasoning as both have stages of goal definition; identification of options; and evaluation of options based on benefits, risks, and preferences. However, mathematical models seem most useful in research or behind the scenes 28 (e.g., advancing theory or preparing management guidelines or decision aids), whereas our model of management reasoning emphasizes interactions at the bedside. We envision that decision-making models and management reasoning could mutually ground, substantiate, and illuminate one another.
시사점
Implications
이전의 개념적 모델을 바탕으로1,2 우리는 관리 추론의 7가지 새로운 특징을 확인했습니다(표 1). [관리 스크립트의 중심 역할]과 [질병 특이적 지식] 및 [프로세스 지식]의 중요성은 이 모델에 특히 두드러지게 추가된 사항입니다. 또한 관리 추론의 시간적 진화를 개괄하는 개념적 모델을 제안하고(그림 1) 진단 추론과 관리 추론의 구분을 더 명확하고 정교하게 만들었습니다(표 1). [임상의와 환자의 관계 구축] 및 [인카운터의 조직화]와 같은 일부 기능은 추론과 무관해 보일 수 있지만, 이러한 활동은 임상의가 말이나 행동에 대한 선택을 요구하며, 이는 결국 인지(추론) 과정을 의미합니다.
Building on our prior conceptual model, 1,2 we have identified 7 new features of management reasoning (Table 1). The central role of the management script and the importance of both illness-specific and process knowledge are particularly salient additions to this model. We have also proposed a conceptual model outlining the temporal evolution of management reasoning (Figure 1) and sharpened and elaborated the distinctions between diagnostic and management reasoning (Table 1). Some features, such as building the clinician–patient relationship and organization of the encounter, may appear unrelated to reasoning; however, such activities require clinicians to make choices about their words or actions, which in turn implies a cognitive (reasoning) process.
이러한 관찰 결과는 [관리 추론]을 [대인 상호작용(협상)]으로 개념화한 이전의 연구 결과를 입증합니다. 1,2 이 발견은 진단 추론에 대한 많은 연구에서 진단에 통합된 일련의 정보에서 개별 환자를 제외하는 경우가 많은 것과는 상당히 대조적입니다. 임상의는 정보(예: 진단, 환자 선호도, 시스템 제약)를 수집하고, 협상하고, 가르치고, 안내하고, 동기를 부여/판매하면서 최종 계획을 '추론'해야 합니다. 이러한 활동은 [한 명의 의료진 내부]에서만 이루어지는 것이 아니라 [의료진, 환자 및 다른 사람들 사이의 공간]에서 이루어집니다. 이러한 관찰은 앞서 자세히 설명한 바와 같이 의료 전문가의 교육 및 평가에 이론적, 실제적 의미를 지니고 있습니다29,30. 1
Our observations substantiate our previous conceptualization of management reasoning as an interpersonal interaction (negotiation). 1,2 This finding is in considerable contrast to many studies of diagnostic reasoning, which often remove the individual patient from the array of information incorporated into a diagnosis. Clinicians must gather information (e.g., diagnosis, patient preferences, system constraints), negotiate, teach, guide, and motivate/sell as they “reason” their way to a final plan. These activities occur in the space between clinician, patient, and others—not exclusively within the clinician. This observation has both theoretical and practical implications for the education and assessment of health professionals, 29,30 as we have previously elaborated. 1
이러한 특징과 모델은 교육에 대한 추가적인 시사점을 제공합니다.
- 첫째, 관리 추론에서 관리 스크립트의 지배적인 역할은 이러한 [인지적 표상을 배양하는 데 집중해야 할 필요성]을 시사합니다. 또한 관리 스크립트 자체는 의료 전문가를 교육하는 데 유용한 도구가 될 수 있는데, 예를 들어 임상의가 환자 사례에 대한 접근 방식에 대해 "소리 내어 생각"할 때 유용할 수 있습니다. 17
- 둘째, '일을 처리하는 방법'에 대한 실용적인 지식이 의료진에게 유용한 기술이라는 사실은 오랫동안 인정되어 왔지만, 이제는 [과정 지식도 관리 추론(즉, 임상의와 환자 간 협상의 일부)에서 중요한 역할]을 한다는 것을 인식하고 있습니다. 과정 지식은 환자 중심 교육, 세일즈맨십(수사학 분야와 설득에 대한 통찰력 31에서 차용한 것일 수 있음), 신뢰 형성, 예후 예측과 같은 기술과 함께 의료 전문가 교육 및 평가에서 보다 전략적으로 강조할 가치가 있습니다.
- 셋째, 우리의 연구 결과는 관리(진단) 추론에 대해 고유하거나 다른 빈도로 요구되는 기술의 개발 및 평가와 관련하여 이전에 제안된 시사점을 경험적으로 확인합니다. 1
These features and model have additional implications for education.
- First, the management script’s dominant role in management reasoning suggests the need to focus on cultivating these cognitive representations. The management script itself may also serve as a useful tool for teaching health professionals, such as when master clinicians “think aloud” about their approach to a patient case. 17
- Second, although it has long been accepted that practical knowledge of how to “get things done” is a useful skill for practitioners, we now recognize that process knowledge also plays a crucial role in management reasoning (i.e., as part of the clinician–patient negotiation). Process knowledge, along with skills such as patient-directed teaching, salesmanship (perhaps borrowing from the field of rhetoric and its insights on persuasion 31), engendering trust, and prognostication, may merit more strategic emphasis in the education and assessment of health professionals.
- Third, our findings empirically confirm previously proposed implications regarding the development and assessment of skills that are likely unique or required with different frequencies for management (vs diagnostic) reasoning. 1
또한 임상 실무에 대한 시사점도 확인했습니다. 임상의의 일상 업무를 지원하기 위해 수많은 도구가 개발되었습니다. 관리 추론의 주요 특징과 해당 모델은 진료 수요를 충족하는 데 있어 이러한 도구의 관련성과 포괄성을 체계적으로 평가하는 데 도움이 됩니다.
- 예를 들어,
- [진료 지침]과 [컴퓨터 기반 지식 리소스]는 [질병 특이적 지식] 문제를 다루고,
- [치료 경로와 프로토콜]은 치료의 [프로세스 지식]을 다루며,
- [의사 결정 보조 도구]는 [공유 의사 결정]을 돕고,
- [기타 컴퓨터 도구]는 [모니터링과 후속 조치]를 지원할 수 있습니다.
- 반대로 역동적인 상호 작용, 세일즈맨십, 임상의와 환자의 관계, 진료 조직, 스크립트 개발을 지원하는 도구는 덜 보편화되어 있습니다.
We also recognize implications for clinical practice. Numerous tools have been developed to support clinicians in their daily routine. The key features and corresponding model of management reasoning facilitate an organized appraisal of the relevance and comprehensiveness of such tools in meeting practice demands.
- For example,
- practice guidelines and computer-based knowledge resources address issues of illness-specific knowledge;
- care pathways and protocols address process knowledge;
- decision aids help shared decision making; and
- other computer tools can support monitoring and follow-up.
- Conversely, tools to support dynamic interplay, salesmanship, clinician–patient relationships, encounter organization, and script development are less prevalent.
마지막으로, 경험적 데이터에 기반을 두고 있지만, 이번 연구 결과는 아직 잠정적이고 다소 개념적인 수준에 머물러 있으므로 추가 연구가 필요합니다.
- 먼저, 관리 스크립트의 역할과 개발을 이해하기 위한 이론적 및 실증적 연구를 제안합니다: 스크립트는 어떻게 활성화, 선택, 인스턴스화되나요? 18 한 스크립트가 다른 스크립트에 대한 헤게모니를 확보하는 방법은 무엇인가요? 어떤 스크립트 기능이 필수적이며, 추론 작업을 간소화하기 위해 (적어도 교육 초기에는) 어떤 기능을 할인할 수 있을까요? 이번 연구 결과는 일반적인 프레임워크("나쁜 소식 속보")를 반영하는 메타 스크립트, 특정 질병에 초점을 맞춘 기본 스크립트, 환자 또는 상황에 맞게 조정된 하위 스크립트로 구성된 가능한 스크립트 계층 구조를 제안하며, 이러한 제안은 확인과 정교화가 필요합니다.
- 둘째, 입원 환자 진료, 종단적(반복적) 상호작용, 비대면 진료(전화 통화, 전자 통신, 환자의 개입 없이 의료 기록 검토), 다른 의료진과의 상호작용 등 다양한 환경에서 관리 추론이 어떻게 나타나는지 살펴보는 추가 연구를 제안합니다. 다양한 경력을 가진 임상의(예: 학생, 대학원 수련의, 일반의, 전문의)를 대조하는 연구도 통찰력을 얻을 수 있습니다.
- 셋째, 이 연구에서는 인종, 민족, 성별이 임상의와 환자 간의 상호작용에 어떤 영향을 미치는지 조사하지 못했습니다. 이러한 특징과 기타 특징을 의도적으로 탐구한다면 관리 추론에 대한 이해를 높이고 잠재적인 관리 불균형을 완화하는 데 도움이 될 것입니다.
- 넷째, 많은 관리 추론이 임상의 내부가 아닌 개인 간의 공간에서 발생한다는 주장을 검증하는 연구가 필요합니다.
- 다섯째, 저희처럼 관찰 가능한 행동에 국한하지 않고 실제 인지 과정을 조명할 수 있는 새로운 연구 방법의 적용을 권장합니다.
Finally, although grounded in empirical data, our findings remain tentative and somewhat conceptual and thus demand further research.
- First, we propose theoretical and empirical work to understand the role and development of management scripts: How are scripts activated, selected, and instantiated? 18 How does one script gain hegemony over another? What script features are essential, and what features could be discounted (at least early in training) to simplify the reasoning task? Our findings suggest a possible script hierarchy, with meta-scripts reflecting general frameworks (“breaking bad news”), primary scripts focusing on a given illness, and subscripts being tailored to the patient or context; this suggestion warrants confirmation and elaboration.
- Second, we suggest further research exploring how management reasoning manifests in different settings, such as inpatient care, longitudinal (repeated) interactions, non–face-to-face care (telephone calls, electronic communication, and review of medical records without patient involvement), and interactions with other health care team members. Research contrasting clinicians of varying experience (e.g., students, postgraduate trainees, generalists, specialists) would also be insightful.
- Third, this study could not examine how race, ethnicity, or gender influences clinician–patient interactions; intentionally exploring these and other features would enhance our understanding of management reasoning and help mitigate potential management disparities.
- Fourth, we need research that examines our claim that much management reasoning occurs in the space between individuals vs within the clinician.
- Fifth, we encourage application of novel research methods permitting illumination of actual cognitive processes rather than restricting to observable behaviors as we did.
Management Reasoning: Empirical Determination of Key Features and a Conceptual Model
PMID: 35830267
Abstract
Purpose: Management reasoning is a critical yet understudied phenomenon in clinical practice and medical education. The authors sought to empirically identify key features of management reasoning and construct a model describing the management reasoning process.
Method: In November 2020, 4 investigators each reviewed 10 video clips of simulated outpatient physician-patient encounters and used a coding form to document key features and insights related to management reasoning. The team used a constant comparative approach to distill 120 pages of raw observations into an 18-page list of management tasks, processes, and insights. The team then had a series of discussions to iteratively refine these findings into a parsimonious model of management reasoning.
Results: The investigators empirically identified 12 distinct features of management reasoning: contrasting and selection among multiple solutions; prioritization of patient, clinician, and system preferences and constraints; communication and shared decision making; ongoing monitoring and adjustment of the management plan; dynamic interplay among people, systems, and competing priorities; illness-specific knowledge; process knowledge; management scripts; clinician roles as patient teacher and salesperson; clinician-patient relationship; prognostication; and organization of the clinical encounter (sequencing and time management). Management scripts seemed to play a prominent and critical role. The model of management reasoning comprised 4 steps: instantiation of a management script, identifying (multiple) options and beginning to teach the patient, shared decision making, and ongoing monitoring and adjustment. This model also conceives 2 overarching features: that management reasoning is personalized to the patient and that it occurs between individuals rather than exclusively within the clinician's mind.
Conclusions: Management scripts constitute a key feature of management reasoning, along with teaching patients about viable options, shared decision making, ongoing monitoring and adjustment, and personalization. Management reasoning seems to be constructed and negotiated between individuals rather than exclusively within the clinician.