인식론, 문화, 정의, 권력: 의학 훈련을 위한 비-생물과학적 지식(Med Educ, 2017)
Epistemology, culture, justice and power: non-bioscientific knowledge for medical training
Ayelet Kuper,1,2,3 Paula Veinot,3 Jennifer Leavitt,4 Sarah Levitt,5 Amanda Li,3 Jeannette Goguen,3,6 Martin
Schreiber,3,6 Lisa Richardson1,3,7 & Cynthia R. Whitehead1,8,9
소개
Introduction
역량 프레임워크는 미래 및 현재 의사의 훈련과 평가를 안내하는 이상적인 방법으로 널리 받아들여지고 있다. 이러한 프레임워크는 국제적으로 개발, 적응 및 규제 권한이 주어졌다.1-8 의사 역량에 대한 가장 초기적이고 가장 영향력 있는 포괄적 정의 중 하나는 의사가 실천하기 위해 유능해야 하는 7가지 역할을 요약한 캐나다 CanMEDS 프레임워크이다. 이 프레임워크는 캐나다에서 상당한 규제 권한을 얻었으며 캐나다 왕립의과대학(RCPSC)에 의해 성문화되었으며, 캐나다 가정의과대학(CCFP)의 승인을 받았으며, 학부(의과대학) 및 대학원(거류지) 의료 교육의 인증 표준에 채택되었다. CanMEDS 의 역할은 전 세계적으로 채택되고 채택되어 현재 '세계에서 가장 널리 사용되는 역량 프레임워크 중 하나'를 나타내고 있다. 이들은 상당한 공개적, 전문적인 상담을 통해 개발되었으며, 따라서 현재 유능한 의사들의 사회적 기대를 대변하는 것으로 간주되고 있다. 따라서 의료 훈련에서 사회적 책임에 대한 현재 강조는 모든 7개의 캔메드 역할의 효과적인 교육을 지원하기 위해 적절한 내용을 의료 커리큘럼에 포함하는 것의 중요성을 더욱 강조한다.
Competency frameworks have become widely accepted as representing an ideal way to guide the training and assessment of future and current physicians. These frameworks have been developed, adapted and given regulatory power internationally.1-8 One of the earliest and most influential comprehensive definitions of physician competence is the Canadian CanMEDS framework, which outlines seven roles in which physicians must be competent in order to practise.1, 2 This framework has gained significant regulatory authority in Canada and has been codified by the Royal College of Physicians and Surgeons of Canada (RCPSC),1, 2, 9 endorsed by the Canadian College of Family Physicians (CCFP),10 and adopted in accreditation standards for both undergraduate (medical school) and postgraduate (residency) medical education. The CanMEDS roles have also been adopted and adapted worldwide, such that they now represent ‘one of the world's most widely used competency frameworks’.11 They were developed with significant public and professional consultation and are therefore currently seen as representing societal expectations of competent physicians.12-15 The current emphasis on social responsibility16, 17 in medical training thus further underscores the importance of including in medical curricula appropriate content to support the effective teaching of all seven CanMEDS roles.
CanMEDS 는 필요하긴 하지만 의사가 의료 전문가 역할에 포함되는 생물의학 지식과 기술력만을 보유하도록 훈련하는 것으로는 충분하지 않다는 것을 분명히 한다. 오히려 교육생들이 잘 협력하고 효과적으로 소통하며 개별 환자와 시스템 변화를 옹호하는 학문적이고 인정 많은 전문가가 되도록 해야 한다. 정의에 따르면, 그러한 역량은 단순히 타고난 개인적 자질이나 태도일 뿐만 아니라, 가르치고 그들의 습득을 평가할 수 있어야 한다. 그러나 한 세기 이상 동안 의학 교육은 의학을 생물의학과 동일시했고, 환자 치료를 위한 생명과학의 객관적인 사용으로서 그 실천을 구축했다. 의과대학과 레지던트 커리큘럼이 주로 생물과학 지식으로 구성되는 것과 같이 역사적으로 제한적으로 수용 가능한 커리큘럼 콘텐츠를 생각하고 아는 특권적인 방법들이다. 물론 의학계의 생체과학 지식 증가로 임상관리가 크게 개선됐지만, 많은 의학 교육자들은 현대 의학 교육과정이 생명과학만으로는 충분하지 못함을 강조해 왔다. 특히, 6개의 비의료 전문가(때로는 '내과적'11이라고도 함) CanMEDS 역할의 대다수는 생명과학이 아닌 사회과학 및 인문(SSH)에 기반을 두고 있기 때문에, 우리는 CanMEDS 가 주로 생체과학 지식으로 구성된 커리큘럼에서 적절하게 가르치고 평가되기를 기대할 수 없다.
CanMEDS makes clear that, although necessary, it is not sufficient to train physicians to possess only the biomedical knowledge and technical skills encompassed in the Medical Expert role. Rather, we must also ensure that trainees become scholarly, compassionate professionals who collaborate well, communicate effectively, and advocate for individual patients and systems change.1, 2 By definition, such competencies cannot merely be innate personal qualities or attitudes, but must be able to be taught and their acquisition assessed.18-20 Yet for over a century medical education equated medicine with biomedical science and constructed its practice as the objective use of bioscience for patient care.21-28 These particular privileged ways of thinking and knowing22-24, 28-31 historically limited acceptable curricular content28, 32-34 such that medical school and residency curricula continue to be comprised primarily of bioscientific knowledge. Although clinical care has, of course, greatly improved as a result of the medical community's ever-increasing bioscientific knowledge, many medical educators have highlighted the insufficiency of bioscience as the sole basis for contemporary medical curricula.21, 26, 35-40 In particular, as the majority of the six non-Medical Expert (sometimes called ‘Intrinsic’11) CanMEDS roles are based in the social sciences and humanities (SSH) rather than in bioscience,21 we cannot expect them to be taught and assessed adequately in a curriculum comprised primarily of bioscientific knowledge.
최근 출판물 및 보고서는 비의료 전문가 역할의 현재 교수 및 평가의 부적절성에 대한 의사의 인식을 강조하고 있다. 레지던트들과 그들의 프로그램 책임자들은 비의료 전문가 역할을 가르치기 위해 종종 사용되는 지나치게 단순화된 접근법에 대한 우려를 특히 확인했으며, 많은 임상의 교육자들은 이러한 역할을 지원하기 위해 무엇을 가르쳐야 하는지 모른다는 주장을 하고 있다. 이러한 격차를 해소하기 위해, 그리고 현재 역량 프레임워크의 내용 중 많은 부분에 대한 비생물학적 기반을 인식하여, 최근 의료 커리큘럼에 필요한 비생물학적 지식의 측면을 문서화하려는 여러 시도가 있었다. 이러한 노력은 필요한 지식 자체를 탐구하기 보다는 비생물학적 지식을 잘 이해해야 할 수 있는 교육 주제(예: 담배 사용, 가정 폭력, 생명 윤리)의 목록으로 이어졌다. CanMEDS 의 역할을 뒷받침하는 데 필요한 지식에 대한 철저한 이해는 아직 개발되지 않았다. 현재까지 CanMEDS 역량 프레임워크의 기초가 되는 비생물학적 지식에 대한 설명은 본 논문의 주요 저자가 2011년에 발표한 '사고 실험'으로서 문헌에 존재했다.
Recent publications and reports have highlighted physician perceptions of the inadequacy of current teaching and assessment of all six non-Medical Expert roles.14, 41-45 Residents and their programme directors have especially identified concerns about overly simplistic approaches that are often employed to teach the non-Medical Expert roles,44, 46-50 and many clinician-educators claim simply not to know what to teach to support these roles. To address this gap, and in recognition of the non-bioscientific bases of much of the content of current competency frameworks, there have been several attempts recently to document aspects of necessary non-bioscientific knowledge for medical curricula. These efforts have led to the listing of curricular topics (e.g. tobacco use, domestic violence, bioethics) that might require non-bioscientific knowledge to be well understood,51-55 rather than exploring the necessary knowledge itself. A thorough understanding of the knowledge required to underpin the CanMEDS roles has not yet been developed; to date, the delineation of the non-bioscientific knowledge underlying the CanMEDS competency framework has existed in the literature only as a ‘thought experiment’ published in 2011 by the principal author of this paper.21
따라서 이 연구의 전반적인 프로그램의 목표는 CanMEDS 프레임워크로 대표되는 의사 역량에 대한 캐나다 사회적 기대를 충족시키는 의사를 훈련시키고 이러한 발견의 이행을 보급, 합법적, 번역, 구현 및 평가하기 위해 의료 커리큘럼에 필요한 지식을 식별하는 것이다. 본 논문에서, 우리는 다음의 연구 질문에 답하는 이 연구 프로그램의 1단계 결과를 제시한다. 여섯 가지 non-Medical Expert CanMEDS 역할에 완전히 역량을 갖춘 의사의 개발을 가장 잘 지원하기 위해 어떤 형태의 지식이 의료 커리큘럼에 포함되어야 하는가?
The goal of this overall programme of research is therefore to identify the knowledge needed in medical curricula to train physicians who meet Canadian societal expectations of physician competency, as represented by the CanMEDS framework, and to disseminate, legitimate, translate, implement and evaluate the implementation of those findings. In this paper, we present the results of Phase 1 of this research programme, in which we answer the following research question: What forms of knowledge beyond bioscience should be included in medical curricula to best support the development of physicians who are fully competent in the six non-Medical Expert CanMEDS roles?
방법들
Methods
CanMEDS 를 의료 역량 모델로 사용하여 SSH 내에서 생체 과학 외부의 광범위한 학문 분야의 전문가를 식별하여 각 비의료 전문가 CanMEDS 역할을 지원하기 위해 각 분야의 전문 지식을 구체적으로 식별하기 위해 의료 전문가를 제외한 모든 의사 역량 영역에서 작업했다. 우리는 CanMEDs 2005에서 설명한 역할을 사용했지만, 2015년에 있을 몇 가지 변화에 대해 점점 더 잘 알고 있었습니다(J R Frank, [전화로], 2011). 우리의 의도는 의료 커리큘럼에 추가하기 위해 전체 학문 SSH 과정을 만들지 않는 것이었다. 의학 교육자들이 역사적으로 의학 전문가 역할을 지원하기 위해 의료 커리큘럼에 통합된 물리 또는 화학의 측면을 식별한 것처럼, 우리는 SSH에서 의료 커리큘럼에 유사하게 통합될 경우 현재 정의된 역량있는 의사의 개발을 지원할 수 있는 요소를 식별하려고 했다. 참가자들에게 요약된 바와 같이, 이러한 요소에는 다음이 포함됩니다.
- 지식의 형태: 인식론적 토대57 및 권위에 대한 철학적 주장
- 이론:
- 광범위한 사회적 힘에 대해 말하는, 보편적인 적용 가능성을 주장하는 거시적 수준의 이론들63;
- 특정 분야 또는 분야에서 사용되는 중범위 및 미시적 수준의 이론들,
- 그리고 객관적 패러다임과 관련된 실증주의,
- 사실: 절대 진리의 객관적 개념 안에서 개념화된 사실들뿐만 아니라 특정 맥락 내에서 합의될 수 있는 사회적으로 구성된 사실들.68
Using CanMEDS as our model of medical competency, we identified experts in a wide range of academic disciplines outside bioscience – within the SSH – to work through all domains of physician competency except that of Medical Expert in order to concretely identify the knowledge from each of their area(s) of expertise to support each non-Medical Expert CanMEDS role. We used the roles as delineated in CanMEDS 2005,2 but we were also increasingly aware (J R Frank, personal communication [by telephone], 2011) of some of the changes that were to come in 2015.56 Our intention was not to create full disciplinary SSH courses to add to medical curricula. Much as medical educators have historically identified aspects of physics or chemistry that are integrated into medical curricula to support the Medical Expert role, we sought to identify those elements from the SSH that, if similarly integrated into medical curricula, would support the development of competent physicians as currently defined. As outlined to our participants, these elements included:
- forms of knowledge: epistemological underpinnings57 and philosophical claims to authority;58, 59
- theories: macro-level theories60-62 that speak to broad social forces63 and make claims to universal applicability;64 mid-range and micro-level theories that are used in specific disciplines or fields,65, 66 and the positivism associated with the objectivist paradigm,67 and
- facts: facts conceptualised within an objectivist notion of absolute truth, as well as socially constructed facts that can be agreed on within a particular context.68
연구팀
Research team
우리 연구팀은 우리의 연구 질문과 관련된 몇 가지 관점을 대표합니다. SSH 분야의 석박사 학위를 가진 개업 의사가 주도하고 있으며, 대규모 의학부 내에서 임상 실습과 연구가 이루어진다. 연구팀의 다른 세 명의 구성원은 SSH 석사 학위를 가진 의사 교수진(보건 직업 교육 2명, 페미니스트 과학 연구 1명)이며, SSH 박사 학위를 가진 네 번째 의사 교수진은 상급 교육 및 리더십에서 근무했다. 교수진과 대학에서의 역할. 우리 팀원 중 3명이 의대생으로 더 참여하게 되었다. (한 명은 과학사 석사 과정을 밟았다.) 그들 모두 현재 상주 내과 의사이다. 저희 팀의 최종 인원은 건강 증진에 이력이 있는 건강 분야의 경험 많은 정성 연구자입니다. 임상의로서, 우리는 모두 환자와 그들의 가족과 공동체의 질병 상태뿐만 아니라 사회적 맥락과 개인의 필요를 해결하는 온정의료의 중요성에 대한 깊은 헌신을 공유한다; 연구자로서, 우리는 의료 훈련생들에게 지식과 기술을 확인하고 주입하기 위한 혁신적인 방법을 찾으려고 노력한다.이러한 훌륭한 보살핌을 제공해야 한다.
Our research team represents several points of view relevant to our research question. It is led by a practising physician with masters and doctoral degrees in SSH disciplines whose clinical practice and research take place within a large faculty of medicine. Three other members of the research team are physician faculty members with SSH masters degrees (two in health professions education, one in feminist science studies) who are heavily involved in medical education administration and curriculum design; a fourth physician faculty member with an SSH PhD has served in senior educational and leadership roles in both the faculty and the university. Three more of our team members became involved as medical students (one following a masters degree in the history of science); all of them are now resident physicians. The final member of our team is an experienced qualitative researcher in the health domain with a background in health promotion. As clinicians, we all share a deep commitment to the importance of compassionate medical care that addresses the social contexts and individual needs, as well as the disease states, of our patients and their families and communities; as researchers, we try to find innovative ways to identify and to instil in medical trainees the knowledge and skills required to provide such excellent care.
샘플링 전략
Sampling strategy
우리는 (대학 웹사이트 및 기관 데이터베이스 부여를 통해) 지역 대학 교수진에 대한 목적적 샘플링을 사용하여 다음과 같은 초기 참가자를 식별했다.
- (i) non-Medical Expert CanMEDS 역할과 잠재적으로 관련이 있다고 간주된 광범위한 SSH 분야 중 하나에 대한 공식적인 전문 지식(즉, PhD 또는 동등한 말단 학위)
- (ii) 의료, 기타 보건 직업 또는 건강과 질병의 다른 측면에 대한 학문적 관심
We identified initial participants using purposive sampling (through university websites and granting agency databases) for local university faculty members with:
- (i) formal expertise (i.e. a PhD or equivalent terminal degree) in one of a broad range of SSH disciplines we considered to be potentially relevant to the non-Medical Expert CanMEDS roles, as well as
- (ii) an academic interest in medicine, other health professions, or other aspects of health and disease.
SSH 전문가들 중 일부는 건강 직업 교육을 연구했지만, 대부분은 건강, 질병, 질병, 장애, 건강 관리 시스템 또는 건강 직업을 연구했다. 우리 스스로 임상의로서 우리는 SSH에서 광범위한 대학원 교육을 받았지만 그럼에도 불구하고 의학계의 지배적인 의학 교육에 대한 견해에 익숙해졌다는 사실을 유념했다. 따라서 임상의사가 작성한 많은 기존 의료 커리큘럼에 대한 논문을 보완하기 위해 커리큘럼에 대한 새로운 아이디어를 도출할 뿐만 아니라 허용 가능한 의료 커리큘럼과 의료 지식의 한계에 대한 임상의 선입견을 피하기 위해 임상 교육을 받은 참가자를 제외했다.
Some of these SSH experts studied health professions education, but most studied health, illness, disease, disability, the health care system or the health professions. As clinicians ourselves, we were mindful of the fact that although many of us have extensive graduate training in the SSH, we had nonetheless all been acculturated into the medical community's dominant views of medical education. We therefore excluded participants with clinical training in order to avoid such clinician preconceptions about the limits of the acceptable medical curriculum and medical knowledge, as well as to elicit fresh ideas about the curriculum in order to complement the many existing papers on medical curricula written by clinicians.
비록 우리는 잠재적으로 관련이 있는 학문(사회학, 인류학, 역사학, 정치학, 경제학, 철학, 윤리, 교육, 심리학, 수사학, 언어학, 문학 연구, 종교, 고전, 음악, 드라마)의 초기 목록을 만들고 의도적으로 개인들을 찾아내는 것에서 시작했다. 그런 다음 눈덩이 샘플링을 통해 이 초기 목록을 확장했다(추가 참가자를 찾기 위해 초기 참가자의 조회에 의존하는 비확률적 방법). 수집된 관점의 편차를 극대화하고 의료 교육과 관련된 분야에 대한 우리의 가정에 대해 완화할 수 있도록 훈련 분야와 특정 개인 모두에 대한 것이다. 우리는 단일 분야 내에서 다양한 의견을 수렴하고, 주요 분야의 다양한 목소리를 보장하며, 여러 기관의 다양한 연구 영역에서 전문 지식을 활용하기 위해 여러 지역 대학에서 참가자를 모집하는 것으로 시작했다. 우리는 궁극적으로 우리 지역 내에 더 멀리 있는 여러 대학을 포함하도록 표본을 확장했다.
Although we began with an initial list of potentially relevant disciplines (sociology, anthropology, history, political science, economics, philosophy, ethics, education, psychology, rhetoric, linguistics, literary studies, religion, classics, music and drama) and purposively identified individuals, we then expanded this initial list by snowball sampling (a non-probability method that relies on referrals from initial participants to find additional ones69-71) both for disciplines and for specific individuals in order to maximise variation in the perspectives gathered and to mitigate against our own assumptions about disciplines relevant to medical education. We began by recruiting participants from multiple local universities in order to gather a range of opinions within single disciplines, to ensure multiple voices from key disciplines, and to take advantage of pockets of expertise in different research areas at different institutions; we ultimately extended our sampling to include several universities further afield within our region.
데이터 수집
Data collection
우리는 데이터 수집 프로세스 초기에 55개의 반구조적 인터뷰와 1개의 소규모 포커스 그룹을 수행했다. 첫째, 참가자들이 거의 중앙 위치에 올 수 없었고, 둘째, 포커스 그룹은 동일한 수의 참가자들과의 개별 인터뷰보다 더 적은 정보를 생성했기 때문에 우리는 추가 포커스 그룹을 수행하지 않았다. 전체적으로, 개인들은 우리의 포커스 그룹에 인터뷰하거나 참여했습니다. 참가자들은 인터뷰에 앞서 CanMEDs 의사 역량 프레임워크가 포함된 정보 패키지를 받았는데, 이는 의료 교육에서 CanMEDs 역할의 역사, 정의 및 현재 용도를 설명하는 프로젝트 팀이 작성한 문서, 그리고 그 연구의 수석 조사관이 우리의 연구 프로젝트의 목표를 요약한 기사가 담겨 있다. 우리는 참가자가 선택한 장소 또는 전화로 인터뷰를 진행했습니다. 우리는 참가자들의 허락을 받아 모든 인터뷰를 녹음했습니다.
We conducted 55 semi-structured interviews72-75 plus one small focus group76, 77 early in the data-gathering process. We conducted no additional focus groups because, firstly, participants were rarely available to come to a central location and, secondly, the focus group generated less information than individual interviews with the same number of participants. In total, 58 individuals were either interviewed or participated in our focus group. Participants received an information package in advance of the interview containing the CanMEDS Physician Competency Framework,1 a shorter document written by the project team describing the history, definitions and current uses of the CanMEDS roles in medical education, and a published article by the principal investigator of the study outlining the goals of our research project.21 We conducted interviews at a location of the participant's choosing or by telephone. We audio-recorded all interviews with the permission of participants.
각 인터뷰는 질적 연구 방법에 대해 스스로 훈련받은 의대생이나 질적 연구에 경험이 있는 연구 보조원이 CanMEDS 의 역할에 대해 직접 가르치며 진행했다. 각 인터뷰 동안, 인터뷰 진행자는 참가자에게 비의료 전문가 역할을 설명한 다음, 반구조적인 인터뷰 가이드를 사용하여 각 역할에 대한 철저한 이해를 뒷받침하는 학문적 전문지식 영역의 지식, 이론 및 사실 형태에 대한 토론에 인터뷰 대상자를 참여시켰다. 우리는 또한 참가자들에게 그들이 우리와 공유하고 있는 자료와 관련된 유용한 커리큘럼 자료, 텍스트 및 교육학적 기술을 식별하도록 요청했다. 우리는 동시 분석을 바탕으로 연구 내내 인터뷰 가이드를 반복적으로 조정했습니다. 우리 스스로 또는 눈덩이 샘플링을 통해 식별된 모든 관점이 적절히 표현되고 주제적 포화가 달성될 때까지 인터뷰는 계속되었다.
Each interview was conducted either by a medical student trained by ourselves in qualitative research methods or by a research assistant experienced in qualitative research and taught by ourselves about the CanMEDS roles. During each interview, the interviewer described each non-Medical Expert role to the participant and then, using a semi-structured interview guide, engaged the interviewee in a discussion of the forms of knowledge, theories and facts from his or her area(s) of academic expertise that would underpin a thorough understanding of each role. We also asked participants to identify any useful curricular resources, texts and pedagogical techniques relevant to the material they were sharing with us. We iteratively adjusted the interview guide throughout the study based on our concurrent analysis. Interviewing continued until all the perspectives identified by ourselves or through snowball sampling had been adequately represented and thematic saturation70, 78, 79 had been achieved.
분석.
Analysis
한 연구원은 각 인터뷰의 오디오테이프를 듣고 연구 참가자가 제안한 비생물학적 형태의 지식, 이론, 사실이 포함된 인터뷰 부분을 각 non-Medical Expert CanMEDS 역할에 따라 옮겨 적었습니다. 우리는 의미 응축과 직접 인용을 사용하여 대본을 추가로 추출하여 약 300페이지의 관련 데이터를 산출했다. 우리는 데이터를 정리하기 위해 이 추상화된 스크립트를 nvivo Version 10.0(QSR International Pty Ltd, 멜버른, Vic, Australia)에 업로드했습니다. 우리는 데이터 수집과 동시에 하향식(CanMEDs 역할에 의한) 및 상향식(구조주의 비판적 프레임워크 내에서) 접근 방식을 사용하여 데이터를 코드화했으며, 데이터 수집이 진행됨에 따라 상향식 주제별 코딩 구조를 지속적으로 수정하고 이전 스크립트로 반복적으로 돌아왔다. 우리가 포화 상태에 도달했다고 생각했을 때(샘플에 포함할 분야에 대한 눈덩이 샘플링을 모두 소진하고 캔 MED 역할 또는 주제 부호화 구조와 관련하여 참가자들로부터 더 이상 새로운 개념을 도출하지 않았을 때), 광범위한 학문적 경험을 가진 두 명의 연구 팀 구성원(AK, CW)은SSH와 건강 영역(PV)의 경험 많은 정성 연구원이 분석을 전면 검토했다. 우리는 확립된 범주에 도전하고 참가자들, CanMEDS 역할 및 테마에 걸쳐 데이터를 비교했다.
- (i) 데이터의 개념 모델을 공식화한다.
- (ii) 실제로 포화 상태에 도달했는지 확인한다.
- (iii) 상향식 주제 간 및 이러한 주제와 CanMEDS 의 역할 간 관계를 설정한다.
One researcher listened to the audiotape of each interview and transcribed the sections of that interview that contained the non-bioscientific forms of knowledge, theories and facts suggested by the research participant for each non-Medical Expert CanMEDS role. We further abstracted the transcripts using meaning condensation and direct quotations, resulting in approximately 300 pages of relevant data. We uploaded these abstracted transcripts into nvivo Version 10.0 (QSR International Pty Ltd, Melbourne, Vic, Australia) in order to organise the data. We coded the data using both top-down (by CanMEDS role) and bottom-up (thematically within a constructivist critical framework) approaches concurrently with data collection, constantly revising our bottom-up thematic coding structure as data collection progressed, as well as returning iteratively to earlier transcripts. When we thought we had reached saturation (when we had exhausted our snowball sampling for disciplines to include in our sample and were no longer eliciting novel concepts from our participants in relation to either the CanMEDS roles or our thematic coding structure), two members of the research team (AK, CW) who are MDs with extensive academic training in SSH, as well as an experienced qualitative researcher in the health domain (PV), reviewed the analysis in full; we challenged established categories and compared data across participants, across CanMEDS roles and across themes to:
- (i) formulate a conceptual model of the data;
- (ii) ascertain that we had indeed reached saturation, and
- (iii) establish relationships among bottom-up themes and between these themes and the CanMEDS roles.
분석을 통해 데이터 수집 프로세스가 마무리되었음을 확인한 후, 데이터로부터 예비 기밀 보고서를 작성하고 두 그룹과 공유했다.
- (i) 최종 공식 입력(연구 과정에 대한 지속적인 참여에 더하여)을 위한 전체 연구 팀(의대생 및 SSH 대학원 교육을 받은 의사)
- (ii) 회원 확인에 자원한 인터뷰 참가자 58명 중 18명(우리가 그들의 생각을 정확하게 표현했는지, 그들이 우리의 보고서에 '자신의 목소리를 낼 수 있는지' 확인하기 위해)
이 두 그룹의 피드백은 보고서의 사소한 수정(주로 캐나다 원주민 보건과 관련된 올바른 명명법을 명확히 하고 다양한 SSH 용어의 정의를 추가)을 필요로 했다.
Once we had confirmed through our analysis that we had concluded our data-gathering process, we created a preliminary confidential report from our data that was shared with two groups:
- (i) the full research team (medical students and physicians with interest or graduate training in SSH) for their final formal input (in addition to their ongoing involvement over the course of the study), and
- (ii) 18 of our original 58 interview participants who volunteered to take part in member checking80 (to ascertain that we had accurately represented their ideas and they could ‘hear their own voices’ in our report).
The written feedback from these two groups necessitated only minor modifications to the report (primarily clarifying correct nomenclature related to Canadian Aboriginal health and adding definitions of various SSH terms).
수정된 예비 기밀 보고서는 SSH Phds를 가진 서로 다른 보건 직업의 7명의 임상의에 의해 검토되었으며, 연구 결과를 구현할 가능성이 가장 높은 커뮤니티 내에서 구성원 검사를 받을 수 있도록 허용되었다. 이는 우리의 연구팀의 보고서 이외의 임상의의 목소리를 분석에 추가했다. 다시 한번 말하지만, 이전에 연구에 참여하지 않았던 이 마지막 그룹의 서면 피드백은 보고서에 사소한 수정(다양한 용어의 정의를 더 명확히 하고 지분성 및 반사성과 같은 개념의 중요성에 더 중점을 두는 등)만을 필요로 했다.
The modified preliminary confidential report was then reviewed by seven clinicians from different health professions (including medicine) with SSH PhDs in order to allow it to be member-checked within the community most likely to implement its findings; this added further clinician voices to our analysis beyond those of our research team. Again, written feedback from this last group, the members of which were not previously involved in our study, necessitated only minor modifications to the report (such as further clarifying definitions of various terms and adding more emphasis to the importance of concepts such as equity and reflexivity).
윤리
Ethics
이 프로젝트는 캐나다 Tri-Council 정책 성명 2.1조에 따라 토론토 대학의 연구 윤리 사무소에서 윤리 승인 요건을 면제받았다. 인간을 포함하는 연구를 위한 윤리적 행동, 즉 '어떤 경우에는, 연구는 정보를 얻기 위해 연구의 초점이 아닌 개인들과의 상호작용을 포함할 수 있다. […] 이러한 개인은 본 정책의 목적을 위한 참가자로 간주되지 않는다.'81 그럼에도 불구하고 우리는 모든 연구 참가자에게 서면 사전 동의를 구했고 이를 받았다. 최종 간행물에서 인정을 받고자 하는 참가자는 본 문서의 승인 섹션에 나열되어 있습니다.
This project was formally exempted from requirements for ethics approval by the University of Toronto's Research Ethics Office under Article 2.1 of the Canadian Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans, which states, in part: ‘In some cases, research may involve interaction with individuals who are not themselves the focus of the research in order to obtain information. […] Such individuals are not considered participants for the purposes of this Policy.’81 We nonetheless sought and received written informed consent from all study participants. Those participants who wished to be acknowledged in our final publication are listed in the Acknowledgements section of this paper.
결과.
Results
비의료 전문가 CANMED 역할과 관련된 여러 SSH 분야
Multiple SSH disciplines relevant to non-Medical Expert CanMEDS roles
처음에 non-Medical Expert CanMEDS 역할과 관련된 지식을 포함할 가능성이 높은 분야(예: 보건 사회학, 의료 역사, 중요 장애 연구)에 전문 지식을 보유한 24명 이상의 지역 SSH 연구자를 식별했다. 그 후, 우리의 참가자들은 (우리가 처음에 고려하지 않았던) 다른 관련 전문 분야와 다양한 분야의 포함 기준에 맞는 (그리고 눈덩이 샘플의 일부로 접촉한) 우리 시와 지역 내 대학의 다른 SSH 연구원의 긴 목록을 식별할 수 있었다. 58명의 참가자들이 근무하고 있는 대학과 그들의 학문 전문 분야는 표 1에 제시되어 있다.
We initially identified more than two dozen local SSH researchers who had expertise in disciplines (e.g. sociology of health, history of medicine, critical disability studies) that were a priori likely to encompass knowledge relevant to the non-Medical Expert CanMEDS roles. Our participants were then able to identify other relevant areas of expertise (some of which we had not initially considered), as well as a long list of names of other SSH researchers at universities within our city and region who fit our inclusion criteria in various disciplines (and whom we contacted as part of our snowball sample). The universities at which our 58 participants work and their areas of academic expertise are listed in Table 1.
| Universities | Areas of academic expertise |
McMaster University Ontario College of Art and Design Ryerson University University of Ottawa University of Toronto University of Waterloo York University |
Anthropology Architecture (inc. landscape architecture) Art education Art history Behavioural medicine/science Comparative literature Critical disability studies Education English Environmental planning Ethics Fine arts Gender/women's studies Geography Health economics Health policy/health systems Health promotion Health psychology History Labour Law Performance arts (inc. music and theatre) Philosophy Philosophy of science Planning Political science Religious studies Rhetoric Social psychology Social science and health Sociology |
- Note that some participants identified academic expertise in more than one area
비의료 전문가 캔메이드 역할과 관련된 SSH의 통합 지식 개념 모델
Integrated conceptual model of knowledge from the SSH relevant to non-Medical Expert CanMEDS roles
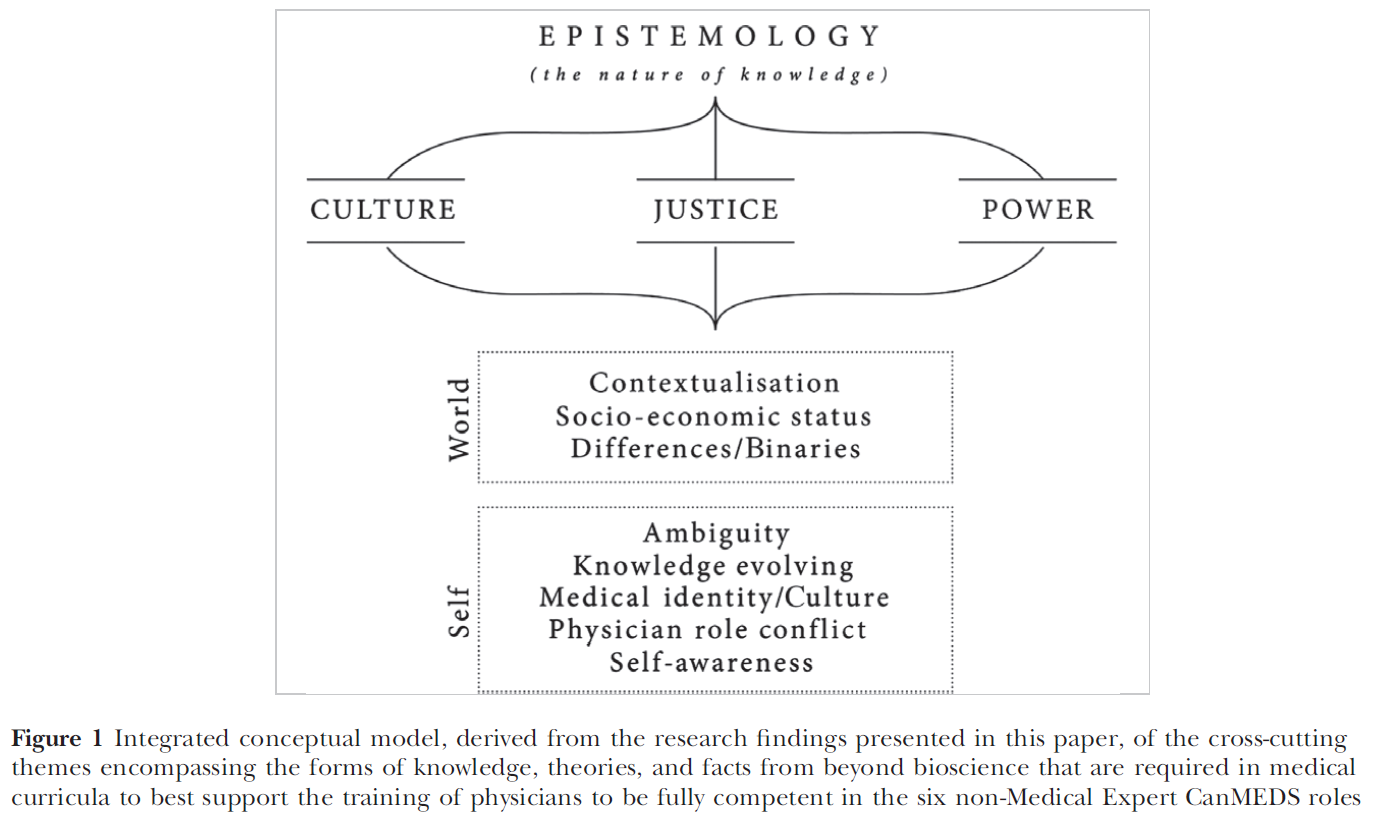
우리는 non-Medical Expert CanMEDS역할을 뒷받침하는 SSH의 지식의 통합 개념 모델을 형성하는 12개의 상호 관련 테마를 데이터에서 식별했다. 이 주제들은 학문분야 범위를 넘나들었고 여러 개의 대화록으로 잘 표현되었다. 이러한 주제들 중에서, [(사회적 지식의 구성된 본질과 다양한 패러다임에서 지식이 어떻게 생산되는지를 포함한) 지식의 본질(인식론)]에 대한 이해는 다른 주제들이 적절하게 가르쳐지거나 이해될 수 없는 기초적인 교육적 요소로 여겨졌다. 나머지 11개 테마 중, 우리의 연구 결과는 상호 연관된 세 가지 앵커링 테마를 강조했다. 문화, 정의, 권력. 이러한 앵커링 테마는 CanMEDS의 모든 역할에 다양한 정도로 필수적이며, 또한 모두 나머지 8개의 교차 주제, 즉 미래의 의사가 세상과 (다른 사람과 관련된 대상) 그리고 자신(개인에게 적용되는 측면)과의 관계에 대한 일련의 풍부한 콘텐츠 영역과 연결된다. 이 모든 주제와 그 사이의 관계는 그림 1에 나타나 있다. 인식론, 문화, 정의, 권력이라는 근본적이고 앵커링된 주제에 좀 더 폭넓게 초점을 맞추고 나머지 8개 주제에 대해서는 간략히 짚어보는 등 각 주제를 차례로 다룰 예정이다. 이러한 각 주제는 온라인 부록 S1에 훨씬 더 자세히 설명되어 있다.
We identified 12 interrelated themes in our data that form an integrated conceptual model of the knowledge from the SSH that underpins the non-Medical Expert CanMEDS roles. These themes cut across disciplinary lines and were well represented in multiple transcripts. Of these themes, an understanding of the nature of knowledge (Epistemology), including the constructed nature of social knowledge and how knowledge is produced in various paradigms, was seen as the foundational curricular component without which the other themes could not be appropriately taught or understood. Among the remaining 11 themes, our findings highlighted three interrelated anchoring themes: Culture, Justice and Power. These anchoring themes are essential to all of the CanMEDS roles to varying degrees; they also all link in turn to each of the remaining eight cross-cutting themes, a series of rich content areas about the future physician's relationships to the world (aspects related to others) and to the self (facets applying to the individual him/herself). All of these themes, and the relationships between them, are represented in Fig. 1. We will address each theme in turn, focusing more extensively on the foundational and anchoring themes of Epistemology, Culture, Justice and Power, and touching briefly on the remaining eight themes. Each of these themes is also described in much greater detail in Appendix S1, online.
인식론은 지식의 본질과 범위를 가리킨다. 지식이란 무엇이며, 어떻게 습득할 수 있는지, 주어진 주제나 실체가 어느 정도까지 알 수 있는지에 대해 질문한다. 교차된 주제로서의 인식론은 사실상 모든 인터뷰 대상자에 의해 확인되었다. 구성주의에 상당한 강조가 있었다: 하나의 고정된 진리는 없고 현실에 대한 우리의 인식은 우리의 역사적, 사회적, 경제적, 문화적, 성별, 계급적 위치에 기초하여 구성된다는 개념이다. 이 주제는 지식이 무엇인지, 다양한 형태의 지식에 대한 한계, 아는 사람이 제거될 수 없는 특정 사회, 역사, 문화적 맥락에서 지식이 어떻게 창조되는지에 대한 이해를 포함한다. 우리의 데이터에서, 이 주제 내에서 중요한 초점 영역은 다음을 포함한다:
- 객관성과 주관성 사이의 긴장,
- 증거로서의 '무엇'이 중요한지에 대한 질문,
- 경험적 지식의 한계,
- 다른 직업에서 아는 방법,
- 특히 환자들 사이에서 지식의 내러티브 형태,
- 건강 지식을 정의하는 데 있어 문화와 위치의 역할
Epistemology refers to the nature and scope of knowledge. It questions what knowledge is and how it can be acquired, and the extent to which any given subject or entity can be known. Epistemology as a cross-cutting theme was identified by virtually all interviewees. There was considerable emphasis on constructivism: the notion that there is no single fixed truth but that our perceptions of reality are constructed based on our historical, social, economic, cultural, gender and class locations. This theme includes understanding of what knowledge is, the limitations of different forms of knowledge, and how knowledge is created in certain social, historical and cultural contexts from which the knower cannot be removed and which affect what he or she is able to perceive and how he or she interprets phenomena. In our data, prominent areas of focus within this theme include:
- the tension between objectivity and subjectivity;
- the question of what ‘counts’ as evidence (what is privileged, included or excluded);
- limits to empirical knowledge;
- ways of knowing in other professions;
- narrative forms of knowledge, particularly among patients, and
- the roles of culture and location in defining health knowledge.
문화는 특정 집단의 공유된 행동, 이상, 가치, 신념으로 정의될 수 있다. 이것은 타당하다고 여겨지게 된 기본적인 가정들의 패턴이며, 새로운 그룹 구성원들에게 느끼고 지각하고 행동하는 방법으로 암시적으로 가르쳐진다. 의학은 그 자체로 하나의 문화이다(표 2의 의학적 정체성/문화 참조). 참가자들은 의학 문화가 사회의 만연하고 체계적인 사회적 불평등에 어떻게 기여할 수 있는지를 의대생들에게 조명하는 것이 도움이 될 것이라고 제안했다. 그러나 문화는 건강 결과에 직간접적인 영향을 미치는 건강의 사회적 결정 요인이기도 하다. 문화가 건강에 미치는 영향, 개인의 건강 관리에 접근하는 능력, 그리고 건강에 대한 개인의 신념뿐만 아니라 문화적 차이에 대한 인식과 존중을 명시적으로 함양하고 존중하기 위한 의료 커리큘럼의 필요성에 대한 강한 지지가 있었다. 이러한 점에서 다른 문화에 대한 가정, 즉 명시적이고 암묵적인 편견에 대한 반사적인 인식은 매우 중요한 것으로 느껴졌다. 문화적 역량, 문화적 겸손, 문화적 안전의 연계된 개념도 이러한 맥락에서 강조되었다. 성공적인 의사소통 및 환자와 의사 관계와의 관련성은 특히 강조되었다. 마침내, 문화적 헤게모니, 또는 지배의 개념은 다른 직업에 대한 의학의 전통적인 지배와 식민지화의 매개체로서의 지속적인 레거시과 관련된 많은 참여자들에 의해 제기되었다. 이는 캐나다 원주민 공동체와 관련하여 특히 중요하지만 다른 소수민족 집단에게 돌봄을 전달하는 의미도 내포하고 있다.
Culture can be defined as the shared behaviours, ideals, values and beliefs of a particular group. It is a pattern of basic assumptions that have come to be considered valid and are implicitly taught to new group members as ways to feel, perceive and behave. Medicine is itself a culture (see also Medical identity/Culture in Table 2); participants suggested it would be helpful to illuminate for medical students how medical culture can contribute to their society's pervasive, systematic social inequities. However, culture is also a social determinant of health with direct and indirect effects on health outcomes. There was strong support of the need for medical curricula to explicitly foster awareness of, and respect for, cultural differences, as well as knowledge of the impact of culture on health, on an individual's ability to access health care, and on an individual's beliefs about health. A reflexive awareness of one's assumptions about other cultures – of one's explicit and implicit biases – was felt to be critical in this regard. The linked concepts of cultural competence, cultural humility and cultural safety were also highlighted in this context; their relevance to successful communication and to the patient–physician relationship was particularly emphasised. Finally, the concept of cultural hegemony, or dominance, was raised by many participants, relating both to medicine's traditional dominance over other professions and to its ongoing legacy of use as an agent of colonisation, which is particularly significant in Canada in relation to Aboriginal communities but also has implications for the delivery of care to other minoritised groups.
우리의 참여자들은 두 가지 상호 연계된 방식으로 정의를 논의하였다.
- (i) 공정성과 형평성과 같은 개념을 언급했던 도덕성, 법률, 직업윤리,
- (ii) 사회 정의.
'도덕성'으로서 정의의 범위 내의 쟁점들은 다음을 포함한다.
- 행동 강령 및 기타 규정된 윤리 행동 규칙
- 전문직업성에 대한 사회계약 관점
- 정직, 공감, 진실성과 같은 원칙을 통합한 윤리적 상상력의 개발
- 특정 집단이 다른 집단에 대해 특혜를 주는 도덕적 기준을 인식하고 의문을 제기할 수 있는 능력
- 환자와 신체로부터 파생된 지식의 적절한 소유권을 포함한 연구 윤리의 이해, 그리고
- 연구 및 임상 실무에서 산업계의 영향력을 인정
Justice was discussed by our participants in two interlinked ways:
- (i) as morality, law and professional ethics, which referred to concepts like fairness and equity, and
- (ii) as social justice.
Issues within the purview of justice as morality included:
- codes of conduct and other prescribed rules of ethical behaviours;
- the social contract view of professionalism;
- the development of an ethical imagination that incorporates principles such as honesty, empathy and integrity;
- the ability to recognise and question moral standards that privilege certain groups over others;
- an understanding of research ethics, including the appropriate ownership of knowledge that is derived from patients and their bodies, and
- a recognition of industry influence in research and clinical practice.
다양한 윤리적 틀이 논의되었다. 절차적 정의(예: 자원의 분배에 관한 의사결정 과정의 공정성)와 분배적 정의(예: 자원의 실제 분배의 공정성)의 구별과 같은 것이다. 또한 응용 철학(예: 결과적 추론 대 원리 기반 추론)이기도 했다. 교육생들에게 윤리적 문제를 토론할 수 있는 보다 강력한 언어를 제공하기 위한 방법으로 몇 가지 도덕 이론(예: 공리주의, 페미니스트 윤리, 가치 윤리)도 제안되었다.
A variety of ethical frameworks were discussed, such as the distinction between procedural justice (e.g. fairness in the decision-making process regarding the distribution of resources) and distributive justice (e.g. fairness in the actual distribution of resources), as was applied philosophy (e.g. consequential reasoning versus principle-based reasoning). Several moral theories (e.g. utilitarianism, feminist ethics, value ethics) were also suggested as ways to provide trainees with more robust language with which to be able to discuss ethical issues.
정의의 두 번째 측면인 사회정의는 모든 사람들의 이익을 위한 사회의 사회적 경제적 자원의 분배로 정의될 수 있다. 이 영역 내에서 참가자들은 정의와 권력의 관계(의사가 사회적 변화를 옹호하기 위해 자신의 영향력과 권한을 사용할 수 있다는 개념 포함)와 계층과 건강 사이의 연관성을 강조했다. 정의와 경제적 원동력 사이의 긴장감은 [효율성과 비용 효과성]이나, [개별 환자를 옹호하고 사회 전반의 자원을 보존해야 하는 의사의 책임 사이]의 double-agency conflict을 지적했다. 참여자들은 또한 사회 정의를 다양성과 연결시켜 일부 환자들이 다른 환자들보다 의료 및 기타 서비스에 접근하는 데 더 많은 장벽을 경험한다고 지적하고, 그러한 사회적 불이익이 여러 소수자 집단에 속한 개인들에게 복합적으로 작용했다고 강조했다.
The second aspect of Justice, social justice, can be defined as the distribution of a society's social and economic resources for the benefit of all people.82 Within this area, participants highlighted the relationship between justice and power (including the notion that physicians might use their influence and authority to advocate for social change) and the link between class and health. They pointed out the tension between justice and economic drivers such as efficiency and cost-effectiveness, as well as the related double-agency conflict between a physician's responsibilities to advocate for individual patients and to preserve the resources of society at large. Participants also linked social justice to diversity, pointing out that some patients experience more barriers to accessing health care and other services than others, and emphasising that such social disadvantage was compounded for individuals belonging to multiple minoritised groups.
권력은 개인, 집단 또는 기관의 신념, 행동, 가치에 영향을 미치거나 통제하는 것으로 정의되며, 데이터 내에서 세 번째 고정 주제였다. 우리의 참가자들은 건강 관리의 네 가지 특정 측면과 관련된 힘의 문제를 분명히 밝혔다.
- (i) 환자와 의사 사이의 관계
- (ii) 의사와 다른 보건 전문가 간의 관계
- (iii) 의료 시스템 내의 제도적 계층 구조
- (iv) 국가와 사법 시스템을 포함한 법률 및 정책 환경
Power, which can be defined as having influence or control over the beliefs, behaviours and values of individuals, groups or institutions, was the third anchoring theme within our data. Our participants articulated issues of power related to four specific aspects of health care:
- (i) relationships between patients and physicians;
- (ii) relationships between physicians and other health professionals;
- (iii) institutional hierarchies within the health care system, and
- (iv) legal and policy environments including the state and the judicial system.
환자-의사 관계의 관점에서 참가자들은 지식과 언어, 비언어적 의사소통 형태에 내재된 힘뿐만 아니라 신뢰, 관계, 기관 및 공유된 의사 결정의 문제를 포함하여 환자와 의사 사이의 권력 차이의 여러 측면에 크게 초점을 맞췄다. 이들은 의사가 자신의 권한을 인정하고 책임질 필요가 있다고 지적했다. 그리고 그렇게 하기 위해서는 계층, 성별, 민족성 및 기타 차이점 원천과 같은 개인과 그룹 간의 권력 차이에 inform하는 사회적 구조에 대한 이해가 필요하다. (차이/이중값, 표 2 및 부록 S1 참조). 참가자들은 또한 의사와 의사가 아닌 동료들 사이의 권력 역학에 대해 토론하며, 의사가 다른 건강 전문가에 비해 갖는 권위의식과 훈련 중 사회화되는 권위의식을 지적했다.
In terms of the patient–physician relationship, participants focused heavily on multiple aspects of the power differential between patients and their physicians, including the power inherent in knowledge, in language, and in non-verbal forms of communication, as well as issues of trust, rapport, agency, and shared decision making. They pointed out that physicians need to acknowledge and take responsibility for their own authority and that, in order to do so, they need to have an understanding of the social constructs that inform variations in power among individuals and groups, such as class, gender, ethnicity and other sources of difference (see also Difference/Binaries, Table 2 and Appendix S1). Participants also discussed the power dynamics between physicians and their non-physician colleagues, pointing to the traditional position of power held by physicians over other health professionals and to the sense of authority to which they are socialised during their training.
개인과 그룹 간의 상호작용에 대한 논평 외에도, 참가자들은 병원, 의료 시스템 전체 및 국가와 같은 기관과 관련하여 '권력'을 개념화했다. 국가가 의사들에게 부여한 정당성의 한 형태인 의료계의 자율성에 대한 개념은 많은 참석자들에 의해 논의되었다. 그들은 의사들이 의료 시스템의 문지기이자 합법적인 질병과 치료의 정의의 중재자로서 엄청난 권한을 부여받았으며, 이러한 권한과 자원에 대한 접근은 의사들이 그들의 힘을 (변화를 옹호하는 것을 포함하여) 공공의 이익을 위해 긍정적으로 활용할 책임을 부여한다고 설명했다. 그들은 이 권력의 역사적 뿌리와 진화는 환자 기대, 의료 전문가의 실천 범위, 자본주의 경제에서 의료 자금 지원 조직의 변화라는 맥락에서 주목했다. 그들은 의사들이 국가에 대한 그들의 권력에 대해 인식하고 그들의 일을 형성하기 위해 의학의 정치적 차원에 대한 지식을 사용할 필요가 있다고 강조했다. 따라서 그들은 의대생들에게 공공 정책의 기초, 정책 변화의 과정, 그리고 그들의 관할 구역에서 입법 과정을 가르칠 것을 제안했다.
In addition to commenting on the interactions between individuals and groups, participants conceptualised Power in relation to institutions, such as hospitals, the health care system as a whole, and the state. The notion of the self-regulation of the medical profession, a form of legitimacy granted to physicians by the state, was discussed by many participants. They explained that physicians have been granted immense authority as gatekeepers to the health care system and as arbiters of the definitions of legitimate diseases and their treatment, and that this authority and access to resources gives physicians the responsibility to leverage their power positively in the interests of the public, including by advocating for change. They noted the historical roots and evolution of this power in the context of changes in patient expectations, in health professional scopes of practice, and in the organisation of health care funding in capitalist economies. They emphasised that physicians need to be aware of their power with respect to the state and to use this knowledge of the political dimension of medicine to shape their work. They therefore suggested that medical students be taught the basics of public policy, of the process of policy change, and of the legislative process in their jurisdictions.
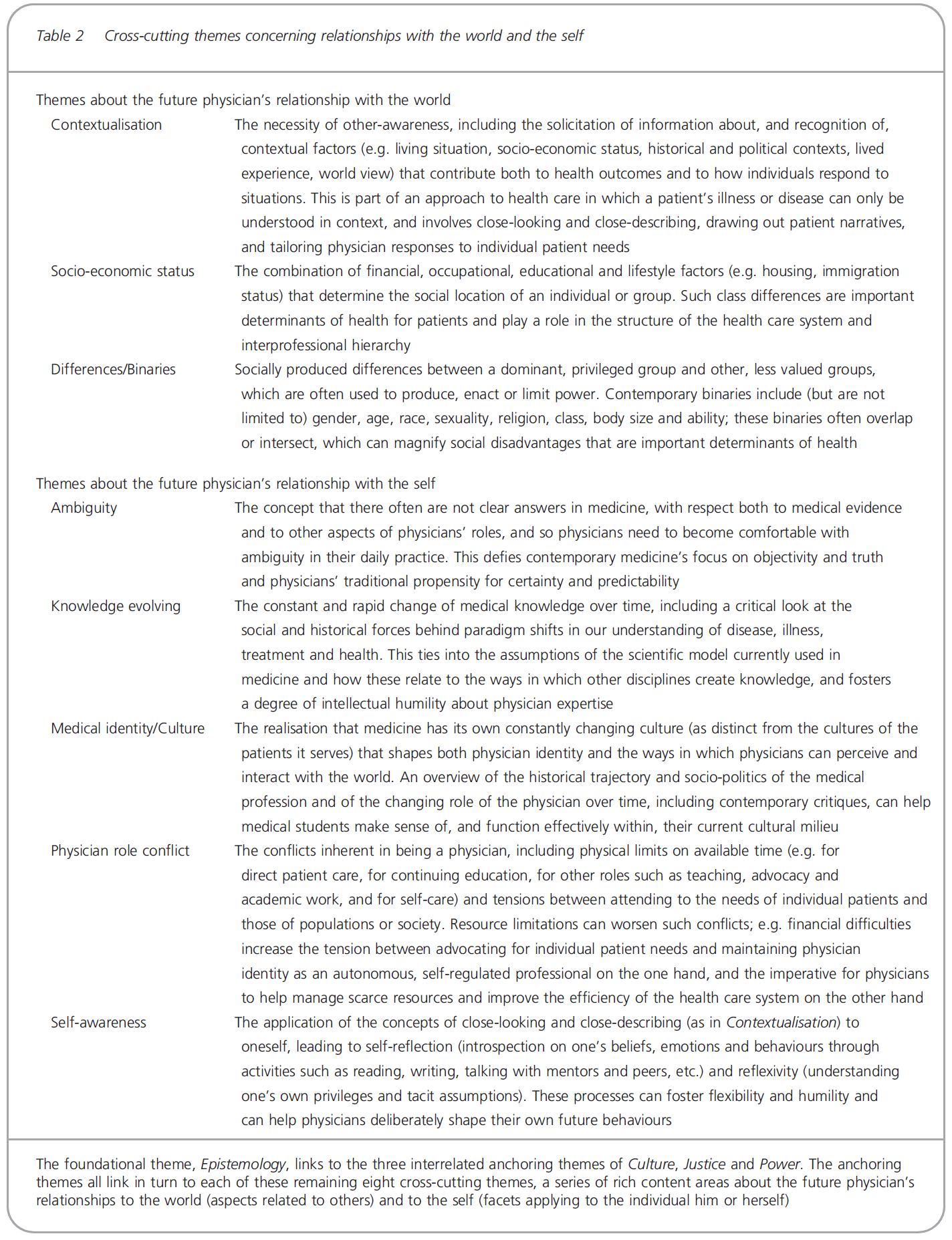
인식론, 문화, 정의, 권력을 넘어, 나머지 8개의 교차 주제는 미래 의사가 세계와 관계(맥락화, 사회경제적 지위 및 차이/이질) 및 자신과의 관계에 초점을 맞추고 있다(그림 1). 이러한 주제는 표 2에 간략하게 설명되어 있으며 부록 S1에 훨씬 더 자세히 설명되어 있다.
Beyond Epistemology, Culture, Justice and Power, the remaining eight cross-cutting themes focus on the future physician's relationships with the world (Contextualisation, Socio-economic status and Differences/Binaries) and with the self (Ambiguity, Knowledge evolving, Medical identity/Culture, Physician role conflict and Self-awareness) (Fig. 1). These themes are described briefly in Table 2 and in much greater detail in Appendix S1.
비의료 전문가 CanMEDs 역할과 관련된 SSH 지식의 교차 특성
The cross-cutting nature of SSH knowledge with respect to non-Medical expert CanMEDS roles
우리는 처음에 데이터에서 식별된 주제 중 어떤 것이 non-Medical Expert CanMEDS 역할과 관련이 있는지를 구별하고자 했다. 하지만 이것이 불가능하다는 것이 금세 우리에게 분명해졌다. 비록 몇몇 주제들이 다른 주제들보다 일부 역할과 더 밀접하게 관련되어 있지만, 그 주제들은 정말로 교차적이었다: 즉, 모든 주제들은 비의료 전문가 역할과 연결되었다. 우리는 (nvivo 10.0에서 이미 코딩한 추상화된 스크립트 데이터의 약 300페이지 내에서) 각 횡단 테마에 대해 상향 코딩한 데이터 청크와 각 캔 MED 역할에 대해 하향 코딩한 데이터 청크를 비교하여 이 교차점을 추가로 탐색했다. 표 3에 수치로 제시된 이 비교의 결과는, 비록 일부 주제와 CanMEDS 의 역할이 특히 밀접한 관련이 있지만(예: 문화와 커뮤니케이터 역할, 권력과 콜라보레이터 역할, 의사 역할 충돌 및 건강 옹호자 역할), 12개 주제 각각에는 6개 역할 각각과 관련하여 별도로 코딩된 자료가 포함되어 있다. 이 흥미로운 발견은 non-Medical Expert CanMEDS 역할의 개념적 통합을 지지하는 증거를 제공할 수 있다.
We had initially intended to distinguish which of the themes identified in our data were linked to each of the non-Medical Expert CanMEDS roles. However, it quickly became clear to us that this would not be possible. Although some themes related more closely to some roles than to others, the themes were truly cross-cutting: that is, every theme was linked to all of the non-Medical Expert roles. We explored this intersection further by comparing (within the approximately 300 pages of abstracted transcript data we had already coded in nvivo 10.0) the chunks of data that we had coded bottom-up for each cross-cutting theme with the chunks of data we had coded top-down for each CanMEDS role. The results of this comparison, which are presented numerically in Table 3, confirmed that although some themes and CanMEDS roles are particularly closely related (e.g. Culture and the Communicator role, Power and the Collaborator role, Physician role conflict and the Health Advocate role), each of the 12 themes includes material that had also been coded separately as relating to each of the six roles. This intriguing finding may provide evidence in support of a conceptual integration of the non-Medical Expert CanMEDS roles.

특정 비의료 전문가 캔메이드 역할과 관련된 SSH의 구체적인 커리큘럼 내용
Concrete curricular content from the SSH relevant to particular non-Medical expert CanMEDS roles
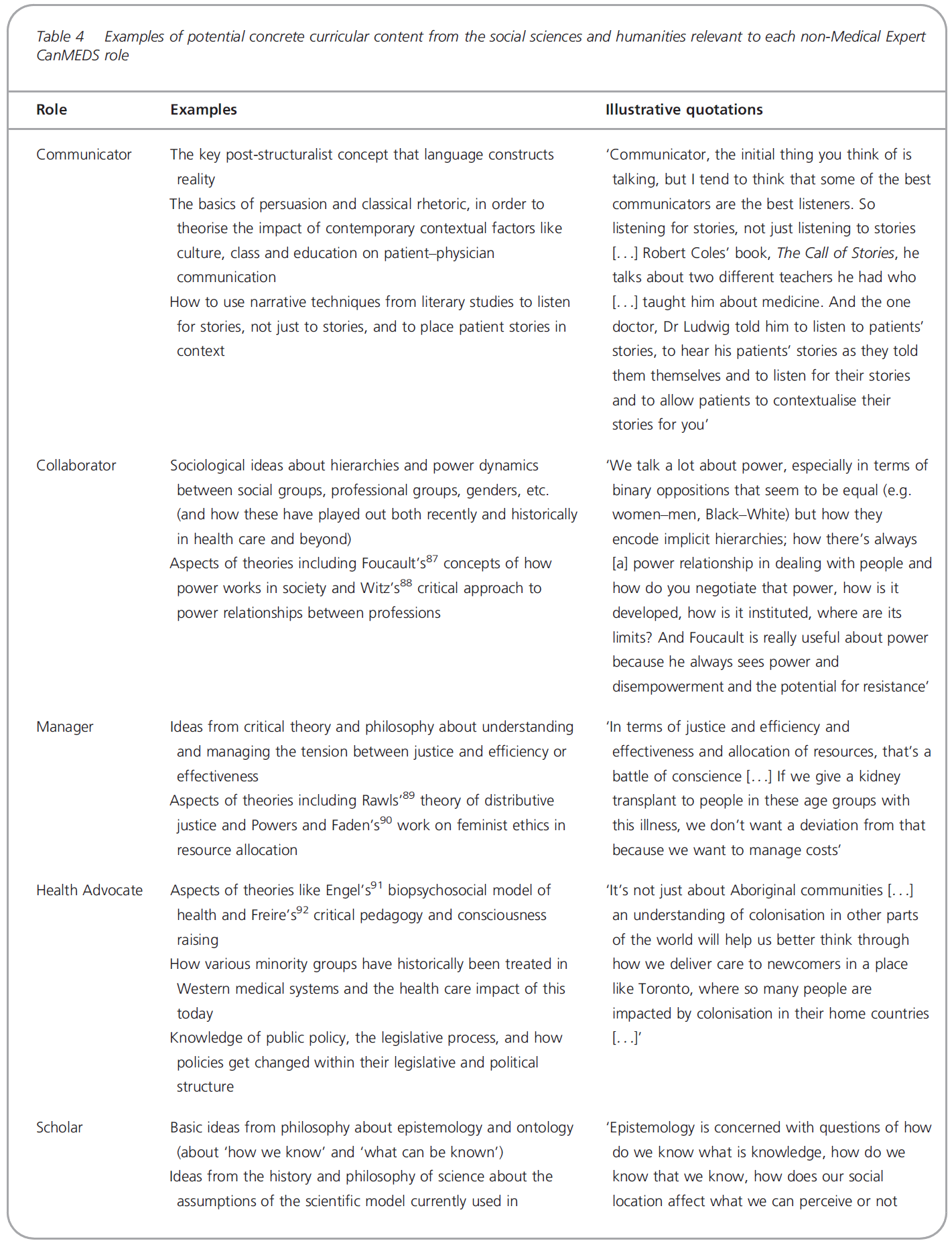
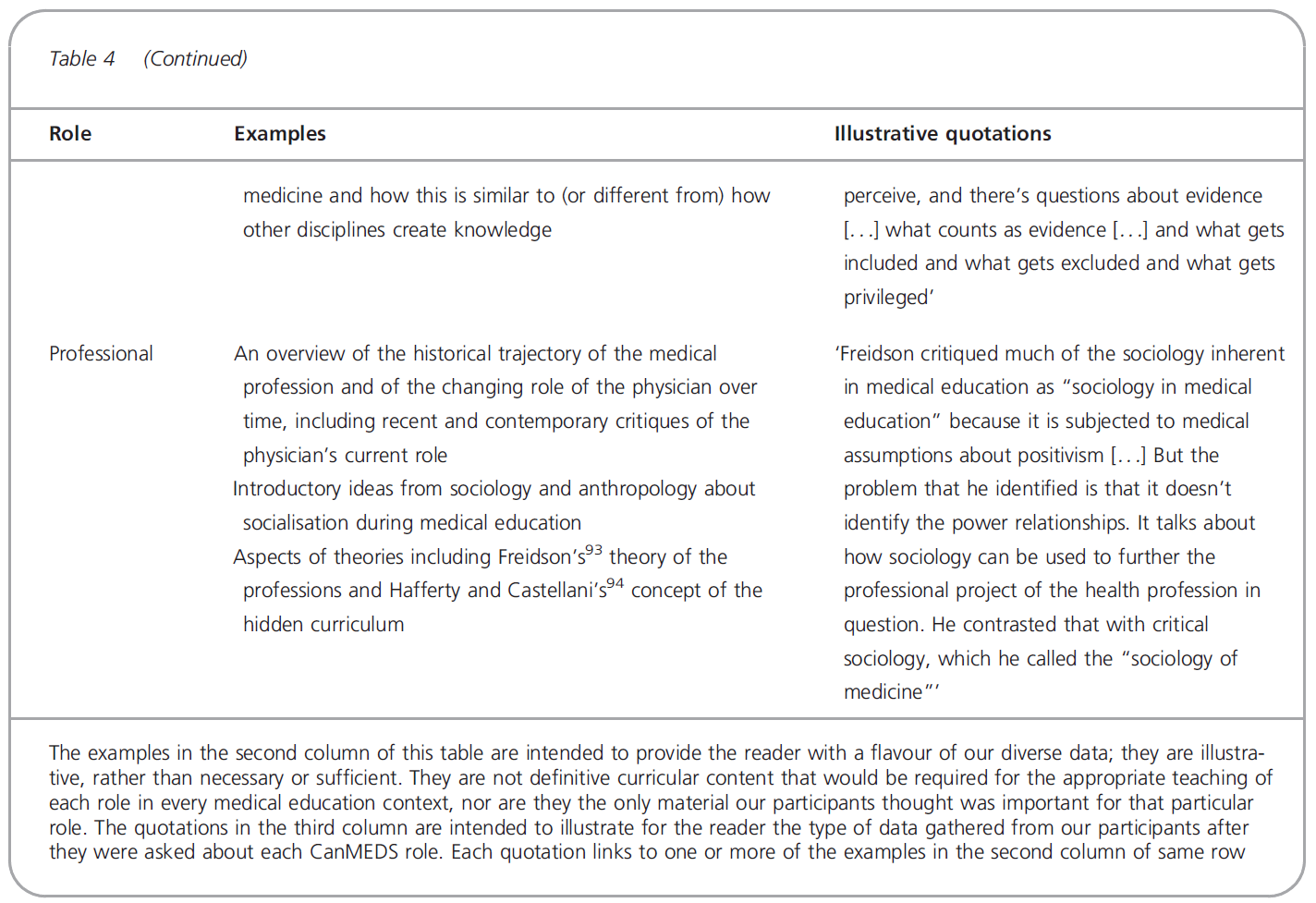
12개의 교차 주제에 대한 개념적으로 풍부한 기초를 넘어, 우리의 데이터는 참가자들이 non-Medical Expert CanMEDS역할과 각각 관련된 것으로 식별한 방대한 양의 구체적인 커리큘럼 콘텐츠를 포함한다. 이 자료의 폭과 다양성을 유지하기 위해 좀 더 간략하게 요약하기보다는 역할별로 분류해 교육과정 기획에 활용할 수 있도록 6개의 대형 문서로 정리했다. 표 4는 참가자들이 각 역할과 관련이 있다고 생각하는 지식의 간략한 표본을 보여줍니다. 표 4의 예는 필요하거나 충분하지 않다. 즉, 모든 의료 교육 맥락에서 각 역할의 적절한 교육에 필요한 지식의 결정적 형태도 아니며, 참가자들이 특정 역할에 대해 중요하다고 인식되는 유일한 자료도 아니다. 오히려, 그것들은 독자들에게 우리의 다양한 데이터의 맛을 제공하는 예시이다.
Beyond the conceptually rich basis for our 12 cross-cutting themes, our data contain an immense amount of concrete curricular content identified by our participants as being related to each of the non-Medical Expert CanMEDS roles. In order to maintain the breadth and variety of this material, rather than summarising it more briefly, we have sorted it by role and compiled it into six large documents for use in curriculum planning. Table 4 contains a brief sampling of the knowledge our participants thought was relevant for each role. It is important to note that the examples in Table 4 are intended to be neither necessary nor sufficient; that is, they are neither the definitive forms of knowledge that would be required for the appropriate teaching of each role in every medical education context nor the only material our participants perceived as important for that particular role. Rather, they are illustrative examples that provide the reader with a flavour of our diverse data.
논의
Discussion
우리의 연구는 non-Medical Expert CanMEDS 역할에 대한 개념적 토대를 형성하고 의사 역량에 대한 캐나다 사회적 기대를 충족하는 의사를 훈련시키기 위해 의료 교육 내에서 필요한 비생물학적 콘텐츠 유형에 대한 경험적 증거를 제공하는 정의 가능한 지식이 있음을 보여준다. 비록 이 내용의 많은 부분이 대부분의 의학 교육 맥락에서 참신해 보이지만, 대학의 다른 곳에서 우리의 학문적 동료들은 적절한 순서 지정과 실질적으로 그것을 가르친 엄청난 경험을 가지고 있다. 우리는 훈련생과 실무자들이 CanMEDS 의 역할을 보다 정교하게 제정함에 따라 의과대학에서 레지던트에 이르기까지 의학교육 연속체의 다양한 단계에 적합한 재료의 깊이를 결정할 때 그러한 경험을 활용할 수 있다.
Our study shows that there is a definable body of knowledge that forms the conceptual underpinnings for the non-Medical Expert CanMEDS roles, and provides empirical evidence for the types of non-biomedical content required within medical education to train practitioners who meet Canadian societal expectations of physician competency. Although much of this content appears novel within most medical education contexts, our academic colleagues elsewhere in the university have enormous experience in both appropriately sequencing and practically teaching it. We can draw on that experience as we determine the depth of materials appropriate to various stages of the medical education continuum, from medical school through to residency and then to continuing medical education, as trainees and practitioners become more sophisticated in their enactment of the CanMEDS roles.
우리의 방법론은 의료 교육자들이 사용할 수 있는 실질적인 실질적인 자료를 제공했다(부록 S1). 우리는 많은 구체적인 커리큘럼 선택권을 제공하는 이와 같은 연구를 통해 교육자들이 비의료 전문가 역할을 가르치는 것이 덜 벅차기를 바란다. 의료 전문가 역할 이외의 역량 교육을 지원하려면 프레임워크에 포함시킨 것과 같이 SSH의 엄격한 콘텐츠 지식을 통합하는 커리큘럼 변화가 절대적으로 필요하다. 이러한 분야의 전문가인 의학 교육자의 상대적 부족은 다음의 필요성을 지적한다.
- 광범위한 학술 의사 채용
- 대학 전체의 교수진과의 파트너십(많은 의과대학이 이미 기초의학과 학과와 제휴하고 있는 것처럼)
- 교수개발.
그러나 이러한 내부 전문지식의 부족은 (다른 새로운 의약품 관련 영역에서 그랬던 것처럼) 극복할 수 있는 과제이다.
Our methodology has provided a substantial body of practical materials for use by medical educators (Appendix S1). We hope that studies such as this, which provide many concrete curricular options, will make it less daunting for educators to teach the non-Medical Expert roles. Curricular change that incorporates rigorous content knowledge from the SSH, such as we have included in our framework, is absolutely necessary if we are to support the teaching of competencies other than those of the Medical Expert role. The relative lack of medical educators who are experts in these areas points to the need
- for broader academic physician recruitment,
- for partnership with faculty members from across the university (just as many medical schools already partner with basic biomedical science departments), and
- for significant faculty development.
However, this lack of internal expertise is a challenge that can be overcome (as it has been in other novel medicine-related domains83).
좀 더 이론적 수준에서, 우리의 데이터(역할과 6개 모두를 가로지르는 주제 사이에 내용이 겹친다)는 non-Medical Expert CanMEDS 역할의 개념적 통합에 대한 명확한 증거를 제공한다. 출판된 문헌에서는 이러한 역할이 인위적인 분할이며, 이러한 역할의 교육과 평가의 통합에 대한 주장이 제기되어 왔다. 다른 곳에서 지적되었듯이, CanMEDS 의 역할은 오늘날 존재하며(그리고 시간이 지남에 따라 변화) 좋은 의사에 대한 우리의 현대적 개념에 맞는 사회적 구조이며 자연스럽지도 않고 불가피하지도 않다. 현재 의사 역량의 해부도는 시간이 지남에 따라 감소할 수 있다. 그 사이에 우리의 발견들, 특히 우리의 횡단 테마는 전체론적으로 의사 역량의 기초를 가르치는 데 교육학적으로 유용한 메커니즘을 제공한다.
On a more theoretical level, our data (both the content overlap between roles and the themes that cut across all six of them) provide clear evidence for the conceptual integration of the non-Medical Expert CanMEDS roles. There have been complaints in the published literature that these roles are artificial divisions – that the constructs they represent are all deeply interrelated – and arguments for the integration of the teaching and assessment of these roles.42, 44, 84 As has been pointed out elsewhere, the CanMEDS roles as they exist today (and as they have shifted over time)1, 2, 9 are social constructs that fit with our contemporary conception of the good physician and are neither natural nor inevitable.44, 85 It may be that the current anatomisation of physician competence will decrease over time. In the interim, our findings, particularly our cross-cutting themes, provide a pedagogically useful mechanism for teaching the underpinnings of physician competence in a holistic way.
제한사항Limitations
이 연구에는 몇 가지 중요한 한계가 있습니다. 예를 들어, 우리는 우리의 연구 결과가 CanMEDS 가 개발되고 연구가 수행된 영어권, 북미, 유럽 중심 환경에 매우 구체적이라는 것을 인정해야 한다. 이것은 우리가 사용한 역량 프레임워크의 적용 가능성뿐만 아니라 다른 문화적 맥락에서 의사와 환자에 대한 우리의 응답자들에 의해 요약된 지식의 형태의 관련성에 중요한 제한을 둔다. 즉, 본 논문에서 제시된 개념 모델과 그에 수반되는 교육 자료 모두 본질적으로 문화적-특이적이다. 그러므로 우리는 다른 문화적 밀리에우스에서 그들의 문맥에 적합한 자료들을 도출하기 위해 유사한 방법론의 사용을 탐구하는데 관심이 있는 협력자들을 매우 환영할 것이다.
There are several important limitations to this study. We must, for example, acknowledge that our findings are very specific to the English-speaking, North American, Eurocentric environment in which CanMEDS was developed and in which our study was conducted. This places important limits not only on the applicability of the competency framework we used,86 but also on the relevance of the forms of knowledge outlined by our respondents to physicians and patients in other cultural contexts; in other words, both the conceptual model presented in this paper and its accompanying curricular materials are innately culturally specific. We would therefore very much welcome collaborators who would be interested in exploring the use of a similar methodology in different cultural milieus to derive materials appropriate for their contexts.
마찬가지로, 우리는 매우 널리 사용되는 역량 프레임워크에 초점을 맞췄지만, 문화적으로 우리와 꽤 일치하는 관할 구역에서는 다른 역량 프레임워크가 사용됩니다. 그럼에도 불구하고 캔메드에 표현된 많은 역량은 이러한 다른 프레임워크에도 존재하며, 이는 잠재적으로 우리의 발견의 광범위한 관련성을 지적한다. 또한, 우리의 방법론의 간단한 특성으로 인해 다른 사람들이 자신의 특정 상황에 대한 우리의 발견을 개선하기 위해 우리의 연구를 확장할 수 있어야 한다.
Similarly, although we focused on a very widely used competency framework,11 other competency frameworks3, 4, 6 are used in jurisdictions that are culturally quite congruent with our own. Nonetheless, many of the competencies represented in CanMEDS are also present in these other frameworks, which points to the potentially broader relevance of our findings. In addition, the straightforward nature of our methodology should allow others to extend our work in order to refine our findings for their own specific contexts; again, we would very much welcome collaborators interested in doing this.
마지막으로, 지난 몇 년 동안 CanMEDS 의 역할과 주변 언어의 세부 사항 중 일부가 바뀌었다는 점에 주목해야 한다. 이 과정은 연구를 시작한 시점과 거의 동시에 시작되었으며(J R Frank, 개인 커뮤니케이션 [전화로], 2011), 2015년 10월에 CanMEDs 2015를 출시했다. 우리는 RCPSC 웹사이트에 요약되어 있고 개념적 재구성이 아닌 일관성과 실제 적용에 초점을 맞추고 있는 2005년과 2015년 캔 MED 문서 사이의 변경 사항을 면밀히 검토했다. SSH 외부의 분야를 이용하는 하나의 주요 새로운 콘텐츠 영역(환자 안전 및 품질 개선)을 제외하고, 대부분의 변경 사항(지도자 역할의 가장 명백한 명칭 포함)은 언어와 조직의 명확화이다. 역할 간에는 몇 가지 사소한 내용 변화가 있지만(예: 비-의사 의료 전문가와의 커뮤니케이션이 이제 공동작업자 역할로 보다 명시적으로 이동됨) 이러한 변화는 참여자들이 언급한 개념적 중복을 크게 완화하지는 못합니다. 마지막으로, 우리는 참여자들이 2005년에 암묵적으로 식별한 몇 가지 개념(예: 문화적 안전)의 2015년 CanMEDS에서 명시적인 인정을 받았으며, 이를 위해 커리큘럼 및 교육학 자료를 이미 개발했다.
Finally, it should be noted that some of the details of, and language around, the CanMEDS roles have changed over the past several years. This process began at about the same time that we initiated our study (J R Frank, personal communication [by telephone], 2011) and culminated in the release of CanMEDS 2015 in October 2015.2 We have closely examined the changes between the 2005 and 2015 CanMEDS documents, which are summarised on the RCPSC website56 and which focus on coherence and practical application rather than a conceptual reframing. The vast majority of changes (including the most obvious, the renaming of the Manager role as the Leader role) are clarifications of language and organisation, with the exception of one major new content area (patient safety and quality improvement) which draws on disciplines outside the SSH. There are some minor shifts of content between roles (e.g. communicating with non-physician health care professionals has now moved more explicitly into the Collaborator role), but these do not substantially mitigate the conceptual overlaps noted by our participants. Finally, we note the explicit recognition in CanMEDS 2015 of a few concepts (e.g. cultural safety) identified by our participants as implicit in 2005 and for which we have already developed curricular and pedagogical materials.
미래 방향
Future directions
비록 이 연구는 원래 지적 연습에서 출발했지만, 우리는 결국 우리의 발견을 실행하고자 하는 프로그램을 찾을 수 있기를 바랐다. 교육과정 갱신에 대한 현지의 관심과 캐나다 인증 요건에서 CanMEDs의 지속적인 사용으로 인해, 우리는 실제로 여러 캐나다 학부 및 대학원 프로그램에서 자발적인 협력자(관리자, 교육자 및 학생)를 찾았다. 또한 CanMEDS 이후 자신의 역량 프레임워크를 모델링한 전문 분야의 다른 보건 전문가를 양성하는 프로그램에서도 협력자를 찾았다. 이 협력자 팀과 함께, 우리는 각 프로그램에 특화된 커리큘럼 콘텐츠의 다중 사이트 롤아웃을 시작했고, 현재 단일 기관에서 서로 다른 수준의 교육(의대, 레지던트, 교수진 개발) 간에 SSH 콘텐츠를 나선화하는 모델 커리큘럼을 구축하고 있다.
우리가 개발한 새로운 커리큘럼 자료에 대한 표준 평가와 더불어, 학장에서 의대생에 이르는 커리큘럼 이해관계자들의 의견을 수렴하여 복잡한 개입에 대한 구현 과정에 대한 엄격한 현실주의 평가를 수행하고 있다. 우리는 이 연구의 발견을 향후 출판물에 공유하고자 한다.
Although this study originally grew out of an intellectual exercise,21 we had hoped that we would eventually locate a programme willing to implement our findings. Due perhaps to current local interest in curriculum renewal and to the continued use of CanMEDS in Canadian accreditation requirements at multiple levels, we have indeed found willing collaborators (administrators, educators and students) at multiple Canadian undergraduate and postgraduate programmes, as well as in programmes that train other health professionals in professions that have modelled their own competency frameworks after CanMEDS. Together with this team of collaborators, we have begun a multi-site rollout of curricular content specific to each programme and are now building model curricula that will spiral SSH content between different levels of education (medical school, residency, faculty development) at a single institution. In addition to a standard evaluation of the novel curricular materials we have developed, we are also conducting a rigorous realist evaluation of the implementation process for this complex intervention, gathering input from curricular stakeholders ranging from deans to medical students; we intend to share the findings from this work in future publications.
doi: 10.1111/medu.13115. Epub 2016 Nov 15.
Epistemology, culture, justice and power: non-bioscientific knowledge for medical training
PMID: 27862175
DOI: 10.1111/medu.13115
Abstract
Context: While medical curricula were traditionally almost entirely comprised of bioscientific knowledge, widely accepted competency frameworks now make clear that physicians must be competent in far more than biomedical knowledge and technical skills. For example, of the influential CanMEDS roles, six are conceptually based in the social sciences and humanities (SSH). Educators frequently express uncertainty about what to teach in this area. This study concretely identifies the knowledge beyond bioscience needed to support the training of physicians competent in the six non-Medical Expert CanMEDS roles.
Methods: We interviewed 58 non-clinician university faculty members with doctorates in over 20 SSH disciplines. We abstracted our transcripts (meaning condensation, direct quotations) resulting in approximately 300 pages of data which we coded using top-down (by CanMEDS role) and bottom-up (thematically) approaches and analysed within a critical constructivist framework. Participants and clinicians with SSH PhDs member-checked and refined our results.
Results: Twelve interrelated themes were evident in the data. An understanding of epistemology, including the constructed nature of social knowledge, was seen as the foundational theme without which the others could not be taught or understood. Our findings highlighted three anchoring themes (Justice, Power, Culture), all of which link to eight more specific themes concerning future physicians' relationships to the world and the self. All 12 themes were cross-cutting, in that each related to all six non-Medical Expert CanMEDS roles. The data also provided many concrete examples of potential curricular content.
Conclusions: There is a definable body of SSH knowledge that forms the academic underpinning for important physician competencies and is outside the experience of most medical educators. Curricular change incorporating such content is necessary if we are to strengthen the non-Medical Expert physician competencies. Our findings, particularly our cross-cutting themes, also provide a pedagogically useful mechanism for holistically teaching the underpinnings of physician competence. We are now implementing our findings into medical curricula.
© 2016 John Wiley & Sons Ltd and The Association for the Study of Medical Education.
'Articles (Medical Education) > 교육과정 개발&평가' 카테고리의 다른 글
| 비판적 '보기'를 향하여: 비판적 페다고지의 영향에 대한 베이지안 분석(Adv Health Sci Educ Theory Pract. 2022) (0) | 2022.05.25 |
|---|---|
| 의사소통, 학습, 평가: 디지털 학습 환경의 차원 탐색(Med Teach, 2019) (0) | 2022.03.18 |
| 보건의료전문직 교육의 평가 - 성과 측정은 충분한가? (Med Educ, 2022) (0) | 2022.01.14 |
| 역량을 넘어: 의학교육의 전인적 관점을 향하여 (Med Educ, 2022) (0) | 2022.01.07 |
| 시스템 기반 의료 다시 생각하기: 졸업후교육의 구조적 역량, 건강 형평성, 사회적 책임(Acad Med, 2020) (0) | 2021.12.12 |