위임의 핵심 용어 명확화(Med Teach, 2021)
Clarifying essential terminology in entrustment
Daniel J. Schumachera , Olle ten Cateb , Arvin Damodaranc , Denyse Richardsond,e, Stanley J. Hamstraf,g,h, Shelley Rossi , Jennie Hodgsonj, Claire Touchiek, Laura Molgaardl , Wade Goftonm, Carol Carraccion and On behalf of the ICBME Collaborators
전 세계 보건 전문가를 위한 많은 교육 프로그램에 의해 수용된 운동인 역량 기반 의료 교육(CBME)은 종종 이정표, 역량 및 위탁의 프레임워크를 사용하여 구현된다. 실제로, 위임 프레임워크를 사용하는 널리 사용되는 CBME 접근방식인 위탁 가능한 전문 활동(EPA)은 지난 10년 동안 전 세계적으로 상당한 관심을 끌었다. 위임 프레임워크와 EPA의 신속하고 광범위한 채택의 의도하지 않은 결과는 이 접근방식의 핵심 개념에 대한 해석의 범위이다. 많은 간행물은 개인 또는 프로그램이 EPA를 개발하는 방법을 상세히 설명했지만, 개념과 원칙을 정확히 정의하는 데는 제한적인 주의를 기울였다. 그 결과 EPA가 공식화되고 위임 의사결정의 기반이 되는 핵심 개념과 원칙을 설명하는 언어의 명확성이 부족하다. 이러한 혼동을 해결하기 위한 유용한 시도가 있었지만, 이러한 노력은 종종 특정 영역에 초점을 맞추지 못했다.
Competency-based medical education (CBME), a movement embraced by many education programs for health professions worldwide, is often implemented using the frameworks of milestones, competencies, and entrustment (Licari and Chambers 2008; Bok 2015; Molgaard et al. 2018; Powell and Carraccio 2018). Indeed, entrustable professional activities (EPAs), a prevailing CBME approach using the entrustment framework, have garnered substantial interest worldwide over the past decade (Chen et al. 2015; Carraccio et al. 2017; Duijn et al. 2019; Meyer et al. 2019; Molgaard et al. 2019; O’Dowd et al. 2019; Shorey et al. 2019). An unintended consequence of the rapid, widespread adoption of the entrustment framework and EPAs is the range of interpretations of the central concepts of this approach. Many publications have detailed how individuals or programs are developing EPAs, but limited attention has been paid to precisely defining concepts and principles (O’Dowd et al. 2019; Shorey et al. 2019). The result is a lack of clarity in the language describing the key concepts and principles upon which EPAs are formulated and entrustment decision-making is based (ten Cate 2014; ten Cate et al. 2016; Taylor et al. 2017; Tekian 2017; Melvin et al. 2019). Useful attempts have been made to address this confusion; however, these efforts have often limited their focus to specific areas (Englander et al. 2013; ten Cate 2013, 2020; Sklar 2015; ten Cate et al. 2015; Post et al. 2016; Taylor et al. 2017; Tekian 2017).
본 문서는 (1) 의료 교육 전반에 걸친 위탁 의사결정 개념에 대한 공통 사전 제안 및 (2) 위탁의 맥락과 결과에 대한 공통 정신 모델을 옹호함으로써 위탁 구조에 대한 보다 포괄적인 설명을 제공하는 것을 목표로 한다. 우리는 [언어를 명확히] 하고 [용어를 보다 정확하게 정의]하는 것이 교육자, 연구자 및 저자를 위한 참조가 되어서, 혼란을 줄이고 매우 필요한 공유 정신 모델을 발전시킬 수 있다고 믿는다. 우리는 언어가 살아있는 것이라는 것을 인정하며 어떤 작가도 언어의 사용에 대해 완전한 통제권을 가질 수 없다는 것을 인정한다. 우리가 위임에 관한 명확화에 기여하고자 하는 이유는, 언어가 교육과 평가 관행을 형성할 수 있는 힘을 가지고 있다는 확신 때문이며, 이것이 현재의 글쓰기에 대한 우리의 동기를 부여한 근본적인 목적이다. 본 문서는 개념과 정의가 저자들의 관점을 반영한다는 본질적인 한계를 가지고 있지만, 우리는 모두 국제 CBME 공동작업자 그룹의 일원이며 이 주제에 대해 경험이 있을 뿐 아니라 헌신적이라는 점에 주목할 가치가 있다고 생각합니다.
This article aims to offer a more comprehensive clarification of the entrustment construct by (1) proposing a common lexicon for the concepts of entrustment decision-making across the continuum of medical education and (2) advocating a common mental model for the context and consequences of entrustment. We believe clarifying language and more precisely defining terminology as a reference for educators, researchers, and authors contributing to this literature can reduce confusion and advance a much-needed shared mental model. We acknowledge that language is a living thing and no authors can ever have full control over its use. The reason we want to contribute to clarification around entrustment talk is our conviction that language has the power to shape education and assessment practices, and it is this underlying purpose that has motivated us for the current writing. Although this paper has the inherent limitation that the concepts and definitions reflect the authors’ views, we believe it is worth noting that we are all members of the International CBME Collaborators group and are both dedicated to this topic as well as experienced in it.
위임체계 및 위임 가능한 전문활동
The entrustment framework and entrustable professional activities
다양한 수준의 감독활동을 할 수 있는 신뢰의 관점에서 학습과 평가를 고려하는 위임 프레임워크는 여러 가지 장점이 있습니다.
- 첫째, 위임 프레임워크는 양질의 관리를 제공하기 위해 얼마나 많은 감독이 필요하거나 필요하지 않은지를 고려하게 함으로써, [환자를 학습 및 평가 공식의 한 부분으로] 가져온다.
- 둘째, EPA를 구체적으로 사용하는 경우, 위임 프레임워크는 (학습자가 중요한 역량을 통합할 것으로 요구되는) 전문직의 진정한 활동authentic activity을 관찰하고 지도하도록 임상 감독자를 배치한다.
- 마지막으로, 그리고 아마도 가장 중요한 것으로, [EPA는 개인이 신뢰받을 수 있는 실제 전문적 실천요강의 단위를] 나타내며, 결국 [인구집단의 요구]에 따라 [감독 없이 practice하고, 다른 사람들을 감독할 수 있는 능력]으로 귀결된다(Vandewaetere et al. 2015).
The entrustment framework, which considers learning and assessment through the lens of being trusted to perform activities with various levels of supervision, has several strengths.
- First, the entrustment framework brings care of the patient into the learning and assessment equation by considering how much supervision is, or is not, needed to provide quality care.
- Second, when using EPAs specifically, the entrustment framework positions clinical supervisors to observe and coach authentic activities of the profession that require the learner to integrate critical competencies.
- Finally, and perhaps most importantly, EPAs represent actual units of professional practice that individuals can be trusted to do with varying levels of supervision, culminating in the ability to practise without supervision and to supervise others, based on the needs of populations served (Vandewaetere et al. 2015).
따라서 교육적 실무의 목적을 위해, 전문적 활동을 위임받는 과정에서 학습자를 지원할 학습 경험을 확인하고 개발하는 직업 EPA에서 역방향 비전 프로세스에 참여한다.
Thus, for educational practice purposes, one engages in a backward visioning process from the profession’s EPAs to identifying and developing learning experiences that will support learners’ in their progress toward becoming entrusted with those professional activities.
독립적 진료행위, 감독되지 않은 진료행위, 자율성, 감독 및 감독 구분
Differentiating independent practice, unsupervised practice, autonomy, supervision, and oversight
독립적 진료행위
Independent practice
EPA 및 그와 관련된 위임 감독 척도에 대한 초기 작업은 관리 제공이 궁극의 '독립적 진료행위' 수준으로 개선됨에 따라 감독을 점진적으로 축소하는 데 초점을 맞췄다(Ten Cate 등. 2010). 그러나 [독립성]을 개념화하는 것은 어려운 일이다(Schumacher et al. 2013). 교육 환경에서 독립이라는 단어는 개인이 교사나 감독자에게 의존하지 않는다는 것을 나타내기 위해 사용될 수 있지만, [직장 동료들로부터의 독립]이라는 개념으로 합해질 수 있다. [독립]을 [의사가 환자의 병을 고치는 기술이나 지혜의 고립된 원천이라는 시대착오적인 개념]과 혼동해서는 안 된다. 설령 시골에 혼자 있는 의사라도 간호사, 조수, 또는 그들이 협력할 수 있는 다른 건강 관리 동료들을 갖게 될 것이다.
Early work on EPAs and their related entrustment-supervision scales focused on gradually lessening supervision as care delivery improves to an ultimate level of ‘independent practice’ (ten Cate et al. 2010). However, the conceptualization of independence has been challenged (Schumacher et al. 2013). The word independence in an educational setting may be used to signify that an individual is not dependent on a teacher or a supervisor, but it may also be conflated with independence from co-workers. Independence should not be confused with the anachronistic notion that a medical professional is an isolated wellspring of skills or wisdom, fixing whatever ails a patient. Even a solo practitioner in a rural area will have a nurse, assistant, or other health care colleagues with whom they can collaborate.
그들은 또한 질문에 대한 답을 찾기 위해 접근할 수 있는 자원을 갖게 될 것이다. 예를 들어, 그들은 인터넷에서 의료 문헌과 기타 자원을 검색할 수 있고, 전화나 전자적 수단을 통해 컨설턴트 및 기타 의료 기관과 연결할 수 있다. 따라서 이러한 점을 고려한다면, 의사는 독립적으로 진료하고 있지 않다. '독립'이란 단어는 의사가 전적으로 그들 자신의 지식, 기술, 능력, 그리고 수단에만 의존한다는 것을 의미한다. 따라서, 우리는 이 단어를 사용하지 않을 것이며, 대신 의료 서비스가 실제로 제공되는 방식과 일치하는 [감독되지 않은 진료행위]를 사용할 것이다.
They will also have resources that they can access to seek answers to their questions; for instance, they can search the medical literature and other resources on the Internet, and they can connect with consultants and other health care providers via telephone or electronic means. These individuals are not practising independently, which would imply they are left entirely to their own knowledge, skills, abilities, and means. Thus, our preference is to avoid this word altogether and instead speak of unsupervised practice, which is consistent with how health care is actually delivered.
자율성
Autonomy
종종 감독supervision이 자율성autonomy에 반대되는 것으로 간주하는 경우가 많다(Schumacher et al. 2013). 이 틀에서 개인은 [감독을 받거나 자율성을 부여받을] 수 있다. 우리는 이러한 관점을 지지하지 않으며, Schumacher 등이 제안한 [자기 결정 이론에서 정한 자율성의 정의]를 채택할 것이다: 자신의 의지에 따라 행동한다(Ryan and Deci 2000; Schumacher et al. 2013). 감독을 받는 안전한 환경에서 이러한 능력을 부여하면, 학습자는 [현재의 competence 수준(할 수 있는 것)]에서 [capability를 입증하는 것(할 수 있지만 아직 하지 못한 것)]으로 나아갈 수 있다.
Often supervision is thought of as the antithesis of autonomy, as if they are at opposite ends of the same spectrum (Schumacher et al. 2013). In this framing, an individual can either be supervised or be granted autonomy. We do not support this view but rather align with Schumacher and colleagues who suggest adopting the definition of autonomy set forth in self-determination theory: acting of one’s own volition (Ryan and Deci 2000; Schumacher et al. 2013). Granting this ability in the safe setting of being supervised allows individuals to progress from their current level of competence (what they can do) to demonstrating their capability (what they are able to do but have not yet done) (Fraser and Greenhalgh 2001).
이는 학습을 발전시킬 뿐만 아니라, 감독자가 개인의 성과에 대한 leading edge를 밀고 관찰하여 감독을 줄일 수 있는 준비 상태에 대한 결정을 내릴 수 있도록 한다. 자율성은 accountability and liability을 반영하는 법적인 의미를 가지고 있지만, 많은 ealy-career autonomous medical professional들은 그들의 고품질 진료행위을 강화하기 위해 멘토링이나 코칭을 필요로 하거나 원하고 있다(Donahue et al. 2021; Duijn et al. 2020).
This not only advances their learning but also positions supervisors to push toward and observe the leading edges of individuals’ performance to make determinations about their readiness for less supervision. Autonomy has a legal connotation reflecting accountability and liability, but many early-career autonomous medical professionals need or desire mentorship or coaching to strengthen their high-quality practice (Donahue et al. 2021; Duijn et al. 2020).
감독과 감시
Supervision and oversight
감독은 일반적으로 [다른 의사의 치료와 행동을 감독하는 것]으로 임상 환경을 생각하면 이해가 쉽다. 그러나 '감독'의 정의가 달라지면서 복잡성이 발생하였다(Lingard와 Goldszmidt 2020).
- 임상 감독은 영국 심리학 저널에서 다음과 같이 정의되었다.
- '선배/자격 보건의가 사례 중심적이고 동료(감독관)의 작업을 지원, 지시 및 안내하는 강도 높은 관계 기반 교육과 훈련을 공식적으로 제공하는 것'
- 품질관리, 감독자의 역량과 역량 유지 및 촉진, 감독자의 효과적인 업무 지원 등의 기능을 수행한다.'(Millne 2007).
- Kilminster와 동료들은 의학교육에 대한 감독을 다르게 정의하며,
- '[안전하고 적절한 환자 진료를 제공하는 수련생 경험]의 맥락에서 [개인, 전문적, 교육적 발달 문제에 대한 지침과 피드백을 제공]하는 것'으로 정의한다(Kilminster et al. 2007).
Supervision is generally well understood in the clinical setting as overseeing another practitioner’s care and actions. However, definitions of supervision diverge, creating complexity (Lingard and Goldszmidt 2020).
- Clinical supervision has been defined in the British Journal of Psychology as
- ‘the formal provision, by senior/qualified health practitioners, of an intensive relationship-based education and training that is case-focused and which supports, directs, and guides the work of colleagues (supervisees).
- Its function includes quality control, maintaining and facilitating the supervisees’ competence and capability, and helping supervisees to work effectively’ (Milne 2007).
- Kilminster and colleagues define supervision in medical education differently, as
- ‘the provision of guidance and feedback on matters of personal, professional, and educational development in the context of a trainee’s experience of providing safe and appropriate patient care’ (Kilminster et al. 2007).
이 두 가지 정의 모두 일반적으로 국어사전에 반영되어 있는, 감독에 대한 [보다 공식적이거나 위계적인 역할 설명(말 그대로 '위에서-본다')이 부족하다. 임상 감독으로서의 감독은 의료 교육 분야에서 케네디와 동료의 작업에 의해 잘 설명된다(Kennedy et al. 2007). 감독에 대한 guidance and oversight 관점을 결합함으로써, ten Cate는 목적에 더 적합한 것으로 보이는 임상 감독을 위한 새로운 정의를 제안했다.
- [관찰 및 지도]에 의한 [의료 관련 학습 및 효과적인 업무]에 대한 [지침 및 지원]을 제공하는 것으로서,
- 필요한 경우, [책임자의 위치]에서 [정확하고 안전하게 업무를 수행하도록 보장]하는 업무 또는 활동의 수행
Both of these definitions suffer from a lack of a more formal or hierarchical role description of supervision (literally ‘over-sight’), reflected in common dictionaries. Supervision as clinical oversight is also well elaborated by the work of Kennedy and colleagues in medical education (Kennedy et al. 2007). Combining both the guidance and oversight perspectives of supervision led ten Cate to propose a new definition for clinical supervision that seems a better fit for the purpose:
- ‘The provision of guidance and support in learning and working effectively in health care by observing and directing,
- when necessary, the execution of tasks or activities to ensure that they are done correctly and safely, from a position of being in charge’ (ten Cate 2018).
신뢰도, 신뢰, 위임, 임시 및 최종 위임 결정, 위임 가능성 및 준비 상태
Trustworthiness, trust, entrustment, ad hoc and summative entrustment decisions, entrustability, and readiness
신뢰도
Trustworthiness
신뢰성trustworthiness은 [사람들이 여러분에게 의지할 수 있도록 하는 항상 선하고 정직하고 성실한 특질(옥스포드 영어 사전)]이라는 의미를 가지며, 다른 사람이 (그 사람을) 신뢰할 수 있게 기여 하는 개개인이 보이는 일군의 특질이나 행동으로 구성된다. 그 다음에 신뢰trust를 다룬다. 신뢰성만으로는 위임 결정을 내리기에 충분하지 않기 때문이다.
Trustworthiness (‘the quality of always being good, honest, sincere, etc. so that people can rely on you’ – Oxford English Dictionary) consists of traits or behaviours that individuals demonstrate, which contribute to others trusting them. We address trust next, as trustworthiness alone is not sufficient to make entrustment decisions.
케네디와 동료들은 의학 교육의 맥락에서 학습자의 신뢰성의 네 가지 구성 요소를 보고한다.
- (1) 지식과 기술,
- (2) 양심(즉, 철저성과 의존가능성),
- (3) 분별력(즉, 자신의 한계를 인식하고, 도움을 구하려는 의지),
- (4) 진실성(Kennedy et al. 2008)
Kennedy and colleagues report four components of trustworthiness of learners in the context of medical education:
- (1) knowledge and skill,
- (2) conscientiousness (i.e. thoroughness and dependability),
- (3) discernment (i.e. awareness of limitations and willingness to seek help), and
- (4) truthfulness (Kennedy et al. 2008).
이 작업 20년 전, 경영 문헌에서 메이어와 동료들은 신뢰성의 핵심 요소로서 [능력, 무결성 및 자비심]을 제안했다(Colquitt et al. 2007). 능력, 즉 지식과 기술은 직무에 분명히 내재되어 있지만, 신뢰성을 결정하는 다른 특성은 그렇지 않다. 이것은 [일반적general 신뢰성]이 [작업-특이적 신뢰성]과 구별되어야 하는지에 대한 의문을 제기한다. [일반적인신뢰성]은 정직, 도움을 구하는 것, 그리고 신뢰성과 같은 특징을 보이는 경향이 있는 개인을 가리키는 데 사용될 수 있습니다.
Two decades before this work, in the management literature, Mayer and colleagues proposed ability, integrity, and benevolence as key components of trustworthiness (Colquitt et al. 2007). Ability, or knowledge and skill, is obviously inherent to a task, but the other characteristics that determine trustworthiness are not (ten Cate and Chen 2020). This raises the question whether general trustworthiness should be distinguished from task-specific trustworthiness. General trustworthiness can be used to refer to an individual who tends to display features such as honesty, help-seeking, and dependability.
그러나 이 사람조차도 주어진 작업에 필요한 지식과 기술을 갖추지 못할 수 있습니다. 따라서 [작업-특이적 신뢰성]을 입증하지 못할 수 있습니다.
- 자기자신의 한계를 알고 있는 진실되고 양심적인 소아과 의사를 떠올려보라. 그들은 일반적인 신뢰를 가지고 있는 것으로 보일 수 있다. 또한, 귀 감염이 발생한 어린이를 관리하기 위한 [과제-특이적 신뢰성]이 뛰어날 수 있습니다. 그러나 신경외과에 대한 교육을 받지 않은 이상 소아 뇌종양을 절제하는 지식과 기술은 거의 제한적입니다. 그러므로, 그들은 이 수술 절차에 대한 [작업-특이적 신뢰성]이 부족하다.
However, even this person may not possess the requisite knowledge and skill for a given task. Therefore, they may not demonstrate task-specific trustworthiness.
- Consider a truthful, conscientious pediatrician who is aware of their limitations. They may be seen as possessing general trustworthiness. They may also possess excellent task-specific trustworthiness for managing a child presenting with an ear infection. However, unless also trained in neurosurgery, they almost certainly have very limited, if any, knowledge and skill for resecting a pediatric brain tumor. Therefore, they lack task-specific trustworthiness for this surgical procedure.
[일반적 신뢰성]과 [작업-특이적 신뢰성]의 이러한 차이는 일반적 신뢰성은 작업 특이적 신뢰성의 필요조건이지만 충분 조건은 아닌 이유를 보여준다. 마찬가지로, 일반적인 신뢰도는 특정 작업에 대한 준비 상태와 동일하지 않다.
This distinction between general and task-specific trustworthiness underscores why general trustworthiness alone is necessary but not sufficient for being trusted to perform a specific task. Similarly, general trustworthiness does not equate with readiness for a specific task.
신뢰, 위임, 임시 및 최종 위임 결정
Trust, entrustment, and ad hoc and summative entrustment decisions
신뢰trust는 명사이자 동사이다. 명사로서 trust에 대한 정의는 Mayer와 동료의 것이 가장 많이 인용된다.
- '다른 당사자를 감시하거나 통제할 수 있는 능력에 관계 없이, [신뢰자trustor에게 중요한 특정 행위]를 [다른 당사자가 수행하리라는 기대에 따라] 타 당사자의 행동에 취약해질 수 있는 의지'
Trust is both a noun (a psychological attitude) and verb (the act of relying on someone or something) (Castelfranchi and Falcone 2010). Mayer and colleagues’ definition of the noun is most cited:
- ‘the willingness of a party to be vulnerable to the actions of another party based on the expectation that the other will perform a particular action important to the trustor, irrespective of the ability to monitor or control that other party’ (Mayer et al. 1995).
동사로서 Trust보다 '위임entrustment'에 더 관련이 있는 것은 Enstruting이다.
- (누군가에게) 개인, 조직 등에 가치 있거나 중요한 것에 대한 책임을 부여하는 것
More relevant for entrustment than the verb trust is entrusting:
- ‘to assign the responsibility for something valued or important to a person, organization, etc.’ (Oxford English Dictionary).
위임은 trustor가 다른 개인(trustee)에게 부여하는 것이다. 타인을 위임하는지의 여부에 있어 인지된 신뢰성trustworthiness이 주요 요소이기는 하지만, 타인을 위임하는 과정은 다른 요인의 영향을 받고 미묘한 차이를 보인다. Dijksterhuis, Hauer 등은 작업장의 위임 결정에 영향을 미치는 다섯 가지 요소 그룹을 설명하였다.
Entrustment is granted by a trustor to another individual (a trustee). While perceived trustworthiness is a primary factor in whether or not another individual is entrusted, the process of entrusting another is nuanced and influenced by other factors. Dijksterhuis, Hauer and others have described five groups of factors that affect entrustment decisions in the workplace:
- the trustee,
- the trustor,
- the task,
- the context, and
- the trustee–trustor relationship (Dijksterhuis et al. 2009; Hauer et al. 2014).
따라서, 한 preceptor에 의해 간접적인 감독을 받을 준비가 되어 있는 것으로 보이는 학습자라도, [연습생을 알지 못하는 다른 preceptor]에게는 신뢰를 받지 못할 수 있다. 환자의 질병의 심각성, 제공되어야 할 치료의 어려움과 위험, 낮이든 밤이든 상관의 경험과 신뢰 성향, 그리고 임상 환경의 분주함이 모두 연습생에게 맡기는 임시 결정의 역할을 한다. 위임은 학습자의 준비와 무관하게 수행될 수도 있고 발생하지 않을 수도 있습니다. 이것은 심리상태로서의 [신뢰trust]와 행위로서의 [위임entrustment]의 차이를 강조한다. 신뢰는 필요하지만 위임 결정을 내리기에는 충분하지 않다.
- 개인은 신뢰할 수 있고 신뢰자와 긍정적인 관계를 맺을 수 있지만, 관련된 상황 및 위험 때문에 trustor들이 업무를 맡기지 않을 수도 있다.
- 마찬가지로, [높은 수준의 신뢰성를 보이는 개인]일지라도, [신뢰에 대한 신뢰자의 제한된 성향]과 [다른 고려사항] 때문에 특정 업무가 위임되지 않을 수 있다.
이러한 이슈로 인해 학자들은 [위임 결정]으로부터 [신뢰]를 분리하게 되었다.
Thus, a learner who may seem ready for indirect supervision (or who is entrusted with indirect supervision) by one preceptor may not be trusted by a different preceptor who is not acquainted with the trainee. The severity of illness of the patient, the difficulty and risk of the care to be provided, the time of day or night, the experience and trust propensity of the supervisor, and the busyness of the clinical environment all play a role in ad hoc decisions to entrust trainees. Entrustment may or may not happen, even independent of the learner’s readiness for it. This underscores the differentiation between trust as a state of mind and entrustment as an act. Trust is necessary but not sufficient to make an entrustment decision.
- An individual may be trustworthy and have a positive relationship with the trustor but many not be entrusted with a task because of the context and risk involved.
- Similarly, an individual who demonstrates a high level of trustworthiness may not be entrusted with a specific task because of a trustor’s limited inclination to trust and other considerations.
These issues have led scholars to separate trust from entrustment decisions (Mayer et al. 1995; Damodaran et al. 2017; Holzhausen et al. 2017; ten Cate et al. 2020).
[신뢰trust]와 [위탁entrustment]의 관계를 복잡하게 만드는 것은, 감독자들마다 상황, 업무, 심지어 위험과 상관없이 신뢰 성향이나 신뢰 의지에 있어서 서로 다르다는 점이다. [신뢰 성향trust propensity]은 인지된 위험과 실제 위험을 고려해야 한다. [실제 위험]은 [맥락과 과제]에 내재되어 있다. 그러나 [인지된 위험]은 감독자마다 다를 수 있으며 따라서 [trustor에게 내재적instrinsic]이다. 쇼크 상태의 환자를 삽관하기 어려운 경우와 같이 위험이 높은 경우 실제 위험과 인지 위험 사이에 일반적인 합의가 있을 수 있습니다. 그러나, 한 교사가 다른 교사가 하지 못하게 하는 일을 할 수 있도록 하기 위해, 교사의 위험 관용과 경험 수준에 따라 위험에 대한 다른 인식이 있을 수 있습니다.
Complicating the relationship between trust and entrustment, supervisors differ in their trust propensity, or their willingness to trust a person regardless of the context, task, and even risk involved (ten Cate 2017). Trust propensity necessitates consideration of perceived and actual risk. Actual risk is intrinsic to the context and task. However, perceived risk may differ across supervisors and is therefore intrinsic to the trustor. There may be general agreement between actual and perceived risk when risk is high, such as with a difficult intubation of a patient in shock. However, there may be different perceptions of risk based on a preceptor’s risk tolerance (determining their trust propensity) and experience level, such that one preceptor may allow learners to do things another preceptor would not let them do.
마찬가지로 신뢰 성향은 [인식된 편익]과 [실제 편익]에 따라 달라질 수 있다. 예를 들어, 수탁자를 병원에 혼자 두고 집으로 돌아가 이 결정으로 인해 야간 혜택을 받는 교사를 예로 들 수 있다. 이는 또한 보다 멀리 떨어진 감독을 통해 자신감을 쌓을 기회를 원하는 수탁자에게 도움이 될 수 있으며, 그렇지 않을 경우 준비되지 않은 수탁자가 노출될 수 있다. 즉, 학습자에게 업무를 맡기는 경향은 위탁자가 인지하는 위험과 혜택에 영향을 받습니다(10개 항목 2017).
Similarly, trust propensity may vary on the basis of perceived and actual benefits. For example, a preceptor who leaves the trustee alone in the hospital and goes home for the night benefits from this decision. This may also benefit the trustee who desires the opportunity to build confidence through practising with more distant supervision or it may leave an unprepared trustee exposed. In short, the tendency to entrust learners with tasks is influenced by the trustor’s perceived risks and benefits of entrusting (ten Cate 2017).
신뢰할 수 있고, 신뢰할 수 있으며, 실무에 대한 준비 상태
Entrustable, entrustability, and readiness for practice
직장에서의 신뢰성trustworthiness이라는 단어는 지식 및 능력뿐만 아니라 성격적 특성을 떠오르게 한다. 그 결과 [일반적 신뢰성]과 [업무 특이적 신뢰성] 사이의 미묘한 차이 때문에 [(당신을) 아직 신뢰할 수 없다]는 피드백은 쉽게 오해를 받는다. 이러한 오해를 해소하기 위해, 학습자를 설명할 때 trustworthiness라는 단어를 entrustable 이라는 단어로 대체하는 경우가 많습니다. 때때로, 이것은 학습자가 가지고 있는 신뢰성의 수준을 논의함으로써 운영화된다. 그러나, '위임'이라는 단어는 학습자가 [수행하는 활동activity]을 특징지으며, 해당 활동을 [수행하는 사람the person]에게 할당되는 것이 아니다(10년, 2005년, 2020년).
As the word trustworthiness in the workplace brings to mind character traits as well as knowledge and abilities, feedback that one is not yet trustworthy is easily misunderstood because of the nuances between general and task-specific trustworthiness. To address this misunderstanding, individuals often substitute the word trustworthiness with the word entrustable when describing learners. Sometimes, this is operationalized by discussing the level of entrustability that a learner possesses. However, the word entrustable was meant to characterize activities that a learner performs and not to be assigned to the person who is performing them (ten Cate 2005, 2020).
이러한 오용 때문에 Cate는 학습자를 enstrustable 또는 pre-entrustable로 qualifying하는 것이 부정확할 뿐만 아니라, [ordinal entrustment-supervision scale를 잘못 해석하는 것]으로 이어질 수 있다고 지적했다. [적절한 감독 수준에 대한 결정이나 권고]가 아니라, 이 scale을 [숙련도의 연속형 척도]로 볼 오해가 있다는 것이다. 이 척도는 이러한 방식으로 사용하도록 만들어진 것이 아니다. 더욱이, [상사가 물리적으로 존재하는 것]과 [물리적으로 존재하지 않는 것] 사이의 등급은 비논리적이다. 감독관은 유령과 같은 모습으로 존재할 수 없다. 감독관은 있든지 없든지 둘 중 하나다. 이러한 이유로, 당사는 학습자를 위임 또는 사전 위임으로 지칭하는 것뿐만 아니라, 위임의 정도degree of entrustability를 기술하는 척도를 사용하지 않는 것에 동의합니다. 오히려, 우리는 [practice을 위한 준비 상태]라는 용어를 사용하는 것을 지지한다.
This misuse has led ten Cate to argue that qualifying learners as entrustable or pre-entrustable (Association of American Medical Colleges 2014; Englander et al. 2016) not only is inaccurate but may also lead to a misinterpretation of ordinal entrustment-supervision scales, moving away from the discrete recommendations or decisions of a level of supervision and instead interpreting the scales as a continuous measure of proficiency (ten Cate 2020). These scales are not intended to be used in this manner. Furthermore, a rating between a supervisor being physically present and being not physically present is illogical. A supervisor cannot be present as a ghostly apparition. Either they are present or they are not present. For this reason, we agree with discouraging the use of scales that describe degrees of entrustability as well as referring to learners as entrustable or pre-entrustable. Rather, we advocate using the term readiness for practice.
다양한 단계의 교육 및 전문 분야에 대한 위임 결정 표현
Expressing entrustment decisions for various stages of training and specialties
위임의 개념은 훈련 단계와 의료 실무 분야 전반에 걸쳐 안정적이다(즉, supervision없이 practice할 준비가 되어 있다는 것은 특정 작업에 대한 감독 없이 일할 수 있다는 것을 의미하며, 이는 그 사람이 학생이든 전공의든 수의사든 치과의사든 마찬가지다). 그러나 특정 단계의 훈련 및 실무에 대해서는 위임 감독 척도에 사용되는 언어의 추가 관리 및 특수성이 보장될 수 있다(Rekman et al. 2016; 10 Kate et al. 2020). 대부분의 경우 일반적인 5단계 위임 관리 규모가 사용됩니다.
The concept of entrustment is stable across stages of training and fields of heath care practice (i.e. readiness to practice without supervision means an individual can work without supervision for a given task whether they are a student, a resident, a veterinarian, or a dentist). However, additional levels of supervision and specificity of language used in entrustment-supervision scales may be warranted for particular stages of training and fields of practice (Rekman et al. 2016; ten Cate et al. 2020). Most often, a generic five-level entrustment-supervision scale is used:
- May be present but may not practise the EPA;
- May practise the EPA under direct, proactive supervision, with supervisor physically present in the room;
- May practise the EPA under indirect, reactive supervision, with supervisor not physically present but quickly available;
- May practise the EPA unsupervised;
- May act as supervisor for others for the EPA (ten Cate et al. 2010).
이것은 학부 의대 교육을 위해 Chen과 동료들에 의해 더욱 정교하게 설명되었습니다. 그들은 학생들이 무언가를 관찰하는 것조차 허락되지 않을 수도 있는 하위 단위에 추가적인 수준을 추가하였습니다(Chen 등. 2015).
This has been further elaborated by Chen and colleagues for undergraduate medical education; they have added additional levels at the lower end where a student may potentially not even be allowed to observe something (Chen et al. 2015).
주어진 분야 내에서 실무 분야와 전문 분야 간에 위임-감독 척도를 달리해야 할 필요성도 주목할 필요가 있다.
- Hatala와 동료들이 지적하듯이, 많은 [내과 과업]들이 [외과]와 같은 시술 전문분야의 과업들보다 less well-circumscribed되어 있다(Hatala et al. 2019). 내과에서 많은 학습자 활동을 면밀히 모니터링하지만 직접 관찰하지는 않는다. (하탈라 외. 2019; 멜빈 외. 2019)
- 또한, 마취과 의사의 핵심위임질문에 대한 Weller와 동료의 인식은 다음과 같다. '수술방을 떠나도 될까?' (그리고 담당 레지던트를 떠나도 될까?)
- 마지막으로, 미국의 소아과 커뮤니티에서 인기 있는 Chen 위임-감독 척도의 언어는 해당 커뮤니티에서 위임 및 감독에 대한 정신적 모델의 요구를 충족하고 그에 맞게 조정되었다(Schumacher et al. 2020).
The need for differing language for entrustment-supervision scales between fields of practice and specialties within a given field is also important to note.
- As Hatala and colleagues note, many internal medicine tasks are less well-circumscribed than the tasks in procedural specialties such as surgery (Hatala et al. 2019). Much learner activity in internal medicine is closely monitored but not directly observed (Hatala et al. 2019; Melvin et al. 2019).
- Furthermore, Weller and colleagues’ perception of the core entrustment question in the minds of anesthesiology attendings is: ‘Can I leave the operation theatre?’ (and leave the resident in charge) (Weller et al. 2014).
- Finally, in the pediatric community in the United States, the language of the popular Chen entrustment-supervision scale has been adapted to meet the needs of, and align with, the mental model of entrustment and supervision in that community (Schumacher et al. 2020).
때때로 분야와 전문 분야 간의 감독에 대한 정신적 표현의 차이에서 비롯된 이러한 언어 문제는 일률적인 해결책으로는 해결될 수 없다. 우리는 감독 수준의 일반적인 프레임워크가 남아있어야 한다고 생각하지만, 그 프레임워크 내에서 수정adaptation하는 것이 유익하다. 본 문서에서는 상황에 맞는 적절한 위임-감독 척도를 도출하는 방법에 대한 지침을 제공할 수 없지만, 다양한 분야와 전문 분야의 교육자와 학자들은 가장 효과적인 언어 및 필요한 수의 감독에 대해 자세히 설명할 수 있다.
These language issues, sometimes stemming from differences in mental representations of supervision between field and specialties, cannot be resolved with a one-size-fits-all solution. We believe that the generic framework of levels of supervision should remain, but within that framework adapations are beneficial. Guidelines around how to derive contextually suitable entrustment-supervision scales cannot be offered in this paper, but educators and scholars in various fields and specialties can elaborate for their field or specialty the most effective language and the required number of supervision levels.
소급평가 대 예비위임
Retrospective evaluation versus prospective entrustment
위임-감독 척도는 두 가지 방법으로 사용되었습니다.
Entrustment-supervision scales have been used in two ways:
- (1) O-SCORE 척도의 경우처럼, 목격한 작업에 얼마나 많은 감독, 지침 및 지원이 필요했는지 보고한다. (내가 직접 해야 했다, 구두로 지시하면 되었다 등)
- (2) 아직 진행되지 않은 상황을 포함하여, 학습자가 향후 특정 활동을 수행할 때 얼마나 많은 감독을 필요로 하는지를 권고한다.
- (1) to report how much supervision, guidance, and/or assistance was needed and provided for a witnessed task, as in the case of the O-SCORE scale (with levels specified as: I had to do, I had to talk them through, etc.) (Gofton et al. 2012; Rekman et al. 2016) and
- (2) to recommend how much supervision a learner requires in the execution of specific activities in the future, including as-yet-undefined situations.
- 전자는 [발생한 관찰(즉, 후향적)을 보고하는 역할]을 하고 숙련도의 판단을 이끄는 척도이다.
후자는 전향적 위임 결정을 제공하기 위해 관찰자의 추가적인 추론을 필요로 한다. - The first is a scale that serves to report on observations that have occurred (i.e. retrospectively) and that lead to a judgment of proficiency.
The second requires additional inference by the observer to render a prospective entrustment decision.
후향적 평가는 위험, 유익성 및 결과에 대한 알려진(개인적으로는 가변적 추정치이지만) 사후 판단으로 판단되는 특정 맥락에 위치한다. 본질적으로 위임 결정은 전향적인 결정이기에, 미래의 상황, 위해성, 유익성 및 결과를 미리 알 수는 없다. [위임-감독 척도]라는 용어를 사용하여 과거에 얼마나 많은 supervision가 제공되었는지를 반영하는 것은 물론, 향후 감독 수준에 대한 권고 사항도 포함하고 있음을 강조합니다.
Retrospective evaluations are situated in a specific context with known (albeit individually variable estimates of) risks, benefits, and outcomes, judged in hindsight. With entrustment decisions, which are inherently prospective, the contexts, risks, benefits, and outcomes are unknown. We suggest using the term entrustment-supervision scale, as we have done in this paper, to stress that this scale not only reflects how much supervision was provided in the past but also includes a recommendation for a future level of supervision, implying entrustment for the future.
[전향적 위임 결정]은 [일반적 신뢰성 및 업무-특이적 신뢰성]을 모두에 기초해야 한다. 이것은 다음의 두 가지를 설명한다.
- 필요할 때 정직하고 양심적이며 도움을 구하는 학습자의 일반적인 경향과
- 아마도 이후에 수행해야 할 과제에 대한 학습자의 지식과 기술(과제별 신뢰도)
Prospective entrustment decisions should be based on considering both general and task-specific trustworthiness. This accounts for
- a learner’s general tendency to be honest, conscientious, and seek help when needed (general trustworthiness) as well as
- a learner’s knowledge and skill for the tasks they will probably be called upon to perform (task-specific trustworthiness).
이 중 후자를 고려할 때에는 학습자가 지식과 기술을 적용함에 있어, 알려진 것에서 알려지지 않은 것으로 [외삽extrapolate할 수 있는 능력에 대한 판단]을 고려해야 한다.
This latter consideration should consider judgments about a learner’s abilities to extrapolate from the known to the unknown in applying their knowledge and skills.
잠재적 위임 결정을 내릴 때 일반적인 신뢰도를 고려할 때, ten Cate 와 Chen은 의료 분야에서 위탁을 가능하게 하는 학습자 특성 연구에 기초하여 다섯 가지 요소 그룹을 기술했다. 역량, 무결성, 겸손, 신뢰성 및 대리. 이것들은 우리가 이전에 논의한 신뢰성 구조trustworthiness construct와 잘 맞아떨어진다. 우리가 위임 결정을 내릴 때, 만약 개인이 입증된 능력 이상으로 위임을 받는다면, 그 결정과 미래의 상황에 관련된 위험은 개인의 [일반적 신뢰도]에 크게 의존하는 위탁 결정에 의해 완화된다.
When considering general trustworthiness in making a prospective entrustment decision, ten cate and Chen have delineated five groups of factors on the basis of studies of learner charcteristics that enable entrustment with tasks in health care: capability, integrity, humility, reliability, and agency (ten Cate and Chen 2020). These align well with the trustworthiness constructs we discussed previously. If we consider these features when making an entrustment decision, if and when an individual is entrusted beyond their demonstrated competence, the risk involved in that decision and the future situation is mitigated by the entrustment decision leaning heavily on the individual’s general trustworthiness.
위험을 추가로 평가하기 위해, ten Cate와 Hoff는 위임-기반 논의를 평가 툴킷의 일부로 포함할 것을 제안했다. 그러한 논의에는 위험과 합병증에 대한 인식에 대한 논의와 감독 감소의 위험을 측정하기 위한 '만약에…한다면 어떻게 했을 것인가'라는 질문을 부과하는 등의 간단한 대화가 포함된다.
To further assess risk, ten Cate and Hoff have proposed including entrustment-based discussions as part of an assessment toolkit (ten Cate and Hoff 2017). Such discussions are multiple brief conversations that include discussing awareness of risks and complications as well as imposing ‘what would you have done if…’ questions to gauge the risks of decreased oversight.
위임어 실용화
Practical use of entrustment language
엄격한 정의를 넘어 정의된 용어를 실천할 수 있는 잠재 능력까지 확대하여 일부 위임 권고는 실제 위임 결정으로 이어질 수 없다는 점을 되새김으로써 마무리하겠습니다. 예를 들어 의대생과 전공의는 종종 기준이든 법률이든 또는 두 가지 모두이든, 명시된 어느 정도의 감독을 필요로 한다. 학습자가 완전히 유능하고 감독 없이 일할 준비가 되어 있다고 하더라도, 전문 분야에 대한 면허 또는 인증을 받지 않은 사람은 법률상 금지될 수 있습니다. 이것은 현행법에 따라 훈련 중에 제정될 수 있는 위임 결정의 범위에 제한을 둔다. 어떤 전공의에게 [감독되지 않은 진료행위]을 맡길 준비가 되었다고 판단되는 경우, 그러한 진료행위이 허용되어야 합니까?
Extending beyond strictly definitions to the potential ability to put defined terms into practice, we will end by reflecting on the fact that some entrustment recommendations cannot lead to an actual entrustment decision. For example, medical students and residents often require some level of oversight that is specified in standards, laws, or both. Even if a learner is completely competent and ready to work unsupervised, law may prohibit this if the person is not licensed or certified for a specialty. This places a limit on the scope of entrustment decisions that can be enacted during training under current legislation. If individuals are deemed ready to be entrusted with unsupervised practice, should that be permitted?
최근 보고서는 의료 직무의 '걱정스러운 진급'와 그에 따른 [교육생 책임 감소]에 주목하고 있다. 이로 인해 졸업생이 중요한 환자 진료 업무를 수행할 준비를 충분히 하지 못할 수 있다. 그러나 아직 교육 중인 개인에 대해 [감독되지 않은 의료행위]에 위임할 준비가 되어 있는 것에 대한 결정을 허용하는 것은 [유효한 위임 결정에 대한 충분한 증거가 있을 때]를 정의해야 하는 의료 교육계에 큰 책임을 지게 한다. 어렵겠지만, 우리는 이것이 우리가 성취하고자 하는 목표라고 믿는다.
Recent reports have noted the ‘worrisome seniorization’ of tasks in health care and consequent decrease in responsibilities for trainees (Halpern and Detsky 2014; Dacey and Nasca 2019). This may jeopardize the readiness of graduates to perform critical patient care tasks (Mattar et al. 2013; Donahue et al. 2021). However, allowing decisions about readiness to be entrusted with unsupervised practice to be made for individuals who are still in training places enormous responsibility on the medical education community to define when there is sufficient evidence for valid entrustment decisions. While lofty, we believe this is a goal that we should seek to achieve.
이를 달성하려면 연습생은 의료 기관이나 병원 내에서 자격 증명을 받아야 합니다. 그래야 감독 없이 일할 수 있습니다. 졸업 전에 위탁 결정의 제정을 가능하게 하는 조치를 취하지 않고, 이러한 결정에는 궁극적으로 충분한 의미가 있는가? 안전망이 줄어들 때까지 누군가가 practice을 시작할 때까지 기다리는 것보다, 감독자의 감독 이상의beyond 안전망이 있는 교육 프로그램의 한계 내에서 위탁 결정을 내리는 것]이 덜 위험할 수 있다.
Achieving this would also require trainees to be credentialed within a practice or hospital so that they could be permitted to work without supervision. Without taking the step of enabling enactment of entrustment decisions before graduation, is there ultimately sufficient meaning in those decisions? It is probably less risky to make entrustment decisions within the confines of a training program, where there are safety nets beyond supervisor oversight (nursing staff, colleagues, etc.) than to wait until someone goes into practice, where the possibility of a safety net lessens.
결론
Conclusion
위임은 의료 감독관이 작업장에서 학습자를 감독하는 동안 수행하는 작업을 토대로 의료진의 관리 제공에 대한 판단을 내리도록 요구하는 평가 프레임워크이다. 또한 환자와 안전한 양질의 치료 제공을 고려한다. 만약 우리가 공유된 위임 언어에 합의할 수 있다면, 이 구조의 특징은 교육생들을 보다 총체적인 교육으로 포용할 수 있는 것이다. 그러나 유용한 프레임워크로서의 위임의 모든 편익은 프로그램 내에서, 프로그램 간에, 그리고 훈련과 실습의 연속선 전체에서 합당한 일관성을 가지고 사용될 경우에만 실현될 것이다. 이것은 우리가 본 문서에서 제공하려고 시도한 위임 언어에 대한 공통의 이해가 필요합니다.
Entrustment is an assessment framework that asks clinical supervisors to make judgments about a trainee’s care delivery on the basis of what they do while supervising learners in the workplace. Moreover, it brings the patient and the provision of safe, quality care into consideration. If we can agree on a shared language of entrustment, these characteristics of this construct present the opportunity to embrace a more holistic education of trainees. However, the full benefit of entrustment as a useful framework will only be realized if it is used with reasonable consistency within programs, between programs, and across the continuum of training and practice. This requires a common understanding of the language of entrustment, which we have attempted to provide in this paper.
Med Teach. 2021 May 14;1-8.
doi: 10.1080/0142159X.2021.1924365. Online ahead of print.
Clarifying essential terminology in entrustment
Daniel J Schumacher 1, Olle Ten Cate 2, Arvin Damodaran 3, Denyse Richardson 4 5, Stanley J Hamstra 6 7 8, Shelley Ross 9, Jennie Hodgson 10, Claire Touchie 11, Laura Molgaard 12, Wade Gofton 13, Carol Carraccio 14, ICBME Collaborators
Affiliations collapse
Affiliations
- 1Cincinnati Children's Hospital Medical Center, University of Cincinnati College of Medicine, Cincinnati, OH, USA.
- 2Center for Research Development of Education, University Medical Center Utrecht, Utrecht, The Netherlands.
- 3Prince of Wales Clinical School, Faculty of Medicine, UNSW Sydney, Sydney, Australia.
- 4Department of Medicine, University of Toronto, Toronto, Canada.
- 5The Royal College of Physicians and Surgeons, Ottowa, Canada.
- 6Accreditation Council for Graduate Medical Education, Chicago, IL, USA.
- 7University of Ottawa, Ontario, Canada.
- 8Department of Medical Education, Feinberg School of Medicine, Northwestern University, Chicago, IL, USA.
- 9Department of Family Medicine, University of Alberta, Edmonton, Canada.
- 10Virginia-Maryland College of Veterinary Medicine, Blacksburg, VA, USA.
- 11The Medical Council of Canada, University of Ottawa, Ottawa, Canada.
- 12University of Minnesota College of Veterinary Medicine, St. Paul, MN, USA.
- 13Royal College of Physicians and Surgeons of Canada, University of Ottawa, Ottawa, Canada.
- 14American Board of Pediatrics, Chapel Hill, NC, USA.
- PMID: 33989100
- DOI: 10.1080/0142159X.2021.1924365AbstractKeywords: undergraduate education; Clinical assessment; outcomes-based; postgraduate education.
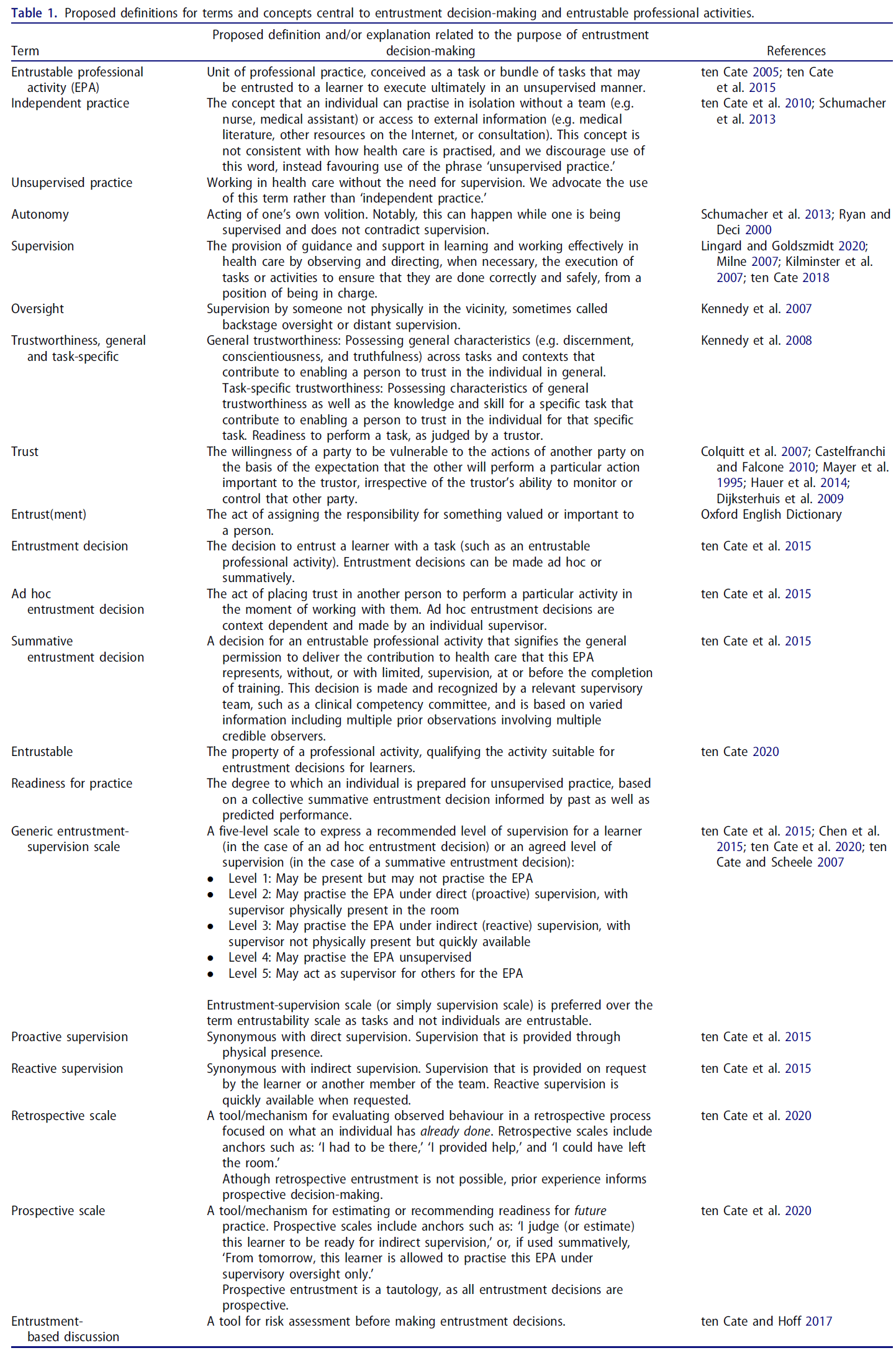
- With the rapid uptake of entrustable professional activties and entrustment decision-making as an approach in undergraduate and graduate education in medicine and other health professions, there is a risk of confusion in the use of new terminologies. The authors seek to clarify the use of many words related to the concept of entrustment, based on existing literature, with the aim to establish logical consistency in their use. The list of proposed definitions includes independence, autonomy, supervision, unsupervised practice, oversight, general and task-specific trustworthiness, trust, entrust(ment), entrustable professional activity, entrustment decision, entrustability, entrustment-supervision scale, retrospective and prospective entrustment-supervision scales, and entrustment-based discussion. The authors conclude that a shared understanding of the language around entrustment is critical to strengthen bridges among stages of training and practice, such as undergraduate medical education, graduate medical education, and continuing professional development. Shared language and understanding provide the foundation for consistency in interpretation and implementation across the educational continuum.
'Articles (Medical Education) > 임상교육(Clerkship & Residency)' 카테고리의 다른 글
| 인지심리학은 어떻게 의학교육의 얼굴을 바꾸었는가 (Adv Health Sci Educ Theory Pract, 2020) (0) | 2021.08.27 |
|---|---|
| 감정적 사건의 보초병: 전공의의 수치심 경험의 특징, 트리거, 효과(Acad Med, 2019) (0) | 2021.08.03 |
| 위험과 이득 관리하기: 위임 결정의 핵심 이슈(Med Educ, 2017) (0) | 2021.07.16 |
| 위임 결정: 환자를 평가 공식으로 가져오기 (Acad Med, 2017) (0) | 2021.07.16 |
| ISBAR를 활용한 환자인계 가르치기(BMC Med Educ, 2020) (0) | 2021.07.13 |