비-서구 문화권에서 의료 전문직업성 프레임워크: 내러티브 개괄(Med Teach, 2016)
Medical professionalism frameworks across non-Western cultures: A narrative overview
A. Al-Rumayyana, W. N. K. A. Van Mookb,c, M. E. Magzoubd, M. M. Al-Erakye,f, M. Ferwanaa, M. A. Khana and D. Dolmansb
서론
Introduction
지난 25년 동안, 의료 전문직업성에 대한 정의와 합의에 관한 상당한 문헌이 출판되었습니다. 그러나 서양문화의 전문 의료기관이 실시한 연구에서는 이를 [사회와 의료전문직의 계약 이행]으로 규정했다. 1980년대 초 미국내과학회(ABIM)는 다음과 같은 전문성 요소를 결정하는 휴머니즘 프로젝트를 시작했습니다: 책임감, 이타심, 탁월함, 의무, 성실성, 명예. 이 프로젝트는 적어도 미국 사회에서 현대 의학 전문성의 요소와 의미를 정의하는 데 중요한 공헌으로 여겨졌다.
Over the past 25 years, substantial literature has been published on definitions and consensus on medical professionalism (Cruess et al. 2000; ABIM Foundation et al. 2003). However, studies done by professional medical organizations in Western culture thus defined it as a fulfillment of the medical profession’s contract with society (Sohl & Bassford 1986; Pellegrino & Relman 1999). In the early 1980s, the American Board of Internal Medicine (ABIM) started its project on Humanism in which the following elements of professionalism were determined: accountability, altruism, excellence, duty, integrity, and honor (Evetts 2003; Zijlstra-Shaw et al. 2012). This project was considered an important contribution to defining the elements and meaning of contemporary medical professionalism at least in the American society.
이와 관련, 미국 내과의사협회, 미국 내과의사협회, 미국 내과의사위원회 및 유럽 내과의사연맹은 2002년에 의료 전문성에 관한 의사 헌장을 제정했다. 이 중요한 문서에는 사회 정의, 환자 자율성, 환자 복지의 우선을 포함한 의료 전문직업성의 세 가지 기본 토대와 10가지 전문직업적 책임을 함께 열거되어 있다.
- 환자와의 정직성,
- 전문적 역량,
- 환자의 기밀성에 대한 헌신,
- 질 향상 및 진료 접근성 향상,
- 환자와의 적절한 관계 유지,
- 과학적 지식,
- 신뢰 유지,
- 이해 충돌 관리,
- 전문직업적 책임
- 유한 자원의 분배.
In a related important development, the American College of Physicians, the American Society of Internal Medicine, the American Board of Internal Medicine, and European Federation of Internal Medicine established a Charter for Physician on medical professionalism in 2002. This important document listed three basic foundations of medical professionalism including, social justice, patient autonomy, and primacy of patient welfare, (General Medical Council 2001) along with 10 professional responsibilities, that include:
- honesty with patients,
- professional competence,
- commitment to patients’ confidentiality,
- improving quality and access to care,
- maintaining appropriate relationships with patients,
- scientific knowledge,
- maintaining trust,
- managing conflicts of interest,
- professional responsibilities, and
- just distribution of finite resources (ABIM Foundation et al. 2003).
그 결과, 역량 기반 커리큘럼과 전문 트레이닝 프로그램이 도입되고 있어 전문성은 학부·대학원 연수·평가 프로그램의 불가결한 부분이 되고 있습니다. 이러한 변화들 중 일부는 일부 사회와 문화로 제한될 수 있는 반면, 다른 것들은 다른 것들보다 더 두드러진다.
As a result, the competence-based curriculum and professional training programs are being introduced, and professionalism is made an integral part of undergraduate and postgraduate training and assessment programs. Some of these changes may be limited to some societies and cultures, whereas others are more prominent in others.
의대생에게 의학 전문직업성을 가르칠 때는 [환자의 이익을 의사의 이익보다 우선시]하는 것을 포함한 기본적인 사회적 계약을 반영해야 한다(Cruess 2006). 따라서 Physician Charter의 편집자가 말한 것처럼, 의료 전문직업성의 사회문화적 맥락의 중요성은 더욱 가치 있고 두드러진다. "이 문서는 헌장 저자들이 의술을 실천한 서양 문화 이외의 문화에서 의학의 전통을 반영하는가?" (Blank et al. 2003) 의료 전문직업성에 대한 보편적인 진실은 없다. Ho et al(2011)은 의료전문성 적용성의 서구적 틀에 도전하여 대만 이해관계자의 가치와 문화유산을 반영한 전문성 틀을 제안했다(Irvine 1997). 많은 연구자들은 의학 전문직업성은 [어떤 문화에서든 맥락적 연결에 관한 명확한 기술이 필요하다]고 제안했다. 문화적 배경은 이론적으로는 전문직업성 개념에 문화적 특정 요소를 추가할 수 있지만(Hafferty 2006), 다른 한편으로는 매우 제한적인 것으로 나타났다. 전문직업성 개념에 대한 영역이 중복되어 있어 전문직의 전문직업성적 특성에 대한 공감대는 아직 검증되지 않았다.
When medical professionalism is taught to medical students, it should reflect the underpinning social contract including placing the of patients’ interests above those of physicians (Cruess 2006). The importance of a sociocultural context of medical professionalism thus becomes more valuable and outstanding as voiced by the Physician Charter editor; “Does this document reflect the tradition of medicine in cultures other than those in the West, where the authors of the charter have practiced medicine?” (Blank et al. 2003).There is no universal truth about medical professionalism. Ho et al. (2011) challenged the Western framework of medical professionalism applicability and proposed a framework of professionalism reflecting the values and the cultural heritage of Taiwanese stakeholders (Irvine 1997). Many researchers suggested that medical professionalism needs a clear description that should be contextually linked to any culture (Van De Camp et al. 2004; Wear & Kuczewski 2004; Hafferty 2006; Woodruff et al. 2008). Cultural backgrounds may theoretically add cultural-specific elements to the concept of professionalism (Hafferty 2006), but on the other hand these are herein shown to be very limited (Cruess et al. 2010). The areas on the concept of professionalism are overlapping; therefore, the consensus on professional characteristics for professionals is not yet validated.
의학교육에서 [여러 문화권에 걸친 전문직업성의 개념화]를 강조하는 것은 [사회적 핵심 가치와 지역사회의 필요성에 대한 인식 차이]에 대응한 것이다. 동양 세계의 가치와 신념은 [집단의 역동성과 존엄화된 페르소나]의 관점에서 유교적 전통에 의해 추진되는propelled 반면, [전문직업성의 진화와 담론]은 서양 문화에서 더 두드러진다(Cruess 2006). 포함된 연구 중 일부에서는 서양의 전문직업성 개념을 문자 그대로 활용했고, 다른 연구에서는 다른 출처의 개념을 인용했다. 이러한 인용은 문화적 전통이 의료 전문성에 미치는 영향에 다른 개념을 가져왔다.
The emphasis on conceptualization of professionalism in medical education across cultures has come in response to perceived differences in societal core values and community needs. While Eastern world values and beliefs are propelled by Confucian traditions in terms of group dynamics and dignified persona (Ho et al. 2011), the evolution and discourse of professionalism are more prominent in the Western culture (Cruess 2006). In some of the included studies, utilization of the Western concept of professionalism was literal (Akhund et al. 2014; Nishigori et al. 2014), and other studies (Ho et al. 2011; Chandratilake et al. 2012; Al-Eraky et al. 2014) included cited concepts from other sources (Cruess et al. 2002; Cruess 2006; Cruess et al. 2010). These citations brought different concepts on the influence of cultural traditions on medical professionalism.
비서방 문화권, 특히 중국과 사우디아라비아의 다른 조사자들은 이러한 추세를 따랐다. Pan 등은 [모든 맥락을 포용하며, 모든 맥락에 적용할 수 있는 전문적 프레임워크는 없다]고 주장했다. 이 연구는 세 가지 비서구적인 전문성 프레임워크를 식별한다. 목표는 세 가지이다.
- (1) 세 가지 프레임워크와 그 문화 고유의 요소를 설명한다.
- (2) 세 가지 프레임워크 간의 공통점을 설명한다.
- (3) 그 차이점을 설명한다.
Other investigators from non-Western cultures especially China and Saudi Arabia followed this trend Pan et al. (2013). They all advocated that there is no professionalism framework that is comprehensive and applicable in all contexts. This study identifies three non-Western framework of professionalism; the aim is three folds:
- (1) to describe the three frameworks and their culture-specific elements,
- (2) to describe the commonalities among the three frameworks, and
- (3) to describe the differences between them.
방법들
Methods
이 연구의 목적을 실현하기 위해 내러티브 개괄narrative overview을 사용했다. 서술적 개요는 일반적으로 각 기사의 내용을 요약한 형식으로 저자들의 연구 결과를 보고한다. 이 방법을 사용하는 가장 큰 이유는 기준에 부합하는 기사를 4개만 발견했기 때문입니다. 둘째, 저자들이 비서양 문화권의 전문성 등 중요한 이슈를 조명해 토론을 자극하고 현안 질문에 답하려 할 때 가장 적합하다. 우리의 경우, 우리는 포괄적인 문헌 검토와 기사 선정 기준의 파악을 통해 앞서 언급한 연구 질문에 답하려고 노력하고 있다.
A narrative overview was used to realize the objectives of this study. A narrative overview reports the authors’ findings in a condensed format that typically summarizes the contents of each article (Green et al. 2006). The main justification of using this method is the fact that we found only four articles that met the criteria. Second, it is most suitable when the authors intend to bring an important issue such as professionalism in non-Western cultures to light for stimulating discussion and try to answer a pending question. In our case, we are trying to answer our research questions addressed earlier through conducting a comprehensive literature review, and identifying selection criteria of articles.
문헌 검색
Literature search
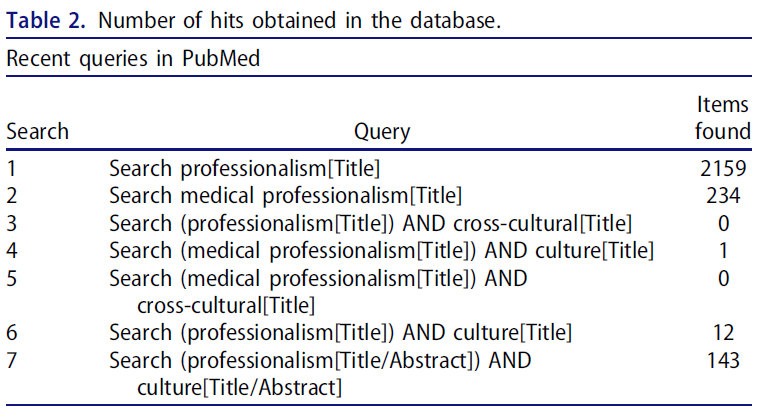
이 검토에는 1947년부터 현재까지 가장 중요한 국제 생물의학 문헌을 다루는 PubMed, Embase(최신 데이터베이스, PsychInFO, Educational Resources Information Center(ERIC; 교육 정보 센터), 사회학적 추상화, TIMELIT(Topics in Medical Education) 등 여러 방법이 사용되었다. PubMed는 1966년부터 시작되는 문헌을 다루는 우리의 연구와 더 관련이 있다. 2002년부터 2014년까지 PubMed 데이터베이스에 대한 검색을 제한했습니다. 그 해 「Physician Charter」가 확립되었기 때문입니다. 표 1은 검색에 사용된 용어를 보여 줍니다. 선택된 모든 연구의 참조는 이후 손으로 검색되었다. 체계적인 검토, RCT, 보고서 및 저널 기사를 포함한 정량적 및 정성적 연구가 연구의 목적으로 사용되었다. 표 2는 데이터베이스의 히트 수를 나타내고 있습니다. 두 명의 검토자는 총계와 요약본을 스캔하여 선택된 모든 연구의 포함 기준을 평가했다. 기사의 참조 리스트를 스캔 해, 의료 프로페셔널리즘과 같은 중요한 작업을 통합할 수 있는 한층 더 관련 있는 연구를 취득했습니다. 그 후, 동일한 두 검토자가 편견의 위험을 고려하여 전문 기사를 검색하여 검토하였다.
Multiple methods was used in this review including: PubMed; Embase (an up-to-date database, PsychINFO, Educational Resources Information Centre (ERIC); Sociological Abstracts; and Topics in Medical Education (TIMELIT) were covering the most important international biomedical literature from 1947 to the present day. PubMed is more relevant to our study which covers the literature starting from 1966. We limited our search on PubMed database from 2002 to 2014 because the “Physician Charter” was established in that year. Table 1 showed the terms used for the search. References of all selected studies were subsequently hand-searched. Quantitative and qualitative research including systematic reviews, RCT, reports, and journal articles was used for the purpose of the study. Table 2 showed the numbers of hits in the database. Two reviewers assessed the inclusion criteria of all selected studies by scanning the totals and the abstracts. The reference list of the articles was scanned to retrieve the further relevant studies enabling us to incorporate seminal work such as the Medical Professionalism. Subsequently, full text articles was retrieved and reviewed by the same two reviewers taking in consideration the risk of biases.

포함 기준
Inclusion criteria
비서양 문화에서 의료 전문성을 다루는 연구는 다음과 같은 선정 기준에 따라 선정되었습니다.
(1) 의사, 의대생, 의대교사, 의료교육자, 구급대원을 모집한 의료전문성에 관한 모든 종류의 원본 기사
(2) 비서양 문화 전반에 걸친 의료 전문성과 그 치수를 정의한 연구
(3) 영어로 출판된 연구
Studies addressing medical professionalism in non-Western culture were selected based on the following selection criteria:
- (1) any type of original article on medical professionalism that recruited physicians, medical students, medical teachers, medical educators, and paramedical staff,
- (2) research that defined medical professionalism and its dimensions across non-Western cultures, and
- (3) studies published in English language.
제외 기준
Exclusion criteria
비의료/패러메디컬을 포함한 서양 문맥에서 수행된 연구는 제외되었다.
Studies conducted in Western context, included non-medical/paramedical, and in non-English language were excluded.
결과.
Results
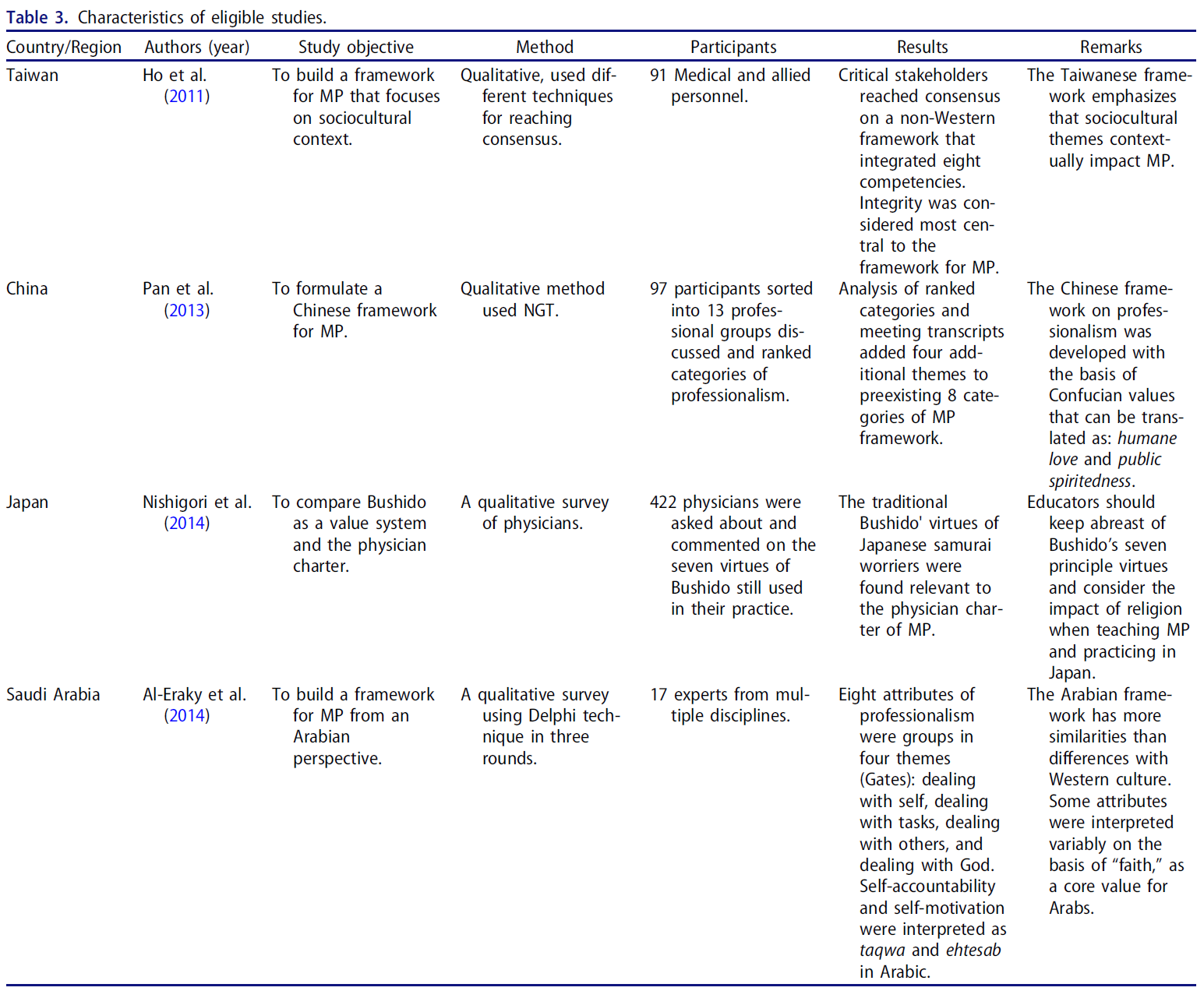
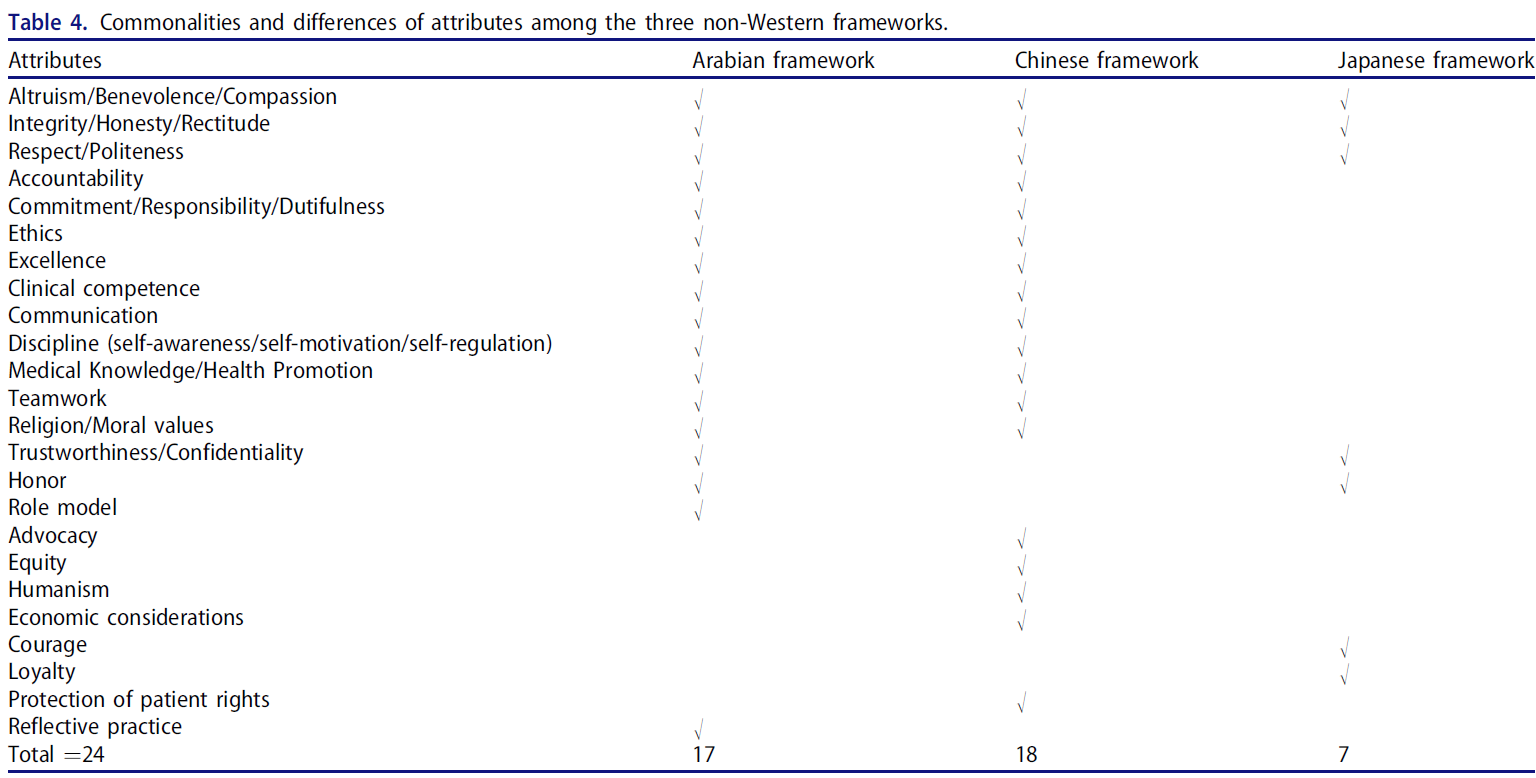
144개의 전문이 추가 검토를 위해 최종 후보 명단에 올랐으며, 131개의 연구는 비의료 전문성에 중점을 두었기 때문에 제외되었다. 비서양 문화에서 전문직업성을 다룬 기사는 13건뿐이었다. 이 13개 연구 중 [오직 4개 연구]만이 문화 특이적 요소를 포함하는 독특한 비서구적 프레임워크를 가지고 있었다. 이 네 가지 연구로부터 오직 세 개의 다른 프레임워크만이 중국어로 확인되었고 대만 연구는 둘 다 하나의 프레임워크에 초점을 맞추고 있었다. 표 3은 포함된 연구의 특성을 보여준다. 상자 1 ~ 3은 세 가지 프레임워크를 설명합니다. 다른 9개의 연구는 서양의 관점을 통해 전문성을 보기 때문에 제외되었다. 표 4는 3개의 비서양 문화에서 발견된 24개의 속성을 보여줍니다. 3개의 프레임워크에서 공통되는 속성은 3개뿐이며, 12개의 속성은 적어도 2개의 문화에서 공유됩니다. 나머지 9가지 속성은 각 문화마다 고유하다. 즉, 적어도 하나의 문화에서 발견된다.
One hundred and forty-four full-texts were shortlisted for further review; 131 studies were excluded due to its focus on non-medical professionalism. Only 13 articles addressed professionalism in non-Western culture. From these 13 studies, only 4 studies had a unique non-Western framework which includes culture-specific elements. From these four studies, only three different frameworks were identified as the Chinese and the Taiwanese studies were both focusing on one framework. Table 3 presents the characteristics of the included studies. Boxes 1–3 describe the three frameworks. The other nine studies were excluded because they look at professionalism through a Western lens. Table 4 presents 24 attributes found in the three non-Western cultures. Only 3 attributes are common among the three frameworks, while 12 attributes are shared by at least two cultures. The remaining nine attributes are unique to each culture i.e. are found at least in one culture.
Box 1 중국 문화의 관점에서 본 프레임워크
Box 1 Framework from Chinese cultural perspective
중국의 문화적 관점에서 Ho et al(2011) 프레임워크는 그리스 사원 형태의 스턴의 의료 전문성 프레임워크로 구성되며,
- 3개의 기본 원칙(소통, 임상 능력, 윤리),
- 4개의 기둥(설명성, 휴머니즘, 우수성, 이타주의) 및
- 빔(integrity)을 포함하고 있다. 빔은 기둥을 위에서 가로지르고 있다. 빈 기둥이 있어서 전문직업성의 가치를 추가하는데 사용할 수 있다.
From China’s cultural perspective, Ho et al. (2011) framework consists of Stern’s medical professionalism framework in the shape of a Greek temple and includes
- three basic principles (communication, clinical competence, and ethics),
- four pillars/columns (accountability, humanism, excellence, and altruism), and
- a beam (integrity), the beam across the top of the columns. Included blank columns are to be used for additional values for professionalism.
그들은 중국 문화에서 integrity과 관련된 문화 개념인 자중(자기 존엄과 존경)을 사용했다. 저자들은 존경과 자긍심을 갖는 것이 전문성 발달의 기본 단계라고 생각하고 그것을 지지 기둥의 맨 위에 대들보로 배치했다. 의료 전문성의 이러한 속성은 서양 문화와 유사하지만, 모든 참가자들이 Zizhong의 개념과 관련된 "integrity"을 추가하기로 동의했기 때문에 이 프레임워크는 Stern에서 벗어난다. 이 틀은 대만과 중국 신앙체계의 문화적 뿌리에 깊이 박혀 있다. Ho와 그녀의 동료들에 대한 연구는 그들의 문화적 맥락에서 전문직업성의 개념을 개발하기 위해 공동체의 의료 전문가들과 구성원들이 포함되었다.
They used the cultural concept of Zizhong (self-dignity and respect) which is associated with integrity in Chinese culture. The authors consider that to be respectful and self-dignified is a fundamental steps in professional development and placed it as a beam on the top of the supporting column. Although these attributes of medical professionalism are similar to Western culture, this framework derails from Stern as all participants agreed to add “integrity” relating to the concept of Zizhong. This framework is deeply embedded in cultural roots of the Taiwanese and Chinese belief system. The study of Ho and her coworkers included allied health professionals and members from the community to develop the concept of professionalism in their cultural context.
Pan et al(2013)은 동일한 개념을 사용했다. 그러나 팀워크, 건강증진, 자기관리, 경제 등 네 가지 카테고리를 통합했다. 이 연구에 따르면, 8개의 범주가 integrity, 임상 능력, 커뮤니케이션, 휴머니즘, 윤리, 이타주의, 설명 책임, 탁월성을 포함한 기존의 틀을 제공했습니다. 이러한 범주는 Ho et al(2011) 및 서구 지향 문화 체계와 유사하다.
Pan et al. (2013) used the same concept. However, they integrated four additional categories of: teamwork, health promotion, self-management, and economics. According to this study, eight categories offered a preexisting framework, which included integrity, clinical competence, communication, humanism, ethics, altruism, accountability, and excellence. These categories are similar to Ho et al. (2011) and Western-oriented cultures frameworks.
박스 2 아라비아 프레임워크
Box 2 The Arabian framework
[아라비아 맥락]이란 아랍어를 공용어로 하고, 이슬람교가 대다수 인구의 종교인 중동의 아라비아 국가들에 의해 행해지고 있는 문화, 전통, 믿음, 그리고 행동의 혼합으로 인식될 수 있다. 이러한 행동과 전통은 반드시 이슬람 교리로부터 나온 것은 아니지만, 이러한 나라들 사이에서는 몇 가지 공통된 가치관이 표준으로 받아들여지고 있다. 비록 인종 집단, 부족, 지역 문화, 그리고 지역 실체에 차이가 있지만, 아랍 세계는 여러 독립 국가의 집합이라기 보다는 하나의 중요한 사회이다. 아라비아 맥락에서 알-에라키 외 연구진(2014)은 이슬람의 가치에 기초한 아라비아 문화의 맥락에서 의료 전문성의 [4대문 모델]을 설명했다. 8개의 전문적 속성이 다음과 같은 4개의 테마로 분류되었다.
- (1) 자기자신을 다루는 것: 자기인식(taqwa)와 자기관리(ehtesab).
- (2) 과제를 다루는 것: 수월성 다루기, 전문성 개발에 대한 헌신, 성찰적 실천
- (3) 타인을 다루는 것: 환자, 동료 및 학생에 대한 존중, 전문적 기밀 유지
- (4) 알라(신)를 다루는 것: 기존 문헌과 다르게, 자기-책무와 자기-동기가 알라(신)와 연계되어서, 이것은 (사람이 아닌) 알라로부터 전문직이 받는 보상이라고 정의했다.
The Arabian context can be perceived as the blend of culture, traditions, beliefs, and behaviors that are being practiced by nations of Arabian countries in the Middle East, where Arabic is the official language and Islam is the religion of majority of the population. Those behaviors and traditions are not necessarily derived from Islamic doctrines, but some common values have been accepted as the norm among populations of these countries. Although there are differences in ethnic groups, tribes, local cultures, and regional entities, the Arab world is a single, overarching society rather than a collection of several independent states. In Arabian context, Al-Eraky et al. (2014) described the Four Gates model of medical professionalism in the context of Arabian culture that is based on the value of Islam. Eight professional attributes were grouped into four themes which include:
- (1) dealing with self that includes two attributes of self-awareness (taqwa) and self-management (ehtesab),
- (2) dealing with tasks that deals with excellence, commitment to professional development, and reflective practice,
- (3) dealing with others that reflects attributes of respect for patients, colleagues and students, and maintaining professional confidentiality, and
- (4) dealing with Allah (God), a different stream in the literature that reflects attributes of self-accountability and self-motivation that link with Allah defined it as a reward professionals receive from Allah, not from people.
박스3 일본문화의 관점에서 본 프레임워크
Box 3 Framework from Japanese cultural perspective
니시고리 외 연구진(2014년)은 일본의 문화적 맥락에 대해 "무사의 길"은 전문성에 대응한다는 가치체계라고 표현했다. 이 개념은 사무라이의 고대 무사들로부터 추출된 일본의 개인 행동 규범을 상징한다. 무사도의 틀에서 일곱 가지 주요 덕목은 청렴, 정직, 자애, 공손, 용기, 명예, 충직이다.
With respect to Japanese cultural context, Nishigori et al. (2014) described the concept of Bushido as a value system that means, “the way of the warrior,” is corresponding to professionalism. This concept symbolizes a Japanese code of personal conduct extracted from the ancient warriors of Samurai. Seven principal virtues were grouped in the framework of Bushido are
rectitude (gi),
honesty (sei),
benevolence (jin),
politeness (rei),
courage (yu),
honor (meiyo), and
loyalty (chugi).
청렴은 사람이 이성에 따라 흔들림 없이 생각하고, 결정하고, 행동하는 방식을 나타냅니다. 그것은 사무라이의 가장 중요한 속성으로 여겨지는 첫 번째 속성이다.
용기(氣)는 일본의 틀에 특화된 두 번째 덕목이며, 즉 위험에 직면했을 때 어떻게 서고 걷고 행동하고 적절한 행동을 하는지를 나타내는 용기(氣)의 정신이다.
세 번째 덕목인 자애(진)는 사랑, 동정, 연민의 개념을 결합한다. 그것은 인간의 영혼에서 가장 높은 속성으로 평가된다. 그것은 의학에 의해 "인혜로운 예술로서의 약"으로 번역되어 왔다.
일본인은 병원 직원이나 가족 등 집단의 이익과 요구에 대한 충성심을 중시해 개인의 이익과 요구보다 집단의 요구를 중시한다. 그러므로, 무사도는 가족과 그 구성원의 이익을 결합했다.
Rectitude (gi) represents the way a person thinks, decide, and behave based on reason, without wavering. It is the first attribute considered as the most important attribute of the Samurai.
Courage (yu) is the second virtue which is culture specific to Japanese framework means the spirit of bearing and daring, in other word, how one stands, walks, behaves, and doing the appropriate acts when facing danger.
Benevolence (jin), as a third virtue, combines the concepts of love, sympathy, and pity. It is valued as the highest attribute in the soul of human. It has been translated by medical practice as “medicine as a benevolent art.”
The Japanese have considered loyalty (chu-gi) to the interests and needs of the group such as hospital staff and family, and they place the needs of groups above individual interest and needs. Therefore, Bushido combined the interests of family and its members.
논의
Discussion
이 섹션에서는 먼저 세 가지 프레임워크에 대해 논의한 후 이들 간의 공통점과 차이점에 대해 논의한다.
In this section, we will discuss first the three frameworks followed by discussion of commonalities and differences among them.
중국의 프레임워크는 전문직업성의 개념화에 [자기존엄, 팀워크, 건강증진, 자기관리] 등의 측면에서 새로운 범주의 전문직업성을 추가했다. Pan et al (2013) 프레임워크의 강점은 지명된 그룹 기술(NGT)을 사용하는 다원적 전문가 그룹이 중국뿐만 아니라 다른 아시아 문화에서 의료 프로페셔널리즘의 사회적 문화적 속성을 우선시했다는 것이다.
The Chinese framework added new categories of professionalism in terms of self-dignity, team work, health promotion, and self-management to the conceptualization of professionalism. The strength of Pan et al.’s (2013) framework is that multidisciplinary expert groups using Nominated Group Technique (NGT) prioritized social and cultural attributes of medical professionalism which can benefit health-care providers not only in China but also in other Asian cultures.
아랍 문화에서 4대문 모델은 종교 중심 사회에서는 효과가 있을 수 있지만, 비이슬람 아랍 학생이나 교사, 또는 인도주의적 가치를 가진 기관에서는 효과가 없을 수 있습니다. 4개 게이트 모델은 4개의 논리적 영역(게이트)에서 결합되는 연결된 전문적 품질의 구조적 패턴으로 연결하기 위해 독립형 속성의 짧은 목록으로서 의료 전문성에 대한 고전적 인식에서 변화를 제안한다.
The Four-Gates Model in the Arab culture may work for faith-driven societies, but not for non-Muslim Arab students or teachers, or in institutions with humanistic values. The Four-Gates model suggests a move from the classical perception of medical professionalism as a short list of standalone attributes, to link them in a structural pattern of connected professional qualities as coupled in four logical domains (Gates).
자기 책임(self-accountability)을 사용하는 대신, Al-Eraky et al(2014)는 taqwa라는 용어를 도입했다. 프로페셔널리즘에서, 행동과 그 결과에 대한 의사의 본질적인 감각은 그들이 알라에게 대답할 수 있기 때문이다. 자기 동기부여에 대해서는, 의사들이 교육, 학습, 연구에 최선을 다하고 그 대가로 알라로부터 보상을 기대하는 새로운 ehtesab의 구조가 도입되었다. 흥미롭게도, 4게이트의 관심의 중심은 개인이고, 이는 8가지 속성 중 4가지 속성에서 "자신"의 존재로 나타난다. 의료 전문성은 우선 복잡한 의료 시스템에서 일할 수 있도록 전문가들을 준비시키는 것부터 시작됩니다. 요약하면, 6개의 속성으로 이루어진 마지막 3개의 테마는 각각 서구 문화의 틀과 비슷하지만, 이 아라비아 문화 관점에 대한 연구는 사회적 책무social accountability의 개념을 신의 대한 책무divine accountability과 연결시켰다. 위에서 설명한 바와 같이, 프로페셔널리즘의 보편적 속성은 지역 규범과 신념 체계에 따라 다양한 맥락에서 다르게 해석된다.
Instead of using self-accountability, Al-Eraky et al. (2014) introduced the term taqwa; in professionalism, an intrinsic sense of doctor for action and its consequences because they are answerable to Allah. For self-motivation, a new construct of ehtesab in which doctors perform their best in teaching, learning, and research and in return expect reward from Allah was introduced. Interestingly, the center of attention of the Four-Gates is the individual, which is reflected with the presence of “self” in four out of eight attributes. Medical professionalism starts by preparing professionals – themselves – to work in a complex health-care system. In summary, although the last three themes each consisting of six attributes are similar to frameworks of Western culture, this study on the Arabian cultural perspective linked the concept of social accountability with divine accountability. As indicated above, the universal attributes of professionalism are interpreted differently in various contexts, based on the local norms and belief systems.
일본의 문화에 대해서는 의사 헌장 등 자주 언급되는 서양의 전문 가이드의 특성을 부시도 개념과 비교했다. 그들은 종교, 전통, 미덕의 효과를 포함한 속성들 사이의 유사점과 차이점을 설명했다. 연구진은 일본 문화에서 부시도의 7가지 원칙은 의학 전문성에 적용 가능하며 의사 헌장에 상당하다고 주장했다. 눈에 띄는 차이는 부시도에는 있지만 몇 가지가 '의사 헌장'에는 없다는 것이다. 무사도에는 일반적으로 '사회를 위한 행동 규범'으로 설명되는, '청렴' '용기' '예의' '명예' 등이 있다. 반대로 환자 자율성의 개념은 부시도 체제에서는 누락되어 있지만 서양 문화에서는 높이 평가되고 있다.
In regard to the Japanese culture, the attributes of a frequently referenced professionalism Western guide such as the Physician Charter were compared to the Bushido concept. They described the similarities and differences between the attributes including the effect of religion, traditions, and virtues. The researchers suggested that in Japanese culture Bushido’s seven principles were applicable to medical professionalism and were fairly comparable to Physician Charter (Nishigori et al. 2014). The notable differences pointed out was the omission of several commitments such as rectitude, courage, politeness, and honor in the Physician Charter that are mentioned and discussed in Bushido, as the Charter described medical professionalism, whereas Bushido explained generally as a code of conduct for the society. Prominent of other differences is the concept of patient autonomy of the individual which is omitted in the Bushido framework but is highly regarded in Western culture.
따라서 전문성에 대한 비서구적 관점을 다루는 연구는 의료인의 전문적 속성에 관한 몇 가지 주요 유사점과 차이점을 확인했다. 이러한 유사성과 차이는 다음 섹션에서 자세히 다룰 것이다.
The studies addressing non-Western perspectives on professionalism thus identified several key similarities and differences regarding professional attributes of medical practitioners. These similarities and differences will be addressed in more details in the next sections.
서양 이외의 연구에서 인용된 전문성의 공통점
Commonalities of professionalism cited in non-Western studies
이 세 가지 틀은 아랍 문화에 대한 믿음과 중국과 일본 문화에 대한 전통과 같은 문화적 규범에 의해 주도되고 깊이 영향을 받는다. 3개의 기사에서 총 24개의 속성이 식별되었다(표 4). 많은 개념들이 비서양적 문맥을 다루는 연구들 사이에서 비교될 수 있을 뿐만 아니라, 서양 문화와도 매우 유사했다. 예를 들어 이타주의, 정직과 진실성, 존경, 책임, 팀워크, 윤리, 임상 능력, 헌신과 소통, 환자의 권리와 환자의 보호 등이다.
특히 동양에서 존중respect은 [강한 유대감connectivity]을 가지고 있으며, 가르치는 것뿐만 아니라 의료 환경에서 전문직업성을 실천하는 데에도 영향을 미친다. 이는 서양에서도 마찬가지지만, 현대 서구 사회에서는 교육과 환자 진료에 대한 의미가 다르다. 서양 이외의 사회에서는, 의학 교사와 학생, 그리고 의사와 환자의 직업적인 관계는, 가부장적 접근에 근거하고 있다. 이는 주로 전문직이 결정을 내리는 가부장적 접근에 기반하고 있으며, 서양에서는 더 이상 일반적인 관행으로 여겨지지 않는다. 요약하자면, 요소적 유사성은 전문성의 세 가지 비서구적 프레임워크 모두에서 공통분모이다.
These three frameworks are driven and deeply influenced by cultural norms such as faith in Arab culture and tradition in Chinese and Japanese cultures. A total of 24 attributes were identified from the three articles (Table 4). Many concepts not only were comparable among the studies addressing non-Western context, but also very much comparable to Western culture, such as altruism, honesty and integrity, respect, accountability, teamwork, ethics, clinical competence, commitment and communication, and protection of patient’s rights (Chiu et al. 2010; Adkoli et al. 2011; Ho et al. 2011; Pan et al. 2013; Akhund et al. 2014; Al-Eraky et al. 2014; Nishigori et al. 2014) and patients (Cruess et al. 2010; Chandratilake et al. 2012; Leung et al. 2012; Akhund et al. 2014). Notably, in the Eastern world (Al-Eraky et al. 2014; Nishigori et al. 2014), respect has a strong connectivity and influences not only in teaching but also practicing professionalism in medical settings. This is also true in the Western world, but its meaning for teaching and patient care is different in the contemporary Western society. In the non-Western society, the professional relationship between a medical teacher and a student, and likewise, the doctor and the patient is based on the paternalistic approach where decisions are usually made by professionals (Cruess et al. 2010), which has been abandoned as common practice in the Western world, moving toward shared decision-making. In summary, elemental similarities are common denominators in all three non-Western frameworks of professionalism.
서양 이외의 연구에서 인용된 전문성의 차이
Differences of professionalism cited in non-Western studies
세 가지 비서양 프레임워크에서 기술된 몇 가지 중요한 측면은 서구 프레임워크에서 두드러지게 누락되었다. 앞서 말한 세 개의 틀에 대한 깊은 문화적 영향의 공통점은 또한 각각의 문화가 MP에 반영되는 그들만의 고유한 가치를 가지고 있기 때문에, 그들 사이의 주요한 차이점의 원천이다. 세 개의 틀 사이의 주요한 차이점은 문화, 우선순위 그리고 각 특성에 대한 해석과 관련이 있다. 예를 들어, 9개의 attribute는 3개의 프레임워크에서 공통 또는 공유되지 않습니다.
Several important aspects described in three non-Western frameworks were notably absent from the Western frameworks. The commonalities stated earlier by the deep cultural influence on the three frameworks are also a source of major differences between them due to the fact that each culture has its own unique values that are reflected in MP. The main differences between the three frameworks are related to culture and prioritization as well as interpretation of attributes. For instance, nine attributes are not common or shared by the three frameworks.
Ho et al(2011)이 Zzong 문화 개념에서 도출한 자기 존엄성과 존중Self-dignity and respect 은 Integrity과 동일하다. Al-Eraky et al(2014)은 알라(신)를 다루는 형태로 아라비아 문화의 의료 전문성의 틀에 독특한 차원을 도입했으며, 이 주제 아래 자기 책임(taqwa)과 자기 동기 부여(ehtesab)가 기술되었다. Pan et al(2013)과 Ho et al(2011)의 프레임워크는 특히 건강 증진, 자기 관리, 팀워크 및 전문성 촉진을 위한 경제적 고려사항 등 4가지 추가 주제 측면에서 다른 두 모델과 다르다.
Self-dignity and respect derived from the Zizhong culture concept by Ho et al. (2011) equate with integrity; Al-Eraky et al. (2014) introduced a unique dimension to the framework of medical professionalism in Arabian culture in the form of dealing with Allah (God), and under the umbrella of this theme, self-accountability (taqwa) and self-motivation (ehtesab) were described. Pan et al.’s (2013) and Ho et al.’s (2011) framework differs from the other two models in terms of four additional themes, especially health promotion, self-management, team work, and economic consideration in promoting professionalism.
이 리뷰는 비서방 연구 간의 차이점을 비교하면서 중국, 홍콩, 대만 지역에서 옹호, 형평성, 인본주의 및 경제적 고려의 속성을 발견한 반면 사우디아라비아와 일본의 문화에서는 전문성의 필수적인 속성을 발견했다. 이러한 속성은 의료 전문가 정신의 필수 요소로 간주되지 않는다. 이전 절에서 설명한 이러한 유사점과 차이점은 사회적, 경제적, 문화적 배경과 관련이 있다.
While comparing the differences between the non-Western studies, this review found the attributes of advocacy, equity, humanism, and economic considerations essential attributes of professionalism in the region of China, Hong Kong, and Taiwan whereas in Saudi Arabia and Japan’s culture, these attributes are not considered essential elements of medical professionalism. These similarities and differences described in the previous sections relate to social, economic, and cultural backgrounds.
실제적 의미
Practical implication
또, 이 조사 결과나 문화의 직업적 속성에 대한 영향에 근거해, 아랍 문화에 대한 신앙이나 일본 문화에 있어서의 부시도등의 사회문화적 요소를 배경 변수로 포함시키는, 직업적 속성에 긍정적이든 부정적이든, 확장된 전문성의 틀을 제안할 수 있다. 속성의 우선순위 부여는 각 문화에 대한 중요성을 반영합니다. 제안된 모델은 환자 및 제공자 만족도와 같은 건강 고발자에 대한 전문적인 속성의 결과인 세 번째 수준을 추가하여 완성할 수 있다.
Based on the findings and the effect of culture on professional attributes, the study may propose an extended framework of professionalism to include sociocultural factors as background variables such as faith in Arabic culture and Bushido in Japanese culture; these background factors positively or negatively influence professional attributes. The prioritization of the attributes reflects the importance to each culture. The proposed model may be completed by adding a third level which is the outcome of professional attributes on health indictors such as patient and provider satisfaction as well as better health care.
이 연구는 전문직업성이 맥락적이라는 강력한 증거를 제시하며, 따라서 논리적으로 보자면, 의학 교육에서 전문직업성을 가르치고 평가할 때 [고유한 문화적 요소]를 커리큘럼과 CPD 프로그램에 포함시켜야 할 것이다. 그러나 제안된 확장된 전문성 모델과 다양한 맥락에서 전문성을 가르치고 평가하는 데 미치는 영향을 개발하고 경험적으로 테스트하기 위해서는 추가 연구가 필요합니다.
This study provides strong evidence that professionalism is contextual, and therefore including culture-specific elements in curricula and continuous professional development programs regarding teaching and assessing professionalism in medical education seems a logical consequence. Further research is however needed to develop and empirically test the suggested extended model of professionalism and the impact on teaching and assessing professionalism in different contexts.
연구의 한계
Limitations of the study
이 연구의 한계 중 하나는 방법으로서의 서술적 검토의 활용이다. 소수의 연구에 의존하는 이러한 유형의 검토는 발견의 일반화에 영향을 미치는 편향적인 요소를 우주에 가져올 수 있다 29-30. 다만, 개요를 실시하는 모든 스텝에 주의해, 보다 객관적으로 하기 위한 모든 조치를 취했습니다.
One of the limitations of this study is the utilization of narrative review as a method. This type of review which depends on few studies may bring an element of bias which affects generalization of findings to the universe 29-30. However, we took all the measures to make it more objectives by carefully following all the steps of conducting an overview.
결론들
Conclusions
이 서술적 개요는 네 가지 주요 발견을 드러냈습니다.
첫째, 일본, 아랍권, 중국을 대표하는 알-에라키 외 연구진(2014년), 호 외 연구진(2011년), 판 외 연구진(2013년)의 세 가지 문화 맞춤형 비서구 프레임워크 개발을 시도한 연구는 4개뿐이었다. Pan et al(2013)은 Ho와 관련자들에 의해 개발된 프레임워크를 확장했다. 이러한 연구는 문화 고유의 요소를 출발 지역을 대표하는 의료 전문직업성의 독특한 개념적 프레임워크에서 제공했다.
둘째, 확인된 세 개의 비서구 프레임워크는 보편적으로 칭찬받는 속성의 공통점을 가지고 있지만, 그것들은 다양한 문화에서 다르게 해석되었다. 예를 들어, Integrity은 중국 유교적 가치에서 Zizhong과 관련이 있는 반면, 자기 동기 부여와 자기 책임성은 아라비아 문맥에서 각각 taqwa와 ehtesab으로 해석되었다. 따라서 그 차이는 속성의 해석과 우선순위 부여에 관한 것이다. 의료 전문가 정신은 상황에 따라 다릅니다. 모든 국가에서 인정받을 수 있는 단일한 프로페셔널리즘의 틀은 없다. 전문직이 무엇에 전념하는지를 이해하고 그 개념을 의대생과 의사의 전문적 정체성 형성에 반영하기 위해서는 문화지향적 전문성 개념이 필요하다. 마지막으로, 저자는 의료에 대한 결과로 이어지는 속성의 배경으로서 문화를 포함하는 확장된 프레임워크를 제안한다.
This narrative overview revealed four major findings.
First, only four studies attempted to develop a three culture-tailored non-Western framework for medical professionalism (Nishigori et al. 2014); Al-Eraky et al. (2014), Ho et al. (2011), and Pan et al. (2013) representing Japan, Arab world, and China, respectively were identified. Pan et al. (2013) extended the framework developed by Ho and associates (Ho et al. 2011). These studies provided culture-specific elements in a unique conceptual framework of medical professionalism representing the region they originated from.
Second, the three identified non-Western frameworks have commonalities of universally praised attributes, but they were interpreted differently in various cultures. For instance, integrity was relevant to Zizhong in Chinese Confucian values, while self-motivation and self-accountability were interpreted as taqwa and ehtesab in Arabian context, respectively. The differences thus concern the interpretation and prioritization of the attributes. Medical professionalism is context-specific. There is no single framework on professionalism that can be globally acknowledged. A culture-oriented concept of professionalism is necessary to understand what the profession is dedicated to and to incorporate the concept into the medical students’ and physicians’ professional identity formation. Finally, the authors propose an extended framework to include culture as background to attributes leading to an outcome on health care.
Med Teach. 2017 Apr;39(sup1):S8-S14.
Medical professionalism frameworks across non-Western cultures: A narrative overview
PMID: 28417688
Abstract
Background: Medical professionalism is context-specific, but most literature on professionalism stems from Western countries. This study is about benchmarking of different frameworks on professionalism and interpreting the commonalities and discrepancies of understanding professionalism across different cultures. We need to study the cultural underpinning of medical professionalism to graduate future "global" practitioners who are culturally sensitive enough to recognize differences (and also similarities) of expectations of patients in various contexts.
Aim: This study aims at describing culture specific elements of three identified non-Western frameworks of professionalism, as well as their commonalities and differences.
Method: A narrative overview was carried out of studies that address professionalism in non-Western cultures in the period 2002-2014.
Results: Out of 143 articles on medical professionalism, only four studies provided three structured professionalism frameworks in non-Western contexts. Medical professionalism attributes in non-Western cultures were influenced by cultural values. Out of the 24 identified attributes of professionalism, 3 attributes were shared by the three cultures. Twelve attributes were shared by at least two cultures, and the rest of the attributes were unique to each culture.
Conclusions: The three frameworks provided culture-specific elements in a unique conceptual framework of medical professionalism according to the region they originated from. There is no single framework on professionalism that can be globally acknowledged. A culture-oriented concept of professionalism is necessary to understand what the profession is dedicated to and to incorporate the concept into the medical students' and physicians' professional identity formation.
'Articles (Medical Education) > 전문직업성(Professionalism)' 카테고리의 다른 글
| 집단적 자기치유와 흔적: 군집지능은 어떻게 팀적응에 대해서 다르게 생각할 수 있게 해줄까? (Med Educ, 2020) (0) | 2022.04.11 |
|---|---|
| '그들'에서 '우리'로: 그룹 경계를 팀 포함성으로 연결하기 (Med Educ, 2019) (0) | 2022.04.11 |
| 대만 의과대학생의 문화간 전문직업성 딜레마 내러티브: 서양의학과 대만문화의 긴장(Adv Health Sci Educ Theory Pract. 2017) (0) | 2022.03.24 |
| 보건의료전문직 학생이 경험하는 전문직업성 딜레마: 단면 연구(J Interprof Care. 2020) (0) | 2022.03.24 |
| 성격은 무엇인가? 두 개의 미신과 하나의 정의(New Ideas in Psychology, 2020) (1) | 2022.03.21 |