정서적 학습과 정체성 발달: 대만과 네덜란드 의대생의 문화간 질적 비교 연구(Acad Med, 2017)
Emotional Learning and Identity Development in Medicine: A Cross-Cultural Qualitative Study Comparing Taiwanese and Dutch Medical Undergraduates
Esther Helmich, MD, PhD, Huei-Ming Yeh, MD, MPH, Chi-Chuan Yeh, MD, MEd, Joy de Vries, MSc,
Daniel Fu-Chang Tsai, MD, PhD, and Tim Dornan, MD, PhD

의사가 된다는 것은 새로운 직업적 정체성을 개발하는 것, 즉 의사로서 생각하고 행동하고 느끼는 법을 배우는 것을 의미합니다.1 직업적 정체성 형성이 의학교육의 궁극적 목표라는 인식이 증가하고 있지만,1 현재 이 과정에 대한 이해는 제한적입니다. 정체성 개발은 전문직업성 과실이 발생했을 때만 문제가 될 수 있습니다. 이러한 전문직업성 과실의 여파로, 학생들의 행동은 전문직 정체성에 기여하는 문화적으로 결정된 규범, 가치, 감정을 고려하지 않고 판단될 수 있습니다. 최근에 설명한 사례 중 하나는 네덜란드 의료 환경에서 시리아에서 수련받은 의사가 환자와의 공동 의사 결정에 적절히 참여하지 않은 경우입니다.2 의료 수련의의 정서적 경험과 특정 사회문화적 환경 내에서 이러한 경험과 정체성 발달 간의 상호 관련성을 더 잘 이해하면 멘토링이 보다 맞춤화되고 문화적으로 민감해져 특정 맥락에서 적절할 수도 있고 그렇지 않을 수도 있는 기본 가치를 구체적으로 다룰 수 있게 됩니다.3 또한 의료 전문가 정체성 형성의 문화 간 차이에 대한 더 많은 지식은 다른 국가와 문화에서 수련받은 의대생과 전문가에 대한 상호 이해를 개선하고, 세계화 시대에 이주하는 의사를 위한 재인증 절차에 정보를 제공할 수 있습니다.2
Becoming a doctor means developing a new professional identity, or learning to think, act, and feel as a physician.1 Despite increasing recognition that professional identity formation is the ultimate goal of medical education,1 current understanding of this process is limited. Identity development may only become an issue when professionalism lapses arise. In the aftermath of such lapses, students’ behavior may be judged without taking into account the culturally determined norms, values, and emotions that contribute to professional identity. One such example, which we recently described,2 is the case of Syrian-trained physicians not adequately engaging in shared decision making with patients in the Dutch health care context.2 A better understanding of medical trainees’ emotional experiences and the interrelatedness between these experiences and identity development within specific sociocultural environments would allow mentoring to be more tailored and culturally sensitive, specifically addressing underlying values that may or may not be appropriate in a specific context.3 Moreover, more knowledge about cross-cultural differences in medical professional identity formation could improve mutual understanding of medical students and professionals trained in different countries and cultures, and may inform recertification procedures for migrating physicians in a globalizing world.2
정체성 형성에 영향을 미치는 가치와 감정을 탐구하기 위해, 우리는 근본적인 핵심 가치를 탐구함으로써 정체성 이론과 사회적 정체성 이론을 통합한 Hitlin4 이 제안한 개인 정체성 개념을 사용합니다. 이러한 핵심 가치는 개인적, 사회적, 문화적으로 동시에 강렬한 영향을 받습니다.4 무엇이 좋은 행동인지에 대한 핵심 가치와 개념은 도덕적 자아의 기초가 됩니다.4 따라서 개인적 또는 도덕적 정체성은 개인의 핵심이며, 따라서 매우 감정적일 수 있습니다. 첫 임상 경험을 하는 의대 1학년 학생을 대상으로 한 이전 경험적 연구에서 우리는 이미 정체성 발달과 감정 간의 상호작용을 탐구한 바 있습니다.5
To explore the values and emotions that influence identity formation, we use the notion of personal identity as proposed by Hitlin,4 who brings together identity theory and social identity theory by exploring underlying core values. These core values are simultaneously intensely personal and socially and culturally influenced.4 Core values and conceptions of what is good behavior serve as a basis for the moral self.4 Thus, personal or moral identities are core to a person, and, therefore, can be highly emotional. In previous empirical work studying first-year medical students in their first clinical experiences, we have already explored this interplay between identity development and emotions.5
본 연구의 목적은 유럽과 아시아의 문화적 맥락에서 의과대학에서의 정서적 경험과 정체성 발달을 탐구하는 것이었습니다. 우리는 서양과 동양 문화의 도덕적, 사회적 힘이 의대생의 감정과 정체성 발달에 중요한 다른 방식으로 영향을 미친다고 제안했습니다.
- 유대-기독교 전통에서 발전한 서구 생명윤리의 핵심 개념은 개인의 자율성입니다.6
- 유교 사상에 기반한 동양 문화는 사회적 관계를 중시합니다.7,8
우리는 감정, 규범 및 가치의 경험과 표현에 있어 문화적 차이가 학생들이 의사가 되는 동안 다양하고 변화하는 정체성을 구성하는 방식에 영향을 미친다는 것을 발견할 수 있을 것으로 예상했습니다.
The aim of the current study was to explore emotional experiences and identity development in medical school in European and Asian cultural contexts. We proposed that moral and social forces in Western and Eastern cultures affect medical students’ emotions and identity development in importantly different ways.
- A central notion within Western bioethics, as developed in Judeo-Christian traditions, is autonomy of the individual.6
- Eastern cultures, which are built on Confucian thought, place a strong emphasis on social relationships.7,8
We expected to find that cultural differences in the experience and expression of emotions, norms, and values affect how students construct their different and shifting identities while becoming a doctor.
방법
Method
윤리적 고려 사항
Ethical considerations
이 연구의 네덜란드 부분에 대해서는 네덜란드 의학교육협회의 윤리위원회에서 윤리적 검토를 받았습니다. 대만에서는 국립대만대학병원 윤리위원회로부터 윤리적 승인을 받았습니다.
For the Dutch part of this study, ethical review was granted by the ethical board of the Dutch Association for Medical Education. In Taiwan, ethical approval was obtained from the ethical committee of National Taiwan University Hospital.
연구 패러다임
Study paradigm
이 연구의 주요 프레임워크는 사회문화적 프레임워크이며, 이는 정서적 경험을 사회적 실천에 내재된 것으로 개념화한다는 것을 의미합니다. 의학 학습은 임상 환경에서 사회적 행위자(환자, 간호사, 의사, 기타 학생 및 의료진), 인공물(준비물, 기구, 전자 환자 파일), 기호(언어)와의 상호작용을 통해 이루어지며, 이러한 사회적 관행은 역사적으로 형성됩니다.9,10 이러한 사회문화적 환경 속에서 학생들은 감정을 경험하고, 감정을 전달하고, 의미를 부여하는 방법을 배우게 됩니다. 감정은 개별적으로 느끼고 해석하지만, 의대생은 고유한 규범과 가치를 지닌 특정 의료 상황과 문화적 환경 내에서 어떤 감정을 경험하고 표현해야 하는지, 어느 정도까지 표현해야 하는지를 배우는 사회화된 사람입니다. 가치는 특정 상황과 관련이 있고 행동과 사건의 선택 또는 평가를 안내하기 때문에,4 이전 연구에서와 마찬가지로,5 학생들에게 감정적이라고 인식한 특정 경험에 대해 서술하고 반성하도록 요청했습니다.
The main framework for this study is a sociocultural one, meaning that we conceptualize emotional experience as embedded in social practice. Learning medicine takes place in clinical settings during interaction with social agents (patients, nurses, doctors, and other students and health workers), artifacts (arrangements, instruments, electronic patient files), and symbols (language) over time; that is, these social practices are historically shaped.9,10 It is within these sociocultural environments that students experience emotions, learn to communicate them, and give meaning to them. While emotions are individually felt and interpreted, medical students are socialized persons who learn which emotions should be experienced and expressed, and to what extent, within specific medical contexts and cultural environments that have distinct norms and values. Because values pertain to specific situations and guide selection or evaluation of behavior and events,4 as in our previous study,5 we asked students to narrate and reflect on specific experiences that they perceived as being emotional.
참가자
Participants
현재 대만의 7년제 고등 의학 교육 프로그램에서는 5학년과 6학년에서 임상 실습이 이루어집니다. 대만에서는 5학년 학생들이 환자를 처음 경험하고 6학년 학생들은 환자와 더 깊이 접촉하게 됩니다. 7학년 학생들은 인턴십에 참여합니다. 네덜란드 학생들은 6년간의 수련 프로그램 중 4학년에 인턴십에 들어가며, 핵심적인 인턴십은 4학년과 5학년으로 예정되어 있습니다.
In the present seven-year postsecondary medical education program in Taiwan, clerkships take place in Years 5 and 6. In Taiwan, Year 5 students have initial patient experiences and Year 6 students have deeper contacts with patients. Students in Year 7 are in internships. Dutch students enter clerkships in Year 4 of a six-year training program in which their core clerkships are scheduled in Years 4 and 5.
2014년 가을, 우리는 네덜란드와 대만 학생들 중 내과, 외과, 소아과, 안과, 가정의학과, 정신과 등 다양한 핵심 클락십에 등록한 학생들을 의도적으로 샘플링하여 현재와 이전의 다양한 직업 경험을 조사했습니다. 다양한 연령과 성별의 학생들이 참여하여 각 국가의 학생 코호트를 대표할 수 있도록 했습니다.
In fall 2014, we purposively sampled Dutch and Taiwanese students who were enrolled in different core clerkships (i.e., internal medicine, surgery, pediatrics, ophthalmology, family medicine, and psychiatry), after having completed different clerkships in the months before, leading to a broad range of current and previous professional experiences. We included students across a range of age and gender, ensuring that the participants were representative of the student cohorts in the respective countries.
일반적으로 질적 연구, 특히 담론 분석에서 데이터의 양이 너무 많으면 분석의 질이 떨어질 수 있으므로, 한 번의 분석에 너무 많은 데이터가 포함될 수 있다는 점을 예상하면서도 최종 분석을 위해 데이터 세트를 줄이기 전에 각 국가에서 10~12명의 참가자가 충분하다고 선험적으로 결정했습니다.
In qualitative research in general and discourse analysis in particular, a too-large amount of data may erode the quality of analysis, so we decided a priori that 10 to 12 participants from each country would be sufficient, anticipating that this would even lead to too much data for one analysis, but appreciating that this would offer a broad perspective to start with, before reducing the data set for final analysis.
데이터 수집
Data collection
데이터 수집의 주요 방법으로 오디오 일기를 사용했으며,11 학생들에게 다음 프롬프트를 사용하여 감정적 경험을 이야기하도록 요청했습니다: 무슨 일이 있었나요? 무엇을 느끼고/생각하고/행동했나요? 이것이 의사로서의 성장과 어떻게 상호작용하는가?
We used audio diaries as the central method for data collection,11 asking students to narrate emotional experiences using the following prompts: What happened? What did you feel/think/do? How does this interplay with your development as a doctor?
오디오 일기는 대만 학생은 중국어로, 네덜란드 학생은 네덜란드어로 녹음했습니다. 대만 참가자들은 6학년 첫 4주(1~4주차) 동안 일주일에 최소 3번의 일기를 작성했습니다. 네덜란드 참가자들 역시 5학년 첫 4주 동안 매주 최소 3개의 오디오 일기 항목을 작성하도록 요청받았습니다. 두 그룹의 학생들을 대상으로 한 이 두 기간은 가장 직접적으로 비교할 수 있는 기간이었습니다.
The audio diaries were recorded in Chinese by Taiwanese students and in Dutch by Dutch students. Taiwanese participants made at least three diary entries per week during the first four weeks (Weeks 1–4) of Year 6. Dutch participants were also asked to keep at least three audio diary entries per week in the first four weeks of Year 5. These two periods for the two groups of students were the most directly comparable.
오디오 일기 항목의 길이는 두 학생 샘플 간에 차이가 있었는데, 대만 학생들의 일기 항목이 네덜란드 학생들보다 훨씬 길어 네덜란드 학생들과 추가 인터뷰를 진행했습니다. 2014년 가을에 실시된 이 인터뷰는 40분에서 60분 정도 진행되었으며, 네덜란드 박사 과정 학생(J.d.V.)이 학생들에게 일기에 서술한 감정적 경험을 회상하고 그러한 감정과 사건에 대해 자세히 설명해 달라고 요청했습니다. 인터뷰에서 수집한 데이터는 일기에서 수집한 데이터와 다를 수 있지만, 후속 분석을 용이하게 하기 위해 대만 학생들에 비해 일기에 덜 반영된 것으로 보이는 네덜란드 학생들의 경험에 대한 이해를 풍부하게 하기 위해 의도적으로 이 추가 데이터 수집을 사용하기로 결정했습니다.
The length of the audio diary entries differed between the two student samples, with Taiwanese diary entries being much longer than those of Dutch students, leading us to carry out additional interviews with Dutch students. These interviews, also conducted in fall 2014, lasted between 40 and 60 minutes and were carried out by a Dutch PhD student (J.d.V.), who asked students to recall the emotional experiences they narrated in their diaries and elaborate on those emotions and events. Although data collected in interviews may differ from those gathered in diaries, we deliberately chose to use this additional data collection to enrich our understanding of the experiences of the Dutch students, who appeared to be less reflective in their diaries than their Taiwanese colleagues, in order to facilitate subsequent analysis.
데이터 선택 및 번역
Selection and translation of data
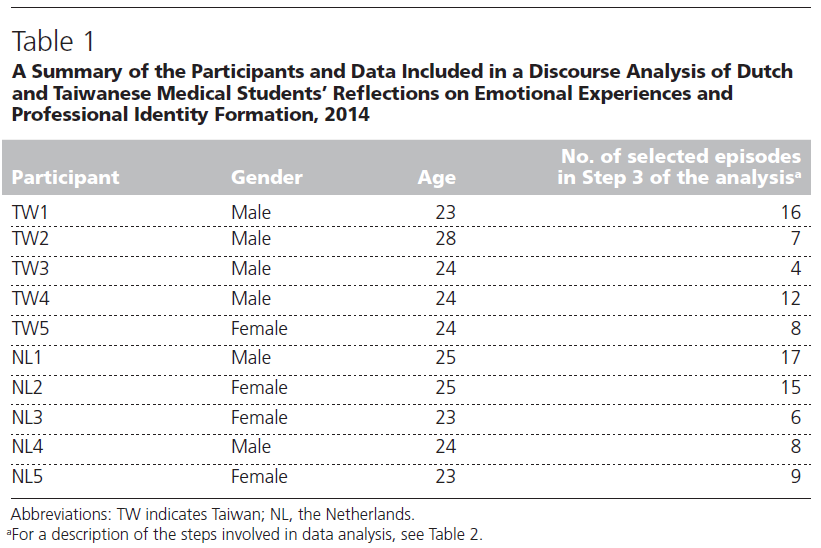
앞서 언급한 바와 같이, 일반적으로 질적 연구와 담화 분석은 데이터가 너무 많으면 어려움을 겪을 수 있으므로 심층 분석을 위해 각 국가별로 5개의 일기만 포함하기로 결정했습니다. 양국의 연구팀은 먼저 각국의 10~12개 일기를 모두 원어로 녹음하고 녹취록을 읽으며 비판적으로 검토했습니다. 풍부하면서도 간결한 데이터 세트를 얻기 위해 각 지역 팀은 학생들이 정서적 경험과 정체성 발달과의 상호 작용을 가장 명확하게 서술하고 반영한 일기 5권을 선정했습니다. 이 일기들은 대만의 전문 번역 회사와 네덜란드의 의대생이 영어로 번역한 후 연구팀원들이 수정하거나 다듬었습니다. 참가자는 국가별(대만의 경우 "TW", 네덜란드의 경우 "NL")로 코딩되었고 번호가 부여되었습니다. 표 1은 참가자의 인구통계학적 세부 사항과 최종 데이터 세트에 대한 설명을 보여줍니다.
As stated above, qualitative research in general and discourse analysis more specifically may suffer from too much data, so we decided that only 5 diaries for each country would be included for in-depth analysis. The research teams in both countries first critically reviewed all 10 or 12 diaries from each country in the original language, listening to recordings and reading through transcripts. To reach a rich but concise data set, each local team selected the 5 diaries in which students most explicitly narrated and reflected on emotional experiences and the interplay with identity development. These diaries were translated into English by a professional translation company in Taiwan and a medical student in the Netherlands and were corrected or refined by members of the research team. Participants were coded by country (“TW” for Taiwan or “NL” for the Netherlands) and a number. Table 1 shows demographic details of participants and a description of the final data set.
데이터 분석
Data analysis
우리는 이전 간행물에서 설명한 바 있는 바흐친의 담론 이론에 기원을 둔 비판적 담론 분석 유형을 사용했습니다.12 담론 방법론에는 다양한 스펙트럼이 있습니다. 대화 분석과 같은 미시 언어 분석13과 푸코주의 담화 분석으로 대표되는 거시 분석14은 스펙트럼의 반대편에 있다고 볼 수 있습니다. Gee15,16는 이러한 극단 사이에 위치한 일련의 담화 도구를 제공하여 문장과 단락 수준에서의 언어 선택과 전체 데이터 세트 내의 언어 사용 패턴이 어떻게 사회적 관행을 구성하는지에 주목했습니다. 이전 연구와 이번 연구에서는 사람들이 자신의 정체성을 구성하기 위해 사용할 수 있는 다양한 담론을 어떻게 사용하는지 조사하기 위해 피규어드 월드 이론17의 개념을 적용했습니다. 형상화된 세계는 규범, 가치, 언어, 감정, 관행과 관련하여 개인이 사회적 또는 "형상화된" 의학 세계 내에서 자신의 정체성을 어떻게 서술하고 구성하는지를 탐구하기 위해 이전에 의학교육에서 사용되었던 비판적 문화 이론입니다.12,18,19 이 이론을 의학교육에 적용할 때 정체성 형성은 네 가지 다른 "담론적 맥락"에서 이루어지며, 이는 사람들과 그들이 말하는 것이 정체성 형성의 가능성을 창출하는 방식으로 정의됩니다:
- (1) 환자, 의료 서비스 제공자 및 기타 사람들에 의해 채워지는 '형상화된' 세계,
- (2) 학생, 환자 및 기타 의학 세계의 '인물'에게 부여되는 위치 또는 지위,
- (3) 사람들이 언어를 사용하여 '자기 저자화'하거나 스스로 특정 지위 또는 정체성을 만드는 방법,
- (4) '세계 만들기' 또는 미래의 이상 세계를 상상하기 위해 언어를 사용하는 방법.
We used a type of critical discourse analysis that has its origins in Bakhtin’s discourse theory as described in an earlier publication.12 There is a spectrum of discourse methodologies. Microlinguistic analysis, such as conversation analysis,13 and macroanalysis, typified by Foucauldian discourse analysis,14 can be regarded as opposite ends of the spectrum. Gee15,16 provided a set of discourse tools that sit between those extremes, directing attention to how choice of language at the level of sentences and paragraphs, and patterns of language usage within whole data sets, construct social practices. In our previous study, and in the current one, we applied concepts from Figured Worlds theory17 to investigate how people use different discourses available to them to construct their identities. Figured Worlds is a critical cultural theory, previously used within medical education to explore how individuals narrate and construct their identities within the social or “figured” world of medicine, relating to norms, values, language, emotions, and practices.12,18,19 Within this theory, as applied to medical education, identity formation takes place in four different “discursive contexts,” defined as how people and the things they say create possibilities for identity formation:
- (1) a “figured” world, populated by patients, health care providers, and other people;
- (2) positions, or status, granted to students, patients, and other “figures” in the world of medicine;
- (3) how people use language to “self-author” or create specific positions or identities for themselves; and
- (4) how they use language for “world making,” or imagining future ideal worlds.
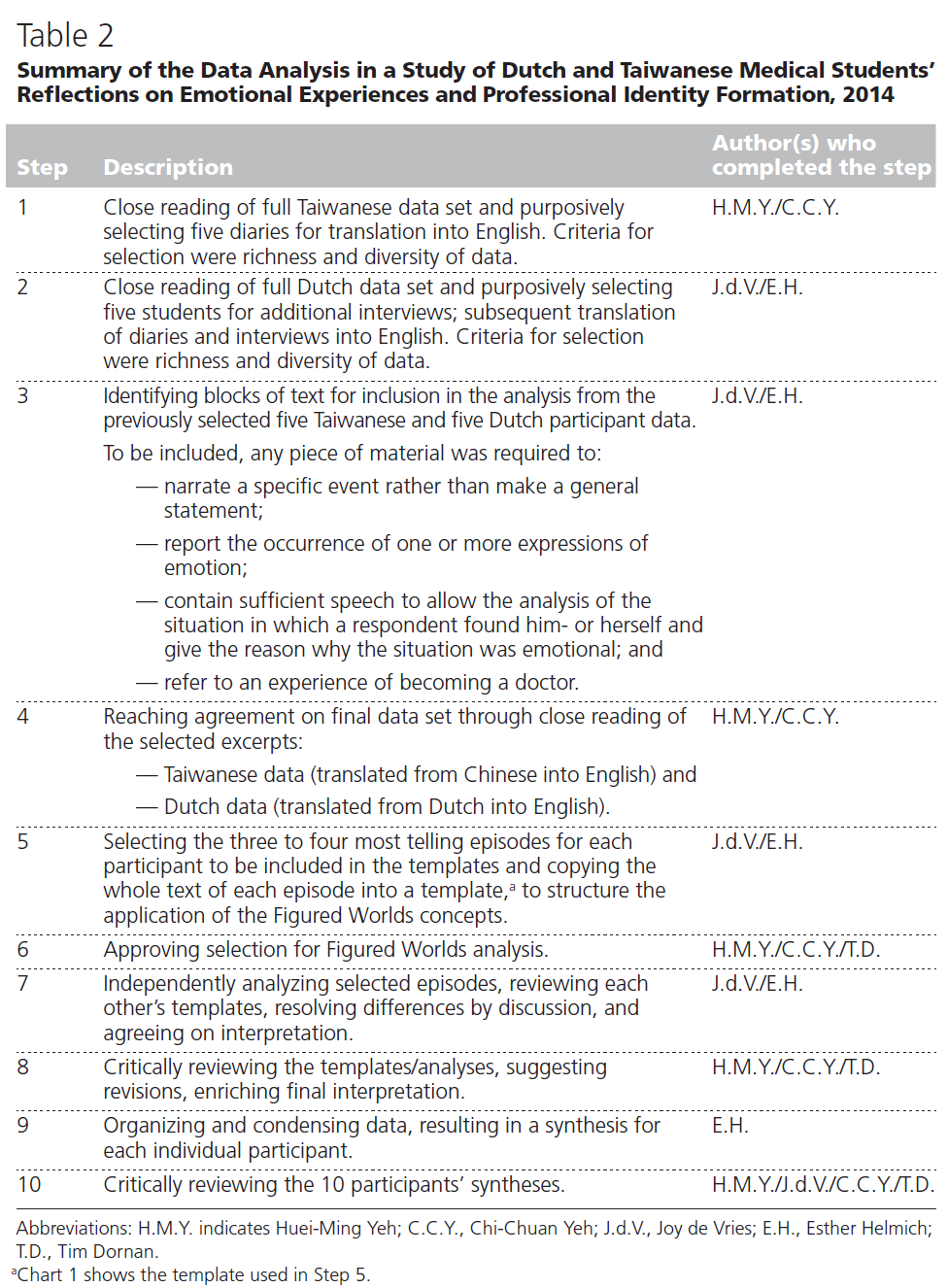
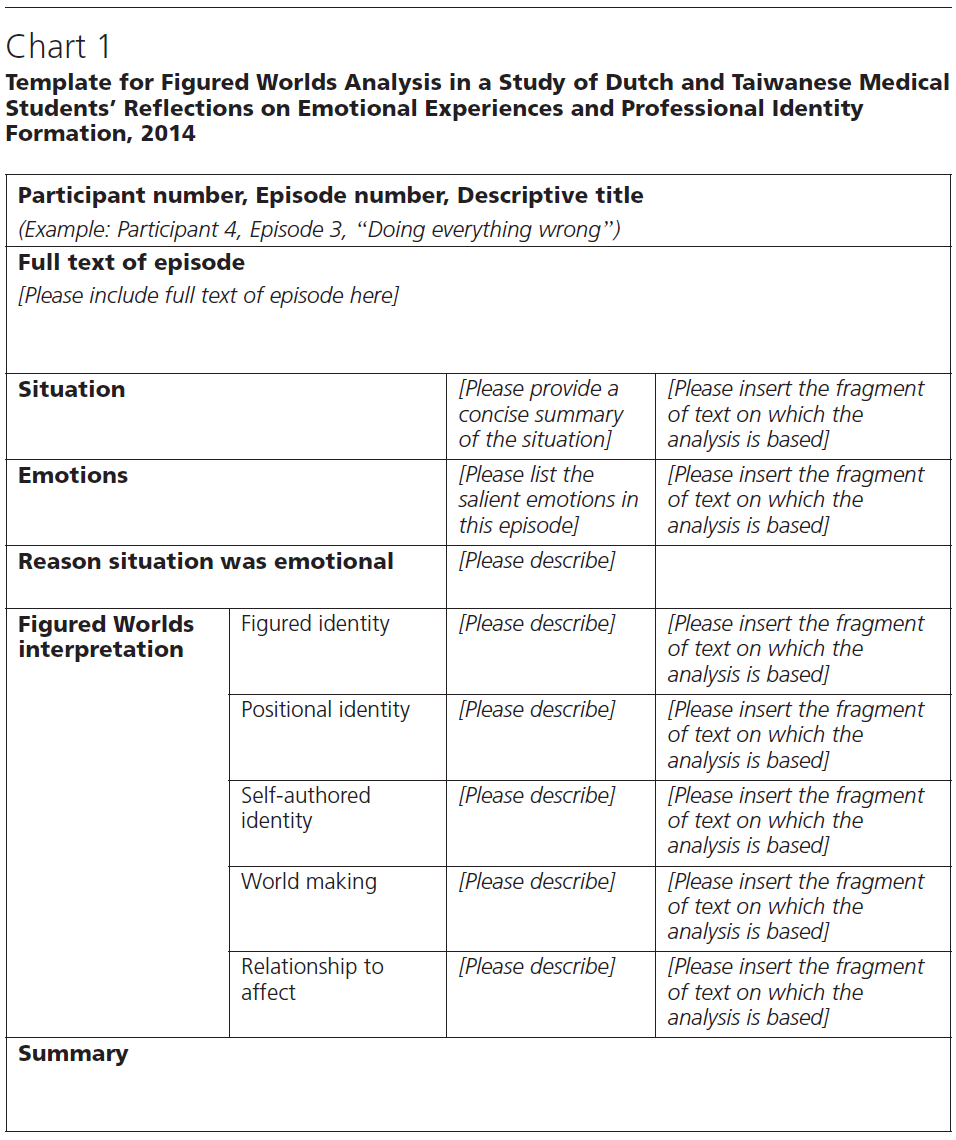
분석 과정에는 감정적으로 두드러진 에피소드를 나타내는 텍스트 블록을 식별한 다음, 해당 텍스트를 에피소드 및 참여자별로 분석하여 개인 내 및 개인 간 반응 패턴을 탐색할 수 있도록 하는 작업이 수반되었습니다. 데이터 분석의 신뢰성과 공신력을 높이기 위해 네덜란드의 두 책임 연구원(E.H., J.d.V.)은 각 단계에서 내린 결정에 대해 수시로 논의했으며, 대만 팀이 별도로 검토하고 승인했습니다. 데이터 삼각 측량에 도달하기 위한 수단으로 각 팀은 정기적으로 원어로 된 전체 데이터 세트로 돌아갔습니다. 담화 분석은 참가자가 말하고자 하는 바를 이해하는 것이 아니라 경험에 대해 이야기하는 데 사용되는 언어를 연구하는 것이라는 전제에 따라, 참가자에게 다시 돌아가 구성원 확인을 하지 않았습니다. 데이터 분석 중에 내린 결정과 진화하는 해석은 숙련된 담화 분석가(T.D.)를 포함한 전체 팀원들과 Skype 회의에서 논의했습니다. 표 2와 도표 1은 데이터 분석의 단계와 사용된 템플릿을 보여줍니다.
The analytical process entailed identifying blocks of text representing emotionally salient episodes, followed by analyzing those texts by episode and participant to allow the exploration of intraindividual as well as interindividual patterns of response. To enhance trustworthiness and credibility of data analysis, the two Dutch lead researchers (E.H., J.d.V.) frequently discussed the decisions made in each step of the process, which was then separately reviewed and approved by the Taiwanese team. As a means to reach data triangulation, each team regularly returned to the full data set, in the original language. Following the premise that discourse analysis is not about understanding what participants meant to say, but about studying the language used to talk about experiences, we did not return to participants for a member check. Decisions made during data analysis and the evolving interpretations were discussed in Skype meetings with the whole team, including an experienced discourse analyst (T.D.). Table 2 and Chart 1 show the steps of data analysis and the template used.
연구팀의 모든 구성원은 의료 전문가로서 교육을 받았으며, 두 명은 의학교육학 박사 학위를, 한 명은 유교 윤리학 박사 학위를 소지하고 있습니다. 대만인 팀원들은 모두 유럽이나 북미에서 일정 기간 동안 거주한 경험이 있습니다. 문화 간 이해를 돕기 위해 제1저자(E.H.)는 대만을 직접 방문하여 연구를 진행했습니다.
All members of the research team have been trained as health care professionals; two members of the team hold PhDs in medical education (E.H., T.D.), and one is a professor in Confucian ethics (D.T.). The Taiwanese members of the team have all lived in Europe or North America for some amount of time. To further facilitate cross-cultural understanding, the first author (E.H.) made a study visit to Taiwan.
연구 결과
Results
상상의 세계
Figured worlds
양국의 참가자들은 피규어 세계에서의 많은 감정적 경험을 이야기했으며, 이는 직업적 정체성 형성에 큰 영향을 미쳤습니다.
- 대만 참가자들은 다양한 의사, 간호사, 동료, 환자, 친척이 있는 생동감 넘치는 세계를 상상했습니다.
- 반면 네덜란드 학생들은 한두 명의 지도 의사만 있는 학습 세계를 상상했습니다. 다른 의료 전문가, 환자, 친척은 네덜란드 학생들에게는 눈에 띄지 않는 인물이었습니다.
- 대만 학생들의 이야기에는 저녁 식사 시간도 없이 열심히 일하고 헌신하는 의사, 학생들을 지원하고 감싸주는 간호사, 환자와 다투는 전문의 등 다양한 인물이 등장했으며, 일부 환자는 화를 내거나 무례하고 뻔뻔하며 귀찮고 불합리한 행동을 하는 반면, 다른 환자는 고마워하며 케이크를 선물로 가져오는 등 다양한 모습을 보여주었습니다.
- 네덜란드 학생들은 주로 의사가 되기 위한 실질적인 측면을 이야기했으며, 특히 스킬 개발에 중점을 두었습니다. 직장에서 관찰한 것에 대한 이야기는 상대적으로 적었고, 의사가 되는 것이 어떤 것인지에 대한 성찰은 제한적이었습니다.
Participants in both countries narrated many emotional experiences in the figured world of medicine, which strongly influenced their professional identity development.
- Participants from Taiwan figured lively worlds with many different doctors, nurses, peers, patients, and relatives.
- Dutch students, in contrast, figured learning worlds with only one or two supervising doctors. Other health professionals, patients, and relatives were less prominent figures for the Dutch students.
- The rich variety of figures in the Taiwanese narratives included hard-working and dedicated doctors not having time for dinner, nurses supporting and covering for the students, and professionals quarreling with patients; some patients were angry or behaved in rude, shameless, troublesome, and unreasonable ways, while other patients were thankful and brought cakes as gifts.
- Dutch students mostly narrated practical aspects of becoming a doctor, focusing particularly on skills development. They had relatively little to say about what they observed in workplaces, and provided only limited reflections on how it would be to be doctors themselves.
대만 학생들은 교사가 자신의 도덕적 발달에 어떤 영감을 주고 지원했는지 서술한 반면, 네덜란드 학생들은 의료 현장에서의 실제 경험과 의사가 구체적인 임상 역할을 어떻게 생각하는지에 대해 더 자주 서술했습니다:
Taiwanese students narrated how teachers inspired and supported their moral development, whereas Dutch students more often narrated their practical experiences in medical workplaces, and how doctors figured specific clinical roles:
학생으로서 다양한 선생님들로부터 자극을 받는다는 것은 놀라운 일입니다. 외부에서 오신 선생님들은 의료원 내 선생님들과는 전혀 다른 의견을 제시해 주십니다. 때로는 선생님들의 자극이 수업 내용을 뛰어넘을 때도 있습니다. (TW3)
As a student, it’s marvelous to receive some stimulation provided by different teachers. Teachers from outside will provide a completely different opinion from teachers in the medical center. Stimulation of the teachers surpasses the course content sometimes. (TW3)
일주일 내내 의사들이 그 작은 아이를 위해 당황하고 수백 가지를 시도하는 것을 보았습니다...... 그 아이를 위해 의사들이 쏟은 노력에 감명을 받았습니다. (NL2)
All week I had seen how the doctors puzzled and tried a hundred different things for that little child.… I was impressed by the effort the doctors put in [for] that child. (NL2)
포지션 정체성
Positional identities
두 나라의 참가자들은 임상 학생으로서 자신의 위치에 대해 어려움을 겪었으며, 환자 치료에 참여할 기회를 통해 장차 의사가 될 자신을 자리매김할 때 매우 행복하다고 느꼈습니다. 두 그룹 모두 자신을 가르치고 평가하는 임상 감독자와 관련된 자신의 위치에 대해 어려움을 토로했습니다.
- 대만 참가자들은 네덜란드 참가자보다 임상 계층 구조에서 자신의 상대적 위치에 대해 더 많이 이야기했습니다. 대만 참가자들은 자신의 역할을 최소화하고 자신을 낮추며 작은 직책을 맡았습니다. 그들은 잘못을 저지르거나, 윗사람을 실망시키거나, 의료 실수를 하는 것을 두려워했습니다. 그들은 선생님을 높이 평가했으며, 선생님들이 자기 수양을 기르는 데 도움을 준 것에 대해 존경과 감사를 표했습니다.
- 반면 네덜란드 참가자들은 자신을 낮은 위치에 두지 않았고 교육자에 대해 더 비판적이었습니다. 이들은 스스로를 양질의 교육을 받을 법적, 사회적 권리와 자율적으로 행동할 수 있는 충분한 기회를 가진 학습자로 인식했습니다. 그들은 병동에 있는 것에 대한 보상을 받을 자격이 있으며, 학습자이기 때문에 실수를 해도 괜찮다고 말했습니다.
Participants in both countries struggled with their positions as clinical students and felt extremely happy when opportunities to participate in patient care positioned them as doctors-to-be. Both groups described difficulties in their positions relative to clinical supervisors, who both taught and assessed them.
- Taiwanese participants spoke more about their relative positions in the clinical hierarchy than did Dutch participants. Taiwanese participants minimized their roles, lowering themselves and constructing minor positions. They were afraid of doing things wrong, disappointing elders, and making medical errors. They held their teachers in high esteem, expressing respect and gratitude for how teachers helped them cultivate self-discipline.
- Dutch participants, in contrast, constructed less lowly positions for themselves and were more critical toward their educators. They identified themselves as learners with legal and social rights to high-quality teaching and ample opportunities for autonomous action. They said they should be entitled to rewards for being on the wards and that being a learner made it acceptable to make mistakes.
대만과 네덜란드의 참가자들은 수술 중 리트랙터를 잡는 것과 같은 불리하고 비참여적인 직책에 대해 이야기했습니다. 반면에 이러한 사회적 위치가 때때로 학습 기회를 제공하기도 했습니다:
Participants in both Taiwan and the Netherlands talked about unfavorable, nonparticipatory, positional identities, such as holding retractors during surgery. On the other hand, such social positions sometimes afforded learning opportunities:
그 과정에서 제가 한 일은 리트랙터를 잡는 것이었습니다. 다행히도 저는 이 수술을 명확하게 볼 수 있었습니다. 선배는 수술 내내 설명을 해주었습니다. 전체 과정이 느리기 때문에 선배는 저를 가르칠 시간이 많았습니다. 다른 선배도 자세히 설명해 주셨어요. (TW1)
What I did in the process was hold a retractor. Fortunately, I had a clear view of this surgery. The senior explained throughout the surgery. Because she was slow in the whole process, she had a lot of time to teach me. Another senior also had a lot of time to tell me the details. (TW1)
팀 내에서 제가 맡은 역할이 전혀 없었고, 이미 역할이 분담되어 있었기 때문에 제가 할 필요가 없었기 때문에 소생술 중에 정확히 어떤 일이 일어나는지 침착하게 지켜볼 수 있었습니다. (NL2)
I absolutely fulfilled no role within the team, and I wasn’t necessary because the roles were already divided, so I could, uh, yes, pretty calmly watch what happens exactly during a resuscitation. (NL2)
직책의 정체성과 이에 대응하는 방식은 두 나라 모두 비슷했지만, 네덜란드 참가자의 직책에는 어느 정도 자율성이 부여되는 경우가 더 많았습니다:
Although the positional identities and the ways participants responded to these were comparable in the two countries, Dutch participants’ positions more often gave them a measure of autonomy:
가장 좋았던 점은 제가 뉴스를 전할 수 있다는 것이었습니다. (NL1)
What I considered the nicest part was that I was allowed to tell the news. (NL1)
네덜란드 참가자들은 환자를 의존적이고 도움이 필요한 존재로 포지셔닝하는 경향이 있었습니다. 환자의 자기 결정 능력에 대해서는 언급하지 않았습니다. 반면 대만 참가자들은 환자를 배울 것이 많은 능동적인 주체로 포지셔닝했습니다. 대만 참가자들은 환자에 대해 분노와 조급함을 드러내고 환자들의 행동에 좌절감을 느끼는 경우도 있었습니다. 그들은 환자들이 무례하고 학생, 사무원, 레지던트, 병원 관리자 등 지위가 낮은 사람들에게 비난을 퍼붓는 것에 대해 이야기했습니다.
Dutch participants tended to position patients as dependent and needing help. They did not refer to patients’ capacity for self-determination. Taiwanese participants, in contrast, positioned patients as active agents from whom they had much to learn. On other occasions, Taiwanese participants displayed anger and impatience toward patients and felt frustrated by their behavior. They spoke of how patients were rude and placed blame on people with low status, such as students, clerks, residents, and hospital administrators.
자기 저작
Self-authoring
형상화된 정체성과 지위적 정체성은 주로 사회 구조와 다른 사람들의 대리인에 의해 결정되는 반면, 개인이 자율적인 사회적 행위자로서 주체성을 행사할 수 있는 것은 자기 저작을 통해서입니다. 대만과 네덜란드 참가자들이 자신의 정체성을 저작하는 방식에는 상당한 차이가 있었습니다. 이러한 차이는 자기 수양, 자율적 행동의 가능성, 의료 수련생으로서의 자기 결정에 대해 이야기하는 방식에서 분명하게 드러났습니다.
Whereas figured and positional identities are largely determined by social structures and other people’s agency, it is by self-authoring that individuals are able to exercise agency as autonomous social actors. There were significant differences between how Taiwanese and Dutch participants authored their identities. These differences were apparent in how they spoke about self-cultivation, their possibilities for autonomous action, and their self-determination as medical trainees.
양국의 참가자들은 스스로를 환자에 대한 연민, 취약한 사람들을 돌보고자 하는 강한 의지, 강하고 유능한 직업적 정체성을 개발하는 사람으로 묘사했습니다.
- 대만 참가자들은 좋은 의사가 된다는 것이 무엇을 의미하는지에 대해 더 풍부한 언어를 사용하는 경향이 있었습니다.
- 네덜란드 참가자들은 성취와 경쟁에 초점을 맞춘 보다 제한된 정체성을 작성했습니다.
- 의사가 되는 과정에서 두 나라 참가자들은 서로 다른 유형의 자율성을 작성했습니다.
- 네덜란드 참가자들은 자율적인 행동과 '실제적인' 참여를 통해 자율성을 형성한 반면,
- 대만 참가자들은 자기 수양과 강력한 직업적 가치관 개발을 통해 자율성을 형성했습니다.
- 네덜란드 학생들은 교육 시스템이 제공하는 더 많은 참여적 위치에서 능동적이고 자기 통제적인 정체성을 스스로 만들어갈 가능성이 더 높았습니다:
Participants from both countries authored themselves as compassionate toward patients, having a strong wish to care for vulnerable people, and developing strong and competent professional identities. Taiwanese participants tended to use richer language to author what it means to be a good doctor. Dutch participants authored a more limited identity focused on achievement and compe tence. In the process of becoming a doctor, participants from the two countries authored different types of autonomy. Dutch participants authored autonomous action and “hands-on” participation, while Taiwanese participants authored autonomy through self-cultivation and developing strong professional values. From the more participatory position afforded by their education system, Dutch students were more likely to self-author an active and self-regulating identity:
"예스"라고 말할 수 있는 순간이었습니다. 제가 하는 일에 자신감이 생겼고, 일이 잘 풀렸고, 제 스스로 해냈어요. 인턴십 기간 동안 이런 일을 더 자주 처리하고 싶어요! 제가 직접 일을 책임지고 진행했기 때문에 무슨 일이 일어나고 있는지 통제할 수 있었어요. 정말 기분이 좋았어요! (NL5)
This was such a “yes” moment. I felt confident about what I was doing, and it went well, and I did it on my own. I want to handle it like this more often during my internships! I myself was responsible for what was happening, and therefore I did have the control about what was happening. It was a great feeling! (NL5)
대만 참가자들의 역량에 대한 자기 주도적 평가는 개인적인 성취보다는 환자에게 도움이 되는 방향으로 이루어졌습니다:
Taiwanese participants’ self-authoring of competence was less directed toward personal achievement and more toward benefiting patients:
제가 질문을 더 잘하는 것도 장점이기 때문에, 전임자들이 할 수 없었던 많은 것을 환자에게서 배울 수 있었습니다. 그러다 보니 자연스레 성취감도 커졌어요. 또한 제가 가진 지식으로 환자가 자신의 질병에 대해 더 잘 알 수 있도록 도울 수 있어서 기쁩니다. (TW4)
The fact that I’m better at asking questions is also a plus, so I was able to learn a lot of things from the patient that my predecessors weren’t able to. This gave me a great sense of fulfillment naturally. I’m also glad to be able to help the patient learn more about his own illness with my knowledge. (TW4)
세상 만들기
World making
문화적 가치는 이상적인 세계를 구성하는 담론, 특히 의사-환자 또는 학생-교사 관계에 관한 담론에서 가장 두드러졌습니다. 예를 들어, 의사가 나쁜 소식을 전할 때 매우 신중해야 하는 이유를 설명할 때 환자의 자기 결정권에 대한 명시적인 표현을 발견한 것은 대만 참가자들의 이야기에서만 발견할 수 있었습니다:
Cultural values were most apparent in discourse that constructed ideal worlds, particularly regarding doctor–patient or student–teacher relationships. It was only in the narratives of the Taiwanese participants that we found explicit speech about self-determination of patients—for example, when they explained why doctors should be very careful in breaking bad news:
환자와 아버지는 이 말을 듣고도 의사에게 감정적으로 반응하지 않는 것 같았지만, 저는 놀랐습니다...... 앞으로 의사가 된다면 환자에게 나쁜 소식을 재치 있게 전해야겠습니다. 예를 들어 병명을 영어로 적어서 건네주면 "아, 이건 진행성 경화증이에요."라고 직접 말하지 않고 인터넷으로 확인할 수 있게 할 수 있을 것 같아요. 환자들이 상황을 알고 정신적으로 대비할 수 있도록 힌트를 줄 수 있는 방법이 있다고 말하고 싶습니다. (TW5)
The patient and his father did not seem to respond to the doctor emotionally upon hearing these words, though I was astonished.… When I become a doctor in the future, I shall break bad news to my patients tactfully. For instance, I could write down the name of the disease in English and hand it to them, so that they would be able to check online instead of having me tell them directly, like, “Oh this is progressive sclerosing disease.” I would say there are possible ways to give hints to the patients, so that they would know the situation and be prepared mentally. (TW5)
저희는 전문적인 경험을 통해 환자의 자율성과 공동 의사 결정이 네덜란드 의료 담론에서 중요한 이상이라는 것을 알고 있지만, 네덜란드 참가자들의 이야기에는 이러한 내용이 표현되지 않았습니다.
Although we know from our own professional experience that patient autonomy and shared decision making are valued ideals in the discourse of Dutch health care, this was not expressed in the narratives of our Dutch participants.
양국의 참가자들은 환자와의 적절한 관계를 발전시키고 미래의 세계에서 좋은 의사와 교사가 되는 방법을 담론적으로 탐구했습니다:
Participants in both countries discursively explored how to develop appropriate relationships with patients and become good doctors and teachers in future worlds:
환자가 아무리 사랑스러워 보여도 의사와 환자 사이에는 분명한 경계가 있어야 합니다. 정신과에서는 특히 이런 명확한 선을 유지하는 것이 중요합니다. 나는 의사요, 당신은 환자입니다. 이 점은 우리가 끊임없이 상기해야 하는 부분입니다. 우리는 항상 그 선의 존재를 기억하고 잘 그려야 합니다. 올바른 방식으로 선을 그릴 수 있다면 그것은 거의 예술이 될 것입니다. (TW4)
There needs to be a fine line between doctor and patient, no matter how lovely the patient may seem. Maintaining this kind of clear line is especially important in the Psychiatry Division. I’m a doctor, you’re a patient—this is something we constantly have to remind ourselves of. We must always remember the existence of the line, and draw it well. If you’re able to draw the line in just the right way, it almost becomes an art. (TW4)
오늘 배운 것은... 인턴을 감독할 때... 인턴도 사소한 실수를 할 수 있고 그것은 인턴에게 충분히 짜증나는 일이며 즉시 화를 내지 않으면 정말 편안하고 강인한 것이 좋다는 것입니다. (NL2)
What I’ve learned from today is when … I’m going to supervise interns … that even interns can make little mistakes and it’s annoying enough to them and it’s really comfortable if you don’t immediately get mad at them and it’s good to be strong. (NL2)
감명 깊게 읽었던 책이 생각나네요.... 이 얘기를 꺼낸 이유는 저도 저 스스로를 선한 사람이라고 생각하기 때문인데요, 더 정확히 말하면 누구도 차별받지 않고 정의롭고 공평하기를 바라는 사람입니다. (TW5)
I could recall a book that touched me very much.… The reason why I mentioned this is because I consider myself a beneficent person, too; or, to be more accurate, I am a person hoping for justice and fairness for everyone, and no one should be discriminated. (TW5)
대만과 네덜란드의 학생들은 거의 동일한 문제를 다루었지만 언어, 자료, 성찰 방식은 달랐습니다.
Students in both Taiwan and the Netherlands addressed largely the same issues but used different language, resources, and ways of reflecting.
토론
Discussion
의대생은 의사가 되는 과정에서 자신이 들어가게 될 세계, 타인에게 부여되고 허용되는 지위, 스스로 구상하는 정체성, 미래에 대해 상상하는 '이상적인' 세계에서 비롯된 많은 감정을 경험합니다. 문화마다 학생들은 서로 다른 세계와 서로 다른 미래의 정체성을 상상하며, 학생과 환자 모두의 자율성에 대한 서로 다른 문화적 구성을 반영하고 이에 반응합니다.
In the process of becoming a doctor, medical students experience a lot of emotions originating from the figured worlds they are entering, the positions they are granted and allow to others, the identities they envision for themselves, and the “ideal” worlds they imagine for the future. In different cultures, students imagine different worlds and different future identities, reflecting and responding to different cultural constructs of both student and patient autonomy.
기본 가치
Underlying values
네덜란드가 서구 세계 전체나 북서유럽 전체를 대표할 수 없고, 대만이 아시아 또는 동아시아 전체를 대표할 수는 없겠지만, 우리의 연구 결과는 두 가지 주요 도덕 체계를 반영하는 몇 가지 기본 가치로 우리를 안내합니다: 서양의 생명윤리와 중국의 유교. 교육과 실습을 통해 학생들은 좋은 행동에 대한 다양한 가치와 개념을 배우고 관찰하며, 이를 통해 도덕적 자아를 발달시킬 수 있습니다.
Although the Netherlands can by no means represent the whole Western world, or even the entirety of Northwest Europe, and Taiwan will never be able to represent the whole Asian or East Asian world, our findings lead us into some underlying values reflecting two different major moral systems: Western bioethics and Chinese Confucianism. During education and practical training, students learn about and observe different values and conceptions of what is good behavior, which will result in the development of a moral self.
자율성과 도덕적 발달.
Autonomy and moral development.
우리는 자율적인 사회적 행위자로서 참가자들이 두 가지 맥락에서 주체성을 행사하는 방식에서 상당한 차이를 발견했습니다.
We found significant differences in how participants, as autonomous social actors, exercised agency in the two contexts.
연구에 참여한 네덜란드 학생들은 성취와 역량에 중점을 두었습니다. 그들은 의료 전문가이자 유능한 커뮤니케이터로서 환자를 돌볼 수 있는 숙련된 의사가 되기 위해 필요한 자율적 행동과 '실제' 실습 참여의 중요성을 강조했습니다. 그들은 스스로를 자율적이고 자기 조절적 학습자로 규정하고, 좋은 의사가 되기 위해 필요한 기술과 이를 추구하는 방법에 대한 명확한 아이디어를 가지고 있습니다. 경험적 증거에 따르면 실제 실습에서 네덜란드 학생들은 종종 자기조절 학습에 완전히 참여하지 못하는 경우가 많지만,20 학생들의 내러티브는 역량 또는 성과 기반 의료 교육21, 자기 주도적 또는 자기조절 학습22, 합리적이고 자의식적이며 자율적인 개인에 대한 (서구) 문화적 이상에 대한 현재의 지배적인 담론을 분명히 기반으로 하고 있습니다.6,23,24
Dutch students in our study strongly focused on achievement and competence. They emphasized the importance of autonomous action and participation in “hands-on” practice, which is needed to become a skilled doctor who, as a medical expert and competent communicator, is able to care for patients. They authored themselves as autonomous, self-regulating learners, having clear ideas about the skills needed to be a good doctor and how to pursue those. Although empirical evidence shows that Dutch students in real practice are often not able to engage fully in self-regulated learning,20 the narratives of the students clearly build upon current dominant discourses around
- competence or outcomes-based medical training21;
- self-directed or self-regulated learning22; and
- the (Western) cultural ideal of the rational, self-conscious, autonomous individual.6,23,24
대만 학생들은 교사가 제공하는 영감과 도덕 교육, 환자가 공유하는 삶의 경험과 지혜를 높이 평가하면서 반성적 관찰에 더 많이 참여하는 것으로 나타났습니다. 그들의 연설에는 좋은 사람, 좋은 의사가 되기 위한 근본적인 도덕적 가치를 반영하는 매우 풍부한 언어가 포함되어 있었으며, '선한 일'을 하고 사회에 기여하기 위해 명시적으로 노력했습니다. 언뜻 보기에는 의료 수련생으로서의 자기 결단이 잘 드러나지 않을 수 있지만, 실질적인 기술 교육보다는 도덕적 발달에 중점을 두는 것은 자율성을 표현하는 또 다른 방식이라고 할 수 있습니다. "최근 대만의 의학교육 개혁에서는 '좋은 의사가 되기 전에 좋은 사람이 되는 것'이 공통적으로 강조되고 있습니다. 대만 사회의 문화적 가치는 도덕적 자기 수양과 사회 정치적 복지 증진에 헌신하는 이타적 신사, 즉 '춘제'를 양성하는 것을 교육 목표로 삼는 유교 철학의 영향을 많이 받았습니다.24 고대 중국 의료 윤리의 대표적인 슬로건인 '전신전수'("인의예지, 인술")는 유교 윤리의 토대를 충분히 반영하고 있습니다. 스승을 공경하고 '도'('바른 도리')를 준수하는 것 또한 어릴 때부터 일반적으로 가르치는 유교 속담입니다. 대만 학생들의 반성문에서 "착한 일 하기", "사회에 기여하기", "스승에 대한 감사"를 강조하는 이유도 이 때문일 수 있습니다. 유교 철학의 특징인 덕 윤리는 이러한 '좋은 의사' 양성에 대한 성찰에 당연히 기여합니다.
Taiwanese students were found to engage more in reflective observation, highly valuing the inspiration and moral education provided by teachers and the life experience and wisdom shared by patients. Their speech contained very rich language, reflecting underlying moral values related to becoming both a good person and a good doctor, explicitly striving for “doing good,” and contributing to society. Although their self-determination as medical trainees might be less visible at first sight, the emphasis on moral development rather than on practical skills training can be considered a different way of expressing autonomy. “Being a good person before becoming a good doctor” has been commonly emphasized in recent medical education reform in Taiwan. The cultural values of Taiwanese society are much influenced by the Confucian philosophy whose educational goal is to cultivate altruistic gentlemen, “chun-tze,” who are committed to both moral self-cultivation and social-political welfare promotion.24 A distinctive and representative slogan of ancient Chinese medical ethics, “jen-hsin-jen-shu” (“a heart of humaneness, the skill of humaneness”), reflects fully its foundation of Confucian ethics. Respecting teachers and adhering to the “dao” (“the righteous way”) is also a Confucian saying generally taught since childhood. This might explain partly why the reflective narratives of Taiwanese students so much emphasized “doing good,” “contributing to society,” and “appreciating teachers.” The virtue ethics characteristic of Confucian philosophy understandably contributes to such “good doctor” cultivation reflection.
자율성과 관련성.
Autonomy and relatedness.
의사와 환자의 자율성에 대한 참가자들의 서로 다른 문화적 구성은 자기 결정권을 다른 사람과의 관계에서 어느 정도 찾았습니다.
- 대만 학생들의 일기에는 다른 사람에 대한 언급이 많았고, '우리'에 대한 이야기가 많이 나왔습니다. 반면
- 네덜란드 학생들은 '나'를 더 자주 언급하고 개인의 성취에 더 중점을 두는 것으로 나타났습니다.
- 대만 학생들은 교사, 학교 선후배, 임상 감독자, 환자 등 다양한 사람들을 언급했습니다. 대만 학생들은 네덜란드 학생들보다 다른 사람의 역할, 특히 환자에 대한 자신의 역할에 대해 훨씬 더 많이 반영하고 있었습니다.
Participants’ different cultural constructs of physician and patient autonomy located self-determination to a greater or lesser extent in relationships with other people. In the Taiwanese diaries, there was a lot of reference to other people, and a lot of “we” talk. In contrast, Dutch students seemed to refer more often to “I,” and place more emphasis on their personal achievement. Taiwanese students included many different people, such as teachers, older schoolmates, clinical supervisors, and patients. They were reflecting much more about the role of other people, and in particular their role toward patients, than Dutch students did.
유교 윤리에는 이와 관련이 있을 수 있는 몇 가지 기본 가치가 있습니다. 타오25는 "중국인의 사고에서 개인은 결코 독립된 개체로 인식되지 않으며, 항상 다른 사람들과의 관계에서 각각 특정한 역할을 하는 네트워크의 일부로 간주된다"는 Liang의 관찰을 인용합니다. Tu26는 고전적 유교적 의미의 '자아'는 관계의 중심이자 영적 발전의 역동적 과정이라고 주장합니다. 차이24는 또한 유교적 인격 개념을 수직적 차원(자율적이고 자기 수양적인 인격)과 수평적 차원(관계적이고 이타적인 인격)의 두 가지 차원으로 해석합니다. 관계적 인격체 개념은 대만의 의사-환자 관계에서 중요한 역할을 합니다.24 따라서 대만 학생들은 네덜란드 학생들보다 성찰 일기에 다른 구성원을 더 많이 포함시켰으며, 그들의 정체성을 단순히 "나"가 아닌 "우리"의 사고에 더 많이 표현한 것으로 생각할 수 있습니다. 대인 관계는 대만 그룹에서 두드러진 특징이 되었습니다.
There are certain underlying values in Confucian ethics that might be relevant here. Tao25 quotes Liang’s observation that “[i]n the Chinese thinking, individuals are never recognized as separate entities; they are always regarded as part of a network, each with a specific role in relation to others.” Tu26 argues that “self” in the classical Confucian sense is both the center of relationships and a dynamic process of spiritual development. Tsai24 also interprets the Confucian concept of persons as two-dimensional—the vertical dimension (the autonomous, self-cultivating one) and the horizontal dimension (the relational, altruistic one). The concept of relational personhood plays an important role in the Taiwanese doctor–patient relationship.24 Therefore, it is conceivable that Taiwanese students included other members in their reflective diaries more than their Dutch counterparts, and their identities expressed were more in the thinking of “we” rather than merely “I.” The person-in-relationship became a distinctive feature in the Taiwanese group.
이는 대만 학생들이 나쁜 소식을 전하는 것에 대해 이야기할 때 언급했던 것과도 관련이 있습니다.
- 네덜란드에서는 환자의 자율성, 정직성, 공동 의사 결정과 같은 윤리적 또는 직업적 규범과 가치관이 바탕이 되어 매우 나쁜 진단이라도 환자에게 직접 솔직하게 공개할 수 있습니다.
- 대만에서는 환자를 가족과 더 넓은 사회 집단의 일원 또는 관계에 있는 사람으로 간주하는 근본적인 가치관이 다르기 때문에 항상 '제3의 목격자'를 두고 가족을 통해 간접적으로 나쁜 소식을 전하게 됩니다.
This also pertains to what Taiwanese students mentioned in their narratives about breaking bad news.
- In the Netherlands, underlying ethical or professional norms and values, such as patient autonomy, honesty, and shared decision making, lead to a frank disclosure of even a very bad diagnosis directly to the patient as an individual.
- The underlying values in Taiwan are different, pertaining to the patient as a member of their family and broader social group, or a person-in-relationship, which results in always having a “third witness” in the room, and breaking bad news indirectly—for example, via family members.
네덜란드 학생들은 인간관계에 대한 언급이 많지 않았고, 노골적인 도덕적 발언을 하지도 않았습니다. 그럼에도 불구하고, 특히 자아를 형성하고 세상을 만들어가는 과정에서 다른 사람을 돌보고 싶다는 강한 의지를 표명했으며, 이는 실제로 책임을 지는 데 필요한 역량을 개발해야 한다는 의미로 표현되었습니다.
Dutch students did not make much reference to relationships, nor did they make explicit moral statements. Nevertheless, in particular in their self-authoring and world making, they expressed a strong wish to care for other people, phrased as the need to develop the competence needed to actually take responsibility.
의학교육에 대한 시사점
Implications for medical education
학생들의 내러티브는 의학적 실천의 창으로 간주될 수 있습니다. 세계 여러 지역의 의학교육 시스템을 자세히 연구함으로써 우리는 다양한 윤리 시스템, 다양한 문화적 가치, 그리고 다른 사회에서 의사가 된다는 것 또는 훌륭한 의료 전문가가 된다는 것이 무엇을 의미하는지에 대해 많은 것을 배울 수 있습니다. 이러한 이해는 전 세계의 전문직에 대한 관념에 영향을 미치는 다양한 가치를 설명하고, 전문직 정체성 형성이 어떻게 작동하고 상황에 따라 어떻게 영향을 받는지에 대한 통찰력을 넓힘으로써 의학교육 분야를 발전시키는 데 도움이 될 수 있습니다. 이는 문화적 차이에 대한 인정과 인식을 향상시키고, 예를 들어 반성적 관찰과 능동적 참여의 어포던스를 고려할 때 문화에 특화된 개입의 개발을 촉진할 수 있는 잠재력을 가지고 있습니다. 본 연구는 특히 서로 다른 근본적인 문화적 가치와 관련된 두 가지 학습 방법의 가치를 명확하게 보여줍니다. 우리는 두 나라의 학생과 의학교육자 모두가 서로에게서 배울 수 있다고 제안하고 싶습니다. 네덜란드 학생들의 학습 과정은 중등학교나 의과대학에서 윤리 교육을 강화하고 좋은 의사가 된다는 것이 무엇을 의미하는지에 대한 토론을 유도함으로써 더욱 심화될 수 있습니다. 성찰에 쉽게 참여하고 자신의 생각과 가치를 표현하는 데 능숙하지만 임상 환경에서 주체성이 떨어지는 대만 학생의 경우, 경험 학습에 더 집중하면 학습 과정을 향상시킬 수 있습니다.
Student narratives can be considered a window to medical practice. By engaging in a detailed study of medical education systems in different parts of the world, we can learn a lot about different ethical systems, about different cultural values, and about what it means to become a doctor or to be a good medical professional in different societies. These understandings may help advance the medical education field by explicating the different values that inform notions about professionalism all around the world and by broadening our insight into how professional identity formation works and how it is influenced by context. This has the potential to enhance the recognition and appreciation of cultural differences and stimulate the development of culture-specific interventions—for example, in considering the affordances of reflective observation versus active participation. The present study clearly shows the value of both ways of learning, especially related to different underlying cultural values. We would like to suggest that both students and medical educators from the two countries can learn from each other. The learning process of students in the Netherlands might be deepened by providing more ethical education in secondary school or medical school, and by provoking discussion about what it means to be a good doctor. For Taiwanese students, who easily engage in reflection and are very good at expressing their thoughts and values, but who show less agency in the clinical environment, more focus on experiential learning might enhance their learning process.
향후 연구를 위한 제한점 및 제안
Limitations and suggestions for future research
직업 정체성 개발은 분명히 상황에 따라 다릅니다. 본 연구는 두 개의 다른 국가에서 이 과정과 그 기본 가치에 대한 자세한 연구를 제공합니다. 연구 결과는 이러한 유형의 담론 분석에서 흔히 볼 수 있는 다소 작은 데이터 세트를 기반으로 하지만, 심층적인 접근을 가능하게 합니다. 우리의 해석은 강력한 이론적 프레임워크의 사용과 연구팀원들의 격렬한 토론과 현장 방문을 통해 정보를 얻었습니다. 그러나 제1저자가 네덜란드인(E.H.)이므로 본 논문의 결과 발표는 부득이하게 서구의 관점에서 이루어질 수밖에 없습니다. 예를 들어, 저(E.H.)는 자율성에 대해 생각할 때 네덜란드의 의료 실무 및 의학교육에 대한 배경과 경험을 바탕으로 생각하며, 이러한 개인적인 이해를 참고 자료로 사용할 것입니다. 대만인 제1저자는 유교 철학을 설명하는 것으로 시작하여 이 도덕 체계의 핵심 개념 중 하나를 참조로 선택했을 수 있습니다. 따라서 다른 문화권의 정체성 발달에 대한 이해를 높이기 위해서는 다른 국가와 문화권, 다른 연구팀, 다른 제1저자와 함께 더 많은 연구를 수행할 필요가 있다고 생각합니다.2
Professional identity development clearly is context-specific. Our research provides a detailed study of this process and its underlying values in two different countries. Our results are based on a rather small data set, which is typical for this type of discourse analysis, but allows for an in-depth approach. Our interpretations were informed by the use of a strong theoretical framework and by intense discussions and site visits by members of the research team. As the first author is Dutch (E.H.), however, the presentation of the results in this paper unavoidably will be from a Western perspective. When I (E.H.), for example, think about autonomy, I do so from my Dutch background and experience in medical practice and medical education, and will use this personal understanding as a point of reference. A Taiwanese first author might have started with describing Confucian philosophy, and might have chosen one of the core notions from this moral system for reference. Therefore, we suggest that more research needs to be done in different countries and cultures, with different research teams and with different first authors, to further increase our understanding of identity development in different cultures.2
Emotional Learning and Identity Development in Medicine: A Cross-Cultural Qualitative Study Comparing Taiwanese and Dutch Medical Undergraduates
PMID: 28353499
Abstract
Purpose: Current knowledge about the interplay between emotions and professional identity formation is limited and largely based on research in Western settings. This study aimed to broaden understandings of professional identity formation cross-culturally.
Method: In fall 2014, the authors purposively sampled 22 clinical students from Taiwan and the Netherlands and asked them to keep audio diaries, narrating emotional experiences during clerkships using three prompts: What happened? What did you feel/think/do? How does this interplay with your development as a doctor? Dutch audio diaries were supplemented with follow-up interviews. The authors analyzed participants' narratives using a critical discourse analysis informed by Figured Worlds theory and Bakhtin's concept of dialogism, according to which people's spoken words create identities in imagined future worlds.
Results: Participants talked vividly, but differently, about their experiences. Dutch participants' emotions related to individual achievement and competence. Taiwanese participants' rich, emotional language reflected on becoming both a good person and a good doctor. These discourses constructed doctors' and patients' autonomy in culturally specific ways. The Dutch construct centered on "hands-on" participation, which developed the identity of a technically skilled doctor, but did not address patients' self-determination. The Taiwanese construct located physicians' autonomy within moral values more than practical proficiency, and gave patients agency to influence doctor-patient relationships.
Conclusions: Participants' cultural constructs of physician and patient autonomy led them to construct different professional identities within different imagined worlds. The contrasting discourses show how medical students learn about different meanings of becoming doctors in culturally specific contexts.
'Articles (Medical Education) > 세계화, 다양한 국가' 카테고리의 다른 글
| 보건의료전문직 국가면허시스템의 진화: 라오스의 질적기술사례연구 ( Hum Resour Health. 2017) (0) | 2023.11.19 |
|---|---|
| 라오스의 의학교육(Med Teach, 2019) (0) | 2023.11.19 |
| 이타주의인가, 국가주의인가? 의과대학 규제에 대한 글로벌 담론 살펴보기 (Med Educ, 2022) (0) | 2023.05.04 |
| 일반의 진료와 의사면허시험 (British Journal of General Practice 2022) (0) | 2022.11.09 |
| 베를린은 학부의학교육과정을 개편하기 시작했다: 개발의 역사, 원칙, 종결 돌아보기 (GMS J Med Educ. 2019) (0) | 2022.10.08 |