학습자의 환자중심성 개발을 위한 계획된 의학교육 전략 최전화: 현실주의 고찰(Med Educ, 2022)
Optimising planned medical education strategies to develop learners' person-centredness: A realist review
Aarti Bansal1 | Sarah Greenley2 | Caroline Mitchell3 | Sophie Park4 | Katie Shearn5 | Joanne Reeve1

1 소개
1 INTRODUCTION
[사람 중심성]은 임상의가 효과적인 의료 서비스를 제공하는 데 필수적인 속성으로 인식되고 있으며, 의학교육에서 옹호되는 성과이다. 사람 중심의 의사소통 기술 훈련은 많은 의학 교육 커리큘럼의 확립된 부분이다. 3 그러나, 사람 중심의 태도가 의학 교육이 진행됨에 따라 증가하지 않으며, 오히려 감소할 수 있다는 우려가 있었다. 최근 몇 년 동안, 종적 통합 임상실습(LIC)과 같은 특정 유형의 의학교육이 어떻게 [사람 중심성]을 지원할 수 있는지에 대한 증거를 여러 연구가 제시해 왔다. 그러나, 우리는 사람 중심성를 발전시키는 것을 목표로 하는 계획된 광범위한 의학 교육 프로그램이 어떻게, 왜, 그리고 어떤 상황에서 성공하는지 아직 충분한 이해를 하지 못하고 있다. 이 지식은 우리가 사람 중심 의사들의 발전을 위해 의학 교육을 최적화하기 위해 중요하다.
Person-centredness is recognised as an essential attribute for clinicians to deliver effective health care1 and is an espoused outcome for medical education.2 Person-centred communication skills training is an established part of many medical education curricula3; however, there has been concern that person-centred attitudes do not increase in learners as they progress through medical education and may decline.4-10 In recent years several studies have offered evidence on how certain types of medical education, such as longitudinal integrated clerkships (LICs),11-13 can support person-centredness. However, we still have insufficient understanding as to how, why and in what circumstances the range of planned medical education programmes that aim to develop person-centeredness are successful or not. This knowledge is important if we are to optimise medical education for the development of person-centred practitioners.
[사람 중심성]은 [무엇이 건강과 임상적 역할을 구성하는지]에 대한 사람의 관점을 가이드하는 [해석주의적 인식론적 틀]에 기초한다. 이 관점은 [실증주의적 생의학적 관점]과 대조적으로 설명되는 경우가 많다.
- [실증주의적 생의학적 관점]에서는 [환자의 질병에 대한 보고]는 질병 과정의 존재를 나타내기 위해 취해지며, 임상의의 '전문가' 역할은 환자의 질병을 치료하거나 개선하기 위한 정확한 진단과 관리로 제한된다.
- [사람 중심적 관점]은 그 사람이 [생물심리사회적 요인과 다른 요인의 복잡한 상호 작용]이며, 그들의 건강 목표가 그들의 고유한 맥락과 그들에게 중요한 점의 관점에 의해 inform되는, 독특한 개인임을 인식한다.
- 그것은 환자의 주관적인 지식과 전문성을 인정하며, 공유된 의사 결정 과정에서 동등한 파트너로서 환자와 협력하고자 한다.
- 또한 관계의 질이 건강 결과에 영향을 미치며, [의료 전문가의 자기 인식]이 사람 중심 접근법의 중요한 구성 요소임을 인정한다.
Person-centredness is based on an interpretivist epistemological framework14 which guides one's perspective on what constitutes health and one's clinical role.
- It is often described in contrast to a positivist biomedical perspective in which patients' reports of illness are taken to indicate the existence of disease processes and the clinician's ‘expert’ role is limited to accurate diagnosis and management of disease to cure or improve the patient's illness.15
- A person-centred perspective recognises that the person is a unique individual whose health is a complex interplay of biopsychosocial and other factors and whose health goals will be informed by their unique context and in terms of what matters to them.16, 17
- It recognises patients' subjective knowledge and expertise and seeks to work with patients as equal partners in a shared decision making process.16
- It also recognises that the quality of relationships influences health outcomes and that health care professionals' self-awareness is a vital component of a person-centred approach.18, 19
경험적 문헌에 대한 미드와 바워의 리뷰는 환자 중심성의 다섯 가지 개념 영역을 설명한다.
- 생물심리사회적 관점,
- '사람으로서의 환자',
- 권력과 책임의 공유,
- 치료 동맹,
- '사람으로서의 의사'
Mead and Bower's review of the empirical literature describe five conceptual domains of patient-centredness:
- biopsychosocial perspective,
- ‘patient-as-person’,
- sharing power and responsibility,
- therapeutic alliance and
- ‘doctor-as-person.’20
사람 중심 이론은 임상 실무에 대한 사람 중심 접근에 대한 개념적이고 증거적인 근거를 포함한다.
Person-centred theory involves the conceptual and evidential rationale for a person-centred approach to clinical practice.21
'환자 중심'과 '사람 중심'이라는 용어는 종종 상호 교환적으로 사용되며, 이러한 용어를 뒷받침하는 개념 영역에는 상당한 중복이 있다. 최근 몇 년 동안, 환자로서의 지위뿐만 아니라 개인의 인격을 인정하는 '사람 중심'이라는 용어로의 움직임이 있었다. 그러므로 우리는 리뷰에서 '사람 중심'이라는 용어를 사용하기로 결정했다.
The terms ‘patient-centred’ and ‘person-centred’ are often used interchangeably, and there is considerable overlap in the conceptual domains underpinning these terms. In recent years, there has been a move towards the term ‘person-centred’ to acknowledge the personhood of an individual and not just their status as a patient.22 We therefore chose to use the term ‘person-centred’ in our review.
의료 교육에서 사람 중심의 교육은 종종 [스킬과 역량]의 관점에서 개념화된다. 그러나 연구에 따르면 생물의학 임상의의 관점은 사람 중심의 치료를 제공하는 데 장애가 될 수 있으며, 사람 중심의 접근법은 '당신은 뭐가 문제에요?'에 초점을 맞추는 것에서 '당신에게 중요한 것이 무엇인가요?'에 초점을 맞추는 관점의 전환을 필요로 한다고 주장되어 왔다. 다양한 정책 논문은 [사람 중심 진료에 전념하는 노동력]이 사람 중심 진료 제공에 필수적인 기둥이며, [사람 중심 가치와 원칙]이 사람 중심 행동을 안내하는 데 필수적이라고 권고한다. 의료 교육 전략에 격차가 있는지, 현재 의사소통 능력 훈련에 초점을 맞추고 있는 것이 사람 중심의 이론을 간과할 수 있는지 물었다.
Teaching of person-centredness in medical education is often conceptualised in terms of skills and competencies.23 However, studies have shown that biomedical clinician perspectives may be a barrier to delivering person-centred care24, 25 and it has been argued that a person-centred approach requires a perspective shift from a focus on ‘what is the matter with you?’ to ‘what matters to you?’26 Various policy papers recommend that a workforce committed to person-centred practice is an essential pillar in delivering person-centred care1, 27 and that person-centred values and principles are essential to guiding person-centred behaviours.28 We queried whether there is a gap in medical education strategy and if the current focus on communication skills training may overlook person-centred theory.
우리의 검토는 다음 질문에 대한 답을 찾기 위해 노력했다.
- 사람 중심성 개발에 계획된 의료 교육 개입의 성공 또는 실패로 이어지는 특정 맥락에서 촉발된 핵심 메커니즘은 무엇인가?
- 이러한 설명들이 교육 정책, 관행, 연구에 어떤 영향을 미칠까?
Our review sought to answer the following questions:
- What are the key mechanisms, triggered in particular contexts, that lead to the success or failure of planned medical educational interventions in developing person-centredness?
- How might these explanations influence educational policy, practice, and research?
우리의 검토의 목적은 의료 교육자와 정책 입안자에게 유용한 검증 가능한 이론을 만드는 것이었다. 이러한 이유로, 우리는 더 넓은 의료 환경에서 발생하고 의료 교육이 제한된 영향력을 가질 수 있는 경험 있는 교육 과정과는 반대로 계획된 교육 커리큘럼에 초점을 맞추기로 선택했습니다. 우리는 사람 중심의 결과를 관점으로 개념화하여 학습자의 수준에 검토를 집중하기로 결정했다.
The objective of our review was to produce testable theory useful to medical educators and policymakers. For this reason, we chose to focus on the planned education curriculum as opposed to the experienced curriculum which occurs in the wider health care context and over which medical education may have limited influence. We conceptualised the outcome of person-centredness as a perspective and so chose to focus our review at the level of the learner.
2 방법
2 METHODS
우리는 이것이 정책과 실무를 알리기 위해 고안된 실용적인 방법론적 접근 방식이기 때문에 [현실주의 검토]를 수행하기로 결정했다. [현실주의 연구]는 의학 교육(29)과 같은 복잡한 개입을 조사하고 질적, 양적 및 혼합 방법 연구를 합성하는 데 특히 적합하다. 개입이 작동하는지 여부를 이해하고자 하는 표준 체계적 검토와 달리, 현실주의 검토는 설명적인 초점을 가지고 있으며, 어떤 상황에서 어떤 것이 누구에게 효과가 있는지 이해하려고 한다. 우리의 연구는 관점의 수준에서 결과를 이해하는 데 초점을 맞췄고, 따라서 '메커니즘'의 개념을 사용하는 것은 [인간 추론 수준]이며, 여기서 그것은 그들이 제공하는 교육 프로그램에 대한 학습자의 반응을 나타낸다. 본 논문은 현실주의자 및 메타나래티브 증거 합성에 따른 검토를 보고한다. 발전하는 표준(RAMESES) 출판 표준. 심사는 학부 및 대학원 의학 교육(AB, JR, SP, CM) 경험이 풍부한 의사 4명과 현실주의 방법론자(KS), 정보전문가(SR) 등 6명으로 구성된 팀이 진행했다.
We chose to conduct a realist review as this is a practical methodological approach designed to inform policy and practice. Realist research is also particularly suitable for investigating complex interventions, such as those in medical education,29 and for synthesising qualitative, quantitative and mixed-methods research. Unlike standard systematic reviews that seek to understand whether an intervention works, realist reviews have an explanatory focus and seek to understand what works for whom and in what circumstances.30 Our research focused on understanding outcomes at the level of perspective and so our use of the concept of ‘mechanism’ is at the level of human reasoning,31 where it represents learners' responses to the educational programme they are offered. This paper reports the review according to the Realist and Metanarrative Evidence Syntheses: Evolving Standards (RAMESES) publication standards.32 The review was conducted by a six-person team which included four doctors with extensive experience in undergraduate and postgraduate medical education (AB, JR, SP and CM), a realist methodologist (KS) and an information specialist (SR).
2.1 단계(i): 초기 프로그램 이론 개발
2.1 Step (i): Developing an initial programme theory
우리의 첫 번째 단계는 데이터 수집과 분석을 안내하는 초기 프로그램 이론을 설명하는 것이었다. 우리는 Shearn 등이 개략적으로 설명한 세 가지 전략을 채택했다.
- 우리 연구팀이 보유한 암묵적 이론을 추출하고,
- 실질적인 교육 학습 이론의 개념을 사용하며,
- 학문적 및 회색 문헌의 탐색적 검색에서 암묵적 이론을 추출한다.
범위 지정 검색에 대한 자세한 내용은 개방형 과학 프레임워크에서 확인할 수 있다. 이러한 출처는 그들이 대표하는 학습 유형을 기반으로 3개의 초안 프로그램 이론으로 구성된 초기 프로그램 이론을 구성하도록 구성된 이론 개념을 생성했다.
- 인지적(사람 중심 치료의 대상),
- 구성주의적(교육적 학습 환경)
- 경험적(경험적 배치)
우리의 초기 프로그램 이론의 세부사항은 부록 S1에 있다.
Our first step was to describe an initial programme theory to guide data collection and analysis. We adopted three of the strategies outlined by Shearn et al.33:
- extracting tacit theories held by our research team,
- using concepts from substantive educational learning theory and
- extracting tacit theories from exploratory searches of the academic and grey literature.
Details of our scoping searches are available at the open science framework (https://osf.io/qnkfh/?view_only=d1d36e578dd449a78ec62b13e2efebc5). These sources produced theory concepts that were configured to form an initial programme theory consisting of three draft programme theories based on the types of learning they represented:
- cognitive (theory of person-centred care),
- constructivist (transformative learning environments) and
- experiential (clinical placements).
The detail of our initial programme theory is in Appendix S1.
우리의 초기 프로그램 이론은 학부 및 대학원 의학 교육을 계획하고, 제공하고, 받는 이해 관계자들과 함께 점검되었다. 그들의 피드백은 [초기 프로그램 이론]이 연구 질문에 답하는 데 유용한 출발점을 제공했다는 것을 확인시켜 주었다. 이해관계자 그룹은 전문 그룹 차원에서 검토 범위를 논의했으며 의사의 진단 및 관리 책임이 모든 보건 전문가와 공유되지 않고 사람 중심의 접근방식 개발에 특정 영향을 미칠 수 있다는 점에서 의대생과 의사에게 검토를 집중하기로 합의했다. 학부 및 대학원 학습 전반에 걸쳐 공통적인 메커니즘이 있을 수 있으므로 의학교육의 연속체에 걸친 논문들이 포함되어야 한다는 데 의견이 일치했다.
Our initial programme theory was checked with stakeholders planning, delivering and receiving undergraduate and postgraduate medical education. Their feedback confirmed that the initial programme theory provided a useful starting point for answering the research question. The stakeholder group discussed the scope of the review in terms of professional groupings and agreed to focus the review on medical students and doctors given that the diagnostic and management responsibilities of doctors are not shared with all health professionals and may have a specific impact in the development of a person-centred approach. It was agreed that there were likely to be mechanisms in common across undergraduate and postgraduate learning and so papers from across the continuum of medical education should be included.
2.2 단계 (ii) : 증거 찾기
2.2 Step (ii): Searching for evidence
우리의 초기 프로그램 이론은 우리의 체계적인 검색 전략을 개발하기 위한 프레임워크를 제공했다. 이전의 범위 지정 검색을 통해 검색 전략을 구체화할 수 있었습니다. 예를 들어, '전문성'이라는 용어로 발견된 대부분의 논문은 숨겨진(경험은 있지만 계획되지 않은) 커리큘럼의 영향에 관한 반면, 우리의 리뷰는 [계획된 커리큘럼]에 초점을 맞췄다. 우리는 '의학 교육'과 '사람 중심' 및 관련 동의어에 대한 자유 텍스트 및 데이터베이스별 주제 제목 용어의 부울 조합을 통해 여러 전자 데이터베이스(2019년 7월 15일 OVID 인터페이스를 통한 Medline, Embase 및 HMIC)를 검색했다. 각 데이터베이스에 대한 전체 검색 전략은 부록 S2에서 확인할 수 있습니다.
Our initial programme theory provided the framework to develop our systematic search strategy. Earlier scoping searches allowed us to refine our search strategy. For example, most papers found under the term ‘professionalism’ were concerned with the impact of the hidden (experienced but not planned) curriculum, whereas our review focus was on the planned curriculum. We searched multiple electronic databases (Medline, Embase and HMIC via the OVID interface and ERIC via the EBSCO interface on 15 July 2019) through Boolean combinations of free-text and database-specific subject heading terms for ‘medical education’ and ‘person-centred’ and related synonyms. Full search strategies for each database can be found in Appendix S2.
우리는 이러한 용어를 사용하지 않고 사람 중심의 가치, 태도 및 신념에 대한 데이터를 포함할 수 있는 유용한 논문을 놓치고 싶지 않았기 때문에, 결과outcome에 대한 검색 용어를 포함함으로써 검색을 제한하지 않았다. 또한 범위 지정 단계에서 회색 문헌에 대한 이전 검색에서 확인된 관련 연구가 포함되었다. 우리는 이것이 의료 교육에서 환자 중심성과 사람 중심성의 개념이 확립된 시기라고 추론했기 때문에 이 검색은 영어와 2000년 이후 발표된 결과로 제한되었다. 인용 추적 및 저자와의 접촉을 포함한 CLASTER 방법을 사용하여 매우 관련성이 높은 연구와 관련된 추가 논문이 발견되었다. 합성이 진행되면서 '감정 거리를 유지하는 것으로 이해되는 전문성'에 대한 이론의 새로운 요소가 등장했고, 현실주의 합성에서도 권장되는 것처럼, 이 이론의 요소를 뒷받침하거나 반박하거나 다듬을 증거를 찾기 위해 구글 스콜라를 이용해 추가 검색을 했다.
We did not limit the search by including search terms on outcomes as we did not want to miss useful papers that may include data on person-centred values, attitudes and beliefs without using these terms. In addition, relevant studies identified from a previous search for grey literature at the scoping stage were included. The search was limited to the English language and to results published since 2000 as we reasoned that this was when the concepts of patient-centredness and person-centredness became established in medical education. Additional papers relating to highly relevant studies were found using the CLUSTER method34 including citation tracking and contact with authors. As the synthesis progressed, a new element of theory emerged on ‘professionalism being understood as maintaining emotional distance’, and as is recommended in realist synthesis,35 we did additional searching, using Google Scholar, to look for evidence to support, refute or refine this element of theory.
2.3 단계 (iii): 문서의 선정 및 평가
2.3 Step (iii): Selection and appraisal of documents
논문의 선택은 주로 [RAMESS 식별된 관련성 원칙]에 기초했으며, 기사가 연구 질문을 조명하고 이론 개발에 기여했는지 여부이다. 포함 대상 연구 유형에 대한 제한은 없었다. 심사는 AB가 주도했으며, JR, CM, SM, KS 또는 SG가 추상 및 전체 텍스트 단계에서 두 배로 평가한 타이틀의 10%를 무작위로 샘플링했다. 우리는 의대생과 의사를 위한 [계획된 교육 개입]이 있는 논문을 [사람 중심성과 관련된 결과]에 대한 데이터와 함께 포함시켰다. 현실주의 종합에서, 이론 개발을 지원하기 위해 학문적 경계를 넘어서는 관련 데이터의 포함이 권장된다. 따라서 우리는 다른 보건 전문가들이 프로그램 이론의 전반적인 개발을 지지한다고 생각했기 때문에 다른 의료 전문가들과 관련된 세 개의 논문을 우리의 검색에 포함시키기로 합의했다. 숨겨진 커리큘럼에 관한 논문, 개입이 없거나 개입에 대한 설명이 너무 짧아 설명을 도출할 수 없는 논문은 제외했다. 공식 의료 교육 프로그램의 일부가 아닌 특정 정책 맥락에 특정한 의료 개입도 제외되었다(예: 미국의 개인 중심 의료 가정 개입). 또한 행동 수준에서 결과만 보고한 논문(예: 의사소통 능력 향상)도 제외했다. 완전한 포함 및 제외 기준은 PROPERO 데이터베이스에 게시된 프로토콜(CRD4202020168197) 내에서 확인할 수 있다.
Selection of articles was based primarily on the RAMESES identified principle of relevance, whether the article illuminated the research question and contributed to theory development.35 There was no restriction on the type of study eligible for inclusion. Screening was led by AB with a random sample of 10% of titles double appraised by JR, CM, SM, KS or SG at both abstract and full-text stages. We included papers with a planned educational intervention for medical students and doctors with data on outcomes related to person-centredness. In realist synthesis, the inclusion of relevant data from across disciplinary boundaries is encouraged to support theory development. We therefore agreed to include three papers that were returned in our search, which related to other health professionals as we felt they supported the overall development of programme theory. We excluded papers that were about the hidden curriculum, where there was no intervention or where the description of the intervention was too brief to derive explanation. Health care interventions that were specific to a particular policy context and not part of a formal medical educational programme, were also excluded (e.g. person-centred medical home interventions in the USA). We also excluded papers that only reported outcomes at behavioural level (e.g. improvement in communication skills). Full inclusion and exclusion criteria can be found within the protocol published on the PROSPERO database (CRD42020168197).
2.4 단계 (iv) : 데이터 추출 및 정리
2.4 Step (iv): Extracting and organising data
데이터를 추출하기 전에 먼저 포함된 전체 텍스트 논문을 모두 읽고 데이터에 익숙해지십시오. 각 논문의 연구 특성과 요약 결과에 대한 데이터를 Excel 스프레드시트로 추출했습니다. 또한, 각 논문은 연구 결과가 일관되고 타당하다고 간주되었는지 여부에 따라 엄격(높거나 낮음)에 대해 평가되었다. 코딩은 둘 다였다.
- 귀납적, 즉, 코드는 데이터에서 식별되었다.
- 연역적, 즉 초기 프로그램 이론에 의해 정보를 제공받았다.
Before extracting the data, first read all the included full-text papers to familiarise herself with the data. Data on study characteristics and summary findings for each paper was extracted into an Excel spreadsheet. In addition, each paper was assessed for rigour (high or low) based on whether its findings were considered coherent and plausible. Coding was both
- inductive, i.e., codes were identified from the data, and
- deductive, i.e., they were informed by the initial programme theory.
각 논문은 NVivo 12(QSR International, Warrington, UK) 정성 데이터 분석 소프트웨어에 업로드되어 세분화된 수준의 텍스트 코딩을 용이하게 했다. 이러한 코드화된 데이터는 개념으로 묶인 다음 'if-then' 설명문으로 발전되었다. 그런 다음 각 논문의 조사 결과에 대한 설명이 Excel 스프레드시트로 옮겨져 논문 간 설명을 쉽게 볼 수 있게 되었습니다. 이러한 설명은 색상으로 구분되어 있어서 초안 프로그램 이론을 지지, 정제 또는 반박했는지 또는 새로운 이론에 영감을 주었는지 쉽게 확인할 수 있었다. 우리의 현실주의 합성에 포함된 연구의 세부 사항이 포함된 표는 부록 S3에서 이용할 수 있다.
Each paper was uploaded onto NVivo 12 (QSR International, Warrington, UK) qualitative data analysis software, to facilitate coding of text at a granular level. These coded data were grouped into concepts and then developed into ‘if–then’ explanatory statements. Explanations of each paper's findings were then transferred to the Excel spreadsheet for ease of looking at explanations across papers. These explanations were colour coded so we could easily see if they supported, refined or refuted the draft programme theories or whether they inspired new theory. A table with details of studies included in our realist synthesis is available in Appendix S3.
2.5 단계(v): 데이터 합성
2.5 Step (v): Data synthesis
데이터 합성 과정에는 결과에 대한 현실적인 인과적 설명을 개발하는 데 도움이 되도록 [데이터와 이론 사이를 지속적으로 이동]하는, [몇 가지 반복적인 사이클]이 포함되었다. 새로운 연구 결과는 설명의 일관성과 타당성을 보장하기 위해 정기적인 연구팀 회의에서 비판적인 평가를 받았다. 우리의 현실적인 설명 이론을 개발하기 위해, 우리는 특정 교육 전략과 결과 사이에 반복적인 패턴(반규칙성)이 있는지 알아보기 위해 논문을 통해 살펴봤다. 그런 다음 결과 및/또는 저자 제안을 찾고 이러한 결과가 어떻게 발생했는지 설명할 수 있는지 유괴적 추론을 사용했다. 그런 다음 데이터 합성은 우리의 이론에 대한 확인 및 확인 증거와 학습자 관점의 변화 또는 결여를 설명할 수 있는 새로운 설명을 위해 데이터를 살펴보는 것을 포함했다.
The data synthesis process involved several iterative cycles where we continually moved between data and theory to help us develop realist causal explanations for outcomes. The emerging findings were subject to critical appraisal at regular research team meetings to ensure the coherence and validity of the explanations. To develop our realist explanatory theories, we looked across papers to see if there were repeated patterns (demi-regularities) between particular educational strategies and outcomes. We then looked for results and/or author suggestion and used abductive reasoning to see if we could explain how these outcomes occurred (mechanisms). Data synthesis then involved looking across the data for confirmatory and disconfirmatory evidence for our theories and, indeed, novel explanations that might explain the change in learner perspective or lack thereof.
[학습 전 학습자의 관점]은 학습에 대한 반응을 나타내는 데이터로부터 추론되었다. 우리는 사람 중심의 관점을 지원하는 것을 목표로 한 모든 개입 전략이 사람 중심의 관점으로 기울어진 참가자들의 관점을 검증했다는 것을 발견했다. 보다 [생물의학적 관점으로 기울어진 학습자들]은 학습에 대해 다양한 반응을 보였으며, 이는 우리의 질적 및 양적 데이터 모두에 반영되는 지배적인 학습자의 관점이었다. 이 단계에서 우리는 [생물의학적 관점으로 기울어진 학습자]에게 교육 전략이 미치는 영향에 대한 설명을 제공하는 데이터 하위 집합에 검토를 집중하기로 결정했다. RAMESES 지침에 따라, 우리는 [학습자의 사람 중심성]을 지원하기 위해 [계획된 의료 교육 전략]이 [어떻게 최적화될 수 있는지]에 대한 문제를 해결하는 측면에서, 교육자와 정책 입안자로서 이 초점이 그들에게 가장 유용할 것이라는 데 동의한 이해관계자들과 함께 점검했다.
A learner's perspective prior to learning was inferred from data indicating their response to the learning. We found that all interventional strategies that aimed to support person-centredness validated the perspective of participants who leaned towards a person-centred perspective. Learners who leaned towards a more biomedical perspective had variable responses to learning and this was the predominant learner perspective reflected in both our qualitative and quantitative data. At this stage, we chose to focus our review on the subset of data that provided explanations of the impact of educational strategies on learners who leaned towards a biomedical perspective. In line with RAMESES guidance,35 we checked with our stakeholders who agreed this focus would be most useful to them as educators and policymakers in terms of addressing the question of how planned medical educational strategies can be optimised to support learners' person-centredness.
[이론 구성]을 구체화하는 데 몇 가지 모델을 사용할 수 있다. 우리는 [학습자 컨텍스트]를 [교육 전략]과 분리하는 것이 관점의 변화로 이어지는 메커니즘을 분리하는 데 도움이 된다는 것을 발견했다. 따라서 우리는 현실주의적 인과적 설명에 문맥-개입-메커니즘-결과 구성(CIMOc)을 사용하기로 결정했다. 우리는 결과에 따라 CIMOc를 그룹화했고, 역작업은 사람 중심의 관점의 변화로 이어지는 메커니즘(또는 그렇지 않은)을 촉발시킨 교육 전략의 주요 특징을 조사하여 전체 프로그램 이론을 구성할 수 있었다.
Several models are available for articulating theory configurations.36, 37 We found that separating the learner context from the educational strategy helped us to isolate the mechanisms leading to changes in perspective. We therefore chose to use the context–intervention–mechanism–outcome configuration (CIMOc) for our realist causal explanations. We grouped CIMOcs based on their outcome and working backwards were able to investigate the key features of the educational strategies that triggered the mechanisms leading to a change in person-centred perspective (or not) and so to construct an overall programme theory.
3 결과
3 RESULTS
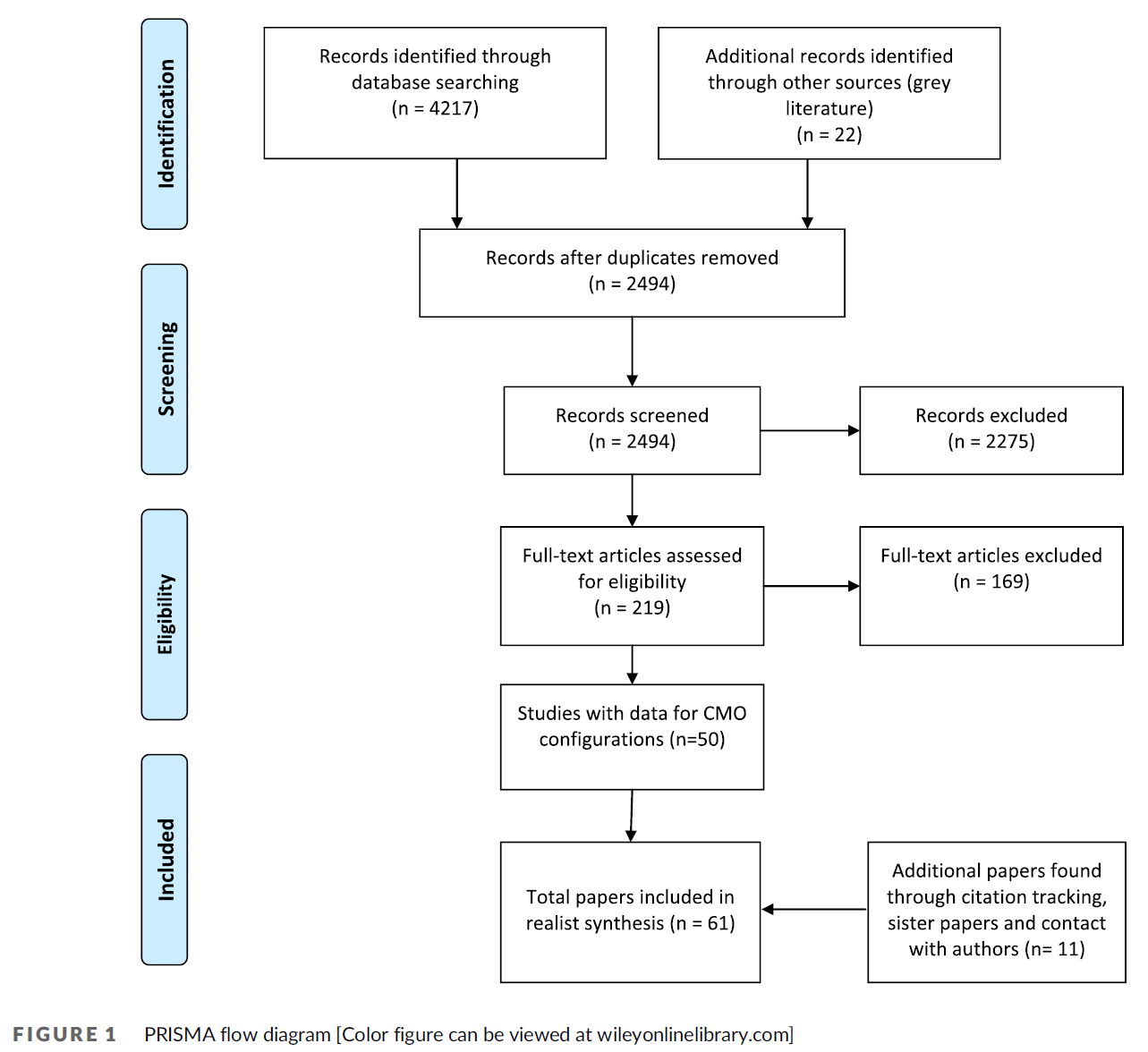
초기 검색 결과 4217개의 결과가 나왔다. 그림 1은 최종 현실주의 합성에 61개의 논문 또는 문서가 포함되게 된 필터링 과정을 보여줍니다. 8개의 논문이나 문서가 같은 '개입'을 보고 있었기 때문에 교육개입이 53개였다.
- 37번의 개입에서 학습자는 학부생이었습니다.
- 11학년 때, 그들은 훈련 중인 대학원 박사들이었습니다.
- 5명 중, 그들은 숙련된 임상의사 또는 다학제 팀들이었습니다.
교육 개입은 전 세계에 걸쳐 이루어졌지만, 대다수가 북아메리카와 유럽(북미 23명, 유럽 20명, 아시아 5명, 호주 4명, 아프리카 1명)에서 왔다.
The initial search yielded 4217 results. Figure 1 illustrates the filtering process that resulted in 61 papers or documents being included in the final realist synthesis. Eight papers or documents were looking at the same ‘intervention’, so the number of educational interventions looked at was 53.
- In 37 interventions, learners were undergraduates;
- in 11, they were postgraduate doctors-in-training; and
- in five, they were experienced clinicians or multidisciplinary teams in work.
The educational interventions spanned the globe, although the majority were from North America and Europe (23 in North America, 20 in Europe, five in Asia, four in Australia and one in Africa).
중재적 전략은 크게 세 가지 유형이 있었다:
- 사람 중심의 의사소통 기술 훈련,
- 사람 중심 이론과 개입이 없이 사람 중심 이론의 다양한 조합을 제공하는 환자 경험
- 환자 내러티브 또는 일정시간에 걸친 실제 환자와의 관계(의미 있는 경험)에 참여하고, 반응을 이해할 수 있는 기회.
There were three main types of interventional strategy:
- person-centred communication skills training,
- patient experiences without person-centred theory and interventions that offered various combinations of person-centred theory,
- engagement with patient narrative or real patients over time (meaningful experience) and opportunities to make sense of responses to learning.
개입 기간은 짧은 단일 세션에서 4년 동안 소규모 그룹에서의 정규 학습에 이르기까지 매우 다양했다. 질적 데이터를 제공한 논문은 37편, 정량적 데이터가 14편, 질적 데이터와 정량적 데이터가 모두 8편, 데이터가 없는 개입(자매 논문)에 대한 서술이 2편이었다.
The length of interventions varied widely from brief single sessions to regular learning in small groups over 4 years. Thirty-seven papers offered qualitative data, 14 had quantitative data, eight papers had both qualitative and quantitative data and two were descriptions of interventions (sister papers) without data.
3.1 정제된 프로그램 이론
3.1 Refined programme theory
우리의 정제된 프로그램 이론은 사람 중심성을 개발하는 것을 목표로 하는 교육 개입이 어떻게 성공할 수도 있고 아닐 수도 있는지를 설명하는 9개의 CIMOc로 구성된다(표 1). 우리의 분석에 따르면 이러한 설명은 의학 교육 연속체(학부, 대학원 및 지속적인 전문 개발)에 걸쳐 기울어진 사람들에게 적용되었다. 그림 2는 우리의 정제된 프로그램 이론을 시각적으로 나타낸 것이다.
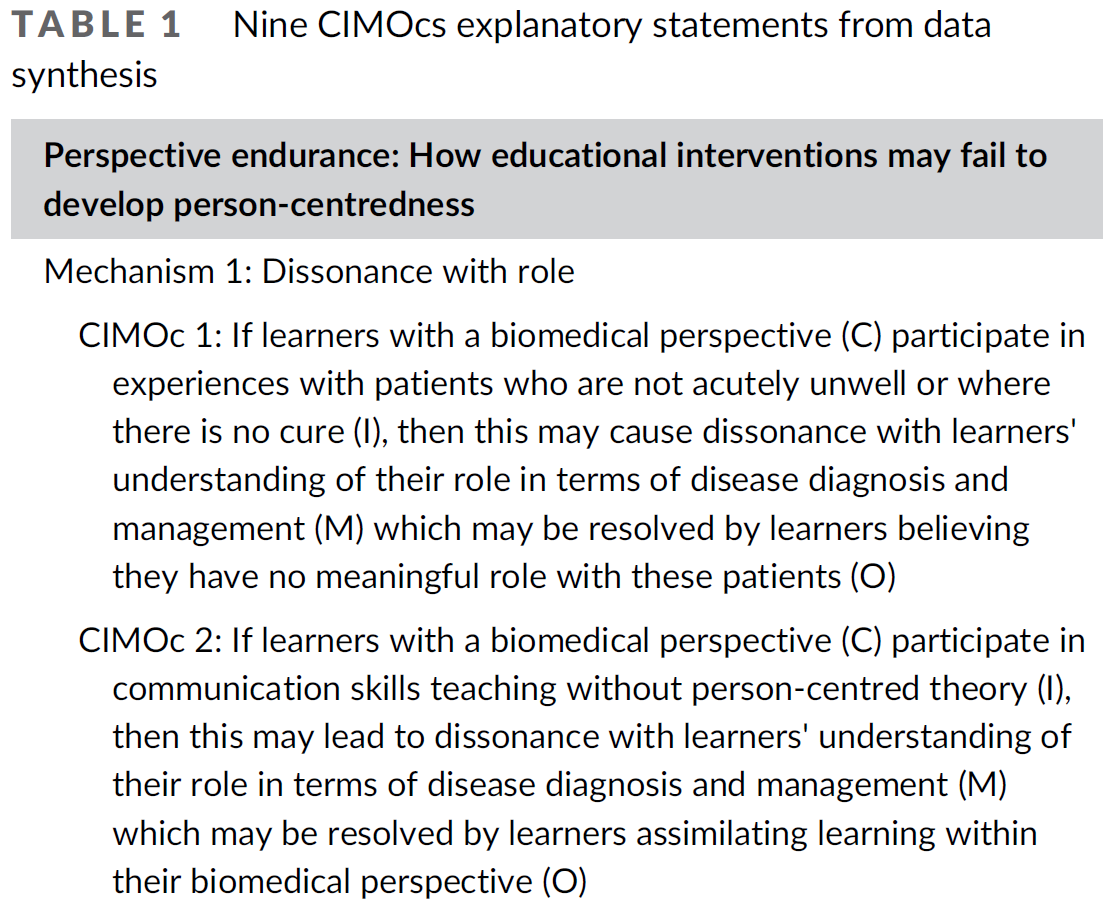
Our refined programme theory consists of nine CIMOcs that explain how educational interventions that aim to develop person-centredness may or may not succeed (Table 1). Our analysis found that these explanations applied to leaners across the medical education continuum (undergraduate, postgraduate and continuing professional development). Figure 2 is a visual representation of our refined programme theory.


3.2 관점 지속: 교육적 개입이 어떻게 사람 중심성을 발전시키지 못할 수 있는가?
3.2 Perspective endurance: How educational interventions may fail to develop person-centredness
5개의 설명문(CIMOcs 1–5)은 [사람 중심성을 증가시키는 것을 목표로 하는 교육 개입이 어떻게 실패하는지]를 설명한다. 학습자에게서 촉발된 관점지속을 이끌어내는 메커니즘은 모두 [인지적 부조화]와 관련이 있다: 믿음, 가치관 또는 태도가 서로 일치하지 않을 때 발생하는 불편함과 불확실성. 우리의 분석은 역할, 인식론 및 더 넓은 커리큘럼의 인지된 생물의학적 초점과 관련된 세 가지 유형의 부조화를 설명했다.
Five explanatory statements (CIMOcs 1–5) explain how educational interventions that aim to increase person-centredness may fail to do so. The mechanisms triggered in learners that led to perspective endurance all relate to cognitive dissonance: the discomfort and uncertainty that results when beliefs, values or attitudes are not consistent with each other.38 Our analysis described three types of dissonance related to role, epistemology and the perceived biomedical focus of the wider curriculum.
3.2.1 메커니즘 1: 역할에 대한 이해와 불일치
3.2.1 Mechanism 1: Dissonance with understanding of role
학습자들이 [의사로서의 역할에 대한 이해]에는 [역할의 목적]과 [직업적 행동으로 간주되는 것]이 포함되었습니다. 역할과의 불일치에 기여한 대부분의 개입은 사람 중심의 의사소통 기술 훈련을 포함한다. 몇 가지 개입에는 비교적 짧지만 환자 또는 사람 중심 이론과의 의미 있는 연결이나 연속성을 제공하지 않는 환자들에 대한 경험이 포함되었다. 분석에 따르면 역할에 대한 이러한 이해의 불일치가 세 가지 결과로 이어졌습니다.
Learners' understanding of their role as a doctor included the purpose of the role and what was considered professional behaviour. Most interventions that contributed to dissonance with role involved person-centred communication skills training.39-49 A few interventions involved experiences with patients that were relatively brief but did not offer meaningful connection or continuity with patients or any person-centred theory.50-52 Analysis revealed that dissonance in this understanding of role led to three outcomes.
CIMOc 1: 학습자는 의미 있는 역할은 없다고 생각합니다.
CIMOc 1: Learners believe they have no meaningful role
학습자들이 의사의 주요 역할이 [생물의학적 질병 진단과 관리를 통해 도움을 주는 것]이라고 믿었고, 학습 개입에서 포함된 환자가 급성 질환을 갖지 않았을 때, 일부는 이 학습이 그들의 미래 역할과 관련이 있음을 이해하기 어려워했다.
Where learners believed that the main role of the doctor is to help through biomedical disease diagnosis and management, and the learning intervention involved patients who were not acutely unwell,49, 50, 53, 54 some struggled to see the relevance of this learning to their future role.
한 사람은 비교적 건강한 환자를 따라다니라는 것은 '멍청한 생각'이라며 '대학 시절 봉사활동은 충분히 했다'고 말했다.
One commented that the requirement to follow a patient, who was relatively well, was a ‘dumb idea’, adding, ‘I did enough volunteering during undergraduate’.53
상황이 매우 어렵고, 저는 아마도 환자를 돕고 싶지만 그럴 방법이 없어서 부족하다고 느낄 것입니다.
The situation is extremely difficult, and I would probably feel inadequate, wanting to help the patient but having no means to do that …46
두 경우 모두 [환자의 요구가 질병 진단과 관리 전문성과 맞지 않아, 유의미한 역할이 없다는 느낌]이 기존 관점을 지속하게 만들었다.
In both situations, the feeling that they had no meaningful role with patients whose needs did not fit with an expertise in disease diagnosis or management, resulted in perspective endurance.
CIMOc 2: 학습자는 생체 의학 관점에서 학습을 동화합니다.
CIMOc 2: Learners assimilate learning within their biomedical perspective
환자와 좋은 관계를 유지하는 것이 중요하다고 생각합니다.
왜냐하면 환자는 당신이 말한 대로 할 가능성이 높기 때문입니다.
I think it's important to have a good relationship with your patients because they are more likely to do what you say …49
커리큘럼이 끝날 무렵, 우리 연구의 학생들은 공개적으로 환자를 초대했고 그들은 듣고 있었습니다...
학생들은 종종 환자의 인생 경험을 생략했으며, 환자의 감정에 반응하지 않았습니다.
At the end of the curriculum the students in our study were inviting the patient openly and they were listening … The students often omitted patients' life experiences and did not respond to their emotions.48
CIMOc 3: 학습자는 전문적인 규범을 유지하고 정서적 고통으로부터 자신을 보호하기 위해 환자와의 정서적 연결을 피합니다.
CIMOc 3: Learners avoid emotional connection with patients to maintain professional norms and protect self from emotional distress
학습자의 질적 논평은, [임상적 객관성을 유지]하기 위해, [환자로부터 감정적인 분리]를 수반하는 전문적인 행동을 이해한다는 것을 보여주었다. 고통 받는 사람들과 연결되는 것을 포함하는 학습자들의 경험적 학습이 그들의 전문적인 역할에 대한 이해는 어떻게 대응해야 할지에 대한 불확실성으로 이어졌다. 학습자들은 [자신이 느끼는 괴로움을 어떻게 관리해야 할지]에 대한 불확실성뿐만 아니라, [한 명의 인간이자 전문가로서 대응해야 하는 갈등]도 경험했다. 학습자들은 전문적인 규범으로 이해하고 있는 것을 유지하고 또한 정서적 고통으로부터 자신을 보호하기 위해 환자들과의 정서적 연결을 피함으로써 그들의 불협화음과 불확실성을 해결했다. 이러한 [정서적 연결의 회피]는 학습자의 행동에서 관찰되었을 뿐만 아니라, 학습자가 학습에 대한 반응에서도 논의되었다.
Learners' qualitative comments revealed that they understood professional behaviour to involve emotional detachment from patients in order to remain clinically objective. Where learners' experienced learning that involved connecting with people who were suffering, this understanding of their professional role led to uncertainty on how to respond. Learners experienced a conflict between responding as a human being or as a professional, as well as uncertainty on how to manage the distress that they felt. Learners resolved their dissonance and uncertainty by avoiding emotional connection with patients to maintain what they understood to be professional norms and also to protect themselves from emotional distress. This avoidance of emotional connection was both observed in learner behaviour45, 48 as well as discussed by learners in response to their learning.43, 46, 52, 57
한 학생은 그들 중 한 명이 죽어가는 부부와의 만남에 대해 썼다. 배우자가 죽음의 화제에 접근하자 울기 시작했다.
그 학생은 그녀를 위로하고 싶었지만 자제했다.
그 여자의 어깨에 손을 얹었더라면 좋았을 텐데, 왜냐하면 그것은 전문적인 것이 아니었을지라도 인간적인 것이었을 것이기 때문이다.
One student wrote about her meeting with a married couple where one of them was dying. The spouse started to cry when they approached the topic of death. The student wanted to comfort her but refrained: I wish I'd put my hand on the woman's shoulder because that would have been human, even though it would not have been professional.52
내가 너무 관여하게 되면 내 삶은 너무 괴로워진다. 제게 가장 어려운 것은 환자의 감정에 너무 얽매이지 않고 '전문적인 역할'을 유지하는 것일지도 모릅니다.
If I become too involved, my own life becomes too distressing. The most difficult thing for me … may be keeping up ‘the professional role’, not getting too involved in the patient's feelings.46
3.2.2 메커니즘 2: 인식론과의 불일치
3.2.2 Mechanism 2: Dissonance with epistemology
CIIMc 4: 학습자들은 (인간 중심성에 대한) 학습이 미래의 임상 실습에 덜 중요하다고 믿습니다.
CIMOc 4: Learners believe learning is less important to future clinical practice
Many papers revealed that learners had a positivist view of knowledge and considered valid knowledge to be composed of ‘hard’ objective facts. Knowledge that required interpretation or was based on individual experience was considered less scientific and less valid as illustrated by how it referred to as ‘soft’, ‘touchy-feely’ or ‘fluffy’.40, 42, 58
선다운 의과대학 학생들이 의학의 '과학적'에 반대하며 윤리 교육을 논하고 정신 질환의 주제에 대해 어렵고 위협적이며 구체적으로는 덜 과학적이라고 말하는 방식은 모두 지식의 이해를 나타내는 것으로 보였다.
'하드' 형태와 '소프트' 형태 사이에서 상당히 강하게 양극화 되어 있었습니다.
The ways in which Sundown Medical School students opposed the ‘scientific’ to the ‘human’ side of medicine, discussed their ethics teaching, and related to the subject of mental illness as difficult, threatening and less concretely scientific all appeared to be indicative of understandings of knowledge that were quite strongly polarised between ‘hard’ and ‘soft’ forms …42
이러한 의대생들과 (아마도 일부 또는 심지어) 많은 의대생들에게 사회과학의 담론적인 성격은
종종 그것을 덜 확실하고, 자연과학의 '팩트'보다 조건적이며, 따라서 덜 타당해 보이게 한다.
For these medical students and (maybe some or even) many medical scientists, the discursive nature of social science often makes it seem less certain, more contingent than natural scientific ‘fact’ and therefore less valid.51
많은 학생들은 또한 환자의 생활 환경, 특히 사회적 관계와 근무 환경을 탐구하는 것에 대해 양심의 가책을 느꼈다고 보고했다. 그 학생들은 건강과 질병에 대한 [심리적 사회적 요인의 관련성에 대한 지식의 부족]을 드러냈다. 따라서, 그들은 전체론적 관점을 부자연스럽게 인식했다.
Many students also reported scruples about exploring the patient's life circumstances, in particular, social relations and working conditions. The students revealed a lack of knowledge about the relevance of psychosocial factors to health and disease. Thus, they perceived a holistic perspective as unnatural.44
서로 다른 개입을 가진 코호트를 비교한 정량적 데이터를 가진 논문은 사람 중심 이론이 학습에 명확하게 통합되지 않은 코호트에서 사람 중심 태도의 감소를 보였다. 이 CIMOc 를 지원하는 데이터는 학부 및 대학원 환경 및 모든 지리적 영역에서 발견되었다.
Papers with quantitative data that compared cohorts with different interventions showed a decline in person-centred attitudes in cohorts where person-centred theory was not clearly integrated into learning.59, 60 The data supporting this CIMOc were found across undergraduate and postgraduate settings and from all geographical areas.41, 42, 44, 51, 53, 56, 61, 62
3.2.3 메커니즘 3: 광범위한 커리큘럼에 초점을 맞춘 불일치
3.2.3 Mechanism 3: Dissonance with focus of the wider curriculum
CIIMc 5: 학습자는 향후 임상 실습을 위해 학습의 중요성을 최소화합니다.
CIMOc 5: Learners minimise importance of learning for future clinical practice
[핵심 교육과정의 일부인지 여부]와 [교육과정 내 질병 기반 학습에 부여된 상대적 무게]에 따라, 학습의 상대적 중요성에 대해 많은 학습자들이 힌트를 얻었다. 이는 학습자들이 '과학적' 학습만큼 중요하지 않거나, 미래 실천에 중요하지 않다고 믿고, 지식을 [위계적 범주]로 계속 분리하도록 이끌었다.
Many learners took their cue about the relative importance of learning based on whether it was part of the core curriculum and the relative weight given to disease-based learning in the curriculum. This led learners to continue to separate knowledge into hierarchical categories, believing that person-centeredness was not as important as ‘scientific’ learning or as important to future practice.42, 43, 54, 55, 61, 63
또 다른 학생은 학문적으로 능숙하고 공감적이기를 원했지만
의과대학 전체에서 [생물-의학적으로 능숙해지는 것]이 더 높은 우선 순위를 받는다고 느꼈다.
그의 생각에, 사람들은 의과대학 동안 단지 진단하고, 환자를 참조하고, 시간표와 관련된 것만 배운다.
Another student wanted to be both academically skilled and empathetic but felt that being bio-medically skillful is given higher priority throughout medical school. In his opinion, one learns only to diagnose, refer patients, and relate to a time schedule during medical school.43
3.3 관점 변환: 교육적 개입이 사람 중심성을 개발하는 데 어떻게 성공할 수 있는가?
3.3 Perspective transformation: How educational interventions may succeed in developing person-centredness
데이터 합성(CIMOCs 6–9)의 네 가지 설명문은 교육 개입이 [사람 중심성에 대한 관점 변환으로 이어지는 방법]을 설명한다(표 1). 이 네 가지 진술에 대한 비판적 분석을 통해 사람 중심의 변화를 촉진하는 두 가지 중요한 메커니즘이 확인되었다.
- 임상실무에서 사람 중심의 관련성에 대한 명확성 제고
- 감정을 처리하고 가정에 도전할 수 있도록 지원
Four explanatory statements from our data synthesis (CIMOCs 6–9) explain how educational interventions may lead to perspective transformation towards person-centredness (Table 1). Critical analysis of these four statements identified two overarching mechanisms that prompted change towards person-centredness:
- greater clarity on the relevance of person-centredness to clinical practice and
- support to process emotions and challenge assumptions.
36편의 논문은 사람 중심성을 향한 관점 변환에 대한 설명에 기여했다.이 논문들 중에서, 31개의 개입은 사람 중심의 이론, 의미 있는 경험, 학습에 대한 응답을 이해할 수 있는 기회 등 두 가지 메커니즘을 촉발할 수 있는 요소의 조합을 제공했다. 이러한 설명에 기여한 다섯 편의 논문만이 이론이나 분별력 없는 경험을 제공했다. 이 다섯 가지 개입에서 제공된 경험은 본질적으로 종단적이거나 환자를 돌보는 데 있어 적극적인 사람 중심 역할을 포함했으며, 이 두 가지 모두 학생들이 임상 실습에 대한 사람 중심성의 관련성에 대해 개인적으로 성찰할 수 있게 해주었을 가능성이 높다.
Thirty-six papers contributed to explanations on perspective transformation towards person-centredness.49, 58, 59, 63-95 Out of these papers, 31 interventions offered a combination of the components that enabled both mechanisms to be triggered: person-centred theory, meaningful experiences and opportunity to make sense of one's responses to learning. Only five papers that contributed to these explanations offered experiences without theory or sense-making opportunities.63, 68, 73, 84, 87 The experiences offered in these five interventions were either longitudinal in nature or involved an active person-centred role in caring for patients, both of which are likely to have enabled students to personally reflect on the relevance of person-centredness to clinical practice.
3.3.1 메커니즘 1: 임상 실무에서 [사람 중심성의 관련성]을 명확히 함
3.3.1 Mechanism 1: Clarity on relevance of person-centredness to clinical practice
CIMOc 6: 건강을 [전체론적으로 이해]하고, [돌봄의 개인화]를 가치 있게 생각합니다.
CIMOc 6: Understand health as holistic and value personalisation of care
[사람 중심의 이론을 의미 있는 경험에 적용한 개입]은, 학습자가 환자 치료에 대한 사람 중심의 접근 방식의 관련성을 이해하는 데 도움이 되었다. 이러한 개입에 대한 이론의 기여는 사람 중심 접근법에 대한 개념과 이론적 근거에 대한 교훈적 소개에서부터 이론과 응용에 대한 정기적인 대화형 참여에 이르기까지 다양했다. 간단한 이론적 틀을 사용한 개입은 나머지 개입이 토론을 통해 또는 경험을 통해 이 이론을 실제에 적용하는 것을 지원하는 경우 관점에 대한 중요한 변화를 지원할 수 있다.
Interventions that applied person-centred theory to meaningful experiences helped learners understand the relevance of a person-centred approach to patient care. The contribution of theory to these interventions varied from didactic introductions on the concepts and rationale for a person-centred approach60, 71, 72, 74, 82, 94 to regular discursive and interactive engagement with theory and application.58, 65, 70, 77, 85, 89 Interventions with brief theoretical framing could support significant changes to perspective if the rest of the intervention supported the application of this theory to practice through discussion or through experience.60, 75, 82, 94
심장병동에서 우리는 그녀의 최근 가슴 통증, 새로운 경색 또는 심리적인 불평의 원인에 대해 논의했고 그녀가 혈관조영술을 다시 거부하자 다음 환자에게 달려갔다. 나중에 생각해보면, 그녀는 혈관조영술이나 개입을 원하지 않고 모든 심장 약물의 최대 용량을 복용하고 있기 때문에 그 병인은 관련이 없을 수 있다. 그녀의 집에 손님으로서, 저는 그녀의 옆에 서 있기보다는 옆에 앉습니다. 그리고 저는 서두르지 않을 수 밖에 없습니다. 나는 그녀가 사람이지 침대 번호가 아니라는 것을 깨달았다.
In the cardiology ward we debated about the cause of her latest complaint of chest pain, new infarct or psychological and then rush on to the next patient when she refused angiogram again. On hindsight, the aetiology may not be relevant as she does not want any angiogram or intervention and she is on maximum doses of every cardiac medication. As a guest in her home, I sit beside her rather than stand over her, and I am forced not to rush. I realise she is a person and not a bed number …84
3.3.2 메커니즘 2: [감정을 처리하고 가정을 비판적으로 성찰]할 수 있도록 지지
3.3.2 Mechanism 2: Support to process emotions and reflect critically on assumptions
학생들은 당뇨병의 병태생리학과 그 합병증에 대한 이해에도 불구하고, '그것이 일상적으로 어떻게 누군가에게 영향을 미치는지, 그리고 그들이 어떻게 그것을 그들의 모든 일상 활동에 맞추어야 하는지'에 대해 전혀 알지 못한다고 말했다.
학생들은 자신들의 토론으로 인해 '바닥에 깔렸다'고 스스로를 표현했다.
Students remarked that despite their understanding of the pathophysiology of diabetes and its complications, they ‘had no appreciation how it really impacts someone on a daily basis and how they really have to fit it into all their daily activities’. The students described themselves as ‘being floored’ by their discussion.65
사람 중심으로의 관점 변환에 대한 가장 명확한 질적 데이터에 대한 개입은 모두 학습자에게 학습에 대한 응답을 이해할 수 있는 기회를 제공했다. [피어와 퍼실리테이터의 관계적 연속성이 있는 소규모 그룹 환경]은 이 메커니즘을 촉발할 가능성이 가장 높은 [소속감과 신뢰의 확립]을 가능하게 했다. 학습자가 소그룹 학습을 정기적으로 제공받은 논문들을 넘어, 학습자가 자신의 감정을 표현하고 자신의 생각과 가정에 비판적으로 반영할 수 있도록 하는 '안전'과 '비판단' 설정의 중요성을 표현했다.
The interventions with the clearest qualitative data on perspective transformation towards person-centredness all offered opportunities for learners to make sense of their responses to their learning.49, 53, 58-60, 66, 67, 70, 72, 76, 78, 80, 82, 88-92, 95-98 Facilitated small group environments where there was relational continuity of peers and facilitator enabled the establishment of belonging and trust most likely to trigger this mechanism. Across papers where learners were offered regular small group learning, they expressed the importance of a ‘safe’ and ‘non-judgemental’ setting to enable them to express their feelings and reflect critically on their thoughts and assumptions.49, 53, 58, 70, 77, 80, 92, 96, 98
CIMOc 7: [경청과 공감]을 치료적 가치로 평가
CIMOc 7: Value listening and empathy as therapeutic
저는 환자들이 필요하다면 더 많은 시간을 함께 보낼 것입니다. 하지만 저는 어떤 면에서 그것이 저를 마르게 하는 것이라고 느꼈습니다. 저는 좌절감을 느낄 것입니다. 제가 무엇을 할 수 있을까요? … 하지만 [지금] 저는 그저 경청하고 그들과 함께 있는 것만으로도 괜찮다고 생각합니다. 그리고 저는 그것이 어떤 면에서 그들에게 더 도움이 된다고 생각합니다.
그리고 그것은 환자들을 위해 여러분이 할 수 있는 훌륭한 일입니다.
저는 단지 제 스스로 그것을 배울 필요가 있었다고 생각합니다.91
I will spend extra time with my patients if they need it, but I felt in some ways that it was kind of sucking me dry … I would feel frustrated, like what else can I do? … but [now] I feel OK just to listen and be present with them … and I think that in some ways that helps them more … and that is a wonderful thing that you can do for patients … I just needed to learn that myself, I guess.91
학생으로서 나의 안녕을 걱정하는 사람들이 있다는 점에서 그것은 나의 태도를 바꾸어 놓았다.
그리고 내가 받았기 때문에, 나도 돌려주고 싶다.
It has changed my attitude in the sense of knowing that there are people who care about my wellbeing as a student. And because I have received, I also want to give back.98
CIMOc 8: [건강을 전체론적인 것으로 이해]하고 [진료의 개인화]를 가치 있게 생각합니다.
CIMOc 8: Understand health as holistic and value personalisation of care
그녀가 소그룹에서 배운 당뇨병의 경험의 다양성에 영향을 받은 또 다른 학생은 '나는 같은 질병을 가진 사람들이 모두 정말 다르다는 것을 깨닫게 되었다'고 말했고,
다른 학생은 '그들을 알아가고 그들에게 무엇이 중요한지를 알아내는 것이 문제이다'라고 결론을 내렸다.
Another student, influenced by the diversity of the experiences with diabetes she had learned about in small group stated, ‘I came to the realization that people are all really different that have this same disease’, while another student concluded, ‘it's just kind of a matter of getting to know them and finding out what's important to them’.65
CIMOc 9: [자기 인식의 중요성] 이해
CIMOc 9: Understand the importance of self-awareness
매달, 직원들과 함께 일하는 교수진들과 어텐딩들은 그들의 경험에 대해 팀원들에게 보고하기 위해 만난다.
가장 놀랍고 일관된 관찰은 얼마나 자주 인턴들이 환자에 대해 알게 된 사실에 '놀랍다'고 보고하는가 하는 것이다.
이러한 보다 깊은 통찰력으로 인해 더 나은 환자 치료를 제공할 수 있는 기회가 반복적으로 생겨났습니다.
Each month, faculty and attendings working with the house staff meet to debrief the team about their experiences. The most striking and consistent observation is how often house staff report ‘being surprised’ by what they have learned about their patients. This deeper insight, in turn, has repeatedly led to opportunities to provide better patient care.85
소규모 그룹에 대한 일부 개입은 특히 마음챙김과 같은 [특정한 자기 인식 훈련 기술]을 포함했고, 이것들은 학습자들이 그들의 감정과 생각을 더 잘 인지하고 그것들을 다루기 위한 전략을 제공하는 데 도움을 주었다.
이 과정은 저에게 자기 인식에 관한 것이었습니다.
저는 신체적으로나 감정적으로 제게 무슨 일이 일어나고 있는지 더 잘 인식하는 법을 배웠습니다.
또한 삶의 스트레스를 다루기 위한 새로운 도구들을 배웠다.
This course has been about self-awareness for me. I have learned to better recognize what is going on for me physically and emotionally. I have also learned a new set of tools for dealing with the stresses in life.98
4 토론
4 DISCUSSION
4.1 조사결과 요약
4.1 Summary of findings
우리의 현실주의 검토는 사람 중심성 개발을 목표로 하는 계획된 의료 교육 프로그램이 어떻게, 왜, 그리고 어떤 상황에서 성공하는지 답하기 위해 시작되었다. 우리는 이 리뷰를 개별 학습자의 수준에서 위치시키고, 사람 중심성을 관점으로 개념화했으며, 생물의학적 관점으로 기울어진 학습자의 반응에 리뷰를 집중했다. 의료 교육은 의료 종사자들에게 사람 중심성을 개발하는 것이 어렵다는 것을 널리 관찰되어 왔다. 우리의 검토에 대한 설명은 이 문제에 대한 이해를 심화시키고 향후 실무에 대한 새로운 해결책을 제공한다. 우리의 [정제된 프로그램 이론]은 학습자가 사람 중심성을 향하도록 도울 수 있는 두 가지 주요 개입 전략을 발견했다.
- 의미 있는 경험에 적용되는 사람 중심 이론과
- 학습자가 기존의 의미 프레임워크에 도전하는 데 필요한 감정적 작업과 비판적 반성을 할 수 있도록 지원하는 소규모 그룹 환경
Our realist review set out to answer how, why and in what circumstances planned medical education programmes that aim to develop person-centredness are successful or not. We located this review at the level of individual learner, conceptualised person-centredness as a perspective and focused our review on the responses of learners who leaned towards a biomedical perspective. It has been widely observed that medical education has found it challenging to develop person-centredness in health care practitioners.4-10 The explanations in our review deepen our understanding of this problem and offer new solutions for future practice. Our refined programme theory found two main interventional strategies that can help learners towards person-centredness:
- person-centred theory applied to meaningful experiences and
- small group environments that support learners to do the emotional work and critical reflection needed to challenge existing meaning frameworks.
4.2 의미 있는 경험에 적용되는 사람 중심 이론
4.2 Person-centred theory applied to meaningful experiences
우리의 합성은 [적용된 사람 중심 이론]의 핵심적 역할, 즉 임상 실습에 대한 사람 중심 접근법에 대한 개념적이고 증거적인 근거를 발견했다. 사람 중심 이론의 역할은 교육 개입이 어떻게 실패했는지와 그들이 사람 중심성을 개발하는 데 어떻게 성공했는지에 대한 설명에서 강조되었다. 이전의 연구들은 [객관적인 사실]을 더 높게 평가하는 [의학교육의 지식 위계]가 학습자의 [사람 중심성 발달을 저해한다는 것]을 보여주었다. 학습자의 가치와 전문적인 역할 이해는 학습에 대한 참여를 가이드하는 것으로 나타났으며, [생물의학 중심적 관점]을 강하게 가지고 있을수록 사람 중심 학습에 대한 참여도가 떨어지는 것과 관련이 있다. 또한 사람 중심의 기술 훈련이 태도의 변화 없이 특정 행동을 사용하는 임상의의 증가로 이어질 수 있다는 것이 관찰되었다. 우리의 연구 결과는 [사람 중심 이론의 학습이 부족함]으로 인해 [어떻게 지식 및 역할에 대한 기존 관점과 불일치가 발생하는지]를 설명함으로써, 이러한 연구에서 학습을 확장한다. 우리의 발견은 학습자들이 기존 지식의 토대 위에서 어떻게 새로운 지식을 구성하는지 설명하는 [구성주의 학습 이론]과 일치한다.
Our synthesis found a key role for applied person-centred theory: the conceptual and evidential rationale for a person-centred approach to clinical practice. The role of person-centred theory was highlighted in explanations for both how educational interventions failed and how they succeeded in developing person-centredness. Previous studies have shown that a knowledge hierarchy in medical education, where objective facts are more highly valued, undermines the development of person-centredness in learners.100, 101 Learners' values and professional role understanding has been shown to guide their engagement with learning, with more biomedical perspectives associated with poorer engagement with person-centred learning.102, 103 It has also been observed that person-centred skills training can lead to an increase in clinicians using certain behaviours without a change in their attitudes.47, 104 Our findings extend the learning from these studies by explaining how a lack of person-centred theory in learning creates dissonance with existing perspectives on knowledge and role which either results in learners minimising the importance of such learning or incorporating learning into existing meaning perspectives. Our findings are in line with constructivist learning theories, which explain how learners construct new knowledge on the foundations of existing knowledge.105
우리의 결과는 또한 사람 중심 이론이 [전문직업적 행위에 대한 이해]와 어떻게 관련이 있는지를 보여준다. 이전의 연구들은 의대생들과 의사들이 고통을 피하기 위한 전략으로 [감정적 분리]를 사용하는 것을 묘사했다. 우리의 결과는 [사람 중심 이론의 적용을 제공하지 않는 개입]은 [역할에 대한 생물의학적 이해(질병 관리)와 전문성(감정적 분리)의 불일치]로 이어질 수 있고, 그 결과로 [학습자가 명확한 생물의학적 역할을 인식하지 못하는 상황을 회피하게 된다]는 것을 보여주었다. 우리의 연구 결과는 또한 사람중심 이론의 적용이 어떻게 학습자가 생물의학 전문지식이 제한된 상황에서 환자를 지원하는 역할을 수용하는 데 도움이 될 수 있는지 설명하며, 이는 학습자가 전문적인 역할에 대한 확장된 이해를 개발하는 데 도움이 된다.
Our results also show how person-centred theory is relevant to an understanding of professional conduct. Previous studies have described medical students and doctors using emotional detachment as a strategy to avoid distress.106, 107 Our results showed that interventions that do not offer applied person-centred theory may lead to dissonance with a biomedical understanding of role (disease management) and professionalism (emotional detachment) and thus to an avoidance of situations where learners do not perceive a clear biomedical role. Our findings also explain how applied person-centred theory can help learners embrace their role in supporting patients in situations where their biomedical expertise is of limited use, by helping them develop an expanded understanding of professional role.
캐나다의 16개 의과대학 커리큘럼에 대한 최근 연구는 [학습자들이 사람 중심의 개념에 대한 교육을 받고 있는지에 대해 의문]을 제기했다. 의학 교육에서 [명확한 사람 중심 이론의 부족]은 [왜 학생과 의사 모두가 사람 중심성에 대해 피상적이고 불명확한 이해를 가지고 있는지]를 보여주는 연구들을 설명하는데 도움이 될 수 있다. 학습자는 사람 중심의 실천을 [학문적 및 정책 논문에 설명된 패러다임적 실천의 변화]와 대조적으로, '암묵적'이고 '(말하지 않아도) 당연한' 것으로 간주할 수 있다. [사람 중심성에 대한 피상적인 이해]는 [스스로는 사람 중심이라는 임상의의 믿음]과 [(실제로는 그렇지 않은) 임상적 행위] 사이에서 관찰되는 차이를 설명할 수 있다.
A recent study of 16 medical schools curricula in Canada questioned if learners are receiving teaching on person-centred concepts.108 A lack of explicit person-centred theory in medical education may help to explain why studies have shown that both students and doctors hold superficial and unclear understandings of person-centredness.109, 110 Learners may regard person-centred practice as ‘implicit’ and ‘obvious’109 in contrast to a paradigmatic shift in practice described in academic and policy papers.15-17, 20, 27, 111, 112 Superficial understandings of person-centredness may explain the gap observed between clinicians' belief that they are person-centred and their clinical practice.110
또한 학습자의 사람 중심성을 측정하기 위해 검증된 척도를 사용하는 연구는 '공유sharing'에 비해 '돌봄caring'에서 더 높은 점수를 일관되게 보여준다.
- '돌봄caring'은 자신의 역할을 여전히 '도와주는' 것으로 보는 생물의학적 관점에 더 쉽게 통합될 수 있는 반면,
- '공유sharing'는 환자와의 편의적이고 협력적인 접근방식을 필요로 하는 '함께 일하는'로 관점을 전환이다.
사람 중심의 실천 이론에 대한 명확한 개념적 틀과 증거적 근거가 없으면 학습자는 사람 중심의 전문 실천에 전념하기 어려울 수 있다.
Furthermore, studies that use validated scales to attempt to measure learners' person-centredness consistently show higher scores in ‘caring’ compared to the ‘sharing’.4, 24
- It may be that ‘caring’ is more easily integrated into a biomedical perspective where one still sees one's role as ‘doing for’,
- whereas ‘sharing’ involves a shift in perspective to ‘working with’ which requires a facilitative, partnership approach with patients.113, 114
Without an explicit conceptual framework and evidential rationale for the theory of person-centred practice,21 it may hard for learners to commit to person-centred professional practice.
우리의 결과는 [사람 중심 이론이 의미 있는 경험에 적용]될 때, 이것은 사람 중심 이론이 임상 실습에 대한 관련성에 대한 이해를 촉발시켰다는 것을 보여주었다. 의미 있는 경험에는 다음이 포함된다.
- 실제 환자 이야기를 접하는 것,
- 일정 시간에 걸쳐 환자를 사람으로 알아가는 기회,
- 환자 치료에 있어 적극적인 사람 중심 역할을 할 수 있는 기회
Our results showed that when person-centred theory was applied to meaningful experiences, this triggered an understanding of the relevance of person-centredness to clinical practice. Meaningful experiences included
- engaging with real patient stories,
- opportunities to get to know patients as people over time, as well as
- opportunities to take an active person-centred role in their care.
우리의 연구 결과는 환자의 [질병 궤적에 전체에 대한 접근]이 환자 중심성에 대한 학습에 중요한 맥락이라는 것을 보여준 최근의 현실주의 검토와 일치한다. 우리의 연구 결과는 또한 [환자-교육자]의 증가와, [환자를 돌볼 수 있는 적극적인 기회]를 요구하는 문헌을 지지한다. 우리의 결과는 이러한 임상 배치가 의미 있는 경험을 위한 자원으로 어떻게 작용할 수 있는지를 강조함으로써 사람 중심성을 강화하기 위해 입증된 교육 접근법인 LIC에 대한 문헌에 대한 이해를 넓히는 데 도움이 된다.
Our findings fit with a recent realist review that showed that access to patients' whole illness trajectories was an important context for learning about patient-centredness.101 Our findings also support literature that calls for an increase in patient-educators115 and active opportunities to care for patients.116 Our results help to extend an understanding of the literature on LICs, an educational approach that has been demonstrated to enhance person-centredness,11, 12 by highlighting how these clinical placements may act as a resource for meaningful experiences.
4.3 센스 메이킹 지원
4.3 Support for sense making
학습자가 [자신의 감정을 처리]하고, [(부조화를 포함한) 학습에 대한 반응을 비판적으로 성찰할 수 있는 기회]를 통해 [새로운 의미 프레임워크와 자아 인식을 개발]할 수 있었다. 도비는 학습자들이 [자기 인식과 자기 지식]이 [사람 중심의 실천에 중요하다는 사실]을 놓칠 수 있다고 주장해왔다. 그녀는 자기인식을 기르는 데 필요한 정서적 업무와 비판적 성찰을 지원하는 교육이 의료교육 커리큘럼 개혁의 토대가 될 것을 요구해왔다. 보다 최근에, 사람 중심의 관행을 강화하기 위해 의료 교육에 대화형 학습을 통합하는 것이 제안되었다. 대화형 학습은 교사와 학습자가 비위계적 환경에서 만나 환자 경험을 반영할 수 있는 정기적인 기회를 포함한다. 광범위한 건강 관리 맥락에서, 다학제 팀에게 임상 실습에 대한 감정 및 인지 반응을 처리할 수 있는 기회를 제공하는 [슈워츠 라운드]는 사람 중심의 태도를 지지하는 것으로 나타났다.
The opportunity for learners to process their emotions and critically reflect on their responses to learning, including dissonance, allowed them to develop new meaning frameworks and self-awareness. Dobie has argued that learners can miss the fact that self-awareness and self-knowledge are crucial to person-centred practice.117 She has called for education that supports the emotional work and critical reflection needed to develop self-awareness to be the foundation for medical educational curricular reform. More recently, incorporation of dialogic learning into medical education has been proposed to enhance person-centred practice.118 Dialogic learning involves regular opportunities for teachers and learners to meet in non-hierarchical settings to reflect on patient experiences. In the wider health care context, Schwartz rounds, which provide multidisciplinary teams the opportunity to process their emotional and cognitive responses to clinical practice, have been shown to support person-centred attitudes.119
[센스 메이킹]을 가장 지원할 가능성이 높은 개입의 특징은, [학습자와 그룹 퍼실리테이터의 관계적 연속성을 가진 정기적인 소규모 그룹]이었다. 이러한 연속성은 참가자들이 자신의 감정을 표현하고, 정직한 평가에 참여하고, 가정에 도전할 수 있을 만큼 충분히 안전하다고 느낄 수 있도록 하는 [신뢰 관계를 발전]시킬 수 있게 했다. 이러한 조건은 우리의 발견에 설명력을 추가하는 [변혁적 학습]을 촉진하는 것으로 알려진 조건을 반영한다. [변혁적 학습 이론]은 성인 학습자가 기존의 의미 체계를 바꾸려면, [자신의 가치, 의미, 목적을 비판적으로 성찰할 수 있는 지원]이 필요하다고 말한다. 우리의 리뷰에서, 우리는 비판적 성찰과 감정 처리가 함께 이루어졌다는 것을 발견했고, 이것은 비판적 성찰의 능력이 감정을 처리하는 능력에 따라 달라질 수 있다는 것을 보여주는 변혁적 학습 육성에 대한 최근의 연구에서 뒷받침된다.
The characteristics of interventions most likely to support sense making were regular small groups with relational continuity of learners and group facilitator. This continuity allowed relationships of trust to develop which enabled participants to feel safe enough to express their emotions, engage in honest appraisal and challenge their assumptions. These conditions mirror those known to foster transformative learning, which adds explanatory power to our findings.120 Transformative learning theory states that for adult learners to change their existing meaning framework, they need support to critically reflect on their values, meanings and purposes.121 In our review, we found that critical reflection and emotional processing took place together and this is supported by more recent work on fostering transformative learning which shows that the capacity for critical reflection may depend on the ability to process emotions.122
4.4 전체 커리큘럼에 대한 교육 개입의 관계
4.4 Relationship of educational interventions to whole curriculum
우리의 검토는 [커리큘럼의 더 넓은 초점과 일치]한다고 여겨질 수 있는 [사람 중심의 개입]을 발견하지 못했다. 의미 있는 경험에 이론을 적용하고 센스 메이킹을 지원하는 것을 포함하여, [모든 개입은 커리큘럼의 생의학적 초점과 상충되는 것]이었고, 일부 학습자들이 [향후 임상 실습에 대한 학습의 중요성을 최소화]하도록 이끌었다. [인식론적 부조화]의 중요성을 인식하였기에, 우리는 [사람 중심의 실천]을 지원하기 위한 [전체 커리큘럼 접근방식]의 강화를 요구한다.
Our review did not find any person-centred interventions that were perceived to be in line with the wider focus of the curriculum. All interventions, including those that applied theory to meaningful experiences and support for sense making, were perceived to be at odds with the biomedical focus of the curriculum and led some learners to minimise the importance of the learning for their future clinical practice. Our recognition of the importance of epistemological dissonance reinforces calls for a whole curriculum approach to support person-centred practice.123
4.5 장점과 한계
4.5 Strengths and limitations
가치관, 태도 및 신념에 의해 정보에 입각한 참여자 관점의 수준에 위치한 사람 중심성에 우리의 리뷰를 집중함으로써, 우리는 의료 교육이 왜 사람 중심주의의 증가로 이어지지 않았는지, 그리고 이것에 대해 결정적으로 무엇을 할 수 있는지에 대한 이해의 차이를 해결하는 데 도움을 줄 수 있었다. 현실주의 접근 방식을 사용하여, 우리는 학습자의 관점과 중재적 구성 요소의 상호 작용으로 촉발되는 메커니즘을 추론할 수 있었다. 우리의 검토는 계획된 커리큘럼에 초점을 맞추기로 결정함으로써 정책 입안자들에게 사람 중심의 의사 개발을 지원하기 위한 개입을 개발하고 테스트하는 데 사용할 수 있는 실용적인 발견을 제공한다.
By focusing our review on person-centredness, which sits at the level of participant perspective, informed by values, attitudes and beliefs, we have been able to help address the gap in understanding around why medical education has not led to an increase in person-centeredness and crucially what can be done about this. By using a realist approach, we have been able to infer the mechanisms that are triggered by the interaction of interventional components with learner perspectives. By choosing to focus our review on the planned curriculum, our review offers policymakers pragmatic findings that can be used to develop and test interventions to support the development of person-centred doctors.
우리의 연구 결과에는 몇 가지 한계가 있다. 몇 가지 개입을 제외하고, 대부분의 논문은 참가자의 관점의 단기 변화에 대한 데이터를 제공했다. 이 검토는 사람 중심의 관점으로의 장기적 전환과 이를 지원하는 방법에 대한 증거를 뒷받침하는 문헌의 차이를 식별한다. 우리의 연구는 인간 중심성 개발을 목표로 하는 계획된 개입에 초점을 맞추었고, 인간 중심성 개발에 영향을 미칠 수 있는 평가와 같은 광범위한 교육 관행을 포함하지 않았다. 또한, 우리의 연구는 학습자의 관점이 어떻게 형성되었는지에 대해 의문을 제기했고, 사람 중심 접근법의 정규화와 실행에 대한 의료 제공의 영향을 검토하기 위해 향후 작업이 필요하다. 마지막으로, 의료 교육의 상당한 비율은 의료의 더 넓은 맥락에서 발생하며, 계획된 의료 교육은 이러한 상황을 형성하는 데 제한적인 영향을 미친다. 따라서, 우리의 연구 결과는 사람 중심의 의사의 발전을 어떻게 지원할 것인가라는 더 큰 질문에 대한 부분적인 대답일 뿐이다.
There are several limitations to our research findings. Apart from a few interventions,40, 53, 58, 91 most papers offered data on short-term changes in participant perspectives. This review identifies a gap in the literature supporting evidence about longer term transformation towards a person-centred perspective and how to support this. Our research focused on planned interventions that aimed to develop person-centredness and did not include wider educational practices, such as assessment, which may impact the development of person-centredness. Also, our research did interrogate how learner perspectives were formed, and future work is needed to examine the influence of health care delivery on the normalisation and practice of a person-centred approach. Finally, a significant proportion of medical education takes place in the wider context of health care, and planned medical education has a limited influence in shaping this context. Therefore, our findings are only a partial answer to the larger question of how to support the development of person-centred doctors.
4.6 교육실무에 대한 시사점
4.6 Implications for educational practice
우리의 연구 결과는 [왜 기술 기반 접근법이 의사들의 인간 중심성 개발을 지원하기에 충분하지 않을 수 있는지]를 설명한다. 구성주의 학습 이론에 따라, 우리의 리뷰는 [교육 개입이 학습자의 기존 의미 관점과 상호 작용한다는 것]을 발견했다. 따라서, 생물의학에서 임상 실습으로 더 사람 중심의 접근으로 전환하기 위해, 의대생과 의사들은 [사람 중심의 실천이 왜 건강에 중요한지]를 이해할 필요가 있다. 이것은 [사람 중심 이론에 대한 명시적 학습]과 [의미 있는 경험을 통해 임상 실습에서 그것의 관련성을 경험할 기회]를 통합함으로써 달성될 수 있다.
Our findings explain why a skills-based approach may be insufficient to support the development of person-centredness in doctors. In line with constructivist learning theory, our review finds that educational interventions interact with learners' existing meaning perspectives. Therefore, in order shift from a biomedical to a more person-centred approach to clinical practice, medical students and doctors need to understand why person-centred practice matters to health. This may be achieved by integrating explicit learning on the theory of person-centeredness with opportunities to experience its relevance in clinical practice through meaningful experiences.
교육적 접근법은 또한 [관점 변환에 필요한 감정적 작업을 인식하고 다룰 필요]가 있다. [감정을 처리하고, 반응에 대해 비판적으로 성찰할 수 있는 정기적인 기회]는 사람 중심으로의 관점을 바꿀 수 있는 새로운 의미 프레임워크의 생성을 지원한다. 동료와 촉진자의 연속성과 함께 정기적인 소규모 그룹 학습이 커리큘럼 전체에 통합될 필요가 있다. 마지막으로, 사람 중심성 개발을 최적화하기 위해 이러한 구성 요소는 교육학 및 전체 커리큘럼 수준에서 통합되어야 한다.
Educational approaches also need to recognise and address the emotional work needed for perspective transformation. Regular opportunities to process emotions and critically reflect on responses support the creation of new meaning frameworks that enable a shift in perspective towards person-centredness. Regular, supportive small group learning, with continuity of peers and facilitators, needs to be integrated throughout the curriculum. Finally, to optimise the development of person-centredness, these components need to be integrated at both pedagogical and whole curricular level.
4.7 연구에 대한 시사점
4.7 Implications for research
우리의 현실주의 검토는 의료 교육 환경에서 효과적일 수 있는 증거 기반 전략에 대한 통찰력을 제공하며, 우리의 정제된 프로그램 이론은 의료 교육자와 정책 입안자들이 실제로 구현할 수 있는 검증 가능한 이론을 제공한다. 추가 연구는 실제로 교육 모델을 개발하고 평가하기 위해 경험적인 작업을 통해 우리의 이론을 테스트하고 다듬어야 한다. 특히, 우리는 프로그램 이론의 구현이 [실천에서 지속적인 사람 중심성으로 이어질 수 있는지에 대한 평가]를 요구한다.
Our realist review provides insights into evidence-based strategies that may be effective in medical education settings, and our refined programme theory offers a testable theory for medical educators and policymakers to implement in practice. Further research should test and refine our theory through empirical work to develop and evaluate educational models in practice. In particular, we call for evaluation of whether implementation of our programme theory can lead to persistent person-centredness in practice.
실천에 대한 사람 중심성의 관련성을 이해하는 것은 [자기 결정 이론의 자율적 동기의 개념]과 밀접하게 일치한다. 자율적 동기 부여는 학습자가 활동의 가치를 이해하고 그것이 자신의 감각과 일치할 때 발전하며, 몇 가지 경험적 연구는 [자율적 동기 부여]가 [활동의 지속성]과 매우 관련이 있다는 것을 보여주었다. 적용된 사람 중심 이론이 사람 중심 접근법에 대한 지속적인 변화를 지원할 수 있는지 여부를 테스트하기 위한 종단적 연구는 향후 연구에 귀중한 영역이 될 것이다. 게다가, 비록 우리의 검토의 초점이 의대생과 의사들에 집중되었지만, 우리의 연구 결과는 다른 건강 직업들과 관련이 있을 수 있다.
Understanding the relevance of person-centredness to practice is closely aligned with the concept of autonomous motivation in self-determination theory.124 Autonomous motivation develops when learners understand the value of an activity and it aligns with their sense of self, and several empirical studies have shown that autonomous motivation is highly related to persistence of an activity.125, 126 Longitudinal studies to test if applied person-centred theory can support a sustained change towards person-centred approaches would be a valuable area for future research. Furthermore, although the focus of our review was on medical students and doctors, our findings may be relevant to other health professions.
5 결론
5 CONCLUSION
우리의 연구 결과는 [커뮤니케이션 기술 기반 교육 전략이 사람 중심성을 개발하기에 충분하지 않을 수 있는 이유]에 대한 설명을 제공한다. 사람 중심의 경험을 [사람 중심의 경험이 왜 중요한지에 대한 이론]과 통합하고, [센스 메이킹을 지원할 수 있게 하는 것]은 [사람 중심의 경험을 위한 관점적 전환]을 지원할 수 있다. 우리의 연구 결과는 사람 중심성을 지원하는 것을 목표로 하는 의료 교육 전략의 개발에 inform하기 위한 프로그램 및 정책 입안자에게 테스트 가능한 이론을 제공한다.
Our findings offer explanations as to why communication skills-based educational strategies may be insufficient to develop person-centredness. Integrating person-centred experiences with theory on why person-centredness matters, and enabling support for sense making, may support perspective transformation towards person-centredness. Our findings offer programme and policymakers testable theory to inform the development of medical education strategies that aim to support person-centredness.
Med Educ. 2022 May;56(5):489-503. doi: 10.1111/medu.14707. Epub 2021 Dec 22.
Optimising planned medical education strategies to develop learners' person-centredness: A realist review
PMID: 34842290
DOI: 10.1111/medu.14707
Free article
Abstract
Context: Person-centeredness is a stated aim for medical education; however, studies suggest this is not being achieved. There is a gap in our understanding of how, why and in what circumstances medical education interventions that aim to develop person-centredness are successful.
Methods: A realist review was conducted with a search of Medline, Embase, HMIC and ERIC databases and the grey literature using the terms 'medical education' and 'person-centred' and related synonyms. Studies that involved a planned educational intervention in medical education with data on outcomes related to person-centredness were included. The analysis focused on how and why different educational strategies interact with biomedical learner perspectives to trigger mechanisms that may or may not lead to a change in perspective towards person-centredness.
Results: Sixty-one papers representing fifty-three interventions were included in the final synthesis. Nine context-intervention-mechanism-outcome configuration (CIMOc) statements generated from the data synthesis make up our refined programme theory. Where educational interventions focused on communication skills learning or experiences without person-centred theory, learners experienced dissonance with their biomedical perspective which they resolved by minimising the importance of the learning, resulting in perspective endurance. Where educational interventions applied person-centred theory to meaningful experiences and included support for sense making, learners understood the relevance of person-centeredness and felt able to process their responses to learning, resulting in perspective transformation towards person-centredness.
Conclusion: Our findings offer explanations as to why communication skills-based interventions may be insufficient to develop learners' person-centredness. Integrating experiential person-centred learning with theory on why person-centredness matters to clinical practice and enabling learners to make sense of their responses to learning, may support perspective transformation towards person-centredness. Our findings offer programme and policymakers testable theory to inform the development of medical education strategies that aim to support person-centredness.
© 2021 The Authors. Medical Education published by Association for the Study of Medical Education and John Wiley & Sons Ltd.
'Articles (Medical Education) > 임상교육(Clerkship & Residency)' 카테고리의 다른 글
| 집단적 역량: 개인적 전문성에서 협력적 전문성으로 (Perspect Med Educ, 2020) (0) | 2022.06.22 |
|---|---|
| 안쓰러운 늘어진 여성: 의과대학생을 위한 골반진찰 학습자료의 상황분석(Med Educ, 2022) (0) | 2022.04.20 |
| 무대에서 연기하기: 직접관찰에 관한 전공의의 인식(Med Educ, 2017) (0) | 2022.02.27 |
| 전문직 정체형 형성을 촉진하기: 코칭 대 역량(Acad Med, 2020) (0) | 2022.02.24 |
| 피드백과 코칭(Eur J Pediatr, 2022) (0) | 2022.02.24 |