EPA 프레임워크의 논리: 스코핑 리뷰 (Med Educ, 2022)
The logic behind entrustable professional activity frameworks: A scoping review of the literature
Marije P. Hennus1 | Marjel van Dam2 | Stephen Gauthier3 | David R. Taylor3 | Olle ten Cate4
1 소개
1 INTRODUCTION
신뢰할 수 있는 전문 활동(EPA)은 역량 적용을 위한 명확한 목적을 제공하는 보건 전문가 교육에서 빠르게 진화하는 개념을 나타낸다.
- [역량]은 교육자가 임상 실습에 제공하는 능력을 반영하는 반면,
- EPA는 이러한 역량이 필요한 의료의 과제이다.
EPA는 개별적인 직업별 작업(또는 작업 묶음)으로, 일반적으로 식별 가능한 환자 치료 행위이며, 여기에는 여러 역량(중요한 지식, 적절한 기술 및 태도 포함)의 통합이 필요하다. 학습자는 기본적으로 이러한 작업을 수행함으로써 EPA를 위해 훈련되고 있으며, 처음에는 엄격한 감독 하에 점차 자율적으로 훈련되고 있다. EPA에서 유능해지기 위한 진행은 소위 [위탁-감독 척도]를 따른 학습자의 여정을 반영한다. 이러한 척도는 학습자가 안전한 환자 치료를 보장하기 위해 필요한 감독 수준을 포착하는 것을 목표로 한다. 역량이 증가함에 따라 감독 강도를 시간이 지남에 따라 신중하게 낮춰야 한다. 전체적으로 본다면, 일련의 EPA는 전문 교육을 위한 커리큘럼의 틀을 정의하고 알리기 위해 사용될 수 있으며, 실제로 전문직의 핵심 활동을 반영한다. 이와 같이 EPA 기반 커리큘럼은 임상 훈련과 평가를 임상의가 일상 업무에서 실제로 수행하는 작업과 연결할 수 있는 잠재력을 가지고 있다. 결과적으로, 점점 더 많은 수의 대학원 의학 훈련 프로그램이 커리큘럼을 재설계하기 위해 그것들을 사용하기 시작했다.
Entrustable professional activities (EPAs) represent a rapidly evolving concept in health professionals' education that offers clear purpose for the application of competencies. Whereas
- competencies reflect the capabilities trainees bring to clinical practice,1
- EPAs are the tasks of health care for which these competencies are needed.
An EPA is a discrete profession-specific task (or bundle of tasks), typically an identifiable act of patient care, which requires the integration of multiple competencies (including vital knowledge, appropriate skills and attitudes).2, 3 Learners are essentially being groomed for EPAs by performing these tasks, initially under strict supervision and gradually more autonomously. Progression towards becoming competent in an EPA reflects a learner's journey along so-called entrustment-supervision scales. These scales aim to capture the level of supervision a learner requires to ensure safe patient care; with increasing competence, the intensity of supervision should be carefully lowered over time.4, 5 Taken collectively, a set of EPAs can be used to define and inform the framework of a curriculum for specialty training and, in fact, reflects the profession in its core activities. As such, an EPA-based curriculum has the potential to link clinical training and assessment to the work that clinicians actually do in daily practice.6 Consequently, an increasing number of postgraduate medical training programmes have begun using them to redesign their curricula.7, 8
EPA는 이해관계자 간에 내용 타당성과 수용성을 모두 제공할 수 있는 신중하게 구성된 접근방식을 요구한다. EPA의 개발 과정을 안내하는 데 도움이 되는 지침이 존재하지만, [예비 프레임워크 초안을 작성하기 위해 사용할 논리]를 결정하는 것은 중요하고 종종 어려운 첫 번째 단계를 제시한다. EPA 프레임워크의 논리는 개발자가 직업의 관행을 전문 작업 단위로 분해하기 위해 사용하는 관점으로 정의할 수 있다. 현존하는 문헌에서 발견된 보고된 접근법에는 다음이 포함된다.
- 역할 ('다른 분야의 컨설턴트 전문가 역할'),
- 절차 ('일반적인 폐 및 중환자 치료 절차를 안전하고 효율적으로 수행')
- 질병 관리 ('패혈증 환자 관리')
- 환자 범주 ('청소년 의료') 및
- 기능 ('외래 환자 클리닉 실행')
EPAs require a carefully constructed approach that can deliver both content validity and acceptance among stakeholders.9 Although guidelines exist to help guide the developmental process of EPAs,3, 10 deciding what logic to use to draft a preliminary framework poses a crucial and often difficult first step. The logic of an EPA framework can be defined as the perspective used by the developers to break down the practice of a profession into units of professional work.11 Reported approaches found in extant literature include
- roles (‘Act as the consultant specialist for other disciplines’),
- procedures (‘Safely and efficiently perform common pulmonary and critical care procedures’),
- disease management (‘Management of a patient with sepsis’),
- patient categories (‘Adolescent healthcare’) and
- functions (‘Running the outpatient clinic’).7, 8
유사한 분야에서도 서로 다른 접근법이 사용되어 왔다. 예를 들어 폐 및 중환자 의료에 대한 [미국] 펠로우십 교육을 위한 '기능' 및 '역할 기반' EPA를 [네덜란드] EPA의 보다 '질병 관리' 지향 EPA 프레임워크와 비교한다. '모든 사람에게 맞는 하나의 크기'라는 격언은 EPA 프레임워크의 개발에 분명히 적용되지 않는다. 설정, 목적, 교육 프로그램에 기반한 맞춤화가 불가피해 보인다.
Even within similar disciplines, different approaches have been used. Compare for instance the predominantly ‘function-’ and ‘role-based’ EPAs for American Fellowship Training in Pulmonary and Critical Care Medicine12 with the more ‘disease management’ orientated EPA-framework of their Dutch counterparts.13 The ‘one size fits all’ adage clearly does not hold true for the development of EPA frameworks; customisation based on setting, purpose and/or training programme seems inevitable.
이 범위 문헌 검토는 대학원 의학 교육 및 펠로우십 프로그램에 걸쳐 EPA 프레임워크 개발에 사용된 지배적인 논리와 추가 연구를 위한 영역을 강조할 뿐만 아니라 EPA 개발을 위한 모범 사례 지침을 잠재적으로 알리기 위한 그들의 합리성을 매핑하는 것을 목표로 했다.
This scoping literature review aimed to map the dominant logics used in the development of EPA frameworks across postgraduate medical education and fellowship programmes and their rationales to potentially inform best practice guidelines for EPA development in addition to highlighting areas for further research.
2 방법
2 METHODS
2.1 설계
2.1 Design
주제에 대한 기존 연구 결과를 수집, 평가 및 제시하는 반복적이고 유연한 방법인 범위 검토가 수행되었다. 우리는 철저한 검토를 추구하지 않고 지배적인 EPA 논리를 식별하고 매핑하기 위해 시작했기 때문에 체계적인 검토 대신 범위를 사용했다. 이는 체계적 검토 및 메타 분석을 위한 선호 보고 항목(PRISMA)의 범위 검토 확장에 따라 보고되었다.
A scoping review, an iterative and flexible method to collect, evaluate and present findings from existing research on a topic,14 was performed. We used a scoping, instead of a systematic review, as we did not seek to be exhaustive but set out to identify and map dominant EPA logics.15 This was reported in accordance with the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA)'s extension for Scoping Reviews.16
2.2 검색 전략
2.2 Search strategy
문헌 본문의 범위를 평가하기 위해, 우리는 Khalil 등으로부터 채택된 스코핑 리뷰에 대한 증거 기반 다단계 접근법을 사용했다. 2005년 1월부터 2020년 12월까지의 연구는 타당성과 폭 및 포괄성의 균형을 맞추기 위해 3단계 문헌 검색을 사용하여 확인되었다.
- 1단계는 제목과 초록에 포함된 텍스트 단어(위탁가능 프로페셔널 활동*)를 2명의 저자(MH, MD)가 독립적으로 선별하여 MEDLINE과 Embase에 대한 제한된 검색으로 구성되었다.
- 두 번째 단계는 이 텍스트 단어들을 포함된 모든 데이터베이스(구글 스콜라, 스코푸스, 웹 오브 사이언스 추가)에서 검색어로 사용했다. 이러한 데이터베이스는 EPA에 대한 문헌을 포괄하고 함께 고려할 때 가능한 포괄적으로 선택되었다. 이 검토에서 사용된 검색 구문에 대한 자세한 내용은 지원 정보(부록 1)에서 확인할 수 있습니다.
- 세 번째 단계에는 확인된 모든 보고서 및 추가 연구를 위한 논문의 참조 목록 분석이 포함되었다.
To assess the extent of the body of literature, we used an evidence-based multistage approach to scoping reviews adapted from Khalil et al.17 Studies from January 2005 until December 2020 were identified using a three-step literature search in order to balance feasibility with breadth and comprehensiveness.
- The first stage consisted of a limited search of MEDLINE and Embase by screening of text words (Entrustable Professional Activit*) contained in the title and abstract by two authors (MH, MD) independently.
- The second stage used these text words as search terms across all included databases (adding Google Scholar, Scopus and Web of Science). These databases were chosen to span literature on EPAs and to be as comprehensive as possible when considered together. The full details of the search syntaxes used in this review can be found in the Supporting Information (Appendix 1).
- The third stage included analysis of the reference lists of all identified reports and articles for additional studies.
2.3 연구 선정
2.3 Study selection
2.3.1 포함 기준
2.3.1 Inclusion criteria
포함시킬 수 있는 연구들은 다음과 같은 연구였다.
- (i) 개발된 EPA 프레임워크의 논리를 설명하거나 최소한 EPA 제목을 제공한다.
- (ii) 대학원 의학 교육 또는 펠로우십 프로그램 및
- (iii) 영어로 쓰여졌다.
포함된 연구는 대조, 요약 및 결과 보고가 가능하도록 표와 서술 형식으로 차트화되었습니다.
Eligible for inclusion were studies that
- (i) either described the logic of developed EPA frameworks and/or provided at least the titles of EPAs for
- (ii) a postgraduate medical education or a fellowship programme and
- (iii) were written in English.
Included studies were charted in a tabular and narrative format allowing for collation, summarising and reporting of results.
2.3.2 배제 기준
2.3.2 Exclusion criteria
다음과 같은 문헌은 제외되었다.
- (i) 주 원고, 보충 데이터 및 온라인 보충 데이터에 EPA 프레임워크를 제공하지 않아 기본 논리를 분석할 수 없었다.
- (ii) EPA의 규모와 복잡성의 결정에 영향을 미칠 수 있으므로 (하위) 전문 교육 프로그램의 단일 EPA 또는 일부 EPA에 대해서만 설명한다.
- (iii) 학부생, 대학원 의학 교육(GME)에 입학하는 신규 졸업생의 평가 및 기타 보건 전문직(예: 간호사, 수의사, 약사)을 위한 EPA 프레임워크를 제공했다.
Papers were excluded if they
- (i) did not provide an EPA framework in either the main manuscript, supplemental data and/or online supplemental data, making it impossible to analyse the underlying logic;
- (ii) described only a single EPA and/or EPAs for a part of a (sub)specialty training programme as this may have impacted decisions of size and complexity of the EPAs; and/or
- (iii) offered an EPA framework for undergraduates, for the evaluation of newly graduated students entering graduate medical education (GME) and/or for other health professions (e.g., nurses, veterinarians and pharmacists).
2.4 선별과정
2.4 Screening process
두 명의 저자(MH, MD)는 검색 과정에서 반환된 모든 제목과 초록을 독립적으로 선별하여 포함 기준을 충족하지 않는 논문을 거부하였다. 논문을 포함하거나 제외하는 결정을 제목 및/또는 요약에 기초하여 내릴 수 없는 경우, 그 결정을 알리기 위해 전문에 접근했다. 현시점에서 불확실성이 여전했다면 제3의 저자(SG)가 심판 역할을 해 합의를 이끌어냈다.
Two authors (MH, MD) independently screened all titles and abstracts returned during the search process, rejecting papers that did not meet the inclusion criteria. If a decision to either include or exclude a paper could not be made based on title and/or abstract, the full text was accessed to inform the decision. If uncertainties still remained at this point, a third author (SG) served as referee to help reach consensus.
2.5 논리의 분류
2.5 Categorisation of logic
심사 과정 동안 데이터의 반복 분석(종종 근거 분석이라고 함)을 이용한 귀납적 코딩 스타일을 두 명의 저자(MH, MD)가 독립적으로 사용하여 코드 초안을 작성했다. 이후 팀 미팅(MH, MD, SG, DT, OtC)을 개최하여 10편의 논문의 파일럿 코딩에 대해 논의하고, 이후 데이터 코딩과 추출을 MH와 MD가 수행하는 코딩 절차를 미세 조정하였으며, 두 저자는 제3저자(SG)와 함께 논문 내 포함된 모든 논문과 코딩된 EPA 로직을 독립적으로 읽고 재독하였으며, 사용된 논리에 대한 합의가 즉시 이루어지지 않았을 때 심판 역할을 맡았습니다.
During the screening process, an inductive coding style using iterative analysis of the data (often referred to as Grounded Analysis) was be used by two authors (MH, MD) independently resulting in draft codes.18 Hereafter, a team meeting (MH, MD, SG, DT and OtC) was held to discuss a pilot coding of 10 papers and to fine-tune the coding procedure, following which data coding and extraction were performed by MH and MD. Both authors independently read and re-read all of the included papers and coded EPA logics within the papers with the third author (SG) serving as referee for papers when consensus on the logic used was not immediately reached.
3 결과
3 RESULTS
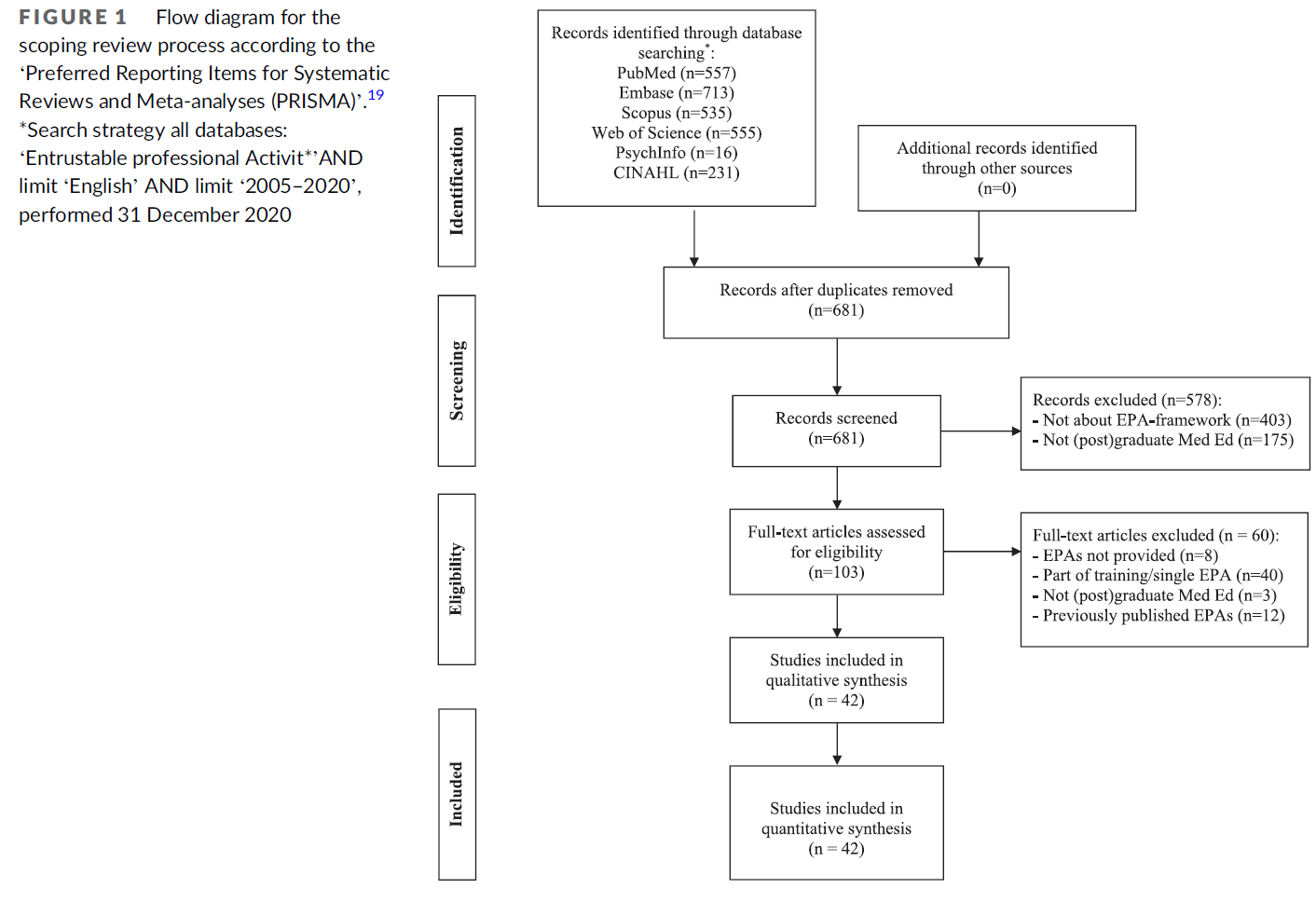
검색전략은 총 2607개의 인용을 확인하였으며, 중복제외 후 681개의 인용을 도출하였다. 이 중 42편의 논문이 이 검토에 포함되도록 선택되었다(PRISMA 다이어그램의 경우 그림 1 참조).
In total, the search strategy identified 2607 citations, resulting in 681 citations after de-duplication. Of these, 42 papers were selected for inclusion in this review (for a PRISMA diagram see Figure 1).
3.1 EPA 프레임워크의 논리를 설명하는 논문의 일반적인 특성
3.1 General characteristics of papers describing the logic of EPA frameworks
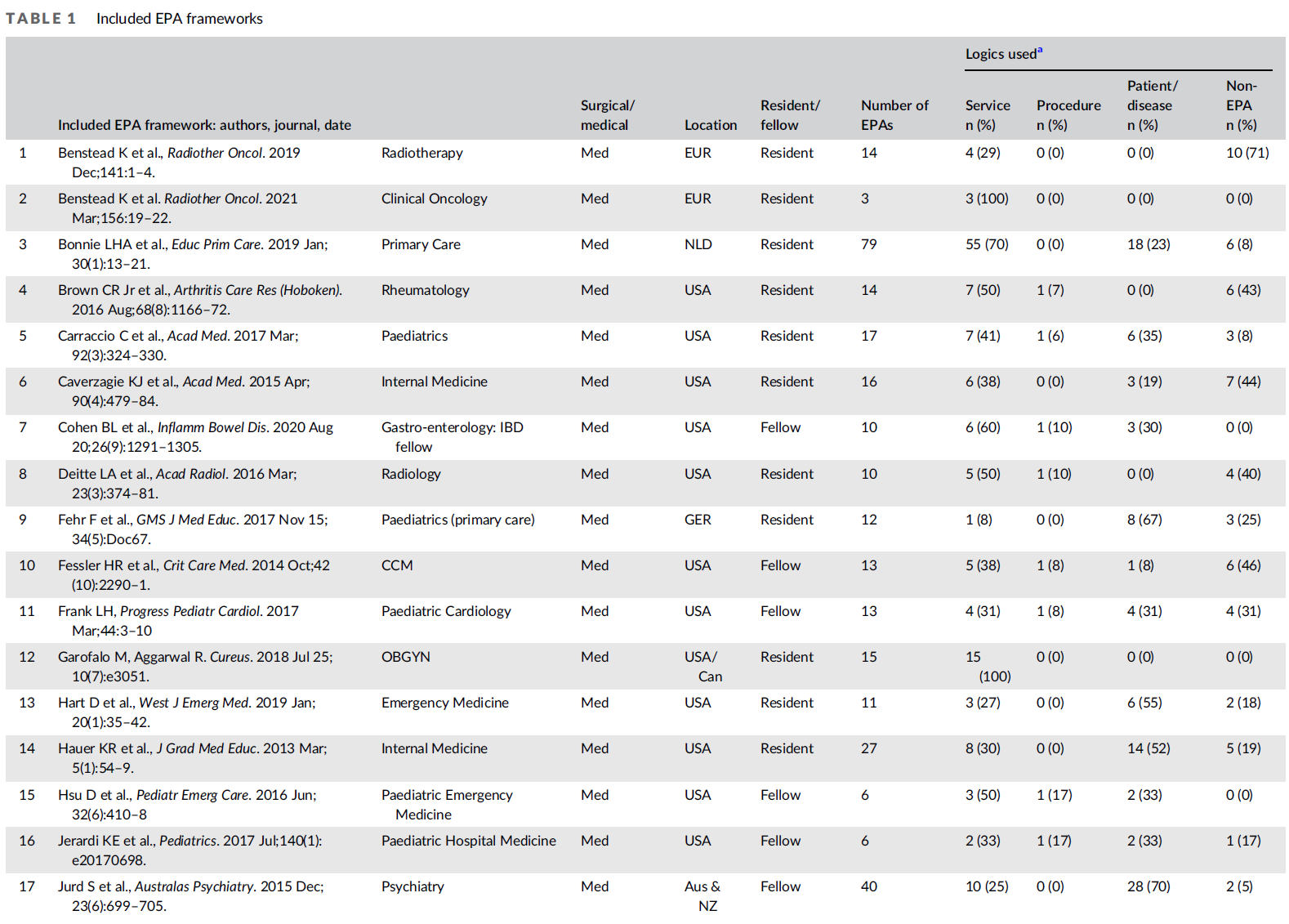
Microsoft Excel 버전 16.54(표 1)를 사용하여 관련 연구 데이터(예: 출판 연도, 국가, 전문성 및 교육 수준)를 추출하고 표로 작성했습니다. 포함된 논문의 주요 특성은 표 2에 요약되어 있습니다. 대학원 또는 펠로우십 프로그램에 대한 EPA 프레임워크의 논리를 설명하는 대부분의 연구는 미국(n = 22; 52%), 캐나다(n = 6; 14%), 네덜란드(n = 4; 10%)(표 2)에서 수행되었다. 보고된 전공의 범위 전체에서 가정의학과(n=4;10%), 내과학과(n=4;10%), 소아과(n=3;7%), 정신과(n=3;7%)가 가장 많았다. 또한 프레임워크의 69%는 전공의용(n = 29), 31%는 전임의용(n = 13)으로 개발되었다.
Relevant study data (e.g., publication year, country, specialty and level of training) were extracted and tabulated using Microsoft Excel Version 16.54 (Table 1). Key characteristics of included papers are summarised in Table 2. Most studies describing the logic of EPA frameworks for postgraduate or fellowship programmes were conducted in the United States (n = 22; 52%), Canada (n = 6; 14%) and the Netherlands (n = 4; 10%) (Table 2). Across the reported range of specialties, family medicine (n = 4; 10%), internal medicine (n = 4; 10%), paediatrics (n = 3; 7%) and psychiatry (n = 3; 7%) were the most common. Furthermore, 69% of the frameworks had been developed for residency (n = 29), 31% for fellowships (n = 13).



3.2 다양한 EPA 프레임워크 로직
3.2 Variety of EPA-framework logics
총 862개의 EPA가 EPA 프레임워크(범위 3-79)당 14개의 EPA의 중위수로 42개 조항에 설명되었다(표 1). 데이터의 반복 분석을 사용한 귀납적 코딩 스타일을 기반으로 다음 논리가 확인되었습니다(예시).
- 1) 임상 서비스를 포함한 서비스 제공: 직접('중상환 신생아의 영양 요구 관리') 및 간접 환자 치료('가족 회의 촉진') 및
비임상 의료 서비스('혈액 성분 수혈과 관련된 부작용 평가 및 보고') - 2) 프로시져 ('삽관, 기관지경, 흉부천자, 중심 정맥 카테터 배치 및 초음파를 포함한 일반적인 중환자 치료 절차 수행' 및
- 3) 질병 또는 환자 그룹('비감염성 질염성 질염 환자 식별 및 관리') (표 1)
A total of 862 EPAs were described in the 42 articles with a median of 14 EPAs per EPA framework (range 3–79) (Table 1). Based on an inductive coding style using iterative analysis of the data, the following logics were identified (with examples):
- 1) service provision including clinical services for direct (‘Managing nutritional needs of critically ill newborns’) and indirect patient care (‘Facilitating family meetings’) as well as non-clinical health care services (‘Evaluating and reporting adverse events involving the transfusion of blood components’);
- 2) procedures (‘Performing common critical care procedures, including intubation, bronchoscopy, thoracentesis, central venous catheter placement, and ultrasound’; and
- 3) disease or patient groups (‘Identifying and managing patients with noninfectious GI luminal disease’) (Table 1).
눈에 띄는 것은, 보고된 모든 EPA의 13%(n = 109)가 의사가 서비스하는 사람들의 의료 요구를 효과적으로 충족시키기 위해 필요한 능력을 기술했다. (예: '평생 학습 참여', '전문적 행동 시연'). 이러한 EPA는 종합적인 위탁 결정에 적합하지 않기 때문에, 이 그룹은 4) 비 EPA로 분류되었다.
Notably, 13% (n = 109) of all reported EPAs described abilities physicians require to effectively meet the health care needs of the people they serve (e.g. ‘Engaging in life-long learning’, ‘Demonstrating professional behavior’). As these EPAs are not suitable for summative entrustment decisions, this group was categorised as 4) non-EPAs.
대부분의 논문(n = 37; 88%)은 EPA 프레임워크 개발에 2개 이상의 논리를 사용했다(표준 = 3, 범위 = 1~4). 질병 또는 환자 그룹과 서비스 제공이 가장 많이 사용된 논리(각각 39%와 37%)였다(표 1).
The majority of papers (n = 37; 88%) used two or more logics in the development of EPA frameworks (median = 3, range = 1–4). Disease or patient groups and service provision were the most common logics used (39% and 37%, respectively) (Table 1).
4 토론
4 DISCUSSION
이 검토에서, 우리는 대부분의 프로그램이 EPA의 프레임워크를 확립하기 위해 [논리의 조합을 사용한다]는 것을 발견했다. 그러한 프로그램의 개발자들이 의도적으로 이러한 분류를 선택했을 수도 있고 아닐 수도 있지만, 많은 사람들은 단지 하나의 논리적 분류를 찾지 않고 최선의 접근법이 무엇인지 알아내는 데 시간을 보냈을 것이다. 지금까지 '최선의' 접근법에 대한 권고안이 제시되지 않았으며, 의료 전문 분야와 다른 보건 전문 교육 프로그램 간의 차이는 방어 가능한 것으로 보인다. 빠르게 확장되는 문헌에 비추어, 우리는 실제로 사용되어 온 지배적인 논리를 탐색하고 EPA 프레임워크를 만들기 위한 새로운 이니셔티브에 유용할 수 있는 권장 사항을 증류하고자 했다.
In this review, we found that most programmes use a mix of logics to establish a framework of EPAs. Whereas the developers of those programmes may, or may not, have deliberately chosen these categorizations, many will have likely spent time to figure what the best approach would be, without finding just one logical categorisation. So far, no recommendations for a ‘best’ approach20 have been offered, and differences between medical specialties, and among other health professions educational programmes, seem defensible. In light of the quickly expanding literature, we sought to explore the dominant logics that have been used in practice and to distil recommendations that may be useful for new initiatives to create EPA frameworks.
4.1 EPA의 광범위한 서비스 범위
4.1 The broad service range of EPAs
EPA를 정의할 때 [EPA의 목적]을 염두에 두는 것이 유용하다. 여러 출판물들은 그것의 정의와 EPA가 역량과 어떻게 다른지 상세히 설명하였다. '전문 실무 단위'로서 EPA는 전문 업무를 개념화하기 때문에 반드시 교육 모델이 될 필요는 없다. 그들은 주로 전문 교육을 위한 커리큘럼을 개발하고 직장 평가 절차를 만드는 데 사용되었다. 그러나 [필수 작업essential tasks]을 정의하는 것이 항상 명확한 것은 아닙니다. 또한, EPA는 고유한 우선 순위, 의무 및 목적을 가진 국가 또는 심지어 [국제 기구]에 의해 점점 더 공식화되고 있다. 이는 지역적으로 EPA를 선택하거나 식별하는 자유를 제한하며 프로그램, 기관 또는 국가를 넘어서는 [총괄적 위임 결정]을 인정하는 역할을 한다. 가까운 장래에 EPA는 예를 들어 관련된 교육생과의 부작용 발생 시 책임에 대한 분쟁이 발생하거나 [의료행위 범위의 정당성]이 위태로울 때 사법기관에 의해 인정될 수 있다. 그것은 자격 증명으로 인정되고, 위탁되고, 인증될 수 있는 전문 실무 단위의 건전한 공식화의 필요성을 강조한다.
In defining EPAs, it is useful to keep their purpose in mind. Multiple publications have elaborated on its definition and how EPAs differ from competencies.3, 10, 21 EPAs, as ‘units of professional practice’, are not necessarily an educational model as they just conceptualise professional tasks.10 They have primarily been used to develop curricula and create workplace assessment procedures for specialty training; however, defining the essential tasks is not always clear-cut. Furthermore, EPAs are increasingly formulated by national or even international bodies with unique priorities, mandates and purposes.22-26 This limits the freedom to choose or identify EPAs locally and serves to acknowledge summative entrustment decisions beyond a programme, institution or country. In a foreseeable future, EPAs may be acknowledged by legal bodies, for example, when disputes arise about accountability in case of adverse events with trainees involved27 or when the legitimacy of a scope of practice is at stake. That stresses the need for a sound formulation of the units of professional practice that can be acknowledged, entrusted and certified as a credential.
최근 몇 년 동안 교육 후 EPA의 잠재적 역할이 더 많은 관심을 받고 있다. 3개의 네덜란드 UMC의 상주 코디네이터는 최근 EPA에게 재인증의 핵심 지위를 줄 것을 간청했다. 또한, EPA의 사용은 어떤 직원이 어떤 의료 특권을 가지고 어떤 훈련을 어떤 수준에서 수행할지 명시하도록 요청하는 'Joint Commission'가 수행하는 것과 같은 [병원 자격 증명 요건]과 자연스럽게 일치fit한다. 이는 EPA의 추가 목적 역할을 한다.
In recent years, the potential role of EPAs after training has received more attention.28, 29 Residency coordinators of three Dutch UMCs recently pleaded to give EPAs a core status in recertification.30 In addition, the use of EPAs naturally fits with requirements of hospital credentialling, such as done by the ‘Joint Commission’,31 which ask to specify which employees have which health care privileges and which tasks are to be performed by which trainees under which level of supervision. This serves as an additional purpose of EPAs.
4.2 주요 논리의 장단점
4.2 Pros and cons of the main logics
EPA 프레임워크 개발을 위한 논리를 선택하는 것은 어려울 수 있다. 각 접근방식은 아래에 논의된 바와 같이 장점과 단점이 있기 때문이다.
The choice of a logic for developing an EPA framework may be difficult, as each approach comes with benefits and drawbacks as discussed below.
4.2.1 서비스 제공
4.2.1 Service provision
[서비스 제공 EPA]는 [일반적으로 임상의의 스케쥴에 포함된 활동]을 반영하므로, 장점은 손쉽게 인식, '지정assigned', 금지prohibited된다. 그것들은 [광범위하고 일반적]이며, 위임 결정은 이러한 서비스 중에 발생할 수 있는 프로시져와 질병에 대한 [적절한 경험]을 전제로 한다. 이로 인해 EPA가 주니어 학습자들에게 덜 적합하게less suitable 된다. EPA '표준 외래 환자 상담'을 예로 들 수 있는데, 이는 보다 상급 의료 교육생에게 논리적이고 적합한 활동이다. 이 EPA에는 의대생에게 적합한 독립적 EPA로서 기능할 수 있는 '의학 이력서 작성' 및 '전체 표준 신체검사 수행'과 같은 활동이 포함될 것으로 추정된다. 또한, [서비스 제공 EPA]는 사례 특이성이 부족할 수 있으며, 결과적으로 감독 임상의가 적용apply하기 어려울 수 있다. 평가 시 표본 추출에 주의하지 않는 한, 이 접근 방식은 또한 특정 EPA에 대한 평가가 포함된 환자의 프레젠테이션 전반에 걸쳐 일반화될 수 있다고 가정한다.
These EPAs reflect activities as they are usually scheduled for clinicians and are therefore easily recognised, ‘assigned’ and/or prohibited. They are broad and general, and entrustment decisions assume adequate experience with procedures and diseases that may be encountered during these services. This makes them less suitable for junior learners.3 Take for example the EPA ‘standard outpatient consultation’, a logical and suitable activity for more advanced medical trainees. This EPA will presumably include activities like ‘taking a medical history’ and ‘performing a full standard physical examination’, activities that in itself may serve as suitable standalone EPAs for medical students. Furthermore, service provision EPAs may lack case specificity and as a result can be challenging for supervising clinicians to apply.6 Unless there is careful attention to sampling in assessment, this approach also presumes assessments for a given EPA can be generalised across included patients' presentation.
4.2.2 프로시져
4.2.2 Procedures
일부 전공 분야의 경우 프로시져(또는 프로시져의 클러스터)가 선호 EPA(예: 내시경 및 수술)가 될 수 있다. 일반적으로 잘 훈련될 수 있는 명확하고 잘 표시된 작업이다. 프로시져를 EPA로 채택하는 위험은 [개별적으로 고려할 때 매우 작거나 좁은 범위의 기술에 초점]을 맞춘다는 것이다. 작고 따라서 많은 절차적 EPA가 본질적으로 문제가 되는 것은 아니지만, 학습자에게 이러한 자격을 부여하기 위한 심각한 [총괄적 위임 결정]의 절차는 까다로운 일이 될 수밖에 없다. 또한, 이러한 소규모 EPA는 신뢰에 대한 여러 조건을 포함하기보다는 [정신운동 능력에만 초점을 좁힐 위험]도 수반한다.
For some specialties, procedures (or clusters of procedures) can be preferred EPAs (e.g. endoscopies and surgeries); they are clear and well-demarcated tasks that generally can be trained well. The risk of adopting procedures as EPAs is that they may be very small when considered individually and that the focus is on a narrow range of skills.3, 6 Small and thus many procedural EPAs are not inherently problematic, but serious summative entrustment decisions to qualify learners for these are bound to lead to cumbersome procedures.3, 6 Furthermore, these small EPAs incorporate the risk that the focus will narrow to psychomotor skills only, rather than including multiple conditions for trust.
4.2.3 질병 또는 환자군
4.2.3 Disease or patient group
[비시술적 전문분야]의 경우 [질병]이 빨리 떠오른다; [질병 X를 가진 환자를 관리하는 것]은 분명한 임무처럼 들린다. 질병이 논리로 나타나는 단점은 [감별 진단이 첫 번째 과제임을 무시하는 것]이다. 또한 질병은 학습자가 취급할 수 있는 공식적인 자격을 얻기보다는 '만난 것'의 체크박스 항목이 될 위험이 있는 [길고 상세한 목록]을 초래할 수 있다. [프로시져 EPA]와 유사하게, 질병에 대한 의료 전문지식을 중심으로 한 [좁은 범위의 역량에 초점]을 맞출 수 있다. 질병을 EPA의 논리로만 사용하는 것은 유용하고 실용적이지 않을 수 있다. 예를 들어 [진단 및 리퍼referral 후 치료가 일반적인 경우]에는 [질병 또는 질병 그룹]이 유용한 논리가 될 수 있다.
For non-procedural specialties, diseases come to mind quickly; managing patients with disease X sounds like a clear task. A draw-back of diseases as a logic is the disregard of differential diagnosis as a first task. Further, diseases may result in long and detailed lists with the risk of becoming checkbox items of what the learner ‘has encountered’ rather than having received a formal qualification to handle.3, 6 Analogously to the procedural EPA, it can focus on a narrow range of competencies centred on medical expertise for a disease. Using diseases only as the logic for EPAs may not be useful and practical. In some cases, diseases or disease groups can be a useful logic, for example, when treatment after diagnosis and referral is common practice.
4.2.4 비EPA
4.2.4 Non-EPAs
우리는 발표된 모든 'EPA'가 종합위탁 결정에 적합한 것은 아니며, 어떤 것은 EPA로서 유용성이 떨어진다고 판단했다. 우리는 모든 EPA의 13%(표 1)를 비 EPA로 분류했으며, 종종 의사가 서비스하는 사람들의 의료 요구를 효과적으로 충족시키는 데 필요한 능력을 설명한다. '평생 학습 참여', '전문적 행동 시연', '환자 안전 강화', '환자 개개인에 대한 옹호' 등이 대표적이다. 이러한 활동을 수행하는 것을 금지하는 것에서 직간접적인 감독 하에 허가하는 것으로의 전환을 상상하는 것은 어렵다. 우리는 훈련에 대한 이러한 목표의 중요성에 이의를 제기하지 않지만, 그것들은 독립적 EPA와는 다른 방식으로 훈련에 통합되어야 한다. EPA로 유용하게 개념화되지 않은 훈련 목표를 다루는 몇 가지 방법이 최근 텐 카테와 슈마허에 의해 제공되었다.
We deemed not all published ‘EPAs’ as suitable for summative entrustment decisions and hence are less useful as EPAs. We qualified 13% (Table 1) of all EPAs as non-EPAs, often describing the abilities physicians require to effectively meet the health care needs of the people they serve. Examples include ‘Engaging in life-long learning’, ‘Demonstrating professional behavior’, ‘Enhancing patient safety’ and ‘Advocating for individual patients’. It is difficult envision the transition from a prohibition to perform these activities to permission to do so with direct or indirect supervision. We do not dispute the importance of these objectives for training, but they should be incorporated in training in a different way than stand-alone EPAs. Several ways to deal with objectives of training that are not usefully conceptualised as EPAs were recently provided by ten Cate and Schumacher.32

이 연구의 몇 가지 한계를 고려해야 한다. 첫째, 의학 대학원 및/또는 동료 훈련 프로그램의 발표된 EPA 프레임워크만 포함되었기 때문에 선택과 출판 편향의 문제가 있다. 네덜란드의 모든 전문 교육 프로그램에서 사용되는 EPA 유형의 요약을 포함하는 최근 논문은 유사한 논리를 발견했으며 부분적인 '회색 문학' 확인으로 볼 수 있다. 우리의 검토에서, 주요 이해관계자 그룹과 관련된 초기 EPA 프레임워크에 대한 근거는 일반적으로 설명되지 않았다. 개발자는 처음부터 시작했거나 통치 기관이나 국가 기관이 부과한 지침과 요구사항을 따랐을 수 있다. 다음으로, 적격 기사들은 외과 전문분야의 거의(n = 2)를 포함하였고, 이는 잠재적으로 논리로서 '구조'를 과소평가하게 만들었다. 그러나 이러한 유형의 논리의 중요성은 네덜란드에서 더 높은 발생률로 뒷받침된다. 보고된 일부 EPA는 둘 이상의 논리 범주로 분류될 수 있다. EPA 세트에 따라 EPA는 한 세트에서는 환자 범주이고 다른 세트에서는 서비스 범주일 수 있다.
Several limitations of this study must be considered. First, there is the issue of selection and publication bias as only published EPA frameworks of medical postgraduate and/or fellow training programmes were included. A recent paper that includes a summary of the types of EPAs used by all specialty training programmes in the Netherlands found similar logics and can be seen as a partial ‘grey literature’ confirmation.26 In our review, the rationales for the initial EPA frameworks as relates to key stakeholder groups were usually not described. Developers may have started from scratch or have followed guidelines and requirements imposed by governing institutions or national bodies. Next, eligible articles included few (n = 2) from surgical specialties, potentially leading to an underestimation of ‘procedures’ as a logic. The importance of this type of logic, however, is supported by its higher occurrence in the Netherlands.26 Some reported EPAs could be categorised in more than one logic category; depending on the set of EPAs, an EPA may be a patient category in the one set and a service in the other.
수용된 권장 사항을 따름으로써 [개선할 수 있는 많은 EPA 제목]을 접했는데, 이는 논리 범주에 대한 의구심을 해소했다. 예를 들어, '검사 결과 전달'은 전문 실무의 독립적 단위로 간주할 가치가 거의 없기 때문에 확실히 더 성숙한 EPA에 내포될 수 있는 조기 교육 EPA일 수 있으며 부정사infinitive로 더 잘 공식화될 수 있다('진단 시험 결과의 소통'). 우리가 했던 [범주화의 한계]는 [full EPA description]에 대한 통찰력을 거의 갖지 못했다는 것이다. 예를 들어, 우리는 '예방'을 비 EPA로 인정했지만, 규격에는 EPA가 서비스 제공 논리에 속하는 것으로 간주하도록 만들 수 있는 매우 구체적인 하위 활동의 번들 또는 목록이 포함되어 있었을 수 있다. 단지 '예방'을 위해 임상의사를 인증하는 것은 종합적인 위탁 결정에 필요한 명확성이 부족하다. 마지막으로, EPA의 효과나 유효성을 설명하는 제한된 연구가 존재하며, 현재까지 우리는 어떤 논리 범주의 우월성을 지지할 이유가 없다. 향후 연구는 일반적인 EPA 사용에 대한 타당성 증거를 제공하는 것뿐만 아니라 설명된 논리의 사용(또는 우월성)을 뒷받침하는 데 초점을 맞춰야 한다.
We encountered many EPA titles that could be improved, if accepted recommendations10 were followed, which we gave the benefit of the doubt for a logic category. For example, ‘Communicates results of exams’ might be an early training EPA that would definitely be nested in a more mature EPA, as it is hardly worth considering it a stand-alone unit of professional practice, and it might be better formulated with an infinitive (‘Communicating diagnostic exam results’). A limitation of our categorisation is that we rarely had insight into the full EPA description. For example, we qualified ‘Prevention’ as a non-EPA, but the specifications might have included a bundle or list of very concrete sub-activities that could have made us consider the EPA as belonging to the service provision logic. Certifying clinicians just for ‘prevention’ lacks the necessary clarity for a summative entrustment decision. Finally, limited studies exist describing the effectiveness or validity of EPAs, and to date, we have no reason to support superiority of any one logic category. Future research should be directed at providing validity evidence for not only the use of EPAs in general but also to support the use (or superiority) of the described logics.
5 결론
5 CONCLUSION
이 연구는 대학원 의학 교육 및 펠로우십 프로그램에 걸쳐 EPA 프레임워크 개발에 사용되는 논리를 매핑하기 시작했다. '서비스 제공', '절차' 및/또는 '질병 또는 환자 그룹'이라는 세 가지 주요 논리가 식별될 수 있다. 각 논리에 대해 명확한 정의는 예, 이점 및 한계와 함께 제공됩니다. EPA에서 직업의 필수 업무를 포착하려고 할 때, 발견된 논리 유형 중 두세 가지를 조합하여 사용하는 것이 가장 적합해 보인다. 이러한 결과는 향후 EPA 프레임워크 개발자에게 유용한 발판을 제공할 수 있다.
This study set out to map the logics used in development of EPA frameworks across postgraduate medical education and fellowship programmes. Three dominant logics could be identified, namely, ‘service provision’, ‘procedures’ and/or ‘disease or patient groups’. For each logic, a clear definition is provided together with examples, benefits and limitations. When trying to capture the essential tasks of a profession in EPAs, the use of a combination of two or three of the types of logic found seems most suitable. These findings may provide helpful scaffolding for future EPA-framework developers.
The logic behind entrustable professional activity frameworks: A scoping review of the literature
PMID: 35388517
PMCID: PMC9542438
DOI: 10.1111/medu.14806
Free PMC article
Abstract
Introduction: Entrustable professional activities (EPAs), discrete profession-specific tasks requiring integration of multiple competencies, are increasingly used to help define and inform curricula of specialty training programmes. Although guidelines exist to help guide the developmental process, deciding what logic to use to draft a preliminary EPA framework poses a crucial but often difficult first step. The logic of an EPA framework can be defined as the perspective used by its developers to break down the practice of a profession into units of professional work. This study aimed to map dominant logics and their rationales across postgraduate medical education and fellowship programmes.
Methods: A scoping review using systematic searches within five electronic databases (Medline, Embase, Google Scholar, Scopus and Web of Science) was performed. Dominant logics of included papers were identified using inductive coding and iterative analysis.
Results: In total, 42 studies were included. Most studies were conducted in the United States (n = 22; 52%), Canada (n = 6; 14%) and the Netherlands (n = 4; 10%). Across the reported range of specialties, family medicine (n = 4; 10%), internal medicine (n = 4; 10%), paediatrics (n = 3; 7%) and psychiatry (n = 3; 7%) were the most common. Three dominant logics could be identified, namely, 'service provision', 'procedures' and/or 'disease or patient categories'. The majority of papers (n = 37; 88%) used two or more logics when developing EPA frameworks (median = 3, range = 1-4). Disease or patient groups and service provision were the most common logics used (39% and 37%, respectively).
Conclusions: Most programmes used a combination of logics when trying to capture the essential tasks of a profession in EPAs. For each of the three dominant logics, the authors arrived at a definition and identified benefits, limitations and examples. These findings may potentially inform best practice guidelines for EPA development.
© 2022 The Authors. Medical Education published by Association for the Study of Medical Education and John Wiley & Sons Ltd.
'Articles (Medical Education) > 임상교육(Clerkship & Residency)' 카테고리의 다른 글
| 신뢰와 위험: 의학교육을 위한 모델 (Med Educ, 2017) (0) | 2022.11.06 |
|---|---|
| EPA 프레임워크의 논리와의 고군분투 (Med Educ, 2022) (0) | 2022.11.06 |
| 간접 환자돌봄의 교육적 가치 최적화하기 (Med Educ, 2022) (0) | 2022.11.01 |
| 내과와 외과에서 교수자와 학습자 정체성의 사회적 구성(Med Educ, 2022) (0) | 2022.10.04 |
| 성격이 중요한가? 일반외과의사로서 내향성과 외향성의 경험과 인식(Teach Learn Med. 2022) (0) | 2022.09.20 |