어떻게 임상감독자는 수련생에 대한 신뢰를 형성하는가: 질적 연구(Med Educ, 2015)
How clinical supervisors develop trust in their trainees: a qualitative study
Karen E Hauer,1 Sandra K Oza,2 Jennifer R Kogan,2 Corrie A Stankiewicz,2 Terese Stenfors-Hayes,3
Olle ten Cate,4 Joanne Batt1 & Patricia S O’Sullivan

도입
INTRODUCTION
의학 훈련의 목표는 학습자들이 [unsupservised practice]에 대비시키는 것이다. 따라서 의료 감독관은 교육생들의 성과를 감독하는 동시에, [독립적으로 활동할 수 있는 기회]를 늘려야 할 책임이 있다. 감독관은 교육생 성과에 대한 일부 측면을 [직접 관찰]하는 한편, [다양한 책임]을 [일정 거리를 두고 감독하면서 교육생에게 맡기는 명시적 또는 암시적 결정을 내린다.1 신뢰는 '미래에 대한 의존'을 수반하며, 개인에게 무언가를 맡기는 것은 '누군가의 보살핌에 책임을 부여하거나 맡기는 것'이다.3
The goal of medical training is to prepare learners for unsupervised practice. Clinical supervisors are therefore charged with overseeing trainees’ performance while also granting them increasing opportunities to perform independently. Whereas supervisors observe some aspects of their trainees’ performance directly, they also explicitly or implicitly make decisions to entrust their trainees with various responsibilities that they supervise at some distance.1 Trust entails ‘dependence on something future’2 and to entrust an individual with something is to ‘assign a responsibility to or put something into someone’s care’.3
의학교육에 관한 연구에서 [교육생에 대한 감독자의 신뢰에 기여하는 요인]을 식별하였다.
- 지식과 기술에서 드러났듯이, [훈련생들의 역량]은 자신의 한계를 인정하고 도움을 구하고자 하는 의지, 자기 효율성 및 양심성 모두 독립적인 연습을 위한 상급자의 신뢰에 영향을 미칩니다.
- [감독관의 자체적인 임상 및 감독 기술과 경험]은 교육자의 개인적 신뢰 성향과 마찬가지로 훈련생의 역량 수준을 식별하는 능력에 영향을 미칩니다.
- [작업 환경의 맥락과 문화]는 작업의 복잡성과 익숙성과 함께 책임의 할당과 완수에 영향을 미칩니다. 작업 부하 및 독립성에 대한 전공의의 요구가 높으면 [상사가 준비가 되었다고 느끼기 전에] 전공의의 독립성을 확보할 수 있다.
- [감독관과 수습생 사이의 관계]는 서로 능력과 스타일을 분별하는 또 하나의 중요한 위탁 판단에 기여한다. 감독관과 연습생은 서로 공감대를 형성하고 서로의 접근 방식과 기대 사항을 학습하면서 역할과 책임을 반복적으로 협상할 수 있습니다.
- [감독관과 수습생 사이의 상호 신뢰 수준]은 연습생의 독립적 실무 준비 상태에 대한 감독관의 평가에 영향을 미칩니다.
Studies in medical education have identified factors that contribute to supervisors’ trust in trainees.4
- Trainees’ competence, as manifested in their knowledge and skills, recognition of their own limitations, willingness to seek help, self-efficacy and conscientiousness all influence their supervisors’ trust in them for independent practice.5–7
- The supervisor’s own clinical and supervisory skills and experience influence his or her ability to identify a trainee’s level of competence,8 as does the supervisor’s personal tendency to trust.
- The context and culture of the work environment, along with task complexity and familiarity, influence the assignment and completion of responsibilities.9 Demanding workloads and residents’ own desire for independence may lead residents to be afforded independence before their supervisors feel they are ready.5,10,11
- The relationship between supervisor and trainee constitutes another important contributor to judgements of entrustment as the two discern one another’s abilities and styles. The supervisor and trainee may negotiate roles and responsibilities iteratively as they develop rapport and learn each other’s approaches and expectations.12
- The degree of mutual trust between supervisor and trainee informs the supervisor’s assessment of the trainee’s readiness for independent practice.6
신뢰는 [점진적으로 더 큰 독립성을 위한 준비]에 대한 판단을 프레임을 형성하고, 따라서 (마일스톤 기반 교육에서 가치롭게 여겨지는) workplace learning에 대한 발달적 접근방식과 일치한다.13,14 그러나 감독자, 연습생 및 사회적 맥락 간의 관계에 대한 맥락적 및 사회문화적 측면의 관련성을 고려한다. 학습이 일어나고, [사회문화적 관점]은 연습생이 사회적 맥락 안에서 상호작용하면서 학습이 어떻게 나타나는지를 설명할 수 있다.15
Trust frames judgements about readiness for progressively greater independence and thus aligns with the developmental approach to learning in the workplace valued in milestone-based education.13,14 However, given the relevance of contextual and socio-cultural aspects of the relationships among the supervisor, trainee and the social context in which learning occurs, a socio-cultural perspective can elucidate how learning emerges as a trainee interacts within a social context.15
신뢰는 [연습생에 대한 태도]와 [그 신뢰에 따라 다르게 수행되는 행동]을 모두 포함한다. Vygotsky의 ZPD는 [학습자의 역량]과 [관리자의 안내로 달성할 수 있는 역량]의 차이를 설명합니다. 이 격차를 목표로 하는 감독은 기술 습득과 숙달을 촉진합니다.
Trust encompasses both an attitude towards a trainee and an action performed differently based on that trust.16 Vygotsky’s17 zone of proximal development describes the gap between learners’ capability and the capability they could achieve with supervisors’ guidance; supervision aimed at this gap promotes skill acquisition and mastery.
연구 및 이론을 통해 교육생에 대한 감독자의 신뢰에 기여하는 요소가 상호 작용하여 신뢰의 발전을 도모하는 방법과 직장 내에서 감독하는 감독자가 신뢰의 의미를 이해하는 방법에 관한 문헌상의 차이를 확인하였습니다.
Informed by research and theory, we identified a gap in the literature relating to how factors that contribute to supervisors’ trust in trainees interact to foster the development of trust and how supervisors understand the meaning of trust as they supervise within the workplace.
방법 METHODS
설계
Design
이것은 다른 개인이 어떤 현상을 어떻게 경험하는지를 조사할 수 있는 현상학적phenomenographic 접근방식을 사용한 정성적 연구이다. 20,21 본 연구에서는 신뢰가 어떻게 발달하고 경험되는지의 차이, 그리고 이러한 차이가 연구의 '결과 공간'을 구성한다.20
This is a qualitative study using a phenomenographic approach, which enables examination of how different individuals experience a phenomenon, which in this study is trust.20,21 The differences in how trust develops and is experienced, and how these may relate to one another, constitute the ‘outcome space’, or findings, of the study.20
현상학은 발견물 간의 상호작용을 높이 평가하며, [신뢰의 발달]은 [사회적 맥락 내에서 여러 요인]에 의해 영향을 받는 것으로 알려져 있다.
Phenomenography appreciates the interactions among findings, and the development of trust is known to be influenced by multiple factors within a social context.
참가자 및 설정
Participants and setting
감독관들은 이메일 초대장을 받았고, 무응답자들은 이메일 알림 메시지를 3개까지 받았다. 참가자들은 15달러짜리 커피 카드를 받았다.
Supervisors received an e-mail invitation to participate; non-respondents received up to three e-mail reminders. Participants received a US$15 coffee card.
데이터 수집
Data collection
참가자들은 2013년 7월부터 2014년 1월까지 7개 항목의 인구통계 조사와 30분 동안의 반구조적 인터뷰를 직접 또는 전화로 완료했습니다. 감독자는 [신뢰의 발전]과 [환자 관리 책임을 가진 전공의를 신뢰하는 것]이 의미하는 바를 설명하였다(부록 S1, 온라인 참조).
Participants completed a seven-item demographic survey and a 30-minute semi-structured interview in person or by telephone between July 2013 and January 2014. Supervisors described the development of trust and what it means to trust a resident with patient care responsibilities (see Appendix S1, available online)
분석
Analysis
연구팀이 새로운 주제(포화도)가 등장하지 않는다고 판단할 때까지 데이터 분석은 데이터 수집과 동시에 수행되었다.22 현상학적 접근방식과 일관되게, 데이터 분석은
- 감독자가 전공의에 대한 신뢰의 의미를 어떻게 개념화하고 신뢰를 발전시켰는지,
- 서로 다른 경험(데이터의 범주 또는 코드에 포착된 대로)이 어떻게 상호 및 정보에 입각한 감독 행동과 관련되는지를 식별하기 위한 것이다.20, 21,23
[신뢰 형성에 기여한다고 기존 연구에서 기술된 요인]들은 새로운 이해의 식별을 제한하지 않고, 질적 데이터 분석의 초기 방향을 알려주는 [sensitising concepts]으로 작용했다.24
Data analysis was carried out concurrently with data collection until the research team determined that no new themes were emerging (saturation).22 Consistent with a phenomenographic approach, data analysis aimed to identify
- how supervisors conceptualised the meaning of trust in their residents and developed trust, and
- how aspects of their different experiences (as captured in categories or codes in the data) related to one another and informed supervision behaviours.20,21,23
Previously described factors that contribute to trust formation served as sensitising concepts, which inform the initial direction of qualitative data analysis without limiting the identification of new understandings.24
1차 조사자는 예비 코드북(정의와 예가 포함된 코드 목록)을 개략적으로 설명한 다음 신뢰의 의미에 대한 인터뷰 질문과 관련된 9개의 추가 대본 부분을 읽고 식별된 테마를 반영하도록 코드북을 다듬었다. 세 명의 조사관(SKO, JRK, JB)이 이 그룹 중에서 각각 5개의 추가 녹취록을 읽고 코드북의 주제를 확인하고 확장했다. 조사자들은 이러한 주제에 대해 토론하고 코드북을 완성했다.
The primary investigator outlined a preliminary codebook (list of codes with definitions and examples), and then read the portions of nine additional transcripts that related to the interview question about the meaning of trust and refined the codebook to reflect identified themes. Three investigators (SKO, JRK, JB) read five additional transcripts each from among this group and confirmed and expanded the themes in the codebook. The investigators discussed these themes and finalised the codebook.
코드들 사이의 관계를 찾기 위해 주요 데이터를 검토함으로써, 저자들은 신뢰 형성의 경험을 기술하는 수치를 만들었다(그림 1).
By examining the primary data to find relationships among the codes, the authors generated a figure describing the experience of trust formation (Fig. 1).
우리는 그 [연구 결과의 신뢰성을 높이기 위한 조치]를 취했다.
- 우리는 학습자에 대한 신뢰를 경험하는 관리자 역할을 하는 임상의와 분석 내내 서로의 가정에 의문을 제기하고 이의를 제기하기 위해 대화에 참여하는 비임상 연구원으로 구성된 팀을 포함함으로써 반사성reflexivity을 고려했다.
- 연구팀은 또한 조사관 삼각 측량 과정을 이용했다. 코딩에 직접 관여하지 않은 조사자들은 주요 발견물을 검토하고 관찰, 의료 교육 및 연구에 대한 전문 지식을 활용하여 발견물을 명확히 하고 비평했다.
- 모델 개발을 위해, 1차 조사자는 그림을 설계한 후 반복적으로 공동 조사자들과 공유했으며, 공동 조사자는 초안 모델을 연구 결과와 비교하고 추가하거나 강조할 영역에 대한 피드백을 제공했다. 이러한 변화에는 신뢰 판단에서의 추론 역할, 감독자의 역할 변화가 다양한 방식으로 나타났다는 사실, 그리고 두 현장의 서로 다른 버전의 일정 비동기화가 신뢰에 영향을 미쳤다는 사실이 포함되었다.
- 1차 조사자는 두 연구 현장의 교수진 감독관에게 대규모 프레젠테이션으로 연구 결과를 제시했고, 연구 결과에 대한 추가 피드백과 비판을 받았고, 최종 원고와 모델에 통합되었다.
We took steps to enhance the trustworthiness of the findings.
- We considered reflexivity26 by including a team of clinicians who serve as supervisors who experience trust in learners, and non-clinician researchers, who together engaged in dialogue to question and challenge one another’s assumptions throughout the analysis.
- The study team also used a process of investigator triangulation.20 The investigators not directly involved in coding reviewed the major findings and used their expertise in supervision, medical education and research to help clarify and critique findings.
- For model development, the primary investigator designed the figure and then iteratively shared it with co-investigators, who compared the draft model with the study results and provided feedback about areas to add or emphasise. These changes included the role of inference in judgements of trust, and the facts that supervisors’ role shift manifested in varying ways, and that different versions of schedule asynchrony at the two sites affected trust.
- The primary investigator presented study results in grand rounds presentations to faculty supervisors at the two study sites and received further feedback and critique of the findings, which were then incorporated into the final manuscript and model.
결과 RESULTS
이 분석에는 43개의 인터뷰가 포함되었다. 인터뷰는 평균 약 27분 동안 진행되었다(범위: 18-44분).
The analysis included 43 interviews. Interviews lasted an average of approximately 27 minutes (range: 18–44 minutes).
신뢰의 의미
Meaning of trust
많은 감독관들은 신뢰의 의미를 [전공의의 역량]과 [팀 리더쉽]에서 보여지는 것으로 설명했다. 감독자는 전공의의 역량을 다음을 통해서 인식한다.
- 팀 내에서 환자 진료를 위한 주요 의사 결정권자로서 전공의가 독립적으로 내리는 임상적 의사 결정
- 환자 및 의료팀 구성원과의 커뮤니케이션
Many supervisors described the meaning of trust as exemplified by awareness of the resident’s competence and team leadership. Supervisors perceived resident competence as demonstrated
- by the resident’s independent making of clinical decisions as the primary decision maker for patient care within the team and
- through his or her communication with patients and health care team members.
팀 리더십은 [전공의의 일상적인 조직과 팀 라운드 및 관리 계획의 실행, 그리고 전문 리더십과 환자 관리의 역할 모델링] 등을 통해 팀 내에서 나타났다. 전공의의 [환자진료 역량]과 [더 많은 주니어 팀 구성원의 감독관 팀 리더십 역량]은 종종 동시에 발생했으며, 회진 행동을 통해 역량을 유추하였다.
Team leadership manifested within the team in the resident’s daily organisation and execution of team rounds and care plans and role modelling of professional leadership and patient care. Resident competence in patient care and team leadership as a supervisor of more junior team members often co-occurred, with competence inferred through rounds behaviours:
[수준 이하의 리더십 기술]을 가진 임상 역량의 관찰은 상사의 신뢰를 떨어뜨렸다. 신뢰의 의미에 대한 또 다른 특성은 감독의사 자신의 관점에서 도출되며, [감독의사가 제공해야 한다고 느끼는 수준의 감독이나 적절한 환자 치료가 이루어지고 있다고 인식했을 때] 느끼는 편안함을 가리킨다.
The observation of clinical competence with substandard leadership skills diminished supervisors’ trust. Another characterisation of the meaning of trust derived from the perspective of self, and referred to either the supervision that supervisors felt obligated to provide or the comfort they felt when they perceived that appropriate patient care was occurring.
감독관은 전공의가 자신의 한계를 인식하고 언제 도움을 청해야 하는지를 알 때 신뢰할 수 있었다.
Supervisors trusted according to residents’ recognition of their own limitations and their knowing when to seek help:
[전공의의 환자 관리에 대한 신뢰]는 인턴과 학생에 대한 전공의의 감독 및 코칭, 팀 회진 관리에 나타난 팀 리더십에서 추론할 수 있습니다.
Trust in a resident’s patient care was inferred from team leadership exhibited in the resident’s supervision and coaching of interns and students, and management of team rounds:
[리더십]은 [조직력, 더 많은 후배 팀원들과의 지식 공유, 긍정적이고 전문적인 기질 발휘]를 포괄했다. 팀 리더십은 위탁해야 할 활동이자 환자의 문제 관리 및 절차 수행과 같은 임상 활동에 대한 전공의의 신뢰성에 대한 'proxy'으로서 정보 제공으로 설명되었다.
Leadership encompassed organisational skills, sharing of knowledge with more junior team members, and the display of a positive, professional disposition. Team leadership was described both as an activity to be entrusted and as informative as a ‘proxy’ about the resident’s trustworthiness for clinical activities such as managing patient problems and performing procedures.
신뢰는 어떻게 발전하는가
How trust develops
감독자들은 시간 경과에 따라 신뢰를 어떻게 발전시켰는지(그림 1; 그림의 항목은 다양한 출발점부터 신뢰 장벽과 가속기에 의해 영향을 받는 감독자 신뢰 형성의 기간, 신뢰 결과의 실현에 이르기까지) 설명했다.
Supervisors described how they experienced trust developing over time (Fig. 1; items from the figure are indicated in italics in the text) from various starting points, through a period of supervisor trust formation influenced by barriers and accelerators to trust, and to the realisation of trust outcomes.

참가자들은 새로운 전공의와 일하기 시작하자마자 신뢰에 대해 생각하는 것에 대해 설명했다. 서로 다른 감독자들은
- (i) 적은 감독/높은 신뢰: '신뢰의 도약leap of faith'으로 묘사된다
- (ii) 높은 감독/낮은 신뢰: '시행착오'로 묘사된다. 높은 감독이 발생하고, 문제가 발생하면 감독이 더 높아짐
- (iii) 신뢰와 지침 측면에서 어디에서 시작해야 할지에 대한 불확실성
...등 세 가지 다른 출발 지점을 표시했다.
Participants described thinking about trust as soon as they started working with a new resident. Different supervisors indicated three different starting points:
- (i) less supervision/more trust, described as a ‘leap of faith’;
- (ii) more supervision/less trust, described as ‘trial and error’ in which high supervision occurred and problems prompted more supervision, and
- (iii) uncertainty about where to start in terms of trust and guidance.
승인된 출발점과 상관없이 감독관은 초기 감독에 유사한 전략을 사용했다. '배후'에서 전공의의 업무를 확인하고 즉시 도울 수 있도록 하는 등의 조치입니다. 전공의를 신뢰한다고 말한 많은 사람들조차, 신뢰의 정당성을 확실히 하기 위해 여전히 전공의 업무를 자주 확인했습니다. '높은 신뢰'의 포지션에서 시작한 어느 감독관은 의도적으로 고가용성high availability을 확보했습니다.
Regardless of the starting point endorsed, supervisors used similar strategies for initial supervision, such as checking the resident’s work ‘behind the scenes’ and making themselves readily available. Many who said they trusted the resident still frequently checked resident work to ensure that trust was justified. One supervisor starting from a position of high trust qualified it with intentionally high availability:
[출발점]은 [매우 불확실한 시기]라는 것을 알게 된 또 다른 사람은 다음과 같이 설명했다.
Another, who found the starting point a time of great uncertainty, explained:
두 명의 감독관은 전공의의 임상적 추론을 조사하기 위해 [전공의와 임상 시나리오를 검토]함으로써 신뢰의 결정을 신속하게 하기 위한 전략을 채택했다. 이는 팀의 환자 또는 가상의 시나리오와 관련된 시나리오일 수 있다. '낮은 신뢰'로 시작한 일부 사람들은 시간이 지남에 따라 신뢰를 더 쌓으면서도, 감독 수준을 줄여나가는 데 어려움을 겪었다.
Two supervisors employed strategies to expedite the determination of trust by reviewing clinical scenarios with the resident in order to probe the resident’s clinical reasoning; these might be scenarios related to patients on the team or hypothetical scenarios. Some with a starting point of low trust had difficulty decreasing their supervision, even when they did develop more trust over time.
전공의에 대한 사전 지식은 종종 이용 가능했지만, 감독자들은 그 유용성에 대해 상반된 견해를 보였다. 전공의에 대한 사전 지식은 전공의의 평판, 다른 감독관들, 프로그램의 감독자 역할을 통해 이용 가능한 정보 , PGY1 또는 외래 환경에서의 전공의와의 이전 작업 등으로부터 파생derived 되었다. 감독관들은 종종 전임 감독관으로부터 전공의에 대한 'signout'을 받았지만, 이 정보는 비특정적인 것으로 인식했다.
Whereas prior knowledge of the resident was often available, supervisors expressed ambivalence about its usefulness. Prior knowledge of a resident derived from the resident’s reputation, other supervisors, information available through the supervisor’s leadership role in the programme, or previous work with the resident as a PGY1 or in the ambulatory setting. Although supervisors often received ‘signout’ about the resident from the prior supervisor, they perceived this information as non-specific:
보통 "그 전공의는 훌륭하고, 인턴도 훌륭하다"입니다. 그러니까, 자세한 디테일은 전혀 없어요(073)
It’s usually “resident is great; interns are wonderful”. So, you know, not a whole lot of detail. (073)
감독자들은 전공의의 성과에 대한 사전 지식을 어떻게 하면 그들의 감독 및 신뢰도 판단에 가장 잘 반영할 수 있는지 물었다. 그들은 그들 자신의 경험에 반하는 전공의에 대한 부정적인 사전 지식과 긍정적인 사전 지식 모두의 예를 설명했다. 따라서 일부 감독관들은 '전공의에 대한 아무런 사전 판단을 하지 않음'으로써 편견을 피하는 것이 최선의 접근법이라고 결론 내렸다.
Supervisors questioned how best to incorporate prior knowledge of resident performance into their supervision and judgements of trustworthiness. They described examples of both negative and positive prior knowledge about the resident that contradicted their own experience. Therefore, some supervisors concluded that the best approach was to avoid bias by ‘giving the resident a clean slate’.
신뢰에 대한 판단은 보통 몇 시간에서 며칠 사이에 빠르게 이루어졌다. 많은 감독관들은 '몇 일', '통화 주기'(4일) 또는 때로는 '1주에서 2주 사이의 마법의 숫자'로 신뢰에 대한 결론을 도출하기에 충분한 인상을 형성한다고 설명했습니다. 일부에서는 이러한 과정이 거주자 주도 라운드를 관찰하고 임상 의사결정에 참여하는 첫날 내에 발생했다고 보고했다.
Judgements about trust usually occurred quickly, within hours to days. Many supervisors described forming impressions that sufficed to draw conclusions about trust within ‘a few days’, ‘a call cycle’ (4 days) or sometimes as long as ‘a magic number somewhere between 1 and 2 weeks’. A few reported that this process occurred within the first day of observing the resident leading rounds, teaching and engaging in clinical decision making.
신뢰 개발을 위한 정보의 출처
Sources of information for trust development
전공의의 환자진료에 대한 신뢰는 표준, 직접 관찰 또는 이해관계자 입력(그림 1)과 비교하여 알 수 있었다.
Trust in a resident’s patient care was informed by comparison with a standard, direct observation or stakeholder input (Fig. 1).
[표준과의 비교]는 여러 가지 방법으로 이루어졌다. [자신과의 비교]가 흔하게 신뢰의 정보원이 되었다. 감독관들은 '거울'과 '내 눈과 귀의 연장'과 같은 용어를 사용하여 [자기 자신이 했음직한 행동]을 기준으로 삼아 전공의의 수행능력을 평가하였다.
Comparison with a standard occurred in several ways. Comparison with self frequently informed trust. Supervisors used terms such as ‘mirror’ and ‘extension of my eyes and ears’ to describe how they appraised residents’ performance based on what they themselves would have done. One explained how trust means that:
일부는 또한 전공의를 과거 전공의 시절 자신의 모습과 비교하였다. 자기자신이 전공의였을 때 무엇을 했을지 추측했다. 이러한 비교는 의사 결정, 환자 평가 및 관리, 커뮤니케이션 영역에서 광범위하고 일반적인 경우가 많았다. 특정 예에는 전공의에 대해서 감독관이 다음을 느낀 것이다.
- 자신이 했을 것보다 더 많은 검사를 지시했거나(027),
- 특정 환자 문제에 대해 유사한 우려를 나타냈거나(034),
- 주치의가 알아차린 것과 동일한 환자 데이터 및 인터벤션을 (074)식별했거나
Some also compared the resident with their past selves, surmising what they would have done when they were residents. These comparisons were often broad and general, across domains of decision making, patient evaluation and management, and communication. Particular examples included the supervisor feeling that a resident
- ordered more tests than he or she would have done (027),
- showed a similar amount of concern about particular patient problems (034), or
- identified the same patient data for discussion and intervention that the attending noticed (074).
일부 감독관들은 전공의들의 행동이 (자신이 했던 행동과) 다른데도 신뢰가 어떻게 생겼는지 설명했다. 이러한 감독자들은 환자 관리의 정확성과 부정확성을 구분하기 위해 노력했다. 한 전문가는 '성격과 스타일, 역량(027)'을 평가하는 것에서 발전하는 과정을 설명했다. 일부 감독관은 동등하게 좋은 대안 접근방식을 나타내는 차이를 인정했고, 일부 전공의는 자신이 했던 것보다 더 나은 결정을 내리는 것을 관찰했다. 일부에서는 [의사결정을 뒷받침하는 근거에 대한 전공의의 설명]이 신뢰를 회복했다고 설명했다.
Some supervisors described how trust occurred even when residents’ behaviours differed fromtheir own. These supervisors sought to distinguish differences that constituted correct versus incorrect patient management. One explained evolving fromassessing ‘what’s their personality and what’s their style, to what’s their competence’ (027). Some acknowledged differences that represented an equally good alternative approach, whereas a few observed residents making better decisions than they would have. Some explained that residents’ explanations of the reasoning supporting differing decisions restored trust:
감독자들은 또한 [규범적인 접근법]을 사용하여 신뢰를 일반적으로 결정했다. 전공의의 교육 수준, 소속 기관, 교육 시점에 따른 관리자의 개인적 기대치를 기준으로 비교하는 것이다.
Supervisors also commonly determined trust using a normative approach. The comparison standard for a resident’s performance was the supervisor’s personal expectation based on the resident’s training level, institution, or time of year:
임상 치료 및 팀 리더쉽을 [직접 관찰]한 결과 신뢰에 대한 판단도 알 수 있었다. 직접 관찰에 대한 참가자의 예제는 보통 [팀 라운드]의 이벤트를 다룬다. 감독관은 팀 구성원이나 환자에게 올바른 질문을 하고, 의사 결정을 내리고, 적절한 관리 계획을 수립하는 데 있어 전공의가 신뢰할 수 있는 능력을 보여주는 것을 강조했습니다.
Direct observation of clinical care and team leadership also informed judgements of trust. Participants’ examples of direct observation usually addressed events on team rounds. Supervisors highlighted a resident’s skills in asking the right questions of team members or patients, making decisions, and generating appropriate management plans as indications that the resident could be trusted:
[이해관계자의 의견stakeholder input]은 (전공의에 대한) 다른 팀원들의 의견을 포함하며, 신뢰성에 대한 흔하게 언급되지 않은 정보의 원천이었다. 몇몇 감독관은 PGY1이나 학생들로부터 전공의의 리더십에 대한 피드백을 듣거나, 양질의 환자 진료를 제공하는 인턴을 관찰함으로써, 전공의에 대한 신뢰를 추정infer했다. 몇몇 감독관들은 환자들이 고품질의 안전한 치료를 받았다는 관찰을 바탕으로 신뢰를 판단했다. 이러한 설명은 특정 기준을 참조하지 않았다. 자신의 관리에 대한 인식에 대한 직접적인 환자 의견에서 도출되는 경우는 드물지만, 환자가 적절한 치료를 받았거나 자신의 관리에 만족한다는 유추를 통해 도출된다.
Stakeholder input, which included input from other team members, was an uncommonly mentioned source of information about trustworthiness. A few supervisors mentioned hearing feedback from the PGY1s or students about the residents’ leadership, or observing the interns providing quality patient care, and inferring the resident’s trustworthiness. A few supervisors defined trust based on the observation that patients had received high quality, safe care. These descriptions did not refer to specific criteria. They rarely derived from direct patient comments about their perceptions of their care, but rather through inferring that patients were treated appropriately or were satisfied with their care.
신뢰 형성을 가로막는 장애물과 가속기
Barriers to and accelerators for trust formation
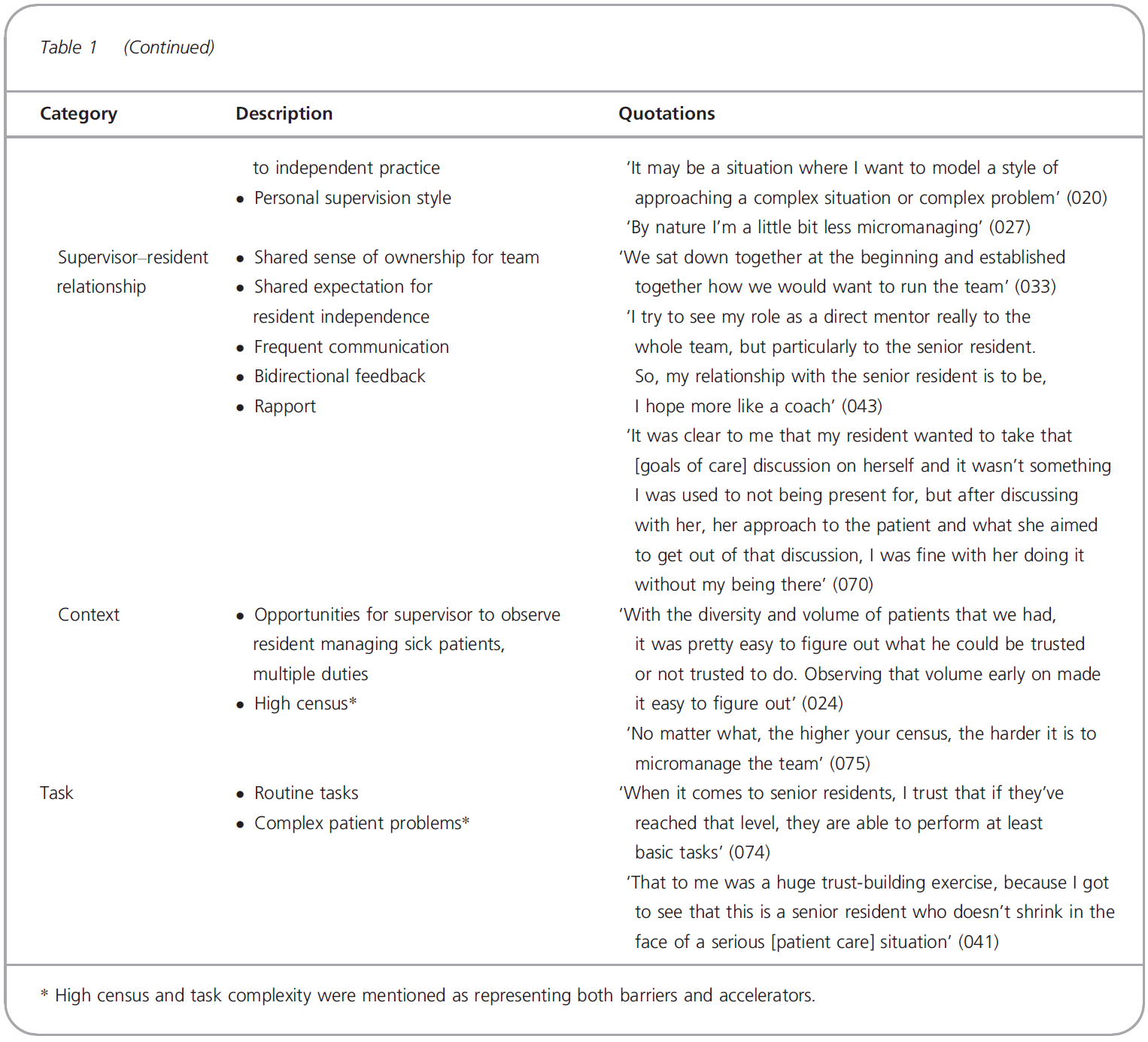
표 1에 나타낸 것과 같이 전공의, 감독자, 전공의-감독자 관계, 맥락 및 과제와 관련된 신뢰의 발전에 대한 장벽과 가속기. 신뢰의 장벽은 다음과 같은 것들이 있었다.
- 'red flags'라고 볼 수 있는 전공의의 성향과 전문직업성에 대한 우려
- 다른 팀 구성원, 과제 및 업무량, 일정이 잘 맞지 않는 것과 같은 상황적 어려움
- 감독관 자기자신이 덜 신뢰는 스타일이면서, 전공의 업무를 더 많이 확인하는 스타일인 것
Barriers and accelerators to the development of trust related to the resident, the supervisor, the resident– supervisor relationship, the context and the task, as shown in Table 1. Barriers included
- concerns about the residents’ disposition and professionalism that could raise ‘red flags’,
- contextual challenges related to other team members, tasks and workload, and schedule asynchrony, and
- a supervisor’s style in terms of his or her propensity to trust less and check resident work more.
신뢰를 잘못 두었던 경험 후에 신뢰의 장벽이 생기기도 하였다. 이러한 사례는 참가자 사이에서 드물었고, 예제는 전반적으로 우수한 의사결정을 입증한 전공의를 대상으로 하는 경향이 있었지만, 특히 복잡한 환자를 마주했을 때 상황을 적절히 관리하는 방법을 알지 못하는 것으로 입증되었고 신속하게 도움을 구하지 못했다. 신뢰를 잘못 둔misplacement 다른 예는, 전공의가 [직접적인 감독에서 벗어나 교육 수준을 초과하는 것으로 간주되는 절차를 수행]하거나 [보증된 역량보다 더 자신 있어 보였을 때] 발생했다.
Barriers to trust also arose after experiences of misplacing trust. These were uncommon among our participants and examples tended to address residents who demonstrated generally good decision making, but, when faced with a particularly complex patient, proved not to know how to manage the situation appropriately and failed to seek help promptly. Other examples of the misplacement of trust arose when residents appeared more confident than their competence warranted or undertook a procedure considered to be above their training level while away from direct supervision.
한 주치의는 후자의 설명을 'ICU[중환자실]의 주치의조차도 카우보이 같은 태도에 충격을 받았다.'(042)고 했다.
- (열정과 그에 걸맞는 자신감으로 보여지는) 전공의의 참여
- 적절한 태스크 복잡성,
- 전공의의 역량 수준에서 도전적인 업무량 및 관리 기회
- 상사의 신뢰 의지
...등이 모두 신뢰를 높였습니다
One attending physician explained the latter as: ‘Even the ICU [intensive care unit] attending was shocked at this cowboy kind of attitude’ (042).
- Resident engagement as demonstrated by enthusiasm and befitting confidence,
- appropriate task complexity,
- workload and management opportunities that were challenging for the resident’s competence, and
- the supervisor’s willingness to trust
...all enhanced trust.
[감독자와 전공의의 빈번한 의사소통]과 [역할 및 상호작용에 대한 기대치 공유]는 신뢰를 조성하는 감독자와 전공의 관계를 특징지었다. 감독관이 경험이 더 많고, 신뢰하려는 의지가 높을수록 전공의가 특히 아픈particularly sick 환자를 관리하는 것을 관찰할 수 있는 기회와 결합되어 신뢰 또한 형성되었다.
Frequent supervisor–resident communication and shared expectations of roles and interactions characterised supervisor–resident relationships that fostered trust. Greater supervisor experience and willingness to trust, coupled with opportunities for observing the resident manage particularly sick patients, also engendered trust.
신뢰의 결과
Outcomes of trust
[감독관 역할의 변화]는 감독관 자신의 역할과 행동에 변화를 수반한다. 감독관은 전공의 업무를 확인하는 데 소요된 시간을 기준으로 신뢰의 의미를 공통적으로 설명했다.
Supervisor role shift entailed changes in supervisors’ own roles and behaviours. Supervisors commonly characterised the meaning of trust based on how much time they spent checking resident work:
그러한 결과 중 하나는 일차적으로 임상 치료를 제공하는 것에서 PGY1과 학생을 가르치는 것 또는 전공의의 컨설턴트로 근무하는 것에 이르기까지 개인적인 변화와 관련이 있었다. 또 다른 신뢰의 결과는 감독관 역할에 대한 감독관의 태도 변화로서, 감독관의 불안감 감소, 편안함 및 야간 수면 능력 향상을 반영했다. 한 감독관은 '...제가 밤에 얼마나 쉽게 잤는지'(081)에 대해 언급했다.
One such outcome concerned a personal change fromprimarily providing clinical care to teaching PGY1s and students or serving as a consultant to the resident. Another outcome of trust was a change in supervisors’ attitudes towards their supervisory roles, reflected in their experiencing less anxiety, feeling more relaxed and a greater ability to sleep at night; one supervisor remarked on ‘...just how easy I slept at night’ (081).
감독자들은 [전공의에 대한 신뢰]가 전공의가 환자진료 제공에 보다 독립적으로 참여할 수 있게 한다고 인식했다. 감독관이 전공의 업무의 많은 부분을 확인하는 것에서 벗어나자, 전공의는 향상된 독립성에 감사하는 듯 했다.
Supervisors perceived that their trust in the resident enabled the resident to participate more independently in the provision of patient care. As a supervisor moved away from checking as many aspects of the resident’s work, the resident seemed to appreciate increased independence:
감독관들은 신뢰 형성의 결과로 [팀 기능]과 [팀 역학]의 변화를 강조했습니다. 모든 팀 구성원 간의 공감대 형성 및 관계 형성은 서로 함께 즐거워하고 웃는 것으로 나타나며, 감독관 관계가 성공했음을 보여주었고, 감독관은 코치 또는 멘토 역할을 담당했습니다. 이러한 유형의 성공은 '암묵적' 또는 '명백한'으로 묘사되었다.
Supervisors highlighted changes in teamfunctioning and teamdynamics as an outcome of trust formation. Rapport and relationship building among all team members, as manifested by enjoyment of one another’s company and laughter, showed that a supervisory relationship was successful, with the supervisor serving in a coach or mentor role. This type of success was described as ‘implicit’ or ‘obvious’.

고찰
DISCUSSION
우리의 연구결과는 감독자들이 어떻게 임상실무에 대한 전공의의 신뢰도를 판단하고, 신뢰를 바탕으로 감독을 제정하고, 이러한 신뢰의 후속 결과를 경험하는지를 설명한다. 신뢰는 종종 전공의 개개인에 대한 사전 지식으로 알 수 없는 출발점에서부터 발전한다. 대신, [일반 성과 표준에 대한 상사의 이해]와 [리더십 및 임상 관리에 대한 상사의 관찰]에 의해 신뢰가 형성될 수 있다.
Our findings describe how supervisors judge a resident’s trustworthiness for clinical practice, enact supervision based on trust, and experience the subsequent outcomes of this trust. Trust develops from a starting point often uninformed by prior knowledge of the individual resident. Instead, trust formation can be informed by supervisors’ understanding of general performance standards and their observations of leadership and clinical care.
현상학을 사용하여 집중적인 작업 관계에서 신뢰의 발달에 대한 참가자들의 다양한 관점을 특성화하고(그림 1), 신뢰에 대한 [초기 접근방식의 범위]와 [여러 기여 인자의 중요성]을 인식할 수 있었습니다.
The use of phenomenography enabled us to characterise different perspectives among participants regarding the development of trust during intensive working relationships (Fig. 1), and to appreciate the range of initial approaches to trust and importance of different contributing factors.
신뢰의 핵심은 [감독자-훈련자 관계]이며, 이는 신뢰에 기여하는 덜 자주 기술되는 요소이다. 이는 업무 관계와 지속적인 의사소통에 대한 공유된 기대치에 의해 강화될 수 있다. 인간관계는 [두 개인 간의 유사성으로 육성될 수 있는 대인관계 역학]과 더불어, [그들 사이의 접촉의 양] 포함한다.4 관계는 관리자가 각 학습자의 감독 요구에 맞춰 자신의 감독을 조정할 수 있는 능력을 강화합니다.27 예를 들어, 강한 관계를 통해 교육생은 도움을 구하고 피드백을 받고 변경 사항을 적용하는 데 있어 보다 편안함을 느낄 수 있습니다.28
At the core of trust is the supervisor–trainee relationship, a less frequently described factor contributing to trust, that is enhanced by shared expectations of the working relationship and ongoing communication. Relationship encompasses an interpersonal dynamic that can be fostered with similarity between two individuals, as well as the amount of contact between them.4 A relationship enhances the supervisor’s ability to adjust his or her supervision to each learner’s supervision needs.27 For example, with a strong relationship, the trainee can feel more comfortable in seeking help, receiving feedback and incorporating changes.28
우리의 연구 결과는 신뢰의 발전이 시작점에서 결과까지 진행되는 과정으로 어떻게 이해될 수 있는지를 보여준다. 단, 시작점, 영향 요소 및 결과는 감독관마다 다르다. 아마도 놀랍게도, 감독관들은 그들이 기존에 가지고 있었거나, 전공의에 대해 받은 매우 일반적인 사전 정보의 가치에 대해 상반된 의견을 피력했다. 일부 감독관은 전공의 교육 수준에 따라 신뢰를 쌓았지만, 다른 감독관은 몇 시간에서 며칠 사이에 신속하게 신뢰를 결정했다. [인상 형성impression formation]에 관한 연구는 신뢰는 초기 상호작용에 의해 영향을 받을 수 있으며 이러한 맥락에서 감독자들은 훈련생들을 넓은 그룹으로 분류하는 것을 목표로 할 것임을 시사한다. 입원 팀에 대한 빈번한 로테이션과 짧은 관계로 인해 감독자와 전공의는 [빠른 적응을 촉진하는 상호작용 스타일]을 가치 있게 생각하고 기대할 수 있다.
Our findings illustrate how the development of trust can be understood as a process that progresses from a starting point through to outcomes, although starting points, influencing factors and outcomes vary among supervisors. Perhaps surprisingly, supervisors expressed ambivalence about the value of the often very general prior information they held or received about residents. Although some supervisors based their trust on the resident’s training level, others made a determination of trust rapidly within a period of hours to days. Work on impression formation suggests that trust may be influenced by early interactions and that in this context supervisors will aimto categorise trainees into broad groups.30 The current context of frequent rotations and brief relationships on in-patient teams may lead supervisor and resident to value and expect interactional styles that encourage rapid acclimation.31
마찬가지로, ['신속한 신뢰']는 팀이 시간적 압박 환경 내에서 공유된 목표와 명확히 정의된 역할에 기초하여 신속하게 신뢰를 개발하는 방법을 정의한다.32 의료팀 내에서 발생하는 것과 같이 고부담 상황에서 신속하게 협력해야 하는 상황은 [신속한 신뢰의 필요성]을 촉발한다. 이러한 맥락은 신뢰의 형성이 [장기적인 관계]와는 어떻게 다를 수 있는지에 대한 의문을 제기한다. Levin 등은 신뢰는 시간이 누적되면 [개인적 유사성이나 일반적인 행동 기대]보다는 [공유된 관점에 대한 지식]에 기초하게 된다고 설명한다.
Similarly, ‘swift trust’ defines the ways that teams rapidly develop trust based on shared goals and clearly defined roles within a timepressured environment.32 Situations that require teams to start working together quickly in high-stakes contexts, such as occur within medical teams, prompt the need for swift trust. This context raises the question of how the formation of trust might differ in longer-term relationships. Levin et al. describe how, with time, trust is based less on personal similarity or common behavioural expectations and more on knowledge of shared perspectives.33
우리의 참가자들은 신뢰를 발전시키는 과정을 복잡하고 때로 모호하다고 묘사했다. 감독자는 주변 지도부 또는 기타 소스에서 수집한 정보를 사용하여 환자 치료 활동에 대한 신뢰를 추정했다. 다른 이들은 유사한 방식으로 [특정 행동을 충분히 직접 관찰하지 않을 때] 대리 정보가 신뢰의 발전에 어떻게 정보를 제공할 수 있는지를 설명했다. 7,34 우리의 감독자들은 또한 종종 광범위한 일반 용어를 사용하여 전공의의 성과를 고려했다. 긴즈버그 외 연구진도 마찬가지로 감독관들이 국가 프레임워크에 정의된 여러 역량과 맞지 않는 '메타 역량'을 사용하여 연습생의 성과를 어떻게 설명했는지에 주목한다.35
Our participants described the process of developing trust as complex and sometimes nebulous. Supervisors inferred trust for patient care activities using information gleaned fromrounds leadership or other sources. Others have similarly described how proxy information can inform the development of trust in the absence of sufficient direct observation of specific behaviours.7,34 Our supervisors also often considered resident performance using broad, general terms. Ginsburg et al. similarly note how supervisors described a trainee’s performance using ‘meta-competencies’ that did not align with the multiple competencies defined in a national framework.35
우리의 참가자들은 전공의의 성과를 평가할 때 환자 치료 결과의 일반적인 평가를 사용했지만, 그들이 사용한 메트릭스 또는 그들이 기대한 특정 성과에 대해서는 그다지 상세하게 설명하지 않았다. 이러한 상황은 아마도 방어나 부정직과 같은 red flag 행동을 하지 않는 것 외에, [상사의 신뢰를 얻는 행동]을 개발하거나 입증하기 위해 어떤 조치를 취해야 할지에 대해 전공의들을 불확실하게 만들 수 있다.
Our participants used general assessments of patient care outcomes in assessing resident performance, but did not describe in much detail the metrics they used or the particular outcomes they expected. This situation may leave residents uncertain about what steps to take to develop or demonstrate behaviours that earn supervisors’ trust, other than perhaps avoiding red flag behaviours such as defensiveness or dishonesty.
장벽과 가속요인의 상호작용이 신뢰 형성의 진화에 영향을 미쳤다(표 1). 일반적으로 팀원들이 지속적으로 비동기적으로 로테이션하는 복잡한 시스템으로 구성된 임상 환경과 관련된 당사 참가자들에게 장벽이 있다고 언급됩니다. 이 연구를 위한 이론적 프레임워크로 돌아가면, 이러한 장벽은 학습이 발생하는 사회적 맥락이 어떻게 전공의의 참여를 가능하게 하거나 방해할 수 있는지, 그리고 결과적으로 신뢰를 얻을 수 있는 기회를 보여준다.
The interaction of barriers and accelerators influenced the evolution of trust formation (Table 1). Commonly cited barriers for our participants related to the clinical environment, which comprises a complex system in which team members continually and asynchronously rotate. Returning to the theoretical frameworks for this study, these barriers show how the social context in which learning occurs can enable or impede residents’ participation, and consequently their opportunities to earn trust.
실천 커뮤니티에 대한 Wenger의 연구는 전공의가 지엽적인 참여 위치에서 환자 치료의 보다 중심적인 역할로 이동해야 한다는 것을 시사한다. 즉, 환자 관리의 제공에 있어 관리자의 역할이 중심적인 역할에서 오히려 지원적인 역할로 바뀔 수 있는 상황이다. 반대로, 다른 이들은 전공의들이 [보다 정교한 coverage schedule의 요즘 시대]에 팀장이나 관리자의 역할을 할 수 있다고 보고했다.
Wenger’s work on communities of practice37 suggests that residents should move from a position of peripheral participation to a more central role in patient care, a situation that would shift the supervisor’s role from one that is central to the provision of patient care to one that is, rather, supportive. Conversely, others have reported that residents may increasingly play the role of team leader, or manager, in the current era of more elaborate coverage schedules.38
일단 신뢰가 쌓이면, 우리의 모델은 그 신뢰의 결과를 나타낸다. 신뢰 형성은 환자관리에 대한 전공의의 참여를 전체 팀에게 유리하게 향상시킴에 따라 관리자의 역할을 변화시킨다(그림 1). 전공의에 대한 신뢰의 판단은 감독자가 자기자신의 역할을 보는 관점을 보호자가 아닌, [컨설턴트 및 교사]로서 바꾸게끔 영향을 미친다. 이러한 변화의 중요성은 직장에서 학습을 촉진하는 사람으로서 임상 교사의 역할을 강조하는 문헌에 의해 뒷받침된다.39 신뢰를 획득한 전공의들은 돌봄제공자 및 팀 리더로서 감독이 더 적은 상태에서도 기능할 수 있는 것으로 설명되었다.
Once trust is established, our model indicates the consequences of that trust. Trust formation shifts supervisors’ roles as it elevates residents’ participation in care, to the benefit of the entire team (Fig. 1). A judgement of trust in the resident influences the supervisor’s view of his or her own role as a consultant and teacher, rather than as a care provider. The importance of this shift is supported by literature emphasising the role of a clinical teacher as a facilitator of learning in the workplace.39 Residents in our study who earned trust were described as able to function with less supervision as care providers and team leaders.
우리의 연구 결과는 학습자 평가 및 커리큘럼 설계에 영향을 미칩니다. 신뢰는 팀 업무의 핵심 요소이기 때문에, 상사는 신뢰를 조기에 평가할 수 있을 때 이득을 얻는다.
- 위임 기반 평가 척도 및 EPA을 사용하여 신뢰의 개발을 표준화할 수 있다.41,42
- 연습생 성과에 대한 다양한 측면의 관찰, 해석 및 문서화를 구조화하기 위한 메커니즘은 감독자 간에 전공의 성과에 대한 유용한 의사소통 시스템을 가능하게 할 수 있다.
- 표준 기준 프레임을 정의하고, 의미 있고 이해할 수 있는 평가 척도를 구성하고, 교육생들의 기술과 환자 치료 결과에 대한 감독관의 동시적concurrent 평가를 가능하게 하는 것 또한 신뢰를 바탕으로 평가를 강화할 것이다.44
Our findings have implications for learner assessment and curriculumdesign. As trust is a key component of teamfunctioning, supervisors benefit when trust can be assessed early.
- The development of trust could be standardised using trust-based ratings scales and entrustable professional activities.41,42
- Mechanisms to structure the observation, interpretation and documentation of varied aspects of trainee performance might enable a systemof useful communication about resident performance fromone supervisor to the next.
- Defining a standard frame of reference,43 constructing meaningful and understandable rating scales, and enabling supervisors’ concurrent assessment of trainees’ skills and patient care outcomes would also enhance assessment based on trust.44
신뢰의 복잡성과 역동적으로 진화하는 특성을 고려할 때, 평가 척도의 사용은 교육생의 임상 관리에 대한 교수진의 관찰, 계산된 위험 및 미래 지향적 판단으로서의 신뢰의 성격에 대한 평가 훈련 및 기준 훈련과 결합되어야 한다. 우리의 연구 결과는 또한 신뢰는 전공의에게 [지식과 능력의 leading edge에서 학습 요구에 맞는 기회]를 제공하는 커리큘럼 구조와 감독 설계에 정보를 제공할 수 있다는 것을 보여준다. ZPD과 일관되게, [학습자가 혼자 할 수 있는 것]과 [가이드를 받아 할 수 있는 것] 사이의 영역 내 학습 활동을 목표로 하는 프로그램은 학습과 개발을 극대화할 수 있다.
Given the complexity and dynamically evolving nature of trust, the use of rating scales would need to be combined with faculty members’ observations of trainees’ clinical care, rater training about the nature of trust as a calculated risk and forward-looking judgement, and frame of reference training.43 Our findings also show that trust can informthe design of curricular structures and supervision that provide residents with opportunities aligned with their learning needs at the leading edge of their knowledge and abilities. Consistent with the zone of proximal development, targeting learning activities within the zone between what a resident learner can do alone and what he or she can do with guidance enables a programme to maximise learning and development.17
4 Hauer KE, ten Cate O, Boscardin C, Irby DM, Iobst W, O’Sullivan PS. Understanding trust as an essential element of trainee supervision and learning in the workplace. Adv Health Sci Educ Theory Pract 2014;19 (3):435–56.
SUPPORTING INFORMATION
Appendix S1. Trust Study Interview Guide.
| Appendix S1 Trust Study Interview Guide Introduction: Thank you for participating in this interview. We appreciate your time and willingness to share your thoughts and experiences. Our goal is to understand, from your perspective as an attending, how you interact with and supervise a senior resident. The purpose of this study is to understand the process of supervision, not to gather any information about specific residents. Please do not use any team members or patient names or identifying information. I would like to record this interview and have it transcribed. Your name and any identifying information will be removed from the transcript and will not be used during the analysis. Is it okay with you if I record the interview? TURN ON RECORDER This is an interview with (interviewer) with Dr. (study ID). Today is (date). We know that attendings are making decisions about when to trust their resident to act independently and when to supervise more closely. We are interested in learning about attendings’ decisions about when to give residents more or less independence. Please focus your answers on your experience with your current senior resident (not the intern). 1. What does it mean to you to trust a resident with patient care responsibilities? (Probe as needed) · How do you know that? · How do you decide when you are comfortable letting the resident work independently? · Can you say more about that? ... |
Med Educ. 2015 Aug;49(8):783-95.
doi: 10.1111/medu.12745.
How clinical supervisors develop trust in their trainees: a qualitative study
Karen E Hauer 1, Sandra K Oza 2, Jennifer R Kogan 2, Corrie A Stankiewicz 2, Terese Stenfors-Hayes 3, Olle Ten Cate 4, Joanne Batt 1, Patricia S O'Sullivan 1
Affiliations expand
- PMID: 26152490
- DOI: 10.1111/medu.12745Abstract
- Context: Clinical supervisors oversee trainees' performance while granting them increasing opportunities to work independently. Although the factors contributing to supervisors' trust in their trainees to conduct clinical work have been identified, how the development of trust is shaped by these factors remains less clear.Methods: Internal medicine in-patient supervisors at two institutions were interviewed about the meaning and experience of developing trust in resident trainees. Transcribed data were coded and analysed using a phenomenographic approach.Conclusions: From a general starting point, supervisors develop trust in residents informed by observation, inference and information gathered from the team and patients. Judgements of trust yield outcomes defined by supervisors' changing roles, the increasingly independent provision of care by residents, and team functioning. The implications of these findings for graded resident autonomy aligned with learning needs can inform the design of training environments to enable readiness for unsupervised practice.
- Results: Forty-three supervisors participated. Supervisors characterised the meaning of trust from the perspectives of trainee competence and leadership or from their own perspective of needing to provide more or less supervision. Supervisors initially considered trust to be usually independent of prior knowledge of the resident, and then used sources of information about trust to develop their judgements of trust. Sources, which incorporated inference, included supervisors' comparisons with a standard, direct observation of the trainee as a team leader or care provider, and stakeholder input from team members, patients and families. Barriers against and accelerators to trust formation related to the resident, supervisor, resident-supervisor relationship, context and task. Trust formation had implications for supervisors' roles, residents' increasingly independent provision of care, and team functioning.
- Objectives: This study was designed to determine how supervisors develop and experience trust in resident (postgraduate years 2 and 3) trainees in the clinical workplace.
- © 2015 John Wiley & Sons Ltd.
'Articles (Medical Education) > 임상교육(Clerkship & Residency)' 카테고리의 다른 글
| ISBAR를 활용한 환자인계 가르치기(BMC Med Educ, 2020) (0) | 2021.07.13 |
|---|---|
| 양질의 의료 유도하기: EPA, 역량, 마일스톤의 적용을 통한 수련생 평가와 지도감독의 정렬(Acad Med, 2016) (0) | 2021.07.13 |
| 위임결정내리기: 밀러의 피라미드 확장(Acad Med, 2021) (0) | 2021.07.13 |
| 교육과 보건을 변혁할 의과대학생을 위한 밸류-추가 임상시스템 학습 역할: 의과대학과 보건시스템 사이의 파트너십 빌딩을 위한 가이드(Acad Med, 2017) (0) | 2021.05.31 |
| 적응적 전문성(When I say...) (Med Educ, 2017) (0) | 2021.05.21 |