의학교육 도구로서 서사의학: 체계적 문헌고찰(Med Teach, 2019)
Narrative medicine as a medical education tool: A systematic review
M. M. Milota, G. J. M. W. van Thiel and J. J. M. van Delden
소개
Introduction
기술과 빅데이터가 임상 상호작용에서 차지하는 역할이 점점 더 두드러지면서, 위험은 각 환자의 질병 서사의 특이성과 중요성에 대한 관심이 줄어들 것이라는 점이다. 디지털 의학이 부상하는 것은 [두 종류의 경쟁하는competing 서사]의 출현과 일치할 수 있다: [디지털 기술을 통해 수집된 디지털 서사]와 [그러한 기술을 사용하는 환자의 경험적이고 개인적인 서사]이다.
With the increasingly prominent role that technology and big data play in clinical interactions, the risk is that less attention will be paid to the singularity and significance of each patient’s illness narrative. It is not unconceivable that the rise of digital medicine may correspond with the emergence of two sorts of competing narratives: the digital narratives collected via digital technologies and the experiential, personal narratives of the patients using such technologies.
서사 의학 또는 서사 기반 의학은 "질병에 대한 과학적 이해를 증진시키기 위해 서사적 기술을 사용하는 의학에 대한 접근"을 구성하며, 따라서 이러한 서사적 분열naarative schism을 방지하는 하나의 수단으로 볼 수 있다. [서사 의학을 가르치고 실천하는 사람들]은 그것이 [현대적이고 기술적으로 향상된 의학에 대한 대안이 되기 위한 의도가 아니라]고 주장한다. 오히려, 그것은 [근거 기반 의료행위]가 의사와 환자 사이의 대화적 임상적 만남에서 나타나는 [개인적 증거]와 짝을 이룰 수 있고 또 짝을 이루어야 한다는 것을 의료 전문가들에게 밝히는 수단으로 보여진다. 지지자들은 임상 환경에서 [내러티브에 대한 더 나은 관심과 인정]이 [의사의 의학병리학적 지식]과 [환자의 이야기에 포함된 경험적 지식] 사이의 차이를 메우는데 도움을 줄 수 있다고 주장한다.
Narrative medicine, or narrative-based medicine, constitutes “an approach to medicine that employs narrative skills to augment scientific understandings of illness” (Lewis 2011) and can thus be seen as one means of preventing this narrative schism. Those who teach and practice narrative-based medicine claim that it is not intended to be an alternative to modern, technologically enhanced, medicine. Rather, it is seen as a means of revealing to medical professionals that evidence-based practices can and should be paired with the personal evidence that emerges in a dialogic clinical encounter between a doctor and patient (Holmgren 2011; Chin-Yee 2018). Proponents claim that better attention to and appreciation of narratives in the clinical setting can help doctors bridge the gap between their mediopathological knowledge and the experiential knowledge contained in their patients’ stories (Greenhalgh 1999; Greenhalgh and Hurwitz 1999; Launer 1999; Hurwitz 2000).
따라서 서사의학 교육 개입은 의대생들이 그들의 "서사적 역량narrative competence"을 증가시킴으로써 환자와 공유 의사 결정 과정에 참여할 수 있도록 준비하는 중요한 수단으로 작용한다. 이러한 개입은 학생들이 [경청과 관찰 기술을 연마하고, 공감 능력을 자극하며, 성찰과 관점수용 능력을 증가]시키는 것을 목표로 한다. 또한 서사 의학 지지자들은 서사 의학이 더 [상호작용적이고 공감적인 의사-환자 참여의 자극]에만 맞추어져 있지 않다고 주장한다. 영화, 음악, 그림, 조각, 문학 등 예술에 대한 노출과 결합된 [자기성찰 연습]의 이득은 아마도 [동료들과 대중들과의 더 좋고 의미 있는 관계] 뿐만 아니라 [더 나은 자아 인식]으로 이어질 것이다.
Narrative medicine educational interventions thus serve as an important means of preparing medical students’ to engage in the shared-decision making process with their patients (Charon 2008; Charon and DasGupta 2011) by increasing their “narrative competence” (Charon 2007). Such interventions aim to help students
- hone their listening and observation skills,
- stimulate their empathic abilities, and
- increase their capacity for reflection and perspective-taking (Marchalik 2017).
In addition, narrative medicine’s supporters contend that it is not only geared toward the stimulation of a more interactive and empathetic doctor-patient engagement; the dividends of a concerted training in self-reflective practices combined with an exposure to the arts—be it film, music, paintings, sculpture, or literature—will supposedly lead to a better sense of self as well as better and more meaningful relationships with one’s colleagues and the public (Charon 2001; 2006; Yu 2017).
꾸준한 연구 결과는 의료 전문가 훈련에서 [서사 기반 의료행위] 사용의 가치를 계속 보여주고 있다. 최근의 체계적인 검토는 이러한 연구의 영향을 종합하고 분석하기 위해 시도되었다. 하이데트 외 연구진(2016)은 콜롬비아의 서사의학 프로그램에 대한 연구보고를 포함한 의료교육의 예술 기반 과정에 대한 체계적인 검토를 통해 이러한 과정이 의대생들의 공감력, 의사소통, 관찰력, 윤리적 추론 능력 향상과 연결될 수 있음을 발견했다. 바버와 모레노-레기자몬의 서사의학 교육에 대한 문헌검토는(2017)은 9개의 연구만을 포함했지만, 그럼에도 불구하고 이들 출판물에서 네 개의 새로운 주제에 대한 증거를 발견했다.
- 의사소통 기술을 강조, 특히 공감 능력 증가
- 개인적이고 전문적인 성장
- 참여 학생들의 즐거움 또는 즐거움
- 숙련된 촉진자가 이끄는 소그룹 환경의 눈에 띄는 교육 구조
A steady output of studies continues to valorize the use of narrative-based practices in the training of health care professionals. Recent systematic reviews have attempted to synthesize and analyze the impact of these studies. Haidet et al.’s (2016) systematic review of arts-based courses in medical education, which included studies reporting on Columbia’s narrative medicine program, found that such courses could be linked to increased empathy, communication, observation, and ethical reasoning skills in medical students. Barber and Moreno-Leguizamon’s (2017) literature review of narrative medicine education included only nine studies, but nevertheless found evidence of four emergent themes in these publications:
- a stress on communication skills, in particular increased empathy;
- personal and professional growth;
- pleasure, or enjoyment on the part of participating students; and
- a noticeable educational structure of small group settings led by skilled facilitators.
저자들은 이러한 보고된 결과의 가치를 인정하면서도 서사의학 교육의 "더 높은 임상적 가치를 확립하기 위한 대규모 자료가 부족하다"고 결론짓는다. 비엘 외 연구진(2017)의 의과대학 교육에서 서술의학에 대한 연구는 이 경우 31개의 관련 출판물을 검토하는 등 그 범위가 더 넓었다. 바버처럼, 저자들은 학생들의 반사적, 공감적, 대인관계적, 사회적 간 능력에 대한 서술적 의학 개입의 가치와 잠재적 이익을 인정하지만, 그들은 "수집된 데이터를 바탕으로, 의학 교육에서 NM[서술적 의학] 접근법의 구조화된 모델이 없다"고 결론짓는다.
While the authors acknowledge the value of these reported results, they conclude that “there is insufficient large-scale data to establish a higher clinical value” (p. 202) of narrative medicine education. Wieżel et al.’s (2017) study of narrative medicine in medical school education was more expansive in its scope, in this case reviewing 31 relevant publications. Like Barber, the authors acknowledge the value and potential benefits of narrative medicine interventions on students’ reflective, empathic, interpersonal, and intersocial capabilities, yet they conclude that “based on the collected data, there is no structured model of NM [narrative medicine] approach in the medical education” (p. 564).
이 연구는 [서사의학을 가르치는 모델]에 대한 문헌에서 사용 가능한 효과의 증거가 무엇인가라는 질문에 대한 포괄적인 답변을 제공함으로써 지속적인 지식 격차를 메우는 것을 목표로 한다.
This study aims to fill a persistent knowledge gap by offering a comprehensive answer to the question: what evidence of effect is available in the literature about models for teaching narrative medicine?
방법들
Methods
우리의 목표는 서사 기반 의학에 대한 이론적 출판물에서 제안된 교육 전략이 보건 교육 환경에 체계적으로 적용되었는지 여부를 확인하는 것이다. 이러한 이유로, 우리의 건강교육 체계적 검토는 임상적 환경이나 비건강교육 환경에서 서사의학 사용을 설명하는 기사가 아니라 의료교육 또는 의료실무자의 지속적인 전문적 발전에 대한 구체적인 서사의학 개입에 대해 보고하는 기사에 초점을 맞출 것이다. 이 검토는 다음의 세 가지 하위 질문에 답하려고 시도할 것이다:
- 첫째, 건강 교육에 서술 기반 의학의 구조화된 모델의 증거가 있는가? 그리고 만약 그렇다면, 그것이 일관되게 적용되고 있는가?
- 둘째, 서술 기반 강의실 개입이 측정 가능한 결과를 초래한다는 증거가 있는가?
- 마지막으로 보고된 결과의 품질과 특성은 무엇입니까?
Our goal is to ascertain whether or not the pedagogic strategies proposed in the theoretical publications about narrative-based medicine were systematically applied in health education settings. For this reason, our health education systematic review (Gordon 2018) will focus on articles that report on specific narrative medicine interventions in medical education or in the continuing professional development of medical practitioners, not on articles that describe the use of narrative medicine in clinical settings or in non-health education settings. This review will attempt to answer the following three sub-questions:
- first, is there evidence of a structured model for narrative-based medicine in health education, and if so, is it consistently applied?
- Second, is there evidence that narrative-based classroom interventions result in measurable outcomes?
- Finally, what is the quality and nature of the reported outcomes?
문헌 검색
Literature search
우리의 체계적인 검토는 두 단계로 실행되었다. 첫째, 우리는 전자 데이터베이스를 검색했고, 둘째, 우리는 서술 의학 관련 주요 저자와 기사를 대상으로 반복적인 검색을 실행했다. 첫 번째 단계의 기사는 다음과 같은 전자 데이터베이스에서 얻었다. PubMed, Medline, Psychinfo, EBSCO 학술 검색 프리미어 및 간호 및 관련 건강 문헌 누적 지수(CINAHL)가 포함되어 있습니다. 별도의 검색 문자열 목록은 부록에서 확인할 수 있습니다. 가장 관련성이 높은 출처를 검색하기 위한 수단으로 제목, 추상 또는 키워드에 "의학" 또는 "의학 기반 의학"이 포함된 기사를 검색했습니다. 또한 1999년에 서술 의학 또는 서술 기반 의학을 개념으로 설명하는 첫 번째 이론적 출판물과 잠재적 강의실 개입이 출판됨에 따라 2000년부터 발행된 논문으로 검색을 제한했다. 검색어에 대한 합의가 이루어지자 한 저자(M.M.)가 2017년 11월 6일 초기 검색을 실행했다. 이 검색은 2018년 5월 31일에 반복되었다.
Our systematic review was executed in two phases: first, we searched electronic databases; second, we ran an iterative search targeting key authors and articles related to narrative medicine. Articles in the first phase were obtained from the following electronic databases: PubMed, Medline, Psychinfo, EBSCO Academic Search Premier, and the Cumulative Index to Nursing and Allied Health Literature (CINAHL). A list of the separate search strings can be found in the Supplementary Appendix; as a means of retrieving the most relevant sources, we searched for articles that included “narrative medicine” or “narrative-based medicine” in the title, abstract, or keywords. We also limited our search to articles published from 2000 onwards as the first theoretical publications describing narrative medicine or narrative-based medicine as a concept and potential classroom intervention were published in 1999. Once we had reached consensus about the search terms, one author (M.M.) ran an initial search on November 6, 2017. This search was repeated on May 31, 2018.
두 번째 단계에서는 컬럼비아 대학의 서사의학 프로그램의 공동 설립자인 Rita Charon, Sayantani Das Gupta Craig Irvine 및 Maura Spiegel을 대상으로 서사의학 강의실 개입에 대한 주요 기사를 별도로 검색했다. 그런 다음 관련 출처를 찾기 위해 이러한 기사의 참조 목록을 검토했다. 우리는 또한 우리의 연구 질문과 관련이 있을 수 있는 추가 기사를 식별하기 위해 서사의학, 공감 및 의학 교육의 예술에 대한 체계적인 리뷰에서 인용된 작품들을 조사했다. 중복을 제거한 뒤 378건의 글이 남았다.
For the second phase, we ran a separate search on PubMed by author, in this case for the co-founders of Columbia University’s Narrative Medicine Program—Rita Charon, Sayantani DasGupta Craig Irvine, and Maura Spiegel—in order to identify key articles about narrative medicine classroom interventions. We then examined the reference lists of these articles for further relevant sources. We also examined the works cited in systematic reviews on narrative medicine, empathy, and the arts in medical education to identify any additional articles that could be relevant to our research questions (Kuper 2006; Batt-Rawden et al. 2013; Cowen 2016; Barber and Moreno-Leguizamon 2017; Wieżel et al. 2017). After removing duplicates, 378 articles remained.
기사선정
Article selection
두 명의 저자(M.M.과 G.V.T.)는 다음과 같은 자격 기준에 기초하여 제목과 요약본을 스캔하여 Cvidence의 전체 텍스트 검토를 위한 관련 기사를 독립적으로 식별했다.
Two authors (M.M and G.v.T.) independently identified relevant articles for full-text review in Covidence by scanning the titles and abstracts on the basis of the following eligibility criteria.
- 포함 기준:
- 학부, 대학원 또는 대학원 수준의 의료 또는 의료 교실 환경에서 서술적 의학 커리큘럼, 과정, 세미나 또는 교수 관행을 설명하는 출판물
- 의료 서비스 제공자를 위한 교수진 개발 전문 개발 개입을 설명하는 연구
- 질적 및/또는 정량적 평가를 통해 교육학적 도구로서 서술적 의학의 영향을 시험하려는 출판물.
- 학부, 대학원 또는 대학원 수준의 의료 또는 의료 교실 환경에서 서술적 의학 커리큘럼, 과정, 세미나 또는 교수 관행을 설명하는 출판물
Inclusion criteria: publications that describe narrative medicine curricula, courses, seminars, or teaching practices in a medical or paramedical classroom setting at the undergraduate, graduate, or postgraduate level; studies describing a faculty development professional development intervention for health care providers; publications that attempt to test the impact of narrative medicine as a pedagogic tool with qualitative and/or quantitative assessment.
- 제외 기준:
- 임상 환경에서 서술적 의학 사용에 대해 보고하는 출판물
- 서술 의학에 대해 이론화하지만 특정 강의실 환경에서 그것의 사용을 설명하지 않는 출판물
- 비의료 환경에서 서술형 의학의 사용을 설명하는 출판물(예: 수의학교)
- 서술적 의학을 교육학적 도구로 명시적으로 언급하고 사용하지 않는 출판물
- 비영어 출판물; 체계적인 문학 평론
- 임상 환경에서 서술적 의학 사용에 대해 보고하는 출판물
Exclusion criteria: publications that report on the use of narrative medicine in a clinical setting; publications that theorize about narrative medicine but do not describe its use in a specific classroom setting; publications that describe the use of narrative medicine in a non-medical setting (for example, veterinary school); publications that do not explicitly mention and use narrative medicine as a pedagogic tool; non-English publications; systematic literature reviews.
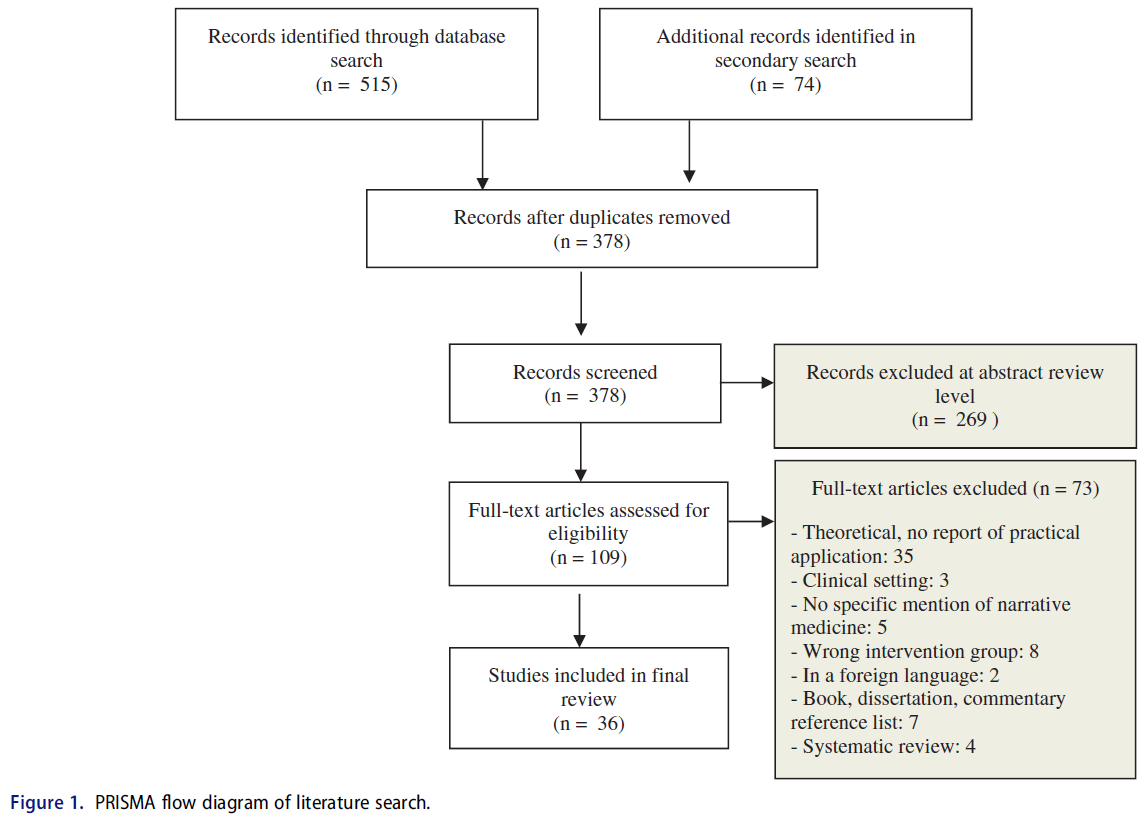
포함 목록을 비교하기 위해 회의를 하고 갈등을 해결한 후, 한 연구원(M.M.)은 자격에 대한 전문 분석을 실시했다. 서사의학 강의실 개입에 대한 총 36개의 연구가 최종 분석에 포함되었다. 그림 1에는 검색 프로세스의 흐름도가 나와 있습니다.
After meeting to compare inclusion lists and resolving any conflicts, one researcher (M.M.) conducted a full-text analysis for eligibility. In total, 36 studies reporting on a narrative medicine classroom intervention were included in the final analysis. Figure 1 contains a flow diagram of the search process.
데이터 추출
Data extraction
한 저자(M.M.)는 전체 텍스트를 검토하고 다음과 같은 일반 정보를 추출했다: 저자, 출판 연도, 강의실 개입 현장, 연구 유형(개입 보고서, 정성 및/또는 정량적 평가 구성요소), 서술 의학 과정 수준 및 분야, 과정 유형(선택, 필수, 교수 개발), 코스 기간 및 참가자 수(참가자 수 포함)에 대해 설명합니다.
또한, 이 추출물은 보고된 서술 의학 과정 내용의 더 자세한 측면을 기록했습니다. 여기에는 다음이 포함됩니다. 코스 자체에 사용된 공식 및 비공식 평가 도구(예: 동료 피드백 또는 의사-작가 및 전문가와의 글쓰기 워크샵 세션)뿐만 아니라 코스에 사용된 특정 예술 형식 또는 이론적 텍스트, 특정 쓰기 과제, 공식 및 비공식 평가 도구 마지막으로, 추출은 또한 교육학적 개입에 대한 정성적 및/또는 정량적 평가를 포함하는 연구에서 보고된 방법, 목표 및 결과를 기록하였다.
One author (M.M.) reviewed the full texts and extracted the following general information: authors, year of publication, site of classroom intervention, type of study (report of intervention, qualitative and/or quantitative assessment component), the narrative medicine course level and field, type of course (elective, required, faculty development), the duration of course, and the number of participants, if mentioned.
In addition, the extraction recorded more detailed aspects of the reported narrative medicine course content. This included: specific art forms or theoretical texts used in the course, specific writing assignments as well as formal and informal assessment tools used in the course itself (for example, peer feedback or writing workshop sessions with a physician-writer and expert). Finally, the extraction also recorded the methods, objectives, and outcomes reported in the studies that included a qualitative and/or quantitative assessment of a pedagogic intervention.
증거 등급
Evidence grading
서술형 의학 강의실 개입의 결과를 평가하려고 시도한 연구는 Kirkpatrick 기반 결과 척도 및 증거 척도를 모두 포함하는 BEME(Best Evidence in Medical Education) 글로벌 평가 척도를 사용하여 평가되었다. Kirkpatrick 모델은 원래 기업 조직의 교육 프로그램을 평가하는 수단으로 고안되었으며, 의료 교육을 포함한 고등 교육(Praslova 2010)에서 프로그램의 효과를 측정하는 표준 도구가 되었다. BEME 글로벌 척도는 표 1에서 확인할 수 있습니다.
Studies that attempted to assess the outcomes of a narrative medicine classroom intervention were rated using the Best Evidence in Medical Education (BEME) Global Rating Scale, which includes both a Kirkpatrick-based outcomes scale and a strength of evidence scale (Hammick et al. 2010). Originally conceived as a means of assessing training programs in business organizations (Kirkpatrick 1959, 1976, 1996), the Kirkpatrick model has become a standard tool for gauging the effectiveness of programs in higher education (Praslova 2010) including medical education (Issenberg et al. 2005; Littlewood et al. 2005; Steinert et al. 2006; Colthart et al. 2008; Tochel et al. 2009; Sullivan 2011). The BEME Global Scale can be found in Table 1.

데이터 추출을 완료한 후 한 작성자(M.M.)는 BEME Global Scale을 사용하여 포함된 기사를 코드화했습니다. 이 단계가 완료되면 두 번째 작성자(G.V.T.)는 무작위로 선택된 5개의 기사에 대한 독립적인 채점을 완료했다. 그 후 두 저자는 그들의 점수를 비교하고 의견 차이를 해결하기 위해 만났다. 보충 표 2는 증거와 결과 점수의 BEME 강도뿐만 아니라 데이터 추출의 핵심 정보를 제공한다.
After completing the data extraction, one author (M.M.) coded the included articles using the BEME Global Scale. Once this step was completed, a second author (G.v.T.) completed an independent grading of 5 randomly selected articles. The two authors then met to compare their scores and resolve disagreements. Supplementary Table 2 provides key information from the data extraction as well as the BEME strength of evidence and outcome scores.
결과.
Results
서사기반 의료 개입을 위한 구조화된 모델의 증거
Evidence of structured model for narrative-based medicine interventions
보건 교육에서 서술 의학에 대한 이론적 출판물은 일반적으로 세 가지 기본 단계로 구성된 교육학적 전략을 설명한다.
- 첫 번째 단계는 환자 내러니트, 문학 텍스트, 영화 단편, 예술 작품 또는 음악 작품과의 [성찰적 참여]를 포함한다. 컬럼비아의 내러티브 메디컬 프로그램에서 이 단계는 특정 형태의 예술을 [자세히 읽거나 비판적으로 분석하는 것]을 포함하며, 그들의 내러티브 의학 강의실에서 대표적인 방법으로 여겨진다.
- 이 참여 동안 얻은 통찰력은 [관련된 쓰기 과제 또는 개인적인 성찰]을 통해 교육학적 전략의 두 번째 단계에서 강화된다.
- 만남은 세 번째 단계에서 더욱 풍성해지는데, 이것은 이러한 [작은 자기 성찰 행위들을 공유하고 토론하는 것]으로 구성되어 있다.
Theoretical publications about narrative medicine in health education typically describe a pedagogic strategy consisting of three basic steps.
- The first step involves a reflective engagement with a patient narrative, literary text, film fragment, art work, or piece of music. At Columbia’s Narrative Medicine Program, this step includes a close reading—or critical analysis—of the art form and is considered the signature method in their narrative medicine classrooms (Charon, DasGupta, et al. 2016, p. 181).
- The insights gained during this engagement are reinforced in the second step of the pedagogic strategy by means of a corresponding writing assignment or personal reflection.
- The encounter is further enriched in the third step, which consists of sharing and discussing these small acts of self-reflection (Balmer and Richards 2012, p. 2).
다시 말해서, [서사의학 강의실 개입]은
- 예술 형태나 서사를 만나거나 분석하고,
- 이 만남을 성찰하고,
- 주의 깊게 관찰되고 뒷받침되는 환경에서 자신의 발견을 다른 사람들과 공유하는 것을 포함한다.
In other words, a narrative medicine classroom intervention entails
- encountering and/or analyzing an art form or narrative,
- reflecting upon this encounter, and
- sharing one’s discoveries with others in carefully monitored and supportive environment (Charon, DasGupta, et al. 2016).
본 검토에서 서사의학을 교육학적 도구(N = 36)로 사용하는 것에 대해 보고한 연구들 중, (밀접한) 읽기-반성-응답의 3단계 과정의 증거는 대부분의 기사(N = 22)에서 찾을 수 있다. 소수의 과정에서는 성찰적 글쓰기와 토론만 포함했습니다(N = 12). 극소수는 서면 반영(N = 2)을 포함하지 않았다.
Of the studies in this review that reported on their use of narrative medicine as a pedagogic tool (N = 36), evidence of this three-step process of (close) reading-reflecting-responding could be found in the majority of the articles (N = 22). A minority of courses only included reflective writing and discussion (N = 12). A very small minority did not include written reflection (N = 2).
측정 가능한 결과의 증거
Evidence of measurable outcomes
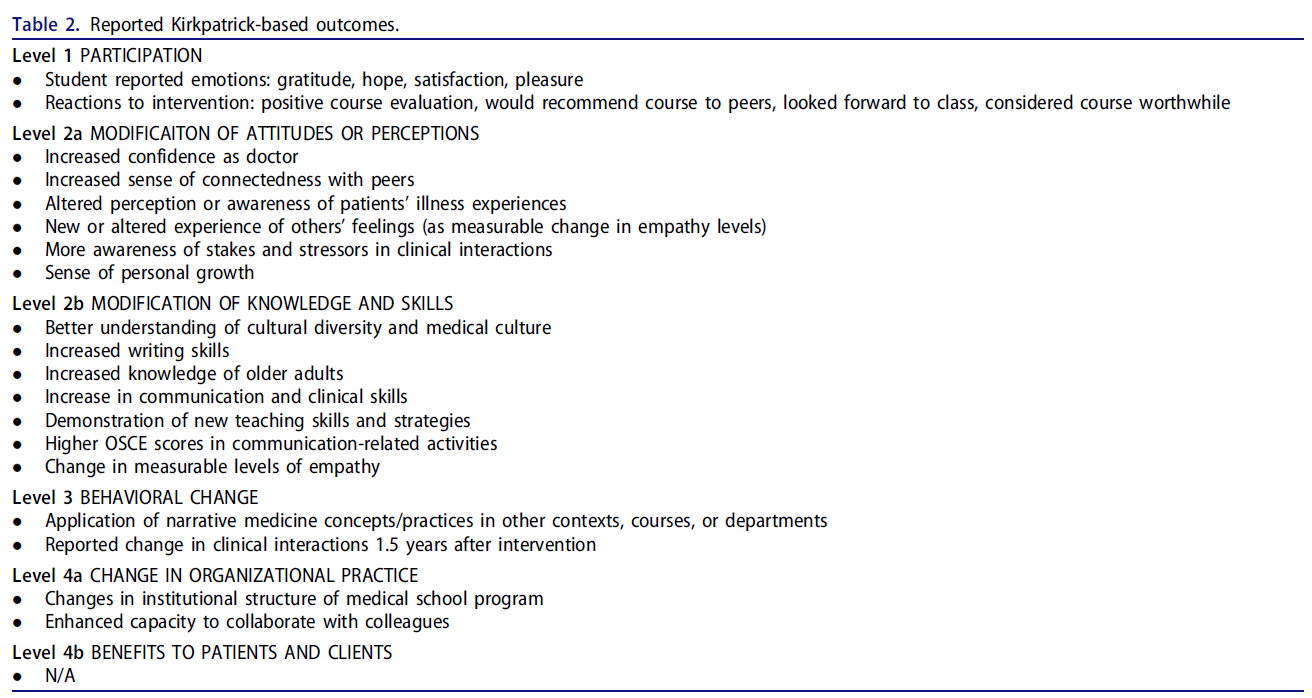
이 검토에서 23개의 연구는 그들의 서술적 의학 교실 개입의 영향을 평가했다. Kirkpatrick 모델에 따라 분류된 연구 결과의 간략한 요약은 표 2에서 확인할 수 있다. 이러한 연구의 측정 및 결과에 대한 자세한 설명은 부록에서 확인할 수 있다.
In this review, 23 studies assessed the impact of their narrative medicine classroom interventions; a brief summary of the findings categorized according to the Kirkpatrick model can be found in Table 2. A detailed description of the measures and outcomes of these studies can be found in the Supplementary Appendix.
1단계: 참여
Level one: participation
대부분의 연구에는 1단계 또는 2단계 평가가 포함되었다. 수준 1 결과 측정치(N = 14)를 포함하는 연구는 성과척도로서 조사 또는 피드백 양식에 압도적으로 의존했지만 서사의학, 개입 자체에 대한 긍정적인 학생 반응과 감사, 희망, 만족 또는 기쁨과 같은 긍정적인 효과를 보고했다.
The majority of the studies included level one or two assessments. Studies that included level one outcome measures (N = 14) overwhelmingly relied on surveys or feedback forms as outcome measures but reported positive student reactions to the narrative medicine interventions themselves (Winkel 2010; Ross 2014) and positive effects, such as a sense of gratitude, hope, satisfaction, or pleasure (DasGupta and Charon 2004; Feigelson and Muller 2005; Garrison 2011; Chretien 2015).
2단계: 태도, 인식, 지식 또는 기술의 수정
Level two: modification of attitudes, perceptions, knowledge, or skills
예를 들어, 참가자들의 태도나 인식의 변화에 대해 보고한 연구들(레벨 2a; N = 16)은 그들의 동료들과 더 넓은 전문 커뮤니티에 대한 정체성 증가, 그들의 일에 대한 더 많은 만족과 웰니스 감각, 또는 문화적 다양성에 대한 더 나은 인식을 발견했다. 임상실습 3학년 학생들을 위한 서사의학 환자 스토리텔링 과정에 대한 크레티엔의(2015) 평가 연구는 예시적인 예를 제공한다. 그 과정 동안, 학생들은 환자를 인터뷰하고, 그들의 인터뷰를 서술형으로 쓰고, 그들의 인터뷰 대상자들과 이 쓰여진 작품을 공유해야 했다. 강의가 끝난 후 포커스 그룹과 학생과 참여 환자 모두를 대상으로 한 인터뷰가 진행됐다. 학생들은 이 연습을 통해 다음을 했다고 보고했다
- 환자로부터 질병 이상의 것을 발견하는데 도움을 주었고,
- 천천히 듣고 들을 수 있는 기회를 갖도록 더 개방적으로 만들었으며,
- 이야기들이 환자 치료에 긍정적인 영향을 미칠 수 있다는 것을 확실히 보여주었다.
Studies that reported on modification of participants’ attitudes or perceptions (level 2a; N = 16) found, for example,
- increased identification with their peers and the broader professional community (Feigelson and Muller 2005; Balmer and Richards 2012; Al-Imari et al. 2016),
- more satisfaction with their work and sense of wellness (Feigelson and Muller 2005; Graham 2009), or
- a better awareness of cultural diversity (DasGupta et al. 2006).
Chretien’s (2015) assessment study of a narrative medicine patient storytelling course for third-year medical clerkship students provides an illustrative example. During the course, students had to interview patients, write up their interview as a narrative, and share this written work with their interviewees. Focus groups and interviews with both students and participating patients were conducted after the course was completed. Students reported that the exercise
- helped them discover that patients are more than their disease,
- made them more open to taking the opportunity to slow down and listen, and
- made clear to them that stories can positively impact patient care.
상당수의 연구는 또한 서사의학 개입의 직접적인 결과로 지식이나 기술의 수정을 평가했다(수준 2b; N = 14). Liben(2012)은 서사의학 워크숍의 교수진 참가자들이 후속 테스트에서 서사적 용어 습득을 입증하고 나중에 이러한 서사의 기술을 교육 및 임상 환경에 적용했다고 보고했다. 마찬가지로, Ross(2014)는 서사의학 과정(평균 점수 51.6–71.5, p < 0.001)을 완료하기 전후에 실시한 서사적 기술 평가에서 유의미한 향상을 기록했다. 커닝햄(2018)은 학생들이 자신의 서술적 성찰에서 다음과 같은 주제를 다루었다는 것을 발견했다: 자기 인식, 공감, 정서적 거리와 연민의 균형. 다른 연구들은 의사소통에 대한 이해와 능력이 향상되었다고 보고했다.
A considerable number of studies also assessed the modification of knowledge or skills as a direct result of the narrative medicine intervention (level 2b; N = 14). Liben (2012) reported that faculty participants in a narrative medicine workshop demonstrated the acquisition of narrative terms in a follow-up test and later applied these narrative skills in teaching and clinical settings. Similarly, Ross (2014) recorded significant improvement in a narrative skills assessment administered before and after the completion of a narrative medicine course (mean scores 51.6–71.5, p < 0.001). Cunningham (2018) found that students addressed the following themes in their written narrative reflections: self-awareness, empathy, and balancing emotional distance and compassion. Other studies reported an enhanced understanding of and capability in communication (Garrison 2011; Arntfield et al. 2013; Welch 2016).
많은 연구들은 학생들이 그들의 환자에 대한 공감과 연결성을 증가시켰다고 보고했다. Sands(2008)는 또한 baseline에 비해서 Interpersonal Reactivity Index를 사용한 개입 후 평가에 따라 공감적 관심empathic concern의 개선을 발견했다. 하지만, 서사의학 개입 전후에 공감 수준을 평가하려는 모든 시도가 긍정적인 결과를 가져온 것은 아니다. 서사의학 세미나 세션에 참석하면 번아웃을 줄이고, 공감 능력을 높이고, 반사 능력을 높이고, 주민들이 업무에서 접하는 다중 스트레스 요인을 처리하는 데 도움이 될 것이라는 윙클 외(2016)의 가설을 Maslach Burnout Inventory, Interpersonal Reactivity Index 및 Self-Care Inventory를 통해 검증하였으며, 참가자가 서술 의학 세미나를 마친 후 1년 후 기준에서 시행하였다. 그 결과에서, 서사의학 개입 이후 공감적 관심이 약간 증가했다고 보고했습니다(+0.76, p = 0.01). 그러나 전체 수준에서 저자들은 번아웃 수준은 높은 수준을 유지했지만 점수에서 큰 차이를 발견하지 못했다.
A number of studies reported that students had an increased sense of empathy for and connection to their patients (DasGupta and Charon 2004; Maurer 2006; Vannatta and Vannatta 2013; McDonald 2015). Sands (2008) also found an improvement in empathic concern (p = 0.056) according to baseline and post-intervention assessments using the Interpersonal Reactivity Index. This being said, not all attempts to assess empathy levels before and after a narrative medicine intervention resulted in positive results. Winkel et al.’s (2016) hypothesis that attending narrative medicine seminar sessions would reduce burnouts, enhance empathy, increase reflective capabilities, and help residents process the multiple stressors the encountered on the job, was tested by means of a Maslach Burnout Inventory, Interpersonal Reactivity Index, and Self-Care Inventory administered at the baseline and one year after participants’ completion of the narrative medicine seminars. The study reported a small increase in empathic concern after the narrative medicine intervention (+0.76, p = 0.01). Yet at the aggregate level, the authors found no significant difference in scores, although burnout levels remained high.
3단계: 행동 변화
Level three: behavioral change
이 검토에 포함된 세 가지 연구는 서술 기반 의학 개입의 결과로 행동 변화를 명시적으로 측정하기 위한 시험을 설계하고 실행했다. 이러한 연구에는 여러 측정 도구가 포함되었으며 세 가지 중 두 가지에는 데이터 삼각측량이 포함되었다. Bhavarju는 서사의학 교수 훈련 개입의 영향을 평가하기 위해 사전 및 사후 리커트 척도 설문지를 사용하여
- 쓰기 및 쓰기 연습 리딩에 대한 자신감 향상(3.1–4.2)과
- 독서토론 리딩에 대한 높아진 자신감(3.7–4.4)을 확인했다. 참가자들은 또한
- 강의에 서사의학 도구를 통합한다(2.0–2.7)고 보고했다.
Three studies included in this review designed and executed tests to explicitly measure behavioral change as a result of a narrative-based medicine intervention (Balmer and Richards 2012; Arntfield et al. 2013; Bhavaraju and Miller 2014). These studies included multiple measurement tools and two of the three included data triangulation (Balmer and Richards 2012; Arntfield et al. 2013). Using pre- and post-intervention Likert Scale questionnaires to assess the impact of a narrative medicine faculty training intervention, Bhavaraju found an
- increase in participants’ confidence in writing and leading writing exercises (3.1–4.2) and
- increased confidence in leading literary discussions (3.7–4.4). Participants also reported
- integrating narrative medicine tools in their teaching (2.0–2.7).
발머의 교수 교육 프로그램 분석은 전문적 성장(교습 전략 학습, 여러 과정에 이러한 전략 적용), 개인적 성장(관점 수용), 집단적 및 공동적 지원의 증거를 발견했다. (다른 사람, 소속감, 그리고 풍부한 연결감을 봅니다.) Arntfield의 학부 서사의학 선택과목 평가는 3가지 데이터 수집 및 분석 수단을 사용했다. 즉, 개입 전 익명 조사, 포커스 그룹, 개입 후 1.5년 후 추적 조사이다. 따라서 이 연구의 결과는 Kirpatrick 모델의 여러 수준으로 분류될 수 있지만, 참가자들은 커뮤니케이션에 대한 이해와 능력의 향상 형태로 행동 변화를 보고했다.
Balmer’s analysis of a faculty training program found evidence of professional growth (learning teaching strategies, applying these strategies to multiple courses), personal growth (perspective taking), and collective and communal support (seeing the “other,” affiliation, and a sense of rich connectedness). Arntfield’s assessment of an undergraduate narrative medicine elective course used three means of data collection and analysis: an anonymous pre-intervention survey, a focus group, and a follow-up survey 1.5 years after the intervention. The outcomes of this study could thus be categorized on multiple levels of the Kirpatrick model, but participants reported behavioral changes in the form of enhanced understanding of and capability in communication.
레벨 4: 조직 관행 또는 환자 상호 작용의 변화
Level four: change in organizational practice or patient interaction
임상 기술 개발에 대한 서술적 의학 강의실 개입의 장기적인 결과를 측정하기 위한 두 가지 연구가 시도되었다. 조직 관행의 변화와 관련하여, Arntfield의 연구 참가자들은 [(환자의 관점에 대한 개선된 인식이란 형태로) 더 나은 치료 전달]을 보고하였다. 발머의 연구의 목표는 진행 중인 [프로세스-지향 서사의학 교수개발 프로그램]이 참가자들에게 미치는 영향을 탐구하는 것이었다. 그리고 저자들은 그들의 의도가 개인 개입 자체를 평가하는 것이 아니라, [대인 관계와 제도적 관행의 진화하는 변화를 살펴보는 것]이라고 명시적으로 말했다. 이 연구는 교수진 개발 프로그램의 참가자들이 나중에 컬럼비아의 새로운 커리큘럼의 규범과 관행을 형성하는 데 도움을 주었다고 결론지었다. 두 연구 모두 교수세미나의 영향에 대한 분석에서 질적 방법만을 사용했지만, 그럼에도 불구하고 참여자들은 [서사의학적 실천을 더 많이 포함하도록 대학의 의과대학 커리큘럼을 형성]하는 데 결정적이고 측정 가능한 수단hand을 가지고 있다고 확신했다.
Two studies attempted to measure the long-term results of a narrative medicine classroom intervention on clinical skill development (Balmer and Richards 2012; Arntfield et al. 2013). Regarding changes in organizational practice, participants in Arntfield’s study reported better delivery of care in the form of a better awareness of patients’ perspectives. The goal of Balmer’s study was to explore the impact of an ongoing, process-oriented narrative medicine faculty development program on participants, and the authors explicitly stated that their intention was to look at evolving changes in interpersonal relationships and institutional practices, not to assess the individual interventions themselves. The study concluded that the participants in the faculty development program later helped shape the norms and practices in Columbia’s new curriculum. Both studies used solely qualitative methods in their analyses of the impact of the ongoing faculty seminars but were nevertheless confident that those who participated had a decisive and measurable hand in shaping the university’s medical school curriculum to include more narrative medicine practices.
증거품질
Quality of evidence
이 연구에 포함된 소수의 출판물(N = 13)은 개입의 결과를 평가하려고 시도하지 않았으며, 대신 서사의학 수업을 위한 교육 도구 개발에 대한 보고를 선택했다. 예로는 작업장 테마 및 설계(DasGupta 2003) 또는 학생 및 교직원 피드백 가이드에 대한 설명이 있습니다. 이 문서들은 비공식적인 증언 증거나 저자들의 개인적인 의견을 포함하고 있기 때문에, 그들은 오직 1의 BEME 증거 점수만을 수여받을 수 있었다.
A minority of publications included in this study (N = 13) did not attempt to assess the outcomes of their intervention, choosing instead to report on their development of pedagogic tools for the narrative medicine classroom. Examples include descriptions of workshop themes and designs (DasGupta 2003) or student and faculty feedback guides (Wald 2010; 2011; Charon, Hermann, et al. 2016). As these articles included informal testimonial evidence or the authors’ personal opinions, they could only be awarded a BEME strength of evidence score of 1.
나머지 논문의 대부분(N = 16)을 2로 채점했는데, 이는 일반적으로 표본 크기가 작거나 하나의 평가 도구만 사용되었기 때문에 결과가 모호하다는 것을 의미한다. BEME 척도에서 5개의 연구를 3점 만점으로 채점했는데, 이는 이러한 연구의 결론이 결과와 연관될 가능성이 높다는 것을 의미한다. 단 하나의 연구만이 4점을 채점했는데, 이는 결과가 분명하고 사실일 가능성이 높다는 것을 의미한다. 우리의 평가에 따르면, 이 체계적인 검토에 포함된 어떤 연구도 명확한 결과를 제공하지 않았다.
We scored the majority of the remaining articles (N = 16) with a 2, meaning that the results were ambiguous, usually because of the small sample size or the fact that only one assessment tool was used. We scored five studies as a 3 on the BEME scale, meaning that conclusions in these studies could likely be linked to the results; only one study scored a 4, meaning the results were clear and likely to be true. According to our appraisal, none of the studies included in this systematic review provided unequivocal results.
논의
Discussion
이 체계적 검토는 다음의 세 가지 하위 질문에 대한 답변을 시도했다.
- 첫째, 교육에서 서술 기반 의학의 구조화된 모델의 증거가 있는가?
- 둘째, 서술 기반 강의실 개입이 측정 가능한 결과를 초래한다는 증거가 있는가?
- 마지막으로 보고된 결과의 품질과 특성은 무엇입니까?
This systematic review attempted to answer the following three sub-questions:
- first, is there evidence of a structured model for narrative-based medicine in education?
- Second, is there evidence that narrative-based classroom interventions result in measurable outcomes?
- Finally, what is the quality and nature of the reported outcomes?
교육학적 접근 방식의 일관성
Consistency in pedagogic approach
우리의 검토는 서술 기반 보건 교육 개입에 대한 일관되고 복제 가능한 방법론과 교육학적 접근법의 명확한 증거를 발견했다. 기사에 설명된 세미나나 강좌는 거의 항상 읽기-성찰-응답read-reflect-respond의 동일한 3단계 모델을 따른다.
사실, 마지막 단계(응답/응답)는 이 연구에 포함된 모든 기사에 포함되었습니다. 특히 성찰 운동은 중요한 전문적 기술인 [임상추론]과 직접적으로 연결될 수 있다. Maurer(2006)가 설명했듯이, 성찰 연습은 학생들이 자신의 경험과 편견의 원천을 포함한 광범위한 정보를 처리하도록 훈련시킴으로써 학생들의 임상 추론 기술을 촉진하고 개선할 수 있다.
Our review found clear evidence of a consistent and replicable methodology and pedagogic approach for narrative-based health education interventions. The seminars or courses described in the articles almost always followed the same three-step model of read-reflect-respond; in fact, the last step (response/discussion) was present in all of the articles we included in this study. The reflective exercises, in particular, can be directly linked to an important professional skill: clinical reasoning. As Maurer (2006) describes, reflective exercises can promote and refine students’ clinical reasoning skills by training them to process a wide range of information, including their own experiences and sources of bias.
측정 가능한 결과의 차이
Variance in measurable outcomes
BEME Global Scale의 증거 강도와 Kirkpatrick 기반 결과를 사용하여 평가되는 학습 유형과 결과의 품질을 코드화함으로써, 우리는 교육학적 전략으로서 서술 의학에 대한 더 넓은 관점을 취할 수 있었다. 이 검토에 포함된 연구의 우세성은 Kirkpatrick의 처음 두 가지 결과 수준(참여, 태도나 인식의 수정, 지식과 기술의 수정)에 대해 보고했는데, 아마도 이 두 수준이 테스트와 설문조사를 통해 평가하기가 더 쉽기 때문일 것이다. 그러나 이러한 연구는 두 가지를 시사한다.
- 첫째, 이 학생들은 과정 설계자에 의해 요약된 서술적 의학의 목표와 목적에 따라 기술을 배웠다.
- 둘째, 이 학생들은 그들이 수강한 과정의 목표와 목적을 의식한다.
By using the BEME Global Scale strength of evidence and Kirkpatrick-based outcomes to code the type of learning being assessed and the quality of the results, we were able to take a broader view of narrative medicine as a pedagogic strategy. The preponderance of studies included in this review reported on Kirkpatrick’s first two outcome levels (participation, modification of attitudes or perceptions, and modification of knowledge and skills), probably because these two levels are easier to assess with tests and surveys. Still, these studies indicate two things:
- first, these students have learned skills in accordance with the goals and purpose of narrative medicine as outlined by course designers;
- second, these students are conscious of the goals and purpose of the course they have taken.
이 검토의 연구는 선택 과목과 필수 과목 모두에 대해 보고했지만, 서사의학 과목을 적극적으로 선택한 학생들은 과목의 목적과 내용에 더 긍정적인 경향이 있었을 수 있다는 점에 주목할 필요가 있다. 유념해야 할 또 다른 포인트는 포함된 연구의 참여자 수가 적었다는 것이다. 이는 서사의학 활동이 소규모 그룹 환경에 가장 적합하다는 사실에 기인한다. 그럼에도 불구하고, 이것은 의과대학 프로그램에서 서술형 의학의 광범위한 통합을 주장하기 더 어렵게 만든다.
While the studies in this review reported on both elective and required courses, it is worth noting that students who actively chose to take a narrative medicine course may have been more positively predisposed to the course aims and content. Another point to keep in mind is that the number of participants in the included studies was low; this is arguably due to the fact that narrative medicine activities are best suited to small group settings. Nevertheless, this makes it more difficult to argue for the broader integration of narrative medicine in medical school programs.
증거의 강도의 차이
Variance in strength of evidence
증거의 강도가 항상 이상적인 것은 아니지만, 서사의학 개입의 결과를 평가하려고 시도한 연구는 거의 전적으로 긍정적인 결과를 측정할 수 있었다. 결과가 대수롭지 않거나 심지어 부정적이었던 사람들은 겉으로 보기에 예상치 못한 결과에 대해 상세한 설명을 해주었다. 예를 들어, Winkel 외(2016)와 Liu 외(2016)는 태도나 인식의 작은 변화, 심지어 부정적인 변화에 대한 잠재적 설명으로 과중한 작업량, 스트레스, 피로, 그로 인한 직업에 대한 환멸과 같은 개입 요인을 들었다. 많은 미국 의과대학과 레지던트 프로그램의 스트레스와 집중적인 특성 때문에, 우리는 이러한 설명들이 타당하다는 것을 알았다.
While the strength of the evidence was not always ideal, the studies that attempted to assess the outcomes of a narrative medicine intervention were able to measure almost exclusively positive outcomes. Those whose results were insignificant or even negative provided detailed explanations for the seemingly unexpected outcomes. For example, Winkel et al. (2016), and Liu et al. (2016) cited intervening factors like heavy workloads, stress, fatigue, and a resulting disillusionment with the profession as potential explanations for the small, even negative, modifications in attitudes or perceptions. Due to the stressful and intensive nature of many American medical school and residency programs, we found these explanations reasonable.
이 검토의 장점과 단점
Strengths and weaknesses of this review
우리 연구에 포함된 기사에 보고된 결과는 유망하지만, 편향의 핵심 원천인 연구의 위치를 다룰 필요가 있다. 보고된 36개의 서사의학 과정 또는 세미나 중 89%(N = 32)가 미국에서 수행되었으며, 이 중 36%(N = 13)가 컬럼비아 대학교에서 유래되었다. 첫눈에, 이것은 콜롬비아나 미국을 바깥에서 이 교육학 도구의 전이가능성에 대한 우려를 불러일으킬 수 있다. 하지만, 우리가 BEME 증거 등급의 강도에 대해 3점 또는 4점을 받은 6개의 연구 중, 단지 3점만이 컬럼비아에서 유래되었습니다. 다른 세 가지 연구는 미국과 캐나다의 다른 대학에서의 개입에 대해 보고했다. 게다가, 아마도 더 많은 교육자들이 그것의 목표와 구현 수단에 대해 알게 되면서, 시간이 지남에 따라 비 콜롬비아 출판물의 증가를 볼 수 있다. 2003년과 2010년 사이에 발표된 이 검토에 포함된 11개 연구 중 55%(N = 6개)가 컬럼비아 출신이었고, 대조적으로 2011년부터 2018년까지 발표된 25개 연구 중 28%(N = 7개)만이 컬럼비아 출신이었다. 서술적 의학 교육 개입에 대한 국제 출판물들의 보도와 함께 유사한 패턴이 나타날지는 두고 봐야 한다.
While the results reported in the articles included in our study are promising, a key source of bias needs to be addressed: the location of the studies. Of the 36 reported narrative medicine courses or seminars, 89% (N = 32) were conducted in the United States and 36% (N = 13) of these originated from Columbia University. At first sight, this may raise concerns about the transferability of the pedagogic tools beyond Columbia or the US. However, of the six studies that we scored a 3 or 4 on the BEME strength of evidence scale, just three originated from Columbia. The other three studies reported on interventions at other universities in the US and Canada. Furthermore, one can see an increase in non-Columbia publications over time, presumably as more educators learned about its goals and means of implementation. Of the 11 studies included in this review that were published between 2003 and 2010, 55% (N = 6) were from Columbia; in contrast, of the 25 studies published from 2011 to 2018, just 28% (N = 7) were from Columbia. It remains to be seen whether or not a similar pattern will emerge with international publications reporting on narrative medicine educational interventions.
비엘 외 연구진(2017)과 바버와 모레노-레기자몬 연구진(2017)은 체계적인 리뷰에 따르면, [의대 개입의 맥락에서 명확한 서사의학 방법론을 찾을 수 없었다]고 결론짓는다. 우리의 연구는 그 반대라는 것을 보여줍니다. 이러한 변화는 우리 연구에서 장점을 구성하는 두 가지 요인의 결과일 수 있다. 첫째, 우리의 평가 방법인 BEME 글로벌 등급 척도는 보고된 결과에 대한 보다 미묘한, 투명한 분석을 용이하게 했다. 둘째, 우리의 체계적인 검토는 바버의 9개 기사 중 3개 기사만 중복되고 27개 기사 중 8개 기사만 중복되는 등 더 크고 다른 연구 세트를 산출했다. 우리가 BEME에게 가장 높은 증거 점수를 준 6개의 기사 중, 오직 3개만이 비엘의 연구에 포함되었고 1개는 바버의 연구에 포함되었다.
Wieżel et al. (2017) and Barber and Moreno-Leguizamon’s (2017) conclude in their systematic reviews that they could find no clear narrative medicine methodology in the context of medical school interventions; our study indicates the opposite. This variation can be the result of two factors, both of which constitute strengths in our study. First, our method of assessment, the BEME Global Rating Scale, facilitated a more nuanced and transparent analysis of the reported outcomes. Second, our systematic review yielded a larger and different set of studies, with only three overlapping articles out of Barber’s nine included articles and just 8 overlapping articles out of Wieżel’s 27 included articles. Of the six articles that we gave the highest BEME strength of evidence scores, only three of were included in Wieżel’s study (Arntfield et al. 2013; Bhavaraju and Miller 2014; Chretien 2015) and one in Barber’s (Chretien 2015).
우리는 서사기반 의학 개입이 의대생들에게 긍정적이고 측정 가능하며 복제 가능한 영향을 미치며 의대생의 전문적이고 개인적인 발전을 자극하는 의미 있는 도구가 될 수 있다고 결론짓는 것이 타당하다고 생각한다. 이 검토에 포함된 연구는 또한 이러한 개입이 자기 성찰과 공감을 자극할 수 있으며 학생들이 다른 관점이나 각도에서 환자에 대해 생각할 수 있도록 도와줌으로써 의사와 환자 관계에 대한 개념을 수정하는 데 도움이 될 수 있음을 나타낸다. 그러나 서사의학 수업 개입의 장기적 영향을 검증하기 위한 종단적 연구가 없다면, 우리는 서술적 의학 개입이 미래에 더 참여적이고 공감적이며 궁극적으로 효과적인 의료 전문가로 귀결될 것이라고 분명하게 결론 내릴 수 없다.
We consider it reasonable to conclude that narrative-based medicine interventions have a positive, measurable, and replicable effect on medical students and could constitute a meaningful tool to stimulate medical students’ professional and personal development. The studies included in this review also indicate that such interventions can stimulate self-reflection and empathy and that they can help students think about their patients from a different perspective or angle, thus helping them revise their notions about the doctor-patient relationship. Yet without longitudinal studies to verify the long-term impact of narrative medicine classroom interventions, at this point, we cannot unequivocally conclude that narrative medicine interventions will result in more engaged, empathic, and ultimately effective medical professionals in the future.
결론들
Conclusions
컬럼비아의 서사의학 프로그램의 설립자들은 "서사에 진입하는 것, 그리고 세계에 대한 자신의 관점을 바꾸는 것이 (서사의학) 교육의 핵심"이라고 주장한다(Charon et al., p. 147 서사의학의 경우, 훈련의 이점은 세 가지가 되어야 한다.
- 환자의 관점을 드러내며,
- 자기 성찰을 촉진하며,
- 동료들 사이에 정서적 지원을 제공하는 수단이어야 한다.
다시 말해서, 그 결과는 나중에 의료 전문가들이 자신에 대한 인식, 그들의 감정과 행동에 의미 있게 성찰할 수 있는 능력, 동료들과의 관계, 그리고 환자들과의 상호 작용 속에서 명확하게 드러나야 한다.
The founders of Columbia’s narrative medicine program claim that “to enter a narrative and have one’s perspective of the world altered is at the heart” of the pedagogic practice (Charon et al. 2016, p. 147). In the case of narrative medicine, the benefits of the training should be threefold:
- to reveal patients’ perspectives,
- to facilitate self-reflection, and
- as a means of providing emotional support amongst colleagues (Holmgren et al. 2011, p. 261).
In other words, the results should later be apparent in medical professionals’ awareness of themselves, in their ability to reflect meaningfully upon their emotions and actions, in their relationships with their colleagues, and in their interactions with their patients.
이 연구의 기사들은 서술 의학은 앞서 언급한 두 범주(—더 미묘한 환자 관점과 더 큰 자기 성찰 능력—)에서 긍정적인 결과를 이끌어 낼 수 있다고 주장해 왔다. 그러한 개입의 장기적 영향이 환자에 의해 느껴지는지 또는 그러한 개입이 환자 치료에 긍정적인 영향을 미치는지는 여전히 불분명하다. 서사의학의 기본 목표 중 하나가 정말로 겸손, 개방, 공감으로 환자의 이야기에 접근하는 것이라면, 이러한 목표들을 교실 환경에서 임상적 만남으로 옮기는 것은 더 많은 연구와 가치 발현을 할 가치가 있다. 다시 말해서, 서사의학의 이상적 실천과 실제 실천 사이의 격차에 대한 더 많은 연구가 필요하다. 매일매일 환자를 진료할 때, [서사의학 수업에서 가르친 해석과 성찰의 기술]이 졸업 후 실제로 학생들에 의해 구현되는지, 어떻게, 그리고 어느 정도까지 구현되는지를 봐야 한다.
While the articles in this study have argued that narrative medicine can lead to positive results in the first two aforementioned categories—more nuanced patient perspectives and a greater capacity for self-reflection—it is still unclear whether the long-term impact of such interventions are felt by patients, or whether such interventions positively impact patient care. If one of the cornerstone goals of narrative medicine is indeed to approach a patient’s story with humility, openness, and empathy (Yu 2017), the transfer of these goals from the classroom setting to the clinical encounter deserves further study and valorization. In other words, more research into the gap between the ideal and real practice of narrative medicine is needed to determine if, how, and to what extent the skills of interpretation and reflection taught in the narrative medicine classroom are actually implemented by students after graduation when they engage with patients in their everyday practice.
이 검토가 시사한 바와 같이, 교육학적 개입으로서의 서사의학은 일관되게 복제 가능한 도구와 전략을 가지고 있다. 그리고, 서사기반 접근법의 목표와 미덕을 찬양하는 이론적 출판물이 부족하지 않지만, 그러한 출판물을 뒷받침하는 이념적 합의가 있는지 여부를 결정하기 위해 더 많은 연구가 필요하다. 예를 들어, scoping review 는 서사 기반 접근 방식에서 의료인의 가치와 자질이 필수적이거나 중요하다고 간주되는지를 명확히 하는 데 도움이 될 수 있다. 이러한 연구는 또한 이러한 가치와 자질을 다른 의과대학 및 전문 의료 환경에서 암시적 또는 명시적으로 가르치는 역량과 비교하는 방법을 결정할 수 있다.
As this review has indicated, narrative medicine as a pedagogic intervention has a consistent replicable set of tools and strategies. And, while there is no lack of theoretical publications extolling the goals and virtues of a narrative-based approach, more research is needed to determine whether or not there is an ideological consensus undergirding such publications. A scoping review could help clarify, for example, which values and qualities of a medical practitioner are considered essential or important from a narrative-based approach. Such a study could also determine how these values and qualities compare with the competencies implicitly or explicitly taught in other medical school and professional health care settings.
용어집Glossary
내러티브(기반) 의학: 질병의 이야기를 인식하고, 흡수하고, 해석하는 이러한 기술을 가진 의학의 실천; 건강 관리의 새로운 틀로서, 그것은 치료를 받고 있는 사람들을 인식하고 존중하는 것보다 효과적인 건강 관리 시스템을 만드는 것을 목표로 한다.
Narrative-(based) medicine: The practice of medicine with these skills of recognizing, absorbing, interpreting by the stories of illness; as a new frame for health care, it aims to create an effective health-care system than recognizing and respecting the persons undergoing care.
Marini MG. 2015. Narrative medicine: bridging the gap between evidence-based care and medical humanities. eBook: Springer. p. 143.
Narrative medicine as a medical education tool: A systematic review
PMID: 30983460
Abstract
Aim: Narrative medicine has been promoted as an innovative and effective means of stimulating medical students' professional development by teaching them to approach their patients' experiences of illness with more understanding and compassion. This systematic literature review aims to answer the following question: what evidence of effect is available in the literature about models for teaching narrative medicine? Methods: We conducted a narrative review of 36 articles and used the Best Evidence in Medical Education (BEME) Global Scale and Kirkpatrick Scale for strength and importance of evidence to categorize reported assessment strategies and to evaluate the effectiveness of their narrative medicine programs. Results: We found evidence that narrative medicine is an effective pedagogic tool with a clear and replicable structure and methodology. We also determined that a positive impact could be measured when pertaining to participation and modification of attitudes, knowledge, and skills. However, unequivocal evidence of the effect of narrative medicine on students' behavior or ongoing interaction with colleagues and patients is still lacking. Conclusion: While many recent publications describe the goals and virtues of a narrative-based approach, more research is needed to determine whether or not there is an ideological consensus undergirding this approach. In addition, it is still unclear whether the long-term impact of narrative medicine classroom interventions are felt by patients, or whether such interventions positively impact patient care.
'Articles (Medical Education) > 교수법 (소그룹, TBL, PBL 등)' 카테고리의 다른 글
| 조언과 멘토링을 넘어: 의학교육에서 코칭을 위한 역량(Med Teach, 2021) (0) | 2022.08.12 |
|---|---|
| 유토피아에서 디스토피아까지: CBME의 러닝 애널리틱스에서 과정을 기록하기(Acad Med, 2021) (0) | 2022.05.31 |
| 성찰적 실천으로서 감정: 피드백 실천과 연구를 위한 새로운 담론(Med Educ, 2022) (0) | 2022.04.19 |
| 해부학에 대해서 왜 충분히 알지 못하는가? 내러티브 리뷰(Med Teach, 2011) (0) | 2022.04.16 |
| 해부학 교육의 베스트 프랙티스: 비판적 문헌고찰(Ann Anat, 2016) (0) | 2022.04.16 |