간접 환자돌봄의 교육적 가치 최적화하기 (Med Educ, 2022)
Optimising the educational value of indirect patient care
Danielle O'Toole1 | Marina Sadik1 | Gabrielle Inglis1 | Justin Weresch1 | Meredith Vanstone1,2

1 소개
1 INTRODUCTION
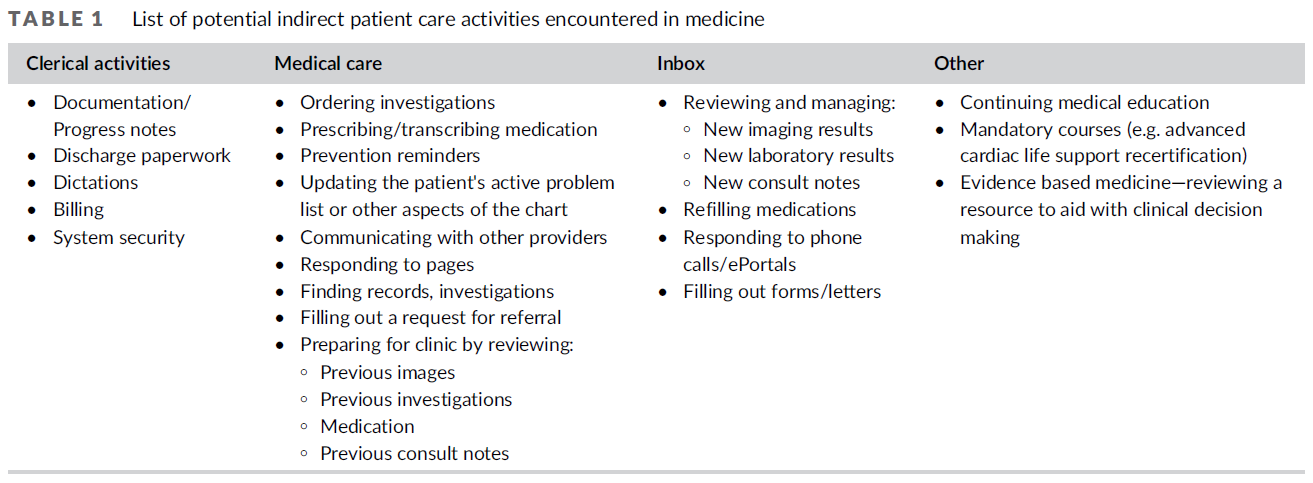
환자 치료의 활동은 환자와 직접 상호작용하는 시간에 국한되지 않는다. 일반적인 의사는 50% 이상의 시간을 간접 환자 치료 활동(IPCA) 또는 대면상호작용이 필요하지 않은 치료 작업에 소비합니다. IPCA는 비동기 업무, 사무실 외부 방문 및 데스크톱 의료라고도 할 수 있다. 표 1은 전자건강기록(EHR)의 '수신함' 관리 등 IPCA의 여러 가지 범주의 예를 제공한다. 여기에는 영상 및 실험실 결과 검토 및 관리, 상담 노트, 양식 작성 및 처방된 의약품의 보충이 포함된다.
The activities of patient care are not confined to time spent directly interacting with a patient. A typical physician spends more than 50% of their time on indirect patient care activities (IPCA), or care tasks that do not require a face-to-face interaction.1-3 IPCA may also be called asynchronous tasks, activities outside of office visits and desktop medicine.4-7 Table 1 provides examples of several different categories of IPCAs, such as managing the ‘inbox’ of the electronic health record (EHR), which includes reviewing and managing imaging and laboratory results, consult notes, completing forms and refilling prescribed medications.
EHR의 채택과 관련하여 IPCA에 들어가는 시간도 증가했다. EHR은 의료 전, 치료 중 및 치료 후 의료 정보에 대한 신속한 액세스를 제공하기 때문에 2008년과 2012년 사이에 임상 실습에 널리 채택되었다. EHR의 잠재적 이점에도 불구하고, 기술의 통합은 과제를 가져왔다.
- 환자-의사 상호 작용의 변화,
- 치료의 의미 있는 측면에서의 주의 산만,
- 의료진에게 사무 업무를 재배포하고 새로운 업무를 창출(예: 의약품 조정, 데이터 입력 및 전자 처방).
일부 활동 유형의 작업량을 줄였습니다. (예: 처방 및 일부 실험실 관련 작업)
어떤 활동의 작업량은 늘어났다. (예: 예방 관리 작업 및 다른 받은 편지함 항목 검토)
이에 따라, EHR은 의료 행위를 재구성하여 IPCA에 소요되는 시간을 전반적으로 증가시켰다.
The time requirements of IPCAs have increased in relation to the adoption of EHRs.1, 8-11 The EHR was widely adopted into clinical practice between 2008 and 2012,7 because it provides rapid access to medical information before, during and after care with aims of improving quality care and safety.12-14 Despite the potential benefits of the EHR, the integration of technology has brought about challenges, including
- altering patient–physician interaction,
- distracting from meaningful aspects of care,
- redistributing clerical tasks to the clinician and creating new tasks (e.g. medication reconciliation, data entry and electronic prescribing).4, 12, 15-18
It has reduced the workload of some types of activities (e.g. prescribing and some lab-related tasks), while increasing others (e.g. preventative care tasks and reviewing other inbox items).3, 7, 19, 20 Accordingly, this technology has re-shaped medical practice, resulting in an overall increase in the time spent on IPCAs.1, 8-11
IPCA는 많은 전문분야와 관련이 있다. 예를 들어, 심장내과, 내과, 정형외과 전문의들도 마찬가지로 시간의 50%를 간접적인 환자 활동에 사용한다. 정신과, 집중치료, 응급의학에서도 같은 경향이 보고되고 있다. 이러한 결과는 호주, 독일 및 영국을 포함하여 EHR 사용이 일반적인 고소득 국가에서 일관된다. IPCA는 특히 가정의에게 부담이 될 수 있다. 가정의학과 의사는 환자의 '메디컬 홈'인 만큼 다른 의사가 지시한 조사와 치료를 검토하고 관리하는 경우가 많아 자주 호출된다. 일반 가정의의의 경우, EHR의 출현은 환자와 함께 보내는 매 시간마다 컴퓨터에서 1~2시간씩, 진료 시간 외(오전 8시~오후 6시)에 소요되는 평균 1.5시간의 추가 EHR 시간을 의미했다.
IPCAs are relevant to many specialties. For example, cardiology, internal medicine and orthopaedic specialists similarly spend 50% of their time on indirect patient activities.3 The same trend has been reported in psychiatry,21 intensive care22 and emergency medicine.23, 24 These findings are consistent across high income countries where EHR use is common, including Australia,25 Germany26 and the United Kingdom.23 IPCAs may be especially taxing for family physicians. As the patient's ‘medical home’, family physicians who are often called to review and sometimes manage the investigations and treatments ordered by other physicians. For the average family physician, the advent of EHRs has meant 1–2 hours on the computer for every hour spent with patients, and an average of 1.5 hours of additional EHR time spent outside of clinic hours (8 AM–6 PM).4, 27
IPCA의 증가하는 부담은 의사의 일과 삶의 균형이라는 지속적인 도전을 악화시켜 직무 만족에 영향을 미치고 번아웃을 증가시킨다. 의학 교육자들은 학습자들이 그들의 경력 전반에 걸쳐 지속 가능한 방식으로 IPCA를 처리할 수 있도록 준비해야 하는 해당 과제에 직면해 있다. 학습자가 이러한 작업을 관리하는 방법을 배우는 것의 중요성을 인식하지 못할 수 있다는 증거가 있으며, 한 연구에서 전공의는 임상 문서 요구 사항이 과도하며, 그로 인해 환자 치료에 직접 참여할 수 있는 시간을 단축하고 더 가치 있다고 인식되는 교육 활동에 참여할 수 있는 기회가 줄었다고 보고했다. [직무 만족도와 일과 삶의 균형을 모두 유지하면서, 고품질의 환자 치료의 균형을 유지하는 방식으로 IPCA를 관리하는 방법]을 배우는 것이 중요함에도 불구하고, 이 분야의 교육자들을 지도하기 위한 교육 연구는 거의 수행되지 않았다. 훈련에서 이러한 IPCA의 영향과 이 중요한 교육을 가장 잘 제공하는 방법을 이해하는 것은 주민들이 이 중요한 역량을 획득하도록 돕는 중요한 부분이다.
The growing burden of IPCAs exacerbates the perennial challenge of work-life balance for physicians, affecting job satisfaction, and increasing burnout.28-35 Medical educators face the corresponding task of preparing learners to handle IPCAs in a sustainable way throughout their career. There is evidence that learners may not appreciate the importance of learning how to manage these tasks, with residents in one study reporting that clinical documentation requirements are excessive, compromising time to participate in direct patient care and decreasing opportunities to participate in educational activities perceived as more valuable.36 Despite the importance of learning how to manage IPCAs in a manner that balances high quality patient care while maintaining both job satisfaction and a work–life balance, little educational research has been conducted to guide educators in this area. Understanding the impact of these IPCAs in training and how best to deliver this vital education is an important part of helping residents obtain this critical competency.
교육 프로그램이 IPCA의 교수와 위임을 어떻게 최적화할 수 있는지 더 잘 이해하기 위해, 우리는 가정의학과에 위치한 질적 연구를 수행하여 미래의 실습을 위해 가족 의사를 적절하게 준비시켰다. '가족의학 거주자, 최근 졸업생 및 임상 감독관은 [간접 환자 치료 활동의 교육적 영향과 중요성]을 [어떻게 인식]하고 있는가?'
To better understand how education programmes may optimise the teaching and entrustment of IPCAs, we conducted a qualitative study located in the discipline of Family Medicine to adequately prepare family physicians for future practice, asking ‘How do family medicine residents, recent graduates and clinical supervisors perceive the educational impact and importance of indirect patient care activities’?
2 방법
2 METHODS
2.1 설계 연구
2.1 Study design
이것은 임상 교육 요구 사항 탐색과 같은 사회적 과정 연구에 적합한 방법론인 [구성주의 근거이론 연구]입니다. 이 방법론의 구성주의적 기반은 [학습자가 자신의 일의 맥락을 이해할 수 있는 다양한 방법을 강조]하며, 다음과 같은 힘에 의해 형성된다
- 교육 정책(예: 인증 요건 및 시험),
- 직업 및 작업 환경의 암묵적이고 명시적인 규범,
- 가정의가 된다는 것은 무엇을 의미하며, 가정의가 어떤 유형의 일을 해야하는지에 대한 사회적 기대
근거 이론이 요구하는 데이터 수집과 분석 사이의 반복을 통해 우리는 한 그룹의 예비 통찰력을 바탕으로 다음 라운드에서 데이터 수집을 구축하고 형성하여 우리의 조사에 응답하고 심화시킬 수 있었다.
This is a constructivist grounded theory study,37 a methodology appropriate for the study of a social process such as navigating a clinical education requirement. The constructivist underpinnings of this methodology highlighted the different ways that learners may understand the context of their work, shaped by forces such as
- education policy (e.g. accreditation requirements and exams);
- implicit and explicit norms of the profession and work environment;
- social expectations about what it means to be a family physician and what kind of work family physicians should do.
The iteration between data collection and analysis required by grounded theory allowed us to build on preliminary insights from one group, building and shaping data collection in the next round to respond to and deepen our inquiry.
2.2 연구 상황
2.2 Study context
이 연구는 캐나다 도시에 위치한 단일 가정의학 레지던트 프로그램의 맥락에서 수행되었다. 의료 거주자는 가정의학과 의사가 되기 위해 2년간의 일반 전문의 교육 프로그램을 이수하며, 일부에서는 3년차 고급 기술 교육을 선택적으로 받을 수 있습니다. 이 대규모 레지던트 프로그램은 의학-박사 대학과 연계되어 있으며, 매년 3개의 훈련장에서 200명의 레지던트들을 수용한다. 2개의 교육장은 학계 가정의학 실습과 연계되어 있으며, 1곳은 지역사회에 기반을 둔 여러 가정의학 실습이 있다.
- Academic practices는 의료 전문가의 교육과 가르침이 교수진의 역할의 큰 부분을 차지하는 의과대학과 관련된 것이다. 이러한 practice에서, 교수진 의사는 일반적으로 매일 2~3명의 학습자를 감독한다.
- 지역 사회 practice는 지역 사회 내의 일반적인 가정의학 관행이며 의사는 일반적으로 한 번에 한 명의 학습자를 감독한다.
This study was conducted in the context of a single Family Medicine residency programme located in urban Canada. Medical residents complete a 2-year generalist training programme to become Family Physicians, with an optional third year of enhanced skill training available to some. This large residency programme is affiliated with a medical-doctoral university, admitting 200 residents each year across three training sites. Two training sites are affiliated with academic family medicine practices, and one with multiple community-based family medicine practices.
- Academic practices are those associated with a medical school, where education and teaching of health care professionals are a large part of the role of faculty physicians. In these practices, faculty physicians typically supervise two to three learners each day.
- Community practices are general family medicine practices within the community and physicians typically supervise one learner at a time.
2.3 이론 렌즈
2.3 Theoretical lens
본 연구에서는 [Billett의 직장 학습 이론]을 민감 개념으로 사용하였다. [민감 개념]은 연구 중인 현상에 대한 연구자들의 생각에 INFORM하는 배경 아이디어입니다. 직장 학습 이론은 연구를 시작할 때 선임 연구원(MV)에게 알려졌고, 이는 작업의 개념화와 설계 방식에 영향을 미쳤다. 이 이론은 [작업장이 교육 기회를 제공]하는데, 이 [교육기회는 학습자가 효과적으로 학습하기 위해 확인하고 참여하도록 선택해야 하는 것]이라는 우리의 가정을 형성했다. [학습 기회의 식별]은 교육 및 조직 구조의 지도와 직장에 존재하는 다른 사람들의 입력에 의해 형성된다.
- 이 이론적 렌즈는 IPCA를 학습자와 그들의 임상 교사들에게 [인식될 수도 있고 그렇지 않을 수도 있는 교육적 어포던스]로 생각하는 우리의 생각에 영향을 미쳤다.
- [인터뷰 가이드의 구축과 개선 과정]에서, 이 이론은 학습자가 학습 기회에 대해 인식하고 결정하는 방법, 그리고 직장에서 어떤 선호도가 식별을 장려하거나 바람직한 특정 학습 기회를 만드는지에 대해 조사하기로 한 우리의 결정에 영향을 미쳤다.
- 우리는 분석 중에 이 이론이 직장 학습에 대해 제공한 배경 문맥을 넘어 이 이론에 명시적으로 관여하지 않았다.
We used Billett's workplace learning theory as a sensitising concept in this work.38 Sensitising concepts are background ideas, which inform the researchers' thinking about the phenomenon under study.39 Workplace learning theory was known to the senior researcher (MV) at the onset of the study, influencing the way the work was conceptualised and designed. This theory shaped our assumptions that workplaces offer educational opportunities that learners must both identify and choose to engage with to learn effectively.38 The identification of learning opportunities is formed by the guidance of educational and organisational structures and the input of others present in the workplace.38
- This theoretical lens influenced our thinking of IPCA as an educational affordance that may or may not be recognised by learners and their clinical teachers.
- During the construction and refinement of the interview guide, this theory influenced our decision to probe about the way that learners recognise and make decisions about learning opportunities, and what affordances in the workplace encourage the identification or make desirable particular learning opportunities.
- We did not engage explicitly with this theory during analysis, beyond the background context it provided about workplace learning.
2.4 참가자
2.4 Participants
직장 학습의 맥락적 특성으로 인해 본 연구는 단일 가정의학 레지던트 프로그램을 중심으로 진행되었으며, 현재 학습자, 현 교육자 및 지난 5년 이내에 졸업한 동문들을 모집합니다. 대상자는 현재 가정의학과 전공의('거주자')와 이 프로그램에서 지도자 역할을 하는 임상의-교육자('교육자') 및 지난 5년 이내에 이 프로그램을 졸업한 가정의사('초기 직업의사')이다.
Due to the contextual nature of workplace learning, we conducted this study around a single family medicine residency programme, recruiting current learners, current educators and alumni who have graduated within the past 5 years. Eligible participants were
- current family medicine residents (‘residents’),
- clinician-educators who have a preceptor role within this programme (‘educators’), and
- family physicians who graduated from this programme within the past 5 years (‘early career physicians’).
2.5 샘플링 및 모집
2.5 Sampling and recruitment
우리는 세 참가자 그룹 각각에 대해 서로 다른 샘플링 전략을 사용했다. 프로그램 사무소에서 발송된 이메일, 프로그램 리드 전공의, 임상 공간의 포스터, 공동 저자 팀의 그룹 학습 세션 시작 시 이루어진 연구에 대한 발표를 통해 전공의를 모집했다. 잠재적 거주 참가자는 연구 보조자나 선임 저자(MV)에게 연락하도록 요청하여 그들의 신원이 의사 공동 저자에게 알려지지 않도록 했다. 처음 5년간 의사는 프로그램 동문들을 위한 온라인 페이스북 그룹들과 연구팀의 전문 네트워크를 통해 이메일을 통해 모집되었다. 교육자들은 연구팀이 보낸 이메일을 통해 모집되었다.
We used different sampling strategies for each of the three participant groups. Residents were recruited through e-mails sent from the programme office and lead residents of the programme, posters in clinical spaces and announcements about the study made at the beginning of group learning sessions by the co-author team. Potential resident participants were asked to contact the study research assistant or senior author (MV) so their identities were not known to physician co-authors, who may have held a position of authority over them. Physicians in the first 5 years were recruited through online Facebook groups for programme alumni and by e-mail through the professional networks of the research team. Educators were recruited through e-mails sent by the research team.
우리는 [편의 샘플]로 시작했고, 예비 데이터 수집을 이론적으로 관련된 초기 데이터 분석에서 식별되어감에 따라서 참여자 임상 경험(위치, 임상 실습 및 기간)의 다양성을 보장하기 위해 [목적적이고 이론적으로 정보에 입각한 접근 방식]으로 이동했다.
We started with a convenience sample and after preliminary data collection moved to a purposeful, theoretically informed approach to ensure diversity in participant clinical experience (location, clinical practice and duration), as these aspects were identified in initial data analysis as theoretically relevant.
이것은 [근거 이론 연구]였기 때문에, 우리는 데이터 충분성에 대한 판단을 안내하기 위해 [이론적 포화] 개념을 사용했다. 우리는 [이론에 기여하는 범주의 완전성]과 [이론적으로 지시된 유형의 샘플링 완료]와 관련해서 [이론적 포화]를 이해한다. 포화 식별은 데이터 분석 전반에 걸쳐 발생하는 프로세스로, 여러 분석가와의 논의를 통해 운영됩니다. 각 범주가 잘 개념화되어 있고, 식별된 이론이 모든 관련 데이터를 설명할 수 있다는 것을 확인한 후, 분석 그룹은 [전반적으로 보면, 이론에 아무것도 추가되지 않을 것]이기 때문에 [새로운 데이터 수집의 return이 감소한다]는 데 동의했다. 이 시점에서 우리는 코호트 및 수련 장소와 관련해서 [이론적으로 관련된 일부 관점]이 샘플에 강하게 존재하지 않는다는 점에 주목했다. 이러한 관점을 포함하기 위해 추가 자료를 찾았지만, 참여자의 다양성을 확대하기 위해 완료된 새로운 인터뷰는 새로운 분석 방향을 제시하지 못했다.
As this was a grounded theory study, we used the concept of theoretical saturation to guide our judgements of data sufficiency.37, 40 We understand theoretical saturation to relate to the completeness of categories that contribute to a theory, and the completion of theoretically-indicated types of sampling. The identification of saturation is a process occurring throughout data analysis, operationalised through discussion with multiple analysts. After identifying that each category was well conceptualised, and the identified theory could account for all relevant data, the analytic group agreed that new data collection had diminishing returns, as it would not necessarily add anything to the overall theory.40 At this point we noted that some theoretically-relevant perspectives, related to cohort and training site, were not strongly present in the sample. We sought additional data to include these perspectives, but new interviews completed to expand the diversity of participants did not suggest new analytic directions.
2.6 데이터 수집
2.6 Data collection
데이터는 포커스 그룹과 개별 인터뷰를 통해 수집되었다. 포커스 그룹은 경력 단계별로 동질적이었다. 인터뷰와 포커스 그룹은 MV, MS, 그리고 연구 조수에 의해 촉진되었다. 이 개인들은 모두 질적 연구에 대해 훈련된 비-의사이며, 참가자들에게 알려지지 않은 여성들이다. 개별 인터뷰는 스케줄링이 참가자의 포커스 그룹 가입을 허용하지 않거나 참가자가 인터뷰에 대한 선호도를 표시한 경우에 수행되었다. 각 참가자 그룹에 대해 별도의 인터뷰 가이드(보충자료로 포함)를 개발하고 데이터 수집이 진행됨에 따라 다듬었다. 인터뷰 가이드는 문헌, 가정의학과 교사 및 학습자로서의 실제 경험, 연구 중인 문제에 대해 레지던시 프로그램에 제출한 피드백을 바탕으로 다학제 팀에 의해 개발되었습니다. 예비 포커스 그룹의 통찰력을 사용하여 미래 참가자의 모집 및 데이터 수집을 구체화하면서 한 번에 한 참가자 그룹에 초점을 맞추기 위해 데이터 수집을 단계화했다. 인터뷰 가이드는 초기 분석 통찰력을 반영하고, 이론적으로 관련된 문제에 대해 프로빙하고, 조사 범위를 세분화하기 위해 수정되었다. 전공의들은 우리의 처음이자 마지막 그룹이었기 때문에 우리는 프로젝트 진행 중에 발전한 새로운 분석 통찰력을 확인할 수 있었다.
Data were collected via focus groups and individual interviews. Focus groups were homogeneous by career stage. The interviews and focus groups were facilitated by MV, MS and a research assistant. These individuals are all women trained in qualitative research, non-physicians and unknown to the participants. Interviews were conducted when scheduling did not permit participants to join a focus group, or where the participant indicated a preference for an interview. Separate interview guides (included as supplementary material) were developed for each participant group and refined as data collection progressed. Interview guides were developed by our multi-disciplinary team based on literature, practical experience as family medicine teachers and learners, and feedback submitted to the residency programme about the issue under study. We staged our data collection to focus on one participant group at a time, using insight from preliminary focus groups to shape recruitment and data collection of future participants. Interview guides were amended to reflect initial analytic insights, to probe about theoretically relevant issues, and to refine the scope of inquiry. Residents were our first and our last group, so we could affirm emerging analytic insights that developed over the course of the project.
2.7 데이터 분석
2.7 Data analysis
데이터 분석은 구성주의 근거 이론을 상징하는 단계적 프로세스로 진행되었습니다. 이는 초기 데이터가 수집되는 즉시 시작하여 예비 통찰력을 향후 데이터 수집에 inform하는 것이다. 여러 분석가가 개방형 귀납적 코딩에 참여하여 팀 전체와 만나 잠재적인 집중 코딩에 대한 아이디어를 논의했습니다. 이 미팅을 통해 식별된 범주는 추가 코딩 라운드에서 운영되었으며, 이를 통해 우리는 집중적인 코딩 스키마를 생성하도록 조정, 확장 및 정교해졌다. 이 코딩 스키마의 적용은 연역적(귀납적 코딩을 통해 개발된 스키마를 적용)과 귀납적(확장, 정제, 정교화) 사이에서 다양한 코딩 과정을 통해 이루어졌다. [귀납적]에서 [연역 – 귀납적]으로의 이러한 움직임은, 우리의 분석이 데이터에 기반을 두도록 보장했다. 이러한 과정을 통해 테마를 귀납적으로 파악하였다. 우리는 연구 질문에 직접적으로 반응하는 주제를 개발하여 [교사 및 학습자의 경험을 설명]하는 것과 관련된 주제와 [가정의학의 교수 및 학습 개선을 위한 제안] 사이의 균형을 이루기 위해 노력했다.
Data analysis proceeded in a staged process emblematic of constructivist grounded theory, beginning as soon as initial data were collected so preliminary insights informed future data collection. Multiple analysts engaged in open inductive coding, meeting with the whole team to discuss ideas for potential focused coding. The categories identified through this meeting were operationalised in an additional round of coding, through which we refined, expanded and elaborated to produce a focused coding schema. Application of this coding schema was accomplished through multiple rounds of coding that varied between deductive (applying the schema developed through inductive coding) to inductive (expanding, refining and elaborating schema). This movement from inductive to deductive–inductive ensured that our analysis remained grounded in the data. Through this process, themes were inductively identified. We developed themes, which were directly responsive to the research question, striving to achieve a balance between those relevant to describing the experiences of teachers and learners and those relevant to suggestions for improving teaching and learning in family medicine.
2.8 윤리
2.8 Ethics
이 연구는 해밀턴 통합연구윤리위원회(11547)의 승인을 받았으며, 모든 참여자는 각 데이터 수집 세션 시작 시 전자적으로 그리고 구두로 사전 동의를 제공하였다. 우리는 연구팀의 의사 교육자와 거주자 참여자 사이의 권력 불균형을 잠재적 윤리적 문제로 식별했다. 상주 참가자를 보호하기 위해, 우리는 의사 연구 팀원들이 원본 오디오 파일이나 확인된 녹취록을 포함하여 상주 참가자를 식별할 수 있는 정보에 접근하지 못하도록 보장했다.
This study was approved by the Hamilton Integrated Research Ethics Board (11547), and all participants provided informed consent electronically and again verbally at the beginning of each data collection session. We identified the power imbalance between the physician educators on the research team and the resident participants as a potential ethical issue. To protect resident participants, we ensured that physician research team members did not have access to any information which would identify resident participants, including original audio files or identified transcripts.
3 결과
3 RESULTS
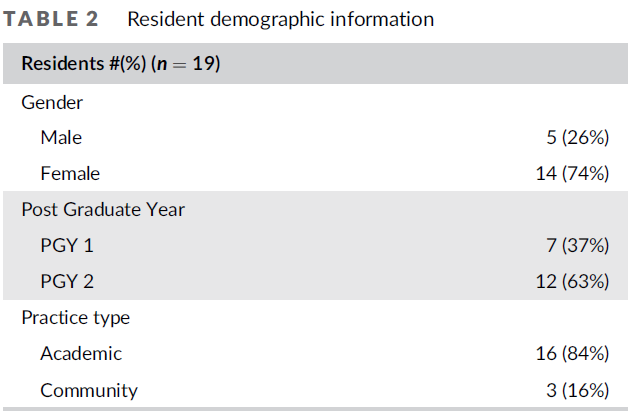
우리는 19명의 거주자(R), 16명의 의사(P), 7명의 경험 있는 의사 교육자(E)로부터 인터뷰 및 포커스 그룹 데이터를 수집했다. 각 포커스 그룹에 3~6명의 참가자가 참여한 가운데 6개의 개별 인터뷰와 11개의 포커스 그룹을 실시하였다. 가정의학 실천 유형의 광범위한 다양성으로 인해, 우리는 표 2-4에 practice 유형을 학문적, 공동체적, 비전통적인 것으로 요약했다. '비전통적 행위'은 예를 들어 병원 의사, 입원 환자 정신 건강 기관, 사망 의료 지원, 완화 치료 및 교도소 보건/교정 시설과 같은 집중적인(제너럴리스트가 아닌) 행위을 의미한다. 참여자 인구통계 정보는 표 2-4에서 확인할 수 있다.
We collected interview and focus group data from 19 residents (R), 16 physicians in the first 5 years of practice (P) and 7 experienced physician educators (E). We conducted 6 individual interviews and 11 focus groups with three to six participants in each focus group. Due to the broad variability of family medicine practice types, we have summarised practice types in Tables 2–4 as academic, community and non-traditional. ‘Non-traditional practices’ refer to focused (rather than generalist) practices, for, for example, hospitalist, in-patient mental health unit, Medical Assistance in Dying, Palliative care and prison health/correctional facilities. Participant demographic information can be found in Tables 2–4.


우리는 먼저 모든 그룹의 참가자들이 [IPCA가 가정의사로서의 경력 기간 동안 반드시 지녀야 하는 무게로 작용한다]는 분석 결과에 대해 논의한다. 다음으로, 우리는 그들의 경력 초기에 그 무게를 부담으로 보았고, 더 많은 경험 있는 그룹들이 그 무게는 가정의학에서 지속 가능한 경력을 쌓는 데 필요한 힘을 기를 수 있는 기회라고 어떻게 이해했는지 설명한다. IPCA 작업을 부담 또는 강도 훈련으로 느끼게 하는 이유에 대한 이러한 논의에서 참가자들은 몇 가지 악화 및 완화 요인(모호한 기대, 작업량 불평등에 대한 인식, 환자 및 작업에 대한 교수 및 친숙함)을 식별했으며, 이는 차례로 논의된다. 우리는 표준화, 점진적 도입, 작업량에 대한 투명성, 명시적 교육 및 피드백과 경계 설정 등 IPCA의 교육 가치를 최적화하는 방법에 대한 거주 프로그램에 대한 참가자 권고를 설명함으로써 이 섹션을 마무리한다.
We first discuss the analytic finding that participants in all groups identified IPCA work as a weight they must carry for the duration of their career as family physicians. Next, we describe how those earlier in their career viewed that weight as a burden, and more experienced groups understood that weight to be a chance to develop the strength needed for a sustainable career in family medicine. In these discussions of what made IPCA work feel more like a burden or strength training, participants identified several exacerbating and alleviating factors (ambiguous expectations, perceptions of workload inequity, teaching and familiarity with patients and tasks), which are discussed in turn. We conclude this section by describing participant recommendations to residency programmes about how to optimise the educational value of IPCAs: standardisation, gradual introduction, transparency about workload, explicit teaching and feedback and boundary setting.
3.1 IPCA의 무게: 부담 또는 근력 훈련?
3.1 The weight of IPCAs: Burden or strength training?
모든 참가자들은 그들의 실천 단계에 관계없이 IPCA가 가정의학의 필요하지만 불쾌한 부분이라는 인식을 공유했다. 그들은 IPCA가 환자 치료를 위해 필요하다는 것을 인식했지만, 끝이 없어 보이는 서류작업의 '과중한 책임'(P6)도 설명했다. 참가자 그룹이 분화된 곳은 이 무게를 짊어지는 것의 성격과 영향을 [부담]으로 보았는지, 그들의 경력 동안 [이 무게를 짊어지는 데 필요한 힘이나 힘을 기를 수 있는 기회]로 보았는지에 대한 것이다.
All participants, no matter their stage of practice, shared the perception that IPCAs are a necessary but unpleasant part of family medicine. They recognised that IPCAs are required for patient care, but also described the ‘crushing responsibility’ (P6) of the seemingly never-ending stream of paperwork. Where participant groups diverged was how they framed the nature and impact of carrying this weight, as either a burden or an opportunity to develop the strength needed to carry this weight throughout their career.
[전공의들과 초기 직업 의사들]은 IPCA의 중요성을 교육 기회보다는 부담으로 강조했다. '그것은 나에게 어떤 교육적 가치보다 훨씬 더 많은 스트레스를 주었다.' (R12) 그들은 이러한 활동에 소비하는 시간이 학습, 일과 삶의 균형, 웰빙, 그리고 다른 교육 목표를 달성하는 능력을 저해하는 방법을 기술했다. '나는 확실히 그것이 압도적이라고 느낀다. 나는 그것이 지속가능하다고 느끼지 않는다'(P7). 그들이 이 무게를 견디기 위해 개발한 전략에는 늦게까지 머무르거나 휴가 기간을 사용하여 이러한 작업을 수행하는 것이 포함되어 있었다. '휴가시간을 이용해 매주 하루씩 전일제 가정의학과를 쉬었습니다'(R9)
Residents and early career physicians emphasised the weight of IPCAs as a burden rather than an educational opportunity: ‘it provided me way more stress than any educational value’ (R12) They described the ways that time spent on these activities impeded their learning, work–life balance and wellness, and ability to achieve other educational goals: ‘I definitely feel like it's overwhelming. I don't feel like it's sustainable’ (P7). The strategies they developed to carry this weight included staying late or using vacation time to accomplish these work tasks: ‘I've used my vacation time to take one day off every week of full-time family medicine’ (R9).
[독립의료를 하는 참가자]들은 IPCA의 무게에 대해 전공의들과 다르게 말했다. 그들은 이러한 업무가 환자 치료와 가족 의사의 업무 일부를 위해 필요하다는 것을 더 잘 인식했다. '당신이 이 양식을 완성할 때 당신은 당신의 환자에게 자금이나 자원 같은 것에 대한 접근권을 주는 것이고, 당신은 당신이 그들과 마주 앉아 있을 때보다 모든 면에서 혹은 그 이상으로 당신의 환자를 돕고 있는 것이다.'(E4)
Participants who were in independent practice spoke differently about the weight of IPCAs than residents. They were more apt to recognise that these tasks are necessary for patient care and part of the work of a family physician: ‘when you complete this form you are giving your patient access to funding or resources or whatever, you're helping your patient every bit as much or maybe more than when you're sitting face-to-face with them’ (E4).
[의사 경력 첫 5년 동안 의사]들은 레지던트 시절 IPCA 작업의 이점을 현재 진료에 반영했습니다. 'ODSP [Ontario Disability Support Program] 양식에는 분명히 재간finesse이 있습니다. 바보같이 들리지만, 그것들을 작성하면서 전공의로서 배우는 art가 있습니다. … 레지던트로서 그런 걸 알아내서 엉덩이를 박살내면서 시간을 보내서 다행이다, 그래, 스태프가 되면서 부담이 줄었다(P5).' 이 학습의 일부는 IPCA의 업무 스타일 변경을 포함하여, IPCA의 부담을 다루기 위한 전략을 개발하는 것이었다.
Physicians in the first 5 years of their career recognised the benefits of the IPCA work they did in residency to their current practice: ‘There's obviously a finesse to ODSP [Ontario Disability Support Program] forms, it sounds silly to say but there is an art to filling them out and learning those things as a resident is helpful. … I'm glad that I spent time as a resident figuring that stuff out and busting my butt, then yeah, it reduced the burden when I became staff’ (P5). Part of this learning was developing strategies to deal with the burden of IPCAs, including changing their practice style:
'우리가 실제로 '지혜로운 선택'[불필요한 의학적 조사와 개입을 줄이기 위한 캠페인]과 같은 것들을 따르고, 검사와 조사 횟수를 줄인다면, [우리는 환자들과 더 많은 개인적, 신체적 접촉]을 할 뿐만 아니라, 들어오는 다른 데이터로부터도 부담을 덜 수 있을 것이다'(E7)
‘If we actually followed things like Choosing Wisely [campaign to reduce unnecessary medical investigation and intervention], and decreased the number of tests and investigations and things like that, we would not only have more personal, physical contact with our patients, but we would also have less burden from other data that is coming in’ (E7)
대부분 이러한 전략과 교훈은 실용적인 방법으로 학습되었으며, 많은 의사들은 [IPCA를 지속 가능한 방식으로 관리하는 방법을 배우는 것]이 전공의의 중심 학습 목표라고 설명했다. '나는 그들을 설득하려고 노력하며, 지금 일을 잘 하면, 앞으로 보상이 있을 것이다.(P7)' 여기서, 우리는 모든 직업 단계의 교육자들이 [전공의 수련에서 IPCA의 무게]를 [부담으로 인식할 뿐만 아니라, 오랜 경력을 위해 자신을 훈련할 수 있는 기회로 인식]하고 있음을 확인했다. '그것보다 더 중요한 것은 우리 모두가 마라톤을 할 수 있는지 확인하고 그 과정에서 우리의 건강과 건강을 해치지 않도록 하는 것이다.'(E1)
Mostly, these strategies and lessons were learned in a practical way, and many physicians described that learning how to manage IPCAs in a sustainable way is a central learning objective for residents: ‘I do try to convince them, put the work in now and it will pay dividends moving forward’ (P7). Here, we identified that educators of all career stages perceive the weight of IPCAs in residency not solely as a burden, but also as an opportunity to train oneself for a long career: ‘more important than that is making sure we can all do the marathon and that we don't burn out and compromise our health and wellness in the process’ (E1).
3.2 악화 및 완화 요인
3.2 Exacerbating and alleviating factors
참가자들은 IPCA가 부담스럽다는 데 일관되게 동의했지만, 그러한 부담을 악화시키거나 완화하는 조건도 설명했다.
While participants consistently agreed that IPCAs are burdensome, they also described conditions that exacerbate or alleviate that burden.
3.2.1 모호한 기대치
3.2.1 Ambiguous expectations
전공의와 최근 졸업한 직원들은 [모호한 기대]를 요인으로 식별하여 IPCA의 부담을 가중시켰다. 실천에서 독립하기 전에, 전공의들은 그들의 지도자들의 목표, 우선순위, 과정을 따라야 한다. 이 영역에 대한 명확하고 일관된 지침이 없으면 IPCA 부담이 증가합니다. '당신은 또한 특정 시간대에 그것을 끝내야 한다는 압박감을 느끼지만, 만약 그것이 당신의 물건이라면 당신은 "나는 이것을 내일 볼 것이다"와 같을 수 있다.(P5)
Residents and recently graduated staff identified ambiguous expectations as a factor, which exacerbated the burden of their IPCAs. Before becoming independent in their practice, residents must follow the goals, priorities and processes of their preceptors. Without clear and consistent instructions in this area, IPCA burdens are increased: ‘You also feel the pressure to get it done on a certain timeline, whereas if it was your own stuff you could be like “I'll look at this tomorrow”’ (P5).
3.2.2 작업량 형평성에 대한 거주자의 인식
3.2.2 Resident perceptions of workload equity
전공의 집단 특유의 또 다른 악화 요인은 할당된 작업의 양이나 강도에서 [전공의 간의 불평등한 차이]에 대한 인식이었다. 예를 들어, 농촌 실무에서 일하는 거주자들은 그들의 IPCA 부하가 학계 가족 보건 팀 내에서 일하는 거주자들보다 훨씬 적다고 보고했다. 일부 참가자들은 이를 [지도교사preceptor]의 선택 때문이라고 보았다. '운이 좋게도 어떤 지도교사를 얻었는지에 따라 얼마나 많은 사람들이 받은 편지함을 관리해야 하는지에는 큰 차이가 있었습니다. 우리는 같은 사이트에 있었고 같은 수의 환자를 보았지만 일부 사람들은 다른 사람들보다 받은 편지함과 바쁜 업무에 훨씬 더 많은 시간을 보냈다.'(P1)
Another exacerbating factor unique to the resident group was perceptions of inequitable differences between residents in the volume or intensity of assigned work. For example, residents working in rural practices reported that their IPCA load was much less than those working within academic family health teams. Some participants attributed this to preceptor choice: ‘there were huge discrepancies in how much people had to manage the inbox based on what preceptor they got lucky enough to get. We were at the same site and seeing the same population of patients yet some people spent significantly more time on their inbox and busy work than others did’ (P1).
[작업을 관리하는 데 사용할 수 있는 리소스]에서도 비슷한 불평등이 발견되었습니다. 일부 관행은 전공의가 IPCA 업무를 다른 사람에게 위임할 수 있도록 허용한 반면, 다른 관행에서는 전공의가 직접 이 작업을 하도록 했다. 전공의들은 지도교사가 할 수 있는 방식으로 업무를 위임하는 것이 허용되지 않아 업무량이 증가하고 만족도가 감소했다고 보고했다.
'라벨을 인쇄하기 위해 프린터를 찾고 환자의 소변을 적신 다음 그것을 보내고 포장하기 위해 뛰어다니는 것은 거주 시간을 잘 사용하지 않습니다. 실제로 그럴 사람이 있어야 하고, 대부분의 클리닉에는 있지만, 우리에게는 없습니다.'
A similar inequity was seen in the resources available to manage this work. Some practices permitted residents to delegate IPCA tasks to others, while in other practices residents were required to do this work themselves. Residents reported that not being allowed to delegate work in the way their preceptors were able to do increased their workload and decreased their satisfaction: ‘It's not a good use of resident time to be running around trying to find a printer to print off labels, to then dip that patient's urine, to then send it off and package it up. There actually should be someone to do that, and in most clinics, there is, but for us, there's not’ (R9).
3.2.3 교육
3.2.3 Teaching
[모든 경력 단계의 교육자]들은 [전공의를 가르치는 데 필요한 시간, 인내심, 코칭]이 그들 자신의 IPCA 부담을 악화시킨다는 것을 확인했다. 전공의들은 그 일을 맡음으로써 IPCA 직원들의 요구를 완화하고 있다는 것을 인식했지만, 교육자들은 전공의들에게 위임하는 것은 시간, 인내, 유연성이 필요하다고 설명했다. '내가 원하는 방식으로 교육하는 것은 매우 시간이 많이 걸리기 때문에, 내가 해야 할 약간의 투자와 균형을 이루게 된다.' (E2)
Educators of all career stages identified that the time, patience, and coaching required to teach residents exacerbated their own IPCA burden. While residents perceived that they were alleviating the IPCA demands of staff by taking on that work, educators described that delegating to residents required time, patience and flexibility. ‘Teaching, if done in the way that I like to do it, it's very time consuming and so it balances out a bit of the investment that I do to have some tasks taken off my plate.’ (E2).
3.2.4 친숙함(환자, 진료소 및 전문 지식)
3.2.4 Familiarity (patients, clinic and expertise)
[환자와 친숙하지 않은 것]은 [전공의] 뿐만 아니라 [대리의사 직무locum work(다른 사람의 업무를 인계받거나 명단을 구축)로 인해 환자와 친숙하지 않을 수 있는 경력 첫 5년 동안 의사]의 IPCA 업무량을 악화시켰다. 의료진의 의사는 자신이 잘 알고 있는 환자의 경우 스스로 주문한 결과를 검토하는 데 있어 효율성을 설명했습니다. '또한 일단 실습을 하고 나면 환자를 잘 알게 되는 이점이 있기 때문에, 그러한 요소들은 환자를 좀 더 낫게 만드는 데 도움이 됩니다.'(P1)
Not being familiar with a patient exacerbated the workload of IPCAs for residents as well as for physicians in the first 5 years of their career who may not be familiar with patients due to locum work, taking over someone else's practice or building their roster. Staff physicians described the efficiency in reviewing results they ordered themselves, for a patient they were well-familiar with ‘You also have the benefit of knowing your patients well once you're out in practice, so those factors help make it a bit better.’ (P1).
3.3 권장 사항
3.3 Recommendations
참가자들은 IPCA에 대한 전공의 교육 경험을 개선하기 위한 전공의 프로그램에 대한 권고 사항을 제공했습니다. 참가자들은 프로그램이 [IPCA에 대한 전공의 참여를 표준화하고 학습자와 교사 모두에게 지침과 기대를 명확하게 전달할 것]을 권고했다. '교육 목표와 기대는 무엇인가에 대한 유닛의 집단적 메시지가 있다는 것이 중요하다.' (E5) 이는 교육 현장 전반의 IPCA 워크로드에 대한 인식된 불평등을 개선하기 위한 방법으로 간주되었습니다. 전공의들은 또한 프로그램이 학습자에게 IPCA를 완료하기 위한 [전용 시간]을 제공할 것을 권고했다. [전용Dedicate 시간]은 전공의가 직무의 다양한 구성 요소를 학습할 때 담당 의사와 동일한 업무량을 수행하는 데 필요한 추가 시간을 설명하는 데 도움이 될 것이다.
Participants provided recommendations to residency programmes for improving the resident educational experience with IPCAs. Participants recommended that programmes standardise resident involvement in IPCAs and clearly communicate instructions and expectations to both learners and preceptors: ‘It is important that there is a collective message that comes from the unit about … what are the educational goals, [and] what are the expectations.’ (E5) This was seen as a way to ameliorate the perceived inequity in IPCA workload across training sites. Residents also recommended that programmes provide learners with dedicated time to complete IPCAs. Dedicated time would help account for the additional time residents require to do the same workload of a staff physician as they learn the various components of the task.
또한, 참가자들은 IPCA를 처리할 수 있는 능력을 개발하기 위해서는 [점진적인 도입]이 중요하다고 제안했다. 참가자들은 이것이 업무량을 줄이고 IPCA 관련 스트레스를 완화하는데 도움이 될 수 있다고 믿고 있으며, 특히 임상 치료의 다른 측면을 배우면서 레지던트 초기에 더욱 그렇다. '그것은 아무도 모르는 내 동료 레지던트들의 첫 6개월 동안 정말 많은 사람들을 태워버렸다. 그들은 시스템을 몰랐고, 프로그램을 몰랐고, 어떻게 거주자가 되는지도 몰랐으며, 동시에 1,000명의 수신함을 어떻게 하는지도 몰랐다.' (P4)
Further, participants suggested that a gradual introduction was important to develop capacity to handle IPCAs. Participants believe this may reduce the workload and help relieve IPCA-related stress, especially early in residency as they learn the other aspects of clinical care. ‘It really burnt out a lot of my co-residents in their first six months of residency when they didn't know anybody. They didn't know the system, they didn't know the program, they didn't know how to be a resident, and also how to do an inbox of 1,000 people at the same time.’ (P4).
또한, 이 접근 방식은 IPCA 자체의 보다 효과적이고 효율적인 학습을 가능하게 할 것으로 여겨졌다. 개업 의사들은 독립적인 개업에서 IPCA의 [예상 업무량 및 필연적 업무량]에 대한 투명성을 높였고, 이는 가정의학 경력의 일부로서 전공의들이 [IPCA의 현실을 이해하고 예측]하는 데 도움이 될 것이라고 추론했다. 가정의학의 중요한 구성 요소로서 IPCA의 현실을 논의하는 것은 이러한 [작업량에 대한 전공의들의 인식]에 도움이 될 수 있으며, IPCA를 완료하는 지속 가능한 방법을 개발하도록 장려한다. "실제로 당신이 그것을 어떻게 제시하느냐에 달려 있다고 생각합니다. 예를 들어, 이것은 당신이 내 일을 하는 것에 대한 것이 아니라, 내가 당신에게 다른 종류의 교육을 제공하는 것에 관한 것입니다. 결국 당신을 좋은 가정의사로 만들 것입니다." (E5)
In addition, it was felt this approach would allow for more effective and efficient learning of IPCAs themselves. Practicing physicians encouraged more transparency about the expected and inevitable workload of IPCAs in independent practice, reasoning that this would help residents understand and anticipate the reality of IPCAs as part of a career in family medicine. Discussing the reality of IPCAs as a significant component in family medicine may help residents' perception of this workload, encouraging them to develop sustainable ways to complete IPCAs: ‘I think it depends on how you actually present it, like, this is not about you doing my work, but this is about me providing you with a different kind of education, that in the end will make you a good family doctor’ (E5).
마지막으로, 모든 그룹의 참가자들은 IPCA에 대한 보다 명확한 교육, 피드백 및 커뮤니케이션, 특히 청구서, 차트 유지보수, 양식 및 사례 보고/검토를 권고했다. 이러한 교육은 전공의들이 보다 많은 지원을 통해 보다 점진적인 방식으로 지식을 쌓을 수 있도록 도울 뿐만 아니라 교육적으로 중요한 내용을 강조하고 열린 소통의 기회를 제공할 것이다. '학습 욕구, 학습 목표, 이러한 학습 기회의 가치, 전공의가 학습에 대해 어떻게 느끼고 관리하는지, 나아가면서 상황을 조정하고 모두가 함께 작업하도록 하는 것이 중요하다고 생각합니다.' (E1)
Finally, participants in all groups recommended more explicit teaching, feedback and communication on IPCAs, especially billing, chart maintenance, forms and case debriefing/reviewing. This teaching would not only help residents build on their knowledge in a more gradual way with more support, but it would also provide an opportunity to highlight educationally important content and provide opportunities for open communication. ‘I think it's important to have ongoing conversation about learning needs, learning goals, the value of these learning opportunities, how the resident is feeling about it and managing it and be tweaking things as you go and really have everybody working together on it.’ (E1).
마지막으로 IPCA는 끝이 없습니다. 그러므로, 개인의 삶, 정신 건강, 건강을 보호하고 탈진을 피하기 위해 [제한을 두는 것]이 중요하다. 참가자들은 환자와의 경계 설정(예: 필요할 때 환자가 추가 예약을 하도록 권장), 자신에 대한 경계 설정(예: 긴급하지 않은 받은 편지함 항목을 다음날로 남겨두는 것) 및 [IPCA 작업을 완료까지의 시간을 제한하는 것]의 중요성을 반복적으로 표현했다. [솔선수범]하는 것은 전공의들이 독립 실무자와 동일한 전략을 구현할 수 있도록 지원했습니다. '나는 매우 효율적인 지도교사가 있었고, 우리는 결코 늦지 않았다. 그리고 그녀는 나에게 받은 편지함의 균형을 맞추는 법을 가르쳐 주었다. 환자를 보고, 가는 동안 차트를 작성하고, 당신과 함께 집에 가는 최소한의 일을 가져갔다. 그리고 오늘날까지 나는 여전히 그렇게 실천하고 있다. 그리고 그것은 임상적 부분과 IPCA 부분의 균형을 맞추는 방법을 배우는 것만으로도 큰 도움이 되었다고 생각합니다.' (P1)
Finally, IPCAs are never-ending; thus, it is important to set limits to protect one's personal life, mental health, wellness and avoid burnout. Participants repeatedly expressed the importance of
- setting boundaries with patients (e.g. encouraging patients to schedule an additional appointment when necessary),
- boundaries for oneself, (e.g. leaving non-urgent inbox items for the next day) and
- blocking off time to complete IPCA tasks.
Leading by example helped residents implement the same strategies as independent practitioners: ‘I had a very efficient preceptor, we never ran late … and she really taught me how to balance inbox, seeing patients, charting as you go, taking minimal work home with you, and to this day I still practice that way. And I think that was very helpful, just learning how to balance the clinical and the IPCA part.’ (P1).
4 토론
4 DISCUSSION
McMaster Family Medicine Residention 프로그램에서 전공의를 위한 간접 환자 치료 활동의 교육적 영향을 조사했습니다. 모든 참가자는 이 작업량이 필요하지만 종종 충족되지 않는다는 것을 인식했습니다. 그러나 이 작업에 대한 임상의의 관점은 이 작업에 대한 인식과 참여에 영향을 미쳤다. 불평등에 대한 모호한 기대와 인식은 학습자가 이러한 과제에 대한 혐오를 악화시켰다. 참가자들은 이 작업의 교육적 가치를 향상시키기 위해 명시적인 교육 및 피드백과 함께 IPCA에 대한 표준화된 단계적 도입에 초점을 맞출 것을 권고했다.
We explored the educational impact of indirect patient care activities for residents in the McMaster Family Medicine Residency programme. All participants recognised this workload as necessary, though often unfulfilling. However, the clinician's perspective on this work as either a burdensome additional weight or an opportunity to strengthen their management skills impacted their perception and engagement in the work. Ambiguous expectations and perceptions of inequity exacerbated learner dislike for these tasks. The participants recommended a focus on a standardised graduated introduction to IPCAs, with explicit teaching and feedback to improve the educational value of this work.
[빌렛의 직장 학습 이론]은 학습이 효과적이기 위해서는 학습자가 [교육 기회를 식별하고 참여하도록 선택해야 한다]고 설명한다. 이 연구는 IPCA를 [비교육적 초과근무로 인식하는 것]이 학습자의 이러한 과제에서 학습하는 능력을 저해한다는 점을 강조했다. 이것은 임상 작업장에서 배우는 것이 목적인 '학습자'으로서의 직업적 정체성을 가진 전공의들 사이에서 특히 심각할 수 있다. 스스로를 의료 사업에서 실천을 준비하는 '견습생'으로 보는 전공의들은 IPCA 업무를 효과적으로 관리하기 위한 전략을 배울 기회를 더 많이 볼 수 있다. 우리는 [숨겨진 커리큘럼]이 IPCA의 가치를 떨어뜨리는 방식에 주의를 기울여야 한다. 예를 들어, IPCA 과제가 임상의 시간 중 상당한 부분을 차지하지만 지도, 평가 또는 교육적 가중치를 거의 받지 않는 경우, 전공의는 IPCA 과제가 중요하지 않고 가치가 없다고 생각하는 법을 배울 수 있다. 이 작업을 ['행정적' 작업]이 아닌 '간접적 환자 치료'로 지칭하는 것은 이러한 작업의 가치와 중요성을 강조하는 데 도움이 될 수 있어 환자에게 의료 서비스를 제공하는 전공의의 역할에 관심이 쏠린다. 또한 IPCA 작업을 지속 가능하고 효과적으로 관리하기 위한 시스템에 대한 공식적인 교육 및 피드백 제공을 통합하면(예: 신뢰할 수 있는 전문 활동 또는 핵심 역량) 학습자가 이러한 작업의 교육적 가치를 인식하는 데 도움이 될 수 있다. 뉴질랜드, 호주, 영국의 왕립 일반 실무자 대학과 같은 일부 교육 기관들은 [간접 환자 치료 기술]이 독립 실무에 필요한 역량이라고 명시적으로 밝혔습니다.
Billett's workplace learning theory describes that for learning to be effective, learners must both identify and choose to engage with educational opportunities. This study highlighted that the perception of IPCAs as non-educational extra work impedes learners' ability to learn from these tasks. This may be particularly acute amongst residents whose professional identity is as a ‘student’ whose purpose in the clinical workplace is to learn.41, 42 Residents who see themselves as an ‘apprentice’ preparing to practice in the business of medicine may be more likely to see opportunities for learning strategies to effectively manage IPCA work. We must be attentive to the ways in which the hidden curriculum de-values IPCA work.43 For example, when IPCA tasks take up a significant portion of clinician time but are seldom coached, assessed or given much educational weight, residents may learn to think of them as unimportant and not valuable.42 Referring to this work as Indirect Patient Care rather than ‘administrative’ work may help emphasise the value and importance of these tasks, drawing attention to the resident's role in providing health care to the patient. In addition, incorporating formal ways to teach and provide feedback on systems for sustainably and effectively managing IPCA work (e.g. as an entrustable professional activity or core competency) may also be helpful in helping learners recognise the educational value of these tasks. The groundwork has been laid here by some educational bodies, including the Royal College of General Practitioners in New Zealand,44 Australia45 and the United Kingdom,46 each of which have explicitly stated that indirect patient care skills are a required competence for independent practice.
IPCA 작업을 적절하게 수행할 수 있는 것 외에도, 이러한 작업은 추가 교육 가치를 제공합니다. 의료 전문가로서의 기술 외에도, [목적적 IPCA 교육]은 효율성, 우선순위 부여, 적절한 전문적 의사소통 및 협업을 포함한 전문성, 옹호 및 리더십의 이전 가능한 기술을 강조한다. 이러한 기술은 캐나다 면허 대학인 College of Family Physicians of Canada가 제공하는 레지던트 훈련 프로필의 핵심 전문 활동의 최근 출판에서 강조된다. 이 문서에는 [IPCA 관리(EHR 관리, 받은 편지함 관리, 양식 작성 및 처방 관리 포함)]뿐만 아니라 [자가 및 지속 가능한 의료 행위 관리]를 의료의 유능한 관행에 중요한 핵심 전문 활동으로 나열합니다. 적절한 훈련과 적응적 전문지식의 렌즈를 통해 이 프로그램은 학습자가 다양한 리소스로 다양한 임상 맥락에서 IPCA의 가중치를 해결할 수 있도록 준비할 수 있을 것이다.
Beyond being able to adequately perform IPCA work, these tasks offer additional education value. In addition to skills as a medical expert, purposeful IPCA education highlights transferable skills in professionalism, advocacy and leadership including efficiency, prioritisation, appropriate professional communication and collaboration. These skills are underscored in the recent publication of core professional activities in the residency training profile provided by the College of Family Physicians of Canada, the Canadian licensing college.47 This document lists managing IPCAs (including maintaining the EHR, managing the inbox, completing forms and managing prescriptions) as well as managing self-care and a sustainable practice both as core professional activities critical to the competent practice of medicine. With appropriate training and a lens of adaptive expertise, the programme would be able to prepare learners to tackle the weight of IPCAs in varied clinical contexts with varied resources.48
IPCA는 종종 전공의 수련의 예기치 않은 구성 요소이다. 직원들은 종종 진료 시간 4시간 이내에 IPCA의 상당 부분을 완료하기 때문에 이 업무량은 일반적으로 의대생에게는 보이지 않는다. 이것은 전공의들이 IPCA 관리에 필요한 긴 시간, 특히 더 유연한 시간을 예상하여 가정의학을 선택한 경우에 특히 낙담하는 이유에 대한 잠재적인 설명을 제공한다. 참가자들의 목소리처럼, [IPCA의 예상치 못한, 충족되지 못한, 그리고 때로는 지속 불가능한 업무량]은 가정의학과 졸업생들이 포괄적인 가정의학을 실천하기로 선택하는 감소와 활동 수준과 환자 패널 크기의 감소에 영향을 미치는 많은 요소 중 하나일 수 있다. 졸업생들은 [이러한 예상치 못한 부담스러운 업무량을 보상]하기 위해 [(환자 패널이 크고 포괄적인) 가정의학 진료에서 벗어남]으로써 [지속 가능한 실천을 유지하기 위한 경계]를 설정하고 있을 수 있다.
IPCAs are often an unexpected component of residency. As staff often complete a significant portion of IPCAs outside of clinic hours4 this workload is typically unseen by medical students. This offers a potential explanation for why residents are particularly disheartened by the longer hours needed to manage IPCAs, especially if they selected family medicine in anticipation of more flexible hours.49 As voiced by our participants, the unexpected, unfulfilling, and sometimes unsustainable workload of IPCAs may be one of the many elements impacting a decline in family medicine graduates choosing to practice comprehensive family medicine and the decline of activity level and patient panel size.50, 51 Graduates may be setting boundaries to maintain a sustainable practice by moving away from comprehensive family medicine practice52 with a large patient panel to compensate for this unexpected and onerous workload.
4.1 교육자에게 미치는 영향
4.1 Implications for educators
이 연구는 가정의학 전공의들이 그들의 의료행위를 관리할 수 있도록 준비하기 위한 [새로운 커리큘럼의 필요성]을 강조했고, [전공의들의 교육적 헌신과 시간]에 대한 상충하는 요구를 염두에 두면서 이 중요한 환자 치료 부분을 통합했다. 53 여기에는 IPCA의 존재에 대한 투명성, 예상 작업량, 그리고 지속 가능한 경영을 위한 기대치와 전략이 포함된다. 예를 들어, 스텝이 학습자가 볼 수 있는 방식으로 자체 IPCA 작업을 완료한다면, 이 작업의 효율성을 높이기 위해 이러한 작업 및 역할 모델링 전략을 표준화한다.
This study has highlighted the need for new curricula to prepare Family Medicine residents to manage their practices, integrating this vital piece of patient care while being mindful of competing demands on residents' educational commitments and time.53 This includes transparency around the existence of IPCAs, the anticipated workload, expectations and strategies for sustainable management. For example, when staff complete their own IPCA work in a way that is visible to the learner, they are normalising these tasks and role modelling different strategies to increase efficiency of this work.
연구 참가자들은 IPCA를 단계적이고 점진적인 방식으로 도입할 것을 권고했다. 예를 들어, EHR 수신함에 대한 소개는 관심 있는 문서 또는 특정 문서를 보낸 후 전공의가 수신함의 모든 구성 요소를 관리할 때까지 전공의가 직접 주문한 항목을 보낸 후 특정 범주의 조사(즉, 참조 노트, 처방, 혈액 검사 및 진단 영상)를 수행할 수 있다. 이 접근법은 특정 학습 목표를 허용하기 위해 [양은 줄이면서 더 집중된 교육]을 촉진할 수 있다. Inbox을 언제 어떻게 도입해야 하는지에 대한 지침을 가지고 있으면 전공의들 사이의 투명성과 형평성이 향상될 것이고, 프로그램이 의도된 역량을 명확히 하고 정기적인 피드백을 촉진하도록 장려할 것이다. 이러한 전략은 전공의들에게 명확성과 구조를 만들어 줄 뿐만 아니라 학습자들이 적응적이고 자기 조절적인 학습 전략을 개발할 수 있도록 돕는 학습 환경을 촉진할 것이다. 전공의들이 스스로의 학습을 조절하고 적응할 수 있을 때, 그들은 의학 분야에서 평생의 경력을 지속할 수 있는 능력을 강화하고 있다. 전공의 프로그램은 이러한 적응적이고 자기 통제적인 행동을 촉진하기 위해 의도적으로 그리고 의도적으로 그러한 학습 환경을 계획해야 한다.
Study participants recommended that IPCAs be introduced in a stepwise, gradual way. For example, introduction to the EHR inbox can begin by sending interesting or specific documents, then items the resident themselves ordered, followed by a particular category of investigations (i.e. consult notes, prescriptions, blood work and diagnostic imaging) until the resident is managing all components of the inbox. This approach may facilitate focused education with reduced quantity to allow for specific learning goals. Having a guideline as to when and how inbox should be introduced will improve the transparency and equity amongst residents, encourage the programme to articulate the intended competency and to promote regular feedback. These strategies will not only create clarity and structure for residents, they also promote a learning environment that helps learners develop adaptive, self-regulated learning strategies.54 When residents are able to regulate and adapt their own learning, they are bolstering their ability to sustain a life-long career in medicine. Residency programmes should intentionally and purposefully plan such learning environments to promote these adaptive, self-regulated behaviours.54
4.2 강점과 한계
4.2 Strengths and limitations
수집된 데이터는 단일 레지던트 프로그램에서 수집되었으며 다른 가정의학 프로그램이나 다른 전문 분야로 이전할 수 없습니다. 상당한 모집 노력에도 불구하고, 참여에 자원한 전공의들은 우리 레지던트 프로그램의 대규모 학술 교육 현장에서 불균형적으로 뽑혔다. 지역사회 기반 현장에서 주민을 모집하는 것이 과제였는데, 이는 다양한 현장에서 IPCA의 교육 경험의 불일치를 시사하는 것일 수 있다. 참가자들이 자신의 경력 단계와 관련된 IPCA에 대해 말하는 방식에 차이가 있었기 때문에 다양한 수준의 전문 경험과 초점을 가진 참가자들의 통합이 강점이다.
The data collected was from a single residency programme and may not be transferable to other family medicine programmes or other specialties. Despite significant recruitment efforts, the residents who volunteered to participate were disproportionately drawn from the large academic teaching sites in our residency programme. It was a challenge to recruit residents from the community-based sites, which may be an indication of a discrepancy in the educational experience of IPCAs in the various sites. The incorporation of participants with varying levels of professional experience and focus is a strength, as there were differences in the way that participants spoke about IPCAs, related to their career stage.
5 결론
5 CONCLUSION
결론적으로, IPCA는 우리 의료 시스템의 필수적이고 증가하는 구성요소이다. 우리 가정의학 전공의들이 이러한 업무를 효과적이고 [지속 가능한 방식]으로 관리하도록 훈련받는 것이 필수적이다. 지속 가능성에 초점을 맞추지 않으면 IPCA는 인구 수요를 충족시키기 위해 충분한 수의 일반 가정의사를 모집하고 유지하는 데 장애가 될 위험이 있다. 이를 달성하기 위해서는 IPCA에 대한 점진적인 도입, 교육 및 피드백, 동료 간의 형평성을 포함할 수 있는 교육 혁신이 필요합니다. 이 교육을 제공하지 못하면, 수련을 마친 전공의가 독립적인 임상 실습으로의 이행하는 것에 대한 위험, 그리고 일부 사람들에게는 포괄적인 진료를 떠나서 더 세부전문과목으로 진입할 위험이 따른다. 그러나 교육 혁신은 충분하지 않다. 상응하는 보수 없이 업무량이 증가했을 때 나타나는 시스템적 영향을 인식하고, family practice의 지속 가능성을 높이는 의료 시스템 변화를 옹호해야 한다.
In conclusion, IPCAs are a necessary and increasing component of our health care system. It is essential to ensure our family residents are trained to manage these tasks in an effective and sustainable manner. Without a focus on sustainability, IPCAs risk becoming a barrier to recruiting and retaining sufficient numbers of generalist family physicians to serve population needs. Achieving this will require educational innovation, which may include a gradual introduction to IPCAs, with teaching and feedback, and equity amongst peers. Failing to provide this education carries the risk of more challenging transitions to independent clinical practice for graduating residents, and for some, attrition out of comprehensive practice and into sub-specialisation. However, educational innovation is not sufficient. We need to recognise the systemic implications of an increased workload without corresponding remuneration and advocate for health system change, which increases the sustainability of family practice.
Optimising the educational value of indirect patient care
PMID: 35972822
DOI: 10.1111/medu.14921
Abstract
Introduction: Indirect patient care activities (IPCA) such as documentation, reviewing investigations and filling out forms require an increasing amount of physician time. While an essential part of patient care, rising rates of IPCA work correspond with increases in physician burnout and job dissatisfaction. It is not known how best to prepare residents in IPCA-heavy specialties (e.g. family medicine) for this aspect of their career. This study investigates how educators and residency programmes can optimise IPCA work during residency to best prepare residents for future practice.
Methods: Using Constructivist Grounded Theory, we conducted focus groups and individual interviews with 42 clinicians (19 family medicine residents, 16 family physicians in the first 5 years of practice and 7 family physician educators). All participants were connected to one family medicine residency programme. We analysed interview data iteratively, using a staged approach to constant comparative analysis.
Results: While residents, early career physicians and educators perceived the educational value of IPCAs differently, they all reported IPCAs as a necessary weight that family physicians carry throughout their career. Some residents described IPCAs as a burden, creating inequities in workload and interfering with other learning and personal opportunities. In contrast, educators conceptualised IPCAs as an opportunity to build and develop the skills required to carry the weight of IPCAs throughout their career. We make specific recommendations for helping residents recognise this educational opportunity, such as clarifying expectations, navigating equity, understanding purpose and maintaining consistency when teaching IPCAs.
Conclusion: IPCAs are a key competency for many medical residents but require explicit pedagogical attention. If the educational opportunities are not made explicit, residents may miss the opportunity to develop strategies for practice management, professional boundaries, and administrative efficiencies.
© 2022 Association for the Study of Medical Education and John Wiley & Sons Ltd.
'Articles (Medical Education) > 임상교육(Clerkship & Residency)' 카테고리의 다른 글
| EPA 프레임워크의 논리와의 고군분투 (Med Educ, 2022) (0) | 2022.11.06 |
|---|---|
| EPA 프레임워크의 논리: 스코핑 리뷰 (Med Educ, 2022) (0) | 2022.11.05 |
| 내과와 외과에서 교수자와 학습자 정체성의 사회적 구성(Med Educ, 2022) (0) | 2022.10.04 |
| 성격이 중요한가? 일반외과의사로서 내향성과 외향성의 경험과 인식(Teach Learn Med. 2022) (0) | 2022.09.20 |
| 다른 학생과의 실습 겹침: 의과대학생 학습 경험에 미치는 영향(Teach Learn Med. 2022) (0) | 2022.09.20 |