미국 3년제 의과대학의 종합적 역사: 한 학기의 리뷰(Med Educ Online, 2018)
Comprehensive history of 3-year and accelerated US medical school programs: a century in review
Christine C. Schwartz, Aparna S. Ajjarapu, Chris D. Stamy and Debra A. Schwinn
소개 및 목적
Introduction and purpose
지난 10년간 미국의 의대 교육 지도자들이 혁신적인 교육과정 개혁에 나섰다. 4년 연속 임상 및 생물의학 교육을 통합하고 능동적 학습을 추가하는 것 외에도, 일부 의과대학은 보다 포괄적인 기간, 특히 3년 내에 의학 교육을 제공하는 실험을 시작했다. 이 운동은 특히 미국 역사상 다양한 맥락에서 두 번 시도되고 포기된 적이 있기 때문에 약간의 논란을 불러일으켰다. 그러나 미국의 가속화된 의학 교육에 대한 배경 정보를 연구할 때, 기사는 일반적으로 특정 학교 및/또는 특정 기간에 초점을 맞추고 있기 때문에 3년제 MD 학교에 대한 포괄적인 역사적 검토는 없는 것으로 보인다. 과거로부터 배울 수 있다는 점을 감안하여, 우리 연구단은 지난 세기 동안 미국의 가속화된 allopathic MD 교육 프로그램에 대해 출판된 원고에 대한 철저한 역사적 검토에 착수했다. 우리의 목적은 의과대학이 시간이 지남에 따라 3년제 의학교육을 선택한 후 이를 포기한 이유를 조사하는 것이다.
Over the last decade, US medical school education leaders have embarked on innovative curriculum reform. In addition to integrating clinical and biomedical science teaching over a 4-year continuum and adding active learning, some medical schools have begun experimenting with delivering medical education in a more comprehensive period, specifically 3 years. This movement has created some controversy, particularly since it has been tried and abandoned twice before in US history in various contexts. Yet in researching background information on accelerated medical education in the United States, there appears to be no comprehensive historical review of 3-year MD schools, since articles generally focus on specific schools and/or specific time periods. Given that we can learn from the past, our research group embarked on an exhaustive historical review of manuscripts published about accelerated allopathic MD education programs in the United States over the last century. Our purpose is to examine reasons medical schools had for choosing, and then abandoning, accelerated 3-year medical education over time.
상세 내역
Detailed history
초기 의료 커리큘럼 표준화: 1800년대-1930년대
Initial medical curriculum standardization: 1800s–1930s
1800년대에 미국의 의과대학 대부분은 소규모의 영리for-profit 비-대학 소속이었으며, 고아범위하며 표준화되지 않은 교육과정과 교육목표를 가지고 있었다. 1847년에 미국 의학 협회(AMA)가 설립되었고 후에 AMA 의학 교육 위원회(CME)가 시작되어 1904년에 [표준화된 의과 대학 교육과정]을 제공하였다. 이 새로운 교육과정의 창시자는 1890년대에 [의대생들을 위한 엄격한rigorous 임상 실습]을 도입한 캐나다의 의사인 윌리엄 오슬러 경이었다. 1900년대 초에 아브라함 플렉스너는 카네기 재단으로부터 미국의 의학 교육을 검토하라는 의뢰를 받았다[2]. 오스러가 이끄는 존 홉킨스에서의 교육에 감명받은 플렉스너는 오슬러가 이야기한 집중 임상훈련에 앞서 2년의 과학 교육이 선행돼야 한다고 강조했고, 이는 총 4년의 교육과정으로 이어졌다. During the 1800s the majority of medical schools in the United States were small, for-profit, non-university affiliated, and had wide-ranging non-standardized curricula and educational goals. In 1847, the American Medical Association (AMA) was established and later the AMA Council of Medical Education (CME) was initiated, ultimately providing a standardized medical school curriculum in 1904 [1]. A founding father of this new curriculum was the Canadian physician, Sir William Osler, who introduced rigorous clinical clerkships for medical students in the 1890s. In the early 1900s, Abraham Flexner was commissioned by the Carnegie Foundation to review medical education in the United States [2]. Impressed by the education at John Hopkins, headed by Osler, Flexner emphasized that 2 years of science education should precede Osler’s intensive clinical training, comprising a total of 4 years of medical school .
1910년의 플렉스너 보고서(PDF 원본 문서는 카네기 재단 기록 보관소를 통해 온라인으로 제공됨)는 의학 교육에 대한 결정적 프레임워크를 제공했다는 점에서 혁명적이었으며, 본질적으로는 [통합된consolidated 대학 부속 의과대학]의 물결 속에 [표준화된 모델]을 낳았다. 1934년까지 38개의 의학전문대학원 중 8개를 제외한 모든 대학원이 대학 의과대학과 관련이 있었다. 제1차 세계 대전(1918년) 이후 의료 기술과 역량의 급속한 확장이 일어나 의과대학에 이어 곧바로 의사-교육자에 의해서 감독받는 진료(인턴십)로 이어졌다. 1930년, 의예과 요구사항도 명확해졌는데, 일반 화학, 물리학, 생물학이 각각 2학기씩, 유기 화학이 1학기씩이었다.
The Flexner report of 1910 (pdf of the original document is available online through the Carnegie Foundation archives) was revolutionary in providing a critical framework for medical education, essentially resulting in a model that became standardized in a wave of consolidated university affiliated medical schools. ‘By 1934 all but eight of the 38 approved graduate schools of medicine were related to university medical schools’ [3]. Post WWI (1918), rapid expansion of medical techniques and capabilities occurred, leading to physician-teacher supervised patient care immediately following medical school (internship) [2]. By 1930, premedical science requirements had also become clearly established, including two semesters each of general chemistry, physics, and biology, and one semester of organic chemistry.
3년제 가속 의료 커리큘럼 도입: 1930년대-1940년대
Introduction of the 3-year accelerated medical curriculum: 1930s–1940s
제2차 세계 대전(1939-1945) 동안, 미국은 국내외에서 의사 부족에 직면했고, 그래서 3년제 가속 의과대학 프로그램은 의사들을 더 빨리 교육하기 위한 제안 해결책으로 도입되었다[4]. 버지니아 의과대학은 제2차 세계 대전 동안 3년제 가속 의학 프로그램을 가진 최초의 학교들 중 하나였다. 의사 부족 문제를 해결하라는 압박을 받은 미국 연방정부는 대학과 의과대학에 3년제 가속 의료 프로그램을 더 폭넓게 도입할 것을 촉구했다.
- 실제로 FSMB은 3년 뒤 졸업하는 학생들이 합법적으로 의료행위를 할 수 있도록 면허를 관리하는 법령을 개정했다.
- 이러한 새로운 3년 커리큘럼을 적절히 개발하는 데 시간이 거의 주어지지 않았기 때문에, AMA 이사회는 어려움을 극복하는 데 도움을 주기 위해 연락 위원회liaison committee를 구성했다.
- 또한, AMA의 의료 교육 및 병원 위원회는 가속화된 의료 프로그램의 품질 저하 우려로 인해 높은 의료 교육 수준을 유지하기 위한 검사를 감독할 책임이 있다[6].
During World War II (1939–1945), the nation faced physician shortages at home and abroad, so 3-year accelerated medical school programs were introduced as a proposed solution to educate physicians faster [4]. The Medical College of Virginia was one of the first schools to have a 3-year accelerated MD program during World War II [5]. Pressured with solving physician shortages, the US federal government urged universities and medical colleges to adopt 3-year accelerated medical programs more broadly.
- Indeed, the Federation of State Medical Boards revised laws and regulations governing licensure so students graduating in 3 years could legally practice medicine.
- Because very little (if any) time was given to appropriately develop these new 3-year curricula, the AMA Board of Trustees organized a liaison committee to aid in overcoming difficulties encountered.
- In addition, the AMA’s Council on Medical Education and Hospitals took responsibility to oversee inspections to maintain high standards of medical education due to concerns of deterioration of quality with accelerated medical programs [6].
흥미롭게도, 군의관들이 민간인 신분으로 제대하자, 많은 사람들이 그들의 제한된 지식을 인정하여 '리프레셔' 강좌가 인기를 얻었다. 군에 있는 많은 수의 의사들에게 보낸 설문조사에서 거의 60%(12,534/21,029명)가 긴 재교육 과정(6개월 이상)을 수강하기를 원했고, 이는 졸업후 의학교육(GME) 프로그램을 더 개발하라는 압력으로 이어졌다. 1955-1956년까지 85개의 인가 또는 개발 중인 의과대학 중 63개가 어느 정도 PGME 프로그램에 참여하고 있었다. 1940년대 말에 이르러서는 GME는 더 공식적으로 구체화되었고 병원 기반 전공의 수련는 전문화의 경로가 되었다[7]. 국립보건원(NIH)의 영향력은 정부 지원 연구비를 통해 의사 과학자들의 초기 발전에 도움을 주었다.
Interestingly, once military physicians were discharged into civilian status, many recognized their limited knowledge so ‘refresher’ courses gained attraction. In a survey sent to a large sample of physicians in the military, nearly 60% (12,534/21,029) wanted to take long refresher courses (6-months or more) and this led to pressure to develop more post graduate medical education (GME) programs. ‘By the academic year 1955–1956, 63 of the 85 approved or developing medical schools were engaged to some degree in post-graduate medical education programs’ [3]. By the end of the 1940s, GME materialized more formally and hospital based residencies became the path to specialization [7]. The influence of the National Institutes of Health (NIH), with its government-funded research grants, aided early development of physician scientists.
연방 법률 변경 및 대체 가속 경로 도입: 1950-1971
Federal legislation changes and introduction of alternative accelerated pathways: 1950–1971
1950년에서 1960년 사이에는 이전 10년에 비해 새로운 3년제 프로그램의 확대나 개발이 거의 없었다. 의사 부족에 대한 우려는 1960년대에 계속되었고, 이러한 우려에 대응하여 보건 전문 학교의 확장을 지원하기 위한 연방 법안이 통과되었다. 1963년에는 [보건전문직 교육 지원 프로그램HPEAP]이 시행되어 보건전문직의 지원을 제공하였다. 이 지원에는 보건 전문학교(알로패스 및 골병리 의학, 치의학, 수의학, 검안법, 약학, 족부학, 공중보건 및 간호학)의 신설construction 지원뿐만 아니라 치과, 알로패스 MD 및 골병리 DO 의학과 학생들에게 대출을 제공했다[8].
Between 1950 and 1960, there was little expansion or development of new 3-year programs compared to the previous decade. Mounting concern regarding physician shortages plagued the 1960s and, in response to these concerns, federal legislation was passed to support expansion of health profession schools. In 1963, the Health Professions Education Assistance Program was implemented to provide support for the health professions. This support included construction aid for health profession schools (allopathic and osteopathic medicine, dentistry, veterinary, optometry, pharmacy, podiatry, public health, and nursing) as well as providing loans to students of dentistry, allopathic MD and osteopathic DO medicine [8].
1965년, 이 법률에 대한 새로운 개정이 이루어졌다. 여기에는 다음이 포함되었다.
New amendments to this legislation were made in 1965, which included
- 기본 및 특별 개선 보조금
- 건설 자금에 대한 새로운 요건(예: 기존의 요구사항보다 더 오랜 기간을 교육용으로 건물을 사용해야 함)
- 학생 장학금 프로그램에 대한 자금 지원 확대 및 최대 대출액 증가(학생당 연간 최대 장학금 2,500달러 및 학생당 연간 최대 2,500달러),
- 대출 탕감 프로그램을 만드는 것.
- basic and special improvement grants,
- new requirements for construction funding (e.g., requiring buildings be used for education for a longer period of time than previously required),
- increasing funding for student scholarship programs and increased maximum loan amount ($2,500 maximum scholarship per student/year and $2,500 maximum annual loan per student), and
- creating loan forgiveness programs.
[기본 보조금]은 학생 1인당 추가 비용 외에 승인된 각 학교에 일시금을 제공하여 보건전문직 학교의 등록enrollment을 확대하는 것을 목표로 했다[9]. [특별 보조금]은 인가를 촉진하고 특별 프로그램을 수립하였다[8,9].
Basic grants aimed to expand enrollment in health professions schools by providing a lump sum to each approved school in addition to extra money per student [9]. Special grants stimulated accreditation and established special programs [8,9].
보건 전문직 교육 지원 프로그램HPEAP은 [국가 보건 서비스단NHSC]과 같은 프로그램에 대한 자금 지원의 인가를 증가시켰는데, 이는 각 학교에게 자금 지원을 받으려면 부속 병원의 1년차 전공의 중 일차의료 수련을 받는 비율을 높일 것을 요구하였다. 1976년 개정된 보건 전문직 교육 지원법은 소외 지역의 보건 전문가를 위한 임상 훈련 프로그램을 제공한 기존 [지역 보건 교육 센터AHEC]의 capacity을 증가시키기 위한 자금 지원을 승인했다[10]. 이러한 보조금은 성공적으로 학생 등록과 졸업을 증가시켰다[8].
The Health Professions Education Assistance Program increased authorization of funding to programs such as the National Health Service Corps, which required schools to ensure that an increasing percentage of first-year residencies in affiliated hospitals were reserved for primary care training in order to receive capitation support. The 1976 version of the Health Professions Education Assistance Act authorized funding to increase the capacity of existing Area Health Education Centers, which provided clinical training programs for health professionals in underserved areas [10]. These grants successfully increased student enrollment and graduation [8].
[의료 종사자 부족에 대한 우려]로 인해, 1966년과 1971년 사이에 연합 건강 직업 인력 훈련법, 1970년 건강 훈련 개선법, 1971년 간호사 훈련법, 1971년 종합 보건 인력 훈련법 등 많은 다른 연방 법률이 통과되었다[8]. 포괄적 의료 인력 훈련법CHMTA은 의료 종사자 교육에 대한 연방 정부의 헌신을 높이고, 가정의학 의사 수련에 긴급성을 더했으며, 의료 전문직 중 소수자 수를 늘리고, 소외 지역의 부족을 완화한 것으로 유명하다. 이 법률은 1970년대에 3년제 의료 프로그램을 확장하는 데 중요한 역할을 했다[8].
Due to the concern about healthcare worker shortages, a flurry of other additional federal legislations were passed between 1965 and 1971, including the Allied Health Professions Personnel Training Act in 1966, Health Training Improvement Act in 1970, Nurse Training Act in 1971, and Comprehensive Health Manpower Training Act in 1971 [8]. The Comprehensive Health Manpower Training Act was notable for elevating federal commitment to training healthcare workers, giving new urgency to training family practitioners, increasing numbers of minorities in health professions, and alleviating shortages in underserved areas. This piece of legislation was crucial to the expansion of 3-year medical programs in the 1970s [8].
특히 1950년대와 1960년대에 MD 학위를 위한 다른 혁신적인 대안 경로가 도입되었다. 이들 프로그램은 의사 양성에 필요한 전체 시간을 단축하기 위해 마련됐으며, 학부 과정 3년과 의대 3년(BA-MD 프로그램)을 결합한 3+3 프로그램이 포함됐다. 1960년대에는 전국적으로 60명의 학생들이 BA-MD 프로그램에 입학했다. 이 숫자는 1976년까지 매년 약 400명으로 증가했다. 1950년대와 1960년대에 개발된 개선된 고등학교 및 학부 과정 덕분에 의대생들은 과거보다 더 높은 수준의 의과대학 과정을 시작할 수 있었고, 이는 2차 세계대전 당시보다 3년제 의과대학 프로그램의 성취가능성achieable을 더 높여주었다. 실제로 1967년까지 의대 지원자의 40% 이상이 생화학을 일부라도 배우고 왔다.
Of note, during the 1950s and 1960s, other innovative alternative pathways to an MD degree were introduced. These programs were designed to shorten the overall time needed to train a physician and included 3 + 3 programs that combined 3 years of undergraduate courses with 3 years of medical school (BA-MD programs). In the 1960s, 60 students were admitted into BA-MD programs nationally. That number grew to around 400 students per year by 1976 [11]. Due to improved high school and undergraduate collegiate programs developed during the 1950s and 1960s, medical students were able to start at a more advanced level than had been possible in the past, which enabled 3-year medical school programs to be more achievable than they had been during the WWII era. Indeed, by 1967 over 40% of medical school applicants had some exposure to biochemistry [12].
BA-MD 프로그램의 학생들은 일반적으로 학업적으로 성공했다. 예를 들어, 보스턴 대학교의 BA-MD 프로그램에 입학한 학생 중 50%는 우등으로 학사 학위를 받았고, 10%는 우등으로 MD 학위를 받았다[13]. 1966년부터 1996년까지 통합 BA-MD 프로그램에서 학생들의 성과 결과 데이터를 검토한 결과, 표준화된 의료 위원회 시험 점수와 임상 성과에 따라 결정되는 역량이 기존의 의대 학생들과 차이가 없었다. 이러한 결과는 학생들이 성공적인 의사가 될 학생을 고등학교에서 바로 선발할 수 있음을 보여주었다[14]. 1960년대는 또한 의과대학 학급 규모가 커지는 추세를 보였다. 예를 들어, 1960년과 1970년 사이에 미네소타 의과대학은 신입생 반을 164명에서 227명으로 늘렸다[15명].
Students in BA-MD programs generally succeeded academically. For example, 50% of students who entered Boston University’s BA-MD program received their BA degree with honors and ≥10% received their MD degree with honors [13]. A review of performance outcome data of students in combined BA-MD programs from 1966 to 1996 showed no difference in competency from traditional medical school students as determined by scores on standardized medical board exams and clinical performance. These results demonstrated that students could be selected from high school to become successful physicians [14]. The 1960s also saw a trend toward larger medical school class sizes. For example, between 1960 and 1970, the University of Minnesota Medical School increased its freshman class from 164 to 227 students [15].
3년제 가속 의과대학 프로그램의 급증: 1970년대와 1980년대
A spike in the number of 3-year accelerated medical school programs: 1970s–1980s
베트남 전쟁 (1955~1975) 기간 동안 의사 부족 문제를 해결하는 것 외에도, 1970년대는 3년 과정의 급속한 개발로 이어진 추가적인 요소가 있었다: 바로 학생 부채를 줄이는 것이다. 이러한 목적은 성공하였으며, 1970년대에 돈을 벌기 위해 일하는 의대생들이 줄어든 것에서 드러난다. 1963년에는 의대 4학년의 45%가 주당 평균 16시간을 일했고, 1971년에는 더 적은 수의 4학년(34%)이 주당 평균 14시간을 일했으며, 1974년에는 4학년 중 26%만이 주당 평균 10시간을 일했다. [16] [학생 부채 감소, 의사 부족 문제 해결, 정부 재정적 인센티브에 관한 국가적 논의]는 1970년부터 1973년까지 3년제 프로그램에 등록하는 학생 수 증가에 주된 기여요인으로 보고되었다. 실제로, 이 기간 동안 3년제 가속 의학 프로그램에 등록하는 학생은 1970-1971학년의 671명에서 1973-1974년 2,597명으로 387% 증가했다. 3년제 의료진 등록이 가장 크게 증가한 것은 1971년 종합보건인력양성법CHMTA의 시행 이후였으며, 1972-1973년에 1080명이던 의과대학 입학이 다음 해에는 2,273명으로 증가했다. 1971년 포괄적 보건 인력 훈련법에 따라 연방 역량 기금은 3년 내에 졸업하는 학생 1인당 2,000달러의 보너스를 제공했다[19]. 이러한 상황 속에, 1973년에 이르자 모든 미국 의과대학의 약 1/3(n = 33)이 졸업에 3년짜리 MD 경로를 제공했다[9,20].
In addition to addressing physician shortages during the Vietnam War era (1955–1975), much like during WWII, the 1970s had an additional factor that led to the rapid development of 3-year programs: the desire to reduce student debt. A successful push to reduce student debt may be revealed in decreased numbers of medical students working for pay in the 1970s. ‘In 1963, 45% of medical school seniors worked an average of 16 hours a week; in 1971, fewer (34%) of seniors worked an average of 14 hours a week; and, by 1974, only 26% of seniors worked an average of 10 hours per week’ [16]. National discussion regarding reducing student debt, the need to address physician shortages, and government financial incentives were reported as major contributors to increased enrollment in 3-year programs from 1970 to 1973 [17]. Indeed, during this time, enrollment in 3-year accelerated MD programs increased 387%, from 671 students in the 1970–1971 academic year to 2,597 in 1973–1974 [8] (out of a total of 15,000 medical graduates per year [18]). The greatest increase in 3-year MD enrollment was seen after implementation of the 1971 Comprehensive Health Manpower Training Act, with first year medical school enrollment increasing from 1,080 in 1972–1973 to 2,273 during the subsequent academic year [8]. Under the Comprehensive Health Manpower Training Act of 1971, federal capitation funding provided a bonus of $2000 per student graduating in 3 years [19]. Given this context, by 1973 approximately one-third (n = 33) of all US medical schools offered a 3-year MD path to graduation [9,20].
1970년대 가속 의료 프로그램 개발에 대한 긍정적인 태도와 관심은 3년 프로그램을 포함한 전반적인 의과 대학 등록의 증가로 이어졌고, 다른 가속 경로를 제공하는 다수의 학교가 확장되었다. 가속화된 프로그램의 확장을 촉진하는 학생들에게도 장점이 있었다. 이에 유의해야 할 점은 1970년부터 1975년까지 의과대학 입학 경쟁률이 높아졌다는 사실이다,
- 1970년에는 11,350명 모집에 25,000명이 지원했다
- 1975년에는 15,000명 모집에 43,000명이 지원했으며, 이로 인해 대학 입학률은 45%에서 35%로 떨어졌다[11].
Positive attitudes and interest in developing accelerated medical programs during the 1970s resulted in increased overall medical school enrollment, including 3-year programs, and expansion in a number of schools offering other accelerated pathways. There were advantages for students that facilitated expansion of accelerated programs as well. In this regard, it should be noted that rising competition for admission into medical school occurred from 1970 to 1975;
- in 1970, there were 25,000 applications for 11,350 openings.
- By 1975, there were 43,000 applications for 15,000 places, which caused the percent of matriculates to fall from 45% to 35% (1970 to 1975, respectively) [11].
학생들은 가속화된 MD 프로그램에 대한 조기 입학이 광범위한 일반 입학 풀 내에서 경쟁을 피하기 위한 방법일 수 있다고 판단했을 수 있다[11]. 우수한 지원자들이 새로운 3년제 MD 프로그램에 지원하였고, 이러한 학생들은 전체 기관의 명성에 중요한 요소인, [peers와 비교한 입학 지표와 성과를 향상]시켰기 때문에 의과대학에도 도움이 되었다[11]. 흥미롭게도 3년제 MD 프로그램에 대한 교수진의 태도는 전문 분야에 따라 다양했습니다. 오하이오 주립 의과대학이 1970년에 4년제 프로그램에서 3년제 MD 프로그램으로 전환했을 때, 교수 태도에 대한 연구는 가정의학과 예방의학과 교수진이 3년제 MD 프로그램에 대해 가장 긍정적인 것으로 결정했다[20].
Students may have reasoned that early admission to accelerated MD programs might be a way of avoiding increasing competition within the broader general admission pool [11]. This was also beneficial for medical schools since outstanding candidates were attracted into new 3-year MD programs, and these students in turn boosted admission metrics and performance of their peers, an important component of overall institutional prestige [11]. Faculty attitudes toward 3-year MD programs varied, interestingly, by specialty. When Ohio State University School of Medicine transitioned from a 4-year program to a 3-year MD program in 1970, a study of faculty attitudes determined that family medicine and preventive medicine faculty were most positive toward 3-year MD programs [20].
3년 가속 MD 프로그램 중단: 1970년대 후반-80년대
Discontinuation of 3-year accelerated MD programs: late 1970s–1980s
1970년대에 도입되어 개발된 3년제 가속 의과대학 프로그램 중 다수는 그렇게 오래 유지되지 못했다. 학업 스트레스가 높았고 가속 MD 프로그램을 수강하는 학생의 약 25%가 자발적으로 교육을 1~2년 연장했다[9]. 또한, 학생과 교직원은 자료의 압축에 대한 압박을 언급했다. 프로그램을 마친 학생들은 '지쳤다'고 말했으며, 교직원들은 끊임없이 확장되는 의학 지식을 더 짧은 기간 안에 가르쳐야 한다는 것에 불만을 느꼈다[9]. 그 밖에 3년제 교육과정에선 가정의학과 농촌의학과 노인학 순환학 등의 과소대표underrepresentation, 심화윤리 및 약물남용 교육 부족 등이 지적됐다. 또한 최종적으로 레지던트 추천서를 준비할 교수진에게 제한적으로 노출되었고, 학생들이 레지던트 프로그램을 인터뷰할 시간이 거의 없었으며, 방학 시간도 최소화되었다[17]. 아마도 가장 중요한 것은 가속화된 MD 프로그램이 순 의사 양성net physician output을 증가시키지 않았다는 것이다. 이는 3년제 프로그램을 시작하는 주요 목표 중 하나였다[9]. 학급 규모의 증가 없이, 3년제 의료 프로그램은 3년제 첫 번째 학급이 4년제 학생들과 함께 졸업할 때 의사들의 무리를 만들었다. 그 후, 졸업하는 학생들의 순수는 더 이상 증가하지 않고 평형 상태로 유지되었다.
Many of the 3-year accelerated medical school programs introduced and developed in the 1970s did not stay open long-term. Academic stress was high and about 25% of students in accelerated MD programs voluntarily extended their education by 1 or 2 years [9]. Additionally, students and faculty cited feeling pressured by compression of the material; students completing programs stated that they felt ‘exhausted,’ and faculty felt dissatisfied with trying to teach ever-expanding medical knowledge into a shortened timeframe [9]. Other issues cited with 3-year curricula included under-representation of family medicine, rural medicine, and gerontology rotations, as well as lack of in-depth ethics and substance abuse training. In addition, there was limited exposure to faculty members who would ultimately prepare residency recommendation letters, little time for students to interview with residency programs, and minimal vacation time [17]. Perhaps most importantly, accelerated MD programs did not increase net physician output, which was one of the main goals of starting such programs [9]. Without an increase in class size, 3-year medical programs created a bolus of physicians when the first class of 3-year students graduated along with fourth year students. Thereafter, the net number of students graduating remained stable (reached steady state), without further increase.
주의할 점은 3년제 MD 교육과정의 페다고지는 distinct하며, 따라서 단순한 4년제 교육과정의 압축을 넘어서야 한다는 것이다. 이것은 때때로 1970년대에 어렵게 배워졌다. 예를 들어, 애리조나 대학교는 1972년에 4년제에서 3년제 MD 프로그램으로 전환되었다가 1977년에 다시 4년제 프로그램으로 전환되었다. 애리조나는 처음에는 72주의 기초과학(임상 전) 자료를 56주로 압축한 뒤 2교시 및 3년 MD 커리큘럼에서 64주로 늘렸다. 애리조나 의대생들은 필요하다면 4년 또는 그 이상으로 그들의 교육을 연장할 수 있는 선택권이 있었다. 애리조나에서 처음 3개 반의 학생 중 1/3은 재학기간을 3년 이상으로 연장했으며, 이 옵션을 선택한 학생은 [의학 전공분야를 탐구]하는 데 더 많은 시간을 선택하는 대신, 대부분의 추가 시간을 [기초 과학 학습 속도를 늦추는 데] 사용했다[17]. 안타깝게도 원래 예정된 3년 기간에 끝마치지 못한 학생들은 종종 '약하거나 부족하다'는 오명을 쓰게 되었고, 그렇게 교수들에게 인식되었다[9,18].
It is important to note that pedagogy for a 3-year MD curriculum is distinct and therefore should go beyond compression of a school’s 4-year curriculum. This was sometimes learned the hard way in the 1970s. As an example, the University of Arizona went from a 4-year to a 3-year MD program in 1972, and then converted back to a 4-year program in 1977. Arizona had compressed 72 weeks of basic science (pre-clinical) material into 56 weeks initially, and then increased it to 64 weeks in the second class and subsequent classes in their 3-year MD curricula. Medical students at Arizona had the option to extend their schooling to four or more years if needed. One-third of students in the first three classes at Arizona extended their time beyond 3 years, and students who took this option used the majority of additional time to slow down the pace of basic science learning rather than choosing more time to explore medical specialties [17]. Unfortunately, students who extended their time beyond the originally committed 3 years were often stigmatized and perceived by faculty as ‘weak or deficient’ [9,18].
다른 학교들도 MD 커리큘럼이 압축된 것에 부담을 느꼈다. 오하이오 주립 대학교에서는 3년제 교육과정에 참여하는 교수진의 평균 만족도 점수가 100점 만점에 60.5점(34~93점)이었으며, 교수진의 50%가 4년제 MD 프로그램으로 복귀하는 것을 선호했다[20점]. USMLE 점수와 레지던트 일치 결과에 따르면 3년제와 4년제 학생들 간의 성과에 큰 차이가 없다는 연구 결과가 나왔지만, 1970년대 말까지 대부분의 3년제 MD 프로그램은 4년제 커리큘럼을 선호하여 중단되었다. 실제로 1973-1974 학년 이후, 이러한 프로그램에 대한 등록이 지속적으로 감소하였고, 1974-1975년에는 2,434명이던 3년제 MD 학생이 1978-1979년에는 1,455명으로 감소했다[23]. 3년 MD 프로그램을 종료하게 된 전반적인 이유에는 [재정적 인센티브를 제거한 연방 기금 중단, 의사 부족의 감소, 가속화된 기간에 대한 전반적인 불만족] 등이 포함되었다[22].
Other schools felt pressure from their compressed MD curriculum as well. At Ohio State, the mean satisfaction score of faculty participating in the 3-year curriculum was 60.5 out of 100 (range of 34–93), with 50% of faculty favored returning to a 4-year MD program [20]. Although studies showed no major difference in performance between 3-year and 4-year students, as measured by USMLE scores and residency match results, by the end of the 1970s most 3-year MD programs were discontinued in favor of 4-year curricula [13,17,21,22]. Indeed, after the 1973–1974 academic year, a persistent decline in enrollment in these programs occurred, with 2,434 3-year MD students in 1974–1975 declining to 1,455 in 1978–1979 [23]. Overall reasons given for ending 3-year MD programs included discontinuation of federal funding that eliminated financial incentives, declining physician shortages, and overall dissatisfaction with the accelerated time frame [22].
3 + 3 MD 잔류 프로그램의 성장과 함께 의사 훈련 기간 해결: 1980년대-2000년대
Addressing the length of physician training with growth of 3 + 3 MD-residency programs: 1980s–2000s
1970년대 말까지 대부분의 3년 MD 프로그램이 해체되었지만, 이후 수십 년 동안 MD-전공의 통합 프로그램은 의사의 전반적인 훈련 기간을 줄이기 위한 시도로 이루어졌다. 1975년부터 2000년까지 미국 전공의의 수는 37,140명에서 98,806명으로 두 배 이상 증가했다. 4년제 커리큘럼이 있는 일부 의과대학은 학생들이 로테이션 인턴십을 이수하면 4학년을 대체한 것으로 갈음하는 것waive the fourth year을 허용하기 시작했다[17]. 1980년대와 1990년대에 25개의 미국 의과대학은 내과 3 + 3에 있는 여러 프로그램 외에도 가정의학과 3 + 3 (MD 잔류) 프로그램을 가지고 있었다[21]. 흥미로운 점은 가정의학과 3+3 졸업생이 기존(4+3) 졸업자보다 치프 레지던트로 선택될 확률이 높았다. 그러나 이러한 3+3 프로그램 대부분은 주로 GME 인증 문제로 인해 종료되었다[22].
Although there was dissolution of most 3-year MD programs by the end of the 1970s, over the next few decades, growth occurred in combined MD-residency programs in an attempt to reduce the overall length of training of a physician. From 1975 to 2000, the number of residents in the United States had more than doubled, from 37,140 to 98,806 [18]. Some medical schools with 4-year curricula began allowing students to waive the fourth year if they completed a rotating internship [17]. In the 1980s and 1990s, 25 US medical schools had family medicine 3 + 3 (MD-residency) programs in addition to several in internal medicine 3 + 3 [21]. Interestingly, family medicine 3 + 3 graduates were more likely to be chosen as chief residents than traditional (4 + 3) graduates. Most of these 3 + 3 programs ended, however, primarily due to GME accreditation issues [22].
3년제 가속 의대 프로그램 현황: 2010-2017
Current state of 3-year accelerated medical school programs: 2010–2017
세기의 전환과 함께 의과대학 교과과정에서는 거대한 개혁이 일어났다. 2005년 이후 미국 의과대학의 75%가 능동적 학습과 임상 및 생물의학 과학의 통합 강화를 포함한 혁신적인 교육학을 시작했다[2]. 이는 21세기에 의사가 성공하기 위해서는 성인 학습을 최적화하고 업데이트된 의료 지식을 통합하는 개정된 커리큘럼이 필요하다는 일반적인 인식을 보여준다. 교육 개혁의 일환으로 2010년 이후, 3년제 MD 프로그램이 9개의 allopathic 의과대학에서 다시 등장했으며, 이들 학교의 80%는 3년제 학생들의 1차 진료에 초점을 맞추고 있다[21]. 레지던트 면접을 위해 여행하는 데 사용할 수 있는 3년 MD 커리큘럼의 제한된 시간을 고려할 때, 거의 모든 프로그램은 학생들에게 보장된 지역 레지던트 자리를 제공한다[21,24,25].
With the turn of the century, vast reforms have occurred in medical school curricula. Since 2005, 75% of US medical schools have initiated innovative pedagogy, including active learning and enhanced integration of clinical and biomedical sciences [2]. This shows general recognition that revised curricula that optimize adult learning and incorporate updated medical knowledge are needed for physicians to succeed in the twenty-first century. As part of curricular reform, since 2010, 3-year MD programs have re-emerged in nine allopathic medical schools, with 80% of these schools focusing on primary care for their 3-year students [21]. Given the limited time available in 3-year MD curricula to travel for residency interviews, almost all of these programs offer their students guaranteed local residency positions [21,24,25].
과거 추세에 대한 요약
Summary of historical trends
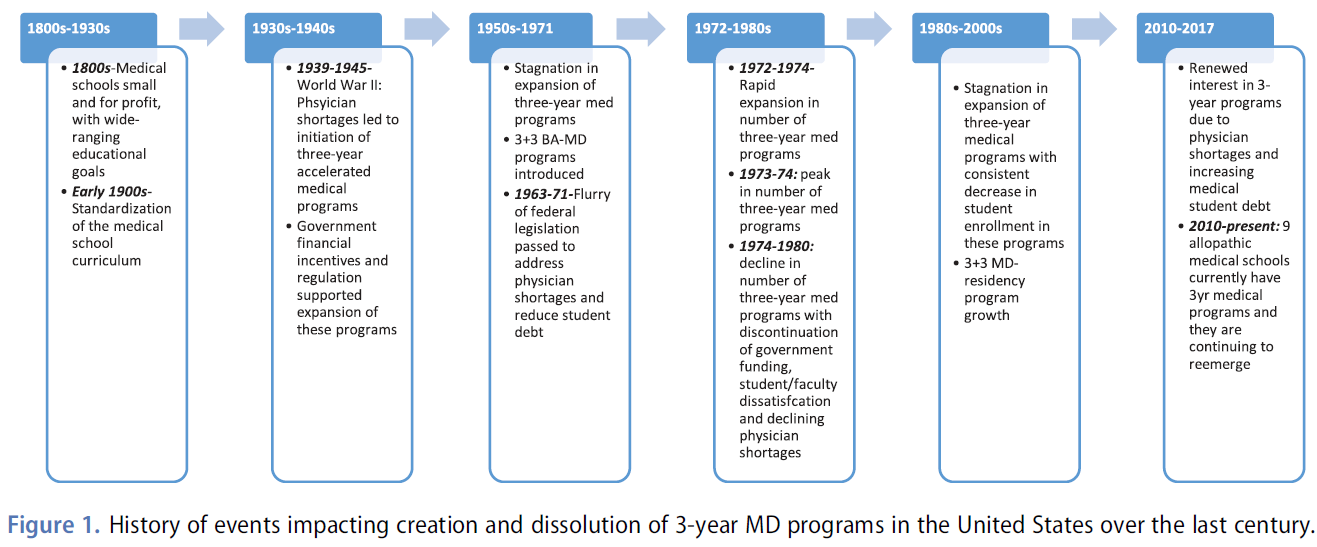
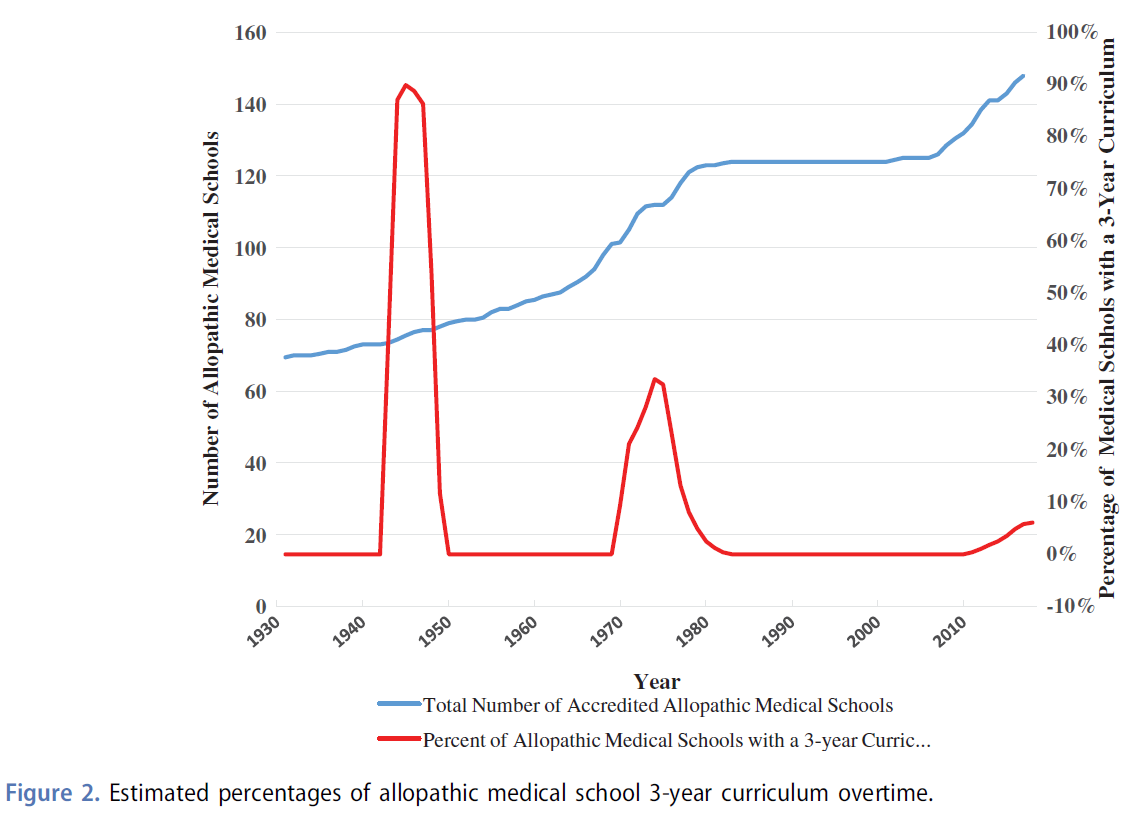
그림 1은 지난 세기 동안 미국에서 3년 MD 프로그램의 생성 및 해체에 영향을 미친 역사적 사건을 요약한 것입니다. 그림 2는 1930년부터 2017년까지의 총 의대생의 증가를 3년 커리큘럼으로 인가된 알로패스 의대 비율과 병치하여 보여준다[9,12,20,22–38]. 그림 2에서 볼 수 있듯이, 3년제 의과대학 중 가장 많은 비율이 2차 세계대전(90%)에 발생했고, 그 다음이 1970년대(40%)였다. 가장 최근에 3년제 교육과정을 갖춘 의과대학이 부활한 것은 1940년대와 1970년대에 급증했던 것에 비하면 훨씬 덜 두드러진다.
Figure 1 summarizes historical events impacting creation and dissolution of 3-year MD programs in the United States over the last century. Figure 2 documents the rise in total medical students from 1930 to 2017 juxtaposed against percentages of accredited allopathic medical schools with 3-year curriculum over the same period [9,12,20,22–38]. As can be seen in Figure 2, the greatest percentage of medical schools with a 3-year program occurred in the WWII era (≈90%) followed by the 1970s (≈40%). The most recent resurgence of medical schools with 3-year curricula is far less pronounced compared to spikes in the 1940s and 1970s.
시간에 따른 새로운 테마
Emerging themes across time
가속 3년 의료 교육을 검토할 때 지난 세기에 걸쳐 두 가지 주요 주제(학습 교훈)가 나타난다.
- 첫 번째 주제는 3년제 의료 교육의 재정적 이익(예: 학생 부채 감소 및 의료 교육비 절감)이 현실에서 원래 생각했던 것만큼 간단하지 않고 기관의 더 넓은 맥락에 의존한다는 것이다.
- 두 번째(교육학적) 주제는 4년제 의료 교육에 대한 접근법과 구별되는 3년제 의료 교육을 위한 새롭고, 통합적이며, 능률적인 커리큘럼 개발의 중요성이다.
Two major themes (learning lessons) emerge across the last century when examining accelerated 3-year medical education.
- The first theme is that financial benefit of 3-year medical education (e.g., decreased student debt and lower medical education costs) is an ideal that is not as straightforward in reality as originally conceived and depends on broader context of institutions.
- A second (pedagogical) theme is the importance of developing new, integrated, and streamlined curricula for 3-year medical education, distinct from the approach to 4-year medical education.
가속/3년제 의과대학의 재정적 이점 및 비용
Financial advantages and costs of accelerated/3-year medical schools
의대생 부채(학부와 의전원을 합친 것)는 여전히 미국에서 중요한 문제로 남아 있다. 1990년부터 2003년까지 의과대학 학비와 등록금은 83%에서 167%까지 인상되었다[35]. 다만 상황이 복잡하기 때문에 3년제 MD프로그램이 단순히 1년치 등록금만 없앤다고 해서 의대 부채를 줄인다고 보는 것은 잘못됐다는 점에 유의해야 한다. 실제로 일부 3년제 의과대학은 4년제 학교와 동일한 등록금을 부과하고 있다[28,36]. 이는 현재 미국 LCME가 MD 학위를 취득하기 위해서는 130주가 필요하기 때문인데, 이는 여름 동안 수업을 추가하고 방학 및 레지던트 면접 시간을 모두 줄임으로써 3년 프로그램에서 달성된다[22,37]. 제도적 관점에서, 그러한 구조조정은 종종 새로운 교사와 다른 비용을 필요로 한다. 그러나 현재 많은 3년제 프로그램이 레지던트 자리를 보장하기 때문에 일부 혜택이 생깁니다. 이를 통해 학생들은 4학년 때 들어가는 면접 비용을 $1000–$5,000 절감할 수 있습니다[39].
Medical student debt (combined undergraduate and medical school) remains an important problem in the United States. From 1990 to 2003, medical school tuition and fees grew between 83% and 167% [35]. It should be noted, however, that it is erroneous to assume that 3-year MD programs decrease medical school debt by simply eliminating 1 year of tuition since the situation is more complex. In fact, some 3-year medical schools charge the same tuition as 4-year schools [28,36]. This is because currently the US LCME requires 130 weeks for a MD degree, which is achieved in 3-year programs by adding classes during summers and by decreasing both vacation time and residency interview time [22,37]. From an institutional perspective, such restructuring often requires a new set of teachers and other expenses. Some benefits do accrue, however, since many current 3-year programs today guarantee residency positions; this can lead to immediate $1000–$5000 savings to students in eliminating senior year interview expense [39].
3년제 MD 프로그램 수료자는 기존 의대생에 비해 1년 일찍 취업해 경제적 혜택을 받는다. 이 추가 연도는 추가적인 1년의 실습과 그에 따른 임상 수입을 허용하여 학자금 대출 상환을 용이하게 할 수 있다. 오늘날 노동력에서 얻은 1년의 재정적 혜택은 일반 내과 전문의의 경우 16만 달러, 내과 하위 전문의의 경우 23만 달러인 것으로 보고되었다[35]. 이런 현실은 의학교육의 큰 경제적 부담을 줄이는 가장 효과적인 재정수단이 의학교육비 자체를 줄이는 데 있지 않고, 인력진입을 앞당겨 대출금을 더 빨리 갚을 수 있도록 하는 데 있을 수 있다는 지적이다. 가속도가 학부, 의과대학, 레지던트 단계에서 일어나든 마찬가지일 것이다.
Graduates of 3-year MD programs do acquire financial benefit by entering the workforce 1 year early compared to traditional medical students. This extra year allows an additional year of practice and resultant clinical income that could facilitate repayment of student loans. Financial benefit of 1 year gained in the workforce today has been reported to be $160,000 for general internists and $230,000 for internal medicine subspecialists [35]. This reality points out that the most effective financial means for decreasing the large financial burden of medical education may not lie in reducing the price of medical education per se, but rather by allowing earlier entry into the workforce so loans can be paid back sooner. This would be true whether acceleration occurs at the undergraduate, medical school, or residency level.
독특한 교육학으로서의 3년제 의과대학
3-year medical school as a distinct pedagogy
이렇게 많은 세부 자료를 강의/학습하기가 어렵기 때문에, 표준 4년제 교육과정을 3년으로 압축하면서 교직원과 학생 불만이 크게 발생하는 것도 시간이 흐르면서 나타나는 주제다. 이는 가속화된 의학교육 프로그램의 성공을 달성하기 위해 새롭고 능률적이며 통합된 커리큘럼을 만드는 것이 중요함을 시사한다. 현재 미국의 의학 교육 커리큘럼 개혁 노력과 성인 학습에 대한 효과적인 접근법에 대한 새로운 이해를 고려할 때, 이와 관련하여 선제적 개입이 처음으로 가능하다. 이것은 3년 MD 프로그램으로의 전환을 고려하는 리더들에게 중요한 교육학 수업이자 (필요한 투자로 인한) 현실 점검이다.
Another theme present over time is that strong faculty and student dissatisfaction occurs with compression of a standard 4-year curriculum into 3 years since it is difficult to teach/learn such a large body of detailed material. This suggests that creating new, streamlined, and integrated curricula will be important for achieving success in accelerated medical education programs. Given current medical education curriculum reform efforts in the United States, and new understanding of effective approaches to adult learning, for the first time proactive intervention is possible in this regard. This is an important pedagogy lesson, and reality check (due to investments required), for leaders considering moving toward 3-year MD programs.
하나의 미래관
One view of the future
앞으로 가속화된 3년 MD 프로그램의 주요(실현되지 않은) 이점은 학생마다 개별화된 훈련을 제공할 기회를 제공함으로써 현재 4년 커리큘럼 내에서 유연성을 제공하는 데 있을 수 있다. 모든 형태의 교육을 뒷받침하는 기술의 폭발로 인해, 동기식 및 비동기식 학습이 가능해졌으며, 이것은 이러한 프로그램에서 학생과 교수진 모두에게 향상된 만족과 유연성을 가져올 수 있다. 실제로, 3년에 걸쳐 기초 과학 및 임상 훈련을 이수하면 학생들은 더 오래된 (2 + 2) 4년 커리큘럼 내에서 불가능했던 연구, 이중 학위, 리더십 훈련 및 팀 기반 종적 경험과 같은 학술 의료 센터에서 이용할 수 있는 다른 풍부한 기회를 활용할 수 있다. 임상의학에만 집중하는 것을 선호하는 학생들에게는 1년 일찍 취업할 수 있다는 것이 대출 상환에 도움이 되고 따라서 중요한 경제적 이익을 얻을 수 있기 때문에 잠재적인 장점이다.
Moving forward, a major (unrealized) advantage of accelerated 3-year MD programs may be in providing flexibility within current 4-year curricula by offering an opportunity to individualize training for a given student. With an explosion of technology undergirding all forms of education, synchronous and non-synchronous learning is now possible and this may result in enhanced satisfaction and flexibility for both students and faculty in these programs. Indeed, completing basic science and clinical training over 3 years may enable students to take advantage of other rich opportunities available in academic medical centers such as research, dual degrees, leadership training, and longitudinal team-based experiences otherwise not possible within older, more traditional (2 + 2) 4-year curricula. For students who prefer to focus solely on clinical medicine, ability to enter the work force 1 year early is a potential advantage since it helps with loan repayment and therefore can have important financial benefit.
의료 교육을 개별화할 때의 단점(예: 주어진 의과대학 내에서 두 개의 병렬 3년 및 4년 MD 커리큘럼이 나란히 있는 경우)은 주로 추가 비용에 따라 발생한다. 이는 특히 소규모 그룹 학습에 이미 훨씬 더 많은 교수진의 참여가 필요한 시대에 순추가 등록금 없이 필요한 교수 자원이 증가했기 때문이다. 과거에 이러한 경로를 시행했을 때처럼 정부 보조금이 없다면, 이러한 미래관은 오늘날 재정적으로 점점 더 제한된 환경에서 지속되기 어려울 수 있다. 하지만, 교육학적인 관점에서, 진정으로 개인화된 교육을 상상하는 것은 매력적입니다.
Disadvantages in individualizing medical education (e.g., having two parallel 3-year and 4-year MD curricula in tandem within a given medical school), revolves predominantly around added cost. This is due to increased faculty resources needed without net added tuition, particularly in an era where modern innovations in medical school curricula already require significantly more faculty involvement for small group learning. In the absence of government subsidies, as occurred in the past when this pathway was implemented, such a view of the future may be difficult to sustain in today’s increasingly fiscally limited environment. However, from a pedagogical perspective, it is enticing to envision truly individualized education.
결론
Conclusion
미국의 의학 교육 역사를 통틀어 3년제 MD 프로그램(제2차 세계 대전, 1970년대, 현재)의 시행과 관심의 물결이 세 차례 있었다. 성장기마다 나타나는 공통적인 요인에는 [의사 부족 문제를 해결]에 대한 우려가 포함된다. 역사적으로, 의사 부족을 진정으로 해결하기 위해서는, 3년제 또는 4년제 의과대학의 [학년 당 학급 규모를 늘려야 한다]는 사실이 재발하고 있다. 가속화된 MD 커리큘럼의 성장에 박차를 가하는 다른 영향으로는 정부 자금과 1970년대 이후 의료 교육 비용 절감에 대한 관심이 있다. 위에서 언급한 바와 같이, 가속화된 의료 프로그램의 재정적 인센티브는 주로 학생들이 1년 일찍 직장에 들어갈 수 있는 능력에 있으며, 이는 여러 다른 교육 시점을 단축함으로써 효과적으로 달성될 수 있다. 3년 MD 프로그램 중단의 이유는 [의사 부족에 대한 우려가 감소하게 되면] 외부(정부/주) 자금 지원이 줄어드는 것과 가속화된 프로그램에 참여하는 [의대생과 교수진이 표출한 불만]이었다. 이러한 우려에도 불구하고 3년제 MD교육 수료생은 4년제 졸업생과 동등한 국가고시 성적을 거두고 있다.
Throughout the history of medical education in the United States, there have been three waves of interest and implementation of 3-year MD programs (WWII era, 1970s, and current). Common factors driving every period of growth include concern over addressing physician shortages. Historically, a reoccurring finding is that to truly address physician shortages, increasing class size of 3-year or 4-year medical school is needed. Other influences spurring growth of accelerated MD curricula have been governmental funding and, since the 1970s, an interest in reducing the cost of medical education. As stated above, financial incentive from accelerated medical programs lies predominantly in the ability of students to enter the workforce 1 year early, which can be effectively achieved by shortening several different educational time points. Reasons given for discontinuation of 3-year MD programs were elimination of external (government/state) funding, which waned in periods of declining concern over physician shortages, and dissatisfaction expressed by medical students and faculty participating in accelerated programs. In spite of these concerns, 3-year MD education graduates perform comparably with 4-year graduates on national examination scores.
강의에 사용되는 기술의 확장과 의과대학 수준의 수업들이 점차적으로 대학 학부 과정으로 이전되는 것을 고려하면, 과거에 비해 짧은 기간의 의사 양성이 오늘날 더 실현 가능할지도 모른다. 연구 등 대안적인 과정을 이수하고 싶은 학생들에게는 3년제 MD 프로그램이 기존 4년제 커리큘럼에서는 접할 수 없는 개별화를 위한 틀도 제공할 수 있다. 하지만, 지난 날을 살펴보면 이 또한 주의를 필요로 한다. 3년제 교육과정의 표준화가 어렵고 장기적인 지속 가능한 모델을 추구한다면 이러한 교육학을 조직하는 데 집중된 시간과 노력이 할당되어야 한다. 과거 3년 MD 프로그램에서 접한 맥락과 이슈를 검토함으로써 앞으로 새로운 프로그램이 가장 사려 깊고 성공적으로 설계될 수 있기를 바라는 것이 저자의 바람이다.
Given expansion of technology used in teaching, and gradual transfer of medical school level classes to university undergraduate coursework, training physicians in a shortened duration may be more feasible nowadays compared to the past. For students who would like to complete alternative coursework such as research, 3-year MD programs can also provide a framework for individualization not accessible in traditional 4-year curricula. However, history also suggests caution. Standardizing 3-year curriculum is difficult and focused time and effort must be allotted to organizing such pedagogy if a long-term sustainable model is sought. By reviewing the context and issues encountered with 3-year MD programs in the past, it is the author’s hope that new programs can be designed in the most thoughtful and successful manner possible going forward.
doi: 10.1080/10872981.2018.1530557.
Comprehensive history of 3-year and accelerated US medical school programs: a century in review
PMID: 30376794
PMCID: PMC6211283
DOI: 10.1080/10872981.2018.1530557
Abstract
Within the context of major medical education curricular reform ongoing in the United States, a subset of schools has re-initiated accelerated (3-year) medical education. It would be helpful for education leaders to pause and consider historical reasons such accelerated medical schools were started, and then abandoned, over the last century to proactively address important issues. As no comprehensive historical review of 3-year medical education exists, we examined all articles published on this topic since 1900. In general, US medical educational curricula began standardizing into 4-year programs in the early 1900s through contributions from William Osler, Abraham Flexner, and establishment of the American Medical Association (AMA) Council of Medical Education (CME). During WWII (1939-1945), accelerated 3-year medical school programs were initiated as a novel approach to address physician shortages; government incentives were used to boost the number of 3-year medical schools along with changed laws aiding licensure for graduates. However, this quick solution generated questions regarding physician competency, resulting in rallying cries for oversight of 3-year programs. Expansion of 3-year MD programs slowed from 1950s to 1960s until federal legislation was passed between the 1960s and the 1970s to support training healthcare workers. With renewed government financial incentives and stated desire to increase physician numbers and reduce student debt, a second rapid expansion of 3-year medical programs occurred in the 1970s. Later that decade, a second decline occurred in these programs, reportedly due to discontinuation of government funding, declining physician shortage, and dissatisfaction expressed by students and faculty. The current wave of 3-year MD programs, beginning in 2010, represents a 'third wave' for these programs. In this article, we identify common societal and pedagogical themes from historical experiences with accelerated medical education. These findings should provide today's medical education leaders a historical context from which to design and optimize accelerated medical education curricula.
Keywords: 3-year medical school; Review; US; accelerated; curriculum.
'Articles (Medical Education) > 인문사회의학(의사학, 의철학 등)' 카테고리의 다른 글
| 의학교육에서 우리의 인종적 과거를 다루기: 푸코적 관점(Teach Learn Med. 2021) (0) | 2023.08.09 |
|---|---|
| 물고기의 힘: 비판적 사고, 인문학적 사고, 다른 방식의 앎(Acad Med, 2022) (0) | 2022.08.14 |
| When I say . . . 젠더 (Med Educ, 2019) (1) | 2021.07.31 |
| 의료의 휴머니즘: 무엇을 의미하며, 왜 어느 때보다 중요한가? (Acad Med, 2019) (0) | 2021.05.15 |
| [AAMC] 의료인문학 교육활동 (Getting Started Guide Part 2) (0) | 2020.12.10 |