안쓰러운 늘어진 여성: 의과대학생을 위한 골반진찰 학습자료의 상황분석(Med Educ, 2022)
‘Poorly relaxed women’: A situational analysis of pelvic examination learning materials for medical students
Sarah Towle
1 소개
1 INTRODUCTION
[환자 중심적이고 문화적으로 역량있는 의료]는 환자 경험을 개선하고 건강 격차를 최소화하는 중복된 방법으로 의학교육에서 옹호된다. 논란의 여지 없이, 이러한 접근법은 골반 검사(PE)와 같은 민감한 절차에서 추가적인 중요성을 가진다. 환자 취약성에 대한 검사의 성향과 관련 건강 차이(상세히 아래에 나와 있음)는 모두 검사가 임상적으로 시행될 때 이러한 접근법의 필요성을 강조한다.
Patient-centred and culturally competent care are championed in medical education as overlapping methods of improving patient experiences and minimising health disparities.1-4 Arguably, these approaches hold added significance in sensitive procedures such as the pelvic examination (PE). Both the examination's proclivity for patient vulnerability and its associated health disparities (detailed below) highlight the necessity of these approaches when the examination is clinically administered.5-10
[환자 중심 진료]는 20세기 중반에 시작되었다. 여성 건강 운동의 영향을 받아, 그것은 부분적으로 '질병 중심의 의학'과 [의학적 가부장주의]에 대한 반발로 나타났다. 임상 의사, 의료 교육자 및 의료 기관의 실천 모델로 채택되었지만 [환자 중심 진료]의 [정의]를 둘러싼 논란은 여전하다. 기본적으로 환자 중심의 치료는 환자를 정확하게 진단하는 것 외에도, 임상의가 환자를 [한 명의 사람으로 알고 있다]는 생각을 중심으로 이루어진다. 이 접근법의 가치와 원칙에는 사회 세계의 맥락에서 환자를 인정하고, 정확하고 시의 적절한 의료 정보를 제공하며, 환자 선호도를 존중하며, 정보에 입각한 의사 결정에 환자를 참여시키는 것이 포함된다.
Patient-centred care has origins in the mid-20th century. Influenced by the women's health movement, it emerged partly as backlash to both ‘illness-oriented medicine’ and medical paternalism.11 Though it has been adopted as a model of practice by clinicians, medical educators and healthcare institutions, debate remains surrounding the definition of patient-centred care.11 Fundamentally, patient-centred care revolves around the idea of the clinician knowing the patient as a person, in addition to accurately diagnosing disease.12 Values and tenets of this approach include
- acknowledging the patient in the context of their social worlds,
- providing accurate and timely medical information,
- respecting patient preferences and
- engaging patients in informed decision making.1-4
[환자 중심 진료]와 맞물려, 의학에서 [문화적 역량]은 다양한 사회적 문화적 배경을 가진 환자들을 치료하는 능력을 의미한다. 문화적 역량을 갖춘 진료를 운영하려면, [환자 배경에 대한 인식]과 [그 배경이 임상적 만남에서 권력의 차이에 어떻게 영향]을 미치는지, 그리고 [잠재적인 문화적 수용을 제공하는 것]이 모두 필요하다. 비록 의과대학 커리큘럼에 문화적 역량을 통합하려는 상당한 움직임이 있었지만, 그 틀과 학습자의 저항에는 여전히 과제가 남아 있다. 종종 임상 기술이 커리큘럼에서 더 우선시되고, 학생에게 문화적 역량이란 '소프트 사이언스'보다 학생들이 선호된다고 한다.
Aligned with patient-centred care, cultural competence in medicine refers to the ability to treat patients of diverse social and cultural backgrounds.13 Administering culturally competent care involves having both an awareness of patient background and how that background affects power differentials in clinical encounters, as well as providing potential cultural accommodations.3, 14 Though there have been considerable moves to incorporate cultural competence into the medical school curriculum,13 challenges remain in its framing and learner resistance; it is said that clinical skills are often prioritised in the curricula and favoured by students over the ‘soft-science’ of cultural competence.13, 15
PE는 다음과 같은 것들로 구성된다.
- 외부 생식기 검사.
- 질 및 자궁경부 검체검사(샘플 채취가 가능한 경우)
- 부속지, 자궁, 난소 및 방광의 양면 검사
- 때로는 직장이나 직장-질 검진
PE가 비록 외래 환자 시술이지만 신체적, 심리적 의원성iatrogenic 효과를 일으키는 것으로 유명하다. 여기에는 출혈, 경련, 불편함, 고통, 두려움, 불안, 취약성, 수치심, 당혹감, 타락, 통제력 및 존엄성 상실 등의 느낌도 포함된다. 젊은 환자, 성폭행 생존자, LGBTQ+ 커뮤니티 회원, 흑인 여성 등에서 부정적 반응이 높아지는 것으로 나타났다. 이러한 집단에서 산부인과학적 건강 격차는 지속되며, 이는 과거에 검사에서 겪은 부정적인 경험과 관련이 있다.
The PE consists of
- an inspection of the external genitalia;
- a speculum examination of the vagina and cervix (where samples may be taken);
- a bimanual examination of the adnexa, uterus, ovaries and bladder; and
- sometimes a rectal or rectovaginal examination.16, 17
Though an out-patient procedure, it is noted for causing physical and psychological iatrogenic effects: bleeding,18-20 cramping,20 discomfort or pain,6, 17, 18, 21, 22 as well as feelings of fear,6, 17 anxiety,17 vulnerability,17 shame,23 embarrassment,5, 6 degradation,5 and loss of control and dignity.24, 25 Negative reactions have been shown to be heightened in young patients,6, 22, 26, 27 survivors of sexual assault,28-30 members of the LGBTQ+ community31, 32 and Black women.28 Gynaecological health disparities persist in these populations and have been linked to previous negative experiences with the examination.7, 10, 33
페미니스트 연구 결과에 의해 뒷받침된 학자들과 제공자들은 골반 건강 관리pelvic health care에 있어, [환자 중심주의와 문화적 역량]의 중요성을 오랫동안 지적해 왔다. 일반적으로 환자 경험을 개선하는 것으로 알려진 수정사항에는 다음이 포함된다.
- 샤페론 허용,
- 사용 발 받침대 포기,
- 일상적인 양면 검사 중단(일부에서는 의학적으로 불필요하다고 간주)
- 검체 자가 삽입 제공
특정 모집단에 대해서는 다른 변형이 유용할 수 있습니다.
- 신체 부위에 대한 선호 용어 체크(성별 다양성 환자)
- 환자(생존 환자 및 불안 환자)에게 검사 통제권이 유지되게끔 확인
Feminist scholars and providers—backed by research findings—have long noted the importance of patient-centeredness and cultural competence in pelvic health care.24, 34-38 Modifications known to generally improve patient experience include
- allowing for chaperones,39
- forgoing the use footrests,38
- ceasing the routine bimanual examination (deemed by some to be medically unnecessary)16, 17 and
- offering speculum self-insertion.24, 35
Other modifications may be of value for specific populations:
- checking in on preferred terminology for body parts (gender diverse patients),24 as well as
- ensuring control of the examination remains with the patient (survivors and/or anxious patients).24, 35
최근 개발된 인간유두종 바이러스에 대한 [환자 자가 샘플링]은 자궁경부암 검진에 대한 환자 참여를 개선하며, 트랜스 및 원주민 환자 사이에서 선호된다. 그 결과 양성 소견이 발견되었을 때 과소 선별된 모집단에 대한 후속 조치가 증가한다. 임상적 수용이 부족하기 때문에, 이러한 접근법의 일부와 관련하여 의료 훈련에서 보다 효과적인 인식 전략이 필요하다는 의견이 제시되었다.
Patient self-sampling for human-papilloma virus—a recent development—improves patient participation in cervical cancer screening, is preferred among trans and Indigenous patients, and results in increased follow-up in under-screened populations when a positive result is found.40-43 It has been suggested that more effective awareness strategies are needed in medical training regarding some of these approaches, given their lack of clinical uptake.44
[산부인과 교육 협력자(GTA) — 교육 목적으로 PE를 받고, 의대생에게 피드백을 제공하는 여성 자원봉사자]의 도입을 포함하여, 이러한 접근 방식의 교리를 바탕으로 [PE 학습 practice]을 추가로 주입하기 위한 의료 커리큘럼의 진전이 이루어졌다. 그러나 커리큘럼의 단점은 여전히 존재한다. GTA 프로그램은 주로 백인 자원봉사자 46명으로 구성되며, 경우에 따라서는 어떤 행위는 자원봉사자들에게 부정적인 영향을 미치는 것으로 비판을 받아왔다.1 또 다른 흔하지만 문제가 되는 PE 학습 방법은 의료 교육생들이 [사전 동의 없이 마취 하에 환자를 대상으로 검사를 수행]할 때 발생한다. 이러한 관행이 대중에게 [환자 자율성 위반]으로 특징지어지며, 이를 [금지하려는 입법 움직임]이 있음에도, 학생들과 임상의사들 사이에서 받아들여지고 있다. 이 모든 것은 학생들이 환자 커뮤니티와 상호 작용하기 전에 환자 중심적이고 문화적으로 적합한 PE 접근법에 대한 개선된 노출이 필요할 수 있음을 시사한다. — 궁극적으로 사전 교육, 즉, 강의실 환경에서 이뤄져야 한다.
Strides have been made in the medical curriculum to further instil PE learning practices with the tenets of these approaches, including the introduction of gynaecological teaching associates (GTAs)—female volunteers who undergo PEs for educational purposes and provide feedback to medical students.45-47 However, curriculum shortcomings still exist. GTA programmes have been criticised for both consisting of predominantly White volunteers46 and, in some cases, maintaining practices that negatively impact volunteers.1 Another common yet problematic PE learning method occurs when medical trainees perform exams on patients under anaesthesia without prior consent.1-4, 47, 56 This practice has garnered acceptance among students and clinicians despite its public characterisation as a violation of patient autonomy and legislative moves to ban the practice.57-59 All this suggests that students may need improved exposure to patient-centred and culturally competent approaches to the PE before they interact with patient communities—ultimately in pre-clinical, classroom settings.
이 연구는 학부 의과대학 커리큘럼에서 PE를 수행하는 방법에 대한 텍스트 및 시각 기반 학습 자료를 조사한다. 이러한 자료들은 학생들이 체육을 처음 접하고 나중에 그 과정을 수행할 수 있는 기초를 형성한다. 그러한 자료의 분석은 수천 명의 의료 전문가에게 주어진 기술 정보에 대한 중요한 통찰력을 제공하며, 그 안의 메시지는 학생들의 의학에 대한 장기적인 믿음과 인식에 영향을 미칠 수 있다. 비판적으로 샘플링된 문서의 상황 분석을 통해, 본 연구는 의료 교육의 지식 격차를 메우고 텍스트 및 시각 기반 PE 학습 자료를 개선하여, 이후의 임상 학습에서 부족할 수 있는, 보다 [환자 중심적이고 문화적으로 적합한 접근 방식]을 포함할 수 있는지 여부 및 그 방법에 대한 정보를 제공하는 것을 목표로 한다.
This study investigates text- and visual-based learning materials on how to perform the PE in undergraduate medical school curricula. Materials such as these serve as the first introduction students have to the PE and form the foundation through which they later perform the procedure. Analyses of such materials provide important insight into the technical information given to thousands of medical professionals,60 and messages therein may impact students' long-term beliefs and perceptions in medicine.60, 61 Through a situational analysis of critically sampled documents, this study aims to fill a knowledge gap in medical education and provide information on if and/or how text- and visual-based PE learning materials could be improved upon to include more patient-centred and culturally competent approaches that may be lacking in later clinical learning.
2 방법
2 METHODS
저는 캐나다 대학 의과대학에서 체육에 필요한 필수 텍스트 기반 학습 자료에 대한 상황 분석을 수행했습니다. [상황 분석]은 'theory/methods package'로 묘사되며, 페미니스트 보건 연구에서 강한 역사를 가지고 있으며, 종종 [근거이론이라는 정성적 방법론의 확장]으로 간주된다. [근거 이론]이 데이터 내에서 발생하는 기본적인 사회적 프로세스를 밝히는 것을 목표로 한다면, [상황 분석]은 [전반적인 관심 상황에 대한 인식]을 통합한다. 연구자들은 사회적 구조, 집단, 제도 및 역사/현재의 현실 내에서 주제를 정하기 위해 [하드 데이터]를 뛰어넘는다.
I conducted a situational analysis of required text-based learning materials on the PE from undergraduate Canadian medical schools. Described as a ‘theory/methods package’, situational analysis has a strong history in feminist health research and is often considered an extension of the qualitative methodology of grounded theory.62 Where grounded theory aims to uncover basic social processes occurring within the data, a situational analysis incorporates an awareness of the overall situation of concern; researchers go beyond the hard data to situate their topic within social structures, collectives, institutions and histories/present-day realities.63
[상황 분석]은 또한 [지배적인 담론이 개인, 집단, 지식 및 관점을 배제하거나 삭제할 수 있는 권력을 가지고 있다]는 [푸코의 담론적 권력의 후기 구조주의 이론]에 근거한다. 기존의 정성적 분석이 이러한 학습 자료의 내용에 대한 설명을 초래하는 반면, 상황 분석은 환자와 연습생에 대한 PE의 현실에 내 데이터를 배치하고, 이러한 문서의 지배적인 담론이 학생들의 관점과 미래의 임상적 만남을 형성할 수 있는 방법을 밝혀준다.
Situational analyses also draw on Foucault's post-structuralist theories of discursive power—that dominant discourses have the power to exclude or erase individuals, groups, knowledges and perspectives.62, 64 Whereas conventional qualitative analyses would result in descriptions of the content in these learning materials, a situational analysis situates my data in the realities of the PE for patients and trainees and brings to light how dominant discourses in these documents can shape students' perspectives and future clinical encounters.65, 66
내 데이터는 캐나다에서 가장 큰 5개 학부 의과대학에서 의도적으로 샘플링되었고 학생들에게 PE를 수행하는 방법을 보여주는 모든 필수 교과서, 임상 기술 가이드 및 PowerPoint 프레젠테이션으로 구성되었다. 이 학교들은 캐나다에서 가장 많은 수의 의사들을 훈련시키기 때문에 선택되었습니다. 캐나다에 위치한 연구원으로서, 나의 목표는 국가 차원의 의료 교육자들에게 PE에 대한 전반적인 커리큘럼 피드백을 제공하는 것이었다. 이 연구는 캐나다 의대에 초점을 맞추고 있지만, 북미 의과대학에는 특정한 형태의 학습 표준화가 존재하며, 이 연구의 결과는 캐나다와 미국 전역의 의과대학에 일반화될 수 있다.
My data were purposively sampled67 from the five largest undergraduate medical schools in Canada and composed of all required textbooks, clinical skills guides and PowerPoint presentations that demonstrated to students how to perform the PE. These schools were selected because they train the largest number of doctors in Canada. As a researcher situated in Canada, my goal was to provide overall curricula feedback on the PE for medical educators at a national level. Though this study focuses on Canadian medical schools, certain forms of standardisation in learning exist in North American medical schools, and the results of this study could be generalised to medical schools across Canada and the United States.
공공 웹사이트 검색은 물론, 의과대학의 관리자, 교수진 및/또는 개인 정보 보호 담당자들에게 연락하고 요청하는 것을 포함했다.
- (i) 학부 의대생을 위한 필수 교과서 목록
- (ii) 임상 기술 및/또는 PE의 교육에 사용되는 내부 자료
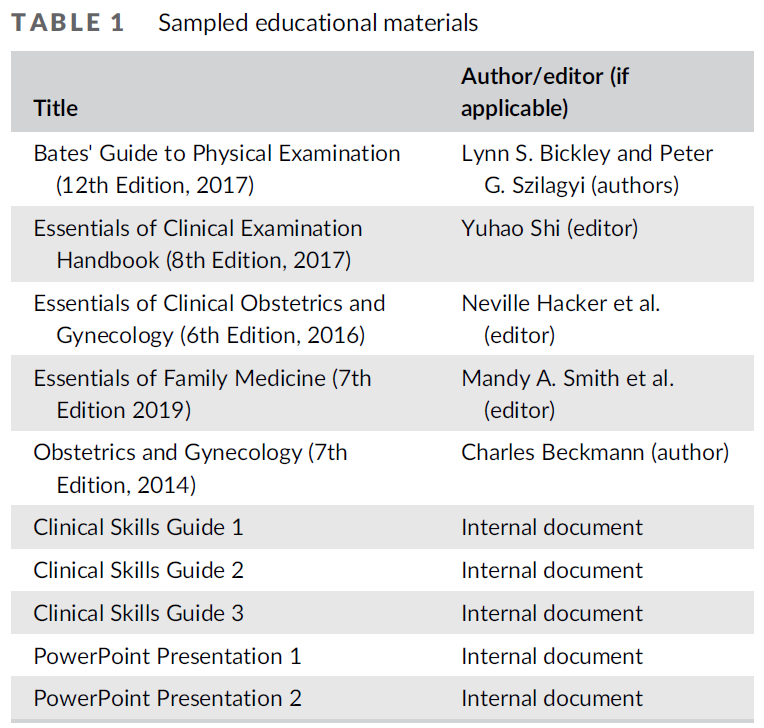
학생들이 여전히 교과서를 참조하는지 여부에 대한 의문이 있었지만, 필수 구매 및 필수 읽기로 지정된 내용만 포함되었다. 이를 통해 가능한 한 포괄적인 PE 학습 자료를 검사할 수 있었습니다. PE의 묘사를 포함할 수 있는 재료의 총 수는 28개였다. 이 28개에서 PE의 묘사가 포함되지 않은 자료를 제거하고 중복 자료를 제거한 후, 10개의 교육 자료 샘플이 남아 있었다(표 1에 나열). 특정 교과서는 맥길 대학교 도서관을 통해 온라인 또는 실제 사본으로 접근되었다. 내부 자료는 공개적으로 사용할 수 없는 경우 익명으로 나열됩니다.
Data collection involved searching public websites as well as reaching out to administrators, faculty and/or privacy officers at the medical schools and requesting
- (i) a list of any required textbooks for undergraduate medical students and
- (ii) any internal materials used for learning clinical skills and/or the teaching of the PE.
Though questions arise as to whether students still refer to textbooks, only those that were specified as required purchases and/or required reading were included. This allowed for an examination of PE learning materials that was as comprehensive as possible. The total number of materials that could contain depictions of PEs was 28.2 After eliminating materials within this 28 that did not contain depictions of the PE and removing duplicates, a sample of 10 educational materials remained (listed in Table 1). Specific textbooks were accessed via McGill University Library, either online or in physical copy. Internal materials are listed anonymously given that they are not publicly available.
데이터를 분석하기 위해, 나는 discursive data와 관련하여 일반적으로 사용되는 상황 분석의 분석 도구 중 하나인 [위치 매핑positional mapping]을 사용했다. [위치 맵position map]을 사용하면 데이터가 질적으로 코딩되지만, [취해진 위치와 담론에서의 침묵]에도 주의를 기울인다. 그런 다음 이러한 결과는 [좌표 지도]에 표시되며, [축]은 [논쟁 중인 문제]를 나타내고, [플롯 점]의 위치는 [위치의 prevalence]을 나타냅니다. 이론으로 정점을 찍기 보다는, 지도는 데이터 내의 모순과 부재는 물론 여러 위치를 완전히 표현할 수 있게 해준다.
To analyse the data, I employed positional mapping, one of the analytic tools of situational analysis commonly used in relation to discursive data.62, 63 With position maps, data are qualitatively coded, but attention is paid to positions taken and silences in the discourses. These results are then plotted on coordinate maps, with the axes representing contested issues and the location of the plot point representing the position's prevalence. Rather than culminating in a theory, the maps allow for multiple positions as well as contradictions and absences within the data to be fully articulated.62, 63
샘플의 초기 판독은 세트에 익숙해지도록 수행되었다. 이후 10개의 샘플을 정성 데이터 소프트웨어 NVivo(NVivo 12, QSR International, USA)로 가져오고, 프로그램의 코딩('노드'라고도 함) 프레임워크를 사용하여 콘텐츠(담화 및 이미지)를 귀납적으로 코딩하는 수동 프로세스가 수행되었다. 분석은 다음 질문에 의해 유도되었다.
- 환자 중심성 및 문화적 역량과 관련하여 의대생이 사용하는 PE 학습 자료에서 환자를 어떻게 대표하고 있는가?
이 심층적인 프로세스에는 데이터의 반복적 검토, 기본 및 최종 보조 코드/노드 적용, 세부 메모가 포함되었습니다. '데이터에서 취한 위치'는 코드에서 나온 반면, '침묵silences'은 메모 작성 과정에서 구체화되었다. 예를 들어, 메모를 하면서, 나는 더 광범위한 관심 상황(환자 중심적이고 문화적으로 유능한 PE) 중에서 [어떤 개념이 데이터에 제한되거나 누락되어있는지limited or absent] 주목했다.
An initial reading of the samples was undertaken to become familiar with the set. The 10 samples were then imported into the qualitative data software NVivo (NVivo 12, QSR International, USA), and the manual process of inductively coding the content (discourse and images) was carried out using the program's coding (also called ‘nodes’) framework. The analysis was guided by the following question:
- How are patients represented in PE learning materials used by medical students with respect to patient-centeredness and cultural competencies?
This in-depth process involved multiple passes of the data, applying primary and eventual secondary codes/nodes, and the taking of detailed memos. The ‘positions taken in the data’ emerged from the codes, whereas the ‘silences’ materialised during the memo-making process. For instance, while making memos, I noted which concepts of the broader situation of concern (a patient-centred and culturally competent PE) may be limited or absent in the data.
몇 번의 검토passes 후 코딩 및 메모 작성 프로세스에서 [새로운 위치와 새로운 침묵]이 더 이상 나타나지 않을 때(이 방법을 '분석적 충분성' 62라 칭함), 결과는 스프레드시트로 내보내고 주제와 관련된 그룹으로 정리되었다. 여기서부터 지도 축은 데이터의 일반적인 긴장 영역을 식별하여 개발되었다.
- (i) 환자 불편과 피할 수 없는 장애에 대한 PE 과제와 그에 대한 임상적 인식
- (ii) 임상 의사의 행동 대 환자의 목소리
그 다음 이 방법에 의해 제안된 템플릿을 사용하여 마이크로소프트 워드의 지도에 해당하는 위치와 정적을 표시하였다.
After several passes and when new positions and silences were no longer emerging from the coding and memo-making process (what this method refers to as ‘analytic sufficiency’62), the results were exported into a spreadsheet and organised into thematically related groups. From here, map axes were developed by identifying common areas of tension in the data:
- (i) a clinical awareness of PE challenges versus the inescapability of patient discomfort and
- (ii) the clinician's actions versus the patient's voice.
Corresponding positions and silences were then plotted onto maps in Microsoft Word using templates suggested by this method.
이 연구는 문서 분석에 초점을 맞추고 인간 참여자들에 대한 연구나 실험을 포함하지 않았기 때문에, 맥길 대학 의학부의 맥길 기관 검토 위원회의 규정에 따라 윤리 승인이 필요하지 않았다.
Because this study focused on analysing documents and did not involve research or experimentation with human participants, ethics approval was not required as per the rules of the McGill Institutional Review Board in the Faculty of Medicine at McGill University.
3 결과
3 RESULTS
상황 분석 결과는 두 개의 위치 지도에 표시된다(그림 S1 및 S2). 아래에서는 이 분석의 세 가지 중요한 주제에 대해 논의합니다.
Results of the situational analysis are depicted in two positional maps (Figs S1 and S2). Below, I discuss three overarching themes from this analysis.
3.1 균질하고 규범적인 신체: 시대에 뒤떨어진 언어
3.1 Homogeneous and normative bodies: Outdated language
자료에서 나타난 가장 일반적인 주제는 [신체에 대한 동질적이고 규범적인 개념]이었다. 시각적으로나 담론적으로, 대부분의 문서(80%)에서 환자들은 [백인의, 시스젠더의, 장애가 없는, 가임 연령의, 이전 외상 이력이 없는 것]으로 구성되었다. 규범적이거나 '표준화된' 신체는 기초 기술을 배우기 위한 의료 훈련에서 선호되는 경우가 많으며, 이는 부분적으로 이러한 동질성을 설명할 수 있다.
The most prevalent theme that emerged from the data was a homogeneous and normative notion of the body. Both visually and discursively, patients were constructed as White, cis-gendered, abled-bodied, of child-bearing age and without a previous history of trauma in most (80%) of the documents. Normative or ‘standardised’ bodies are often preferred in medical training for learning foundational skills, which may partially explain this homogeneity.
신체 변화가 언급되더라도, 그것은 [심지어 이 표준 구조 내에서조차, 특정 신체들이 어떻게 임상의에게 PE를 더 도전적으로 만들 수 있는지]에 대한 언급이었다.
When bodily variation was mentioned, it was in reference to how, even within this normative construct, certain bodies can make the PE more challenging for the clinician:
많은 처녀질 오리피스는 하나의 검사 손가락을 인정한다…
만약 introitus이 위축되고 타이트해진다면, 나이 든 여성에게도 유사한 기술이 나타날 수 있다.
Many virginal vaginal orifices admit a single examining finger … Similar techniques may be indicated in elderly women if the introitus has become atrophied and tight. (Bickley and Szilagyi, p. 30, emphasis added)
그레이브스 경첩은 옆쪽이 더 넓고, 더 높고, 구부러진 날을 가지고 있다. 대부분의 경산부 여성에게 가장 적합하다.
그것의 넓고 구부러진 날들은 시각화를 위해 경산부 여성의 느슨한 질벽을 유지한다.
The Graves speculum has blades that are wider, higher, and curved on the sides; it is more appropriate for most parous women. Its wider, curved blades keep the looser vaginal walls of multiparous women separated for visualization. (Beckmann, p. 13, emphasis added)
난소는 비만이나 잘 이완되지 않은 여성에게서 촉진되기 어렵다.
Ovaries are difficult to palpate in obese or poorly relaxed women. (Clinical Skills Guide 3, p. 8, emphasis added)
여기서의 언어 선택은 성차별적이고 불필요하게 성차별화된 담론을 나타낸다. 예를 들어, 여성 순결의 사회적 구조는 유지되고, 경산 여성은 질적으로 '느슨한' 것으로 묘사된다. 또한, 프로시져가 참아내기 어려운 것이 아니라, (PEs의 유일한 수용자로 생각되는) 여성이 '잘 이완되지 않은 것'으로 묘사된다. 여기서, 우리는 환자의 동질적(비다양적) 묘사와 여성 신체와 관련된 [시대에 뒤떨어지고, 종종 낙인적인 용어와 개념]의 사용과 관련하여 자료에서 문화적 역량이 부족하다는 것을 주목할 수 있다. 이러한 강연들은 의학 및 사회에서 성별과 성 고정관념을 영속시키는 역할을 한다.
The language choices here are indicative of sexist and unnecessarily sexualised discourse. The social construct of female virginity is upheld, multiparous women are described as vaginally ‘loose,’ and women (suggested to be the sole receiver of PEs) are ‘poorly relaxed’ rather than the procedure being challenging to tolerate, for instance. Here, one can note a lack of cultural competency in the materials both with respect to homogeneous (non-diverse) depictions of patients and with the use of outdated and often stigmatising terms and concepts related to the female body. These discourses serve to perpetuate gender and sexuality stereotypes in medicine and in society more broadly.
대부분의 문서가 신체에 대한 규범적 개념을 설명했지만, 두 개의 내부 가이드는 분명히 다양한 환자를 언급하였다. 하나는 퀴어 및 트랜스 환자를 위한 성별을 포함하는 접근 방식을 강조하고 다른 하나는 원주민과 LGBTQ+ 관점을 포함하는 외상 정보 치료의 원칙에 대한 두 페이지를 할애하였다.
Though most of the documents depicted normative notions of the body, two internal guides did overtly refer to diverse patients: one emphasising a gender-inclusive approach for queer and trans patients and the other dedicating two pages to the principles of trauma-informed care inclusive of Indigenous and LGBTQ+ perspectives (Clinical Skills Guide 3, pp. 11–12; PowerPoint Presentation 2, pp. 20–23).
3.2 환자의 주체성과 선호도가 제한된다.
3.2 Limited patient agency and preferences
모든 문서에서 강조된 것은 [환자가 PE 수행 여부를 결정할 수 없다]는 개념이었다. 임상의가 PE가 표시된 것으로 판단한 경우, PE가 발생하게 됩니다. 두 개의 교과서 및 한 개의 내부 가이드의 다음 예는 이러한 권한을 보여줍니다.
Underscored in all documents was the notion that patients were not in control of deciding whether the PE was to be performed. If the clinician had determined that a PE was indicated, it was to occur. The following examples from two textbooks and one internal guide demonstrate this authority:
환자에게 당신의 시험 계획을 설명하시오. (Smith 등, 페이지 328; 강조 추가)
Explain to the patient your plans for the exam. (Smith et al., p. 328; emphasis added)
내진을 할 때 앞으로 일어날 모든 것을 그것이 일어나기 전에 설명해야 합니다.
Everything that is going to happen during the pelvic examination should be explained before it occurs. (Beckmann, p. 11; emphasis added)
환자로부터 진행 허가를 받습니다.
[Obtain] permission from the patient to proceed. (Clinical Skills Guide 2, p. 3)
여기서는 환자의 의사input과 관계없이, 이미 검사가 결정되었습니다. 환자 동의(또는 때때로 표현된 '허락')가 언급되지만, [이미 검사가 진행 중이거나 결정된 것]이라는 구성 내에 있다. [임상적 권위]는 문서 내에 너무나도 팽배해서, [환자가 검사를 거부할 경우] 어떻게 해야 할지 아무도 제안하지 않았고, [우려를 하는 환자에 대한 대안적인 행동 방침]이 제시되지 않았다.
Here, the examination has been decided upon before, independent of patient input. Though patient consent—or ‘permission’ as it was sometimes phrased—is mentioned, it is within the construct of the examination already being in motion or decided on. Clinical authority was so prevalent in the documents that none suggested what to do if a patient declined an examination; no alternative courses of actions were suggested for apprehensive patients.
환자의 주체성agency가 문서에 나타나 있을 경우에는(40%), [이미 하고 있는 프로시져]를 환자에게 맞춤화할 수 있는 방법과 관련하여 다음이 언급된다.
- 거울 사용(임상 기술 가이드 2 및 PowerPoint 프레젠테이션 2)
- 시술 중 신발 착용(비클리와 실라지) 또는
- 산만함을 위한 기술 장치 사용(임상 기술 가이드 3)
When patient agency was represented in the documents (40%), it occurred with respect to how the patient could customise an already occurring procedure:
- use of a mirror (Clinical Skills Guide 2 and PowerPoint Presentation 2),
- wearing shoes during the procedure (Bickley and Szilagyi) or
- using technological devices for distraction (Clinical Skills Guide 3).
PE 경험을 개선하는 것으로 알려진 최근 및 거의 틀림없이 더 효과적인 아래와 같은 옵션들은 없었다.
- 일상적인 상황에서 bimanual examination을 포기한다. (딱 하나에만 있었음)
- 발판 사용 금지,
- 스페큘럼의 자가 삽입 또는 자기 스왑 테크닉
Recent and arguably more effective options known to improve the PE experience were absent:
- forgoing the bimanual examination in routine circumstances (excluded from all but one),
- disuse of footrests,
- self-insertion of speculum and/or self-swabbing techniques.
이러한 측면에서 자료는 환자 중심의 치료 원칙(일부 환자의 선호도 존중)을 지지했지만, [특정 모집단에 대한 검사를 개선하는 것으로 알려진 것을 포함하여], 모든 가능한 옵션에 대해 학생들에게 경고하기에는alerting 불충분했다. 이전 연구의 결론은, [의료 훈련단계에서 학생은 아직 임상행위를 습득하기 전이므로, 새로운 PE 옵션을 도입하기에 이상적인 시기]인 것으로 확인되었다. 그렇지 않으면 학생들은 이러한 원천 자료에 노출되지 않을 수도 있다.
In this regard, although the materials upheld a tenet of patient-centred care—respect for (some) patient preferences—they were inadequate in alerting students to all options, including those known to improve the examination for specific populations. Conclusions from previous studies have identified medical training as the ideal introduction to novel PE options given their current lack of uptake in clinical practice.44 Students may otherwise never be exposed to these techniques if not in these source materials.
3.3 환자는 [PE가 이뤄지는 도중]이라는 특정 단계에서 [취약성과 제한된 능력]을 경험한다.
3.3 Patients are vulnerable and experience limited capacity at specific stages during the PE
데이터에서 나타난 분명한 주제는, PE의 임상 부분 동안 (임상의사 및 연습생에 대한) 환자의 상대적 취약성이었다. 데이터의 담화는 PE에는 두 가지 뚜렷한 사회적 요소인 [PE 전후]와 [PE 중]이 있음을 보여주었다. 다음 예제는 환자 참여(질문할 능력, 동의할 능력, 결과 수신 능력 등)가 [전후 구성 요소에서 얼마나 강하게 indicate되는지], 그리고 [옷을 벗은 것]이 환자의 능력capacity에 대한 취약성과 중단을 어떻게 의미하는지 보여줍니다.
A clear theme that emerged from the data was patient vulnerability relatively to the clinician and/or trainee during the clinical portion of the PE. Discourses in the data demonstrated that there were two distinct social components of the PE: the before/after and the during. The following example demonstrates how patient engagement—such as the ability to ask questions, give permission and receive results—is heavily indicated in the before/after component and how being unclothed signifies both a vulnerability and a disruption to the capacity of the patient:

[프로시져 중의 취약성]이라는 주제는 임상의에게도 적용된다. 몇몇 문서에서는 임상의사(특히 교육생 및/또는 남성)가 '의료법적 보호'를 위해 환자가 알지 못하는 [샤프롱chaperones]을 병실에 배치해야 하는 방법을 강조하였다(임상기술지침서 1, 페이지 1).
Themes of vulnerability during the procedure also applied to the clinicians; several documents highlighted how clinicians—specifically trainees and/or males—must have chaperones unknown to the patient in the room for ‘medico-legal protection’ (Clinical Skills Guide 1, p. 1).
검사의 두 번째 구성 요소(프로시져 자체)에서, 담론은 [환자의 편안함]에서 벗어나, [PE의 임상적 스텝]으로 이동했습니다. 학습 목적을 위한 절차를 묘사하는 동안 임상적 초점을 어느 정도 맞출 것으로 예상된다. 비록 본문들이 [프로시져가 이뤄지는 동안 환자와의 의사소통의 필요성]을 일찍이 강조했지만, 종종 이 개념은
- (i) 임상 단계 동안 전혀 언급되지 않거나
- (ii) 허가를 구하는 질문이나 이의 제기 기회가 아닌. [진술]로 표현된다.
- '만지는 느낌이 날거에요',
- '경경을 삽입하려고 한다는 것을 환자에게 말한다',
- '불편한 환자에게 긁는 느낌이 들 수 있다고 알려준다'
이러한 재료는 PE의 두 구성 요소 사이에서 접근 방식이 달랐다고 할 수 있다. [환자와 환자 참여]는 프로시져 전후에, [임상 스킬]은 프로시져 동안에 중요하게 다뤄졌다.
In the second component of the examination (the procedure itself), discourses shifted away from patient comfort and towards the clinical steps of the PE. An amount of clinical focus during depictions of any procedure for learning purposes is to be expected. Though texts had earlier highlighted the need for patient communication during the procedure, often, this concept was either
- (i) not referenced at all during the clinical steps or
- (ii) expressed as statements rather than permission-seeking questions or opportunities for dissent (i.e. ‘you are going to feel touch’, ‘let the patient know you are about to insert the speculum’ and ‘inform patient she may feel an uncomfortable scraping sensation’).
It could be said that these materials diverged in their approach between the two components of the PE: patients and patient engagement were centred in the before/after, whereas clinical skills were centred during.
4 토론
4 DISCUSSION
내 분석은 캐나다 학부 의과대학에서 샘플링된 PE를 수행하는 방법에 대한 텍스트 및 시각 기반 학습 자료가 이 연구의 프레임워크에 명시된 [환자 중심 치료 및 문화적 역량의 원칙]에 대해 환자를 적절하게 나타내지 못한다는 것을 보여준다. 환자의 다양성, (언어를 통한) 존중, 환자의 선호와 주체성agency는 모두 다 프로시져를 묘사할 때 결여되어 있었다. 하지만 이러한 개념은 부가적인 비중을 가지고 있으며, 다른 형태의 학습에서 학생들에게 소개되지 않을 수도 있다. 이와 같은 강의실 자료는 의학 교육에서 하나의 요소에 불과할지 모르지만, 그러나, 나는 이러한 묘사가 여전히 여기서 그리고 의학 교육과정에 더 광범위하게 중요하다고 주장한다.
My analysis demonstrates that text- and visual-based learning materials on how to perform the PE sampled from Canadian undergraduate medical schools inadequately represent patients with respect to the tenets of patient-centred care and cultural competence set out in this study's framework. Patient diversity, respect (via language), preferences and agency were all limited in depictions of a procedure where these concepts arguably carry added weight and may not be introduced to students in other forms of learning. Classroom materials such as these may illustrate a single component of medical education; however, I argue that these depictions still matter here and for the medical curriculum more broadly.
[환자 중심성]과 관련하여, [환자 관점에 대한 노출]이 [의대생의 자신감과 정보 보유를 크게 향상시킨다]는 연구 결과가 나오면서, 이 치료 모델은 전체 의료 커리큘럼의 중요한 측면으로 반복적으로 확인되었다. 앞서 언급한 바와 같이, PE는 환자와 학생 모두에게 예외적인 절차입니다. 프로시져 학습 자료에서 환자 중심의 접근 방식을 강조한다면, PE가 적어도 하나의 우선 순위가 되어야 한다고 추정할 수 있다.
With respect to patient-centeredness, this model of care has repeatedly been identified as an important aspect of the entire medical curriculum,11, 68 with research demonstrating that exposure to the patient perspective significantly improves medical students' confidence and retention of information.69 As mentioned, the PE is an exceptional procedure for both patients and students.70 If patient-centred approaches were to be emphasised in procedural learning materials, it could be presumed that the PE should be at least one priority.
이 사례들에서 환자중심적 접근방식이 배제되었음을 확인하며 배운 것이, [환자 중심주의가 필수적이라고 여겨지는 다른 분야의 결함]도 말해 줄 수 있다. 예를 들어 만성 통증, 장애 또는 말기 질환을 앓고 있는 환자 또는 산부인과 환자가 있다. 학생들은 교육과정 전반에 걸쳐 환자 중심주의를 보다 명시적으로 가르칠 필요가 있다고 보고했고, 학부 커리큘럼은 환자 중심적인 관점보다 '질병 기반 관점'에 더 치우친 것으로 나타났다. 이 연구의 결과는 교실 학습 자료가 환자 중심주의를 개선할 수 있는 의료 교육의 한 측면이 될 수 있음을 보여준다.
What we learn from their exclusion in these cases may speak to deficiencies in other fields where patient-centeredness has been identified as imperative: patients with chronic pain,71 disabilities72 or terminal illness,73 or in obstetrics,74-76 for instance. Students have reported that patient-centeredness needs to be more explicitly taught throughout the curriculum,77 and undergraduate curricula have been shown to be more inclined towards ‘disease-based perspectives’ over patient-centred ones.78 The results of this study demonstrate that classroom learning materials could be one aspect of medical education where patient-centeredness could be improved upon.
문화적 역량과 관련하여, 본 연구의 분석은 의료 커리큘럼에서 환자 묘사를 다양화하기 위해 추가 작업이 필요할 수 있음을 보여준다. 이는 이 주제에 대한 다른 조사 결과와 일치합니다. 피부과와 같은 다른 의학 분야의 학습 자료에서 인종적 동질성은 예를 들어 학생들의 진단 기술을 저해하는 것으로 알려져 왔다. 또한 특정 모집단의 부재(심지어 술기 장비technical material 수준의 부재조차)는 의사들이 [인종과 질병 위험 사이의 연관성]이 있게 만듦으로써, 기존 건강 격차를 유지하거나 악화시킬 수 있다는 점에 주목했다. 북미 의대생들은 [성소수자(LGBTQ+) 환자와 관련된 주제]에 대해 학부 커리큘럼에 적은 시간을 할애하고 있으며, 이 모집단에 적절한 상담을 제공할 준비가 되어 있지 않다고 느낀다고 보고한다. 페미니스트 이론가들에 따르면, 의학교육에서 [환자를 동질적으로 묘사하는 것]은 [신-식민지주의neo-colonialism의 한 형태]로 간주되며, 모든 신체가 아니라 [일부 신체에만 복무하도록 설계된 '우생학의 논리']를 영속시킨다. 강의실 자료를 포함한 포괄적인 리소스는 다양한 환자 그룹과 상호작용하는 데 있어 학생들의 문화적 역량을 향상시키기 위한 중요한 방법으로 확인되었습니다. 본 연구의 결과는 환자 표현이 개선되어야 하는 커리큘럼의 한 측면(PE 강의실 자료)을 드러내지만, 또한 의료 훈련의 모든 단계에서 문화적 역량 기술이 얼마나 더 강조되어야 하는지에 대한 더 광범위한 예시로도 작용한다.
With respect to cultural competency, the analysis from this study demonstrates that further work may be needed to diversify patient depictions in the medical curriculum. This aligns with other findings on this topic. Racial homogeneity in learning materials from other fields of medicine—such as dermatology—has been noted to impede diagnostic skills of students,79 for instance. It has also been noted that the absence of certain populations—even at the level of technical materials—may inform the association doctors make between race and disease risk, thereby maintaining or exacerbating existing health disparities.60, 61 North American medical students report that a small amount of time is dedicated in the undergraduate curriculum to topics related to LGBTQ+ patients80 and that they feel unprepared to provide appropriate counselling to this population.81 According to feminist theorists, homogeneous depictions of patients in medical education are considered a form of neo-colonialism82 and perpetuate a ‘logic of eugenics’ designed to serve some bodies instead of all.83 Comprehensive resources—including classroom materials—have been identified as a critical method for improving cultural competency in students by heightening their awareness of and comfort in interacting with diverse patient groups.84 The results of this study reveal one aspect of the curriculum where patient representation needs to be improved (PE classroom materials) but also serve as a broader example of how cultural competency skills may need further emphasis across all stages of medical training.
본 연구의 한계 측면에서, 이 프로젝트의 범위는 중요한 사례 표본을 추출할 수 있도록 허용되었으며, 학교 커리큘럼에 따른 차이가 존재한다는 점에 유의해야 한다. 앞서 언급한 바와 같이, 이 난해한 데이터에 존재하는 특정 결함은 의료 훈련의 다른 곳에서 다루어질 수 있다. 이 주제에 대한 추가 연구는 학습 자료를 더 광범위하게 조사할 수 있다.
- 넓은 관점(즉, 강의실 및 표준화된 환자 세션에서 학습에 대한 더 많은 문서 또는 민족지학적 관찰)
- 샘플 관점(즉, 더 많은 학교)
미래의 연구는 또한 다른 '예외적' 절차 또는 일반적으로 PE를 통한 환자 관점에 대한 지식과 인식과 관련하여 의대생들의 학습 경험에 대해 인터뷰할 수 있다.
In terms of limitations of this study, the scope of this project allowed for a critical-case sampling, and it must be noted that jurisdictional variations across school curricula do exist. As previously mentioned, certain deficiencies present in this discursive data may be addressed elsewhere in medical training. Further research into this subject could examine learning materials more extensively, from both
- a breadth perspective (i.e. more documents and/or ethnographic observations of learning in classroom and standardised patient sessions) and
- a sample perspective (i.e. more schools).
Future studies could also interview medical students about their learning experiences with respect to their knowledge and awareness of patient perspectives with the PE, with other ‘exceptional’ procedures or in general.
5 결론
5 CONCLUSION
PE의 가르침은 의학 교육의 문제를 제기했으며, 계속해서 그러하고 있다. 텍스트 및 시각 기반 커리큘럼은 의대생들이 배우는 방법의 한 측면을 나타내지만, 이러한 자료에서 담론은 중요하고, 그들의 해석은 다양한 환자 커뮤니티의 경험과 건강 결과에 영향을 미칠 수 있다. 이러한 이유로 교과서와 기술 기술 지침서의 기본 수준에서도 환자 중심적이고 문화적으로 유능한 접근법이 의료 커리큘럼뿐만 아니라 PE의 사례 연구에서도 더욱 강조되어야 한다. PE 훈련은 큰 진전을 이뤘고, 이 연구의 특이치 사례에서 볼 수 있듯이, 여전히 그것의 교육을 개선하기 위한 노력이 이루어지고 있다. 그러나 보다 [다양하고 포용적인 의료행위를 향한 진전]은 결코 유한하지 않으며, 바이오메디컬도 예외가 아니다. 커리큘럼은 지속적인 분석과 개선이 필요하며, PE와 다른 '예외' 절차에 대한 묘사는 특정한 주의를 필요로 할 수 있다.
The teaching of the PE has posed and continues to pose challenges in medical education. Text and visual-based curricula represent one facet of how medical students learn, but discourses in these materials matter, and their interpretations can impact the experiences and health outcomes of various patient communities. It is for these reasons that—even at the basic level of textbooks and technical skills guides—patient-centred and culturally competent approaches must be further emphasised both here in this case study of the PE as well as in the medical curriculum more broadly. PE training has come a long way, and efforts are still being made to improve its teaching, as reflected in this study's outlier cases. But progress towards more diverse and inclusive practices is never finite, and biomedicine is no exception. Curricula need constant analysis and improvement, and depictions of the PE and other ‘exceptional’ procedures may require specific attention.
'Poorly relaxed women': A situational analysis of pelvic examination learning materials for medical students
PMID: 35086164
DOI: 10.1111/medu.14737
Abstract
Background: Certain clinical pelvic examination (PE) teaching methods have been critiqued for prioritising student learning over patient autonomy and for not accurately representing diverse patient communities. As such, patient-centred and culturally competent approaches to the PE may need further emphasis in the medical curriculum-in particular, in content delivered to students before patient interaction. Classroom materials serve as students' first exposure to the sensitive procedure. This research explores how patients are represented in these materials.
Methods: A situational analysis was conducted on 10 purposively sampled PE learning materials for the 2019/20 academic year from five undergraduate medical schools in Canada. Situational analysis focuses on analysing discourse but is epistemically aligned with post-structuralism (most notably Foucault's theories involving discursive power) and allows for specific consideration of 'silences' in the data. Collected data were analysed using cartographic approaches according to this methodology, with particular attention paid to the tenets and frameworks of patient-centred and culturally competent care.
Results: Overall, content in these materials misrepresented and under-represented patients. Materials contained both outdated and unnecessarily sexualised language, in addition to a lack of patient diversity. Clinical authority was often centred over patient agency, and several updated PE techniques known to improve patient experience were absent. Patient-centred and culturally competent approaches were therefore inadequately highlighted in most of the materials.
Conclusions: Depictions contained in these materials may be perpetuating stereotypes and biases in medicine and may be working to maintain teaching practices that cause harm to patients (standardised and regular) who students interact with in both clinical and educational settings. Efforts may be needed to improve classroom materials on the PE so that they more adequately centre patients and provide opportunities to discuss culturally competent approaches to the procedure that (i) may not be covered in other parts of the PE curriculum and (ii) can reduce known health disparities.
© 2022 Association for the Study of Medical Education and John Wiley & Sons Ltd.
'Articles (Medical Education) > 임상교육(Clerkship & Residency)' 카테고리의 다른 글
| 협력적 스킬 학습에 그룹 크기가 중요한가? 무작위대조군 연구(Med Educ, 2021) (0) | 2022.08.10 |
|---|---|
| 집단적 역량: 개인적 전문성에서 협력적 전문성으로 (Perspect Med Educ, 2020) (0) | 2022.06.22 |
| 학습자의 환자중심성 개발을 위한 계획된 의학교육 전략 최전화: 현실주의 고찰(Med Educ, 2022) (0) | 2022.04.19 |
| 무대에서 연기하기: 직접관찰에 관한 전공의의 인식(Med Educ, 2017) (0) | 2022.02.27 |
| 전문직 정체형 형성을 촉진하기: 코칭 대 역량(Acad Med, 2020) (0) | 2022.02.24 |